
Submitted:
25 August 2025
Posted:
26 August 2025
You are already at the latest version
Abstract
Background: Anticoagulation is the cornerstone of thromboembolic event prevention. Adversely, anticoagulants (ACs) are linked to a variety of adverse events. We aimed to assess the link between vitamin K antagonists (VKA) and direct anticoagulant (DOACs) use and acute kidney injury (AKI) using the FDA Adverse Events Reporting System (FAERS) Database. Methods: We conducted a disproportionality analysis on the adverse events (AEs) of interest in the FAERS database using the reporting odds ratio (ROR), proportional reporting ratio (PPR) with the Yates correction (x2yates), and the information component (IC). Results: A total of 20,253 cases of AKI associated with use of ACs were analyzed. Edoxaban, dabigatran and warfarin showed greater association with AKI (ROR 2,63; ROR 1,46; ROR). In cases with manifest bleeding, edoxaban, dabigatran, warfarin and rivaroxaban had a stronger statistical association with AKI. Rivaroxaban showed greater association with AKI compared to other ACs when used concomitantly with Aspirin (ROR 2,25). Conclusion: We showed increased odds of reporting AKI with use of edoxaban, dabigatran and warfarin compared to other anticoagulants. In cases with reported bleeding, AKI was more commonly reported with all five analyzed anticoagulants, except for apixaban, highlighting its favorable side-effect profile. Caution and clinical awareness are needed when prescribing ACs to vulnerable populations.
Keywords:
anticoagulant
; anticoagulant-related nephropathy
; acute kidney injury
; FAERS
; disproportionality analysis
1. Introduction
Anticoagulation therapy is the cornerstone of preventing thromboembolic events, especially in patients with atrial fibrillation and deep venous thrombosis [1,2,3]. Oral anticoagulants (OACs) can roughly be categorized into vitamin K antagonists (VKA), mainly warfarin, and direct oral anticoagulants (DOACs) – apixaban, rivaroxaban, dabigatran and edoxaban. With invention and implementation of DOACs, certain side effects such as an increased risk of bleeding have been reduced, but remain present [4,5]. Beyond overt bleeding, one more clinically important complication has gained increasing recognition in recent years – anticoagulant-related nephropathy (ARN). Originally associated with warfarin use, ARN has since been acknowledged as a possible complication of all ACs [6,7].
Typically associated with glomerular hemorrhage and tubular obstruction by red blood cell casts [8], pathogenesis of ARN seems to be multifactorial in nature. Acute glomerular injury and/or a significant reduction in the total number of nephrons are described as possible prerequisites for ARN [9]. This consideration is particularly relevant for patients with pre-existing CKD, who frequently exhibit reduced nephron mass and heightened susceptibility to glomerular damage, thereby increasing their risk of developing ARN [10]. In addition, lower levels of antioxidative enzymes, such as glutathione, commonly observed in CKD patients, may further exacerbate renal vulnerability by impairing the clearance of oxidative byproducts, especially heme and iron in the setting of hematuria [10,11].
The Food and Drug Administration Adverse Event Reporting System (FAERS) database provides a valuable tool for evaluating the association between OACs and acute kidney injury (AKI). In this study, we aim to characterize the frequency and severity of ARN in patients receiving OAC therapy.
2. Materials and Methods
We conducted a disproportionality pharmacovigilance study using the publicly available FAERS database quarterly reports. A total of 85 reports from January 2004 until March 2025 were analyzed for cases associated with 5 FDA-approved anticoagulant medications: apixaban (Eliquis), rivaroxaban (Xarelto), edoxaban (Lixiana), dabigatran (Pradaxa) and warfarin (Coumadin, Jantoven). Both generic and brand names were included in the search. Prior to analyzing the cases, we deduplicated them using their unique identification code called “PRIMARYID” found in the “DEMO” file of each quarterly report. Each drug reported in case is categorized as a primary suspect, secondary suspect, a concomitant drug or an interacting drug. We analyzed cases where an AC drug was either a primary or a secondary suspect. When looking at possible synergistic effects of Aspirin on AKI in patients with AC use, we included cases where Aspirin was either a concomitant or an interacting drug in cases where either one of the AC drugs were primary or secondary suspects.
The preferred terms code of the Medical Dictionary for Regulatory Activities (MedDRA) was utilized to search for AKI terms, which included a total of 19 terms (Supplementary Table S1). When analyzing for co-occurrence of AKI and bleeding, we included the 20 most commonly reported bleeding AEs associated with AC use (Supplementary Table S1). A flow chart showing the case selection process is illustrated on Figure 1.
After obtaining the data, we conducted a disproportionality analysis using the reporting odds ratio (ROR), proportional reporting ratio (PPR) with the Yates correction (x2yates), and the information component (IC). The formulas of these methods are listed below:
To be statistically significant, mentioned disproportionately reported signals needed to meet the following criteria [12]:
- ROR025 (lower limit of the 95% confidence interval of ROR) >1 and adverse events >3.
- The IC025 (lower limit of the 95% credible interval of IC) >0.
- Use of PRR detects a signal when the number of co-occurrences is 3 or more and the PRR is 2 or more with an associated x2 value of 4 or more.
- EB05, a lower one-sided 95% confidence limit of EBGM, is considered significant when it is greater than or equal to 2.
Data cleaning and disproportionality analysis was performed using RStudio software (Version: 2025.05.1+513, Posit team (2025), Integrated Development Environment for R. Posit Software, PBC, Boston, MA).
3. Results
At the time of analysis, a total of 22,645,242 adverse event reports were registered in the FAERS database from January 1st, 2004, until March 31st, 2025. Of those, 874,340 were associated with anticoagulant use. After removing duplicate cases, a total of 441,807 cases were analyzed – apixaban (n = 170,909, 38.7%), rivaroxaban (n = 177,365, 40.1%), edoxaban (n = 5,196, 1.2%), dabigatran (n = 55,735, 12.6%) and warfarin (n = 32,602, 7.4%). Of these, 20,253 (4.6%) reported acute kidney injury, while 8,625 (1.9%) reported acute kidney injury in association with bleeding (Table 1).
When removing cases with unknown or incorrectly reported gender, cases with male patients predominated with 51.0%. The total average age was 72.9 ± 14.1, with warfarin cases showing the youngest average age (70.6 ± 14.4). The most common reason for AC use was atrial fibrillation (21.3%), followed by cerebrovascular accident prophylaxis (17.7%), thrombosis prophylaxis (6.3%) deep vein thrombosis (4.9%) and pulmonary embolism (3.1%). Most cases (43.8%) were reported in the United States, followed by France (8.3%) and Japan (7.2%). Hospitalization was the most common outcome (46.9%), with 10.1% cases ending in death. Almost all cases (96.7%) were reported as serious (Table 1).
When looking at cases of AKI with co-occurrence of bleeding, the predominating gender was male (54.6%), most reports were from the United States (59.3%), most common indication for AC use was atrial fibrillation (27.4%), and the most common outcome was hospitalization (58.7%) (Table 2).
According to the disproportionality analysis, edoxaban, dabigatran and warfarin had significant associations with acute kidney injury compared to other ACs (ROR 2.63, PPR 2.45, x2yates 494.57 with p <0.001, IC 1.27; ROR 1.46, PPR 1.43, x2yates 392.65 with p <0.001, IC 0.44; ROR 1.14, PPR 1.13, x2yates 25.27 with p <0.001, IC 0.17) (Table 3).
When looking at cases of AKI with bleeding, all ACs except for apixaban showed significant association compared to other ACs (Table 4).
When applying the disproportionality analysis on anticoagulant-related cases where acetylsalicylic acid (Aspirin) was labeled either a concomitant or an interacting drug, only rivaroxaban showed association to AKI (ROR 2.25, PPR 2.21, x2yates 20.12 with p<0.001, IC 0.63) (Table 5).
4. Discussion
Drug-induced nephropathy is an increasing problem in both the inpatient and outpatient settings. An estimated 27% of all AKI shows a drug-induced injury pattern on a kidney biopsy [13]. Most commonly implied medication groups are antibiotics and NSAIDs [14], however a growing prevalence in use of anticoagulants has linked them to possible AKI. A specific difficulty in discerning the exact epidemiology of ARN is the need for biopsy as a confirmatory test – something often deferred in the setting of possible over-anticoagulation. This makes ARN mostly a clinical diagnosis, based on changes in laboratory findings such as elevation of creatinine levels or INR, and connection between the start of OAC use and subsequent clinical and kidney function deterioration.
Anticoagulants are most commonly used in thromboembolic prophylaxis in atrial fibrillation (Table 1). Patients with AF often have concomitant kidney disease, as CKD is considered an independent risk factor for development of AF [15]. In addition, CKD is one of the strongest risk factors for development of ARN [8,16]. An important consideration with use of OAC in patients with CKD is supratherapeutic dosing. As mentioned, AF and CKD tend to cooccur [17,18]. This leads to possible OAC toxicity and over-anticoagulation in the setting of worsening kidney function. Some DOACs, primarily edoxaban and apixaban, are reduced by half of the original dose, leaving room for overdosing patients if kidney function is not monitored closely. Studies have found that dabigatran shows a dose-dependent elevation in serum creatinine levels and aPTT [19]. This accents the importance of dose adjustment for individual patients and their kidney function, as dabigatran, but also other DOACs to a varying degree, are excreted by the kidneys [20,21,22,23].
Our results showed an association between edoxaban, dabigatran and warfarin use and AKI. The most notable association was for edoxaban use, with an ROR of 2.63, indicating a near threefold higher odds of reported AKI. Of the three, the weakest association was seen with warfarin. This could be due to the decreasing trend of warfarin prescription since the approval of DOACs for stroke prophylaxis (as seen in Table 1).
Since one of the main pathophysiological explanations for ARN is propensity for bleeding and possible haemorrhagic damage of glomeruli, we separately performed an analysis of all cases in which AKI was reported with concomitant bleeding. In such cases, dabigatran, rivaroxaban, and warfarin showcased increased ROR compared to these ACs cases without bleeding, standing in line with previously described mechanisms of kidney injury. Disproportionality signals for edoxaban cases slightly reduced in strength but stayed positive, likely due to low number of cases in which both AKI and bleeding were reported with edoxaban use, as the drug is the most novel of all analysed ACs. Consensus on edoxaban nephrotoxicity is yet to be established, as literature shows diverging opinions. This might be due to the novelty of the drug and the reduced number of its prescriptions compared to other DOACs. Still, many studies lean on the side of caution with edoxaban, underscoring that it’s likely less safe in regard to kidney injury compared to its counterparts. The strength of this association is evident in our findings, where edoxaban had the highest ROR despite having the least number of reported cases of all the analyzed OACs (Table 1 and Table 2).
Apixaban is the only drug that showed no association with AKI regardless of concomitant bleeding. These findings do suggest that, among the newer DOACs, apixaban may carry the lowest nephrotoxic potential, consistent with clinical data showing apixaban’s relatively benign renal profile [24], and general safety [25], while edoxaban and dabigatran may confer a higher AKI risk.
We also analyzed reported data with patients on dual therapy (aspirin and OAC), commonly used in patients for AF and other concomitant conditions. One striking observation was a synergistic effect with aspirin in combination with rivaroxaban, with a significant ROR of 2.25. This suggests that the addition of an antiplatelet can amplify the risk of AC-related nephropathy and further amplifies the importance of OAC selection when initiating these patients on dual therapy. Although no prospective trial has focused on renal outcomes of such dual therapy, accumulating evidence from case reports, pharmacovigilance, and cohort studies suggests a synergistic nephrotoxic effect when aspirin is combined with an OAC. A single-center biopsy series of 41 ARN cases found that a subset had been on concurrent antiplatelet therapy at the time of AKI [16]. The adverse events associated with the addition of aspirin to DOAC without a clear indication was studied in a 2021 JAMA cohort, which examined 3280 patients and showed that nearly one-third of patients with AF and/or VTE who were treated with a DOAC received ASA without a clear indication. Compared to DOAC monotherapy, concurrent DOAC and ASA use was associated with increased bleeding and hospitalizations [17], mechanistically also leading to higher incidence of ARN, demonstrated in our results.
Clinicians managing patients on OACs should maintain a high index of suspicion for ARN, especially in those who have recently initiated therapy [26,27]. In the case of kidney injury, temporary discontinuation of VKA and DOACs, along with introduction of another agent or dose correction of VKA, is often needed. Minimizing antiplatelet therapy along with other supplements that can potentially provoke bleeding (e.g., Vitamin E) is also recommended. In severe cases that are proven by biopsy, corticosteroids can play an important role in their management. Alongside these measures, if biopsy demonstrates anticoagulant-related nephropathy, a warfarin-treated patient should be switched to a DOAC, whereas a DOAC-treated patient might benefit from dose reduction or a switch to a different anticoagulant strategy [10,28,29]. Clinicians should be aware of ARN as a possible culprit in AKI, and counsel patients on prompt reporting of hematuria or dark urine.
Ultimately, this FAERS-based analysis reveals an association between anticoagulant use (particularly edoxaban, dabigatran, rivaroxaban, and warfarin) and AKI that is biologically plausible and supported by literature [30,31,32]. The major strength of this analysis lies in its use of a rich, open-access database that includes extensive real-world data from multiple countries. Further prospective studies are needed to confirm causality. Judicious selection and dosing of anticoagulants, close monitoring of renal function (especially in the first couple of months of initiating therapy), and special caution taken with dual therapy alongside aggressive management of bleeding risk factors to safeguard the kidneys while providing essential anticoagulant therapy.
This study has several limitations typical of pharmacovigilance-based analyses. The FAERS database relies on voluntary reporting, making it subject to underreporting, reporting bias, and incomplete or inconsistent data. Therefore, the causality cannot be established. We decided to report cases that included ACs as both the primary and secondary possible suspect for an adverse event. This was done in order to cast a wider net on the database, have a greater data sample to analyse and reduce the chance of underreporting the association between ACs and AKI. In comparison to other studies that used only primary suspects, our approach may dilute the strength of the association between medication and adverse event. In addition, many potential confounding factors (e.g., comorbidities, baseline renal function, nephrotoxic medications) could not be fully accounted for.
Researching CKD, or in general patients and cases that pertain to kidney function, is inherently a limitation in itself. Multiple studies have shown that patients with kidney disease are overwhelmingly underrepresented in research and are often excluded from clinical trials and studies [33,34,35]. This, in turn, puts into question the generalization of study results and places further burden on treating this group of patients in an evidence-based manner.
To overcome these limitations, prospective cohort studies may help reduce bias and better clarify relationship between AC use and AKI. Furthermore, comparative studies assessing the renal safety profiles of ACs, particularly in patients with CKD, are needed to generate more reliable evidence.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org, Table S1: List of MedDRA terms used for data mining.
Author Contributions
Conceptualization: P.J.; methodology: P.J., C.C., N.J., S.M. and D.S.; validation: P.J.; formal analysis: P.J. and S.M.; investigation: P.J., C.C. and N.J.; resources: P.J., C.C. and N.J.; writing—original draft preparation P.J., C.C. and N.J.; writing—review and editing: P.J., C.C. and N.J; supervision: S.M. and D.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
No acknowledgments.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Soria Jiménez, C.E.; Papolos, A.I.; Kenigsberg, B.B.; Ben-Dor, I.; Satler, L.F.; Waksman, R.; Cohen, J.E.; Rogers, T. Management of Mechanical Prosthetic Heart Valve Thrombosis: JACC Review Topic of the Week. J Am Coll Cardiol 2023, 81, 2115–2127. [Google Scholar] [CrossRef]
- Vitolo, M.; Lane, D.A.; Boriani, G.; Lip, G.Y.H. The Importance of Adherence and Persistence with Oral Anticoagulation Treatment in Patients with Atrial Fibrillation. European Heart Journal - Cardiovascular Pharmacotherapy 2021, 7, f81–f83. [Google Scholar] [CrossRef]
- Diavati, S.; Sagris, M.; Terentes-Printzios, D.; Vlachopoulos, C. Anticoagulation Treatment in Venous Thromboembolism: Options and Optimal Duration. Curr Pharm Des 2022, 28, 296–305. [Google Scholar] [CrossRef]
- Zhu, J.; Alexander, G.C.; Nazarian, S.; Segal, J.B.; Wu, A.W. Trends and Variation in Oral Anticoagulant Choice in Patients with Atrial Fibrillation, 2010-2017. Pharmacotherapy 2018, 38, 907–920. [Google Scholar] [CrossRef] [PubMed]
- Geller, A.I.; Shehab, N.; Lovegrove, M.C.; Weidle, N.J.; Budnitz, D.S. Bleeding Related to Oral Anticoagulants: Trends in US Emergency Department Visits, 2016–2020. Thromb Res 2023, 225, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Oliver, T.; Salman, L.A.; Ciaudelli, B.; Cohen, D.A. Anticoagulation-Related Nephropathy: The Most Common Diagnosis You’ve Never Heard Of. The American Journal of Medicine 2019, 132, e631–e633. [Google Scholar] [CrossRef] [PubMed]
- Brodsky, S.V.; Satoskar, A.; Chen, J.; Nadasdy, G.; Eagen, J.W.; Hamirani, M.; Hebert, L.; Calomeni, E.; Nadasdy, T. Acute Kidney Injury During Warfarin Therapy Associated With Obstructive Tubular Red Blood Cell Casts: A Report of 9 Cases. American Journal of Kidney Diseases 2009, 54, 1121–1126. [Google Scholar] [CrossRef]
- Brodsky, S.V.; Collins, M.; Park, E.; Rovin, B.H.; Satoskar, A.A.; Nadasdy, G.; Wu, H.; Bhatt, U.; Nadasdy, T.; Hebert, L.A. Warfarin Therapy That Results in an International Normalization Ratio above the Therapeutic Range Is Associated with Accelerated Progression of Chronic Kidney Disease. Nephron Clinical Practice 2010, 115, c142–c146. [Google Scholar] [CrossRef]
- Brodsky, S.; Eikelboom, J.; Hebert, L.A. Anticoagulant-Related Nephropathy. J Am Soc Nephrol 2018, 29, 2787–2793. [Google Scholar] [CrossRef]
- Zakrocka, I.; Załuska, W. Anticoagulant-Related Nephropathy: Focus on Novel Agents. A Review. Adv Clin Exp Med 2022, 31, 165–173. [Google Scholar] [CrossRef]
- Moreno, J.A.; Martín-Cleary, C.; Gutiérrez, E.; Toldos, O.; Blanco-Colio, L.M.; Praga, M.; Ortiz, A.; Egido, J. AKI Associated with Macroscopic Glomerular Hematuria: Clinical and Pathophysiologic Consequences. Clin J Am Soc Nephrol 2012, 7, 175–184. [Google Scholar] [CrossRef]
- Sakaeda, T.; Tamon, A.; Kadoyama, K.; Okuno, Y. Data Mining of the Public Version of the FDA Adverse Event Reporting System. Int J Med Sci 2013, 10, 796–803. [Google Scholar] [CrossRef]
- Praga, M.; Sevillano, A.; Auñón, P.; González, E. Changes in the Aetiology, Clinical Presentation and Management of Acute Interstitial Nephritis, an Increasingly Common Cause of Acute Kidney Injury. Nephrol Dial Transplant 2015, 30, 1472–1479. [Google Scholar] [CrossRef]
- Perazella, M.A. Pharmacology behind Common Drug Nephrotoxicities. Clin J Am Soc Nephrol 2018, 13, 1897–1908. [Google Scholar] [CrossRef] [PubMed]
- Ha, J.T.; Freedman, S.B.; Kelly, D.M.; Neuen, B.L.; Perkovic, V.; Jun, M.; Badve, S.V. Kidney Function, Albuminuria, and Risk of Incident Atrial Fibrillation: A Systematic Review and Meta-Analysis. American Journal of Kidney Diseases 2024, 83, 350–359.e1. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Liao, D.; Yang, M.; Wang, S. Anticoagulant-Related Nephropathy Induced by Direct-Acting Oral Anticoagulants: Clinical Characteristics, Treatments and Outcomes. Thromb Res 2023, 222, 20–23. [Google Scholar] [CrossRef] [PubMed]
- Webster, A.C.; Nagler, E.V.; Morton, R.L.; Masson, P. Chronic Kidney Disease. Lancet 2017, 389, 1238–1252. [Google Scholar] [CrossRef]
- Gargiulo, R.; Suhail, F.; Lerma, E.V. Cardiovascular Disease and Chronic Kidney Disease. Dis Mon 2015, 61, 403–413. [Google Scholar] [CrossRef]
- Ryan, M.; Ware, K.; Qamri, Z.; Satoskar, A.; Wu, H.; Nadasdy, G.; Rovin, B.; Hebert, L.; Nadasdy, T.; Brodsky, S.V. Warfarin-Related Nephropathy Is the Tip of the Iceberg: Direct Thrombin Inhibitor Dabigatran Induces Glomerular Hemorrhage with Acute Kidney Injury in Rats. Nephrol Dial Transplant 2014, 29, 2228–2234. [Google Scholar] [CrossRef] [PubMed]
- Kubisz, P.; Stanciakova, L.; Dobrotova, M.; Samos, M.; Mokan, M.; Stasko, J. Apixaban - Metabolism, Pharmacologic Properties and Drug Interactions. Curr Drug Metab 2017, 18, 609–621. [Google Scholar] [CrossRef]
- Potpara, T.S.; Ferro, C.J.; Lip, G.Y.H. Use of Oral Anticoagulants in Patients with Atrial Fibrillation and Renal Dysfunction. Nat Rev Nephrol 2018, 14, 337–351. [Google Scholar] [CrossRef]
- Kvasnicka, T.; Malikova, I.; Zenahlikova, Z.; Kettnerova, K.; Brzezkova, R.; Zima, T.; Ulrych, J.; Briza, J.; Netuka, I.; Kvasnicka, J. Rivaroxaban - Metabolism, Pharmacologic Properties and Drug Interactions. Curr Drug Metab 2017, 18, 636–642. [Google Scholar] [CrossRef]
- Hahn, K.; Lamparter, M. Prescription of DOACs in Patients with Atrial Fibrillation at Different Stages of Renal Insufficiency. Adv Ther 2023, 40, 4264–4281. [Google Scholar] [CrossRef] [PubMed]
- Harel, Z.; McArthur, E.; Jeyakumar, N.; Sood, M.M.; Garg, A.X.; Silver, S.A.; Dorian, P.; Blum, D.; Beaubien-Souligny, W.; Yan, A.T.; et al. The Risk of Acute Kidney Injury with Oral Anticoagulants in Elderly Adults with Atrial Fibrillation. Clin J Am Soc Nephrol 2021, 16, 1470–1479. [Google Scholar] [CrossRef]
- Lau, W.C.Y.; Torre, C.O.; Man, K.K.C.; Stewart, H.M.; Seager, S.; Van Zandt, M.; Reich, C.; Li, J.; Brewster, J.; Lip, G.Y.H.; et al. Comparative Effectiveness and Safety Between Apixaban, Dabigatran, Edoxaban, and Rivaroxaban Among Patients With Atrial Fibrillation. Ann Intern Med 2022, 175, 1515–1524. [Google Scholar] [CrossRef] [PubMed]
- Gen, S.; Higashi, R.; Nagae, N.; Kigure, R.; Kamikubo, Y.; Nobe, K.; Ikeda, N. Edoxaban-Induced Acute Interstitial Nephritis. CEN Case Rep 2025, 14, 301–305. [Google Scholar] [CrossRef]
- Mezue, K.; Ram, P.; Egbuche, O.; Menezes, R.G.; Lerma, E.; Rangaswami, J. Anticoagulation-Related Nephropathy for the Internist: A Concise Review. Am J Cardiovasc Dis 2020, 10, 301–305. [Google Scholar] [PubMed]
- Shaw, D.J.; Kaiser, S.; Kong, A.; Joshi, S. An Inconspicuous Offender: Apixaban-Induced Anticoagulant-Related Nephropathy. Cureus 2023, 15, e44672. [Google Scholar] [CrossRef]
- Belčič Mikič, T.; Kojc, N.; Frelih, M.; Aleš-Rigler, A.; Večerić-Haler, Ž. Management of Anticoagulant-Related Nephropathy: A Single Center Experience. J Clin Med 2021, 10, 796. [Google Scholar] [CrossRef]
- Alshammari, T.M.; Ata, S.I.; Mahmoud, M.A.; Alhawassi, T.M.; Aljadhey, H.S. Signals of Bleeding among Direct-Acting Oral Anticoagulant Users Compared to Those among Warfarin Users: Analyses of the Post-Marketing FDA Adverse Event Reporting System (FAERS) Database, 2010–2015. Ther Clin Risk Manag 2018, 14, 803–809. [Google Scholar] [CrossRef]
- Nathan, K.T.; Conn, K.M.; van Manen, R.P.; Brown, J.E. Signal Detection for Bleeding Associated with the Use of Direct Oral Anticoagulants. Am J Health Syst Pharm 2018, 75, 973–977. [Google Scholar] [CrossRef]
- Guo, M.; Thai, S.; Zhou, J.; Wei, J.; Zhao, Y.; Xu, W.; Wang, T.; Cui, X. Evaluation of Rivaroxaban-, Apixaban- and Dabigatran-Associated Hemorrhagic Events Using the FDA-Adverse Event Reporting System (FAERS) Database. Int J Clin Pharm 2021, 43, 1508–1515. [Google Scholar] [CrossRef]
- Maini, R.; Wong, D.B.; Addison, D.; Chiang, E.; Weisbord, S.D.; Jneid, H. Persistent Underrepresentation of Kidney Disease in Randomized, Controlled Trials of Cardiovascular Disease in the Contemporary Era. J Am Soc Nephrol 2018, 29, 2782–2786. [Google Scholar] [CrossRef] [PubMed]
- Konstantinidis, I.; Patel, S.; Camargo, M.; Patel, A.; Poojary, P.; Coca, S.G.; Nadkarni, G.N. Representation and Reporting of Kidney Disease in Cerebrovascular Disease: A Systematic Review of Randomized Controlled Trials. PLoS One 2017, 12, e0176145. [Google Scholar] [CrossRef] [PubMed]
- Konstantinidis, I.; Nadkarni, G.N.; Yacoub, R.; Saha, A.; Simoes, P.; Parikh, C.R.; Coca, S.G. Representation of Patients With Kidney Disease in Trials of Cardiovascular Interventions: An Updated Systematic Review. JAMA Intern Med 2016, 176, 121–124. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow diagram depicting the selection process for anticoagulant-related AKI and AKI with bleeding cases.
Figure 1.
Flow diagram depicting the selection process for anticoagulant-related AKI and AKI with bleeding cases.
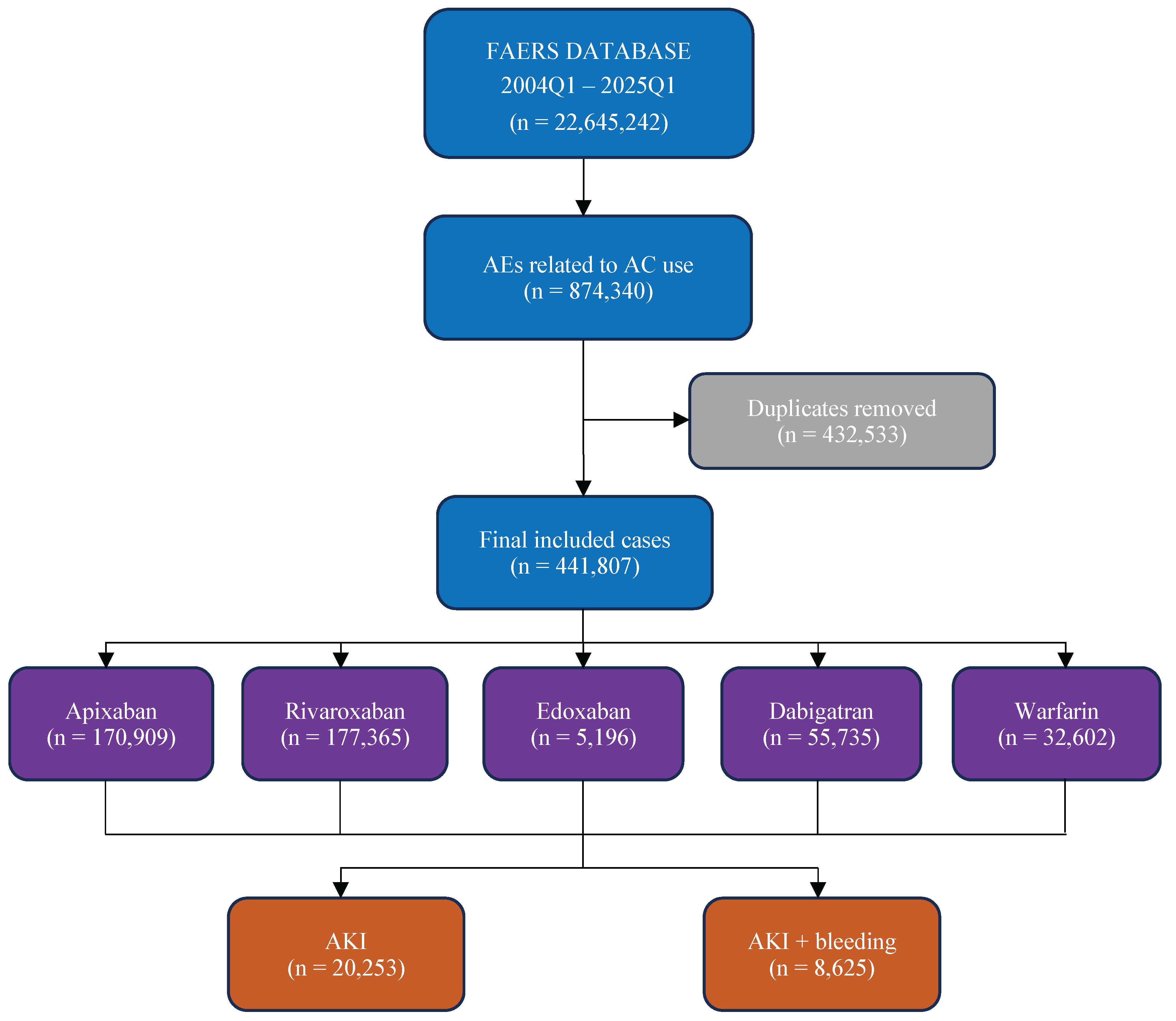

Table 1.
Demographic data of anticoagulant-related acute kidney injury cases.
| Apixaban | Rivaroxaban | Edoxaban | Dabigatran | Warfarin | Total | |
| Number of Cases | 6581 (32.5) | 7977 (39.4) | 569 (2.8) | 3453 (17.0) | 1673 (8.3) | 20253 |
| Mean age ± SD | 72.6 ± 16.4 | 72.5 ± 12.3 | 76.3 ± 17.7 | 75.4 ± 11.8 | 70.6 ± 14.4 | 72.9 ± 14.1 |
| Gender | ||||||
| Male | 2937 (44.6) | 283 (3.6) | 245 (43.1) | 500 (14.5) | 103 (6.2) | 4068 (20.1) |
| Female | 2896 (44.0) | 253 (3.2) | 209 (36.7) | 451 (13.1) | 67 (4.0) | 3876 (19.1) |
| Unknown | 748 (11.3) | 7441 (93.3) | 115 (20.2) | 2502 (72.5) | 1503 (89.8) | 12309 (60.8) |
| Countries | ||||||
| United States | 1927 (29.3) | 5103 (64.1) | 6 (1.0) | 1361 (39.4) | 493 (29.6) | 8890 (43.9) |
| Japan | 827 (12.6) | 288 (3.6) | 185 (32.5) | 25 (0.7) | 129 (7.7) | 1454 (7.2) |
| France | 821 (12.5) | 539 (6.8) | 0 (0) | 248 (7.2) | 68 (4.1) | 1676 (8.3) |
| Canada | 770 (11.7) | 140 (1.8) | 4 (0.7) | 78 (2.6) | 72 (4.3) | 1064 (5.3) |
| Germany | 630 (9.6) | 409 (5.1) | 155 (27.2) | 195 (5.6) | 17 (1.0) | 1406 (6.9) |
| Indications | ||||||
| Cerebrovascular accident prophylaxis | 1719 (26.1) | 1598 (20.1) | 1 (0.2) | 243 (7.0) | 36 (2.2) | 3597 (17.8) |
| Atrial fibrillation | 370 (5.6) | 1854 (23.3) | 184 (32.3) | 1653 (47.9) | 254 (15.2) | 4315 (21.3) |
| Deep vein thrombosis | 156 (2.4) | 722 (9.1) | 18 (3.2) | 29 (0.8) | 76 (4.6) | 1001 (4.9) |
| Thrombosis prophylaxis | 148 (2.2) | 916 (11.5) | 75 (13.2) | 64 (1.9) | 66 (4.0) | 1269 (6.3) |
| Pulmonary embolism | 141 (2.1) | 366 (4.6) | 14 (2.5) | 34 (1.0) | 69 (4.1) | 624 (3.1) |
| Years | ||||||
| 2015 | 260 (4.0) | 607 (7.6) | 0 (0) | 207 (6.0) | 133 (8.0) | 1207 (6.0) |
| 2016 | 348 (5.3) | 1452 (18.2) | 5 (0.9) | 228 (6.6) | 121 (7.3) | 2154 (10.6) |
| 2017 | 437 (6.6) | 1040 (13.1) | 7 (1.2) | 343 (9.9) | 126 (7.6) | 1953 (9.6) |
| 2018 | 609 (9.3) | 1144 (14.4) | 15 (2.6) | 322 (9.3) | 249 (14.9) | 2339 (11.5) |
| 2019 | 758 (11.5) | 591 (7.4) | 14 (2.5) | 285 (8.3) | 207 (12.4) | 1855 (9.2) |
| 2020 | 750 (11.4) | 1397 (17.5) | 27 (4.7) | 203 (5.9) | 186 (11.2) | 2563 (12.7) |
| 2021 | 849 (12.9) | 259 (3.3) | 42 (7.4) | 110 (3.2) | 132 (7.9) | 1392 (6.9) |
| 2022 | 1034 (15.7) | 299 (3.8) | 151 (26.5) | 102 (3.0) | 127 (7.6) | 1713 (8.5) |
| 2023 | 639 (9.7) | 208 (2.6) | 134 (23.6) | 70 (2.0) | 75 (4.5) | 1126 (5.6) |
| 2024 | 604 (9.2) | 193 (2.4) | 148 (26.0) | 46 (1.3) | 61 (3.7) | 1052 (5.2) |
| Outcomes | ||||||
| Other outcomes | 3535 (53.7) | 1934 (24.2) | 271 (47.6) | 794 (23.0) | 591 (35.3) | 7125 (35.2) |
| Hospitalized | 2153 (32.7) | 4574 (57.3) | 240 (42.2) | 1780 (51.5) | 753 (45.0) | 9500 (46.9) |
| Died | 398 (6.0) | 1008 (12.6) | 39 (6.9) | 419 (12.1) | 177 (10.6) | 2041 (10.1) |
| Life-threatening | 216 (3.3) | 295 (3.7) | 8 (1.4) | 170 (4.9) | 70 (4.2) | 759 (3.7) |
| Disabled | 44 (0.7) | 31 (0.4) | 9 (1.6) | 44 (1.3) | 24 (1.4) | 152 (0.7) |
| Seriousness | ||||||
| Serious | 6347 (96.4) | 7842 (98.3) | 567 (99.6) | 3207 (92.9) | 1619 (96.8) | 19582 (96.7) |
| Non-Serious | 234 (3.6) | 135 (1.7) | 2 (0.4) | 246 (7.1) | 54 (3.2) | 671 (3.3) |
Table 2.
Demographic data of anticoagulant-related acute kidney injury cases with co-occurrence of bleeding.
Table 2.
Demographic data of anticoagulant-related acute kidney injury cases with co-occurrence of bleeding.
| Apixaban | Rivaroxaban | Edoxaban | Dabigatran | Warfarin | Total | |
| Number of Cases | 1359 (15.8) | 4243 (49.2) | 156 (1.8) | 1934 (22.4) | 933 (10.8) | 8625 |
| Mean age ± SD | 69.8 ± 19.5 | 72.4 ± 11.9 | 77.3 ± 16.9 | 75.1 ± 11.8 | 71.3 ± 13.4 | 72.5 ± 13.7 |
| Gender | ||||||
| Male | 659 (48.5) | 114 (2.7) | 73 (46.8) | 315 (16.3) | 71 (7.6) | 1232 (14.3) |
| Female | 573 (42.2) | 79 (1.9) | 55 (35.3) | 278 (14.4) | 39 (4.2) | 1024 (11.9) |
| Unknown | 127 (9.3) | 4050 (95.4) | 28 (17.9) | 1341 (69.3) | 823 (88.2) | 6369 (73.8) |
| Countries | ||||||
| United States | 361 (26.6) | 3530 (83.3) | 6 (3.8) | 956 (49.4) | 262 (28.1) | 5115 (59.3) |
| Japan | 113 (8.3) | 44 (1.0) | 31 (19.9) | 9 (0.5) | 56 (6.0) | 253 (2.9) |
| France | 106 (7.8) | 105 (2.5) | 0 (0.0) | 91 (4.7) | 15 (1.6) | 317 (3.7) |
| Canada | 175 (12.9) | 55 (1.3) | 1 (0.6) | 40 (2.1) | 36 (3.9) | 307 (3.6) |
| Germany | 193 (14.2) | 106 (2.5) | 61 (39.1) | 110 (5.7) | 5 (0.5) | 475 (5.5) |
| Indications | ||||||
| Cerebrovascular accident prophylaxis | 345 (25.4) | 943 (22.2) | 0 (0.0) | 126 (6.5) | 18 (19) | 1432 (16.6) |
| Atrial fibrillation | 117 (8.6) | 1064 (25.1) | 40 (25.6) | 996 (51.5) | 150 (16.1) | 2367 (27.4) |
| Deep vein thrombosis | 55 (4.0) | 501 (11.8) | 7 (4.5) | 17 (0.9) | 51 (5.5) | 631 (7.3) |
| Thrombosis prophylaxis | 85 (6.2) | 625 (14.7) | 11 (7.0) | 31 (1.6) | 40 (4.3) | 792 (9.2) |
| Pulmonary embolism | 38 (2.8) | 226 (5.3) | 6 (3.8%) | 16 (0.8) | 35 (3.7) | 321 (3.7) |
| Years | ||||||
| 2015 | 50 (3.7) | 306 (7.2) | 0 (0.0) | 83 (4.3) | 59 (6.3) | 498 (5.8) |
| 2016 | 89 (6.5) | 972 (22.9) | 3 (1.9) | 104 (5.4) | 77 (8.3) | 1245 (14.4) |
| 2017 | 118 (8.7) | 641 (15.1) | 4 (2.6) | 178 (9.2) | 71 (7.6) | 1012 (11.7) |
| 2018 | 152 (11.2) | 639 (15.1) | 8 (5.1) | 185 (9.6) | 136 (14.6) | 1120 (13.0) |
| 2019 | 158 (11.6) | 296 (6.9) | 4 (2.6) | 157 (8.1) | 129 (13.9) | 744 (8.6) |
| 2020 | 145 (10.7) | 895 (21.1) | 6 (3.8) | 103 (5.3) | 101 (10.8) | 1250 (14.5) |
| 2021 | 97 (7.1) | 105 (2.5) | 19 (12.2) | 47 (2.4) | 71 (7.6) | 339 (3.9) |
| 2022 | 206 (15.2) | 58 (1.4) | 46 (29.5) | 32 (1.7) | 81 (8.7) | 423 (4.9) |
| 2023 | 144 (10.6) | 55 (1.3) | 21 (13.5) | 30 (1.6) | 34 (3.7) | 284 (3.3) |
| 2024 | 128 (9.4) | 24 (0.6) | 34 (21.8) | 9 (0.5) | 16 (1.7) | 211 (2.4) |
| Outcomes | ||||||
| Other outcomes | 557 (41.0) | 565 (13.3) | 51 (32.7) | 381 (19.7) | 276 (29.6) | 1830 (21.2) |
| Hospitalized | 599 (44.1) | 2835 (66.8) | 79 (50.6) | 1090 (56.4) | 460 (49.3) | 5063 (58.7) |
| Died | 114 (8.4) | 657 (15.5) | 20 (12.8) | 262 (13.5) | 122 (13.1) | 1175 (13.6) |
| Life-threatening | 60 (4.4) | 141 (3.3) | 3 (1.9) | 101 (5.2) | 30 (3.2) | 335 (3.9) |
| Disabled | 6 (0.4) | 9 (0.2) | 2 (1.3) | 11 (0.6) | 13 (1.4) | 41 (0.5) |
| Seriousness | ||||||
| Serious | 1336 (98.3) | 4207 (99.2) | 155 (99.4) | 1845 (95.4) | 901 (96.6) | 8444 (97.9) |
| Non-Serious | 23 (1.7) | 36 (0.8) | 1 (0.6) | 89 (4.6) | 32 (3.4) | 181 (2.1) |
Table 3.
Disproportionality analysis of anticoagulant-related acute kidney injury cases.
| Drug | Cases | ROR | PPR | Chi Square | p value | IC |
| Apixaban | 6581 | 0.76 (0.73-0.78) | 0.77 (0.74-0.79) | 329.24 | <0.001 | -0.38 (-0.42- -0.34) |
| Rivaroxaban | 7977 | 0.97 (0.95-1.00) | 0.97 (0.95-1.00) | 3.31 | 0.069 | -0.02 (-0.05-0.00) |
| Edoxaban | 569 | 2.63 (2.40-2.87) | 2.45 (2.26-2.65) | 494.57 | <0.001 | 1.27 (1.18-1.35) |
| Dabigatran | 3453 | 1.46 (1.41-1.52) | 1.43 (1.38-1.49) | 392.65 | <0.001 | 0.44 (0.41-0.48) |
| Warfarin | 1673 | 1.14 (1.08-1.20) | 1.13 (1.08-1.19) | 25.27 | <0.001 | 0.17 (0.12-0.22) |
Abbreviations: ROR – reporting odds ratio; PPR – proportional odds ratio; IC – information component.
Table 4.
Disproportionality analysis of anticoagulant-related acute kidney injury cases with co-occurrence of bleeding.
Table 4.
Disproportionality analysis of anticoagulant-related acute kidney injury cases with co-occurrence of bleeding.
| Drug | Cases | ROR | PPR | Chi Square | p value | IC |
| Apixaban | 1359 | 0.29 (0.28-0.31) | 0.30 (0.28-0.32) | 1926.26 | <0.001 | -1.29 (-1.34- -1.23) |
| Rivaroxaban | 4243 | 1.47 (1.41-1.54) | 1.46 (1.40-1.53) | 319.14 | <0.001 | 0.30 (0.27-0.34) |
| Edoxaban | 156 | 1.59 (1.35-1.86) | 1.57 (1.34-1.83) | 31.60 | <0.001 | 0.64 (0.48-0.80) |
| Dabigatran | 1934 | 2.07 (1.96-2.18) | 2.03 (1.93-2.13) | 793.86 | <0.001 | 0.84 (0.79-0.89) |
| Warfarin | 933 | 1.55 (1.44-1.66) | 1.53 (1.43-1.64) | 156.02 | <0.001 | 0.56 (0.49-0.63) |
Abbreviations: ROR – reporting odds ratio; PPR – proportional odds ratio; IC – information component.
Table 5.
Disproportionality analysis of anticoagulant-related acute kidney injury cases with concomitant use of Aspirin.
Table 5.
Disproportionality analysis of anticoagulant-related acute kidney injury cases with concomitant use of Aspirin.
| Drug | Cases | ROR | PPR | Chi Square | p value | IC |
| Apixaban | 26 | 0.86 (0.55-1.32) | 0.86 (0.56-1.32) | 0.35 | 0.554 | -0.17 (-0.60-0.26) |
| Rivaroxaban | 69 | 2.25 (1.58-3.22) | 2.21 (1.56-3.13) | 20.12 | <0.001 | 0.63 (0.33-0.92) |
| Edoxaban | 1 | 0.57 (0.08-4.15) | 0.58 (0.08-4.08) | 0.03 | 0.864 | -0.78 (-2.76-1.2) |
| Dabigatran | 20 | 0.59 (0.37-0.96) | 0.6 (0.37-0.96) | 4.15 | 0.042 | -0.59 (-1.07- -0.12) |
| Warfarin | 9 | 0.42 (0.21-0.84) | 0.43 (0.22-0.84) | 5.87 | 0.015 | -1.09 (-1.77- -0.41) |
Abbreviations: ROR – reporting odds ratio; PPR – proportional odds ratio; IC – information component.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



