Submitted:
30 June 2024
Posted:
01 July 2024
Read the latest preprint version here
Abstract
Discoloration of endodontically treated teeth poses a significant aesthetic concern for many individuals, impacting their confidence and self-image. Ceramic veneers have emerged as a popular solution for the aesthetic restoration of such teeth. This paper explores the role of ceramic veneers in addressing tooth discoloration, examining their efficacy, durability, and aesthetic outcomes, via a clinical case. Various factors influencing the selection of ceramic veneers as a treatment modality, including shade matching, preparation techniques, and adhesive bonding, are discussed. Additionally, advancements in materials and techniques have enhanced the versatility and aesthetic appeal of ceramic veneers, making them a valuable option for achieving natural-looking and durable aesthetic restorations in individuals with discolored endodontically treated teeth.
Keywords:
ceramic veneer
; aesthetic
; discolored teeth
; restoration
; endodontically treated teeth
1. Introduction
Many different materials and treatment options are available in restorative aesthetic dentistry for the anterior aesthetic zone. One of the most common therapeutic approaches is the use of ceramic veneers. The high aesthetic performance, excellent biocompatibility of ceramic materials, advancements in bonding techniques with dental tissues, and the longevity of restorations have made ceramic veneers a reliable treatment solution for the anterior aesthetic zone, despite being a sensitive clinical and laboratory process [1,2,3,4,5,6,7]. The use of veneers is primarily indicated for restoring anterior teeth with abrasions, fractures, tooth decay, enamel defects, hypoplasia, or replacing old and extensive resin composite fillings that have been retreated or do not have satisfactory aesthetic results. Ceramic veneers can also be used to change the shape of teeth or close spaces, often in combination with orthodontic treatment. Additionally, they provide aesthetic solutions for cases of discolored teeth due to tetracycline use, fluorosis, or endodontic treatment. The use of ceramic veneers for the aesthetic restoration of discolored endodontically treated teeth in the anterior aesthetic zone, although not a very common technique, is gaining ground in aesthetic dentistry due to its conservative nature compared to placing a full crown [8,9,10,11].
This paper presents the use of ceramic veneers for the aesthetic restoration of endodontically treated teeth that have undergone discoloration, examining their efficacy, durability, and aesthetic outcomes, via a clinical case.
2. Clinical Case
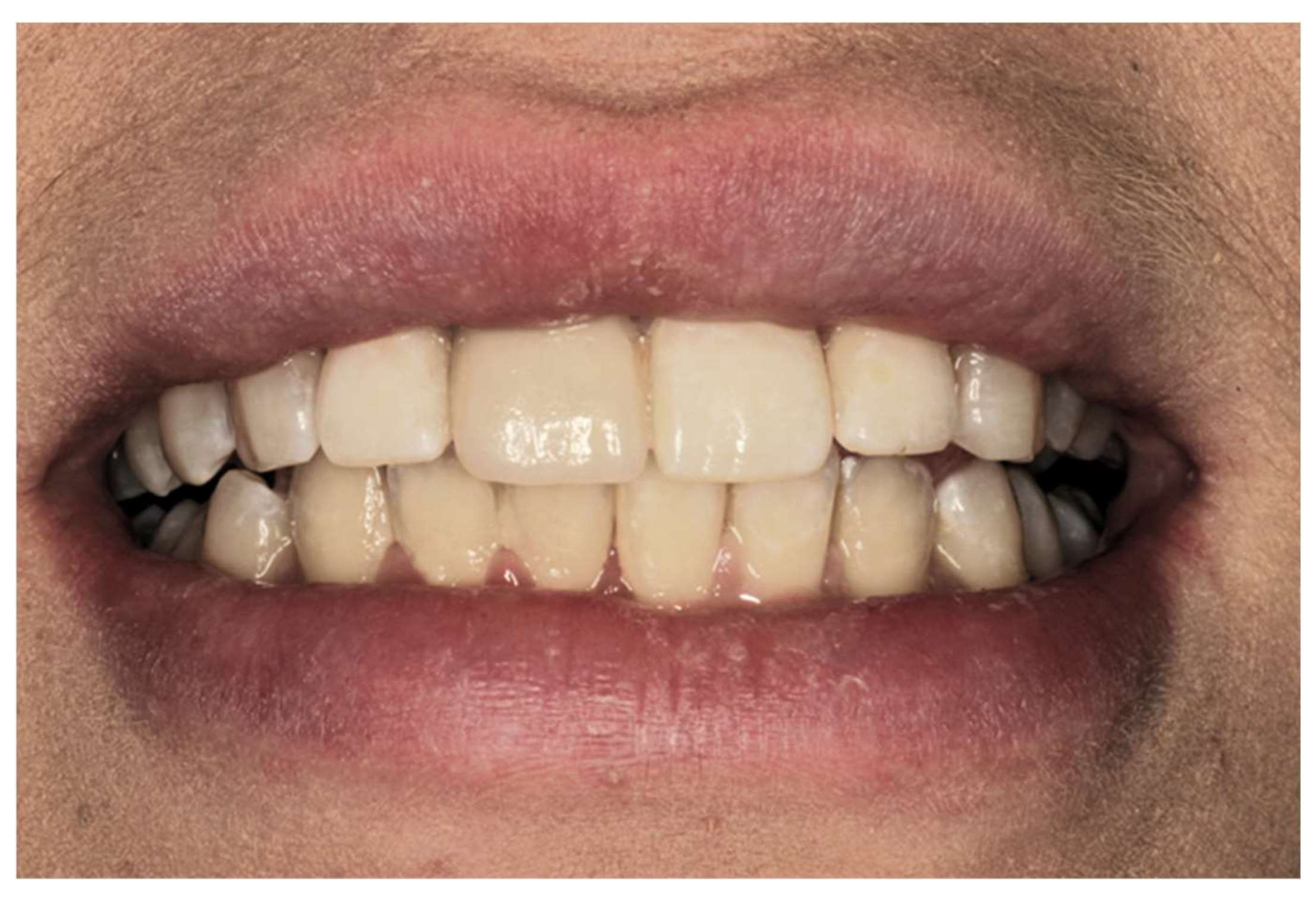
A 43-year-old woman presented at the private dental clinic due to discoloration of tooth 11. (Figure 1) The patient reported that this tooth had undergone endodontic treatment five years ago. The patient’s general medical history was clear, with no underlying diseases. The overall clinical condition of the patient’s teeth was good, and the condition of the periodontal tissues was satisfactory. An X-ray examination was performed to assess the quality of the endodontic treatment of the specific tooth, which was found to be satisfactory. The patient was presented with all alternative treatment options, and it was ultimately decided to restore the specific discolored tooth with a ceramic veneer, following internal bleaching to reduce the degree of discoloration.
The tooth was opened on the palatal surface, and the pulp chamber was cleaned from the remnants of the endodontic treatment material. After sealing the root canal orifice with glass ionomer cement, the ready-to-use whitening gel (active ingredient: 35% H2O2) was applied directly into the pulp chamber using a special syringe, and the cavity was hermetically closed with temporary filling material. Four days later, the patient was recalled to assess the progress of the whitening. During the recall appointment, the temporary filling was removed, the cavity was cleaned from the whitening agent, and then the whitening agent was reapplied, followed by temporary filling for an additional 3 days. The final result of the internal whitening is depicted in Figure 2.
After the internal bleaching procedure, tooth preparation for the ceramic veneer followed. Before the preparation, a diagnostic wax-up was performed to serve as a reference point. The preparation was limited to the buccal surface, and the amount of tooth substance removal was kept to a minimum. Specifically, no more than 0.5-1 mm of tooth structure was removed to preserve enamel across almost the entire preparation, ensuring both mechanical retention and bonding capability with the ceramic veneer. Preparation was performed using the guided depth cutting technique with L.V.S. diamond burs (Laminate Veneer System, Komet Co). The cervical margin of the preparation was defined at the gingival level in a chamfer shape. The preparation extended towards the adjacent surfaces but stopped short of the contact points with neighboring teeth to preserve them intact. Additionally, there was a reduction of the incisal edge by 1.5 mm through a reverse beveling of the enamel. This created a larger enamel surface, necessary for better bonding and resistance in an area subject to significant stress. Finally, all undercuts and sharp edges were smoothed out during the final stage of preparation.
After the preparation was completed, retraction cord was placed and the final impression was taken (Figure 3). The double-mix impression technique was employed using addition silicone materials. Following disinfection, the final impression was digitized using a tabletop scanner (extraoral), and the laboratory process for fabricating the ceramic veneer proceeded using digital methods (Cad-Cam). The prosthetic design initiates by delineating the finish line and determining the insertion axis. Subsequently, a virtual wax-up is created utilizing a database of dental morphologies, considering specific criteria like the cervical margin, material thickness, antagonist teeth, etc. This is succeeded by the computer-aided manufacturing process (CAM), facilitating the fabrication of the complete prosthetic veneer in full translucent zirconia 5Y TZP.
After the fabrication of the ceramic veneer, it was clinically evaluated to assess its marginal fit and aesthetic outcome, followed by its bonding in the patient’s mouth. Zirconia veneer was prepared for bonding with 50-mm Al2O3 airborne-particle abrasion at 0.1 MPa air pressure for 10 seconds. Ceramic primer containing silane and MDP monomer (Monobond Plus, Ivoclar Vivadent AG) was applied to the veneer and then dried with oil-free air. The enamel tooth surfaces were treated with 37% phosphoric acid (Total Etch Gel, Ivoclar Vivadent AG) for 15 seconds, rinsed with water, and airdried. Bonding agent (Adhese Universal, Ivoclar Vivadent AG) was applied and light-polymerized for 10 seconds. Light-polymerized resin cement (Variolink Esthetic LC, Ivoclar Vivadent AG) was applied with the applicator tip to the intaglio of the veneers and evenly spread with a microbrush. The restoration was placed on the tooth and seated under firm finger pressure to achieve the desired cement thickness. An oxygen inhibiting gel (Liquid Strip, Ivoclar Vivadent AG) was applied after excess cement was removed. The natural and aesthetic appearance of the prostheses was very satisfactory for the patient. (Figure 4)
3. Discussion
Treating aesthetic and functional issues of the aesthetic zone with ceramic veneers is one of the most prevalent therapeutic approaches. Ceramic veneers offer a predictable solution for conservative restorations of the facial surface of anterior teeth, serving as an alternative to full crowns and direct composite resin restorations. Their main advantages include excellent biocompatibility, high aesthetic performance, and the conservative nature of tooth preparation.
One indication for ceramic veneers is the aesthetic restoration of discolored teeth. The presence of discolorations in the anterior aesthetic region of the dental arches constitutes one of the most significant aesthetic problems and concerns an increasing percentage of patients nowadays. They have a negative impact on self-esteem, external appearance, interpersonal relationships, and the projection of one’s image to the social environment [12,13]. Endodontically treated teeth often exhibit changes in color, particularly in the challenging area of the clinical cervical region, leading dentists to opt for the restoration of these teeth with full-coverage crowns [14,15]. Ceramic veneers provide a reliable and conservative alternative in these cases, as there is no need for preparation of the palatal or lingual surfaces of the teeth, while the preparation of the facial surface is limited to 0.5-1 mm.
For better aesthetic results, in cases of intrinsic discoloration, an internal tooth whitening procedure may precede, as was done in this specific case. Applying whitening techniques to discolored endodontically treated teeth achieves their decolorization, thus facilitating the dentist in their aesthetic restoration. Whitening endodontically treated teeth is a minimally invasive solution for improving their color [14,15,16]. The materials causing discoloration typically consist of organic residues with extensive carbon chain monomers or dimers, often containing complexes of atoms from other chemical elements, phenylic and carbonylic rings, generally referred to as chromophore groups. Whitening agents act as oxidative agents on these chromophore groups, modifying the polarity and shape of the discolored molecules [17]. Clinical examination should be accompanied by radiographic evaluation of endodontic treatment. Root canal obturation should be adequate in height and width to prevent bacterial microleakage and the spread of whitening agents to periapical tissues [18,19]. Endodontically treated teeth should be asymptomatic, with the absence of clinical and radiographic findings indicative of periapical lesion development [19]. Τhe application of hydrogen peroxide (H2O2) for whitening endodontically treated teeth was first reported by Harlan [20]. The mechanism of action of hydrogen peroxide is quite complex. Its target molecules are the chromophoric organic compounds responsible for discoloration. Its strong oxidizing action leads to the formation of active oxygen radicals and peroxide anion compounds. The oxidation products act on the chromogenic compounds, breaking them down into smaller, colorless, and more soluble molecules [19,20,21,22].
Various types of ceramic materials are recommended for making veneers, including lithium disilicate, feldspathic ceramic, feldspathic ceramic reinforced with leucite, and lithium silicate reinforced with zirconia [23,24,25,26]. These ceramics are prized for their high translucency, owing to their abundant glass matrix content, which ensures pleasing aesthetics. Moreover, they exhibit strong adhesion to adhesive agents following conditioning with hydrofluoric acid (4-10%) and subsequent silanization [27]. Consequently, these ceramics are preferred for veneer production [23,24]. Nonetheless, they come with certain limitations, particularly their inability to effectively conceal significant dental discolorations and their increased fragility when reduced in thickness [25].
Alternatively, ceramics with a high crystalline content, such as yttria-stabilized tetragonal zirconia polycrystals (Y-TZP), were initially primarily utilized for framework fabrication, given their notable fracture resistance and capacity to conceal substrate discolorations [27]. However, computer-aided design and computer-aided manufacturing (CAD-CAM) technology and the improved translucency of recently developed high strength monolithic zirconia have made them clinically acceptable for bonded restorations [27,28]. The higher translucency is achieved by altering the grain size and sintering temperature and by adding more yttria to reduce the residual pores and reduce the impurities [27,28]. Also, in recent years, several manufacturers have enhanced the composition of Zr to create a polychromatic multilayer, aiming to mimic the shade gradient observed in natural teeth. This design involves the incisal portion of the veneer being the most translucent, with chroma and opacity increasing gradually towards the gingival portion [29,30]. Initially, pre-shade layers of the same Zr composition were created to form a polychromatic multilayer, presenting as uniform Zr. It has been indicated that the only difference among the various layers of this uniform multilayer zirconia material is the pigment composition, leading to distinct shades while maintaining similar translucency [29,30]. Following that, ultra-translucent Zirconia (Zr) materials were introduced, featuring distinct microstructures among the layers. These included Tetragonal Zirconia Polycrystals (TZP) and Partially Stabilized Zirconia (PSZ) layers with diverse compositions and properties, resulting in the development of a polychromatic multilayer hybrid composition of Zirconia [30,31]. The varying Yttrium content and chemical composition of the layers result in diverse formulations, leading to differences in the physical properties within the material. Consequently, several manufacturers suggest that advancements in different grades of ultra-translucent Zirconia have made monolithic translucent Zirconia a feasible choice for restoring anterior teeth with indirect veneer restorations [32,33].
In contrast to lithium disilicate veneers, achieving strong bonding to zirconia has presented greater challenges. Polycrystalline zirconia is chemically inert and not susceptible to attack by hydrofluoric acid, resulting in less effective adhesion compared with silica-based ceramics [34]. So, studies indicate that a combination of micromechanical and chemical pretreatment is essential for establishing durable resin bonds with zirconia restorations over the long term. Airborne-particle abrasion using Al2O3 is effective in creating mechanical bonds, while an adhesive resin cement or a ceramic primer containing monomers like 10-methacryloyloxydecyl dihydrogen phosphate (MDP) is advised for achieving chemical bonding to zirconia [35,36,37,38]. According to research by Blatz et al., the APC Zr Bonding Concept is a useful technique for creating strong, durable resin bindings to Zr [39]. The three primary processes of zirconia cementation are referred to as the APC Zirconia Bonding Concept [39]:
Step A: The process entails air-abrading the entire surface of the zirconia intended for bonding. This is achieved using either plain alumina particles or alumina particles coated with silica.
Step B: MDP or phosphate-monomer-based primer is applied to the air-abraded zirconia surfaces.
Step C: Utilizes a dual-cure adhesive composite to guarantee thorough polymerization of the composite beneath the zirconia restoration.
A case series with a follow-up period of up to five years has shown a 100% survival rate for ultra-translucent Zirconia veneers bonded with adhesive resin cement after airborne particle abrasion and silica coating. No noticeable failures such as debonding, veneer fracture, or secondary caries were observed [40,41,42]. Additionally, when bonded with a resin-based adhesive system, the fracture resistance of monolithic all-ceramic restorations is increased compared to conventional cementation methods [42,43].
4. Conclusions
Based on all the aforementioned, we can draw the following conclusions:
- Ceramic veneers provide a reliable and conservative alternative for the aesthetic restoration of endodontically treated teeth that have undergone discoloration.
- For better aesthetic results, in cases of intrinsic discoloration, an internal tooth whitening procedure may precede.
- Considering bonding and cementation, adhesively cemented high translucency monolithic zirconia seems to be a suitable option for veneers.
Author Contributions
“Conceptualization, P.G. and A.G.; methodology, P.G. and A.G.; investigation, P.G.; resources, P.G.; writing—original draft preparation, P.G.; writing—review and editing, P.G., A.G.; supervision, A.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study because Research Ethics Committee (REC) of the University of West Attica deemed that no personal data is being collected, and therefore, the request in question does not fall within the competence of the REC. (UNI.W.A.- Outg. 48581 - 17/06/2024 Aigaleo).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Fradeani, M.; Redemagni, M.; Corrado, M. Porcelain laminate veneers: 6-12year clinical evaluation-a retrospective study. Int J Periodontics Restorative Dent 2005, 25(1), 9–17. [Google Scholar] [PubMed]
- Calamia, JR. Etched porcelain veneers: the current state of the art. Quintessence Int 1985, 16(1), 5–12. [Google Scholar] [PubMed]
- Galiatsatos, A.; Bergou, D. Five-year clinical performance pf porcelain laminate veneers. Quintessence Int 2002, 33, 185–189. [Google Scholar]
- Dumfahrt, H.; Schaffer, H. Porcelain laminate veneers. A retrospective evaluation after 1 to 10 years of service: part II-clinical results. Int J Prosthodont 2000, 13(1),9-18.
- Friedman, M. A 15-year review of porcelain veneer failure – A clinician’s observations. Compend Contn Educ Dent 1998, 19, 625–628. [Google Scholar]
- Edward, J.; Swift, Jr.; Mark, J.; Friedman. Critical appraisal porcelain veneer outcomes, part I. J Esthet Restor Dent 2006, 18(1),54-157.
- Maciej Zarow, Louis Hardan, Katarzyna Szczeklik. Porcelain veneers in vital vs non-vital teeth: a retrospective clinical evaluation. Bioengineering (Basel)2023,10(2),168-175.
- Amrani Alaoui, Y.; Hicham, S.; Amal, EY. Veneers on Devitalized Teeth: The Role of Adhesive Dentistry in Aesthetic and Functional Therapies. Integr J Med Sci 2024, 11, 1–5. [Google Scholar] [CrossRef]
- Freire, A.; Regina Archegas, L. Porcelain Laminate Veneer on a Highly Discoloured Tooth: A Case Report. J Can Dent Assoc 2010, 76, 305. [Google Scholar]
- Chen, J.; Shi, C.; Wang, M.; Zhao, S.; Wang, H. Clinical Evaluation of 546 Tetracycline-Stained Teeth Treated with Porcelain Laminate Veneers. J Dent 2005, 33, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Kelleher, M.G.D.; Roe, F.J.C. The safety-in-use of 10% carbamide peroxide (Opalescence) for bleaching teeth under the supervision of a dentist. Br Dent J 1999, 187, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Davis, L.G.; Ashworth, P.D.; Spriggs, L.S. Psychological effects of aesthetic dental treatment. J Dent 1998, 26, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Watts, A. ; Addy M: Tooth discoloration and staining: a review of the literature. Br Dent J 2001, 190, 309–316. [Google Scholar] [CrossRef] [PubMed]
- van der Burgdt, T.P.; Plasschaert, A.J.M. Bleaching of Tooth Discoloration caused by endodontic sealers. J Endod 1986, 12, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Leendert, B.; Jordan, RE. ; Skinner DH: A conservative bleaching treatment for the non-vital discolored tooth. Compendium of Continuing Education in Dentistry 1984, 5, 471–5. [Google Scholar]
- Dahl, JE. Tooth bleaching-A critical review of the biological aspects. Crit Rev Oral Biol Med 2003, 14, 292–304. [Google Scholar] [CrossRef] [PubMed]
- Attin, T.; Paqué, F.; Ajam, F.; Lennon, AM. Review of the current status of tooth whitening with the walking bleach technique. Int Endod J 2003, 36, 313–329. [Google Scholar] [CrossRef] [PubMed]
- Poyser, N.J.; Kelleher, M.G.D.; Briggs, P.F.A. Managing discoloured non-vital teeth: The inside/outside bleaching technique. Dent Update 2004, 31, 204–214. [Google Scholar] [CrossRef] [PubMed]
- Harlan, AW. The removal of stains from teeth caused by administration of medical agents and the bleaching of a pulpless tooth. Am J Dent Sci 1884/1885, 18:521.
- Cotton, FA.; Wilkinson, G. Oxygen. In: Advances in inorganic chemistry. A comprehensive text. Cotton FA, Wilkinson G, editors. Interscience Publisher. New York, 1972; p.403-420.
- Gregus, Z.; Klaassen CD: Mechanisms of toxicity. In: Cassarett and Doull’s toxicology, the basic science of poisons. Klaassen CD, editor. McGraw-Hill Companies Inc. New York: 1995; p.35-74.
- Soares, PV.; Spini, PH.; Carvalho, VF.; Souza, PG.; Gonzaga, RC.; Tolentino, AB.; Machado, AC. Esthetic rehabilitation with laminated ceramic veneers reinforced by lithium disilicate. Quintessence Int 2014, 45(2), 129–133. [Google Scholar] [PubMed]
- Conrad, HJ.; Seong, WJ.; Pesun, IJ. Current ceramic materials and systems with clinical recommendations: A systematic review. J Prosthet Dent 2007, 98(5), 389–404. [Google Scholar] [CrossRef] [PubMed]
- Trinkner, TF.; Roberts, M. Fluorapatite-leucite glass ceramic veneers for aesthetic anterior restorations. Pract Proced Aesthet Dent 2001, 13(1), 37–41. [Google Scholar] [PubMed]
- Manicone, PF.; Lammetti, RP.; Raffaelli, L. An overview of zirconia ceramics: Basic properties and clinical applications. J Dent 2007, 35(11), 819–26. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y. Making yttria-stabilized tetragonal zirconia. Dent Mater 2014, 30(10), 1195–203. [Google Scholar] [CrossRef] [PubMed]
- Harada, K.; Raigrodski, AJ.; Chung, KH.; Flinn, BD.; Dogan, S.; Mancl, LA. A comparative evaluation of the translucency of zirconia and lithium disilicate for monolithic restorations. J Prosthet Dent 2016, 116, 257–63. [Google Scholar] [CrossRef] [PubMed]
- Kolakarnprasert, N.; Kaizer, M.R.; Kim, D.K.; Zhang, Y. New multi-layered zirconia: Composition, microstructure and translucency. Dent Mater 2019, 35, 797–806. [Google Scholar] [CrossRef] [PubMed]
- Alrabeah, G.; Al-Sowygh, A.H.; Almarshedy, S. Use of Ultra-Translucent Monolithic Zirconia as Esthetic Dental Restorative Material: A Narrative Review. Ceramics 2024, 7, 264–275. [Google Scholar] [CrossRef]
- Toma, F.R.; Porojan, S.D.; Vasiliu, R.D.; Porojan, L. The effect of polishing, glazing, and aging on optical characteristics of multi-layered dental zirconia with different degrees of translucency. J Funct Biomater 2023, 14, 68. [Google Scholar] [CrossRef] [PubMed]
- Kongkiatkamon, S.; Rokaya, D.; Kengtanyakich, S.; Peampring, C. Current classification of zirconia in dentistry: An updated review. Peer J 2023, 11, e15669. [Google Scholar] [CrossRef] [PubMed]
- Kolakarnprasert, N.; Kaizer, M.R.; Kim, D.K.; Zhang, Y. New multi-layered zirconia: Composition, microstructure and translucency. Dent Mater 2019, 35, 797–806. [Google Scholar] [CrossRef] [PubMed]
- Matsuzaki, F.; Sekine, H.; Honma, S.; Takanashi, T.; Furuya, K.; Yajima, Y.; Yoshinari, M. Translucency and flexural strength of monolithic translucent zirconia and porcelain-layered zirconia. Dent Mater J 2015, 34(6), 910–7. [Google Scholar] [CrossRef] [PubMed]
- Koizumi, H.; Nakayama, D.; Komine, F.; Blatz, MB.; Matsumura, H. Bonding of resin-based luting cements to zirconia with and without the use of ceramic priming agents. J Adhes Dent 2012,14:385-92.
- Inokoshi, M.; De Munck, J.; Minakuchi, S.; Van Meerbeek, B. Meta-analysis of bonding effectiveness to zirconia ceramics. J Dent Res 2014, 93, 329–34. [Google Scholar] [CrossRef] [PubMed]
- Özcan, M.; Bernasconi, M. Adhesion to zirconia used for dental restorations: A systematic review and meta-analysis. J Adhes Dent 2015, 17, 7–26. [Google Scholar] [PubMed]
- Kern, M.; Thompson, VP. Sandblasting and silica coating of a glass-infiltrated alumina ceramic: Volume loss, morphology, and changes in the surface composition. J Prosthet Dent 1994, 71, 453–61. [Google Scholar] [CrossRef] [PubMed]
- Blatz, M.B.; Conejo, J. cementation and bonding of zirconia restorations. Compend Contin Educ Dent 2018, 39 (Suppl. S4), 9–13. [Google Scholar] [PubMed]
- Silva, N.R.; Araújo, G.D.; Moura, D.M.; Araújo, L.D.; Gurgel, B.D.; Melo, R.M.; Bottino, M.A.; Özcan, M.; Zhang, Y.; Souza, R.O. Clinical Performance of Minimally Invasive Monolithic Ultratranslucent Zirconia Veneers: A Case Series up to Five Years of Follow-up. Oper Dent 2023, 48, 606–617. [Google Scholar] [CrossRef] [PubMed]
- Dikicier, S.; Korkmaz, C.; Atay, A. Surface roughness and characteristics of CAD/CAM zirconia and glass ceramics after combined treatment procedures. BMC Oral Health 2022, 22, 524. [Google Scholar] [CrossRef] [PubMed]
- Shetty, R.; Pinge, SS.; Shetty, S.; Banga, P.; Zahid, M. Zirconia monolithic veneers: A durable and cosmetic alternative to regular veneers; Adv Hum Biol 2022, 12,22-5.
- Papia, E.; Larsson, C.; du Toit, M.; Vult von Steyern, P. Bonding between oxide ceramics and adhesive cement systems: A systematic review. J Biomed Mater Res B Appl Biomater 2014, 102, 395-413. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Intraoral photograph at the first visit.

Figure 2.
The final result after the internal bleaching of the tooth.

Figure 3.
The tooth before the final impression.

Figure 4.
The final result.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



