Submitted:
22 August 2024
Posted:
25 August 2024
Read the latest preprint version here
Abstract
Indigenous Peoples in Canada are disproportionately affected by chronic hepatitis C virus (HCV) infection. HCV prevalence in Indigenous Peoples is estimated at approximately five to 10-fold higher than it is in non-Indigenous persons, while the reported rate of newly diagnosed HCV cases in First Nations communities was six times the respective rate in the general Canadian population in 2022. This review explores the reasons underlying the disproportionate burden of hepatitis C virus (HCV) infection in Indigenous Peoples, including significant over-representation of Indigenous Peoples in the major risk categories for HCV acquisition, such as substance abuse, incarceration, homelessness or inadequate shelter, and disruption of family/social supports. The impact of these risk factors is aggravated by many access barriers to healthcare services despite the availability of universal healthcare system and free curative antiviral therapies. These stem from the legacy of colonialism, discrimination and disenfranchisement, and are exacerbated by racism in the justice and healthcare systems, stigmatization and victimization. Recent recognition of historical harms and early steps towards nation-to-nation reconciliation along with support for culturally safe, wholistic and Indigenous People-led wellness programs instill hope that elimination strategies to eradicate HCV infection in Indigenous populations will be successful in Canada.
Keywords:
hepatitis C
; Indigenous health
; First Nations
; Inuit
; Métis
; epidemiology
; colonial trauma
; prevalence
; incidence
; racism
1. Introduction
First Peoples or Indigenous populations in what is now called Canada consist of not only the three distinct groups known as First Nations, Inuit and Métis, but encompasses over 70 languages, various origin stories, more than 600 Nations, over 3400 reserved land locations, and over 1.8 million people, constituting 5% of the Canadian population (4). Indigenous People are not only the fastest growing population segment at over 9% growth, but also the youngest population in Canada where over a quarter are younger than 25 (4). This description gives the impression of a vibrant cultural group thriving within one of the largest and healthiest countries of the world, but the lived reality retains shadows of history vividly seen through review of the hepatitis C virus (HCV).
Colonial Context of Hepatitis
In the colonizing and settling phase of Canada’s history over 3,400 reserved land locations were set aside to contain First Nations on what are now called reserves, where just over 37% of registered status First Nation’s people currently live (4). Indigenous Peoples, as co-signatories of the historical and modern treaties reside close to areas of natural resource extraction and are disproportionally affected by environmental degradation and social disruption resulting from the “boom and bust” business cycle, especially after companies maximize profits and move out of the area, often abandoning their responsibilities to support lands rehabilitation and creation of sustainable regional development.
Between 1960 and 2023, Canada’s population has more than doubled, while the country’s gross domestic product (GDP) increased more than 50-times from about 40 billion to 2.1 trillion dollars (5). The economic development of such a magnitude has required mobilization of large segments of Canadian society and the country’s resources, and while this has increased an overall economic participation, it has exacerbated pre-existing socio-economic inequality and has come at a tremendous cost to the natural environment and the wellbeing of Indigenous populations.
This ongoing exploitation and colonization of land and its resources builds on the continued experience of colonial and assimilation-based legislation and policies. Starting with broken Treaties between Indigenous Peoples and the Dominion of Canada, continuing with the Indian Act of 1876 and evolving into forced attendance at residential schools and abusive control and abductions of Indigenous children through the child welfare system across the country has shaped the current lived experience for Indigenous populations. This daily experience also includes discrimination, marginalization, disruption and transgenerational trauma while creating significant barriers in accessing education, employment, housing, food, security, healthcare services, clean water and sanitation.
These economic, legislative and population dynamics have inflicted a lasting disruption to the use of traditional languages, ways of learning, land-based diet and lifestyle, generational knowledge transfer, spirituality practices, coping strategies and the relational community circle previously experienced by Indigenous Peoples and has resulted in a loss of Indigenous ways of being of a magnitude nearly impossible to quantify. While the vast and lasting harms of failed assimilation policies are becoming more broadly acknowledged in Canada, the nation-to-nation reconciliation process is still in its infancy.
Institutional Racism in Canadian Healthcare
Institutional or systemic racism can be defined as institutions-driven inequalities that are based on policies or practices that inherently discriminate – either deliberately or not - against one or more population groups (6). In practice, systemic racism may be seen as a tendency by one social group to marginalize another social group in a form of exclusion from the application of the federal law (7) underfunding basic childcare services (8), creating obstacles to access health services (9) and otherwise subjecting it to a different standard of service (10). Selective application of the law and law enforcement has been implicated in the excessive use of traffic stops of Indigenous Peoples in 2014-2017 (11) and disproportionate incarceration rates of Indigenous Peoples. To the latter point, while Indigenous Peoples made up about 5% of the total Canadian Population in 2022, they comprised approximately 32% of the total inmate population in Canada with even higher proportion of Indigenous women in-custody, at approximately 50% of all female inmates in the federal penitentiaries (12).
Canadian history presents examples of more subtle, but comparably harmful institutional racism policies and practices. One is how Indigenous Peoples health data has been misused and appropriated throughout the Canadian history to inform colonization processes and to sustain racist policies of subjugation (13). By using the Indian Act and the limited representativeness and damaging depictions of Indigenous Peoples in the health and social data they collected, government agencies and the Royal Canadian Mounted Police “pathologized and took action against [Indigenous communities] in a form of forceful removal of more than 150,000 Indigenous children from their families in the residential school system and the ‘60s scoop’” (14). In examining how information about Indigenous People has been collected and used in the past, the Royal Commission on Aboriginal Peoples in Canada concluded that Indigenous Peoples “have not been consulted about what information should be collected, who should gather that information, who should maintain it and who should have access to it” (15). According to a recent report by the First Nations Information Governance Centre in Alberta, Canada, both “the context & purposes of data have historically been determined outside First Nations communities and the misuse of data has led to situations of misappropriation and broken trust” (14).
Some progress has been made but much more is needed since the publication of the 1996 Report of the Royal Commission on Aboriginal Peoples and the release in 2015 of the Calls to Action by the Truth and Reconciliation Commission (16), which was established to document and inform Canadians about the experiences of Indigenous People who attended residential schools. The impact of racist colonial policies on the availability, accessibility, timeliness, accuracy and comprehensiveness of health outcome data in Indigenous Peoples as some of the populations bearing the brunt of the disease burden continues today.
National and jurisdictional level health reports rarely provide an insight into the burden of disease or treatment outcomes and not being able to see themselves in the national or provincial/territorial data has been an on-going concern of First Nations and Inuit organizations in Canada (17) Furthermore, lack of population-specific disease burden data continues to hamper efforts to achieve a meaningful reduction in the burden of nationally notifiable HCV infection and to “redress the legacy of residential schools and advance the process of Canadian reconciliation” (18) .
The immense loss and disruption experienced as intergenerational trauma when dissociated from culture and relational support strategies, instead becomes a catalyst for coping behaviours often deemed harmful and or illegal. Although harm reduction may be viewed as a term associated with supply of clean needles, condoms, legally produced psychoactive substances and offering of medical supervision within a substance use context, these medical approaches represent only a small part of many evolving distinctions-based culturally-grounded and wholistic wellness supporting activities.
Unfortunately, harm reduction services in some jurisdictions have been curtailed despite evidence demonstrating positive impact and cost-effectiveness, as well as connecting persons who use drugs to health supports, social services and drug treatment networks. Studies in Australia report harm reduction services specifically supporting needle and syringe programming prevented an estimated 96,000 HCV infections and over 32,000 HIV (human immunodeficiency virus) infections, thus saving four dollars in direct health care costs for every dollar invested in harm reducing needle syringe programs (19, 20).
Harm reduction and wellness support activities may assist people in regaining their sense of self-worth, self-determination, and opportunities to re-engage in community. Pursuing individual and community wellness may include revitalization of Indigenous languages, on-the-land healing, countering and preventing institutional and community racism, connecting to the land, traditional harm reduction practices and supporting awareness or prevention strategies. While HIV is still seen as the face of life-altering health outcomes with the potential to impact interactions between family and community, there is a growing appreciation of the similar life-altering impacts of HCV at the personal, family, community, and population levels.
Hepatitis C
Hepatitis C is a blood-borne virus whose chronic infection wreaks havoc on liver function, results in more life years lost than any other infectious disease in Canada and creates considerable risk for further liver disease and hepatocellular cancer (21). In 2019, an estimated 1% of Canadians had evidence of exposure to HCV (anti-HCV positive), while about 0.5% were living with chronic hepatitis C (22). This stands in stark contrast with respective estimates of 7.4% and 3.5% in Indigenous populations of Canada (22). The Indigenous/non-Indigenous prevalence ratio from the 2019 data is higher than the ratio reported in an earlier analysis of HCV infection in Manitoba at 2.4 times the HCV infection prevalence in non-First Nations population (23, 24).
While national estimates of awareness of HCV status in Indigenous populations are lacking, a recent analysis suggested 24% of Canadians with evidence of past or current HCV infection were not aware of their infection status (22), and earlier analyses put it between 44% (25) and 84% (26).
Between 2012 and 2022, the reported (crude) rate of newly diagnosed cases of HCV infection in First Nations communities in Canada has more than doubled from 72.2 per 100,000 in 2012 to peaking at 165.3 per 100,000 in 2018 (Figure 1). By 2022, the reported rate (112.4 per 100,000) was 32% lower than that in 2018 (Indigenous Services Canada, unpublished data, 2024 (Figure 1). During the same time, the rate of newly reported cases of HCV infection in the general Canadian population increased by 15% only from 29.4 per 100,000 in 2012 to peaking at 33.9 per 100,000 in 2018 (Figure 1). By 2021 (the most recent year with available national statistics), the reported Canadian rate of 19.7 per 100,000 was 42% lower than that in 2018 (27). The ratio of the reported rates for newly diagnosed HCV infection between First Nations living on-reserve and the general Canadian population has widened from 2.5 in 2012 to 5.2 in 2021 (Figure 1).
In 2022, among First Nations People in Canada, the highest rate of HCV diagnoses was reported in those aged 35-59 years (186.5 per 100,000) followed by those aged 18-34 years (171.7 per 100,000) (28). While rates of HCV diagnoses in First Nations males (114.1 per 100,000) and First Nations females (110.5 per 100,000) residing on-reserve were similar, when stratified by age group and sex, the highest age-specific rate was in younger females and older males, illustrating the need for tailored age- and sex-specific public health interventions (Figure 2), and highlighting the interconnected issues around power dynamics, partner violence and economic dependence (29, 30). In comparison, the reported HCV cases among males in Canada for 2020 was 22.9 per 100,000 and the rate among females was 13.7 per 100,000 (31).
The Colonial Legacy and Transmission of HCV
A devastating effect of the colonial legacy in Canada is the disproportionately high prevalence of HCV among Indigenous Peoples. The simplistic explanation is that Indigenous Peoples are significantly and disproportionately overrepresented in all the significant behavioral and social determinants or factors that lead to HCV acquisition, including substance use, incarceration, homelessness or crowded housing, non-sterile tattoo or piercing, and other determinants of risk activity for HCV acquisition and transmission. Of these factors the most extensive dataset can be obtained by examining rates of federal and provincial incarceration where Indigenous Peoples are seven-fold more likely than non-Indigenous people to be incarcerated in a federal institution (32, 33). In the provincial prisons included in ten provinces, the range varies from approximately four-fold greater incarceration rate in British Columbia all the way to a shocking twenty-six-fold increase in the province of Saskatchewan (33). Beyond the simplistic explanations, examining the root causes of these high incarceration rates shows a disturbing picture of disenfranchisement, discrimination, racism in the justice system, and rupture of traditional social and family supports. Muir et al. (34) studied a cohort of Indigenous adults in three Ontario cities, smaller, medium-sized and large (Thunder Bay, London, Toronto, respectively). They found that three factors contributed to high rates of incarceration: experiences of racism, removal from and/ or disturbance of family support, and victimization (34). Compounding the overrepresentation in determinants of HCV acquisition noted above, other factors sharply exacerbate ongoing HCV transmission: high rates of food insecurity and resulting malnutrition, inadequate access to basic healthcare, lack of HCV awareness and testing, reduced access to curative therapy coexistent with ongoing vectors for continuing horizontal transmission.
Access to Testing and Treatment
Direct acting antiviral (DAA) treatment options are available at no cost to eligible Canadians, including Indigenous Peoples, providing an improved treatment experience for HCV. Although sustained virologic response (SVR) rates after treatment completion in Indigenous Peoples match those of non-Indigenous populations, the rates of engaging in and completing treatment are markedly lower (35-39). Because access to prevention, harm reduction, testing and care varies widely among jurisdictions the prevalence of HCV varies as well and is reported to be from four to eleven times that of the general population. Variability is evident between First Nation members living off reserve in Ontario, Canada with longer median time from a positive HCV-antibody test result to HCV-RNA testing than individuals living on-reserve (288 days off reserve versus 68 days on reserve) (40). It is notable that 17% with a positive HCV antibody do not follow up with the next step to complete the HCV-RNA testing, and of those who do, 60% do not initiate treatment (40).
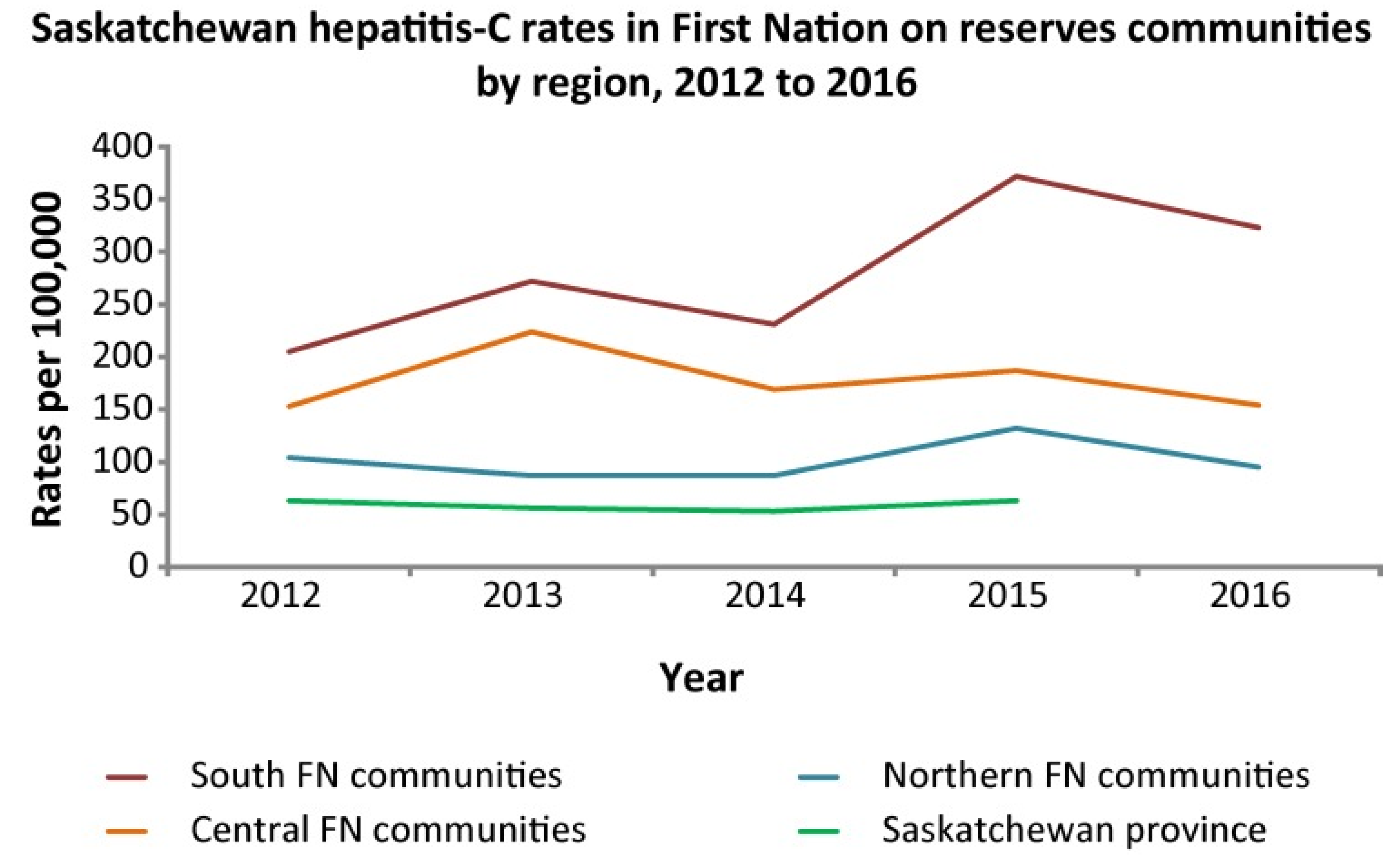
The Canadian provinces of Alberta and Saskatchewan, have limited on-reserve First Nations data. In Alberta, the highest rates of HCV occur in off reserve First Nations People (Figure 3). The COVID-19 pandemic may have decreased testing, and access to testing in recent years which could explain the recent decrease in HCV incidence. Efforts are underway to increase awareness and access to testing using standard serological testing as well as Dried Blood Spot (finger prick blood droplets placed on card and mailed for laboratory HCV-antibody and RNA processing) and Point of Care Rapid testing. In terms of geographical variation, interestingly in Saskatchewan FN, the rate of HCV is highest in the southern part of the province (Figure 4) (41).
Colonial Influence on Experience of Hepatitis
The etiology of the current disparate experience of hepatitis by Indigenous populations in Canada cannot be discussed without clear linkage to colonial disruptions that continue to the present time. The Indian Act of 1876, although enacted in the last century with the intent to terminate Indigenous culture and the social, political and economic relationships shaping distinct Indigenous Peoples, continues to dictate the funding and governance structure for health, education, lands, and leadership. Indigenous People living through, or having family members who experienced the colonizing disruptions and confines of forced attendance in residential school, being removed from their family by the child welfare system, or experiencing the injustices of the judicial system where we see a disparate number of Indigenous Peoples incarcerated, we see impacts not only to current physical, mental, emotional and spiritual wellbeing but also disruption of interpersonal relationships in the next generations, increased rates of numerous infectious and chronic diseases, and the draw to addictions as seen through multiple generations (42-45). Research with Indigenous young people conducted in British Columbia showed a significant association between childhood maltreatment (residential school, child welfare system, foster care, sexual abuse) and HCV infection (46). Many of the socio-economic systems in Canada conceived at the time of the Indian Act still influence healthcare services development, and access to it as evidenced by the reticence of Indigenous communities and community members to engage in hepatitis treatment (43).
Efforts toward the World Health Organization Goal of hepatitis elimination by 2030 outlined in the Blueprint to Inform Hepatitis Elimination Efforts identify priority populations as: People who are incarcerated (PWI); People who inject drugs (PWID); Indigenous Peoples (First Nations, Metis & Inuit); Gay, Bisexual and other men who have sex with men; Newcomer and Immigrants from countries with high prevalence rates; and people born between 1945-1975 (47) Over-representation of Indigenous Peoples is evident in several of these priority populations, skewing not only the data but also the stigma (21, 38, 48). By identifying Indigenous populations as a priority group are we actually supporting health equity or further stigmatizing an already heavily stigmatized population group? Among PWUD we must consider the socio-demographics within 28% of that group who also identify as Indigenous (49). The dual or intersectional stigma of racism, and HCV status, or identification with more than one of the priority population groups not only complicates the personal experience of interactions with healthcare systems but often compounds self-stigma, which may be seen as non-commitment to testing, treatment or as loss to follow-up (45, 50).
Strategies for Change through Promising Practice
Within the context of HCV, there continues to be gaps in equity, access, supports, and culturally competent care. However, especially over the past decade or so, significant changes and improvements have started, or are in progress. In many respects this is part of a greater societal change spurred by a very belated recognition of the harms, injustices and inequities suffered by Indigenous people over the past five centuries. In particular the Truth and Reconciliation Commission (3) has shed light on many of these issues and made a number of recommendations to address them. Canada has developed the United Nations Declaration on the Rights of Indigenous Peoples Act that received Royal Assent in 2021, which sets out that “the minimum standards for the survival, dignity and well-being of Indigenous Peoples of the world” must be implemented in Canada (51). Priority populations require unique priorities which include recognition, respect, relationships, and reconciliation efforts alongside concerted focus supporting cultural perspectives on wellness (52-54).
In terms of healthcare and with specific reference to HCV diagnosis and management, a number of important initiatives are underway. Increasing the representation of First Nations, Inuit and Métis in the Canadian health workforce in response to the 2015 Truth and Reconciliation Commission of Canada Calls to Action (3) will help foster trust and therapeutic alliance to improve health outcomes through the cascade of prevention, treatment and care. Indigenous patients may be more comfortable accessing care with Indigenous health providers raising the priority need to increase Indigenous health initiatives at medical and nursing schools, while supporting cultural safety training and Indigenous health workforce development alongside Indigenous Physicians Association of Canada, Canadian Indigenous Nurses Association, Office of Indigenous Health at the Royal College of Physicians and Surgeons of Canada, the Indigenous Health Committee at the College of Family Physicians of Canada and Indigenous Services Canada.
Addressing social determinants of health while expanding Indigenous health workforce alongside continued development and mobilizing of telehealth options, supporting remote access to HCV diagnosis and therapy, mobile outreach services, Dried Blood Spot testing, rapid Point of Care testing for antibody and viral load, as well as innovations such as at-home testing, and assessing current bureaucratic hurdles to lab diagnosis and treatment payment/reimbursement. Funding, training, and capacity supports must be provided to support increased awareness of HCV and confidence to treat among primary care providers and community health infrastructure supporting Indigenous populations. Specialists in urban centres can build treatment pathways supporting virtual access to culturally aware and low barrier testing and treatment. Increasing access to HCV prevention and management through primary care supports, substance use prevention, harm reduction programming, addiction treatment and recovery supports, supporting distinctions-based self-determined solutions led by and with Indigenous Peoples are collective contributions to HCV elimination efforts.
Creating a supportive environment for Substance Use Disorders recovery, or a Recovery Capital approach, can be a useful model, which by definition includes internal and external resources that can be drawn upon to initiate and sustain recovery. Such approaches go beyond clinical approaches, and include family and community capital in shaping a healing environment to support long-term success (55, 56).
Culturally connected resources to increase awareness and support prevention are integral to improving access. It is imperative to co-create multidisciplinary care supports focusing on competing psychosocial needs and social issues faced daily by equity-denied populations while allocating priority funding explicitly supporting cultural inclusion, wellness-based approaches and community-wide initiatives designed and led by Indigenous People (40, 45, 48, 50, 57, 58).
There a several examples across Canada where efforts are underway to provide connected care models. The Alberta ECHO program supports virtual access to a prescribing hepatologist for liver disease consults and HCV treatment in remote and Indigenous communities (54, 58). Through care conversations with Indigenous health care providers in Alberta the need for relevant HCV awareness resources was raised and Indigenous Knowledge Keepers collaborated to co-create and produce a DocuStory film showcasing HCV awareness through a liver wellness narrative approach (59).
Feedback from Indigenous communities in Alberta requesting increased access to HCV testing, prioritized policy change facilitating Dried Blood Spot testing as an option offering destigmatizing and low-barrier testing for multiple health concerns including HCV-antibody and HCV RNA through a finger prick that can be performed without extensive medical training (60). This creates testing options for home use, health fairs, mass screening or anywhere a lab is not readily accessible or to create an option for those who do not access mainstream healthcare facilities while providing an opportunity to build relationship, reconnect for results, and support wellness. Nurse-led programs across Canada provide exemplary opportunities for engagement and patient engagement relationship that support high levels of HCV testing and treatment success (61). Saskatchewan has co-created multi-disciplinary community-led models focusing on de-stigmatization and increasing access to the HCV treatment path utilizing a mentored connection (62). British Columbia co-created a ‘seek and treat’ model for micro-elimination working through nurses who visited people and their friend or family connections in their supportive housing sites to provide HCV treatment path services such as testing and treatment (62).
Addictions medicine and urban supportive care centres are also including HCV awareness, prevention, testing and treatment alongside social supports and harm reduction approaches to provide wrap-around supports in many settings including Calgary, Alberta (63) Toronto, Ontario (57) and Vancouver, British Columbia (64). Building relational and wellness supports for people impacted by the correctional system in Canada is also the focus of initiatives to provide testing, treatment or linkage to care (65). Although these programs may not be Indigenous-led they are seeking connected models of care that provide wellness supports that engage Indigenous people within urban populations. There are also many Indigenous-led efforts supporting destigmatization and wholistic perspectives across Canada. An example is the work of Kimamow Atoskanow Foundation in Alberta, Canada (66) shaping rural and land-based supports around wellness and cultural teachings on sexual health. The Ontario Aboriginal HIV/AIDS Strategy (OAHAS) provides culturally respectful and sensitive programming supporting physical, mental, emotional and spiritual aspects of life through supporting prevention, harm reduction, health promotion and partnerships in wellness for Indigenous Peoples in Ontario, Canada (67). And the Communities, Alliances and Networks (CAAN) organization partners to support HCV and HIV community readiness resources, education, funding, and programming (68).
Momentum for change includes creation of several Indigenous-led community organizations, initiatives, and collaborative co-developed community engagement and education resources. The initiatives mentioned here are by no means a comprehensive list, instead these examples are mentioned as a means to inspire consideration of potential for Indigenous-led advocacy in impacting current policy, disparate data, initiating or supporting community-based programming.
4. Discussion
Authors should discuss the results and how they can be interpreted from the perspective of previous studies and of the working hypotheses. The findings and their implications should be discussed in the broadest context possible. Future research directions may also be highlighted.
5. Conclusions
Conversation around HCV provide a clear example of the gaps in data and how this impacts initiatives, funding, education, testing and elimination efforts due to absent or inconsistent data collection and management nationally.
The high rates of HCV prevalence and annual incidence in Indigenous Peoples in Canada are a legacy of the colonial trauma of the past that continues in many respects to the present day. Indigenous Peoples are overrepresented in most of the behavioral determinants that lead to HCV acquisition. These include substance use, incarceration, homelessness, and substantial barriers to culturally safe prevention, high quality testing, curative DAA therapy and care. Many opportunities exist for improving the relationship between the justice system, police services, corrections infrastructure and Indigenous Peoples to address the racism, inequity and abuses both in judiciary policy as well as improving healthcare access and HCV treatment access within these structures.
As the data suggests, there are likely regional variations so intentional strategies are needed, as such is the case in Saskatchewan where the southern communities are clearly disproportionately impacted with higher HCV incidence. Furthermore, there are specific needs to provide interventions for young Indigenous females, who appear to be disproportionately impacted. With this in mind the COVID-19 pandemic demonstrated that Indigenous communities can implement focused in-community testing for infectious diseases, and localized approaches are effective at educating community members on health topics as well as conducting screening and providing personal and supportive wholistic care. It is also striking how the factors affecting initial engagement in care and retention in supportive care, are the pivotal piece in contributing to achieving SVR. We are hopeful that these important measures will eventually result in elimination of HCV in Indigenous Peoples in Canada.
Author Contributions
Conceptualization: KPRD, SSL. Literature review: KPRD, DW, MT, CS, TW. Data acquisition: DW, MT, CS. Data analysis: all authors. Writing first draft: all authors. Intellectual input and revision of draft: all authors. Final approval for submission: all authors.
Funding
This work was not funded by any outside agency.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Acknowledgments
We gratefully and respectfully acknowledge that we live and work on traditional lands of Indigenous People across what is now Canada. We are grateful for opportunities to learn from Indigenous Ways of Knowing, Being, Doing and Connecting as Indigenous Science and respectfully seek to build capacity within healthcare toward inclusion of these perspectives.
Conflicts of Interest
KPRD: speaking or consulting fees from Abbvie, Gilead, SRx Pharmacy, CATIE, Canadian Liver Foundation, International conference on Hepatitis and health in Substance Users (INHSU). DW: nil to declare. MT: employee of Government of Canada (Indigenous services Canada). CS: employee of Government of Canada (Indigenous services Canada). TW: employee of Government of Canada (Indigenous services Canada). HL: nil to declare. SSL: Speaking or consulting fees from: Abbvie, Gilead, Grifols, Jazz, Mallinckrodt, Oncoustics, and Justice Canada (HCV ‘Tainted Blood’ file).
Abbreviations
| HCV | Hepatitis C virus |
| ISC | Indigenous Services Canada |
| PWUD | Person who use drugs |
| SVR | Sustained Virological Response |
Glossary
1 Greenwood et al., 2022. Introduction to Determinants of First Nation, Inuit and Metis Peoples’ Health in Canada.
| Child welfare system / Foster Care / 60’s Scoop / Millennium Scoop | The current and past government run systems forcibly removing Indigenous children from their families, homes, and communities and placing them in non-Indigenous settings. Severing connection to culture, language and land and forcing assimilation and inter-generational trauma through discrimination, racism, neglect, physical, sexual, and emotional abuse (1). |
| Colonization | The acts of European entities rooted in religion, politics, economics and power used to subjugate and exploit Indigenous People in the process of settling Canada (1). |
| Decolonize | The undoing or divesting of colonial power of culture, languages, education, health and bureaucracy (1). |
| Indian Act of 1876 | Federal legislation regulating Indigenous People’s ability to live and access land, status, education, health supports and other aspects of daily life. Numerous amendments, revisions and re-enactments since the original document but still continues to impact all aspects of life for Indigenous People in what is now Canada (2). |
| Indigenous | Inclusive reference to the First Nation (Indigenous People who are not Inuit or Metis), Inuit (Indigenous People of the arctic and sub-arctic areas of Canada) and Metis (descendants of unions between Indigenous People and European fur traders creating a unique cultural entity) Peoples within what is known today as Canada (1). |
| Intergenerational Trauma | Past and ongoing traumatic events related to the colonizing of Canada inform the transfer of thoughts, behaviours, coping mechanisms, and health status with Indigenous People (1). |
| Knowledge Keeper | Trusted and respected Indigenous community member recognized for their experiences, the knowledge they have received, and their willingness to share these with others (1). |
| Reserve | Tracts of land set aside for use by specified Indigenous group of people, but the Crown or federal government retains title to this land. Historically specific rules controlled passage to and from these lands (2). |
| Residential School | Institutions set up by religious entities with government funding to forcibly house Indigenous children who were removed from their families, homes and communities and sometimes taken across the country. These schools took over 150,000 children age 5-16 years and focused on manual labor skills versus educational excellence. Over 6,000 children died or disappeared from these schools (2). |
| Two-Eyed Seeing | Approach to learning and understanding by seeing from one eye with Indigenous ways of knowing and from the other eye with Western ways of knowing (1) |
| Treaty | An agreement, recognized constitutionally between First Nations and the government of Canada, outlining obligations in return for access to land (2). |
| Truth and Reconciliation Commission and Calls to Action | The commission (2008-2015) was an element of the settlement for residential school survivors, and their families and communities, and established 94 calls to action to be taken by the government as steps to rectify harms and work toward reconciliation between Indigenous and non-Indigenous people of Canada (1)(3). |
| 2 Joseph & Joseph. 2019. Indigenous Relations | Insights, tips and suggestions to make reconciliation a reality. Indigenous Relations Press. |
References
- Greenwood M dLS, Stout R, Larstone R), Sutherland J. Introduction to Determinants of First Nation, Inuit and Metis Peoples’ Health in Canada., 2022.
- Joseph, B. Indigenous Relations: Insights, tips and suggestions to make reconciliation a reality: Indigenous Relations Press, 2019.
- https://www.rcaanc-cirnac.gc.ca/eng/1450124405592/1529106060525. In.
- https://www.statcan.gc.ca/en/subjects-start/indigenous_peoples. In.
- https://countryeconomy.com/countries/canada. In.
- https://www.thecanadianencyclopedia.ca/en/author/takwa-souissi#:~:text=Takwa%20Souissi%20is%20a%20lawyer,actualit%C3%A9%20and%20Premi%C3%A8res%20en%20Affaires. In.
- https://www.canlii.org/en/ca/scc/doc/2016/2016scc12/2016scc12.html. In.
- https://s3.documentcloud.org/documents/2698184/Jugement.pdf. In.
- https://decisions.chrt-tcdp.gc.ca/chrt-tcdp/decisions/en/item/232587/index.do?r=AAAAAQAOY2FyaW5nIHNvY2lldHkB. In.
- https://www.canada.ca/en/indigenous-services-canada/news/2021/09/government-of-canada-honours-joyce-echaquans-spirit-and-legacy.html. In.
- https://rapportspvm2019.ca/en/grands_dossiers/. In.
- https://oci-bec.gc.ca/sites/default/files/2023-10/Annual%20Report%20EN%20%C3%94%C3%87%C3%B4%20Web.pdf. In.
- Kovach, M. https://www.researchgate.net/publication/235413280_Indigenous_methodologies_Characteristics_conversations_and_contexts, 2009.
- k, M. https://afnigc.ca/wp-content/uploads/2024/01/Data_Resources_Report.pdf. In.
- https://publications.gc.ca/Collection-R/LoPBdP/EB/prb9924-e.htm. In.
- https://publications.gc.ca/site/eng/9.801236/publication.html. In.
- https://indigenousdatatoolkit.ca/project/the-fnigcs-a-first-nations-data-governance-strategy/. In.
- https://publications.gc.ca/site/archivee-archived.html?url=https://publications.gc.ca/collections/collection_2015/trc/IR4-8-2015-eng.pdf. In.
- Quon, A. https://www.cbc.ca/news/canada/saskatchewan/sask-drug-policy-1.7087683. In; 2024.
- https://www.health.gov.au/. In: Australian Government Department of Health & Ageing.
- Shoukry NH, Feld JJ, Grebely J. Hepatitis C: A Canadian perspective. Can Liver J 2018;1:1-3. [CrossRef]
- Popovic N, Williams A, Perinet S, Campeau L, Yang Q, Zhang F, Yan P, et al. National Hepatitis C estimates: Incidence, prevalence, undiagnosed proportion and treatment, Canada, 2019. Can Commun Dis Rep 2022;48:540-549.
- Sadler MD, Lee SS. Hepatitis C virus infection in Canada’s First Nations people: a growing problem. Can J Gastroenterol 2013;27:335. [CrossRef]
- Uhanova J, Tate RB, Tataryn DJ, Minuk GY. The epidemiology of hepatitis C in a Canadian Indigenous population. Can J Gastroenterol 2013;27:336-340. [CrossRef]
- Trubnikov M, Yan P, Archibald C. Estimated prevalence of Hepatitis C Virus infection in Canada, 2011. Can Commun Dis Rep 2014;40:429-436.
- Rotermann M, Langlois K, Andonov A, Trubnikov M. Seroprevalence of hepatitis B and C virus infections: Results from the 2007 to 2009 and 2009 to 2011 Canadian Health Measures Survey. Health Rep 2013;24:3-13.
- https://diseases.canada.ca/notifiable/. In.
- https://www.canada.ca/en/indigenous-services-canada.html. In.
- El-Bassel N, Shaw SA, Dasgupta A, Strathdee SA. People who inject drugs in intimate relationships: it takes two to combat HIV. Curr HIV/AIDS Rep 2014;11:45-51. [CrossRef]
- Stoicescu C, Cluver LD, Spreckelsen TF, Mahanani MM, Ameilia R. Intimate partner violence and receptive syringe sharing among women who inject drugs in Indonesia: A respondent-driven sampling study. Int J Drug Policy 2019;63:1-11. [CrossRef]
- https://www.canada.ca/en/public-health.html. In.
- Singh D, Prowse S, Anderson M. Overincarceration of Indigenous people: a health crisis. CMAJ 2019;191:E487-E488.
- Owusu-Bempah A, Kanters S, Druyts E, Toor K, Muldoon KA, Farquhar JW, Mills EJ. Years of life lost to incarceration: inequities between Aboriginal and non-Aboriginal Canadians. BMC Public Health 2014;14:585. [CrossRef]
- Muir NM, Rotondi M, Brar R, Rotondi NK, Bourgeois C, Dokis B, Hardy M, et al. Our Health Counts: Examining associations between colonialism and ever being incarcerated among First Nations, Inuit, and Metis people in London, Thunder Bay, and Toronto, Canada. Can J Public Health 2023. [CrossRef]
- Nitulescu R, Young J, Saeed S, Cooper C, Cox J, Martel-Laferriere V, Hull M, et al. Variation in hepatitis C virus treatment uptake between Canadian centres in the era of direct-acting antivirals. Int J Drug Policy 2019;65:41-49.
- O’Neil CR, Buss E, Plitt S, Osman M, Coffin CS, Charlton CL, Shafran S. Achievement of hepatitis C cascade of care milestones: a population-level analysis in Alberta, Canada. Can J Public Health 2019;110:714-721.
- Ortiz-Paredes D, Amoako A, Ekmekjian T, Engler K, Lebouche B, Klein MB. Interventions to Improve Uptake of Direct-Acting Antivirals for Hepatitis C Virus in Priority Populations: A Systematic Review. Front Public Health 2022;10:877585.
- Parmar P, Corsi DJ, Cooper C. Distribution of Hepatitis C Risk Factors and HCV Treatment Outcomes among Central Canadian Aboriginal. Can J Gastroenterol Hepatol 2016;2016:8987976.
- Saeed S, Thomas T, Dinh DA, Moodie E, Cox J, Cooper C, Gill J, et al. Frequent Disengagement and Subsequent Mortality Among People With HIV and Hepatitis C in Canada: A Prospective Cohort Study. Open Forum Infect Dis 2024;11:ofae239.
- Mendlowitz AB, Bremner KE, Krahn M, Walker JD, Wong WWL, Sander B, Jones L, et al. Characterizing the cascade of care for hepatitis C virus infection among Status First Nations peoples in Ontario: a retrospective cohort study. CMAJ 2023;195:E499-E512.
- Skinner S, Cote G, Khan I. Hepatitis C virus infection in Saskatchewan First Nations communities: Challenges and innovations. Can Commun Dis Rep 2018;44:173-178.
- Fayed ST, King A, King M, Macklin C, Demeria J, Rabbitskin N, Healy B, et al. In the eyes of Indigenous people in Canada: exposing the underlying colonial etiology of hepatitis C and the imperative for trauma-informed care. Can Liver J 2018;1:115-129.
- O’Keefe-Markman C, Lea KD, McCabe C, Hyshka E, Bubela T. Social values for health technology assessment in Canada: a scoping review of hepatitis C screening, diagnosis and treatment. BMC Public Health 2020;20:89.
- Gordon J, Bocking N, Pouteau K, Farrell T, Ryan G, Kelly L. First Nations hepatitis C virus infections: Six-year retrospective study of on-reserve rates of newly reported infections in northwestern Ontario. Can Fam Physician 2017;63:e488-e494.
- Pearce ME, Jongbloed K, Demerais L, MacDonald H, Christian WM, Sharma R, Pick N, et al. "Another thing to live for": Supporting HCV treatment and cure among Indigenous people impacted by substance use in Canadian cities. Int J Drug Policy 2019;74:52-61.
- Pearce ME, Jongbloed K, Pooyak S, Christian WM, Teegee M, Caron NR, Thomas V, et al. The Cedar Project: exploring the role of colonial harms and childhood maltreatment on HIV and hepatitis C infection in a cohort study involving young Indigenous people who use drugs in two Canadian cities. BMJ Open 2021;11:e042545.
- https://www.canhepc.ca/sites/default/files/media/documents/blueprint_hcv_2019_05.pdf. In.
- Krajden M, Cook D, Janjua NZ. Contextualizing Canada’s hepatitis C virus epidemic. Can Liver J 2018;1:218-230.
- Zietara F, Crotty P, Houghton M, Tyrrell L, Coffin CS, Macphail G. Sociodemographic risk factors for hepatitis C virus infection in a prospective cohort study of 257 persons in Canada who inject drugs. Can Liver J 2020;3:276-285.
- Amoako A, Ortiz-Paredes D, Engler K, Lebouche B, Klein MB. Patient and provider perceived barriers and facilitators to direct acting antiviral hepatitis C treatment among priority populations in high income countries: A knowledge synthesis. Int J Drug Policy 2021;96:103247.
- https://www.sac-isc.gc.ca/eng/1690909773300/1690909797208. In.
- https://www.indigenousrelationsacademy.com/products/indigenous-relations. In.
- Lourenco L, Kelly M, Tarasuk J, Stairs K, Bryson M, Popovic N, Aho J. The hepatitis C epidemic in Canada: An overview of recent trends in surveillance, injection drug use, harm reduction and treatment. Can Commun Dis Rep 2021;47:561-570.
- Dunn KP, Williams KP, Egan CE, Potestio ML, Lee SS. ECHO+: Improving access to hepatitis C care within Indigenous communities in Alberta, Canada. Can Liver J 2022;5:113-123.
- Granfield R, & Cloud, W.. Coming clean: Overcoming addiction without treatment. New York: New York University Press, 1999.
- Cloud W, & Granfield, R: A life course perspective on exiting addiction: The relevance of RC in treatment.. In: Nordic Council for Alcohol and Drug Research). Volume 44: NAD Publication, 2004; 185-202.
- Lettner B, Mason K, Greenwald ZR, Broad J, Mandel E, Feld JJ, Powis J. Rapid hepatitis C virus point-of-care RNA testing and treatment at an integrated supervised consumption service in Toronto, Canada: a prospective, observational cohort study. Lancet Reg Health Am 2023;22:100490.
- Dunn KPR, Oster RT, Williams KP, Egan CE, Letendre A, Crowshoe H, Potestio ML, et al. Addressing inequities in access to care among Indigenous peoples with chronic hepatitis C in Alberta, Canada. Lancet Gastroenterol Hepatol 2022;7:590-592.
- Dunn, KP. https://cumming.ucalgary.ca/resource/echo/home. In.
- Young J, Ablona A, Klassen BJ, Higgins R, Kim J, Lavoie S, Knight R, et al. Implementing community-based Dried Blood Spot (DBS) testing for HIV and hepatitis C: a qualitative analysis of key facilitators and ongoing challenges. BMC Public Health 2022;22:1085.
- Brown SJ, Cosgrove LT, Lee SS. Achieving HCV micro-elimination in rural communities. Can Liver J 2021;4:1-3.
- Pandey M, Konrad S, Reed N, Ahenakew V, Isbister P, Isbister T, Gallagher L, et al. Liver health events: an indigenous community-led model to enhance HCV screening and linkage to care. Health Promot Int 2022;37.
- Gale, N. https://www.catie.ca/programming-connection/shelter-based-hepatitis-c-treatment-at-the-calgary-drop-in-centre. In.
- Bartlett SR, Wong S, Yu A, Pearce M, MacIsaac J, Nouch S, Adu P, et al. The Impact of Current Opioid Agonist Therapy on Hepatitis C Virus Treatment Initiation Among People Who Use Drugs From the Direct-acting Antiviral (DAA) Era: A Population-Based Study. Clin Infect Dis 2022;74:575-583.
- Kronfli N, Dussault C, Bartlett S, Fuchs D, Kaita K, Harland K, Martin B, et al. Disparities in hepatitis C care across Canadian provincial prisons: Implications for hepatitis C micro-elimination. Can Liver J 2021;4:292-310.
- https://treeofcreation.ca/. In.
- https://www.oahas.org/. In.
- https://caan.ca/. In.
Figure 1.
Rate (per 100,000) of newly reported cases of HCV among First Nations communities vs. general Canadian population, 2011-2022. Data courtesy of Indigenous Services Canada, 2024.
Figure 1.
Rate (per 100,000) of newly reported cases of HCV among First Nations communities vs. general Canadian population, 2011-2022. Data courtesy of Indigenous Services Canada, 2024.
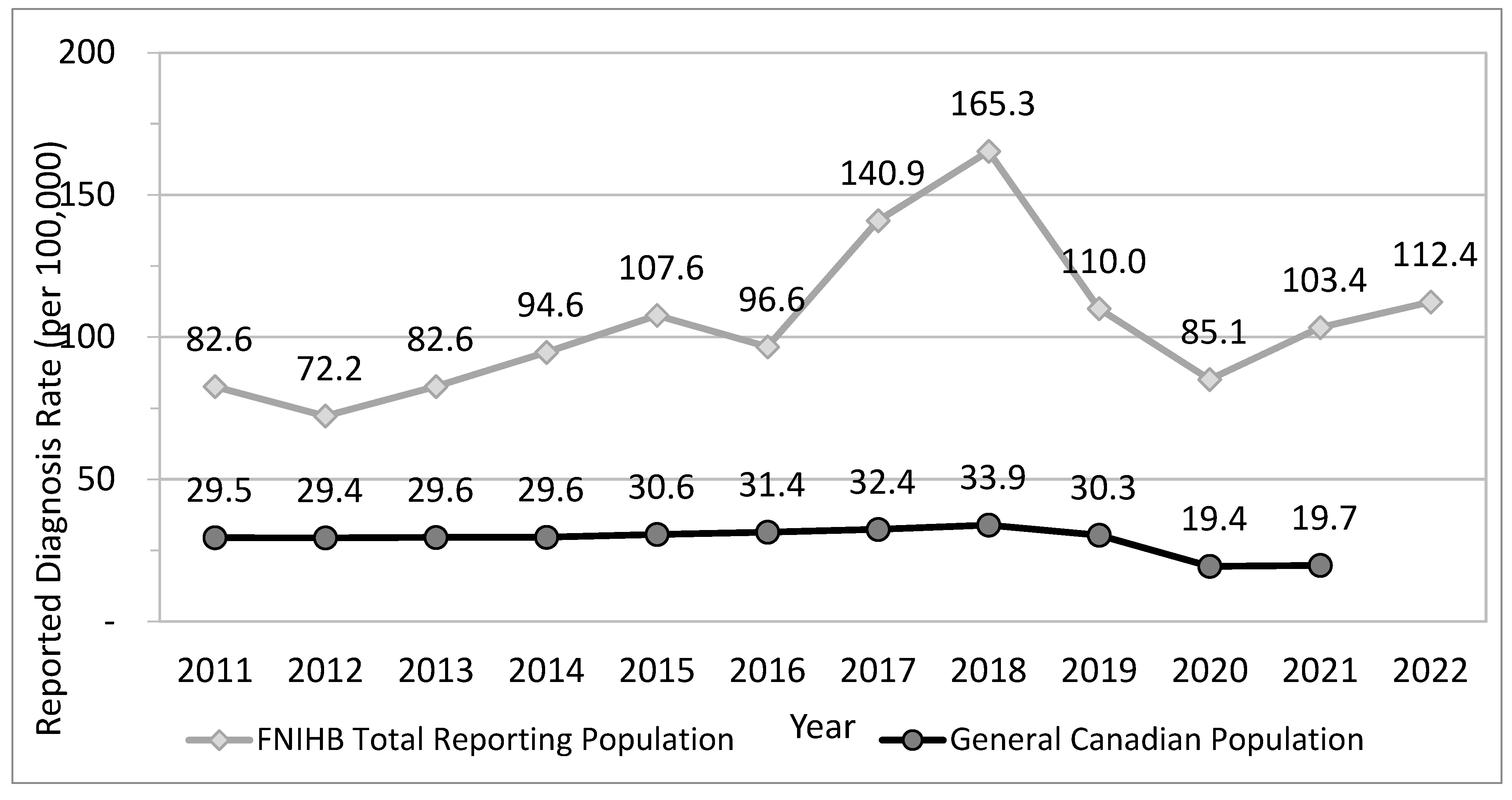
Figure 2.
Rate (per 100,000) of newly reported cases of HCV among First Nations communities by age group and sex, 2022. Data courtesy of Indigenous Services Canada, 2024.
Figure 2.
Rate (per 100,000) of newly reported cases of HCV among First Nations communities by age group and sex, 2022. Data courtesy of Indigenous Services Canada, 2024.
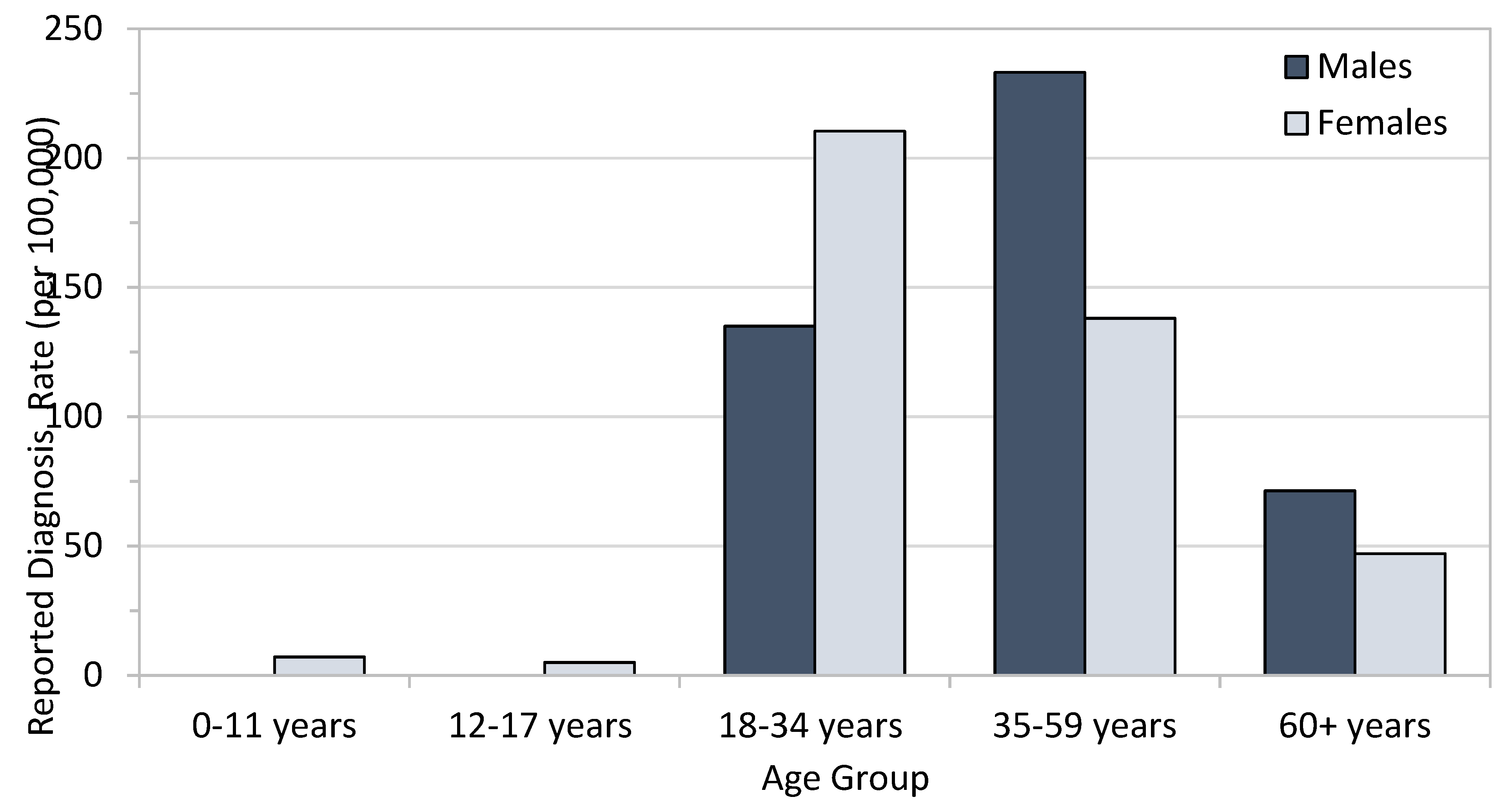
Figure 3.
Rate of reported HCV infections by population group in Alberta, 2017-2022. Sources: FNIHB AB CDC Database; Government of Alberta, Alberta Health; ISC, Indian Registry.
Figure 3.
Rate of reported HCV infections by population group in Alberta, 2017-2022. Sources: FNIHB AB CDC Database; Government of Alberta, Alberta Health; ISC, Indian Registry.
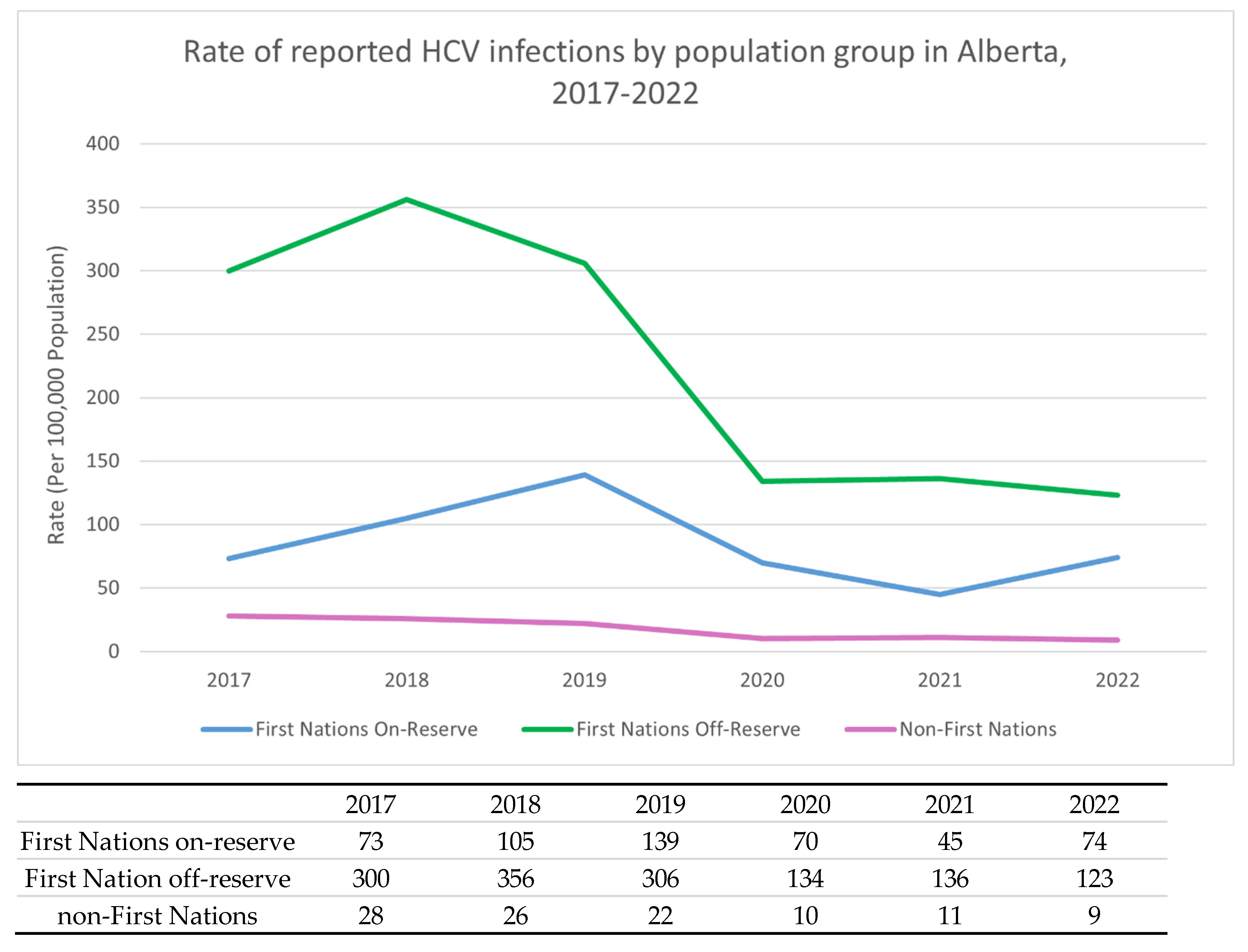
Figure 4.
HCV diagnosis rates in Saskatchewan province per 100,000 population, 2012-2016. Reproduced from Skinner et al. (41).
Figure 4.
HCV diagnosis rates in Saskatchewan province per 100,000 population, 2012-2016. Reproduced from Skinner et al. (41).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



