Submitted:
08 August 2024
Posted:
09 August 2024
You are already at the latest version
Abstract
Background: Introduction of new technologies in the management of oral disease has revolutionized treatment approaches, offering less invasive options and improved patient outcomes. Among oral cavity diseases, sialolithiasis is the most common disorder of the salivary glands. It involves the formation of calculi or stones within the salivary ducts, primarily affecting the submandibular gland due to its tortuous duct and the alkaline nature of its saliva. In particular, Laser-assisted techniques have shown significant promise in enhancing the precision and safety in the management of sialolith removal. This article aims to present a case report and also explores the scientific evidence supporting these innovative methods, highlighting their benefits and limitations in clinical practice.; Methods: The research was conducted using PubMed and Scopus search engines with a combination of relevant keywords, including laser, laser-assisted, laser treatment in combination with sialolith, sialolith removal, and sialoadenectomy. Selected articles were carefully reviewed to identify studies reporting data on the effectiveness of laser-assisted sialolith removal; Results: The results of the literature review indicate a growing interest in the application of Diode Laser and CO2, with evidence suggesting improved clinical outcomes and reduced postoperative pain compared to traditional methods; Conclusions: Although lasers offer enhanced safety and reduced morbidity and bleeding, which ensures optimal visibility, their high cost and the need for specialized training are limitations. Further randomized clinical trials and longer follow-up studies are needed to better evaluate their use in sialolith removal.
Keywords:
Sialolith Removal
; Minimally Invasive Surgery
; Laser Techniques
; Diode Laser
; Submandibular Duct
1. Introduction
Sialolithiasis is a condition characterized by the development of one or more oval or round-shaped calcifications, known as sialoliths, occurring in the salivary minor and major glands. Calcifications might impact glandular parenchyma or the associated ducts. [1] The pathogenesis of stones occurs due to the accumulation of organic debris in the duct lumen, associated with the deposition of calcium salts on the material. Both the organic and inorganic components originate from saliva. [2] Among the diseases affecting salivary glands, sialolithiasis is the most prevalent, accounting for approximately half of all benign salivary gland disorders. Sialolithiasis most commonly occurs in the submandibular gland, comprising 80% of cases, followed by the parotid gland (5-20%) and the sublingual and minor glands (1-2%). [3] The tendency for sialolithiasis to develop in the submandibular gland is attributed to its mucous and alkaline secretion, as well as the antigravitational design of the pertinent excretory duct, which is both lengthy and has a tortuous path around the mylohyoid muscle. [1,2] About 40% of submandibular calculi are found in the distal portion of Wharton’s duct, while calculi in the parotid gland tend to be located within the glandular parenchyma. [4] Sialoliths may be asymptomatic or associated with painful swelling when their size obstructs the duct, with symptoms typically exacerbating during meals. Chronic duct obstruction may, in fact, result in inflammation and infection. Typically ranging from 5 to 10 mm in size, sialoliths are referred to as megaliths or giant sialoliths when they exceed 15 mm, although this is a rare occurrence. The onset of symptoms is influenced by the dilation of the duct and the growth rate of the calculus, which is estimated to be between 1 and 1.5 mm per year. Besides radiographic examinations, specific imaging techniques such as computed tomography (CT), ultrasound, and contrast-enhanced sialography may be necessary for diagnostic purposes.
This is because non-palpable stones often yield false-negative results in radiography. [2] Additionally, sialendoscopy is also noteworthy as a diagnostic tool. [5]
Once diagnostic confirmation is achieved, treatment may be performed. Patients with small sialolithiasis may benefit from conservative measures, including hydration, moist heat application, and gland massage. Sialendoscopy can also be employed; this minimally invasive technique allows for endoscopic visualization of the salivary ductal system. It serves as both a diagnostic and interventional tool for addressing inflammatory and obstructive conditions within the ductal system. Sialendoscopy has been shown to be an alternative to traditional surgery for stones measuring up to 4-5 mm in diameter, particularly when they are free within the duct lumen and mobile. Furthermore, the use of ultrasound for stone fragmentation has been found to enhance treatment outcomes. Despite significant technological advancements, 5-10% of patients with sialolithiasis are unable to be successfully treated using minimally invasive techniques. [6] Stones may be removed through surgical treatment conducted under local anesthesia and on an outpatient basis. However, for stones situated in the proximal part of the duct or within the submandibular gland, the preferred treatment is sialoadenectomy. This surgical procedure, however, is not without complications, which may include hypertrophic scar formation and potential injury to surrounding anatomical structures. [7] To mitigate the morbidity associated with sialoadenectomy, a minimally invasive approach such as transoral sialolithotomy may be employed. [8] Over time, various types of Lasers have been utilized in dentistry as alternatives to traditional surgery, including CO2 Laser, Diode and Nd:YAG Laser. Among these, Diode Laser has emerged as the most advantageous due to its shallower penetration depth compared to Nd:YAG. Its higher absorption by hemoglobin, oxyhemoglobin, and melanin ensures greater safety for adjacent tissues. [9] Additionally, it exhibits excellent cutting and coagulation capabilities, making it a superior alternative to conventional soft tissue surgery. [10,11] Laser offers several advantages, including enhanced coagulation properties, high-quality incisions, minimal bleeding, a low risk of nerve damage, and a reduced incidence of comorbidities [12].
This study aims to present a case of a patient with a clinical diagnosis of sialolithiasis of the submandibular gland duct, treated with surgical excision performed by Diode laser and to review the scientific evidence regarding the utilization of Laser in sialolithiasis surgery.
2. Materials and Methods
2.1. Case Report
A 60-year-old male patient referred to our observation at the Complex Unit of Odontostomatology of the University of Bari ‘Aldo Moro’ complaining a 6-days history of fever, swelling, and pain in the left sublingual region.
At the intraoral palpation a firm mobile mass in the left sublingual region was observable, with edema of the submandibular duct and pus drainage (Figure 1).
The patient underwent an OPT X-ray and a mandibular occlusal radiograph, which revealed a round radiopaque area located in the sublingual region within the duct of the submandibular gland. (Figure 2 and Figure 3).
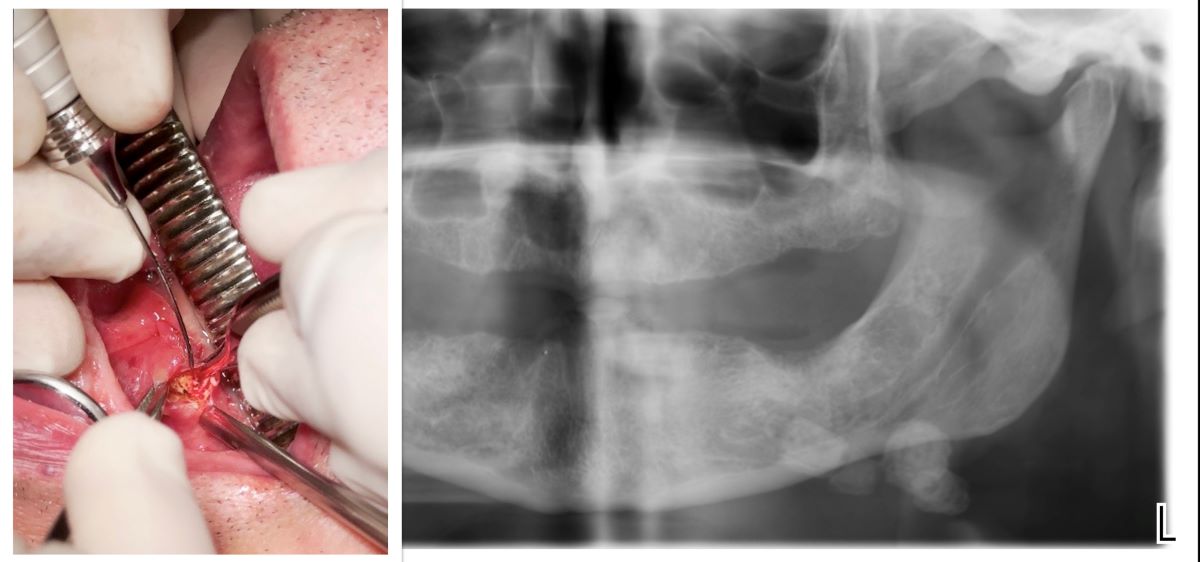
A first diagnosis of submandibular sialolithiasis was established. Patient provided informed consent and underwent surgical excision of the lesion with Diode laser. Local anesthetic infiltration was administered in the sublingual region near the salivary calculus with an injection of 4% articaine combined with 1:100,000 epinephrine. A Diode laser module, equipped with a 300-μm optical fiber emitting at a wavelength of 910 nm, with an output power of 2 W (Lasotronix, Poland), was set to continuous wave mode. Intraoral access was achieved performing a linear incision along the path of Wharton’s duct on the floor of the mouth, posterior to the sublingual caruncle. (Figure 4.) Tissues were dissected using blunt forceps. (Figure 5.)
The absence of bleeding expedited the procedure and made it more comfortable for both the operator and the patient. The sialolith obstructing the submandibular duct was removed and measured approximately 18 mm in diameter. (Figure 6.) No sutures were necessary, and the wound healed by secondary intention after 4 weeks. Submandibular manipulation were suggested during healing to promote saliva drainage. No intra- and post-operative complications were detected.
Postoperatively, patient assumed amoxicillin and clavulanic acid (875 mg + 125 mg) every 12 hours for 6 days and did not experience edema or bruising, no pain or discomfort. Follow-up evaluations on days 7, (Figure 7.) 14, and 30 post-surgery (Figure 8.) revealed that the patient was asymptomatic. Regular follow-ups every 6 months were performed.
2.2. Literature Review
A detailed search strategy was crafted based on the PICO criteria, followed by an electronic search. The PICO question posed was: “What are the contemporary applications of laser technology in the sialoliths removal?” Table 1 summarizes the workflow based on the PICO criteria.[13].
An extensive literature search was performed using the PubMed, Scopus, and Web of Science databases to identify pertinent studies on the role and applications of Laser in the removal of sialoliths. Also, a manual review of the reference lists from all full-text articles and relevant reviews identified through the electronic search was undertaken. Further manual searches were conducted in the following journals: Journal of Oral and Maxillofacial Surgery, International Journal of Oral and Maxillofacial Surgery, Lasers in Medical Science, Journal of Clinical Laser Medicine & Surgery, Photomedicine and Laser Surgery, Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Journal of Laser Applications.The search utilized a combination of keywords and Medical Subject Headings (MeSH) terms, including: ((Laser [Mesh] OR (laser assisted) OR (laser treatment)) AND ((Sialolith [Mesh] OR (AI) OR (Sialolith Removal) OR (Sialadenectomy))). The inclusion criteria covered studies of any evidence level: randomized clinical trials, observational studies (cohort, case-control), case series, and case reports. Articles published in English from 1990 to 2024 were included. Clinical studies had to be based on human subjects diagnosed with salivary gland stones, explicitly excluding animal studies. Exclusion criteria eliminated review articles, letters to editors, and studies lacking full-text availability. Table 2 provides a summary of the search strategy.
Two independent reviewers screened the titles and abstracts of the retrieved articles to identify potentially relevant studies. Full-text articles were subsequently evaluated for eligibility according to the defined inclusion criteria. From the selected articles, authors extracted the following information: the names of the author(s), the publication year, and the study design. Also, authors recorded the total number of patients treated, details on the Laser type and settings, the site of the sialolith, complications during and after the procedure, follow-up details, and treatment outcomes.Obtained data were analyzed through both qualitative and quantitative methods. Overall, the study approach systematically located, evaluated, and compiled existing data on the role and applications of Laser in sialolith removal, providing valuable insights into the current state of the field and suggesting directions for future research.
3. Results
In July 2024, the search came to an end. 780 article titles were screened, and 40 abstracts were chosen for additional examination. 20 articles were examined in their entirety to see if they satisfied the inclusion requirements. Following additional review, 7 articles were eliminated for the following reasons:
- Full text not available (n = 5);
- Clinica study on animals (n = 2).
4. Discussion
Laser-assisted oral surgery represents an innovative frontier in modern dental practice. In recent years, the application of Laser technology has paved new pathways for enhancing clinical outcomes in oral diseases. Given the current understanding of therapeutic approaches using Laser, this review aims to evaluate the existing knowledge and evidence on the use of Laser for salivary gland sialolithiasis. In dentistry, various devices are used, including Diode Lasers, Nd:YAG (Neodymium-Doped Yttrium Aluminium Garnet), Er:YAG (Erbium-Doped Yttrium Aluminium Garnet), Er,Cr:YAG (Erbium, Chromium: Yttrium Scandium Gallium Garnet), and CO2 (Carbon Dioxide). In this review, it was observed that the devices described in the documented case reports and case series were Diode laser and the CO2 laser.
From the four articles [18,19,20,21] describing clinical cases assisted by the CO2 laser, a total of 87 patients underwent surgical removal of sialoliths from salivary glands. These patients included 38 females and 49 males, with ages at diagnosis ranging from 8 to 85 years. According with the literature, calculi may arise in any salivary glands although this condition mostly affects the submandibular glands from 80% to 92% and the parotid from 6% to 20% [22]. In fact, 76 calculi were located into the Wharton’s duct while only 5 into Stensen’s duct. The diagnosis of sialolithiasis is primarily clinical, based on patient-reported symptoms, palpation, and inspection. An accurate differential diagnosis is essential for establishing a proper treatment plan. [23] Stones located in the distal Wharton’s duct and the hilum might often be detected through bimanual palpation of the submandibular gland and the floor of the mouth. However, detecting parotid stones through palpation is significantly more challenging due to the complex anatomy of the duct system. Imaging plays a crucial role in the precise localization of sialoliths, while computed tomography (CT) and magnetic resonance imaging (MRI) are generally unnecessary for diagnosing sialolithiasis. [24] In all the reported cases, symptoms included oral pain and swelling. Radiological imaging was used to support the clinical diagnosis, specifically occlusal and panoramic radiographs in all cases. Only Yang et al. [21] relied solely on palpation for diagnosing 12 patients, while for those presenting neck swelling and pain, a CT scan was performed. Surgical excision is required for definitive diagnosis and treatment of this condition. Traditional surgery is considered more invasive due to the potential risk to damage critical structures such as the lingual nerve, facial nerve, marginal mandibular nerve, and hypoglossal nerve, as well as the risks of haemorrhage, hematoma, and the likelihood of postoperative hypertrophic scarring at the surgical site. [25] All authors conclude that the use of Lasers minimizes the invasiveness of treatments. They also emphasize that the technique is relatively straightforward, requiring only local anesthesia with minimal analgesia. This procedure may be performed on an outpatient basis through an intraoral approach. A major advantage is the minimal bleeding in the surgical field, which ensures optimal visibility. [26,27]
The CO2 laser achieves hemostasis, thereby reducing bleeding, shortening the duration of the intervention, and minimizing operative morbidity. All these factors help reduce the patient’s emotional and physical stress, thereby promoting better recovery of the traumatized tissues. [28] Furthermore, it enhances patient comfort by eliminating the need for primary wound closure with sutures. CO2 Laser has an absorption peak that closely matches that of water, making it especially effective for soft tissues with high water content. In all cases, a continuous-wave CO2 Laser was used at power settings ranging from 5W to 10W. This approach ensured that surrounding tissues were not damaged, as the thermal effects were confined to the treated area. [29,30] None of the 87 reported cases required sutures at the end of the procedure, thereby minimizing or eliminating the risk of postoperative sublingual ranula formation. This method supports effective salivary drainage without the need for marsupialization or drain placement. In the study by Yang et al. [21] only one case developed a ranula, while no complications were observed in the other patients during follow-up. All the aforementioned features facilitate postoperative rehabilitation with minimal swelling, bleeding, infection, and pain, reducing the need for extensive medication. Traditionally, patients undergoing intraoral Laser treatment require only analgesics and anti-inflammatory drugs following surgery. Therefore, in the study of Azaz et al. [18] 4 patients had antibiotics for 5 days, in which the surgical removal of the sialolith was challenging. A total of 29 patients who underwent surgical removal of sialoliths from salivary glands using a Diode Laser have been reported in the four articles included in this review. These 29 patients comprised 12 females and 17 males, with ages at diagnosis ranging widely from 33 to 93 years. The authors of these four articles also agree that for the diagnostic suspicion of sialolithiasis, clinical examination combined with imaging tests is essential. The observed signs in these patients included swelling in the gland area and the ability to detect the gland itself through bimanual palpation. To confirm the diagnosis, Angiero et al. [17] used CT scans for only some patients. In their study, stones could be palpated through superficial ductal localization in 15 patients, while in 10 patients, the stones were quite small. Additionally, in four patients, gland infection complicated palpation, necessitating further examination. Sialolithiasis predominantly affects the submandibular gland, accounting for 80% of cases, followed by the parotid gland (5-20%) and the sublingual and minor glands (1-2%) In their case reports, Haas O.L. et al. [14] utilized both occlusal radiography and CBCT. Notably, the 93-year-old patient in his second case report—who is also the oldest patient identified in our study—had previously undergone surgery for sialolithiasis 15 years prior. In some cases, radiographic examination alone provided sufficient information to proceed with surgery [15,16] Prior to surgery, local anesthetic infiltration was commonly administered. In the cases described by Kılınç et al. [16] and l as Haas OL et al. [14], a 4% articaine solution with 1/100,000 epinephrine was used to achieve local vasoconstriction. In contrast, Angiero decided for a topical anesthetic, specifically EMLA (lidocaine and prilocaine), rather than local anesthesia. During the procedure, an 810-830 nm Diode Laser was used in all examined cases. Notably, in the two cases described by Haas O.L. [14], device was paired with a 400 µm optical fiber emitting a 980 nm (infrared) wavelength. The irradiation energy was 2.5 W for the 27 cases reported by Haas O.L. and Angiero [14,17], while a higher energy of 4 W was used in the case described by Kılınç et al. [16] Almost all of the procedures described were performed without the use of sutures, allowing a secondary intention healing. The only exception was the case described by Kılınç et al [16] where the duct was marsupialized in the floor of the mouth with Vicryl 5.0 sutures after the calculus was removed. For postoperative care, Kılınç, Y. [16] prescribed an antibiotic regimen consisting of amoxicillin-clavulanate every 12 hours for 5 days and Rovamycin every 12 hours for 5 days, along with a nonsteroidal anti-inflammatory drug (flurbiprofen 100 mg every 12 hours for 3 days) and an oral rinse (chlorhexidine gluconate 0.2%, three times daily for 7 days). Haas O.L. [14] recommended oral amoxicillin (500 mg every 8 hours for 7 days) and oral acetaminophen (750 mg every 6 hours for 3 days). In contrast, Angiero et al. [17] did not deem analgesics necessary for his 25 patients, prescribing only rinses for hygiene purposes. Of the 29 patients, only 2 required repeated treatment, one due to incomplete removal of the stones and the other due to an inability to achieve duct patency. Thus, the treatment was considered unsuccessful in 2 out of 29 cases. The overall complication rate during the healing period was low. Only 3 patients experienced symptoms such as odynophagia, trismus, and submandibular swelling, which resolved within 2-3 days.
Importantly, in all the articles included in this review no cases of paresthesia were reported. Paresthesias, which may affect the mandibular branch of the facial nerve, the hypoglossal nerve, or the lingual nerve, are among the most serious complications associated with traditional surgery. This highlights the minimally invasive nature of Laser technology, [31] which reduces side effects and operational risks, such as hypertrophic scarring, while providing superior coagulation for better visibility of the operative field. [32] Additionally, Lasers minimizes complications in patients with coagulation disorders. The study found positive outcomes with Lasers use in patients on anticoagulants, [33] who do not need to discontinue their medication for the procedure, particularly in elderly patients and those with diabetes [34].
5. Conclusions
This study highlights the growing interest in modern medicine towards the utilization of new technologies that reduce the invasiveness of treatments. All authors of the articles included in this review emphasized that the use of Diode and CO2 Lasers minimizes invasiveness in the surgical removal of sialoliths from salivary glands. All authors reported improved visibility of the surgical site, attributed to the absence of bleeding, compared to traditional surgery. Among the intraoperative advantages consistently reported were reduced operative time and the avoidance of suturing the surgical site. Furthermore, all authors noted that postoperative edema was nearly absent, and patients experienced minimal pain. However, based on the collected data, it cannot be concluded that the use of Diode and CO2 Lasers is associated with a reduction in postoperative antibiotic and/or analgesic therapies.
Despite the use of Laser being associated with enhanced safety and significantly reduced morbidity, and all authors agreeing that this technique is an excellent alternative to traditional surgery, certain limitations must be considered, these include the high cost of equipment and the need to train healthcare personnel in the use of new technologies.
Additionally, further randomized clinical trials and studies with longer follow-up periods are necessary to more accurately evaluate the use of lasers in salivary gland surgery.
Author Contributions
Conceptualization, G.D., M.F. and S.C.; methodology, S.C.; validation S.C.; formal analysis, G.D., G.G., M.V., F.D.T. and S.C.; investigation M.V., R.B. and S.C.; resources, R.B., F.D., G.D., M.F. and S.C..; data curation G.D., M.F. and S.C.; writing—original draft preparation, G.D., M.F. and S.C.; writing—review and editing, G.D., M.F., F.D.T. and R.B.; visualization, G.D., M.F. and S.C.; supervision, S.C.; project administration, S.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Sánchez Barrueco A, Alcalá Rueda I, Ordoñez González C, Sobrino Guijarro B, Santillán Coello J, Tapia GD, Guerra Gutiérrez F, Campos González A, Brenna A, Cenjor Españo C, Villacampa Aubá JM. Transoral removal of submandibular hilar lithiasis: Results on the salivary duct system, glandular parenchyma, and quality-of-life recovery. Eur Arch Otorhinolaryngol. 2023 Nov;280(11):5031-5037.
- Togni L, Mascitti M, Santarelli A, Contaldo M, Romano A, Serpico R, Rubini C. Unusual Conditions Impairing Saliva Secretion: Developmental Anomalies of Salivary Glands. Front Physiol. 2019 Jul 3;10:855. [CrossRef]
- Ungari C, Cicconetti A, Cerbelli E, Sulpasso A, Filiaci F. Giant submandibular sialolith: A case report. Clin Ter. 2022 May 25;173(3):217-221. [CrossRef]
- Romero NJ, Fuson A, Kieliszak CR, Joshi AS. Sonolocation during submandibular sialolithotomy. Laryngoscope. 2019 Dec;129(12):2716-2720. [CrossRef]
- Dabirmoghaddam P, Hosseinzadehnik R. Interventional sialendoscopy with endoscopic sialolith removal without fragmentation. Indian J Otolaryngol Head Neck Surg. 2013 Apr;65(2):111-5. [CrossRef]
- Soriano-Martín D, García-Consuegra L, Junquera L, Rodríguez-Santamarta T, Olay S, Junquera-Olay S. Sialendoscopy approach in treating juvenile recurrent parotitis: A systematic review. J Otolaryngol Head Neck Surg. 2023 Aug 19;52(1):53. [CrossRef]
- Nofal A, El-Anwar MW, Al Shawadfy MA, Fouad YA. Drain-Less Submandibular Gland Excision With Preserved Facial Artery. Ear Nose Throat J. 2022 Dec 1:1455613221142735. [CrossRef]
- Witt RL, Iro H, Koch M, McGurk M, Nahlieli O, Zenk J. Minimally invasive options for salivary calculi. Laryngoscope. 2012 Jun;122(6):1306-11. [CrossRef]
- Capodiferro S, Maiorano E, Loiudice AM, Scarpelli F, Favia G. Oral laser surgical pathology: A preliminary study on the clinical advantages of diode laser and on the histopathological features of specimens evaluated by conventional and confocal laser scanning microscopy. Minerva Stomatol. 2008 Jan-Feb;57(1-2):1-6, 6-7.
- Capodiferro S, Maiorano E, Scarpelli F, Favia G. Fibrolipoma of the lip treated by diode laser surgery: A case report. J Med Case Rep. 2008 Sep 12;2:301. [CrossRef]
- Dell’Olio F, Baldassarre ME, Russo FG, Schettini F, Siciliani RA, Mezzapesa PP, Tempesta A, Laforgia N, Favia G, Li-mongelli L. Lingual laser frenotomy in newborns with ankyloglossia: A prospective cohort study. Ital J Pediatr. 2022 Sep 5;48(1):163. [CrossRef]
- Capodiferro S, Limongelli L, D’Agostino S, Tempesta A, Dolci M, Maiorano E, Favia G. Diode Laser Management of Primary Extranasopharyngeal Angiofibroma Presenting as Maxillary Epulis: Report of a Case and Literature Review. Healthcare (Basel). 2021 Jan 1;9(1):33. [CrossRef]
- da Costa Santos CM, de Mattos Pimenta CA, Nobre MR. The PICO strategy for the research question construction and evidence search. Rev Lat Am Enfermagem. 2007 May-Jun;15(3):508-11. [CrossRef]
- Haas OL Jr, Scolari N, da Silva Meirelles L, Favoretto AX, de Oliveira RB. Sialolith removal in the submandibular region using surgical diode laser: Report of two cases and literature review. Oral Maxillofac Surg. 2018 Mar;22(1):105-111. [CrossRef]
- Mathew J, Pothanikat JJK, Vinod Kumar RB, Padikadan NO, Arakkal NJ. Extremely Large Submandibular Sialolith Removal - A Case Report. Ann Maxillofac Surg. 2022 Jul-Dec;12(2):237-239. [CrossRef]
- Kılınç, Y. and Çetiner, S. (2014) Surgical Removal of a Giant Sialolith by Diode Laser. Open Journal of Stomatology, 4, 484-488. [CrossRef]
- Angiero F, Benedicenti S, Romanos GE, Crippa R (2008) Sialolithiasis of the submandibular salivary gland treated with the 810- to 830-nm diode laser. Photomed Laser Surg 26(6):517–521.
- Azaz B, Regev E, Casap N, Chicin R (1996) Sialolithectomy done with a CO2 laser: Clinical and scintigraphic results. J Oral Maxillofac Surg 54(6):685–688.
- Barak S, Horowitz I, Katz J, Kaplan I (1991) Experiences of the CO2 laser in the surgical treatment of intraoral salivary gland pa- thology. J Clin Laser Med Surg 9(4):295–299.
- Barak S, Katz J, Mintz S (1993) Use of the carbon dioxide laser to locate small sialoliths. J Oral Maxillofac Surg 51(4):379–381.
- Yang SW, Chen TA (2011) Transoral carbon dioxide laser sialolithectomy with topical anaesthesia. A simple, effective, and minimally invasive method. Int J Oral Maxillofac Surg 40(2):169– 172.
- Williams MF. Sialolithiasis. Otolaryngol Clin North Am. 1999 Oct;32(5):819-34.
- Favia G, Capodiferro S, Turco M, Cortelazzi R. Lithiasis of minor salivary glands of the upper lip. Clinico-pathological report of a case with unusual presentation. Minerva Stomatol. 2004 Apr;53(4):179-83.
- Iro H, Dlugaiczyk J, Zenk J. Current concepts in diagnosis and treatment of sialolithiasis. Br J Hosp Med (Lond). 2006 Jan;67(1):24-8. [CrossRef]
- Hald J, Andreassen UK (1994) Submandibular gland excision: Short- and long-term complications. ORL J Otorhinolaryngol Relat Spec 56(2):87–91.
- Sutter E, Giacomelli-Hiestand B, Rücker M, Valdec S. Der CO2-Laser und seine Anwendung in der Stomatologie [CO2 laser application in stomatology]. Swiss Dent J. 2019 Mar 11;129(3):214-215. German.
- Boj JR, Poirier C, Hernandez M, Espassa E, Espanya A. Case series: Laser treatments for soft tissue problems in children. Eur Arch Paediatr Dent. 2011 Apr;12(2):113-7.
- Macrì M, D’Albis G, D’Albis V, Antonacci A, Abbinante A, Stefanelli R, Pegreffi F, Festa F. Periodontal Health and Its Relationship with Psychological Stress: A Cross-Sectional Study. J Clin Med. 2024 May 16;13(10):2942. [CrossRef]
- Tenore G, Palaia G, Mohsen A, Ambrogiano S, Gioia CRTD, Dominiak M, Romeo U. Could the super-pulsed CO2 laser be used for oral excisional biopsies? Adv Clin Exp Med. 2019 Nov;28(11):1513-1517.
- Sutter E, Giacomelli-Hiestand B, Rücker M, Valdec S. Der CO2-Laser und seine Anwendung in der Stomatologie [CO2 laser application in stomatology]. Swiss Dent J. 2019 Mar 11;129(3):214-215. German. [CrossRef] [PubMed]
- Pal M, Saokar A, Gopalkrishna P, Rajeshwari HR, Kumar S. Diode laser-assisted management of intraoral soft tissue overgrowth: A case series. Gen Dent. 2020 Jul-Aug;68(4):28-31.
- Romanos GE, Gutknecht N, Dieter S, Schwarz F, Crespi R, Sculean A. Laser wavelengths and oral implantology. Lasers Med Sci. 2009 Nov;24(6):961-70. [CrossRef]
- Ortega-Concepción D, Cano-Durán JA, Peña-Cardelles JF, Paredes-Rodríguez VM, González-Serrano J, López-Quiles J. The application of diode laser in the treatment of oral soft tissues lesions. A literature review. J Clin Exp Dent. 2017 Jul 1;9(7):e925-e928. [CrossRef]
- Al-Mohaya MA, Al-Malik AM. Excision of oral pyogenic granuloma in a diabetic patient with 940nm diode laser. Saudi Med J. 2016 Dec;37(12):1395-1400. [CrossRef]
Figure 1.
Clinical presentation of a left sublingual swelling in the region of Wharton duct.

Figure 2.
OPT X-ray image of the patient.
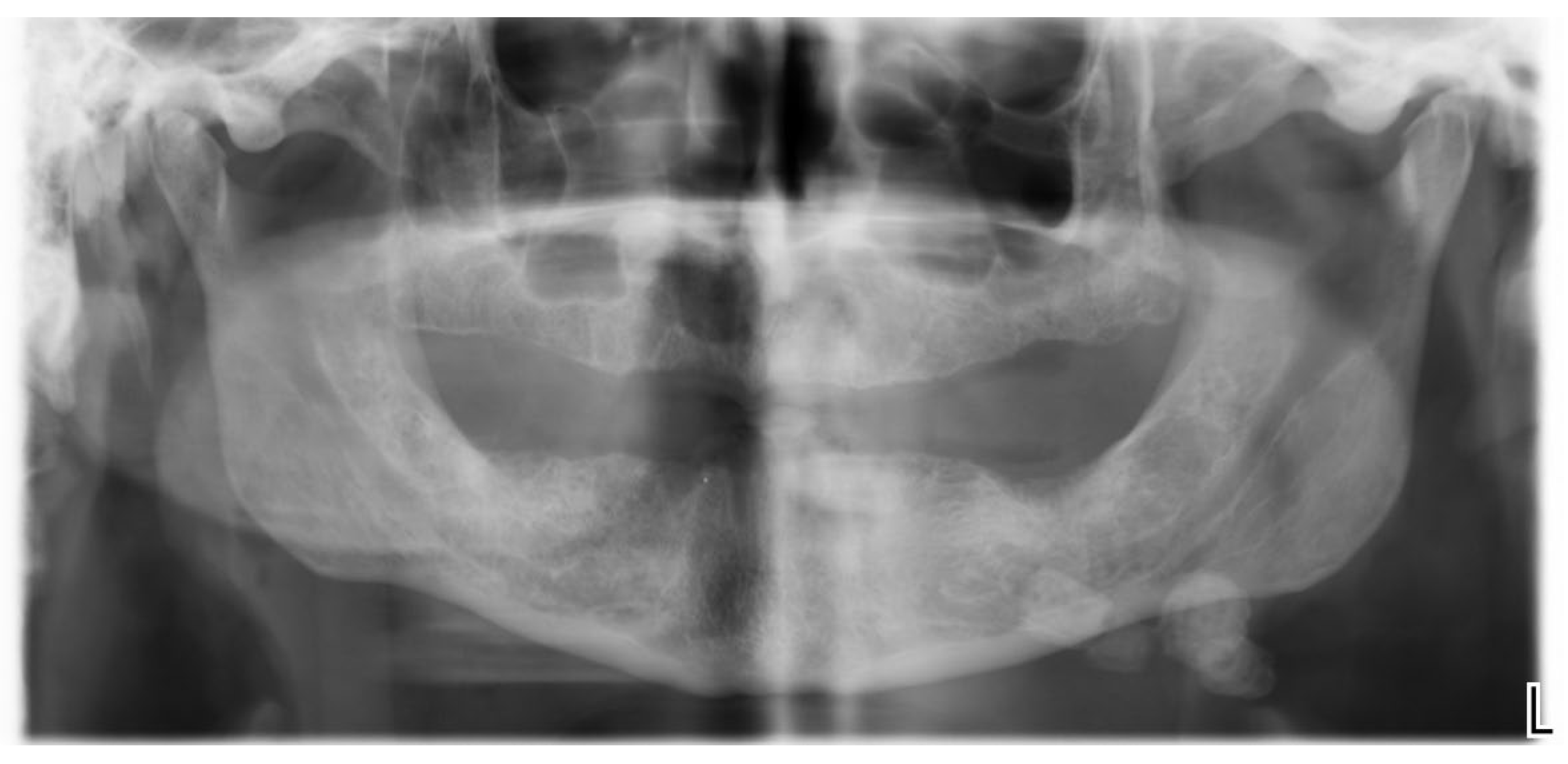
Figure 3.
Mandibular occlusal radiograph showing sublingual region.
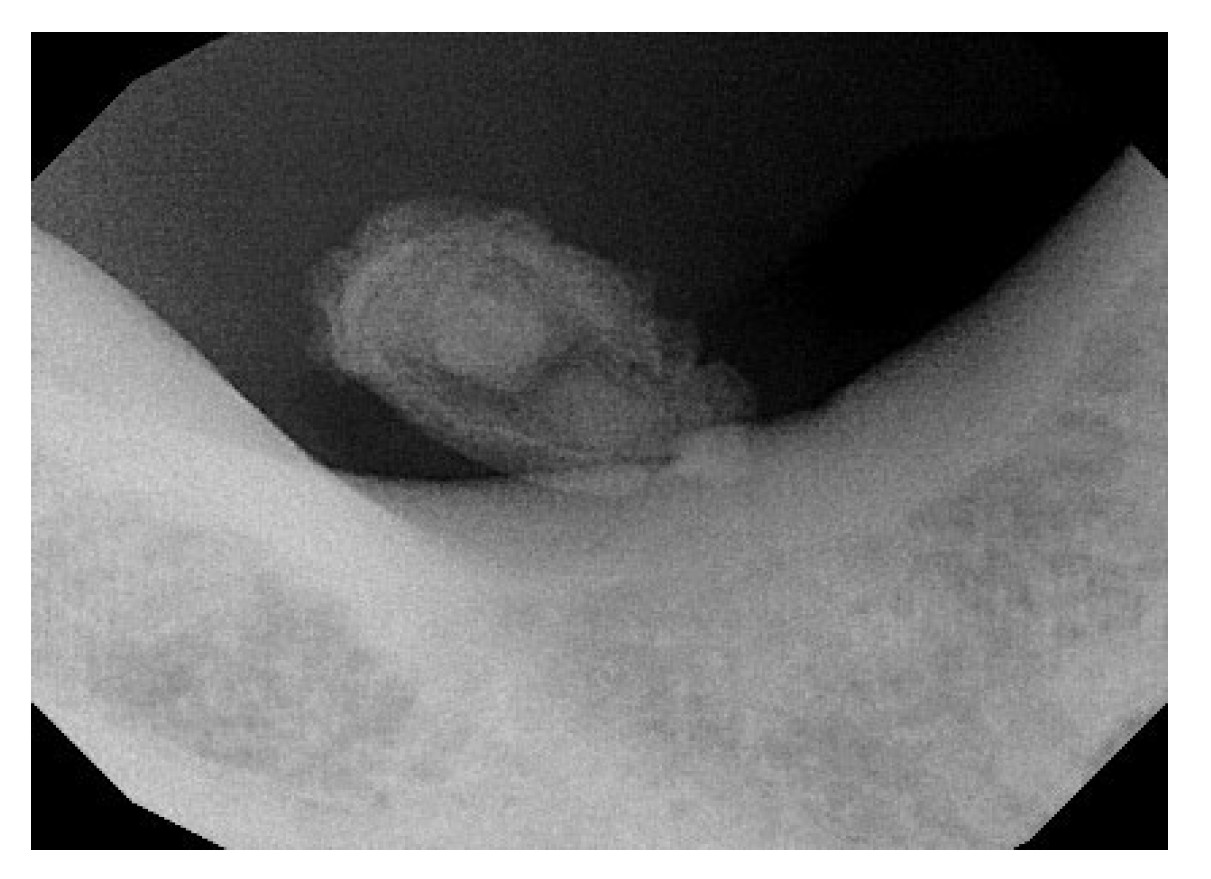
Figure 4.
Intraoperative image of the Diode Laser incision in the region of Wharton duct.

Figure 5.
The Surgical incision designed drawn parallel to duct and deeply till to calcucus localization and its isolation.
Figure 5.
The Surgical incision designed drawn parallel to duct and deeply till to calcucus localization and its isolation.

Figure 6.
Detail of the removed calculus.

Figure 7.
Seven days follow-up of the treated region.

Figure 8.
Follow-up at 1 month showing complete tissue healing.


Table 1.
Research question and PICO workflow summary.
| Focused Question |
What are the current uses of laser in sialolith removal? |
|---|---|
|
PICO criteria Population Intervention or Exposure Comparison Outcome |
Patients diagnosed with salivary gland stones (sialolithiasis). Electronic literature searches: #1 ((Laser [Mesh] OR (laser assisted) OR (laser treatment)) #2: ((Sialolith [Mesh] OR (Sialolith Removal) OR (Sialoadenectomy)) Traditional interventions or other non-laser techniques for stone removal. Effectiveness of the intervention (complete stone removal), healing times, recurrence rates, complications (bleeding, infection, tissue damage), post-operative pain, patient satisfaction. |
Table 2.
Summary of research strategy.
| Search Strategy |
|
|---|---|
|
Database search Electronic Journals |
PubMed, Scopus, Web of Science database Journal of Oral and Maxillofacial Surgery, International Journal of Oral and Maxillofacial Surgery, Lasers in Medical Science, Journal of Clinical Laser Medicine & Surgery, Photomedicine and Laser Surgery, Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, Journal of Laser Applications |
|
Selection criteria Inclusion criteria Exclusion criteria |
Study Type: Randomized clinical trials, observational studies (cohort, case-control), case series, and case reports. Language: Studies published in English and other major languages. Publication Date: Studies published within the last 30 years. Full-Text Access: Studies for which the full text is available. Review articles, letter to editors Animal studies. Multiple publications on the same patient population. Full text not available/accessible. |
Table 3.
Clinical features and outcomes of included studies.
| A total of 8 full-text papers were included for data extraction after 2 more articles which respected the inclusion criteria were found through manual searching. [14,15,16,17,18,19,20,21] All collected data from the analysis of the selected articles were compiled into a table for a comprehensive examination. (Table 3.) First Author (Year) Country |
Study Design | N° cases, Gender,age |
Sialolith locations | Laser type | Laser setting | Farmacological therapy | Complications |
Follow-up |
Outcome or Conclusions |
|---|---|---|---|---|---|---|---|---|---|
| Haas OL H. et al. (2018) [14] | Case series | 2 cases, 1 M: 33 Y 1F: 93 Y |
Distal part of the submandibular duct and could be palpated intraorally. | Diode laser | 400-μm optical fiber emitting at a wavelength of 980 nm (infrared), 2.5 W output power, and in continuous pulse mode. | Amoxicillin (500mg) every 8h for 7 days and oral acetaminophen (750 mg) every 6h for 3 days | No intraoperative complications were reported | Evaluated on days 7,14, and 30 free surgery. | The diode laser is a safe, minimally invasive option for this procedure, offering enhanced coagulation, high-quality incisions, no bleeding, low nerve damage risk, and minimal comorbidities |
| Mathew J et al. (2022) [15] | Case report | 1 case, 1M: 50 Y |
Behind the lower right second permanent molar | Diode laser | 810 μm | - | Asymptomatic with undisturbed salivary flow | One year. | Newer treatment modalities offer effective alternatives to conventional surgical methods for sialoliths. |
| Kılınç et al. (2014) [16] | Case report | 1 cases, 1F: 57Y |
In the anterior part of the left side of the floor in the mouth. | Diode Laser | 810 nm of wavelength, 4.0 W of power, 0.5 ms continuous wave and 1000 Hz of frequency was selected. | Antibiotic: Amoxicillin clavulonate 1000 mg , every 12 h for 5 d. Rovamycine every 12 h for 5 d). Anti-inflammatory: 100 mgr flurbiprofen every 12 h for 3 d | No sign of infection was observed, and salivary flow was normal. | 10th days. | An 810-nm diode laser is a safe and effective technique, offering excellent cutting and coagulation with a low complication rate, making it suitable for this surgical procedure. |
| Angiero et al. (2008) [17] | Case series | 25 cases. | Wharton’s duct | Diode laser | Wavelength of 810-830nm ,2,5W CW with 5-10 sec irradiation time (energy density 12,5-25J,, flexible fibre 300-320 em | None of the patients required analgesic therapy | Postoperatively, three patients experienced odynophagia, impaired mouth opening, and submandibular swelling, which subsided in 2-3 days. | For up to 6 years. | It Is a valid alternative to traditional surgery |
| Azaz et al. (1996) [18] | Case series | 49 cases, 26 M ,23W: (15Y-18Y) |
Wharton’s duct :47 Stensen duct: 2 |
CO2 laser | 1020 8W CW | Four patients had antibiotics for 5 days | Four patients experienced discomfort | 7 days after for the follow up. And after one years. | Excellent results with no bleeding, minimal scarring, and little discomfort. Sialadenectomy should be considered for patients who suffer from recurrent symptoms. |
| Barak et al. (1991) [19] | Case series | 21 cases, 14M, 7W. |
Wharton’s duct: 10 patients.Submandibular/sublingual glands:8 patients.Stensen duct: 3 patients. | Co2 laser | 5W/10W in continuous mode | - | No complication | Three weeks. | Complete healing after three weeks |
| Barak et al. (1993) [20] | Case series | 6 cases, 2M (22-54 Y) 4W (19-32 Y) |
Wharton’s duct: 4 patients. Submandibular gland: 2 patients. |
Co2 laser | 10W in continuous mode | - | No complication. Postoperative Swelling in 2 patients (Hilus of submandibular gland) | 1 year. | Complete healing in 7 to 20 days |
| Yang et al. (2011) [21] | Case series | 19 cases, 12M, 7FW (8- 54 Y) |
In the posterior half of Wharton’s duct. | Co2 laser | 4-6W in continuous mode | - | One patient developed ranula formation after laser surgery | 1-3,5 years. | The results suggest that transoral CO2 laser sialolithectomy is a simple, safe, and low-complication procedure suitable for outpatient treatment. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



