
Submitted:
04 September 2024
Posted:
04 September 2024
You are already at the latest version
Abstract
Background: Antimicrobial consumption data in Latin America is scarce and usually spread out within different sources for AMC calculations, making it difficult to both standardize and compare regions through similar time frames. The main objective was to analyze antimicrobial consumption trends in Social Security tertiary care hospitals in Costa Rica in the period spanning January 2017 to December 2021, using both defined daily doses (DDD)/100 bed days and DDD/100 discharges. Methods: Retrospective observational study of antimicrobial consumption. Global consumption trends were calculated and expressed in DDD/100 bed days and DDD/100 discharges. Trends in antimicrobial consumption were analyzed using a simple linear regression model to determine potential differences in antimicrobial usage throughout the study’s duration. Results: A statistically significant increase in the consumption expressed in DDD/100 discharges was observed in the following groups: carbapenems: 35.62% (p<0.0001), trimethoprim-sulfamethoxazole: 62.50% (p<0.0001), echinocandins: 20.73% (p=0.01) and azole antifungals: 61.58% (p<0.0001). Additionally, a statistically significant increase of 40.43% in the consumption of azole antifungals expressed in DDD/100 bed days was observed (p=0.0008). In contrast, a statistically significant decrease in consumption expressed in DDD/100 discharges was identified for cephalosporins -21.97% (p<0.0001) and macrolides -51.67% (p<0.0001). Conclusions: This five-year analysis demonstrated trends over time in overall antimicrobial consumption measured in DDD/100 bed days do not correlate with trends in DDD/100 discharge rates. Continually, the comparison between DDD/100 bed days and DDD/100 discharges allows for complementary comparisons to be made regarding antimicrobial exposure in a clinical setting.
Keywords:
Antimicrobial consumption
; Antimicrobial stewardship
; Defined daily dose
1. Introduction
Antimicrobial resistance (AMR) poses a major threat to global human health [1]. A study published in 2019 established a link between AMR and approximately 4.95 million deaths, with increased projections to 10 million deaths per annuum by 2050 [2]. Liberal antimicrobial use is one of the main drivers of AMR; hence, surveillance and optimal use of the latter are among the key strategies to mitigate AMR and are included in the five main objectives of the World Health Organization (WHO) Global Action Plan (GAP) on AMR [3].
Most of the antimicrobial consumption occurs in outpatient and community care. However, in hospital settings, the density of antimicrobial use is much higher, and highly vulnerable patients are in close spatial proximity to one another, thus contributing to the increased risk of the development and spread of resistant microbial pathogens [4]. Additionally, fungal diseases represent a growing concern with a significant impact on mobility and mortality as has been previously observed with bacteria, it is known that the improper use of antifungals poses a selective pressure that is a key driver for the emergence and dissemination of antifungal resistant strains in clinical settings [5,6].
Monitoring AMC in health facilities is an important element of all Antimicrobial Stewardship Programs (ASP) [7]. To facilitate standardizing results and the ability to compare consumption information across time and different hospitals, the most widely implemented system is the defined daily doses (DDD), according to the WHO Anatomical Therapeutic Chemical (ATC) system [8,9,10]. Standardizing measures of hospital activity and hospital consumption data must correspond strictly to the time under surveillance and hospital activity units covered (bed days and/or discharges) [4,9]. Its role is to detect points most susceptible to improvements and to evaluate the impact of interventions through the comparison between hospitals of the same level, and the analysis of time series in a single center, as well as being used as support for the study of the ecological impact [8,11].
In Costa Rica, a country with a total population of 5,044,197 inhabitants, public healthcare facilities belong to the Social Security (Caja Costarricense de Seguro Social- CCSS) network model, which is independent from the Ministry of Health. This model is based on three attention levels, where the third level stands as the maximum complexity. Furthermore, an institutional medicines policy has been developed based on the WHO List of Essential Medicines model, which seeks to satisfy most of the population’s health necessities. Medication is accessible to patients through the universal coverage provided by CCSS [12,13,14,15].
Nonetheless, the Ministry of Health of Costa Rica established its own National Action Plan to Mitigate Antimicrobial Resistance in 2018, in which surveillance of AMC in healthcare settings was mandatory. This initiative is yet to be implemented, thus rendering knowledge on this topic scarce across Costa Rica and its neighboring Central-American nations [16,17].
The objective of the present study was to analyze antimicrobial consumption trends in Social Security’s tertiary care hospitals across Costa Rica throughout the period 2017-2021, using both DDD/100 bed days and DDD/100 discharges as measurements of hospital activity.
The introduction should briefly place the study in a broad context and highlight why it is important. It should define the purpose of the work and its significance. The current state of the research field should be carefully reviewed, and key publications cited. Please highlight controversial and diverging hypotheses when necessary. Finally, briefly mention the main aim of the work and highlight the principal conclusions. As far as possible, please keep the introduction comprehensible to scientists outside your particular field of research. References should be numbered in order of appearance and indicated by a numeral or numerals in square brackets—e.g., [1] or [2,3], or [4,5,6]. See the end of the document for further details on references.
2. Results
2.1. Indicators of Hospital Activity
Table 1 presents the mean of unadjusted DDD, bed days, discharges and length. During these five years, a slight increase in DDD was observed. In contrast, the number of bed days and discharges showed a downward trend (-0,13% and -0,15%, respectively). Contrastingly, the length of reported stay did not report a statistically significant change in the same time frame.
2.2. Antimicrobial Consumption Trends in the Period 2017-2021
Global trends of antimicrobial consumption during this period are shown in Table 2. Evidently, overall consumption of antimicrobial medication increased in DDD/100 discharges from 270.63 to 313.25 (+15.75%, p=0.0007). On the other hand, the consumption calculated in DDD/100 bed days showed no statistically significant changes, ranging from 61.35 to 61.78 (+0.70%, p= 0.31). In this general overview, despite antibiotics having a decreased use, they still showed a significantly increased used when compared to antivirals. However, no statistical difference was discerned across the period. (Figure 1). Antifungal were the only group with statistically significant increases in both DDD/100 bed days from 26.30 to 32.49 (+23.53%, p=0.05) and DDD/100 discharges from 80.41 to 123.52 (+53.61%, p <0.0001).
Detailed consumption of the main antimicrobial groups are shown in Table 3. The consumption of cephalosporins (J01D) is presented as the most used antimicrobial group, followed by penicillin (J01C) and carbapenems (J01DH, J01DF). The following groups showed a statistically significant increase in consumption, measured in DDD/100 discharges: carbapenems from 699.00 (2017) to 948.00 (2021) representing an increase of 35,62% (p<0.0001), trimethoprim-sulfamethoxazole from 475.60 (2017) to 772.85 (2021) with an increase of 62.50% (p<0.0001), echinocandins from 156.94 (2017) to 189.48 (2021) increasing its consumption by 20.73% and azole antifungals 647.18 (2017) to 1045.72 (2021) with an increase of 61.58% (p<0.0001). Also, a statistically significant increase of 40.43% in the consumption of azole antifungals expressed in DDD/100 bed days was reported, from 116.52 (2017) to 163.64 (2021) (p=0.0008). In contrast, a statistically significant decrease in consumption expressed in DDD/100 discharges was identified for cephalosporins -21.97% from 2495.15 (2017) to 1946.72 (2021) and macrolides -51.67% from 360.60 (2017) to 174.26 (2021) (p<0.0001). Macrolides also showed a –51.67% decrease in the consumption expressed in DDD/100 bed days, from 50.42 (2017) to 25.39 (2021) (p=0.005).
3. Discussion
Latin American countries do not regularly measure their antimicrobial consumption, and only a few occasionally review the overall consumption of antibiotics within their territory [17]. Due to these inconsistencies, data in this region is scarce, and usually spread out within different sources for AMC calculations, making it difficult to both standardize and compare regions through similar time frames.
This is the first multicentric study with standardized methodology that analyzes antimicrobial consumption trends in Social Security acute tertiary care hospitals in Costa Rica. Furthermore, another advantage this study presents is that it was carried out with data from the two hospitals in Costa Rica with the greatest complexity. Monitoring the consumption of antimicrobials in the hospital setting is a necessary measure, both for cost optimization reasons and to develop further strategies to suppress the apparition of resistant strains. Additionally, the study may become useful when evaluation stewardship programs follow the results and trends presented previously [9,18].
Variations in in-hospital antimicrobial use may be due to several factors. Firstly, it may depend on both hospital and patient characteristics, in addition to any pre-existing antibiotic policies, as well as the physician’s education or beliefs held by different health care systems. However, a substantial part of the differences in AMC metrics may be the result of differences in methods to measure antimicrobial use [19].
The most widely accepted AMC measure is defined daily dose (DDD). DDD is the assumed average maintenance dose per day for a drug used for its main indication in adults [20]. The WHO methodology ATC/DDD allows for data to be collected on an aggregated level and does not rely only on person-level data, which is largely unavailable in many countries. The flexibility in the choice of data sources for AMC enables countries with limited resources to use pre-existing data sources to build up sustainable systems for AMC surveillance [17].
Even though the ATC/DDD system for all drugs was available since the 1980s, it was not widely used, and in some cases misunderstood. This resulted in widespread confusion, thanks to misinformed publications along with incomplete and unspecified publication of antibiotic guidelines [19].
Most publications that quantify antimicrobial consumption trends in the hospital setting with this methodology use DDD/100 bed days as the standard denominator. This parameter reflects the hospital's exposure to antimicrobials, but does not describe neither number nor proportion of patients treated with antimicrobials, while parameters such as DDD/100 discharges provides information on exposure per patient and helps to interpret consumption trends over time as it shows changes in hospital activity [18,21].
Results from this study showed that trends over time in overall antimicrobial consumption and consumption per groups in DDD per 100 bed-days consistently do not correlate with trends in DDD per 100 discharges (Table 2 and Table 3). Differences in trends between the two units of measurement seem to be the result of changes in resource indicators over time, both bed days and discharges had statistically significant increase changes during the study period however the length of stay remained stable.
Comparing AMC results with other hospitals across different geographical regions remains a challenge, given the heterogeneity in methodologies employed in this type of study. Despite this challenge, some similarities were found in the literature.
The WHO Global Antimicrobial Resistance and Use Surveillance System (GLASS) report from 2022 provided information on 36 countries, territories and areas (CTAs) on the status of AMC surveillance implementation on data from 2020 [22,23]. However, interpreting data from this report becomes a challenge, given the small number of reporting CTAs and the wide variety of AMC data collection. AMC data from 26 CTAs have been included in the analysis reporting on all antimicrobials. This data demonstrates that antibacterials are mainly the most consumed class of antimicrobials. Despite the variation in the consumption of antibacterial pharmacological subgroups across CTAs, penicillins were often the most frequently consumed subgroup, with a median consumption of 7.1 (range, 1.0-24.2) DDD per 1000 inhabitants per day, representing 34% of total antibacterial consumption. Among cephalosporins, third-generation cephalosporins (J01DD) were the most frequently prescribed chemical subgroups within cephalosporins in 12 CTAs, with a median relative consumption of 43% (range, 9-99%). Consumption of antimycotics and antifungals for systemic use (J02, D01B) and antivirals (ATC J05) was reported by 12 CTAs, resulting in a median value of 0.9 (range, 0.03-3.35) and 1.7 (range, 0.8-3.36) DDD per 1000 inhabitants per day, respectively[22,23].
Regional data from the Annual Epidemiological Report of 2022 of the European Centre for Disease Prevention and Control reports that in the hospital sector in 2022, penicillins (J01C) represented the highest proportion of hospital consumption in 18 European countries, and cephalosporins and other beta-lactams (J01D) represented the highest proportion of hospital consumption in nine countries [24]. Additionally, between 2013 and 2022 a statistically significant increases were observed in the hospital sector for tetracyclines (J01A), sulfonamides and trimethoprim (J01E), and other antibacterials (J01X). No significant trend was detected for consumption of penicillins (J01C), cephalosporins and other beta-lactams (J01D), and macrolides, lincosamides and streptogramins (J01F).
In addition to the WHO’s world report, as well as European data, a study was conducted in 2019 across Latin America. This study showed highly variable AMC from 1.91 DDD/1000 inhabitants in private institutions in Paraguay to 36.26 DDD/1000 inhabitants in Argentina. Furthermore, this study demonstrated that penicillin was the most consumed group in all countries included except Paraguay, while macrolides and lincosamides were ranked second across the board [17].
In our analysis, we included information from specific regions and countries. For example, Catalonia, a region of Spain with 7,5 million inhabitants, where the most frequently used groups of antibiotics in the period 2007 to 2019 were penicillin(J01C), quinolones (J01M), cephalosporins (J01DB, J01DC, J01DD and J01DE), other antibiotics (J01X) and carbapenems (J01DH). In 2009, these antibiotic groups represented 88.9% of total antibiotic consumption in this region. Additionally, a study conducted in México with hospitals from secondary and tertiary-care level hospitals during 2016 and 2017, where AMC was quantify using DDD/100 occupied bed-days showed that the antimicrobials with the higher consumption were cephalosporines, carbapenems and vancomycin [25].
Similarly in Gansu Province in China a study from 2012 to 2020 reported that the top three antibiotics used were J01C (beta-lactam antibacterials, penicillins), J01F (macrolides, lincosamides and streptogramins), and J01D (other beta-lactam antibacterials, cephalosporins), accounting for 45.15%, 31.40%, and 11.99% respectively [26]. Similarly, our study found that the antibiotics most used were cephalosporins, penicillis and carbapenems.
With regards to the correlation of antimicrobial consumption trends in the Canadian Antimicrobial Resistance Surveillance System Report, published in 2022 by the Public Health Agency of Canada, showed AMC trends between 2017 and 2021, reporting that the national antimicrobial consumption decreased by 26.9%, from 17.0 to 12.5 DDDs per 1,000 inhabitants per day, both the healthcare sector and the community sector experienced declines at 25.3% (1.4 to 1.0 DDDs per 1,000 inhabitants per day) and 27.0% (15.7 to 11.4 DDDs per 1,000 inhabitants per day) respectively, with the most pronounced period at the start of the COVID-19 pandemic (2020 to 2021). During this five-year period, at least 90.0% of antimicrobials (DDDs per 1,000 inhabitants per day) were dispensed in the community [27].
A study from Colombia conducted from 2019 to 2020 demonstrated changes in the reported of DDD/100 occupied beds for specific antibiotics, such as ceftriaxone in ICU wards (2019: 17,584; 2020: 19,857). In addition, the antibiotic consumption showed an increase for piperacillin/tazobactam (from 91,606 to 94,076), ertapenem ( from 5,793 to 6,051), and cefepime (26,809 to 38,780) from 2019 to 2020 [28]. Similarly, our results are in line with these findings. An increased consumption was observed n carbapenems and penicillin. Despite this, our study is not fully comparable, given a different methodology was employed.
One of the most significant findings is an increase of 35.62% in the Carbapenem use trend expressed in DDD/100 discharges. This overall increase in the use of carbapenems could lead to the apparition of carbapenem-resistant bacteria. COVID-19 could be partially culpable for this increase, although this is yet to be confirmed. Despite COVID-19 being a viral disease, antibiotic treatment including broad-spectrum antibiotics was prescribed to all patients regardless of the severity of illness, especially near the beginning of the pandemic. This practice was supported by reported, suspected, or confirmed secondary bacterial infections in COVID-19 patients [29].
Additionally, a study from Catalonia in reported a worrisome increase in use of Carbapenem by 88.43%, from 3.37 DDD/100-Patient Day (PD) to 6.35 DDD/100-PD (p<0.001). This eight-year surveillance study (2008 to 2015) showed a sustained and widespread increase in carbapenem use. This trend is consistent with tendencies observed in other European countries. Meropenem was the most prescribed carbapenem, while consumption of imipenem-cilastatin showed a downward trend [30].
Continually, a peculiar finding was the downward trend in cephalosporins consumption. A possible explanation is the substitution of cephalosporins with broad-spectrum antibiotics during the pandemic period. Since 2018, Antimicrobial Stewardship programs have been operating in hospitals included in this study, promoting de-escalation and shortened therapies. Furthermore, a downward trend in macrolide consumption was observed. This downward trend could be explained by the finding that antibiotics of the macrolide family have long been considered drugs of potential utility in the management of infections caused by S. pneumoniae. However, with the emergence of macrolide resistance, their clinical value in pneumococcal infections is questioned. Recent reports show that macrolide resistance in S. pneumoniae is geographically variable, ranging from 30 to 50% globally [31].
In contrast, an upward trend was seen with sulfamethoxazole and trimethoprim due to an internal policy for empiric prescriptions established by the AMS program in 2018; restricting the use of some antibiotics with high prevalence of resistance such as cephalexin, cephalothin, clindamycin, gentamicin and oxacillin, the prescription of these antibiotics must be justified with an antibiogram or according to preexisting protocols.
Moreover, an increasing trend in the consumption of azole antifungals was reported. This finding becomes highly concerning, especially considering the implications of antifungals concerning the mobility and mortality of mycoses. The clinical consequences of this resistance are observed in treatment failures and changes in the prevalence of fungal species like Candida auris, which is spreading at an alarming rate throughout United States health-care facilities and is considered an “urgent antimicrobial resistance threat” by the health agency [32].
It is important to mention that this study is not without limitations. Firstly, we cannot be certain that the prescribing practices observed were representative of other hospitals of lower complexity in Costa Rica. Additionally, the results could have had an influence derived from the Covid 19 pandemic like other studies. Furthermore, other analysis between hospitals of different complexity, other reference hospitals and private institutions and stratifying services in ICU, medical and surgical would improve the quantity of data obtained and more robust conclusions could be formulated. One of the most reported methodologies in the literature to monitor AMC at a hospital level is the Point-Prevalence Survey of hospital antibiotic use. Even though these surveys are also useful to identify AMS priorities they do not allow for evaluation of duration of therapy, and more research is needed to understand current antibiotic prescribing patterns with respect to duration because this has been a major driver of inappropriate antibiotic use [33].
4. Materials and Methods
4.1. Setting and Study Design
This retrospective observational study was conducted in General Tertiary Care Hospitals from CCSS. According to available data, two out of the three hospitals were included: Hospital San Juan de Dios (635 beds) and Hospital México (466 beds). These hospitals provide care for approximately 3,000,000 people in medical and surgical services, as well as intensive care units (ICU) and ambulatory care facilities. This study was approved by the Costa Rican Social Security Ethics Committee: CEC-CENTRAL-CCSS (Protocol #R022-SABI-00319).
4.2. Data Collection
Data was collected monthly starting from January 2017 to December 2021, with the support of the pharmacy department software “Integrated Pharmacy System” (SIFA). Sixty-one antimicrobials for systemic use (J01, J02 and J05) according to the WHO- ATC classification, representing 46 different active principles were included in the antimicrobial consumption quantification. Pediatric hospital wards, as well as units that do not generate high rates of discharge or occupied bed days (e.g emergency services) were excluded from the data collection process. Global consumption trends were calculated and expressed in DDD/100 bed days and DDD/100 discharges employing the WHO ATC-DDD Index 2023 for all five years, as the assumed average maintenance dose per day for a drug used for its main indication adults. Before starting the study, the responsible pharmacists were trained in WHO ATC-DDD calculation and usage of the DDD Excel Calculator to guarantee a homogeneous collection of data[9,10].
4.3. Statistics Analysis
Trends in antimicrobial consumption were analyzed using a simple linear regression model to determine potential differences in antimicrobial usage throughout the period of study. Simple linear regression was tested to determine whether there was a significant difference between the calculated coefficient and zero. The comparison of DDD, patient days, discharges, and average bed days between 2017 and 2021 was carried out using the Wilcoxon signed-rank test. P values of < 0.05 were considered statistically significant. Statistical analysis was performed using SASÒ Studio OnDemand for Academics (SASÒ Institute Inc, USA).
5. Conclusions
Throughout this five-year study, the trends over time in overall antimicrobial consumption and consumption per groups in DDD per 100 bed-days consistently do not correlate with trends in DDD per 100 discharges. A concerning increase in carbapenem consumption expressed in DDD/100 discharges was observed, a pattern possibly explained by the overuse of board-spectrum antibiotics during pandemic. In contrast a downward trend in cephalosporins consumption was noticed, this decrease is possibly due to AMS interventions established since 2018 in the participating hospitals. The increasing use of azole antifungals could lead to the development of fungal species resistant to the molecules available in our region. Furthermore, it is important to conclude that the comparison between DDD/100 bed days and DDD/100 discharges allows us to complement information about antimicrobial exposure in a clinical setting, with DDD/100 bed days it is possible to describe antibiotic exposure at a hospital level, but only DDD/100 discharges can indicate exposure at a patient level. Knowing the consumption of antimicrobials in a health institution is the first step to improving the rational use and reducing bacterial resistance of these drugs. To determine this consumption, the measurement standards must be standardized and validated to be able to compare within the institution and with other institutions.
Author Contributions
Conception and design: CFB, SG and ARE, analysis and interpretation of data: CFB, SG, ARE, MRC, DGZ and JCC, drafting of the paper or revision for intellectual content: CFB, SG, LEH, ARE, MRC, DGZ and JCC. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was approved by the Costa Rica Social Security Ethics Committee: CEC-CENTRAL-CCSS (Protocol #R022-SABI-00319).
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
This study is a part of a PhD program in Pharmacology of the Universitat Autònoma de Barcelona (Spain). These data were previously presented as a poster, in the XXVII Spanish Society of Infectious Diseases and Clinical Microbiology (SEIMC) Congress (2024), number 0640.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Global action plan on antimicrobial resistance Available online:. Available online: https://www.who.int/publications-detail-redirect/9789241509763 (accessed on May 19, 2024).
- Murray, C.J.L.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Aguilar, G.R.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. The Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Antimicrobial resistance. https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance. (accessed on 24 February 2020).
- World Health Organization. GLASS | Global antimicrobial resistance surveillance system (GLASS) report. https://www.who.int/glass/resources/publications/early-implementation-report-2017-2018/en/. (accessed on 20 February 2024).
- CDC 2019 Antibiotic Resistance Threats Report Available online:. Available online: https://www.cdc.gov/antimicrobial-resistance/data-research/threats/index.html (accessed on May 21, 2024).
- Hassoun, N.; Kassem, I.I.; Hamze, M.; El Tom, J.; Papon, N.; Osman, M. Antifungal Use and Resistance in a Lower–Middle-Income Country: The Case of Lebanon. Antibiotics 2023, 12, 1413. [Google Scholar] [CrossRef] [PubMed]
- Pan American Association of Infectology. Guide for the implementation of an Antimicrobial Stewardship Program at a Hospital Level. Asociación Panamericana de Infectología: https://www.apiinfectologia.org/guia-para-la-implementacion-del-proa-a-nivel-hospitalario/. 2020.
- How to measure and monitor antimicrobial consumption and resistance. Enfermedades Infecc. Microbiol. Clínica 2013, 31, 16–24. [CrossRef] [PubMed]
- Fondevilla, E.; Grau, S.; Echeverría-Esnal, D.; Gudiol, F.; Group, on behalf of the Vinc.P. Antibiotic consumption trends among acute care hospitals in Catalonia (2008–2016): impact of different adjustments on the results. Expert Rev. Anti Infect. Ther. 2021. [Google Scholar] [CrossRef] [PubMed]
- Norwegian Institute of Public Health- World Health Organization. ATCDDD - ATC/DDD Index. https://atcddd.fhi.no/atc_ddd_index/. 19 May 2024.
- Gutiérrez-Urbón, J.M.; Gil-Navarro, M.V.; Moreno-Ramos, F.; Núñez-Núñez, M.; Paño-Pardo, J.R.; Periáñez-Párraga, L. Indicators of the hospital use of antimicrobial agents based on consumption. Farm. Hosp.
- National Institute of Statistic and Census-INEC. Total population of Costa Rica. https://inec.cr/noticias/poblacion-total-costa-rica-5-044-197-personas (accessed on 19 May 2024 ).
- The National Health System in Costa Rica. Caja Costarricense de Seguro Social: https://www.binasss.sa.cr/opacms/media/digitales/El%20Sistema%20nacional%20de%20salud%20en%20Costa%20Rica.%20Generalidades.pdf. (accessed on 20 May 2024).
- Pan American Health Organization. WHO Model List of Essential Medicines 2021. https://www.paho.org/es/documentos/22a-lista-modelo-oms-medicamentos-esenciales-ingles. (accessed on 20 May 2024).
- Official List of Medicines- CCSS. https://www.ccss.sa.cr/flip/lom/#pag/1. (accessed on 20 May 2024).
- National action plan to fight antimicrobial resistance 2018-2025. Ministry of Health-Costa Rica 2018. https://www.ministeriodesalud.go.cr/index.php/biblioteca-de-archivos-left/documentos-ministerio-de-salud/vigilancia-de-la-salud/normas-protocolos-guias-y-lineamientos/resistencia-a-los-antimicrobianos/1861-plan-de-accion-nacional-de-lucha-contra-la-resistencia-a-los-antimicrobianos-costa-rica-2018-2025/file. (accessed 20 May 2024).
- Marin, G.H.; Giangreco, L.; Dorati, C.; Mordujovich, P.; Boni, S.; Mantilla-Ponte, H.; Alfonso Arvez, Ma.J.; López Peña, M.; Aldunate González, Ma.F.; Ching Fung, S.M.; et al. Antimicrobial Consumption in Latin American Countries: First Steps of a Long Road Ahead. J. Prim. Care Community Health 2022, 13, 21501319221082346. [Google Scholar] [CrossRef] [PubMed]
- Collado Borrell, R.; Losa García, J.E.; Alba Álvaro, E.; Toro Chico, P.; Moreno, L.; Pérez Encinas, M. Evaluación del consumo de antimicrobianos mediante DDD/100 estancias versus DDD/100 altas en la implantación de un Programa de Optimización del Uso de Antimicrobianos. Rev. Esp. Quimioter. 2015, 28, 317–321. [Google Scholar]
- Kuster, S.P.; Ruef, C.; Ledergerber, B.; Hintermann, A.; Deplazes, C.; Neuber, L.; Weber, R. Quantitative Antibiotic Use in Hospitals: Comparison of Measurements, Literature Review, and Recommendations for a Standard of Reporting. Infection 2008, 36, 549–559. [Google Scholar] [CrossRef] [PubMed]
- Morris, A.M. Antimicrobial Stewardship Programs: Appropriate Measures and Metrics to Study their Impact. Curr. Treat. Options Infect. Dis. 2014, 6, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Filius, P.M.G.; Liem, T.B.Y.; van der Linden, P.D.; Janknegt, R.; Natsch, S.; Vulto, A.G.; Verbrugh, H.A. An additional measure for quantifying antibiotic use in hospitals. J. Antimicrob. Chemother. 2005, 55, 805–808. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global antimicrobial resistance and use surveillance system (GLASS) report: 2022. https://www.who.int/publications-detail-redirect/9789240062702. (accessed on 19 May 2024).
- Ajulo, S.; Awosile, B. Global antimicrobial resistance and use surveillance system (GLASS 2022): Investigating the relationship between antimicrobial resistance and antimicrobial consumption data across the participating countries. PLOS ONE 2024, 19, e0297921. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Antimicrobial consumption in the EU/EEA (ESAC-Net) - Annual Epidemiological Report for 2022. https://www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-consumption-europe-2022. (accessed on 2014 June 15).
- Miranda-Novales, M.G.; Flores-Moreno, K.; López-Vidal, Y.; Rodríguez-Álvarez, M.; Solórzano-Santos, F.; Soto-Hernández, J.L.; Ponce de León-Rosales, S.; Miranda-Novales, M.G.; Flores-Moreno, K.; López-Vidal, Y.; et al. Antimicrobial resistance and antibiotic consumption in Mexican hospitals. Salud Pública México 2020, 62, 42–49. [Google Scholar] [CrossRef]
- Wenxuan Cao, Hu Feng, Yongheng Ma, et al. Long-term trend of antibiotic use at public health care institutions in northwest China, 2012–20 —— a case study of Gansu Province. BMC Public Health (2023) 23:27.
- Government of Canada. Canadian Antimicrobial Resistance Surveillance System (CARSS) Report 2022. https://www.canada.ca/en/public-health/services/publications/drugs-health-products/canadian-antimicrobial-resistance-surveillance-system-report-2022.html. (accessed on 15 June 2024).
- Lopez, M.; Martinez, A.; Celis Bustos, Y.; Thekkur, P.; Nair, D.; Verdonck, K.; Perez, F. Antibiotic consumption in secondary and tertiary hospitals in Colombia: national surveillance from 2018–2020. Rev. Panam. Salud Pública 2023, 47, 1. [Google Scholar] [CrossRef] [PubMed]
- Sokolović, D.; Drakul, D.; Vujić-Aleksić, V.; Joksimović, B.; Marić, S.; Nežić, L. Antibiotic consumption and antimicrobial resistance in the SARS-CoV-2 pandemic: A single-center experience. Front. Pharmacol. 2023, 14. [Google Scholar] [CrossRef] [PubMed]
- Grau, S.; Fondevilla, E.; Echeverría-Esnal, D.; Alcorta, A.; Limon, E.; Gudiol, F. Widespread increase of empirical carbapenem use in acute care hospitals in Catalonia, Spain. Enfermedades Infecc. Microbiol. Clínica 2019, 37, 36–40. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, B.E.; Mercado, E.H.; Pinedo-Bardales, M.; Hinostroza, N.; Campos, F.; Chaparro, E.; Del Águila, O.; Castillo, M.E.; Saenz, A.; Reyes, I.; et al. Increase of Macrolide-Resistance in Streptococcus pneumoniae Strains After the Introduction of the 13-Valent Pneumococcal Conjugate Vaccine in Lima, Peru. Front. Cell. Infect. Microbiol. 2022, 12, 866186. [Google Scholar] [CrossRef] [PubMed]
- Nelson, R. Emergence of resistant Candida auris. Lancet Microbe 2023, 4, e396. [Google Scholar] [CrossRef] [PubMed]
- Fabre, V.; Cosgrove, S.E.; Secaira, C.; Torrez, J.C.T.; Lessa, F.C.; Patel, T.S.; Quiros, R. Antimicrobial stewardship in Latin America: Past, present, and future. Antimicrob. Steward. Healthc. Epidemiol. 2022, 2, e68. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Total use of antimicrobials expressed in DDD/100 bed days (a) and DDD/100 discharges (b) in tertiary care hospitals in Costa Rica 2017-2021.
Figure 1.
Total use of antimicrobials expressed in DDD/100 bed days (a) and DDD/100 discharges (b) in tertiary care hospitals in Costa Rica 2017-2021.
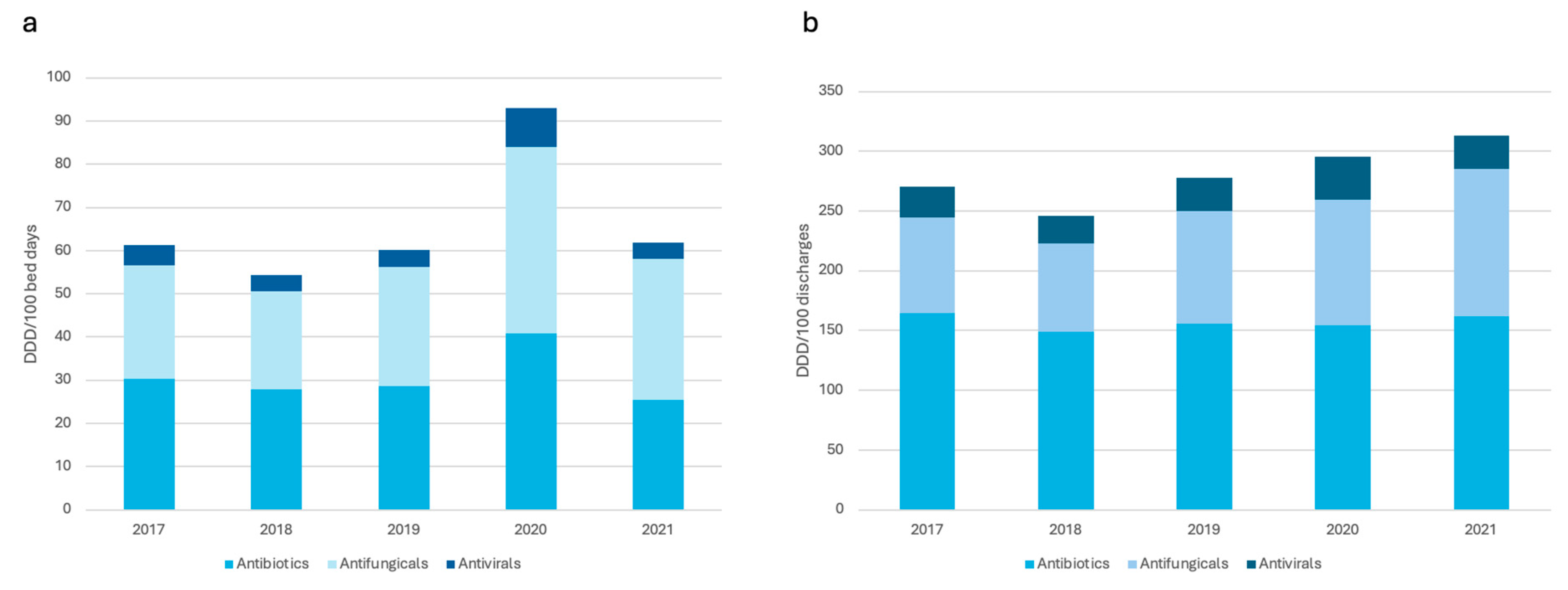

Table 1.
Mean of defined daily doses (DDD), bed days, discharges and length of stay in 2017 and 2021 among tertiary care hospitals in Costa Rica.
Table 1.
Mean of defined daily doses (DDD), bed days, discharges and length of stay in 2017 and 2021 among tertiary care hospitals in Costa Rica.
| Mean | Year | % | P value | |
|---|---|---|---|---|
| 2017 | 2021 | |||
| DDD | 622.94 | 890.74 | 0.43 | 0.0004 |
| Bed days | 14478.46 | 12555.54 | -0.13 | 0.0010 |
| Discharges | 2011.75 | 1702.83 | -0.15 | 0.0004 |
| Length of stay | 7.33 | 7.48 | 0.02 | 0.06 |
DDD: defined daily doses (unadjusted), % difference between 2017 and 2021, p values less than 0.05 were considered statistically significant.
Table 2.
Antimicrobial consumption (J01, J02, J05) in Tertiary Care Hospitals in Costa Rica from 2017 to 2021, expressed in DDD/100 bed days and DDD/100 discharges.
Table 2.
Antimicrobial consumption (J01, J02, J05) in Tertiary Care Hospitals in Costa Rica from 2017 to 2021, expressed in DDD/100 bed days and DDD/100 discharges.
| Total | 2017 | 2018 | 2019 | 2020 | 2021 | % increase | Trend | P value |
|---|---|---|---|---|---|---|---|---|
| Total antimicrobials (J01, J02, J05) | ||||||||
| DDD/100 bed days | 61.35 | 54.30 | 60.13 | 93.05 | 61.78 | 0.70 | 3.96 | 0.31 |
| DDD/100 discharges | 270.63 | 245.68 | 277.80 | 295.44 | 313.25 | 15.75 | 13.50 | 0.0007 |
| Total antibiotics (J01) | ||||||||
| DDD/100 bed days | 30.36 | 27.92 | 28.67 | 40.86 | 25.51 | -15.97 | 0.32 | 0.84 |
| DDD/100 discharges | 164.29 | 149.18 | 155.53 | 154.64 | 161.92 | -1.44 | 0.072 | 0.96 |
| Total antifungicals (J02) | ||||||||
| DDD/100 bed days | 26.30 | 22.68 | 27.60 | 43.21 | 32.49 | 23.53 | 3.29 | 0.05 |
| DDD/100 discharges | 80.41 | 73.59 | 94.49 | 104.61 | 123.52 | 53.61 | 11.72 | <0.0001 |
| Total antivirals (J05) | ||||||||
| DDD/100 bed days | 4.69 | 3.70 | 3.87 | 8.98 | 3.77 | -19.61 | - 0.34 | 0.57 |
| DDD/100 discharges | 25.93 | 22.91 | 27.78 | 36.19 | 27.81 | 7.25 | 1.70 | 0.14 |
DDD: defined daily dose (unadjusted); %: difference between 2017 and 2017, p values less than 0.05 were considered statistically significant.
Table 3.
Antimicrobial consumption (J01, J02 and J05) trends of the main groups from 2017 to 2021, expressed in DDD/100 bed days and DDD/100 discharges.
Table 3.
Antimicrobial consumption (J01, J02 and J05) trends of the main groups from 2017 to 2021, expressed in DDD/100 bed days and DDD/100 discharges.
| Total | 2017 | 2018 | 2019 | 2020 | 2021 | % | Trend | P value |
|---|---|---|---|---|---|---|---|---|
| Tetracyclines (J01A) | ||||||||
| DDD/100 bed days | 15.14 | 13.83 | 12.72 | 16.86 | 13.78 | -8.98 | 0.031 | 0.94 |
| DDD/100 discharges | 88.75 | 93.84 | 91.26 | 91.37 | 88.57 | -0.20 | -0.28 | 0.63 |
| Penicillins (J01C) | ||||||||
| DDD/100 bed days | 264.03 | 218.55 | 233.13 | 339.47 | 221.26 | -16.20 | 3.53 | 0.80 |
| DDD/100 discharges | 1390.00 | 1165.89 | 1212.08 | 1278.22 | 1344.66 | -3,26 | 2.16 | 0.93 |
| Cephalosporis (J01D) | ||||||||
| DDD/100 bed days | 430.66 | 405.92 | 369.09 | 485.73 | 296.08 | -31.24 | -18.93 | 0.29 |
| DDD/100 discharges | 2495.15 | 2313.39 | 2239.63 | 1999.53 | 1946.72 | -21.97 | -141.07 | <0.0001 |
| Carbapenems, monobactams (J01DH, J01DF) | ||||||||
| DDD/100 bed days | 146.13 | 147.72 | 172.54 | 260.09 | 156.77 | 7.28 | 13.36 | 0.27 |
| DDD/100 discharges | 699.00 | 644.69 | 791.78 | 793.57 | 948.00 | 35.62 | 64.68 | <0.0001 |
| Marcolides, lincosamides (J01F) | ||||||||
| DDD/100 bed days | 50.42 | 61.99 | 44.17 | 46.65 | 25.39 | -49.64 | -6.54 | 0.005 |
| DDD/100 discharges | 360.60 | 347.88 | 305.84 | 240.73 | 174.26 | -51.67 | -47.98 | <0.0001 |
| Sulfonamides and trimethoprim (J01E) | ||||||||
| DDD/100 bed days | 74.42 | 77.82 | 100.60 | 176.83 | 107.19 | -44.03 | 16.45 | 0.06 |
| DDD/100 discharges | 475.60 | 515.66 | 616.71 | 780.73 | 772.85 | 62.50 | 85.95 | <0.0001 |
| Aminoglycosides (J01G) | ||||||||
| DDD/100 bed days | 69.62 | 56.59 | 63.76 | 88.93 | 71.01 | 1.99 | 3.51 | 0.24 |
| DDD/100 discharges | 339.28 | 258.60 | 307.13 | 277.29 | 419.03 | 23.50 | 17.81 | 0.26 |
| Quinolones (J01M) | ||||||||
| DDD/100 bed days | 68.01 | 56.02 | 59.38 | 113.04 | 84.09 | 23.64 | 8.91 | 0.08 |
| DDD/100 discharges | 389.65 | 332.23 | 329.36 | 424.43 | 527.55 | 35.39 | 36.80 | 0.02 |
| Other antibacterias (J01XA01): Vancomycin | ||||||||
| DDD/100 bed days | 176.02 | 166.40 | 181.72 | 241.48 | 139.66 | -20.65 | 0.23 | 0.98 |
| DDD/100 discharges | 814.88 | 773.91 | 820.56 | 809.67 | 878.52 | 7.80 | 16.30 | 0.03 |
| Other antibacterias (J01XX08): Linezolid | ||||||||
| DDD/100 bed days | 46.41 | 28.18 | 47.76 | 76.56 | 34.61 | -25.42 | 2.47 | 0.62 |
| DDD/100 discharges | 175.82 | 121.69 | 185.60 | 190.10 | 202.50 | 15.17 | 12.17 | 0.08 |
| Azole Antifungicals (J02AB, J02AC) | ||||||||
| DDD/100 bed days | 116.52 | 105.78 | 124.21 | 179.35 | 163.64 | 40.43 | 16.78 | 0.0008 |
| DDD/100 discharges | 647.18 | 599.22 | 778.78 | 822.70 | 1045.72 | 61.58 | 102.05 | <0.0001 |
| Echinocandins Antifungicals (J02AX) | ||||||||
| DDD/100 bed days | 41.26 | 30.28 | 41.36 | 79.92 | 31.33 | -24.06 | 2.97 | 0.59 |
| DDD/100 discharges | 156.94 | 136.72 | 166.16 | 223.39 | 189.48 | 20.73 | 15.17 | 0.01 |
| Antivirals (J05A) | ||||||||
| DDD/100 bed days | 23.45 | 18.49 | 19.34 | 44.88 | 18.86 | -19.57 | 1.72 | 0.57 |
| DDD/100 discharges | 25.93 | 22.91 | 27.78 | 38.19 | 27.81 | 7.25 | 1.70 | 0.14 |
DDD: defined daily dose (unadjusted); %: difference between 2017 and 2017, p values less than 0.05 were considered statistically significant.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



