Submitted:
31 July 2024
Posted:
02 August 2024
You are already at the latest version
Abstract
Background: Tumor mutational burden (TMB) is increasingly recognized as a vital biomarker for predicting the efficacy of immune checkpoint inhibitors (ICIs) in cancer treatment. Despite its growing importance, the effectiveness of TMB as a predictive marker are well established in lung cancer and melanoma but remain ambiguous for breast and prostate cancers. Objective: This study aims to evaluate the role of TMB in predicting response to ICIs across four major cancer types—lung, melanoma, breast, and prostate—and to address the variability in TMB's predictive value in different cancers. Methods: A comprehensive review of the current literature was performed, analysing studies that investigated TMB and its association with ICI therapy outcomes in the specified cancer types. Results: The analysis reveals a strong consensus on the predictive value of TMB in lung cancer and melanoma, where high TMB levels are associated with improved clinical outcomes and better responses to ICIs. In contrast, the evidence for breast and prostate cancers is less conclusive, with variability in results highlighting the need for further research. Specifically, high TMB in these cancers does not consistently predict better responses to ICIs, suggesting that additional biomarkers or refined criteria might be necessary. Conclusion: TMB is a promising biomarker for predicting responses to ICI therapy, particularly in lung cancer and melanoma. However, its predictive value in breast and prostate cancers remains uncertain, underscoring the need for more extensive studies. Future research should focus on standardizing TMB evaluation methods and exploring additional biomarkers to improve treatment personalization and outcomes in these cancer types.
Keywords:
Tumor Mutational Burden (TMB)
; Immune Checkpoint Inhibitors (ICIs)
; Biomarkers
; Cancer Immunotherapy
; Cancer Treatment Outcomes
; Personalized Medicine
1. Introduction
The therapeutic options for many types of cancer were revolutionized by using immune checkpoint inhibitors (for short, ICIs). Generally speaking, these treatments have showed improved effectiveness and a reduced toxicity profile compared to chemotherapy. However, ICIs can initiate unique immune-related side reactions and in a small number of patients can trigger an accelerated progression of disease, called hyperprogression. Cancer patients treated with ICIs presents some different patterns of evolution, even long-term disease control and remission. Given these differences it is very important to determine a proper biomarker, in order to select the patients eligible for ICIs treatment [1].
Nowadays, the only biomarker proven to predict the benefit of the ICIs therapy is PD-L1(programmed death ligand 1). However, it is important to note that even PD-L1 is not a predictive marker for all types of malignancies treated with ICIs or combinations between ICIs and chemotherapy. Several clinical studies demonstrated that the genetic profile of the tumour can represent an effective biomarker. TMB (tumour mutational burden) measured value’s importance has been recently validated by a phase III trial whose primary endpoint was to underline that patients with high TMB have a better response to ICIs [2].
In this article we will discuss about the importance of TMB in different types of cancer and the possibility of becoming the newest biomarker for ICIs treatment.
2. What is TMB?
TMB can be defined as tumour's total number of mutations. TMB value can vary depending on the technique used to measure it [1]. Currently, the measurement is performed using NSG (next generation sequencing). Several NGS approaches are developed, and the target region ranges from genome-wide analysis (WGS- whole genome sequencing) to whole-exome analysis (WES- whole exome sequencing). Recently, the FDA approved the gene panel assay FoundationOne CDx and also authorised MSK-IMPACT for testing solid tumours for genetic alterations [3,4].
3. Testing Method: WES
Whole exome sequencing allows the exploration of all the protein-coding regions of the human genome. This technology facilitates the examination of genetic mutations associated with cancer, abnormalities that are mainly located in the exome regions. In WES the focus is on specific regions of the genome, the protein-coding fragment. This allows us to identify genetic abnormalities that will impact protein function [5]. WES is a powerful tool for the detection of various genomic changes both in coding and noncoding DNA that are influential in cancer development [6]. Changes in the exome can lead to different amino acids substitutions in protein. This event can lead to weakened activity of multiple tumour suppressors, such as APC in colorectal cancer, VHL in renal cell carcinoma or BRCA in breast cancer [7,8,9]. There are also modifications in cell cycle regulators, such as TP53 or RB1, and in repair mechanisms, which will predispose to cancer development. By measuring the TMB (mutational burden) we can monitore the activity of those systems [10,11].
Currently, there are 2 primary types of NGS methods: DNA amplification-based sequencing (Illumina, Ion Torrent) and single molecule real-time sequencing (Pacific Biosciences, Oxford Nanopore. The tissue samples analysed can be liquid-based (blood sample), freshly frozen, formalin-fixed or paraffin-embedded (FFPE). Each type of sample requires its own specific isolation kits [5].
The first step of WES is an adequate examination of the sample, made by a pathologist. The used sample should contain a proper amount of tumour cells in order to make a difference between germline and somatic mutations. It is important to keep in mind that the DNA quality deteriorates with time and also after FFPE conservation [5]. After the examinations of the samples, the data processing starts, usually with a quality control. The low-quality reads are eliminated. The next step is to align the reads to a reference genome, then a second quality control and finally, the removal of the duplecated reads. The entire process is shown in Figure 1 [5].
The main advantage of the WES technique is that it can scan the entire genome of a sample and provide information about the low-frequency mutations, that collectively can determine a phenotypic appearance [12].
4. Corelation between TMB and Immuntherapy
Nowadays, the immune checkpoint inhibitors have become the standard therapy for various solid tumors, such as melanoma, NSCLC or renal cell carcinoma [13]. The response to this therapy can be measured by a reliable biomarker, TMB, which represents the total number of mutations per coding sequence in the tumour genome. Currently, using WES to detect TMB is a widely accepted method [5]. Despite the potential of TMB as a predictive biomarker, there remains a lack of consensus regarding its definition, determination method and adequate cut-off values. For example, the Foundation Medicine has divided the TMB into 3 categories: high TMB (>20 mut/MB), intermediate TMB (6-19 mut/Mb) and low TMB (less then 5 mut/Mb) [14]. Regarding this issue, the Friends of Cancer Research have established a team whose primary goal is to standardize the use of TMB [14].
5. The interpretation and reporting the TMB value
The TMB quantification is influenced by 4 main factors [1]:
- Tumour purity: this represents the overall percentage of cancerous cell within a tumour sample. This measurement is analyst-dependent and also can lead to errors due to the fact that the used sample may not represent the tumour's region which will be analysed.
- Library construction and sequencing: this is represented by DNA fragments with a defined length which will be analysed using various bioinformatics programs.
- The pipeline used to call mutations: represents the algorithm used to remove germline variants. This is a vital step in the identification of different somatic mutations which are responsible for producing tumour neo-antigens. These antigens will be eventually recognised as non-self by the immune system.
- The capacity to extrapolate TMB values from the restricted genomic space sampled by gene panels: this step is based on the in silico analysis performed on samples to determine the concordance between WE- based TMB and panel-based TMB [1].
6. Can We Use TMB as a Predictive Biomarker?
Typically, T cells recognize different neo-antigens produced by various mutational mechanisms and presented by MHC molecules from the cancerous cell’ surface and target those cells for destruction. To evade T cells and to supress the immune system, a tumour has the capacity to produce proteins that, normally, function as checkpoints that attenuate immune responsiveness. The main reason for using immune checkpoints is to block the interaction between T cells and tumour proteins, with the aim to reactivate the immune system. Once the immune system is reactivated, T cells can differentiate normal cells from cancerous ones. This process is facilitated by the presence on the cell’ surface of immunogenic antigenes. Since these molecules arise from mutations, the more neo-antigenes that are present, the higher the TMB. This is the hypothesis that supports the idea the higher the TMB, the greater the chances of responding to a treatment based on ICIs [1]. However, there is also evidence that approximately 60% of patients with high-TMB do not have a malignancy that responds to ICIs [16].
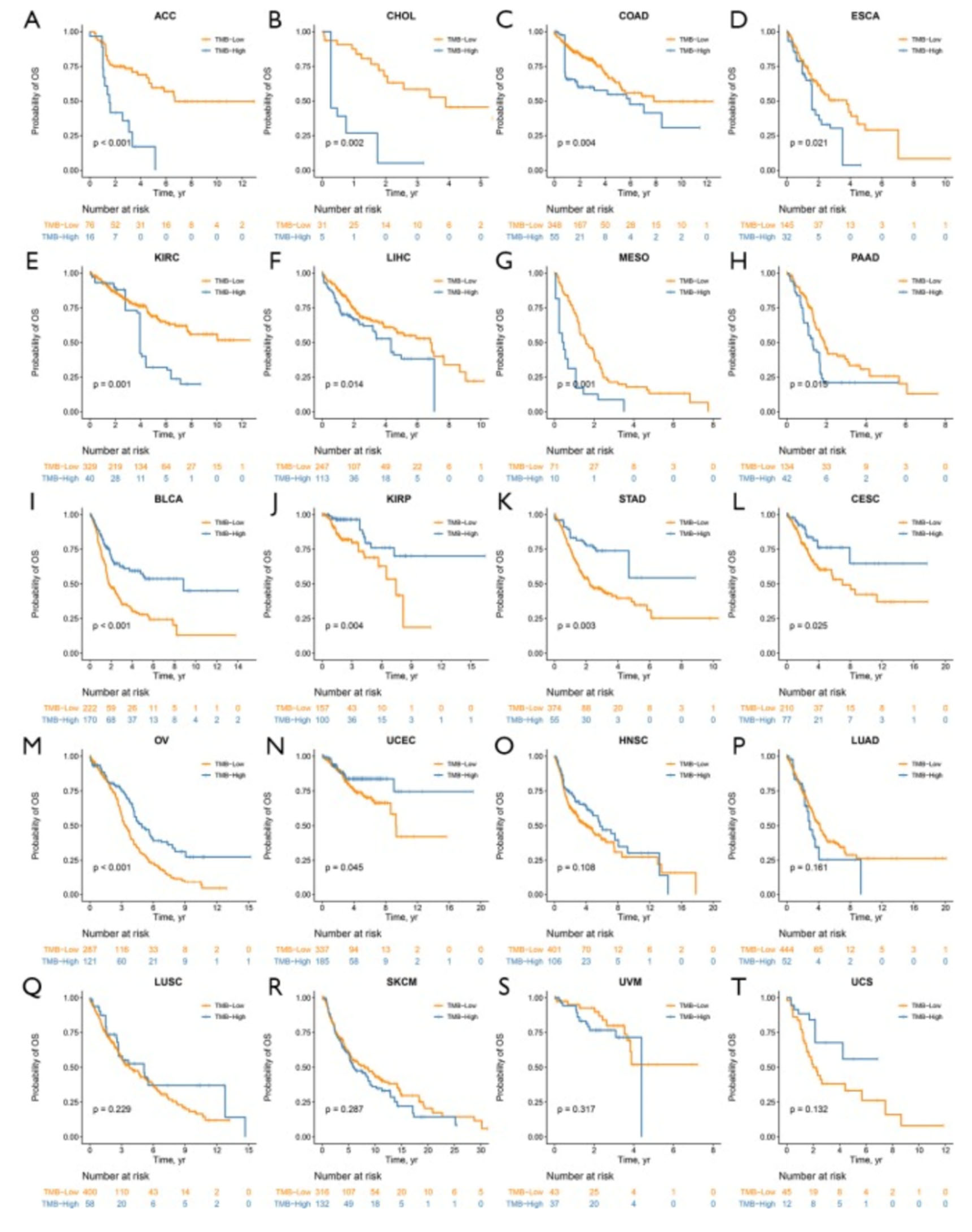
In order to determine whether TMB can be used as a predictive biomarker or not, several studies were conducted. The most informative study conducted by Hao-Xiang Wu and his team [17]. In this study 20 primary solid cancers from 6035 patients were analysed and for each type, the impact of TMB on the overall survival (OS) was evaluated using the Kaplan-Meier method. Survival analysis showed in the end that TMB has a significant impact in OS in 14 cases out of 20. According to this, the impact of the TMB was classified into 3 categories: TMB-worse group (it includes 8 types of malignancies- the patients with a high-TMB has a poorer prognostic compared with those with a lower value), TMB-better group (6 types of cancers- the patients with a higher-TMB has a better prognosis and a decreased mortality rate) and the TMB-similar group where the value of TMB didn't have an impact on OS [17,18].
Figure 2.
The inverse probability of treatment weighted Kaplan-Meier survival curves of the impact of tumor mutational burden (TMB) on overall survival. High TMB was associated with worse survival in adrenocortical carcinoma (A), cholangiocarcinoma (B), colon adenocarcinoma (C), esophageal carcinoma (D), kidney renal clear cell carcinoma (E), liver hepatocellular carcinoma (F), mesothelioma (G) and pancreatic adenocarcinoma (H). While high TMB predicted better prognosis in bladder urothelial carcinoma (I), kidney renal papillary cell carcinoma (J), stomach adenocarcinoma (K), cervical squamous cell carcinoma and endocervical adenocarcinoma (L), ovarian serous cystadenocarcinoma (M), and uterine corpus endometrial carcinoma (N). In head and neck squamous cell carcinoma (O), lung adenocarcinoma (P), lung squamous cell carcinoma (Q), skin cutaneous melanoma (R), uveal melanoma (S) and uterine carcinosarcoma (T), TMB did not have a significant impact on overall survival [17].
Figure 2.
The inverse probability of treatment weighted Kaplan-Meier survival curves of the impact of tumor mutational burden (TMB) on overall survival. High TMB was associated with worse survival in adrenocortical carcinoma (A), cholangiocarcinoma (B), colon adenocarcinoma (C), esophageal carcinoma (D), kidney renal clear cell carcinoma (E), liver hepatocellular carcinoma (F), mesothelioma (G) and pancreatic adenocarcinoma (H). While high TMB predicted better prognosis in bladder urothelial carcinoma (I), kidney renal papillary cell carcinoma (J), stomach adenocarcinoma (K), cervical squamous cell carcinoma and endocervical adenocarcinoma (L), ovarian serous cystadenocarcinoma (M), and uterine corpus endometrial carcinoma (N). In head and neck squamous cell carcinoma (O), lung adenocarcinoma (P), lung squamous cell carcinoma (Q), skin cutaneous melanoma (R), uveal melanoma (S) and uterine carcinosarcoma (T), TMB did not have a significant impact on overall survival [17].
7. Next we will evaluate the association between TMB and different types of cancers: melanoma+ lung vs. prostate+ breast
7.1. Melanoma and TMB evaluation
In order to determine if the TMB’s value is associated or not with the response to PD-L1 monotherapy. Pembrolizumab and Nivolumab, 2 main PD-L1 inhibitors have drastically changed the prognosis in those patients diagnosed with melanoma. Although the patients acquire long-term responses, only 35-40% of them benefit from these treatments [18].
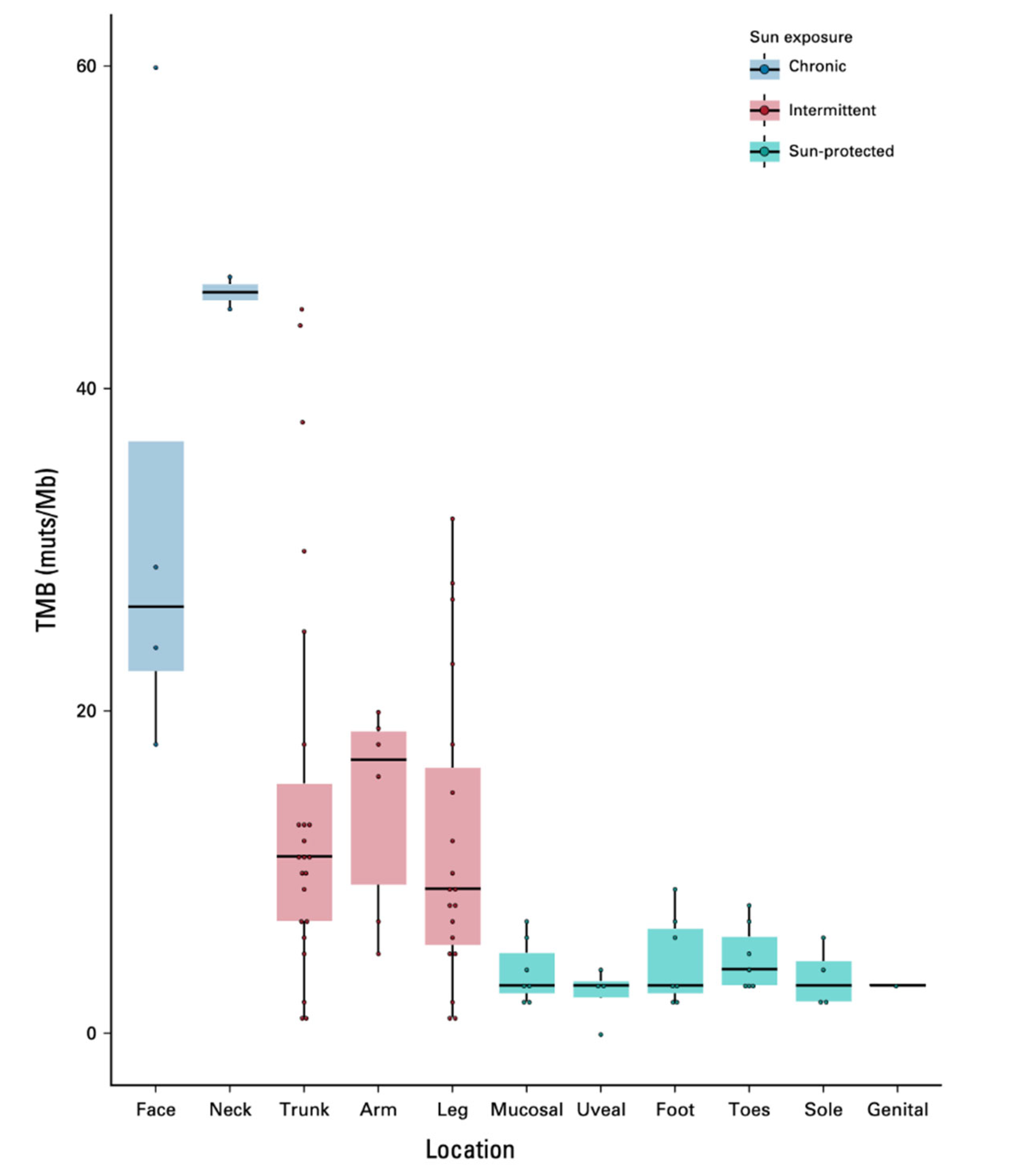
Apparently encouraging, TMB can be used as a predictive biomarker for ICIs and is likely to be included in the future treatment protocols. In Dousset et al study, 102 patients with advanced malignant melanoma were included. Their clinic-pathological characteristics, as well as tumour genomic outcomes were collected. An important aspect of this study was the patients' distribution by sun-exposure pattern in 3 different groups: chronically exposure (head and neck), intermittently exposure (arms, trunk, legs) and protected regions (feet, toes, soles, genitals, mucosal and uveal region) as is shown in Figure 3 [18]. For these patients, the TMB was analysed on the recently metastatic sample prior to administration of PD-L1 inhibitors therapy.
The analysed group was primarily composed of men (57%) and the median age at diagnosis was 59.3 years. The majority of melanomas were superficial (36% of cases), followed by unknown primary site (19.6%) and nodular type melanoma (16,8). The rarest locations were identified as: acral lentiginous (12 cases out of 102, 11,8%), mucosal melanoma (9 cases, 8,8%), uveal melanoma (5 cases, 5) and naevocytoid and desmoplastic, 1 case for each type. The BRAF mutation was evaluated as well, and a positive result was received in 34 cases. Out of 102 patients, 80 were treated with anti-PD-L1 monotherapy. TMB was assessed in 94 cases and the median value was 12,4 mut/Mb.
The primary endpoint of this study was to determine if the sun exposure may influence the TMB and consequently the ICIs treatment response. As is shown in figure 3, the TMB was significantly higher in chronically exposed areas (37,2 mut/Mb vs. 13,6 mut/Mb and 4 mut/Mb respectively).
7.2. Lung cancer and TMB evaluation
Pulmonary cancer is the most common cause of death from cancer, worldwide [19]. It includes different histologically subtypes, of which non-small cell lung cancer (for short NSCLC) represents approximately 85% [20]. Only a small percentage (20-25%) of patients with NSCLC have an early-stage diagnosis. In this case, elective resection is done with curative intent [19]. Over the last years, a better understanding of NSCLC’ biology led to the identification of various predictive biomarkers, for example EGFR, BRAF mutations or ALK and ROS1 rearrangements. Due to these findings, several target therapies have arisen. In NSCLS a targetable alteration is found in approximately 50% of patients, so for the other half it is imperative to find a biomarker to improve the clinical outcomes [21].
Nowadays, the only biomarker approved is PD-L1 expression, assed by immunohistochemistry (IHC), an inexpensive technique and performed using standard histopathology equipment. The PD-L1 expression is an important criterion during the process of splitting patients in those who will receive treatment with Pembrolizumab in monotherapy (in this case the PD-L1 cut-off is >=50%) [22] and those who will receive a dual-immunotherapy Nivolumab plus Ipilimumab (PD-L1 cut-off of 1%) [22]. The cut-off's values are explained by the multitude of assays used by investigators in clinical trials. By knowing that we can sustain the affirmation that PD-L1 is a heterogeneous variable and that is important to standardize it. For this reason, there is a need for identifications of other biomarkers, including TMB [21].
Over time, the specialized literature has presented numerous studies supporting the correlation between increased TMB and survival rate. However, there are also studies that suggest the opposite. These inconsistencies highlight the importance of large-scale analyses to universally establish the predictive value of TMB as a predictive biomarker.
To support the idea of a negative correlation, we will present the conclusions of a retrospective study performed on 136 NSCLC patients [24]. Chae et al underwent ctDNA testing in one institution, with an additional validation cohort analysed in another institution. The median age of the cohort was 69 years, 83 of them were females, 99 were ADK cases with 70,6% of them, presenting smoking history. The ctDNA TMB was measured by counting all detected mutations of the sequencing length. After the analysis, the conclusion was that a higher ctDNA TMB was significantly linked with the history of smoking (p < .05, chi-squared test). Among patients treated with immune checkpoint inhibitors (n=20), increased TMB was correlated to shorter progression-free survival (PFS) and overall survival (OS; 45 vs. 355 days; hazard ratio [HR], 5.6; 95% confidence interval [CI], 1.3–24.6; p < .01, and OS 106 days vs. not reached; HR, 6.0; 95% CI, 1.3–27.1; p < .01, respectively). There was also a small number of patients (n=12) in whom there was nonsignificant correlation. In conclusion, this study suggested that a higher TMB can be associated with a negative clinical outcome [24]. Additionally, the authors of the study emphasize the importance of large-scale studies, given that their analysis had several limitations, such as the insufficient length of the tested DNA and the use of a single type of commercially available kit for this testing.
7.3. Prostate +breast cancers and TMB evaluation
Both prostate and breast cancers have only recently incorporated immunotherapy as a treatment option. As a result, TMB testing is not as commonly performed for these two types of malignancies as it is for melanoma and lung cancer.
One of the most common malignancies seen in women is breast cancer (BC) and various biomarkers, such as ER, PR and HER2, are currently used for therapeutic decision-making [25]. Although, there are several treatments protocols for BC, almost 30% of patients develop advance disease which requires another treatment strategy. The reduced efficacy of targeted therapies and the relatively poor prognosis of advanced BC patients have underscored the need to explore new treatment approaches, including immunotherapy [26,27]. Recent studies have shown that Pembrolizumab and Atezolizumab plus Nab-paclitaxel offer promising clinical benefits for patients with advanced triple-negative BC. As an initial step, PD-L1 was proposed as a biomarker for immunotherapy efficacy, but there were some concerns about its accuracy, since testing PD-L1 has its own challenges (for example variability among assays or lack of standardization).
In BC patients, TMB has not been well characterized, but we will discuss some studies presented in literature. Mei et all analysed 62 advanced BC cases between January 2014 and June 2018. The samples were tested by Foundation Medicine and TMB by FoundationOne CDx next generation sequencing (NGS). The TMB values were classified into 3 groups: low (1-5 mut/Mb), intermediate (6-19 mut/Mb) and high (>=20 mut/Mb). The demographic features of the study included median age (53.8 years old, range 30–78), the majority were metastatic cases (49, 79.0%). Fifty-two (83.9%) cases were invasive ductal carcinoma (IDC), 6 cases (9,7%) were invasive lobular carcinoma, 2 cases (3,2%) were metaplastic carcinoma and another 2 cases were neuroendocrine carcinomas [25].
From a biomarker perspective, we note that 36 cases (58,1%) were ER positive, 38 cases (61,3%) were PR positive, 5 cases (8.1%) were HER2 positive and 22 cases (35,5%) were triple negative. Among 62 cases, 3 of them (4,8%) had high TMB, 27 (43,6%) had intermediate TMB and the majority (32 cases, 51,6%) had low TMB. Since cases with the high and intermediate groups were not so numerous, the team decided to combine these two and compared them with the low TMB group.
As a first conclusion of this study was represented by the evidence of associations between increased TILs and the group of cases with intermediate/high TMB compared with the association between TILs level and low TMB group (p = 0.0018). There were no other correlations between TMB and another clinicopathologic characteristics. There were several gene mutations evaluated in this study and their correlation the TMB level and correlation with TMB and consequently with the response to ICIs. The second most important conclusion was linked with the commonly seen genetic mutation. The most common mutation identified among the 62 cases was TP53 (59.7%), followed by PIK3CA (33.9%). Interestingly, out of the 6 BC cases with BRCA (1/2) mutations analysed, 5 had intermediate or high TMB, while only one case exhibited low TMB (p = 0.0002) [24]. 34 DNA damage repair (DDR) genes were included in the NGS panel of this study. 13 cases exhibited at least one DDR gene mutation, while the remaining 49 cases did not show any DDR gene mutations. Clinicopathologic features and TMB, as well, were compared between cases with and without DDR mutations. BCs with DDR mutations had a higher TMB compared to those without DDR mutations (12.08 vs. 6.57 average mutations; p = 0.043). There were no differences observed for other clinicopathologic characteristics and the two groups [25].
Although is one of the first studies about the impact of TMB in breast cancer, the authors sustain that more analysis should be made on this topic, due to the fact that immunotherapy is a relatively new option for BC treatment and no major data are not available in the literature. The limited sample size (n = 62) restricted the significance of this analysis. Future studies with larger cohorts are necessary to confirm these results.
Prostate cancer is the second most common type of malignancy seen in males [28]. For this type of cancer, challenges in treatment persist, particularly for castration-resistant prostate cancer (CRPC). Metastatic CRPC is associated with a poor prognosis, with a median survival period of less than 2 years [29]. Recently, immune checkpoint inhibitors targeting programmed cell death 1 and its ligand (PD-1/PD-L1) and cytotoxic T-lymphocyte antigen-4 (CTLA-4) have shown promising preliminary results in various tumours. However, the effectiveness of immunotherapy remains limited by low efficacy. Potential predictive biomarkers, such as tumour mutational burden (TMB), are currently evaluated.
Graf et al. performed a study aimed at assessing the outcomes of patients treated with immune checkpoint inhibitors (ICIs) versus taxane chemotherapy, with a focus on tumour mutational burden (TMB) [30]. Immune checkpoint inhibitors (ICIs) can induce significant responses and provide long-term benefits in some patients with metastatic cancer who have undergone numerous prior treatments. However, the rate of clinical benefit varies significantly by tumour type. Unfortunately, for patients with metastatic castration-resistant prostate cancer (mCRPC), the objective response rate to ICI treatments is reported to be 3% for those without programmed cell death ligand 1 (PD-L1) expression and 5% for those with PD-L1-expressing tumours [31]. For this reason, there has been increasing interest in identifying other biomarkers that could pinpoint mCRPC patients who are more likely to achieve greater clinical benefits from ICIs compared to alternative treatments.
In this study, a total of 741 men were evaluated between January 2011 and April 2021. They were subjected to genomic testing through the comprehensive genomic profiling (CGP) assays provided by Foundation Medicine. Patients were included in this study if they received either single-agent anti–PD-1 axis therapy or single-agent taxane in the mCRPC setting and had their TMB assessed through tissue biopsy. The main clinopathological characteristics were represented by the median age, 70 (ranges between 64-76 years) and the baseline median pretreatment PSA levels of 79.4 ng/mL. A total of 108 patients (18.8%) had tumors with ECOG scores of 2 or greater, and 644 patients (86.9%) had received prior systemic treatments for mCRPC. A total of 45 patients (6.1%) received ICIs, while 696 patients (93.9%) received taxanes. Patients who received ICIs and those who received taxanes showed no significant differences in age, pretherapy PSA levels, ECOG scores, practice setting (community vs. academic), prior NHT use, prior prescribed opioid use, and biopsy site. However, it is important to note that patients who received ICIs had higher TMB compared to those receiving taxanes (3.5 [1.7-15.0] mut/Mb vs. 2.5 [1.3-3.8] mut/Mb; P < .001).
PSA levels were evaluated in 607 patients. Among them, 14 patients had a TMB above 10 mut/Mb and were treated with ICIs. Of these, 4 exhibited a reduction in PSA levels by approximately 50%. In contrast, none of the patients with a TMB below 10 mut/Mb showed a reduction in PSA levels greater than 50%. For patients treated with taxanes, no relationship between TMB value and PSA level was demonstrated.
The FDA approved cut-off for TMB was 10 mut/Mb. As conclusions, the study showed that both TTNT (time to next treatment) and OS (overall survival) were adjusted by received drug class (ICIs vs. Taxanes). The patients’ group with TMB <10 mut/Mb and ICIs therapy had a worse average TTNT then those treated with taxanes (median [IQR], 2.4 [1.1-3.2] months vs. 4.1 [2.2-6.3] months; HR, 2.65, 95% CI, 1.78-3.85; P < .001). The reverse pattern for TTNT was observed for those with TMB> 10 mut/Mb (median [IQR], 8.0 [3.4 to unknown] months vs. 2.4 [2.43-7.33] months; HR, 0.37; 95% CI, 0.15-0.87; P = .02). The OS evaluation does not present major differences between those with TMB< 10 mut/Mb despite the treatment choice (median [IQR], 4.2 [2.1-8.1] months vs. 6.0 [3.1-9.7] months; HR, 1.08; 95% CI, 0.68-1.74; P = .73). However, in those cases with TMB greater then 10 muts/Mb the OS has an elevated value when ICIs were administered, compared to taxanes (median [IQR], 19.9 [8.1 to unknown] months vs. 4.2 [2.69-6.12] months; HR, 0.23, 95% CI, 0.10-0.57) [30].
Despite the evidence of improved clinical outcome for the group with high TMB and ICIs therapy, the study has some limitations: it is not a randomized study, the treatment was chosen by the clinician and the number of patients that received ICIs was reduced compared to the taxane group. Also, the biopsy timing was not considered. This leaves room for future studies to demonstrate the effectiveness of using TMB in a larger cohort of patients undergoing immunotherapy treatment.
8. Discussion
Representing some of the most severe forms of cancer globally, lung, breast and prostate cancer and melanoma continue to pose challenges for clinicians when it comes to selecting the optimal management protocol. The key to successful treatment lies in the individualization of the protocol, based on the clinical and pathological characteristics of each patient. From the perspective of evaluating treatment efficacy, there is an increasing need to identify a marker that can highlight the category of patients who are most likely to respond therapeutically.
Immunotherapy marks a significant advancement in cancer treatment. The mechanism is based on the reactivation of the tumour immune cycle, which will restore the body’s natural anti-tumour immune response. Currently, there are at least 4 types of immunotherapy strategies: immune checkpoint inhibitors (ICIs) such as Programmed Cell Death Protein-1 (PD-1) and Cytotoxic T-Lymphocyte Antigen 4 (CTLA-4), chimeric antigen receptor T-cell therapy, tumour vaccines, and lastly, peripatetic immunotherapy. Although these therapies have significantly improved clinical oncology outcomes, not all patients have experienced the benefits. Therefore, it is essential to determine which patients are most likely to respond favourably to immunotherapy [32].
To date, PD-L1 (programmed death ligand 1) is the only biomarker used to predict the response to ICIs (immune checkpoint inhibitors). However, since its evaluation varies depending on the kit used by medical teams, there is a need for the detection of a reliable marker for predicting therapeutic response. Lastly, several studies have detected another biomarker that can be used for predicting the response. Tumour mutational burden (for short TMB) represents the total number of mutations (substitutions, insertions or deletions) that occurs in a tumour sample [18]. TMB can be divided into 3 categories: low, intermediate, and high, depending on the cut-off value considered by each medical team. This cut-off value itself represents a limitation of any study on this topic, as there is currently no consensus on this value.
Various research have demonstrated that TMB offers some advantages over other biomarkers. Firstly, TMB can be measured in the blood, which is beneficial in cases where tumour tissue specimens are unavailable. Secondly, unlike PD-L1, which can only predict the response to PD-1/PD-L1 inhibitors, TMB can forecast the response to various immunotherapies, including PD-1/PD-L1 inhibitors, anti-CTLA4 antibodies (such as ipilimumab) [33].
The incidence of somatic mutations varies across different tumour types, with NSCLC exhibiting the highest mutation frequency, ranging from 0.1 to 100 mut/Mb [33]. A retrospective analysis performed Rizvi and his team [35] demonstrated that the efficacy of ICI therapy in NSCLC patients is related to the TMB value. Patients with high TMB demonstrated better efficacy and higher survival rates compared to those with a lower TMB. Klempner [36] additionally observed that a TMB cut-off value of 10 mut/Mb could predict the efficacy of ICI in NSCLC patients, with higher TMB thresholds correlating with longer progression-free survival (PFS). In most of the NSCLC studies, targeted Next Generation Sequencing (NGS) suggest a TMB cut-off value around 10 mut/Mb. While many studies have shown the predictive value of TMB for ICI therapy in NSCLC patients, some have reported negative outcomes, particularly concerning long-term survival. This discrepancy may be due to the limited attention and research on TMB in this context [33].
In addition to studies related to lung cancer, the specialized literature also includes studies analysing cases of malignant melanoma treated with ICIs. In Eckardt's study [36], the effectiveness of using TMB as a biomarker for patients treated with ICIs was demonstrated. Furthermore, the study's approach to the BRAF mutation, identified as a potential predictive biomarker for cases treated with targeted therapies, such as Dabrafenib, was also noteworthy. Those 2 markers were classified as independent viable predictive biomarkers for relapse-free survival period (ranges between 21-100%) in patients diagnosed with malignant melanoma.
Melanomas with BRAF mutations associated with high TMB are likely to benefit from adjuvant anti-PD-1 therapy. Conversely, patients with low TMB may gain more from adjuvant BRAF and MEK inhibitors, assuming their tumour tissue is less heterogeneous. However, the lack of direct comparative studies on this topic means that both adjuvant treatment options should be discussed with patients who have BRAF mutations [37].
Lastly, prostate and breast malignancies have a poor response to ICIs treatment, but in the last years, important improvements have been made in this direction. Because of that, several studies have started to investigate the importance of TMB value in these types of cancers. There is one preliminary study [38], that analysed 48 patients diagnosed with metastatic prostate/breast cancer and demonstrated that TMB, in these cases, is not directly associated with a better treatment response to ICIs. Instead, it was associated with a significantly higher number of genomic alterations and more pronounced MSI. These findings suggest that, with further research, TMB and MSI could potentially be correlated with a favourable response to ICIs in the future. Although minimal activity was observed in the group of patients with blood TMB evaluation/MSI-not detected, clinical benefit was noted in patients with notable MSI defects [38].
9. Conclusions
In conclusion, the evaluation of tumour mutational burden (TMB) holds significant promise as a predictive biomarker for response to immune checkpoint inhibitors (ICIs) across various cancer types. Our analysis of current literature highlights a more established consensus regarding the importance of TMB in lung cancer and melanoma, where high TMB has been associated with better clinical outcomes. However, the role of TMB in breast and prostate cancers remains less clear, indicating a need for further research in these areas.
Despite the variability in findings, the potential of TMB to guide personalized immunotherapy treatment is undeniable. As we continue to explore and refine our understanding of TMB, especially in less well-defined cancers such as breast and prostate, it becomes essential to conduct large-scale, randomized studies. These studies will aid in standardizing TMB evaluation and confirming its predictive efficacy, ultimately advancing the precision of cancer treatment and enhancing patient prognoses.
References
- Addeo, Alfredo et al. “TMB or not TMB as a biomarker: That is the question.” Critical reviews in oncology/hematology vol. 163 (2021): 103374. [CrossRef]
- Büttner, Reinhard et al. “Implementing TMB measurement in clinical practice: considerations on assay requirements.” ESMO open vol. 4,1 e000442. 24 Jan. 2019. [CrossRef]
- FDA. FDA announces approval, CMS proposes coverage of first breakthrough-designated test to detect extensive number of cancer biomarkers. 2017. Available from: https://www.fda. gov/NewsEvents/Newsroom/PressAnnouncements/ucm587273.htm.
- FDA. FDA unveils a streamlined path for the authorization of tumor profiling tests alongside its latest product action. 2018. Available from: https://www. fda. gov/NewsEvents/Newsroom/PressAnnouncements/ucm585347.htm.
- Bartha Á, Győrffy B. Comprehensive Outline of Whole Exome Sequencing Data Analysis Tools Available in Clinical Oncology. Cancers. 2019; 11(11):1725. [CrossRef]
- Schaub, M.A.; Boyle, A.P.; Kundaje, A.; Batzoglou, S.; Snyder, M. Linking disease associations with regulatory information in the human genome. Genome Res. 2012, 22, 1748–1759. [Google Scholar] [CrossRef] [PubMed]
- Minde, D.P.; Anvarian, Z.; Rudiger, S.G.; Maurice, M.M. Messing up disorder: How do missense mutations in the tumor suppressor protein APC lead to cancer? Mol. Cancer 2011, 10, 101. [Google Scholar] [CrossRef]
- Gnarra, J.R.; Tory, K.; Weng, Y.; Schmidt, L.; Wei, M.H.; Li, H.; Latif, F.; Liu, S.; Chen, F.; Duh, F.M.; et al. Mutations of the VHL tumour suppressor gene in renal carcinoma. Nat. Genet. 1994, 7, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Farmer, H.; McCabe, N.; Lord, C.J.; Tutt, A.N.; Johnson, D.A.; Richardson, T.B.; Santarosa, M.; Dillon, K.J.; Hickson, I.; Knights, C.; et al. Targeting the DNA repair defect in BRCA mutant cells as a therapeutic strategy. Nature 2005, 434, 917–921.
- Torgovnick, A.; Schumacher, B. DNA repair mechanisms in cancer development and therapy. Front. Genet. 2015, 6, 157.
- Luchini, C.; Bibeau, F.; Ligtenberg, M.J.L.; Singh, N.; Nottegar, A.; Bosse, T.; Miller, R.; Riaz, N.; Douillard, J.Y.; Andre, F.; et al. ESMO recommendations on microsatellite instability testing for immunotherapy in cancer, and its relationship with PD-1/PD-L1 expression and tumour mutational burden: A systematic review-based approach. Ann. Oncol. Off. J. Eur. Soc. Med Oncol. 2019.
- Pongor, L.; Kormos, M.; Hatzis, C.; Pusztai, L.; Szabo, A.; Gyorffy, B. A genome-wide approach to link genotype to clinical outcome by utilizing next generation sequencing and gene chip data of 6697 breast cancer patients. Genome Med. 2015, 7, 104.
- Hargadon, K.M.; Johnson, C.E.; Williams, C.J. Immune checkpoint blockade therapy for cancer: An overview of FDA-approved immune checkpoint inhibitors. Int. Immunopharmacol. 2018, 62, 29–39.
- Chalmers, Zachary R et al. “Analysis of 100,000 human cancer genomes reveals the landscape of tumor mutational burden.” Genome medicine vol. 9,1 34. 19 Apr. 2017. [CrossRef]
- FoCR. Friends of Cancer Research Announces Launch of Phase II TMB Harmonization Project; FoCR: Washington, DC, USA, 2018.
- Goodman, Aaron M et al. “Tumor Mutational Burden as an Independent Predictor of Response to Immunotherapy in Diverse Cancers.” Molecular cancer therapeutics vol. 16,11 (2017): 2598-2608. [CrossRef]
- Wu HX, Wang ZX, Zhao Q, Chen DL, He MM, Yang LP, Wang YN, Jin Y, Ren C, Luo HY, Wang ZQ, Wang F. Tumor mutational and indel burden: a systematic pan-cancer evaluation as prognostic biomarkers. Ann Transl Med. 2019 Nov;7(22):640. [CrossRef] [PubMed]
- Dousset, Léa et al. “Positive Association Between Location of Melanoma, Ultraviolet Signature, Tumor Mutational Burden, and Response to Anti-PD-1 Therapy.” JCO precision oncology vol. 5 PO.21.00084. 16 Dec. 2021. [CrossRef]
- Bravaccini S, Bronte G, Ulivi P. TMB in NSCLC: A Broken Dream? Int J Mol Sci. 2021 Jun 18;22(12):6536. [CrossRef] [PubMed]
- Wankhede D, Grover S, Hofman P. The prognostic value of TMB in early-stage non-small cell lung cancer: a systematic review and meta-analysis. Ther Adv Med Oncol. 2023 Aug 31;15:17588359231195199. [CrossRef] [PubMed]
- Greillier, Laurent et al. “The clinical utility of tumor mutational burden in non-small cell lung cancer.” Translational lung cancer research vol. 7,6 (2018): 639-646. [CrossRef]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Cs ̋oszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. KEYNOTE-024 Investigators. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2016, 375, 1823–1833.
- Hellmann, M.D.; Paz-Ares, L.; Bernabe Caro, R.; Zurawski, B.; Kim, S.W.; Carcereny Costa, E.; Park, K.; Alexandru, A.; Lupinacci, L.; de la Mora Jimenez, E.; et al. Nivolumab plus Ipilimumab in Advanced Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2019, 381, 2020–2031.
- Young Kwang Chae, Andrew A. Davis, Sarita Agte, Alan Pan, Nicholas I. Simon, Wade T. Iams, Marcelo R. Cruz, Keerthi Tamragouri, Kyunghoon Rhee, Nisha Mohindra, Victoria Villaflor, Wungki Park, Gilberto Lopes, Francis J. Giles, Clinical Implications of Circulating Tumor DNA Tumor Mutational Burden (ctDNA TMB) in Non-Small Cell Lung Cancer, The Oncologist, Volume 24, Issue 6, June 2019, Pages 820–828. [CrossRef]
- Mei, P., Freitag, C.E., Wei, L. et al. High tumor mutation burden is associated with DNA damage repair gene mutation in breast carcinomas. Diagn Pathol 15, 50 (2020). [CrossRef]
- Nanda R, Chow LQ, Dees EC, et al. Pembrolizumab in patients with advanced triple-negative breast Cancer: phase Ib KEYNOTE-012 study. J Clin Oncol. 2016;34:2460–7.
- Schmid P, Adams S, Rugo HS, et al. Atezolizumab and nab-paclitaxel in advanced triple-negative breast Cancer. N Engl J Med. 2018;379:2108–21.
- Wang L, Pan S, Zhu B, Yu Z, Wang W. Comprehensive analysis of tumour mutational burden and its clinical significance in prostate cancer. BMC Urol. 2021 Feb 25;21(1):29. [CrossRef] [PubMed]
- Zhu Y, Ye D. Chinese Expert Consensus on the Diagnosis and Treatment of Castration-Resistant Prostate Cancer (2019 Update). Cancer Manag Res. 2020;12:2127–40.
- Graf RP, Fisher V, Weberpals J, et al. Comparative Effectiveness of Immune Checkpoint Inhibitors vs. Chemotherapy by Tumor Mutational Burden in Metastatic Castration-Resistant Prostate Cancer. JAMA Netw Open. 2022;5(3):e225394. [CrossRef]
- Antonarakis ES, Piulats JM, Gross-Goupil M, et al. Pembrolizumab for treatment-refractory metastatic castration-resistant prostate cancer: multicohort, open-label phase II KEYNOTE-199 Study. J Clin Oncol. 2020;38 (5):395-405. [CrossRef]
- Donisi C, Pretta A, Pusceddu V, Ziranu P, Lai E, Puzzoni M, Mariani S, Massa E, Madeddu C, Scartozzi M. Immunotherapy and Cancer: The Multi-Omics Perspective. International Journal of Molecular Sciences. 2024; 25(6):3563. [CrossRef]
- Ma X, Zhang Y, Wang S, Yu J. Predictive value of tumor mutation burden (TMB) with targeted next-generation sequencing in immunocheckpoint inhibitors for non-small cell lung cancer (NSCLC). J Cancer. 2021 Jan 1;12(2):584-594. [CrossRef] [PubMed]
- Berland L, Heeke S, Humbert O, et al. Current views on tumor mutational burden in patients with non-small cell lung cancer treated by immune checkpoint inhibitors. J Thorac Dis. 2019; 11(Suppl 1): S71-S80.
- Rizvi NA, Hellmann MD, Snyder A, et al. Cancer immunology. Mutational landscape determines sensitivity to PD-1 blockade in non-small cell lung cancer. Science. 2015; 348: 124-128.
- Klempner SJ, Fabrizio D, Bane S, et al. Tumor Mutational Burden as a Predictive Biomarker for Response to Immune Checkpoint Inhibitors: A Review of Current Evidence. Oncologist. 2020; 25(1): e147-e159.
- Eckardt, J., Schroeder, C., Martus, P. et al. TMB and BRAF mutation status are independent predictive factors in high-risk melanoma patients with adjuvant anti-PD-1 therapy. J Cancer Res Clin Oncol 149, 833–840 (2023). [CrossRef]
- Pedro Barata, Reagan Barnett, Albert Jang et al. Assessment of blood-based tumor mutational burden on clinical outcomes in advanced breast and prostate cancer treated with immune checkpoint inhibitors, 28 May 2024, PREPRINT (Version 1) available at Research Square. 28 May. [CrossRef]
Figure 1.
From tissue to date- steps of whole exome sequencing. Tissue preprocessing starts with the identification of tumour regions by an experienced pathologist, followed by DNA extraction, library construct and amplification. Data procession commences with the quality check of reads. If the quality of trimmed reads is sufficient, the alignment of the reads to a reference genome is launched. When Binary Alignment Map (BAM) files are processed, the calling of single nucleotide variants, insertions and deletions, and copy number variants comes next, using one or more of the numerous existing algorithms. The date can be further utilized to detect microsatellite instability status, intratumor heterogeneity, tumour mutational burden, and homologous recombination deficiency [5].
Figure 1.
From tissue to date- steps of whole exome sequencing. Tissue preprocessing starts with the identification of tumour regions by an experienced pathologist, followed by DNA extraction, library construct and amplification. Data procession commences with the quality check of reads. If the quality of trimmed reads is sufficient, the alignment of the reads to a reference genome is launched. When Binary Alignment Map (BAM) files are processed, the calling of single nucleotide variants, insertions and deletions, and copy number variants comes next, using one or more of the numerous existing algorithms. The date can be further utilized to detect microsatellite instability status, intratumor heterogeneity, tumour mutational burden, and homologous recombination deficiency [5].
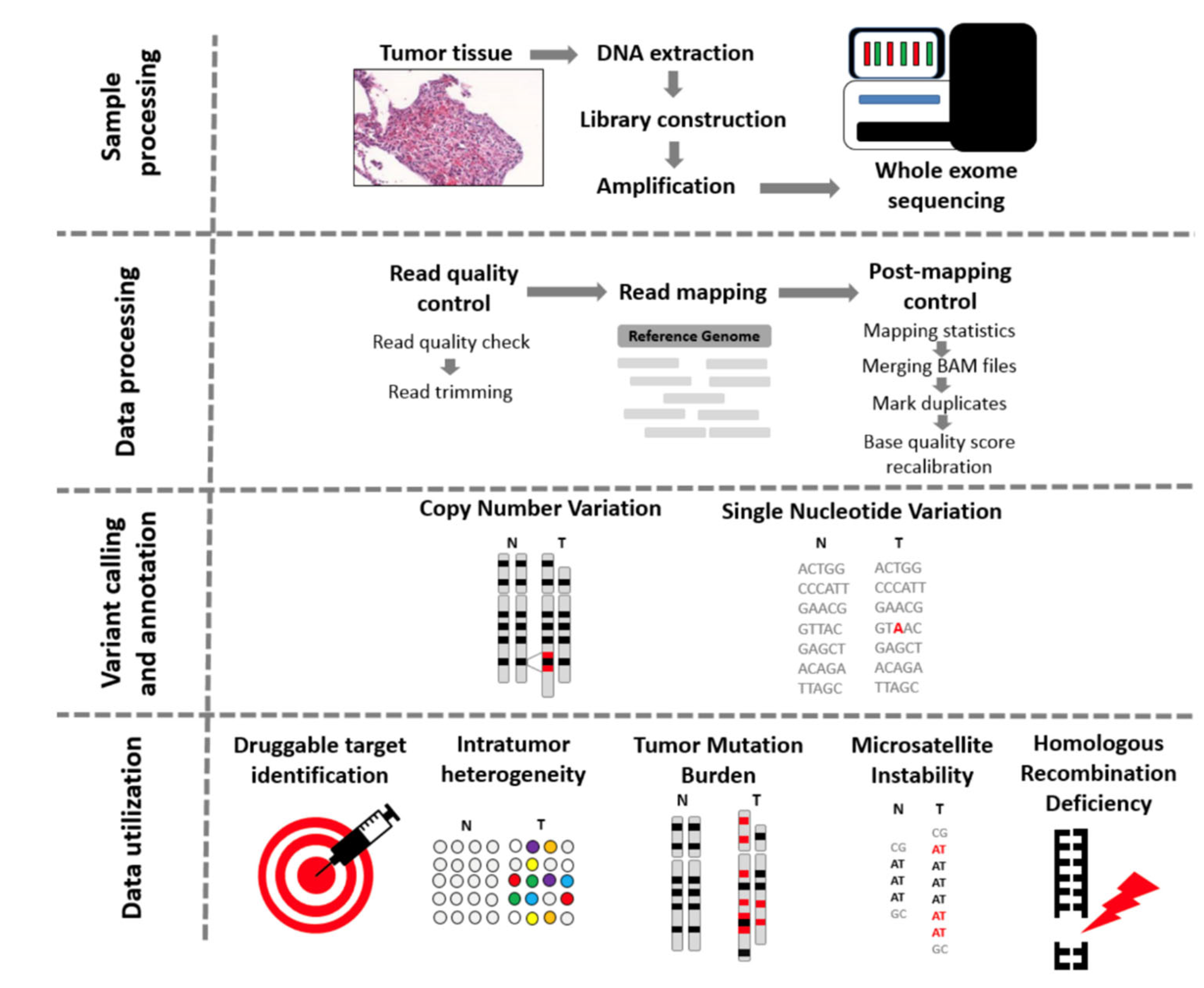
Figure 3.
TMB (muts/Mb) measure according to sun exposure of the site of primary melanoma [18].
Figure 3.
TMB (muts/Mb) measure according to sun exposure of the site of primary melanoma [18].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



