
Submitted:
03 September 2024
Posted:
05 September 2024
You are already at the latest version
Abstract
Background: Cancer-Related Fatigue (CRF) is a prevalent and debilitating symptom in breast cancer patients, significantly impacting their quality of life and potentially affecting postoperative outcomes. Despite advances in breast cancer treatment, the long-term implications of CRF on prognosis remain unclear. Methods: This retrospective cohort study included 310 postoperative breast cancer patients from two large comprehensive hospitals. We systematically collected demographic, medical history, lifestyle, psychological status, and CRF data. Univariate and multivariate Cox regression analyses were performed to identify independent prognostic factors. Random forest survival analysis, propensity score matching, Kaplan-Meier survival analysis, and restricted cubic spline analysis were utilized to comprehensively evaluate the relationship between CRF and postoperative prognosis. Results: Higher CRF scores were associated with worse postoperative outcomes (HR = 1.07, 95% CI: 1.03-1.10, P < 0.001). Other independent prognostic factors included higher HADS scores (HR = 1.09, 95% CI: 1.01-1.17, P = 0.032), not undergoing breast-conserving surgery (HR = 0.43, 95% CI: 0.20-0.89, P = 0.024), and not receiving endocrine therapy (HR = 7.13, 95% CI: 2.64-19.22, P < 0.001). Random forest survival analysis highlighted CRF as the most critical variable impacting prognosis. Propensity score matching effectively balanced baseline characteristics, and Kaplan-Meier survival curves demonstrated significantly lower survival rates in high-CRF patients both before and after matching (P < 0.05). Restricted cubic spline analysis revealed a nonlinear relationship between CRF scores and disease progression risk, with significant risk increases beyond specific thresholds. Conclusions: CRF is a crucial predictor of disease progression in postoperative breast cancer patients. Higher CRF and HADS scores, non-breast-conserving surgery, and lack of endocrine therapy are associated with poorer prognosis. These findings underscore the importance of comprehensive postoperative care, including effective management of fatigue and psychological health, to improve patient outcomes. Future research should focus on prospective studies and targeted interventions for CRF to validate these findings and enhance clinical practices.
Keywords:
Breast cancer
; Cancer-Related Fatigue
; Propensity Matching Analysis
; Survival analysis
; Restricted cubic splines
Introduction
Breast cancer is the most common malignancy among women worldwide, with its incidence and mortality rates increasing annually1. According to the World Health Organization (WHO), breast cancer has become one of the major threats to women's health2. In China, the incidence of breast cancer is also rising, making it the most prevalent malignancy among women3-4. Despite significant advances in early diagnosis and treatment, improving the long-term quality of life for patients remains an urgent issue. The primary treatment modalities for breast cancer include surgery, chemotherapy, radiotherapy, and hormone therapy. Surgery forms the cornerstone of breast cancer treatment by removing tumor tissue to control the disease. Chemotherapy and radiotherapy are commonly used adjuvant treatments aimed at eliminating residual cancer cells and reducing the risk of recurrence5-6. Hormone therapy is suitable for hormone receptor-positive breast cancer patients and works by regulating hormone levels to inhibit tumor growth. Although these treatments significantly improve survival rates, they also bring side effects such as fatigue, pain, and psychological issues7.
Postoperative rehabilitation for breast cancer is crucial for enhancing patients' quality of life. This rehabilitation includes not only physical recovery but also psychological and social recovery. Through scientific rehabilitation training and psychological counseling, postoperative discomfort can be alleviated, thereby improving the quality of life8-9. However, during the postoperative rehabilitation process, Cancer-Related Fatigue (CRF) is a common and severely troubling issue for patients. CRF affects not only the physical function of patients but also their psychological state and social life10.
CRF is a persistent, subjective fatigue related to cancer and its treatment, which cannot be alleviated by rest or sleep. CRF is distinct from normal fatigue, characterized by its long duration and high severity, significantly impacting patients' daily life and work ability11. CRF has been defined as an independent symptom by the Union for International Cancer Control (UICC) and the National Comprehensive Cancer Network (NCCN), warranting heightened attention from clinical healthcare providers12. The main symptoms of CRF include persistent fatigue, lack of energy, difficulty concentrating, memory decline, low mood, and sleep disturbances. Patients often feel that even with adequate rest, they cannot regain their physical and mental strength. This persistent fatigue affects not only the patient's physical activity but also limits their social interactions and professional life13.
CRF has a significant negative impact on the quality of life for postoperative breast cancer patients. Existing studies have reported that CRF is a high-risk factor for poor prognosis after breast cancer surgery. However, current research still has questions about the long-term impact of CRF on postoperative prognosis and the best assessment points14-15. This study retrospectively analyzes data from postoperative breast cancer patients at two centers, using Cox regression analysis, random forest survival analysis, propensity score matching analysis, and restricted cubic spline analysis to comprehensively evaluate the relationship between CRF scores and postoperative prognosis in breast cancer patients, exploring the potential link between CRF and poor prognosis in breast cancer.
Methods
Study Design
This study aims to explore the relationship between Cancer-Related Fatigue (CRF) and disease progression after breast cancer surgery, utilizing a retrospective cohort study design. The study subjects are patients who underwent breast cancer surgery at two large comprehensive hospitals. Systematic collection of medical histories and follow-up data will be conducted to comprehensively analyze the relationship between CRF and postoperative prognosis in breast cancer patients.
Patient Sources
- Research Centers The study subjects are from the breast surgery departments of two large comprehensive hospitals.
- Inclusion Criteria 1) Female patients aged between 18 and 70. 2) Underwent radical breast cancer surgery. 3) Received at least one postoperative treatment (chemotherapy, radiotherapy, or hormone therapy). 4) Signed informed consent.
- Exclusion Criteria 5) Concurrent severe diseases (e.g., cardiovascular diseases, severe liver or renal insufficiency). 6) Cognitive impairments or mental disorders preventing questionnaire completion. 7) Other factors that may affect CRF assessment (e.g., recent major surgeries).
Data Collection
Data will be collected from the hospital HIS system and discharge follow-up system at both centers, including:
- Demographic Information Age: Recorded at the time of surgery. Marital Status: Classified as single (never married, divorced, or widowed) or married.
- Medical History Information Disease Stage: Recorded according to the TNM staging system (Stages I, II, III). Pathological Type: Specific types of breast cancer. Surgical Method: Types of surgery performed (radical mastectomy, breast-conserving surgery, etc.). Postoperative Treatment Plans: Detailed records of adjuvant treatments (chemotherapy, radiotherapy, hormone therapy). Body Mass Index (BMI): Calculated based on height and weight.
- Lifestyle Information Exercise Frequency: Frequency of postoperative exercise, classified as daily, weekly, or monthly. Sleep Quality: Assessed using the Pittsburgh Sleep Quality Index (PSQI), including seven components: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction. Classified as good, average, or poor.
- Psychological Status Hospital Anxiety and Depression Scale (HADS): HADS consists of 14 items, assessing anxiety (7 items) and depression (7 items), with each item scored from 0 to 3. The total score for each dimension ranges from 0 to 21, with higher scores indicating more severe anxiety or depression.
- Fatigue Assessment Cancer-Related Fatigue Scale (CFS): The CFS includes 10 items, each scored from 0 to 10, with a total score ranging from 0 to 100. Higher scores indicate greater fatigue.
Statistical Analysis
All statistical analyses in this study were performed using R software version 4.0.3 and SPSS version 25.0. A two-sided P-value of less than 0.05 was considered statistically significant.
- Descriptive Analysis
The baseline characteristics of the patients were summarized using descriptive statistics. Continuous variables were reported as means ± standard deviations or medians with interquartile ranges (IQR) depending on the distribution of the data, which was assessed using the Shapiro-Wilk test. Categorical variables were presented as counts and percentages. To compare baseline characteristics between the recurrence and stable groups, t-tests or Mann-Whitney U tests were used for continuous variables, and chi-square tests or Fisher's exact tests were used for categorical variables.
- 2.
- Univariate and Multivariate Cox Proportional Hazards Regression
The association between each covariate and the postoperative prognosis was first evaluated using univariate Cox proportional hazards regression. Variables with P-values < 0.05 in the univariate analysis were included in the multivariate Cox regression model to identify independent prognostic factors. The results of the Cox regression analyses were reported as hazard ratios (HR) with 95% confidence intervals (CI).
- 3.
- Propensity Score Matching (PSM)
To address potential confounding factors between the high-CRF and low-CRF groups, we applied propensity score matching (PSM) to balance the baseline characteristics. Propensity scores were calculated using a logistic regression model based on clinically relevant covariates, including age, TNM stage, surgical method, endocrine therapy, and psychological status. A 1:1 matching scheme was employed using the nearest-neighbor method without replacement and a caliper width of 0.2 of the standard deviation of the logit of the propensity score. The effectiveness of matching was assessed by calculating the standardized mean differences (SMD) for each covariate, with an SMD < 0.1 considered indicative of good balance between the groups.
- 4.
- Kaplan-Meier Survival Analysis
Survival curves were generated using the Kaplan-Meier method to compare the survival rates between the high-CRF and low-CRF groups, both before and after propensity score matching. Differences in survival between the groups were evaluated using the log-rank test, with a P-value < 0.05 indicating statistical significance. Kaplan-Meier survival curves were presented graphically, showing the time to disease progression across different CRF levels.
- 5.
- Random Forest Survival Analysis
To further assess the importance of each variable in predicting postoperative prognosis, we utilized random forest survival analysis. This method allows for the evaluation of complex interactions between variables. The random forest model was constructed using 500 decision trees, with variables randomly sampled at each split. The variable importance score was calculated for each predictor, and the top contributing variables were ranked based on their importance to overall survival.
- 6.
- Restricted Cubic Spline Analysis
To explore the potential nonlinear relationship between CRF scores and disease progression risk, restricted cubic spline analysis was performed. The model included 3 knots, and the spline regression allowed for a flexible analysis of the continuous CRF score and its association with disease progression. The results were graphically represented, showing a threshold effect, with the risk of progression significantly increasing beyond a specific CRF score.
Results
- Baseline Characteristics Analysis
A total of 310 postoperative breast cancer patients were included in the study, with 34 cases experiencing disease recurrence and 276 cases remaining stable. There were no significant differences in age and BMI between the recurrence and stable groups (P > 0.05). However, significant differences were observed in HADS scores, SSRS scores, and CFS scores between the two groups (P < 0.05). The recurrence group had significantly higher HADS and CFS scores and significantly lower SSRS scores compared to the stable group, indicating higher levels of anxiety, depression, and fatigue, but lower social support in the recurrence group. Specific data are shown in Table 1.
- 2.
- Univariate and Multivariate Cox Regression Analysis
Univariate Cox regression analysis indicated that TNM stage, surgical method, endocrine therapy, HADS, SSRS, and CFS were significantly associated with postoperative prognosis in breast cancer patients. In multivariate analysis, surgical method, endocrine therapy, HADS, and CFS scores remained independent prognostic factors. Specifically, not undergoing breast-conserving surgery, not receiving endocrine therapy, higher HADS scores, and higher CFS scores were associated with poorer postoperative prognosis. Detailed results are shown in Table 2.
- 3.
- Random Forest Survival Analysis Results
Figure 1 shows the importance ranking of variables in the random forest survival analysis. The CFS demonstrated the highest importance among all variables, indicating its significant impact on postoperative prognosis in breast cancer patients. Other important variables included HADS scores, surgical method, and endocrine therapy.
- 4.
- Propensity Score Matching Analysis Results
Table 3 and Figure 2 presents the standardized mean differences of covariates between the high-CFS and low-CFS groups before and after propensity score matching. After matching, the differences in covariates between the groups were significantly reduced, indicating that the matching process effectively balanced the baseline characteristics between the groups.
- 5.
- Kaplan-Meier Survival Analysis Before and After Propensity Score Matching
Figure 3A and 3B show the Kaplan-Meier survival curves for high-CFS and low-CFS groups before and after propensity score matching. Before matching, the survival rate of the high-CFS group was significantly lower than that of the low-CFS group (P < 0.05). After matching, the survival rate difference between the two groups persisted but was reduced (P < 0.05).
- 6.
- Restricted Cubic Spline Analysis Before and After Propensity Score Matching
Figure 4 illustrates the restricted cubic spline analysis results of CFS scores and the risk of disease progression before and after propensity score matching. Both analyses indicate a nonlinear relationship between CFS scores and the risk of disease progression, with a significant increase in risk beyond a certain threshold. The optimal CFS score threshold was 28 before matching and 36 after matching.
Discussion
This study found that CRF is a significant prognostic factor for disease progression in postoperative breast cancer patients. Multivariate Cox regression analysis confirmed that higher CRF scores (HR = 1.07, 95% CI: 1.03-1.10, P < 0.001), higher HADS scores (HR = 1.09, 95% CI: 1.01-1.17, P = 0.032), not undergoing breast-conserving surgery (HR = 0.43, 95% CI: 0.20-0.89, P = 0.024), and not receiving endocrine therapy (HR = 7.13, 95% CI: 2.64-19.22, P < 0.001) were all associated with poorer postoperative prognosis. The random forest survival analysis further validated CRF as the most critical variable affecting prognosis, underscoring the necessity of addressing CRF in clinical practice. In addition, propensity score matching analysis demonstrated that the baseline differences between high-CRF and low-CRF groups were significantly reduced, indicating that the impact of CRF on prognosis is independent of other confounding factors.
Our findings are consistent with prior research. Abrahams et al. highlighted the important role of CRF in the long-term outcomes of cancer survivors, supporting the negative impact of CRF on postoperative prognosis16. However, unlike previous studies focusing solely on fatigue, our analysis also revealed the significant influence of psychological distress in conjunction with CRF on patient prognosis. This is in line with the work of Schmidt et al, who emphasized that psychological distress is a key determinant of cancer progression and mortality17. These results further support the integration of psychological health and physical recovery as central aspects of postoperative rehabilitation18. In comparison to existing literature, the uniqueness of this study lies in its comprehensive analysis of CRF alongside other postoperative factors, utilizing multiple approaches such as random forest survival analysis to thoroughly assess the impact of CRF. This multi-level, multivariate evaluation offers a broader perspective for postoperative rehabilitation strategies19.
The results of this study highlight the need for a holistic approach to postoperative breast cancer rehabilitation, which addresses not only physical recovery but also psychological well-being. Patients with higher CRF scores are more likely to experience disease recurrence, potentially due to the profound impact of fatigue on their physical activity, psychological state, and overall recovery capacity. The dual influence of psychological distress and fatigue may weaken immune function and reduce participation in recovery activities, thereby increasing the risk of disease progression20-22. These findings further support the theoretical framework that emphasizes the integration of CRF management and psychological interventions into standard postoperative care, particularly for high-risk patients, to provide personalized and comprehensive care plans. From a clinical perspective, the identification of CRF as an independent prognostic factor implies that fatigue management should be a key component of postoperative rehabilitation. Clinicians can reduce CRF and improve prognosis by implementing interventions such as fatigue management programs, exercise therapies, and psychological counseling23. Additionally, this study highlights the significant impact of psychological health on postoperative recovery, suggesting that systematic psychological health screening and support should be incorporated into rehabilitation, especially for patients with severe anxiety or depression24. The protective effect of breast-conserving surgery on long-term quality of life and prognosis also provides valuable guidance for surgical decision-making25. Similarly, the significant role of endocrine therapy in improving the prognosis of hormone receptor-positive breast cancer patients underscores the importance of standardized endocrine treatment protocols26.
Study Limitations
Despite the valuable insights gained from this study, several limitations must be acknowledged. First, the retrospective design may introduce selection bias, and the reliance on self-reported assessments for CRF and psychological distress is subject to individual subjective perceptions, which could affect accuracy. Future studies should adopt a prospective design and incorporate more objective measures of fatigue and psychological well-being to validate these findings. Additionally, variability in treatment protocols between the two study centers could limit the generalizability of the results. Therefore, future research should include a more diverse patient population and apply standardized treatment protocols to further validate these results across different settings.
Future Research Directions
Future research should focus on prospective cohort studies to further explore the long-term impact of CRF and psychological distress on postoperative prognosis. Moreover, studies on targeted interventions aimed at managing CRF could provide practical strategies to improve the prognosis of breast cancer patients. Cultural differences in CRF and its impact should also be examined to develop intervention strategies tailored to different regions and populations. Finally, future studies could investigate the underlying biological mechanisms linking CRF with immune function and postoperative outcomes, potentially offering new avenues for clinical treatment.
Conclusion
In conclusion, this study demonstrates that CRF is a crucial independent factor affecting the prognosis of postoperative breast cancer patients. Higher CRF and HADS scores, not undergoing breast-conserving surgery, and not receiving endocrine therapy were all associated with poorer outcomes. These findings emphasize the importance of comprehensive postoperative care that includes effective management of both fatigue and psychological health to improve patient outcomes. Future research should focus on prospective studies and targeted interventions for CRF to further validate these findings and enhance clinical practice.
Declaration of Competing Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Ethics Statement
The studies involving human participants were reviewed and approved by the ethics committees of Huaibei People's Hospital. Written informed consent for participation was waived in accordance with the national legislation and the institutional requirements.
Manuscript Approval
All authors: Fang Chen, Bingyun Liu, Xiaoqian Cao, Ping Chen, Chen Wang, Peng, Ding, Fenglian Su, Cong Liu.
Author Contributions
FC, XQC, CL: Conception and design. FC, BYL, FLS, PD, PC: Acquisition of data. FC, CL: Data analysis and interpretation. FC, CL: Drafting the revising.
Funding
This study was supported by grants from The Huaibei Science and Technology Plan Project (2021HK005).
Data Availability Statement
The original data could be provided on reasonable request from the authors. Requests to access these datasets should be directed to F.C.
References
- Schmidt, M.E.; Chang-Claude, J.; Vrieling, A.; Heinz, J.; Flesch-Janys, D.; Steindorf, K. Fatigue and quality of life in breast cancer survivors: temporal courses and long-term pattern. J. Cancer Surviv. 2012, 6, 11–19. [Google Scholar] [CrossRef]
- Minton, O.; Berger, A.; Barsevick, A.; Cramp, F.; Goedendorp, M.; Mitchell, S.A.; Stone, P.C. Cancer-related fatigue and its impact on functioning. Cancer 2013, 119, 2124–2130. [Google Scholar] [CrossRef] [PubMed]
- Berger AM, Mooney K, Alvarez-Perez A, Breitbart WS, Carpenter KM, Cella D, Cleeland C, Dotan E, Eisenberger MA, Escalante CP, Jacobsen PB, Jankowski C, et al. Cancer-Related Fatigue, Version 2.2015. Journal of the National Comprehensive Cancer Network : JNCCN 2015;13: 1012-39.
- Bower, JE. Cancer-related fatigue--mechanisms, risk factors, and treatments. Nature reviews Clinical oncology 2014;11: 597-609.
- Glaus, A.; Crow, R.; Hammond, S. A qualitative study to explore the concept of fatigue/tiredness in cancer patients and in healthy individuals. Support. Care Cancer 1996, 4, 82–96. [Google Scholar] [CrossRef]
- Fuhrmann, K.; Mehnert, A.; Geue, K.; Hinz, A. Fatigue in breast cancer patients: psychometric evaluation of the fatigue questionnaire EORTC QLQ-FA13. Breast Cancer 2014, 22, 608–614. [Google Scholar] [CrossRef]
- de Raaf PJ, de Klerk C, van der Rijt CC. Elucidating the behavior of physical fatigue and mental fatigue in cancer patients: a review of the literature. Psycho-oncology 2013;22: 1919-29.
- Schmidt, M.E.; Chang-Claude, J.; Seibold, P.; Vrieling, A.; Heinz, J.; Flesch-Janys, D.; Steindorf, K. Determinants of long-term fatigue in breast cancer survivors: results of a prospective patient cohort study. Psycho-Oncology 2015, 24, 40–46. [Google Scholar] [CrossRef]
- Goldstein, D.; Bennett, B.; Friedlander, M.; Davenport, T.; Hickie, I.; Lloyd, A. Fatigue states after cancer treatment occur both in association with, and independent of, mood disorder: a longitudinal study. BMC Cancer 2006, 6, 240–240. [Google Scholar] [CrossRef]
- Henry-Amar M, Busson R. Does persistent fatigue in survivors relate to cancer? The Lancet Oncology 2016;17: 13512.
- Potthoff, K.; E Schmidt, M.; Wiskemann, J.; Hof, H.; Klassen, O.; Habermann, N.; Beckhove, P.; Debus, J.; Ulrich, C.M.; Steindorf, K. Randomized controlled trial to evaluate the effects of progressive resistance training compared to progressive muscle relaxation in breast cancer patients undergoing adjuvant radiotherapy: the BEST study. BMC Cancer 2013, 13, 162–162. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.E.; Wiskemann, J.; Krakowski-Roosen, H.; Knicker, A.J.; Habermann, N.; Schneeweiss, A.; Ulrich, C.M.; Steindorf, K. Progressive resistance versus relaxation training for breast cancer patients during adjuvant chemotherapy: Design and rationale of a randomized controlled trial (BEATE study). Contemp. Clin. Trials 2013, 34, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.E.; Wiskemann, J.; Armbrust, P.; Schneeweiss, A.; Ulrich, C.M.; Steindorf, K. Effects of resistance exercise on fatigue and quality of life in breast cancer patients undergoing adjuvant chemotherapy: A randomized controlled trial. Int. J. Cancer 2015, 137, 471–480. [Google Scholar] [CrossRef]
- Steindorf, K.; Schmidt, M.E.; Klassen, O.; Ulrich, C.M.; Oelmann, J.; Habermann, N.; Beckhove, P.; Owen, R.; Debus, J.; Wiskemann, J.; et al. Randomized, controlled trial of resistance training in breast cancer patients receiving adjuvant radiotherapy: results on cancer-related fatigue and quality of life. Ann. Oncol. 2014, 25, 2237–2243. [Google Scholar] [CrossRef]
- Ferguson, J.M.; Marquis, J.N.; Taylor, C.B. A script for deep muscle relaxation. DisNervSyst. 1977, 38, 703–8. [Google Scholar]
- Abrahams, H.J.G.; Gielissen, M.F.M.; Schmits, I.C.; Verhagen, C.A.H.H.V.M.; Rovers, M.M.; Knoop, H. Risk factors, prevalence, and course of severe fatigue after breast cancer treatment: a meta-analysis involving 12 327 breast cancer survivors. Ann. Oncol. 2016, 27, 965–974. [Google Scholar] [CrossRef]
- Schmidt, M.E.; Chang-Claude, J.; Seibold, P.; Vrieling, A.; Heinz, J.; Flesch-Janys, D.; Steindorf, K. Determinants of long-term fatigue in breast cancer survivors: results of a prospective patient cohort study. Psycho-Oncology 2015, 24, 40–46. [Google Scholar] [CrossRef]
- Person, H.; Guillemin, F.; Conroy, T.; Velten, M.; Rotonda, C. Factors of the evolution of fatigue dimensions in patients with breast cancer during the 2 years after surgery. Int. J. Cancer 2020, 146, 1827–1835. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, D.; Bennett, B.K.; Webber, K.; Boyle, F.; de Souza, P.L.; Wilcken, N.R.; Scott, E.M.; Toppler, R.; Murie, P.; O'Malley, L.; et al. Cancer-Related Fatigue in Women With Breast Cancer: Outcomes of a 5-Year Prospective Cohort Study. J. Clin. Oncol. 2012, 30, 1805–1812. [Google Scholar] [CrossRef]
- de Jong, N.; Candel, M.J.J.M.; Schouten, H.C.; Abu-Saad, H.H.; Courtens, A.M. Prevalence and course of fatigue in breast cancer patients receiving adjuvant chemotherapy. Ann. Oncol. 2004, 15, 896–905. [Google Scholar] [CrossRef]
- de Jong, N.; Candel, M.J.J.M.; Schouten, H.C.; Abu-Saad, H.H.; Courtens, A.M. Course of mental fatigue and motivation in breast cancer patients receiving adjuvant chemotherapy. Ann. Oncol. 2005, 16, 372–382. [Google Scholar] [CrossRef]
- Karshikoff, B.; Sundelin, T.; Lasselin, J. Role of Inflammation in Human Fatigue: Relevance of Multidimensional Assessments and Potential Neuronal Mechanisms. Front. Immunol. 2017, 8, 21. [Google Scholar] [CrossRef] [PubMed]
- Bandani-Susan, B.; Montazeri, A.; Haghighizadeh, M.H.; Araban, M. The effect of mobile health educational intervention on body image and fatigue in breast cancer survivors: a randomized controlled trial. Ir. J. Med Sci. 2022, 191, 1599–1605. [Google Scholar] [CrossRef]
- Haghighat, S.; Akbari, M.E.; Holakouei, K.; Rahimi, A.; Montazeri, A. Factors predicting fatigue in breast cancer patients. Support. Care Cancer 2003, 11, 533–538. [Google Scholar] [CrossRef]
- Ku, G.D.l.C.; Karamchandani, M.; Chambergo-Michilot, D.; Narvaez-Rojas, A.R.; Jonczyk, M.; Príncipe-Meneses, F.S.; Posawatz, D.; Nardello, S.; Chatterjee, A. Does Breast-Conserving Surgery with Radiotherapy have a Better Survival than Mastectomy? A Meta-Analysis of More than 1,500,000 Patients. Ann. Surg. Oncol. 2022, 29, 6163–6188. [Google Scholar] [CrossRef]
- Bartlett, J.; Sgroi, D.; Treuner, K.; Zhang, Y.; Ahmed, I.; Piper, T.; Salunga, R.; Brachtel, E.; Pirrie, S.; Schnabel, C.; et al. Breast Cancer Index and prediction of benefit from extended endocrine therapy in breast cancer patients treated in the Adjuvant Tamoxifen—To Offer More? (aTTom) trial. Ann. Oncol. 2019, 30, 1776–1783. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Random forest parameter selection and importance ranking of variables.
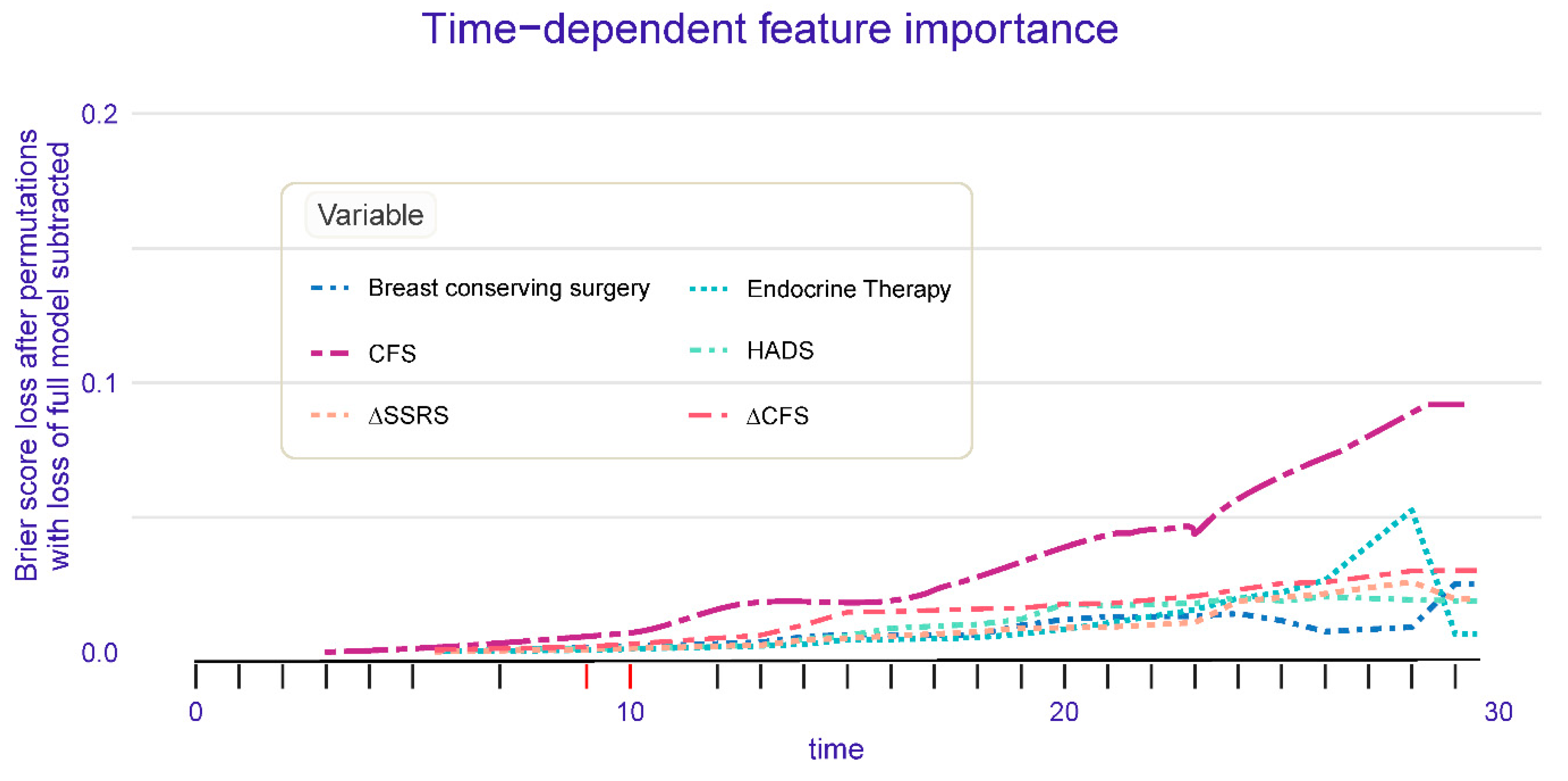
Figure 2.
(A) Sample Distribution for Propensity Matching Analysis; (B) Propensity score matching analysis of the standardized mean difference results for the different variables.
Figure 2.
(A) Sample Distribution for Propensity Matching Analysis; (B) Propensity score matching analysis of the standardized mean difference results for the different variables.
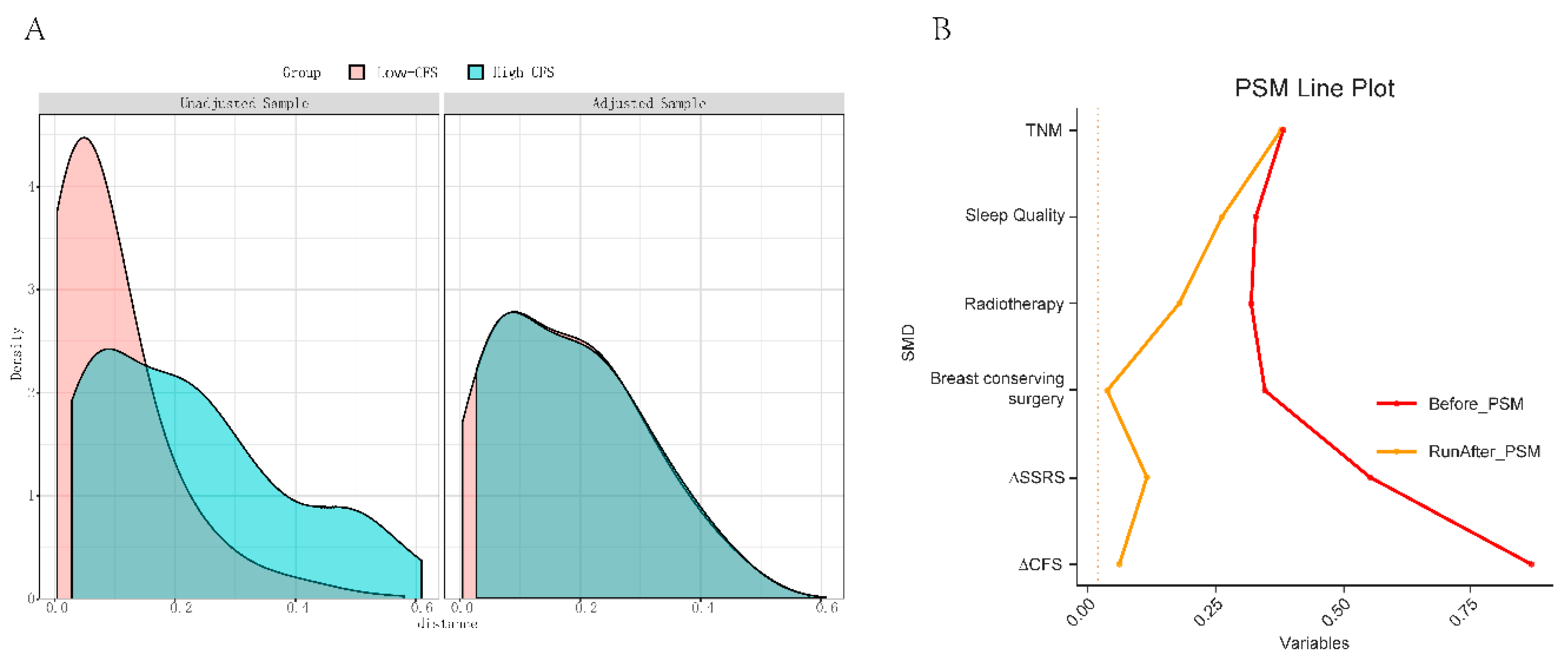
Figure 3.
(A) Survival analysis of Low/High CFS patients before propensity score matching; (B) Survival analysis of Low/High CFS patients after propensity score matching.
Figure 3.
(A) Survival analysis of Low/High CFS patients before propensity score matching; (B) Survival analysis of Low/High CFS patients after propensity score matching.
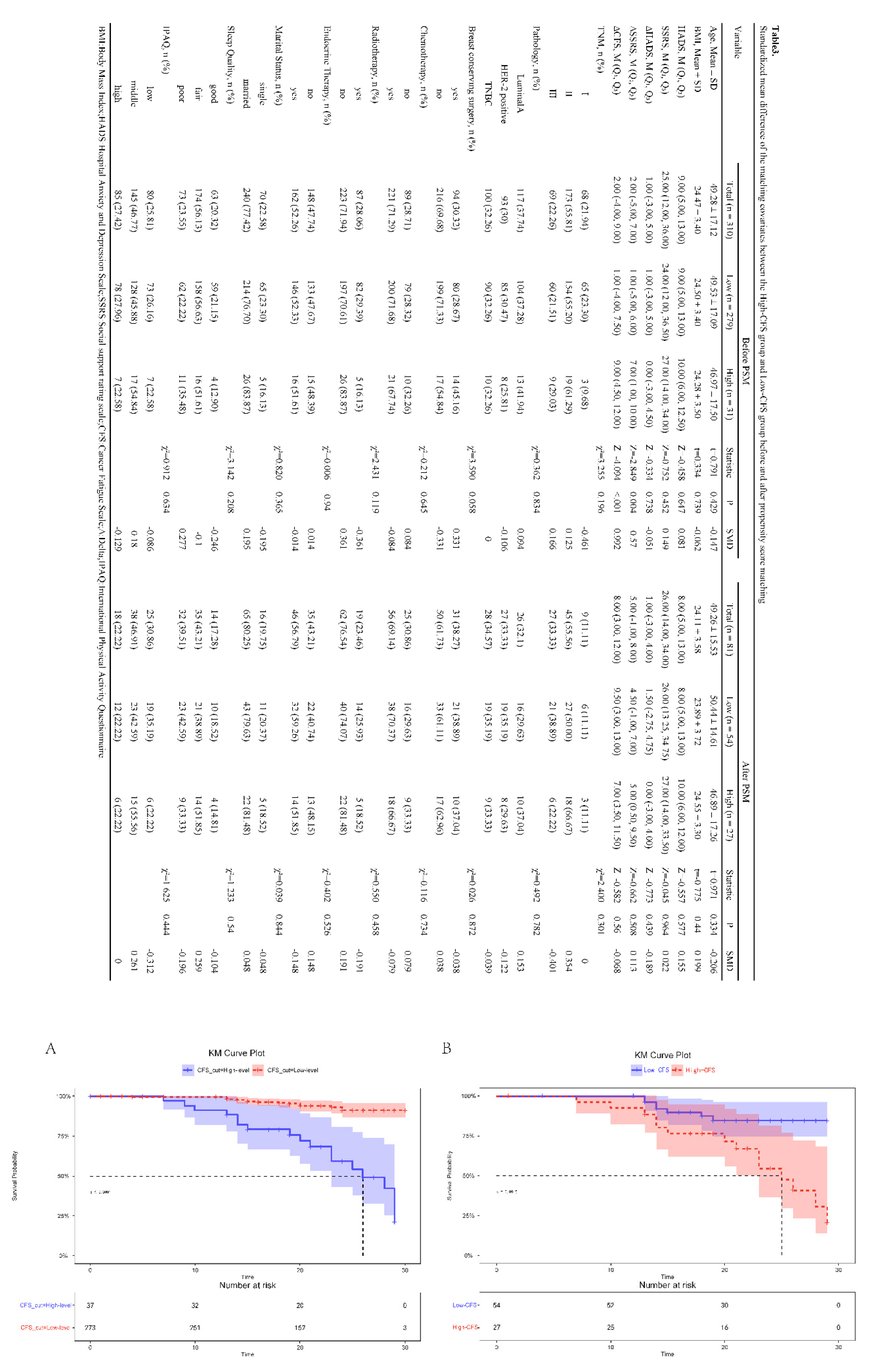
Figure 4.
The optimal cut-off value of cancer fatigue scale by restricted cubic spline. (A) Before propensity score matching; (B) After propensity score matching.
Figure 4.
The optimal cut-off value of cancer fatigue scale by restricted cubic spline. (A) Before propensity score matching; (B) After propensity score matching.
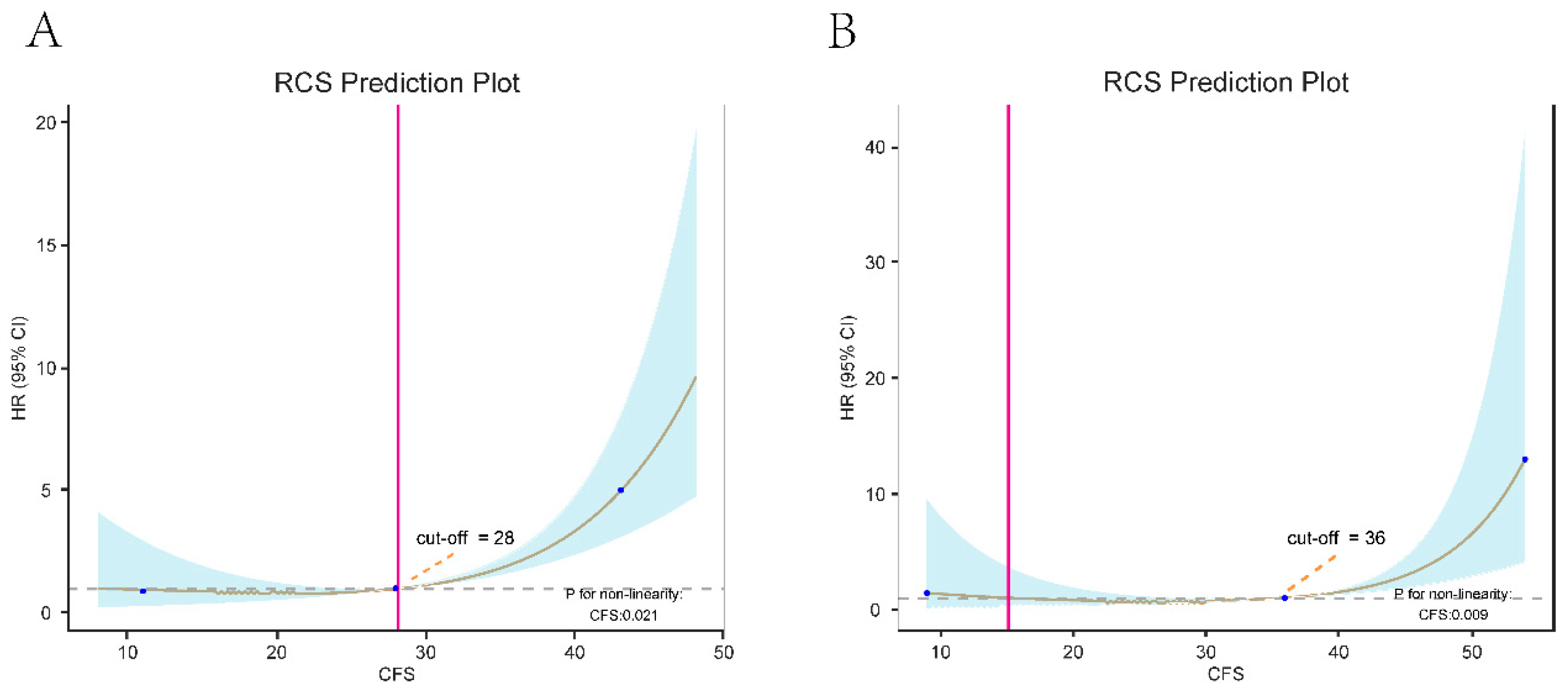

Table 1.
Baseline characteristics of 310 included patients.
| Variable | Total (n = 310) | Stable (n = 276) | Recurrence (n = 34) | Statistic | P | SMD |
| Age, Mean ± SD | 49.28 ± 17.12 | 49.22 ± 16.94 | 49.76 ± 18.79 | t=-0.176 | 0.861 | 0.029 |
| BMI, Mean ± SD | 24.47 ± 3.40 | 24.55 ± 3.38 | 23.83 ± 3.59 | t=1.172 | 0.242 | -0.202 |
| HADS, M (Q₁, Q₃) | 9.00 (5.00, 13.00) | 9.00 (5.00, 13.00) | 11.00 (7.00, 14.50) | Z=-2.145 | 0.032 | 0.438 |
| SSRS, M (Q₁, Q₃) | 25.00 (12.00, 36.00) | 24.50 (12.00, 36.00) | 27.50 (17.00, 38.25) | Z=-0.889 | 0.374 | 0.154 |
| CFS, M (Q₁, Q₃) | 28.00 (18.25, 37.00) | 27.00 (17.00, 35.25) | 44.00 (26.00, 53.50) | Z=-5.393 | <.001 | 1.018 |
| ∆HADS, M (Q₁, Q₃) | 1.00 (-3.00, 5.00) | 0.00 (-3.00, 4.00) | 2.00 (0.00, 5.00) | Z=-1.775 | 0.076 | 0.388 |
| ∆SSRS, M (Q₁, Q₃) | 2.00 (-5.00, 7.00) | 1.00 (-5.00, 6.00) | 5.00 (1.00, 9.00) | Z=-2.961 | 0.003 | 0.66 |
| ∆CFS, M (Q₁, Q₃) | 2.00 (-4.00, 9.00) | 1.00 (-4.00, 7.25) | 8.50 (3.25, 12.00) | Z=-4.155 | <.001 | 0.987 |
| TNM, n (%) | χ²=4.804 | 0.091 | ||||
| Ⅰ | 68 (21.94) | 65 (23.55) | 3 (8.82) | -0.519 | ||
| Ⅱ | 173 (55.81) | 153 (55.43) | 20 (58.82) | 0.069 | ||
| Ⅲ | 69 (22.26) | 58 (21.01) | 11 (32.35) | 0.242 | ||
| Pathology, n (%) | χ²=0.756 | 0.685 | ||||
| LuminalA | 117 (37.74) | 104 (37.68) | 13 (38.24) | 0.011 | ||
| HER-2 positive | 93 (30) | 81 (29.35) | 12 (35.29) | 0.124 | ||
| TNBC | 100 (32.26) | 91 (32.97) | 9 (26.47) | -0.147 | ||
| Breast conserving surgery, n (%) | χ²=11.808 | <.001 | ||||
| yes | 94 (30.32) | 75 (27.17) | 19 (55.88) | 0.578 | ||
| no | 216 (69.68) | 201 (72.83) | 15 (44.12) | -0.578 | ||
| Chemotherapy, n (%) | χ²=0.501 | 0.479 | ||||
| no | 89 (28.71) | 81 (29.35) | 8 (23.53) | -0.137 | ||
| yes | 221 (71.29) | 195 (70.65) | 26 (76.47) | 0.137 | ||
| Radiotherapy, n (%) | χ²=3.376 | 0.066 | ||||
| yes | 87 (28.06) | 82 (29.71) | 5 (14.71) | -0.424 | ||
| no | 223 (71.94) | 194 (70.29) | 29 (85.29) | 0.424 | ||
| Endocrine Therapy, n (%) | χ²=11.286 | <.001 | ||||
| no | 148 (47.74) | 141 (51.09) | 7 (20.59) | -0.754 | ||
| yes | 162 (52.26) | 135 (48.91) | 27 (79.41) | 0.754 | ||
| Marital Status, n (%) | χ²=1.355 | 0.244 | ||||
| single | 70 (22.58) | 65 (23.55) | 5 (14.71) | -0.25 | ||
| married | 240 (77.42) | 211 (76.45) | 29 (85.29) | 0.25 | ||
| Sleep Quality, n (%) | χ²=7.417 | 0.025 | ||||
| good | 63 (20.32) | 61 (22.10) | 2 (5.88) | -0.689 | ||
| fair | 174 (56.13) | 155 (56.16) | 19 (55.88) | -0.006 | ||
| poor | 73 (23.55) | 60 (21.74) | 13 (38.24) | 0.339 | ||
| IPAQ, n (%) | χ²=0.404 | 0.817 | ||||
| low | 80 (25.81) | 70 (25.36) | 10 (29.41) | 0.089 | ||
| middle | 145 (46.77) | 129 (46.74) | 16 (47.06) | 0.006 | ||
| high | 85 (27.42) | 77 (27.90) | 8 (23.53) | -0.103 |
BMI: Body Mass Index; HADS: Hospital Anxiety and Depression Scale; SSRS: Social support rating scale; CFS: Cancer Fatigue Scale; ∆: Delta; IPAQ: International Physical Activity Questionnaire.
Table 2.
Univariate and multivariate Cox analysis.
| Variables | β | S.E | Z | Univariate P |
HR (95%CI) | Multivariate | ||||
| β | S.E | Z | P | HR (95%CI) | ||||||
| TNM Ⅰ Ⅱ Ⅲ |
0.73 1.14 |
0.62 0.65 |
1.18 1.75 |
0.237 0.08 |
1.00 (Reference) 2.08 (0.62 ~ 7.01) 3.13 (0.87 ~ 11.22) |
|||||
| Pathology LuminalA HER-2 positive TNBC |
0.08 -0.27 |
0.4 0.43 |
0.19 -0.62 |
0.851 0.535 |
1.00 (Reference) 1.08 (0.49 ~ 2.36) 0.76 (0.33 ~ 1.79) |
|||||
| Breast conserving surgery yes no |
-1.18 | 0.35 | -3.42 | <.001 | 1.00 (Reference) 0.31 (0.16 ~ 0.60) |
-0.85 | 0.38 | -2.26 | 0.024 | 1.00 (Reference) 0.43 (0.20 ~ 0.89) |
| Chemotherapy no yes | 0.24 | 0.4 | 0.59 | 0.558 | 1.00 (Reference) 1.27 (0.57 ~ 2.80) |
|||||
| Radiotherapy yes no | 0.89 | 0.48 | 1.83 | 0.068 | 1.00 (Reference) 2.42 (0.94 ~ 6.27) |
|||||
| Endocrine Therapy no yes |
1.43 | 0.43 | 3.37 | <.001 | 1.00 (Reference) 4.20 (1.82 ~ 9.68) |
1.96 | 0.51 | 3.88 | <.001 | 1.00 (Reference) 7.13 (2.64 ~ 19.22) |
| Marital Status single married | 0.52 | 0.49 | 1.07 | 0.285 | 1.00 (Reference) 1.68 (0.65 ~ 4.36) |
|||||
| Sleep Quality good fair poor |
1.26 1.87 |
0.74 0.76 |
1.7 2.46 |
0.09 0.014 |
1.00 (Reference) 3.53 (0.82 ~ 15.16) 6.46 (1.46 ~ 28.67) |
1.03 0.89 |
0.76 0.79 |
1.35 1.12 |
0.178 0.261 |
1.00 (Reference) 2.79 (0.63 ~ 12.45) 2.42 (0.52 ~ 11.35) |
| IPAQ low middle high Age BMI HADS, M SSRS, M CFS, M ∆HADS, M ∆SSRS, M |
-0.03 -0.26 0.01 -0.06 0.09 0.01 0.09 0.07 0.07 |
0.4 0. 470. 010. 050. 040. 010. 020. 040. 03 |
-0.07 -0.55 0.64 -1.29 2.51 0.78 5.37 1.89 2.59 |
0. 9430. 5850. 5250. 1960. 0120. 434<. 0010. 059 0.01 |
1.00 (Reference) 0.97 (0.44 ~ 2.14) 0.77 (0.30 ~ 1.96) 1.01 (0.99 ~ 1.03) 0.94 (0.85 ~ 1.03) 1.09 (1.02 ~ 1.17) 1.01 (0.99 ~ 1.04) 1.09 (1.06 ~ 1.13) 1.08 (1.00 ~ 1.16) 1.07 (1.02 ~ 1.13) |
0.08 0.07 0.06 |
0.04 0.02 0.03 |
2.15 3.9 2.22 |
0.032 <.001 0.026 |
1.09 (1.01 ~ 1.17) 1.07 (1.03 ~ 1.10) 1.07 (1.01 ~ 1.13) |
| ∆CFS, M | 0.1 | 0.03 | 4.05 | <.001 | 1.11 (1.06 ~ 1.17) | 0.07 | 0.03 | 2.23 | 0.026 | 1.07 (1.01 ~ 1.14) |
BMI: Body Mass Index; HADS: Hospital Anxiety and Depression Scale; SSRS: Social support rating scale; CFS: Cancer Fatigue. Scale; ∆:Delta; IPAQ: International Physical Activity Questionnaire; HR: Hazard Ratio, CI: Confidence Interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



