Submitted:
24 July 2024
Posted:
26 July 2024
You are already at the latest version
Abstract
Schizophrenia is a complex mental disorder influenced by genetic and environmental factors, including diet. Oxidative stress and inflammation play a crucial role in the pathophysiology of schizophrenia. Nutritional deficiencies, such as lack of omega-3 fatty acids, vitamin D, and B vitamins, during prenatal and postnatal periods can nega-tively impact neurodevelopment and increase the risk of schizophrenia. Patients with schizophrenia show imbalances in antioxidant enzymes such as: glutathione peroxidase (GPx), superoxide dismutase (SOD), catalase (CAT) and reduced levels of antioxidants (vitamin E, vitamin C), leading to increased oxidative stress markers such as malondialdehyde (MDA). Cytokine-mediated inflammation, microglial activation, and gut dysbiosis are associated with schizophrenia onset and symptom severity. There is no clear and universally accepted diet for the treatment of schizophrenia, which is considered the most popular. However, various diets and nutritional methods are being researched and applied to alleviate the symptoms of schizophrenia and improve the general health of patients, including the mediterranean diet, ketogenic diet, gluten-free diet and DASH diet. A healthy diet rich in anti-inflammatory and antioxidant nutrients can help manage schizophrenia by reducing oxidative stress, preventing complications, and improving quality of life. Omega-3 fatty acids, vitamin D and B vitamins are par-ticularly important for brain development and function. In this review we will focus on the influence of diet on schizophrenia. Additional research is needed to develop per-sonalized dietary recommendations for patients with schizophrenia.
Keywords:
Schizophrenia
; Diet
; Nutrients
; Obesity
; Oxidative Stress
; Inflammation
; Antioxidants
1. Introduction
Common mental disorders such as schizophrenia, depression, and anxiety are major public health concerns worldwide. These conditions currently represent the greatest challenge to disability in developed countries, severely limiting the capacity for daily functioning. Poor nutrition, lack of physical exercise, and smoking have long been recognized as primary contributors to common non-communicable diseases such as heart disease, type 2 diabetes, and cancer [1] .
Schizophrenia is a chronic, complex, and debilitating mental disorder that involves issues with cognition, mood, reality perception, and interpersonal relationships [2]. The literature suggests that schizophrenia can result from a combination of genetic and environmental factors, including stress, diet, lack of physical activity, and medication [3]. Diagnosing schizophrenia requires specialized professionals to identify a complex group of symptoms, which include cognitive impairments, disorganization, and negative and positive symptoms. These signs are clearly defined in international disease classifications such as the Diagnostic and Statistical Manual of Mental Disorders (DSM) and the International Classification of Diseases (ICD) [4].
In the field of psychiatry, nutritional interventions have been much studied in recent times, with an emphasis on nutrient supplementation and the adoption of specific dietary strategies to prevent and treat mental disorders [5]. The field of 'nutritional psychiatry' has developed rapidly in recent years, with several studies related to dietary or nutrient-based interventions being initiated, and more preclinical and epidemiological data becoming available [6]. The last ten years have seen a steady increase in research examining the links between nutrition and mental health. Various studies have confirmed that nutrition is a factor preceding the onset of psychiatric symptoms, indicating a direction of causality [7].
An increasing number of studies suggest that certain modifiable lifestyle behaviors are also risk factors for common mental disorders. The quality of diet has become a primary focus in recent research concerning lifestyle and mental health [1]. Previous studies have established a strong connection between diet, cognitive functions, and mental health. For example, a systematic review analyzing various dietary patterns and cognitive functions showed that increased carbohydrate intake (such as sugars) is linked to a decline in overall cognitive performance, while saturated fats were associated with reduced memory and learning. Conversely, protein intake has been observed to positively impact executive function and memory [8].
Diet and mental health are connected through changes in molecular biomarkers as well as alterations in brain structure and function. Nutrition studies indicate that the relationship between eating habits and mental disorders (or cognitive ability) may be influenced by gut-brain communication [8]. A growing body of evidence points to the significant impact of the gut microbiome on the development and progression of obesity. Dysbiosis, characterized by reduced diversity and changes in the composition of the gut microbiome, is associated with overweight and obesity [3]. Another recent trend in nutritional psychiatry involves research examining the influence of modulating the gut microbiota through dietary interventions and probiotic and prebiotic supplements in treating various neuropsychiatric conditions [7].
The general public's diet falls significantly short of the standards recommended by the World Health Organization for a healthy diet. Young people, who are at the highest risk for developing schizophrenia, tend to have particularly poor diets, often consuming large quantities of fast food. Research indicates that individuals with schizophrenia have even more inadequate diets compared to the general population [9]. They exhibit an excessive preference for unhealthy foods, especially fast food and foods high in fats and carbohydrates, which characterize their dietary habits [10].
2. Prenatal Nutritional Deficiency
Increasing evidence from the field of nutritional psychiatry shows that diet is crucial for psychological well-being throughout life. Recently, nutrition has become essential in modifying brain functions and its plasticity, as there is a connection between poor childhood nutrition and an increased risk of developing psychiatric disorders later in life [11]. For example, folic acid deficiency during prenatal and postnatal periods can negatively affect neurological development and increase the likelihood of developing mental health issues [12]. Deficiency of several nutrients, such as folic acid, essential fatty acids, retinoids, vitamin D, and iron, has been associated with an increased risk of schizophrenia due to malnutrition during pregnancy [13].
Famine as a natural phenomenon offers the opportunity to study the link between prenatal malnutrition and adult health, including schizophrenia, in the long term [14]. One of the best documented presentations with negative consequences for central nervous system growth is prenatal malnutrition [13]. Most of the research on this topic focuses on the Dutch famine of 1944-1945 and the Chinese famine of 1959-1961 [15]. Epidemiologic evidence suggests that exposure to poor diet in early pregnancy almost doubles the risk of schizophrenia in offspring. For this reason, the diet of pregnant women, especially in the early stages of pregnancy, has an impact on epigenetic changes in the fetus [13].
Proper prenatal nutrition is crucial for optimal brain development. Research in epidemiology increasingly shows that exposure to nutritional deprivation may increase the risk of schizophrenia [16]. The latest update of the neurodevelopmental theory of schizophrenia has indicated that there are several risk factors that may act together on a genetically predisposed individual at different developmental stages, contributing to the clinical syndrome of schizophrenia. An important risk factor is vitamin D deficiency, especially during pregnancy and childhood [17].
Vitamin D deficiency is extremely common in people suffering from schizophrenia and other mental health problems. Epidemiologic research has shown that people born in late winter/early spring, in high latitude areas and in urban settings are at increased risk of schizophrenia, indicating that this risk may be influenced by vitamin D deficiency. This association is suggested by studies of African and Caribbean migrant populations, among whom vitamin D levels tend to be low. Migrant populations from Africa and the Caribbean have increased rates of psychosis [18]. Furthermore, the offspring of individuals migrating from more equatorial regions to colder climates are also at increased risk of schizophrenia, as are the offspring of city dwellers compared with those living in rural regions [19]. Serum vitamin D levels were negatively related to the severity of symptoms of psychosis. The lower the vitamin D concentrations, the higher the overall negative symptom scores [20]. A minor way to obtain vitamin D is through diet, as some foods contain this vitamin such as fatty fish. Vitamin D can also be consumed by taking supplements or eating fortified foods such as some dairy products. From a global perspective, vitamin D deficiency is among the most common micronutrient deficiencies [21].
Vitamin D is a fat-soluble vitamin and has diverse biological effects on the body [22]. Vitamin D deficiency is linked to a wide variety of neuropsychiatric problems and neurodegenerative disorders [23] The effects of vitamin D in the brain are diverse, including promoting antioxidant and neurotrophic action, as well as regulating various neurotransmitter systems (including dopamine). In animal studies, the offspring of vitamin D-deficient rodents show brain structural changes similar to those seen in schizophrenia, such as thinning of the cortex, enlargement of lateral ventricles and increased brain size due to increased proliferation and reduced shedding of neurons [24]. In psychotic disorders, vitamin D has been positively associated with peripheral gray matter volume, possibly indicating a neuroprotective effect [25].
Similar to other major neuropsychiatric illnesses, schizophrenia usually begins in the late teens or early 20s, with a slightly delayed onset in women [26]. Disruption of normal brain growth during prenatal or early postnatal periods can lead to brain dysfunction, suggesting that an affected central nervous system may play a crucial role in the development of this condition. Indeed, individuals with schizophrenia, compared to healthy individuals, show a significant reduction in total brain volumes and density of gray and white matter, while showing significant increases in the volumes of the lateral and third ventricles [27,28].
Schizophrenia is viewed as a brain dysfunction because the control of all functions and behaviors is executed by the human brain. The brain contains the highest amount of lipids of all the body’s organs [27]. Lipids and lipid intermediates are indispensable elements in the organization and functioning of the brain. In fact, brain tissue contains the second-highest percentage of fat after adipose tissue, and fat makes up half of the brain's dry weight [29]. Over 60% of the lipids present in the membrane are phospholipids. Brain phospholipids include two categories of polyunsaturated fatty acids: omega-3 and omega-6. Docosahexaenoic acid (DHA) is crucial for the normal development of the nervous system and is particularly important in maintaining biological functions (receptor binding, neurotransmission, signal transduction, and cognitive abilities, including learning and memory) [27].
Humans cannot naturally produce omega-3 and omega-6 polyunsaturated fatty acids and must obtain these essential substances from their diet. This essential nature could support the substantial epidemiological evidence showing an inverse relationship between omega-3 fatty acid intake and the prevalence of psychiatric disorders [30]. Fatty fish is a food rich in essential fatty acids and vitamin D, both of which may be implicated in the development of schizophrenia. It is suggested that a low maternal intake of fish and seafood during pregnancy may increase the risk of low IQ and suboptimal neurological development in the child, thereby linking to a higher risk of mental disorders in adulthood, such as schizophrenia [31]. Nutrition has a crucial impact on brain development, mental health and mental disorders. The importance of omega-3 polyunsaturated fatty acids in the maintenance of physical health is well known, as they are involved in a variety of physiological functions related to neurogenesis, neurotransmission and neuroinflammation, and play essential roles in brain development, activity and aging [32].
Lack of long-chain omega-3 polyunsaturated omega-3 polyunsaturated fatty acids impairs neuronal development and may contribute to various mental health problems [33]. In schizophrenia, changes in the structure of phospholipids in cell membranes may influence various aspects of pathophysiology, such as neurotransmission, immune activation and antioxidant protection. Studies have shown a deficiency of omega-3 polyunsaturated fatty acids in patients with schizophrenia compared to healthy individuals, thus supporting this hypothesis. The addition of omega-3 polyunsaturated fatty acids could be useful in preventing the onset of psychosis, especially among those at increased risk [34].
Various experimental studies have clearly shown the influence of omega-3 fatty acids on brain structures and activities. For proper differentiation and function, dissociated brain cell cultures require omega-3 and omega-6 fatty acids [35]. Simultaneously, a lack of alpha-linolenic acid in the diet affects brain development, disrupting the structure and chemical composition of neuron membranes (including oligodendrocytes and astrocytes), myelin, and nerve endings [36]. This is accompanied by the appearance of neurosensory and behavioral disorders. There is a known relationship between the amount of alpha-linolenic acid in the maternal diet during gestation and lactation and the accumulation of these compounds in the fetus's or newborn’s brain until an optimal level is reached [37].
Currently, many patients with schizophrenia continue to experience residual symptoms and cognitive difficulties despite optimal pharmacological treatment. Although there is a continual search to enhance the effectiveness of antipsychotic agents, no strategy has proven to be markedly superior. Omega-3 fatty acids are considered important for their potential to increase favorable side effects and their ability to repair metabolic issues of phospholipids in synaptic membranes, which can lead to dysfunction of dopaminergic and serotonergic neurotransmitter receptors. Omega-3 fatty acids can mitigate the negative consequences of medications through their anti-inflammatory actions and pose a low risk of causing damage. Supplementation and diet are two ways to increase omega-3 intake. Equally crucial are dietary changes to reduce the amount of omega-6 consumed. For example, industrially derived seed oils, such as safflower, sunflower, and vegetable oils, contain large amounts of omega-6 fatty acids [38].
Pregnancy is characterized by rapid growth of maternal and fetal tissues, which involves an increased demand for energy and nutrients [39]. Lack of essential nutrients during critical growth phases can cause long-term brain dysfunction [40]. The food consumed by the mother during pregnancy, as part of the period known as the "first 1000 days," is considered extremely important for the optimal development of offspring, reducing the risk of diseases throughout life, and overall long-term health [39].
Some time ago, it was noted that schizophrenia may be associated with vitamin B deficiency [41]. B vitamins are crucial in cellular metabolism functions, including homocysteine regulation, transmission processes, and oxidation-reduction reactions. Experts have emphasized that certain B vitamins, such as vitamin B6, vitamin B12, folic acid, and choline, may be linked to the onset and progression of schizophrenia [42,43]. Studies have determined that severe folic acid deficiency increases the likelihood of neurodevelopmental disorders, psychiatric disorders, and dementia, while changes in vitamin B12 levels can lead to neuropsychiatric problems, mental disorders, reduced cognitive abilities, mood disorders, aggressive behavior, fatigue, and paranoid psychosis [44].
Neurotropic B vitamins, such as B1, B2, B3, B6, B9, and B12, are important for the health of the central nervous system, playing essential roles as coenzymes, among other functions. Mammals cannot produce B vitamins, so they must obtain them from their food in sufficient quantities. Most B vitamins come from plant or animal sources, such as meat, eggs, and dairy. Only vitamin B12 comes from an animal source. A lack of B vitamins has been linked to various neurodevelopmental issues, with one of the most significant being schizophrenia (29). Many studies have found that the main etiological factor for schizophrenia is a deficiency in vitamin B12 and elevated homocysteinemia. Not only can a deficiency in vitamin B12 cause schizophrenia, but vitamins B6 and B9 can also contribute to the condition, and symptoms can be reduced by supplementing these vitamins alongside antipsychotics [45].
Epidemiologic, biochemical and genetic association studies have demonstrated that folate deficiency is a risk factor for schizophrenia [46]. Essential for the synthesis of DNA and neurotransmitters, it plays an important role in regulating gene expression. An adequate amount of folate during pregnancy can reduce the risk of congenital anomalies, such as neural tube defects. Research has shown that a lack of folate during pregnancy can significantly increase the likelihood of schizophrenia in offspring. Previous studies have linked low blood levels of folic acid to more severe symptoms among patients with schizophrenia [47].
There are natural amounts of folate in various foods such as green leafy vegetables, fruits, nuts, beans, seafood, eggs, dairy products, meat, poultry and cereals. Spinach, liver, asparagus and Brussels sprouts are among the foods rich in folic acid [48] which is essential for the proper functioning of neurons. It is confirmed to be crucial for people with schizophrenia in managing energy levels. A lack of folic acid, either alone or in conjunction with monoamine precursors such as vitamins B6 and B12, can increase the risk of schizophrenia or exacerbate existing mood disorders [45]. As a complex, B vitamins are essential for various brain functions. Further studies conducted to investigate the precise mechanisms of B vitamins in brain functions will provide the possibility of using B vitamins to improve mental health and prevent psychological disorders [49].
3. Obesity in schizophrenia: the role of diet and antidepressants
Numerous factors contribute to weight gain in patients suffering from schizophrenia or psychosis. The main contributing factors are considered to be a sedentary lifestyle, unhealthy eating habits, genetic susceptibility, and antipsychotic treatment. Weight gain caused by antipsychotics is a significant issue in the care of patients with psychosis [50]. In addition to causing weight gain, antipsychotics are also known for their effect on glucose metabolism, increasing cholesterol and triglyceride levels, and inducing high blood pressure, leading to metabolic syndrome [51]. The prevalence of metabolic syndrome is high among individuals with schizophrenia. The frequent occurrence of both metabolic syndrome and obesity in this population leads to a reduced life expectancy and an increased mortality rate [50]. Changes in body structure are observed early in individuals experiencing their first episode of psychosis, with a greater predisposition to being overweight and obese. Weight gain occurs rapidly after starting antipsychotic treatment and continues, albeit at a slower rate, over the following years [52].
People with severe mental disorders are at increased risk of obesity, cardiometabolic risk factors, and associated morbidity and mortality compared to the general population [53,54]. Several commonly prescribed medications can cause weight gain and, in the case of prolonged treatment, can lead to clinically significant obesity [55]. These negative consequences of medication are key factors leading to decreased quality of life and premature death due to cardiovascular disorders in patients with severe mental disorders compared to the rest of the population [56]. Explanations given for drug-induced weight gain include increased appetite, changes in food preferences towards carbohydrates, and alterations in nutrient metabolism. Other significant factors can explain medication-induced weight gain, such as impaired metabolism due to decreased thyroid function, fluid retention, and the anabolic effect of steroids [55].
Antipsychotic drugs are considered a vital therapeutic choice for many patients with schizophrenia and other psychotic disorders. To offer maximum benefits, the medication must have acceptable side effects and be taken according to medical guidelines [55]. A common negative consequence of many antipsychotics is weight gain. The way weight increases seems to differ depending on the medication, which may be caused by variations in the action of the medications on different neurotransmitter systems such as serotonin, dopamine, choline, histamine, and others [57].
Secondly, antipsychotics are prescribed as the main treatment for alleviating symptoms, preventing the relapse of schizophrenia, and regulating dopamine levels to normal [20]. Despite these aspects, the administration of antipsychotic medications can frequently have side effects such as increased appetite and body weight by disrupting ghrelin and leptin, thus altering food intake and causing weight gain in patients with schizophrenia [58].
The addition of atypical antipsychotics to the field of psychopharmacology has represented a significant advance in the therapy of schizophrenia, providing an effective way to treat the positive and negative symptoms of psychosis. Before their widespread use, there was concern about treatment-related weight gain and the apparent increased risk of diabetes [59]. Among people with schizophrenia, the prevalence of obesity is double that of the general population, affecting more than half of this patient category. In addition to the negative psychosocial impact (distorted self-image and societal stigma) and non-compliance with medication treatment, people with schizophrenia appear to be extremely sensitive to the harmful medical consequences of obesity, such as "metabolic syndrome," which includes a set of cardiovascular risk factors such as abdominal adiposity, insulin resistance, impaired glucose tolerance, dyslipidemia, and high blood pressure [10].
Antipsychotics can lead to increased appetite (Figure 1). People suffering from schizophrenia make inadequate food choices, which means that any increase in appetite is likely to lead to increased consumption of snacks and convenient foods that are high in fat and sugar [60]. Patients diagnosed with schizophrenia have an increased appetite at meals, eat more quickly, and have more meals per day compared to the general population. This irregular food consumption eventually leads to excess energy intake, which contributes to the onset of obesity. Skipping breakfast and irregular eating can lead to compulsive eating, which can contribute to obesity [61]. People diagnosed with schizophrenia adopt inadequate eating habits, characterized by increased consumption of saturated fats, sugar, and alcohol, as well as reduced intake of fish, vegetables, and fruits, which could affect cognitive function [20].
Increased food intake associated with obesity has been observed in the early stages of therapy with chlorpromazine and depot antipsychotic medications (a special formulation of the drug, which is administered by injection and is slowly released into the body over several weeks) [60], and the problem of weight gain and diabetes has been highlighted in connection with atypical antipsychotic treatment [9].
The way antipsychotic medications influence food intake is probably related to their impact on dopamine and serotonin receptors [9]. After treatment with conventional and atypical antipsychotic agents, high levels of circulating leptin have been observed. Leptin, a hormone produced by fat cells, influences the hypothalamus to suppress hunger. The body of obese individuals is often resistant to this characteristic of leptin [62,63].
Differences in weight gain tendency vary between medications, with the greatest effects observed with olanzapine and clozapine [52]. The increased risk of weight gain with these medications is due to their action on serotonin, dopamine, histamine, and muscarinic receptors [50]. Although many studies have focused on new-generation antipsychotics, weight gain can also occur with older antipsychotics, with chlorpromazine being linked to the most significant weight gain. Antipsychotics influence energy levels and change the composition of the gut microbiome, which could lead to weight gain. Appetite control is complex and involves multiple neuropeptides, some of which are influenced by antipsychotic medications [52].
Early dietary interventions in schizophrenia included suggestions about the possible effectiveness of gluten-free diets in reducing symptoms or disease severity [64]. The Mediterranean diet, inspired by the eating habits of Mediterranean countries and the Middle East, emphasizes fresh vegetables, grains, olive oil and herbs; limiting meat consumption, known to reduce blood cholesterol [65]. In addition, it has been noticed that it has positive effects on diabetes, cardiovascular diseases, arthritis and cancer [66,67]. Ketogenic diets are high-fat, low-carbohydrate diets [68]. This provides an alternative source of energy for the brain, replacing glucose, and normalizes schizophrenia-like behaviors [69]. In addition, it has been observed to have a very good therapeutic role in patients with intractable seizures [68]. Dietary Approaches to Stop Hypertension (DASH) is a low-sodium, low-fat diet designed to treat high blood pressure [70,71]. As with ketogenic diets, DASH diets have been shown to be effective for weight loss [72]. The DASH diet and the Mediterranean diet are lifestyle changes that have positive effects on the prevention, risk reduction, and management of chronic disease. Various studies have shown that strict adherence to these dietary choices can have beneficial effects in schizophrenia [2].
People suffering from schizophrenia need to be carefully initially evaluated and constantly monitored for physical health parameters. Plans to treat and prevent should incorporate promoting a healthy lifestyle, proper nutrition, and adequate levels of physical activity [73]. In this context, it is essential to understand how various types of diets can influence antipsychotic-induced obesity (Table 1), a common problem in the treatment of schizophrenia.
Excess weight, which represents a major risk for metabolic syndrome, cardiovascular diseases, and premature mortality, is a common physical health problem among patients with schizophrenia spectrum disorder [84]. Since eating habits influence the quantify and type of food consumed, they can prevent or control obesity, making them modifiable factor It has been observed that a regular or healthy eating pattern impacts overall and abdominal obesity in patients with schizophrenia, and these effects differ by gender [61].
4. Impact of diet on oxidative stress and inflammation in schizophrenia
Free radicals are naturally formed under normal physiological conditions and have a significant impact on various biological processes [85]. However, when these molecules are produced in greater quantities than necessary, they can trigger spontaneous chain reactions that may lead to consequences such as abnormal neuronal development and impaired neuronal function. Free radicals are considered unstable due to the presence of one or more unpaired electrons, which makes them extremely reactive [61,86].
Oxidative stress occurs when there is a disturbance in free radicals, as well as reactive oxygen and nitrogen species, derived from both normal metabolic processes, including neurotransmitters associated with schizophrenia, such as dopamine and glutamate, and various environmental exposures. The lack of effectiveness of the antioxidant system in protecting against free radical production can damage cell membranes, causing dysfunctions that could influence neurotransmission and, ultimately, symptoms associated with schizophrenia [87]. Radicals can interact with polyunsaturated fatty acids, and the cell membranes of tissues exposed to high oxygen levels, such as the brain, are at risk of oxidizing their unsaturated fatty acid content in their phospholipids [86]. The human body's defense system includes antioxidant enzymes such as superoxide dismutase, glutathione peroxidase, and catalase. These enzymes stop the initiation of chain reactions of reactive species. Substances like glutathione, vitamin E, and vitamin C are non-enzymatic antioxidant components that bind to reactive species and stop the extension of chain reactions [88]. To better understand the impact of diet on oxidative stress and inflammation in schizophrenia, it is useful to analyze specific parameters that measure the levels of antioxidant enzymes and non-enzymatic antioxidant components.
A study found that patients on antipsychotic treatment showed lower scores on the Brief Psychiatric Rating Scale (BPRS) and Positive and Negative Syndrome Scale (PANSS) after taking vitamin C, vitamin E, and omega-3 fatty acids [89]. However, it is unclear if the effects are solely due to the vitamin supplementation because they were given in combination. In a study conducted by Bentsen et al. [90], patients with schizophrenia taking antipsychotic medication were given vitamin C (364 mg/day) and vitamin E (1000 mg/day) in a randomized placebo-controlled trial. Results showed that the vitamin supplementation hindered recovery from acute psychosis in patients with low levels of red blood cell polyunsaturated fatty acids (PUFAs) compared to those who received a placebo. The writers suggest that at a certain level, vitamin E may function as a pro-oxidant in the absence of sufficient antioxidant activity, leading to increased oxidative stress; it might also block the positive effects of γ- and δ tocopherols. They propose that vitamin C could offset some negative impacts of vitamin E [91].
Superoxide dismutase, catalase, and glutathione peroxidase make up the enzymatic antioxidant defense system in the human body, stopping the start of reactive species chain reactions [92]. The inability of antioxidants to protect against free radicals can damage cell membranes, causing dysfunctions that could influence neurotransmission and ultimately symptoms in schizophrenia [87]. The non-enzymatic antioxidant components are compounds such as glutathione (GSH), vitamin E and vitamin C, which react with reactive species and thus prevent chain reactions from spreading [92].
Among patients with schizophrenia, research has shown varying results regarding SOD levels, but the majority of evidence indicates an increase in activity as a compensatory response to increased oxidative stress, although low or unchanged levels are also observed in other studies, highlighting the complexity and variability of oxidative balance in schizophrenia. As with SOD, research on CAT levels in patients with schizophrenia has had varied results, reflecting the complexity of oxidative stress and antioxidant defense mechanisms in this disorder. Catalase levels vary with oxidative stress, nutritional status, genetic and epigenetic factors, chronic inflammation, and drug effects.
Studies suggest that MDA levels are usually frequently elevated in patients with schizophrenia, rather than reduced. Elevated MDA levels indicate an increase in oxidative stress in these patients, which is a significant factor in the pathophysiology of the disorder.
Low levels of GPx in patients with schizophrenia are due to several factors, such as chronic oxidative stress, nutritional deficiencies (especially selenium), and the chronic inflammation associated with this condition. All of these can lead to reduced activity or reduced levels of GPx, which is essential for defending against free radicals and maintaining the health of the nervous system. Several studies have consistently observed lower glutathione levels in patients with schizophrenia. These low levels may be caused by a number of factors, such as increased oxidative stress, deficient synthesis, nutrient deficiency, mitochondrial dysfunction, chronic inflammation, environment and lifestyle, and the effects of medications.
Deficiencies of vitamins E and C in patients with schizophrenia may be caused mainly by increased oxidative stress, poor diet, lifestyle factors (such as smoking), metabolic changes and potential effects of medications (Table 2). All these factors together contribute to a decreased efficiency of these essential antioxidants, increasing oxidative stress and possibly affecting the pathophysiology of schizophrenia. Treating the lack of nutrition through diet, lifestyle changes and possibly the addition of supplements could help these individuals.
It is important to monitor these parameters to evaluate the effectiveness of dietary interventions in reducing oxidative stress and inflammation in patients with schizophrenia.
It has been proven that high levels of reactive oxygen species and dysfunction of the antioxidant system can cause significant damage to neuronal structure. Cognitive decline and abnormal behaviors have been associated with oxidative state deterioration. Thus, schizophrenia symptoms may arise due to the degradation of neuronal lipid membranes in certain areas or connections, caused by the excessive presence of reactive oxygen species [100]. The way diet, nutrients, and/or nutritional deficiencies can cause schizophrenia or exacerbate its symptoms is still a subject of research. However, various hypotheses have been proposed. These consist of factors such as inadequate diet, harmful eating habits, and/or nutritional deficiencies associated with the occurrence of hyperhomocysteinemia, oxidative-antioxidative imbalance, impaired immune system, and variations in levels of pro-inflammatory markers. The neuroprogressive hypothesis has highlighted the importance of oxidative stress and inflammation in schizophrenia, suggesting that these changes may represent possible mechanisms in the progression of the disease [2]. To better understand these complex relationships, the Figure 2 below illustrates how nutritional deficiencies can influence the levels of reactive oxygen species and exacerbate schizophrenia symptoms. The effects of nutritional deficiencies on oxidative stress are highlighted, emphasizing the possible mechanisms by which these deficiencies contribute to disease progression.
Research has demonstrated that the disruption of the oxidative stress system can cause obesity by altering diet and promoting fat accumulation in the body [126].
Pro-inflammatory cytokines, microglial cells, astrocytes, and immune cells such as monocytes, macrophages, and T or B lymphocytes are involved in controlling inflammation in the central nervous system. A balanced inflammatory process is crucial for tissue health, but excessive inflammatory reactions can cause additional cellular damage. Uncontrolled inflammation can arise from infectious agents (such as bacteria or viruses), a reaction to neuronal injury from trauma, genetic defects, or environmental toxins [127]. In the central nervous system, inflammation can have neuroprotective or neurotoxic effects depending on the interactions between genetic variations, environmental factors, and inflammatory responses. The latest study on inflammation and schizophrenia indicates that inflammation can increase the risk of schizophrenia and exacerbate its symptoms [20].
Inflammation is considered a risk factor for schizophrenia because it contributes to the pathophysiology and exacerbation of these conditions. Various factors, including diet, can control the level of inflammation [20]. High-calorie foods, saturated fats, and simple carbohydrates can stimulate peripheral inflammatory markers, while foods rich in fiber and vegetables reduce inflammation [5]. Research has examined the role of polyunsaturated fats in psychosis. Two polyunsaturated fats are highlighted in the literature: essential fatty acids omega-3 and omega-6. Omega-6 fatty acids are pro-inflammatory, while omega-3 fatty acids are anti-inflammatory [128].
Accumulated information from previous research shows that inflammation has been identified as a factor in the development of schizophrenia [129]. In addition to the two important players in neuroinflammation, pro-inflammatory cytokines and microglial activation, a diet that causes inflammation exacerbates neuroinflammation by promoting the pathophysiological changes of schizophrenia and the severity of symptoms. Considering the impact that dietary regimes have on inflammatory markers, we emphasize the importance of nutrients such as omega-3 polyunsaturated fatty acids, vitamin D, and vitamin B in the treatment of schizophrenia symptoms [20].
A gut-brain connection should be examined for the link between dietary inflammation and schizophrenia. Changes in the composition of the microbiota and microbial metabolites influence gut health and immune system reactions. Gut imbalance has been noted in patients with schizophrenia, and the increased presence of certain types of bacteria, Succinivibrio and Corynebacterium, has been significantly correlated with the severity of schizophrenia symptoms [130]. Gut imbalance can influence susceptibility to infections and inflammation, leading to the acceleration of schizophrenia onset and symptom intensification. It is believed that dietary substances considered in schizophrenia exert their effects at least partially through the gut-brain axis [20].
The advice to consume anti-inflammatory nutrients or foods as part of a balanced diet has long-term benefits in reducing the side effects of medications. As a result, substances with anti-inflammatory properties are beneficial in reducing the severity of disease symptoms and decreasing risk factors that may trigger schizophrenia [20]. Vegetables, especially those untouched by chemicals or technological processes, contain high levels of antioxidant compounds that can counteract the harmful effects of redox processes in our bodies [131].
5. Conclusions
Schizophrenia is influenced by both genetic and environmental factors, including diet. Nutritional deficiencies, such as lack of omega-3 fatty acids, vitamin D, and B vitamins, during the prenatal and postnatal periods can negatively impact neurodevelopment and increase the risk of schizophrenia. Schizophrenia patients show antioxidant enzyme imbalances and reduced levels of antioxidants, leading to increased markers of oxidative stress. Cytokine-mediated inflammation, microglial activation, and gut dysbiosis are associated with schizophrenia onset and symptom severity. Currently, there is no universally accepted diet for the treatment of schizophrenia. However, different diets and nutritional methods, such as the Mediterranean diet, the ketogenic diet, the gluten-free diet, and the DASH diet, are being researched and applied to alleviate symptoms and improve overall health. A healthy diet rich in anti-inflammatory and antioxidant nutrients can help manage schizophrenia by reducing oxidative stress and improving quality of life. Omega-3 fatty acids are crucial for brain development and function. Omega-3 fatty acid deficiency is associated with an increased risk of schizophrenia. In addition, vitamin D deficiency is common in people with schizophrenia and is related to the severity of symptoms. Adequate levels of vitamin D are important for brain development and function. Also, B vitamins, especially folic acid, vitamin B6 and vitamin B12, play an essential role in cellular metabolism and neurotransmission. Deficiencies of these vitamins are linked to an increased risk of schizophrenia.
As the relationship between diet, nutrition and schizophrenia continues to evolve, it is likely that tailored dietary interventions will become an increasingly important part of comprehensive treatment plans for people with schizophrenia. Future research should focus on identifying the specific dietary patterns, nutrient combinations, and gut microbiome profiles that are most effective in reducing symptoms and improving outcomes for people with schizophrenia.
Author Contributions
Conceptualization, A.V., V.R., and A.C.; methodology, A.V., V.R., and A.C.; resources, A.V., V.R., and A.C.; writing—original draft preparation, A.V., V.R., V.B., G.H. and A.C.; writing—review and editing, A.V., V.R., G.H. and A.C.; visualization, A.V., V.R., and A.C.; supervision, V.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Jacka, F.N.; Mykletun, A.; Berk, M. Moving towards a Population Health Approach to the Primary Prevention of Common Mental Disorders. BMC Med. 2012, 10. [Google Scholar] [CrossRef] [PubMed]
- Onaolapo, O.J.; Onaolapo, A.Y. Nutrition, Nutritional Deficiencies, and Schizophrenia: An Association Worthy of Constant Reassessment. World J. Clin. Cases 2021, 9. [Google Scholar] [CrossRef]
- Tang, P.Y.; Tee, S.F.; Su, K.P. Editorial: The Link between Nutrition and Schizophrenia. Front. Psychiatry 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- El Kirat, H.; Khattabi, A.; Khalis, M.; Belrhiti, Z. Effects of Physical Activity and Nutrient Supplementation on Symptoms and Well-Being of Schizophrenia Patients: An Umbrella Review. Schizophr. Res. 2023, 262. [Google Scholar] [CrossRef] [PubMed]
- Firth, J.; Veronese, N.; Cotter, J.; Shivappa, N.; Hebert, J.R.; Ee, C.; Smith, L.; Stubbs, B.; Jackson, S.E.; Sarris, J. What Is the Role of Dietary Inflammation in Severe Mental Illness? A Review of Observational and Experimental Findings. Front. Psychiatry 2019, 10. [Google Scholar] [CrossRef] [PubMed]
- Sarris, J. Nutritional Psychiatry: From Concept to the Clinic. Drugs 2019, 79. [Google Scholar] [CrossRef]
- Owen, L.; Corfe, B. The Role of Diet and Nutrition on Mental Health and Wellbeing. Proc. Nutr. Soc. 2017, 76. [Google Scholar] [CrossRef]
- Zhang, R.; Zhang, B.; Shen, C.; Sahakian, B.J.; Li, Z.; Zhang, W.; Zhao, Y.; Li, Y.; Feng, J.; Cheng, W. Associations of Dietary Patterns with Brain Health from Behavioral, Neuroimaging, Biochemical and Genetic Analyses. Nat. Ment. Heal. 2024, 2, 535–552. [Google Scholar] [CrossRef]
- Peet, M. Diet, Diabetes and Schizophrenia: Review and Hypothesis. In Proceedings of the British Journal of Psychiatry; 2004; Vol. 184.
- Elman, I.; Borsook, D.; Lukas, S.E. Food Intake and Reward Mechanisms in Patients with Schizophrenia: Implications for Metabolic Disturbances and Treatment with Second-Generation Antipsychotic Agents. Neuropsychopharmacology 2006, 31. [Google Scholar] [CrossRef]
- Schwarzenberg, S.J.; Georgieff, M.K. Advocacy for Improving Nutrition in the First 1000 Days to Support Childhood Development and Adult Health. Pediatrics 2018, 141. [Google Scholar] [CrossRef]
- Enderami, A.; Zarghami, M.; Darvishi-Khezri, H. The Effects and Potential Mechanisms of Folic Acid on Cognitive Function: A Comprehensive Review. Neurol. Sci. 2018, 39. [Google Scholar] [CrossRef] [PubMed]
- Maekawa, M.; Watanabe, A.; Iwayama, Y.; Kimura, T.; Hamazaki, K.; Balan, S.; Ohba, H.; Hisano, Y.; Nozaki, Y.; Ohnishi, T.; et al. Polyunsaturated Fatty Acid Deficiency during Neurodevelopment in Mice Models the Prodromal State of Schizophrenia through Epigenetic Changes in Nuclear Receptor Genes. Transl. Psychiatry 2017, 7. [Google Scholar] [CrossRef] [PubMed]
- He, P.; Chen, G.; Guo, C.; Wen, X.; Song, X.; Zheng, X. Long-Term Effect of Prenatal Exposure to Malnutrition on Risk of Schizophrenia in Adulthood: Evidence from the Chinese Famine of 1959–1961. Eur. Psychiatry 2018, 51. [Google Scholar] [CrossRef] [PubMed]
- Susser, E.; St Clair, D. Prenatal Famine and Adult Mental Illness: Interpreting Concordant and Discordant Results from the Dutch and Chinese Famines. Soc. Sci. Med. 2013, 97. [Google Scholar] [CrossRef]
- McGrath, J.; Brown, A.; St Clair, D. Prevention and Schizophrenia - The Role of Dietary Factors. Schizophr. Bull. 2011, 37. [Google Scholar] [CrossRef]
- Davis, J.; Eyre, H.; Jacka, F.N.; Dodd, S.; Dean, O.; McEwen, S.; Debnath, M.; McGrath, J.; Maes, M.; Amminger, P.; et al. A Review of Vulnerability and Risks for Schizophrenia: Beyond the Two Hit Hypothesis. Neurosci. Biobehav. Rev. 2016, 65. [Google Scholar] [CrossRef] [PubMed]
- Lally, J.; Gaughran, F. Vitamin D in Schizophrenia and Depression: A Clinical Review. BJPsych Adv. 2019, 25. [Google Scholar] [CrossRef]
- Schoenrock, S.A.; Tarantino, L.M. Developmental Vitamin D Deficiency and Schizophrenia: The Role of Animal Models. Genes, Brain Behav.
- Cha, H.Y.; Yang, S.J. Anti-Inflammatory Diets and Schizophrenia. Clin. Nutr. Res. 2020, 9. [Google Scholar] [CrossRef]
- Calvo, M.S.; Whiting, S.J.; Barton, C.N. Vitamin D Intake: A Global Perspective of Current Status. In Proceedings of the Journal of Nutrition; 2005; Vol. 135.
- Wassif, G.A.; Alrehely, M.S.; Alharbi, D.M.; Aljohani, A.A. The Impact of Vitamin D on Neuropsychiatric Disorders. Cureus 2023. [Google Scholar] [CrossRef]
- Hewison, M.; Bouillon, R.; Giovannucci, E.; Goltzman, D.; Meyer, M.; Welsh, J.E. Feldman and Pike’s Vitamin D: Volume Two: Disease and Therapeutics; 2023.
- Cui, X.; McGrath, J.J.; Burne, T.H.J.; Eyles, D.W. Vitamin D and Schizophrenia: 20 Years On. Mol. Psychiatry 2021, 26. [Google Scholar] [CrossRef]
- Van Der Leeuw, C.; De Witte, L.D.; Stellinga, A.; Van Der Ley, C.; Bruggeman, R.; Kahn, R.S.; Van Os, J.; Marcelis, M. Vitamin D Concentration and Psychotic Disorder: Associations with Disease Status, Clinical Variables and Urbanicity. Psychol. Med. 2020, 50. [Google Scholar] [CrossRef] [PubMed]
- Häfner, H.; Nowotny, B. Epidemiology of Early-Onset Schizophrenia. Eur. Arch. Psychiatry Clin. Neurosci. 1995, 245. [Google Scholar] [CrossRef] [PubMed]
- Hsu, M.C.; Huang, Y.S.; Ouyang, W.C. Beneficial Effects of Omega-3 Fatty Acid Supplementation in Schizophrenia: Possible Mechanisms. Lipids Health Dis. 2020, 19. [Google Scholar] [CrossRef] [PubMed]
- Van Erp, T.G.M.; Hibar, D.P.; Rasmussen, J.M.; Glahn, D.C.; Pearlson, G.D.; Andreassen, O.A.; Agartz, I.; Westlye, L.T.; Haukvik, U.K.; Dale, A.M.; et al. Subcortical Brain Volume Abnormalities in 2028 Individuals with Schizophrenia and 2540 Healthy Controls via the ENIGMA Consortium. Mol. Psychiatry 2016, 21. [Google Scholar] [CrossRef]
- Bruce, K.D.; Zsombok, A.; Eckel, R.H. Lipid Processing in the Brain: A Key Regulator of Systemic Metabolism. Front. Endocrinol. (Lausanne). 2017, 8. [Google Scholar] [CrossRef] [PubMed]
- Mocking, R.J.T.; Assies, J.; Ruhé, H.G.; Schene, A.H. Focus on Fatty Acids in the Neurometabolic Pathophysiology of Psychiatric Disorders. J. Inherit. Metab. Dis. 2018, 41. [Google Scholar] [CrossRef] [PubMed]
- Hedelin, M.; Löf, M.; Olsson, M.; Lewander, T.; Nilsson, B.; Hultman, C.M.; Weiderpass, E. Dietary Intake of Fish, Omega-3, Omega-6 Polyunsaturated Fatty Acids and Vitamin D and the Prevalence of Psychotic-like Symptoms in a Cohort of 33 000 Women from the General Population. BMC Psychiatry 2010, 10. [Google Scholar] [CrossRef] [PubMed]
- Lange, K.W. Omega-3 Fatty Acids and Mental Health. Glob. Heal. J. 2020, 4. [Google Scholar] [CrossRef]
- Amminger, G.P.; Schäfer, M.R.; Schlögelhofer, M.; Klier, C.M.; McGorry, P.D. Longer-Term Outcome in the Prevention of Psychotic Disorders by the Vienna Omega-3 Study. Nat. Commun. 2015, 6. [Google Scholar] [CrossRef]
- Bozzatello, P.; De Rosa, M.L.; Rocca, P.; Bellino, S. Effects of Omega 3 Fatty Acids on Main Dimensions of Psychopathology. Int. J. Mol. Sci. 2020, 21. [Google Scholar] [CrossRef]
- Bourre, J.M.; Faivre, A.; Dumont, O.; Nouvelot, A.; Loudes, C.; Puymirat, J.; Tixier-Vidal, A. Effect of Polyunsaturated Fatty Acids on Fetal Mouse Brain Cells in Culture in a Chemically Defined Medium. J. Neurochem. 1983, 41. [Google Scholar] [CrossRef] [PubMed]
- Bourre, J.M.; Pascal, G.; Durand, G.; Masson, M.; Dumont, O.; Piciotti, M. Alterations in the Fatty Acid Composition of Rat Brain Cells (Neurons, Astrocytes, and Oligodendrocytes) and of Subcellular Fractions (Myelin and Synaptosomes) Induced by a Diet Devoid of N-3 Fatty Acids. J. Neurochem. 1984, 43. [Google Scholar] [CrossRef] [PubMed]
- Bourre, J.-M. Acides Gras ω-3 et Troubles Psychiatriques. médecine/sciences 2005, 21. [Google Scholar] [CrossRef] [PubMed]
- Blasbalg, T.L.; Hibbeln, J.R.; Ramsden, C.E.; Majchrzak, S.F.; Rawlings, R.R. Changes in Consumption of Omega-3 and Omega-6 Fatty Acids in the United States during the 20th Century. Am. J. Clin. Nutr. 2011, 93. [Google Scholar] [CrossRef] [PubMed]
- Caffrey, A.; McNulty, H.; Irwin, R.E.; Walsh, C.P.; Pentieva, K. Maternal Folate Nutrition and Offspring Health: Evidence and Current Controversies. In Proceedings of the Proceedings of the Nutrition Society; 2019; Vol. 78.
- Cusick, S.E.; Georgieff, M.K. The Role of Nutrition in Brain Development: The Golden Opportunity of the “First 1000 Days. ” J. Pediatr. 2016, 175. [Google Scholar] [CrossRef] [PubMed]
- Fryar-Williams, S.; Strobel, J.; Clements, P. Molecular Mechanisms Provide a Landscape for Biomarker Selection for Schizophrenia and Schizoaffective Psychosis. Int. J. Mol. Sci. 2023, 24. [Google Scholar] [CrossRef]
- García-Miss, M. del R.; Pérez-Mutul, J.; López-Canul, B.; Solís-Rodríguez, F.; Puga-Machado, L.; Oxté-Cabrera, A.; Gurubel-Maldonado, J.; Arankowsky-Sandoval, G. Folate, Homocysteine, Interleukin-6, and Tumor Necrosis Factor Alfa Levels, but Not the Methylenetetrahydrofolate Reductase C677T Polymorphism, Are Risk Factors for Schizophrenia. J. Psychiatr. Res. 2010, 44. [Google Scholar] [CrossRef]
- Bouaziz, N.; Ayedi, I.; Sidhom, O.; Kallel, A.; Rafrafi, R.; Jomaa, R.; Melki, W.; Feki, M.; Kaabechi, N.; El Hechmi, Z. Plasma Homocysteine in Schizophrenia: Determinants and Clinical Correlations in Tunisian Patients Free from Antipsychotics. Psychiatry Res. 2010, 179. [Google Scholar] [CrossRef] [PubMed]
- Cao, B.; Sun, X.Y.; Zhang, C.B.; Yan, J.J.; Zhao, Q.Q.; Yang, S.Y.; Yan, L.L.; Huang, N. hua; Zeng, J.; Liao, J.Y.; et al. Association between B Vitamins and Schizophrenia: A Population-Based Case-Control Study. Psychiatry Res. 2018, 259. [Google Scholar] [CrossRef]
- Jose, R.; Venketeswaramurthy, N.; Sambath Kumar, R. A Critical Review on Hypothesis, Pathophysiology of Schizophrenia, and Role of Vitamins in Its Management. Asian J. Pharm. Clin. Res. 2018, 11. [Google Scholar] [CrossRef]
- Susser, E.; Neugebauer, R.; Hoek, H.W.; Brown, A.S.; Lin, S.; Labovitz, D.; Gorman, J.M. Schizophrenia after Prenatal Famine Further Evidence. Arch. Gen. Psychiatry 1996, 53. [Google Scholar] [CrossRef] [PubMed]
- Roffma, R.J.L.; Lamberti, S.; Achtyes, E.; Macklin, E.A.; Galendez, G.; Raeke, L.; Silverstein, N.J.; Tuinstra, D.; Hill, M.; Goff, D.C. A Multi-Center Investigation of Folate plus B12 Supplementation in Schizophrenia. Neuropsychopharmacology 2011, 36. [Google Scholar]
- Lewis, C.J.; Crane, N.T.; Wilson, D.B.; Yetley, E.A. Estimated Folate Intakes: Data Updated to Reflect Food Fortification, Increased Bioavailability, and Dietary Supplement Use. Am. J. Clin. Nutr. 1999, 70. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, D.O. B Vitamins and the Brain: Mechanisms, Dose and Efficacy—A Review. Nutrients 2016, 8. [Google Scholar] [CrossRef]
- Dayabandara, M.; Hanwella, R.; Ratnatunga, S.; Seneviratne, S.; Suraweera, C.; de Silva, V.A. Antipsychotic-Associated Weight Gain: Management Strategies and Impact on Treatment Adherence. Neuropsychiatr. Dis. Treat. 2017, 13. [Google Scholar] [CrossRef]
- De Hert, M.; Detraux, J.; Van Winkel, R.; Yu, W.; Correll, C.U. Metabolic and Cardiovascular Adverse Effects Associated with Antipsychotic Drugs. Nat. Rev. Endocrinol. 2012, 8. [Google Scholar] [CrossRef]
- Holt, R.I.G. The Management of Obesity in People with Severe Mental Illness: An Unresolved Conundrum. Psychother. Psychosom. 2019, 88. [Google Scholar] [CrossRef]
- Fleischhacker, W.W.; Cetkovich-Bakmas, M.; De Hert, M.; Hennekens, C.H.; Lambert, M.; Leucht, S.; Maj, M.; McIntyre, R.S.; Naber, D.; Newcomer, J.W.; et al. Comorbid Somatic Illnesses in Patients with Severe Mental Disorders: Clinical, Policy, and Research Challenges. In Proceedings of the Journal of Clinical Psychiatry; 2008; Vol. 69.
- Maayan, L.; Correll, C.U. Management of Antipsychotic-Related Weight Gain. Expert Rev. Neurother. 2010, 10. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, J.G. Induction of Obesity by Psychotropic Drugs. Ann. N. Y. Acad. Sci. 1987, 499. [Google Scholar] [CrossRef]
- De Hert, M.; Dekker, J.M.; Wood, D.; Kahl, K.G.; Holt, R.I.G.; Möller, H.J. Cardiovascular Disease and Diabetes in People with Severe Mental Illness Position Statement from the European Psychiatric Association (EPA), Supported by the European Association for the Study of Diabetes (EASD) and the European Society of Cardiology (ESC). Eur. Psychiatry 2009, 24. [Google Scholar] [CrossRef]
- Allison, D.B.; Mentore, J.L.; Heo, M.; Chandler, L.P.; Cappelleri, J.C.; Infante, M.C.; Weiden, P.J. Antipsychotic-Induced Weight Gain: A Comprehensive Research Synthesis. Am. J. Psychiatry 1999, 156. [Google Scholar] [CrossRef]
- Lu, M.L.; Wang, T.N.; Lin, T.Y.; Shao, W.C.; Chang, S.H.; Chou, J.Y.; Ho, Y.F.; Liao, Y.T.; Chen, V.C.H. Differential Effects of Olanzapine and Clozapine on Plasma Levels of Adipocytokines and Total Ghrelin. Prog. Neuro-Psychopharmacology Biol. Psychiatry 2015, 58. [Google Scholar] [CrossRef] [PubMed]
- Ader, M.; Kim, S.P.; Catalano, K.J.; Ionut, V.; Hucking, K.; Richey, J.M.; Kabir, M.; Bergman, R.N. Metabolic Dysregulation with Atypical Antipsychotics Occurs in the Absence of Underlying Disease: A Placebo-Controlled Study of Olanzapine and Risperidone in Dogs. Diabetes 2005, 54. [Google Scholar] [CrossRef] [PubMed]
- Silverstone, T.; Smith, G.; Goodall, E. Prevalence of Obesity in Patients Receiving Depot Antipsychotics. Br. J. Psychiatry 1988, 153. [Google Scholar] [CrossRef]
- Kim, M.; Yang, S.J.; Kim, H.H.; Jo, A.; Jhon, M.; Lee, J.Y.; Ryu, S.H.; Kim, J.M.; Kweon, Y.R.; Kim, S.W. Effects of Dietary Habits on General and Abdominal Obesity in Community-Dwelling Patients with Schizophrenia. Clin. Psychopharmacol. Neurosci. 2023, 21. [Google Scholar] [CrossRef] [PubMed]
- Hägg, S.; Söderberg, S.; Ahrén, B.; Olsson, T.; Mjörndal, T. Leptin Concentrations Are Increased in Subjects Treated with Clozapine or Conventional Antipsychotics. J. Clin. Psychiatry 2001, 62. [Google Scholar] [CrossRef]
- Zabeau, L.; Lavens, D.; Peelman, F.; Eyckerman, S.; Vandekerckhove, J.; Tavernier, J. The Ins and Outs of Leptin Receptor Activation. FEBS Lett. 2003, 546. [Google Scholar] [CrossRef]
- Dohan, F.C.; Grasberger, J.C.; Lowell, F.M.; Johnston, H.T.; Arbegast, A.W. Relapsed Schizophrenics: More Rapid Improvement on a Milk- and Cereal-Free Diet. Br. J. Psychiatry 1969, 115. [Google Scholar] [CrossRef]
- Tsigalou, C.; Konstantinidis, T.; Paraschaki, A.; Stavropoulou, E.; Voidarou, C.; Bezirtzoglou, E. Mediterranean Diet as a Tool to Combat Inflammation and Chronic Diseases. An Overview. An Overview. Biomedicines 2020, 8. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean Diet and Survival in a Greek Population. N. Engl. J. Med. 2003, 348. [Google Scholar] [CrossRef]
- Dobrosielski, D.A.; Papandreou, C.; Patil, S.P.; Salas-Salvadó, J. Diet and Exercise in the Management of Obstructive Sleep Apnoea and Cardiovascular Disease Risk. Eur. Respir. Rev. 2017, 26. [Google Scholar] [CrossRef] [PubMed]
- Kinsman, S.L.; Vining, E.P.G.; Quaskey, S.A.; Mellits, D.; Freeman, J.M. Efficacy of the Ketogenic Diet for Intractable Seizure Disorders: Review of 58 Cases. Epilepsia 1992, 33. [Google Scholar] [CrossRef] [PubMed]
- Sarnyai, Z.; Kraeuter, A.K.; Palmer, C.M. Ketogenic Diet for Schizophrenia: Clinical Implication. Curr. Opin. Psychiatry 2019, 32. [Google Scholar] [CrossRef] [PubMed]
- Blumenthal, J.A.; Babyak, M.A.; Hinderliter, A.; Watkins, L.L.; Craighead, L.; Lin, P.H.; Caccia, C.; Johnson, J.; Waugh, R.; Sherwood, A. Effects of the DASH Diet Alone and in Combination with Exercise and Weight Loss on Blood Pressure and Cardiovascular Biomarkers in Men and Women with High Blood Pressure: The ENCORE Study. Arch. Intern. Med. 2010, 170. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Wallin, A.; Wolk, A. Dietary Approaches to Stop Hypertension Diet and Incidence of Stroke. Stroke 2016, 47. [Google Scholar] [CrossRef] [PubMed]
- Miller, E.R.; Erlinger, T.P.; Young, D.R.; Jehn, M.; Charleston, J.; Rhodes, D.; Wasan, S.K.; Appel, L.J. Results of the Diet, Exercise, and Weight Loss Intervention Trial (DEW-IT). Hypertension 2002, 40. [Google Scholar] [CrossRef] [PubMed]
- Gurusamy, J.; Gandhi, S.; Damodharan, D.; Ganesan, V.; Palaniappan, M. Exercise, Diet and Educational Interventions for Metabolic Syndrome in Persons with Schizophrenia: A Systematic Review. Asian J. Psychiatr. 2018, 36. [Google Scholar] [CrossRef] [PubMed]
- Bostock, E.C.S.; Kirkby, K.C.; Taylor, B.V.M. The Current Status of the Ketogenic Diet in Psychiatry. Front. Psychiatry 2017, 8. [Google Scholar] [CrossRef]
- Ntalkitsi, S.; Efthymiou, D.; Bozikas, V.; Vassilopoulou, E. Halting the Metabolic Complications of Antipsychotic Medication in Patients with a First Episode of Psychosis: How Far Can We Go with the Mediterranean Diet? A Pilot Study. Nutrients 2022, 14. [Google Scholar] [CrossRef]
- Kraeuter, A.K.; Loxton, H.; Lima, B.C.; Rudd, D.; Sarnyai, Z. Ketogenic Diet Reverses Behavioral Abnormalities in an Acute NMDA Receptor Hypofunction Model of Schizophrenia. Schizophr. Res. 2015, 169. [Google Scholar] [CrossRef]
- Sorić, T.; Mavar, M.; Rumbak, I. The Effects of the Dietary Approaches to Stop Hypertension (DASH) Diet on Metabolic Syndrome in Hospitalized Schizophrenic Patients: A Randomized Controlled Trial. Nutrients 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- Teasdale, S.B.; Ward, P.B.; Rosenbaum, S.; Watkins, A.; Curtis, J.; Kalucy, M.; Samaras, K. A Nutrition Intervention Is Effective in Improving Dietary Components Linked to Cardiometabolic Risk in Youth with First-Episode Psychosis. Br. J. Nutr. 2016, 115. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Zhu, M.; Liu, X.; Zhao, Z.; Han, P.; Lv, L.; Yang, C.; Han, Y. Calorie-Restricted Diet Mitigates Weight Gain and Metabolic Abnormalities in Obese Women with Schizophrenia: A Randomized Controlled Trial. Front. Nutr. 2023, 10. [Google Scholar] [CrossRef] [PubMed]
- Redman, L.M.; Ravussin, E. Caloric Restriction in Humans: Impact on Physiological, Psychological, and Behavioral Outcomes. Antioxidants Redox Signal. 2011, 14. [Google Scholar] [CrossRef] [PubMed]
- Zubrzycki, A.; Cierpka-Kmiec, K.; Kmiec, Z.; Wronska, A. The Role of Low-Calorie Diets and Intermittent Fasting in the Treatment of Obesity and Type-2 Diabetes. J. Physiol. Pharmacol. 2018, 69. [Google Scholar]
- Leidy, H.J.; Clifton, P.M.; Astrup, A.; Wycherley, T.P.; Westerterp-Plantenga, M.S.; Luscombe-Marsh, N.D.; Woods, S.C.; Mattes, R.D. The Role of Protein in Weight Loss and Maintenance. Am. J. Clin. Nutr. 2015, 101. [Google Scholar] [CrossRef] [PubMed]
- Dickerson, F.; Gennusa, J. V.; Stallings, C.; Origoni, A.; Katsafanas, E.; Sweeney, K.; Campbell, W.W.; Yolken, R. Protein Intake Is Associated with Cognitive Functioning in Individuals with Psychiatric Disorders. Psychiatry Res. 2020, 284. [Google Scholar] [CrossRef] [PubMed]
- Bergman, R.N.; Kim, S.P.; Hsu, I.R.; Catalano, K.J.; Chiu, J.D.; Kabir, M.; Richey, J.M.; Ader, M. Abdominal Obesity: Role in the Pathophysiology of Metabolic Disease and Cardiovascular Risk. Am. J. Med. 2007, 120. [Google Scholar] [CrossRef]
- Phaniendra, A.; Jestadi, D.B.; Periyasamy, L. Free Radicals: Properties, Sources, Targets, and Their Implication in Various Diseases. Indian J. Clin. Biochem. 2015, 30. [Google Scholar] [CrossRef]
- Young, G.; Conquer, J. Omega-3 Fatty Acids and Neuropsychiatric Disorders. Reprod. Nutr. Dev. 2005, 45. [Google Scholar] [CrossRef]
- Yao, J.K.; Keshavan, M.S. Antioxidants, Redox Signaling, and Pathophysiology in Schizophrenia: An Integrative View. Antioxidants Redox Signal. 2011, 15. [Google Scholar] [CrossRef] [PubMed]
- Ndhlala, A.R.; Moyo, M.; Van Staden, J. Natural Antioxidants: Fascinating or Mythical Biomolecules? Molecules 2010, 15. [Google Scholar] [CrossRef] [PubMed]
- Arvindakshan, M.; Ghate, M.; Ranjekar, P.K.; Evans, D.R.; Mahadik, S.P. Supplementation with a Combination of ω-3 Fatty Acids and Antioxidants (Vitamins E and C) Improves the Outcome of Schizophrenia. Schizophr. Res. 2003, 62. [Google Scholar] [CrossRef]
- Bentsen, H.; Osnes, K.; Refsum, H.; Solberg, D.K.; Bøhmer, T. A Randomized Placebo-Controlled Trial of an Omega-3 Fatty Acid and Vitamins E+C in Schizophrenia. Transl. Psychiatry 2013, 3. [Google Scholar] [CrossRef]
- Brown, H.E.; Roffman, J.L. Vitamin Supplementation in the Treatment of Schizophrenia. CNS Drugs 2014, 28. [Google Scholar] [CrossRef]
- Ciobica, A.; Padurariu, M.; Dobrin, I.; Stefanescu, C.; Dobrin, R. Oxidative Stress in Schizophrenia - Focusing on the Main Markers. Psychiatr. Danub. 2011, 23. [Google Scholar]
- Buosi, P.; Borghi, F.A.; Lopes, A.M.; da Silva Facincani, I.; Fernandes-Ferreira, R.; Oliveira-Brancati, C.I.F.; Do Carmo, T.S.; Souza, D.R.S.; da Silva, D.G.H.; de Almeida, E.A.; et al. Oxidative Stress Biomarkers in Treatment-Responsive and Treatment-Resistant Schizophrenia Patients. Trends Psychiatry Psychother. 2021, 43. [Google Scholar] [CrossRef]
- Ben Othmen, L.; Mechri, A.; Fendri, C.; Bost, M.; Chazot, G.; Gaha, L.; Kerkeni, A. Altered Antioxidant Defense System in Clinically Stable Patients with Schizophrenia and Their Unaffected Siblings. Prog. Neuro-Psychopharmacology Biol. Psychiatry 2008, 32. [Google Scholar] [CrossRef] [PubMed]
- Reyazuddin, M.; Azmi, S.A.; Islam, N.; Rizvi, A. Oxidative Stress and Level of Antioxidant Enzymes in Drug-Naive Schizophrenics. Indian J. Psychiatry 2014, 56. [Google Scholar] [CrossRef]
- Djordjevic, V.; Lazarevic, D.; Cosic, V.; Knezevic, M.; Djordjevic, V. Age-Related Changes of Superoxide Dismutase Activity in Patients with Schizophrenia. Vojnosanit. Pregl. 2017, 74. [Google Scholar] [CrossRef]
- Djordjević, V. V.; Kostić, J.; Krivokapić, Ž.; Krtinić, D.; Ranković, M.; Petković, M.; Ćosić, V. Decreased Activity of Erythrocyte Catalase and Glutathione Peroxidase in Patients with Schizophrenia. Med. 2022, 58. [Google Scholar] [CrossRef]
- Gawryluk, J.W.; Wang, J.F.; Andreazza, A.C.; Shao, L.; Young, L.T. Decreased Levels of Glutathione, the Major Brain Antioxidant, in Post-Mortem Prefrontal Cortex from Patients with Psychiatric Disorders. Int. J. Neuropsychopharmacol. 2011, 14. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.K.; Leonard, S.; Reddy, R. Altered Glutathione Redox State in Schizophrenia. Dis. Markers 2006, 22. [Google Scholar] [CrossRef] [PubMed]
- Murray, A.J.; Rogers, J.C.; Katshu, M.Z.U.H.; Liddle, P.F.; Upthegrove, R. Oxidative Stress and the Pathophysiology and Symptom Profile of Schizophrenia Spectrum Disorders. Front. Psychiatry 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Dietrich-Muszalska, A.; Kwiatkowska, A. Generation of Superoxide Anion Radicals and Platelet Glutathione Peroxidase Activity in Patients with Schizophrenia. Neuropsychiatr. Dis. Treat. 2014, 10. [Google Scholar] [CrossRef] [PubMed]
- Michel, T.M.; Thome, J.; Martin, D.; Nara, K.; Zwerina, S.; Tatschner, T.; Weijers, H.G.; Koutsilieri, E. Cu, Zn- And Mn-Superoxide Dismutase Levels in Brains of Patients with Schizophrenic Psychosis. J. Neural Transm. 2004, 111. [Google Scholar] [CrossRef] [PubMed]
- Abdalla, D.S.P.; Monteiro, H.P.; Oliveira, J.A.C.; Bechara, E.J.H. Activities of Superoxide Dismutase and Glutathione Peroxidase in Schizophrenic and Manic-Depressive Patients. Clin. Chem. 1986, 32. [Google Scholar] [CrossRef]
- Djordjević, V. Superoxide Dismutase in Psychiatric Diseases. In; 2022.
- Hurşitoğlu, O.; Orhan, F.Ö.; Kurutaş, E.B.; Doğaner, A.; Durmuş, H.T.; Kopar, H. Diagnostic Performance of Increased Malondialdehyde Level and Oxidative Stress in Patients with Schizophrenia. Noropsikiyatri Ars. 2021, 58. [Google Scholar] [CrossRef]
- Rukmini, M.S.; D’Souza, B.; D’Souza, V. Superoxide Dismutase and Catalase Activities and Their Correlation with Malondialdehyde in Schizophrenic Patients. Indian J. Clin. Biochem. 2004, 19. [Google Scholar] [CrossRef]
- Sarandol, A.; Kirli, S.; Akkaya, C.; Altin, A.; Demirci, M.; Sarandol, E. Oxidative-Antioxidative Systems and Their Relation with Serum S100 B Levels in Patients with Schizophrenia: Effects of Short Term Antipsychotic Treatment. Prog. Neuro-Psychopharmacology Biol. Psychiatry 2007, 31. [Google Scholar] [CrossRef]
- Surapaneni, K.; Venkataramana, G. Status of Lipid Peroxidation, Glutathione, Ascorbic Acid, Vitamin E and Antioxidant Enzymes in Patients with Osteoarthritis. Indian J. Med. Sci. 2007, 61. [Google Scholar] [CrossRef]
- Wu, Z.; Zhang, X.Y.; Wang, H.; Tang, W.; Xia, Y.; Zhang, F.X.; Liu, J.; Fu, Y.; Hu, J.; Chen, Y.; et al. Elevated Plasma Superoxide Dismutase in First-Episode and Drug Naive Patients with Schizophrenia: Inverse Association with Positive Symptoms. Prog. Neuro-Psychopharmacology Biol. Psychiatry 2012, 36. [Google Scholar] [CrossRef] [PubMed]
- Gong, Y.; Zhao, R.; Yang, B. Superoxide Dismutase Activity and Malondialdehyde Levels in Patients with Travel-Induced Psychosis. Shanghai Arch. Psychiatry 2012, 24. [Google Scholar] [CrossRef]
- Li, X.R.; Xiu, M.H.; Guan, X.N.; Wang, Y.C.; Wang, J.; Leung, E.; Zhang, X.Y. Altered Antioxidant Defenses in Drug-Naive First Episode Patients with Schizophrenia Are Associated with Poor Treatment Response to Risperidone: 12-Week Results from a Prospective Longitudinal Study. Neurotherapeutics 2021, 18. [Google Scholar] [CrossRef] [PubMed]
- Do, K.Q.; Bovet, P.; Cuenod, M. Schizophrenia: Glutathione Deficit as a New Vulnerability Factor for Disconnectivity Syndrome. Schweizer Arch. fur Neurol. und Psychiatr. 2004, 155. [Google Scholar] [CrossRef]
- Raffa, M.; Atig, F.; Mhalla, A.; Kerkeni, A.; Mechri, A. Decreased Glutathione Levels and Impaired Antioxidant Enzyme Activities in Drug-Naive First-Episode Schizophrenic Patients. BMC Psychiatry 2011, 11. [Google Scholar] [CrossRef] [PubMed]
- Langbein, K.; Hesse, J.; Gussew, A.; Milleit, B.; Lavoie, S.; Amminger, G.P.; Gaser, C.; Wagner, G.; Reichenbach, J.R.; Hipler, U.C.; et al. Disturbed Glutathione Antioxidative Defense Is Associated with Structural Brain Changes in Neuroleptic-Naïve First-Episode Psychosis Patients. Prostaglandins Leukot. Essent. Fat. Acids 2018, 136. [Google Scholar] [CrossRef] [PubMed]
- Palaniyappan, L.; Park, M.T.M.; Jeon, P.; Limongi, R.; Yang, K.; Sawa, A.; Théberge, J. Is There a Glutathione Centered Redox Dysregulation Subtype of Schizophrenia? Antioxidants 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Iwata, Y.; Nakajima, S.; Plitman, E.; Truong, P.; Bani-Fatemi, A.; Caravaggio, F.; Kim, J.; Shah, P.; Mar, W.; Chavez, S.; et al. Glutathione Levels and Glutathione-Glutamate Correlation in Patients with Treatment-Resistant Schizophrenia. Schizophr. Bull. Open 2021, 2. [Google Scholar] [CrossRef]
- Dakhale, G.N.; Khanzode, S.D.; Khanzode, S.S.; Saoji, A. Supplementation of Vitamin C with Atypical Antipsychotics Reduces Oxidative Stress and Improves the Outcome of Schizophrenia. Psychopharmacology (Berl). 2005, 182. [Google Scholar] [CrossRef]
- Sarandol, A.; Sarandol, E.; Acikgoz, H.E.; Eker, S.S.; Akkaya, C.; Dirican, M. First-Episode Psychosis Is Associated with Oxidative Stress: Effects of Short-Term Antipsychotic Treatment. Psychiatry Clin. Neurosci. 2015, 69. [Google Scholar] [CrossRef] [PubMed]
- Gunes, M.; Camkurt, M.A.; Demir, S.; Ibiloglu, A.; Kaya, M.C.; Bulut, M.; Atli, A. Serum Malonyldialdehyde Levels of Patients with Schizophrenia. Klin. Psikofarmakol. Bul. 2015, 25. [Google Scholar]
- Kropp, S.; Kern, V.; Lange, K.; Degner, D.; Hajak, G.; Kornhuber, J.; Rütlier, E.; Emrich, H.M.; Schneider, U.; Bleich, S. Oxidative Stress during Treatment with First- and Second-Generation Antipsychotics. J. Neuropsychiatry Clin. Neurosci. 2005, 17. [Google Scholar] [CrossRef]
- Uddin, S.M.N.; Sultana, F.; Uddin, M.G.; Dewan, S.M.R.; Hossain, M.K.; Islam, M.S. Effect of Antioxidant, Malondialdehyde, Macro-Mineral, and Trace Element Serum Concentrations in Bangladeshi Patients with Schizophrenia: A Case-Control Study. Heal. Sci. Reports 2021, 4. [Google Scholar] [CrossRef] [PubMed]
- Xiang, Y.Z.; Yun, L.T.; Dong, F.Z.; Lian, Y.C.; Gui, Y.W.; Haile, C.N.; Kosten, T.A.; Kosten, T.R. Disrupted Antioxidant Enzyme Activity and Elevated Lipid Peroxidation Products in Schizophrenic Patients with Tardive Dyskinesia. J. Clin. Psychiatry 2007, 68. [Google Scholar] [CrossRef]
- Al-Fartusie, F.S.; Al-Bairmani, H.K.; Al-Garawi, Z.S.; Yousif, A.H. Evaluation of Some Trace Elements and Vitamins in Major Depressive Disorder Patients: A Case–Control Study. Biol. Trace Elem. Res. 2019, 189. [Google Scholar] [CrossRef]
- Myken, A.N.; Ebdrup, B.H.; Sørensen, M.E.; Broberg, B. V.; Skjerbæk, M.W.; Glenthøj, B.Y.; Lykkesfeldt, J.; Nielsen, M. Lower Vitamin C Levels Are Associated with Less Improvement in Negative Symptoms in Initially Antipsychotic-Naïve Patients with First-Episode Psychosis. Int. J. Neuropsychopharmacol. 2022, 25. [Google Scholar] [CrossRef] [PubMed]
- Subotičanec, K.; Folnegović-Šmalc, V.; Korbar, M.; Meštrović, B.; Buzina, R. Vitamin C Status in Chronic Schizophrenia. Biol. Psychiatry 1990, 28. [Google Scholar] [CrossRef] [PubMed]
- Guan, X.; Chen, Y.; Wang, X.; Xiu, M.; Wu, F.; Zhang, X. Total Antioxidant Capacity, Obesity and Clinical Correlates in First-Episode and Drug-Naïve Patients with Schizophrenia. Schizophr. Res. 2024, 264. [Google Scholar] [CrossRef]
- Müller, N.; Weidinger, E.; Leitner, B.; Schwarz, M.J. The Role of Inflammation in Schizophrenia. Front. Neurosci. 2015, 9. [Google Scholar] [CrossRef]
- Innes, J.K.; Calder, P.C. Omega-6 Fatty Acids and Inflammation. Prostaglandins Leukot. Essent. Fat. Acids 2018, 132. [Google Scholar] [CrossRef] [PubMed]
- Miller, B.J.; Goldsmith, D.R. Inflammatory Biomarkers in Schizophrenia: Implications for Heterogeneity and Neurobiology. Biomarkers in Neuropsychiatry 2019, 1. [Google Scholar] [CrossRef]
- Li, S.; Zhuo, M.; Huang, X.; Huang, Y.; Zhou, J.; Xiong, D.; Li, J.; Liu, Y.; Pan, Z.; Li, H.; et al. Altered Gut Microbiota Associated with Symptom Severity in Schizophrenia. PeerJ 2020, 8. [Google Scholar] [CrossRef] [PubMed]
- Deledda, A.; Annunziata, G.; Tenore, G.C.; Palmas, V.; Manzin, A.; Velluzzi, F. Diet-Derived Antioxidants and Their Role in Inflammation, Obesity and Gut Microbiota Modulation. Antioxidants 2021, 10. [Google Scholar] [CrossRef]
Figure 1.
The impact of different types of diets on obesity caused by antipsychotic drugs. ↑, increase/improve; ↓, decrease; ⮕, leads to.
Figure 1.
The impact of different types of diets on obesity caused by antipsychotic drugs. ↑, increase/improve; ↓, decrease; ⮕, leads to.
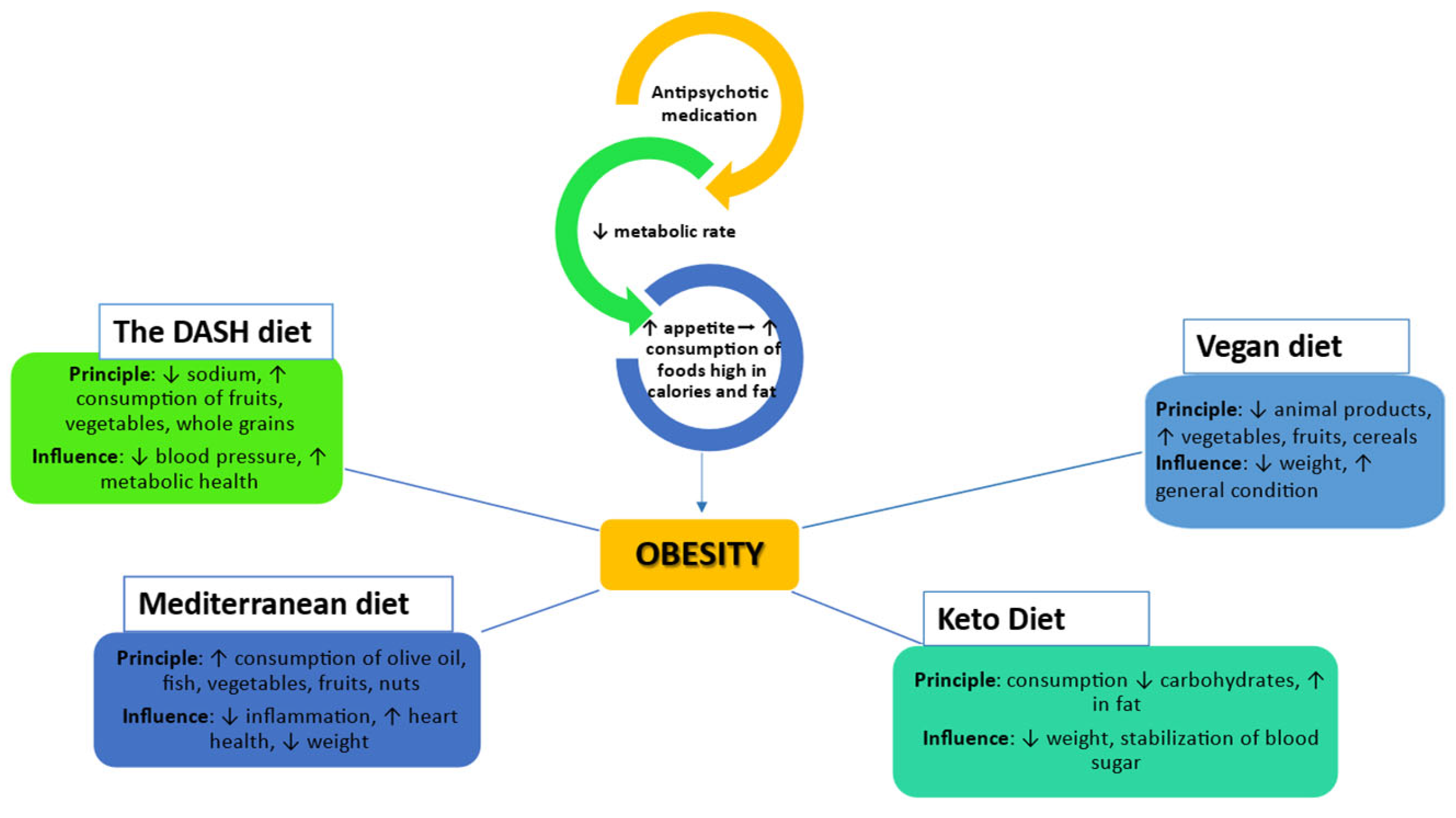
Figure 2.
Impact of nutritional deficits on ROS production and exacerbation of schizophrenia symptoms. ↑, increase; ↓, decrease; CAT, Catalase; Gpx, Glutathione peroxidase; MDA, Malondialdehyde; OS, oxidative stress; ROS, reactive oxygen species.
Figure 2.
Impact of nutritional deficits on ROS production and exacerbation of schizophrenia symptoms. ↑, increase; ↓, decrease; CAT, Catalase; Gpx, Glutathione peroxidase; MDA, Malondialdehyde; OS, oxidative stress; ROS, reactive oxygen species.
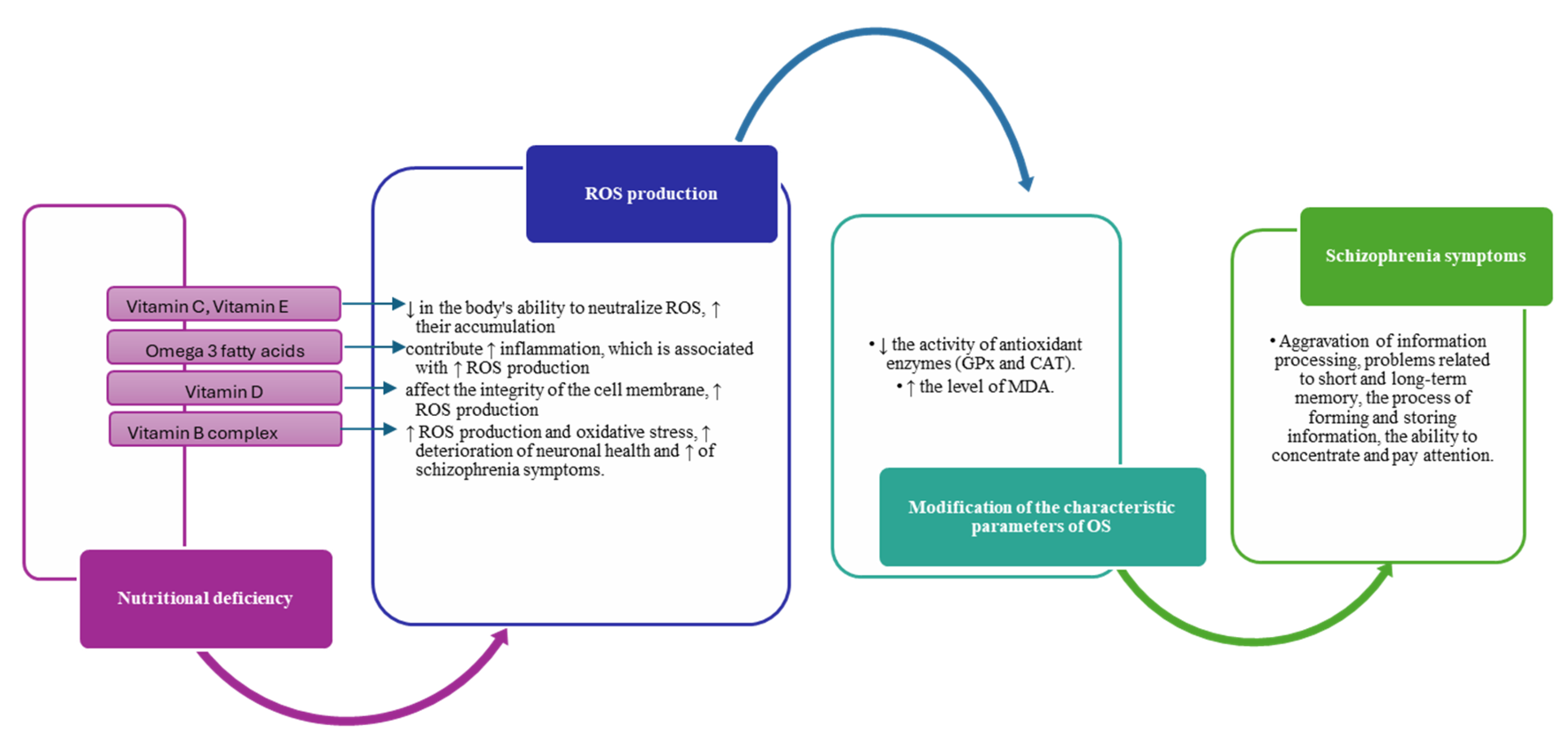

Table 1.
Effects of different types of diets on antipsychotic-induced obesity in patients with schizophrenia.
Table 1.
Effects of different types of diets on antipsychotic-induced obesity in patients with schizophrenia.
| The type of diet | Description | Effects on obesity | Mechanism of action | References |
|---|---|---|---|---|
| Ketogenic Diet | High in fat, moderate in protein, low in carbohydrates | Weight loss, reductions in visceral adipose tissue, glycosylated hemoglobin and triglycerides | Mood stabilization and cognitive function | [74] |
| Mediterranean diet | Rich in vegetables, fruits, fish, olive oil, whole grains | Reduces the risk of obesity and improving metabolism | Improves metabolic and immunity outcomes | [75,76] |
| Diet DASH | Rich in vegetables, fruits, low-fat dairy products, whole grains | lowers triglycerides, lowers fasting blood glucose and improves insulin resistance | Reduce inflammation and oxidative stress, improve vascular and metabolic function. | [77,78] |
| Calorie restriction diet | Caloric restriction with balanced intake of macronutrients | Improves weight and metabolic markers | Reduce inflammation and oxidative stress, improve insulin sensitivity and metabolic health. | [79] [80,81] |
| High Protein Diet | Includes animal and vegetable protein sources | Maintain muscle mass, reducing body fat | Stabilizing blood sugar, reducing inflammation and improving neural function. | [82,83] |
| Gluten-free diet | Exclude all foods containing gluten | Improvements in negative symptoms | Reducing inflammatory responses | [64] |
Table 2.
Biochemical changes of some parameters related to oxidative stress in patients with schizophrenia.
Table 2.
Biochemical changes of some parameters related to oxidative stress in patients with schizophrenia.
| Parameter category | Evaluated parameter | The level found relative to the normal range | References |
|---|---|---|---|
| Antioxidant enzyme | GPx | Normal level | [93] |
| Low level | [94,95,96,97,98,99,100,101] | ||
| SOD | Low level | [93,95,101,102] | |
| Increased level | [103,104,105,106,107,108,109,110] | ||
| CAT | Increased level | [93,105,106,111] | |
| Low level | [97,102] | ||
| GSH | Low level | [112][113,114,115,116] | |
| Biomarkers | MDA | Increased level | [93,95,97,105,108,110,117,118,119,120,121,122] |
| Antioxidants | Vitamin E | Low level | [108,121,123] |
| Vitamin C | Low level | [117,121,124,125] | |
| CAT, catalase; GPx, glutathione peroxidase; GSH, glutathione; MDA, malondialdehyde; SOD = superoxide dismutase. | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



