Submitted:
02 July 2024
Posted:
04 July 2024
Read the latest preprint version here
Abstract
Background/Objectives: Thoracic aortic aneurysms (TAAs) pose critical health risks, often asymptomatic until a rupture or dissection occurs. Current guidelines recommend surgical repair based on specific aortic diameters and risk factors, emphasizing the importance of early detection and intervention. Despite established clinical risk factors for early detection in TAAs, the influence of racial and ethnic disparities on TAAs remains underexplored. This study aims to provide a comprehensive summary of existing research on racial and ethnic disparities in the presentation and outcomes of TAAs. Methods: This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, with the objective of exploring racial and ethnic differences in the presentation and surgical outcomes of patients with TAAs. Results: The findings demonstrated that black patients were younger at presentation and had a higher incidence of ruptured TAAs than non-black patients. Furthermore, compared to non-black patients, black patients had higher rates of cardiac arrhythmia and COPD, as well as comorbidities such as diabetes, hypertension, and renal insufficiency. For black patients undergoing open surgery, the surgical results showed improved 5-year survival rates after repair but higher perioperative mortality rates. All-cause or in-hospital mortality did not significantly differ between the racial groups, according to four studies. Discussion: This review highlights significant racial and ethnic disparities in TAA presentation and outcomes, underscoring the need for personalized risk stratification models. Standardized racial and ethnic definitions are essential for consistent and reliable research. Future studies should focus on refining risk assessment models to enhance diagnostic and therapeutic strategies, ultimately improving patient outcomes across diverse populations.
Keywords:
Thoracic Aortic Aneurysms
1. Introduction
Thoracic aortic diseases encompass a wide spectrum of conditions, with thoracic aortic aneurysms (TAA) and dissections being the most critical1. TAAs often remain asymptomatic until a catastrophic event such as a dissection or rupture occurs, with mortality rates exceeding 90% without intervention2. Hence, early detection and appropriate (surgical) intervention are imperative. Current American and European aortic guidelines recommend surgical repair of the aortic wall in patients with an ascending aorta diameter ≥ 5.5 cm, with a lower threshold of 5.0 cm advised in the presence of risk factors4,5.
Although the exact pathogenesis of TAA is not yet fully understood, several pathological mechanisms such as abnormalities in smooth muscle cell function and differentiation, influenced by their embryonic origins, have been described 6-8. Clinical risk factors have also been explored in the development of TAAs. While sex-specific variations in TAAs have been clearly documented2,3,8, the influence of ethnic and racial disparities on TAAs remains underexplored partly due to significant heterogeneity in defining race and ethnicity worldwide. The impact of these disparities on the diagnosis and management of TAAs is crucial for accurate assessment of individual risk levels for a tailored approach. Improved personalized risk stratification is imperative to optimize diagnostic and therapeutic strategies for TAAs among diverse ethnic groups and to improve patient outcomes. Therefore, this study aims to provide a comprehensive summary of current research on racial and ethnic disparities in TAAs.
2. Materials and Methods
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, with the objective of exploring racial and ethnic differences in the presentation and surgical outcomes of patients with TAAs10.
Search Strategy
A comprehensive systematic literature search was performed in PubMed to identify relevant studies published up to December 31st, 2023. Controlled search terms were utilized, focusing on two primary domains and encompassing all synonyms of the core terms: “aortic aneurysm” and “ethnicity”. Additionally, the reference lists of included articles were meticulously cross-checked to ensure no relevant literature was overlooked. For the complete search strategy see Table I.
Study Selection
Eligibility Criteria
Inclusion criteria were defined to encompass any empirical study involving patients with TAA that reported on at least two ethnic groups. Studies were included if they provided predictive values or outcomes such as mortality, readmission rates, or survival rates.
Due to the significant variability in the definition of race or ethnicity and the absence of universally accepted standards to for defining ethnic groups, our analyses primarily focused on the comparison of black and non-black individuals.
Exclusion criteria included review articles, case reports (or studies with a population of fewer than 15), meta-analysis, conference abstracts only published in abstract form, studies published languages other than English, and studies published prior to 2000.
Screening and Data Extraction
Title and abstract screening were performed by one author (N.B.) to identify potentially relevant articles. Full texts of eligible studies were then assessed according to the predetermined criteria. Data extraction was carried out using a standardized form, which captured information on study population, design, clinical presentation, and surgical outcomes. Separate columns were included for documenting clinical presentation and surgical outcomes for black and non-black patients (see Table II).
3. Results
3.1. Study Selection and Characteristics
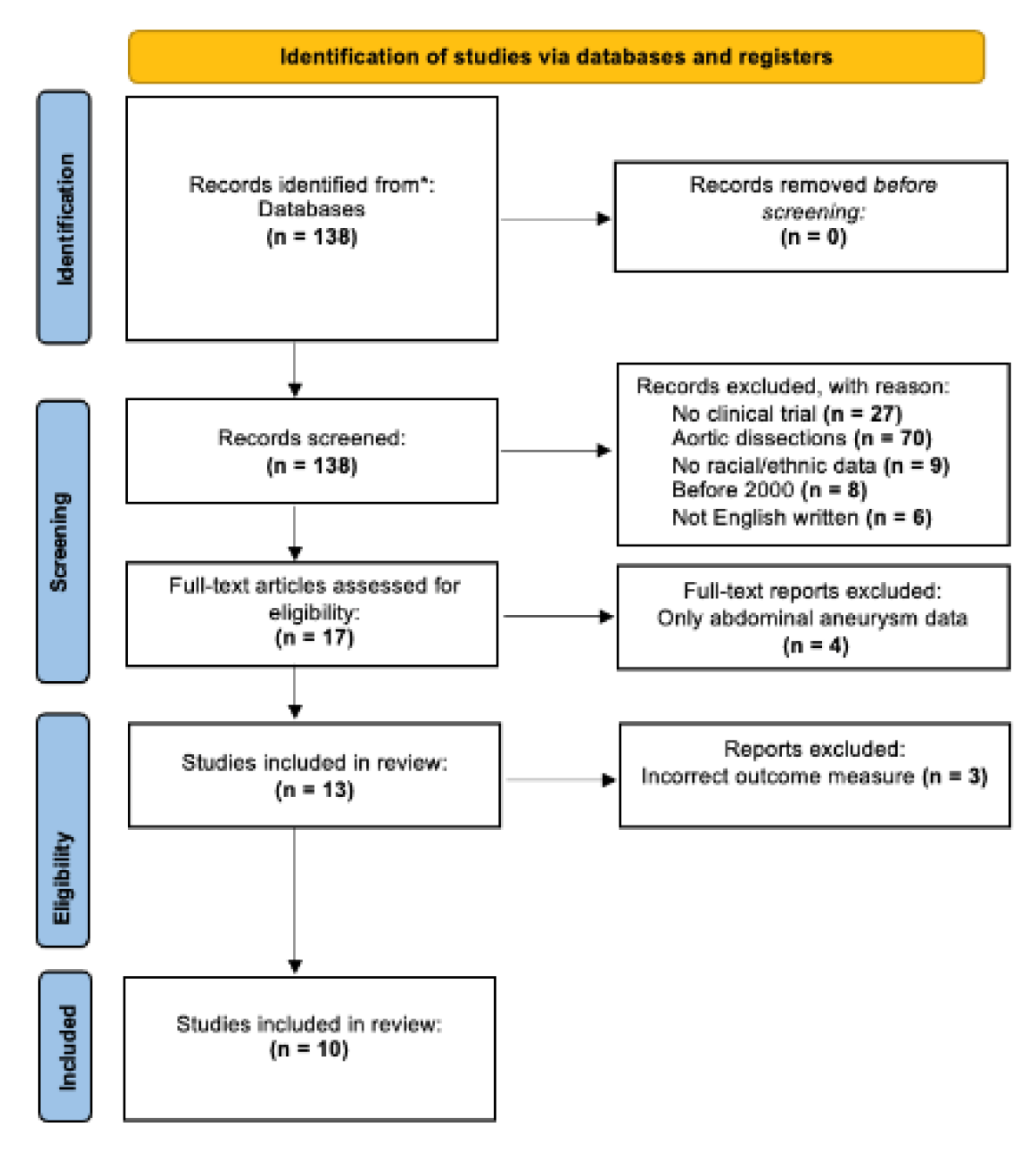
A systematic review of the literature identified 138 unique records. Following title and abstract screening, 121 studies were excluded for not meeting the inclusion criteria, leaving 17 for full-text review. Of these, 4 focused on abdominal aneurysms (AAA) and 3 did not report on relevant outcomes, resulting in 10 studies being included in the final analysis 11-20. See Figure 1 for the PRISMA flow diagram.
3.2. Baseline Characteristics
The included studies encompassed a total of 283,076 patients from diverse ethnic backgrounds, revealing significant variability in incidence and clinical presentation of TAA.
Black patients showed higher incidence of ruptured thoracic aortic aneurysms in black patients compared to non-black patients (7.3% vs. 4.4%; P=0.001)11 among 15,305 patients undergoing TAA repair. Non-black patients tended to present at an older age compared to black patients (74.5 vs. 73.7 years; P=0.001)23, a finding corroborated two other studies14,19.
Black patients also exhibited higher Charlson comorbidity scores (1.51 vs. 0.92; P=0.001)11, with higher rates of renal insufficiency (35.4% vs. 17.8%; P=0.001)19, hypertension (100% vs. 86.5%; P=0.034)19, and diabetes mellitus (18.8% vs. 4.5%; P=0.021)19, while non-black patients had higher rates of COPD (20.1% vs. 6.3%; P=0.003)19 and cardiac arrhythmia (20.6% vs. 10.1%; P=0.037)19.Two other studies supported these findings13,18.
Non-black patients had larger aortic necks (28.2 mm vs. 23.8 mm; P=0.01)18 and a higher prevalence of females with TAA (33.8% vs. 19.3%; P=0.02)18. Conversely, two other studies reported a higher prevalence of females among black patients14,20.
Murphy et al.16 noted that non-black patients had a higher proportion of elective surgeries (48%; P=<0.001), whereas black patients had a higher proportion of emergency surgeries (20%; P=<0.001). These findings were confirmed by the study of Yin et al.12.
3.3. Surgical Outcome
Goodney et al.11 reported on higher perioperative mortality rates when undergoing open surgery (14.4% vs. 6.8%; P<0.001) in black patients compared to non-black patients, with black ethnicity being a significant risk factor (OR: 2.0; 95% CI 1.5-2.5). However, black patients demonstrated better 5-year survival rates post-open repair (71% vs. 61%; P<0.001).
Overall mortality in black patients was higher (13.7% vs. 9.8%; P=<0.001)16 and significant racial differences in in-hospital mortality were found (P<0.0001)14. In line with these results, ribieras and colleagues reported on higher complication rates (34.3% vs. 17.4%; P=0.014) and conversion rates to open repair (2.9% vs. 0%; P=0.011) in black patients compared to non-black patients.
No significant differences in all-cause or in-hospital mortality between black and non-black patients were found in four studies13,18-20. Although the study by Yin et al.12 found no significant cause in overall 30-day mortality rate, after adjustment for demographics, comorbidities, and operative factors, black race was independently associated with a 56% lower 30-day mortality rate after thoracic endovascular aortic repair (TEVAR) (OR: 0.44; 95% CI 0.22-0.85; P=0.01). Johnston et al.15 also reported varied odds ratios for TEVAR performance across ethnic groups as outlined in Table II. Lastly, Vervoort et al. 18 showed a lower reintervention hazard ratio in black patients compared to white patients (HR: 0.7; P=0.01)18.
3.4. Figures, Tables and Schemes
Figure 1.
Flowchart of selected articles according to the PRISMA statement.
4. Discussion
This review aimed to summarize current research on racial and ethnic disparities in the presentation and outcomes of TAAs in order to aid in the development of personalized risk stratification methods. Analysis of ten empirical studies focusing on the dichotomy between black and non-black individuals revealed that black patients with TAA more commonly exhibit comorbidities such as diabetes, heart failure, and renal insufficiency, whereas non-black patients often present with COPD, coronary artery disease, and cardiac arrhythmias. Black individuals tend to present at a younger age and face a nearly doubled risk of ruptured TAA at presentation compared to non-black individuals. Despite these differences, four studies found no significant disparity between the racial groups 13,18-20. Our findings align with existing literature on abdominal aortic aneurysms and aortic dissections,21-24 suggesting potential consistencies in racial impacts across various aortic conditions.
However, lack of standardization in defining race and ethnicity among studies pose considerable challenges. There is a need for consensus on these definitions to improve the reliability of research findings. Future research should address these inconsistencies and develop tailored risk assessment models that consider disparities in comorbidities between racial groups. A personalized risk stratification model could enhance the precision in predicting outcomes and improve preventive and therapeutic strategies for patients with TAA.
A reasonable suggestion would be to adopt standardized racial and ethnic categories, such as those defined by the National Institutes of Health (NIH)25. These categories include American Indian or Alaska Native, Asian, Black or African American, Hispanic or Latino, Native Hawaiian or Other Pacific Islander, and White. The classification should prioritize self-reporting by individuals rather than assignment by observers, aligning with recommendations from recent research26. This approach would facilitate consistency in defining and analysing racial disparities in the presentation and outcomes of thoracic aortic aneurysms (TAA), thereby enhancing the validity and comparability of research findings across studies.
In conclusion, this review demonstrates significant differences in the presentation and surgical outcomes of TAA between racial and ethnic groups. Recognizing these differences is essential for developing tailored interventions and improving outcomes for all patients, regardless of race or ethnicity. Further research is needed to uncover the underlying cause of these disparities and to refine risk stratification models accordingly.
Funding
This research received no external funding
Informed Consent Statement
Not applicable.
Acknowledgments
In this section, you can acknowledge any support given which is not covered by the author contribution or funding sections. This may include administrative and technical support, or donations in kind (e.g., materials used for experiments).
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A

Table 1.
Search strategy: PubMed.
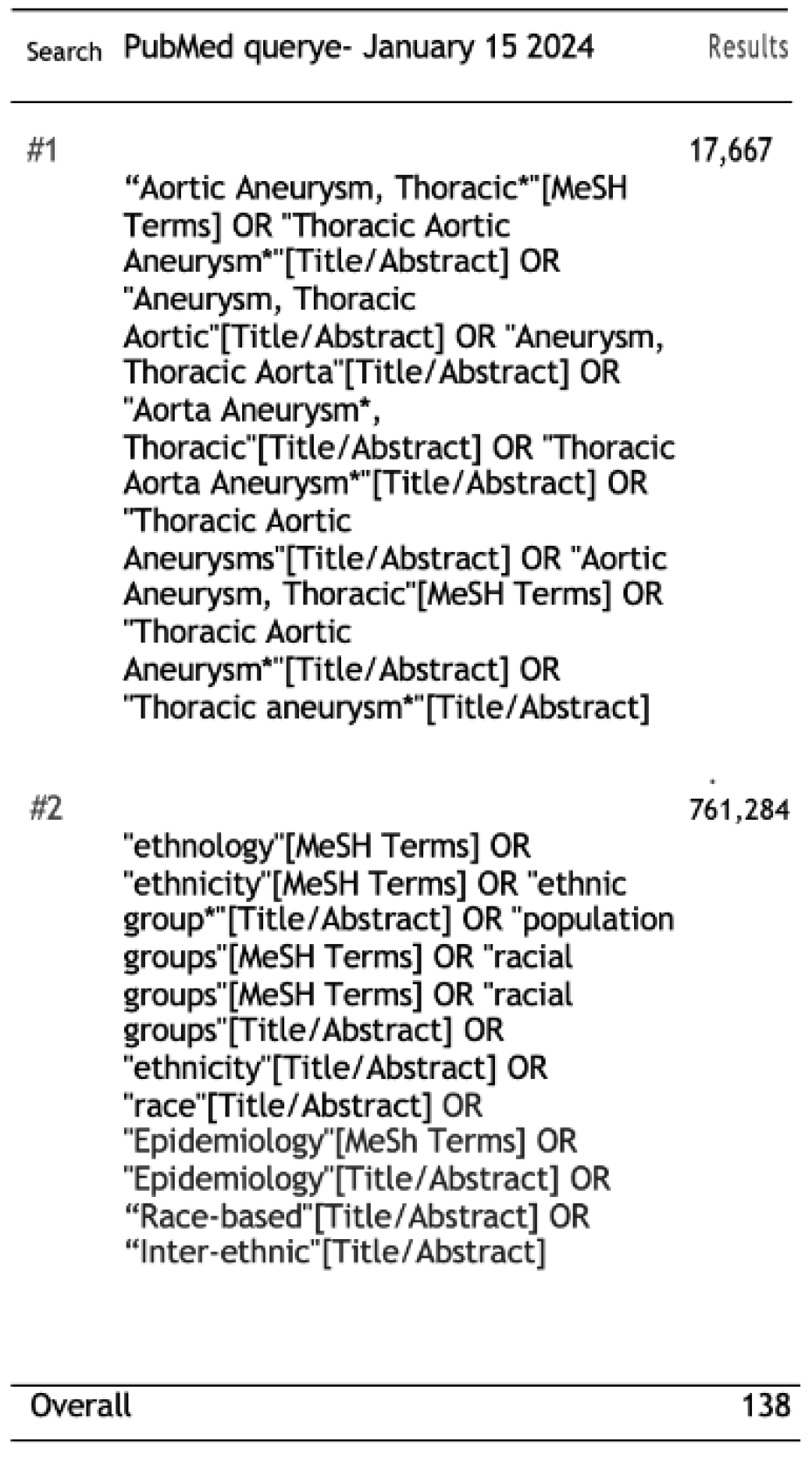
Table 2.
Description of the ten included articles and their characteristics.
| First Author (Year) | Study Type (Method) | Study Population (s) (Controls and Patients) |
Clinical Presentation | Surgical Outcome | ||
|---|---|---|---|---|---|---|
| Non-Black | Black | Non-Black | Black | |||
| Goodney9 (2013) | Retrospective cohort study Intervention: Thoracic aneurysm repair Control: Mortality Data source: Medicare claims (1999-2007) |
N=722 black patients N= 14,583 non-black patients (97% White, 1.0% Native American, 0.9% Hispanic, 0.9% Asian American, 0.1% Pacific Islander, 0.1 % missing) |
Older presentation (74.5 vs 73,7; P=0 .001) 4,4% ruptured TAA. (7.3% vs 4.4%; P=0.001) Non-black patients had a higher ratio of men (56,4% vs. 43,4%; p=0,02) |
Younger presentation (74.5 vs 73.7; P= 0.001) 7,3% ruptured TAA (7.3% vs 4.4%; P=0.001) Black patients had a higher Charlson comorbidity score (1,51 vs 0,92; p=0,001) Black patients had a higher prevalence of diabetes, heart failure, renal failure and history of malignancy (p=0.001) |
Open surgical repair: lower perioperative mortality 6.8% non-black; P < 0.001. 5-year survival: 61% P < 0.001. |
Open surgical repair: higher perioperative mortality 14.4% black; P < 0.001. Operative mortality: OR 2.0; 95% CI 1.5-2.5; P < 0.0001. 5-year survival: 71%; P < 0.001. |
| Yin10 (2021) | Retrospective cohort study Intervention: Thoracic endovascular aneurysm repair Control: 30-day mortality Data source: VQI national data registry |
N= 684 black patients N= 2021 non-black patients (100% white) |
1488 aneurysms (73,6%) | More likely to undergo emergent TEVAR (27.6% vs. 19.8%; P < 0.001). More likely symptomatic (52.3% vs. 36.4%; P < 0.001). More likely to receive blood transfusion (32.1% vs. 23.6%; P < 0.001). |
30-Day Mortality: No significant difference in 30day mortality: (3.4% vs 4.9%; P =0.1) |
30-Day Mortality: Following correction for operative variables, comorbidities, and demographics: black race was independently associated with 56% decrease in risk after Tevar (OR 0.44; 95% CI 0.22-0.85; P = 0.01). Postoperative Complications: No independent association (OR 0.90; 95% CI 0.68-1.17; P = 0.42). 1-year overall survival: log-rank P= 0.024 1-year mortality Hr:0.65; 95% CI, 0.47-0.91; P=0.01 |
| Diaz-Castrillon11 (2022) | Retrospective cohort study Intervention: Thoracic endovascular aneurysm repair Control: In-hospital mortality Data source: Nationwide inpatient sample (NIS) 2010-2017 |
N= 4,959 black N=20,301 non-black (68,1% white, 5,7% Hispanic, 6,5% others) |
CAD more prevalent (34.6% (white) vs. 24.1% (black) vs. 26.8% (Hispanic) vs. 24.7% (others); p < .001). COPD more prevalent (28.7% vs. 15.6% vs. 15.1% vs. 16.5%; p < .001). TEVAR often times elective (58.8% vs. 34% vs. 48.3% vs. 48.2%; p < .001). |
Hypertension more frequent as a comorbidity (92% (black) vs. 83%(white) vs. 85% (Hispanic) vs. 84% (others); p < .001) | Racial disparities do not appear to be associated with in-hospital mortality. | Racial disparities do not appear to be associated with in-hospital mortality. |
| Tanious12 (2019) | Retrospective cohort study Intervention: Thoracic endovascular aneurysm repair Control: In-hospital mortality Data source: Florida State Agency for Health Care Administration 2000-2014 |
N= 1,630 black N= 34,119 non-black (47.7% White, 46.0% Hispanic,1.8%) other.) |
Older presentation 67,42 (black) vs. 73.87 (white) vs. 73,52 (Hispanic) vs. 72,06 (other); P< 0.001 |
Higher prevalence of women 31,5% (black) vs. 16,1 (white) vs. 20,2 (Hispanic) vs. 21,8 (other); P< 0.001 |
Chance of in-hospital mortality: 2,5% (white), 2,8% (Hispanic), 5,1% (other); p<0,0001 |
Chance of in-hospital mortality: 4,0%; P<0,0001 |
| Johnston13 (2013) | Retrospective cohort study Intervention: Thoracic endovascular aneurysm repair Control: TEVAR performance based on race Data source: Nationwide inpatient sample (NIS) 2005-2008 |
N= 4,108 black N = 41,122 non-black (86% white, 6,2% Hispanic, 3,2% Asian or Pacific Islander, 0,8% Native American, 3,7% other) |
NA | 28.6% of black patients received TEVAR, whereas only 19.5% of white patients were treated with TEVAR (P < .001) |
TEVAR performance: Odds ratio: Native American: 2.37 Black: 1.71 Hispanic: 1.70 Asian or Pacific Islander: 1.34 Other: 0.98 White (reference): 1 |
Tevar performance: Odds: Black: 1.71 |
| Murphy14 (2013) | Retrospective cohort study Intervention: Thoracic endovascular aneurysm repair Control: mortality Data source: Nationwide inpatient sample (NIS) 2001-2005 |
N=819 black N= 9,738 non-black (88% white, 5,7% Hispanic, 6,8 other) |
High prevalence for elective surgery: 48%; P < 0,001 |
High prevalence for emergency surgery: 20%; P < 0,001 |
Mortality rate: 9,8%; P < 0,001 | Mortality rate: 13,7%; P < 0,001 |
| Abdulameer15 (2019) | Retrospective cohort study Intervention: Thoracic aneurysm rupture Control: Mortality per million Data source: U.S. National Vital Statistics System 1999-2016 |
N=104,458 total ruptures | NA | NA | Mortality/ million White female: 3,5 White men: 3,3 Asian men: 1,5 Asian women: 2,5 (P<0,001) |
Mortality/ million Black female: 2.3 Black men: 2,6 (P<0,001) |
| Vervoort16 (2021) | Retrospective cohort study Intervention: Elective thoracic endovascular aneurysm repair Control: Reintervention and surgical outcome Data source: Vascular Quality Initiative 2009-2018 |
N= 2,140 black N= 40,431 Non-black (100% white) |
Female sex 33,8% (23), p=0.02 Aortic neck in mm 28,2+/-15,8 p=0,01 CHF: 6,0 (4) p=0,01 Smoking history: 89,7 (61) p < 0,01 |
Female sex 19,3% (212), p=0.02 Aortic neck in mm 23,8+/-5,25 p=0,01 CHF: 13,0 (143) p=0,01 Smoking history: 83,1 (911) p < 0,01 |
All-cause mortality: similar between groups (log-rank P = 0.25) Reintervention: White race statistically associated with reintervention; P = 0.01 |
All-cause mortality: similar between groups (log-rank P = 0.25) Reintervention: hr: 0,7; p=0,01 |
| Ribieras17 (2023) | Retrospective cohort study Intervention: thoracic endovascular aneurysm repair Control: All-couse mortality Data source: Global Registry for Endovascular Aortic Treatment (GREAT) 2010-2016 |
N= 79 black N=359 non-black |
Chronic obstructive pulmonary disease: Black 6.3% vs White 20.1%; P = 0.003 Cardiac arrhythmia: Black 10.1% vs White 20.6%; P = 0.037 |
Younger presentation: 62 years vs 67 years); P < 0.001. Higher BMI 31.0 kg/m2 vs 27.5 kg/m2); P < 0.001. Renal insufficiency: 35.4% vs 17.8%; P = 0.001. Higher incidence of erectile dysfunction in black patients 6.3% vs 2.0%; P = 0.047. Higher incidence of hypertension: common in black patients (100% vs 86.5%; P = 0.034). Higher prevalence of diabetes mellitus: 18.8% vs 4.5%; P = 0.021. |
All-cause mortality: no significant difference |
Complications: 34.3% vs 17.4%; P = 0.014 Conversion to open repair: 2.9% vs 0%; P = 0.011 Type II endoleaks: 5.7% vs 1.0%; P = 0.040 All-cause mortality: no significant difference |
| Murphy18 (2010) | Retrospective cohort study Intervention: Thoracic aneurysm rupture Control: Mortality Data source: U.S. National Vital Statistics System 2001-2005 |
N=104 black N= 699 non-black (93% white, 7% Hispanic) |
Male: 450/650 (white), 32/49 (Hispanic); P < 0,001 | Male: 54/104 P < 0,001 |
Overall mortality: 13.3% (n=117), no differences between patients of varied ethnicity Mortality: 12% (white), 10% (hispanic), 19% (other); p=303 |
Overall mortality: 13.3% (n=117), no differences between patients of varied ethnicity Mortality:12% died; p=0,303 |
| TEVAR thoracic endovascular aneurysm repair; | ||||||
References
- Harky, A., Sokal, P. A., Hasan, K., & Papaleontiou, A. (2020). The Aortic Pathologies: How far we understand it and its implications on thoracic aortic surgery. Brazilian Journal of Cardiovascular Surgery. [CrossRef]
- Gouveia E Melo R, Silva Duarte G, Lopes A, Alves M, Caldeira D, Fernandes E Fernandes R, Mendes Pedro L. Incidence and Prevalence of Thoracic Aortic Aneurysms: A Systematic Review and Meta-analysis of Population-Based Studies. Semin Thorac Cardiovasc Surg. 2022 Spring;34(1):1-16. [CrossRef] [PubMed]
- Crousillat, D. R., Briller, J., Aggarwal, N. R., Cho, L., Coutinho, T., Harrington, C., Isselbacher, E. M., Lindley, K. J., Ouzounian, M., Preventza, O., Sharma, J., Sweis, R., Russo, M. L., Scott, N. S., & Narula, N. (2023). Sex differences in thoracic aortic disease and dissection. Journal of the American College of Cardiology, 82(9), 817–827. [CrossRef]
- Hiratzka LF, Bakris GL, Beckman JA, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Circulation 2010; 121(13):e266–e369. [CrossRef]
- Erbel R , Aboyans V , Boileau C , Bossone E , Bartolomeo RD , Eggebrecht H et al. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The task force for the diagnosis and treatment of aortic diseases of the European Society of Cardiology (ESC). Eur Heart J 2014;35:2873–926.
- Grewal N, Gittenberger-de Groot AC, Poelmann RE, Klautz RJ, Lindeman JH, Goumans MJ, Palmen M, Mohamed SA, Sievers HH, Bogers AJ, DeRuiter MC. Ascending aorta dilation in association with bicuspid aortic valve: a maturation defect of the aortic wall. J Thorac Cardiovasc Surg. 2014 Oct;148(4):1583-90. [CrossRef] [PubMed]
- Grewal N, Klautz RJM, Poelmann RE. Intrinsic histological and morphological abnormalities of the pediatric thoracic aorta in bicuspid aortic valve patients are predictive for future aortopathy. Pathol Res Pract. 2023 Aug;248:154620. [CrossRef] [PubMed]
- Grewal N, Gittenberger-de Groot AC, Lindeman JH, Klautz A, Driessen A, Klautz RJM, Poelmann RE. Normal and abnormal development of the aortic valve and ascending aortic wall: a comprehensive overview of the embryology and pathology of the bicuspid aortic valve. Ann Cardiothorac Surg. 2022 Jul;11(4):380-388. [CrossRef] [PubMed] [PubMed Central]
- Chung, J., Coutinho, T., Chu, M., & Ouzounian, M. (2020). Sex differences in thoracic aortic disease: A review of the literature and a call to action. The Journal of Thoracic and Cardiovascular Surgery, 160(3), 656–660. [CrossRef]
- Page, M.J., McKenzie, J.E., Bossuyt, P.M. et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev 10, 89 (2021). [CrossRef]
- Goodney, P. P., Brooke, B. S., Wallaert, J. B., Travis, L. L., Lucas, F. L., Goodman, D. C., Cronenwett, J. L., & Stone, D. H. (2013). Thoracic endovascular aneurysm repair, race, and volume in thoracic aneurysm repair. Journal of Vascular Surgery, 57(1), 56-63.e1. [CrossRef]
- Yin, K., Alhajri, N., Rizwan, M., Locham, S., Dakour-Aridi, H., & Malas, M. B. (2021). Black patients have a higher burden of comorbidities but a lower risk of 30-day and 1-year mortality after thoracic endovascular aortic repair. Journal of Vascular Surgery, 73(6), 2071-2080.e2. [CrossRef]
- Díaz-Castrillón, C. E., Serna-Gallegos, D., Aranda-Michel, E., Brown, J. A., Yousef, S., Thoma, F., Wang, Y., & Sultan, I. (2022). Impact of ethnicity and race on outcomes after thoracic endovascular aortic repair. Journal of Cardiac Surgery, 37(8), 2317–2323. [CrossRef]
- Tanious, A., Karunathilake, N., Toro, J., Abu-Hanna, A., Boitano, L. T., Fawcett, T. J., Graves, B., & Nelson, P. R. (2019). Racial disparities in endovascular aortic aneurysm repair. Annals of Vascular Surgery, 56, 46–51. [CrossRef]
- Johnston, W. F., LaPar, D. J., Newhook, T. E., Stone, M. L., Upchurch, G. R., & Ailawadi, G. (2013). Association of race and socioeconomic status with the use of endovascular repair to treat thoracic aortic diseases. Journal of Vascular Surgery, 58(6), 1476–1482. [CrossRef]
- Murphy, E. H., Stanley, G. A., Arko, M. Z., Davis, C. M., Modrall, J. G., & Arko, F. R. (2013). Effect of ethnicity and insurance type on the outcome of open thoracic aortic aneurysm repair. Annals of Vascular Surgery, 27(6), 699–707. [CrossRef]
- Abdulameer, H., Taii, H. A., Al-Kindi, S., & Milner, R. (2019). Epidemiology of fatal ruptured aortic aneurysms in the United States (1999-2016). Journal of Vascular Surgery, 69(2), 378-384.e2. [CrossRef]
- Vervoort, D., Canner, J. K., Haut, E. R., Black, J. H., Abularrage, C. J., Zarkowsky, D. S., Iannuzzi, J. C., & Hicks, C. W. (2021). Racial disparities associated with reinterventions after elective endovascular aortic aneurysm repair. Journal of Surgical Research, 268, 381–388. [CrossRef]
- Ribieras, A. J., Challa, A. S., Kang, N., Kénel-Pierre, S., Rey, J., Velázquez, O. C., Milner, R., & Bornak, A. (2023). Race-based outcomes of thoracic aortic aneurysms and dissections in the Global Registry for Endovascular Aortic Treatment. Journal of Vascular Surgery, 78(5), 1190-1197.e2. [CrossRef]
- Murphy, E. H., Davis, C. M., Modrall, J. G., Clagett, G. P., & Arko, F. R. (2010). Effects of ethnicity and insurance status on outcomes after thoracic Endoluminal Aortic aneurysm Repair (TEVAR). Journal of Vascular Surgery, 51(4), S14–S20. [CrossRef]
- Deery SE, O’Donnell TFX, Shean KE, Darling JD, Soden PA, Hughes K, Wang GJ, Schermerhorn ML; Society for Vascular Surgery Vascular Quality Initiative. Racial disparities in outcomes after intact abdominal aortic aneurysm repair. J Vasc Surg. 2018 Apr;67(4):1059-1067. [CrossRef] [PubMed] [PubMed Central]
- Pandit, V., Nelson, P. R., Horst, V., Hanna, K., Jennings, W. C., Kempe, K., & Kim, H. (2020). Racial and ethnic disparities in patients with ruptured abdominal aortic aneurysm. Journal of Vascular Surgery, 72(1), e85. [CrossRef]
- Asfaw A, Ning Y, Bergstein A, Takayama H, Kurlansky P. Racial disparities in surgical treatment of type A acute aortic dissection. JTCVS Open. 2023 Feb 10;14:46-76. [CrossRef] [PubMed] [PubMed Central]
- Yammine H, Ballast JK, Anderson WE, Frederick JR, Briggs CS, Roush T, Madjarov JM, Nussbaum T, Sibille JA, Arko FR 3rd. Ethnic disparities in outcomes of patients with complicated type B aortic dissection. J Vasc Surg. 2018 Jul;68(1):36-45. [CrossRef] [PubMed]
- Racial and ethnic categories and definitions for NIH diversity programs and for other reporting purposes (NOT-OD-15-089). (2015). https://grants.nih.gov/grants/guide/notice-files/NOT-OD-15-089.html.
- Lu C, Ahmed R, Lamri A, Anand SS. Use of race, ethnicity, and ancestry data in health research. PLOS Glob Public Health. 2022 Sep 15;2(9):e0001060. [CrossRef] [PubMed] [PubMed Central]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



