Submitted:
22 July 2024
Posted:
22 July 2024
You are already at the latest version
Abstract
Management of resistant Tuberculosis (TB) can be extremely difficult, especially in case of novel unpredicted complications. In this report, we present a case of a 48-year-old patient with pre-extensive-drug-resistant-(XDR)-TB who received a treatment regimen including Pretomanid, Bedaquiline, Linezolid, Cycloserine and Amikacin and died due to myocarditis. Acquired resistance to first- and second-line drugs developed due to previous poor adherence to medication. The clinical presentation of the patient, along with her initial ultrasonographical, electrocardiogram (ECG) and laboratory examinations, were typical for acute myocarditis, however, the patient was considered unstable and further investigation with Magnetic Resonance Imaging (MRI), pericardiocentesis and endomyocardial biopsy were not performed. To our knowledge, this is the first case of myocarditis in such a patient, the clinical features of which set a high suspicion of drug-induction that could be attributed to the treatment regimen that was administered. Clinicians who manage cases of drug-resistant TB should be aware of this, newly reported, potentially lethal, adverse event.
Keywords:
adverse event 1
; drug-induced myocarditis 2
; pre-extensive-drug-resistant tuberculosis 3
; pretomanid 4
; case report 5
; low ejection fraction 6
1. Introduction
The management of patients with pre-extensive drug resistant Tuberculosis (pre-XDR-TB) is particularly demanding. TB treatment relies on a multi-drug therapy for long duration, and as a result the emergence of adverse reactions is inevitable [1]. Novel anti-Tuberculous (anti-TB) drugs include combinations with fluoroquinolones, aminoglycosides, bedaquiline, pretomanid, linezolid, cycloserine, linezolid and clofazimine [2]. Minor adverse effects are relatively common, and they can be easily managed with symptomatic treatment. However, new unexpected challenges can always emerge in every-day practice, especially in cases of potentially lethal adverse events, which might be related to those novel drugs.
Several anti-TB drugs may be associated with significant cardiac toxicity; bedaquiline, clofazimine, delamanid, and fluoroquinolones (especially moxifloxacin) have been associated with QTc prolongation. If QTc > 500 ms, the suspected drug(s) should be stopped, electrolytes should be checked and corrected if needed, and electrocardiograms should be monitored until normalized [1]. However, there are no reports regarding an association between myocarditis and use of novel anti-TB drugs. To our knowledge, this is the first case of myocarditis in a patient with a history of pre-XDR-TB, the clinical features of which set a high suspicion of drug-induction that could be attributed to the treatment regimen that was administered.
2. Case Report
A 48-year-old Eastern European female, with relapse of cavitary pulmonary pre-extensive drug resistant Tuberculosis (pre-XDR-TB), without extrapulmonary manifestations, for which she had received treatment with first- and second-line drugs in the past, without success, due to poor compliance to the treatment regimens, was admitted to the hospital and initiated an in-hospital treatment regimen with Pretomanid, Bedaquiline, Linezolid, Cycloserine and Amikacin. This extended regimen was selected off label based on the patient’s history of Linezolid use as part of her previous regimens and her drug susceptibility testing (DST) which showed sensitivity to Cycloserine and Amikacin. DST for Linezolid cannot be performed in Greece.
Upon admission, her clinical status was poor due to her extensive pulmonary involvement (Figure 1). Her oxygenation was marginal (SaO2: 92%), she presented with cough, purulent sputum, hemoptysis, fever, night sweats and considerable weight loss (body mass index (BMI): 17.8 Kg/m2). Her sputum smear and culture were positive for pre-XDR-TB. Her history was otherwise unremarkable.
After following the aforementioned treatment regimen for 35 days, her clinical status improved, as her symptoms declined, she gained weight and her smear sample, obtained via bronchoscopy, converted to negative. Despite her physicians’ advice, she was discharged from hospital on her own will, and continued her treatment at home. Five days later, she presented to the emergency department with worsening dyspnea from three days. She was hemodynamically unstable despite fluid resuscitation, while her oxygenation was severely low (pO2: at 37 mmHg at room air) and did not improve sufficiently after initiating treatment with high flow nasal cannula (HFNC), thus she was intubated and admitted to the intensive care unit (ICU).
In the ICU, cardiac ultrasound revealed the following images and videos (Figure 2, Videos S1 and S2).
Cardiac ultrasound was remarkable for severe systolic dysfunction of the LV with akinesia of the mid and apical segments (Video A1, Video A2) compensatory basal hyperkinesis (Video A2), and a total EF of < 20% (Video A1, Video A2). Pericardial fluid was also evident, mainly in front of the right ventricle (~1,9cm), without signs of incipient tamponade (Figure 2).
Laboratory testing revealed an increase in hs-troponin (1655 pg/ml, range < 11,6 pg/ml), SGOT (638 U/L) and SGPT (358 U/L). Electrocardiogram (ECG) was remarkable for negative T waves in I, aVL, V5 and V6 leads and a poor R progression in the precordial leads, without QT-interval prolongation (Figure 3).
Based on the patient’s clinical presentation along with her ECG, cardiac ultrasound and laboratory tests the main diagnosis which was vital to be confirmed or excluded was the acute myocardial infarction. In this case a coronary CT angiography was performed, from which no critical stenosis was found (calcium score = 0). A coronary angiography, although it is an invasive method compared to coronary CT angiography, might be more appropriate in such cases, since it provides the ability to treat a critical stenosis, if any, in the coronary arteries [3], even though in this case, it was proved that the problem was not such.
A massive pulmonary embolus could cause severe hypoxia along with hemodynamic instability and match with the clinical presentation. The patient’s laboratory findings and some of the ECG findings might also be present in a massive pulmonary embolus, however cardiac ultrasound would have revealed different findings, such as an enlarged right ventricle (RV), possibly larger than LV, with or without a D-shaped intraventricular septum, along with signs of RV dysfunction, such as a decreased tricuspid annular plane systolic excursion (TAPSE) and possibly an increased pulmonary artery systolic pressure (PASP) [4], rendering the diagnosis of a massive pulmonary emboli rather unlikely and the performance of a CTPA rather unnecessary.
The patient might also have suffered from pulmonary hypertension due to her chronic pulmonary disease; however pulmonary hypertension is not usually presented with such a fulminant insult [5], thus it would be rather unlikely to be the cause of the patient’s clinical presentation. On the other hand, continuous hemodynamic monitoring would be extremely helpful in this case, however, other, less invasive methods than RHC are available for that [6], thus, at this stage, RHC might have been not only unnecessary, but also risky, since, as an invasive modality, is related with various complications [7]. In this case minimally invasive continuous hemodynamic monitoring confirmed the low CO (cardiac index (CI):1,4L/min/m²).
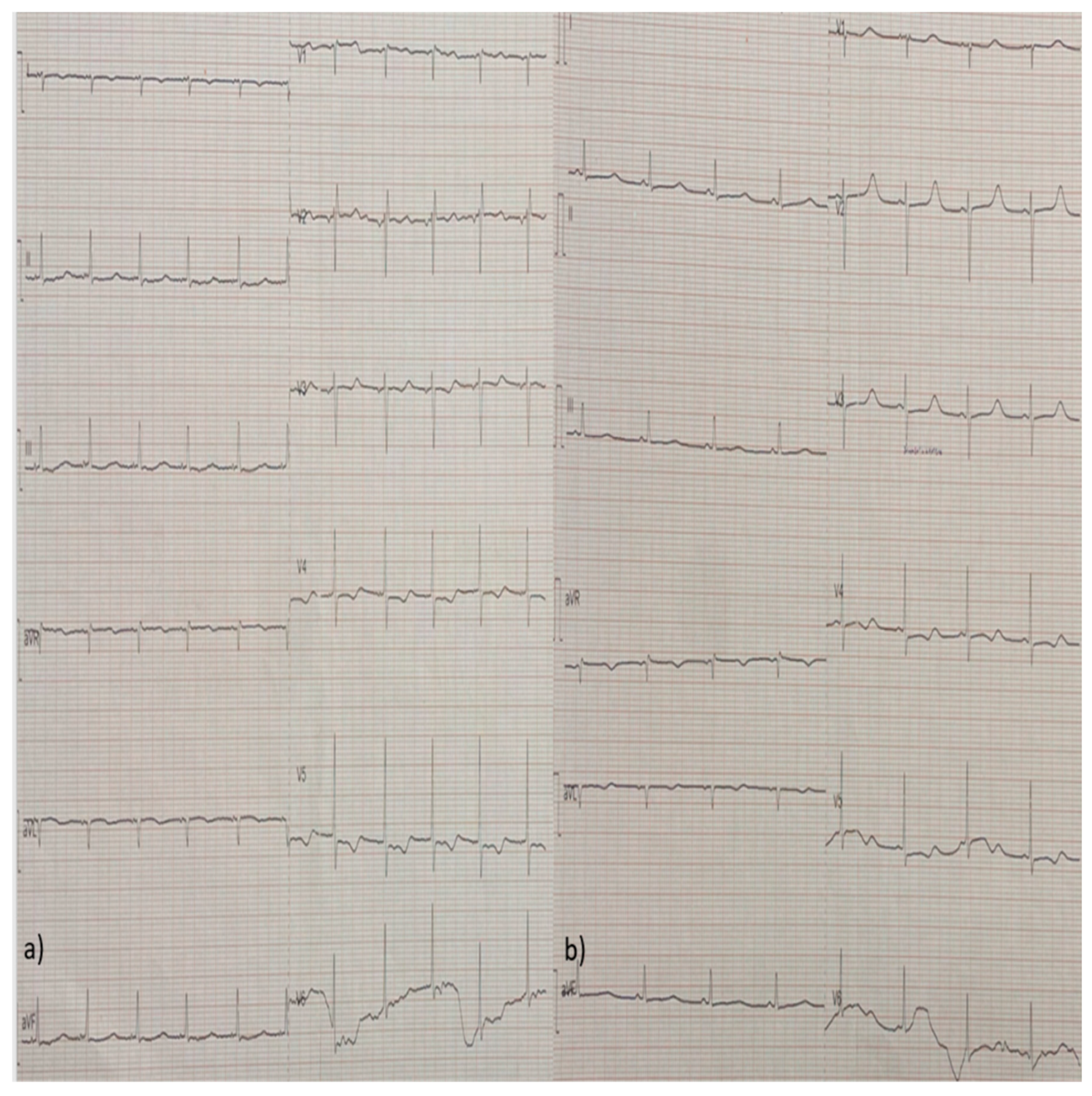
Due to the low CO and the clinical signs of tissue hypoperfusion dobutamine and phenylephrine was initiated, as well as colchicine for the pericardial effusion. In the following days, the patient’s LV systolic function was restored and her pericardial fluid diminished. Her hs-troponin levels also decreased and remained stable between 100-200 pg/ml during her rest hospitalization. She also presented eosinophilia (>1000/μL) between the 5th and 9th day after her admission, which was not related with drug initiation or discontinuation or stool parasites, while her complete serological examinations for infectious and auto-immune diseases came back negative. Her follow-up ECGs were notable for low atrial rhythm, repolarization disorders of the ST-segment and T-wave inversion of varying amplitudes, which progressed in different leads through time (Figure 4a,b, Figure 5a,b, Figure 6a,b, Figure 7a,b and Figure 8a,b).
Despite her cardiac function restoration, the patient was unable to wean from mechanical ventilation due to the severe damages of her lung parenchyma and eventually died four weeks later from septic shock due to Klebsiella pneumonia.
3. Discussion
The clinical presentation of the patient, along with her initial ultrasonographical, ECG and laboratory examinations and their progression throughout the course of her hospitalization, were typical for acute myocarditis [8], although the diagnosis and its aetiology could not be investigated further with cardiac Magnetic Resonance Imaging (MRI) or pericardiocentesis, as the patient was considered unstable and her pericardial fluid was relatively low in quantity. Due to her critical condition, a cardiac biopsy was not performed either.
An obvious cause of the patient’s condition was tuberculosis of the myocardium. However, this possibility seems rather unlikely since the patient reported resolvement of her symptoms and had responded positively to treatment. Furthermore, TB myocarditis is rare (prevalence varies between 0.14% and 2%), and also presents and progresses insidiously rather than acutely [9,10].
In a recent expert consensus document [11], the causes of myocarditis were grouped in three categories: 1) infectious, 2) immunological and 3) drug-induced [11]. In this case, the patient had no history of systemic inflammatory disease and her serological examinations for both auto-immune and infectious diseases were negative, leading to the possibility of drug reaction. Drug-induced myocarditis is characterized by eosinophilic infiltration of myocardium and peripheral eosinophilia, which might be evident in the course of the disease, but can be absent in up to 25% of the cases at admission [11,12,13]. This type of drug hypersensitivity reaction is particularly difficult to recognize, because clinical features such as fever, malaise and skin rush might be absent in most cases [13,14,15]. The latency period from drug initiation to the emergence of myocarditis typically varies between 2-5 weeks for the majority of the implicated substances [13,14,15,16,17,18]. Although our patient’s characteristics match with all the aforementioned clinical features, unfortunately, the diagnosis could not be confirmed with cardia MRI, pericardiocentesis or cardiac biopsy.
Drug-induced acute myocarditis seems to be the most probable diagnosis in this case, however, not only the aetiology of the myocarditis could not be proved with certainty, but also none of the drugs that the patient received has been implicated with such a diagnosis in the past. Amikacin is related with nephron- and ear-toxicity, Linezolid with bone marrow suppression (in this case the patient had also received Linezolid in the past), while Cycloserine is related with psychotic symptomatology and although anti-psychotics are the most frequently related drugs with acute myocarditis [13], the patient was under supervision and had not received a drug of this category, while she was treated in-hospital for her pre-XDR-TB, prior to her ICU admission.
Nevertheless, the patient did receive recently approved anti-TB medications, which alone, or co-administered with other drugs, might have triggered this reaction. More particularly, even though Bedaquiline has been in circulation for quite a while, Pretomanid is a novel anti-TB medication, which, up to early 2021, has been administered in varying dosing regimens, alone, or in combination with other anti-TB drugs, in eight clinical trials with 1168 participants in total [19], and although myocarditis has not been reported as an adverse event [19], the number of patients that have been treated with it, is too small to can safely exclude this case scenario.
Last but not least, after reporting the suspected adverse events of anti-TB drugs, another important issue is to establish whether there is a causal or temporal relationship between the drug and the adverse event. In other words, it is possible that the administered drug and the manifestation of an adverse event may have a close chronological relationship, but still not be a reaction. Pharmacovigilance dictates that clinicians who manage cases of pre-XDR-TB should be aware of such a contingency.
4. Conclusions
In conclusion, the management of pre-XDR-TB is particularly demanding [1], and novel anti-Tuberculous (anti-TB) drugs have been proved extremely helpful [2], however, new unexpected challenges can always emerge in every-day practice, especially in cases of potentially lethal adverse events, which might be related to those novel drugs. This is the first study to report a lethal case of myocarditis that could be attributed to the administration of novel anti-TB drugs, alone, or combined, with other medications for the treatment of pre-XDR-TB.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Video S1. Cardiac ultrasound was remarkable for severe systolic dysfunction of the LV. Video S2. Cardiac ultrasound showing compensatory basal hyperkinesis.
Author Contributions
KSC, PP and CG made substantial contributions to the conception of the study and the acquisition of data. KSC, PP, MA and AE drafted the manuscript. KSA, PP, BT and SM provided related scientific input and collected the clinical data. KSC and AE critically revised the manuscript. ME confirm the authenticity of all the raw data. All authors have accepted responsibility for the entire content of this manuscript and have approved the submission. All authors have read and approved the final manuscript.
Funding
No funding was received.
Informed Consent Statement
Written informed consent was obtained from the patient for the publication of this case report, including any accompanying figures.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- WHO consolidated guidelines on tuberculosis: Module 4: treatment - drug-resistant tuberculosis treatment, 2022 update [Internet]. Geneva: World Health Organization; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK588564/.
- Conradie, F.; Bagdasaryan. T.R.; Borisov, S.; Howell, P.; Mikiashvili, L.; Ngubane, N., Samoilova, A.; Skornykova. S.; Tudor, E.; et al. Bedaquiline-Pretomanid-Linezolid Regimens for Drug-Resistant Tuberculosis. N Engl J Med. 2022, 387(9):810-823. [CrossRef]
- Cury, R.C.; Budoff, M.; Taylor, A.J. Coronary CT angiography versus standard of care for assessment of chest pain in the emergency department. J Cardiovasc Comput Tomogr. 2013, 7(2):79-82. [CrossRef]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.J.; Harjola, V.P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; et al. The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS): The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). Eur Respir J. 2019, 54(3):1901647. [CrossRef]
- Humbert, M.; Kovacs, G.; Hoeper, M.M.; Badagliacca, R.; Berger, R.M.F.; Brida, M.; Carlsen, J.; Coats, A.J.S.; Escribano-Subias, P.; et al. ESC/ERS Scientific Document Group. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J. 2022, 43(38):3618-3731. [CrossRef]
- Teboul, J.L.; Saugel, B.; Cecconi, M.; De Backer, D.; Hofer, C.K.; Monnet, X.; Perel, A.; Pinsky, M.R.; Reuter, D.A.; et al. Less invasive hemodynamic monitoring in critically ill patients. Intensive Care Med. 2016, 42(9):1350-9. [CrossRef]
- Chen, Y.; Shlofmitz, E.; Khalid, N.; Bernardo, N.L.; Ben-Dor, I.; Weintraub, W.S.; Waksman, R. Right Heart Catheterization-Related Complications: A Review of the Literature and Best Practices. Cardiol Rev. 2020, 28(1):36-41. [CrossRef]
- Ammirati, E.; Moslehi, J.J. Diagnosis and Treatment of Acute Myocarditis: A Review. JAMA. 2023, 329(13):1098-1113. [CrossRef]
- López-López, J.P.; Posada-Martínez, E.L.; Saldarriaga, C.; Wyss, F.; Ponte-Negretti, C.I.; Alexander, B.; Miranda-Arboleda, A.F.; Martínez-Sellés, M.; Baranchuk, A. Neglected Tropical Diseases, Other Infectious Diseases Affecting the Heart (the NET‐Heart Project). Tuberculosis and the Heart. J Am Heart Assoc. 2021, 10(7):e019435. [CrossRef]
- Michira, B.N.; Alkizim, F.O.; Matheka, D.M. Patterns and clinical manifestations of tuberculous myocarditis: a systematic review of cases. Pan Afr Med J. 2015, 21:118. [CrossRef]
- Ammirati, E.; Frigerio, M.; Adler, E.D.; Basso, C.; Birnie, D.H.; Brambatti, M.; Friedrich, M.G.; Klingel, K.; Lehtonen, J.; et al. Management of Acute Myocarditis and Chronic Inflammatory Cardiomyopathy: An Expert Consensus Document. Circ Heart Fail. 2020, 13(11):e007405. [CrossRef]
- Lampejo, T.; Durkin, S.M.; Bhatt, N.; Guttmann, O. Acute myocarditis: aetiology, diagnosis and management. Clin Med (Lond). 2021, 21(5):e505-e510. [CrossRef]
- Nguyen, L.S.; Cooper, L.T.; Kerneis, M.;Funck-Brentano, C.; Silvain, J.; Brechot, N.; Hekimian, G.; Ammirati, E.; M’Barek, B.B.; et al. Systematic analysis of drug-associated myocarditis reported in the World Health Organization pharmacovigilance database. Nat Commun. 2022, 13: 25.
- Sagar, S.; Liu, P.P.; Cooper, L.T. Jr. Myocarditis. Lancet. 2012, 379(9817):738-47. [CrossRef]
- Seree-Aphinan, C.; Assanangkornchai, N.; Nilmoje, T. Prolonged Extracorporeal Membrane Oxygenation Support In a Patient with Drug Reaction with Eosinophilia and Systemic Symptoms Syndrome-associated Fulminant Myocarditis - A Case Report and Literature Review. Heart Int. 2020, 14(2):112-117. [CrossRef]
- Mahmood, S.S.; Fradley, M.G.; Cohen, J.V.; Nohria, A.; Reynolds, K.L.; Heinzerling, L.M.; Sullivan, R.J.; Damrongwatanasuk, R.; Chen, C.L.; et al. Myocarditis in Patients Treated With Immune Checkpoint Inhibitors. J Am Coll Cardiol. 2018, 71(16):1755-1764. [CrossRef]
- Ronaldson, K.J.; Fitzgerald, P.B.; Taylor, A.J.; Topliss, D.J.; McNeil, J.J. Clinical course and analysis of ten fatal cases of clozapine-induced myocarditis and comparison with 66 surviving cases. Schizophr Res. 2011, 128(1-3):161-5. [CrossRef]
- Uhara, H.; Saiki, M.; Kawachi, S.; Ashida, A,; Oguchi, S.; Okuyama, R. Clinical course of drug-induced hypersensitivity syndrome treated without systemic corticosteroids. J Eur Acad Dermatol Venereol. 2013, 27(6):722-6. [CrossRef]
- Gils, T.; Lynen, L.; de Jong, B.C.; Van Deun, A.; Decroo, T. Pretomanid for tuberculosis: a systematic review. Clin Microbiol Infect. 2022, 28(1):31-42. [CrossRef]
Figure 1.
Extensive pulmonary involvement of the patient upon admission.
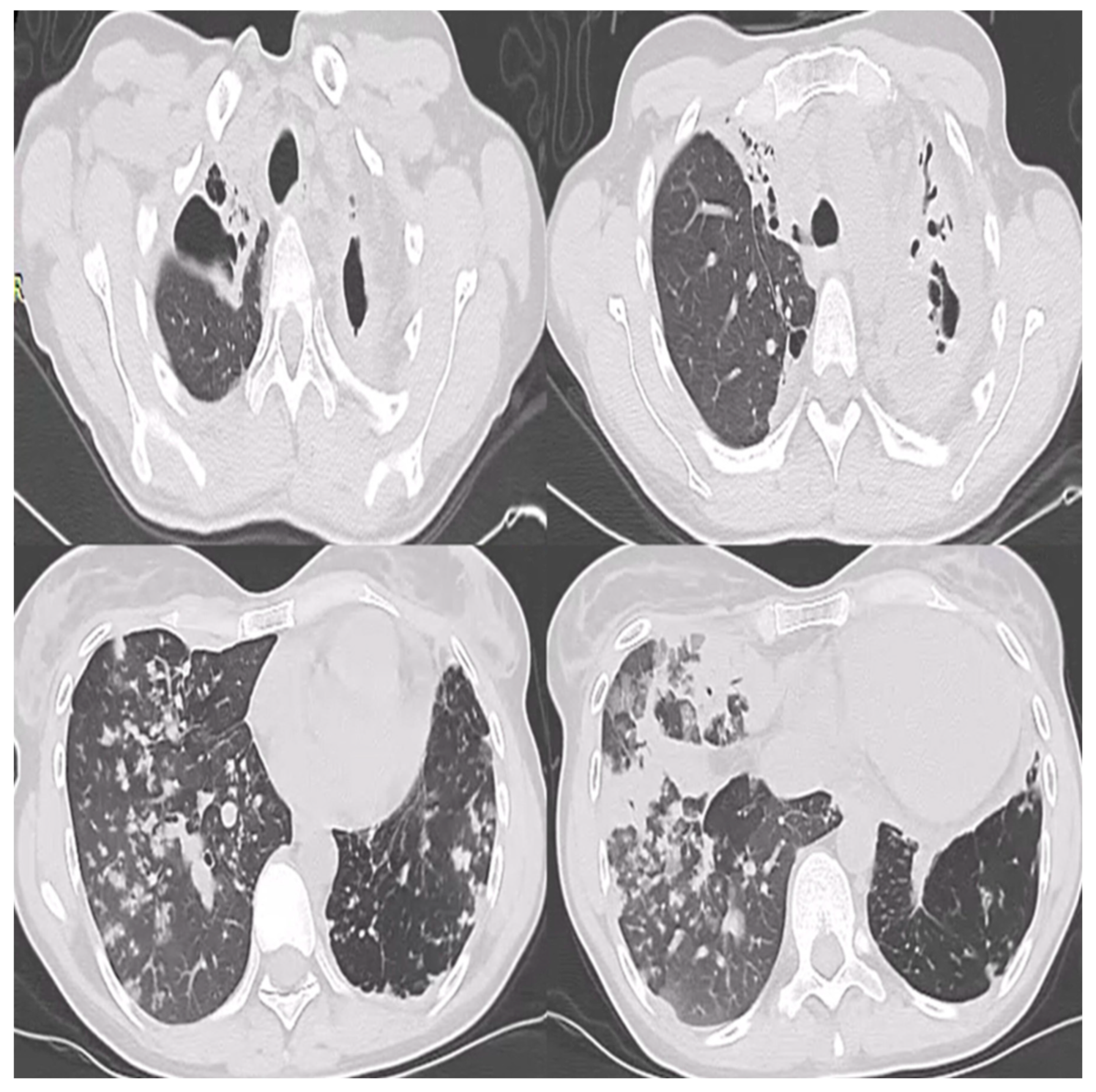
Figure 2.
Cardiac ultrasound findings of the patient showing severe systolic dysfunction and low ejection fraction.
Figure 2.
Cardiac ultrasound findings of the patient showing severe systolic dysfunction and low ejection fraction.
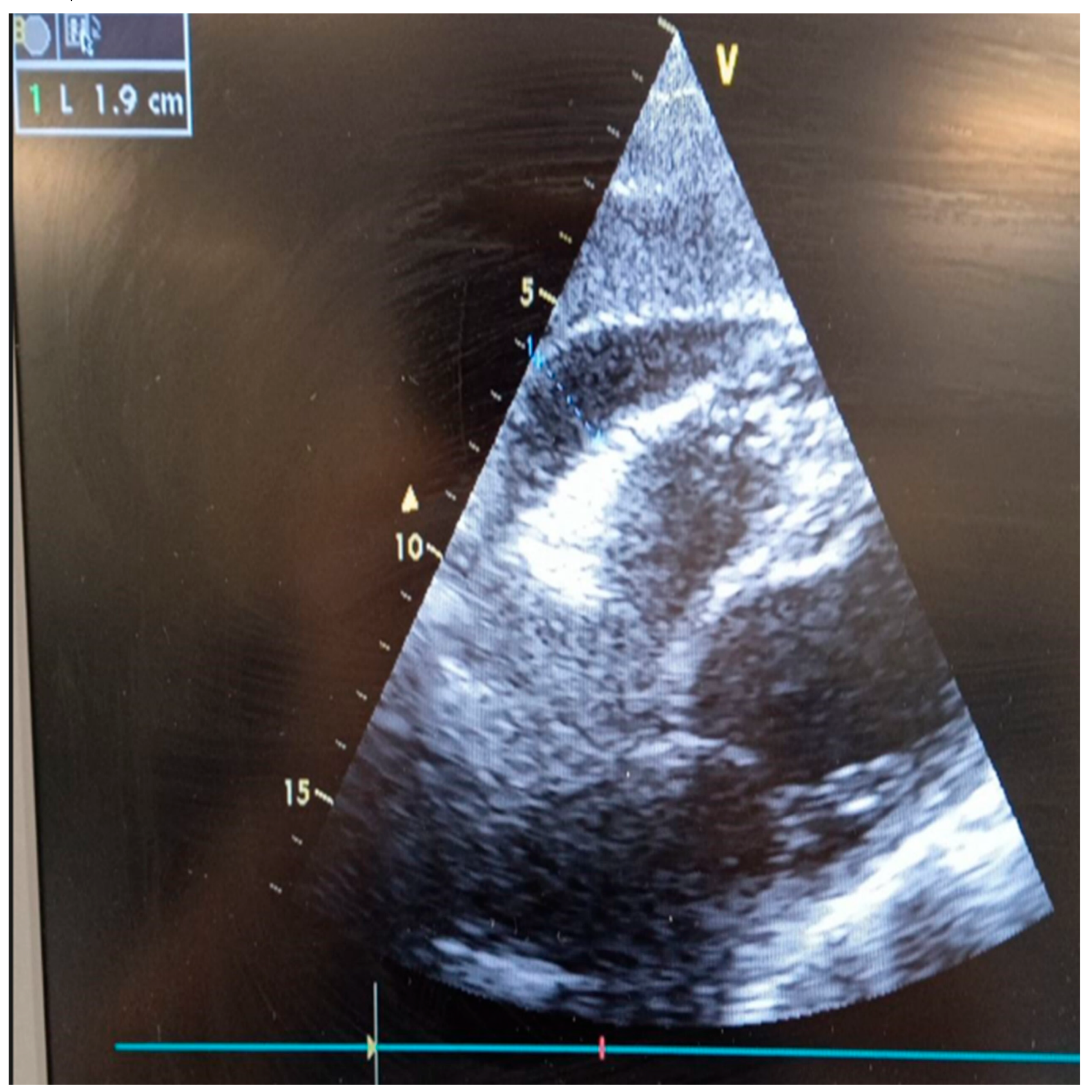
Figure 3.
ECG findings showing negative T waves in I, aVL, V5 and V6 leads and a poor R progression in the precordial leads.
Figure 3.
ECG findings showing negative T waves in I, aVL, V5 and V6 leads and a poor R progression in the precordial leads.
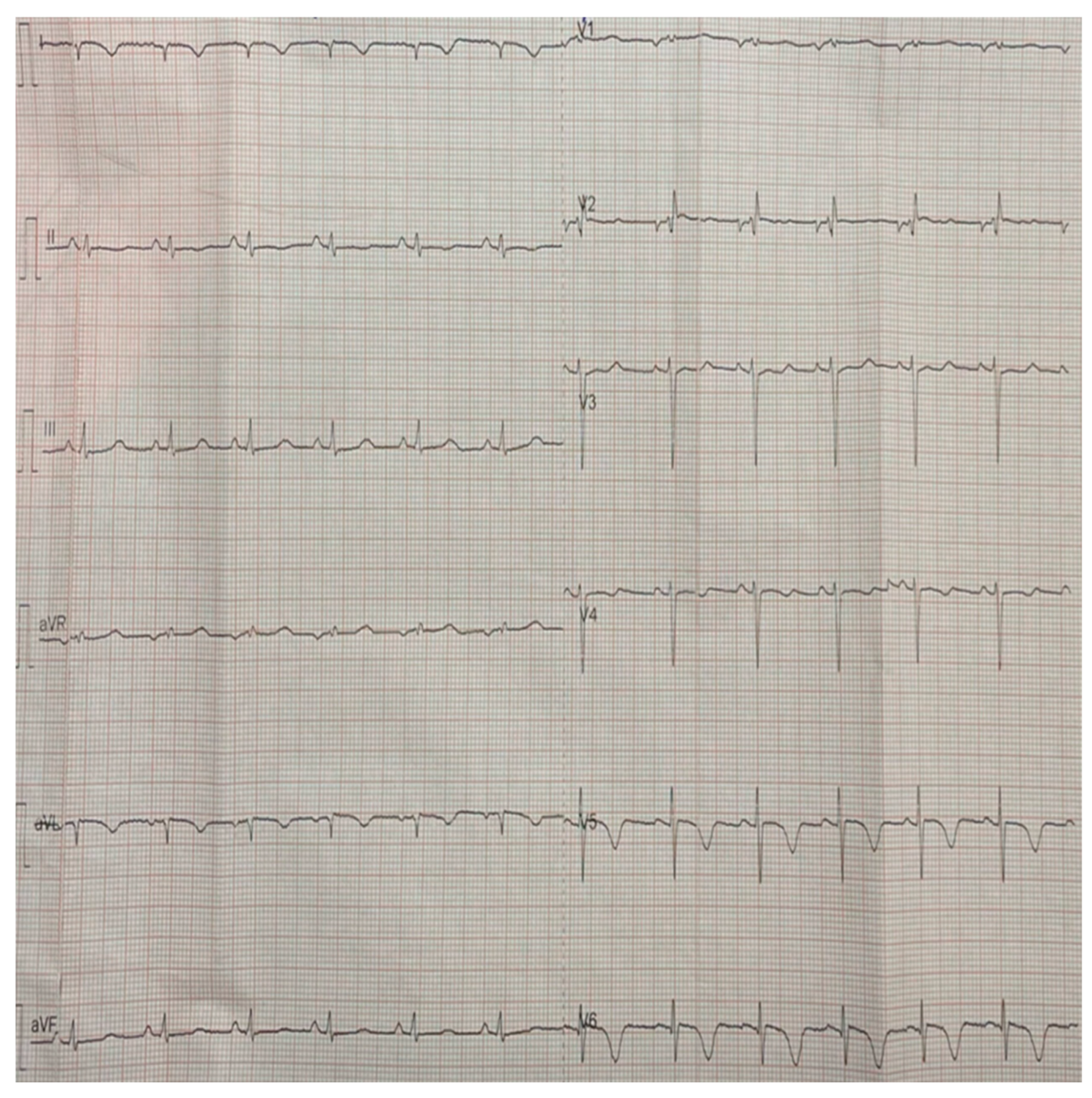
Figure 4.
a-b. Follow-up ECG showing repolarization disorders of the ST-segment and T-wave inversion.
Figure 4.
a-b. Follow-up ECG showing repolarization disorders of the ST-segment and T-wave inversion.
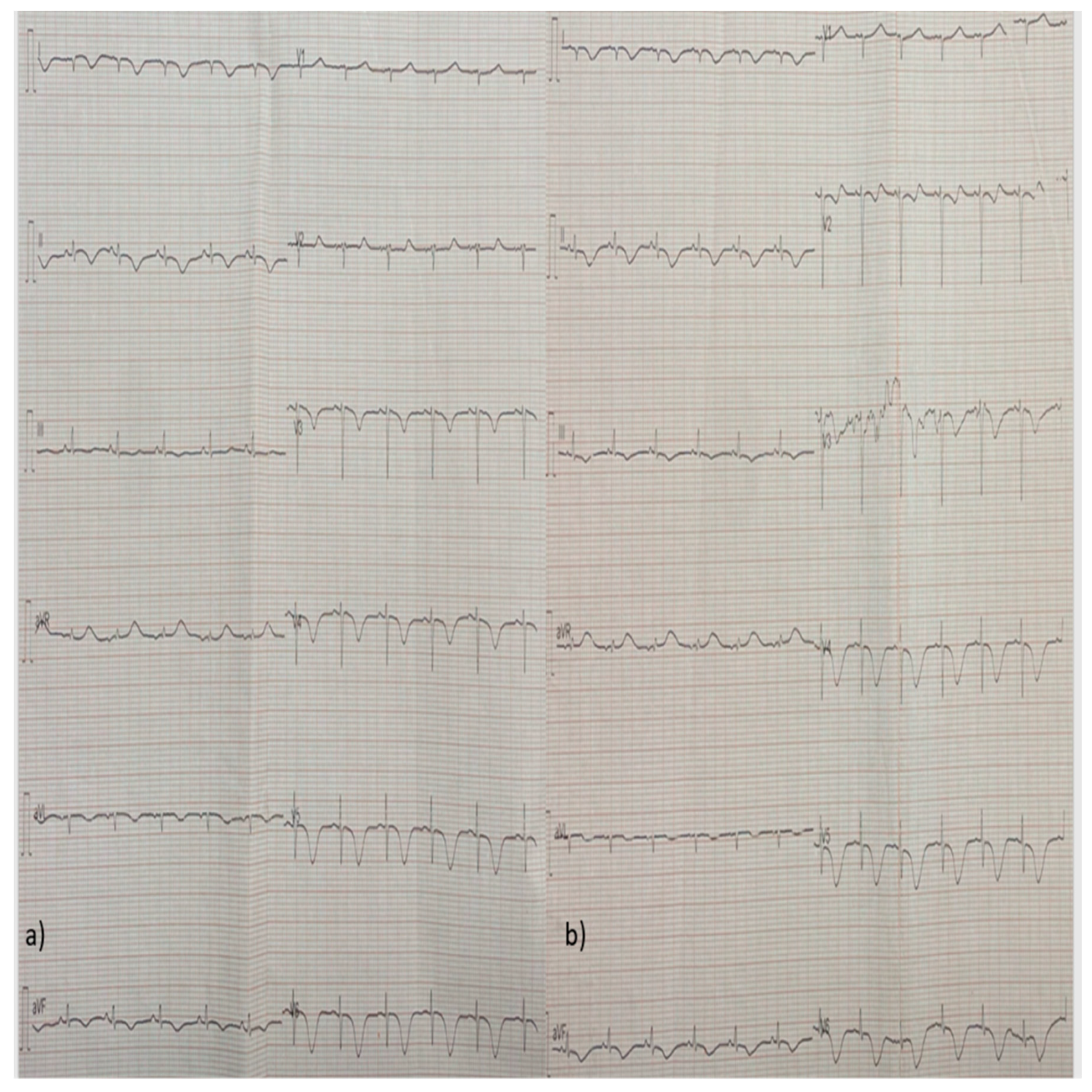
Figure 5.
a-b. Follow-up ECG showing repolarization disorders of the ST-segment and T-wave inversion.
Figure 5.
a-b. Follow-up ECG showing repolarization disorders of the ST-segment and T-wave inversion.
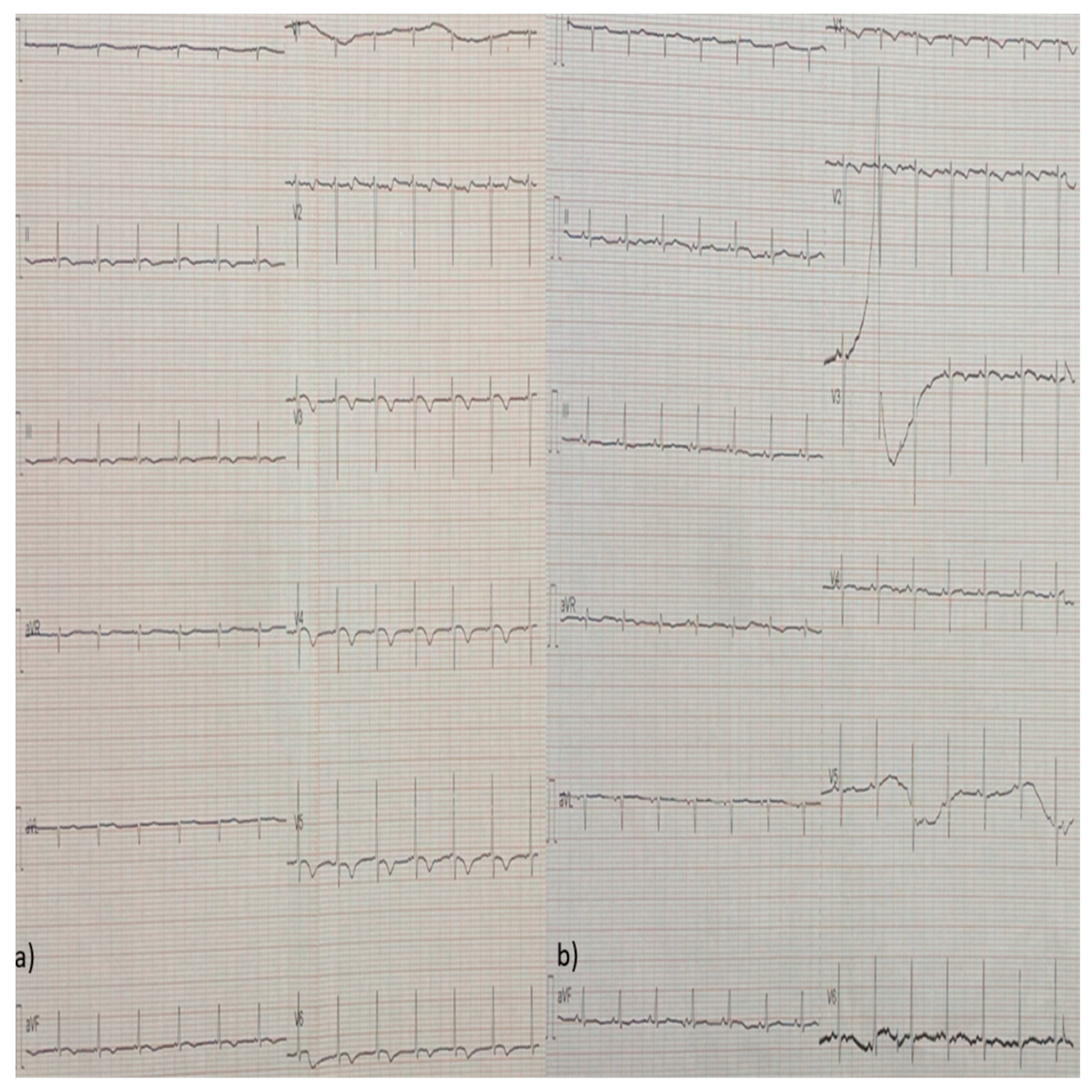
Figure 6.
a-b. Follow-up ECG showing repolarization disorders of the ST-segment and T-wave inversion.
Figure 6.
a-b. Follow-up ECG showing repolarization disorders of the ST-segment and T-wave inversion.
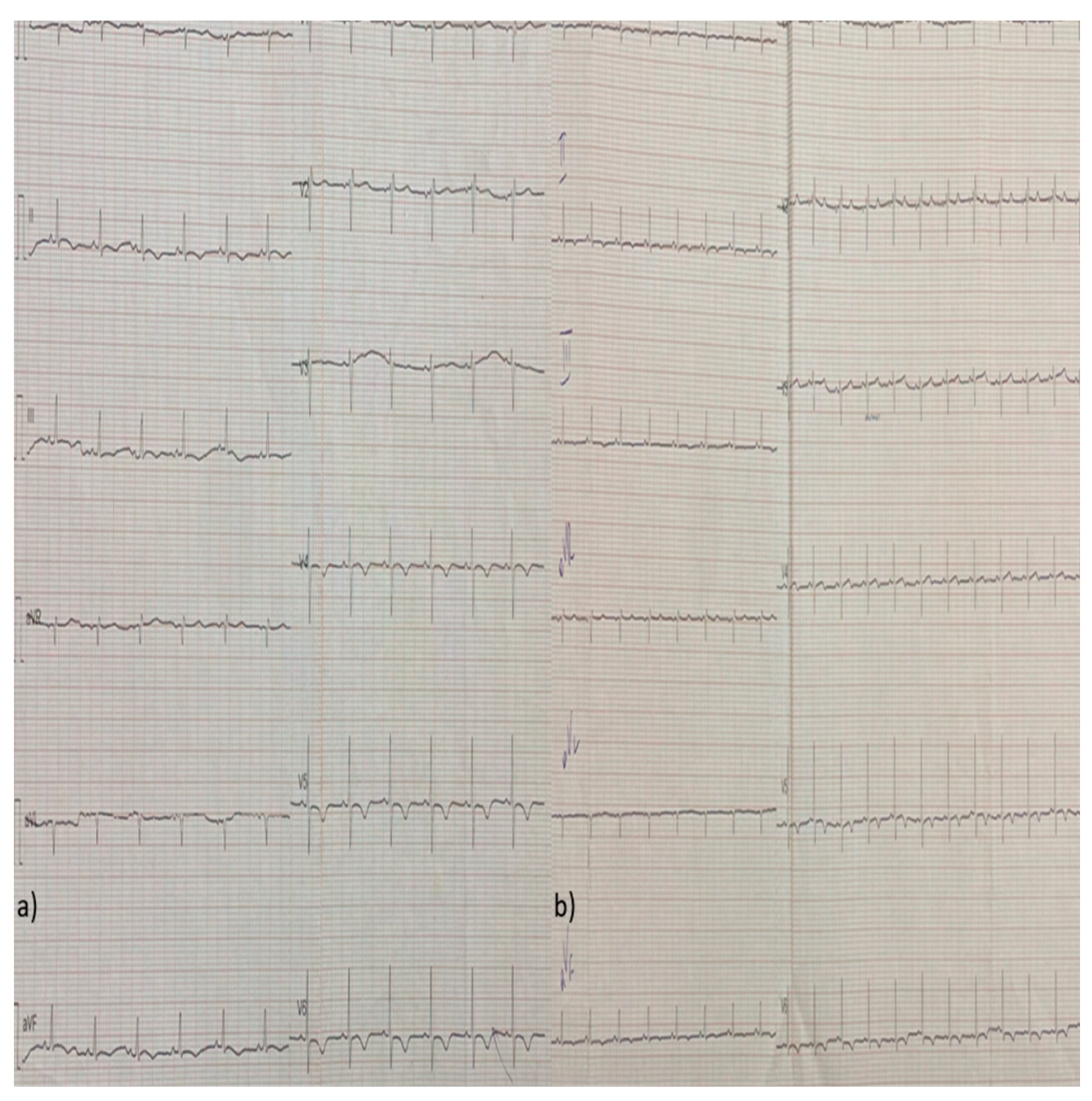
Figure 7.
a-b. Follow-up ECG showing repolarization disorders of the ST-segment and T-wave inversion.
Figure 7.
a-b. Follow-up ECG showing repolarization disorders of the ST-segment and T-wave inversion.
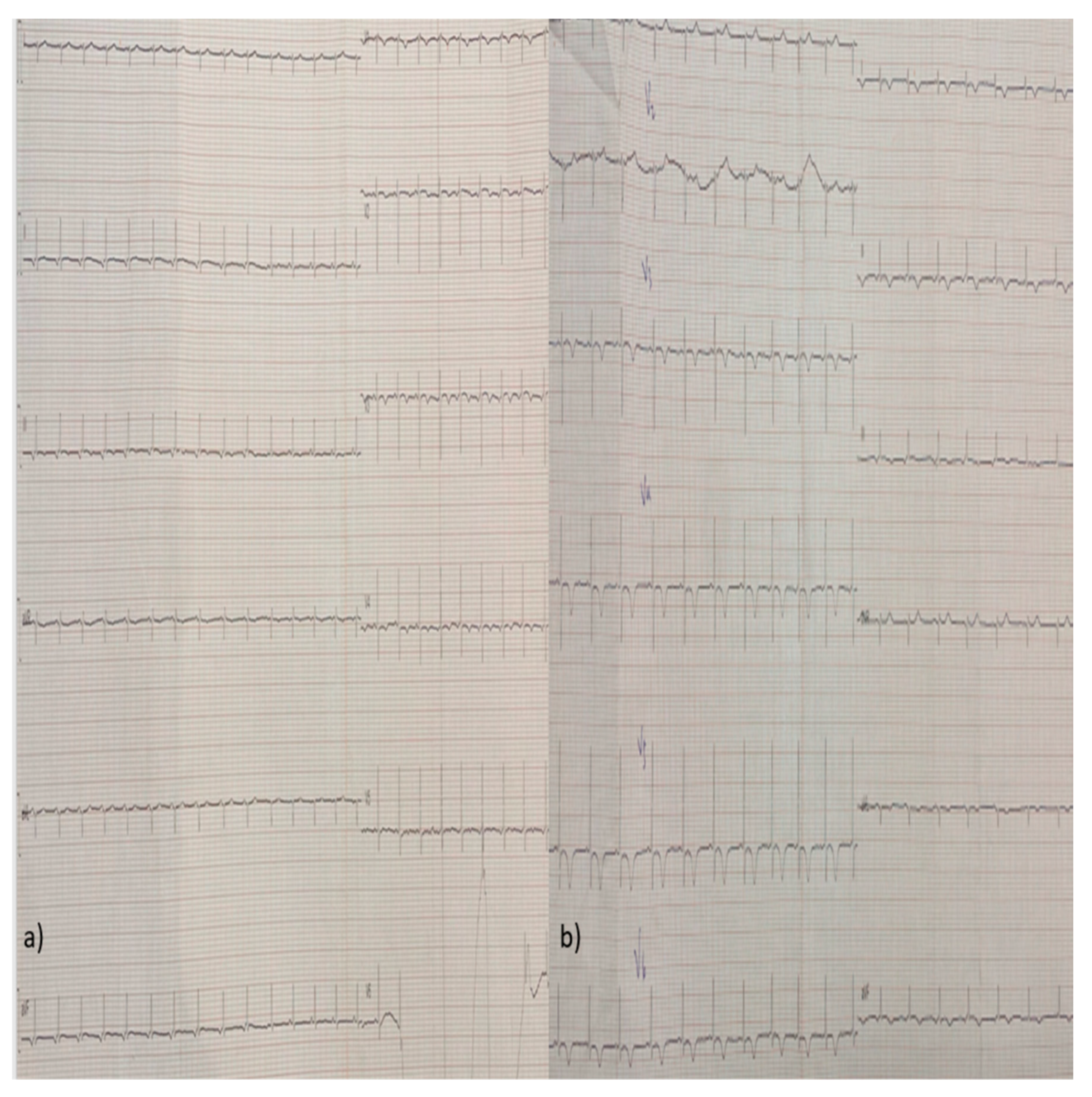
Figure 8.
a-b. Follow-up ECG showing repolarization disorders of the ST-segment and T-wave inversion.
Figure 8.
a-b. Follow-up ECG showing repolarization disorders of the ST-segment and T-wave inversion.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



