
Submitted:
29 June 2024
Posted:
01 July 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Introduction: In Part II of this three-part series, we expose techniques that can be used by the U.S. Centers for Disease Control and prevention (CDC) and Food and Drug Administration (FDA) to manipulate and throttle the Vaccine Adverse Event Reporting System (VAERS), a vaccine safety monitoring system open to the public. The U.S. government’s recommendation of COVID-19 vaccines during pregnancy was more a product of propaganda than of science and plagued with conflicts of interest. The extreme breach of COVID-19 vaccine pregnancy complication safety signals documented in VAERS cannot be disregarded or concealed. As a result, CDC/FDA are moving to closed, government captured platforms, including V-safe, Vaccine Safety Datalink (VSD) system, and the Biologics Effectiveness and Safety (BEST) system. Public transparency of adverse events following COVID-19 vaccination in pregnancy should be increased, not thwarted. Methods: In Part I the CDC/FDA Vaccine Adverse Event Reporting System (VAERS) database was queried from January 1, 1990, to April 26, 2024 for adverse events (AEs) involving pregnancy complications following vaccination. In Part II we investigate tactics discovered in VAERS that concealed vaccine injuries and deaths. Conflicts of interest, as well as specific communications and publications from the CDC/FDA and the New England Journal of Medicine (NEJM) are analyzed. Results: Of all VAERS AE reports, 8.47% (138,983) of COVID-19 reports had no vaccination date and thus were missing from the data presented in Part I of this series. We unconcealed data presented in Part I of this series to include VAERS case reports that were excluded when using standard queries because of an “unknown vaccination date”. The unconcealed data in the 37 AE cases reported in this study (Part II) ranged from 0 - 38% with a mean of 8.2% (standard deviation 9.7%) and the significant breaches of VAERS safety signals in Part I of this series were largely underestimated. Another method of concealing vaccine associated AEs is to exclude the specific vaccine type rendering it as an “unknown vaccine type”. “Unknown vaccine type” has logarithmically increased since the rollout of the COVID-19 vaccines in 2021, ranging from 1 to 400 cases between 1990 to 2018 to 11,461 cases in 2021. CDC/FDA granted $67 million via a Cooperative Agreement grant to Massachusetts Department of Public Health (MDPH) between July 1, 2019, to June 30, 2025. MDPH then made subawards under this grant to 21 influential public and private health and civic organizations, including NEJM’s owner, Massachusetts Medical Society (MMS). As one of the subawardees under the grant, MMS as owner of NEJM received over $426,000 in federal HHS/CDC grant money from 2019 to 2020 for “public health and medical emergency preparedness projects”. Conclusions: CDC/FDA has failed to capture and account for a significant number of AE case reports following COVID-19 in VAERS by a variety of techniques in an apparent attempt to sanitize the data. CDC’s Rochelle Walensky and NEJM’s Editor-in-Chief Eric Rubin pushed novel untested COVID-19 vaccines in pregnant women despite clear evidence from multiple sources that safety signals had been breached.
Keywords:
COVID-19 Vaccines
; Pregnancy Complications
; Cervical Insufficiency
; Miscarriage
; Stillbirth
; Preterm Delivery
; Preeclampsia
; Fetal Growth Restriction
; Fetal Malformations
; Premature Newborn Death
; Newborn Complications
Introduction
In Part I we reviewed how the “Golden Rule of pregnancy” has remained unchanged throughout millennia: Novel and/or potentially harmful substances are never used when new human life is being formed and nurtured within the womb. We reviewed in historical detail the unprecedented human multigenerational carnage caused by the catastrophic diethylstilbestrol (DES) saga, ironically marketed to improve pregnancy outcomes. The thalidomide disaster started after DES, but both overlapped during the span of the 1950’s to 1970’s.
The German pharmaceutical company Chemie-Grünenthal launched thalidomide in the 1950’s for morning sickness in pregnancy.1 While DES was by far a greater disaster, thalidomide is more widely known because of the devastating visual images of its associated malformations known as phocomelia which is characterized by one or more missing limbs. In addition to limb deformities, survivors had other severe handicaps including early onset of age-related issues such as osteoarthritis, joint mobility issues, and coronary heart disease. The thalidomide disaster demonstrates how easily delicate and intricate processes in the developing embryo/fetus can be catastrophically damaged with a novel teratogenic agent in pregnancy. A single 50 mg tablet of thalidomide during the time-sensitive window is sufficient to cause birth defects in up to 50% of pregnancies.2 About 20,000 were injured and 80,000 died from thalidomide. Despite the devastation caused by thalidomide, no one was ever prosecuted, Chemie-Grünenthal was never held accountable, and justice was never served. Reports suggest that Grünenthal entered into an agreement with German Federal Prosecutors and criminal charges withdrawn.2
The purpose of Part II of this three-part series is to explore techniques that appear to be used by the U.S. Centers for Disease Control and prevention (CDC) and Food and Drug Administration (FDA) to manipulate and throttle the Vaccine Adverse Event Reporting System (VAERS) to limit adverse event data that we published in Part I. We also review the systematic discrediting of VAERS in favor of other federal vaccine safety surveillance systems that do not allow voluntary reporting of adverse events and/or are closed to independent scrutiny and public view. These include V-safe, Vaccine Safety Datalink (VSD) system, and the Biologics Effectiveness and Safety (BEST) system. Finally, we explore potential conflicts of interest between:
- CDC/FDA
- Then-CDC Director Rochelle Walensky MD MPH
- NEJM’s Editor-in-Chief, Eric Rubin MD PhD
- NEJM’s Managing Editor, Stephen Morrissey PhD
- CDC vaccine safety officer Tom Shimabukuro MD MPH
- Massachusetts Department of Public Health (MDPH)
- Owner of the NEJM – the Massachusetts Medical Society (MMS)
Methods
Part 1 of this series specifically details the methods used to extract pregnancy related adverse events (AEs) from VAERS using MedAlerts,3 one of only two long-standing platforms used to query the CDC/FDA VAERS database. The study period was from January 1, 1990, through April 26, 2024, a period of 412 months for all vaccines with COVID-19 vaccines only available for 40 months (December 1 2020 to April 26, 2024). The start date was selected as January 1, 1990, because that is generally recognized as the formal start of the VAERS system.
The first column of Table 1 lists 37 pregnancy complications (AEs) investigated. The second column of Table 1 shows the exact MedAlerts “symptom(s)” used to investigate each of the 37 pregnancy AEs. It is noteworthy that the CDC/FDA VAERS database lists AEs by British rather than American spelling. The third column of data in Table 1 (taken directly from Part I) lists the raw data of AEs depicted as follows: COVID-19 vaccines / influenza vaccines / all other vaccines except COVID-19.
In standard VAERS queries AEs that are missing a date of vaccination are not included among the AEs counted, even though this information may be available in the VAERS report in other fields. In Table 2, AEs not available on the standard queries as reported in Part I were unconcealed. In Column 3, AEs are reported as total raw data including the unconcealed AE cases in the following format: COVID-19 vaccines / influenza vaccines / all other vaccines. In Column 4, AEs are reported as a percent of original raw data that were concealed in a similar format: % COVID-19 / % influenza / % of all other vaccines. Not included in the unconcealed AEs in Table 2 are other concealed data that have an “unknown vaccine type” despite the fact it is present in other fields. The unconcealed data in the 37 pregnancy associated AE cases reported in this study (Part II) were analyzed using standard statistical methods.
In 2021, the New England Journal of Medicine (NEJM) published an Editorial entitled “Audio Interview: Covid-19 Vaccines and Pregnancy – A Conversation with CDC Director Rochelle Walensky” with authors Eric J. Rubin, MD PhD, Lindsey R Baden, MD, Rochelle Walensky MD MPH and Stephen Morrissey PhD.4 The interview was recorded on April 16, 2021, and subsequently published 5 days later on April 21, 2021. This audio interview was then transcribed, and relevant time-marks are referenced.4 Research was then conducted on government public spending records. Timelines are constructed based upon published references and other public statements made by relevant public figures.
Results
The data and analytics from Part I are not duplicated here. All 37 AEs in pregnancy far exceed the CDC/FDA safety signal: a PRR of ≥ 2 or a Chi-square of ≥ 4.5 Summary statistics for the 37 AEs mean (n, range) are as follows: PRR 69.2 (46, 5.37 - 499); z statistic 9.64 (46, 3.29 - 27.0); and Chi-square was 74.7 (26, 28.9 - 148). All p values were ≤ 0.001 with the majority being less than 0.000001.
Table 1, Column 3 describes the raw data for each of the 37 AEs expressed as: case numbers in COVID-19 vaccines over 40 months / case numbers in influenza vaccines over 412 months / case numbers in all vaccines (including influenza), excluding only COVID-19 for 412 months.
Of all VAERS reports, 8.47% (138,983) of COVID-19 reports6 and 10.12% (22,834) of influenza reports7 have no vaccination date. Table 2, Column 3 incorporates all applicable cases of unknown vaccination dates for influenza and COVID-19 vaccines. Leaving “date of vaccination” field empty resulted in up to 38% of COVID-19 vaccine associated AEs omitted as noted in Table 2. The unconcealed data in the 37 AEs reported in this study (Part II) ranged from 0 - 38% with a mean of 8.2% (standard deviation 9.7%) as documented in Table 2. These findings demonstrate that the 37 pregnancy associated AEs reported in Part I of this series were largely underestimated due to the concealed data.
Discussion
The findings in Part II document that pregnancy associated AE safety signals in Part I are underestimated because of a variety of intentional or unintentional omitted data missing from some VAERS fields. Danger signals in Table 1 are significantly underestimated because “unknown vaccination date” and “unknown vaccination type” exclude case reports submitted to VAERS from appearing in standard search results. Moreover, these two fields can be manipulated by VAERS administrators to conceal injuries and deaths and to sanitize unprecedented breaches in safety signals. As noted in Table 2 simply leaving “date of vaccination” field empty resulted in up to 38% of AEs omitted. The unconcealed data in the 37 AEs reported in this study (Part II) ranged from 0-38% with a mean of 8.2% (standard deviation 9.7%) as documented in Table 2. These findings demonstrate that the 37 pregnancy associated AEs in Part I of this series were largely underestimated due to the concealed data. Unaccounted for in Table 2 are missing AEs resulting from case report entries with “unknown vaccine type”. Figure 1 notes the exponential rises in case report entries with “unknown vaccine type” in 2021, coincidentally correlating with the rollout of the COVID-19 vaccines in December 2021.
Despite pro-vaccine biases of the CDC/FDA and attempts to conceal and “throttle” deaths and injuries caused by the COVID-19 vaccines,9,10,11 there remains an unprecedented breach of safety signals using the CDC/FDA’s own criteria for safety. The CDC/FDA appear to use many additional methods to conceal data: for example, leaving “age field” unpopulated despite age documentation in the summary12; missing “state and location”13 fields; not documenting COVID-19 vaccine as an official line item; and placing COVID-19 vaccine as a “concomitant medication”14 in the “other medication” variable. There are 282 examples of COVID-19 vaccines being listed as a concomitant medication.14 Many independent experts have documented large numbers of VAERS cases which were dropped, deleted, and never published.15,16
Propaganda: The Government Enlists Private Actors
Promoting the COVID-19 vaccines in pregnancy was never a product of science, but of propaganda. Pfizer and the FDA attempted to conceal the post-market analyses of AEs17 for 55-75 years.18,19 At the same time unprecedented amounts of U.S. tax dollars were invested to promote the alleged safety, efficacy, and necessity of the COVID-19 vaccines20-25 even in the vulnerable population of pregnant women, preborns, and newborns. In early 2021 the COVID-19 Community Corps was awarded billions of federal dollars to recruit “trusted voices” to push vaccines across all channels of communication and the American College of Obstetricians and Gynecologist (ACOG) was one of their founding members.20,21 FOIA request by attorney Thorp demonstrated that ACOG received millions of US tax dollars to enter cooperative agreements with the government requiring them to remain in lock-step with the Department of Health and Human Service (HHS) and CDC’s narrative on the COVID-19 vaccines.22 ACOG controls 60,000 ObGyn physicians in the U.S., Canada and some countries in South America.22 Prominent physicians including an Ob/Gyn were fired from major hospital systems after publicly speaking out against narratives of the hospitals and HHS/CDC.23 HHS allocated $186 billion to more than 420,000 healthcare systems, hospitals, and health care providers across the US in early 2021. These monies included over $306 million to SSM Health and even more to Houston Methodist, both of whom mandated vaccines in their employees and terminated physicians for speaking out against their policies.23 CVS and Walgreens Pharmacies entered into lucrative government contracts to push the lethal HHS narrative and the COVID-19 vaccines while largely refusing to fill prescriptions for hydroxychloroquine and ivermectin.24 Even faith leaders of all major religions were recruited by the federal government to push the vaccines on their congregations in order to eliminate vaccine hesitancy.25
April 16, 2021 NEJM Editor-in-Chief Rubin and Managing Editor Morrissey Host CDC Director Walenksy and Publish Flawed Shimabukuro Study Despite Potenial Conflicts of Interest
On April 16, 2021 CDC Director Rochelle Walensky MD MPH along with Eric Rubin MD PhD and Stephen Morrissey PhD held a public discussion which was published in the New England Journal of Medicine (NEJM) just 5 days later on April 21, 2021.4 Shamelessly, NEJM Editor in Chief Rubin and Deputy Editor Morrissey perceived no conflict of interest in hosting CDC Director Walensky to promote COVID-19 vaccines in pregnancy, despite policies requiring NEJM to disclose all financial associations and ensuring that such associations do not influence NEMJ content.26 The safety of COVID-19 vaccines had never been studied in pregnancy.
The HHS/CDC awarded a $67.1 million federal cooperative agreement grant to Massachusetts Department of Public Health on July 1, 2019, running through June 30, 2025.27 Massachusetts Department of Public Health made 21 subawards to influential public and private civic and health organizations including NEJM’s owner Massachusetts Medical Society (MMS)27. NEJM’s owner MMS was one of the sub-awardees and received over $426,000 from 2019 to 2020 for “public health and medical emergency preparedness projects”.27 Figure 2 outlines these relationships and monetary exchanges of U.S. tax dollars, raising questions about financial conflicts of interest and bias.
On the exact same day that the audio interview of CDC Director Walensky was published in the NEJM, April 21, 2021,4 another CDC article28 was published by the NEJM which promoted the safety and efficacy of the COVID-19 vaccines in pregnancy. Entitled “Preliminary Findings of mRNA COVID-19 Vaccine Safety in Pregnant Persons” this article was rife with author conflicts of interest and apparent sleight-of-hand data manipulation.28 At the time of the article’s publication, lead author Tom T. Shimabukuro MD was director of the Immunization Safety Office at the CDC, also having served as VAERS team lead, acting lead for the Vaccine Safety Datalink (VSD) team, and team lead on the CDC COVID-19 Vaccine Task Force. The HHS/CDC had already been pushing COVID-19 shots as safe and effective (including their prior April 1, 2021, announcement of COVID-19 Community Corps, which paid billions of federal dollars to recruit to push vaccines across all channels of communication). Deeply entrenched in the CDC’s COVID-19 vaccine safety detection mechanisms, and with the CDC actively pushing the vaccines across all channels, lead author Shimabukuro (and other authors employed by the government) had insurmountable conflicts of interest including personal biases related to their own positions at the CDC, professional standing, reputation, and/or gain. Such conflicts of interest fatally compromised the integrity of the NEJM study and its conclusion that there were no safety concerns with the vaccine in pregnancy.
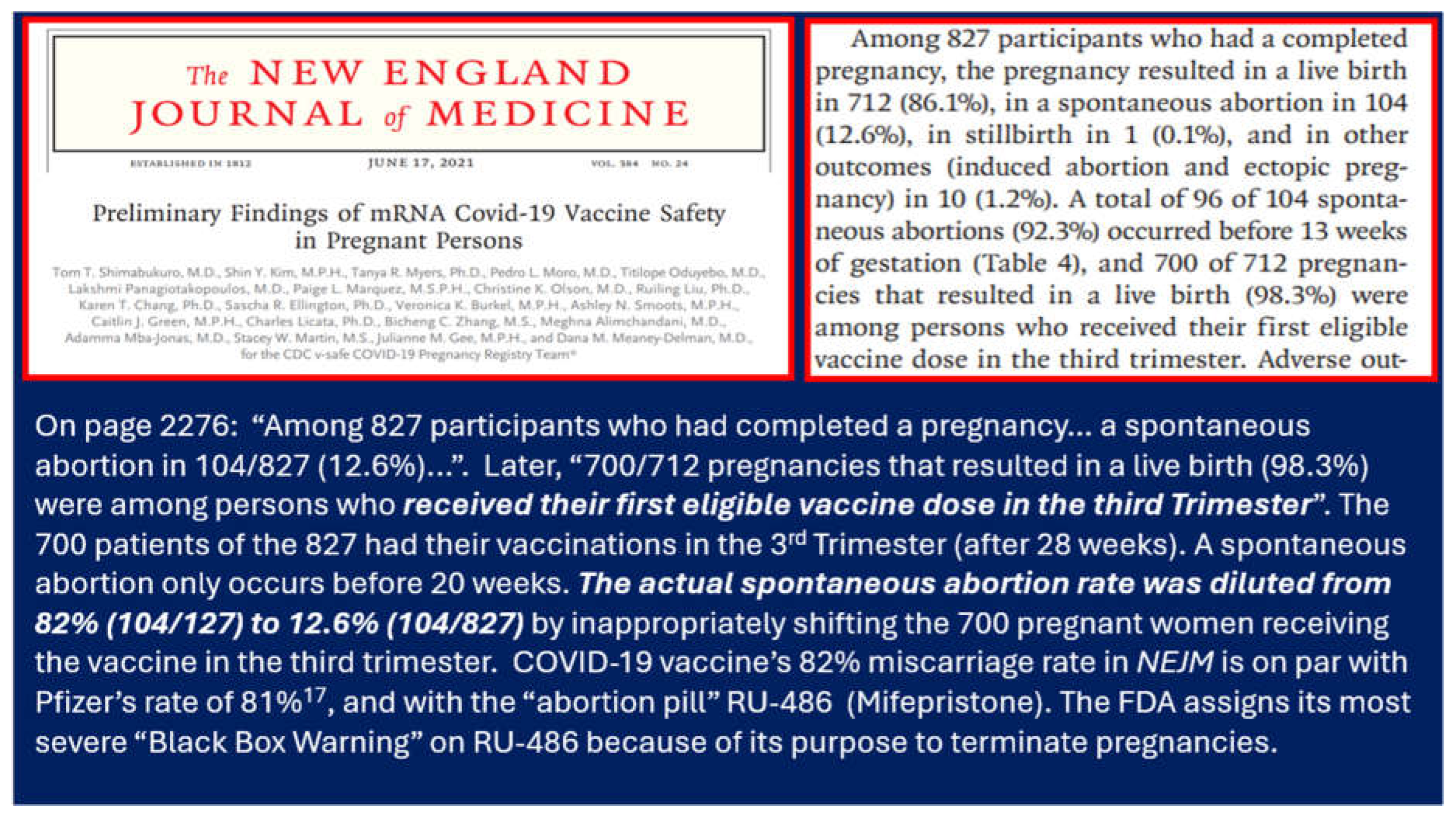
The Shimabukuro study28 was published by the NEJM on the same day as the Walensky propaganda discussion with NEJM Editor-in-Chief Rubin and Managing Editor Morrissey.4 One must ask whether the Shimabukuro28 article was really written by the 21 authors or actually written by the 21 authors or a ghostwriter perhaps from a pharmaceutical industry? Flagrant fatal methodological and statistical errors were made. How could 21 authors including three obstetricians and other physicians and PhD’s have devised such a flawed incoherent study? They studied only 10 weeks of the V-safe data when a pregnancy duration is 40 weeks. Who chose the 10-week interval and why? Who chose when that 10-week interval would begin? The relevant discussion below regarding V-safe’s catastrophic outcomes and lack of transparency makes the NEJM study28 appear even more brazenly manipulated. Figure 3 shows a screen shot from the NEJM article28 proving a spontaneous abortion rate of 82% (104/127), not the study’s claimed risk of 12.6% (104/827).29,30 A 12.6% rate of spontaneous abortion is still far too high in a well-established viable pregnancy after the initial visit. Interestingly, the Shimabukuro article’s actual spontaneous abortion rate of 82% is nearly identical to that of Pfizer’s 5.3.6 post market analysis rate of 81% (page 12)17 - discussed in Part I of this series. The Shimabukuro NEJM article’s28 82% spontaneous abortion rate rivals that of the “abortion pill” (RU486, mifepristone) that carries a mandatory FDA “black box warning”.
April 16, 2021 NEJM Published Discussion Including Rubin, Morrissey, and Walensky Ignores Safety Signals
Figure 3.
The NEJM article by Shimabukuro published online on April 21, 2021, the exact same day that the NEJM audio interview with NEJM Editor-in-Chief Rubin and NEJM Managing Editor Morrissey hosted Walensky, Director of the CDC. Pictured here are screen captured images from the final printed version of the Shimabukuro article on June 17, 2021. The audio recording of Rubin, Morrissey, and Walensky was recorded on April 16, 2021, and was then published on April 21, 2021 – the exact same day the online version of the Shimabukuro NEJM article was published. Pictured below is he printed version of this paper published on June 17, 2021.28 There were extraordinary conflicts of interest with this publication as all authors were federal employees. Shimabukuro was director of the Immunization Safety Office at the CDC, also having served as VAERS team lead, acting lead for the Vaccine Safety Datalink (VSD) team, and team lead on the CDC COVID-19 Vaccine Task Force.
Figure 3.
The NEJM article by Shimabukuro published online on April 21, 2021, the exact same day that the NEJM audio interview with NEJM Editor-in-Chief Rubin and NEJM Managing Editor Morrissey hosted Walensky, Director of the CDC. Pictured here are screen captured images from the final printed version of the Shimabukuro article on June 17, 2021. The audio recording of Rubin, Morrissey, and Walensky was recorded on April 16, 2021, and was then published on April 21, 2021 – the exact same day the online version of the Shimabukuro NEJM article was published. Pictured below is he printed version of this paper published on June 17, 2021.28 There were extraordinary conflicts of interest with this publication as all authors were federal employees. Shimabukuro was director of the Immunization Safety Office at the CDC, also having served as VAERS team lead, acting lead for the Vaccine Safety Datalink (VSD) team, and team lead on the CDC COVID-19 Vaccine Task Force.
Time marks for Walensky’s NEJM audio publication statements are detailed in this reference.4 In the NEJM discussion, Rubin and Walensky4 promoted fear tactics that were unsupported by research studies involving morbidity and mortality of unvaccinated pregnant women and their fetuses/newborns from COVID-19 infection. Walensky stated the following: “women who are pregnant have a 2-3 fold increase in risk of ICU stay, a 2 fold increased risk of mechanical ventilation as well as ECMO [extracorporeal membrane oxygenation], and the babies actually having somewhere between a 2-4 fold increased risk of adverse outcomes”.4 Conversely, a study by Pineles and colleagues31 was published just 20 days later on May 11, 2021 reporting the opposite. In a large cohort of 1,062 pregnant and 9,815 nonpregnant women all hospitalized with COVID-19 and viral pneumonia, Pineles found that pregnancy had a dramatic protective effect compared to non-pregnant women. Pregnancy was associated with a 75% reduction in maternal mortality rates compared to that of the nonpregnant women (0.8% vs 3.5%; OR 0.24, 95% CI 0.12-0.48, p < 0.0001).31 Pineles states that rates found in their study “are consistent with results of multiple other studies” citing Knight32 from June 8, 2020, and Metz33 from February 8, 2021. Both the Knight32 and Metz33 studies were published prior to the statements published by Walensky/Rubin4 on April 21, 2021.
Rubin and Walensky boasted about the validity of VAERS and that it demonstrated no safety concerns for pregnant women in their NEJM interview.4 Yet CDC Director, Walensky and her colleagues at the FDA would have already received the damning Pfizer 5.3.6 post-marketing data completed February 28, 2021.17 Moreover, Pfizer’s post marketing report bears a Bates stamp17 printed on each page indicating receipt by the FDA and its Center for Biologics and Evaluation Research (CBER). As CDC Director, it was Walensky’s responsibility to have reported that document to the world and to have immediately halted the COVID-19 vaccinations. In early 2021 a whistleblower widely circulated this Pfizer document17 on the internet. Attorney Aaron Siri of Informed Consent Action Network (ICAN) obtained the official release of the Pfizer document17 by a Freedom of Information Act request on April 1, 2022. As of their April 16, 2021, published “discussion” which shamelessly promoted the untested COVID-19 vaccines in pregnancy, Rubin, Walensky, and Morrissey certainly would have been aware that multiple pregnancy AEs had already breached VAERS safety signals set forth by the CDC/FDA.
One study author found that the CDC/FDA appears to have deleted cases after publication in VAERS including: 32,365 COVID-19 reports which included 1,144 deaths; 1,535 permanent disabilities; 1,082 life threatening complications; 3,145 hospitalizations; and 5,087 emergency reports.15 Because of an inability to normalize growing numbers of deaths and injuries reported to VAERS, CDC/FDA and Vaccine Safety Committee officers began first ignoring and then denigrating VAERS, inviting other influential sources to question the validity of VAERS which the CDC/FDA was legally responsible for maintaining.
Since this time, it appears what followed was a systemic disregard and undermining of VAERS across all media platforms. As just one example, CDC Vaccine Safety Office Director Shimabukuro in 2023 parroted Walensky’s hollow words in defense of the CDC’s handling of the onslaught of COVID-19 vaccination AEs. When asked about AEs, Walenksy dubiously claimed in her 2021 NEMJ discussion that the CDC took these reports “very seriously”.4 Later, in a January 2023 public safety meeting Shimabukuro parroted Walensky’s words as if they were scripted. In answering a question about how the CDC was handling AEs that were not being captured by the closed Vaccine Safety Datalink (VSD) system, Shimabukuro responded stating that the CDC takes these reports “very seriously”.34 CDC Director Walensky and CDC Vaccine Safety Official Shimabukuro provided false assurances that the CDC took these AEs “very seriously” when the opposite appears to be true.
Other widely influential organizations have attempted to denigrate the credibility of VAERS.35,36 One such influential organization is Johns Hopkins Bloomberg School of Public Health, which claims on its webpage that VAERS has gained “dubious notoriety” during the pandemic because of “anti-vaccination fringe groups” attempting to “spin false stories using VAERS data adding to misinformation about the safety of COVID-19 vaccines”.37 However, John Hopkins has insurmountable financial and other conflicts of interest: Johns Hopkins University reportedly leads all other U.S. universities and colleges as the top recipient of National Institutes of Health (NIH) funding38 and is one of only eight medical research centers in the U.S. chosen to partner with the CDC’s Clinical Immunization Safety Assessment (CISA) project39. In 2022 alone, Johns Hopkins is reported to have received $1.3 billion in government spending.40
While CDC/FDA officials and others with insurmountable conflicts of interest discredit VAERS, they promote other COVID-19 vaccine surveillance systems which are closed to independent scrutiny, including V-safe, Vaccine Safety Datalink (VSD), and Biologics Effectiveness and Safety (BEST).41 As closed systems, both VSD and BEST systems are, in many ways, the antithesis of VAERS.20,41 For example, VAERS relies on open reports of first-person narrative testimony mostly from healthcare providers, but also from the patient or family members about an individual’s own experiences with adverse outcomes following vaccination. By way of comparison, the VSD and BEST systems rely on third-party concealed surveillance and follow narrow protocols for identifying adverse outcomes. The VSD and BEST data are collected and reported by entities having a financial or other interest in the research and outcomes of vaccine safety. While VAERS allows open reporting of all adverse events following COVID-19 vaccination, VSD and BEST allow only pre-specified, closed sets of adverse outcomes, with multiple exclusions which will preclude a symptom from being classified as an AE. If these predetermined and time-limited AEs are detected, no independent public oversight exists to verify that they will ever be reported. Rather than complementing VAERS, the VSD and BEST surveillance systems are designed to counter the VAERS data, handing sole control of the safety data over to the CDC/FDA without transparency, independent scrutiny, or public accountability.
Our data indicates that the CDC/FDA are determined to push the COVID-19 vaccines regardless of their morbidity and mortality. In her NEJM published discussion, CDC Director Walensky proclaimed VAERS to be a valid vaccine safety tool showing reassuring pregnancy outcomes after COVID-19 vaccines on April 16, 2021.4 COVID-19 vaccines were not rolled out until mid to late December 2020 depending upon the state. It would be impossible and highly unethical for someone in a federal medical leadership role to give any reassurances of vaccine safety in pregnancy with only 4 months of data after rollout and zero long-term postnatal follow up of the children. As the authors demonstrate here, VAERS has unequivocally shown the exact opposite of what Walensky claimed – in just 3 years the COVID-19 vaccines in pregnancy exponentially exceed the combined disasters of DES and thalidomide over 4 decades. Because the CDC/FDA is unable to control the input and sanitize the damning VAERS data, they appear to be attempting to replace it with closed and concealed vaccine safety monitoring systems such as V-safe, VSD, and BEST which rely on pre-specified outcomes with no “stopping rules”.20,41,42 In the last half-century, the CDC has abruptly halted vaccination programs without a finding of “causation” and based only on association after only a few deaths (as in the swine-flu vaccine43) and with only a few dozen cases of intussusception (as in the rotavirus vaccine44). Breaking from historical position which prioritized safety, the CDC has now shockingly abolished all “stopping rules.” Egregiously, ignoring “stopping rules” began in early 2021 when Pfizer’s own post-market report proved COVID-19 vaccines the most lethal and injurious medication ever rolled out.17
V-safe Smart Phone Safety Monitoring System Exposed
The CDC/FDA cites HIPPA violations for claims that AEs following COVID-19 vaccination data must remain confidential and in their sole custody, yet this is easily overcome by de-identifying data, exactly as done in VAERS. CDC/FDA have not been transparent with the Pfizer 5.3.6 post-market analysis, VSD, BEST, or V-safe data. The CDC/FDA refused release of their V-safe data until forced to turn it over after multiple legal demands, appeals, and two federal lawsuits were filed.45 While V-safe data itself is frightening, even more egregious is the CDC/FDA stonewalling the release of the data despite legal demands from attorney Aaron Siri and ICAN.45 V-safe’s data showed that 7.7% of its approximate 10 million users reported having to receive medical care after vaccination, 70% of which sought outpatient/urgent clinical care, emergency room care, and/or were hospitalized.45 If that is not shocking enough, an additional 25% reported missing school or work or unable to perform normal activities, for a total of 32.7% of the 10 million plus participants having experienced significant issues.45
According to ICAN’s Freedom of Information Act public records, 10,108,273 cases exist in V-Safe. V-Safe data shows 782,913 (7.7%) participants required medical care. Roughly only 40,214 reports of VAERS and V-Safe are comingled.46 Yet there were 172,942 adolescents in V-safe compared to only about 50% (87,147) of that in VAERS.47,48 It appears that many AEs were directed to V-safe which is closed to public scrutiny and away from VAERS which is publicly accessible.
As of June 18th, 2024, ICAN revealed newly obtained V-safe data including “free texts fields” which were not previously available in the initial V-safe data. To date only 23% (1.8 of 7.8 million) free texts have been released. The foregoing includes 8,679 cases of chest pain/carditis, 295 strokes/infarcts/embolism, 73 deaths, 500 cases of miscarriage, and more than 2,000 reports of menstrual disturbances.49,50,51 This was hidden in the prior V-safe data and 6 million more (77%) of the V-safe free texts are yet to come in future monthly tranches. Three years ago, Walensky and Rubin’s portrayal of the reassuring COVID-19 vaccination data in VAERS and V-safe on April 16, 20214 is now even more shocking. It is no wonder that CDC/FDA would want to transition to completely closed AE reporting systems, such as VSD and BEST.
Pharmaceutical Conflicts of Interest
Recent investigation into the newly appointed members of the Advisory Committee on Immunization Practices (ACIP) shows insurmountable conflicts of interest pharmaceutical industry. The panel roster of the ACIP had dwindled down to less than half of its normal size. In February of 2024 the HHS announced these vacancies were filled and the panel was expanded to 16 voting members, thereby adding 9 members of late.52 The ACIP has a great deal of influence over the CDC’s determination of vaccine recommendations and schedules. Another example of disturbing conflict of interest involving individuals in critical leadership positions is demonstrated by these newly filled ACIP positions: Seven of the nine new ACIP committee members have financial ties to the pharmaceutical industry and vaccine manufacturers. On June 27, 2024, ACIP members voted unanimously to recommend 2024-2025 COVID-19 vaccines as authorized or approved by FDA in persons ≥ 6 months of age.53
In conclusion, COVID-19 vaccine safety mechanisms utilized by the CDC/FDA have insurmountable conflicts and biases. The CDC/FDA appear to have unsuccessfully attempted to sanitize VAERS case reports of AEs following COVID-19 vaccination in pregnancy by a variety of techniques described in this study. CDC/FDA attempted to conceal V-safe data that has now been exposed, much to the credit of attorney Aaron Siri and ICAN. Because of the seemingly failed attempts of the government to conceal the disasters of the COVID-19 vaccines, the CDC/FDA appears to be moving to completely closed surveillance systems without transparency and without any “stopping rules”. These systems include VSD, BEST and others. There appears to be conflicts of interest, perhaps even bordering on collusion, between government agencies, government officials like Walensky and Shimabukuro, and private entities such as The Massachusetts Medical Society who owns the NEJM, and the pharmaceutical industry.
In Part III of this series, we will critically review all the published studies involving COVID-19 vaccinations in pregnancy.
Grant/Financial Information
No funding.
Acknowledgements
The authors appreciate and are grateful for the assistance of others: Dr. Michael Deskevich PhD for his guidance and assistance with our mathematical modeling and statistical analysis. Claire Rogers PA-C for her thoughtful review, editing, and research input. Kirstin Cosgrove BM CCRA for her review, editing, and research input. Dr. Stewart Tankersley for his thoughtful review and suggestions.
Conflicts of Interest/Competing Interest
All the authors declare none.
References
- Vargesson N. Thalidomide-induced teratogenesis: History and mechanisms. Wiley Online Library. Birth Defects Research, part C. Embryo Today: Reviews. https://onlinelibrary.wiley.com/doi/full/10.1002/bdrc.21096 (Accessed 6/29/2024). [CrossRef]
- Harold Evans. The Guardian. Thalidomide: How men who blighted lives of thousands evaded justice. November 14, 2014. https://www.theguardian.com/society/2014/nov/14/-sp-thalidomide-pill-how-evaded-justice. (Accessed 6/29/2024).
- National Vaccine Information Center. Search the U.S. Government’s VAERS Data. MedAlerts.org. https://medalerts.org/index.php. (Accessed 6/29/2024).
- Rubin EJ, Baden LR, Walensky Rp, Morrissey S. Audio Interview [April 16, 2021]: Covid-19 Vaccines and pregnancy – A Conversation with CDC Director Rochelle Wallensky. April 21, 2021. N Engl J Med 2021;384:e73. Time Mark for Walensky fear mongering vaccine hesitant pregnant women 16:00-17:10; Time mark for veracity of VAERS and pregnancy surveillance systems by Walensky 7:10-8:20, by Rubin 9:00-9:32, and again by Walensky 11:40-13:20. Time mark for Walensky “very seriously” comment: 7:10-7:22. https://www.nejm.org/doi/full/10.1056/NEJMe2106836 (Accessed 6/29/2024). [CrossRef]
- CDC VAERS Team. Vaccine Adverse Event Reporting System (VAERS) Standard Operating procedures for Covid-19. February 2, 2022. See page 15 of the following document. https://www.cdc.gov/vaccinesafety/pdf/VAERS-COVID19-SOp-02-02-2022-508.pdf. (Accessed 6/29/2024).
- National Vaccine Information Center VAERS database. Listed by year are 138,983 out of 1,640,416 cases with an unknown vaccine date for COVID-19 vaccines. This is from the 5/31/2024 release of VAERS data, MedAlerts.org. https://medalerts.org/vaersdb/findfield.php?TABLE=ON&GROUp1=VACY&EVENTS=ON&VAX%5b%5d=COVID19&VAX%5b%5d=COVID19-2. (Accessed 6/29/2024).
- National Vaccine Information Center VAERS database. Listed by year are 22,834 out of 225,665 cases with an unknown vaccine date for influenza vaccines. This is from the 5/31/2024 release of VAERS data, MedAlerts.org. https://medalerts.org/vaersdb/findfield.php?TABLE=ON&GROUp1=VACY&EVENTS=ON&VAX%5b%5d=FLU(H1N1)&VAX%5b%5d=FLU3&VAX%5b%5d=FLU4&VAX%5b%5d=FLUA3&VAX%5b%5d=FLUA4&VAX%5b%5d=FLUC3&VAX%5b%5d=FLUC4&VAX%5b%5d=FLUN(H1N1)&VAX%5b%5d=FLUN3&VAX%5b%5d=FLUN4&VAX%5b%5d=FLUR3&VAX%5b%5d=FLUR4&VAX%5b%5d=FLUX&VAX%5b%5d=FLUX(H1N1)&VAX%5b%5d=H5N1&VAXTYpES=Influenza (Accessed 6/29/2024).
- National Vaccine Information Center. From the 5/31/2024 release of VAERS data. MedAlerts.org. From the 5/31/2024 release of VAERS data. Listed by year are 31,432 cases where the vaccine type is unknown. MedAlerts.org. https://medalerts.org/vaersdb/findfield.php?TABLE=ON&GROUp1=VACY&EVENTS=ON&VAX%5b%5d=FLU(H1N1)&VAX%5b%5d=FLU3&VAX%5b%5d=FLU4&VAX%5b%5d=FLUA3&VAX%5b%5d=FLUA4&VAX%5b%5d=FLUC3&VAX%5b%5d=FLUC4&VAX%5b%5d=FLUN(H1N1)&VAX%5b%5d=FLUN3&VAX%5b%5d=FLUN4&VAX%5b%5d=FLUR3&VAX%5b%5d=FLUR4&VAX%5b%5d=FLUX&VAX%5b%5d=FLUX(H1N1)&VAX%5b%5d=H5N1&VAXTYpES=Influenza (Accessed 6/29/2024).
- WELCOMETHEEAGLE88. VAERS Unprecedented Throttle Job Continues in New Reports This Week Aug 18th. 42.9% (1252) of “new” reports published Aug 18 were submitted to VAERS in 2021. August 19, 2023. https://welcometheeagle.substack.com/p/vaers-unprecedented-throttle-job (Accessed 6/29/2024).
- Peter Halligan. Monthly C19, VAERS and injection uptake report. November 4, 2023. https://peterhalligan.substack.com/p/monthly-c19-vaers-and-injection-uptake (Accessed 6/29/2024).
- Aravind Mohanoor. How v-safe INCREASED the under-reporting rate for COVID19 vaccines. The case for Vaccine Data Science – part 5. March 21, 2023. https://vaccinedatascience.substack.com/p/how-v-safe-increased-the-under-reporting (Accessed 6/29/2024).
- Covid-19 vaccine 30% Unknown Ages. https://medalerts.org/vaersdb/findfield.php?TABLE=ON&GROUp1=AGE&EVENTS=ON&VAX[]=COVID19&VAX[]=COVID19-2 (Accessed 6/29/2024).
- Unknown state location 16%. https://medalerts.org/vaersdb/findfield.php?TABLE=ON&GROUp1=STA&EVENTS=ON&VAX[]=COVID19&VAX[]=COVID19-2&STATE=NOTFR (Accessed 6/29/2024).
- Covid-19 as concomitant medication, ~282 reports: https://medalerts.org/vaersdb/findfield.php?TABLE=ON&GROUp1=STA&EVENTS=ON&VAX[]=COVID19&VAX[]=COVID19-2&STATE=NOTFR (Accessed 6/29/2024).
- Deleted Reports Dashboard. https://www.vaersaware.com/deleted-reports-2007-2022 (Accessed 6/29/2024).
- Unpublished ID Numbers Dashboard. https://www.vaersaware.com/unpublished-reports-id-s (Accessed 6/29/2024).
- BNT162b2 5.3.6 Cumulative Analysis of post-authorization Adverse Event Reports. https://phmpt.org/wp-content/uploads/2022/04/reissue_5.3.6-postmarketing-experience.pdf (Accessed 6/29/2024).
- Celia Farber. Court-Ordered Pfizer Documents They Tried To Have Sealed For 55 years Show 1223 Deaths, 158,000 Adverse Events in 90 Days post EUA Release. The Most Shocking Document Release Of The Last 100 years. December 5, 2021. https://celiafarber.substack.com/p/court-ordered-pfizer-documents-they (Accessed 6/29/2024).
- Michelle Maluske. CTV News. ‘Data is power’: Experts weigh-in on court-ordered release of Pfizer vaccine documents. March 11, 2022. https://windsor.ctvnews.ca/data-is-power-experts-weigh-in-on-court-ordered-release-of-pfizer-vaccine-documents-1.5816089 (Accessed 6/29/2024) Maggie M.
- Thorp MM. Jim Thorp MD. Tentacles of a Covert and Exploitative Propaganda Machine Compliments of the US Government America Out Loud October 28, 2022. Tentacles of a Covert and Exploitative Propaganda Machine Compliments of the US Government - America Out Loud (Accessed 6/29/2024).
- Thorp MM, Thorp JA. Government Curated ‘Science’: Corporate Lies, Greed and Human Destruction. America Out Loud December 11, 2022. Government Curated 'Science': Corporate Lies, Greed and Human Destruction - America Out Loud.
- Thorp MM, Thorp JA. FOIA Reveals Troubling Relationship between HHS/CDC & The American College of Obstetricians and Gynecologists. May 7, 2023. https://www.americaoutloud.news/foia-reveals-troubling-relationship-between-hhs-cdc-the-american-college-of-obstetricians-and-gynecologists/ (Accessed 6/29/2024).
- Thorp MM, Thorp JA. COVID-19 Government Relief Funds Turned the Healthcare Industry on Its Head. December 10, 2023. America Out Loud. https://www.americaoutloud.news/covid-19-government-relief-funds-turned-the-healthcare-industry-on-its-head/ (Accessed 6/29/2024).
- Thorp MM, Thorp JA. The Government Cartel paid billions to Walgreens and CVS not to fill Ivermectin – the question is why. May 20, 2024. America Out. https://www.americaoutloud.news/the-government-cartel-paid-billions-to-walgreens-and-cvs-not-to-fill-ivermectin-the-question-is-why/ (Accessed 6/29/2024).
- Thorp MM, Thorp JA. US Government coerced leaders of faith to push COVID-19 vaccines on Americans. January 14, 2024. America Out Loud https://www.americaoutloud.news/us-government-coerced-leaders-of-faith-to-push-covid-19-vaccines-on-americans/ (Accessed 6/29/2024).
- The NEW ENGLAND JOURNAL of MEDICINE. About NEJM: Policies and Practices. https://www.nejm.org/about-nejm/about-nejm#:~:text=Our%20mission%20is%20to%20publish,practice%20and%20improve%20patient%20outcomes (Accessed 6/29/2024).
- AWARD PROFILE Grant Summary Cooperative Agreement FAIN NU90TP92206. Awarding Agency Department of Health and Human Services (HHS) and Recipient: MASSACHUSETTS DEPARTMENT OF PUBLIC HEALTH. Total Awarded Amount. $329.0 Million. https://www.usaspending.gov/award/ASST_NON_NU90TP922006_7523.
- Shimabukuro TT, Kim SY, Myers TR, Moro PL. et al. Preliminary Findings of mRNA Covid-19 Vaccine Safety in Pregnant Persons. April 21, 2021, N Engl J Med 2021;384:2273-2282. https://www.nejm.org/doi/full/10.1056/nejmoa2104983 (Accessed 6/29/2024). [CrossRef]
- Thorp KE, Thorp MM, Thorp EM, Thorp JA. COVID-19 & Disaster Capitalism – Part I. G Med Sci. 2022; 3(1):159-178. See pages 170-171 documenting the data manipulation revealing 82% miscarriage rate in the Shimabukuro article. https://www.doi.org/10.46766/thegms.medethics.22071901 (Accessed 6/29/2024). [CrossRef]
- Thorp MM, Thorp JA. Pushing COVID-19 Shots in Pregnancy: The Greatest Ethical Breach in the History of Medicine. America Out Loud News. February 12, 2023. https://www.americaoutloud.news/pushing-covid-19-shots-in-pregnancy-the-greatest-ethical-breach-in-the-history-of-medicine/ (Accessed 6/29/2024).
- Pineles BL, Goodman KE, Pineles L, O'Hara LM; et al. In-Hospital Mortality in a Cohort of Hospitalized Pregnant and Nonpregnant Patients With COVID-19. Ann Intern Med. 2021 Aug;174(8):1186-1188. Epub 2021 May 11. PMID: 33971101; PMCID: PMC8251936. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8251936/ (Accessed 6/29/2024). [CrossRef]
- Knight M, Ramakrishnan R, Bunch K; et al. Females in hospital with SARS-CoV-2 infection, the association with pregnancy and pregnancy outcomes: A UKOSS/ISARIC/CO-CIN investigation. Scientific Advisory Group for Emergencies; 2021. https://pubmed.ncbi.nlm.nih.gov/32513659/ (Accessed June 29, 2024).
- Metz TD, Clifton RG, Hughes BL, et al; Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) Maternal-Fetal Medicine Units (MFMU) Network. Disease severity and perinatal outcomes of pregnant patients with coronavirus disease 2019 (COVID-19). Obstet Gynecol. 2021;137:571-580. [PMID:] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7984765/ (Accessed 6/29/2024). [CrossRef]
- Food and Drug Administration (FDA). FDA Docket Number FDA-2022-N-2810. “178th Meeting of the Vaccines and Related Biological Products Advisory Committee (VRBPAC)” (recorded live broadcast). Posted on YouTube, January 26, 2023. Accessed February 6, 2023 (cited material located at 6:58:32 – 6:59:42). https://www.fda.gov/advisory-committees/advisory-committee-calendar/vaccines-and-related-biological-products-advisory-committee-january-26-2023-meeting-announcement (Accessed 6/29/2024).
- CDC Newsroom. FDA and CDC Response to the Florida Surgeon General. March 10, 2023. https://www.cdc.gov/media/releases/2023/p0313-letter.html (Accessed 6/16/2024). (Accessed 6/29/2024).
- CDC Vaccine Safety. Clinical Immunization Safety Assessment (CISA) Project. Vaccine Safety Monitoring – CISA. https://www.cdc.gov/vaccinesafety/ensuringsafety/monitoring/cisa/index.html#anchor_1580313832826 (Accessed 6/29/2024).
- Johns Hopkins BLOOMBERG SCHOOL of PUBLIC HEALTH. What VAERS Is [And Isn’t]. May 3, 2022. https://publichealth.jhu.edu/2022/what-vaers-is-and-isnt (Accessed 6/29/2024).
- Nietzel MT. Top 20 Universities For NIH Funding; Johns Hopkins Ranks First Again. February 10, 2024. https://www.forbes.com/sites/michaeltnietzel/2024/02/10/top-20-universities-for-nih-funding-johns-hopkins-ranks-first-again/?sh=2ea1fcb4e25d (Accessed 6/29/2024).
- Clinical Immunization Safety Assessment (CISA) Current CISA Project Sites. https://www.cdc.gov/vaccinesafety/ensuringsafety/monitoring/cisa/index.html#anchor_1580313832826 (Accessed 6/29/2021).
- USASPENDING.gov. RECIPIENT PROFILE THE JOHNS HOPKINS UNVERSITY. https://www.usaspending.gov/recipient/e895f676-c226-223f-b5ed-dda80c2ec73a-C/latest (Accessed 6/29/2024).
- Thorp MM, Thorp JA. VAERS – The Last Bastion of Vaccine Free Speech? June 9, 2023. https://www.americaoutloud.news/vaers-the-last-bastion-of-vaccine-free-speech-2/ (Accessed 6/29/2024).
- Vaccine Safety Database (VSD). 2021. “Rapid Cycle Analysis (RCA) to Monitor the Safety of COVID-19 Vaccines in Near Real-Time with the Vaccine Safety Data Link,” Project #1342, Version 1.1, March 3, 2021, p. 14. Accessed May 31, 2023. https://www.cdc.gov/vaccinesafety/pdf/VSD-1342-COVID19-RCA-Protocol_FinalV1.1_508.pdf. (Accessed 6/29/2024).
- Centers for Disease Control and prevention (CDC). (2024.) “Historical Vaccine Safety Concerns: Swine Flu and Guillain Barré Syndrome – 1976” (following small increased risk of Guillain Barré Syndrome (GBS), which was 1 case for every 100,000 people who received the vaccine, federal officials determined that the possibility of an association of GBS with the vaccine necessitated pausing immunization) https://www.cdc.gov/vaccinesafety/concerns/concerns-history.html (Accessed 6/29/2024).
- Centers for Disease Control and prevention (CDC). (2024.) “Historical Vaccine Safety Concerns: Rotovirus Vaccine and Intussusception – 1988-1999” (following some infants experiencing a rare type bowel obstruction know as intussusception following vaccination, CDC recommended use of the vaccine be suspended in lieu of emergency investigations to determine whether the vaccine was the actual mechanism of causation). https://www.cdc.gov/vaccinesafety/concerns/concerns-history.html (Accessed 6/29/2024).
- Aaron Siri. V-Safe part 1: After 464 Days, CDC Finally Coughed up Covid-19 Vaccine Safety Data Showing 7.7% of people Reported Needing Medical Care. First part of an incredible story that shows just how broken our public “health” apparatus is: Very, very broken. https://aaronsiri.substack.com/p/v-safe-part-1-after-464-days-cdc?utm_source=profile&utm_medium=reader2 (Accessed 6/29/2024).
- Comingled V-Safe and VAERS Reports. https://medalerts.org/vaersdb/findfield.php?TABLE=ON&GROUp1=AGE&EVENTS=ON&CUSTOMSQL=SpLIT+%3D+VSAFE (Accessed 6/29/2024).
- VAERS children age 0-17years. https://medalerts.org/vaersdb/findfield.php?TABLE=ON&GROUp1=AGE&EVENTS=ON&VAX[]=COVID19&VAX[]=COVID19-2&WhichAge=range&LOWAGE=0&HIGHAGE=17.99 (Accessed 6/29/2024).
- WelcomeTheEagle Substack. VaersAware.com. VAERS Dashboard age 0-17 https://www.vaersaware.com/entire-vaers-1990-current (Accessed 6/19/2024) ICAN Informed Consent Action Network. Fourth VSAFE PRODUCTION REVEALS A DISTURBING TREND IN MISCARRIAGES AND MENSTRUAL DISTURBANCES FOLLOW COVID-19 VACCINATION. June 18, 2024. https://icandecide.org/press-release/fourth-v-safe-production-reveals-a-disturbing-trend-in-miscarriages-and-menstrual-disturbances-following-covid-19-vaccination/ (Accessed 6/29/2024).
- Aaron Siri. V-Safe part 10: Federal Judge Orders CDC to Make public 7.8 Million V-safe Free-Text Entries within 12 Months. Tenth part of an incredible story that shows just how broken our public “health” apparatus is: Very, very broken. https://aaronsiri.substack.com/p/v-safe-part-10-federal-judge-orders (Accessed 6/29/2024).
- ICAN Informed Consent Action Network. FOURTH V-SAFE PRODUCTION REVEALS ADISTURBING TREND IN MISCARRIAGES AND MENSTRUAL DISTURBANCES FOLLOWING COVID-19 VACCINATIOIN. Juine 18, 2024 https://icandecide.org/press-release/fourth-v-safe-production-reveals-a-disturbing-trend-in-miscarriages-and-menstrual-disturbances-following-covid-19-vaccination/ (Accessed 6/29/2024).
- New Tranche of VSAFE DROPPED Today (4th Installment of Free-text) Many deaths now documented in the “Free Text” field of the new V-safe data. June 19, 2024. https://welcometheeagle.substack.com/p/new-tranche-of-vsafe-dropped-today (Accessed 6/29/2024).
- ICAN. CDC STACKS ITS VACCINE COMMITTEE WITH PHARMA-AFFILIATED MEMBERS AHEAD OF JUNE 2024 VOTE ON COVID-19 VACCINES. June 14, 2024. https://icandecide.org/press-release/cdc-stacks-its-vaccine-committee-with-pharma-affiliated-members-ahead-of-june-2024-vote-on-covid-19-vaccines/ (Accessed 6/29/2024).
- The ACIP voting members voted YES unanimously on June 27, 2024 to recommend 2024-2025 COVID-19 vaccines as authorized or approved by FDA in persons ≥ 6 months of age. Advance to Timestamp 8:47:40. https://mail.proton.me/u/0/inbox/5OQkV3P7hA3c-280S3lCKWyoQBXhRXaRAuiaOGxKH2z2TB3I2x6B4wewTZlbGfz7TI6O2IV-6iQX_vcYMfeUXA== (Accessed 6/29/2024).
Figure 1.
Unknown vaccine type by year is depicted. This is yet another area where many COVID-19 reports exist but are unaccounted for. As noted in this graph, “unknown vaccine type” has exponentially increased at the onset of Covid vaccination in December, 2020.
Figure 1.
Unknown vaccine type by year is depicted. This is yet another area where many COVID-19 reports exist but are unaccounted for. As noted in this graph, “unknown vaccine type” has exponentially increased at the onset of Covid vaccination in December, 2020.
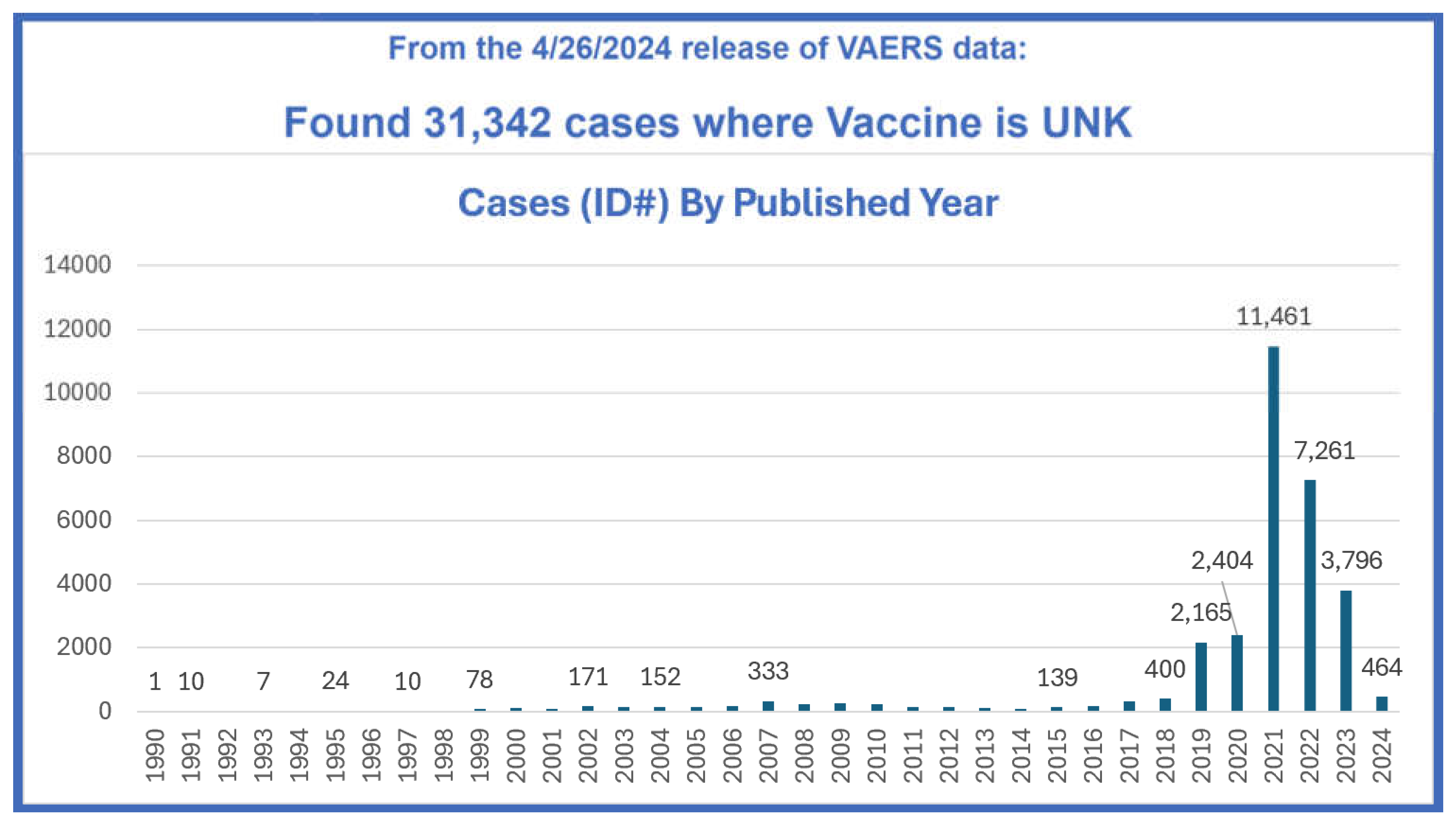
Figure 2.
The money trail from the U.S. Department of Health and Human Services (HHS), through the Massachusetts Department of Public Health, to the Massachusetts Medical Society, the owner of the NEJM. There appears to be a corporate kleptocratic entanglement among the government, Walensky, Shimabukuro, Eric Rubin and the Massachusetts Medical Society.
Figure 2.
The money trail from the U.S. Department of Health and Human Services (HHS), through the Massachusetts Department of Public Health, to the Massachusetts Medical Society, the owner of the NEJM. There appears to be a corporate kleptocratic entanglement among the government, Walensky, Shimabukuro, Eric Rubin and the Massachusetts Medical Society.
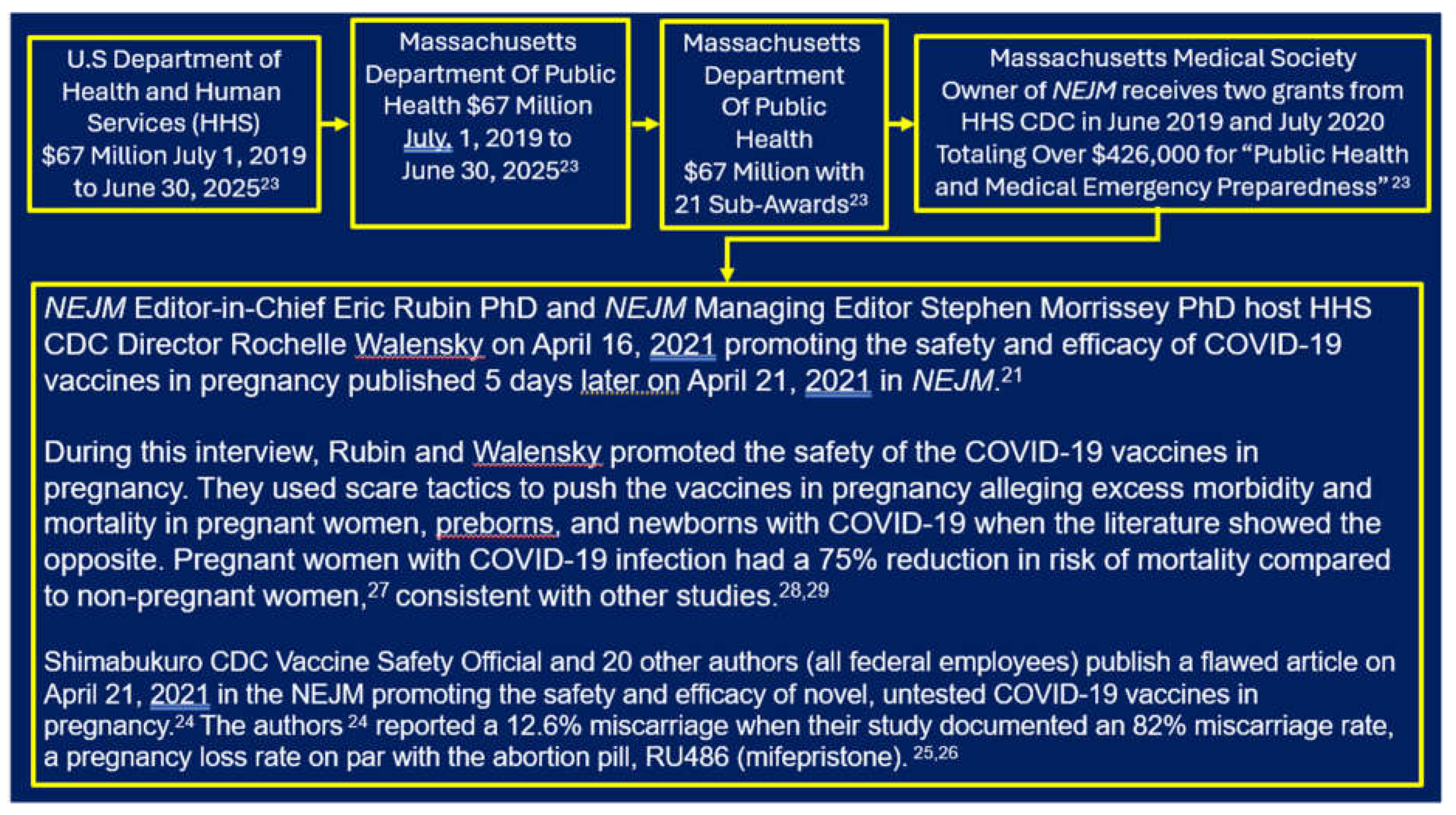

Table 1.
Thirty-seven pregnancy-related adverse events (AEs) were investigated in this study, 27 were antepartum AEs and 10 were postpartum/newborn AEs. The AEs are depicted in Column 1 and the actual MedAlert’s “symptoms” extracted are listed in Column 2. Noteworthy is that the U.S. CDC/FDA VAERS lists these complications in British spelling. Column 3 lists the raw data of AEs depicted as follows: COVID-19 vaccines / Influenza vaccines / All other vaccines except COVID-19.
Table 1.
Thirty-seven pregnancy-related adverse events (AEs) were investigated in this study, 27 were antepartum AEs and 10 were postpartum/newborn AEs. The AEs are depicted in Column 1 and the actual MedAlert’s “symptoms” extracted are listed in Column 2. Noteworthy is that the U.S. CDC/FDA VAERS lists these complications in British spelling. Column 3 lists the raw data of AEs depicted as follows: COVID-19 vaccines / Influenza vaccines / All other vaccines except COVID-19.
| Adverse Event | MedAlerts “Symptoms” Utilized | Adverse Events Raw Data Expressed as COVID-19 Vaccines / Influenza Vaccines / All Other Vaccines |
|---|---|---|
| Miscarriage (spontaneous abortion) | “abortion missed” or “abortion spontaneous” or “abortion spontaneous complete” or “abortion spontaneous complicated” or “abortion spontaneous incomplete” | 3494 / 315 / 936 |
| Fetal chromosome abnormality | “foetal chromosome abnormality” | 17 / 0 / 2 |
| Fetal malformation | “foetal cystic hygroma” or “foetal malformation” or “foetal megacystis” | 40 / 2 / 8 |
| Cervical insufficiency | “cervical incompetence” | 10 / 2 / 9 |
| Premature rupture of membranes | “premature rupture of membranes” | 114 / 14 / 53 |
| Premature labor | “premature labour” | 189 / 53 / 223 |
| Premature delivery | “premature baby” or “premature delivery” |
404 / 142 / 356 |
| Placental calcification | “placental calcification” | 5 / 0 /2 |
| Placental infarction | “placental infarction” | 8 / 0 / 2 |
| Placental thrombosis | “foetal placental thrombosis” | 6 / 0 / 0 |
| Placenta accreta | “placenta accreta” | 3 / 0 / 0 |
| Placental abruption | “premature separation of placenta” | 90 / 14 / 44 |
| Placental insufficiency | “placental insufficiency” | 24 / 0 / 2 |
| Placental disorder | “placental disorder” | 41 / 17 / 55 |
| Fetal-maternal hemorrhage | “foetal maternal hemorrhage” | 7 / 1 / 1 |
| Fetal growth restriction | “foetal growth abnormality” | 21 / 0 / 1 |
| Reduced amniotic fluid volume | “amniotic fluid index decreased” or “amniotic fluid volume decreased” | 17 / 1 / 11 |
| Preeclampsia | “pre-eclampsia” | 147 / 26 / 96 |
| Fetal heart rate abnormality | “foetal heart rate abnormal” or “foetal heart rate acceleration abnormal” or “foetal heart rate deceleration” or “foetal heart rate deceleration abnormal” or “foetal heart rate decreased” or “foetal heart rate disorder” or “foetal heart rate increased” or “foetal heart rate indeterminate” | 228 / 48 / 94 |
| Fetal cardiac disorder | “foetal cardiac disorder” | 22 / 4 / 8 |
| Fetal vascular malperfusion | “foetal vascular malperfusion | 19 / 0 / 0 |
| Fetal arrhythmia | “foetal arrhythmia” | 10 / 0 / 0 |
| Fetal distress | “foetal distress syndrome” | 18 / 6 / 27 |
| Fetal biophysical profile abnormal | “foetal biophysical profile abnormal” | 4 / 0 / 0 |
| Hemorrhage in pregnancy | “haemorrhage in pregnancy” | 164 / 7 / 25 |
| Fetal cardiac arrest | “foetal cardiac arrest” | 21 / 2 / 2 |
| Fetal death (stillbirth) | “foetal death” or “stillbirth” | 477 / 68 / 175 |
| Prematue infant death | “premature baby death” | 12 / 0 / 1 |
| Neonatal asphyxia | “neonatal asphyxia” | 8 / 0 / 3 |
| Neonatal dyspnea | “neonatal dyspnea” | 13 / 0 / 1 |
| Neonatal infection | “neonatal infection” | 5 / 0 / 4 |
| Neonatal hemorrhage | “haemorrhage neonatal” | 4 / 0 / 0 |
| Neonatal insufficient breast milk | “neonatal insufficient breast milk” | 10 / 0 / 0 |
| Neonatal pneumonia | “neonatal pneumonia” | 4 / 0 / 1 |
| Neonatal respiratory distress | “neonatal respiratory distress” | 12 / 0 / 7 |
| Neonatal respiratory distress syndrome | “neonatal respiratory distress syndrome” | 12 / 0 / 23 |
| Neonatal seizure | “neonatal seizure” | 7 / 0 / 6 |
Table 2.
The first two columns are from Table 1. All data of AEs are depicted as follows: COVID-19 vaccines / Influenza vaccines / All other vaccines except COVID-19. Column 3 depicts the unconcealed raw data that was missed from Column 1 due to unknown vaccine type status in VAERS. Column 4 depicts the percent of unconcealed data relative to the original raw data from Column 1.
Table 2.
The first two columns are from Table 1. All data of AEs are depicted as follows: COVID-19 vaccines / Influenza vaccines / All other vaccines except COVID-19. Column 3 depicts the unconcealed raw data that was missed from Column 1 due to unknown vaccine type status in VAERS. Column 4 depicts the percent of unconcealed data relative to the original raw data from Column 1.
| Adverse Event | Original Adverse Events Raw Data COVID-19 / Influenza / All Other Vaccines | Unconcealed Adverse Events Raw Data COVID-19 / Influenza / All Other Vaccines | Percent of Original Raw Data Concealed COVID-19 / Influenza / All Other Vaccines |
|---|---|---|---|
| Miscarriage (spontaneous abortion) | 3494 / 315 / 936 | 393 / 64 / 280 | 11% / 20% / 30% |
| Fetal chromosome abnormality | 17 / 0 / 2 | 1 / 0 / 2 | 6% / 0% / 100% |
| Fetal malformation | 40 / 2 / 8 | 6 / 0 / 3 | 15% / 0% / 38% |
| Cervical insufficiency | 10 / 2 / 2009 | 10 / 2 / 2011 | 0% / 0% / 22% |
| Premature rupture of membranes | 114 / 14 / 53 | 2 / 5 / 13 | 2% / 36% / 25% |
| Premature labor | 189 / 53 / 223 | 10 / 7 / 44 | 5% / 13% / 20% |
| Premature delivery | 404 / 142 / 356 | 36 / 74 / 245 | 9% / 52% / 69% |
| Placental calcification | 5 / 0 /2 | 5 / 0 / 2 | 0% / 0% / 0% |
| Placental infarction | 8 / 0 / 2 | 10 / 0 / 2 | 25% / 0% / 0% |
| Placental thrombosis | 6 / 0 / 0 | 6 / 0 / 0 | 0% / 0% / 0% |
| Placenta accreta | 3 / 0 / 0 | 3 / 0 / 0 | 0% / 0% / 0% |
| Placental abruption | 90 / 14 / 44 | 116 / 19 / 66 | 29% / 36% / 50% |
| Placental insufficiency | 24 / 0 / 2 | 27 / 0 / 3 | 13% / 0% / 50% |
| Placental disorder | 41 / 17 / 55 | 44 / 17 / 74 | 7% / 0% / 35% |
| Fetal-maternal hemorrhage | 7 / 1 / 1 | 7 / 1 / 1 | 0% / 0% / 0% |
| Fetal growth restriction | 21 / 0 / 1 | 23 / 0 / 2 | 10% / 0% / 100% |
| Reduced amniotic fluid volume | 17 / 1 / 11 | 18 / 3 / 13 | 6% / 200% / 18% |
| Preeclampsia | 147 / 26 / 96 | 160 / 29 / 123 | 9% / 12% / 28% |
| Fetal heart rate abnormality | 228 / 48 / 94 | 240 / 49 / 112 | 5% / 2% / 19% |
| Fetal cardiac disorder | 22 / 4 / 8 | 28 / 4 / 14 | 27% / 0% / 75% |
| Fetal vascular malperfusion | 19 / 0 / 0 | 21 / 0 / 0 | 11% / 0% / 0% |
| Fetal arrhythmia | 10 / 0 / 0 | 10 / 0 / 1 | 0% / 0% / 1 |
| Fetal distress | 18 / 6 / 27 | 20 / 9 / 39 | 11% / 50% / 44% |
| Fetal biophysical profile abnormal | 4 / 0 / 0 | 4 / 0 / 1 | 0% / 0% / NA |
| Hemorrhage in pregnancy | 164 / 7 / 25 | 10 / 2 / 5 | 6% / 29% / 20% |
| Fetal cardiac arrest | 21 / 2 / 2 | 1 / 0 / 0 | 5% / 0% / 0% |
| Fetal death (stillbirth) | 477 / 68 / 175 | 562 / 107 / 287 | 18% / 57% / 64% |
| Premature infant death | 12 / 0 / 1 | 12 / 0 / 1 | 0% / 0% / 0% |
| Neonatal asphyxia | 8 / 0 / 3 | 8 / 1 / 7 | 0% / 0% / 133% |
| Neonatal dyspnea | 13 / 0 / 1 | 18 / 0 / 1 | 38% / 0% / 0% |
| Neonatal infection | 5 / 0 / 4 | 5 / 0 / 8 | 0% / 0% / 100% |
| Neonatal hemorrage | 4 / 0 / 0 | 4 / 0 / 0 | 0% / 0% / 0% |
| Neonatal insufficient breast milk | 10 / 0 / 0 | 12 / 0 / 0 | 20% / 0% / 0% |
| Neonatal pneumonia | 4 / 0 / 1 | 4 / 1 / 2 | 0% / 1 / 100% |
| Neonatal respiratory distress | 12 / 0 / 7 | 14 / 0 / 8 | 17% / 0% / 14% |
| Neonatal respiratory distress syndrome | 12 / 0 / 23 | 12 / 0 / 30 | 0% / 0% / 30% |
| Neonatal seizure | 7 / 0 / 6 | 7 / 0 / 6 | 0% / 0% / 0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



