
Submitted:
12 July 2024
Posted:
12 July 2024
You are already at the latest version
Abstract
Background: The safety and effectiveness of factor-Xa (FXa) inhibitors for nonvalvular atrial fibrillation (NVAF) remains inconclusive. We investigated the current dosing of rivaroxaban, apixaban and edoxaban by monitoring drug plasma concentration (PC) and coagulation activity.
Methods and Results: This multicenter clinical study monitored the drug PC levels and two coagulation biomarkers (fibrinogen: FIB, and fibrin monomer complex: FMC) at peak and trough timing in 268 outpatients receiving rivaroxaban (n = 72), apixaban (n = 71), and edoxaban (n = 125) for NVAF. Doses were adjusted according to the dose adjustment criteria of each drug. Based on our previous study, each peak drug PC remained below the cut-off level for predicting bleeding events except in eight patients (three on rivaroxaban, two on apixaban and three on edoxaban) in whom bleeding events occurred; among them, two (one each on rivaroxaban and edoxaban) had a peak drug PC below the cut-off level. Drug PCs widely varied from peak to trough, whereas FMC levels remained within the normal range (< 6.1 µg/ml) regardless of PC variation. These finding suggested that the anticoagulant effects of these drugs persisted throughout the day regardless of the drug PC levels, dosage, and frequency of dosing. Regarding the change in peak drug PC levels over time, rivaroxaban tended to accumulate more than edoxaban (p
Keywords:
anticoagulation monitoring
; apixaban
; atrial fibrillation
; edoxaban
; on label dosing
; rivaroxaban
1. Introduction
The 2021 European Heart Rhythm Association (EHRA) practical guide on the use of direct oral anticoagulants (DOACs) in patients with nonvalvular atrial fibrillation (NVAF) stated that DOACs provide a similar degree of antithrombotic effect as vitamin K antagonists with less bleeding events [1]. However, rivaroxaban has a higher bleeding incidence than apixaban and edoxaban [2,3,4,5,6,7]. Additionally, in patients of extreme body weight (BW), two practical guides for DOAC use suggests that special care is needed for individuals with a BW of ≤60 kg, and that reduced doses of apixaban and edoxaban should be administered [1,8]. Furthermore, the EHRA guidelines stated that monitoring plasma levels of DOAC is suitable for individuals with a BW of<60 kg for whom rivaroxaban or dabigatran was prescribed. Moreover, we previously reported that edoxaban has a more favorable safety profile than rivaroxaban with plasma concentration (PC) monitoring (Hokusetsu DOAC study) [9]. Therefore, we planned this multicenter study to evaluate anti-thrombotic action among three factor Xa (FXa) inhibitors (rivaroxaban, apixaban or edoxaban) (the SET DOAC registry; UMIN000036769) using the same protocol as the Hokusetsu DOAC study. This study aimed to 1) determine which FXa inhibitors is more effective and safer by examining established indexes and their cut-off levels for predicting bleeding events and by evaluating the appropriateness of on-label dosing using established indexes; and 2) confirm their antithrombotic action by monitoring levels of coagulation biomarkers and drug PCs over time as well as PC through the daily variation of each drug.
2. Methods
Study Design and Participants
This observational study included outpatients with NVAF at nine hospitals, including Hokusetsu General Hospital, who consulted from November 2018 to December 2021. We planned to enroll 300 patients each drug; however, due to the COVID-19 pandemic, we were only able to enroll only 280 outpatients (76 for rivaroxaban, 78 for apixaban, and 126 for edoxaban).
We calculated the creatinine clearance (Cr-Cl) using the Cockcroft–Gault formula adjusted for age, BW, serum creatinine (S-Cr) level, and gender. Additionally, we calculated the CHADS2 scores immediately before DOAC treatment initiation based on the presence of heart failure, hypertension (HT), age ≥ 75 years, and stroke history.
Although the Japanese standard on-label dose for rivaroxaban is 15 mg once daily (od), the recommended on-label reduced dose of 10 mg od was used for patients with a Cr-Cl of< 50 mL/min [10]. The standard dose of apixaban is 5 mg twice daily (bid), but 2.5 mg bid is the recommended reduced dose for patients meeting of ≥2 criteria for dose reduction (S-Cr of ≥1.5mg/dl, BW of ≤60kg, and age of ≥80 years). The standard on-label dose of edoxaban is 60 mg od, while 30 mg od is the recommended on-label reduced dose for patients with a BW of ≤60 kg, Cr-Cl of <50 mL/min, or concomitantly using P-glycoprotein inhibitors. Therefore, we selected DOAC doses for patients based on the abovementioned dose recommendations. However, patients who were treated with off-label reduced doses were not included. Additionally, some who had withdrawn their participation before the first blood sampling were also excluded. All patients provided written informed consent, and this study was approved by the ethical review committee at each hospital.
Measured Parameters
Fibrinogen (FBG, with Thrombocheck Fib[L]®, Sysmex, Japan), and soluble fibrin monomer complexes (FMC: with Auto LIA FM®: Sysmex, Japan) were measured using an automated blood coagulation analyzer (CS-5100; Sysmex, Japan). Additionally, under a steady state of at least 4 weeks after the initiation of each DOAC, drug PC levels in each DOACs group were measured via the anti-FXa-derived indirect method using the Biophen® DiXaI kit (Hyphen Biomed, Neuville Sur Oise, France) [11] similar to that in our previous report [9,12]. This kit uses a chromogenic method based on inhibiting a constant and excess quantity of FXa by the drug being assayed, with a calibrator and control for each drug.
Blood Sampling (Figure 1)
After serum was separated from collected blood samples under 4℃ cooling and serum
samples were frozen at each hospital, these frozen samples were analyzed at the Reagent
Engineering (TS), Sysmex Corporation
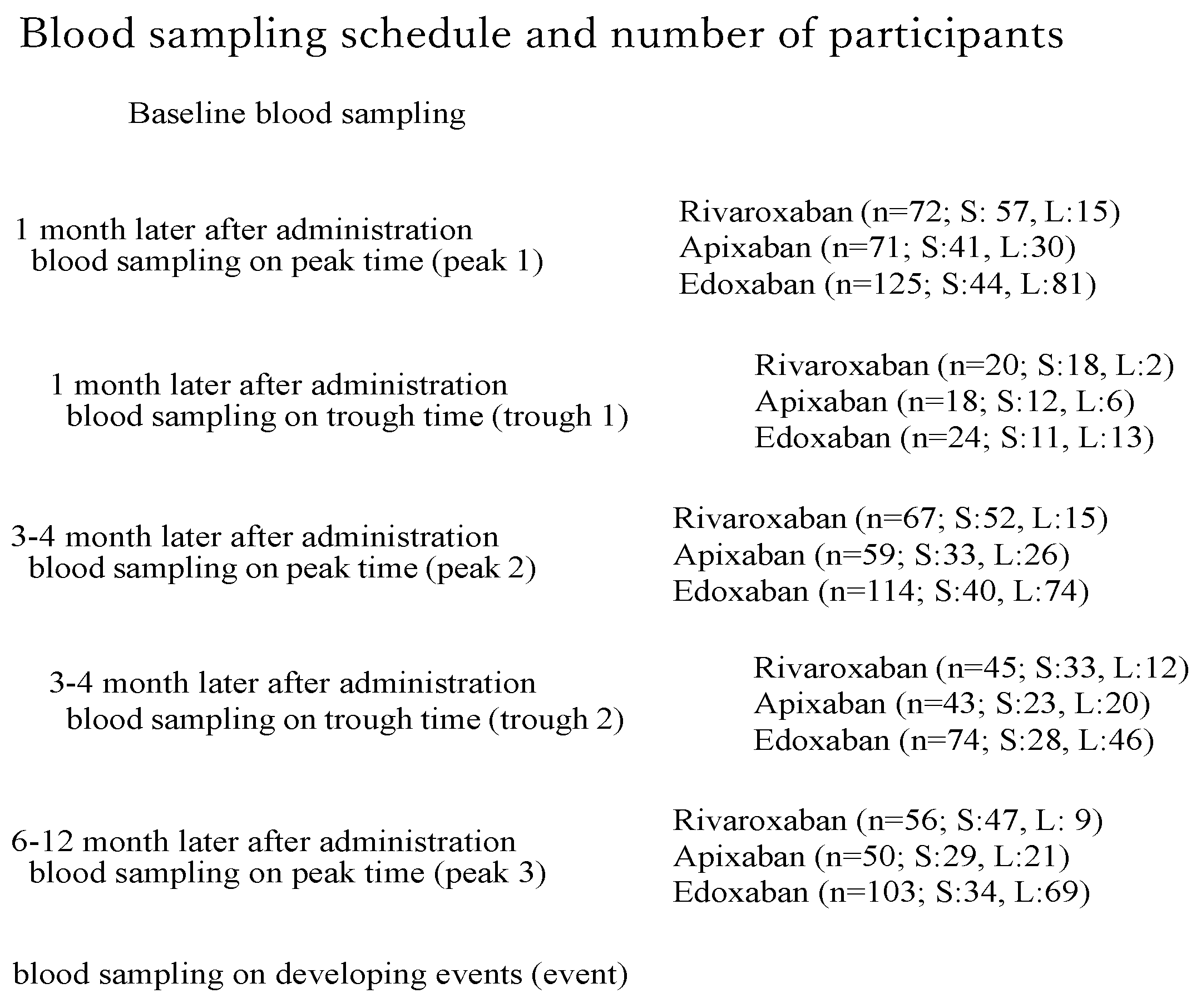
Blood samples were collected 3 h after drug administration to measure the peak drug PC and immediately before drug administration to measure the trough drug PC [1,9,12]. To evaluate the variations in PC levels over time, we also measured the peak drug PC thrice and trough drug PC twice for 6–12 months during continuous DOAC administration (peak 1: 1 month later, peak 2: 3–4 months later, and peak 3: 6–12 months later; trough 1: 1 month later, trough 2: 3–4 months later).
At peak 1, we evaluated the incidence of the drug PC exceeding the cut-off level for predicting the bleeding events. Each cut-off level was based on our previous investigations (404 ng/mL for rivaroxaban, 386 ng/mL for apixaban, and 402 ng/mL for edoxaban) [9,12]. Furthermore, we examined the variation in peak drug PC over time by measuring peak 3 and comparing it with peak 1 and/or peak 2 (for evaluating tending toward drug accumulation).
Bleeding and Thromboembolic Events in DOAC Users
According to the definition by the International Society on Thrombosis and Haemostasis, major bleeding is a clinically overt bleeding associated with a ≥ 2.0 g/dl, decrease in the hemoglobin level, a transfusion requirement of ≥ 2 U of packed red cells or whole blood, involvement of a critical site, or a fatal outcome [13]. Non-major clinically relevant bleeding was defined as clinically overt bleeding that did not meet the criteria for major bleeding, but required medical intervention, unscheduled consultation with a physician, or temporary discontinuation of study treatment and resulted in pain or impairment of daily activities; overt bleeding episodes that did not meet the criteria for major or non-major clinically relevant bleeding were classified as minor bleeding [14]. Thromboembolic events were also defined using the same definition as the outcome and endpoint components in the J-ROCKET AF study [14]. Therefore, additional blood samplings in patients who experienced bleeding events were performed at the time of bleeding, and follow-up was interrupted.
All patients in this study were followed up in each hospital. Blood samples were collected from patients who experienced a bleeding event or neurological symptoms, and the next course of treatment, such as drug interruption or further therapeutic procedures, was determined at each hospital. We also recorded the follow-up outcomes by reviewing outpatient records or via phone calls to the general physician and the patients. Data collection was discontinued on December 30, 2021.
Statistical Analyses
A physician (MS) and statisticians (Hajime Yamakage, M Eng, et al., Satista, Co., Ltd., Kyoto) performed all statistical analyses using SPSS version 24. Statistical analyses were performed based on a 5% level of significance. The Wilcoxon two-sample test was used to compare the continuous variables, and the simple linear regression and correlation test was used to analyze the correlation coefficients. Logistic regression analyses were performed to determine the risk factors related to bleeding events. Data are expressed as means ± standard deviation.
3. Results
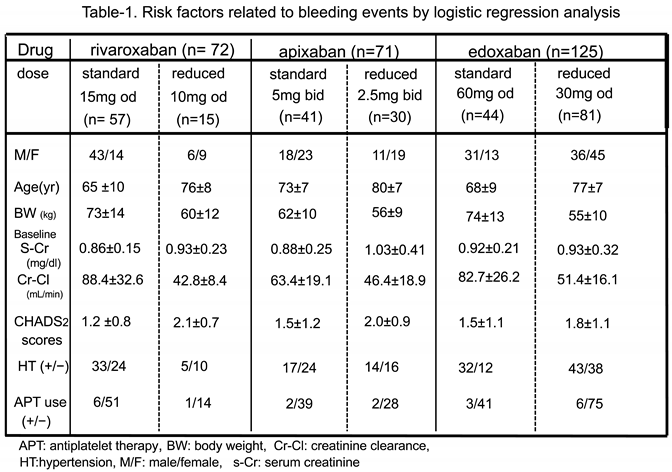
Patient Characteristics (Table 1)
Among the 289 outpatients registered at each hospital, 21 (8 in rivaroxabanm 6 in apixaban and 7 in edoxaban) were excluded because of off-label reduced dose use and/or withdrawal of consents. Table 1 shows the baseline characteristics of the 268 participants (72 rivaroxaban users, 71 apixaban users and 125 edoxaban users). The standard dose users were more in rivaroxaban and apixaban and the reduced dose users were more in edoxaban. The BW was lower, and the age was higher, in patients who received reduced doses than those who received standard doses. Additionally, there were no differences in the baseline Cr-Cl levels, CHADS2 score, the presence of HT, and antiplatelet drug use among those who received standard or reduced doses in all DOAC groups.
Drug PC Levels among Patients who Received Standard and Reduced Doses in all DOAC Groups(Table 2, Figure 2)
Among patients who received standard dose, the peak drug PC levels of rivaroxaban users were 304.1±93.6 ng/mL (n=57; range, 52.1–498.0 ng/mL), 313.5±115.5 ng/mL (n=52; range, 72.1–638.6 ng/mL), and 309.8±101.9 ng/mL (n=47; range, 47.0–474.0 ng/mL) in peaks 1, 2, and 3, respectively. For Apixaban users, the peak drug PC levels were 229.7±85.1 ng/mL (n=41; range, 36.5–414.4 ng/mL), 220.6±81.8 ng/mL (n=32; range, 31.7–373.6 ng/mL), and 266.8±92.7 ng/mL (n= 29; range, 73.3–448.1 ng/mL) in peaks 1, 2, and 3, respectively. For edoxaban users, the peak drug PC levels were 267.4±92.6 ng/mL (n=44; range, 34.0–441.3 ng/mL), 267.7±93.5 ng/mL (n=40; range, 108.8–488.3 ng/mL), and 279.9±75.5 ng/mL (n=34; range, 93.8–471.5 ng/mL) in peaks 1, 2, and 3, respectively. The number of standard dose users who had a peak PC exceeding the cutoff level for predicting bleeding events was more on rivaroxaban than those on apixaban and edoxaban (Figure 2).
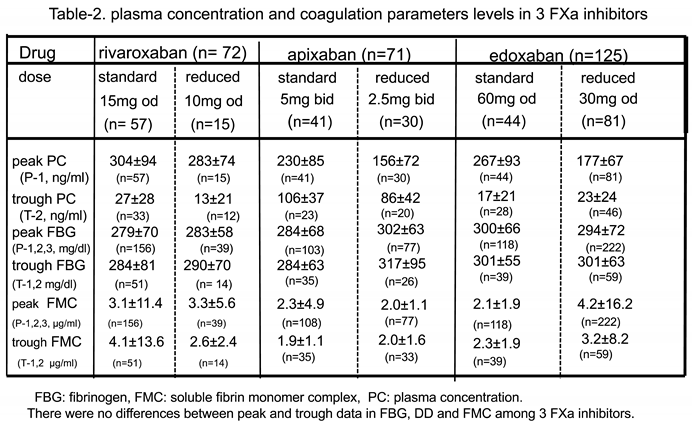
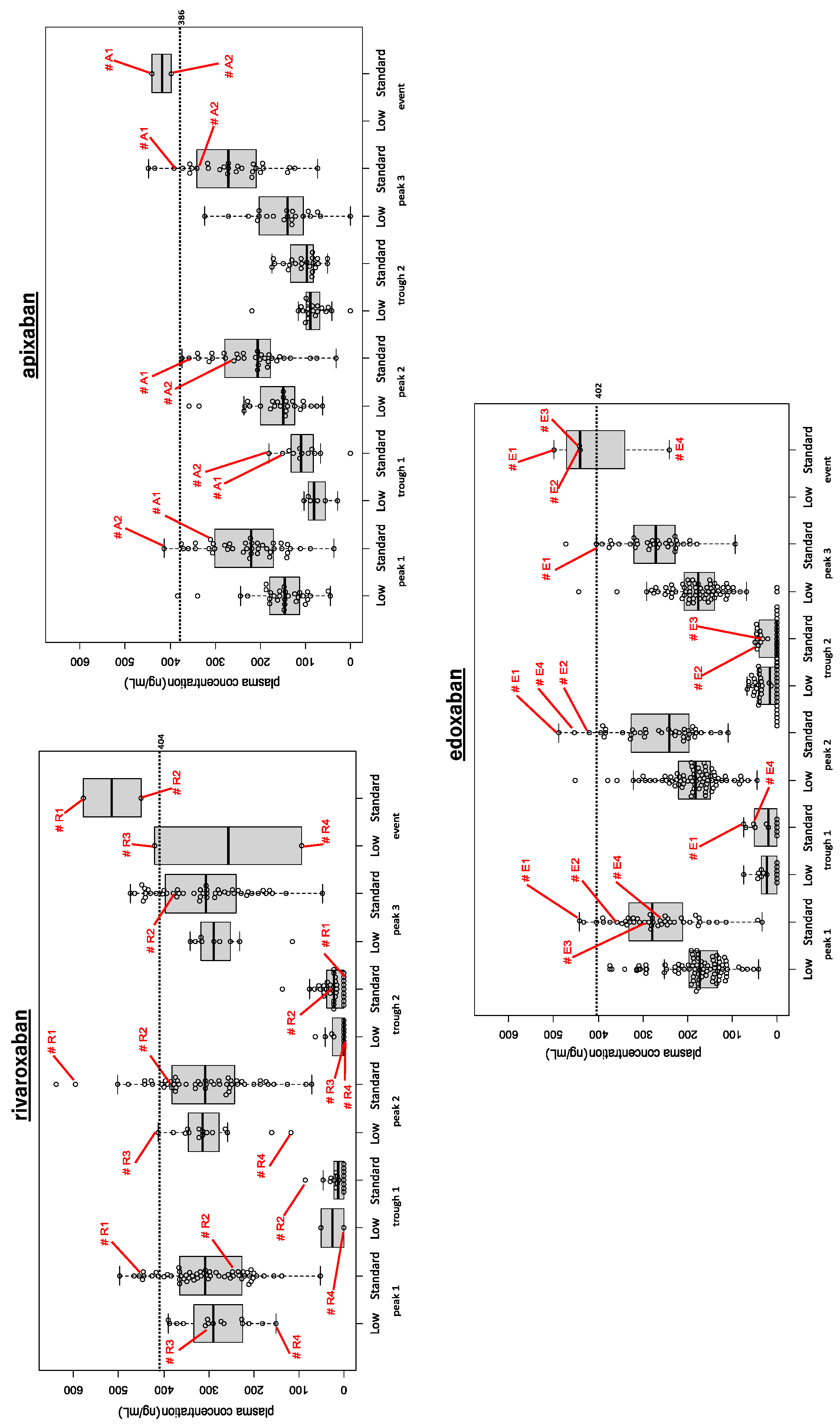
Figure 2.
Alteration in peak (peaks 1, 2, and 3) and trough (troughs 1 and 2) plasma concentration (PC) levels with time. Rivaroxaban (upper left), apixaban (upper right) and edoxaban (lower). The number of patients with a peak PC exceeding the cut-off level for each drug (indicated with dotted line) was higher for rivaroxaban than for apixaban and edoxaban users. The trough PC levels were higher in apixaban users than in rivaroxaban and edoxaban users. Patients who experienced bleeding events (four using rivaroxaban, two using apixaban, four using edoxaban) are indicated with red numbers.
Figure 2.
Alteration in peak (peaks 1, 2, and 3) and trough (troughs 1 and 2) plasma concentration (PC) levels with time. Rivaroxaban (upper left), apixaban (upper right) and edoxaban (lower). The number of patients with a peak PC exceeding the cut-off level for each drug (indicated with dotted line) was higher for rivaroxaban than for apixaban and edoxaban users. The trough PC levels were higher in apixaban users than in rivaroxaban and edoxaban users. Patients who experienced bleeding events (four using rivaroxaban, two using apixaban, four using edoxaban) are indicated with red numbers.
Among patients who received reduced doses, peak drug PC levels of rivaroxaban users were 282.5±74.0 ng/mL (n=15; range, 150.6–390.3 ng/mL), 300.1±77.0 ng/mL (n=15; range, 117.7–412.6 ng/mL), and 273.7±70.2 ng/mL, (n=9; range, 13.7–341.1 ng/mL) in peaks 1, 2, and 3, respectively. For apixaban users, peak drug PC levels were 155.5±71.9 ng/mL (n=30; range, 44.9–383.5 ng/mL), 166.0±71.3 ng/mL (n=26; range, 61.5–358.6 ng/mL), and 150.3±73.2 ng/mL (n=21; range, 0–323.5 ng/mL) in peaks 1, 2, and 3, respectively. For edoxaban users, peak drug PC levels were 177.4±66.7 ng/mL (n=81; range, 41.6–374.7 ng/mL), 190.1±70.5 ng/mL (n=74; range, 43.8–452.2 ng/mL), and 178.0±70.4 ng/mL (n=68; range, 0–444.1 ng/mL) in peaks 1, 2, and 3, respectively.
For peak 1 which blood samples were the most in number, the peak drug PC levels of these three FXa inhibitors were not significantly different in patients who received standard doses. In contrast, among patients who received reduced dose, the peak PC of rivaroxaban was significantly higher than that of apixaban and edoxaban dosing (p<0.05).
Among patients who received standard doses, the trough drug PC levels of rivaroxaban, apixaban and edoxaban were 16.2±22.2 ng/mL (n=18; range, 0–86.3 ng/mL) ng/mL and 27.4±28.4 ng/mL (n=33; range, 0–136.4 ng/mL), 104.6±45.9 ng/mL (n=12; range, 0–180.4 ng/mL and 106.4±36 ng/mL (n=23; range, 51.2–175.2 ng/mL), and 26.3±30.1 ng/mL (n=11; range, 0–75.3 ng/mL) and 17.2±20.8 ng/mL (n=28; range, 0–49.2 ng/mL) in troughs 1and 2, respectively.
Among patients who received reduced doses, the trough PC levels of rivaroxaban, apixaban and edoxaban were 25.1±35.5 ng/mL (n=2; range, 0–50.2 ng/mL) and 13.0±21.4 ng/mL (n=12; range, 0–63.5 ng/mL ng/mL), 73.6±27.5 ng/mL (n=6; range, 28.7–102.4 ng/mL) and 86.0±41.5 ng/mL (n=20; range, 0–218.7 ng/mL), and 21.5±23.8 ng/mL (n=13; range, 0–74.0 ng/mL) and 22.7±23.8 ng/mL (n=46; range, 0–67.3 ng/mL) in troughs 1 and 2, respectively. The trough drug PC levels of patients who received standard and the reduced dose of apixaban were significantly higher than those of rivaroxaban and edoxaban (p < 0.01; Figure 2). Peak 1 and trough 2 had the highest number of samples for standard and reduced doses.
Alterations in Peak PC Over Time among Three DOACs (Figure 2 and Figure 3)
As the primary data, we examined the number and incidence of patients with the peak 1 drug PC levels higher than each drug’s cut-off level for predicting bleeding events and their background characteristics (age, BW, and Cr-Cl). Overall, nine (9/57; 15.8%), one (1/29; 3.4%), and three (3/36; 8.3%) rivaroxaban, apixaban, and edoxaban standard dose users, respectively, had peak 1 drug PC levels higher than the cut-off level. However, there was no difference in the incidence and background characteristics between those with peak 1 drug PC levels higher than the cutoff level and those not having them among these three FXa inhibitors.
Figure 3.
Alteration in peak PC over time in the three FXa inhibitors.The number of patients with peak PC elevation over time (cases with PC level higher in peak 3 than in peak 1 and/or 2 indicated with solid lines, and cases without elevation with dotted lines) was 29/57 (50.9%) for rivaroxaban, and 18/48 for apixaban (37.5%), and 32/101 for edoxaban (31.7%, p < 0.05 vs. rivaroxaban). Also, the number of patients with peak PC levels higher than the cut-off level (indicated with red dotted lines in each drug) in peak 3 (accumulation rate: AR) was 13/29 rivaroxaban users (44.8%, 12 in standard dose and 1 in reduced dose users), and 4/18 apixaban users (22.2%, all standard dose), and 5/32 edoxaban users (15.6%, 4 in standard dose and 1 in reduced dose users, p<0.05 vs rivaroxaban).
Figure 3.
Alteration in peak PC over time in the three FXa inhibitors.The number of patients with peak PC elevation over time (cases with PC level higher in peak 3 than in peak 1 and/or 2 indicated with solid lines, and cases without elevation with dotted lines) was 29/57 (50.9%) for rivaroxaban, and 18/48 for apixaban (37.5%), and 32/101 for edoxaban (31.7%, p < 0.05 vs. rivaroxaban). Also, the number of patients with peak PC levels higher than the cut-off level (indicated with red dotted lines in each drug) in peak 3 (accumulation rate: AR) was 13/29 rivaroxaban users (44.8%, 12 in standard dose and 1 in reduced dose users), and 4/18 apixaban users (22.2%, all standard dose), and 5/32 edoxaban users (15.6%, 4 in standard dose and 1 in reduced dose users, p<0.05 vs rivaroxaban).
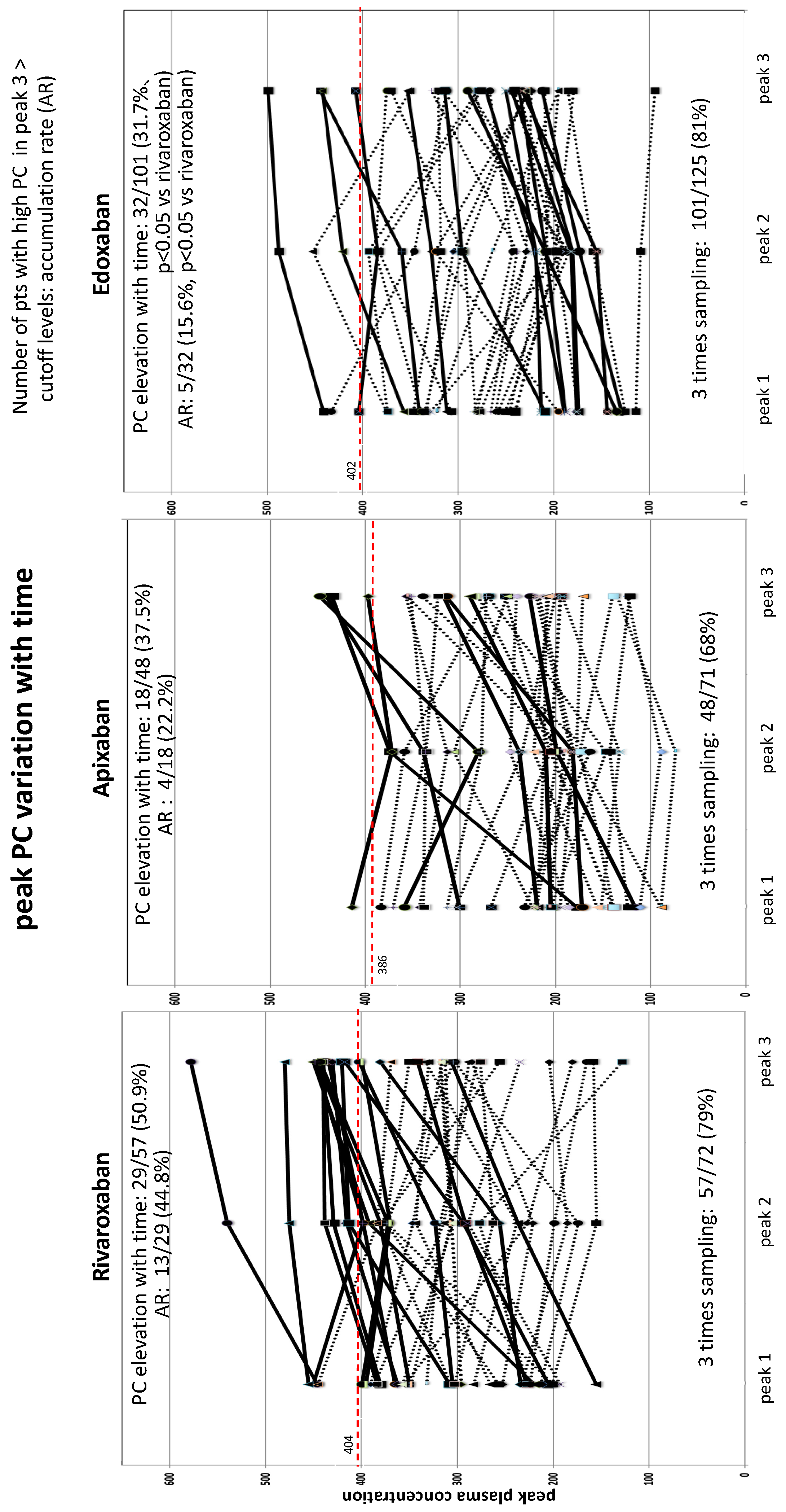
Next, we evaluated the alterations in peak PC levels over time in patients with three samplings under standard dose use (57 rivaroxaban users, 29 apixaban users, and 36 edoxaban users). The number of patients with drug PC elevation over time (PC higher in peak 3 than in peak 1 and/or 2) was 29/57 (50.9%) rivaroxaban users, 18/48 (37.5%, ns vs rivaroxaban) apixaban users, and 32/101 (31.7%, p<0.05 vs rivaroxaban) edoxaban users. Furthermore, among those with elevated drug PC levels over time, the number of patients with drug PC levels higher than the cut-off level in peak 3 (accumulation rate) were 13/29 rivaroxaban users (44.8%, 12 in standard dose and 1 in reduced dose users), 4/18 apixaban users (22.2%, all standard dose), and 5/32 edoxaban users (15.6%, 4 in standard dose and 1 in reduced dose users, p < 0.05 vs rivaroxaban); the incidence of drug accumulation lessened in edoxaban. Also, in both of rivaroxaban and edoxaban users, BW lowered in those with peak PC levels higher than the cut-off level in peak 3 sampling, compared with those with lower one (rivaroxaban; 62 ±11 Kg; n = 13 vs 75 ± 19 Kg; n = 37, p < 0.05, edoxaban; 63 ± 2 kg; n = 4 vs 75 ± 9 Kg; n = 8, p < 0.05), but the statistical difference may be not conclusive because the number of patients were small.
Bleeding and Thromboembolic Events among DOAC Users (Figure 2)
Bleeding events occurred in four rivaroxaban users (two each receiving standard and reduced doses; major in three: [patients R1, R2, and R3] and minor in one [patient R4]; indicated with red numbers), two apixaban users (all receiving standard doses; both major [patients A1 and A2]; indicated with red numbers)., and four edoxaban users (all receiving standard doses; major in three [patients E1, E2, and E4] and non-major in one [patient E3]; indicated with red numbers). As the incidence of bleeding was too low we could not determine the appropriate cut-off levels for detecting bleeding events. Meanwhile, there were no thromboembolic events in this study.
Among the 10 patients who experienced bleeding events, 8 had peak drug PC levels exceeding each drug’s cut-off levels for predicting bleeding events that was caused by drug overdose based on analysis. However, as patients R4 and E4 had drug PC levels below the cut-off level, we supposed that bleeding in these two patients was not drug induced (R4: subcutaneous contact bleeding and E4; gastric bleeding due to ulcerated lesion).
Other Coagulation Biomarkers (Table 2, Figure 4A and Figure 4B)
For the FBG levels (normal range: 200–400 mg/dL), we obtained the integrated peak data (peak FBG) from peaks 1, 2, and 3 sampling and the integrated trough data (tough FBG) from troughs 1 and 2 samplings from all patients. Among patients who received standard and reduced doses of rivaroxaban, the integrated peak and trough FBG levels were 278.9±69.5 mg/dL (n = 156) and 283.7 ±80.6 mg/dL (n = 51), and 283.2 ± 58.4 mg/dL (n = 39) and 289.6±70.4 mg/dL (n = 14), respectively. Among patients who received standard dose and reduced doses of apixaban, the integrated peak and trough FBG levels were 284.4±67.6 mg/dL (n = 103) and 283.5±63.0 mg/dL (n = 35), and 301.5±63.0 mg/dL (n = 77) and 316.9±94.5 mg/dL (n = 26), respectively. Among patients who received standard dose and reduced doses of edoxaban, the integrated peak and trough FBG levels were 300.4 ± 65.9 mg/dL (n = 118) and 300.6 ±55.1 mg/dL (n = 39), 294.1±71.8 mg/dL (n = 222) and 301.4±62.7 mg/dL (n = 59), respectively. This suggests that among all three DOACs, FBG levels at peak and trough timing did not significantly differ regardless of dose. However, some patients had high FBG levels of >500 mg/dL during the peak drug PC or both during the peak and trough drug PC. Nevertheless, these abnormalities were not related to thrombogenesis.
Figure 4.
Relationship between drug plasma concentration (PC) (left) and fibrin monomer complex (FMC) (right) levels during peak and trough timing in patients receiving standard (A) and reduced (B) doses of FXa inhibitors. Although drug PC levels widely varied from peak to trough timing, FMC levels, minimally varied over time regardless of the peak and trough timing of the drug, dose amount, and frequency of dosing. Dotted lines: cut-off levels for predicting bleeding events in each DOAC (left), and normal FMC range (< 6.1 µg /mL) (right).
Figure 4.
Relationship between drug plasma concentration (PC) (left) and fibrin monomer complex (FMC) (right) levels during peak and trough timing in patients receiving standard (A) and reduced (B) doses of FXa inhibitors. Although drug PC levels widely varied from peak to trough timing, FMC levels, minimally varied over time regardless of the peak and trough timing of the drug, dose amount, and frequency of dosing. Dotted lines: cut-off levels for predicting bleeding events in each DOAC (left), and normal FMC range (< 6.1 µg /mL) (right).
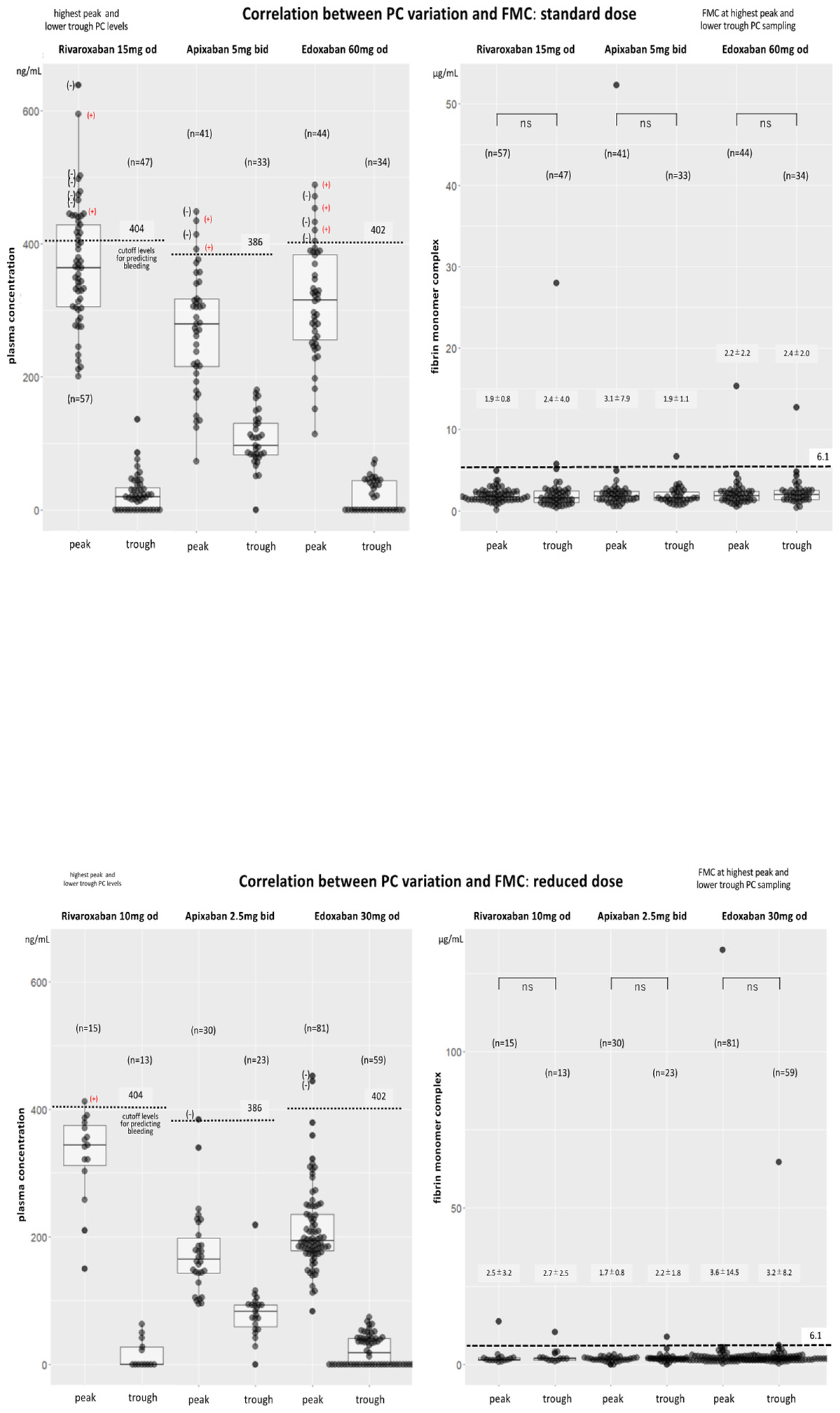
Regarding FMC levels (normal range of < 6.1 µg/mL), we obtained the integrated peak data (peak FMC) from peaks 1, 2, and 3 sampling and the integrated trough data (tough FMC) from troughs 1 and 2 sampling from all patents. Among patients who received standard and reduced doses of rivaroxaban, the integrated peak and trough FMC was 3.1 ±11.4 µg /mL (n = 156) and 4.1 ±13.6 µg/mL (n = 51) and 3.3 ±5.6 µg/mL (n = 39) and 2.6 ±2.4 µg/mL (n = 14), respectively. Among patients who received standard and reduced dose doses of apixaban, the integrated peak and trough FMC levels were 2.3 ±4.9 µg/mL (n = 108) and 1.9 ±1.1 µg/mL (n=35), and 2.0±1.1 µg/mL (n = 77) and 2.0 ±1.6 µg/mL (n=33), respectively. Among patients who received standard and reduced dose doses of edoxaban, the integrated peak and trough FMC levels were 2.1±1.9 µg/mL (n = 118) and 2.3 ±1.9 µg/mL (n = 39), and 4.2±16.2 µg/mL (n = 222) and 3.2 ±8.2 µg/mL (n = 59), respectively. Among all three DOACs, the FMC levels at the peak and trough time did not significantly differ regardless of dose. However, as shown by the FIB levels, some patients had FMC levels of >100 µg/mL only during the peak or both during the peak and trough time. Additionally, large standard deviations were observed among rivaroxaban and edoxaban users. However, we considered that these abnormalities were not caused by thrombogenesis. The integrated FBG and FMC data according to each dose in these three DOACs is shown in Table 2.
We then compared the relationship between drug PC levels and FMC levels at peak and trough timing among three FXa inhibitors. For these comparisons, as peak FMC data, we selected the FMC data at the highest peak PC level from peaks 1, 2, and 3 samplings, and as trough FMC, the FMC data at the lowest PC level from troughs 1 or 2 sampling, in both of standard and reduced dose use. Although the drug PC levels widely varied from peak to trough timings, FMC levels did not significantly vary regardless of dose or frequency of drug administration. Notably, FMC levels were maintained even in patients on once-daily drugs, rivaroxaban and edoxaban (Figure 4A and Figure 4B).
4. Discussion
This multicenter registry study (the SET DOAC registry; UMIN000036769) was performed to evaluate the efficacy and the safety of three FXa inhibitors (rivaroxaban, apixaban, and edoxaban) coupled with monitoring of coagulation biomarkers; PC, FIB and FMC levels, at peak and trough timing. These three DOACs in this study had comparable antithrombotic effects even during the trough timing and regardless of frequency of administration. However, the plasma levels of rivaroxaban tended to accumulate over time when compared to edoxaban.
The concern with once-daily DOACs is that their effects may be reduced when drug PCs are at their trough [15,16]. Meanwhile, twice-daily DOACs have two peaks, and their trough PC levels are not as low as those of once-daily DOACs [15]. Therefore, when considering DOACs for the secondary prevention of stroke, physicians tend to select twice-daily DOACs. Unfortunately, the number of patients in this study was too low to determine the anticoagulant effect of the three DOACs based on their PCs alone. However, levels of coagulant biomarkers used in this study (FBG and FMC) remained low even during trough PCs in patients using once-daily DOACs. This suggests that the risks of thrombotic events when using once-daily DOACs is low.
The efficacy and safety of the three FXa inhibitors have been reported in several large randomized trials [2,3,5,7]. When compared with warfarin, rivaroxaban and edoxaban were noninferior, whereas apixaban was superior, in preventing stroke or systemic embolism. Regarding bleeding events, apixaban and edoxaban resulted in a lower incidence of bleeding compared with warfarin, but there was no significant difference in the incidence of major bleeding between rivaroxaban and warfarin [2]. Meanwhile, two studies reported that apixaban and edoxaban were associated with a lower rate of ischemic stroke compared with rivaroxaban [2,17]. In contrast, one study reported that the incidence of ischemic stroke was not significantly different among the three DOACs plus dabigatran [18]. Additionally, reports comparing once- versus twice-daily DOACs revealed that twice-daily DOACs might have a more balanced risk–benefit profile between thromboembolism and bleeding events [19,20]. However, recent reports have stated that there is no clear difference between once- and twice-daily DOACs in terms of adverse outcomes and that the incidence of adverse outcomes was higher in low adherence than in high adherence, regardless of the dosing frequency [21,22].
Regarding the activity of coagulation biomarkers during trough timing, Shinohara et al. examined the drug PC levels as well as the D-dimer levels and prothrombin fragment 1+2, which represented coagulation biomarkers, in patients who temporarily discontinued edoxaban for catheter ablation [23]. They reported that the drug PC levels further decreased 24 hours after discontinuing edoxaban, but the PC of prothrombin fragment remained unchanged even after 30 h. In our report wherein we evaluated FIB and FMC levels as the coagulation biomarkers, we used FMC as an alternative for assessing thrombosis in addition to FIB as it reflects thrombin activity and can be detected earlier than D-dimer [24]. Therefore, in terms of the level of coagulation biomarkers, there is no clear difference between once- and twice-daily DOACs. Currently, the half-time of FMC remains unclear. The facts that there is no difference in FMC levels between peak and trough timing may be inconclusive.
We could not assess the safety concerning to bleeding of the DOACs in this study as the incidence of bleeding was low. However, in routine practice, rivaroxaban has a higher bleeding incidence than apixaban and edoxaban [2,3,4,5,6,7]. Additionally, in patients of extreme BW, a practical guide to DOAC use suggests that special care is needed particularly for individuals with a BW of ≤60 kg, in whom a lower dose use of apixaban and edoxaban should be administered [1,8]. Also, the EHRA guide indicates to consider PC monitoring when prescribing rivaroxaban or dabigatran in patients with a BW of <60 kg. Furthermore, in a preliminary study from our institute preceding this SET DOAC registry, edoxaban had a more favorable safety profile than rivaroxaban with PC monitoring (Hokusetsu DOAC study), [9]. Regarding bleeding events with rivaroxaban, this study showed that the drug accumulation may be related to the development of bleeding.
The current study had some limitations. Although this study was conducted at several institutions, the number of enrolled patients and the incidence of bleeding events were too low to draw definitive conclusions about the risk of bleeding events among these three drugs. However, we could determine the variation in PC levels over time among the three DOACs, though this result may be affected by the small sample size. In this study, the Biophen DiXaI kit that employed the chromogenic anti-FXa assay was used. We used the cut-off PC level obtained from our previous study. Considering that few kits currently provide a chromogenic assay, the cut-off PC level for predicting bleeding events may vary depending on the kit used. Therefore, another multicenter study may be needed for confirming the results.
5. Conclusions
Coagulant activity, as shown by FMC, was suppressed throughout the day even if the drug PC levels of once-daily DOACs declined to almost zero in trough time, suggesting that the risk of thrombotic events remains low even for these drugs. Compared with edoxaban, rivaroxaban results in drug accumulation, which may cause the elevation of drug PC levels, paticularly higher than the cut-off for bleeding events, over time.
Author Contributions
Conceptualization: M Suwa, M Isao, Y Matsui Data curation: M Suwa, T Suzuki Formal analysis: M Suwa Investigation: M Suwa, M Isao, Y Matsui, H Takahashi, A Yoshida, G Fujiki, M Tanimura, H Shimoyama, H Saitoh, S Yamashita Methodology: M Suwa, M Isao, Y Matsui Resources: T Suzuki, S Uemae, N Matsuo Supervisions: M Kino, M Yoshinaga, M Takagi, M Ichikawa, O Nakajima, I Sasaki Validation: M Suwa, T Suzuki Writing; original draft: M Suwa Writing; review & editing: I Mori, M Kino, M Takagi. All authors have read and agreed to the published version of the manuscript.
Funding
This study received no external funding.
Institutional Review Board statement
This study was approved by the ethical committee at each hospital. The ethical review committee at each hospital approved this study (March ~December 2018).
Informed consent statement
All patients provided written informed consent.
Conflict of Interest
The authors declare no conflicts of interest.
References
- Steffel, J.; Collins, R.; Antz, M.; Cornu, P.; Desteghe, L.; Haeusler, K.G.; Oldgren, J.; Reinecke, H.; Roldan-Schilling, V.; Rowell, N.; et al. 2021 European Heart Rhythm Association practical guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Europace 2021, 23, 1612-1676. [CrossRef] [PubMed]
- Lee, S-R.; Choi, E-K.; Kwon, S.; Han, K-D.; Jung, J-H.; Cha, M-J, Oh, S.; Gregory Y.J. Effectiveness and safety of contemporary oral anticoagulants among Asians with nonvalvular atrial fibrillation. Stroke 2019, 50, 2245-2249. [CrossRef]
- Yao, X.; Abraham, N.S.; Sangaralingham, L.R.; Bellolio, F.; McBane, R.D.; Shah, N.D.; Noseworthy, P.A. Effectiveness and safety of dabigatran, rivaroxaban, and apixaban versus warfarin in nonvalvular atrial fibrillation. J Am Heart Assoc 2016, 5, e003725. [CrossRef] [PubMed]
- Proietti, M.; Romanazzi, I.; Romiti, G.F.; Farcomeni, A.; Lip, G.Y.H. Real-world use of Apixaban for stroke prevention in atrial fibrillation. A systematic review and meta-analysis. Stroke 2018, 49, 98-106. [CrossRef]
- Fralick, M.; Colacci, M.; Schneeweiss, S.; Huybrechts, K.F.; Lin, K.J.; Gagne, J.J. Effectiveness and safety of apixaban compared with rivaroxaban for patients with atrial fibrillation in routine practice: A cohort study. Ann Intern Med 2020, 172, 463-473. [CrossRef] [PubMed]
- Lip, G.Y.H.; Keshishian, A.V.; Zhang, Y.; Kang, A.; Dhamane, A.D.; Luo, X.; Klem, C.; Ferri, M.; Jiang, J.; Yuce, H. et al. Oral anticoagulants for nonvalvular atrial fibrillation in patients with high risk of gastrointestinal bleeding. JAMA Netw Open 2021, 4, e2120064. [CrossRef] [PubMed]
- Cho, M.S.; Yun, J.E.; Park, J.J.; Kim, Y.J.; Lee, J.; Kim, H.K.; Park, D-W.; Nam, G-B. Outcomes after use of standard- and low-dose non-vitamin K oral anticoagulants in Asian patients with atrial fibrillation. Stroke 2019, 50, 110-118. [CrossRef]
- Chen, A.; Stecker, E.; Warden, B.A. Direct oral anticoagulant use: a practical guide to common clinical challenges. J Am Heart Assoc 2020, 9, e017559. [CrossRef] [PubMed]
- Suwa, M.; Nohara, Y.; Morii, I.; Kino, M. Safety and efficacy re-evaluation of edoxaban and rivaroxaban dosing with plasma concentration monitoring in non-valvular atrial fibrillation: With observations of on-label and off-label dosing. Circ Rep 2023, 5, ,80-89. [CrossRef]
- Tanigawa, T.; Kaneko, M.; Hashizume, K.; Kajikawa, M.; Ueda, H.; Tajiri, M.; Paolini, J.G. Mueck, W. Model-based dose selection for phase III rivaroxaban study in Japanese patients with non-valvular atrial fibrillation. Drug Metab Pharmacokinet 2013, 28, 59-70. [CrossRef] [PubMed]
- BIOPHENTMDiXaI http://www.hyphen-biomed.com/images/Notices/BI-BIOPHEN/ANG-D750-02/02-1030 (accessed September 30, 2023).
- Suwa, M.; Morii, I.; Kino, M. Rivaroxaban or apixaban for non-valvular atrial fibrillation: Efficacy and safety of off-label under-dosing according to plasma concentration. Circ J 2019, 83, 991-999. [CrossRef] [PubMed]
- Schulman, S.; Kearon, C. Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in nonsurgical patients. J Thromb Haemost. 2005, 3, 692–694. [CrossRef] [PubMed]
- Hori, M.; Matsumoto, M.; Tanahashi, N.; Momomura, S.; Uchiyama, S.; Goto, S.; Izumi, T.; Koretsune, Y.; Kajikawa, M.; Kato, M.; et al. Rivaroxaban vs. warfarin in Japanese patients with atrial fibrillation. The J-ROCKET AF Study. Circ J 2012, 76, 2104-2111. [CrossRef]
- Gong, I.Y.; Kim, R.B. Importance of pharmacokinetic profile and variability as determinants of dose and response to dabigatran, rivaroxaban and apixaban. Can J Cardiol 2013, 29, S23-33. [CrossRef] [PubMed]
- Lip, G.Y.H.; Agnelli, G. Edoxaban: A focused review of its clinical pharmacology. Eur Heart J 2014, 35, 1844-1855. [CrossRef] [PubMed]
- Ray, W.A.; Chung, C.P.; Stein, C.M.; Smalley, W.; Zimmerman, E.; Dupont, W.D.; Hung, A.M.; Daugherty, J.R.; Dickson, A.; Murray, K.T. Association of rivaroxaban vs apixaban with major ischemic or hemorrhagic events in patients with atrial fibrillation. JAMA 2021, 326, 2395-2404. [CrossRef] [PubMed]
- Chan, Y-H.; Lee, H-F., See, L-C.; Tu, H-T.; Chao, T-F.; Yeh, Y-H.; Wu, L-S., Kuo, C-T.; Chang, S-H.; Lip, G.Y.H. Effectiveness and safety of four direct oral anticoagulants in Asian patients with nonvalvular atrial fibrillation. Chest 2019, 156, 529-543. [CrossRef]
- Clemens, A.; Noack, H.; Brueckmann, M.; Lip, G.Y.H. Twice- or once-daily dosing of novel oral anticoagulants for stroke prevention: A fixed-effects meta-analysis with predefined heterogeneity quality criteria. PLOS ONE 2014, 9, e99276. [CrossRef]
- Vrijens, B.; Heidbuchel, H. Non-vitamin K antagonist oral anticoagulants: Considerations on once- vs twice-daily regimens and their potential impact on medication adherence. Europace 2015, 17, 514-523. [CrossRef] [PubMed]
- Hwang, H-J.; Sohn, I.S.; Jin, E-S.; Bae, Y-J. Adherence and clinical outcomes for twice-daily versus once-daily dosing of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation: Is dosing frequency important? PLOS ONE 2023,18, e0283478. [CrossRef]
- Polymeris, A.A.; Zietz, A.; Schaub, F.; Meya, L.; Traenka, C.; Thilemann, S.; Wallllllgner, B., Hert, L.; Altersberger, V.L.; Seiffge, D.J.;et al. Once versus twice daily direct oral anticoagulants in patients with recent stroke and fibrillation. Eur Stroke J 2022, 7, 221-229.
- Shinohara, T.; Takahashi, N.; Mukai, Y.; Kimura, T. Yamaguchi, K.; Takita, A.; Origasa, H.; Okumura, K.; the KYU-RABLE investigators. Changes in plasma concentrations of edoxaban and coagulation biomarkers according to thromboembolic risk and atrial fibrillation type in patients undergoing catheter ablation: Subanalysis of KYU-RABLE. J Arrhythmia 2021, 37, 70-78. [CrossRef]
- Refaai, M.A.; Riley, P.; Mardovina, T.; Bell, P.D. The clinical significance of fibrin monomers. Thromb Haemost 2018, 118, 1856-1866. [CrossRef]
Figure 1.
Flowchart of blood sampling and patient enrollment.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



