
Submitted:
07 August 2024
Posted:
08 August 2024
You are already at the latest version
Abstract
Extended Reality (XR) technologies—encompassing Virtual Reality (VR), Augmented Reality (AR), and Mixed Reality (MR)—merge elements of the physical world with virtual environments, revolutionizing various sectors, including healthcare. This paper explores the transformative potential of XR when combined with advanced digital tools to enhance therapeutic practices for individuals with disabilities or social isolation. Emphasizing the pivotal role of healthcare professionals, particularly nurses, the study investigates how these experts can effectively integrate XR technologies to maximize therapeutic benefits. The research includes a pre-implementation phase that assesses the knowledge and acceptance levels of both healthcare professionals and the general population. This foundational study highlights the potential of XR in expanding access to artistic and recreational activities, drawing insights from efforts by the Opera di Santa Maria del Fiore (Florence) to democratize timeless artistic experiences. The findings underscore the im-portance of defining key terms and understanding stakeholder readiness before full-scale implementation.
Keywords:
Extended reality (EX)
; Therapeutic practices
; Nurses
; Physiotherapists
; Recreational activities
; Accessibility
1. Introduction
Extended Reality (XR) technologies, including Virtual Reality (VR), Augmented Reality (AR), and Mixed Reality (MR), blend physical world elements into virtual environments [1] and a lot of sectors, including healthcare, have been significantly impacted by technological advancements. Innovative therapeutic approaches are now a reality that expands the possibilities of care. When combined with advanced digital tools, XR has the potential to significantly improve the lives of patients. In this paper we will focus on people with disabilities or experiencing social isolation. Healthcare professionals, especially nurses, play a crucial role in effectively integrating and optimizing these technologies for maximum therapeutic benefit due to their profound understanding of patient care. Prior to proceeding, a precise definition of all terms to be utilized is essential.
1.1. Terminology
Extended Reality
Extended Reality (XR) is an umbrella term that embraces all immersive technologies that extend the reality we experience with our senses by either blending the virtual and “real” worlds or by creating a fully immersive virtual environment. XR includes Virtual Reality (VR), Augmented Reality (AR), and Mixed Reality (MR) [2]. Figure 1 helps us understand the meaning of XR, its components, and the differences between them.
On the left side of Figure 1 there is reality we perceive through our senses. On the right side there is XR XR with all its components, which feature both real and virtual objects in a real-world context in varying proportions, leading up to Virtual Reality (VR), which presents virtual objects in a completely virtual context. On this “ reality-virtuality continuum” [3] after reality, AR is found. AR is a mode offers the user an enhanced perception of the surroundings [4], by adding virtual objects or digital content to the perceived reality. An example of AR are smartphone devices. AR can be experienced by using smartphones’ camera and Apps, that may add additional information to the content the camera is capturing [5]. MR is the result of VR and AR, and it still presents digital and physical element that interact in the user perception [4]. VR, at the end of the continuum, offers the user an alternative to perceiving reality by immersing them in a virtual environment populated with virtual objects.
Extended Reality in Therapeutic Practices
There is a wide range of versatile potential applications for VR systems in the healthcare sector [6]. Application targets are multiple, throughout the entire reality-virtuality continuum: AG is largely used in the field of cognitive rehabilitation, for example assisting cognitive impaired individuals generating prompts and reminders, thereby supporting daily activities and improving cognitive function [7]. AR is especially important for facilitating or enhancing social interactions, helping for example individuals with autism or social anxiety by providing real-time social cues and interaction guidelines [7,8,9]. This type of intervention has proven to be especially significant in treating children with autism spectrum disorder (ASD), emerging as a promising solution[11]. Besides benefiting patients, AR also provides significant support to healthcare professionals. One need only consider its use in their training: simulation, guided support and reminders [11,12] are just some of its uses. MR has the same importance in healthcare professionals’ training [14] and patient’s training [15], and it is especially important in pain management, along with VR. Distracting patients by immersing them in an alternative, calming and engaging scenario really shifts the focus away from the painful sensation, even to the extent of replacing the use of painkillers [15,16,17]. VR: its applications are vast, ranging from the treatment of patients with pruritus [19] to reducing anxiety at the dentist’s office to being used during cardiac surgery [20]. It is also widely used to distract patients during chemotherapy. As Burrai and colleagues [21] explain, VR ”is capable of quickly and effectively producing a positive influence on the psychosomatic axis, …, as it isolates sensory channels from the negative external environment and enables an experience of being physically and psychologically present within virtual scenarios”. EX has a real transformative impact [22] in the healthcare sector. Here some more example: (i) Parkinson disease (PD) is a complex, non-curable, and progressive neurological disease affecting different areas of the human nervous system. This condition not only restricts the movement of patients, but can lead to isolation from the rest of the world [23]. The loneliness resulting from this kind of condition, and from many others leading to reduced mobility and, consequently, limited ability to leave one’s home, finds relief in the use of different EX solutions. Studies [22, 23,24,25,26] show that joining digital communities reduces loneliness, isolation, sense of stigma. Participation is attainable even for those who struggle with keyboard and mouse use or remembering passwords and navigating complex applications due to their physical and cognitive impairments. Indeed, one interesting aspect of EX in the context of healthcare practice is that these devices necessitate new paradigms for human-computer interaction. Traditional interaction requires physical contact with a keyboard and mouse or touchscreen to interact with a computer. In this context, the body can really be left behind to have full experience elsewhere in virtual scenarios. (ii) Social connection and life administration can be enhanced by the use of EX modes for independent-living older adults [28]. (iii) Older people or impaired people can live in “sensor-embedded houses or smart houses” [29], (iv) and a large part of the population can benefit from the utilization of XR technology within sleep health [30]: these authors found that the use of these technologies can be useful in memory reactivation, and that they are well accepted both by patients [31] and healthcare professionals [32]. (v) Agoraphobia and a wide range of treatment for anxiety disorders: these conditions significantly impact individuals’ lives by directly affecting their quality of life [33]. Immersive, controlled, and accessible therapeutic environments created by EX can facilitate gradual exposure to feared situations in a safe and controlled manner [34], so to treat various kind of phobias (e.g., public crowded places, open spaces, etc.) and anxiety disorders. (vi) Rehabilitation for immobility that may derive from trauma, stroke [35], PD, prolonged bed rest in general. Bedridden patients are exposed to all types of frailty, both physical and psychological [36], and they can benefit from EX intervention in the rehabilitation pathway as well in the brain stimulation one. Of particular importance is post-stroke rehabilitation, which is effectively conducted at patients’ homes by physiotherapists [37], that find wearable devices as an emerging and effective option for patient’s recovery. Despite this broad positive outlook of possibilities and future scenarios, there is still the emerging need to fully understand the limitations, risks, and challenges of the technology [38]. There are aspects that must be taken into serious consideration when identifying individuals eligible for this type of therapy, during the administration itself, and in the awareness that unwanted effects may occur. It is the healthcare professionals’ knowledge of the patient and their characteristics, as well as their ability to explain the potential negative effects to the patient, that makes them indispensable for the effective integration of these tools into their therapy. Patients may encounter overstimulation, auditory problems, or motion sickness, and face risks such as addiction, unintended visual and physiological effects, and privacy concerns [37].
Advanced ICT in Healthcare
Advanced information and communication technologies (ICT) offer possibilities for patient care, administrative efficiency, and medical research. Compared to traditional systems, advanced ICT combine telecommunications, computing, and software. These advanced ICT systems allow for faster and higher-volume data processing and transfer [39]. The best-known application is telemedicine. Telemedicine[40] uses ICT to provide remote clinical services, which is particularly beneficial for socially isolated individuals or those with mobility issues. It includes video consultations (i.e., with specialists or other professionals that physically can be elsewhere, even in foreign countries or communications patient-to-healthcare deliverer from home, reducing travels frequency to healthcare facilities), remote monitoring, and digital health records. These last two are of particular importance when addressing the need of accessibility to all the information regarding a patient. The digital health record is a real-time repository of medical history of a person, that enables continuity of care, as no episode or information gets lost, enabling data-driven decision-making, and contributing to cost savings. Remote monitoring uses wearable devices and sensors that can track patients’ vital signs and transmit data to healthcare providers for continuous monitoring and timely interventions. Before describing the potential applications of XR for remote artistic and recreational activities, we focus on the specific and multifaceted role that nurses can play within this new realm of possibilities.
The Role of Nurses in the Digital Health Revolution
Nurses, among all the healthcare professionals, are the linchpin connecting patients with the complex world of healthcare technology [41]. Their role in the integration of XR and ICT is pivotal in ensuring that these technologies are used effectively, ethically, and beneficially for patients. They can be identified as the “human face “of XR and ICT in healthcare. Nurses are crucial in every healthcare system globally [42], as they provide customized care to patients, of whom they deeply understand needs, concerns and preferences. Their clinical knowledge is in this regard pivotal in assessing the suitability of XR and ICT applications for individual patients, and because they can ensure not only a safe, but also an effective use of technologies. Nurses are “agents of change”[43], they build strong therapeutic relationships with patients, which are essential for establishing trust and encouraging technology adoption, ensuring that ethical considerations are prioritized in its use. All the benefits that technology offers are available and utilized by nursing professionals as well: they can be enabled to deliver care remotely, reaching patients in underserved areas or those with mobility limitations, and reduce feelings of isolation. Furthermore, nurses have always incorporated complementary and alternative therapies [44] in their practices, demonstrating mental flexibility in adopting any practice deemed effective for treating the various conditions of patients, showing an overall consideration for their well-being.
This paper is organized as follows: after providing a full-bodied background context and forays into particular aspects, a description of possible use-cases is provided, along with the results of a survey to the general population and to nurses and physiotherapists on the potentialities of XR for remote artistic and recreational activities intended for impaired and socially isolated people (e.g., immobilized due to traumatic outcomes or underlying medical conditions, with anxiety issues such as agoraphobia, etc.), people with mobility problems at home (e.g., very elderly individuals with limited mobility or those affected by mental impairments, etc.), people undergoing treatments at home and/or in the hospital (e.g., chemotherapy, dialysis, etc.). Physical therapists have been involved because they extensively use new technologies in their practice [44, 45, 46] and can help identify patients who might benefit from them.
2. Materials and Methods
To support the possibility of introducing innovative interventions for the well-being of patients, a brief survey was conducted on the knowledge of XR and its acceptability by both the general population and healthcare professionals, specifically nurses and physiotherapists, with specific reference to the content that these technologies could offer. In particular, focusing on involving people in cultural activities to enhance therapeutic practices from a psychological side, some preliminary application scenarios have been identified thanks to the involvement of OPA, Opera di Santa Maria del Fiore (hereinafter referred to as the Opera) as a content provider. The Opera was founded by the Florentine Republic in 1296, with the participation of the city’s ecclesiastical authorities, to oversee the construction of the new Cathedral and its Bell Tower. The Opera is established as a private law legal entity subject to prefectural supervision and, since 1998, has assumed the status of a non-profit organization (Onlus). Among its institutional objectives, it pursues the protection, promotion, and enhancement of the religious, civil, cultural, and historical functions of the Cathedral of Santa Maria del Fiore, as well as all its other monuments and buildings. The Opera includes, beside the Opera del Duomo Museum, the Santa Maria del Fiore Cathedral, with its Dome and Giotto’s bell tower and the Baptistry as well. The Opera is distinguished by its commitment to accessibility, providing innovative tools such as the original podcast series curated by the Opera di Santa Maria del Fiore, available on Spotify® and other podcast. Recently, accessibility to cultural heritage has seen similar initiatives, for example, by the National Archaeological Museum of Naples (MANN) [48]: video tutorials, video tours, and autism-friendly VR experiences for children have been produced and made available to the public. Evidence of the benefits of inclusion in visual art environments are known for a long time [49], not only for impaired people but for the general social inclusion as well [27,49]. The analysis of the data gathered through the surveys testify both the users’ need of inclusive experiences and the interest in participating in cultural activities. This allowed the selection and definition of some specific use cases that potentially can be tested in the near future in order to validate the ideas expressed in this paper empirically.
Selected Use Cases for XR Application
Five Specific Scenarios Were Defined for XR Application within the Context of the Opera:
2. Autonomous Virtual Museum Exploration
This functionality provides an exceptional opportunity for independent exploration of the Opera del Duomo Museum galleries. Visitors have the freedom to navigate virtual galleries or digitized sections of the museum at their own pace, selecting content according to their personal interests. This feature also permits those who have previously engaged in a guided virtual tour to revisit specific areas of the museum autonomously, thus allowing for a deeper engagement with the exhibits. By offering this degree of autonomy, the museum significantly enhances the visitor experience, facilitating a more personalized and self-directed journey through its collections. This option is already available and can be found on the Opera’s website.
3. Virtual Interaction with Artworks
The virtual tour of the Opera del Duomo Museum can also offer an advanced and immersive experience by enabling detailed interaction with individual artworks. By providing virtual proximity to artworks, visitors can thoroughly examine these pieces, transcending the physical distance constraints imposed for the safety and preservation of the objects. Users can access comprehensive content related to the artworks, including in-depth information about the artists, historical context, and techniques used in their creation. Each sculpture within the museum will be digitized to obtain a three-dimensional model, which can be explored in full relief, even from perspectives that are physically inaccessible in the real space. Paintings will be scanned and represented within various frames distributed throughout the virtual exhibition space. Additionally, digital visualizations will facilitate the representation of lost or damaged elements, such as, for example, the reconstruction of a missing sword from a statue. Furthermore, both 2D and 3D animations, along with specific auditory elements for each painting, will be incorporated. A close-up interaction with artworks would encourage visitors to pay attention to specific details, understand their meaning, and relate to the overall artwork, contributing to guide the audience in learning how to observe and understand art. Thus, the creation of educational workshops will facilitate a more intuitive and accessible understanding of the museum’s collections and significantly enhance the overall visitor experience. Figure 2 provides a visual representation of this possibility, illustrating a scenario where a person with mobility issues can use a VR headset to engage in immersive interactions with individual artworks.
4. Virtual Hub for Community Involvement and Artistic Innovation
The virtual model of the Opera del Duomo Museum may incorporate a dedicated room designed as a virtual literary café, intended to facilitate both remote engagement and active participation in a broad spectrum of artistic events. This virtual space would serve as a platform for the exploration and discussion of artistic works, including events that provide insights into the history of a piece or its creation techniques. Additionally, it would host a variety of cultural activities such as virtual book presentations, online concerts, and thematic discussions on shared interests. The primary goal of this virtual café is to connect individuals with common interests, promoting meaningful dialogue and fostering social interaction and inclusivity. By doing so, it aims to alleviate feelings of loneliness and isolation. Figure 3 provides the visual representation of this possibility, illustrating a scenario where remotely connected people can use a VR headset to engage in a virtual community, in which the moderating presence of a virtual expert enables a discussion on the topic of interest.
5. Virtual Insights into the Cultural Heritage of Santa Maria del Fiore Cathedral and Baptistery
A virtual immersion into Florence’s wonders offers a unique and unparalleled experience. Participants can enjoy virtual tours of the ascent to the Dome and Giotto’s Bell Tower of the Santa Maria del Fiore Cathedral, using immersive 360° technology, as displayed in Figure 4. This provides a singular opportunity to admire the panoramic views from above without physical constraints. Additionally, detailed 3D immersive guided videos of the Baptistery’s panels allow for an in-depth exploration of its intricate art and craftsmanship, offering insights that might be missed in a traditional visit. The experience digitally reconstructs the virtual space of the bas-relief, explored following the narrative sequence, and is enhanced by a narrating voice and the animation of some elements. This immersive experience enhances accessibility, providing educational value and convenience to a global audience, and fostering a deeper appreciation for Florence’s rich cultural heritage. When designing a virtual platform, several factors should be considered, including, in the first instance, the heterogeneous target audience in terms of age, gender, physical or cognitive disabilities, and technological skills. To ensure accessibility, it is essential to implement user-friendly interfaces that enable easy navigation for individuals of all ages and technical abilities. Enjoyment of artworks should be facilitated by a combination of videos, graphics, illustrations, animations, sound, and storytelling, all tailored to address each patient’s specific needs and health conditions, to reach the widest possible audience. One potential advantage of this platform should lie in its ability to provide immersive experiences via filter-based searches. Users could select specific virtual content according to their personal interests and psychological state. Certain content may be categorized by the emotional responses it elicits, potentially making it more suitable for either relaxation or stimulation, depending on the user’s needs. Furthermore, immersive solutions could be customized to accommodate individuals’ deficits and remaining abilities, thereby offering not only a service for those experiencing loneliness and social isolation but also a diverse range of options tailored on specific health conditions. This personalized approach should consider both the patient’s health status at the initial interaction with the technology as well as the progression of the therapeutic treatment. Finally, providing various scenarios with different levels of engagement, such as guided tours versus self-exploration, can address the varying degrees of interest in immersive activities. Many individuals, particularly the elderly and those with limited technological skills, may initially have concerns about new technologies and might prefer starting with less immersive experiences. Gradually, as they become more familiar with the technology, they may be more inclined to engage in more immersive activities.
Before proceeding to the real-life test, it was necessary to picture the knowledge and acceptance level, both of healthcare professionals and general population. Two different digital surveys were sent out to respondents using the snowball sampling method. A small group of people was initially contacted by the authors: people who meet the inclusion criteria (being nurses, physiotherapist, and general population) and asked to answer the survey and to recruit other participants, creating a recruiting chain. This method is particularly useful when trying to reach groups of population of whom we do not have a comprehensive list. This is the message the respondents found on the entry page, which they reached via WhatsApp link: “Thank you for considering participation in our survey on extended reality. The purpose of this survey is to gather insights and data for a research study that aims to explore the impact and applications of extended reality technologies. Your participation is entirely voluntary, and you may choose to withdraw at any time without consequence. Please be assured that all responses will be collected anonymously; no personal identifiers will be linked to your answers, ensuring complete confidentiality. The data will be used solely for research purposes and will contribute to a published study on the subject. By proceeding with the survey, you consent to participate under these terms”.
Figure 4.
Virtual insight via VR headset into two of the most visited Florence sites: the Dome and the Baptistery od Santa Maria del Fiore. Photographic Credits: Fabio Muzzi and Antonio Quattrone, courtesy of Opera di Santa Maria del Fiore.
Figure 4.
Virtual insight via VR headset into two of the most visited Florence sites: the Dome and the Baptistery od Santa Maria del Fiore. Photographic Credits: Fabio Muzzi and Antonio Quattrone, courtesy of Opera di Santa Maria del Fiore.

3. Results
General population: A total of 137 people were invited, and 33 completed the questionnaire. The overall completion rate was 24.1%. The respondents answered some general questions allowing us to illustrate the sample from a descriptive point of view, as depicted in Table 1:
The sample consists predominantly of individuals in the 20-30 years (30.3%) and 71-80 years (27.27%) age groups. Other age groups are less represented, with the least being the 31-40 years (3.03%). There is a significant gender imbalance, with females constituting 81.82% of the sample, compared to 18.18% males. A majority of the sample has a higher level of education, with 36.36% having a master’s degree and 24.25% holding a Ph.D. Secondary school education is the least common, represented by only 3.03%. Most participants live in urban areas (81.82%), while a smaller fraction resides in rural settings (18.18%). Most of the sample lives with their family (72.73%), while 27.27% live alone. Over half of the respondents are employed (51.52%). There is a significant portion of retired individuals (45.45%), and a very small percentage is unemployed (3.03%). Most participants leave their house daily (69.7%). A smaller group leaves often (24.24%), while very few leave sometimes or rarely (3.03% each). None reported never leaving the house. The majority rate their health as good (45.45%) or average (36.36%). A smaller group rates their health as excellent (12.12%) or below average (6.06%), with none rating it as poor. Respondents then expressed their views by answering detailed questions on their knowledge, habits and future possibilities for the implementation of different technologies. In Table 2, their responses are described.
The survey reveals a range of responses regarding participation in various activities and the use of VR and AR technologies: (i) health-related activity participation: a significant majority of respondents (48.48%) rarely have to refuse participation in activities due to health issues. Conversely, a smaller proportion (6.06%) frequently faces this challenge, with none experiencing it on a daily basis. (ii) Engagement in remote activities: the frequency of participating in remote activities from home shows that 36.36% of respondents engage in such activities sometimes, while 18.18% do so every day. In contrast, 12.12% never or rarely participate in remote activities. (iii) Awareness and knowledge of immersive experiences: awareness of immersive experiences for remote cultural and recreational activities varies, with 45.45% sometimes having heard of these technologies, while 27.27% have never heard of them. Knowledge about the benefits of remote immersive experiences is generally low, with 37.5% rating it as poor or acceptable. (iv) Interest in specific immersive experiences: virtual tours and digital environments are the most appealing types of immersive experiences, with 78.79% of respondents expressing interest. Access to 3D video libraries and simulations or interactive games also show notable interest, while immersive podcasts for deaf people are the least favoured. (v) Experience with VR and AR technologies: usage of VR or AR technologies for remote participation is relatively low, with 71.88% of respondents having never used them. Among those who have, experiences are mixed, with ratings ranging from very unsatisfactory to very satisfactory. (vi) Training and research participation: most respondents have not participated in training sessions on VR or AR technologies, though there is a moderate interest in receiving such training (43.75% moderately interested). Interest in participating in research studies on these technologies is also moderate, with 40.63% showing moderate interest. (vii) Potential benefits and usage: regarding the potential benefits of using VR or AR technologies, most respondents are open to using them if available. There is a general agreement that these technologies could enhance engagement and motivation in therapeutic contexts, with 43.75% agreeing that such experiences could be beneficial for health. (viii) Interest in virtual cultural experiences: respondents show considerable interest in virtual cultural experiences. Virtual museum tours, interactive explorations, and independent museum visits from home are of particular interest, with the highest levels of interest in exploring and experiencing cultural sites virtually.
Healthcare Professionals
A total of 380 people were invited, and 89 completed the questionnaire. The overall completion rate was 23.4 %. The respondents answered some general questions allowing us to illustrate the sample from a descriptive point of view, as depicted in Table 3:
The sample consisted of healthcare professionals with diverse age ranges, genders, and years of work experience. The age distribution was as follows: 6 participants (6.74%) were between 20-30 years old, 20 participants (22.47%) were between 31-40 years old, another 20 participants (22.47%) were between 41-50 years old, 36 participants (40.45%) were between 51-60 years old, and 7 participants (7.87%) were 60 years old or older. Regarding gender, most of the sample were female, accounting for 67 participants (75.28%), while male participants comprised 22 (24.72%). In terms of work experience, 16 participants (17.98%) had 0-10 years of experience, 23 participants (25.84%) had 11-20 years, and 50 participants (56.18%) had 21-30 years of experience. The professional profiles of the participants were predominantly nurses and physiotherapists. Specifically, 53 participants (59.55%) identified as nurses, while 36 participants (40.45%) were physiotherapists.
Respondents then expressed their views by answering detailed questions on their knowledge, habits and future possibilities for the implementation of different technologies. In Table 4, their responses are described.
The answers reveal that: (i) a significant portion of respondents (48.86%) have sometimes heard of VR or AR technologies enabling remote involvement in immersive cultural and recreational activities, while a smaller proportion (10.23%) report having heard of these technologies very often. The awareness about the use of these technologies specifically for remote patient involvement in cultural and recreational activities is somewhat lower, with 40.91% having heard of it sometimes and only 4.55% very often. (ii) Respondents generally perceive their knowledge of the potential benefits of remote involvement in immersive activities to be poor, with 61.80% rating their knowledge as either very poor or poor. Only 25.84% rate their knowledge as good or very good. (iii) Respondents highlighted various potential benefits of remote participation, including increased access for individuals with severe motor limitations, ease of access from different locations, and opportunities to experience virtual environments. Benefits mentioned also include enhanced cognitive abilities, mood improvement, and facilitation of social interaction. (iv) The most favoured type of immersive experience is virtual tours and digital environments (67.05%), followed by simulations and interactive games (45.45%). VR headsets (47.73%) and access to 3D video libraries (32.95%) also show significant interest. (v) Most respondents (58.62%) have never used VR or AR technologies for remote cultural and recreational activities, and 33.71% rate their current knowledge of these technologies as very poor. Evaluation of their experience with these technologies varies, with a majority finding it either satisfactory or neither satisfactory nor unsatisfactory. (vi) A substantial proportion (74.16%) of respondents have never participated in workshops or training sessions on VR or AR technologies. Interest in receiving training is relatively high, with 62.82% being either very or extremely interested. Similarly, 55.06% express interest in participating in research studies related to VR and AR technologies. (vii) If patients had access to VR or AR technologies, 78.41% of respondents would recommend their use. Additionally, 75% of respondents believe that using these technologies for remote participation could be enjoyable for them. (viii) A majority (65.91%) are confident in their ability to use VR or AR technologies to support their patients, with 65.68% believing that such technologies would enhance their engagement and motivation during therapeutic processes.
4. Discussion
This pre-implementation study originates from the understanding of the possibilities that the Opera has generated in its effort towards making timeless artistic wonders more accessible. Some key findings emerge from the surveys administered to the general population and healthcare professionals. Both surveys revealed varying levels of familiarity with VR and AR technologies. The general population displayed a moderate awareness of these technologies. Conversely, healthcare professionals showed a broader range of familiarity, but generally possessing limited knowledge about their specific applications. Benefits deriving from these tools are not clear, even if both groups believe that they exist and need their attention. Indeed, they identify as possible advantages “increased accessibility”, “cognitive stimulation” and “social interaction”. The positive attitudes towards VR/AR technologies among healthcare professionals and the general population suggest potential for these tools to be integrated into therapeutic and recreational settings. For healthcare professionals, this could mean incorporating VR/AR into patient care plans, while the general population could benefit from more accessible immersive cultural experiences, and this result is really promising for the future of this pre-implementation work. Educational gaps appear clearly, but the high interest in virtual tours and digital environments bodes well for the future implementation of such interventions, as it does not encounter total scepticism or disinterest. Despite the promising potential, challenges remain in the widespread adoption of these technologies. Issues such as high costs, technological accessibility, and the need for specialized training for healthcare professionals must be addressed. Furthermore, the need for specialized training for healthcare professionals is a crucial consideration. Effective implementation of VR and AR in therapeutic contexts will require ongoing education and support to ensure that practitioners can leverage these tools effectively. Addressing these challenges will be essential to achieving widespread adoption and maximizing the benefits of VR and AR technologies.
5. Conclusions
VR has undergone a transition in the past few years that has taken it out of the realm of expensive toy and into that of functional technology [51]. This paper aims to provide an overview of how ICT and EX capabilities can be exploited in engaging the population and their potential inclination to use technology for healthcare purposes. This investigation has started from the analysis of the results of two surveys administered to the general population and to healthcare professionals. Regarding the limitations of this study, the main consideration is that the general population was asked to respond and not the target population, i.e., those experiencing physical or cognitive issues. Prior to the actual trial, healthcare professionals will be involved, for whom a training course on XR and its implementation possibilities in their daily clinical practice will be organised. They will also be familiarised with the use of the VR visors and will be made to live the experiences we have described in the use cases, so that they can be educated on the type of experiences and remote engagement they will propose. They will also be asked to think about the type of population they will select in terms of clinical and feasibility, with a focus on these possible issues: “VR sickness”, that may originate from the fact that some individuals may experience discomfort or nausea when using VR, limiting its effectiveness [52] and the themes of privacy and security while using these tools and technology in general. In conclusion, the integration of extended reality and advanced ICT techniques into therapy offers innovative solutions to enhance the well-being of impaired and socially isolated individuals. By providing immersive, personalized, and accessible therapeutic experiences, these technologies have the potential to revolutionize traditional therapeutic practices, paving the way for a more inclusive and supportive approach to mental and physical health care. Future research and development efforts should focus on overcoming current barriers and optimizing these technologies for broader and more effective use in therapeutic settings. All future research on the topic must be consistent with research ethics, aiming to maximise benefits and minimize risks to participants.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figures from 1 to 4 and survey ptt files.
Author Contributions
Conceptualization, C.B., S.J., S.G., L.C., and M.A.; methodology, C.B., S.J., S.G., L.C., and M.A.; software, C.B., S.J., S.G., L.C., and M.A.; validation, C.B., S.J., S.G., L.C., G.S., M.S., M.A., P.Z., and L.M.; formal analysis, C.B., S.J., S.G., and M.A.; investigation, C.B., S.J., S.G., and M.A; resources, C.B., L.C., G.S., M.S., and L.M.; data curation, C.B., S.J., and S.G.; writing—original draft preparation, C.B., S.J., S.G.; writing—review and editing, C.B., S.J., S.G., and M.A.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
This study did not require ethical approval.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Acknowledgments
Authors would like to thank the Opera di Santa Maria del Fiore for the pictures and the materials shared. We would like to thank in particular Lorenzo Lucchetti, General Director of the Opera di Santa Maria del Fiore.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- C. Andrews, M. K. Southworth, J. N. A. Silva, and J. R. Silva, “Extended reality in medical practice,” Curr. Treat. Options Cardiovasc. Med., vol. 21, pp. 1–12, 2019.
- T. Piumsomboon et al., “Ex-Cit XR: Expert-elicitation and validation of Extended Reality visualisation and interaction techniques for disengaging and transitioning users from immersive virtual environments,” Front. Virtual Real., vol. 3, p. 943696, 2022. [CrossRef]
- P. Milgram, H. Takemura, A. Utsumi, and F. Kishino, “Augmented reality: A class of displays on the reality-virtuality continuum,” in Telemanipulator and telepresence technologies, 1995, vol. 2351, pp. 282–292.
- S. Dargan, S. Bansal, M. Kumar, A. Mittal, and K. Kumar, “Augmented reality: A comprehensive review,” Arch. Comput. Methods Eng., vol. 30, no. 2, pp. 1057–1080, 2023. [CrossRef]
- L. Mucchi et al., “6G Technology as Enabler of Psychophysical Well-being & Social Inclusion Services for Citizen 4.0,” in 2023 IEEE 17th International Symposium on Medical Information and Communication Technology (ISMICT), 2023, pp. 1–6.
- Halbig, S. K. Babu, S. Gatter, M. E. Latoschik, K. Brukamp, and S. von Mammen, “Opportunities and challenges of virtual reality in healthcare–a domain experts inquiry,” Front. Virtual Real., vol. 3, p. 837616, 2022. [CrossRef]
- M. Seelye, M. Schmitter-Edgecombe, B. Das, and D. J. Cook, “Application of cognitive rehabilitation theory to the development of smart prompting technologies,” IEEE Rev. Biomed. Eng., vol. 5, pp. 29–44, 2012. [CrossRef]
- S. Rasouli, G. Gupta, M. Ghafurian, and K. Dautenhahn, “Proposed Applications of Social Robots in Interventions for Children and Adolescents with Social Anxiety,” in Proceedings of the Sixteenth International Conference on Tangible, Embedded, and Embodied Interaction, 2022, pp. 1–7.
- Nojavanasghari, C. E. Hughes, and L.-P. Morency, “Exceptionally social: Design of an avatar-mediated interactive system for promoting social skills in children with autism,” in Proceedings of the 2017 CHI Conference Extended Abstracts on Human Factors in Computing Systems, 2017, pp. 1932–1939.
- Crowell, B. Sayis, J. P. Benitez, and N. Pares, “Mixed reality, full-body interactive experience to encourage social initiation for autism: Comparison with a control nondigital intervention,” Cyberpsychology, Behav. Soc. Netw., vol. 23, no. 1, pp. 5–9, 2020. [CrossRef]
- M.-V. Toma, C. E. Turcu, C. O. Turcu, S. Vlad, D. E. Tiliute, and P. Pascu, “Extended Reality–Based Mobile App Solutions for the Therapy of Children With Autism Spectrum Disorders: Systematic Literature Review,” JMIR Serious Games, vol. 12, p. e49906, 2024. [CrossRef]
- Mather, T. Barnett, V. Broucek, A. Saunders, D. Grattidge, and W. Huang, “Helping hands: using augmented reality to provide remote guidance to health professionals,” in Context Sensitive Health Informatics: Redesigning Healthcare Work, IOS Press, 2017, pp. 57–62.
- Pregowska, M. Osial, D. Dolega-Dolegowski, R. Kolecki, and K. Proniewska, “Information and communication technologies combined with mixed reality as supporting tools in medical education,” Electronics, vol. 11, no. 22, p. 3778, 2022. [CrossRef]
- J. Gerup, C. B. Soerensen, and P. Dieckmann, “Augmented reality and mixed reality for healthcare education beyond surgery: an integrative review,” Int. J. Med. Educ., vol. 11, p. 1, 2020. [CrossRef]
- C. Lopez-Espada and J. Linares-Palomino, “Mixed reality: a promising technology for Therapeutic Patient Education,” Vasa, vol. 52, no. 3, pp. 139–140, 2023. [CrossRef]
- J. Dascal et al., “Virtual reality and medical inpatients: a systematic review of randomized, controlled trials,” Innov. Clin. Neurosci., vol. 14, no. 1–2, p. 14, 2017.
- B. Mallari, E. K. Spaeth, H. Goh, and B. S. Boyd, “Virtual reality as an analgesic for acute and chronic pain in adults: a systematic review and meta-analysis,” J. Pain Res., pp. 2053–2085, 2019. [CrossRef]
- B. K. Wiederhold, K. Gao, C. Sulea, and M. D. Wiederhold, “Virtual reality as a distraction technique in chronic pain patients,” Cyberpsychology, Behav. Soc. Netw., vol. 17, no. 6, pp. 346–352, 2014. [CrossRef]
- V. Leibovici, F. Magora, S. Cohen, and A. Ingber, “Effects of virtual reality immersion and audiovisual distraction techniques for patients with pruritus,” Pain Res. Manag., vol. 14, no. 4, pp. 283–286, 2009. [CrossRef]
- J. L. Mosso-Vázquez, K. Gao, B. K. Wiederhold, and M. D. Wiederhold, “Virtual reality for pain management in cardiac surgery,” Cyberpsychology, Behav. Soc. Netw., vol. 17, no. 6, pp. 371–378, 2014. [CrossRef]
- Burrai, M. G. De Marinis, and M. Piredda, “Virtual Reality During Chemotherapy Infusion: An Innovative Intervention in Holistic Nursing Practice,” Holist. Nurs. Pract., vol. 38, no. 4, pp. 220–226, 2024.
- K. K. Hiran, R. Doshi, and M. Patel, Applications of Virtual and Augmented Reality for Health and Wellbeing. IGI Global, 2024.
- Thangavel, M. Memedi, and K. Hedström, “Information and Communication Technology for Managing Social Isolation and Loneliness Among People Living With Parkinson Disease: Qualitative Study of Barriers and Facilitators,” J. Med. Internet Res., vol. 26, p. e48175, 2024. [CrossRef]
- C. Paquet et al., “Social prescription interventions addressing social isolation and loneliness in older adults: Meta-review integrating on-the-ground resources,” J. Med. Internet Res., vol. 25, p. e40213, 2023. [CrossRef]
- M. The National Academies of Sciences, Engineering, Social isolation and loneliness in older adults: Opportunities for the health care system. National Academies Press, 2020.
- L. F. Berkman and T. Glass, “Social integration, social networks, social support, and health,” Soc. Epidemiol., vol. 1, no. 6, pp. 137–173, 2000.
- J. Holt-Lunstad, T. B. Smith, M. Baker, T. Harris, and D. Stephenson, “Loneliness and social isolation as risk factors for mortality: a meta-analytic review,” Perspect. Psychol. Sci., vol. 10, no. 2, pp. 227–237, 2015.
- M. L. Oppert, M. Ngo, G. A. Lee, M. Billinghurst, S. Banks, and L. Tolson, “Older adults’ experiences of social isolation and loneliness: Can virtual touring increase social connectedness? A pilot study,” Geriatr. Nurs. (Minneap)., vol. 53, pp. 270–279, 2023. [CrossRef]
- M. Chan, D. Estève, C. Escriba, and E. Campo, “A review of smart homes—Present state and future challenges,” Comput. Methods Programs Biomed., vol. 91, no. 1, pp. 55–81, 2008.
- Goldsworthy, J. Chawla, J. Birt, O. Baumann, and S. Gough, “Use of extended reality in sleep health, medicine, and research: a scoping review,” Sleep, vol. 46, no. 11, p. zsad201, 2023.
- X. Zhang et al., “The Impact of VR-CALM Intervention Based on VR on Psychological Distress and Symptom Management in Breast Cancer Survivors,” J. Oncol., vol. 2022, no. 1, p. 1012813, 2022. [CrossRef]
- P. Guilbaud, T. C. Guilbaud, and D. Jennings, “Extended reality, pedagogy, and career readiness: A review of literature,” in International Conference on Human-Computer Interaction, 2021, pp. 595–613.
- P. Dhunnoo, L.-C. Wetzlmair, and V. O’Carroll, “Extended reality-based therapies for the treatment of anxiety disorders: clinical impact, perceptions of patients and healthcare professionals, and comparison of modalities-a systematic review,” 2022.
- Moldoveanu et al., “Immersive phobia therapy through adaptive virtual reality and biofeedback,” Appl. Sci., vol. 13, no. 18, p. 10365, 2023. [CrossRef]
- Janssen et al., “An enriched environment increases activity in stroke patients undergoing rehabilitation in a mixed rehabilitation unit: a pilot non-randomized controlled trial,” Disabil. Rehabil., vol. 36, no. 3, pp. 255–262, 2014. [CrossRef]
- L. Šlosar, M. Peskar, R. Pišot, and U. Marusic, “Environmental enrichment through virtual reality as multisensory stimulation to mitigate the negative effects of prolonged bed rest,” Front. Aging Neurosci., vol. 15, p. 1169683, 2023. [CrossRef]
- S. F. M. Toh, K. N. K. Fong, P. C. Gonzalez, and Y. M. Tang, “Application of home-based wearable technologies in physical rehabilitation for stroke: A scoping review,” IEEE Trans. Neural Syst. Rehabil. Eng., vol. 31, pp. 1614–1623, 2023. [CrossRef]
- K. Stendal and R. D. L. C. Bernabe, “Extended Reality—New Opportunity for People With Disability? Practical and Ethical Considerations,” J. Med. Internet Res., vol. 26, p. e41670, 2024. [CrossRef]
- U. Holtgrewe, “New new technologies: the future and the present of work in information and communication technology,” New Technol. Work Employ., vol. 29, no. 1, pp. 9–24, 2014. [CrossRef]
- S. Sood et al., “What is telemedicine? A collection of 104 peer-reviewed perspectives and theoretical underpinnings,” Telemed. e-Health, vol. 13, no. 5, pp. 573–590, 2007. [CrossRef]
- M. Wynn and L. Garwood-Cross, “Reassembling nursing in the digital age: An actor-network theory perspective,” Nurs. Inq., p. e12655, 2024. [CrossRef]
- W. E. Rosa et al., “Nurses and midwives as global partners to achieve the Sustainable Development Goals in the Anthropocene,” J. Nurs. Scholarsh., vol. 53, no. 5, pp. 552–560, 2021. [CrossRef]
- M. Rafferty, “Nurses as change agents for a better future in health care: the politics of drift and dilution,” Heal. Econ. Policy Law, vol. 13, no. 3–4, pp. 475–491, 2018. [CrossRef]
- R. Lindquist, M. F. Tracy, and M. Snyder, Complementary & alternative therapies in nursing. Springer Publishing Company, 2018.
- J. Schuermans, A. Van Hootegem, M. Van den Bossche, M. Van Gendt, E. Witvrouw, and E. Wezenbeek, “Extended reality in musculoskeletal rehabilitation and injury prevention-A systematic review,” Phys. Ther. Sport, vol. 55, pp. 229–240, 2022. [CrossRef]
- L. Greci, F. Bosco, and V. Croce, “The Social and hUman CeNtered XR: SUN XR Project,” in International Conference on Extended Reality, 2023, pp. 223–231.
- X. Yu, “[DC] Limb Motion Guidance in Extended Reality,” in 2023 IEEE Conference on Virtual Reality and 3D User Interfaces Abstracts and Workshops (VRW), 2023, pp. 967–968.
- Pagliano and B. Ansaldi, “Digital Visualization and Multimedia for Cultural Heritage Accessibility: Designing ‘For All’ Video-Tours at the Archaeological National Museum of Naples (MANN),” SCIRES-IT-SCIentific Res. Inf. Technol., vol. 13, no. 2, pp. 85–102, 2023.
- J. Kennedy, “Inclusion in the museum: A toolkit prototype for people with autism spectrum disorder.” University of Oregon, Arts and Administration Program, 2006.
- V. De Luca et al., “Virtual reality and spatial augmented reality for social inclusion: the ‘Includiamoci’ project,” Information, vol. 14, no. 1, p. 38, 2023.
- M. T. Schulteis and B. O. Rothbaum, “Ethical issues for the use of virtual reality in the psychological sciences,” Ethical issues Clin. Neuropsychol. Lisse, NL Swets Zeitlinger, vol. 243, no. 80, p. 5, 2002.
- E. Chang, H. T. Kim, and B. Yoo, “Virtual reality sickness: a review of causes and measurements,” Int. J. Human–Computer Interact., vol. 36, no. 17, pp. 1658–1682, 2020. [CrossRef]
Figure 1.
Extended reality meaning, components and definitions.
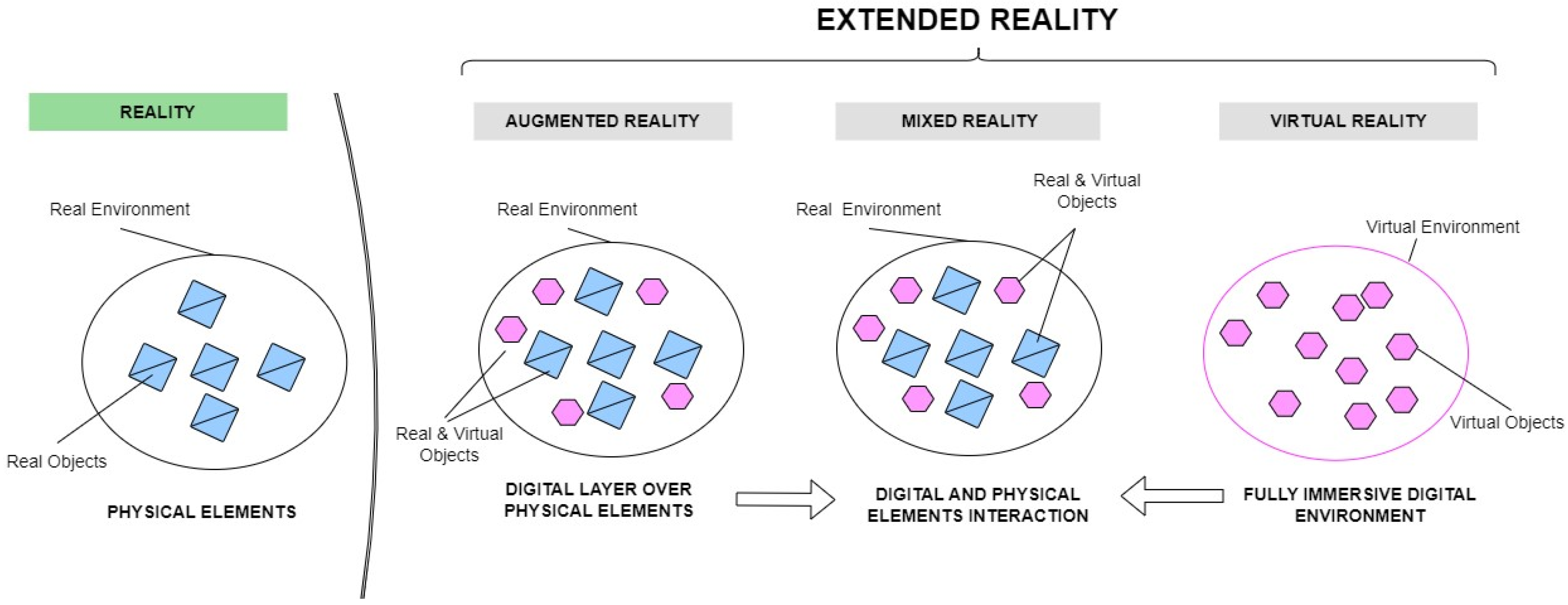
Figure 2.
Scenario representing the use of a VR headset for an immersive experience that enables interactions with individual artwork. Photographic Credits: Antonio Quattrone, courtesy of Opera di Santa Maria del Fiore.
Figure 2.
Scenario representing the use of a VR headset for an immersive experience that enables interactions with individual artwork. Photographic Credits: Antonio Quattrone, courtesy of Opera di Santa Maria del Fiore.
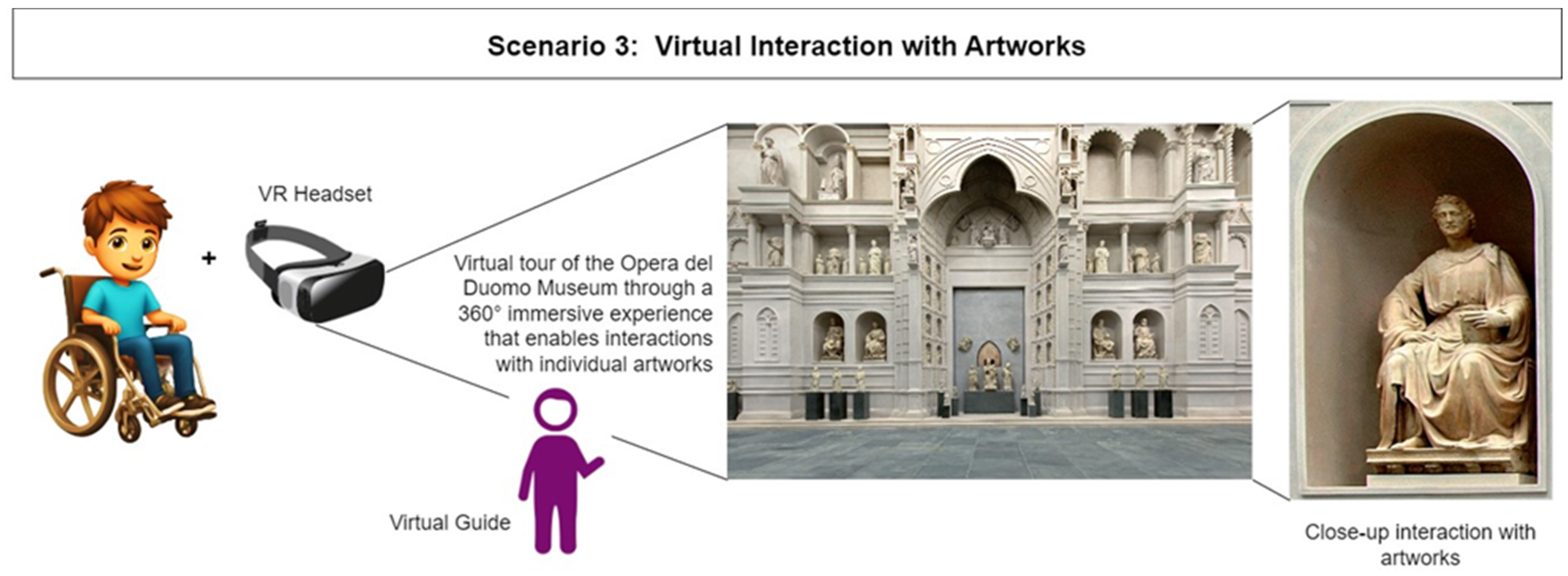
Figure 3.
VR Hub for community discussions on the artistic topic of interest. Photographic Credits: Fabio Muzzi, courtesy of Opera di Santa Maria del Fiore.
Figure 3.
VR Hub for community discussions on the artistic topic of interest. Photographic Credits: Fabio Muzzi, courtesy of Opera di Santa Maria del Fiore.
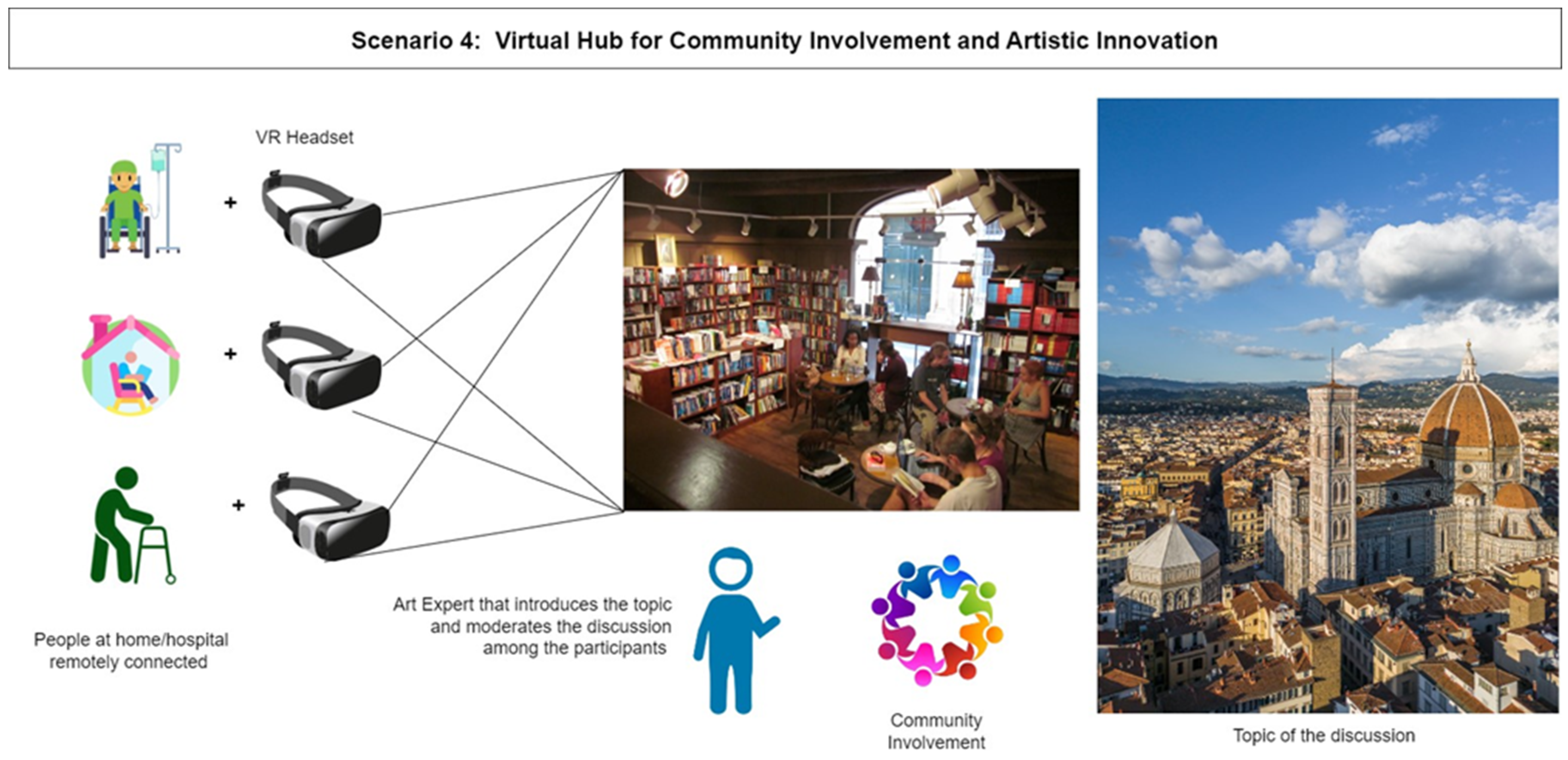

Table 1.
Description of the general population sample.
| General population sample | ||||||||||
| Age ranges | ||||||||||
| N of respondents (% of sample) | ||||||||||
| 20-30 yrs. | 10 (30,3%) | |||||||||
| 31-40 yrs | 1(3.03%) | |||||||||
| 41-50 yrs | 2(6.06%) | |||||||||
| 51-60 yrs | 4(12.12%) | |||||||||
| 61-70 yrs | 7(21,21%) | |||||||||
| 71-80 yrs | 9(27,27%) | |||||||||
| Gender | ||||||||||
| Female | 27 (81,82%) | |||||||||
| Male | 6(18,18%) | |||||||||
| Educational attainment | ||||||||||
| secondary school | 1(3.03%) | |||||||||
| High school | 10(30.3%) | |||||||||
| bachelor’s degree | 2(6.06%) | |||||||||
| Master’s degree | 12(36,36%) | |||||||||
| Ph.D. | 8 (24,25%) | |||||||||
| Living and housing context | ||||||||||
| Urban (city, large town) | 27 (81,82%) | |||||||||
| Rural (small town in the country, mountain) | 6 (18.18%) | |||||||||
| Who do you live with? | ||||||||||
| Alone | 9 (27.27%) | |||||||||
| With my family | 24 (72.73%) | |||||||||
| Employment status | ||||||||||
| Employed | 17 (51.525) | |||||||||
| Unemployed | 1 (3.03%) | |||||||||
| Retired | 15 (45.45%) | |||||||||
| How often do you leave the house? | ||||||||||
| Never | 0 (0%) | |||||||||
| Rarely | 1 (3.03%) | |||||||||
| Sometimes | 1 (3.03%) | |||||||||
| Oftentimes | 8 (24,24%) | |||||||||
| Everyday | 23 (69.7%) | |||||||||
| How would you rate your health? | ||||||||||
| Poor | 0 (0%) | |||||||||
| Below average | 2 (6.06%) | |||||||||
| Average | 12 (36.36%) | |||||||||
| Good | 15 (45.45%) | |||||||||
| Excellent | 4 (12.12%) | |||||||||
Table 2.
Answers provided by the sample “general population”.
| Do you sometimes have to refuse participation in activities of various kinds because of your state of health (difficulty in moving, pain, psychological discomfort, etc.)? | |||
| N. of respondent (% of sample) | |||
| Never | 5 (15.15%) | ||
| Rarely | 16 (48.48%) | ||
| Sometimes | 10 (30.3%) | ||
| Oftentimes | 2 (6.06%) | ||
| Everyday | 0 (0%) | ||
| How often do you participate in remote activities directly from home (online games, smartphone calls, video lectures, video conferences, etc.)? | |||
| Never | 4 (12.12%) | ||
| Rarely | 2 (12.12%) | ||
| Sometimes | 12 (36.36%) | ||
| Oftentimes | 7 (21.21%) | ||
| Everyday | 6 (18.18%) | ||
| Have you ever heard of the use of immersive experiences for remote participation in cultural and recreational activities? | |||
| Never | 9 (27.27%) | ||
| Rarely | 5 (15.15%) | ||
| Sometimes | 15 (45.45%) | ||
| Oftentimes | 4 (12.12%) | ||
| Everyday | 0 (0%) | ||
| How would you rate your current knowledge of the potential benefits of remote participation in immersive cultural and recreational activities? | |||
| Very poor | 5 (15.63%) | ||
| Poor | 12 (37.5%) | ||
| Accettable | 12 (37.5%) | ||
| Good | 3 (9.38%) | ||
| Very good | 0 (0%) | ||
| Please specify what, in your opinion, are the benefits of remote participation in immersive cultural and recreational experiences. (free text) | |||
| “Cultural enrichment, recreation, maintenance of a good mental activity” | |||
| “Deepen knowledge” | |||
| “Increase activities inclusivity. Augmented reality enables more effective and efficient services” | |||
| “It is convenient if the event is far away” | |||
| “Cultural knowledge” | |||
| “Keep interest in life alive; it can help socially” | |||
| “Knowledge, recreation, entertainment” | |||
| “The benefits can vary: it could increase knowledge and exercise memory and learning, all without undertaking demanding and exhausting trips” | |||
| “Be accessible even to those who find it difficult to leave the house” | |||
| “Do more things, have more opportunities” | |||
| “It is certainly very important for mood improvement” | |||
| “Shared multimedia recreational and cultural experiences certainly create points of convergence between people with diverse backgrounds, providing opportunities for connection, interaction, and exchange that can enhance mental and physical well-being. Immersive and remote experiences promote cognitive, emotional, and relational skills” | |||
| Which of the following types of immersive and remote cultural and recreational experiences would you be most interested in participating in? | |||
| N. of respondents (% of sample) | |||
| VR headset | 11 (33.33%) | ||
| Immersive podcasts for deaf people | 2 (6.06%) | ||
| Access to 3D video libraries | 14 (42.42%) | ||
| Virtual tours and digital environments | 26 (78.79%) | ||
| Simulations and interactive games | 12 (36.36%) | ||
| Have you ever heard of VR or AR technologies for remote involvement in immersive cultural and recreational activities? | |||
| Never | 8 (25%) | ||
| Rarely | 3 (9.38%) | ||
| Sometimes | 14 (43.75%) | ||
| Oftentimes | 6 (18.75%) | ||
| How would you rate your current knowledge of the use of Virtual and Augmented Reality technologies for remote immersive experiences? | |||
| Very poor | 9 (29.03%) | ||
| Poor | 15 (48.39%) | ||
| Accettable | 4 (12.9%) | ||
| Good | 2 (6.45%) | ||
| Very Good | 1 (3.23%) | ||
| Have you ever used VR or AR technologies to participate remotely in immersive cultural and recreational activities? | |||
| Never | 23 (71.88%) | ||
| Rarely | 4 (12.5%) | ||
| Sometimes | 5 (15.63%) | ||
| Oftentimes | 0 (0%) | ||
| If you have had this kind of experience, how would you rate your experience with Virtual or Augmented Reality technologies for remote participation in cultural and leisure activities? | |||
| Very unsatisfactory | 1 (8.33%) | ||
| Unsatisfactory | 3 (25%) | ||
| Neither satisfactory nor unsatisfactory | 3 (25%) | ||
| Satisfactory | 3 (25%) | ||
| Very satisfactory | 2 (16.67%) | ||
| Have you ever participated in workshops, seminars or training sessions on the use of Virtual or Augmented Reality technologies for remote participation in cultural and leisure activities? | |||
| Never | 26 (81.25%) | ||
| Rarely | 3 (9.38%) | ||
| Sometimes | 3 (9.38%) | ||
| Oftentimes | 0 (0%) | ||
| Very often | 0 (0%) | ||
| Would you be interested in receiving training in the use of VR or AR technologies for remote participation in cultural and recreational activities? | |||
| Not at all interested | 0 (0%) | ||
| Slightly interested | 12 (37.5%) | ||
| Moderately interested | 14 (43.75%) | ||
| Very interested | 4 (12.5%) | ||
| Extremely interested | 2 (6.25%) | ||
| Would you be interested in participating in research studies or experiments on the application of Virtual Reality or Augmented Reality technologies for cultural and recreational purposes? | |||
| Not at all interested | 2 (6.25%) | ||
| Slightly interested | 8 (25%) | ||
| Moderately interested | 13 (40.63%) | ||
| Very interested | 7 (21.88%) | ||
| Extremely interested | 2 (6.25%) | ||
| Assuming I had access to cultural and recreational content through Virtual or Augmented Reality technologies, I would intend to use them. | |||
| Strongly disagree | 0 (0%) | ||
| I disagree | 0 (0%) | ||
| Neither agree nor disagree | 15 (46.88%) | ||
| I agree | 14 (43.75%) | ||
| Strongly agree | 3 (9.38%) | ||
| I believe that the use of Virtual or Augmented Reality technologies for remote participation in cultural and recreational activities can be enjoyable for me. | |||
| Strongly disagree | 0 (0%) | ||
| I disagree | 2 (6.25%) | ||
| Neither agree nor disagree | 10 (31.25%) | ||
| I agree | 17 (53.13%) | ||
| Strongly agree | 3 (9.38%) | ||
| I believe that the use of VR or AR technologies for remote participation in cultural and recreational activities can be easy for me. | |||
| Strongly disagree | 2 (6.25%) | ||
| I disagree | 6 (18.75%) | ||
| Neither agree nor disagree | 8 (25%) | ||
| I agree | 14 (43.75%) | ||
| Strongly agree | 2(6.25%) | ||
| I believe that the use of VR or AR technologies for remote participation in cultural and recreational activities would be helpful in improving my health. | |||
| Strongly disagree | 0 (0%) | ||
| I disagree | 7 (21.88%) | ||
| Neither agree nor disagree | 11 (34.38%) | ||
| I agree | 13 (40.63%) | ||
| Strongly agree | 1 (3.13%) | ||
| If I were to participate remotely in immersive cultural and recreational activities through VR or AR technologies, I might feel more involved and motivated during a hypothetical therapeutic journey. | |||
| Strongly disagree | 0 (0%) | ||
| I disagree | 1 (3.13%) | ||
| Neither agree nor disagree | 16 (50%) | ||
| I agree | 14 (43.75%) | ||
| Strongly agree | 1(3.13%) | ||
| Would you be interested in participating in virtual guided museum tours from the comfort of your own home? | |||
| Not at all interested | 1 (3.13%) | ||
| Slightly interested | 2 (6.25%) | ||
| Moderately interested | 13 (40.63%) | ||
| Very interested | 14 (43.75%) | ||
| Extremely interested | 2 (6.25%) | ||
| Would you be interested in interacting with individual works in a virtual museum, exploring their details and discovering their history, without having to move from home? | |||
| Not at all interested | 1 (3.13%) | ||
| Slightly interested | 5 (15.63%) | ||
| Moderately interested | 12 (37.5%) | ||
| Very interested | 12 (37.5%) | ||
| Extremely interested | 2 (6.25%) | ||
| Would you be interested in independently exploring a virtual museum without having to leave home? | |||
| Not at all interested | 0 (0%) | ||
| Slightly interested | 5 (15.63%) | ||
| Moderately interested | 13 (40.63%) | ||
| Very interested | 13 (40.63%) | ||
| Extremely interested | 1 (3.13%) | ||
| Would you be interested in attending a virtual café to participate in art events such as book or art presentations without having to move from home, with the aim of discussing and interacting online with other people who share your interests? | |||
| Not at all interested | 2 (6.25%) | ||
| Slightly interested | 5 (15.63%) | ||
| Moderately interested | 13 (40.63%) | ||
| Very interested | 11 (34.38%) | ||
| Extremely interested | 1 (3.13%) | ||
| Would you be interested in immersing yourself in the wonders of the Florentine territory, such as the Dome and Baptistery, from wherever you are? | |||
| Not at all interested | 0 (0%) | ||
| Slightly interested | 4 (12.5%) | ||
| Moderately interested | 12 (37.5%) | ||
| Very interested | 13 (40.63%) | ||
| Extremely interested | 3 (9.38%) | ||
Table 3.
Description of the healthcare professionals’ sample.
| Healthcare professionals’ sample | ||||
| Age ranges | ||||
| 20-30 yrs | 6 (6,74%) | |||
| 31-40 yrs | 20 (22.47%) | |||
| 41-50 yrs | 20 (22.47%) | |||
| 51-60 yrs | 36 (40.45%) | |||
| 60 yrs and more | 7 (7.87%) | |||
| Gender | ||||
| Female | 67 (75.28%) | |||
| Male | 22 (24.72%) | |||
| How many years of work experience do you have? | ||||
| 0-10 yrs | 16 (17.98%) | |||
| 11-20 yrs | 23 (25.84%) | |||
| 21-30 yrs | 50 (56.18%) | |||
| What is your professional profile? | ||||
| Nurse | 53 (59.55%) | |||
| Physiotherapist | 36 (40.45%) | |||
Table 4.
Answers provided by the sample “healthcare professionals”.
| Have you ever heard of VR or AR technologies that enable remote involvement in immersive cultural and recreational activities? | |||||
| Never | 9 (10.23%) | ||||
| Rarely | 8 (9.09%) | ||||
| Sometimes | 43 (48.86%) | ||||
| Oftentimes | 19 (21.59%) | ||||
| Very often | 9 (10.23%) | ||||
| Have you ever heard about the use of immersive experiences for the remote involvement of patients in cultural and recreational activities? | |||||
| Never | 21 (23.86%) | ||||
| Rarely | 20 (22.73%) | ||||
| Sometimes | 36 (40.91%) | ||||
| Oftentimes | 7 (7.95%) | ||||
| Very often | 4 (4.55%) | ||||
| How would you rate your current knowledge regarding the potential benefits of remote involvement of patients in immersive cultural and recreational activities? | |||||
| Very poor | 22 (24.72) | ||||
| Poor | 33 (37.08%) | ||||
| Accettable | 11 (12.36%) | ||||
| Good | 19 (21.35%) | ||||
| Very Good | 4 (4.49%) | ||||
| Please specify what, in your opinion, are the potential benefits of remote participation in immersive cultural and recreational experiences. (free text) | |||||
| Access for individuals with severe motor and environmental control limitations. Ease of access from different locations. Open access times. Opportunity to experience environments built in virtual reality. | |||||
| Adherence to exercise programs. Activation of brain areas in a more extensive and frequent manner. Perception of a greater sense of comprehensive care. | |||||
| Experiential benefits and enhancement of cognitive abilities. Psychological and physical benefits | |||||
| Benefits for mood tone, to prevent social isolation and depression; consequently, improved quality of life for the patient, who will become more engaged and cooperative in the rehabilitation process. | |||||
| Sharing of content with the possibility to enhance skills through augmented reality. Ability to record numerous data related to choices and behaviors, and the option to analyze them post hoc for both statistical purposes and in debriefing sessions. | |||||
| Distraction from pain, inclusivity, allowing people who cannot move to see interesting things they would otherwise never experience | |||||
| Facilitate social interaction that would otherwise be compromised, with positive repercussions on the biopsychosocial sphere. | |||||
| Eliminate sedation in certain procedures, especially pediatric ones | |||||
| Management of chronic pain, management of some side effects of chemotherapy, assistance in visualizing movements for rehabilitation | |||||
| In addition to psychological benefits and mood enhancement (which are applicable to all patients), they provide cognitive and motivational stimuli that can then promote and support gestures, functions, and motor activities. Therapeutic settings can be created that are particularly stimulating, especially in cases where neurological damage is not complete or when motor control is preserved but there is a need to stimulate recruitment to improve it.With repetition, strength can be increased. | |||||
| Which of the following types of immersive and remote cultural and recreational experiences would you be most interested in participating in? | |||||
| VR headset | 42 (47.73) | ||||
| Immersive podcasts for deaf people | 15 (17.05%) | ||||
| Access to 3D video libraries | 29 (32.95%) | ||||
| Virtual tours and digital environments | 59 (67.05%) | ||||
| Simulations and interactive games | 40 (45.45%) | ||||
| How would you rate your current knowledge regarding the use of VR and AR technologies for immersive remote experiences? | |||||
| Very poor | 30 (33.71%) | ||||
| Poor | 36 (40.45%) | ||||
| Accettable | 15 (16.85%) | ||||
| Good | 6 (6.74%) | ||||
| Very Good | 2 (2.25%) | ||||
| Have you ever used VR or AR technologies to remotely participate in immersive cultural and recreational activities? | |||||
| Never | 51 (58.62%) | ||||
| Rarely | 20 (22.99%) | ||||
| Sometimes | 15 (17.24%) | ||||
| Oftentimes | 0 (0%) | ||||
| Very often | 1 (1.15%) | ||||
| How would you evaluate your experience with VR or AR technologies for remote participation in cultural and recreational activities? | |||||
| Very unsatisfactory | 10 (14.08%) | ||||
| Unsatisfactory | 14 (19.72%) | ||||
| Neither satisfactory nor unsatisfactory | 24 (33.8%) | ||||
| Satisfactory | 16 (22.54) | ||||
| Very satisfactory | 7 (9.86%) | ||||
| Have you ever participated in workshops, seminars, or training sessions on the use of VR or AR technologies for remote participation in cultural and recreational activities? | |||||
| Never | 66 (74.16%) | ||||
| Rarely | 10 (11.24%) | ||||
| Sometimes | 12 (13.48%) | ||||
| Oftentimes | 0 (0%) | ||||
| Very often | 1 (1.12%) | ||||
| Would you be interested in receiving training on the use of VR or AR technologies for the remote participation of your patients in immersive cultural and recreational activities? | |||||
| No, not at all | 4 (4.49%) | ||||
| I would be somewhat uninterested | 6 (6.74%) | ||||
| I would be moderately interested | 24 (26.97%) | ||||
| I would be very interested | 36 (40.45%) | ||||
| Yes, I would be extremely interested | 19 (21.35%) | ||||
| Would you be interested in participating in research studies or experiments on the application of VR or AR technologies for cultural and recreational purposes? | |||||
| No, not at all | 3 (3.37%) | ||||
| I would be somewhat uninterested | 10 (11.24%) | ||||
| I would be moderately interested | 27 (30.34%) | ||||
| I would be very interested | 30 (33.71%) | ||||
| Yes, I would be extremely interested | 19 (21.35%) | ||||
| If my patients had access to cultural and recreational content through VR or AR technologies, I would recommend that they use it. | |||||
| Strongly disagree | 0 (0%) | ||||
| I disagree | 2 (2.27%) | ||||
| Neither agree nor disagree | 17 (19.32%) | ||||
| I agree | 49 (55.68%) | ||||
| Strongly agree | 20 (22.73%) | ||||
| I believe that using VR or AR technologies for remote participation in cultural and recreational activities could be enjoyable for me. | |||||
| Strongly disagree | 0 (0%) | ||||
| I disagree | 4 (4.55%) | ||||
| Neither agree nor disagree | 18 (20.45%) | ||||
| I agree | 50 (56.82%) | ||||
| Strongly agree | 16 (18.18%) | ||||
| I am confident in my ability to use VR or AR technologies to support my patients during their care process. | |||||
| Strongly disagree | 0 (0%) | ||||
| I disagree | 4 (4.55%) | ||||
| Neither agree nor disagree | 26 (29.55%) | ||||
| I agree | 45 (51.14%) | ||||
| Strongly agree | 13 (14.77%) | ||||
| If I were to remotely participate in immersive cultural and recreational activities through VR or AR technologies, I would feel more engaged and motivated during my therapeutic process. | |||||
| Strongly disagree | 4 (4.55%) | ||||
| I disagree | 5 (5.68%) | ||||
| Neither agree nor disagree | 32 (36.36%) | ||||
| I agree | 36 (40.91%) | ||||
| Strongly agree | 11 (12.5%) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



