
Submitted:
18 July 2024
Posted:
19 July 2024
You are already at the latest version
Abstract
Deep hypothermic circulatory arrest (DHCA) is safe, but subtle neurodevelopmental deficits may persist far beyond the perioperative period. We investigated the relationship between DHCA duration and neurodevelopmental outcomes in young children undergoing cardiac surgery with DHCA. Children aged < 42 months, including neonates who underwent cardiac surgery using DHCA without regional perfusion techniques, were included as the DHCA group. Children in the same age range undergoing cardiac surgery without DHCA were included as the control group. All patients underwent neurodevelopmental assessment using the Bayley Scales of Infant and Toddler Development (BSTID) by a trained pediatrician. Seventeen of 25 DHCA and six of 10 control patients completed the BSTID assessment. The groups showed no preoperative, operative, or postoperative significant differences. In adjusted multivariable analysis, prematurity and age at assessment were significant changing predictors of each of the BSTID components (p < 0.001), other than the gross motor component, where only age at assessment was a significant adjusting predictor. Longer DHCA was associated with lower fine and gross motor BSTID components; however, the association was not statistically significant (p = 0.06). Use of DHCA without regional perfusion techniques may be associated with less optimal neurodevelopmental outcomes if DHCA has a long duration.
Keywords:
Bayley Scales
; congenital heart diseases
; deep hypothermic circulatory arrest
; neurodevelopmental
1. Introduction
Neurodevelopmental delay is the most common complication in patients undergoing congenital cardiac surgery [1] accounting for about 25–50% of all difficulties in patients surviving surgery [2]. These consists of a delay in fine motor, gross motor, social, speech, and language skills, as well as detrimental effects on cognitive function [3]. The delay is due to the complex pre-, intra-, and postoperative factors [4].
Congenital heart disease (CHD) is the most common birth defect globally, accounting for approximately 6–11 of every 1000 births [4]. In Saudi Arabia, similar numbers were documented in a systematic review published in 2015 [5]. Advances in CHD management have improved vastly in the past few decades, leading to a decrease in the mortality rate of patients undergoing congenital cardiac surgery. However, neurodevelopmental complications in survivors were documented, which can be linked to many factors that could affect the outcome of the surgery, including the age of patients at repair, the length of their intensive care unit (ICU) stays, and use of cardiopulmonary bypass and circulatory arrest [1].
The support technique used is a critical intraoperative source of morbidity in CHD surgery patients. Two standard techniques are deep hypothermic circulatory arrest (DHCA) and low-flow cardiopulmonary bypass (LFCPB). Both techniques have made many complex surgical repairs possible and have markedly decreased the mortality rate in patients undergoing surgery. However, the literature indicates that prolonged periods of DHCA and LFCPB are associated with a high risk of the development of future neurological injury [6,7].
Neurodevelopmental delay affects the quality of life of and imposes a burden on both the patients and their families. While recent literature has established a significant relationship between congenital cardiac surgery and neurodevelopmental complications, a clear connection between the duration of DHCA and LFCPB to neurodevelopmental outcomes was not found.
Here, we sought to explore this question objectively to understand its parameters to provide our patients with a better and healthier lifestyle.
2. Materials and Methods
2.1. Sample
After obtaining ethics approval from Unit of biomedical ethics at King Abdulaziz University. we retrospectively enrolled patients who underwent CHD surgery using DHCA (DHCA group) or without DHCA (control group) at a single center between January 2015 and December 2018.
Using retrospective review of a prospectively maintained database, we identified patients aged below 42 months, who underwent congenital cardiac surgery, and included those whose parents/guardians consented to take part in the study and to a visit for assessment of the child. We excluded those who were older than 42 months at the time of assessment, and those whose parents/guardians did not provide consent. Twenty-three patients were included, with 17 in the DHCA group and six in the control group.
2.2. Data Collection
Data collected included demographic characteristics, height, and weight at operation and at time of the last follow up, procedures performed, associated comorbidities, type of surgery performed, duration of ICU stay, duration of hospital stay, duration of cardiopulmonary bypass (CPB), time of DHCA, early and late complications, and mortality.
2.3. Neurodevelopmental Assessment
After obtaining these data, we contacted the patients’ families and brought them to a neurodevelopmental clinic at our center. After receiving the guardians’ written consent, we performed a Bayley Scales of Infant and Toddler (BSTID) | Third Edition (Bayley-III) assessment, which is a well-known screening tool for measuring the risk of developing neurodevelopmental delay in infants and toddlers from age 1 month to 42 months [8]. The assessment was performed by a developmental pediatric consultant, well experienced with the Bayley-III, which yields cognitive, communicative, and motor composite scores. Personnel performing the test were blinded to group allocation.
2.4. Statistical Analysis
All statistical analyses were carried out using Stata 16.1 (Stata Corp, College Station, TX, USA). A two tailed P-value of less than 0.05 was considered statistically significant. Categorical variables are summarized as frequencies, and continuous variables are summarized as mean and standard deviation, or median.
2.4.1. Data Presentation and Group Comparison
We compared preoperative, operative, and postoperative variables between patients in the DHCA (n = 17) and control group (n = 6). The Shapiro–Wilk test was performed to assess the distribution of the continuous variables. Normally distributed continuous variables were presented as mean and standard deviation and were compared using Student’s t-test. Non-normally distributed data were presented as median and 25–75th percentiles and were compared using the Mann–Whitney U test. Binary and nominal variables are presented as frequencies and percentages and were compared using the chi-square test or Fisher’s exact test if the expected frequency was less than 5.
2.4.2. Linear Regression Analysis
Univariable linear regression analysis was performed to assess factors associated with cognition, receptive communication, expressive communication, fine motor skill, and gross motor skill scores. Variables with a P-value of less than 0.2 in the univariable model were included in a multivariable linear regression model. Backward elimination was performed in the multivariable linear regression model for variables with a P-value exceeding than 0.1, so that the final model only included variables with a P-value ≤ 0.1. The Breusch–Pagan test was used to assess heteroskedasticity, and the distribution of the residual was evaluated to confirm a normal distribution. Multicollinearity was tested using the variance inflation factor. Spearman’s correlation was used to assess the correlation between scores and DHCA duration.
3. Results
3.1. Preoperative Data
We enrolled 35 patients. Seventeen of 25 and six of 10 patients in the DHCA and control groups, respectively, completed the BSTID assessment. The patients who did not undergo the evaluation were well, without symptoms, and their parents declined the evaluation. The median age (25th–75th quartiles) was 31 days (14–103) in the DHCA group. The control group included five males (83.33%), whereas the DHCA group included 10 males (58.82%). Age, sex, weight, genetic syndrome, prenatal diagnosis, mode of delivery, socioeconomic status, or parental education did not differ between the groups. None of the patients’ siblings had neurodevelopmental delay. No patient had a preoperative stroke or prenatal asphyxia. One patient in the DHCA group had undergone previous bilateral hernia repair. (Table 1)
3.2. Operative and Postoperative Data
All patients in the control group had undergone an arterial switch operation. In the DHCA group, the functions performed were stage-I Norwood–Sano (n = 4), aortic coarctation and ventricular septal defect repair (n = 10), interrupted aortic arch repair (n = 2), and arterial switch (n = 1). The cardiopulmonary bypass (CPB) time, excluding the DHCA time, was longer in the control than in the DHCS group (101 [74–123] vs. 61 [56–72], p = 0.002). If the DHCA time was added to CPB time, the difference between the two groups was not significant. No other operative or postoperative differences were statistically significant. The postoperative outcomes did not differ significantly between groups. No hospital mortality was reported in either group (Table 2).
3.3. Neurodevelopmental Assessment
3.4. Factors Affecting Neurodevelopment
DHCA was non-significantly associated with a lower cognitive score (p = 0.08), and the score was negatively correlated with the DHCA duration, but this did not reach statistical significance (p = 0.39) Similarly, DHCA was associated with a lower expressive communication score but did not reach a significant value (p = 0.06) (Table 4).
The fine and gross motor scores tended to be more affected in the DHCA group, although without statistical significance: p = 0.08 and 0.06, respectively (Table 4). Increased duration of DHCA was associated with lower fine (p = 0.26) and gross motor (p = 0.18) components of the BSTID; however, the association failed to reach the preset level of statistical significance (Figure 4).
In adjusted multivariable assessment, prematurity and age at assessment were significant changing predictors of each of the components of BSTID (p < 0.001), except for the gross motor component, for which only age at assessment was a significant predictor.
4. Discussion
Despite widespread recognition of a higher occurrence of neurodevelopmental delay among children with CHD and the priority for applying the neuroprotective strategies, little evidence is available for the optimal intraoperative perfusion strategy [9,10]. We investigated the relationship between DHCA duration and neurodevelopmental outcomes in young children undergoing cardiac surgery with DHCA. In adjusted multivariable analysis, prematurity and age at assessment were significant changing predictors of each of the BSTID components (p < 0.001), except for the gross motor component, where only age at assessment was a significant predictor. Longer DHCA was associated with lower fine and gross motor BSTID components scores, but without statistical significance (p = 0.06).
Many pediatric cardiac surgeons have been using DHCA due to its obvious technical advantages and the ability to ameliorate the morbidity associated with CPB, particularly in the smallest patients and neonates [9]. However, previous studies of DHCA impact on the neurodevelopmental outcome have yielded conflicting findings. A prospective randomized study from the University of Michigan compared the use of DHCA versus the use of regional cerebral perfusion and found no statistically significant difference in developmental testing results at the age of 1 year. Consistent with previous reports, they found the psychomotor development index (PDI) to be significantly more affected than the mental development index (MDI) [11,12]. Kosiorek and colleagues found significant worsening of neurological outcomes in patients undergoing CHD surgery without DHCA [13]. Moreover, a study that used electroencephalograms (EEGs) to monitor patients concluded that seizures were increased in this group, EEG seizure were even more common than clinical seizures, and seizures were associated with increased neurodevelopmental delay and neurological problems [13].
For patients with hypoplastic left heart syndrome and other single-ventricle lesions, a retrospective study by Visconti and colleagues demonstrated no benefit of regional low-flow cerebral perfusion relative to DHCA regarding the neurodevelopmental outcomes at the age of 1 year [14]. Fuller and associates showed that CPB and DHCA times were not predictive of developmental outcomes at 1 year of age after infant cardiac surgery [15]. In the present cohort, DHCA was associated with lower cognitive, expressive communication, fine motor, and gross motor scores, but the associations failed to reach the preset level of statistical significance (p = 0.08, 0.06, 0.08, and 0.06, respectively), which could be due to the small number of patients included in the control group.
In contrast, earlier studies demonstrated that children assigned to DHCA had lower PDI scores at 1 year of age and they had impairment in gross and fine motor skills, as well as speech apraxia at the age of 4 years [2,6] Extended periods of DHCA were found to be associated with neurological damage resulting in adverse neurodevelopmental outcomes [2,16]. Hickey showed a significant correlation of the duration of circulatory arrest with lowered PDI and higher neurologic abnormalities at the age of 1 year[17]. However, a 4-year assessment demonstrated that low-flow CPB and circulatory arrest patients were not different in neurological examination findings or IQ, although the duration of circulatory arrest affected several sub-scores of cognitive function [17].
In the Single Ventricle Reconstruction trial [18], DHCA use or duration were not independent risk factors for neurodevelopment outcomes at the age of 14 months, while an earlier study showed that neither the use nor the duration of DHCA was correlated with a worse outcome for PDI or MDI at 1 year of age after infant cardiac surgery [15].
Consistent with the current study, Wypij and colleagues found that the effect of duration of DHCA on neurodevelopmental outcomes was nonlinear. Moreover, they showed that important late neurodevelopmental outcomes, such as fine motor function, academic achievement, and speech, were generally unaffected when using a shorter duration of DHCA [16].
This discrepancy in the results is likely multifactorial and may be due to the diversity in terms of cardiac diagnoses, perioperative and intraoperative support strategies, and patient-related risk factors, such as gestational age, sex, and ethnicity. Importantly, the studies conducted in a more recent era included considerably different intraoperative support techniques and postoperative management facilities [15]. In the present cohort, despite a fairly exhaustive list of perioperative and patient-related risk factors, adjusted multivariable analyses identified only prematurity as a risk factor for worsened scores on components of the BSTID (p < 0.001), except for the gross motor function.
Beca et al. reported that the severity of brain immaturity at birth is a predictor of the severity of neurodevelopmental impairment at the age of 2 years after infant cardiac surgery [19]. Additionally, CHD may alter brain development and increase vulnerability to hemodynamic instability perioperatively, and to brain injury due to hypoxia and ischemia intraoperatively [1]. A previous report showed that preoperative risk factors of low gestational age and elevated preoperative lactate could classify 84% of mentally and/or motor-delayed children after cardiac surgery [15]. A recent study identified sex, race, birth weight, type of CHD, genetic anomalies, and maternal education as important independent predictors of neurodevelopmental outcomes [1].
Our study had some limitations, including a small sample size, the inherent limitations and risk of bias of a retrospective study design, the potential for selection bias, and lack of generalizability to different populations.
5. Conclusions
The use of DHCA without regional perfusion techniques may be associated with less optimal neurodevelopmental outcomes if the duration of DHCA is long. Future studies with larger sample sizes are needed to delineate the level of significance and length of the period of safe DHCA. Additionally, further studies should investigate safer alternatives to DHCA.
Author Contributions
Writing the manuscript; performed the literature search and review; data collection, made substantial contributions to the conception, design, and edition of the manuscript: Ghunaim AH, Aljabri B, Domain A, Althinayyan GS, Aleissa AI, Alshebly AT, Alyafi RA, Alhablany TM, Nashar AM, Alradi OO
Prepared the figures and tables: Alradi OO, Ghunaim AH, Dohain A, Aljabri A All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding or.
Institutional Review Board Statement
The study was approved by the institutional Review Board of King Abdulaziz University on 19/04/2018 Ref 241-18.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Available upon request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Gaynor, J.W.; Stopp, C.; Wypij, D.; Andropoulos, D.B.; Atallah, J.; Atz, A.M.; et al. Neurodevelopmental outcomes after cardiac surgery in infancy. Pediatrics 2015, 135, 816–825. [Google Scholar] [CrossRef] [PubMed]
- Bellinger, D.C.; Wypij, D.; Kuban, K.C.; Rappaport, L.A.; Hickey, P.R.; Wernovsky, G.; et al. Developmental and neurological status of children at 4 years of age after heart surgery with hypothermic circulatory arrest or low-flow cardiopulmonary bypass. Circulation 1999, 100, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Forbess, J.M.; Visconti, K.J.; Hancock-Friesen, C.; Howe, R.C.; Bellinger, D.C.; Jonas, R.A. Neurodevelopmental outcome after congenital heart surgery: Results from an institutional registry. Circulation 2002, 106(12 Suppl 1), I95–102. [Google Scholar] [CrossRef]
- Du Plessis, A.J. Neurologic complications of cardiac disease in the newborn. Clin Perinatol 1997, 24, 807–826. [Google Scholar] [CrossRef] [PubMed]
- Alenezi, A.M.; Albawardi, N.M.; Ali, A.; Househ, M.S.; Elmetwally, A. The epidemiology of congenital heart diseases in Saudi Arabia: A systematic review. J Public Health Epidemiol 2015, 7, 232–240. [Google Scholar]
- Bellinger, D.C.; Jonas, R.A.; Rappaport, L.A.; Wypij, D.; Wernovsky, G.; Kuban, K.C.; et al. Developmental and neurologic status of children after heart surgery with hypothermic circulatory arrest or low-flow cardiopulmonary bypass. N Engl J Med 1995, 332, 549–555. [Google Scholar] [CrossRef] [PubMed]
- International Cardiac Collaborative on Neurodevelopment (ICCON) Investigators. Impact of operative and postoperative factors on neurodevelopmental outcomes after cardiac operations. Ann Thorac Surg 2016, 102, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Balasundaram, P.l Avulakunta, I,D. Bayley Scales Of Infant and Toddler Development. StatPearls. Treasure Island (FL): StatPearls Publishing Copyright © 2023, StatPearls Publishing LLC.; 2023.
- Pizarro, C.; Sood, E.D.; Kerins, P.; Duncan, D.; Davies, R.R.; Woodford, E. Neurodevelopmental outcomes after infant cardiac surgery with circulatory arrest and intermittent perfusion. Ann Thorac Surg 2014, 98, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Marino, B.S.; Lipkin, P.H.; Newburger, J.W.; Peacock, G.; Gerdes, M.; Gaynor, J.W.; et al. Neurodevelopmental outcomes in children with congenital heart disease: evaluation and management: a scientific statement from the American Heart Association. Circulation 2012, 126, 1143–1172. [Google Scholar] [CrossRef] [PubMed]
- Tabbutt, S.; Nord, A.S.; Jarvik, G.P.; Bernbaum, J.; Wernovsky, G.; Gerdes, M.; et al. Neurodevelopmental outcomes after staged palliation for hypoplastic left heart syndrome. Pediatrics 2008, 121, 476–483. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, C.S.; Bove, E.L.; Devaney, E.J.; Mollen, E.; Schwartz, E.; Tindall, S.; et al. A randomized clinical trial of regional cerebral perfusion versus deep hypothermic circulatory arrest: outcomes for infants with functional single ventricle. J Thorac Cardiovasc Surg 2007, 133, 880–887. [Google Scholar] [CrossRef] [PubMed]
- Kosiorek, A.; Donofrio, M.T.; Zurakowski, D.; Reitz, J.G.; Tague, L.; Murnick, J.; et al. Predictors of neurological outcome following infant cardiac surgery without deep hypothermic circulatory arrest. Pediatr Cardiol 2022, 43, 62–73. [Google Scholar] [CrossRef] [PubMed]
- Visconti, K.J.; Rimmer, D.; Gauvreau, K.; del Nido, P.; Mayer, J.E., Jr; Hagino, I.; Pigula, F.A. Regional low-flow perfusion versus circulatory arrest in neonates: one-year neurodevelopmental outcome. Ann Thorac Surg 2006, 82, 2207-2211; discussion 2211-2213. [Google Scholar] [CrossRef] [PubMed]
- Fuller, S.; Nord, A.S.; Gerdes, M.; Wernovsky, G.; Jarvik, G.P.; Bernbaum, J.; et al. Predictors of impaired neurodevelopmental outcomes at one year of age after infant cardiac surgery. Eur J Cardiothorac Surg 2009, 36, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Wypij, D.; Newburger, J.W.; Rappaport, L.A.; duPlessis, A.J.; Jonas, R.A.; Wernovsky, G.; et al. The effect of duration of deep hypothermic circulatory arrest in infant heart surgery on late neurodevelopment: the Boston Circulatory Arrest Trial. J Thorac Cardiovasc Surg 2003, 126, 1397–1403. [Google Scholar] [CrossRef] [PubMed]
- Hickey, P.R. Neurologic sequelae associated with deep hypothermic circulatory arrest. Ann Thorac Surg 1998, 65 (6 Suppl), S65-69; discussion S69-70, S74-76. [Google Scholar] [CrossRef] [PubMed]
- Newburger, J.W.; Sleeper, L.A.; Bellinger, D.C.; Goldberg, C.S.; Tabbutt, S.; Lu, M.; et al. Early developmental outcome in children with hypoplastic left heart syndrome and related anomalies: the single ventricle reconstruction trial. Circulation 2012, 125, 2081–2091. [Google Scholar] [CrossRef] [PubMed]
- Beca, J. Gunn, J.K.; Coleman, L.; Hope, A.; Reed, P.W.; Hunt, R.W.; et al. New white matter brain injury after infant heart surgery is associated with diagnostic group and the use of circulatory arrest. Circulation 2013, 127, 971–979. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Box plots comparing the cognitive, receptive communication, expressive communication, fine motor, and gross motor scores between groups. (DHCA: deep hypothermic circulatory arrest).
Figure 1.
Box plots comparing the cognitive, receptive communication, expressive communication, fine motor, and gross motor scores between groups. (DHCA: deep hypothermic circulatory arrest).
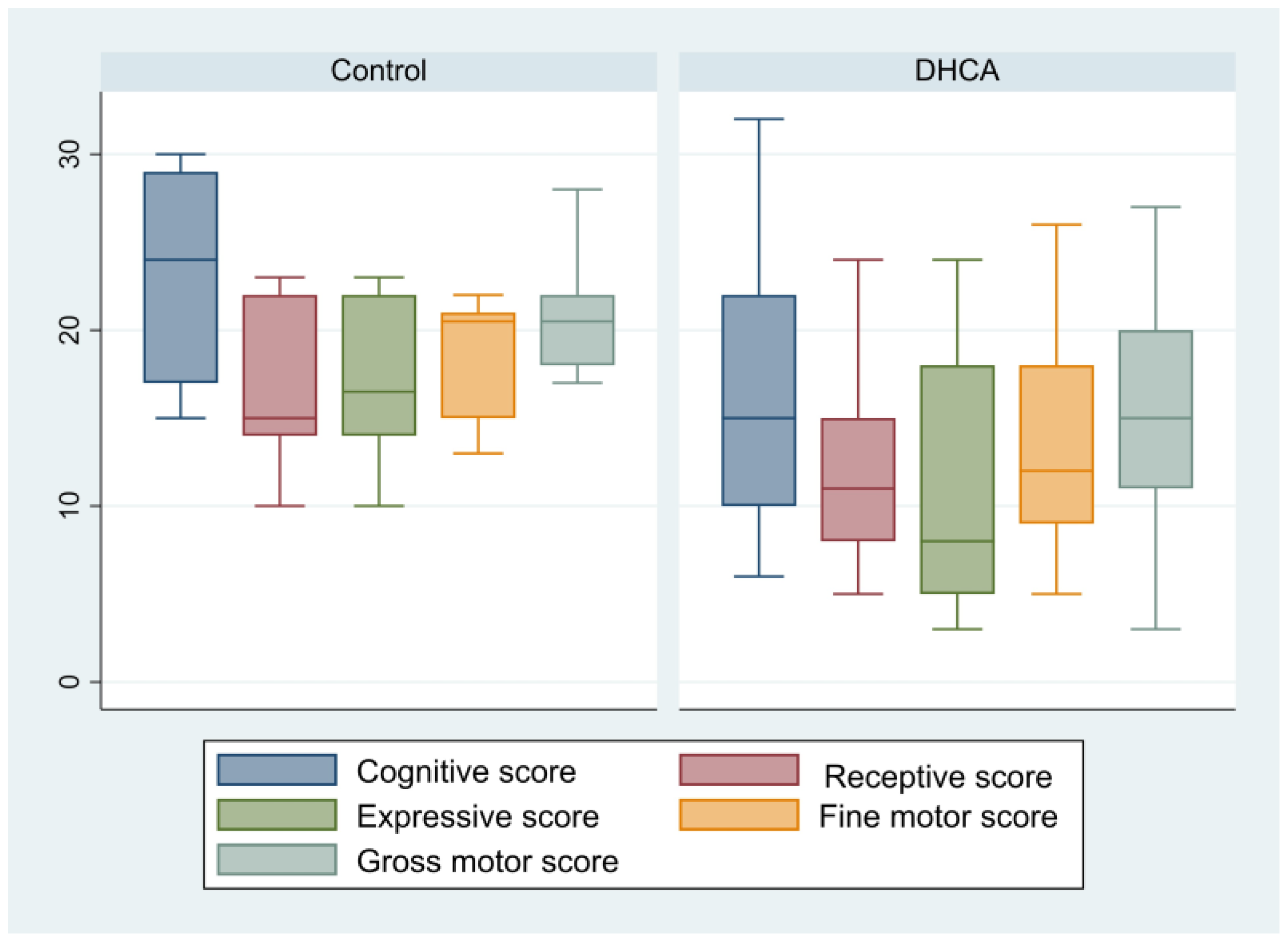

Table 1.
Preoperative patients’ characteristics.
| Total patients (n = 23) |
Control (n = 6) |
DHCA (n = 17) |
P-value | |
| Males | 15 (65.22%) | 5 (83.33%) | 10 (58.82%) | 0.37 |
| Age at intervention (days) | 21 (9–82) | 6 (3–35) | 31 (14–103) | 0.05 |
| Weight at intervention (Kg) | 3.2 (2.5–3.6) | 3.5 (2.9–3.7) | 2.8 (2.5–3.6) | 0.40 |
| Down syndrome | 1 (4.35%) | 0 | 1 (5.88%) | >0.99 |
| Prenatal diagnosis | 5 (22.73%) | 3 (50%) | 2 (12.5%) | 0.10 |
| Preterm labor | 2 (8.7%) | 0 | 2 (11.76%) | >0.99 |
| Socio-economic status Low Middle Upper middle |
12 (57.14%) 7 (33.33%) 2 (9.52%) |
4 (66.67%0 1 (16.67%) 1 (16.67%) |
8 (53.33%) 6 (40%) 1 (6.67%) |
0.50 |
| Father’s education Primary school Secondary school Bachelor’s degree Master’s degree |
1 (4.76%) 10 (47.62%) 9 (42.86%) 1 (4.76%) |
0 1 (16.67%) 4 (66.67%) 1 (16.67%) |
1 (6.67%) 9 (60%) 5 (33.33%) 0 |
0.13 |
| Mother’s education Primary school Middle school Secondary school Bachelor’s degree Master’s degree |
1 (4.76%) 5 (23.81%) 6 (28.57%) 7 (33.33%) 2 (9.52%) |
0 2 (33.33%) 0 3 (50%) 1 (16.67%) |
1 (6.667%) 3 (20%) 6 (40%) 4 (26.67%) 1 (6.67%) |
0.32 |
| Delivery mode Vaginal Cesarean |
16 (69.57%) 7 (30.43%) |
3 (50%) 3 (50%) |
13 (76.47%) 4 (23.53%) |
0.32 |
| Previous non-cardiac surgery | 1 (4.35%) | 0 | 1 (5.88%) | >0.99 |
| Preoperative ventilation (days) | 0 (0–3) | 0 (0–3) | 2 (0–3) | 0.56 |
Continuous data are presented as mean and standard deviation or median (25th–75th percentiles) and categorical data are presented as numbers and percentages. DHCA: deep hypothermic circulatory arrest
Table 2.
Operative and postoperative data.
| Total patients (n = 23) |
Control (n = 6) |
DHCA (n = 17) |
P-value | |
| Duration of CPB (minutes) | 68 (56–78) | 101.5 (74–123) | 61 (56–72) | 0.002 |
| Cross-clamp time (minutes) | 45.57 ± 16.52 | 61.67 ± 18.59 | 39.88 ± 11.65 | 0.003 |
| Highest creatinine (μmol/L) | 55 (46–87.8) | 54.5 (49–70) | 68 (42–91) | 0.93 |
| Highest lactate (mmol/L) | 4.67 (0.48) | 4.87 ± 1.14 | 4.6 ± 0.53 | 0.81 |
| Postoperative acidosis | 17 (77.27%) | 3 (50%) | 14 (87.5%) | 0.10 |
| Postoperative hypoxia | 11 (47.83%) | 4 (66.67%) | 7 (41.18%) | 0.37 |
| Mechanical ventilation (days) | 6 (4–8) | 5 (2–7) | 7 (4–12) | 0.29 |
| ECMO | 1 (4.35%) | 0 | 1 (5.88%) | >0.99 |
| Open sternum | 18 (78.36%) | 4 (66.67%) | 14 (82.35%) | 0.58 |
| Open chest duration (days) | 2 (1.5–3) | 3 (1.5–4) | 2 (1.5–3) | 0.53 |
| Postoperative seizures | 1 (4.35%) | 1 (16.67%) | 0 | 0.26 |
| Pulmonary hemorrhage | 4 (17.39%) | 1 (16.67%) | 3 (17.65%) | >0.99 |
| Lowest Ca level (mg/dl) | 2.04 (1.88–2.14) | 1.98 (1.55–2.12) | 2.05 (1.93–2.14) | 0.34 |
| ICU stay (days) | 12 (7–18) | 9 (5–12) | 15 (7–23) | 0.13 |
| Hospital stay (days) | 16 (12–26) | 11.5 (10–14) | 19 (15–46) | >0.99 |
| Surgical re-exploration | 2 (8.7%) | 0 | 2 (11.76%) | >0.99 |
| Blood stream infection | 6 (26.09%) | 0 | 6 (35.29%) | 0.14 |
| Surgical site infection | 2 (8.7%) | 2 (33.33%) | 0 | 0.06 |
| Heart block | 5 (21.74%) | 1 (16.67%) | 4 (23.53%) | >0.99 |
| Chest drain > 5 days | 2 (8.7%) | 0 | 2 (11.76%) | >0.99 |
Continuous data are presented as mean and standard deviation or median (25th–75th percentiles) and categorical data are presented as numbers and percentages. CPB: cardiopulmonary bypass; DHCA: deep hypothermic circulatory arrest; ECMO: extracorporeal membrane oxygenation; ICU: intensive care unit.
Table 3.
Neurodevelopmental assessment.
| Total patients (n = 23) |
Control (n = 6) |
DHCA (n = 17) |
P-value | |
| Age at assessment (days) | 774.78 ± 343.56 | 865 ± 184.36 | 742.94 ± 284.12 | 0.47 |
| Cognitive score | 18.26 ± 7.99 | 23.17 ± 6.62 | 16.53 ± 7.87 | 0.08 |
| Cognitive At-risk Emerging Competent |
9 (39.13%) 8 (34.78%) 6 (26.09%) |
1 (16.67%) 3 (50%) 2 (33.33%) |
8 (47.06%) 5 (29.41%) 4 (23.53%) |
0.49 |
| Receptive communication score | 14 (8–15) | 15 (14–22) | 11 (8–15) | 0.17 |
| Receptive communication At-risk Emerging Competent |
6 (26.09%) 10 (43.48%) 7 (30.43%) |
1 (16.67%) 3 (50%) 2 (33.33%) |
5 (29.41%) 7 (41.18%) 5 (29.41%) |
>0.99 |
| Expressive communication score | 12.43 ± 6.91 | 17 ± 4.90 | 10.82 ± 6.89 | 0.06 |
| Expressive communication At-risk Emerging Competent |
9 (39.13%) 8 (34.78%) 6 (26.09%) |
1 (16.67%) 3 (50%) 2 (33.33%) |
8 (47.06%) 5 (29.41%) 4 (23.53%) |
0.49 |
| Fine motor score | 14.91 ± 6.03 | 18.67 ± 3.72 | 13.59 ± 6.21 | 0.08 |
| Fine motor At-risk Emerging Competent |
5 (29.41%) 12 (52.17%) 6 (26.09%) |
0 4 (66.67%) 2 (33.33%) |
5 (29.41%) 8 (47.06%) 4 (23.53%) |
0.46 |
| Gross motor score | 16.26 ± 7.21 | 21 ± 3.90 | 14.59 ± 7.43 | 0.06 |
| Gross motor At-risk Emerging Competent |
9 (39.13%) 7 (30.43%) 7 (30.43%) |
0 3 (50%) 3 (50%) |
9 (52.94%) 4 (23.53%) 4 (23.53%) |
0.05 |
Continuous data are presented as mean and standard deviation or median (25th–75th percentiles) and categorical data are presented as numbers and percentages. DHCA: deep hypothermic circulatory arrest.
Table 4.
Factors affecting the cognitive, receptive communications, expressive communications, fine motor and gross motor scores.
Table 4.
Factors affecting the cognitive, receptive communications, expressive communications, fine motor and gross motor scores.
| Univariable | Multivariable | |||
| Coefficient (95% CI) | P-value | Coefficient (95% CI) | P-value | |
| Cognitive score* | ||||
| Age at assessment (months) | 0.53 (0.32–0.74) | <0.001 | 0.59 (0.45–0.74) | <0.001 |
| Preterm | -9.05 (-20.94–2.85) | 0.13 | -13.38 (-19.22–-7.53) | <0.001 |
| CPB duration | 0.11 (-0.02–0.24) | 0.09 | - | |
| DHCA | -6.64 (-14.13–0.86) | 0.08 | - | |
| Receptive communication score** | ||||
| Age at assessment (months) | 0.33 (0.16–0.50) | 0.001 | 0.38 (0.25–0.50) | <0.001 |
| Preterm | -8.24 (-16.45–0.03) | 0.049 | -11 (-15.95–-6.06) | <0.001 |
| CPB | 0.07 (-0.02–0.17) | 0.12 | - | |
| DHCA | -4.03 (-9.52–1.46) | 0.14 | - | |
| Expressive communication score*** | ||||
| Age at assessment (months) | 0.39 (0.17–0.6) | 0.001 | 0.44 (0.26–0.61) | <0.001 |
| Preterm | -8.14 (-18.38–2.09) | 0.11 | -11.35 (-18.3–-4.4) | <0.001 |
| Down syndrome | -9.84 (-24.21–4.49) | 0.17 | - | |
| CPB time | 0.10 (-0.01–0.21) | 0.09 | - | |
| DHCA | -6.18 (-12.57–0.22) | 0.06 | - | |
| Fine motor score **** | ||||
| Age at assessment (months) | 0.39 (0.22–0.55) | <0.001 | 0.42 (0.32–0.53) | <0.001 |
| Male | -3.78 (-9.13–1.58) | 0.16 | - | |
| Preterm | -8.12 (-16.87–0.63) | 0.07 | -10.62 (-14.68–-6.55) | <0.001 |
| Down syndrome | -8.27 (-20.85–4.30) | 0.19 | - | |
| CPB | 0.07 (-0.28–0.17) | 0.15 | - | |
| DHCA | -5.08 (-10.72–0.56) | 0.08 | -2.1 (-4.70–-0.49) | 0.10 |
| Gross motor score ***** | ||||
| Age at assessment (months) | 0.48 (0.30–0.67) | <0.001 | 0.51 (0.39–0.64) | <0.001 |
| Male | -4.78 (-11.13–1.58) | 0.13 | -10.85 (-15.82–-5.87) | <0.001 |
| Preterm | -7.95 (-18.71–2.81) | 0.14 | - | |
| Down syndrome | -10.73 (-25.63–4.18) | 0.15 | - | |
| CPB | 0.10 (-0.01–0.22) | 0.08 | - | |
| DHCA | -6.41 (-13.09–0.27) | 0.06 | -3.04 (-6.22–-0.14) | 0.06 |
*R2 (cognitive score)= 0.80. **R2 (receptive communications score)= 72. ***R3 (expressive communications score)= 0.63. ****R2 (Fine motor score)= 0.84. *****R2 (gross motor score)= 0.84. CPB, cardiopulmonary bypass; DHCA, deep-hypothermic circulatory arrest.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



