
Submitted:
20 August 2024
Posted:
21 August 2024
You are already at the latest version
Abstract
Manual handling is a major risk factor for work-related musculoskeletal disorders and one of the leading causes of disability-adjusted life years globally, necessitating multifaceted risk reduction measures. One potential intervention for manual handling tasks is work technique training assisted by augmented feedback on biomechanical exposures. However, there is a research gap regarding its effectiveness specifically for manual handling tasks in both real work environments and controlled settings, as well as its ability to induce retained reductions in biomechanical exposure. The gap was investigated using a rapid review comprising a literature search using two databases and 11 reviews/overviews to identify studies from the past 20 years, up to studies published by June 1, 2024. Sixteen studies were identified, with 14 of them being of high or moderate methodological quality and were included. Three studies were conducted in real work environments and eleven in controlled settings. Most studies (n = 9) used auditory feedback, followed by vibration feedback (n = 6). In real work environments, the evidence for the effectiveness of sensor-based augmented feedback in reducing biomechanical exposure during administration was considered to be inconsistent and very limited directly after administration. For longer periods after administration, ranging from one week to more than six months, there is currently no evidence demonstrating the effectiveness of the feedback. In controlled settings, there was strong evidence for its effectiveness during and immediately after administration, and limited evidence for effectiveness up to six months post-administration when considering the tasks included in the training. Future research needs are discussed.
Keywords:
augmented feedback
; biofeedback
; intervention
; work postures
; muscle activation
; musculoskeletal disorders
; musculoskeletal pain
; wearables
; work technique
; ergonomics
1. Introduction
1.1. Work-Related Disorders and Work Technique Training in Manual Handling
Work-related diseases and disorders remain a major
global health concern, affecting an estimated 1.7 billion people worldwide who
experience ill musculoskeletal conditions [1].
Musculoskeletal disorders (MSDs), such as low back pain and neck pain, alone
account for an estimated 95 million disability-adjusted life years globally [2]. Work-related musculoskeletal disorders (WMSDs)
and occupational accidents and diseases are estimated to cost 3.9% of the
global gross domestic product and 3.3% within the European Union [3]. Besides impairing work capacity and increasing
the risk of short- and long-term absenteeism, WMSDs can lead to premature exit
from the labor market [4–6]. The etiology of
WMSDs is multifactorial, involving both physical and psychosocial risk factors [7–9]. Major physical risk factors frequently
occurring in workplaces include repetitive and heavy manual handling [7,10–18], demanding postures and movements [7,10,12,18–22], and hand-arm and whole-body
vibrations [7,10,23,24].
Preventive management of hazardous manual handling
encompasses screening and risk assessment of exposures, as well as implementing
risk-reducing measures to eliminate or mitigate the identified hazards [25–30]. The use of mechanical lifting equipment are
commonly employed to reduce WMSD risks related to manual handling tasks [31–34], as well as work technique training aimed at
minimizing adverse postures or movements [35–38].
Work technique training is mandatory in European Union to mitigate hazardous
work-related manual handling [39]. The
training often aims to minimize the occurrence of stressful postures, such as a
flexed or rotated trunk during force exertion, as these postures increase the
risk of WMSDs [33,40–43].
Traditional training to improve work technique
typically comprises theoretical education on safe work techniques and brief
practical training sessions designed to incorporate the technique. While this
approach may be effective in certain contexts, recent systematic reviews have
concluded that such training has typically little to no clinically relevant
impact on reducing WMSDs [38,44–46]. For
greater effectiveness, it has been recommended that training is conducted over
a longer period to facilitate motor learning and include more realistic manual
handling tasks instead of a limited subset of simplified tasks [38]. Such an extension of the training period may
incur high costs, including a prolonged need for an instructor, and may often
be considered infeasible. To address this issue, one potential solution is to
complement traditional training with the use of sensor-based biofeedback
technologies [47]. These technologies provide
various systems for exposure- and risk assessment that can be utilized in work
contexts, and worker training assisted by augmented feedback through visual,
auditory, or tactile cues [47–50].
1.2. Current Research on the Effectivness of Sensor-Based Augmented Feedback Training
Sensor-based biofeedback has been used for several
decades in ergonomics research to reduce adverse exposure in work settings,
with a considerable proportion of studies focusing on computer tasks (e.g., [51–58]). Over the past 10–15 years, several studies
have been published, applying wearable sensor-based systems to reduce adverse
postures and movements in work-related tasks. The application of wearable
sensor technologies, including augmented feedback, to mitigate work-related
musculoskeletal disorders (WMSDs) has been reviewed in several recent studies [47–50,59–65] However, most of these reviews lack an
assessment of the methodological quality of the studies they reviewed [47–50,59,60,64] and have not evaluated the strength
of the evidence for the effectiveness of augmented feedback [47–50,59–61,64].
However, the reviews by Lee et al. [66] and Lind [63]
included both assessments of methodological quality and grading of the evidence
for the effectiveness of sensor-based augmented feedback in reducing adverse
exposures related to WMSDs. Additionally, Frasie et al. [62] assessed the methodological quality and the
strength of the evidence for extrinsic feedback for both MSD prevention and
rehabilitation, and had a broader scope that included feedback from instructors
such as therapists, not limited to only sensor-based feedback. None of these
three reviews exclusively targeted manual handling tasks. Instead, assessment
of the strength of evidence for the effectiveness of augmented feedback was
based on a broad range of diverse tasks, including sedentary computer entry tasks,
odontology tasks, and manual handling tasks such as order picking and patient
transfer. This mixture of tasks ranges from sedentary activities with lower
force exertions and more static postures to tasks with more dynamic movements
and moderate- to high physical exertion demands. Given the distinct nature of
these different task types, there is a need to evaluate the effectiveness of
augmented feedback separately.
The study by Lee et al. [66]
did not differentiate the effectiveness of interventions in controlled settings
from those in real work environments, nor did it assess the strength of
evidence over different time frames to differentiate direct effects from
retained effects. Lind [63] assessed the
strength of evidence separately for studies conducted in controlled settings
versus real work environments, as well as the temporal aspects (short,
moderate, and long-term), the study was however limited to wearable motion
capture systems. Consequently, studies targeting a reduction in adverse
exposure in manual handling using EMG or non-ambulatory sensor-based
technologies were omitted as they did not fulfill the inclusion criteria (e.g.,
[66,67]). Similarly, several studies
evaluating the effectiveness of sensor-based feedback were not included in the
reviews by Lee et al. [66] (e.g., [68–70]) and Frasie et al. [62](e.g., [69,71–73]).
Based on the current literature, there is a gap in
the research literature regarding the evidence for the effectiveness of
sensor-based augmented feedback to mitigate adverse biomechanical exposure in
manual handling tasks. There is also a need to differentiate the evidence for
the effectiveness in real work environments versus controlled settings (i.e.,
laboratory settings) and to distinguish their short-term and long-term effects.
1.3. Aim
This rapid review aims to fill the identified
research gap by evaluating the evidence for the effectiveness of sensor-based
augmented feedback in reducing biomechanical exposure of the upper body in
work-related manual handling tasks. The evaluation of the evidence considers
temporal aspects of feedback deployment (direct, short-term, mid-term, and
long-term effects) as well as the specific settings for its use (real work
environments versus controlled settings).
2. Materials and Methods
A rapid review design was applied, following the
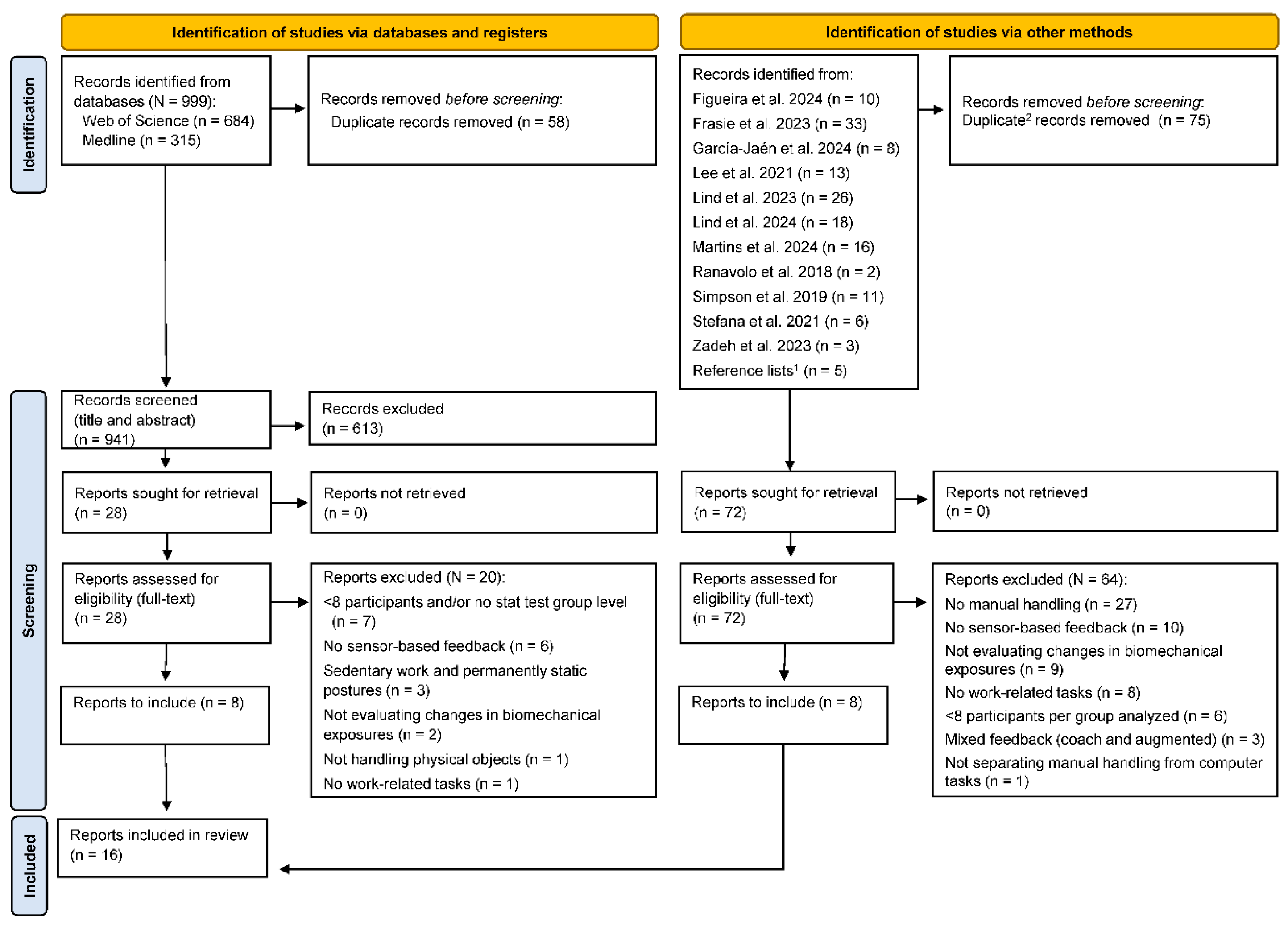
Cochrane Rapid Reviews Methods Group guidelines for rapid reviews [74] and structured using the PRISMA 2020 guidelines
[75].
2.1. Eligibility Criteria
To be eligible, the source had to be a
peer-reviewed journal article written in English, presenting an evaluation of
augmented feedback from data recorded by sensors aimed at reducing
biomechanical exposure in work-related manual handling tasks in an adult
population. Studies focusing on rehabilitation and sports were excluded (Table 1).

Table 1.
The eligibility criteria for the inclusion and exclusion of studies.
| Eligibility criteria | Descriptions |
|---|---|
| Studies evaluating sensor-based instruments or systems that monitor biomechanical exposure targeting the upper body and provide augmented feedback to the wearer based on this information. | Various biomechanical exposures are targeted, including posture, movement, and muscle activity etc. The primary body segments targeted include the neck (e.g., head inclination), spine (cervical to lumbosacral segments), arms (upper and lower), and wrists/hands. Only instruments or systems providing direct feedback to the wearer were considered. For example, evaluations on the effectiveness of an instructor assisted by sensor-based data are outside the scope. The focus on sensor-based augmented feedback excludes other types of augmented feedback, such as from athletic tapes. |
| Studies aiming to reduce adverse biomechanical exposure with the long-term objective of preventing or reducing work-related musculoskeletal disorders (WMSDs). | The study should report (at least briefly) how the reduction of the targeted biomechanical exposure can potentially mitigate adverse health effects, including WMSDs.Studies aiming to increase biomechanical exposure to achieve health benefits, such as interrupting prolonged sustained postures with increase physical activity, are excluded. |
| Studies evaluating augmented feedback on manual handling tasks performed in real work environments or those that simulate work-related manual handling tasks or single operations in controlled settings. | Manual handling operations encompass tasks such as lifting, pushing, pulling, and holding. This review excludes studies focused on predominantly sedentary jobs or tasks involving a significant proportion of static (isometric) postures, such as computer typing, dentistry, or surgical work. Additionally, the emphasis on work-related manual handling tasks excludes studies involving the manipulation of non-physical (virtual) objects. |
| Studies evaluating augmented feedback on adults (18–67 years) from regular working populations or student populations. | If the sample includes participants older or younger than 18–67 years, the data on the effect of feedback must be reported separately for those aged 18–67 years. The focus on regular working populations and student populations means that specific patient populations, such as those with medical conditions that hinder task performance, are excluded. |
| Studies evaluating augmented feedback on at least 8 participants per group receiving the feedback, and where the effect of the feedback is tested statistically | A sample size of fewer than 8 participants per group is acceptable only if justified by power calculations, including descriptions of the assumed effect size. The number of participants refers to those included in the final analysis. |
2.2. Search Strategy
To identify relevant literature, 11 recent reviews
were used as basis along with a systematic electronic literature search to
identify newly published literature (Figure 1).
The reviews covered different periods and scopes. For example, the review by
Frasie et al. [62] covered studies from 1986
to August 2, 2022, whereas Lee et al. [65]
covered studies from 2005 to July 15, 2021. To identify literature published
after 2020, a systematic electronic literature search was conducted using the
databases by Medline and Web of Science. The search period was 1 January 2020,
to 9 June 2024. Additionally, the reference lists of included articles and the
author's personal libraries were used to retrieve additional records. Duplicate
records were removed using the function: Remove Duplicates in Microsoft
365 Excel (Microsoft Corporation, Redmond, WA, USA), followed by manual check
to identify and exclude any potential remaining duplicates.
2.3. Study Selection
The eligibility criteria were applied to the
identified articles by one reviewer (C.M.L.) based on their titles and
abstracts (Figure 1). If eligibility
could not be determined from the titles and abstracts, the full text was then
assessed.
2.4. Methodological Quality Assessment
To assess the methodological quality, the tools to
assess controlled intervention studies, and observational cohort and
cross-sectional studies by the National Heart, Lung, and Blood Institute [76] were used (see Appendix
B, Tables B1 and B2). Recognizing
the potential variance in quality scores arising from different methodological
assessment tools, it was predetermined to restrict the selection to these two
tools.
One reviewer (C.M.L.) assessed the methodological
quality by assessing the pre-defined criteria as follows: fulfilled, not
fulfilled, not applicable, or cannot be assessed due to insufficient reported
(i.e., not reported). Fulfilled criteria were assigned one point, and
criteria that were either not fulfilled or not reported were assigned zero
points. For criteria judged as not applicable, a deduction of the maximum score
was made. Subsequently, the score was utilized to classify the methodological
quality as follows: high quality (≥75% of the maximum score), moderate quality
(50–74% of the maximum score), and low quality (<50% of the maximum score).
Figure 1.
PRISMA 2020 flow diagram of the inclusion process [47,48,49,50,59,60,61,62,63,64,65]. Notes: 1 additional reference was retrieved from the reports included in the database search; 2 duplicate records were included from the database search and those identified from the 11 reviews and overviews.
Figure 1.
PRISMA 2020 flow diagram of the inclusion process [47,48,49,50,59,60,61,62,63,64,65]. Notes: 1 additional reference was retrieved from the reports included in the database search; 2 duplicate records were included from the database search and those identified from the 11 reviews and overviews.
2.5. Strength of Evidence Assessment
The strength of evidence (see Table 2) was assessed by one reviewer (C.M.L.)
utilizing a seven-category scale ranging from no evidence to strong
evidence adapted from Lee et al. [65] and
Lind [63].
| Strength of evidence | Criteria |
|---|---|
| Strong evidence | Consistent findings among three or more studies of at least moderate quality, including at least two of high quality. |
| Moderate evidence | Consistent findings among two or more studies of at least moderate quality, including at least one of high quality. |
| Limited evidence | Findings from at least one study of high quality or two studies of moderate quality. |
| Very limited evidence | Findings from one study of moderate quality. |
| Inconsistent evidence | Inconsistent findings among multiple studies, such as one or multiple studies of at least moderate quality reporting significant result, whereas one or multiple studies of at least moderate quality reporting no significant result. |
| Conflicting evidence | Conflicting results between studies, such as one or multiple studies of at least moderate quality reporting significant result in one direction, whereas one or multiple studies of at least moderate quality reporting significant result in the other direction. |
| No evidence | Insignificant results derived from multiple studies of high or moderate quality. |
2.6. Data Extraction
The following information of the included studies
were extracted by one reviewer (C.M.L):
- Targeted outcome
- Study design (including the use of a control group)
- Setting and tasks performed
- Participants’ characteristics (sex, age, and eligibility)
- Feedback evaluation and duration of the retention tests
- Feedback characteristics (type and modality, targeted body region, and feedback trig-ger)
- Equipment for collecting and analyzing exposure data (including if it is ambulatory)
Additionally, the force demands, and task
complexity of the tasks performed by the participants were subjectively
assessed based on the information reported and general experience with similar
tasks.
Table 3.
Feedback retention categories, modified based from the duration classification by Lind [63].
Table 3.
Feedback retention categories, modified based from the duration classification by Lind [63].
| Duration Classification | Criteria (time elapsed after feedback administration) | Abbreviated names |
|---|---|---|
| During feedback | Simultaneous to feedback administration | During feedback |
| Directly after | Directly after, and up to 8 hours after | Directly after (≤8 hours) |
| Very short term | >8 hours, and up to ≤1 week after | Very short term (≤1 week) |
| Short term | >1 week, and up to ≤1 month after | Short term (≤1 month) |
| Midterm | >1 month, and up to <6 months after | Midterm (<6 months) |
| Long term | 6 months or more after | Long term (≥6 months) |
3. Results
After removing duplicates, a total of 1013 unique
records were identified from the literature search (Figure 1) and underwent screening based on
their titles and abstracts, with 100 undergoing full-text assessment. Upon
application of the eligibility criteria, 16 peer-reviewed articles, each
comprising one relevant study, were deemed fulfilling assessment of inclusion.
3.1. Quality Assessment
The assessment of the methodological quality of the
16 identified studies is shown in Tables 4 and 5.
For two studies, the methodological quality was assessed using both quality
assessment tools resulting in full agreement of the quality ratings between the
tools. Among the 16 identified studies, eight (50%) were classified as having
high quality, while six (38%) were classified as having moderate quality.
Furthermore, two studies (13%) were classified as having low methodological
quality and consequently were excluded. Hence, 14 studies were included in the
synthesis.
The methodological quality criteria with the lowest
fulfillment rates of the 16 initial studies were:
- Not reporting the participation rate of eligible persons of the identified pool of eligible persons (n = 15) (Criterion 3).
- Not blinding (or reporting blinding) of assessors to the participants' group allocation (n = 15) (Criterion 12).
- No clear justification of the sample size to detect difference in the outcome with at least 80% power (n = 13) (Criterion 5).
Table 4.
Methodological quality assessment using the NHLBI tool for observational cohort or cross-sectional studies (see Table B1 for a full description of the criteria).
Table 4.
Methodological quality assessment using the NHLBI tool for observational cohort or cross-sectional studies (see Table B1 for a full description of the criteria).
| Study | Criteria | Quality | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | ||
| Agruss et al. [77] | 1 | 1 | NR | 1 | NR | 1 | 1 | 1 | 1 | 0 | 1 | NR | 1 | 1 | Moderate |
| Boocock et al. [78] | 1 | 1 | NR | 1 | 1 | NA | 1 | 1 | 1 | 1 | 1 | NR | 1 | 1 | High |
| Bootsman et al. [79] | 1 | 1 | NR | NA | NR | 1 | 1 | 1 | 0 | 1 | 1 | NR | 1 | 0 | Moderate |
| Brandl et al. [67] | 1 | 1 | NR | 1 | NR | 0 | 0 | 1 | 1 | 0 | 0 | NR | 1 | 0 | Low |
| Kamachi et al. [80] | 1 | 1 | NR | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | NR | 1 | 1 | High |
| Kernozek et al. [81] | 0 | 0 | NR | 1 | NR | 1 | 1 | 1 | 1 | 0 | 1 | NR | 1 | 1 | Moderate |
| Langenskiöld et al. [72] | 1 | 1 | NR | NA | NR | 1 | 1 | 1 | 0 | 1 | 1 | NR | 1 | 0 | Moderate |
| Lim et al. [71] | 1 | 1 | NR | NA | NR | 1 | 1 | 1 | 1 | 1 | 1 | NR | 1 | 1 | High |
| Lind et al. [82] Sens | 1 | 1 | NR | NA | NR | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | Moderate |
| Lind et al. [69] AE | 1 | 1 | NR | NA | NR | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | High |
| Lind et al. [73] Erg | 1 | 1 | 1 | NA | NR | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | High |
| Oppici et al. [83] | 1 | 1 | NR | NA | NR | 1 | 1 | 1 | 1 | 1 | 1 | NR | 1 | 1 | High |
| Owlia et al. [68] | 1 | 1 | NR | 1 | NR | 1 | 1 | 1 | 0 | 1 | 1 | NR | 1 | 0 | Moderate |
| Punt et al. [66] | 1 | 0 | NR | NR | NR | 1 | 1 | 1 | 1 | 1 | 1 | NR | 1 | 1 | Moderate |
| Ribeiro et al. [84] | 1 | 1 | NR | 0 | NR | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | Low |
| Ribeiro et al. [70] | 1 | 1 | NR | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | High |
Notes: 1: criterion fulfilled; 0: criterion not fulfilled; N/A: not applicable; NR: not reported. Questions: 1. Clear research question; 2. Clear study population; 3. Participation rate; 4. Subjects recruitment; 5. Justified sample size; 6. Temporality of exposure(s) and outcome(s); 7. Sufficient time 8. Dependent variable scaling; 9. Independent variables treatment; 10. Assessment of dependent variable; 11. Assessment of dependent variable; 12. Blinding; 13. Loss to follow-up; 14. Control of confounders.
Table 5.
Methodological quality assessment using the NHLBI tool for controlled intervention studies (see Table B2 for a full description of the criteria).
Table 5.
Methodological quality assessment using the NHLBI tool for controlled intervention studies (see Table B2 for a full description of the criteria).
| Study | Criteria | Quality | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | ||
| Ribeiro et al. [84] | 1 | 0 | 0 | 0 | NR | 0 | 0 | 1 | NR | NR | 0 | 0 | NR | 1 | Low |
| Ribeiro et al. [70] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | NR | NR | 1 | 1 | 1 | 1 | High |
Notes: 1: criterion fulfilled; 0: criterion not fulfilled; NR: not reported. Questions: 1. Study description; 2. Randomization; 3. Concealed allocation; 4. Blinding (providers and participants); 5. Blinding (assessors); 6. Baseline characteristics; 7. Endpoint dropout; 8. Endpoint dropout (between groups); 9. Adherence; 10. Confounding interventions; 11. Quality of outcomes assessment; 12. Justified sample size; 13. Prespecified analysis; 14. Group assignment.
3.2. Study Design, Methodology, and Instruments
3.2.1. Study Design, Settings, Tasks and Participants
As shown in Table 6,
a cross-sectional design was the most common study design, used in 11 studies,
while two studies used a combination of cross-sectional- and longitudinal
designs. Only one study employed a cluster randomized control trial design
(RCT) [70]. A control group was used in half
of the studies, while the rest predominantly compared the effect of the
feedback to the baseline. All studies, except for Lind et al. [82] targeted a reduction in biomechanical exposure
of the spine, including reductions in spine flexion or inclination, moment, or
lumbosacral compression force. Besides the spine, three studies [69,72,82] targeted a reduction in upper arm
elevation exposure. The majority of studies (n = 11) were conducted in
controlled settings, while three studies were carried out in real work
environments where the subjects performed regular work tasks.
As shown in Table 7,
the most common task evaluated was related to handling box-type items, which
was explicitly reported to be used in eight studies (57%). Health care and care
tasks were performed in four studies (29%); two studies exclusively targeted
patient transfer, while the other two included various activities performed in
real work environments. The assumed force demands and task complexity varied
between the studies; about half the tasks were assumed to be of low complexity,
while six studies involved moderate to high task complexity. An example of an
assumed low-complexity task involved lifting a box in a controlled setting from
about 15 cm to knuckle height. In contrast, examples of high-complexity tasks
included a series of various patient transfer tasks in a controlled setting and
various care and health care tasks in real work environments. In terms of force
demands, the majority of studies (79%) were assumed to include or potentially
include high force demands.
As shown in Table 8,
the total number of participants was 444 (median = 20), of whom 43% were men,
51% were women, and 6% had unreported sex. In six studies, the greater majority
(i.e., >60% of the participants) were men; in four studies, the greater
majority were women; while in three studies, there was a balanced sex
distribution (i.e., not more than 60% of any sex). Half of the studies (n = 7)
included younger adults (mean age of 20–29 years); in four studies, the mean
age was 30–39 years; and in two studies, the mean age was 40–49 years. Most of
the studies (n = 9) included novice participants either unfamiliar with the
tasks performed or students for whom the tasks were part of their training,
while five studies included participants familiar with the task or similar tasks.
Table 6.
Study characteristics and targeted outcomes.
| Study | Targeted outcome | Study design | Control group | Setting |
|---|---|---|---|---|
| Agruss et al. [77] | Reduce peak lumbosacral compression | CS | Yes | Cont. |
| Boocock et al. [78] | Reduce lumbosacral posture and trunk flexion | CS | Yes | Cont. |
| Bootsman et al. [79] | Reduce episodes of lower back flexion | CS | No | Real |
| Kamachi et al. [80] | Reduce time in end-range lumbar spine flexion | CS/SLN | Yes | Cont. 1 |
| Kernozek et al. [81] | Reduce peak lumbosacral moment | CS | Yes | Cont. |
| Langenskiöld et al. [72] | Reduce time in adverse trunk inclination and arm elevation | CS | No | Cont. |
| Lim et al. [71] | Reduce sagittal trunk flexion angles | CS | No | Cont. |
| Lind et al. [82] | Reduce time in adverse arm elevation | CS | No | Cont. |
| Lind et al. [69] | Reduce time in adverse trunk inclination and arm elevation | CS | No | Cont. 2 |
| Lind et al. [73] | Reduce time in adverse trunk inclination | CS/SLN | No | Real |
| Oppici et al. [83] | Reduce spine flexion | CS | No | Cont. |
| Owlia et al. [68] | Reduce peak lumbar spine flexion | CS | Yes | Cont. 1 |
| Punt et al. [66] | Reduce low-back load (L5/S1 net moment, trunk inclination and lumbar flexion) | CS | Yes | Cont. |
| Ribeiro et al. [70] | Reduce occurrence of trunk inclination | cluster RCT | Yes | Real |
Notes: CS: cross-sectional; SLN: semi-longitudinal; RCT: randomized control trial; Real: real work environment; Cont: controlled setting; 1 HomeLab at Toronto Rehabilitation Institute; 2 training facility in a real work setting.
Table 7.
Type of manual handling tasks in the studies.
| Study | Force demands | Task complexity | Tasks | Description | |
|---|---|---|---|---|---|
| Agruss et al. [77] | H | L | Lifting | Symmetrical sagittal plane lifts of boxes ('maximum safe load'1) from pallet height to knuckle height at 30-second intervals. | |
| Boocock et al. [78] | H | L | Lifting and lowering | Lifting and lowering a 13-kg box (30×25×25.5 cm) with handles (10 lifts/min) from a platform (height: 15 cm) to an upright standing position, holding it still, and then lowering the box back to the platform. | |
| Bootsman et al. [79] | L–H | H | Health care and home care tasks | Various intensive care and home care tasks. | |
| Kamachi et al. [80] | H | M–H | Patient transfer | A series of simulated patient transfer activities of a patient actor (87 kg), e.g., transfer patient from bed to wheelchair, from wheelchair to couch, and assist patient to stand, don pants and transfer to wheelchair. Additional skill transfer task: patient sling insertion task. |
|
| Kernozek et al. [81] | H | L | Lifting and lowering | Lifting cases of bananas (mean: 18 kg) and various items (13.6–18.1 kg). Items lifted from pallet on the floor to a 2.1-meter height location and from a 2.1-meter height location to the pallet. | |
| Langenskiöld et al. [72] | L–M | L–M | Office-type of manual handling | Organizing 38 documents, lifting 8 large empty boxes, relocating 8 ring binders, and lifting 10 small empty boxes. | |
| Lim et al. [71] | M–H | M | Construction activities | Lifting pouches (25×36 cm, 4.5 kg) from floor height, carrying them 1.2 m, and lowering them. Transferring the pouches using a shovel to a location 1.2 m away. Simulated rebar tying tasks. | |
| Lind et al. [82] | L | L | Mail (letter) sorting | Sorting 30 randomly ordered letters (marked 0–9) to their corresponding letter tray (marked 0–9). | |
| Lind et al. [69] | L–M | M–H | Order picking | Simulated order-picking task resembling real order-picking, with items (0.1–3.1 kg) located in seven positions (heights: 0.15–1.3 m). | |
| Lind et al. [73] | M–H | H | Order picking | Sorting of packages (3–15 kg, 3–6 packages/min) from a container to a storage container (height: 0.3–1.1 m). Handling of containers was also included (including pushing) and registering each handled item. | |
| Oppici et al. [83] | H | L | Lifting and lowering | Lifting (symmetrical sagittal plane lift) a 7.5-kg box from floor height to knuckle height and lowering it back to floor height (10 lifts/min). | |
| Owlia et al. [68] | H | M–H | Patient transfer | A series of simulated patient transfer activities of a patient actor (82 kg), e.g., transfer patient from bed to wheelchair, from wheelchair to couch, and assist patient to stand, don pants and transfer to wheelchair. | |
| Punt et al. [66] | H | L | Lifting and lowering | Lifting and lowering a 10-kg box to three locations: a left/center/right positions and two depth (far and nearby) positions. | |
| Ribeiro et al. [70] | L–H | H | Health care activities | Various health care activities performed within aged care institutions and hospitals. |
Notes: assumed force demands and task complexity, low (L), moderate (M), high (H); 1 maximum safe load refers to a load weight of less than 24 kg and resulting in an individually predicted compression force of less than 3.4 kN.
Table 8.
Participants characteristics.
| Study | Participants: sex, age (mean, SD) and eligibility |
|---|---|
| Agruss et al. [77] | 28 college students (10 men; 18 women), 23.2 (3.4) years. Verbal acceleration feedback group: n = 9; 24.1 (4.8) years. EMG feedback group: n = 10; 22.8 (2.5) years. Control group; n = 9; 22.7 (2.4) years. Eligibility (health status): no having acute or chronic back pain. |
| Boocock et al. [78] | 36 university students1 (sex: NR). Feedback group: (n = 18); 25.7 (4.6) years. Control group: (n = 16); 25.6 (5.1) years.Eligibility (health status): no back injury or complaint in the past 6 months; no history of spinal surgery; without any cardiovascular or neurological conditions; no existing musculoskeletal injury. Other 2: not experienced in manual handling or performed regular handling in their work. |
| Bootsman et al. [79] | 13 nurses (all women); 40 (14) yearsEligibility (health status): no LBP. Other: not having a sedentary job |
| Kamachi et al. [80] | 20 participants (10 men; 10 women). Feedback group (5 female; 5 male); 24 (4) years. Control group (5 female; 5 male); 24 (3) years. Eligibility (health status): no back pain in the last 6 months or any MSDs or issues related to the spine. Other: no previous experience in caregiving or healthcare; able to understand and speak English. |
| Kernozek et al. [81] | 22 warehouse workers (all men); age: NR. Feedback training group (n=11); control group (n = 11). Eligibility (health status): NR. Other 2: regularly performing warehouse lifting or lowering tasks. |
| Langenskiöld et al. [72] | 10 participants3,4 (2 men; 8 women); 43.9 (12.0) years. Eligibility (health status): Not having pain or restrictions in movement. |
| Lim et al. [71] | 14 participants (all men); 26 (5) years.Eligibility (health status): without MSDs. Other: 18–35 years age; no previous experience of construction; no previous training on safe construction work techniques. |
| Lind et al. [82] | 16 university staff/students (7 men; 9 women); 25 (8) years.Eligibility (health status): no musculoskeletal discomfort or disorders that could hinder the manual handling task. |
| Lind et al. [69] | 155 warehouse workers (12 men; 3 women); 39 (12) years.Eligibility (health status): no musculoskeletal discomfort or disorders that could hinder the manual handling task. |
| Lind et al. [73] | 15 warehouse workers (14 men; 1 women) 6; 31 (12) years. Eligibility (health status): no disorders or pain that prevent performing daily work. Other: currently working as order picker. |
| Oppici et al. [83] | 20 university students (13 men; 7 women); 30 ± 6 years. Eligibility (health status): Not having back injury or pain in the last year, undergoing spinal surgery, or any cardiovascular, neurological or musculoskeletal condition at the time of the study, or allergy to adhesives. |
| Owlia et al. [68] | 20 participants (10 men; 10 women). Feedback training group: (6 men; 4 women); 28 (6) years. Control group: (4 men; 6 women); 25 (3) years. Eligibility (health status) 2: no history of back pain in the last six months and no musculoskeletal issues related to the spine. Other 2: adult s (i.e., ≥18 years); having no formal training in caregiving or patient handling; able to understand and speak English. |
| Punt et al. [66] | Control group: 14 participants (7 men and 7 women); 23.7 ± 8 years. Feedback moment group: 29 participants (22 men and 7 women); 25.7 ± 4 years. Feedback inclination group: 28 participants (13 men and 15 women); 24.9 ± 7 years. Feedback lumbar flexion group: 21 participants (15 7 men and 7 7 women); 25.9 ± 10 years. Eligibility (health status) 2: no recent history of low back pain. Other 2: no previously knowledge about the biomechanics of lifting; not having participated in any other studies related to lifting and biomechanics. |
| Ribeiro et al. [70] | 130 healthcare workers (20 men; 110 women); 45 (13) years. Feedback group (10 men; 53 women); 48 (range: 37–55) years. Control group (10 men; 57 women); 47 (range: 32–56) years.Eligibility (health status): performing regular work activities without any limitations such as due to LBP or LBP symptoms. Other: adult health care worker; working at least 20 hours/week. |
Notes: 1 31 participants’ data was analyzed, i.e., 15 of 18 participants in the feedback group completed the full session and all participants in the control group. 2 not explicitly reported as inclusion criteria; 3 data analyzed for 9 participants; 4 nine administrative office workers and one industrial manual handler; 5 the data of 2 participants were excluded from the final analysis due to technical issues; 6 data collection was performed on 20 participants but only 15 completed all sessions and were included in the final analysis; 7 the numbers reported by Punt et al. [66] do not add up.
3.2.2. Feedback Characteristics and Distribution, and Equipment
As indicated in Table
9, feedback effects were most commonly evaluated during the feedback
delivery phase (10 studies) and immediately afterwards (8 studies). Notably,
only four studies [70,73,80,81] evaluated the
retention effect beyond one week, while two studies [70,80]
evaluated the retention effect beyond one month. The duration of the feedback
training session varied considerably, ranging from one or two occasions of a
few minutes to several weeks, as in the study by Ribeiro et al. [70], but typically ranged from about 10–15 minutes
to an hour.
Table 9.
Feedback evaluation and distribution.
| Study | Feedback evaluation | Feedback distribution |
|---|---|---|
| Agruss et al. [77] | During feedback 1 Very short term (≤1 week) |
Baseline – All lifting two 5-min sets (each 10 lifts) without feedback; instructions from video on basics of safe lifting mechanics (all participants) Week 1 – CG: 40 lifts without feedback; FBGs A and B: 10 lifts without feedback; 10 lifts (100% feedback); 10 lifts (50% feedback); 10 lifts without feedback. Week 2 – CG: 40 lifts without feedback; FBGs A and B: 10 lifts without feedback; 5 lifts (100% feedback); 15 lifts (33% feedback); 10 lifts without feedback. Week 3 – All: lifting two 5 min sets (each 10 lifts) without feedback Feedback session duration: ~15 minutes |
| Boocock et al. [78] | During feedback | Order (no baseline): Lifting for 20 min (FBG: with feedback; CG: without feedback) Feedback session duration: ~20 min |
| Bootsman et al. [79] | During feedback Directly after (≤8 hours) |
Order: Baseline (30 min, no feedback); Feedback session 1 (60 min, feedback); Retention test session (60 min, no feedback); Feedback 2 session (60 min, feedback3) Feedback session duration: ~120 min |
| Kamachi et al. [80] | Directly after (≤8 hours) 4 Short term (≤1 month) Midterm (≤6 months) |
Session 1: FBG+CG (no feedback); FBG+CG video training Sessions 2 and 3: FBG (100%8 feedback); CG: (no feedback) Sessions 4 and 6: FBG+CG (no feedback) Sessions 6 and 7: FBG (50%8 feedback); CG (no feedback) Session 8: FBG+CG (no feedback) Retention tests (sessions 9 and 10): previous tasks and a new task to test the skill transfer Sessions 9 (after 2 weeks): FBG+CG (no feedback) Sessions 10 (after 2 months): FBG+CG (no feedback) Feedback session duration: ~60 minutes. Session duration: about 15 min each for session 1–8 (session 1–4 performed on day 1 and session 5–8 on day 2) |
| Kernozek et al. [81] | Short term (≤1 month) | Week 1 (baseline): Lifting 2 (both groups: without feedback) Weeks 2 and 4: Lifting 2 (feedback group: with feedback; control group: not lifting) Weeks 6: Lifting 2 (both groups: without feedback) Feedback session duration: ~30 minutes |
| Langenskiöld et al. [72] | During feedback Directly after (≤8 hours) |
Order: Practice session; Baseline (4-6 min, no feedback); Feedback session (8-12 min, feedback); Retention session (4-6 min, no feedback). Feedback session duration: ~8–12 min |
| Lim et al. [71] | During feedback | Random order: 3 feedback sessions each performed in 3 tasks. Feedback condition: no feedback; feedback from device on the back or the wrist. Tasks: lifting/lowering (mean: 3.4 min); shoveling (mean: 7.2 min); rebar tying (mean: 6.9 min) Feedback session duration: ~35 min |
| Lind et al. [82] | During feedback | Order: Practice session (no feedback); b) Baseline (no feedback); Ergonomics instruction session 1 (no feedback); Feedback session 1 (feedback); Ergonomics instruction session 2 (no feedback); Feedback session 2 (feedback). Session duration: all sessions but practice session (~1 min) Feedback session duration: ~2 min |
| Lind et al. [69] | During feedback Directly after (≤8 hours) |
Order: Practice session (no feedback); Baseline (no feedback); Feedback session 1 (feedback); Feedback session 2 (feedback); post-Feedback session (no feedback). Session duration: all sessions but practice session (~6 min) Feedback session duration: ~12 min |
| Lind et al. [73] | During feedback Directly after (≤8 hours) Very short term (≤1 week) Short term (≤1 month) |
Order: Baseline (no feedback): Feedback session 1 (2 days after baseline; feedback); Feedback session 2 (~7 days after baseline; feedback); post-Feedback session (directly after Feedback session 2; no feedback); Retention session 1 (~1 week after Feedback session 2; no feedback); Retention session 2 (~3 weeks after Feedback session 2; no feedback). Session duration: Baseline (~45 min); Feedback sessions and post-Feedback session (~30 min); Retention sessions (~45 min) Feedback session duration: ~60 min |
| Oppici et al. [83] | During feedback Directly after (≤8 hours) |
All conditions: 30 lifts/lower; 6 min rest; retention test (5 lifts/lower) Order (2 min break between condition): Baseline, Feedback condition (A or B), Feedback condition (B or A) Feedback was not provided during retention test Feedback session duration: ~3 minutes each with audio- and tactile feedback |
| Owlia et al. [68] | Directly after (≤8 hours) 3 | Day 1 – Session 1 (no feedback); Video training (only FBG); Session 2 (no feedback); Sessions 3 and 4 (FBG: feedback; CG no feedback); Day 2 – Session 5 (no feedback); Sessions 6 and 7 (FBG: feedback; CG no feedback); Session 8 (no feedback) Session duration: session 1–7 (~10 min) Feedback session duration: ~about 40 minutes |
| Punt et al. [66] | During feedback Directly after (≤8 hours) |
All sessions: 12 lifts/lower Session 1 (Baseline): no feedback Sessions 2 and 3: feedback for feedback groups; no feedback for control group. Session 4 (retention test): no feedback Feedback session duration: NR |
| Ribeiro et al. [70] | During feedback Very short term (≤1 week) Short term (≤1 month) Midterm (≤6 months) Long term (≥ 12 months) |
Baseline Intervention (for 4 weeks) Retention tests after: 1 week, 1 month, 3 months, 6 months, 12 months. Feedback session duration: 4 work weeks |
Notes: Abbreviations: CG, control group; FBG. Feedback group; NR, not reported; 1 not analyzed statistically; 2 series of six lifts in different conditions; 3 visual feedback and note taking was used in combination with auditory and vibration feedback; 4 the effect observed while provided feedback was reported but not evaluated statistically and was therefore excluded from this analysis.
As shown in Table 10,
the feedback trigger evaluated comprised of distinct cutoff thresholds at one
or two levels (10 studies) or a constant audio tone that gradually increased in
intensity with increased biomechanical load (4 studies). Notably, all the
ambulatory systems used distinct thresholds. An alternative to the gradually
increasing feedback intensity was to use two thresholds to further notify the
user of increased biomechanical exposure, as was used in seven studies.
Conversely, a single threshold level was used in only three studies.
In total, 307 participants received feedback
training. The most common feedback modalities were auditory (9 studies),
vibration (6 studies), and visual (1 study). In all studies, with the exception
of Bootsman et al. [79], only one feedback
modality was provided simultaneously. All studies evaluated feedback initiated
automatically by the system, rather than by the user. Additionally, corrective
feedback was used in all studies, while Langenskiöld et al. [72] also used reinforcing feedback for half of the
participants, in combination with corrective feedback.
As shown in Table 11,
motion capture data (derived from e.g., IMUs and accelerometers) were used as
input for the feedback in all studies, while muscle activity (derived from
sEMG) was only used in the study by Agruss et al. [77].
Among the capture instruments, IMUs were the most common (9 studies, 64%),
followed by optical (video-camera) motion capture systems (3 studies, 21%),
while accelerometers and electromagnetic motion tracking devices were each used
in one study. The use of a commercial system was stated of being used in one
study (i.e., Ribeiro et al. [70]), while
Agruss et al. [77] did not reported the system
used. In the remaining studies, custom solutions that applied a combination of
commercial devices and custom-developed devices and programs were used. Fully
ambulatory systems were evaluated in eight studies, meaning that they are not
restricted to being used in one location at a time, but can be worn by the user
without setting up the equipment.
Table 10.
Feedback characteristics and trigger.
| Study | Feedback type |
Feedback modality | Primary body region(s) | Feedback trigger |
|---|---|---|---|---|
| Agruss et al. [77] | System-initiated Corrective fading Concurrent or terminal1 |
A: audio B: audio (verbal) |
Lumbosacral spine | Gradually increased feedback intensity: Group A: muscle activity (electromyographic) Group B: acceleration index (difference between the dynamically and statically determined lumbosacral peak compression forces) |
| Boocock et al. [78] | System-initiated Concurrent corrective | Audio | Lumbosacral spine | 1 feedback level: >80% of maximum lumbosacral range-of-motion |
| Bootsman et al. [79] | System-initiated Concurrent cumulative) corrective |
Audio and Vibration 2 + Visual 3 |
Lumbosacral spine | 1 feedback level: >20° lower back flexion for >1.5 s (max 1 notification / 5 min) |
| Kamachi et al. [80] | System-initiated Concurrent and fading 4 corrective | Audio | Lumbosacral spine | 2 feedback levels: 20° less than 70% max forward lumbar flexion (intermittent tone); >70% of max forward lumbar flexion (continuous tone). |
| Kernozek et al. [81] | System-initiated Concurrent corrective | Audio | Lumbosacral spine | Gradually increased feedback intensity with increased spinal moments (L5/S1) |
| Langenskiöld et al. [72] | System-initiated Terminal corrective and reinforcing | Vibration | Spine (thoracic–lumbosacral) Upper arm |
1 feedback level per body region: >30° trunk inclination for >10% of the time. >30° arm elevation for >30% of the time. |
| Lim et al. [71] | System-initiated Concurrent (cumulative) corrective | Vibration | Spine (thoracic–lumbosacral) | 2 feedback levels: >45° trunk inclination (3 intermittent vibrations). 3 s continuous vibration if the criteria was reached >2 times within 2 min. |
| Lind et al. [82] | System-initiated Concurrent corrective | Vibration | Upper arm |
2 feedback levels: Arm elevation ≥30° and ≥60° |
| Lind et al. [69] | System-initiated Concurrent corrective | Vibration | Spine (thoracic–lumbosacral) Upper arm |
2 feedback levels per body region: Arm elevation ≥30° and ≥60° Trunk inclination ≥20° and ≥45° |
| Lind et al. [73] | System-initiated Concurrent corrective | Vibration | Spine (thoracic–lumbosacral) | 2 feedback levels: Trunk inclination >30° and >45° |
| Oppici et al. [83] | System-initiated Concurrent corrective 5 | Audio | Lumbosacral spine | Gradually increased feedback amplitude and modulation frequency with increased spine flexion angle. |
| Owlia et al. [68] | System-initiated Concurrent corrective | Audio | Lumbosacral spine | 2 feedback levels: 20° less than 70% of maximum forward lumbar flexion; 70% of maximum forward lumbar flexion. |
| Punt et al. [66] | System-initiated Concurrent corrective | Audio | Lumbosacral spine | Gradually increased feedback intensity. A 6 80% of the average peak sagittal plane moments during baseline. B 7 80% of the average peak trunk inclination angles during baseline. C 8 70% of the average of the observed peak lumbar flexion angles during baseline |
| Ribeiro et al. [70] | System-initiated Concurrent cumulative corrective | Audio | Lumbosacral spine | 2 feedback levels: ≥45° lumbopelvic forward bend (continuous >5 s) ≥45° lumbopelvic forward bending (occurring within 25 s after condition 1). |
Notes: 1 group A: concurrent feedback and group B: terminal feedback; 2 condition 1 (audio and vibration feedback); 3 condition 2 (audio, vibration and visual feedback); 4 2 variations: feedback given each time the criteria were met (i.e., 100%), and fading where provided half the time the criteria were met (i.e., 50%); 5 group B received tactile feedback from Sport leukotape, but this is not included in this synthesis; 6 Moment feedback group; 7 Inclination feedback group; 8 Lumbar flexion feedback group.
Table 11.
Equipment for collecting and analyzing exposure data.
| Study | Equipment (exposure analysis; feedback trigger) | Motion sensor | Ambulatory |
|---|---|---|---|
| Agruss et al. [77] | Group A: NR Group B: Custom |
Prototype version of the video analysis system the V-Task. 6 reflective markers on the wrist, elbow, shoulder, hip, knee, and ankle joint. Group A: additionally, an EMG-system (name and location: NR) |
No |
| Boocock et al. [78] | Custom: custom-designed software (LabView) | 2 IMUs (Shimmer Sensing, Ireland) Location: 1st lumbar spinous process and sacral body (S1) |
Partly |
| Bootsman et al. [79] | Custom: smartphone Android application | 2 IMUs (LSM9DSO, STMicroelectronics, Sweden) Location: 1st and 5th lumbar spine vertebrae |
Yes |
| Kamachi et al. [80] | Custom: PostureCoach v0.2 | 2 IMUs (MTi-3, Xsens Technologies, Enschede, Netherlands) Location: (back) thoracic vertebrae (T10) and approx. to sacrum |
Yes |
| Kernozek et al. [81] | Custom and commercial: motion Monitor software (Innovative Sports Training, Inc., IL, USA); Custom Matlab programs (Version 6.5, The Mathworks Inc., MA, USA); Motion Monitor software. Auditory feedback was controlled by the LiftTrainerTM software. | Ascension Electromagnetic Tracking Device (Ascension Technology Corporation, Burlington,USA) Sensor location: forearms, upper arm, back of the head, cervical (C4) and sacral (S1) region of the spine. |
No |
| Langenskiöld et al. [72] | Custom: Smartphone Android application (ErgoRiskLogger) | 2 IMUs (LPMS-B2 IMU, LP Research, Tokyo, Japan) Location about at the level of 1–2 thoracic vertebrae, and distal part of m. deltoideus. |
Yes |
| Lim et al. [71] | Custom: custom-designed software with hardware Raspberry Pi 3 board and PC | 4 IMUs (Mbientlab MetaMotionR+) Location: 6th thoracic vertebra, right thigh, right shin and dominant wrist |
Partly |
| Lind et al. [82] | Custom: smartphone Android application (ErgoRiskLogger ) | 1 IMU (LPMS-B2 IMU, LP Research, Tokyo, Japan) Location: distal part of m. deltoideus |
Yes |
| Lind et al. [69] | Custom: smartphone Android application (ErgoRiskLogger) | 2 IMUs (LPMS-B2 IMU, LP Research, Tokyo, Japan) Location: 1–2 thoracic vertebrae, and distal part of m. deltoideus |
Yes |
| Lind et al. [73] | Custom: smartphone Android application (ErgoRiskLogger) | 1 IMU (LPMS-B2 IMU, LP Research, Tokyo, Japan) Location: 1–2 thoracic vertebrae |
Yes |
| Oppici et al. [83] | Custom: Visual3D software (CMotion, Inc.) and custom script in MATLAB (The Mathworks Inc., MA, USA); Pure Data via Open Sound Control protocol. | 10-camera motion capture system (Qualisys AB, Gothenburg, Sweden) with 36 reflective markers attached to the trunk, pelvis, thighs, shanks and feet. |
No |
| Owlia et al. [68] | Custom: PostureCoach v0.2 | 2 IMUs (MTi-3, Xsens Technologies, Enschede, Netherlands) Location: 10th thoracic vertebrae and approx. to sacrum |
Yes |
| Punt et al. [66] | Custom: custom-made Matlab (The Mathworks Inc., MA, USA) program | 3 camera arrays of a 3D motion capture system (Optotrak Certus system; Norton Digital Inc.). Light emitting diodes markers attached: both shanks and thighs, pelvis (sacrum) and thorax (T6 spinous process). |
No |
| Ribeiro et al. [70] | Commercial: Spineangel (Movement Metrics Ltd, Hamilton, New Zealand) | 1 triaxial accelerometer (Spineangel) Location: lateral around the hip |
Yes |
Notes: NR: not reported; IMU: inertial measurement unit.
3.3. Effectiveness of Feedback in Real Work Environments
The findings of the studies assessing sensor-based augmented feedback in real work
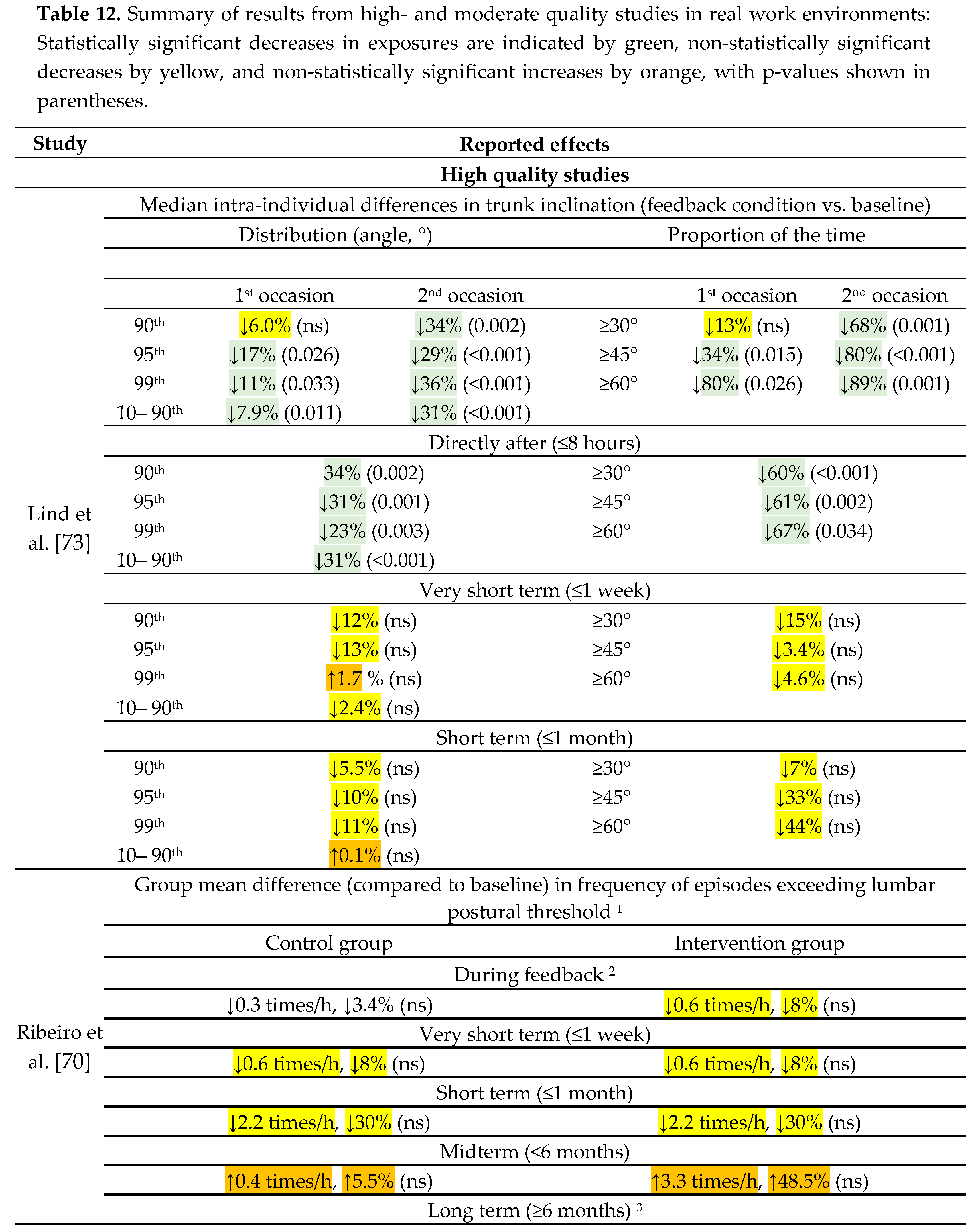
environments, categorized as high- and moderate-quality, are shown in Table 12. Additionally, a summary of the
evidence is presented in Table 15.
3.3.1. Effect during Feedback Administration
The effectiveness of sensor-based augmented
feedback in reducing biomechanical exposure of the upper body in work-related
manual handling tasks during its administration was evaluated in three studies,
two of which were assessed as having high methodological quality. While Ribeiro
et al. [70] observed modest and
non-significant reductions in exposure for the intervention group, Lind et al. [73] reported considerable reductions, which were
most pronounced during the second feedback training session and for peak
exposures. For example, the proportion of time in trunk inclination ≥60°
decreased by 89%, and trunk inclination ≥45° decreased by 80%, both of which
were statistically significant and considered to have clinical relevance if
maintained long-term. Similarly, the study by Bootsman et al. [79] indicated that the effect of feedback training
increased from the first session to the second session, with a 25% significant
reduction in the frequency of poor postures compared to the baseline.
Based on this, the current evidence for the
effectiveness of sensor-based augmented feedback in reducing biomechanical
exposure during administration is considered inconsistent in real work
environments.
3.3.2. Effect Directly after Feedback Administration
The effectiveness of sensor-based augmented
feedback directly after feedback administration was evaluated by Lind et al. [73] and Bootsman et al. [79].
While Lind et al. [73] reported considerable
and statistically significant reductions in trunk inclination—such as a
decreased proportion of time in trunk inclination ≥60° (67%) and ≥45°
(61%)—Bootsman et al. [79] reported a tendency
towards a decreased frequency of poor postures compared to the baseline, but
this was not statistically significant.
Based on this, the current evidence for the
effectiveness of sensor-based augmented feedback in reducing biomechanical
exposure directly after administration is considered very limited in real work
environments.
3.3.3. Retained Effects: Very Short and Short Term
The effectiveness of sensor-based augmented
feedback after periods of up to one week and one month was evaluated in two
high-quality studies by Ribeiro et al. [70]
and Lind et al. [73]. Both studies observed
no statistically significant effects of the feedback on episodes exceeding the
lumbar postural threshold or trunk inclination. However, Lind et al. [73] observed a tendency for reduced peak angles
(i.e., 95th and 99th percentiles) by up to 13% and a decreased portion of
time spent above 60° trunk inclination (up to a 44% decrease), although these
differences compared to baseline were not statistically significant.
Based on this, the assessment of the current
evidence is that there is no evidence supporting the effectiveness of
sensor-based augmented feedback after periods of up to one week and one month
in real work environments.
3.3.4. Retained Effects: Midterm and Long Term
The effectiveness of sensor-based augmented
feedback after periods of up to six months and more than six months was
evaluated in a single high-quality study by Ribeiro et al. [70], for which no significant changes in frequency
of exceeding the lumbar postural threshold due to the feedback was observed.
Based on this, the assessment of the current
evidence is that there is no evidence supporting the effectiveness of
sensor-based augmented feedback after periods of up to six months and more than
six months in real work environments.
3.4. Effectiveness of Feedback in Controlled Settings
The findings of the studies assessing sensor-based
augmented feedback in controlled settings categorized as high- and
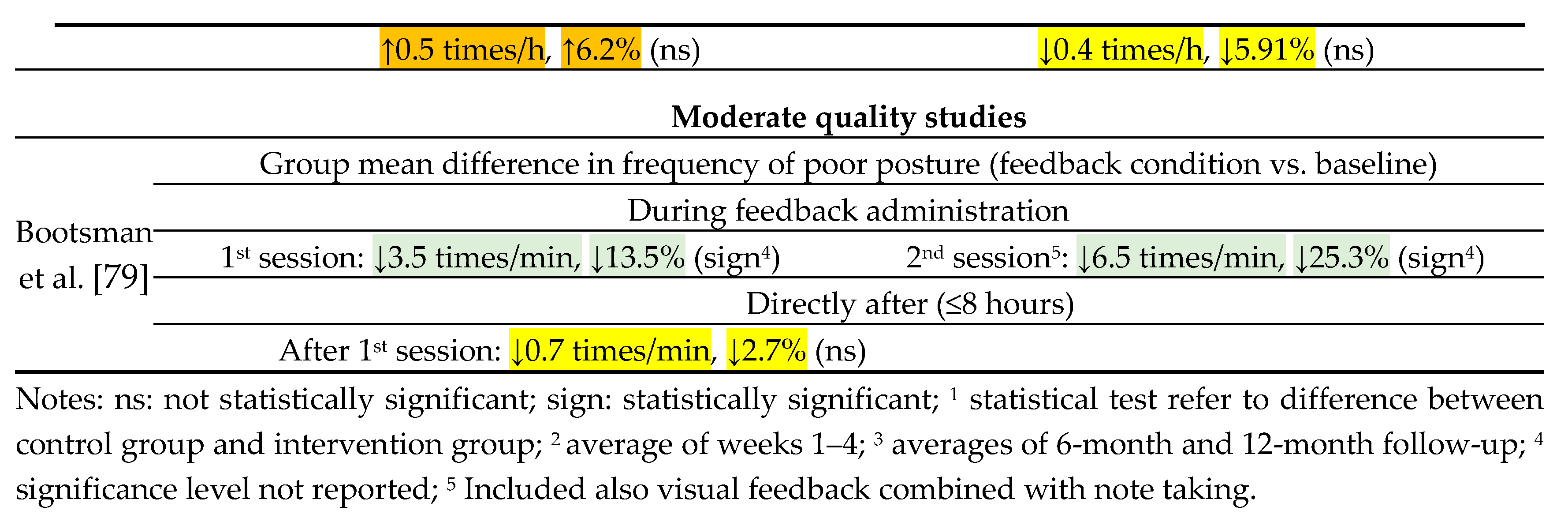
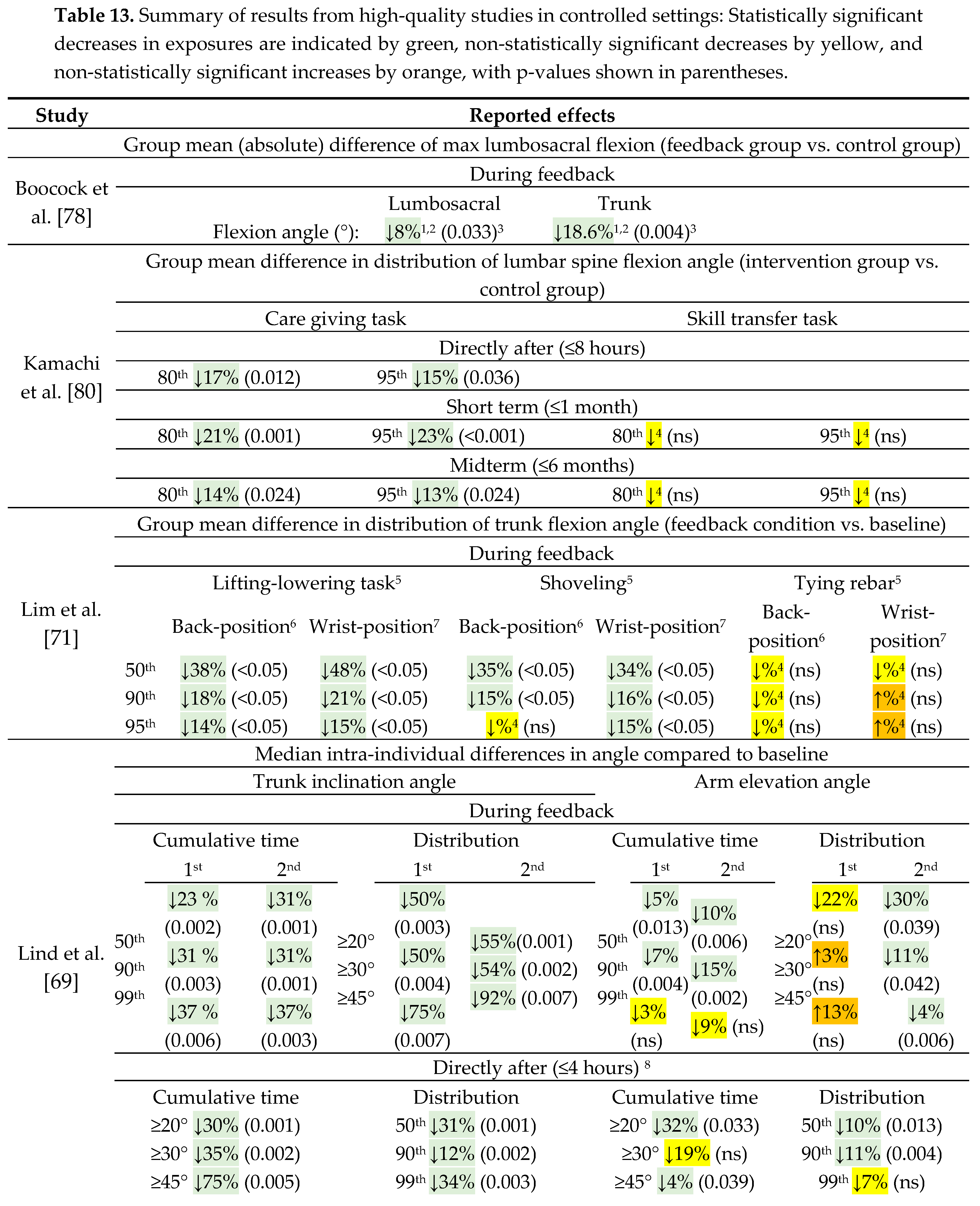
moderate-quality, are shown in Tables 13 and 14,
respectively. Additionally, a summary of the evidence is presented in Table 15.
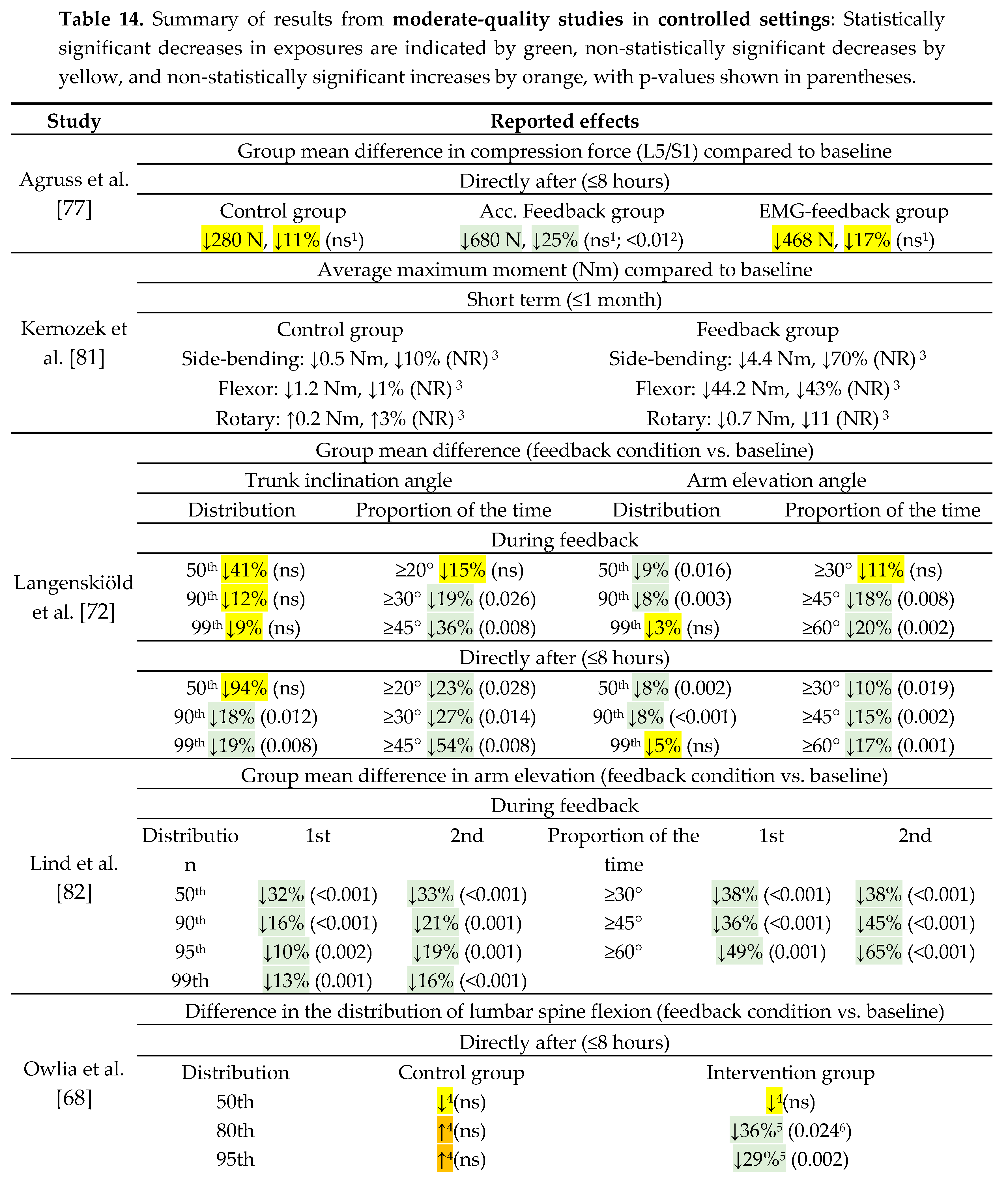
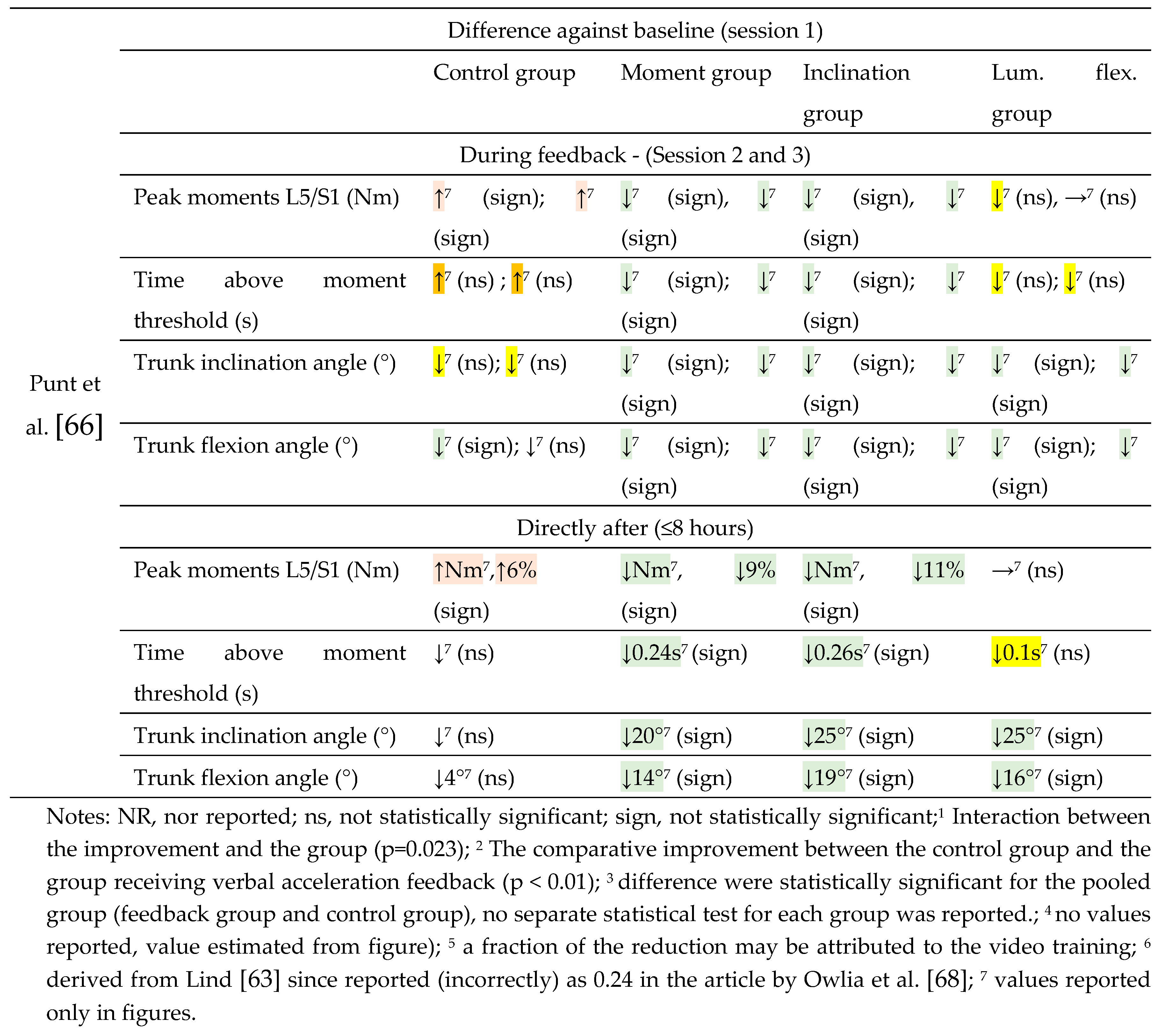
3.4.1. Effect during Feedback Administration
The effectiveness of sensor-based augmented
feedback in reducing or maintaining a reduction in biomechanical exposure in
manual handling in controlled settings during administration was evaluated in
three high-quality studies [69,71,78,83] and
three moderate-quality studies [66,72,82].
The four high-quality studies provided overall consistent, statistically
significant reductions in posture exposure, as did the three moderate-quality
studies. The effectiveness of sensor-based augmented feedback in reducing or
maintaining a reduction in biomechanical exposure during manual handling in
controlled settings was evaluated in four high-quality studies [69,71,78,83] and three moderate-quality studies [66,72,82]. The seven studies provided overall
consistent, statistically significant reductions in posture exposure. For
example, Boocock et al. [78] reported
reductions in lumbosacral flexion and trunk flexion by 8% and 18.6%,
respectively; Lind et al. [69] reported a 92%
decrease in peak trunk inclination (i.e., 99th percentile) during the second
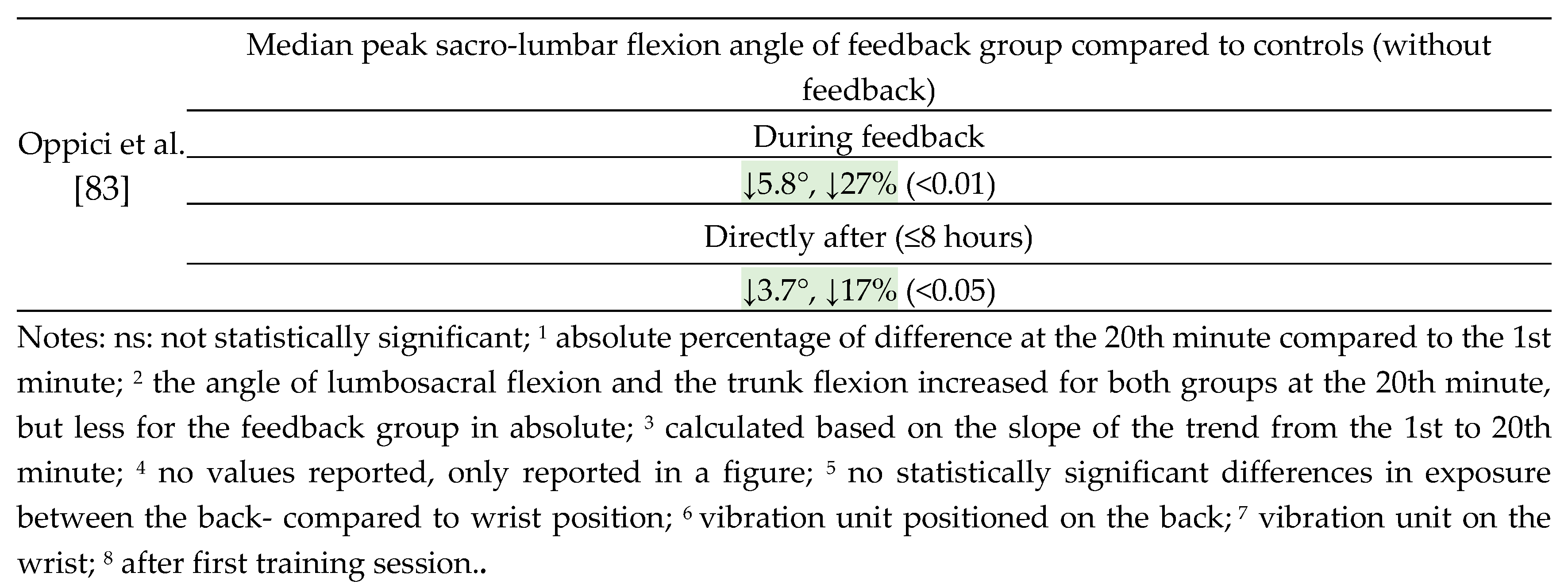
feedback session; and Oppici et al. [83]
reported a 12% reduction in peak sacro-lumbar flexion angle compared to the
baseline.
Based on this, the assessment of the current
evidence in controlled settings is that there is strong evidence supporting the
effectiveness of sensor-based augmented feedback during administration.
3.4.2. Effect Directly after Feedback Administration
The effectiveness of sensor-based augmented
feedback in reducing or maintaining a reduction in biomechanical exposure in
manual handling in controlled settings directly after being administered was
evaluated in three high-quality studies [69,80,83]
and four moderate-quality studies [66,68,72,77].
The three high-quality studies provided consistent, statistically significant
reductions in posture exposure, as did two of the moderate-quality studies. For
example, Kamachi et al. [80] reported a 15%
reduction in peak lumbar spine flexion, Lind et al. [69]
reported a 34% decrease in peak trunk inclination (i.e., 99th percentile), and
Oppici et al. [83] reported a 17% reduction in
peak sacro-lumbar flexion angle compared to the baseline. The study by Agruss
et al. [77] reported a statistically
significant 25% reduction in lumbosacral compression force for the group
receiving feedback based on acceleration and a 17% reduction tendency for the
group receiving feedback based on EMG. Owlia et al. [68]
reported a non-significant difference in median exposure (50th
percentile) of lumbar spine flexion due to feedback training, but a significant
reduction in peak exposure by 29% for the 80th percentile and 36%
for the 95th percentile.
Based on this, the assessment of the current
evidence in controlled settings is that there is strong evidence supporting the
effectiveness of sensor-based augmented feedback directly after it is
administered when considering peak exposure.
3.4.3. Retained Effects: Short and Midterm
The effectiveness of sensor-based augmented
feedback over periods of up to one and six months after administration was
evaluated in one high-quality study by Kamachi et al. [80], and over periods of up to one month after
administration in a moderate-quality study by Kernozek et al. [81]. The study by Kamachi et al. [80] presented a consistent, statistically
significant reduction in posture exposure for the manual handling tasks
included in the feedback training program. The study also assessed the
effectiveness of feedback on a task not included in the training to evaluate
the transfer of the training. For this task, a tendency of reduced exposure was
observed, but it was not statistically significant. In the study by Kernozek et
al. [81], an average decrease in exposure of
maximum spine moment (Nm) of 43% in forward flexion and 70% in lateral flexion
was observed. However, the reporting of statistical tests involved the entire
group of participants and not separately for the feedback group, making it
difficult to conclude whether these large reductions were statistically
significant.
Based on the results in the study by Kamachi et al.
[80], the assessment of the current evidence
in controlled settings is that there is limited evidence supporting the
effectiveness of sensor-based augmented feedback of periods of up to one- and
six months after administration for manual handling tasks included in the
feedback training, and no evidence for its effectiveness to transfer these
effects to more complex tasks or tasks not included in the feedback training.
3.5. Summary of the Effectiveness of Feedback in Real Work Environments and in Controlled Settings.
The summary of the consistency of the evidence for
the effectiveness of sensor-based augmented feedback on manual handling in real
work environments and controlled settings is shown in Table 15.
Table 15.
Summary of the consistency of the evidence for the effectiveness of sensor-based augmented feedback on manual handling in real work environments and controlled settings.
Table 15.
Summary of the consistency of the evidence for the effectiveness of sensor-based augmented feedback on manual handling in real work environments and controlled settings.
| Study | During feedback | Directly after (≤8 hours) | Very short term (≤1 week) | Short term (≤1 month) |
Midterm (≤6 months) | Long term (≥ 6 months) |
|---|---|---|---|---|---|---|
| Real work environments | ||||||
| Strength of Evidence |
Inconsistent | Very limited | No evidence | No evidence | No evidence | No evidence |
| High quality studies | ||||||
| Lind et al. [73] | ++ | ++ | (+)/= | (+)/= | ||
| Ribeiro et al. [70] | = | = | = | = | = | |
| Moderate quality studies | ||||||
| Bootsman et al. [79] | ++ | (+)/= | ||||
| Controlled settings | ||||||
| Strength of Evidence |
Strong | Strong4 | Limited1 / No evidence2 | Limited1 / No evidence2 | ||
| High quality studies | ||||||
| Boocock et al. [78] | ++ | |||||
| Kamachi et al. [80] | ++ | ++ 1 / = 2 | ++ 1 / = 2 | |||
| Lim et al. [71] | + | |||||
| Lind et al. [69] | ++ | ++ | ||||
| Oppici et al. [83] | ++ | ++ | ||||
| Moderate quality studies | ||||||
| Agruss et al. [77] | +/= | |||||
| Kernozek et al. [81] | * | |||||
| Langenskiöld et al. [72] | + | ++ | ||||
| Lind et al. [82] | ++ | |||||
| Owlia et al. [68] | ++ 3 /= 4 | |||||
| Punt et al. [66] | ++ / + | ++ / + | ||||
Notes: ++ overall, consistent statistically significant findings indicate that feedback reduces biomechanical exposure; + overall, statistically significant findings indicate that feedback reduces biomechanical exposure; +/= mixed results with some significant findings indicating that feedback reduces biomechanical exposure and insignificant results in one or both directions; (+)/= overall, insignificant results of a tendency indicating that feedback reduces biomechanical exposure; = overall, insignificant results in both directions; unclear = the results are unclear due to incomplete report of the statistical analysis; 1 effects based on task included in feedback training; 2 effect based on task not included in feedback training; 4 peak exposure; * unclear.
4. Discussion
4.1. General Summary of the Findings
This review adds new knowledge by synthesizing existing studies and evaluating the evidence on the effectiveness of sensor-based augmented feedback in reducing biomechanical exposure, such as posture, movements, and muscle activity, during manual handling tasks. Sixteen studies that evaluated the effectiveness of augmented feedback from sensor-based systems in reducing adverse biomechanical exposure of the upper body were identified met the inclusion criteria. Fourteen of these studies were assessed as having high or moderate methodological quality and were included in the synthesis. Reductions in methodological quality scores were most commonly due to: the lack of reporting participation rate of eligible persons, assessors not being blinded to participants' group allocation, and insufficient justification of sample size.
Eleven studies were conducted in controlled settings and three in real work environments, with 13 employing (partly or fully) a cross-sectional design. A total of 444 participants were included, with a slight majority of women, although more studies had a majority of male participants. Half of the studies involved participants in their 20s, and nine studies included novice participants either unfamiliar with the tasks or students for whom the tasks were part of their training. Handling of box-type items was the most common task (8 studies). Most studies used audio feedback (9 studies) for providing feedback, followed by vibration feedback (6 studies) and visual feedback (1 study). All studies employed corrective feedback initiated by the system, with one study also using reinforcing feedback. The effect of feedback was most commonly evaluated during its delivery phase (10 studies) and immediately afterwards (8 studies). Feedback was rarely evaluated beyond one week (4 studies) or beyond one month (2 studies). IMUs were the most commonly used sensor to trigger feedback (9 studies), while three studies used video-based motion capture systems. The studies exhibited significant heterogeneity regarding the types of exposure and tasks evaluated, feedback administration programs and modalities (e.g., type of feedback and trigger), participant experience and age, and retention periods, limiting the feasibility of meta-analysis.
Considering the current evidence for the effectiveness of work technique training to reduce adverse biomechanical exposures in work-related manual handling utilizing sensor-based augmented feedback. When the feedback was evaluated on tasks performed in real work environments, the evidence for its effectiveness was considered to be inconsistent and very limited directly after administration. For longer periods after administration, ranging from one week to more than six months, there was no evidence demonstrating the effectiveness of the feedback. In controlled settings, there was strong evidence for its effectiveness during and immediately after administration, and limited evidence for effectiveness up to six months post-administration when considering the tasks included in the training.
4.2. General Interpretation of the Results
Compared to the recent reviews by Lind [63] and Lee et al. [65], which have partly overlapping scopes, this study includes five and twelve previously unreviewed studies for the assessment of methodological quality. Of these, four and eleven studies were incorporated into the synthesis of evidence for the effectiveness of augmented feedback. Additionally, five and nine studies assessed by Lind [63] and Lee et al. [65] for methodological quality did not meet the inclusion criteria of the current study due to differences in scope. The evidence in the current review for the effectiveness of sensor-based augmented feedback to reduce biomechanical load in work-related tasks ranges from no evidence to strong evidence, depending on the time frame when the feedback was last provided (i.e., during feedback administration – to more than six months after feedback administration) and the setting where the study was conducted (real work environment versus controlled setting). This finding contrasts with Lee et al. [65], who concluded that the evidence was limited for sensor-based augmented feedback in reducing biomechanical load related to the postures of the spine and arms. The results of the current review highlight the added value of synthesizing literature separately in terms of time frame and setting, allowing for a more granular assessment facilitating the identification of research gaps.
Compared to Lind's review [63], which exclusively targeted motion-based ambulatory systems but also included sedentary tasks such as computer work, the assessment of the strength of evidence mostly overlaps, except for two assessments. First, regarding the evidence for the effectiveness of feedback in real work environments for the time frame between one and six months (midterm), Lind [63] concluded that the evidence was inconsistent. In contrast, the current review found no evidence of its effectiveness. This difference can be attributed to the exclusion of a study by Bazazan et al. [56] that involved control room tasks. Second, the evidence for the effectiveness of feedback in controlled settings directly after its administration (within 8 hours) was graded as moderate to high by Lind [63]. In contrast, the current review graded this evidence as strong and the different grading was attributed the studies by Oppici et al. [83] and Punt et al. [66].
4.2.1. Feedback Modalities and Sensors
The most common feedback modalities were auditory (9 studies) and vibration (6 studies), aligning with previous reviews by Lind [63] and Figueira et al. [50]. In contrast, Lee et al. [65] reported that visual and/or vibrotactile feedback was most frequently used.
IMUs were the most common source of input for augmented feedback, corresponding with the findings of Lind [63], but contrary to Lee et al. [65], where tri-axial accelerometers (without IMUs) were used in the majority of the studies. In the current review, tri-axial accelerometers (without IMUs) were only used in one study. The second most common sources were optical (video-camera) motion capture systems (3 studies, 21%), which contrasts with the review by Lind [63], who focused exclusively on ambulatory systems. Notably, only one of the included studies used sEMG as a source to trigger the feedback.
In most of the studies, the feedback was based on posture. Interestingly, velocity was less frequently used as input, especially in the ambulatory systems, despite the association between angular velocity of body segments and MSDs [85,86,87,88,89]. Recently, quantitative threshold levels based on the angular velocity of the wrist and arms have been proposed [90] offering potential as trigger points for augmented feedback in future systems. It should be noted that the threshold levels stressed are based on accelerometers, and the data need to be adjusted when using other types of sensors [91,92], for which there are some available conversion equations [93].
4.3. Limitations
4.3.1. Limitations of the Evidence
Several aspects need to be considered when interpreting the results of this review. Firstly, the evidence of the effectiveness of sensor-based augmented feedback was based on studies evaluating its effectiveness in isolation from other training strategies, such as instruction from an instructor. In practical use, some may instead use sensor-based feedback combined with guidance of an instructor.
The effectiveness of using an instructor has been reviewed by others [62], and in a few studies, it has been combined with sensor-based augmented feedback [94,95,96]. These latter studies were read in full but excluded from the current review, as it was judged that the instructor could have significantly impacted the results, and the effect of the sensor-based augmented feedback was not analyzed separately from the effect of the instructor. While the effectiveness of augmented feedback may increase when combined with instructor training, this is beyond the scope of the current review. The current literature on the effectiveness of sensor-based augmented feedback combined with instructor training in work-related tasks (such as manual handling) appears to be limited, as only three sources were identified, comprising a total of two studies [94,95,96], with only one study conducted in the last 20 years (i.e., Doss et al. [96]).
The interpretation of the strength of the evidence needs to consider the methodology used to grade it, which includes both the assessment of methodological quality and the criteria for grading the strength of the evidence. Notably, unlike some other approaches (e.g., [97]), studies with a non-RCT design could still fulfill the requirements for high methodological quality. Different grading systems, such as GARDE and other [98,99], may produce diverging results.
Compared to a recent rapid review on the effectiveness of augmented feedback in reducing adverse biomechanical exposure [63], the current review expanded its scope to include not only ambulatory systems but also non-ambulatory systems. This resulted in the inclusion of several additional studies that provided feedback from input via video-based motion capture systems. While the equipment used in these studies are mainly limited to research laboratory settings, the type of feedback evaluated can in principle be transferable to real work environments using more affordable video-based motion capture systems [100] or e.g., IMUs [47].
A strength of the current review, compared to previous reviews, is the focus on one category of tasks, namely manual handling, rather than mixing heterogeneous tasks. Still, the manual handling tasks evaluated differs considerably between studies such as in task complexity but potentially also inherent potential for improvements attribute due to constraints in the environment.
It should be emphasized that the evidence for the effectiveness of sensor-based augmented feedback refers specifically to its potential to reduce certain biomechanical exposures in a limited range of manual handling tasks. The results are constrained by their current applications, including specific training programs, types of feedback, and contexts. This effectiveness may not directly translate to most other manual handling tasks or contexts where the potential for reduced exposure through altered work techniques may be limited. Therefore, generalizing the results beyond these specific conditions is not supported by the current evidence, and the results should be interpreted with these limitations in mind.
The assessment of the evidence for the effectiveness of feedback is predominantly limited to the spine (excluding the cervical section). Therefore, the evidence of the effectiveness of feedback on individual body regions is outside the scope of this review.
The evaluation of the effectiveness of sensor-based augmented feedback training in this review was limited to short-term outcomes such as indirect (or partly direct) indicators of biomechanical load, including predicted lumbar spine compression force, lumbar spine moment, and postural angles (inclination, elevation, and flexion) of the spine or arms. While all of these factors have been associated with an increased risk of WMSDs [7,10,11,12,13,14,15,16,17,18,19,20,21,22,27,101,102,103,104,105], multiple task factors interact. Therefore, direct connections between the feedback trigger and risk of WMSDs should be interpreted with caution, and studies are needed to assess the effectiveness of sensor-based augmented feedback training on longer-term health outcomes such as WMSDs. As discussed by Lind [63], sensor-based feedback training often targets a reduction in exposure in one body region, which sometimes results in sub-optimal compensatory strategies where exposure is increased in other body regions, as observed by Lind et al. [82]. Examples of other negative side effects of augmented feedback include potential increased cognitive load [106].
4.3.2. Limitations of the Review Processes
A rapid review methodology was followed; therefore, the process is less rigorous than that of systematic literature reviews. Rapid reviews have, however, a quicker review process, allowing the inclusion of more recent literature at the time of publication. The guideline for rapid reviews by Cochrane Rapid Reviews Methods Group [74] was followed, but with some deviations.
Two databases were used instead of the recommended three, and a single researcher performed the full screening of all titles and abstracts, instead of two researchers screening 20%. Additionally, one reviewer, instead of two, screened the full-text articles for inclusion. The database search was restricted to articles published between January 1, 2020, and June 9, 2024. Articles published prior to 2020 were instead identified through 11 reviews/overviews, including five labeled as systematic literature reviews, five as reviews (scoping, narrative, or rapid), and one being an overview.
Given the large number of sources with overlapping scopes it seems unlikely that a significant number of relevant studies were missed, although it cannot be entirely assured that one or a few relevant studies were not identified. Similar to a previous rapid review employing a similar mixed approach [63], the current rapid review identified several sources not included in several previous systematic reviews (e.g., [49,50,60,61,62,65]), highlighting the added value of combining multiple approaches in the literature search.
Furthermore, as per the Cochrane guidelines, the methodological quality assessment was performed by one reviewer, but this assessment was not verified by a second reviewer. The thresholds for methodological quality were the same as those used in the previous mentioned rapid review [63], which were more conservative than some previous reviews, where 33% of the methodological quality score was set as the threshold for moderate quality and 66% for high quality [107,108]. While there is no consensus on the most suitable thresholds, it was assumed that studies fulfilling only 1/3 of the methodological criteria could introduce too many biases, increasing the probability of both type-I and type-II errors. For this reason as well, studies assessed as having low methodological quality were excluded from the final analysis of the effectiveness of augmented feedback.
Additionally, contrary to some previous reviews (e.g., [65]), a restriction was set to exclude studies with fewer than eight participants per group unless they provided a power calculation justifying the sample size. This led to the exclusion of several studies (e.g., [109,110,111,112,113,114,115]). It cannot be ruled out that the exclusion of studies with a low sample size (not supported by power calculations including studies having low methodological quality) could have influenced the grading of evidence, by potentially introducing a type-II error due to low statistical power. Conference papers (including conference abstracts) were also excluded (e.g., [109,110,116,117,118]) due to the often less rigorous peer-review process compared to scientific peer-reviewed journal articles.
4.4. Practical Implications and Future Research
This review identified several common methodological shortcomings that should be addressed to improve the quality of future evaluations on the effectiveness of sensor-based augmented feedback. The most frequently identified issues that reduced methodological quality scores were: lack of reporting participation rates of eligible persons, assessors not being blinded to participants' group allocation, and insufficient justification of sample size. Other common issues included insufficient control of confounders and independent variables, particularly the work output per time unit, which was not always controlled or reported. While blinding assessors to participants' group allocation might be less feasible, performing power calculations should be achievable, preferably based on pilot tests where the magnitude of changed exposure is estimated. Otherwise, the sources provided in the current review may be used as an alternative approach to make rough estimation of the needed sample size. Notably, even larger sample sizes may be required when comparing the effects of two or more feedback characteristics, as evaluated by Langenskiöld et al. [72] Lim et al. [71] and Punt et al. [66] and Agruss et al. [77].
Controlling work output per time unit is crucial, as it is otherwise difficult to evaluate potential differences in exposure attributed to the feedback. For example, in Ribeiro et al.'s RCT study [70], the work output per time unit was not reported, and large variations in exposure during the study period were reported for the control group as well.
If the variability in exposure differs considerably across workdays and sessional over the year, it might be difficult to assess potential changes in exposure attributed to the feedback if work output per time unit is not controlled. This challenge is especially significant when evaluating interventions in real work contexts of non-standardized tasks. Therefore, future studies should consider various strategies to estimate work output, e.g., as done by Lind et al. [73] were the participants rated their work output compared to a normal workday, or (preferably) using reliable objective data at the individual level if available.
While this review focused on the effectiveness of sensor-derived augmented feedback in manual handling, multiple studies have focused on sedentary tasks, predominantly computer work [51,52,53,54,55,56,57,58,119,120] and odontology tasks [121,122,123,124]. Due to differences in activities compared to manual handling, the evidence for the effectiveness of augmented feedback from the current review cannot easily be transferred to such tasks. Therefore, future reviews are needed to synthesize its effectiveness in sedentary and predominantly static tasks such as computer work.
Future research should also explore how to optimize sensor-based augmented feedback, including which feedback types are most effective (e.g., modality: auditory, vibration, or visual; timing: concurrent, terminal, or fading). While some included studies targeted such comparisons, their number was too few and heterogeneous to draw conclusions or lacked statistical power (e.g., Langenskiöld et al. [72]).
Besides sensor feedback, tactile feedback from non-technical equipment such as athletic- or kinesio tapes [83,125,126,127] and dowels [128] has been used to reduce adverse spine posture in lifting. Studies indicate these methods have potential in reducing biomechanical exposure and retaining improvements, at least in the short term. For instance, the effectiveness of tactile feedback from sport leukotape was compared against concurrent sensor-based audio feedback, showing similar decreases in biomechanical exposures [83]. Therefore, future reviews should compare sensor-based feedback to other available sources of feedback.
The current review exclusively targeted sensor-based augmented feedback to improve biomechanical exposures in manual handling. Consequently, some otherwise relevant studies that combined augmented feedback from motion capture sensors or EMG were excluded, such as those by Lavender et al. [94,95] and Doss et al. [96], because they also used an instructor to guide the trainee and did not provide a separate analysis of the sensor-based feedback effect. Future reviews are needed to evaluate the potential added value of sensor-based feedback training assisted by an instructor in manual handling.
The potential effectiveness of sensor-based augmented feedback training is likely much lower compared to other measures aligned with the hierarchy of controls [47,129], such as engineering controls and organizational measures, which are generally more effective. Therefore, sensor-based augmented feedback training should not be used as the only measure to mitigate WMSDs, but should (at best) be seen as a complementary strategy to other risk reducing measures. Given indications of altered postural strategies and increased cognitive load due to augmented feedback, future efforts should focus on closely monitoring potential side effects, such as the transfer of load to other body parts and changes in cognitive exposure. Identifying task and work contexts where augmented feedback has the greatest potential to reduce adverse exposure, and where it may be less effective or infeasible, is also important. Additional barriers to implementation may include usability issues, such as ease of use and technology durability [30,130,131,132].
Only a limited number of studies have been performed in real work environments and evaluated the feedback with follow-up periods longer than 8 hours. Therefore, there is a need to evaluate the effectiveness of sensor-based augmented feedback in real work environments over several days, weeks and months. This information may contribute to much-needed knowledge about the optimum intervals for feedback training repetition. There is also a need for studies evaluating health effects, including MSDs and work-disabling conditions, in addition to short-term biomechanical exposures.
While there is strong evidence for the effectiveness of sensor-based augmented feedback in reducing exposure in manual handling during and directly after administration in controlled settings, the long-term effects as well effectiveness in real work environments remain largely unexplored. This limits the recommendation for sensor-based augmented feedback as a risk-reducing measure in work-related manual handling. Consequently, more research is warranted to assess its potential in reducing biomechanical exposure and work-related musculoskeletal disorders (WMSDs) in manual handling.
5. Conclusions
In this rapid review, the current evidence for the effectiveness of work technique training to reduce adverse biomechanical exposures in work-related manual handling utilizing sensor-based augmented feedback was assessed. Sixteen studies meeting the inclusion criteria for assessment of methodological quality were identified, of which seven were assessed as having high methodological quality and seven as having moderate methodological quality, and these were included in the synthesis of the evidence. The most frequent reasons for reductions in methodological quality scores were the lack of reporting participation rate of eligible persons, assessors not being blinded to participants' group allocation, and insufficient justification of sample size. Of the 14 included studies, three were conducted in real work environments and eleven in controlled settings. Most studies used auditory feedback (n = 9), followed by vibration feedback (n = 6). All studies evaluated corrective feedback initiated by the system, whereas reinforcing feedback was additionally evaluated in one study.
In real work environments, the current evidence for the effectiveness of sensor-based augmented feedback in reducing biomechanical exposure during administration is considered inconsistent and very limited directly after administration. For longer periods after administration, ranging from one week to more than six months, there is currently no evidence demonstrating the effectiveness of the feedback.
In controlled settings, there is strong evidence for its effectiveness during and immediately after administration, and limited evidence for effectiveness up to six months post-administration when considering the tasks included in the training. When considering the ability to transfer the reduced exposures following feedback training to other tasks, there is no evidence demonstrating its effectiveness.
The existing literature on the retained effects of work technique training using sensor-based augmented feedback to reduce adverse biomechanical exposures in work-related manual handling over periods extending beyond a workday is limited. This scarcity restricts recommendations for or against its use as a measure to mitigate adverse biomechanical exposures in work-related manual handling. Consequently, the publication of new research could potentially alter the grading of evidence for its effectiveness, particularly studies conducted in real work contexts of short- and long-term, but also short and long-term studies in controlled settings. To improve the methodological quality of future studies, it is essential to address the identified gaps in reporting or performing power calculations, and reporting of participation rates. Additionally, when feasible, blinding of assessors to participants' group allocation should be implemented. Given the limited comparison of different feedback modalities and feedback training programs, research evaluating the effectiveness of various feedback modalities and training programs is also identified as an important research gap to address.
Funding
This research was funded by AFA Insurance (Afa Försäkring), grant numbers 180098 and 180254.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable. Database searches were conducted only for this review.
Conflicts of Interest
The author declares no conflicts of interest.
Appendix A. Search Strings in the Literature Search
Table A1.
The search strings used in Medline on 9 June 2024.
| "feedback" OR "biofeedback" AND “posture$” OR “postural” OR “movement$” OR “muscle activity” OR “EMG” AND “neck” OR “trunk” OR “spine” OR "back" OR “arm$” or “wrist$” OR “hand$” The following terms were excluded “gait”, “child*”, “rehab*”, “parkinson”, “stroke*”, “cerebral palsy”, “spinal cord injury”, “prosthesis”, and “therap*”. The first two search strings were applied “all fields” while the third as well the exclusion were applied to the abstract. Articles in other language than English was excluded. The search covered the period 2020-01-01 to 2024-06-09. |
Table A2.
The search strings used in Web of Science on 9 June 2024.
| "feedback" OR "biofeedback" AND “posture$” OR “postural” OR “movement$” OR “muscle activity” OR “EMG” AND “neck” OR “trunk” OR “spine” OR "upper back" OR "lower back" OR “arm$” or “wrist$” OR “hand$” The following terms were excluded: “gait”, “child”, “rehab”, “parkinson”, “stroke*”, “cerebral palsy”, “spinal cord injury”, “prosthesis”, “therap*”. The search terms were applied to the abstract. Review articles were excluded. Articles in other language than English was excluded. The search covered the period 2020-01-01 to 2024-06-09. |
Appendix B. The Criteria to Assess the Methodological Quality
Table B1. Criteria for assessing the methodological quality of observational cohort and cross-sectional studies.
| Item | Criteria |
| 1. Clear research question | Clearly stated research question or study objective including a description of the outcome (dependent variable) |
| 2. Clear study population | Clearly defined study population and inclusion/exclusion criteria, and consistently applied inclusion/exclusion criteria |
| 3. Participation rate | Participation rate ≥50% of eligible persons of the identified pool of eligible persons |
| 4. Subjects recruitment | Subjects recruited from the same/similar populations, with uniformly applied inclusion/exclusion criteria |
| 5. Justified sample size | Sample size sufficiently justified, and large enough to detect difference in the outcome with at least 80% power |
| 6. Temporality of exposure(s) and outcome(s) | Exposure(s) measured before outcome(s) |
| 7. Sufficient time | Timeframe for feedback described and sufficient long to induce behavioral changes |
| 8. Dependent variable scaling | Dependent variable (e.g., posture, movements or muscle activity) assessed on a continuous or categorical scale |
| 9. Independent variables treatment | Relevant independent variables controlled or measured (as minimum. the amount of work performed per time unit, and clearly defined and consistently implemented feedback trigger) |
| 10. Assessment of dependent variable | Dependent variable(s) assessed more than one time |
| 11.Assessment of dependent variable | Dependent variable clearly defined and adequately assessed |
| 12. Blinding | Assessors blinded to the participants' group allocation |
| 13. Loss to follow-up | Data from at least 80% of participants were included in the final analysis |
| 14. Control of confounders | Key confounding variables that could alter the outcome results were adjusted for |
Table B2. Criteria for assessing the methodological quality of controlled intervention studies.
| Item | Criteria |
| 1. Study description | Study described as a randomized controlled trial and provides adequate details of the study design |
| 2. Randomization | Suitable randomization was employed, such as computer-generated random allocation of participants |
| 3. Concealed allocation | Concealed process of assigning participants to group allocation |
| 4. Blinding (providers and participants) | Blinding (group assignment) of both administrator of the intervention and the participants receiving the intervention |
| 5. Blinding (assessors) | Blinding of assessors evaluating outcomes to participants' group allocation |
| 6. Baseline characteristics | Baseline characteristics reported and balanced between groups, such as age, gender, experience, occupation, job exposure, and disorders |
| 7. Endpoint dropout | The dropout rate ≤20% at the end of the study for each group |
| 8. Endpoint dropout (between groups) | Dropout rate ≤15% between groups at the end of the study |
| 9. Adherence | Adherence to the intervention protocol by participants in all group |
| 10. Confounding interventions | No additional interventions that could confound the study results were occurring, or any such interventions were similar between groups |
| 11. Quality of outcomes assessment | Dependent variable(s) measured using accurate and precise tools/methods |
| 12. Justified sample size | Sample size sufficiently justified, and large enough to detect difference in the outcome between groups with at least 80% power |
| 13. Prespecified analysis | Predetermined analysis of the outcomes |
| 14. Group assignment | Participants analyzed based on their original group allocation |
References
- WHO. Musculoskeletal health. Availabe online: https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions. (accessed on 23 November 2022).
- Kassebaum, N.J.; Arora, M.; Barber, R.M.; Bhutta, Z.A.; Brown, J.; Carter, A.; Casey, D.C.; Charlson, F.J.; Coates, M.M.; Coggeshall, M. , et al. Global, regional, and national disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. The Lancet 2016, 388, 1603–1658. [Google Scholar] [CrossRef]
- Tompa, E.; Mofidi, A.; van den Heuvel, S.; van Bree, T.; Michaelsen, F.; Jung, Y.; Porsch, L.; van Emmerik, M. The value of occupational safety and health and the societal costs of work-related injuries and diseases; Publications Office of the European Union: Luxembourg (LU), 2019. [Google Scholar] [CrossRef]
- Sundstrup, E.; Andersen, L.L. Joint association of physical and psychosocial working conditions with risk of long-term sickness absence: Prospective cohort study with register follow-up. Scand J Public Health 2021, 49, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, J.; Bjorner, J.B.; Andersen, L.L. Physical work demands and expected labor market affiliation (ELMA): Prospective cohort with register-follow-up among 46 169 employees. Scand J Work Environ Health 2022, 48, 641–650. [Google Scholar] [CrossRef]
- Badarin, K.; Hemmingsson, T.; Hillert, L.; Kjellberg, K. The impact of musculoskeletal pain and strenuous work on self-reported physical work ability: a cohort study of Swedish men and women. Int Arch Occup Environ Health 2022, 95, 939–952. [Google Scholar] [CrossRef] [PubMed]
- NRC. Musculoskeletal disorders and the workplace: low back and upper extremities; National Academies Press: Washington (DC), 2001. [Google Scholar]
- Widanarko, B.; Legg, S.; Devereux, J.; Stevenson, M. The combined effect of physical, psychosocial/organisational and/or environmental risk factors on the presence of work-related musculoskeletal symptoms and its consequences. Appl Ergon 2014, 45, 1610–1621. [Google Scholar] [CrossRef] [PubMed]
- Hauke, A.; Flintrop, J.; Brun, E.; Rugulies, R. The impact of work-related psychosocial stressors on the onset of musculoskeletal disorders in specific body regions: A review and metaanalysis of 54 longitudinal studies. Work Stress 2011, 25, 243–256. [Google Scholar] [CrossRef]
- NIOSH. Musculoskeletal Disorders and Workplace Factors.; National Institute for Occupational Safety and Health: Cincinnati, 1997. [Google Scholar]
- van Rijn, R.M.; Huisstede, B.M.; Koes, B.W.; Burdorf, A. Associations between work-related factors and the carpal tunnel syndrome--a systematic review. Scand J Work Environ Health 2009, 35, 19–36. [Google Scholar] [CrossRef]
- da Costa, B.R.; Vieira, E.R. Risk factors for work-related musculoskeletal disorders: A systematic review of recent longitudinal studies. Am J Ind Med 2010, 53, 285–323. [Google Scholar] [CrossRef]
- Garg, A.; Boda, S.; Hegmann, K.T.; Moore, J.S.; Kapellusch, J.M.; Bhoyar, P.; Thiese, M.S.; Merryweather, A.; Deckow-Schaefer, G.; Bloswick, D. , et al. The NIOSH lifting equation and low-back pain, part 1: Association with low-back pain in the BackWorks prospective cohort study. Hum Factors 2014, 56, 6–28. [Google Scholar] [CrossRef]
- Garg, A.; Kapellusch, J.M.; Hegmann, K.T.; Moore, J.S.; Boda, S.; Bhoyar, P.; Thiese, M.S.; Merryweather, A.; Deckow-Schaefer, G.; Bloswick, D. , et al. The NIOSH lifting equation and low-back pain, Part 2: Association with seeking care in the backworks prospective cohort study. Hum Factors 2014, 56, 44–57. [Google Scholar] [CrossRef]
- Hoozemans, M.J.; Knelange, E.B.; Frings-Dresen, M.H.; Veeger, H.E.; Kuijer, P.P. Are pushing and pulling work-related risk factors for upper extremity symptoms? A systematic review of observational studies. Occup Environ Med 2014, 71, 788–795. [Google Scholar] [CrossRef] [PubMed]
- Kozak, A.; Schedlbauer, G.; Wirth, T.; Euler, U.; Westermann, C.; Nienhaus, A. Association between work-related biomechanical risk factors and the occurrence of carpal tunnel syndrome: An overview of systematic reviews and a meta-analysis of current research. BMC Musculoskelet Disord 2015, 16. [Google Scholar] [CrossRef] [PubMed]
- Fox, R.R.; Lu, M.L.; Occhipinti, E.; Jaeger, M. Understanding outcome metrics of the revised NIOSH lifting equation. Appl Ergon 2019, 81, 102897. [Google Scholar] [CrossRef]
- Jahn, A.; Andersen, J.H.; Christiansen, D.H.; Seidler, A.; Dalbøge, A. Occupational mechanical exposures as risk factor for chronic low-back pain: a systematic review and meta-analysis. Scand J Work Environ Health 2023, 49, 453–465. [Google Scholar] [CrossRef]
- Hoogendoorn, W.E.; Bongers, P.M.; de Vet, H.C.; Douwes, M.; Koes, B.W.; Miedema, M.C.; Ariëns, G.A.; Bouter, L.M. Flexion and rotation of the trunk and lifting at work are risk factors for low back pain: results of a prospective cohort study. Spine (Phila Pa 1976) 2000, 25, 3087–3092. [Google Scholar] [CrossRef]
- Gupta, N.; Bjerregaard, S.S.; Yang, L.; Forsman, M.; Rasmussen, C.L.; Rasmussen, C.D.N.; Clays, E.; Holtermann, A. Does occupational forward bending of the back increase long-term sickness absence risk? A 4-year prospective register-based study using device-measured compositional data analysis. Scand J Work Environ Health 2022, 48, 651–661. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Rasmussen, C.L.; Forsman, M.; Søgaard, K.; Holtermann, A. How does accelerometry-measured arm elevation at work influence prospective risk of long-term sickness absence? Scand J Work Environ Health 2022, 48, 137–147. [Google Scholar] [CrossRef]
- Versloot, A.H.C.; Jackson, J.A.; van Rijn, R.M.; Elbers, R.G.; Søgaard, K.; Macri, E.M.; Koes, B.; Burdorf, A.; Chiarotto, A.; Gerger, H. Physical and psychosocial work-related exposures and the occurrence of disorders of the shoulder: A systematic review update. Appl Ergon 2024, 118, 104277. [Google Scholar] [CrossRef]
- Nilsson, T.; Wahlström, J.; Burström, L. Hand-arm vibration and the risk of vascular and neurological diseases-A systematic review and meta-analysis. PLoS One 2017, 12, e0180795. [Google Scholar] [CrossRef]
- Burström, L.; Nilsson, T.; Wahlström, J. Whole-body vibration and the risk of low back pain and sciatica: a systematic review and meta-analysis. Int Arch Occup Environ Health 2015, 88, 403–418. [Google Scholar] [CrossRef]
- Lind, C.M.; Rose, L.M. Shifting to proactive risk management: Risk communication using the RAMP tool. Agron Res 2016, 14, 513–524. [Google Scholar]
- Lind, C.M.; Forsman, M.; Rose, L.M. Development and evaluation of RAMP I - a practitioner's tool for screening of musculoskeletal disorder risk factors in manual handling. Int J Occup Saf Ergon 2019, 25, 165–180. [Google Scholar] [CrossRef]
- Lind, C.M.; Forsman, M.; Rose, L.M. Development and evaluation of RAMP II - a practitioner’s tool for assessing musculoskeletal disorder risk factors in industrial manual handling. Ergonomics 2020, 63, 477–504. [Google Scholar] [CrossRef]
- Macdonald, W.; Oakman, J. The problem with "ergonomics injuries": What can ergonomists do? Appl Ergon 2022, 103, 103774. [Google Scholar] [CrossRef] [PubMed]
- Rose, L.M.; Eklund, J.; Nord Nilsson, L.; Barman, L.; Lind, C.M. The RAMP package for MSD risk management in manual handling – A freely accessible tool, with website and training courses. Appl Ergon 2020, 86, 103101. [Google Scholar] [CrossRef]
- Eliasson, K.; Lind, C.M.; Nyman, T. Factors influencing ergonomists' use of observation-based risk-assessment tools. Work 2019, 64, 93–106. [Google Scholar] [CrossRef] [PubMed]
- Abdul Halim, N.S.S.; Ripin, Z.M.; Ridzwan, M.I.Z. Effects of patient transfer devices on the risk of work-related musculoskeletal disorders: a systematic review. Int J Occup Saf Ergon 2023, 29, 494–514. [Google Scholar] [CrossRef] [PubMed]
- van der Molen, H.F.; Sluiter, J.K.; Hulshof, C.T.; Vink, P.; Frings-Dresen, M.H. Effectiveness of measures and implementation strategies in reducing physical work demands due to manual handling at work. Scand J Work Environ Health 2005, 31 Suppl 2, 75–87. [Google Scholar]
- Marras, W.S.; Allread, W.G.; Burr, D.L.; Fathallah, F.A. Prospective validation of a low-back disorder risk model and assessment of ergonomic interventions associated with manual materials handling tasks. Ergonomics 2000, 43, 1866–1886. [Google Scholar] [CrossRef]
- Zare, M.; Black, N.; Sagot, J.-C.; Hunault, G.; Roquelaure, Y. Ergonomics interventions to reduce musculoskeletal risk factors in a truck manufacturing plant. Int J Ind Ergon 2020, 75, 102896. [Google Scholar] [CrossRef]
- Hoe, V.C.; Urquhart, D.M.; Kelsall, H.L.; Sim, M.R. Ergonomic design and training for preventing work-related musculoskeletal disorders of the upper limb and neck in adults. Cochrane Database Syst Rev 2012, 2012, Cd008570. [Google Scholar] [CrossRef]
- Ouellet, S.; Vézina, N. Work training and MSDs prevention: Contribution of ergonomics. Int J Ind Ergon 2014, 44, 24–31. [Google Scholar] [CrossRef]
- Denis, D.; St-Vincent, M.; Imbeau, D.; Jetté, C.; Nastasia, I. Intervention practices in musculoskeletal disorder prevention: a critical literature review. Appl Ergon 2008, 39, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Denis, D.; Gonella, M.; Comeau, M.; Lauzier, M. Questioning the value of manual material handling training: a scoping and critical literature review. Appl Ergon 2020, 89, 103186. [Google Scholar] [CrossRef] [PubMed]
- EU. Council Directive 90/269/EEC of 29 May 1990 on the minimum health and safety requirements for the manual handling of loads where there is a risk particularly of back injury to workers.; Publications Office of the European Union: Luxemburg (LU), 1990. [Google Scholar]
- McGill, S.M. Evolving ergonomics? Ergonomics 2009, 52, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Plamondon, A.; Denis, D.; Delisle, A.; Lariviere, C.; Salazar, E. Biomechanical differences between expert and novice workers in a manual material handling task. Ergonomics 2010, 53, 1239–1253. [Google Scholar] [CrossRef]
- Marras, W.S.; Walter, B.A.; Purmessur, D.; Mageswaran, P.; Wiet, M.G. The Contribution of Biomechanical-Biological Interactions of the Spine to Low Back Pain. Hum Factors 2016, 58, 965–975. [Google Scholar] [CrossRef]
- Kumar, S. Ergonomics and biology of spinal rotation. Ergonomics 2004, 47, 370–415. [Google Scholar] [CrossRef]
- Clemes, S.A.; Haslam, C.O.; Haslam, R.A. What constitutes effective manual handling training? A systematic review. Occup Med (Lond) 2010, 60, 101–107. [Google Scholar] [CrossRef]
- Verbeek, J.H.; Martimo, K.P.; Karppinen, J.; Kuijer, P.P.; Viikari-Juntura, E.; Takala, E.P. Manual material handling advice and assistive devices for preventing and treating back pain in workers. Cochrane Database Syst Rev 2011. [Google Scholar] [CrossRef]
- Hogan, D.A.; Greiner, B.A.; O'Sullivan, L. The effect of manual handling training on achieving training transfer, employee's behaviour change and subsequent reduction of work-related musculoskeletal disorders: a systematic review. Ergonomics 2014, 57, 93–107. [Google Scholar] [CrossRef]
- Lind, C.M.; Abtahi, F.; Forsman, M. Wearable Motion Capture Devices for the Prevention of Work-Related Musculoskeletal Disorders in Ergonomics-An Overview of Current Applications, Challenges, and Future Opportunities. Sensors (Basel) 2023, 23. [Google Scholar] [CrossRef] [PubMed]
- Ranavolo, A.; Draicchio, F.; Varrecchia, T.; Silvetti, A.; Iavicoli, S. Wearable monitoring devices for biomechanical risk assessment at work: Current status and future challenges-a systematic review. Int J Environ Res Public Health 2018, 15. [Google Scholar] [CrossRef] [PubMed]
- Stefana, E.; Marciano, F.; Rossi, D.; Cocca, P.; Tomasoni, G. Wearable Devices for Ergonomics: A Systematic Literature Review. Sensors (Basel) 2021, 21. [Google Scholar] [CrossRef]
- Figueira, V.; Silva, S.; Costa, I.; Campos, B.; Salgado, J.; Pinho, L.; Freitas, M.; Carvalho, P.; Marques, J.; Pinho, F. Wearables for Monitoring and Postural Feedback in the Work Context: A Scoping Review. Sensors (Basel) 2024, 24. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.E.; Vaidya, S.C.; Herrick, R.T.; Congleton, J.J. The effects of biofeedback on carpal tunnel syndrome. Ergonomics 1993, 36, 353–361. [Google Scholar] [CrossRef]
- Akamatsu, M.; MacKenzie, I.S.; Hasbroucq, T. A comparison of tactile, auditory, and visual feedback in a pointing task using a mouse-type device. Ergonomics 1995, 38, 816–827. [Google Scholar] [CrossRef]
- Faucett, J.; Garry, M.; Nadler, D.; Ettare, D. A test of two training interventions to prevent work-related musculoskeletal disorders of the upper extremity. Appl Ergon 2002, 33, 337–347. [Google Scholar] [CrossRef]
- De Kraker, H.; De Korte, E.; Van Mil, F.; Rijs, B.; Bongers, P. The effect of a feedback signal in a computer mouse on hovering behaviour, productivity, comfort and usability in a field study. Ergonomics 2008, 51, 140–155. [Google Scholar] [CrossRef]
- Lindegård, A.; Grimby-Ekman, A.; Wahlström, J.; Gustafsson, E. Can biofeedback training in combination with ergonomic information reduce pain among young adult computer users with neck and upper extremity symptoms? - A randomized controlled intervention study. Appl Ergon 2024, 114, 104155. [Google Scholar] [CrossRef]
- Bazazan, A.; Dianat, I.; Feizollahi, N.; Mombeini, Z.; Shirazi, A.M.; Castellucci, H.I. Effect of a posture correction-based intervention on musculoskeletal symptoms and fatigue among control room operators. Appl Ergon 2019, 76, 12–19. [Google Scholar] [CrossRef] [PubMed]
- King, T.K.; Severin, C.N.; Van Eerd, D.; Ibrahim, S.; Cole, D.; Amick, B., 3rd; Steenstra, I.A. A pilot randomised control trial of the effectiveness of a biofeedback mouse in reducing self-reported pain among office workers. Ergonomics 2013, 56, 59–68. [Google Scholar] [CrossRef]
- Meijer, E.M.; Sluiter, J.K.; Frings-Dresen, M.H. Effectiveness of a feedback signal in a computer mouse on upper extremity musculoskeletal symptoms: a randomised controlled trial with an 8-month follow-up. Occup Environ Med 2009, 66, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Zadeh, S.M.; MacDermid, J.; Johnson, J.; Birmingham, T.B.; Shafiee, E. Applications of wearable sensors in upper extremity MSK conditions: a scoping review. J Neuroeng Rehabil 2023, 20, 158. [Google Scholar] [CrossRef]
- Martins, D.R.; Cerqueira, S.M.; Santos, C.P. Combining inertial-based ergonomic assessment with biofeedback for posture correction: A narrative review. Comput Ind Eng 2024, 190, 110037. [Google Scholar] [CrossRef]
- García-Jaén, M.; Sebastia-Amat, S.; Sanchis-Soler, G.; Cortell-Tormo, J.M. Lumbo-Pelvic Rhythm Monitoring Using Wearable Technology with Sensory Biofeedback: A Systematic Review. Healthc Inform Res 2024, 12, 758. [Google Scholar] [CrossRef] [PubMed]
- Frasie, A.; Houry, M.; Plourde, C.; Robert, M.T.; Bouyer, L.J.; Roy, J.S. Feedback for the prevention and rehabilitation of work-related musculoskeletal disorders: A systematic review. Work 2023, 76, 61–94. [Google Scholar] [CrossRef] [PubMed]
- Lind, C.M. A Rapid Review on the Effectiveness and Use of Wearable Biofeedback Motion Capture Systems in Ergonomics to Mitigate Adverse Postures and Movements of the Upper Body. Sensors (Basel) 2024, 24, 3345. [Google Scholar] [CrossRef]
- Simpson, L.; Maharaj, M.M.; Mobbs, R.J. The role of wearables in spinal posture analysis: a systematic review. BMC Musculoskelet Disord 2019, 20, 55. [Google Scholar] [CrossRef]
- Lee, R.; James, C.; Edwards, S.; Skinner, G.; Young, J.L.; Snodgrass, S.J. Evidence for the Effectiveness of Feedback from Wearable Inertial Sensors during Work-Related Activities: A Scoping Review. Sensors (Basel) 2021, 21. [Google Scholar] [CrossRef]
- Punt, M.; Nematimoez, M.; van Dieën, J.H.; Kingma, I. Real-time feedback to reduce low-back load in lifting and lowering. J Biomech 2020, 102, 109513. [Google Scholar] [CrossRef] [PubMed]
- Brandl, C.; Brunner, O.; Marzaroli, P.; Hellig, T.; Johnen, L.; Mertens, A.; Tarabini, M.; Nitsch, V. Using real-time feedback of L5/S1 compression force based on markerless optical motion capture to improve the lifting technique in manual materials handling. Int J Ind Ergon 2022, 91, 103350. [Google Scholar] [CrossRef]
- Owlia, M.; Kamachi, M.; Dutta, T. Reducing lumbar spine flexion using real-time biofeedback during patient handling tasks. Work 2020, 66, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Lind, C.M.; Yang, L.; Abtahi, F.; Hanson, L.; Lindecrantz, K.; Lu, K.; Forsman, M.; Eklund, J. Reducing postural load in order picking through a smart workwear system using real-time vibrotactile feedback. Appl Ergon 2020, 89, 103188. [Google Scholar] [CrossRef]
- Ribeiro, D.C.; Milosavljevic, S.; Terry, J.; Abbott, J.H. Effectiveness of a lumbopelvic monitor and feedback device to change postural behaviour: the ELF cluster randomised controlled trial. Occup Environ Med 2020, 77, 462–469. [Google Scholar] [CrossRef]
- Lim, S.; Yang, X. Real-time vibrotactile feedback system for reducing trunk flexion exposure during construction tasks. Appl Ergon 2023, 110, 104019. [Google Scholar] [CrossRef]
- Langenskiöld, C.; Berg, A.; Yang, L. The Effect of Corrective and Encouraging Accumulated Vibrotactile Feedback on Work Technique Training and Motivation-A Pilot Study. Int J Environ Res Public Health 2023, 20. [Google Scholar] [CrossRef]
- Lind, C.M.; De Clercq, B.; Forsman, M.; Grootaers, A.; Verbrugghe, M.; Van Dyck, L.; Yang, L. Effectiveness and usability of real-time vibrotactile feedback training to reduce postural exposure in real manual sorting work. Ergonomics 2023, 66, 198–216. [Google Scholar] [CrossRef]
- Garritty, C.; Gartlehner, G.; Nussbaumer-Streit, B.; King, V.J.; Hamel, C.; Kamel, C.; Affengruber, L.; Stevens, A. Cochrane Rapid Reviews Methods Group offers evidence-informed guidance to conduct rapid reviews. J Clin Epidemiol 2021, 130, 13–22. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. , et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- National Heart, Lung, and Blood Institute (NHLBI), Study Quality Assessment Tools. Availabe online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools. (accessed on 20 November 2023).
- Agruss, C.D.; Williams, K.; Fathallah, F.A. The effect of feedback training on lumbosacral compression during simulated occupational lifting. Ergonomics 2004, 47, 1103–1115. [Google Scholar] [CrossRef]
- Boocock, M.; Naudé, Y.; Taylor, S.; Kilby, J.; Mawston, G. Influencing lumbar posture through real-time biofeedback and its effects on the kinematics and kinetics of a repetitive lifting task. Gait Posture 2019, 73, 93–100. [Google Scholar] [CrossRef]
- Bootsman, R.; Markopoulos, P.; Qi, Q.; Wang, Q.; Timmermans, A.A.A. Wearable technology for posture monitoring at the workplace. Int J Hum Comput Stud 2019, 132, 99–111. [Google Scholar] [CrossRef]
- Kamachi, M.; Owlia, M.; Dutta, T. Evaluating a wearable biofeedback device for reducing end-range sagittal lumbar spine flexion among home caregivers. Appl Ergon 2021, 97, 103547. [Google Scholar] [CrossRef] [PubMed]
- Kernozek, T.; Iwasaki, M.; Fater, D.; Durall, C.; Langenhorst, B. Movement-based feedback may reduce spinal moments in male workers during lift and lowering tasks. Physiother Res Int 2006, 11, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Lind, C.M.; Diaz-Olivares, J.A.; Lindecrantz, K.; Eklund, J. A Wearable Sensor System for Physical Ergonomics Interventions Using Haptic Feedback. Sensors (Basel) 2020, 20, 6010. [Google Scholar] [CrossRef] [PubMed]
- Oppici, L.; Grütters, K.; Garofolini, A.; Rosenkranz, R.; Narciss, S. Deliberate Practice and Motor Learning Principles to Underpin the Design of Training Interventions for Improving Lifting Movement in the Occupational Sector: A Perspective and a Pilot Study on the Role of Augmented Feedback. Frontiers in sports and active living 2021, 3, 746142. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, D.C.; Sole, G.; Abbott, J.H.; Milosavljevic, S. The effectiveness of a lumbopelvic monitor and feedback device to change postural behavior: a feasibility randomized controlled trial. J Orthop Sports Phys Ther 2014, 44, 702–711. [Google Scholar] [CrossRef]
- Marras, W.S.; Schoenmarclin, R.W. Wrist motions in industry. Ergonomics 1993, 36, 341–351. [Google Scholar] [CrossRef]
- Marras, W.S.; Lavender, S.A.; Leurgans, S.E.; Rajulu, S.L.; Allread, W.G.; Fathallah, F.A.; Ferguson, S.A. The role of dynamic three-dimensional trunk motion in occupationally-related low back disorders. The effects of workplace factors, trunk position, and trunk motion characteristics on risk of injury. Spine (Phila Pa 1976) 1993, 18, 617–628. [Google Scholar] [CrossRef]
- Nordander, C.; Ohlsson, K.; Akesson, I.; Arvidsson, I.; Balogh, I.; Hansson, G.; Strömberg, U.; Rittner, R.; Skerfving, S. Exposure-response relationships in work-related musculoskeletal disorders in elbows and hands - A synthesis of group-level data on exposure and response obtained using uniform methods of data collection. Appl Ergon 2013, 44, 241–253. [Google Scholar] [CrossRef] [PubMed]
- Nordander, C.; Hansson, G.Å.; Ohlsson, K.; Arvidsson, I.; Balogh, I.; Strömberg, U.; Rittner, R.; Skerfving, S. Exposure–response relationships for work-related neck and shoulder musculoskeletal disorders – Analyses of pooled uniform data sets. Appl Ergon 2016, 55, 70–84. [Google Scholar] [CrossRef] [PubMed]
- Balogh, I.; Arvidsson, I.; Björk, J.; Hansson, G.Å.; Ohlsson, K.; Skerfving, S.; Nordander, C. Work-related neck and upper limb disorders - Quantitative exposure-response relationships adjusted for personal characteristics and psychosocial conditions. BMC Musculoskelet Disord 2019, 20. [Google Scholar] [CrossRef] [PubMed]
- Arvidsson, I.; Dahlqvist, C.; Enquist, H.; Nordander, C. Action Levels for the Prevention of Work-Related Musculoskeletal Disorders in the Neck and Upper Extremities: A Proposal. Ann Work Expo Health 2021, 65, 741–747. [Google Scholar] [CrossRef]
- Fan, X.; Lind, C.M.; Rhen, I.M.; Forsman, M. Effects of Sensor Types and Angular Velocity Computational Methods in Field Measurements of Occupational Upper Arm and Trunk Postures and Movements. Sensors (Basel) 2021, 21. [Google Scholar] [CrossRef]
- Forsman, M.; Fan, X.; Rhén, I.M.; Lind, C.M. Concerning a Work Movement Velocity Action Level Proposed in "Action Levels for the Prevention of Work-Related Musculoskeletal Disorders in the Neck and Upper Extremities: A Proposal" by Inger Arvidsson et al. (2021). Ann Work Expo Health 2022, 66, 130–131. [Google Scholar] [CrossRef]
- Forsman, M.; Fan, X.; Rhen, I.-M.; Lind, C.M. Mind the gap – development of conversion models between accelerometer- and IMU-based measurements of arm and trunk postures and movements in warehouse work. Appl Ergon 2022, 105, 103841. [Google Scholar] [CrossRef]
- Lavender, S.A.; Lorenz, E.; Andersson, G.B.J. Training in lifting. Prof Saf 2002, 47, 30–35. [Google Scholar]
- Lavender, S.A.; Lorenz, E.P.; Andersson, G.B. Can a new behaviorally oriented training process to improve lifting technique prevent occupationally related back injuries due to lifting? Spine (Phila Pa 1976) 2007, 32, 487–494. [Google Scholar] [CrossRef]
- Doss, R.; Robathan, J.; Abdel-Malek, D.; Holmes, M.W.R. Posture Coaching and Feedback during Patient Handling in a Student Nurse Population. IISE Trans Occup Ergon Hum Factors 2018, 6, 116–127. [Google Scholar] [CrossRef]
- van Tulder, M.; Furlan, A.; Bombardier, C.; Bouter, L. Updated method guidelines for systematic reviews in the Cochrane Collaboration Back Review Group. Spine (Phila Pa 1976) 2003, 28, 1290–1299. [Google Scholar] [CrossRef] [PubMed]
- Furlan, A.D.; Malmivaara, A.; Chou, R.; Maher, C.G.; Deyo, R.A.; Schoene, M.; Bronfort, G.; van Tulder, M.W. 2015 Updated Method Guideline for Systematic Reviews in the Cochrane Back and Neck Group. Spine (Phila Pa 1976) 2015, 40, 1660–1673. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Humadi, A.; Nazarahari, M.; Ahmad, R.; Rouhani, H. In-field instrumented ergonomic risk assessment: Inertial measurement units versus Kinect V2. Int J Ind Ergon 2021, 84, 103147. [Google Scholar] [CrossRef]
- Marras, W.S. The complex spine: The multidimensional system of causal pathways for low-back disorders. Hum Factors 2012, 54, 881–889. [Google Scholar] [CrossRef]
- Gallagher, S.; Marras, W.S.; Litsky, A.S.; Burr, D. Torso flexion loads and the fatigue failure of human lumbosacral motion segments. Spine (Phila Pa 1976) 2005, 30, 2265–2273. [Google Scholar] [CrossRef]
- Andersen, J.H.; Kaergaard, A.; Mikkelsen, S.; Jensen, U.F.; Frost, P.; Bonde, J.P.; Fallentin, N.; Thomsen, J.F. Risk factors in the onset of neck/shoulder pain in a prospective study of workers in industrial and service companies. Occup Environ Med 2003, 60, 649–654. [Google Scholar] [CrossRef]
- Ariëns, G.A.; Bongers, P.M.; Hoogendoorn, W.E.; van der Wal, G.; van Mechelen, W. High physical and psychosocial load at work and sickness absence due to neck pain. Scand J Work Environ Health 2002, 28, 222–231. [Google Scholar] [CrossRef]
- Mayer, J.; Kraus, T.; Ochsmann, E. Longitudinal evidence for the association between work-related physical exposures and neck and/or shoulder complaints: a systematic review. Int Arch Occup Environ Health 2012, 85, 587–603. [Google Scholar] [CrossRef]
- Baer, J.L.; Vasavada, A.; Cohen, R.G. Posture biofeedback increases cognitive load. Psychological research 2022, 86, 1892–1903. [Google Scholar] [CrossRef]
- Padula, R.S.; Comper, M.L.C.; Sparer, E.H.; Dennerlein, J.T. Job rotation designed to prevent musculoskeletal disorders and control risk in manufacturing industries: A systematic review. Appl Ergon 2017, 58, 386–397. [Google Scholar] [CrossRef]
- Wong, W.C.; Cheung, C.S.; Hart, G.J. Development of a quality assessment tool for systematic reviews of observational studies (QATSO) of HIV prevalence in men having sex with men and associated risk behaviours. Emerging themes in epidemiology 2008, 5, 23. [Google Scholar] [CrossRef] [PubMed]
- Breen, P.P.; Nisar, A.; Olaighin, G. Evaluation of a single accelerometer based biofeedback system for real-time correction of neck posture in computer users. Annu Int Conf IEEE Eng Med Biol Soc 2009, 2009, 7269–7272. [Google Scholar] [CrossRef]
- Tino, A.; Carvalho, M.; Preto, N.F.; McConville, K.M. Wireless vibrotactile feedback system for postural response improvement. Annu Int Conf IEEE Eng Med Biol Soc 2011, 2011, 5203–5206. [Google Scholar] [CrossRef] [PubMed]
- Vignais, N.; Miezal, M.; Bleser, G.; Mura, K.; Gorecky, D.; Marin, F. Innovative system for real-time ergonomic feedback in industrial manufacturing. Appl Ergon 2013, 44, 566–574. [Google Scholar] [CrossRef] [PubMed]
- Hermanis, A.; Nesenbergs, K.; Cacurs, R.; Greitans, M.J.J.o.m.; bioengineering. Wearable Posture Monitoring System with Biofeedback via Smartphone. J Biomed Eng 2013, 2, 40–44. [Google Scholar] [CrossRef]
- Cerqueira, S.M.; Silva, A.F.D.; Santos, C.P. Smart Vest for Real-Time Postural Biofeedback and Ergonomic Risk Assessment. IEEE Access 2020, 8, 107583–107592. [Google Scholar] [CrossRef]
- Ferrone, A.; García Patiño, A.; Menon, C. Low Back Pain-Behavior Correction by Providing Haptic Feedbacks: A Preliminary Investigation. Sensors (Basel) 2021, 21. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.; Ruiz Garate, V.; Gandarias, J.M.; Lorenzini, M.; Ajoudani, A. A Directional Vibrotactile Feedback Interface for Ergonomic Postural Adjustment. IEEE Trans Haptics 2022, 15, 200–211. [Google Scholar] [CrossRef]
- Lind, C.M.; Sandsjö, L.; Mahdavian, N.; Högberg, D.; Hanson, L.; Diaz Olivares, J.A.; Yang, L.; Forsman, M. Prevention of Work-Related Musculoskeletal Disorders Using Smart Workwear – The Smart Workwear Consortium. In Human Systems Engineering and Design, Ahram, T., Karwowski, W., Taiar, R., Eds. Springer: Cham, 2019; Vol. 876, pp. 477-483.
- Lind, C.M.; De Clercq, B.; Forsman, M.; Grootaers, A.; Verbrugghe, M.; Van Dyck, L.; Yang, L. Reducing postural exposure in real manual sorting work by means of real time vibrotactile feedback training. Saf Health Work 2022, 13, S147–S148. [Google Scholar] [CrossRef]
- Lind, C.M.; Forsman, M.; Lindecrantz, K.; Eklund, J.A.E. Reducing postural exposure in manual handling – effects of vibrotactile feedback and verbal instructions. In Proceedings of the 50th Nordic Ergonomics and Human Factors Society Conference, Lindblom, J., Österman, C., Eds. Technical University of Denmark: Elsinore, Denmark, 2019.
- Ailneni, R.C.; Syamala, K.R.; Kim, I.S.; Hwang, J. Influence of the wearable posture correction sensor on head and neck posture: Sitting and standing workstations. Work 2019, 62, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Kuo, Y.L.; Huang, K.Y.; Kao, C.Y.; Tsai, Y.J. Sitting Posture during Prolonged Computer Typing with and without a Wearable Biofeedback Sensor. Int J Environ Res Public Health 2021, 18. [Google Scholar] [CrossRef] [PubMed]
- Thanathornwong, B.; Suebnukarn, S.; Ouivirach, K. A system for predicting musculoskeletal disorders among dental students. Int J Occup Saf Ergon 2014, 20, 463–475. [Google Scholar] [CrossRef] [PubMed]
- Thanathornwong, B.; Suebnukarn, S. The Improvement of Dental Posture Using Personalized Biofeedback. Stud Health Technol Inform 2015, 216, 756–760. [Google Scholar] [CrossRef]
- Thanathornwong, B.; Jalayondeja, W. Vibrotactile -Feedback Device for Postural Balance Among Malocclusion Patients. IEEE journal of translational engineering in health and medicine 2020, 8, 2100406. [Google Scholar] [CrossRef]
- Thanathornwong, B.; Suebnukarn, S. A Personalized Pre-operative and Intra-operative Ergonomic Feedback to Improve the Dental Work Posture. Int J Hum Comput 2021, 37, 528–533. [Google Scholar] [CrossRef]
- Pinto, B.L.; Beaudette, S.M.; Brown, S.H.M. Tactile cues can change movement: An example using tape to redistribute flexion from the lumbar spine to the hips and knees during lifting. Hum Mov Sci 2018, 60, 32–39. [Google Scholar] [CrossRef]
- Larson, D.J.; Brown, S.H.M. Effects of trunk extensor muscle fatigue on repetitive lift (re)training using an augmented tactile feedback approach. Ergonomics 2023, 66, 1919–1934. [Google Scholar] [CrossRef]
- Grütters, K.; Narciss, S.; Beaudette, S.M.; Oppici, L. Reducing Lumbar Flexion in a Repetitive Lifting Task: Comparison of Leukotape and Kinesio Tape and Their Effect on Lumbar Proprioception. 2023, 13, 5908. [CrossRef]
- Chan, V.C.H.; Welsh, T.N.; Tremblay, L.; Frost, D.M.; Beach, T.A.C. A comparison of augmented feedback and didactic training approaches to reduce spine motion during occupational lifting tasks. Appl Ergon 2022, 99, 103612. [Google Scholar] [CrossRef]
- NIOSH. Hierarchy of Controls. Availabe online: https://www.cdc.gov/niosh/topics/hierarchy/default.html. (accessed on 3 November 2022).
- Lind, C.M. Assessment and design of industrial manual handling to reduce physical ergonomics hazards – use and development of assessment tools; KTH Royal Institute of Technology: Stockholm, 2017. [Google Scholar]
- Sabino, I.; Fernandes, M.d.C.; Cepeda, C.; Quaresma, C.; Gamboa, H.; Nunes, I.L.; Gabriel, A.T. Application of wearable technology for the ergonomic risk assessment of healthcare professionals: A systematic literature review. Int J Ind Ergon 2024, 100, 103570. [Google Scholar] [CrossRef]
- Schall, M.C., Jr.; Sesek, R.F.; Cavuoto, L.A. Barriers to the Adoption of Wearable Sensors in the Workplace: A Survey of Occupational Safety and Health Professionals. Hum Factors 2018, 60, 351–362. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



