Submitted:
30 August 2024
Posted:
03 September 2024
You are already at the latest version
Abstract
Background. Of as yet, flow in the internal jugular veins has not been quantitatively studied in lateral decubitus position. Optimal venous outflow during sleep has been hypothesized to be potentially protective against neurodegeneration. Methods. Using ultrasonography, we measured the cross-sectional areas and flow volumes in middle parts of the internal jugular veins in group of 25 healthy individuals. These measurements were performed in the supine, upright and lateral decubitus positions. Results. In lateral decubitus positions we revealed collapse of the internal jugular vein located higher, and dilatation of the opposite vein; yet there was also a high heterogeneity of the cross-sectional area changes and in many participants this pattern was not observed. Regarding flow volumes, there was a shift of flow from one vein to the opposite one, depending on which side the person was lying, but in comparison with the supine position the total outflow through both internal jugular veins was not significantly different. Conclusions. In terms of venous outflow, the lateral decubitus position does not differ significantly from the supine one. Working hypothesis of potentially protective effect of this body position during sleep against neurodegeneration, through improved venous outflow, has not been proven, at least in healthy persons.
Keywords:
internal jugular vein
; blood flow
; body position
1. Introduction
Currently, there is a growing body of evidence that in many patients neurodegenerative disease is associated with an impaired functioning of the glymphatic system. A less efficient cleansing of the cerebral parenchyma from pathological or misfolded proteins, such as α-synuclein, β-synuclein, β-amyloid or bacterial curli is thought to be one of the important triggers of neurodegenerative process [1,2,3,4,5]. Since the glymphatic system is primarily active during sleep, optimal conditions for this system seem important [6,7,8,9,10,11]. Of note, some studies suggested that body position during sleep may have an impact on the development of neurodegeneration [12,13,14]. Interestingly, humans prefer either to sleep in the supine or lateral positions [15,16], and the lateral position seems to exhibit a protective effect. Possible mechanisms responsible for such a property of the lateral body position, for the time being, remains elusive. Nonetheless, our team has already proposed that perhaps an impaired cerebral venous drainage can provide reasonable explanation [17].
It has already been demonstrated that an activation of the astroglial-mediated interstitial fluid bulk flow is initiated by a temporary decrease of the cortical blood flow (mediated by the noradrenergic neurons of the locus ceruleus in the brain stem). This activation in turn facilitates the inflow of the cerebrospinal fluid into the cranial cavity from the vertebral canal, and then, to the perivascular space, which initiates the function of the glymphatic system [9,18,19,20]. According to the Kellie-Monroe doctrine, which states that the total volume inside the cranial cavity is constant, an unrestrained influx of the cerebrospinal fluid to the cranial cavity would require that a similar volume of the venous blood flows out from the cranial cavity. Any obstactle compromising venous outflow, at least theoretically, may impair the glymphatic system. Indeed, an abnormal venous outflow through the internal jugular veins (IJVs), which are the main blood vessels draining the brain, has been revealed in many neurodegenerative and neuroinflammatory diseses, such as multiple sclerosis, Parkinson disease, lateral amyotrophic sclerosis and Ménière disease [21,22,23,24,25,26,27,28,29]. Yet, actually there are two alternative outflow routes from the cranial cavity: one comprising the IJVs, and the second built up by the vertebral veins, vertebral epidural plexus and other deep cervical veins. In the supine body position a majority of blood flows out through the IJVs. In the upright body position, because of gravitational effects, these veins collapse and the outflow is shifted toward the vertebral and deep cervical veins, which are characterized by a higher flow resistance but do not collapse easily when the head is elevated above the heart level [30,31,32,33,34]. Interesingly, outflow through the IJVs has not been thoroughly studied in the lateral decubitus position.
In our previous pilot study [17], we found that in the lateral decubitus position the IJV, which in this body posture was above the level of the right atrium, was partially collapsed, while the opposite one remained open and was slightly wider in comparison with the cross-sectional area of this vein in the supine body position. When the patient changed body position to the opposite lateral one, for example from the left to the right side, the IJVs behaved following this pattern: the vein located above the heart level collapsed, and that located below dilatated. Still, in this preliminary study the IJV were not examined quantitatively and only a few individuals were assessed. Current study was aimed at quantitative evaluation of the flow and diameters in the IJVs in different body positions, particularly in in the lateral decubitus ones, in order to better understand flow phenomena in these veins occuring when people are lying down on their side.
2. Materials and Methods
This study was an observational research performed in the healthy subjects. For this purpose, we recruited 25 healthy individuals, 21 women and 4 men. They were aged 20-52 years, mean 33.5 years.
Inclusion criteria of this study comprised:
- participant’s age >18 years,
- no co-morbidities.
Exclusion criteria of the study comprised:
- diagnosis of neurodegenerative disease, such as Parkinson disease, Alzheimer disease, or lateral amyotrophic sclerosis,
- history of cerebral stroke,
- history of surgical or endovascular treatment of carotid or vertebral arteries,
- history of cerebral disease of an inflammatory, infectious or vascular etiology,
- clinically relevant circulatory or respiratory insufficiency.
In all of them ultrasonographic examination of the IJVs in their middle portion (at the level of the thyroid cartilage) were performed. These examinations were done on both sides. In these veins we measured their cross-sectional areas and the mean velocity flow, which was evaluated during one respiratory cycle. All these measurements were done at the same level (which was marked on the skin) in four body positions:
- supine,
- sitting,
- right lateral decubitus, i.e. lying on the right side,
- left lateral decubitus, i.e. lying on the left side.
We also checked the internal jugular veins if there were any anatomical abnormalities, such as stenoses, aneurysmatic dilatations, external compressions, pathologic jugular valves or other intraluminal pathologies. Considering difficulties associated with reliable measurement of the flow in the vertebral and deep cervical veins, we did not evaluate the cross-sectional areas and flow velocities in these veins constituting an alternative outflow route. Instead, we exclusively focused at the total flow in the IJVs. All these examinations were performed with the GE Versana Active ultrasound system (GE HealthCare, Chicago, IL, USA), using the 10 MHz linear probe.
Informed consent was obtained from all individuals participating in this survey. The study was conducted in accordance with the Declaration of Helsinki, and approved by the Bioethical Committee of the University of Opole; approval No UO/0012/KB/2022.
Statistical Analysis
In order to statistically assess the differences between cross-sectional areas and flow volumes in the examined veins, the paired t-test and the one-way ANOVA test were used. The significance of P values all statistical tests used was set at P < 0.05. Statistical analysis was performed using the PAST data analysis package (version 3.0; University of Oslo, Norway).
3. Results
We did not find structural abnormalities, such as aberrant valves or other pathological intraluminal structures in all the IJVs assessed. There were no thrombotic occlusions in the studied veins.
In general, the IJV followed the already revealed pattern: a partial or complete collapse in the sitting body position, and dilatation in the supine and the lateral decubitus positions. In the supine body position the mean cross-sectional area of the right IJV was 96.2 ± 54.4 mm2, and of the left IJV it was 64.8 ± 39.6 mm2. In the sitting body position the mean cross-sectional area of the right IJV was 10.8 ± 6.1 mm2, and of the left IJV it was 10.3 ± 9.3 mm2. In the right lateral decubitus body position the mean cross-sectional area of the right IJV was 88.6 ± 71.1 mm2, and of the left IJV it was 37.2 ± 33.4 mm2. In the left lateral decubitus body position the mean cross-sectional area of the right IJV was 38.4 ± 30.7 mm2, and of the left IJV it was 75.9 ± 51.9 mm2. Graphical representation in given in Figure 1. It can be seen that, on average, the right IJVs were larger in comparison with the left ones, both IJV almost totally collapsed in the sitting body position, and in the lateral body position one IJV constituted about 2/3 of the total outflow area – the right IJV in the right lateral decubitus position, and the left IJV in the left lateral decubitus position. These differences between the cross-sectional areas in particular body positions were statistically significant (P < 0.01). Also the cross-sectional areas of each IJV significantly differed (P < 0.01) between right and left lateral decubitus positions, as has been demonstrated using the paired t-test.
We also found that the flow in the right and left IJV followed the same pattern: it was higher in the supine body position and in the lateral decubitus position ipsilaterally to the vein studied. In the supine body position the flow through the right IJV was 101.1 ± 95.7 mL/min, and through the left IJV it was 55.1 ± 61.6 mL/min. In the sitting body position the flow through the right IJV was 13.3 ± 16.7 mL/min, and of the left IJV it was 11.9 ± 13.9 mL/min. In the right decubitus body position the flow through the right IJV was 74.3 ± 97.5 mL/min 2, and of the left IJV it was 48.8 ± 82.8 mL/min. In the left decubitus body position the flow through the right IJV was 56.7 ± 56.1 mL/min, and of the left IJV it was 99.7 ± 123.9 mL/min. Graphical representation in given in Figure 2.
It can be seen than, on average, the flow through the right IJV was higher in comparison with the left IJV in the supine and right decubitus body position, while in the left decubitus position the left IJV became dominant. There were statistically significant differences (P < 0.05) regarding flow through the IJV in the sitting position in comparison with other body positions, yet the differences in flow through the right or left IJV in the right and left lateral decubitus positions were not statistically significant (the paired t-test; P > 0.05)
However, in many veins the above-described pattern was not seen. There were many IJVs that dilatated in the specific body position, but the flow in this position decreased, or vice versa, the vein reduced its cross-sectional area, but the flow increased. Graphical representation in given in Figure 3.
Then we calculated the total flow through both IJVs. In the supine body position it was 156.1 ± 107.1 mL/min, in the sitting body position it was 25.5 ± 18.7 mL/min, in the right decubitus body position it was 126.1 ± 119.3 mL/min 2, and in the left decubitus body position the flow was 156.4 ± 133.4 mL/min (Figure 4). Statistical analysis showed that although there were statistically significant differenced revealed by the one-way ANOVA test, actually these differences regarded the flow in the sitting position, which was significantly lower in comparison with other body positions. Analysis with the use of the paired t-test did not demonstrate significant differences between total flow volumes through both IJVs in the supine and the lateral decubitus positions (P > 0.05).
Since there was a high heterogeneity regarding the cross-sectional areas and flow volumes in the examined veins, we also analysed if an asymmetry of IJVs had any association with the parameters studied. It is well known that the IJVs exhibit high anatomical variability. In most of people these veins are asymmetric. The right IJV is usually wider, although in some people the left IJV is dominant. Also, the inflow to these veins is typically asymmetric. A symmetric confluence of the sinuses (the connection of the superior sagittal sinus, the straight sinus, and the occipital sinus, which divides into two transverse sinuses) is rarely seen. In a majority of people this anatomical structure is asymmetric. Hence the inflow into the IJVs is not equal and usually the cerebral outflow is primarily directed to the right IJV.
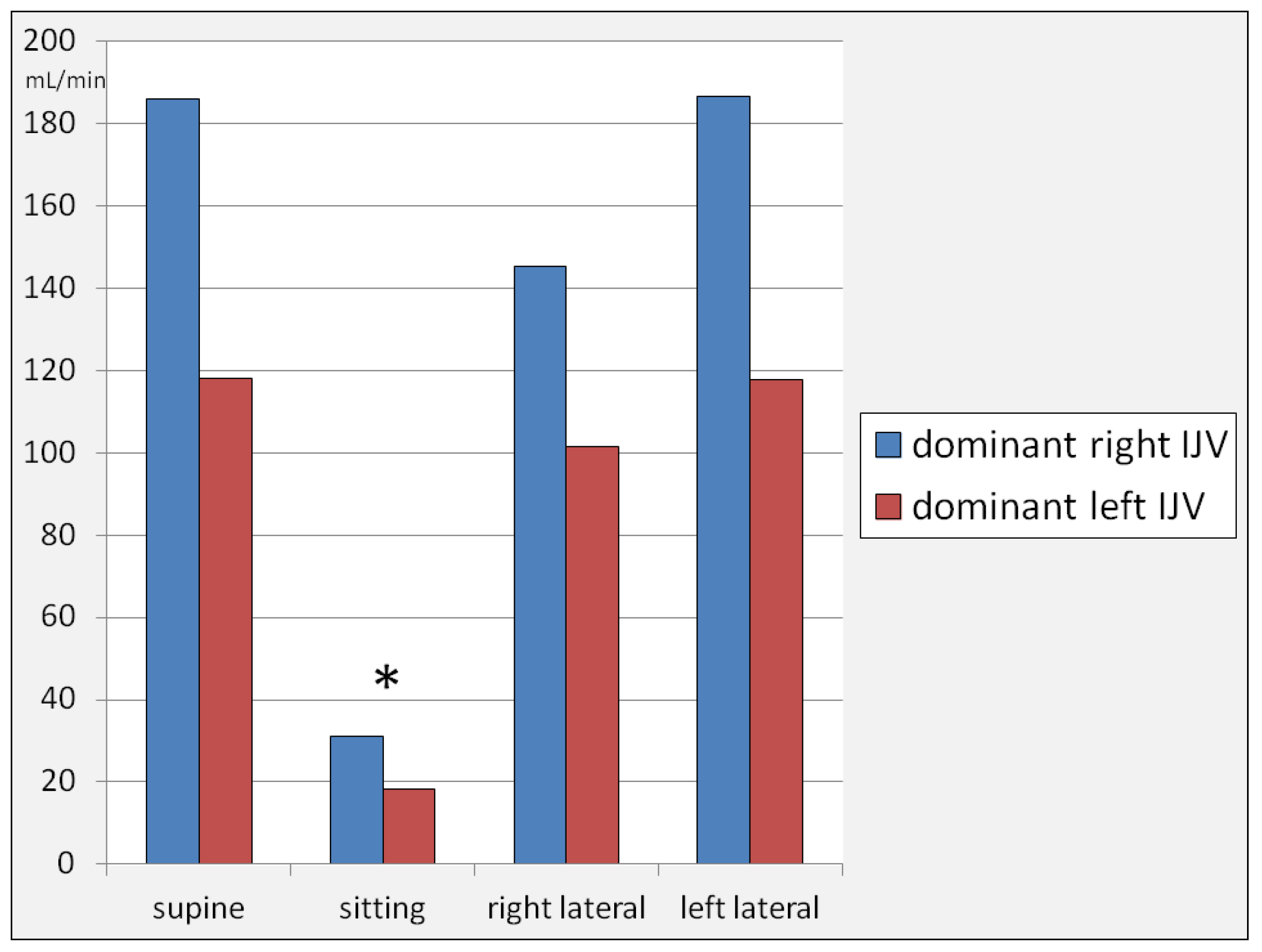
We categorized our participants into two groups: with dominant right IJV, and those with dominant left IJV. For the purpose of this analysis, the dominance of a particular IJV was defined as the vein, in which the flow in the supine body position was higher than in the opposite one. In the studied group there were 14 participants with dominant right IJV and 11 participants with dominant left IJV. Flow volumes in the dominant-right-IJV vs. dominant-left-IJV individuals are shown in Figure 5. In general, flow volumes were higher in the group with dominant right IJV, although these differences were not statistically significant. There was a statistically significant flow reduction through the IJVs in the sitting position, while the differences regarding flow volumes between other body positions were statistically insignificant.
Finally, we calculated the mean flow volume in the right vs. left IJV in all four body positions. The flow was slightly higher on the right side: 61.4 mL/min than on the left side: 53.9 mL/min ; still this difference, evaluated by means of the paired t-test, was not statistically significant (P > 0.05). We also checked in which body position the outflow was the highest. The highest flow volume in the supine body position was revealed in 11 participants, in the 10 individuals it was the highest in the left lateral body position, and in 4 people in the right lateral one.
4. Discussion
The results of our study can be summarized as follows. Firstly, there was a significant reduction of both cross-sectional areas of the IJV and flow volumes through these veins in the sitting body position in comparison with the supine one. It is not a new finding. It is a well known phenomenon, which has already been described two decades ago. In the supine body position, blood flows out from the cranial cavity primarily through the IJVs, which are the continuations of the cerebral venous sinuses. In this body position, at least 70% of blood flows out through the IJVs. However, when the head is elevated, as much as approximately 80% of blood flows out via the paravertebral route [33,34,35,36,37]. It is possible because the jugular and vertebral outflow pathways are anatomically connected in the area of the foramen magnum [33,38]. In our group of the participants we also revealed the above-described phenomenon. Of note, a reduction of flow through the IJVs in the sitting position does not mean that the total cerebral blood flow in this body position is significantly lower. This change rather reflects the shift of venous outflow to the alternative pathways, resulting from collapse of the IJVs, which is due to the negative transmural pressure in these veins [31,32]. Since it is difficult to measure quantitatively the flow in the vertebral veins, spinal epidural plexus and small deep cervical veins with the use of ultrasonography, for the purpose of our investigation it was assumed that the total flow remained unchanged, and that the “missing” flow volume in the IJV has been shifted to the other veins. Previous research has validated this assumption not only clinically, but also in computer simulations [29,40].
Secondly, we found significant changes in the cross-sectional areas of the IJVs in the lateral decubitus body positions. These changes: a collapse of the vein located above the heart level and dilatation of the opposite IJV, were partially in line with the observations coming from our previous small study [17]. Of note, such a behavior of the IJVs, although quite predictable, has not been quantitatively studied before. Still, in a larger cohort not only we revealed a high heterogeneity of the cross-sectional areas changes, which was manifested through very high standard deviations of this parameter, but also we found that in the lateral decubitus body position in many participants the IJVs did not follow the above-described pattern (see: Figure 3). It suggests that the position-dependant change of the shape and flow in the IJV is more complex and is determined by more factors than gravitation alone [30,41]. Below, we will offer possible explanations of this phenomenon.
Thirdly, we found that in the lateral decubitus body positions, the right and left ones, the total outflow through the IJV was not significantly different from such a flow in the supine position. Although there was a shift of the flow from one IJV to the opposite vein, depending on which side the person was lying, the total outflow remained largely unchanged. Of note, such a shift of outflow from the right to the left IJV, or vice versa, was not found in every individual studied, as can be seen in Figure 3.
In conclusion, in terms of venous outflow from the cranial cavity, the lateral decubitus position does not differ significantly from the supine one. Therefore, it could be concluded that this study does not confirm our working hypothesis presented in our previous paper [17]. Yet, there are several caveats to this conclusion.
In this study we examined veins in the healthy individuals. Even if the total cerebral outflow in healthy people does not depend on particular type of the horizontal body position, as our study suggests, it does not mean that in people prone to the development of neurodegeneration, the anatomy and physiology of the IJVs is the same. Therefore, a similar investigation should be performed in patients presenting with neurodegenerative disease. Of note, in 14 out of 25 healthy individuals studied, the highest flow was found in one of the lateral decubitus body positions. Still, this finding was not statistically significant in the cohort examined.
A highly unpredictable behavior of the IJVs in the lateral position, which was seen in some individuals assessed in this study, should be thoroughly explained. These changes in the flow volume and vein diameters are difficult to explain if anatomically the IJVs and the vertebral veins constituted a simple interconnected system, where only gravitation plays a role. Most likely, the reduction of the flow, combined with an increased cross-sectional area, or the reversed phenomenon, resulted from an interplay between anatomical asymmetry of the cerebral sinuses [33], compression of the IJV by bony structures in its upper part [42], especially while lying on one side with the head slightly distorted, and possibly with flow resistance evoked by abnormal flow pattern in the IJV on the otherwise normal jugular valves [43]. Also, slight head rotation during measurements could play a role [44,45,46].
A similar study performed in patients presenting with neurodegeneration appears to be a reasonable next step of this research. Such a survey would enable to validate our initial concept in the settings of neurological disease. Importantly, good explanation of the neurological benefits of sleeping on the side [12,13], of as yet, has not been offered. In our previous paper we hypothesized that in the lateral body position, because of decreased flow resistance in the extracranial veins, cerebral venous outflow is optimal, which in turn optimizes activity of the glymphatic system. In such a way, the brain would be protected against neurodegeneration. In the present study on healthy individuals, this hypothesis has not been confirmed. Still, a different result in patients with presenting with neurodegenerative disease cannot be ruled out. Therefore, such a study is needed.
Of note, a better functioning of the glymphatic system in the lateral body position has been demonstrated in animal studies [45]. It is known that the activity of glymphatic system is primarily regulated by the noradrenergic system of the brain. Activation of the glymphatic system is dependent on a temporary decrease of the cortical blood flow during the non-REM phase of sleep, which is followed by a macroscopic wave of inflow of the cerebrospinal fluid. This change in the cortical blood flow is regulated by the noradrenergic neurons [19]. But why noradrenergic stimulation should be increased while sleeping in the lateral decubitus position, remains elusive. Perhaps the noradrenergic neurons are stimulated by the vestibular nuclei that receive inputs from the semicircular canals, utricle, and saccule of the labyrinth. But of as yet, such anatomical connections have not been revealed. Therefore, a hemodynamic hypothesis, that the inflow of the cerebrospinal fluid should be accompanied by an unrestricted outflow of the venous blood, seems encouraging.
Importantly, there should be some modifications to the design of future studies on this topic. We suspect that some of the counterintuitive changes in the sizes and flow volumes that were seen in our study resulted from compression of the IJV in its upper part by the transverse process of the atlas and/or styloid process of the temporal bone [48]. To exclude such a compression, the upper segment of the IJV, particularly the flow, should be carefully assessed in slightly changed position of the head in relation to the neck. Abnormalities revealed through this test would require further diagnostic workout, e.g. CT scans. It is known that flow abnormalities evoked by even minor stenoses of the IJV located in this area can be hemodynamically relevant [40]. In addition, such flow abnormalities can the flow in the entire course of the IJV and possible disturb function of the jugular valve located downstream [43].
In addition, in future studies on the importance of the sleeping on the side, the pattern of cerebral venous outflow should be considered. Research on the flow in the IJVs has demonstrated that although in a majority of people the IJVs are the main veins responsible for the outflow in the supine body position, the proportion of blood volume utilizing either the jugular or vertebral pathway can differ between people. Therefore, at least an approximate measurement of the flow in the vertebral veins should be performed in future studies.
Also, anatomy of the intracranial venous outflow should be taken into account. Main venous channels draining the brain comprise the superior sagittal sinus, the inferior sagittal sinus, the great cerebral vein, the straight sinus and the occipital sinus. The superior sagittal sinus is the principal blood vessel draining the superficial parts of the cerebral hemispheres, particularly the cerebral cortex. Blood from the deep structures of the brain flows out through the deep venous system, which is composed of the internal cerebral veins and the basal veins of Rosenthal, which finally drain into the great cerebral vein, which in turn empties into the straight sinus. A perfectly symmetric pattern of the cerebral sinuses, with symmetric outflow to the left and right transverse sinuses from both deep and superficial parts of the brain, in rarely encountered [33]. Typically, there is a more or less asymmetric confluence of the sinuses, and in many people there is a completely separated outflow to the right and left side. Sometimes, the superficial structures of the brain are exclusively drained by the right transverse sinus, while deep parts by the left one, or vice versa. Flow evaluation in the context of the intracranial venous anatomy would require a diagnostic imaging of these veins and sinuses. Such an imaging could be done low-invasively, preferentially using the non-contrast methods, e.g. time-of-flight MR angiography [49]. In many neurological patients such a scanning would already be available for evaluation from the previous diagnostic workout. In others it could be done in addition to the scheduled control scans, thus a participation in the study would not add significant risks or inconveniences.
We acknowledge that there are some limitations of our research. The number of assessed individuals was rather small. Also, there were several technical aspects of the measurements, as well as additional parameters that perhaps should have also been evaluated, such as anatomy of the intracranial venous channels or quantitative assessment of the flow in the extra-jugular veins. These issues have been discussed above and probably should be considered during future studies on this topic. Nonetheless, current study can be seen as a useful framework for next research on the role of the cerebral and extracranial venous circulation in the settings of neurodegeneration.
5. Conclusions
In terms of the venous outflow from cranial cavity, the lateral decubitus body position does not differ significantly from the supine one. Our working hypothesis of a potentially protective effect against neurodegeneration of this body position during sleep, through an improved venous outflow from the brain, has not been proven, at least in the healthy persons. Still, further studies on this topic, primarily in patients with neurodegeneration, are warranted.
Author Contributions
Conceptualization, A.K. and M.S. (Marian Simka); methodology, M.S. (Marian Simka); software, M.S. (Marian Simka); validation, M.S. (Marcin Skuła) and M.S. (Marian Simka); formal analysis, M.S. (Marian Simka); investigation, A.K. and J.C.; resources, M.S. (Marian Simka); data curation, A.K. and M.S. (Marian Simka); writing—original draft preparation, M.S. (Marian Simka); writing—review and editing, A.K.; supervision, M.S. (Marian Simka); project administration, M.S. (Marian Simka); funding acquisition, M.S. (Marian Simka) All authors have read and agreed to the published version of the manuscript.
Funding
This study received research grant from the University of Opole.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Bioethical Committee of the University of Opole; approval No UO/0012/KB/2022.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study
Data Availability Statement
Anonymized data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Jessen, N.A.; Finmann Munk, A.S.; Lundgaard, I.; Nedergaard, M. The glymphatic system – a beginner’s guide. Neurochem Res 2015, 40, 2583–2599. [Google Scholar] [CrossRef]
- Mendelsohn, A.R.; Larrick, J.W. Sleep facilitates clearance of metabolites from the brain: glymphatic function in aging and neurodegenerative diseases. Rejuvenation Res 2013, 16, 518–523. [Google Scholar] [CrossRef]
- Mestre, H.; Hablitz, L.M.; Xavier, A.L.; et al. , Aquaporin-4-dependent glymphatic sulute transport in the rodent brain. Elife 2018, 7, e40070. [Google Scholar] [CrossRef]
- Plog, B.A.; Nedergaard, M. The glymphatic system in the CNS health and disease: past, present and future. Annu Rev Pathol 2018, 13, 379–394. [Google Scholar] [CrossRef] [PubMed]
- Tarasoff-Conway, J.; Carare, R.O.; Osorio, R.S.; et al. Clearance systems of the brain – implications for Alzheimer disease. Nat Rev Neurol 2015, 11, 457–470. [Google Scholar] [CrossRef] [PubMed]
- Benveniste, H.; Heerdt, P.M.; Fontes, M.; et al. , Glymphatic system function in relation to anesthesia and sleep states. Anesth Analg 2019, 12, 747–58. [Google Scholar] [CrossRef]
- Liguori, C.; Chiaravalloti, A.; Izzi, F.; et al. , Sleep apneas may represent a reversible risk factor for amyloid-β pathology. Brain 2017, 140, e75. [Google Scholar] [CrossRef] [PubMed]
- Reddy, O.C.; van der Werf, Y.D. The sleeping brain: harnessing the power of the glymphatic system through lifestyle choices. Brain Sci 2020, 10, 868. [Google Scholar] [CrossRef] [PubMed]
- Simka, M. Activation of the glymphatic system during sleep – is the cerebral venous outflow a missing piece of the puzzle? Phlebol Rev 2019, 27, 1–2. [Google Scholar] [CrossRef]
- Xie, L.; Kang, H.; Xu, Q.; et al. , Sleep drives metabolite clearance from the adult brain. Science 2013, 342, 373–377. [Google Scholar] [CrossRef]
- Massey, A.; Boag, M.; Magnier, A.; Bispo, D.; Khoo, T.; Pountney, D. glymphatic system dysfunction and sleep disturbance may contribute to the pathogenesis and progression of Parkinson’s disease. Int J Mol Sci 2022, 23, 12928. [Google Scholar] [CrossRef] [PubMed]
- Levendowski, D.J.; Gamaldo, C.; St.Louis, E.K,; et al., Head position during sleep: potential implications for patients with neurodegenerative disease. J Alzheimer Dis 2019, 67,631-638.
- Gnarra, O.; Calvello, C.; Schirinzi, T.; Beozzo, F.; De Masi, C.; Spanetta, M.; Fernandes, M.; Grillo, P.; Cerroni, R.; Pierantozzi, M.; et al. Exploring the association linking head position and sleep architecture to motor impairment in parkinson’s disease: An exploratory study. J Pers Med 2023, 13, 1591. [Google Scholar] [CrossRef] [PubMed]
- Girolami, S.; Tardio, M.; Loredana, S.; Di Mattia, N.; Micheletti, P.; Di Napoli, M. Sleep body position correlates with cognitive performance in middle-old obstructive sleep apnea subjects. Sleep Med X 2022, 4, 100050. [Google Scholar] [CrossRef] [PubMed]
- De Koninck, J.; Lorrain, D.; Gagnon, P. Sleep positions and position shifts in five age groups: an ontogenetic picture. Sleep 1991, 15, 143–149. [Google Scholar] [CrossRef]
- Zhang, Y.; Xiao, A.; Zheng, T.; Xiao, H.; Huang, R. The relationship between sleeping position and sleep quality: A flexible sensor-based study. Sensors 2022, 22, 6220. [Google Scholar] [CrossRef]
- Simka, M.; Czaja, J.; Kowalczyk, D. Collapsibility of the internal jugular veins in the lateral decubitus body position: a potential role of the cerebral venous outflow against neurodegeneration. Med Hypothes 2019, 133, 109397. [Google Scholar] [CrossRef]
- Russak, A.; Plog, B.A.; Vates, E,; Nedergaard, M. Angiotensin II increases glymphatic flow through a norepinephrine-dependent mechanism. Neurology 2016, 86(suppl.16), P5.214.
- Fultz, N.E.; Bonmassar, G.; Setsompop, K.; Stickgold, R.A.; Rosen, B.R.; Polimeni, J.R.; Lewis, L.D. Coupled electrophysiological, hemodynamic, and cerebrospinal fluid oscillations in human sleep. Science 2019, 366, 628–631. [Google Scholar] [CrossRef]
- Van Egroo, M.; Koshmanova, E.; Vandewalle, G.; Jacobs, H.I.L. Importance of the locus coeruleus-norepinephrine system in sleep-wake regulation: Implications for aging and Alzheimer's disease. Sleep Med Rev 2022, 62, 101592. [Google Scholar] [CrossRef]
- Beggs, C.B.; Chung, C.P.; Bergsland, N.; et al. Jugular venous reflux and brain parenchyma volumes in elderly patients with mild cognitive impairment and Alzheimer’s disease. BMC Neurology 2013, 13, 157. [Google Scholar] [CrossRef]
- Chung, C.P.; Beggs, C.; Wang, P.N.; et al. , Jugular venous reflux and white matter abnormalities in Alzheimer's disease: a pilot study. J Alzheimer Dis 2014, 39, 601–609. [Google Scholar] [CrossRef]
- Menegatti, E.; Zamboni, P. Doppler haemodynamics of cerebral venous return. Curr Neurovasc Res 2008, 5, 260–265. [Google Scholar] [CrossRef]
- Nicolaides, A,N.; Morovic, P,; Menegatti, E. et al., Screening for chronic cerebrospinal venous insufficiency (CCSVI) using ultrasound - recommendations for a protocol. Funct Neurol 2011,26,229-248.
- Simka, M.; Latacz, P.; Ludyga, T.; Kazibudzki, M.; Swierad, M.; Janas, P.; Piegza, J. Prevalence of extracranial venous abnormalities: results from a sample of 586 multiple sclerosis patients. Func Neurol 2011, 26, 197–203. [Google Scholar]
- Zivadinov, R.; Chung, C.P. Potential involvement of the extracranial venous system in central nervous system disorders and aging. BMC Med 2013, 11, 260. [Google Scholar] [CrossRef] [PubMed]
- Filipo, R.; Ciciarello, F.; Attanasio, G.; Mancini, P.; Covelli, E.; Agati, L.; Fedele, F.; Viccaro, M. Chronic cerebrospinal venous insufficiency in patients with Ménière’s disease. Eur Arch Otorhinolaryngol 2015, 272, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Alpini, D.C.; Bavera, P.M.; Hahn, A.; Mattei, V. Chronic cerebrospinal venous insufficiency (CCSVI) in Meniere disease. Case or cause? Sci Med 2013, 4, 9–15. [Google Scholar]
- Haacke, E.M.; Feng, W.; Utriainen, D.; Trifan, G.; Wu, Z.; Latif, Z.; Katkuri, Y.; Hewett, J.; Hubbard, D. Patients with multiple sclerosis with structural venous abnormalities on mr imaging exhibit an abnormal flow distribution of the internal jugular veins. J Vasc Interv Radiol 2012, 23, 60–68. [Google Scholar] [CrossRef]
- Gisolf, J.; van Lieshout, J.J.; van Heusden, K.; et al. , Human cerebral venous outflow pathway depends on posture and central venous pressure. J Physiol 2004, 560, 317–327. [Google Scholar] [CrossRef]
- Schaller, B. Physiology of cerebral venous blood flow: from experimental data in animals to normal function in humans. Brain Res Rev 2004, 46, 243–260. [Google Scholar] [CrossRef]
- Schreiber, S.J.; Lürtzing, F.; Götze, R.; et al. , Extrajugular pathways of human cerebral venous blood drainage assessed by duplex ultrasound. J Appl Physiol 2003, 94, 1802–1805. [Google Scholar] [CrossRef]
- Simka, M.; Waligóra, M.; Kowalczyk, D.; Czaja, J. Anatomy and physiology of venous outflow from the cranial cavity. In Horizons in World Cardiovascular Research.Volume 16. Bennington, E.H., Ed.; Nova Science Publishers Inc: New York, USA, 2019; pp. 139–158. [Google Scholar]
- Zaniewski, M.; Simka, M. Biophysics of venous return from the brain from the perspective of the pathophysiology of chronic cerebrospinal venous insufficiency. Rev Recent Clin Trials 2012, 7, 88–92. [Google Scholar] [CrossRef]
- Cirovic, S.; Walsh, C.; Fraser, W.D.; Gulino, A. . The effect of posture and positive pressure breathing on the hemodynamics of the internal jugular vein. Aviat Space Environ Med 2003, 74, 125–31. [Google Scholar] [PubMed]
- Niggemann, P.; Kuchta, J.; Grosskurth, D.; Beyer, H.K.; Krings, T.; Reinges, M. Position dependent changes of the cerebral venous drainage--implications for the imaging of the cervical spine. Cent Eur Neurosurg 2011, 72, 32–7. [Google Scholar] [CrossRef]
- van Zandwijk, J.K.; Kuijer, K.M.; Stassen, C.M.; Ten Haken, B.; Simonis, F.F.J. Internal jugular vein geometry under multiple inclination angles with 3D low-field MRI in healthy volunteers. J Magn Reson Imaging 2022, 56, 1302–1308. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, S.; Sakuma, I.; Omachi, K.; et al. , Craniocervical junction venous anatomy around the suboccipital cavernous sinus: evaluation by MR imaging. Eur Radiol 2005, 15, 1694–1700. [Google Scholar] [CrossRef] [PubMed]
- Simka, M.; Skuła, M.; Bielaczyc, G. Validation of models of venous outflow from the cranial cavity in the supine and upright body positions. Phlebol Rev 2022, 30, 8–12. [Google Scholar] [CrossRef]
- Simka, M.; Czaja, J.; Kawalec, A.; Latacz, P.; Kovalko, U. Numerical modeling of venous outflow from the cranial cavity in the supine body position. Appl Sci 2024, 14, 3878. [Google Scholar] [CrossRef]
- Holmlund, P.; Johansson, E.; Qvarlander, S.; Wåhlin, A.; Ambarki, K.; Koskinen, L.D.; Malm, J.; Eklund, A. Human jugular vein collapse in the upright posture: implications for postural intracranial pressure regulation. Fluids Barriers CNS 2017, 14, 17. [Google Scholar] [CrossRef]
- Simka, M.; Latacz, P. Numerical modeling of blood flow in the internal jugular vein with the use of computational fluid mechanics software. Phlebology 2021, 36, 541–548. [Google Scholar] [CrossRef]
- Rashid, A.; Iqrar, S.A.; Rashid, A.; Simka, M. Results of numerical modeling of blood flow in the internal jugular vein exhibiting different types of strictures. Diagnostics 2022, 12, 2862. [Google Scholar] [CrossRef]
- Farina, M.; Novelli, E.; Pagani, R. Cross-sectional area variations of internal jugular veins during supine head rotation in multiple sclerosis patients with chronic cerebrospinal venous insufficiency: a prospective diagnostic controlled study with duplex ultrasound investigation. BMC Neurology 2013, 13, 162. [Google Scholar] [CrossRef] [PubMed]
- Gwak, M.J.; Park, J.Y.; Suk, E.H.; Kim, D.H. Effects of head rotation on the right internal jugular vein in infants and young children. Anaesthesia 2010, 65, 272–276. [Google Scholar] [CrossRef]
- Højlund, J.; Sandmand, M.; Sonne, M.; et al. , Effect of head rotation on cerebral blood flow velocity in the prone position. Anesthesiol Res Pract 2012, 2012, 647258. [Google Scholar] [PubMed]
- Lee, H.; Xie, L.; Yu, M.; et al. , The effect of body posture on brain glymphatic transport. J Neurosci 2015, 35, 11034–11044. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Sun, Y.; Chan, C.C.; Fan, C.; Ji, X.; Meng, R. Internal jugular vein stenosis associated with elongated styloid process: five case reports and literature review. BMC Neurol 2019, 19, 1–8. [Google Scholar] [CrossRef]
- Zivadinov, R.; Bastianello, S.; Dake, M.D.; et al. , Recommendations for multimodal noninvasive and invasive screening for detection of extracranial venous abnormalities indicative of chronic cerebrospinal venous insufficiency: a position statement of the International Society for Neurovascular Disease. J Vasc Interv Radiol 2014, 25, 1785–1794.e17. [Google Scholar] [CrossRef]
Figure 1.
Cross-sectional areas of the right and left internal jugular veins in the supine, sitting, right and left lateral decubitus body positions. Differences between cross-sectional areas in particular body positions, assessed by means of the one-way ANOVA test and the paired t-test, were statistically significant (p < 0.05). .
Figure 1.
Cross-sectional areas of the right and left internal jugular veins in the supine, sitting, right and left lateral decubitus body positions. Differences between cross-sectional areas in particular body positions, assessed by means of the one-way ANOVA test and the paired t-test, were statistically significant (p < 0.05). .
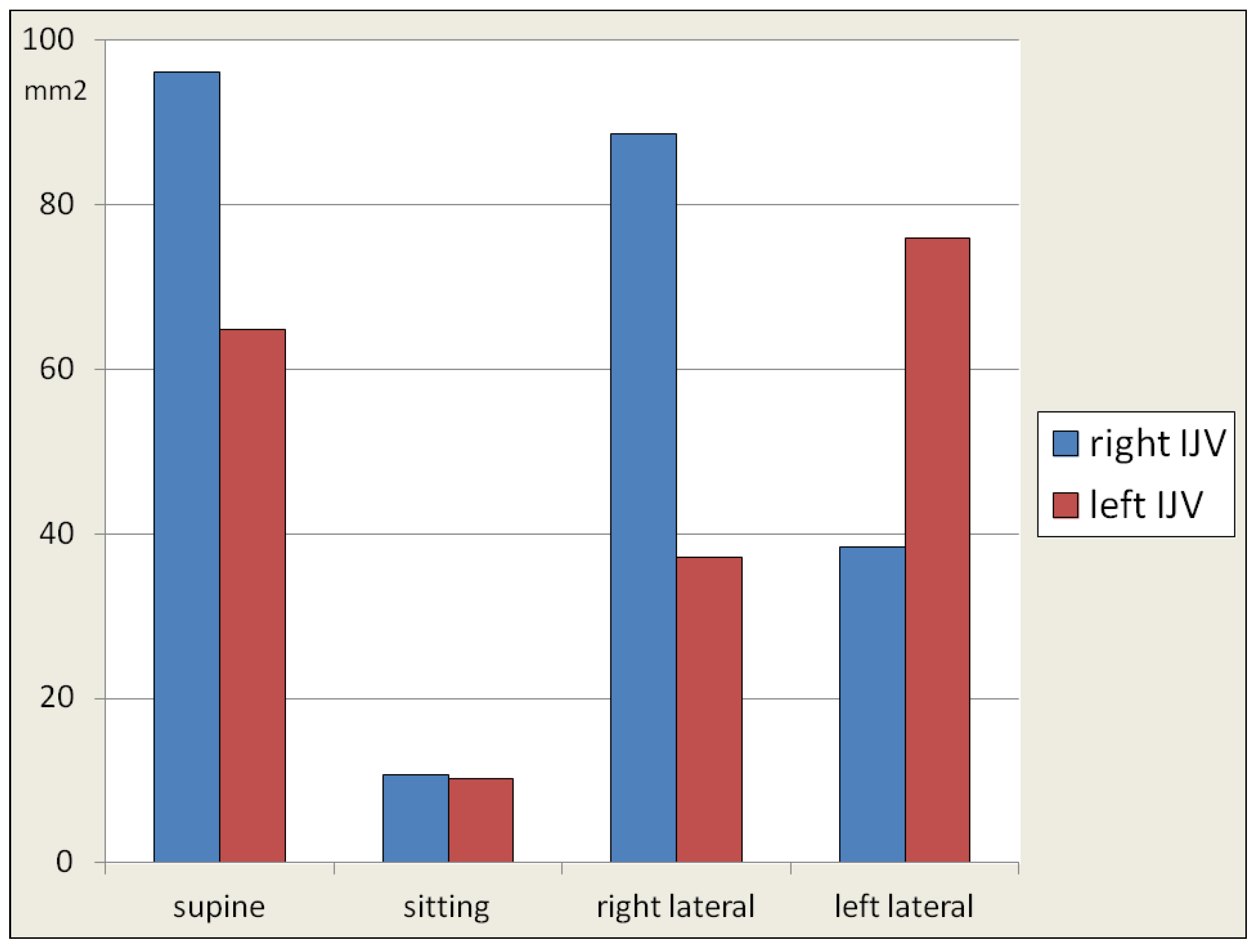
Figure 2.
Flow volumes through the right and left internal jugular veins in the supine, sitting, right and left lateral decubitus body positions. Differences between flow volumes in particular body positions, assessed by means of the one-way ANOVA test and the paired t-test, were statistically significant (p < 0.05), but only regarding the sitting body position.
Figure 2.
Flow volumes through the right and left internal jugular veins in the supine, sitting, right and left lateral decubitus body positions. Differences between flow volumes in particular body positions, assessed by means of the one-way ANOVA test and the paired t-test, were statistically significant (p < 0.05), but only regarding the sitting body position.
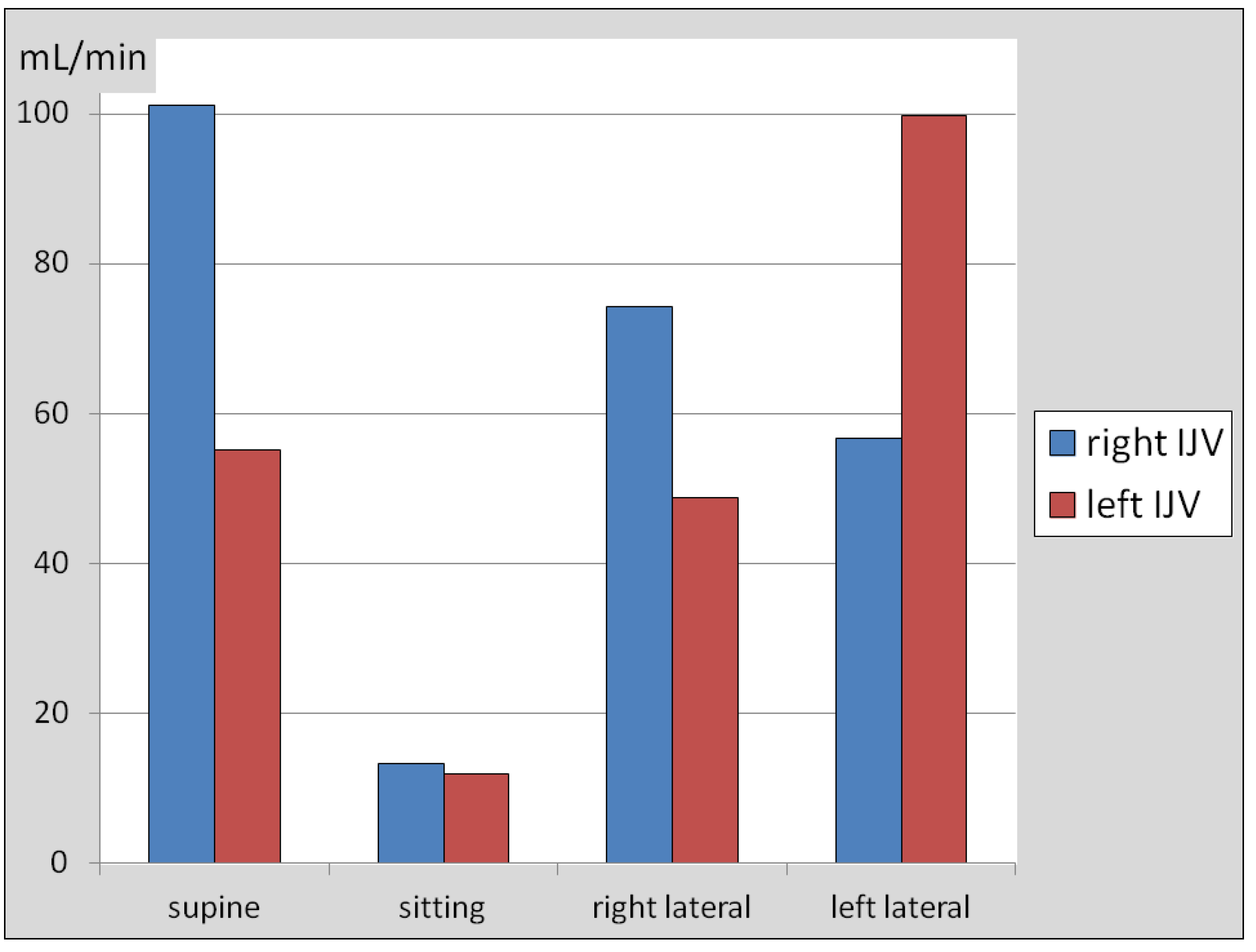
Figure 3.
Change of the cross-sectional area and flow volume in the internal jugular veins in the lateral decubitus body position in comparison with the supine one; ipsilateral lateral decubitus – regards the right IJV in the right lateral decubitus body position, or the left IJV in the left decubitus body position; contralateral lateral decubitus – regards the right IJV in the left lateral decubitus body position, or the left IJV in the right decubitus body position; Area↓: reduction of the cross-sectional area in comparison with the supine body position; Flow↓: reduction of the flow in comparison with the supine body position; Area ↑: increase of the cross-sectional area; Flow ↑: increase of the flow.
Figure 3.
Change of the cross-sectional area and flow volume in the internal jugular veins in the lateral decubitus body position in comparison with the supine one; ipsilateral lateral decubitus – regards the right IJV in the right lateral decubitus body position, or the left IJV in the left decubitus body position; contralateral lateral decubitus – regards the right IJV in the left lateral decubitus body position, or the left IJV in the right decubitus body position; Area↓: reduction of the cross-sectional area in comparison with the supine body position; Flow↓: reduction of the flow in comparison with the supine body position; Area ↑: increase of the cross-sectional area; Flow ↑: increase of the flow.
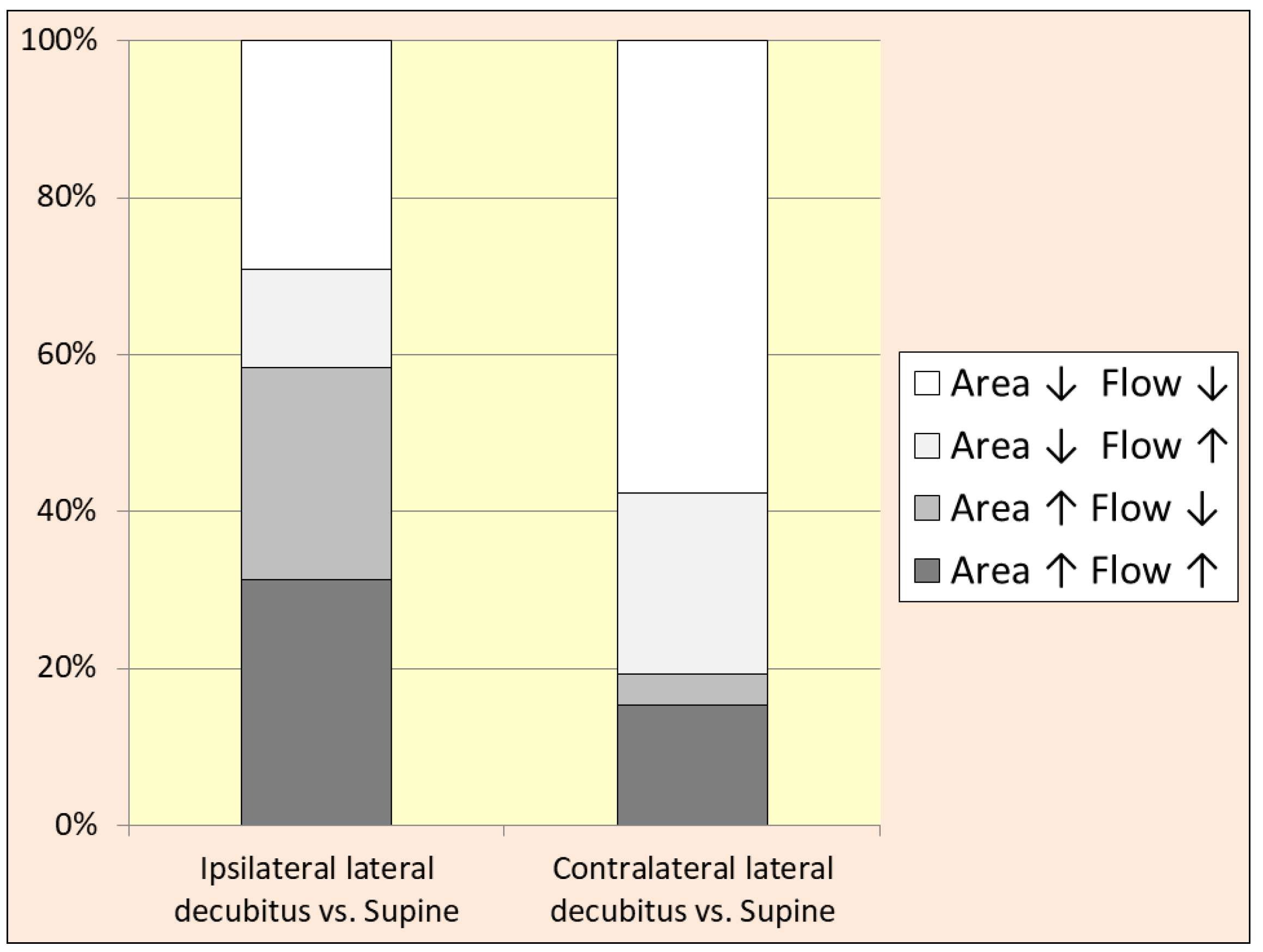
Figure 4.
Total flow volumes in both internal jugular veins in the supine, sitting, right and left lateral decubitus body positions. Flow volume in the sitting body position was significantly different from other position (asterisk), as has been demonstrated by the one-way ANOVA test and the paired t-test. Differences between flow volumes in other body positions were statistically insignificant (P > 0.05).
Figure 4.
Total flow volumes in both internal jugular veins in the supine, sitting, right and left lateral decubitus body positions. Flow volume in the sitting body position was significantly different from other position (asterisk), as has been demonstrated by the one-way ANOVA test and the paired t-test. Differences between flow volumes in other body positions were statistically insignificant (P > 0.05).
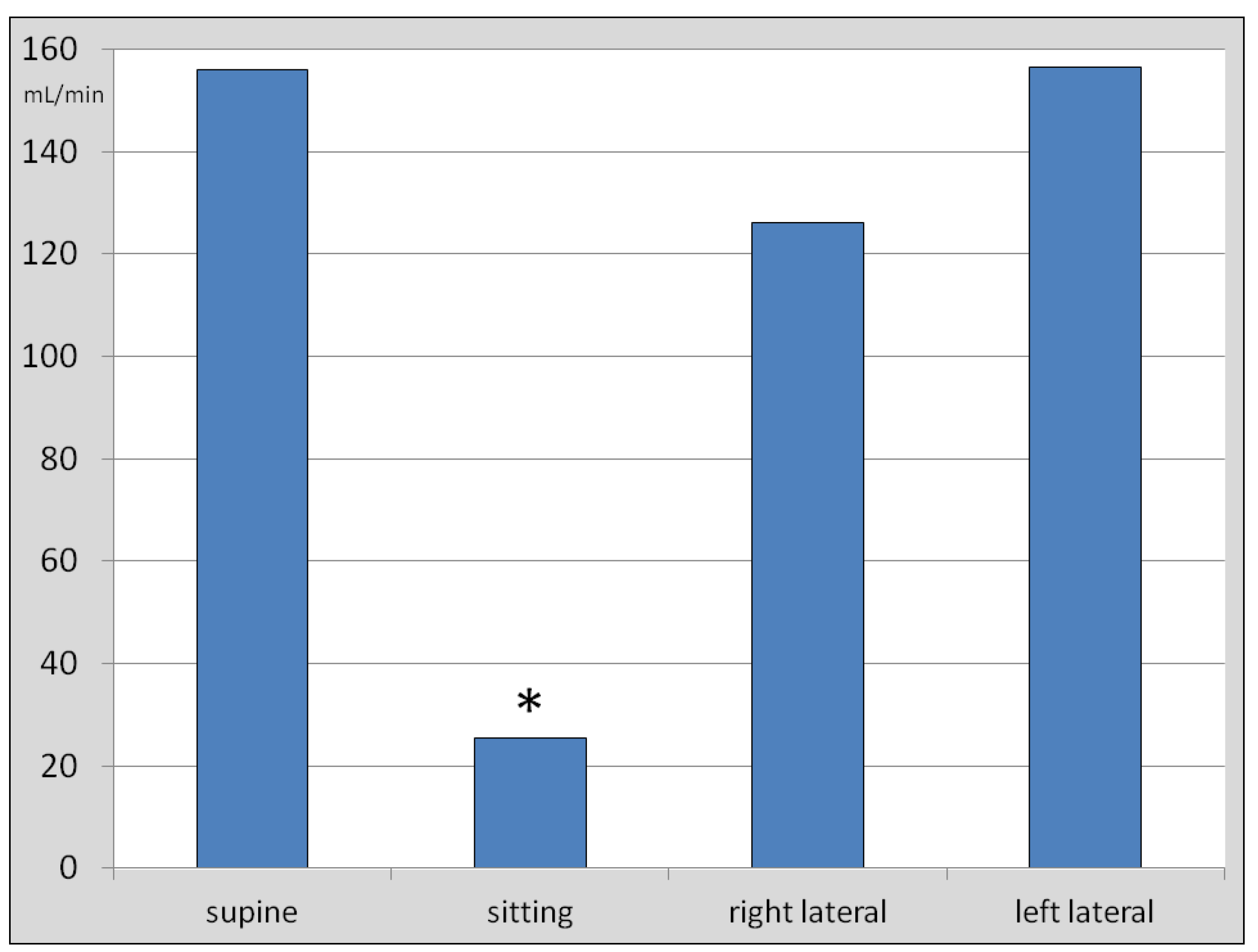
Figure 5.
Total flow volumes in both internal jugular veins in the supine, sitting, right and left lateral decubitus body positions in the individuals presenting with dominant right- or left-sided outflow. Flow volume in the sitting body position was significantly different from other position (asterisk), as has been demonstrated by the one-way ANOVA test and the paired t-test. Differences between the flow volumes in other body positions were statistically insignificant (P > 0.05). Also, there were no statistically significant differences between total flow volumes in the individuals presenting with the right vs. left IJV dominance, regarding flow volumes in the supine, right lateral and left lateral positions.
Figure 5.
Total flow volumes in both internal jugular veins in the supine, sitting, right and left lateral decubitus body positions in the individuals presenting with dominant right- or left-sided outflow. Flow volume in the sitting body position was significantly different from other position (asterisk), as has been demonstrated by the one-way ANOVA test and the paired t-test. Differences between the flow volumes in other body positions were statistically insignificant (P > 0.05). Also, there were no statistically significant differences between total flow volumes in the individuals presenting with the right vs. left IJV dominance, regarding flow volumes in the supine, right lateral and left lateral positions.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



