Submitted:
11 September 2024
Posted:
12 September 2024
You are already at the latest version
Abstract
Background: We explored the potential value of serum MUC5AC (sMUC5AC) as a biomarker to guide perioperative management of early-stage pancreatic ductal adenocarcinoma (PDA) patients receiving neoadjuvant therapy (NAT). Methods: We performed enzyme-linked immunoassays using a human MUC5AC kit (NBP2-76703) in serum samples obtained from The Ohio State University biorepository (between January 2010 and June 2021). Univariate (UV) and multivariate (MV) Cox regression models were used to quantify progression-free survival (PFS); clinical and pathological variables were adjusted in the MV models. UV logistic regression analysis was utilized to examine the association of sMUC5AC with pathological features and survival. 2 Results: Overall, 23 samples (19 FOLFIRINOX, 3 gemcitabine/nab-paclitaxel, 1 FOLFOX) were available for analysis. The median age was 66 years, and 52% were females. sMUC5AC was associated with a) treatment response, margin status, and residual disease (R0 vs. R1/R2) (all P<0.05); b) PFS on both UV (hazard ratio (HR) of 1.4, 95% confidence interval (CI) of 1.07 to 1.82, P=0.01) and MV (HR of 49.2, 95% CI, 4.4 to 1008.3, P=0.002) analyses; and c) PFS in pre-surgery models along with carbohydrate antigen 19-9 (CA19-9) measured on the same day alone (HR of 1.47, 95% CI, 1.06 to 1.93, p=0.04), with CA19-9 on the same day, and NAT regimen (HR of 1.44, 95% CI, 1.12 to 1.93, p=0.01), and with CA19-9 on the same day, NAT regimen, and CA19-9 at diagnosis (HR of 1.52, 95% CI, 1.1 to 2.09, p=0.007). Conclusion: sMUC5AC shows promise to helping to predict outcomes in our preliminary study. Larger prospective studies should validate these findings.
Keywords:
Pancreatic cancer
; MUC5AC
; biomarker
; predicting
; pancreatic ductal adenocarcinoma
; neoadjuvant therapy
; treatment response
; FOLFIRINOX
1. Introduction
Pancreatic ductal adenocarcinoma (PDA) is known for its high mortality rate, even when diagnosed in nonmetastatic stages [1]. The results of the traditional treatment approach – upfront surgery followed by adjuvant therapy (AT) to early-stage tumors (resectable and borderline resectable) – has been disappointing with high recurrence and low survival rates [2,3,4,5,6,7,8,9,10,11]. Multiple institutes now prefer neoadjuvant therapy (NAT) in this population. Recently published trials (NORPACT-1, SWOG 1505, ESPAC-5, CONKO-007, A021501, PREOPANC-1/2) could not definitively address most of the burning questions, including the optimal treatment regimen, the role of radiation, and the duration of perioperative therapy [12,13,14,15,16,17,18]. The NORPACT-1 trial showed perioperative chemotherapy (NAT FOLFIRINOX and AT of physician’s choice) worsens the overall survival (OS) compared to traditional upfront surgery (UpS)/AT (23 vs. 34 months, hazard ratio (HR) of 1.46, P=0.158) [12]. Interestingly, OS was worse for the NAT group despite having a good disease control rate (DCR, 81%) while on NAT, pathological objective treatment response (OR, 56%), and favorable pathological features compared to the UpS group (R0 rate, 56% vs. 39%, P=0.018 and node-positivity 71% vs. 86%, P<0.001).
The evidence suggests that patient selection beyond traditional factors that influence the decision to offer surgery, such as stage of diagnosis, resectability on imaging, and serum carbohydrate antigen 19-9 (sCA19-9) level, is required. The poor sensitivity of sCA19-9 and the latency and evolving diagnostic uncertainty surrounding radiographic changes associated with PDA make both sCA19-9 and imaging suboptimal biomarkers to predict outcomes [19,20]. Thus, there is a need to explore novel, reliable biomarkers that address the above-mentioned aspects of NAT in PDA and provide a real-time snapshot of treatment response (TR) and aggressive tumor behavior (risk of recurrence and unfavorable pathological features). A noninvasive source for biomarkers, such as blood, could guide treating physicians in making necessary adjustments in real-time and developing individualized strategies to improve the outcomes in these patients. We could also extend this knowledge to manage advanced PDAs.
Mucin 5AC (MUC5AC) is a large glycoprotein generally produced in the normal lung and gastrointestinal tracts, working alongside other mucins to shield these organs from infections, inflammation, and various physiological stresses [21,22,23,24,25]. It is believed to play an important role in the malignant transformation of pancreatic cells [26,27,28,29,30,31,32]. We studied its diagnostic value, summarized preclinical evidence suggesting its influence on treatment response, and proved its prognostic value in resected PDA post-NAT in prior publications [33,34,35,36,37]. MUC5AC detected in PDA tissue can be broadly divided into 2 major categories: mature MUC5AC detected in the apical region intracellularly and in the extracellular space, and immature MUC5AC primarily detected in the perinuclear region [30]. Our recent work showed that tissue mature MUC5AC expression level and site of detection in resected PDA post-NAT impacts progression-free survival (PFS) [33]. Prior studies have shown the diagnostic value of serum MU5AC (sMUC5AC), but its prognostic (survival) and predictive (treatment response) value was never clearly defined [38,39,40].
We present the clinical significance of serum MUC5AC (sMUC5AC) in PDA management. We focused primarily on the value of the sMUC5AC level during NAT before surgery, and after surgery in patients who did not receive NAT (UpS). The goal was to develop a blood-based biomarker that aids in monitoring treatment response while patients are receiving NAT and assesses the risk of recurrence post-surgery.
2. Materials and Methods
2.1. Study Design and Population
This retrospective study was conducted at The Ohio State University Comprehensive Cancer Center (OSUCCC), after receiving appropriate Institutional Review Board approvals. The Total Cancer Care Program (TCCP), a division of OSUCCC, identified the patients who underwent resection for PDA at this institution and provided serum samples from the requested study period, January 2010 to June 2021. Any additional clinical or pathologic information was collected by manual electronic medical chart review. For this study, we focused on 2 patient populations: (1) the NAT group, which included patients with serum samples available for sMUC5AC testing while receiving NAT, and (2) the UpS group, consisting of patients with serum samples available for sMUC5AC testing before receiving the first dose of AT.
2.2. ELISA Assay for Human MUC5AC Detection from Human Serum
Serum MUC5AC samples were analyzed using the Human MUC5AC ELISA Kit (Catalog number NBP2-76703, Novus Biologicals, Centennial, CO) following the manufacturer’s instructions. In brief, human MUC5AC protein standards in serial dilutions were prepared; 100 µL of the diluted standards or samples to MUC5AC antibody pre-coated wells of the assay plate, in triplicate, were added and incubated for 90 min at 37 °C. After removing the liquid from each well, 100 μL of Biotinylated Detection anti-human MUC5AC detecting antibody were added to each well, followed by incubation for 1 hour at 37 °C. The solution was aspirated from each well, and 350 uL of wash buffer was added to each well. After soaking for 2 min, the solution was aspirated from each well. We repeated this wash step 3 times. Then, 100 μL of HRP Conjugate working solution were added to each well and incubated for 30 min at 37 °C, followed by 5 iterations of the wash step. Finally, 90 μL of Substrate Reagent were added to each well and incubated for about 30 min at 37 °C, followed by adding 50 μL of Stop Solution to each well to stop the reaction. Each well's optical density (OD value) was determined at once using a microplate reader set to 450 nm. The average levels of sMUC5AC were calculated based on the serial diluted standard concentrations. The sCA19-9 level was taken from the chart review. Based on the collection dates of the samples available to us for sMUC5AC measurement, we identified the required sCA19-9 levels from the patient charts. The sCA19-9 value for undetectable (<15 ng/ml) patients was taken as 0 for analysis.
While categorizing pathological treatment response for this study, patients with extensive tumors with no evident tumor regression or score 3 response were designated as the no-response (NR) group. Patients with residual tumors with evidence of regression or score 2 response and near complete response or single cells or a small group of cancer cells or score 1 response were considered partial-response (PR) and near complete-response (nCR), respectively. The objective response (OR) group refers to patients with PR and nCR. PFS was defined as the time between the date of diagnosis and recurrence after surgery. The OS was defined as the time between the date of diagnosis and death or the last date of follow-up available at the time of data collection (July 2022).
2.3. Statistical Considerations
Descriptive statistics were used to summarize patient baseline characteristics. Univariate logistic regression models assessed the association between pathological features and sMUC5AC levels. PFS and OS analyses were performed through Kaplan-Meier curves and univariate and multivariate Cox regression models over pathological features. A Bonferroni correction was applied for P-value adjustments. All analyses used SAS 9.4 (Cary, NC, USA).
3. Results
We studied the role of sMUC5AC during NAT treatment (before surgery) and the immediate postoperative period in patients who had UpS (before the first dose of AT) separately.
3.1. Role of sMUC5AC in Patients Receiving NAT
We had 23 patients in this group to analyze (median age – 66 years with 52% females). The median time for serum collection was 5 weeks (within the first week (4 days) to 21 weeks) after therapy. Nineteen had FOLFIRINOX, 3 had gemcitabine and nab-paclitaxel (Gem-NP), and 1 had FOLFOX. The mean sMUC5AC level (in ng/mL) was 1.82, with a median of 0.7 (range of 0.4 to 8.3). The mean sCA19-9 level (in ng/mL) was 698, with a median of 181 (range of 0 to 5874). Three patients had undetectable CA 19-9 (<15) on the day their MUC5AC was measured (2 with FOLFIRINOX and 1 with Gem-NP). For the FOLFIRINOX subgroup (n=19), the mean sMUC5AC level (in ng/mL) was 1.74, with a median of 0.7 (0.43 to 8.3). Nine patients did not receive AT. Six patients had 5FU-based AT (1- 5FU only, 5 FOLIRINOX) and 8 had Gem-based AT (3 Gem/Cap, 2 Gem/NP, 3 Gem-only). Median doses received were 6 for in NAT group (range 4-9) and FOLFIRINOX group (range 2-9). Most of the patients (19/23, 83%) had sCA19-9 on the same day as sMUC5AC was measured. Three and 1 patients had sCA19-9 from 2 and 4 days after the sMUC5AC sample collection date, respectively. We discuss the baseline pathological features of this group in Supplementary Table S1.
3.1.1. sMUC5AC Level Is Associated with Clinicopathological Features in the Resected Sample
Logistic regression analysis was done to study the association between pathological features in the resected sample with sMUC5AC levels (Table 1).
sMUC5AC was significantly associated with treatment response (nCR (n=2) vs. PR (n=9) vs. NR (n=12)), margin status, and residual disease. The mean sMUC5AC level (in ng/mL) was higher in patients with PR than nCR and NR (PR > NR > nCR = 2.84 > 1.28 > 0.43 ng/mL, P=0.01) as illustrated in Figure 1.This is also true for the FOLFIRINOX subgroup (nCR (n=2) vs. PR (n=7) vs. NR (n=10), PR > NR > nCR = 3.2 > 0.93 > 0.43 ng/mL, P=0.001). The mean sCA19-9 levels were expectedly higher in NR than nCR and PR (as shown in Supplementary Figure S1), though the differences were not significant (NR > PR > nCR, 958 > 258 > 129, P=0.4) in the NAT group (n=23). The same pattern was observed in the FOLFIRINOX group (NR > PR > nCR, 1061 > 227 > 129 ng/mL, P=0.3).
3.1.2. Association of sMUC5AC Level on Outcome
sMUC5AC significantly impacted PFS on univariate (UVA) (p=0.01) and multivariate (MVA) (HR of 49.2, 95% CI—4.4 to 1008.3, P=0.002) analysis (Table 2, Supplementary Tables S2 & S3). sMUC5AC did not affect OS on UVA or MVA. sCA19-9 was significant for PFS, but the HR was not impressive (1.003017). Multiple factors impacting PFS were included in the multivariate model, including the AT received (5FU-based vs. Gem-based vs. none) and extracellular MUC5AC composite score (EC-M CS). The latter was used to incorporate 2 major aspects of MUC5AC expression in PDA tissues – intracellular mature MUC5AC expression and extracellular MUC5AC detection in MVA for PFS and OS – by using the formula MM H-score × EC-M detection (0 for EC-M negative and 1 for EC-M positive) [33]. The value will be 0 for extracellular MUC5AC-negative tumors and the H-score for the intracellular mature MUC5AC for EC-positive tumors.
3.1.3. Pre-Surgery Model to Predict PFS
We evaluated various models (Table 3), integrating sMUC5AC with clinical factors accessible to the physician administering NAT, including sCA19-9 levels on the day of sMUC5AC measurement, sCA19-9 at diagnosis, and the specific NAT combination used. Our objective was to develop models to predict recurrence risk before surgery, contrasting with the multivariate model in Table 2, which includes critical surgical pathological features (that are available only after surgery). sMUC5AC was the only significant factor, with HR ranging between 1.44 and 1.54 in all models in the NAT group. It was also significant in the FOLFIRINOX subgroup (HR of 1.41 and 1.48). sMUC5AC was insignificant for OS in the analysis (data not shown).
3.1.4. High vs. Low MUC5AC Groups
We further explored the impact of MUC5AC by dividing the NAT based on the means in their respective groups as thresholds (Table 4). The lower sMUC5AC group (n=16) had significantly larger (> 2 cm) tumors, R0, and margin-negative disease and better PFS than the higher sMUC5AC group (n=7). A trend toward significance was observed in the differences between both groups for OS (P=0.08), EC-M CS, and the fraction of patients with nCR vs. PR vs. NR (p=0.09). A similar trend was observed in the FOLFIRINOX sub-group (n=19, the mean sMUC5AC (in ng/mL) was 1.74, with a median of 0.7 (range of 0.43 to 8.3)).
3.2. sMUC5AC as a Predictor for Recurrence Post-Surgery
We evaluated 19 patients with serum samples available post-surgery (UpS-group) and before the first dose of AT (8 Gem-only, 4 Gem-NP, 4 Gem/Cap, 1 5FU, 1 chemoratiation (CRT), and 1 FOLFIRINOX). The median age of this group was 66 years (range 47 to 84) with 42% (8/19) males and a majority Caucasian (18/19, 95% and 1/19, 5% African-American) population. Most (17/19) had sCA19-9 from the same day of sMUC5AC level. One had sCA19-9 1 day before and another had it 1 day after the sMUC5AC collection date. We discussed other baseline pathological features in Supplementary Table S1.
The serum was collected between the week of surgery and 16 weeks (median of 2 weeks). None of the patients had NAT. The mean sMUC5AC level was 1.1 (median 0.87, range of 0.42 to 3.3). The mean sCA19-9 level was 492 (median 0, range of 0 to 3292). sMUC5AC had a trend toward significance for OS (P=0.06) for UVA but not for PFS. sMUC5AC was insignificant in the MVA model with factors tested in presurgery analysis (as in Table 2) for PFS and OS (Supplementary Table S4). The blood-based MVA models evaluating sMUC5AC and sCA19-9 on the same day (as MUC5AC), sCA19-9 at diagnosis, and AT had interesting results (Table 5). sMUC5AC had an HR ranging from 2-3 for PFS, indicating its value irrespective of the pathological features noted in the resected sample. sCA19-9 was undetectable or normal in 12/19 patients and unreliable in most of the models tested (not all models are shown here), further strengthening our argument to combine it with sMUC5AC for designing accurate models.
We evaluated the ability of sMUC5AC to predict recurrence (Table 6). If we take the median for sMUC5AC as the cut-off for an abnormal value, the sensitivity and specificity to predict recurrence during the study period (3/19) were 50% and 67%, respectively. If we take mean sMUC5AC as the cutoff, sensitivity was low (25%), but specificity was 100%. For abnormal sCA19-9 (> 37 U/mL), the sensitivity and specificity were 56% and 100%, respectively; however, when we combined both, the sensitivity increased to 82% and the specificity dropped to 66%. The median PFS was 14.5 months, and the early recurrent groups (<14.5 m) had higher sMUC5AC (mean 0.8 vs. 1.5, P=0.02). Thus, post-surgery sMUC5AC testing could help predict recurrence with or without sCA19-9.
4. Discussion
The clinical significance of tissue MUC5AC in PDA is not clear, and the value of sMUC5AC has not been explored. In a recently published paper, we showed mature MUC5AC detected in extracellular space and intracellular expression influence the outcome in patients undergoing surgery post-NAT [33]. In this small study, we provided preliminary evidence suggesting the potential of sMUC5AC, alone or in combination with sCA19-9, to be a useful biomarker in monitoring treatment resistance and the risk of recurrence in resected PDA patients with or without NAT. The small sample size of this study could not give us definitive (P<0.05) answers, but we can infer that the lower sMUC5AC group had a lower tumor cell turnover (hence, higher nCR or NR), supported by larger size and high sCA19-9, but had better survival because other vital pathological factors (residual disease and margin status) were significantly favorable. This could be linked to tissue MUC5AC expression noted in the resected specimens in this group (lower EC-M CS and EC-M detection rates). Two patients with nCR and 2/12 with NR had the lowest sMUC5AC (0.43 ng/mL). Alternatively, the tumor cell turnover is high in the other group, but these specimens had unfavorable pathological features, possibly due to higher tissue MUC5AC expression. It is important to note that sCA19-9, an indicator of tumor burden, was higher in the lower sMUC5AC group (P>0.05) than the high sMUC5AC group due to larger tumors (3 had undetectable sCA19-9 - taken as 0 ng/mL) but had better PFS. We hypothesize that sMUC5AC is a biomarker for pancreatic tumor cell turnover and aggressive behavior, and sCA19-9 is a biomarker for tumor burden at any time while on systemic therapy. Monitoring both could help predict treatment response and recurrence in PDA patients on NAT.
Our hypothesis explains lower sMUC5AC in NR and nCR than PR groups. Logic suggests that patients with nCR will have PR first. If the tumor responds to therapy but a considerable portion of the viable tumor is left (PR), sMUC5AC rises secondary to the destruction of more tumor cells and the release of MUC5AC into the bloodstream, and the sCA19-9 drops secondary to reducing the size of a viable tumor. If the tumor continues to respond and only a small amount of tumor is left (i.e., nCR), the sMUC5AC level drops and sCA19-9 continues to drop or stay undetectable (Figure 1 & Supplementary Figure S1). sMUC5AC will be low if measured after nCR. When the tumor develops resistance, the cancer cells stop dying, and the tumor burden increases; hence, there is less MUC5AC in the blood and high sCA19-9. In patients who do not produce sCA19-9, sMUC5AC rises with response and plateaus or is stable with no response. We are handicapped by having only 1 serum sample in this study to confirm this, but combining sCA19-9 and MUC5AC levels will make more sense. Alternatively, in patients with NR, PDA cells do not die, less MUC5AC is detected in the blood, and they tend to produce higher amounts of sCA19-9 (Figure 2 & Supplementary Figure S2).
If patient is responding to treatment – dropping serum CA19-9 and rising serum MUC5AC indicating partial response, and later dropping-to-stable serum MUC5AC and dropping serum CA19-9 when there is near complete response. When tumor starts developing resistance, rising CA19-9 along with dropping serum MUC5AC. If patient has innate resistance to the treatment – rising serum CA19-9 along with low serum MUC5AC
In terms of differentiating nCR and NR, we summarized the relationship between sCA19-9 and sMUC5AC, and the pathological TR we noted in the resected sample (Supplementary Table S5). Rising sCA19-9 with low-to-stable sMUC5AC could indicate NR (CA19-9, NR vs. nCR, 1060 vs. 129, P=0.2). Low-to-stable sMUC5AC with dropping sCA19-9 could indicate nCR. However, if sCA19-9 and sMUC5AC rise, it could indicate disease progression. Serial monitoring of sMUC5AC and sCA19-9 could help predict pathological TR and other high-risk features, thereby guiding the NAT strategy. For instance, if a patient starts with rising sMUC5AC and dropping sCA19-9, continuing NAT until sMUC5AC stabilizes or drops could lead to nCR and favorable pathological features in the resected sample. Alternatively, rising sCA19-9 and stable/dropping sMUC5AC within 2-3 weeks of NAT could indicate treatment resistance.
Retrospective studies involving small sample sizes in both groups must be validated through prospective research. Variability in postoperative therapy within the NAT group might have impacted the results. Additionally, the timing of sMUC5AC sample collection was inconsistent across both groups, occurring either before or after NAT. Accurate sCA19-9 measurements were challenging when levels were below 15 ng/mL, as these were recorded as 0 ng/mL. Furthermore, the ELISA method is less sensitive than multiplex assays for detecting small changes in sMUC5AC levels. We lack serial samples to test or confirm our hypothesis or to guide. Nevertheless, we provide preliminary data that could lay the groundwork for future studies.
5. Conclusions
Our work suggests the prognostic value of sMUC5AC while receiving NAT. In the UpS group, elevated sMUC5AC in the early postoperative period before systemic therapy was associated with early recurrence. sMUC5AC and sCA19-9 testing are noninvasive and give real-time snapshots of TR, tumor cell activity, and burden, allowing physicians to make necessary adjustments for PDA treatments, including changing regimens, considering CRT, or proceeding with resection.
6. Patents
MUC5AC in pancreatic adenocarcinoma (PCT/US2024/012771, 24 January 2024)) [patent pending].
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Supplementary Table S1: Baseline characteristics of the population studied; Supplementary Table S2: Multivariate analysis for progression-free survival; Supplementary Table S3: Multivariate analysis for overall survival; Supplementary Table S4: Multivariate and univariate analysis for survival in post-surgery patients; Supplementary Table S5: Relationship between serum CA19-9, MUC5AC, and treatment response; Supplementary Figure S1: Relation between serum MUC5AC and CA19-9 with treatment response.
Author Contributions
Conceptualization, study design, chart review, and writing—original draft preparation – A.M. (Ashish Manne); Methodology and Investigation – Y.B. and W.Y.; Chart review –A.S. and A.S. (Amir Sara); Biostatistics – L.Y.; Writing—review and editing – U.M., R.K.P., K.H., W.Y., A.K., A.M. (Arjun Mittra), J.H., S.R., P.M., S.R., N.J., J.M.C., S.T., A.E., K.T., D.S., S.J., R.S., and M.D.
Funding
The Ohio State University Intramural Research Program Award (Pelotonia, GR126178).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of The Ohio State University (protocol number: 2021C0160; date of approval: 9/30/2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
For ethical reasons, the data presented in this study are available upon request from the corresponding author.
Acknowledgments
This work was supported in part by the Cancer Center Support Grant from the National Cancer Institute (P30 CA016058) and the Clinical and Translational Science Shared Resource at The Ohio State University Comprehensive Cancer Center. Images were created using biorender.com.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Siegel, R.L.; Giaquinto, A.N.; Jemal, A. Cancer statistics, 2024. CA Cancer J Clin 2024, 74, 12–49. [Google Scholar] [CrossRef]
- Neoptolemos, J.P.; Palmer, D.H.; Ghaneh, P.; Psarelli, E.E.; Valle, J.W.; Halloran, C.M.; Faluyi, O.; O'Reilly, D.A.; Cunningham, D.; Wadsley, J.; et al. Comparison of adjuvant gemcitabine and capecitabine with gemcitabine monotherapy in patients with resected pancreatic cancer (ESPAC-4): a multicentre, open-label, randomised, phase 3 trial. Lancet 2017, 389, 1011–1024. [Google Scholar] [CrossRef] [PubMed]
- Conroy, T.; Hammel, P.; Hebbar, M.; Ben Abdelghani, M.; Wei, A.C.; Raoul, J.-L.; Choné, L.; Francois, E.; Artru, P.; Biagi, J.J.; et al. FOLFIRINOX or Gemcitabine as Adjuvant Therapy for Pancreatic Cancer. New England Journal of Medicine 2018, 379, 2395–2406. [Google Scholar] [CrossRef] [PubMed]
- Groot, V.P.; Daamen, L.A.; He, J.; Wolfgang, C.L.; Molenaar, I.Q. Patterns of Recurrence After Surgery for Pancreatic Cancer. In Textbook of Pancreatic Cancer; Springer International Publishing: 2021; pp. 1153–1168.
- Paniccia, A.; Hosokawa, P.; Henderson, W.; Schulick, R.D.; Edil, B.H.; Mccarter, M.D.; Gajdos, C. Characteristics of 10-Year Survivors of Pancreatic Ductal Adenocarcinoma. JAMA Surgery 2015, 150, 701. [Google Scholar] [CrossRef] [PubMed]
- Oettle, H.; Post, S.; Neuhaus, P.; Gellert, K.; Langrehr, J.; Ridwelski, K.; Schramm, H.; Fahlke, J.; Zuelke, C.; Burkart, C.; et al. Adjuvant Chemotherapy With Gemcitabine vs Observation in Patients Undergoing Curative-Intent Resection of Pancreatic Cancer. JAMA 2007, 297, 267. [Google Scholar] [CrossRef]
- Neoptolemos, J.P.; Stocken, D.D.; Bassi, C.; Ghaneh, P.; Cunningham, D.; Goldstein, D.; Padbury, R.; Moore, M.J.; Gallinger, S.; Mariette, C.; et al. Adjuvant Chemotherapy With Fluorouracil Plus Folinic Acid vs Gemcitabine Following Pancreatic Cancer Resection. JAMA 2010, 304, 1073. [Google Scholar] [CrossRef]
- Sinn, M.; Bahra, M.; Liersch, T.; Gellert, K.; Messmann, H.; Bechstein, W.; Waldschmidt, D.; Jacobasch, L.; Wilhelm, M.; Rau, B.M.; et al. CONKO-005: Adjuvant Chemotherapy With Gemcitabine Plus Erlotinib Versus Gemcitabine Alone in Patients After R0 Resection of Pancreatic Cancer: A Multicenter Randomized Phase III Trial. Journal of Clinical Oncology 2017, 35, 3330–3337. [Google Scholar] [CrossRef]
- Jones, R.P.; Psarelli, E.-E.; Jackson, R.; Ghaneh, P.; Halloran, C.M.; Palmer, D.H.; Campbell, F.; Valle, J.W.; Faluyi, O.; O’Reilly, D.A.; et al. Patterns of Recurrence After Resection of Pancreatic Ductal Adenocarcinoma. JAMA Surgery 2019, 154, 1038. [Google Scholar] [CrossRef]
- Izumo, W.; Higuchi, R.; Furukawa, T.; Yazawa, T.; Uemura, S.; Shiihara, M.; Yamamoto, M. Evaluation of preoperative prognostic factors in patients with resectable pancreatic ductal adenocarcinoma. Scandinavian Journal of Gastroenterology 2019, 54, 780–786. [Google Scholar] [CrossRef]
- Munir, R.; Soreide, K.; Ravindran, R.; Powell, J.J.; Harrison, E.M.; Adair, A.; Wigmore, S.J.; Parks, R.W.; Garden, O.J.; Kirkpatrick, L.; et al. Patterns of recurrence after curative-intent surgery for pancreas cancer reinforce the importance of locoregional control and adjuvant chemotherapy. 2018. [CrossRef]
- Labori, K.J.; Bratlie, S.O.; Andersson, B.; Angelsen, J.-H.; Biörserud, C.; Björnsson, B.; Bringeland, E.A.; Elander, N.; Garresori, H.; Grønbech, J.E.; et al. Neoadjuvant FOLFIRINOX versus upfront surgery for resectable pancreatic head cancer (NORPACT-1): a multicentre, randomised, phase 2 trial. The Lancet Gastroenterology & Hepatology 2024, 9, 205–217. [Google Scholar] [CrossRef]
- Sohal, D.P.S.; Duong, M.; Ahmad, S.A.; Gandhi, N.S.; Beg, M.S.; Wang-Gillam, A.; Wade, J.L.; Chiorean, E.G.; Guthrie, K.A.; Lowy, A.M.; et al. Efficacy of Perioperative Chemotherapy for Resectable Pancreatic Adenocarcinoma. JAMA Oncology 2021, 7, 421. [Google Scholar] [CrossRef] [PubMed]
- Fietkau, R.; Ghadimi, M.; Grützmann, R.; Wittel, U.A.; Jacobasch, L.; Uhl, W.; Croner, R.S.; Bechstein, W.O.; Neumann, U.P.; Waldschmidt, D.; et al. Randomized phase III trial of induction chemotherapy followed by chemoradiotherapy or chemotherapy alone for nonresectable locally advanced pancreatic cancer: First results of the CONKO-007 trial. Journal of Clinical Oncology 2022, 40, 4008. [Google Scholar] [CrossRef]
- Ghaneh, P.; Palmer, D.; Cicconi, S.; Jackson, R.; Halloran, C.M.; Rawcliffe, C.; Sripadam, R.; Mukherjee, S.; Soonawalla, Z.; Wadsley, J.; et al. Immediate surgery compared with short-course neoadjuvant gemcitabine plus capecitabine, FOLFIRINOX, or chemoradiotherapy in patients with borderline resectable pancreatic cancer (ESPAC5): a four-arm, multicentre, randomised, phase 2 trial. Lancet Gastroenterol Hepatol 2023, 8, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Groot Koerkamp, B.; Janssen, Q.P.; van Dam, J.L.; Bonsing, B.A.; Bos, H.; Bosscha, K.P.; Haberkorn, B.C.M.; de Hingh, I.H.J.T.; Karsten, T.M.; Van der Kolk, M.B.; et al. LBA83 Neoadjuvant chemotherapy with FOLFIRINOX versus neoadjuvant gemcitabine-based chemoradiotherapy for borderline resectable and resectable pancreatic cancer (PREOPANC-2): A multicenter randomized controlled trial. Ann Oncol 2023, 34, S1323. [Google Scholar] [CrossRef]
- Katz, M.H.G.; Shi, Q.; Meyers, J.; Herman, J.M.; Chuong, M.; Wolpin, B.M.; Ahmad, S.; Marsh, R.; Schwartz, L.; Behr, S.; et al. Efficacy of Preoperative mFOLFIRINOX vs mFOLFIRINOX Plus Hypofractionated Radiotherapy for Borderline Resectable Adenocarcinoma of the Pancreas: The A021501 Phase 2 Randomized Clinical Trial. JAMA Oncol 2022, 8, 1263–1270. [Google Scholar] [CrossRef]
- Versteijne, E.; van Dam, J.L.; Suker, M.; Janssen, Q.P.; Groothuis, K.; Akkermans-Vogelaar, J.M.; Besselink, M.G.; Bonsing, B.A.; Buijsen, J.; Busch, O.R.; et al. Neoadjuvant Chemoradiotherapy Versus Upfront Surgery for Resectable and Borderline Resectable Pancreatic Cancer: Long-Term Results of the Dutch Randomized PREOPANC Trial. J Clin Oncol 2022, 40, 1220–1230. [Google Scholar] [CrossRef]
- Poruk, K.E.; Gay, D.Z.; Brown, K.; Mulvihill, J.D.; Boucher, K.M.; Scaife, C.L.; Firpo, M.A.; Mulvihill, S.J. The clinical utility of CA 19-9 in pancreatic adenocarcinoma: diagnostic and prognostic updates. Curr Mol Med 2013, 13, 340–351. [Google Scholar] [CrossRef]
- Elbanna, K.Y.; Jang, H.J.; Kim, T.K. Imaging diagnosis and staging of pancreatic ductal adenocarcinoma: a comprehensive review. Insights Imaging 2020, 11, 58. [Google Scholar] [CrossRef]
- Bauer, A.K.; Umer, M.; Richardson, V.L.; Cumpian, A.M.; Harder, A.Q.; Khosravi, N.; Azzegagh, Z.; Hara, N.M.; Ehre, C.; Mohebnasab, M.; et al. Requirement for MUC5AC in KRAS-dependent lung carcinogenesis. JCI Insight 2018, 3. [Google Scholar] [CrossRef]
- Rose, M.C.; Voynow, J.A. Respiratory Tract Mucin Genes and Mucin Glycoproteins in Health and Disease. Physiological Reviews 2006, 86, 245–278. [Google Scholar] [CrossRef]
- López-Ferrer, A.; de Bolós, C.; Barranco, C.; Garrido, M.; Isern, J.; Carlstedt, I.; Reis, C.A.; Torrado, J.; Real, F.X. Role of fucosyltransferases in the association between apomucin and Lewis antigen expression in normal and malignant gastric epithelium. Gut 2000, 47, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Bansil, R.; Turner, B.S. Mucin structure, aggregation, physiological functions and biomedical applications. Current Opinion in Colloid & Interface Science 2006, 11, 164–170. [Google Scholar] [CrossRef]
- Kebouchi, M.; Hafeez, Z.; Le Roux, Y.; Dary-Mourot, A.; Genay, M. Importance of digestive mucus and mucins for designing new functional food ingredients. Food Research International 2020, 131, 108906. [Google Scholar] [CrossRef] [PubMed]
- Yamazoe, S.; Tanaka, H.; Iwauchi, T.; Yoshii, M.; Ito, G.; Amano, R.; Yamada, N.; Sawada, T.; Ohira, M.; Hirakawa, K. Identification of HLA-A*0201- and A*2402-restricted epitopes of mucin 5AC expressed in advanced pancreatic cancer. Pancreas 2011, 40, 896–904. [Google Scholar] [CrossRef]
- Nagata, K.; Horinouchi, M.; Saitou, M.; Higashi, M.; Nomoto, M.; Goto, M.; Yonezawa, S. Mucin expression profile in pancreatic cancer and the precursor lesions. J Hepatobiliary Pancreat Surg 2007, 14, 243–254. [Google Scholar] [CrossRef]
- Kim, G.E.; Bae, H.I.; Park, H.U.; Kuan, S.F.; Crawley, S.C.; Ho, J.J.; Kim, Y.S. Aberrant expression of MUC5AC and MUC6 gastric mucins and sialyl Tn antigen in intraepithelial neoplasms of the pancreas. Gastroenterology 2002, 123, 1052–1060. [Google Scholar] [CrossRef] [PubMed]
- Kaur, S.; Kumar, S.; Momi, N.; Sasson, A.R.; Batra, S.K. Mucins in pancreatic cancer and its microenvironment. Nature Reviews Gastroenterology & Hepatology 2013, 10, 607–620. [Google Scholar] [CrossRef]
- Krishn, S.R.; Ganguly, K.; Kaur, S.; Batra, S.K. Ramifications of secreted mucin MUC5AC in malignant journey: a holistic view. Carcinogenesis 2018, 39, 633–651. [Google Scholar] [CrossRef]
- Matsuyama, M.; Kondo, F.; Ishihara, T.; Yamaguchi, T.; Ito, R.; Tsuyuguchi, T.; Tawada, K.; Yokosuka, O. Evaluation of pancreatic intraepithelial neoplasia and mucin expression in normal pancreata. J Hepatobiliary Pancreat Sci 2012, 19, 242–248. [Google Scholar] [CrossRef]
- Yamasaki, H.; Ikeda, S.; Okajima, M.; Miura, Y.; Asahara, T.; Kohno, N.; Shimamoto, F. Expression and localization of MUC1, MUC2, MUC5AC and small intestinal mucin antigen in pancreatic tumors. Int J Oncol 2004, 24, 107–113. [Google Scholar] [CrossRef]
- Manne, A.; Esnakula, A.; Sheel, A.; Sara, A.; Manne, U.; Paluri, R.K.; He, K.; Yang, W.; Sohal, D.; Kasi, A.; et al. Mature MUC5AC Expression in Resected Pancreatic Ductal Adenocarcinoma Predicts Treatment Response and Outcomes. International Journal of Molecular Sciences 2024, 25, 9041. [Google Scholar] [CrossRef] [PubMed]
- Manne, A.; Esnakula, A.; Abushahin, L.; Tsung, A. Understanding the Clinical Impact of MUC5AC Expression on Pancreatic Ductal Adenocarcinoma. Cancers 2021, 13, 3059. [Google Scholar] [CrossRef]
- Manne, A.; Kasi, A.; Esnakula, A.K.; Paluri, R.K. Predictive Value of MUC5AC Signature in Pancreatic Ductal Adenocarcinoma: A Hypothesis Based on Preclinical Evidence. International Journal of Molecular Sciences 2023, 24, 8087. [Google Scholar] [CrossRef] [PubMed]
- Manne, A.; Mneimneh, W.; Elkadi, O.; Escobar, D.E.; Coley, J.; Guzman, G.B.; Fnu, S.M.d.; Alkharabsheh, O.; Khushman, M.d.M. The pattern of mucin 5AC (MUC5AC) expression using immunohistochemistry and its prognostic significance in patients with pancreatic ductal adenocarcinoma. Journal of Clinical Oncology 2020, 38, e16756. [Google Scholar] [CrossRef]
- Manne, A.; Yu, L.; Hart, P.A.; Tsung, A.; Esnakula, A. Differential Expression and Diagnostic Value of MUC5AC Glycoforms in Pancreatic Ductal Adenocarcinoma. Cancers 2023, 15, 4832. [Google Scholar] [CrossRef]
- Kaur, S.; Smith, L.M.; Patel, A.; Menning, M.; Watley, D.C.; Malik, S.S.; Krishn, S.R.; Mallya, K.; Aithal, A.; Sasson, A.R.; et al. A Combination of MUC5AC and CA19-9 Improves the Diagnosis of Pancreatic Cancer: A Multicenter Study. Am J Gastroenterol 2017, 112, 172–183. [Google Scholar] [CrossRef]
- Yue, T.; Maupin, K.A.; Fallon, B.; Li, L.; Partyka, K.; Anderson, M.A.; Brenner, D.E.; Kaul, K.; Zeh, H.; Moser, A.J.; et al. Enhanced discrimination of malignant from benign pancreatic disease by measuring the CA 19-9 antigen on specific protein carriers. PLoS One 2011, 6, e29180. [Google Scholar] [CrossRef]
- Yang, K.S.; Ciprani, D.; O’Shea, A.; Liss, A.S.; Yang, R.; Fletcher-Mercaldo, S.; Mino-Kenudson, M.; Fernández-Del Castillo, C.; Weissleder, R. Extracellular Vesicle Analysis Allows for Identification of Invasive IPMN. Gastroenterology 2021, 160, 1345–1358. [Google Scholar] [CrossRef]
Figure 1.
Comparing serum MUC5AC levels in various pathological response groups. nCR – near complete response, PR-partial response, NR- no response. Serum MUC5AC in ng/mL.
Figure 1.
Comparing serum MUC5AC levels in various pathological response groups. nCR – near complete response, PR-partial response, NR- no response. Serum MUC5AC in ng/mL.
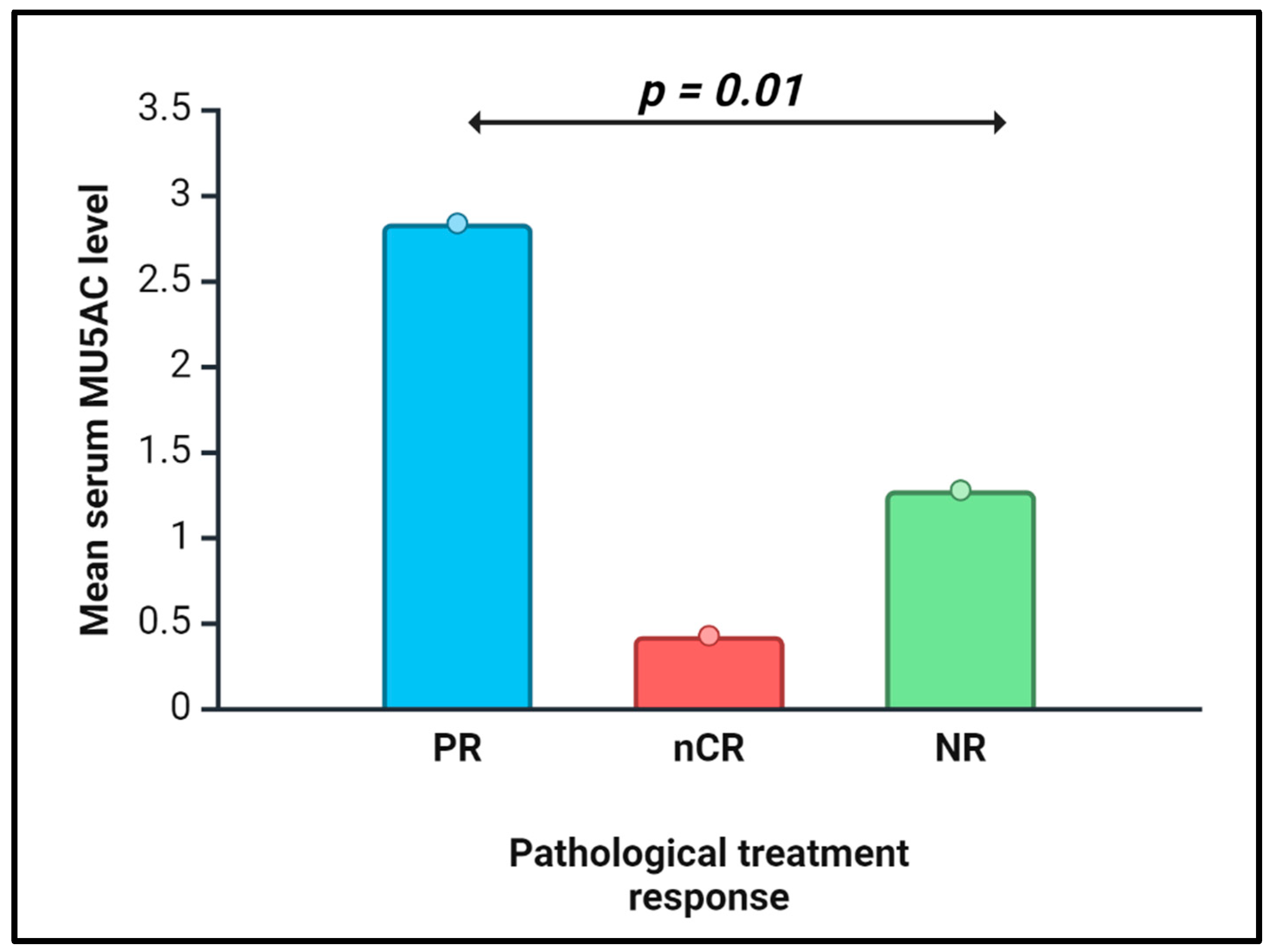
Figure 2.
Serum MUC5AC and CA19-9 levels in patients on chemotherapy – hypothesis. MUC5AC – mucin 5 AC, CA19-9 – Carbohydrate antigen 19-9.
Figure 2.
Serum MUC5AC and CA19-9 levels in patients on chemotherapy – hypothesis. MUC5AC – mucin 5 AC, CA19-9 – Carbohydrate antigen 19-9.
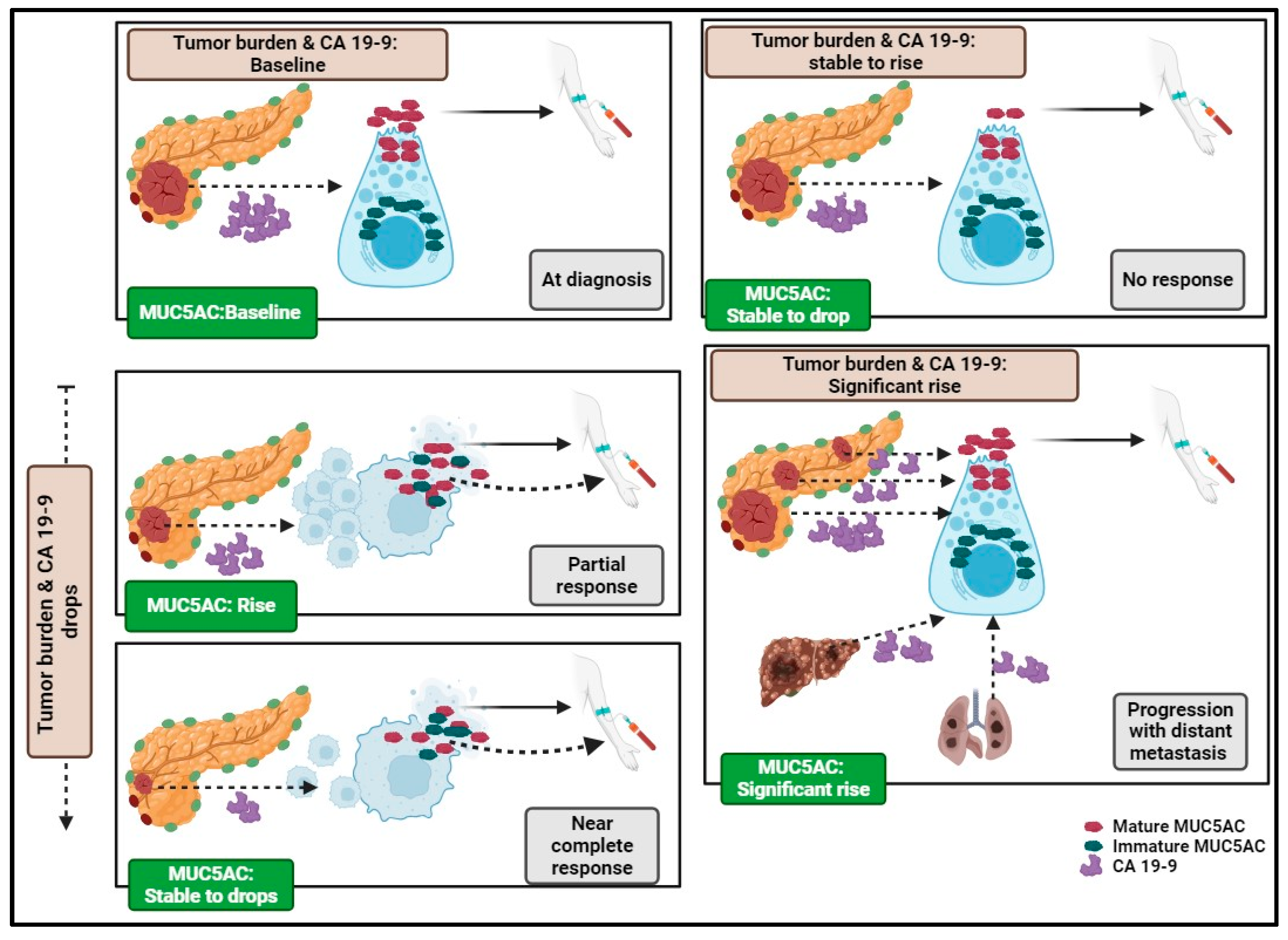

Table 1.
Univariate logistic regression of serum MUC5AC on clinicopathological features.
| Pathological feature | In all NAT (N=23) P-value* |
FOLFIRNOX (N=19) P-value* |
|---|---|---|
| Pathological differentiation, G1-2 vs G3 | Not significant | Not significant |
| Peripancreatic extension | Not significant | Not significant |
| Treatment effect, nCR vs. PR vs. NR | 0.01 | 0.0013 |
| Treatment effect, OR vs. NR | Not significant | 0.005 |
| Lymphovascular invasion | Not significant | Not significant |
| Perineural invasion | Not significant | Not significant |
| Margins-status, positive vs. negative | 0.0119 | 0.03 |
| Residual disease, R0 vs. R1-R2 | 0.002 | 0.007 |
| Tumor size (≤ 2 cms vs. > 2cm) | Not significant | Not significant |
| Node-status (N0 vs. N1-N2) | Not significant | Not significant |
| Premalignant lesion#, yes vs. no | Not significant | Not significant |
| Neoadjuvant CRT | Not significant | Not significant |
* p-values of > 0.05 are not mentioned, # in resected sample, NAT-neoadjuvant therapy, nCR – near complete response, PR-partial response, NR- no response, OR – objective response (nCR + PR), CRT - chemoradiation.
Table 2.
Multivariate and univariate analysis for survival.
| Multivariate analysis | Univariate analysis | |||
|---|---|---|---|---|
| Factor tested | PFS | OS | PFS | OS |
| Serum MUC5AC level | 0.0029 | 0.1371 | 0.01 | 0.09 |
| CA19-9 on the same day* | 0.0013 | 0.2926 | 0.3 | 0.1 |
| Pathological differentiation, G1-2 vs. G3 | 0.0020 | 0.2619 | 0.01 | 0.01 |
| Lymph vascular invasion | 0.0011 | 0.0954 | 0.2 | 0.9 |
| Perineural invasion | 0.0404 | 0.0605 | 0.8 | 0.8 |
| Margins | 0.0060 | 0.0171 | 0.1 | 0.01 |
| Residual disease (R0 vs R1/R2) | 0.0040 | 0.0855 | 0.2 | 0.4 |
| Tumor size, ≤ 2cms vs. 2 cms | 0.0091 | 0.1698 | 0.5 | 0.8 |
| Node status (N0 vs. N1-N2) | 0.0163 | 0.9336 | 0.8 | 0.7 |
| Association with premalignant lesions | 0.1692 | 0.3048 | 0.4 | 0.9 |
| Peripancreatic invasion | 0.7750 | 0.7744 | 0.4 | 0.5 |
| NAT CRT, Yes vs. No | 0.0076 | 0.1435 | 0.8 | 0.4 |
| Pathological treatment response | 0.0072 | 0.3427 | 0.8 | 0.7 |
| Adjuvant therapy received (5FU-based vs. Gem based vs. none) | 0.0112 | 0.0192 | 0.09 | 0.01 |
| Extracellular MUC5AC composite score | 0.1058 | 0.9590 | 0.3 | 0.8 |
| NAT combination received# | 0.1458 | 0.1946 | 0.1 | 0.4 |
PFA – progression-free survival; OS – overall survival; CA19-9 – Serum carbohydrate antigen 19-9, G-grade, NAT-neoadjuvant therapy, CRT – chemoradiation, 5FU – 5-fluorouracil, Gem-gemcitabine; * same day as serum MUC5AC; # FOLFIRINOX vs. FOLFOX vs. Gem/nab-paclitaxel.
Table 3.
Multivariate models for progression-free survival.
| Factor | Prob>ChiSq | Level1 | Level2 | Hazard Ratio | Lower | Upper |
|---|---|---|---|---|---|---|
| Pre-surgery Model-1 for NAT (n=23) | ||||||
| sMUC5AC | 0.0122 | 1.446621 | 1.063369 | 1.93764 | ||
| CA19-9 on the same day | 0.1039 | 1.000247 | 0.999892 | 1.000518 | ||
| NAT received | 0.3767 | 1.446621 | 1.063369 | 1.93764 | ||
| 0.1630 | FOLFOX | FOLFIRINOX | 7.3548982 | 0.1630 | 0.4457831 | |
| 0.9611 | GEM NP | FOLFIRINOX | 0.9688818 | 0.9611 | 0.2718774 | |
| 0.1930 | GEM NP | FOLFOX | 0.1317329 | 0.1930 | 0.006226 | |
| Pre-surgery Model-2 for NAT (n=23) | ||||||
| sMUC5AC | 0.0040 | 1.476825 | 1.120562 | 1.938447 | ||
| CA19-9 on the same day* | 0.0885 | 1.000254 | 0.999908 | 1.00052 | ||
| Pre-surgery Model-3 for NAT (n=23) | ||||||
| sMUC5AC | 0.0077 | 1.520411 | 1.103173 | 2.091129 | ||
| CA19-9 on the same day* | 0.8292 | 1.000046 | 0.99955 | 1.000435 | ||
| CA19-9 at diagnosis | 0.0998 | 1.000209 | 0.999901 | 1.000452 | ||
| NAT received | 0.3792 | |||||
| 0.1658 | FOLFOX | FOLFIRINOX | 7.299006 | 0.4388868 | 121.38777 | |
| 0.8624 | GEM NP | FOLFIRINOX | 1.1210998 | 0.3076474 | 4.0854067 | |
| 0.2307 | GEM NP | FOLFOX | 0.1535962 | 0.0071775 | 3.2868913 | |
| Pre-surgery Model-4 for NAT (n=23) | ||||||
| sMUC5AC | 0.0027 | 1.543962 | 1.157315 | 2.077201 | ||
| CA19-9 on the same day* | 0.7725 | 1.00006 | 0.99958 | 1.000439 | ||
| CA19-9 at diagnosis | 0.1000 | 1.0002 | 0.999906 | 1.00043 | ||
| Pre-surgery Model-1 for FOLFIRINOX (n=19) | ||||||
| sMUC5AC | 0.0192 | 1.413824 | 1.037685 | 1.898663 | ||
| CA19-9 on the same day* | 0.1588 | 1.000212 | 0.999856 | 1.000479 | ||
| Pre-surgery Model-2 for FOLFIRINOX (n=19) | ||||||
| sMUC5AC | 0.0125 | 1.487112 | 1.076844 | 2.059867 | ||
| CA19-9 on the same day* | 0.9629 | 1.00001 | 0.999487 | 1.000414 | ||
| CA19-9 at diagnosis | 0.1288 | 1.0002 | 0.999878 | 1.000454 | ||
NAT-neoadjuvant therapy, sMUC5AC -Serum MUC5AC level, CA19-9 – Serum carbohydrate antigen 19-9; * same day as serum MUC5AC; GEM NP – gemcitabine and nab-paclitaxel combination.
Table 4.
Comparing low and high MUC5AC groups.
| Factors tested | NAT-group (p-value)* | FOLFIRINOX (p-value)* |
|---|---|---|
| Threshold MUC5AC in ng/mL (N) | ≤ 1.82 (n=16) vs. >1.82 (n=7) | ≤ 1.74 (N=14) vs. > 1.74 (n=5) |
| CA19-9 mean (ng/mL) | 831 vs. 361 | 817 vs. 358 |
| nCR vs. PR vs. NR (%) | 12.5/25/62.5 vs. 0/71/29 (0.09) | 14/21/65 vs. 0/80/20 (0.06) |
| OR (%) | 38 vs. 71 (0.1) | 36 vs. 80 (0.08) |
| Mature MUC5AC expression (H-score) | 118 vs. 180 (0.1) | 131 vs. 162 |
| Immature MUC5AC expression (H-score) | 119 vs. 163 (0.1) | 133 vs. 150 |
| EC-mature MUC5AC-detection % | 50 vs. 86 (0.1) | 50 vs. 80 |
| EC-M CS | 85 vs. 176 (0.08) | 96 vs. 156 |
| Pathological differentiation# | 69% vs. 71% | 70 vs. 67 |
|
Tumor size, ≤ 2 cm vs. > 2 cm, % of patients with > 2 cm |
88 vs. 43 (0.02) | 86 vs. 40 (0.04) |
| Residual disease, R0 vs R1/R2, R1/R2% | 38 vs. 100 (0.005) | 36 vs. 100 (0.01) |
| Margin-positive % | 30 vs. 86 (0.03) | 36 vs. 80 (0.08) |
| Node positive % | 82 vs. 57 | 79 vs. 40 (0.1) |
| Perineural invasion-positive % | 94 vs. 71 | 93 vs. 60 (0.08) |
| Peripancreatic extension | 56 vs. 57 | 65 vs. 60 |
| Lymph vascular invasion- positive % | 63 vs. 49 | 57 vs. 20 (0.1) |
| Progression-free survival (in months) | 8 vs. 4 (0.04) | 8 vs. 4 (p=0.07) |
| Overall survival (in months) | 22 vs. 8 (0.08) | 17 vs. 8 |
*if the p-value is >0.1, it is not reported; MUC5AC -Serum MUC5AC level, CA19-9 – Serum carbohydrate antigen 19-9; #G1-2 vs. G3; nCR-near complete response; PR-partial response; NR- no response; OR – objective response; EC-M CS – extracellular MUC5AC composite score.
Table 5.
Post-surgery models for predicting survival.
| Term | P-value | HR | Lower 95% | Upper 95% |
|---|---|---|---|---|
| Post-surgery model for PFS – 1 | ||||
| Serum MUC5AC level | 0.0277 | 3.088526 | 1.137139 | 9.489153 |
| CA19-9 on the same day | 0.0236 | 1.000781 | 1.000114 | 1.00153 |
| Postoperative therapy | 0.09 | 3.088526 | ||
| Post-surgery model for OS – 1 | ||||
| Serum MUC5AC level | 0.0354 | 2.088487 | 0.974643 | 4.058677 |
| CA19-9 on the same day | 0.6035 | 0.999879 | 0.999356 | 1.000302 |
| CA19-9 at diagnosis | 0.0363 | 1.000531 | 0.999937 | 1.001009 |
| Post-surgery model for OS – 2 | ||||
| Serum MUC5AC level | 0.06 | 1.859388 | 0.881738 | 3.476052 |
| CA19-9 on the same day | 0.9 | 1.000004 | 0.999497 | 1.000404 |
| Post-surgery model for OS – 3 | ||||
| Serum MUC5AC level | 0.0288 | 3.340325 | 1.224686 | 12.52107 |
| CA19-9 on the same day | 0.4142 | 0.999796 | 0.999234 | 1.000254 |
| Postoperative therapy | 0.5903 | |||
PFS- progression-free survival, OS- overall survival.
Table 6.
Predicting recurrence using MUC5AC and CA19-9 post-surgery.
| Mean* sMUC5AC |
Median# sMUC5AC | Abnormal sCA19-9^ |
Mean sMUC5AC + sCA19-9 | Median sMUC5AC+ sCA19-9 | |
|---|---|---|---|---|---|
| Sensitivity (%) | 25 | 50 | 44 | 63 | 82 |
| Specificity (%) | 100 | 67 | 100 | 100 | 67 |
| PPV (%) | 100 | 89 | 100 | 100 | 93 |
| NPV (%) | 20 | 20 | 25 | 33 | 40 |
| Accuracy (%) | 37 | 53 | 53 | 68 | 79 |
PPV – positive predictive value, NPV – negative predictive value, sCA19-9 – serum carbohydrate antigen 19-9, sMUC5AC – serum MUC5AC, * Mean of 1.15ng/mL as cut-off, # median of 0.87 ng/mL as cut-off; ^ CA19-9 > 37 U/mL.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



