Submitted:
09 September 2024
Posted:
10 September 2024
You are already at the latest version
Abstract
Background: Several trace minerals have been shown to be associated with thyroid cancer. However, there is a paucity of data on the characteristics of thyroid nodules in different mineral rich regions of the Democratic Republic of Congo (DRC). The objective of this study is to establish the spectrum of thyroid nodules in different regions of the most mineral wealthy country in the world. Method: We conducted a cross-sectional study, performing descriptive statistics and logistic regression with a p value < 0.05 deemed of statistical significance. We enrolled 529 patients diagnosed with thyroid nodules between 2005 and 2019 in two of the richest provinces in minerals (Katanga and South Kivu) and the capital city, Kinshasa. Results: The mean age was 44.2±14.6 years with a female predominance, with a female to male ratio of 5.4. 66.5% of patients had a family history of thyroid disease. 74 patients had simple nodules, whereas 455 had multiple nodules. 87.7% of patients with nodules were euthyroid. The nodules mostly presented a solid structure (72.2%), hypoechogenicity (84.5%), a macronodule (59.8%), calcification (14.4%) and lymphadenopathy (15.5%). 22.3% of these nodules had a malignant character. The independent factors associated with this malignancy were age ≥60 years (aOR=2.81), Katanga as province of origin (aOR=8.19), solid echostructure (aOR=7.69), hypoechogenicity (aOR=14.19), macronodule (aOR=9.13), calcification (aOR=2.6) and the presence of adenopathy (aOR=6.94). Conclusion: By the way of this first of its kind study, we demonstrated that thyroid nodules were more likely to be malignant if found in patients originating from mineral rich region of Katanga. This high frequency of malignancy in mineral rich regions requires measures aimed at early detection in this population, lower threshold for suspicion of malignancy and adequate training of doctors involved in the management of these patients. This study paves the way for future, more extensive and well-funded studies to better understand the relationship of heavy metals and thyroid cancer incidence in the richest country in heavy metals in the world.
Keywords:
Thyroid
; malignancy
; mineral density
; kinshasa
; Katanga
; nodule
Introduction:
Thyroid nodules are very common and usually come to clinical attention when noted by the patient; during routine physical examination; or when incidentally noted during a radiologic procedure, such as carotid ultrasonography, neck or chest computed tomography (CT), magnetic resonance imaging (MRI), or positron emission tomography (PET) scanning have the same risk of malignancy as palpable nodules of the same size [1,2,3]. The history and physical examination have a low accuracy for predicting cancer. However, there are several features of the history that suggest an increased likelihood of malignancy, such as a history of rapid growth of a neck mass, childhood head and neck irradiation, total body irradiation for bone marrow transplantation, family history of thyroid cancer, or thyroid cancer syndromes [1,2,3].
Thyroid nodules are selected for Fine Needle Aspiration (FNA) biopsy based on suspicious ultrasonographic characteristics rather than size alone, as the presence of suspicious ultrasound features is more predictive of malignancy [4,5]. There are several approaches used to categorize thyroid nodules for likelihood of malignancy and to select nodules for biopsy. The American College of Radiology has proposed a system (Thyroid Imaging, Reporting and Data System [TIRADS]) for selecting nodules for FNA [6]. A similar, but not identical system has been proposed in Europe (European Thyroid Imaging, Reporting and Data System [EU-TIRADS]). This latter system has recently been validated in the Congolese population (referefence)and plays a key role in the assessment of thyroid nodules for malignancy; given the fact that FNA is not readily available in the country [7].
The most recent and up to date study on the spectrum of thyroid nodules in the DRC was conducted in a single institution and in a province that is not known to have a soil rich in trace minerals [8]. Several studies around the globe have linked fixed exposure to multiple elements to the development of thyroid cancer [9,10,11]. However, to the best of our knowledge, there are currently no studies on thyroid nodules in the DRC involving patients of mineral rich provinces. Thus, the need of the current study. The objective of this study is to establish the spectrum of thyroid nodules in the DRC, involving patients of provinces rich in minerals in an attempt to improve the management of thyroid nodules in those populations.
Materials and Methods:
This is a cross-sectional and analytical study of 529 records of patients with thyroid nodules, operated on during the period from 2005 to 2019; having benefited from a thyroid ultrasound and an anatomopathology examination in 35 hospitals in Kinshasa, two in Bukavu and one in Katanga. All available records were reviewed. The sampling was exhaustive.
2.1. Variables of Interest
Using a previously established data sheet, investigators sufficiently trained and aware of the objectives of the study collected the following data: province of residence, age, sex, marital status, clinical parameters (history of thyroid cancer in the family, reasons for consultation, parity , gestation, abortion, duration of the mass, arterial pressure, heart rate, observation of the mass, lymphadenopathy on clinical examination), clinical diagnosis, ultrasound parameters (total volume of the thyroid gland, echostructure, echogenicity, presence of nodule , size, calcification, lymphadenopathy on ultrasound, ultrasound diagnosis) and histopathological diagnosis.
Only files containing all the information on the variables of interest described were retained for the final analyses. The period of analysis was guided by the availability of registers in all the laboratories of the hospitals mentioned above.
2.2. Data Analysis
The statistical analyzes of the data were carried out using Statistical Package for the Social Sciences (SPSS) for Windows version 24 software. The descriptive analyzes carried out are the mean, standard deviation for the quantitative data with Gaussian distribution and the absolute (n) and relative (%) frequencies for categorical data. Pearson's Chi-square or Fisher's exact test was performed to compare the proportions (%). The student’s t test was performed to compare the means. Logistic regression was used to search for factors associated with cancerous thyroid nodules in univariate and multivariate analysis with OR calculation and their 95% confidence interval to estimate the degree of association. For all the tests used, the value of p < 0.05 was considered as the threshold of statistical significance.
The notion of confidentiality was essential for our study, the data was collected anonymously and was used only for the drafting of this work.
Results:
Types of thyroid nodules can be found in Figure 1. A total of 529 nodules were identified in the study population, including 74 (14%) single nodules, 47 (8.9%) binodules and 408 (77.1%) multinodules.
The socio-demographic characteristics of nodules are illustrated in Table 1 and show that the mean age of patients was 44.2±14.6 years with a predominance of female sex (84.4%; female to male ratio of 5. 4). Married people were more represented (75.1%) and a large number of samples came from Kinshasa (88.5%). The sociodemographic characteristics of single and multiple nodules were similar (p>0.05).
Multiparas were more represented, 66.5% of patients had a family history of thyroid pathology, most often first degree (58.2%). On clinical examination, 95.1% of patients had antero-cervical mass, 35.3% were obese, 8.7% had lymphadenopathy and 87.7% had normal thyroid function. No significant difference was found between the single and multiple nodules compared to the clinic. As seen in Table 2.
The sonographic characteristics of nodules can be seen in Table 3 showed a predominance of solid echostructure (72.2%), hypoechogenicity (84.5%), a macronodule (59.8%), microcalcification (14.4%) and adenopathy (15 .5%). Anatomopathological analysis of nodules as seen in Table 4, shows that 77.7% of nodules were benign and 22.3% malignant. Colloid goiter was predominant in the benign nodule (73.5%) and papillary carcinoma in the malignant nodule (66.9%); anaplastic carcinoma represented 7.6% of malignant nodules.
Table 5, which breaks down all the nodules according to their pathology character, indicates that the frequency of malignant nodules was significantly higher in patients aged >60 years (p=0.003); from Katanga (p=0.044), in patients with a family history of thyroid pathology (p=0.002) and in patients with cervical lymphadenopathy (p<0.001). Table 6 indicates that the different ultrasound characteristics of the patients were significantly different between the benign and malignant nodules (p<0.05) except for the number of nodules where the difference was not statistically significant (p=0.284).
The risk factors associated with nodule malignancy in univariate analysis were age ≥60 years, Katanga as province of origin, family history of thyroid pathology, presence of clinical and ultrasound lymphadenopathy, solid echostructure, hypoechogenicity, macronodule and calcification.
After adjustment in multivariate analysis, age ≥60 years (aOR: 2.81; 95% CI: 1.14-6.94, p=0.025), Katanga as province of origin (aOR: 8.19; 95% CI: 1.14-12.45, p=0.036), presence of ultrasound lymphadenopathy (aOR: 6.94; 95% CI: 2.79-17.25, p<0.001), solid echostructure( aOR: 7.69; 95% CI: 2.40-24.58, p=0.001), hypoechogenicity (aOR: 14.19; 95% CI: 1.60-25.93, p=0.017), macronodule (aOR: 9.13; 95% CI: 4.19-19.89, p<0.001) and calcification (aOR: 2.60; 95% CI: 1.19-5.7, p=0.017) were major factors independently associated with nodule malignancy (Table 7).
Discussion:
Our nationally representative study revealed that there was a predominance of thyroid nodules among females compared to males. Most patients with a thyroid nodule had a normal thyroid function. Solid structure, hypoechogenicity, micronodule, microcalcification and lymphadenopathy were common ultrasound features among nodules. Advanced age, living in Katanga province, solid echostructure, hypoechogenicity, macronodule, microcalcification and adenopathy were found to be risk factors for malignancy in thyroid nodules.
The clinical importance of the thyroid nodule evaluation is primarily related to the need to exclude thyroid cancer, which is present in 4 to 6.5 percent of thyroid nodules [12]. The female gender and iodine deficiency are two well recognized risk factors for the development of thyroid nodules [8,13]. Our study revealed a female predominance in the occurrence of thyroid nodules which is consistent with findings in the literature. Furthermore, it has been proven in the literature that thyroid nodules are common in the Congolese population, mainly due to the lack of adequate iodine supplement in the typical Congolese meals [8]. The prevalence of cancer is higher in several groups such as children, adults younger than 30, patients with a history of head and neck irradiation, and patients with a family history of thyroid cancer [12,14,15]. Our study revealed a higher frequency of thyroid cancer in patients older than 60 years of age which is similar to the findings of the study done by Kwong et al. [16] but differs from results found in the Sicilian study conducted by Belfiore et al. [15] which found that adults younger than 30 years old were at highest risk of malignant nodules.
Other factors such as exposure to trace minerals and heavy metals have been associated with the development of thyroid cancer [9,10,11]. A study by Petrosino et al. [17] revealed that all patients with head and neck cancer enlisted for the study had heavy metal and polychlorinated biphenyls (PCB) blood levels at least twice the maximum reference level. The levels of heavy metals in hair were at least double the maximum reference. In contrast, all healthy volunteers enrolled showed no significant levels for either metals or PCBs. A study done at Yale University found that urinary cadmium, antimony and tungsten were significantly associated with increased odds of thyroid dysfunctions, including cancer [18]. A similar study done in south Korea among residents living near national industrial complexes revealed that urinary mercury concentration was positively associated with the risk of thyroid cancer among residents living near national industrial complexes [19]. No such study has been carried out in the DRC. Furthermore, no studies have been done to evaluate the frequency of thyroid cancer in different regions of the country rich in heavy metals. DRC is endowed with exceptional natural resources, including minerals such as cobalt, copper, Coltan, mercury, tantalum, tin, gold, lithium, tungsten, manganese, uranium, and many others [20]. The natural resources are not equally distributed within the country, with some regions containing more natural resources than others.
Katanga province is one of the wealthiest regions in the world in terms of natural resources. It has 34% of the world's cobalt reserves and 10% of the world's copper. It is also rich in zinc, lead, uranium, tin, manganese, chromium, mercury, cadmium, silver, gold, germanium, and coal. A 2009 study in the province found substantial exposure to several metals, especially in children. The urinary Cobalt concentrations found in this population are the highest ever reported for a general population [21]. In 2016, researchers discovered extensive metal contamination in the fish in Katanga's Lake Tshangalele, near mining and other metallurgical operations in Likasi, in species commonly eaten by the local population [22]. However, no studies have been carried out in the country to compare the frequency of malignant thyroid nodules in this region and in regions not rich in mineral resources. Our study found that 44.4 % of nodules in the Katanga region were malignant, whereas only 22.2% were malignant in Kinshasa. This trend shows a possible important role played by heavy metals contamination in the carcinogenesis affecting this population.
Although ultrasonography yields limited diagnostic information, it provides extremely valuable and pertinent information about the thyroid gland, its diseases, and adjacent structures. This cumulative ultrasonography evidence, in context, can significantly augment diagnosis as well as clinical, surgical, radiation, ablation, and other management [23,24,25]. Malignant thyroid nodules often have a hypoechoic appearance on ultrasound as evidenced by the studies by Solbiati et al. [26] and Cochand-Priollet et al. [27]. Microcalcifications may be present in both benign and malignant nodules and are therefore only partially predictive of histopathology, however, in a Greek study by Kakkos et al., the prevalence of cancer was significantly higher when there were calcium flecks in a nodule [28]. Our study revealed that hypoechogenicity and microcalcifications were associated with malignancy, findings similar to the current literature. The uniformity of the internal structure of a nodule is not a useful indicator for diagnosis of cancer; cancers may be either entirely solid or contain some component of cystic content. In general, the larger the cystic component, the less likely the nodule is to be malignant [29]. As evidenced in the literature, solid echostructure was associated with malignancy in our study. Large nodule diameter and volume predicts a higher likelihood of thyroid cancer and prognosis [23,30,31,32]. In a large study, conducted by Angell et al., of over 20,000 thyroid nodules, for every centimeter increase in size of a nodule over 1 cm, there was a 15 to 30 percent escalation in malignancy risk [23].
Thyroid follicular epithelial-derived cancers are divided into three categories which are papillary (85%), follicular (12%) and anaplastic (<3%). Papillary and follicular cancers are considered differentiated cancers. Most anaplastic (undifferentiated) cancers appear to arise from differentiated cancers [33]. Papillary and follicular cancers were the most frequent in our study, and anaplastic cancers were higher in frequency than in the literature (7.6 % VS <3%). One could speculate that given lack of access to healthcare, most of these patients with undifferentiated thyroid cancers had longstanding differentiated carcinomas but failed to seek medical attention as routine visit is not part of the Congolese culture.
This study has several limitations, such as missing data or loss of records inherent to its retrospective design, the multiplicity of types of ultrasound devices and operators and the lack of a validated ultrasound examination protocol for the thyroid gland. Furthermore, there is bias since we only took into consideration the patients who had carried out the anatomopathology while those who had not carried out one, were not included in this study. This may have influenced a high frequency of cancers and certain histological types. Finally, limitations in diagnostic facilities in data reporting in a resource-poor health care facility are also potentially limiting.
Despite these limitations this study has the merit of being the first of its kind addressing a very important subject in a country rich in mineral resources.
In conclusion, by the way of this first of its kind study, we demonstrated that the mineral rich region of Katanga was associated with higher frequency of thyroid malignancy. These findings are especially important in a population that lives below the poverty line. Although routine screening for thyroid cancer in a population at low risk for thyroid cancer is not cost effective, such strategy should be implemented in the national guidelines for management of patients in regions rich in mineral resources; especially since there was a higher frequency of undifferentiated cancers. This study paves the way for larger and well-funded studies to confirm these results and help shape the national guidelines.
Author Contributions
John Bukasa-Kakamba, Ayrton Bangolo, Pascal Bayauli, Vignesh K. Nagesh, Maria J. Mou, Princejeet S. Chahal, Sindhuja Chindam, Branly Mbunga, Taieba Mushfiq, Abhishek Thapa, Nidhi L. Rao, Isis Kapinga Kalambayi, Rahul Y. Rajesh, Ipek B. Sarioguz, Vishal K.R. Thoomkuntla, Shamsul Arefin, Navneet Kaur, Manasse Bukasa Mutombo, Satyajeet Singh, Natalia Muto, Surya Vamsi, Pujita Mallampalli, Aliocha Nkodila, Simcha Weissmam, and Jean Rene M'Buyamba-Kabangu searched the literature, wrote, and revised the manuscript. All authors certify that they contributed sufficiently to the intellectual content and data analysis. Each author has reviewed the final version of the manuscript and approves it for publication.
Funding Sources
No Funding was received.
Data Availability Statement
Datasets and script files of this research are available as per request to the corresponding author.
Conflicts of Interest Statement
No potential conflict of interest was reported by the authors.
References
- Steele, S.R.; Martin, M.J.; Mullenix, P.S.; Azarow, K.S.; Andersen, C.A. The significance of incidental thyroid abnormalities identified during carotid duplex ultrasonography. Arch Surg. 2005, 140, 981–5. [Google Scholar] [CrossRef] [PubMed]
- Hagag, P.; Strauss, S.; Weiss, M. Role of ultrasound-guided fine-needle aspiration biopsy in evaluation of nonpalpable thyroid nodules. Thyroid. 1998, 8, 989–95. [Google Scholar] [CrossRef] [PubMed]
- Nam-Goong, I.S.; Kim, H.Y.; Gong, G.; Lee, H.K.; Hong, S.J.; Kim, W.B.; et al. Ultrasonography-guided fine-needle aspiration of thyroid incidentaloma: correlation with pathological findings. Clin Endocrinol (Oxf). 2004, 60, 21–8. [Google Scholar] [CrossRef] [PubMed]
- Leenhardt, L.; Hejblum, G.; Franc, B.; Fediaevsky, L.D.; Delbot, T.; Le Guillouzic, D.; et al. Indications and limits of ultrasound-guided cytology in the management of nonpalpable thyroid nodules. J Clin Endocrinol Metab. 1999, 84, 24–8. [Google Scholar] [CrossRef]
- Papini, E.; Guglielmi, R.; Bianchini, A.; Crescenzi, A.; Taccogna, S.; Nardi, F.; et al. Risk of malignancy in nonpalpable thyroid nodules: predictive value of ultrasound and color-Doppler features. J Clin Endocrinol Metab. 2002, 87, 1941–6. [Google Scholar] [CrossRef]
- Tessler, F.N.; Middleton, W.D.; Grant, E.G.; Hoang, J.K.; Berland, L.L.; Teefey, S.A.; et al. ACR Thyroid Imaging, Reporting and Data System (TI-RADS): White Paper of the ACR TI-RADS Committee. J Am Coll Radiol. 2017, 14, 587–95. [Google Scholar] [CrossRef]
- Bukasa-Kakamba, J.; Bayauli, P.; Sabbah, N.; Bidingija, J.; Atoot, A.; Mbunga, B.; et al. Ultrasound performance using the EU-TIRADS score in the diagnosis of thyroid cancer in Congolese hospitals. Sci Rep. 2022, 12, 18442. [Google Scholar] [CrossRef] [PubMed]
- Bukasa, J.K.; Bayauli-Mwasa, P.; Mbunga, B.K.; Bangolo, A.; Kavula, W.; Mukaya, J.; et al. The Spectrum of Thyroid Nodules at Kinshasa University Hospital, Democratic Republic of Congo: A Cross-Sectional Study. International Journal of Environmental Research and Public Health [Internet]. 2022, 19. [Google Scholar]
- Zaichick, V.; Tsyb, A.F.; Vtyurin, B.M. Trace elements and thyroid cancer. Analyst. 1995, 120, 817–21. [Google Scholar] [CrossRef]
- Zhou, Q.; Xue, S.; Zhang, L.; Chen, G. Trace elements and the thyroid. Front. Endocrinol. 2022, 13, 904889. [Google Scholar] [CrossRef]
- He, J.-l.; Wu, H.-b.; Hu, W.-l.; Liu, J.-j.; Zhang, Q.; Xiao, W.; et al. Exposure to multiple trace elements and thyroid cancer risk in Chinese adults: A case-control study. International Journal of Hygiene and Environmental Health. 2022, 246, 114049. [Google Scholar] [CrossRef] [PubMed]
- Hegedüs, L. Clinical practice. The thyroid nodule. N Engl J Med. 2004, 351, 1764–71. [Google Scholar] [CrossRef] [PubMed]
- Kobaly, K.; Kim, C.S.; Mandel, S.J. Contemporary Management of Thyroid Nodules. Annual Review of Medicine. 2022, 73, 517–28. [Google Scholar] [CrossRef]
- Werk, E.E.; Jr Vernon, B.M.; Gonzalez, J.J.; Ungaro, P.C.; McCoy, R.C. Cancer in thyroid nodules. A community hospital survey. Arch Intern Med. 1984, 144, 474–6. [Google Scholar] [CrossRef]
- Belfiore, A.; Giuffrida, D.; La Rosa, G.L.; Ippolito, O.; Russo, G.; Fiumara, A.; et al. High frequency of cancer in cold thyroid nodules occurring at young age. Acta Endocrinol (Copenh). 1989, 121, 197–202. [Google Scholar] [CrossRef]
- Kwong, N.; Medici, M.; Angell, T.E.; Liu, X.; Marqusee, E.; Cibas, E.S.; et al. The Influence of Patient Age on Thyroid Nodule Formation, Multinodularity, and Thyroid Cancer Risk. J Clin Endocrinol Metab. 2015, 100, 4434–40. [Google Scholar] [CrossRef]
- Petrosino, V.; Motta, G.; Tenore, G.; Coletta, M.; Guariglia, A.; Testa, D. The role of heavy metals and polychlorinated biphenyls (PCBs) in the oncogenesis of head and neck tumors and thyroid diseases: a pilot study. BioMetals. 2018, 31, 285–95. [Google Scholar] [CrossRef] [PubMed]
- Liao, Xiwen, "Exposure To Heavy Metals In Relation To Thyroid Dysfunctions In U.s. Adults" (2019). Public Health Theses. 1833.
- Kim, S.; Song, S.-H.; Lee, C.-W.; Kwon, J.-T.; Park, E.Y.; Oh, J.-K.; et al. Low-Level Environmental Mercury Exposure and Thyroid Cancer Risk Among Residents Living Near National Industrial Complexes in South Korea: A Population-Based Cohort Study. Thyroid. 2022, 32, 1118–28. [Google Scholar] [CrossRef]
- "New initiative to support artisanal cobalt mining in the DRC". Mining Review. 2021-04-01. Retrieved 2022-10-02.
- Banza, C.L.; Nawrot, T.S.; Haufroid, V.; Decrée, S.; De Putter, T.; Smolders, E.; et al. High human exposure to cobalt and other metals in Katanga, a mining area of the Democratic Republic of Congo. Environ Res. 2009, 109, 745–52. [Google Scholar] [CrossRef]
- Squadrone, S.; Burioli, E.; Monaco, G.; Koya, M.K.; Prearo, M.; Gennero, S.; et al. Human exposure to metals due to consumption of fish from an artificial lake basin close to an active mining area in Katanga (D.R. Congo). Sci Total Environ. 2016, 568, 679–84. [Google Scholar] [CrossRef]
- Angell, T.E.; Maurer, R.; Wang, Z.; Kim, M.I.; Alexander, C.A.; Barletta, J.A.; et al. A Cohort Analysis of Clinical and Ultrasound Variables Predicting Cancer Risk in 20,001 Consecutive Thyroid Nodules. J Clin Endocrinol Metab. 2019, 104, 5665–72. [Google Scholar] [CrossRef] [PubMed]
- Cappelli, C.; Castellano, M.; Pirola, I.; Cumetti, D.; Agosti, B.; Gandossi, E.; et al. The predictive value of ultrasound findings in the management of thyroid nodules. Qjm. 2007, 100, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Sipos, J.A. Advances in ultrasound for the diagnosis and management of thyroid cancer. Thyroid. 2009, 19, 1363–72. [Google Scholar] [CrossRef] [PubMed]
- Solbiati, L.; Volterrani, L.; Rizzatto, G.; Bazzocchi, M.; Busilacci, P.; Candiani, F.; et al. The thyroid gland with low uptake lesions: evaluation by ultrasound. Radiology. 1985, 155, 187–91. [Google Scholar] [CrossRef] [PubMed]
- Cochand-Priollet, B.; Guillausseau, P.J.; Chagnon, S.; Hoang, C.; Guillausseau-Scholer, C.; Chanson, P.; et al. The diagnostic value of fine-needle aspiration biopsy under ultrasonography in nonfunctional thyroid nodules: a prospective study comparing cytologic and histologic findings. Am J Med. 1994, 97, 152–7. [Google Scholar] [CrossRef]
- Kakkos, S.K.; Scopa, C.D.; Chalmoukis, A.K.; Karachalios, D.A.; Spiliotis, J.D.; Harkoftakis, J.G.; et al. Relative risk of cancer in sonographically detected thyroid nodules with calcifications. J Clin Ultrasound. 2000, 28, 347–52. [Google Scholar] [CrossRef]
- Bonavita, J.A.; Mayo, J.; Babb, J.; Bennett, G.; Oweity, T.; Macari, M.; et al. Pattern recognition of benign nodules at ultrasound of the thyroid: which nodules can be left alone? AJR Am J Roentgenol. 2009, 193, 207–13. [Google Scholar] [CrossRef]
- Kiernan, C.M.; Solórzano, C.C. Bethesda Category III, IV, and V Thyroid Nodules: Can Nodule Size Help Predict Malignancy? J Am Coll Surg. 2017, 225, 77–82. [Google Scholar] [CrossRef]
- Cavallo, A.; Johnson, D.N.; White, M.G.; Siddiqui, S.; Antic, T.; Mathew, M.; et al. Thyroid Nodule Size at Ultrasound as a Predictor of Malignancy and Final Pathologic Size. Thyroid. 2017, 27, 641–50. [Google Scholar] [CrossRef]
- Lim, S.T.; Jeon, Y.W.; Suh, Y.J. The Prognostic Values of Preoperative Tumor Volume and Tumor Diameter in T1N0 Papillary Thyroid Cancer. Cancer Res Treat. 2017, 49, 890–7. [Google Scholar] [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Types de nodules.
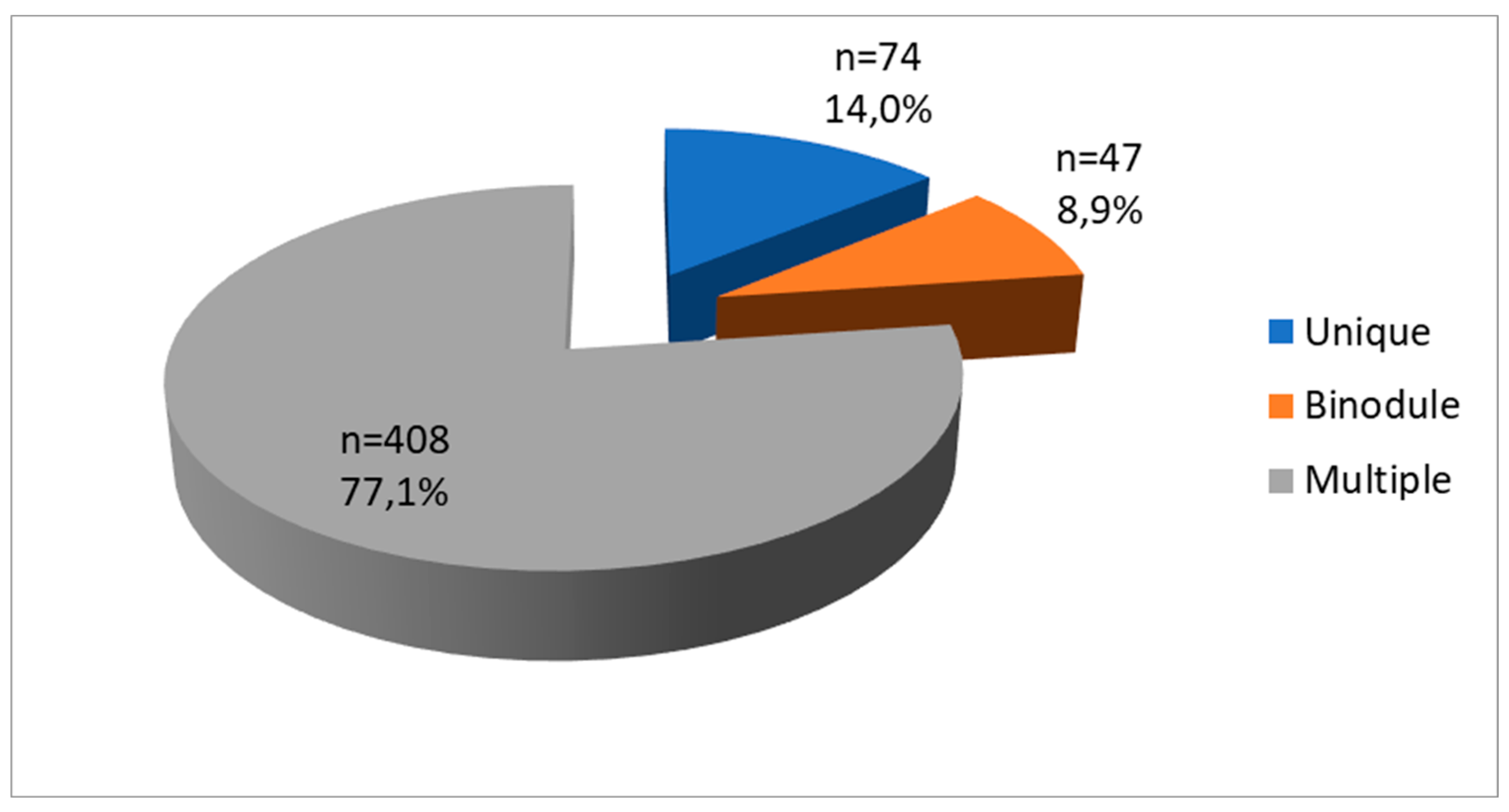

Table 1.
Sociodemographic characteristics according to type of nodules.
| Variables | All (n=529) |
Single (n=74) |
Multiple (n=455) |
p |
|---|---|---|---|---|
| Age | 44.2±14,6 | 45.0±14.9 | 44.0±14.2 | 0.206 |
| ≤20 years | 35(6.6) | 8(10.8) | 7(5.9) | |
| 21-30 years | 54(10.2) | 2(2.7) | 52(11.4) | |
| 31-40 years | 135(25.5) | 19(25.7) | 116(25.5) | |
| 41-50 years | 127(24.0) | 19(25.7) | 108(23.7) | |
| 51-60 years | 96(18.1) | 14(18.9) | 82(18.0) | |
| >60 years | 82(15.5) | 12(16.2) | 70(15.4) | |
| Sex | 0.360 | |||
| Male | 82(15.6) | 13(17.6) | 69(15.3) | |
| Female | 444(84.4) | 61(82.4) | 383(84.7) | |
| Marital Status | 0.636 | |||
| Married | 373(75.1) | 51(77.3) | 322(74.7) | |
| Single | 115(23.1) | 13(19.7) | 102(23.7) | |
| Divorced/Widowed | 9(1.8) | 2(3.0) | 7(1.6) | |
| Origin of the sample | 0.280 | |||
| Kinshasa | 468(88.5) | 64(86.5) | 404(88.8) | |
| Katanga | 18(3.4) | 1(1.4) | 17(3.7) | |
| Sud Kivu | 43(8.1) | 9(12.2) | 34(7.5) |
Table 2.
Clinical characteristics.
| Variables | All (n=529) |
Single (n=74) |
Multiple (n=455) |
p |
|---|---|---|---|---|
| Parity | 0.670 | |||
| Nulliparous | 65(14.6) | 10(16.4) | 55(14.3) | |
| Primiparous | 40(9.0) | 5(8.2) | 35(9.1) | |
| Pauciparous | 102(22.9) | 17(27.9) | 85(22.1) | |
| Multiparous | 239(53.6) | 29(47.5) | 210(54.5) | |
| Gravida | 0.514 | |||
| Nulligravid | 71(16.0) | 11(18.0) | 60(15.6) | |
| Primigravid | 40(9.0) | 3(4.9) | 37(9.6) | |
| Multigravid | 334(75.1) | 47(77.0) | 287(74.7) | |
| Abortion | 83(18.7) | 15(24.6) | 68(17.7) | 0,135 |
| Family history of thyroid pathology | 352(66.5) | 51(68.9) | 301(66.2)) | 0,373 |
| First degree | 205(58.2) | 30(60.0) | 175(57.9) | |
| Second degree | 147(41.8) | 20(40.0) | 127(42.1) | |
| Anterior-cervical mass | 503(95.1) | 71(95.9) | 391(95.8) | 0.099 |
| Overweight | 195(36.9) | 23(31.1) | 172(37.8) | 0.163 |
| Obesity | 187(35.3) | 28(37.8) | 159(34.9) | 0.360 |
| Clinical LAD | 46(8.7) | 10(13.5) | 36(7.9) | 0.091 |
| SBP | 135.6±58.6 | 131.4±13.8 | 135.8±65.5 | 0.786 |
| DBP | 72.6±8.9 | 73.9±8.5 | 72.3±9.2 | 0.485 |
| BMI | 29.8±12.1 | 29.5±3.1 | 29.9±13.6 | 0.959 |
| HR | 83.0±11.0 | 82.0±11.6 | 83.1±10.6 | 0.557 |
| Total volume | 70.9±31.5 | 68.5±30.8 | 70.8±32.2 | 0.596 |
| Thyroid Fonction | 0.631 | |||
| euthyroid | 464(87.7) | 63(85.1) | 401(88.1) | |
| Hyperthyroid | 50(9.5) | 9(12.2) | 41(9.0) | |
| Hypothyroid | 15(2.8) | 2(2.7) | 13(2.9) |
LAD: Lymphadenopathy; SBP: Systolic Blood Pressure; DBP: Diastolic Blood Pressure; BMI: Body Mass Index; HR: Heart Rate.
Table 3.
Sonographic characteristics of nodules.
| Variables | All (n=529) |
Simple (n=74) |
Multiple (n=408) |
p |
|---|---|---|---|---|
| Echostructure | 0.837 | |||
| Solid | 382(72.2) | 53(71.6) | 329(72.3) | |
| Liquid | 12(2.3) | 1(1.4) | 11(2.4) | |
| Mixed | 135(25.5) | 20(27.0) | 115(25.3) | |
| Echogenicity | 0.332 | |||
| Hypoechoic | 447(84.5) | 59(79.7) | 388(85.3) | |
| Isoechoic | 81(15.3) | 15(20.3) | 66(14.5) | |
| Anechoic | 1(0.2) | 0(0.0) | 1(0.2) | |
| Size | 0.360 | |||
| Macronodule | 315(59.8) | 50(67.6) | 265(58.5) | |
| Micronodule | 82(15.6) | 9(12.2) | 73(16.1) | |
| Mixed | 130(24.7) | 15(20.3) | 115(25.4) | |
| Microcalcification | 0.494 | |||
| No | 453(85.6) | 64(86.5) | 389(85.5) | |
| Yes | 76(14.4) | 10(13.5) | 66(14.5) | |
| Adenopathy | 0.352 | |||
| No | 447(84.5) | 61(82.4) | 386(84.8) | |
| Yes | 82(15.5) | 13(17.6) | 69(15.2) |
Table 4.
Characteristics of nodules in pathology.
| Variables | Number (n=529) | Percentage |
|---|---|---|
| Anapathology | ||
| Benign nodules | 441 | 77.7 |
| Malignant nodules | 118 | 22.3 |
| Benign nodules | ||
| Colloid goiter | 302 | 73.5 |
| Adenomatoid goiter | 36 | 8.8 |
| Follicular adenoma | 20 | 4.9 |
| Macrofollicular adenoma | 18 | 4.4 |
| Follicular cyst | 8 | 1.9 |
| Adenomatoid nodule | 5 | 1.2 |
| Thyroid abscess | 3 | 0.7 |
| Follicular adenoma | 3 | 0.7 |
| Microfollicular adenoma | 3 | 0.7 |
| Reactive LAD | 3 | 0.7 |
| Chronic strumitis | 3 | 0.7 |
| Grave’s disease | 2 | 0.5 |
| Non toxic adenoma | 1 | 0.2 |
| Toxic adenoma | 1 | 0.2 |
| Granulomatous thyroid | 1 | 0.2 |
| Dequervain's subacute thyroiditis | 1 | 0.2 |
| Hashimoto’s thyroiditis | 1 | 0.2 |
| Malignant nodules | ||
| Papillary carcinoma | 79 | 66.9 |
| Follicular carcinoma | 26 | 22.0 |
| Anaplastic carcinoma | 9 | 7.6 |
| Lymphoma | 3 | 2.5 |
| Medullary carcinoma | 1 | 0.8 |
LAD: Lymphadenopathy.
Table 5.
Sociodemographic and clinical characteristics according to the anatomopathological character.
Table 5.
Sociodemographic and clinical characteristics according to the anatomopathological character.
| Variables | N | Benign nodule n(%) |
Malignant nodule n(%) |
p |
|---|---|---|---|---|
| Age | 0.003 | |||
| ≤20 years | 35 | 31(87.1) | 4(12.9) | |
| 21-60 years | 412 | 333(80.8) | 79(19.2) | |
| >60 years | 82 | 47(57.3) | 35(42.7) | |
| Sex | 0.061 | |||
| Male | 82 | 58(70.7) | 24(29.3) | |
| Female | 444 | 352(79.3) | 92(20.7) | |
| Province of origin of the sample | 0.044 | |||
| Kinshasa | 468 | 364(77.8) | 104(22.2) | |
| Katanga | 18 | 10(55.6) | 8(44.4) | |
| South Kivu | 43 | 37(86.0) | 6(14.0) | |
| Marital status | 0.256 | |||
| Married | 373 | 293(78.6) | 80(21.4) | |
| Single | 115 | 85(73.9) | 30(26.1) | |
| Divorced/widow | 9 | 7(77.8) | 2(22.2) | |
| Parity | 0,160 | |||
| Nulliparous | 65 | 46(70.8) | 19(29.2) | |
| Primiparous | 40 | 32(80.0) | 8(20.0) | |
| Pauciparous | 102 | 87(85.3) | 15(14.7) | |
| Multiparous | 239 | 187(78.2) | 52(21.8) | |
| Gravida | 0.311 | |||
| Nulligravid | 71 | 51(71.8) | 20(28.2) | |
| Primigravid | 40 | 32(80.0) | 8(20.0) | |
| Multigravid | 334 | 268(80.2) | 66(19.8) | |
| FH of thyroid pathology | 0.022 | |||
| No | 177 | 147(83.1) | 30(16.9) | |
| Yes | 352 | 264(75.0) | 88(25.0) | |
| BMI | 0.505 | |||
| Normal | 25 | 22(88.0) | 3(12.0) | |
| Overweight | 195 | 150(76.9) | 45(23.1) | |
| Obesity | 187 | 146(78.1) | 41(21.9) | |
| Clinical LAD | <0.001 | |||
| No | 100.0 | 397(82.2) | 86(17.8) | |
| Yes | 100.0 | 14(30.4) | 32(69.6) |
FH: Family history; BMI: Body Mass Index; LAD: Lymphadenopathy.
Table 6.
Ultrasound characteristics according to the anatomopathological character.
| Variables | N | Benign nodule n(%) |
Malignant nodule n(%) |
p |
|---|---|---|---|---|
| Echostructure | <0.001 | |||
| Solid | 382 | 268(70.2) | 114(29.8) | |
| Liquid | 12 | 12(100.0) | 0(0.0) | |
| Mixed | 135 | 4(97.0) | 4(3.0) | |
| Echogenicity | <0.001 | |||
| Hypoechoic | 447 | 330(73.8) | 117(26.2) | |
| Isoechoic | 81 | 80(98.8) | 1(1.2) | |
| Anechoic | 1 | 1(100.0) | 0(0.0) | |
| Number | 0.284 | |||
| Unique | 74 | 55(74.3) | 19(25.7) | |
| Binodule | 47 | 33(70.2) | 14(29.8) | |
| Multiple | 408 | 323(79.2) | 85(20.8) | |
| Size | <0.001 | |||
| Macronodule | 315 | 211(67.0) | 104(33.0) | |
| Micronodule | 82 | 81(98.8) | 1(1.2) | |
| Mixed | 130 | 119(91.5) | 11(8.5) | |
| Calcification | <0.001 | |||
| No | 453 | 376(83.0) | 77(17.0) | |
| Yes | 76 | 35(46.1) | 41(53.9) | |
| Adenopathy | <0.001 | |||
| No | 447 | 382(85.5) | 65(14.5) | |
| Yes | 82 | 29(35.4) | 53(64.6) |
Table 7.
Factors associated with risk of malignancy in nodules.
| Variables | Univariate analysis | Multivariate analysis | |||
|---|---|---|---|---|---|
| p | OR (CI 95%) | p | aOR (CI 95%) | ||
| Age | |||||
| ≤20 years | 1 | 1 | |||
| 21-60 years | 0,319 | 1.52(0,67-3.46) | 0.614 | 1,32(0.26-2.24) | |
| >60 years | 0.003 | 2.81(1.37-5.78) | 0.025 | 2.81(1.14-6.94) | |
| Province of origin of the sample | |||||
| South Kivu | 1 | 1 | |||
| Kinshasa | 0.212 | 1.76(0.72-4.29) | 0,116 | 2.47(0.80-7.62) | |
| Katanga | 0.014 | 4,93(1.39-17.54) | 0.036 | 8.19(1.14-12.45) | |
| FH of thyroid pathology | |||||
| No | 1 | 1 | |||
| Yes | 0.022 | 1.63(1.03-2.59) | 0,105 | 1.65(0.90-3.34) | |
| Clinical LAD | |||||
| No | 1 | 1 | |||
| Yes | <0.001 | 10.55(5.40-20.62) | 0,760 | 1.20(0.38-3.82) | |
| Echostructure | |||||
| Liquid | 1 | 1 | |||
| Solid | <0.001 | 15,21(5.50-42.07) | 0.001 | 7.69(2.40-24.58) | |
| Echogenicity | |||||
| Isoechoic | 1 | 1 | |||
| Hypoechoic | <0.001 | 18.72(3.95-28.68) | 0.017 | 14.19(1.60-25.93) | |
| Size | |||||
| Micronodule | 1 | 1 | |||
| Macronodule | <0.001 | 5.33(2.75-10.33) | <0.001 | 9.13(4.19-19.89) | |
| Calcification | |||||
| No | 1 | 1 | |||
| Yes | <0.001 | 5.72(3.42-9.55) | 0.017 | 2.60(1.19-5.70) | |
| Ultrasound LAD | |||||
| No | 1 | 1 | |||
| Yes | <0.001 | 10.74(6.36-18.13) | <0.000 | 6.94(2.79-17.25) | |
FH: Family History; LAD: Lymphadenopathy.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



