
Submitted:
10 September 2024
Posted:
11 September 2024
You are already at the latest version
Abstract
Background. Sarcopenia is characterized by progressive loss of muscle mass and function. It is often associated with frailty, a syndrome linked to physical disability and shortened survival in various diseases, including cancer patients. Low serum alanine aminotransferase (ALT) values, representing low muscle mass (sarcopenia), is a routine blood test that was shown to be associated with increased frailty and subsequently shortened survival in several cancers. In the current study, we aimed to test the association between low ALT and shorter survival in renal cell carcinoma (RCC) patients and survivors.
Methods. This was a retrospective analysis of RCC patients and survivors, both in and out-patients. We defined patients with sarcopenia as those presenting with ALT < 17 IU/L.
Results. We identified records of 3,012 patients diagnosed with RCC. The final cohort included 1,830 eligible patients (mean age 65.6 ± 13.3 years, 68% were men) of whom only 179 underwent surgical treatment. Out of the eligible cohort, 811 patients (44.3% ( had ALT < 17 IU/L. The mean ALT value of patients within the low ALT group was 11.79 IU/L while the mean value in the higher ALT level group was 24.44 IU/L (p < 0.001). Patients in the lower ALT group were older (67.9 vs. 63.7 years; p < 0.001) and had lower BMI (26.6 vs. 28; p < 0.001). In addition, patients with low ALT had lower hemoglobin values (12.14 vs. 12.91 g/dL; p < 0.001), higher serum creatinine (1.49 vs. 1.14; p < 0.001) and higher platelets to lymphocytes ratio (178 vs. 156; p < 0.001). In a univariate analysis, low ALT levels were associated with a 72% increase in mortality (95% CI 1.46-2.02, P < 0.001). In a multivariate model controlled for age, male gender, hemoglobin, platelets, LDH, neutrophil to lymphocytes ratio and platelets to lymphocytes ratio, low ALT levels were associated with a 27% increase in mortality (HR = 1.27, 95% CI 1.08 – 1.51; p = 0.005].
Conclusion. Low ALT values, indicative of sarcopenia and frailty, are associated with shortened survival of RCC patients and survivors and could potentially be applied for optimizing individual treatment decisions.
Keywords:
Renal Cell Carcinoma
; sarcopenia
; frailty
; alanine aminotransferase
; survival
; ALT
1. Background
1.1. Sarcopenia and Frailty Assessment amongst Cancer Patients
Assessment of patient’s physiological reserves is critical for treatment decision-making and estimation of prognosis in cancer patients and survivors. Many cancer patients are surgical candidates, often necessitating major debilitating surgery. Therefore, the Charlson comorbidity index (CCI) and similar indices are commonly used before surgery in cancer patients [1]. Those tools are primarily objective but rather complicated, and other methods for a holistic estimation of patients’ overall capacity are subjective (at times, physicians just “eyeball” their patients) and are therefore difficult to define and standardize. ECOG performance status is a longstanding and universal feature oncologists use prior to medical therapy or radiation. It is short, easily understood and readily estimated. However, It is physician assessed, therefore open to bias and may fail to integrate multimorbidity and frailty [2]. Sarcopenia is characterized by loss of muscle mass and is correlated with frailty, a syndrome that leads to increased likelihood of falls, disability, recurrent hospitalizations, and mortality [3,4,5]. In cancer patients, assessing sarcopenia and frailty improve the selection of patients eligible for major surgery and chemotherapy [6,7]. Both frailty and sarcopenia, have been identified as markers for shortened survival in cancer patients [8].
1.2. Alanine Aminotransferase as a Biomarker for Sarcopenia and Frailty
Alanine aminotransferase (ALT) is a well-known intracellular enzyme, primarily in the liver parenchyma, commonly monitored in routine bloodwork. It catalyzes pyruvate to alanine in the skeletal muscle and alanine to pyruvate in the liver [9]. Elevated ALT blood levels are commonly used as a biomarker for hepatocellular injury, but until recently little was known regarding the clinical significance of lower-than-normal ALT. Several studies have demonstrated that a below normal serum ALT activity, representing low muscle mass (sarcopenia, below expected for the same gender and age) is associated with shortened survival in older adults [10] and in patients hospitalized for various causes [11,12]. Furthermore, it was shown in several types of cancers, that low ALT values are associated with increased frailty and shortened survival [13,14,15,16].
1.3. Renal Cell Carcinoma Patients and Survivors
RCC is the sixth most frequently diagnosed cancer in men and the 10th in women. It’s incidence has been increasing, and up to 17% of patients suffer from distant metastases at the time of diagnosis. Well-established risk factors include older age, smoking, obesity, hypertension, and chronic kidney disease [17,18]. Treatment options for RCC have changed dramatically over the past two decades. Surgery, either radical nephrectomy or nephron-sparing is the mainstay of non-metastatic disease. However, active surveillance of small masses and tumor ablation are viable alternatives. The introduction of immune checkpoint inhibitors has significantly improved the overall survival of advanced RCC patients. Immune checkpoint inhibitors doublets or when administered in combination with a vascular endothelial growth factor tyrosine kinase inhibitor have (VEGFR-TKI) become the standard primary therapy in metastatic disease. Recently, immune checkpoint inhibitors are also offered for neoadjuvant and adjuvant treatment settings in patients undergoing surgery [19]. Prognostic models have been developed for localized disease, based on tumor stage, grade, subtype, and performance status. However, there is a poor level of evidence for their routine use. Traditional risk group assessment for patients with metastatic RCC also use performance status and some blood tests: Low hemoglobin, high calcium and high LDH blood levels are well established factors that help determine patients’ risk group classification. Newly recognized prognostic markers such as platelets count, white blood cell subtypes and platelets to lymphocytes ratio probably represent inflammatory response to the cancer. Newer markers in patients receiving targeted treatments are used routinely but have limited accuracy [20]. Despite being a disease of older and often frail adults, there is little data to guide treatment decisions in those patients with metastatic RCC. The recent approval of many new agents for this disease poses a clinical challenge: how to best utilize these drugs in a population, otherwise under-represented in clinical trials [21,22]. Few studies investigated more accurate parameters, including sarcopenia and frailty in RCC patients. Unsurprisingly, They found that both syndromes correlated with surgical and oncological outcomes [23,24,25,26]. Both need to be assessed at any stage of RCC to define the most suitable treatment strategy ranging from surveillance to aggressive treatment [27,28,29].
1.4. Aim of the Current Study
In the current study, we assessed the association between low serum activity of ALT, suggestive of sarcopenia and frailty, and shorter survival in a large cohort of renal cell carcinoma patients and survivors.
2. Methods
2.1. Study Cohort
In the current study cohort, we included men and women diagnosed with RCC who were treated in a large, tertiary medical center as outpatients or inpatients. Patients underwent either surgery, immunotherapy, targeted therapy, or active surveillance. Following approval by the local institutional review board (IRB approval # SMC-24-1252-D) and a waiver of informed consent in light of the retrospective nature of this study, all relevant patients’ characteristics, demographics, and clinical data were retrieved from their electronic medical records. We excluded patients with ALT activity levels higher than 40 IU that are generally associated with injured liver cells in various types of hepatitis, therefore not a reliable marker for striated muscles’ mass. The final cohort includes patients with ALT levels that were established at the time of RCC diagnosis. The primary outcome of the current study was all-cause mortality. Survival data were available for all subjects from the National Population Registry.
2.2. Statistical Analysis of Data
Normality of continuous variables’ distribution was determined using the Anderson-Darling and Shapiro-Wilk tests. If normally distributed, continuous variables were expressed as mean ± standard deviation (SD), and if skewed, by median with interquartile range (IQR). Categorical variables were presented as numbers and percentages (N; %). Continuous data were compared with the student’s t-test, and categorical data were compared using chi-square or Fisher exact tests. Log-rank test was used to analyze survival, later depicted using a Kaplan–Meier curve. Univariate cox regression modelling was used to determine the unadjusted Hazard Ratio (HR) for the primary outcome, and a multivariate model was constructed to examine the correlation and control for possible confounders. An association was considered statistically significant for a two-sided P value of less than 0.05. All analyses were performed using R software version 4.1.0 (R Foundation for Statistical Computing).
3. Results
A total of 3,012 renal cell carcinoma patients’ records were identified; after applying our exclusion criteria (available epidemiological data and ALT levels within the normal range), the final study population included 1,830 patients. We identified 179 patients who underwent surgical resection, either radical or partial nephrectomy. Within the whole eligible patients’ cohort, 811 (44.3%) had ALT activity levels that were lower than 17 IU/L, therefore, compatible with our definition of patients at high risk of suffering from sarcopenia and frailty. Figure 1 details patient consort flow and exclusion diagram.
The mean age for the entire cohort was 65.3 ± 13.3 years. Relevant patients’ demographics and clinical characteristics are detailed, according to their ALT levels (lower or ≥ 17 IU/L) in Table 1: patients in the low ALT group were, as expected, older (67.9 ± 13.5 vs. 63.7 ± 12.9 years), p < 0.001), had lower body mass index (BMI) values (26.6 ± 4.9) vs. 28 ± 5.1), p < 0.001), had higher percentage of diabetes mellitus (26% vs. 22%, p = 0.036), arterial hypertension (57% vs. 51%, p = 0.017) and atrial fibrillation (9.5% vs. 6.1%, p = 0.008). They also had statistically significant lower values of hemoglobin, higher values of blood creatinine and a higher ratio of platelet to lymphocyte counts. Patients in the lower ALT group had significantly shorter time of survival and/or loss of follow-up (1,822 ± 1,487 vs. 2,045 ± 1,457) days, p = 0.001).
3.1. Univariate Analysis
In a univariate analysis, low ALT levels were associated with a significant 72% increase in mortality (95% CI 1.46 - 2.02, P < 0.001). Figure 2 shows a Kaplan-Meir curve for the crude survival analysis according to ALT levels.
3.2. Multivariate Analysis
In a multivariate model (Table 2), low ALT levels were still associated with a 27% increased risk of mortality (HR = 1.27, 95% CI 1.08 – 1.51, p = 0.005).
4. Discussion
4.1. Personalized vs. Precision Medicine for Cancer Patients
The realms of advanced diagnostics and therapeutics in patients suffering from RCC have significantly advanced during the past several years. Nevertheless, most advancements were in the domains of precision medicine [30,31], addressing diseased tissue itself rather than in the domain of personalized medicine, that is, addressing the patient rather than the disease. Moreover, some authors describe the movement from precision to personalized medicine in the sense of deepening our understanding of the molecular structure of the cancerous tissue [32], with some authors even bundling both precision and personalized medicine together, namely, PPM [33]. The authors of the current manuscript defy this concept, seeing personalized medicine as taking a “zoom-out” from the diseased tissue to the whole gestalt of patient. We concentrate on personalized medicine in terms of sarcopenia and frailty assessment.
4.2. Sarcopenia and Frailty of RCC Patients
As presented at the forefront of this article, sarcopenia, and frailty are a pillar of morbidity in cancer patients as a whole and in RCC patients precisely [25,28]. Massaad et al. evaluated the relative effects of different patients’ characteristics on clinical outcomes among post-operative patients with RCC metastasis. Amongst other variables, sarcopenia and frailty were also assessed [34]. Sarcopenia was assessed by measuring the L3 skeletal muscle index (L3-SMI) on axial CT images at the level of lumbar L3 vertebra, while frailty was assessed using the modified frailty index. Their results found no significant association between these measures and patients’ overall survival. We hypothesize that these findings stem from the fact that all patients were already metastatic, as opposed to our cohort of patients with metastatic and localized disease. Moreover, although strongly validated, their methods for sarcopenia and frailty assessment were rather complex.
Low ALT assessment as part of personalized medicine offered for RCC patients.
Similarly to our groups’ findings in patients with other urinary system malignancies (urinary bladder and prostate), we showed that low ALT blood activity, representing low total body striated muscle mass, is associated with poor prognosis. Relying on previous findings that confirmed the association of low ALT with sarcopenia and frailty, we similarly ascertain RCC patients, that low ALT is a reliable biomarker for sarcopenia and frailty.
5. Conclusions
Low ALT blood levels, measured in RCC patients and survivors, are associated with sarcopenia and frailty. This finding should be assimilated into the scheme of personalized medicine for RCC patients as part of their future plans for surgery, medical therapy, and prognostication.
6. Limitations
This was a single-center, retrospective study and therefore, our conclusions necessitate further verification in larger, multi-centered, preferably prospective studies.
References
- Sinha P, Kallogjeri D, Piccirillo JF. Assessment of comorbidities in surgical oncology outcomes. J Surg Oncol [Internet]. 2014 Oct 1 [cited 2023 Aug 23];110(5):629–35. Available from: https://pubmed.ncbi.nlm.nih.gov/25100618/.
- Simcock R, Wright J. Beyond Performance Status. Clin Oncol (R Coll Radiol) [Internet]. 2020 Sep 1 [cited 2024 Apr 30];32(9):553–61. Available from: https://pubmed.ncbi.nlm.nih.gov/32684503/.
- Cruz-Jentoft AJ, Sayer AA. Sarcopenia. Lancet [Internet]. 2019 Jun 29 [cited 2023 Aug 23];393(10191):2636–46. Available from: https://pubmed.ncbi.nlm.nih.gov/31171417/.
- Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing [Internet]. 2019 Jan 1 [cited 2023 Aug 23];48(1):16–31. Available from: https://pubmed.ncbi.nlm.nih.gov/30312372/.
- Picca A, Coelho-Junior HJ, Calvani R, Marzetti E, Vetrano DL. Biomarkers shared by frailty and sarcopenia in older adults: A systematic review and meta-analysis. Ageing Res Rev [Internet]. 2022 Jan 1 [cited 2023 Aug 23];73. Available from: https://pubmed.ncbi.nlm.nih.gov/34839041/.
- Korc-Grodzicki B, Downey RJ, Shahrokni A, Kingham TP, Patel SG, Audisio RA. Surgical considerations in older adults with cancer. J Clin Oncol [Internet]. 2014 Aug 20 [cited 2023 Feb 6];32(24):2647–53. Available from: https://pubmed.ncbi.nlm.nih.gov/25071124/.
- Ryan AM, Prado CM, Sullivan ES, Power DG, Daly LE. Effects of weight loss and sarcopenia on response to chemotherapy, quality of life, and survival. Nutrition [Internet]. 2019 Nov 1 [cited 2023 Aug 26];67–68. Available from: https://pubmed.ncbi.nlm.nih.gov/31522087/.
- Au PCM, Li HL, Lee GKY, Li GHY, Chan M, Cheung BMY, et al. Sarcopenia and mortality in cancer: A meta-analysis. Osteoporos Sarcopenia [Internet]. 2021 Mar [cited 2023 Feb 6];7(Suppl 1):S28–33. Available from: https://pubmed.ncbi.nlm.nih.gov/33997306/.
- Liu Z, Que S, Xu J, Peng T. Alanine aminotransferase-old biomarker and new concept: a review. Int J Med Sci [Internet]. 2014 Jun 26 [cited 2023 Feb 7];11(9):925–35. Available from: https://pubmed.ncbi.nlm.nih.gov/25013373/.
- Ramaty E, Maor E, Peltz-Sinvani N, Brom A, Grinfeld A, Kivity S, et al. Low ALT blood levels predict long-term all-cause mortality among adults. A historical prospective cohort study. Eur J Intern Med [Internet]. 2014 Dec 1 [cited 2023 Feb 7];25(10):919–21. Available from: https://pubmed.ncbi.nlm.nih.gov/25468741/.
- Ruhl CE, Everhart JE. The association of low serum alanine aminotransferase activity with mortality in the US population. Am J Epidemiol [Internet]. 2013 Dec [cited 2023 Feb 7];178(12):1702–11. Available from: https://pubmed.ncbi.nlm.nih.gov/24071009/.
- Segev A, Itelman E, Avaky C, Negru L, Shenhav-Saltzman G, Grupper A, et al. Low ALT Levels Associated with Poor Outcomes in 8700 Hospitalized Heart Failure Patients. J Clin Med [Internet]. 2020 Oct 1 [cited 2023 Aug 29];9(10):1–10. Available from: https://pubmed.ncbi.nlm.nih.gov/33008125/.
- Uliel N, Segal G, Perri A, Turpashvili N, Kassif Lerner R, Itelman E. Low ALT, a marker of sarcopenia and frailty, is associated with shortened survival amongst myelodysplastic syndrome patients: A retrospective study. Medicine [Internet]. 2023 Apr 25 [cited 2023 May 10];102(17):e33659. Available from: http://www.ncbi.nlm.nih.gov/pubmed/37115069.
- Laufer M, Perelman M, Sarfaty M, Itelman E, Segal G. Low Alanine Aminotransferase, as a Marker of Sarcopenia and Frailty, Is Associated with Shorter Survival Among Prostate Cancer Patients and Survivors. A Retrospective Cohort Analysis of 4064 Patients. Eur Urol Open Sci [Internet]. 2023 Sep 1 [cited 2023 Oct 28];55:38–44. Available from: https://pubmed.ncbi.nlm.nih.gov/37693730/.
- Laufer M, Perelman M, Segal G, Sarfaty M, Itelman E. Low Alanine Aminotransferase as a Marker for Sarcopenia and Frailty, Is Associated with Decreased Survival of Bladder Cancer Patients and Survivors-A Retrospective Data Analysis of 3075 Patients. Cancers (Basel) [Internet]. 2023 Jan 1 [cited 2024 Apr 30];16(1). Available from: https://pubmed.ncbi.nlm.nih.gov/38201601/.
- Hellou T, Dumanis G, Badarna A, Segal G. Low Alanine-Aminotransferase Blood Activity Is Associated with Increased Mortality in Chronic Lymphocytic Leukemia Patients: A Retrospective Cohort Study of 716 Patients. Cancers (Basel) [Internet]. 2023 Sep 17 [cited 2023 Oct 28];15(18):4606. Available from: https://pubmed.ncbi.nlm.nih.gov/37760575/.
- Capitanio U, Bensalah K, Bex A, Boorjian SA, Bray F, Coleman J, et al. Epidemiology of Renal Cell Carcinoma. Eur Urol [Internet]. 2019 Jan 1 [cited 2024 May 1];75(1):74–84. Available from: https://pubmed.ncbi.nlm.nih.gov/30243799/.
- Bukavina L, Bensalah K, Bray F, Carlo M, Challacombe B, Karam JA, et al. Epidemiology of Renal Cell Carcinoma: 2022 Update. Eur Urol [Internet]. 2022 Nov 1 [cited 2024 May 1];82(5):529–42. Available from: https://pubmed.ncbi.nlm.nih.gov/36100483/.
- Chen YW, Wang L, Panian J, Dhanji S, Derweesh I, Rose B, et al. Treatment Landscape of Renal Cell Carcinoma. Curr Treat Options Oncol [Internet]. 2023 Dec 1 [cited 2024 May 1];24(12):1889–916. Available from: https://pubmed.ncbi.nlm.nih.gov/38153686/.
- Klatte T, Rossi SH, Stewart GD. Prognostic factors and prognostic models for renal cell carcinoma: a literature review. World J Urol [Internet]. 2018 Dec 1 [cited 2024 May 1];36(12):1943–52. Available from: https://pubmed.ncbi.nlm.nih.gov/29713755/.
- Maia MC, Adashek J, Bergerot P, Almeida L, dos Santos SF, Pal SK. Current systemic therapies for metastatic renal cell carcinoma in older adults: A comprehensive review. J Geriatr Oncol [Internet]. 2018 May 1 [cited 2024 May 2];9(3):265–74. Available from: https://pubmed.ncbi.nlm.nih.gov/29249644/.
- Esther J, Hale P, Hahn AW, Agarwal N, Maughan BL. Treatment Decisions for Metastatic Clear Cell Renal Cell Carcinoma in Older Patients: The Role of TKIs and Immune Checkpoint Inhibitors. Drugs Aging. 2019 May 1;36(5):395–401.
- Ueki H, Hara T, Okamura Y, Bando Y, Terakawa T, Furukawa J, et al. Association between sarcopenia based on psoas muscle index and the response to nivolumab in metastatic renal cell carcinoma: A retrospective study. Investig Clin Urol. 2022;63(4):415–24.
- Noguchi G, Kawahara T, Kobayashi K, Tsutsumi S, Ohtake S, Osaka K, et al. A lower psoas muscle volume was associated with a higher rate of recurrence in male clear cell renal cell carcinoma. PLoS One [Internet]. 2020 Jan 1 [cited 2024 May 2];15(1). Available from: https://pubmed.ncbi.nlm.nih.gov/31895931/.
- Ishihara H, Nishimura K, Ikeda T, Fukuda H, Yoshida K, Iizuka J, et al. Impact of body composition on outcomes of immune checkpoint inhibitor combination therapy in patients with previously untreated advanced renal cell carcinoma. Urol Oncol [Internet]. 2024 [cited 2024 May 2]; Available from: https://pubmed.ncbi.nlm.nih.gov/38653590/.
- Rosiello G, Larcher A, Fallara G, Cignoli D, Re C, Martini A, et al. A comprehensive assessment of frailty status on surgical, functional and oncologic outcomes in patients treated with partial nephrectomy—A large, retrospective, single-center study. Urologic Oncology: Seminars and Original Investigations. 2023 Mar 1;41(3):149.e17-149.e25.
- Courcier J, De La Taille A, Lassau N, Ingels A. Comorbidity and frailty assessment in renal cell carcinoma patients. World J Urol [Internet]. 2021 Aug 1 [cited 2024 May 1];39(8):2831–41. Available from: https://pubmed.ncbi.nlm.nih.gov/33616708/.
- Campi R, Berni A, Amparore D, Bertolo R, Capitanio U, Carbonara U, et al. Impact of frailty on perioperative and oncologic outcomes in patients undergoing surgery or ablation for renal cancer: a systematic review. Minerva urology and nephrology [Internet]. 2022 Apr 1 [cited 2024 Mar 16];74(2):146–60. Available from: https://pubmed.ncbi.nlm.nih.gov/34714036/.
- Walach MT, Wunderle MF, Haertel N, Mühlbauer JK, Kowalewski KF, Wagener N, et al. Frailty predicts outcome of partial nephrectomy and guides treatment decision towards active surveillance and tumor ablation. World J Urol. 2021 Aug 1;39(8):2843–51.
- Sharma R, Kannourakis G, Prithviraj P, Ahmed N. Precision Medicine: An Optimal Approach to Patient Care in Renal Cell Carcinoma. Front Med (Lausanne) [Internet]. 2022 Jun 14 [cited 2024 May 17];9:766869. Available from: /pmc/articles/PMC9237320/.
- Massari F, Santoni M, Di Nunno V, Cimadamore A, Battelli N, Scarpelli M, et al. Quick steps toward precision medicine in renal cell carcinoma. Expert Rev Precis Med Drug Dev [Internet]. 2018 Sep 3 [cited 2024 May 17];3(5):283–5. Available from: https://www.tandfonline.com/doi/abs/10.1080/23808993.2018.1510289.
- Gambardella V, Tarazona N, Cejalvo JM, Lombardi P, Huerta M, Roselló S, et al. Personalized Medicine: Recent Progress in Cancer Therapy. Cancers (Basel) [Internet]. 2020 Apr 1 [cited 2024 May 17];12(4). Available from: /pmc/articles/PMC7226371/.
- Krzyszczyk P, Acevedo A, Davidoff EJ, Timmins LM, Marrero-Berrios I, Patel M, et al. The growing role of precision and personalized medicine for cancer treatment. Technology (Singap World Sci) [Internet]. 2018 Sep [cited 2024 May 17];6(3–4):79. Available from: /pmc/articles/PMC6352312/.
- Massaad E, Saylor PJ, Hadzipasic M, Kiapour A, Oh K, Schwab JH, et al. The effectiveness of systemic therapies after surgery for metastatic renal cell carcinoma to the spine: a propensity analysis controlling for sarcopenia, frailty, and nutrition. J Neurosurg Spine [Internet]. 2021 Sep 1 [cited 2024 May 17];35(3):356–65. Available from: https://pubmed.ncbi.nlm.nih.gov/34171829/.
Figure 1.
Consort flow diagram of study patients.
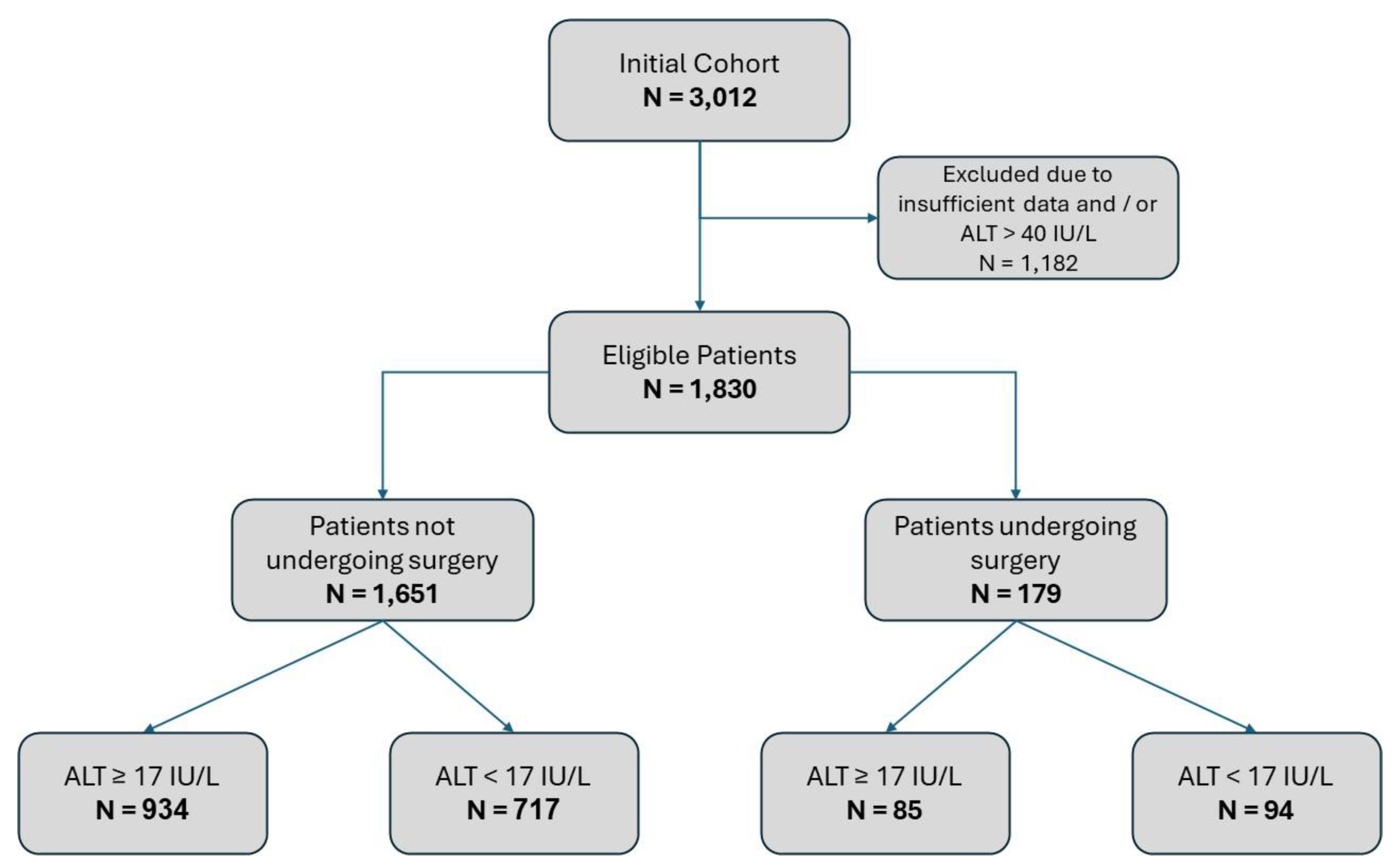
Figure 2.
Kaplan Meir Survival Analysis according to ALT levels.
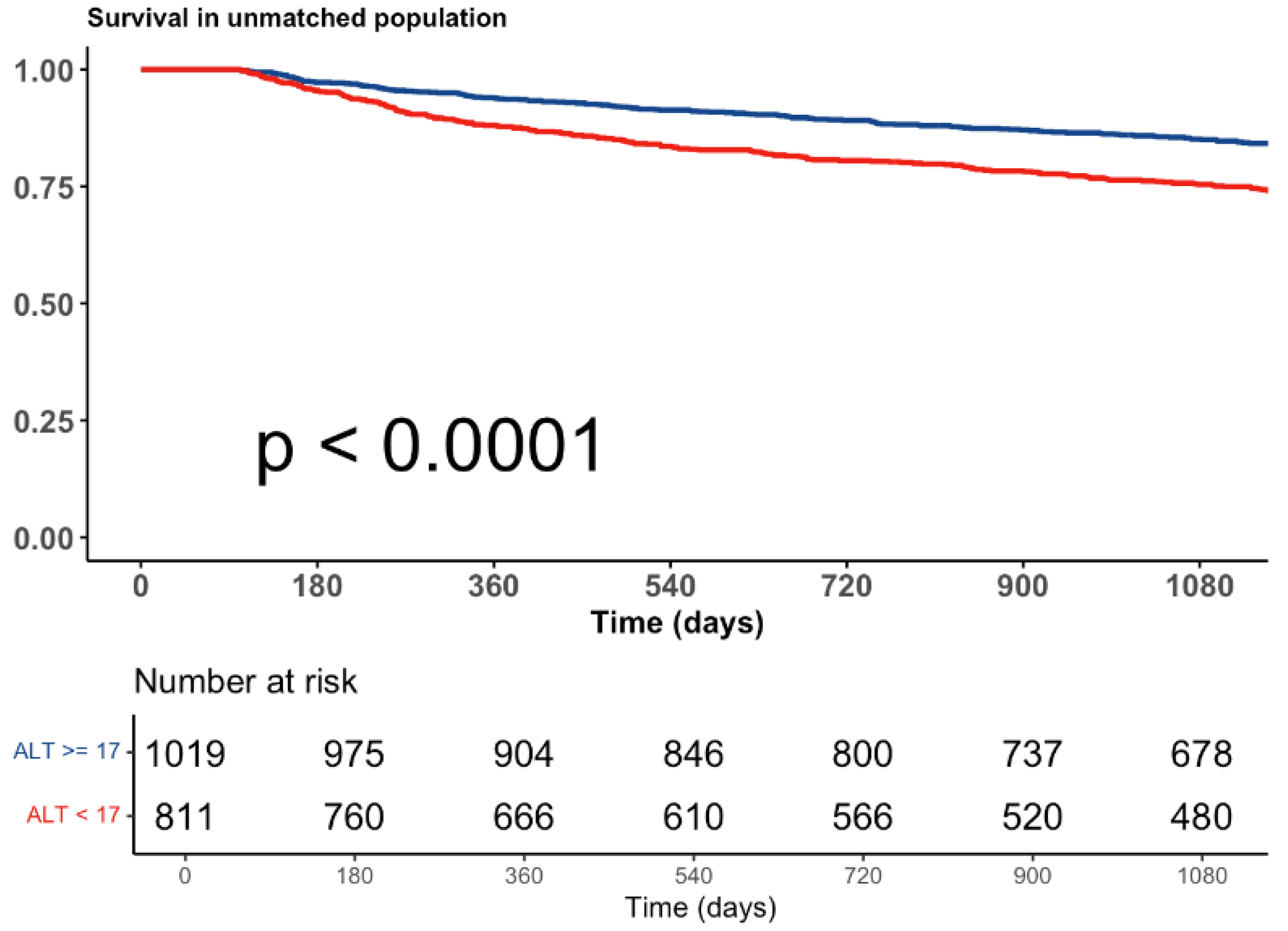

Table 1.
Patients’ characteristics according to ALT serum activity level.
| Whole study cohort N = 1,830 |
ALT ≥ 17 IU/L N = 1,019 |
ALT < 17 IU/L N = 811 |
P value | |
|---|---|---|---|---|
| ALT (Mean IU/L [SD]) | 18.83 (8.01) | 24.44 (6.07) | 11.79 (3.04) | < 0.001 |
| Patients’ demographics | ||||
| Age (years, Mean [SD]) | 65.6 (13.3) | 63.7 (12.9) | 67.9 (13.5) | < 0.001 |
| Male gender (N [%]) | 1,238 (68) | 704 (69) | 534 (66) | 0.155 |
| BMI (Mean [SD]) | 27.4 (5) | 28 (5.1) | 26.6 (4.9) | < 0.001 |
| Clinical background | ||||
| Diabetes Mellitus (N [%]) | 428 (23) | 219 (22) | 209 (26) | 0.036 |
| Dyslipidemia (N [%]) | 657 (36) | 379 (37) | 278 (34) | 0.214 |
| Arterial Hypertension (N [%]) | 980 (54) | 520 (51) | 460 (57) | 0.017 |
| COPD (N [%]) | 113 (6) | 53 (5.2) | 60 (7.4) | 0.065 |
| CHF (N [%]) | 67 (3.7) | 30 (2.9) | 37 (4.6) | 0.088 |
| Atrial Fib. (N [%]) | 139 (8) | 62 (6.1) | 77 (9.5) | 0.008 |
| S/P Stroke (N [%]) | 95 (5.2) | 47 (4.6) | 48 (5.9) | 0.252 |
| Laboratory parameters | ||||
| Albumin (gr/dL, Mean [SD]) | 3.9 (1.38) | 3.93 (0.58) | 3.86 (1.97) | 0.32 |
| Hemoglobin (gr/dL, Mean [SD]) | 12.57 (2.02) | 12.91 (1.9) | 12.14 (2.09) | < 0.001 |
| Platelets (K/mcl, Mean [SD]) | 236 (95) | 233 (91) | 239 (100) | 0.17 |
| Neut. / Lymph. (Mean [SD]) | 4.87 (5.85) | 4.67 (5.06) | 5.12 (6.71) | 0.106 |
| Plt. / Lymph. (Mean [SD]) | 166 (118) | 156 (115) | 178 (121) | < 0.001 |
| LDH (IU/L, Mean [SD]) | 243 (149) | 245 (159) | 240 (135) | 0.496 |
| Calcium (mg/dL, Mean [SD]) | 7.69 (3.43) | 7.56 (3.56) | 7.85 (3.26) | 0.069 |
| Creatinine (mg/dL, Mean [SD]) | 1.29 (1.08) | 1.14 (0.69) | 1.49 (1.4) | < 0.001 |
| Time to death / end of follow-up (days, Mean [SD]) | 1,946 (1,474) | 2,045 (1,457) | 1,822 (1,487) | 0.001 |
Table 2.
Multivariate Analysis.
| Patient characteristics | HR (95% CI) | P Value |
|---|---|---|
| ALT < 17 IU/L | 1.27 [1.08 – 1.51] | 0.005 |
| Age | 1.05 [1.05 – 1.06] | < 0.001 |
| Male gender | 1.6 [1.33 – 1.92] | < 0.001 |
| Hemoglobin (g/dL) | 0.84 [0.81 – 0.87] | < 0.001 |
| Platelets (K/mcl) | 1.00 [1.00 – 1.00] | 0.003 |
| LHD (IU/L) | 1.00 [1.00 – 1.00] | < 0.001 |
| Platelets / Lymphocytes | 1.00 [1.00 – 1.00] | 0.007 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



