
Submitted:
27 June 2024
Posted:
28 June 2024
You are already at the latest version
Abstract
Future healthcare professionals can play a significant role in managing those with
thoughts of suicide. This scoping review aims to determine healthcare students’ knowledge and attitude towards suicide. A systematic search was conducted across five databases: PubMed, CINAHL, EMBASE, PsycINFO, Cochrane, and DARE. Only primary studies written in English, from database inception until 31st December 2023 were included. A total of 44 studies were included. Overall, healthcare students demonstrated low to moderate confidence in managing patients with thoughts of suicide and low levels of relevant education despite acknowledging their importance in preventing suicide. Increased personal exposure to suicide was associated with increased suicide literacy, confidence in managing patients with thoughts of suicide, and reduced stigma. Demographics and culture were shown to affect knowledge and attitude as well. Further research is needed to better understand various contributing factors to healthcare students’ knowledge and attitude regarding suicide. Evaluating healthcare curricula should be considered to implement effective suicide training program.
Keywords:
suicide
; healthcare
; students
; attitudes
; training
1. Introduction
According to the World Health Organisation (WHO), suicide has led to the death of 703 000 people globally every year [1]. It was found to be the fourth cause of mortality among 15-30 year-olds and 77% of suicide was reported to occur in low and middle income countries [1]. Due to stigma, legal, and cultural factors, deaths due to suicide are likely underreported and thus the actual prevalence of suicide might be underestimated[2]. Suicide attempts may results in emotional, physical, and economical consequences in individuals and their loved ones [3]. A systemic review reported that suicide-bereaved individuals experience more rejection, stigma, blame, and shame compared to other bereaved groups [4]. In addition, the economic impact of suicide is estimated to be $5.53 billion annually [5]. Given suicide’s public health significance and its preventable nature, the WHO has identified suicide as a serious public health concern [6] and published a report in 2014 to further boost public health awareness around it [7].
Healthcare providers play a crucial role in identifying and preventing suicide. It was found that 44% of individuals visited their physicians a month before they completed suicide [8], however, only 3% of them had their complaints diagnosed as a mental health issue [9]. Indeed, patients reported they had received inappropriate and depersonalized responses with minimal empathy when they talked about suicide [10]. Meanwhile, the management of persons with thoughts of suicide is often impeded by legal, knowledge, emotional, communication, and logistic difficulties [11,12,13]. As a result, clinicians often hold attitudes of avoidance when dealing with suicide attempters, which has led to low-quality, superficial, and inadequate care [14,15]. In addition, a scoping review reported that pharmacists’ role in suicide prevention was affected by barriers, either personal e.g. lack of confidence, training, knowledge; or institutional e.g. work pressure, lack of time or privacy, nonavailability of resources and referral pathways [16]. This has then resulted in persons with thoughts of suicide often refusing to express themselves or seek help from available resources [10].
Based on the assumption that the behaviour of a person is based on their attitude [17], it is important to assess the attitudes of future healthcare providers. Studies indicate that primary care and community pharmacies are the most visited services by individuals prior to suicide, thus it gives these professionals the opportunity to identify individuals with suicidal ideation or those having a mental health crisis [18,19]. Besides, knowledge of suicide should be evaluated as well to ensure continuous systemic improvement in suicide management and health equity [20]. Future healthcare educational curricula that better fulfil public health need could be designed [21] to respond to the WHO’s call to reduce suicide rate by one third by the year 2030 [1]. This scoping review aims to summarize data from the available literature to provide an overview of healthcare students’ knowledge of and attitudes towards suicide and identify gaps as well as interventions needed.
2. Materials and Methods
2.1. Data Sources and Search Strategies
This scoping review followed the methodology outlined by Arksey and O’Malley [22]. Reporting for this review was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Statement for Scoping Reviews (PRISMA-ScR)[23] ((Supplementary Table S1).
Search terms related to “healthcare students”, “knowledge and attitude”, and “suicide” were developed based on the study objectives and a review of the literature, and then further refined after a discussion with the university librarian, as well as among the researchers. Based on the finalized list, a systematic search was performed in the following databases: PubMed, Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials (CENTRAL), Cumulative Index to Nursing and Allied Health Literature (CINAHL), Excerpta Medica dataBASE (EMBASE), PsycINFO, and Database of Abstracts of Review of Effects (DARE). The full search strategy is listed in Appendix A. Only primary studies written in English from database inception until 31st December 2023 were included in our review. A manual search was undertaken to identify additional studies from references cited in retrieved articles and a free-hand search was also undertaken via Google Scholar.
All articles obtained from the search were imported into EndNote 20 before being uploaded to Covidence for further screening. After removal of duplicates, two researchers screened the title and abstract of the studies independently (Level 1 screening). The full texts of articles deemed possibly suitable based on the inclusion and exclusion criteria were then reviewed independently by the two researchers (Level 2 screening). Any conflicts that arose were resolved by discussion among the screening researchers, and where consensus could not be reached, the lead researcher (SAJ) was consulted. Ethical approval was not needed for this study as it did not involve human subjects.
2.2. Study Selection
Studies that evaluated the attitude and/ or knowledge of suicide of healthcare students from programmes such as medicine, nursing, pharmacists, dentistry, and allied health such as paramedics, oral health therapists, and dental therapists, were included. The following were excluded: (i) studies that involved healthcare students who had special training in psychiatry such as psychiatric trainees, psychology students, mental health nurses, and midwives, (ii) studies that only evaluated healthcare students’ suicide rate and suicidality, (iii) studies that evaluated healthcare students’ attitude and/ or knowledge on physician-assisted suicide, (iv) studies with outcomes that were not specific, such as the attitudes towards both depression and suicide, (v) in studies where evaluation of an intervention was the focus, pre-test attitudes or knowledge assessments were unavailable, (vi) reviews, systematic reviews, meta-analyses, conference abstracts, conference proceedings, in vivo studies, in vitro studies, animal studies, thesis, and letter to editors, (vii) studies that were not in English, and (viii) studies where abstracts and full texts were not available.
2.3. Data Extraction
Two researchers developed a data extraction sheet specific for the review that included the following details: (1) author, year of publication and the country where the study was conducted, (2) study characteristics including objectives, method, sample size, and study instruments, (3) population demographics including gender, age, study programs undertaken and year of study, (4) outcomes including knowledge and attitudes, and (5) personal experience of suicide and mental health issues. The sheet was pilot tested by two researchers on two articles that were to be included in the scoping review. Further changes were made as appropriate to produce the finalized version. Two researchers then independently undertook the data extraction.
2.4. Data Analysis
Thematic narrative analysis was performed guided by Braun and Clarke [24] to develop themes from the included papers. Results were presented in tabular format and common themes were identified.
3. Results
3.1. Study Search
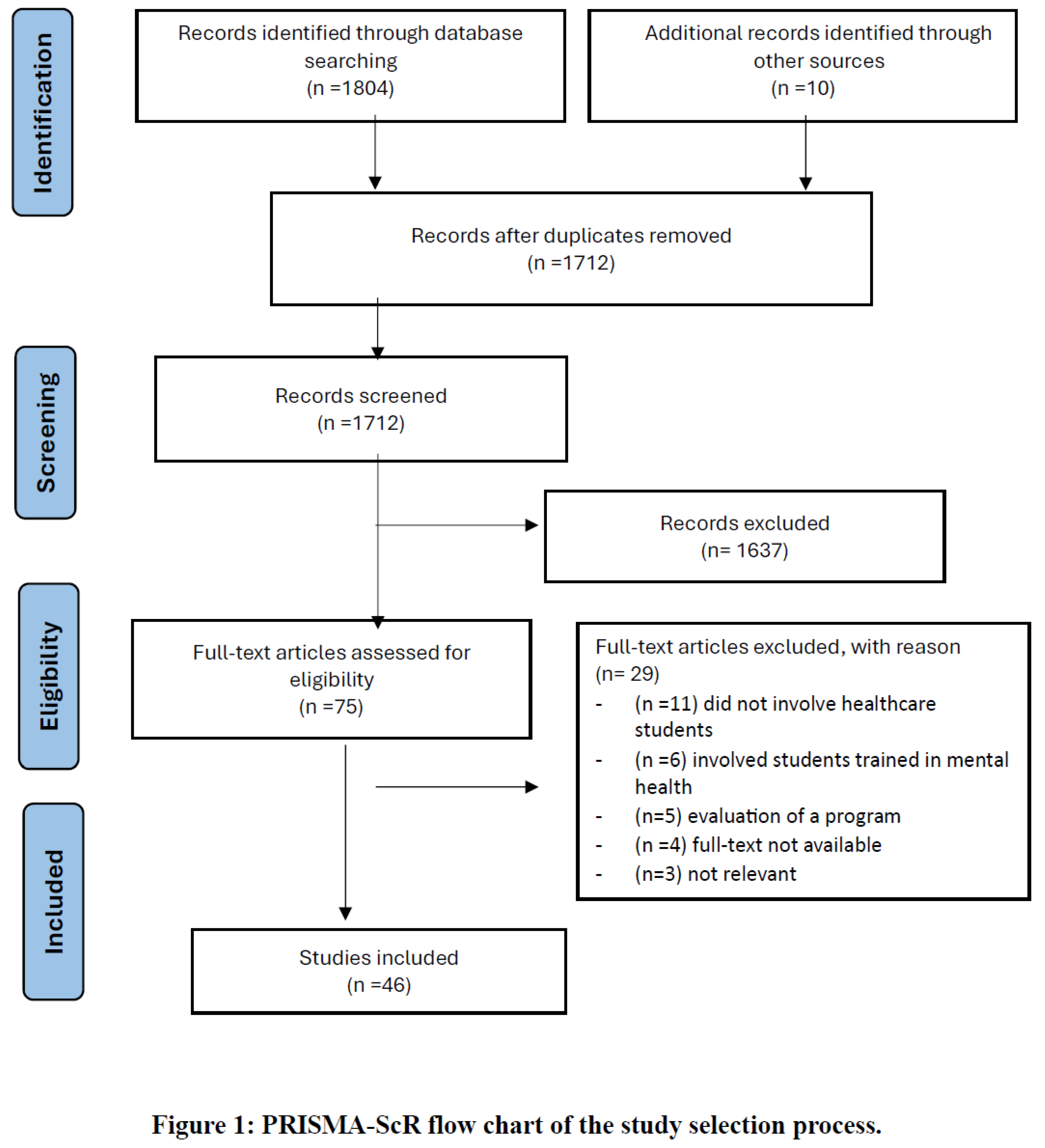
The database search yielded 1804 articles, while the manual search of the reference lists of potentially relevant articles yielded 10 additional studies as in Figure 1. After exclusion of duplicates and Level 1 screening, 46 articles were included for final analysis where 29 were excluded for the following reasons: did not involve healthcare students or no data specific to healthcare students available (n=11), involved healthcare students trained in mental health (n=6), full texts not available (n=4), studies evaluated post-educational programme findings of interest without pre-programme findings reported (n=5), study involved physician-assisted suicide (n=1) or was not related to suicide (n=1), and one study had no separation of results between depression and suicide. Characteristics of the included studies are detailed in Table 1.
3.2. Study Characteristics
Where reported, the studies included a total of 8094 pre-clinical and clinical healthcare students, with around 65% of them being females and the mean age was 22.0 years old. Data was obtained from various countries, including the United States (US) (n=12) [34,50,51,52,58,67,69,70,84,85,87,89,91,95], Australia (n=5) [46,49,53,65,68], Brazil (n=4) [28,35,37,43], Turkey (n=4) [26,38,71,80], Taiwan (n=3) [59,78,82], India (n=3) [41,74,77], Austria (n=2) [26,74], Japan (n=2)[57,70], and one study each from the United Kingdom (UK) [32], Italy [27], Greece [30], Mexico [36], Bangladesh [44], Nepal [45], Portugal [60], Malaysia [61], Sweden [76], Serbia [79], and Hong Kong [90]. Three studies compared attitudes across different cultures i.e. between American and Japanese students [70], Austrian and Turkish students [26], and Austrian and Indian students [74]. Most studies focused on medical (n=24)[25,26,30,34,36,44,46,49,50,52,53,57,61,68,69,70,71,74,76,79,80,85,89,90] and nursing (n=17)[27,28,35,36,37,38,41,43,45,58,59,60,65,67,77,78,82] students, and a small number on pharmacy (n=5) [51,84,87,91,95], dental (n=1)[32], and paramedic (n=1)[65] students. Data collection was mostly through self-reported surveys incorporating validated or unvalidated questionnaires (n=39)[25,26,27,28,30,32,35,37,38,41,44,45,46,49,50,51,52,53,57,61,65,68,69,70,71,74,76,77,79,80,82,84,85,87,89,90,91,95,99] and interviews (n=8)[34,43,58,59,60,67,68,78]. The majority of studies were published after 2013 (n=33),[25,27,28,30,32,35,36,37,38,41,43,44,45,46,49,51,53,58,59,60,61,65,67,69,77,78,84,85,87,89,90,91,95] and about 50% of the studies (n=25)[25,26,27,28,30,36,37,38,41,45,51,53,60,61,70,74,76,77,78,82,84,87,90,91,95] collected information on personal exposure to suicide or mental health issues.
3.3. Key Findings
Two main themes were developed: (1) knowledge on and skills to manage suicide, and (2) attitude towards suicide. These themes and subthemes are illustrated below.
Theme 1: Knowledge on and skills to manage suicide
Subtheme 1: Skills in managing persons with thoughts of suicide. Six studies involving medical [52,68], nursing [58,59,78], and pharmacy [91] students discussed students’ management skills encompassing suicide risk assessment, identifying those at risk, communicating, and dealing with persons with thoughts of suicide. The skills of the students could be described on a spectrum, whereby some students described themselves as having inadequate skills [58,68,78], while others had high skills [52,58,59,91]. It was noted that skills could be improved over time with increasing contact between clinical staff and persons with thoughts of suicide [59,78]. A study by Neimeyer et al [52] found that among medical students, female gender (p<0.00025), senior students (p<0.029) and those completing inpatient psychiatry rotations (p<0.0004) were significantly associated with better skills than their peers.
Subtheme 2: Knowledge of suicide. Seven studies involving medical [44,46,57], nursing [27], and pharmacy [84,91,95] students evaluated the overall knowledge of students. It was noted that students from developed countries such as Italy [27], Australia [46], Japan [57], and the US [84,91,95] were moderately knowledgeable as compared to their counterparts in Bangladesh who had poor suicide literacy [44]. Several factors that were associated with better knowledge were presence of lifetime suicidal ideation (p =0.020),[27] female gender [44,79], personal or family history of suicide attempts [44], those who attributed suicidal ideation to isolation or depression (p= 0.007), undergraduates (p<0.001), native English speakers (p<0.001),[46] and senior students of their respective courses [46,57].
Eight studies discussed medical [69,85], nursing [67,77], pharmacy [87,91,95], and dental [32] students’ knowledge on suicide risk assessment. There were variations among medical and nursing students, with some being somewhat aware of warning signs [85] and comfortable assessing risks [69,77], while others were uncomfortable to perform suicide risk assessments [67]. Pharmacy students generally displayed good knowledge and readiness in assessing suicide risk [87,91], while 80% of dental students were unsure of what to do if a patient revealed suicidal thoughts [32].
Four studies evaluating students’ knowledge on the causes, nature, treatment, and prevention of suicide discovered that medical [44,57,79,85] and pharmacy [84] students tended to have more knowledge on the treatment and prevention aspects as opposed to the causes and nature of suicide. For example, in a study by Sato et al [57], less than 50% of medical students were able to identify mental disorders and romantic relationship breakdown as risk factors for suicide. Only a few were able to identify the association between gender, age, personality, genetic factors, and history of suicide attempts with suicide. In another study, while more than 75% of medical students were able to identify risk factors for suicide, less than half of them were aware of the predictable nature of suicide [79]. In yet another study, less than 60% of pharmacy students scored correctly on the common means used in suicide attempts and myths related to suicide, such as the tendency of certain age groups or gender to attempt suicide [84]. Medical students, however, scored better when tested on treatment and prevention aspects in two surveys [44,79]. Some of the healthcare students, if not most, were aware of appropriate interventions and measures to help persons with thoughts of suicide [79,84,85].
Subtheme 3: Confidence in managing persons with thoughts of suicide. Nine studies involving medical [34,37,85], nursing [27,28,35,37], and pharmacy[87,95] students highlighted healthcare students’ confidence in managing persons with thoughts of suicide including risk perception and confidence in the ability to help a person at risk or a person who attempted suicide. Overall, most students had low, while some had moderate confidence when dealing with suicidal patients. Nursing undergraduates generally displayed low confidence [27,28,35,37]. A survey done by Marques et al [37] found that males (p=0.00), those who completed a psychiatric nursing course (p=0.01), and those who had previous experience participating in a class or laboratory on suicide (p=0.03) had significantly higher confidence compared to their counterparts.
Meanwhile, Krueger [34] discovered that medical students from the US displayed low confidence in their competence in managing persons with thoughts of suicide, and the trend seemed to remain despite their progression through the course [85]. Medical students showed moderate confidence in another Australian study, with those having previous personal exposure and increased contact with psychiatric patients more confident than the rest of the students [53]. On the other hand, pharmacy students displayed moderate confidence in helping persons with thoughts of suicide as depicted in a simulation video case in a study by Pothireddy [87], though they were less confident in deciding on the appropriate timing for medical intervention [95].
Subtheme 4: Education and training experience in suicide. Seven studies highlighted nursing [28,77,82], pharmacy [51,87,95], and dental[32] students’ engagement in relevant areas of education and training. There was a wide variety in engagement among the healthcare students, however overall, it was still low. Some nursing students had more exposure when compared to other healthcare students, specifically Taiwanese and Brazilian students. Around 50% of Taiwanese students had attended relevant educational courses previously and 40% had professional experience in managing suicide [82], while roughly 35% of Brazilian students participated in suicide prevention classes in the past [28]. Meanwhile, only 5% of nursing undergraduates in India had previous exposure to relevant training and experience [77]. Similarly, less than 15% of pharmacy [51,87,95] and dental students [32] had participated in previous extra-curricular education and courses on suicide. However, notably, among the three dental students who completed suicide awareness training two years prior to the study, one student managed to apply the learning in a real life situation [32].
Theme 2: Attitude towards suicide
Subtheme 1: Emotional reactions when facing persons who are suicidal. There were 16 studies that discussed the emotional impact of dealing with a person with thoughts of suicide on medical [25,26,34,50,57,70,89,90], nursing [27,43,58,59,60,65,67,78], and paramedic [65] students. While some medical students described themselves as not being personally affected,[26,50] others reported a wide range of positive and negative emotions when facing persons with thoughts of suicide. Some of them showed great concern [34] and somewhat sympathized with patients [70,90], though this was less likely among Japanese students whereby less than 50% of them felt sorry for the patients as seen in a study by Sato et al [57]. Others displayed grief, guilt [34], a sense of loss [50], and hostility [34,57].
On the other hand, many nursing undergraduates described feeling apprehensive and fearful that their actions or behaviors might worsen suicidal tendencies [58,59,78]. Some were frustrated as patients continuously ruminated on suicidal thoughts or refused to reveal their thoughts to the students [59], while others described powerlessness in response to similar circumstances [59,78]. In interviews conducted by Zohn et al [67] students disclosed remembering feeling shocked, sad, and angry during various encounters with patients. However, some nursing students and paramedic students did show high levels of empathy to persons with thoughts of suicide [65,67], with some feeling the need to advocate for them [67]. Females (p=0.027) were significantly more likely to empathize [65].
Subtheme 2: Negative and stigmatizing attitudes. Twenty studies revealed negative and stigmatizing attitude towards suicide among medical [25,26,30,36,44,46,61,69,70,71,74,76,79,80,90] and nursing [36,38,41,43,58,78] students. Suicide was depicted by some medical and nursing students as irresponsible especially among final year medical students [76,78], taboo [43,61], and an act borne out of the desire to die and manipulate others [43]. Some disagreed that persons with thoughts of suicide were struggling with isolation or depression [38,80]. Suicide was also seen as selfish [58], stupid [78], cowardly [74], an aggressive act [70], done out of an inability to control rage [71], and contagious [90], and hence should not be normalized [46,80] or glorified [38,46]. In a study conducted by Öz et al [38], suicide was significantly more stigmatized among those who were older (p < 0.05) and those with acquaintances who attempted suicide (p < 0.05).
Among medical students, some of them were unable to accept and understand suicide [61,74] as they agreed that no one had the right to take their own life [30]. Suicide was highly stigmatized [44], deemed morally bad [30], and thought to be punishable after death especially among Turkish [26] and male students [26,30]. A survey undertaken by Emul et al [71] in Turkey discovered that medical students had high levels of distrust about suicide attempters as 80% of them refused to rent a house to suicide attempters, and 90% of them refused to leave their children in the care of a suicide attempter.
Subtheme 3: Permissive or neutral attitudes. Twenty-seven studies highlighted medical [25,26,30,44,46,49,61,69,70,74,76,79,80,89,90], nursing [27,28,35,37,38,41,43,45,60,77,82], and pharmacy [51] students’ relatively permissive attitude toward suicide. Some medical students were reported to have low levels of stigma [46,49]. They disagreed on the taboo placed on the topic [26,80], as they saw suicide as a mental illness or due to despair [30,46,76], particularly among those who were religious [25] and females who were from Austria (p<0.01) [26]. Those with more exposure and knowledge in terms of psychiatry and suicide were also more likely to agree that suicide was an act of communication [61,79], be it to grab the attention of someone [30,79] or for the retaliation or welfare of others [90]. Various possible contributing factors of suicide were acknowledged, including social isolation and depression [44], insecurity [79], and social factors [90]. Regardless, students tended to be neutral in normalizing [49,61], glorifying [44,49], and accepting [26] suicidal behaviour. Japanese students especially were more likely to acknowledge the right to suicide and glorify suicide [70], while Austrians tended to accept suicidal behaviour [26]. Those who were older (p= 0.023), male (p= 0.007), and had a personal history of mental illness (p= 0.005) were significantly more likely to understand and accept suicide as well [61].
Meanwhile, the majority of nursing students held a neutral [45] or positive attitude [28,35,37] toward suicide. Some of them did not have a particular stand on the aspects of morality [82], the right to suicide [27,28,82], suicide as a means of communication [41,43,77,82], and seeing suicide as a mental illness [82]. Others acknowledged the multifactorial influence of suicidal behaviour [60], and hence were less likely to condemn suicidal behaviour [28,35,41]. This was significant among those with a personal lifetime suicidal ideation (p= 0.040) [28], those who were older (p < 0.001) [41], and those with increased exposure to suicide via reading materials (p = 0.01)[37] or practicum (p < 0.001) [41].
Subtheme 4: Perceived nature of suicide. Nineteen studies discussed the perception of medical [34,36,49,68,69,70,71,74,79,80,85,89,90], nursing [36,43,45,60,77], pharmacy [91], and dental [32] students on the nature of suicide. Medical [68,69,79,80,85], pharmacy [91], and dental [32] students were inclined to agree that suicide is preventable, despite the fact that more than 50% of students [71,100] were unsure or disagreed on the predictability of suicide especially those who had a lack of clinical exposure to persons with thoughts of suicide [45,71]. On the contrary, nursing students agreed that suicide was difficult to identify and prevent [60] as the underlying cause of socioeconomic disparity [77] and society’s stigma [60] was not resolved.
Some medical [80] and nursing [43] students also reported that suicide was incomprehensible to them, especially those who were of a younger age (p=0.046) and had never attended relevant psychiatric training (p= 0.021) [45]. Medical students from Turkey [71,80] were more likely to agree that suicide was an impulsive act with low controllability [49], whereas students from Austria [74] and the US [89] were inclined to agree on the deliberate nature of suicide.
Subtheme 5: Role in suicide prevention and management. Twenty studies highlighted medical (n=12)[25,26,34,36,50,68,69,76,80,85,89,90], nursing (n=6) [36,41,58,67,77,82], pharmacy (n=3) [51,87,91], and dental (n=1)[32] students’ perceived role in suicide prevention and management. The majority of students from all fields expressed their agreement on their professional role to prevent [32,34,41,51,69,77,82] and manage [82] suicide except one study where more than 50% of nursing students were defensive about any prevention effort for suicide [77]. Most of them disagreed that suicide prevention or treatment was wasteful [36,69,77] or a misuse of medical resources [76]. They believed that with nurses playing a supportive role in the healthcare system [67,87,90], persons with thoughts of suicide could get better [87].
Despite showing concern for suicide prevention [50] and management via psychiatric treatment and antidepressants [76], some medical students reported being underequipped with suicide prevention skills [80]. They expressed interest for further relevant training as they acknowledged the importance of acquiring suicide prevention skills as a future healthcare professional [68]. Amiri et al [25] and Eskin et al [26] found that students had high social acceptance and desire to help their suicidal friends, especially those who were female (p=.012) [25]. Students would also intervene at times when needed [85], including inquiring into suicidal behaviour, especially among the Austrians [26], or accompanying the person to the healthcare services [85].
4. Discussion
This scoping review provides an overview of healthcare students’ knowledge of and attitude towards suicide. Learning how healthcare students view and think about suicide is vital as this will affect the care provided to the patients in the future. From here, strategies could be devised to develop or improve educational programmes and build healthcare professionals that are able to provide holistic management and care to aid the survival of patients who are suicidal [101].
From this scoping review, it was found that on the whole, healthcare students were generally concerned about persons with thoughts of suicide. Findings involving healthcare professionals were similar, as they tended to admit patients at risk and consult other colleagues after witnessing inpatient suicides [102,103]. Healthcare students also demonstrated relatively high levels of knowledge towards prevention and treatment of suicide, as opposed to the cause and nature, highlighting the tendency of the public be reactive rather than proactive when dealing with mental health issues [104].
This scoping review also found that some nursing students were better prepared with higher professional skills in the management of persons with thoughts of suicide and had good knowledge, given their relatively better training and exposure to suicide [105], which was still overall quite low. This finding supports the literature in highlighting the importance of training in improving knowledge and attitude towards suicide [106,107,108,109,110,111,112,113,114]. Overall, they still reported low confidence in providing management due to the fear of saying something inappropriate and making the situation worse [115]. The findings among nursing students were similar to that from nursing professionals, whereby a majority of them reported low confidence in management given the minimal training and education on suicide received [116,117]. In our scoping review, nursing students saw suicide as a means to communicate, and agreed that victims were often struggling with isolation or depression, consistent with present studies [118,119]. However, they tended to avoid talking about suicide as they felt anxious and powerless from the inability to help and the lack of therapeutic response despite best care [120]. Nursing students were also less likely to stigmatize and judge against persons with thoughts of suicide. This was inconsistent with findings among nursing professionals who viewed suicide as morally wrong or as a mental illness [121,122,123,124,125], although they showed an improvement in attitude over time due to increased training and education on suicide [126,127].
Like doctors [128], medical students were also more likely to condemn the rights to suicide, as they tended to stigmatize against suicide and agree that suicide is not a normal phenomenon that should be glorified. This could be due to the association of suicide with personal weakness, which was commonly stigmatized against in an academically competitive environment [129]. The lack of training and education played a role as well [106,107,108,109,110,111,112,114,130]. Negative attitude and stigma against suicide has been reported to lead to compromised healthcare [131,132,133], and this could explain the lower ability of medical students in managing persons with thoughts of suicide. The provision of less than optimal care to those with thoughts of suicide was also noted in a study involving primacy care physicians [134,135,136,137].
Cultural and religious influences could shape attitudes towards suicide. For example, Austrian and Japanese students were more likely to normalize and glorify suicide. For the Japanese, suicide was historically honourable when done to gain control on life [138] or over death [139]. Meanwhile, findings for Austrian students indicated that suicide was seen as a deliberate act and a decision with rationale [74] and should be respected. Meanwhile, Turkish students were more likely to believe that suicide would lead to punishment after death, as Islam viewed suicide as sinful[140] and prohibited suicide strictly [141]. In this review, Indian students completely rejected suicide since it was seen as a cowardly and impulsive act from uncontrolled emotions and mental illness [74]. Traditionally in the Indian culture, suicide is deemed as a sign of “weakness of mind”, and that those who carried out suicide were expected to be “stronger” and “seek solution from God” [114]. Those who attempted suicide are blamed and showered with guilt [114], although Hinduism (adhered to by 80% of Indian population)[142] does not specifically prohibited suicide [143], indicating a larger role of culture compared to religion in this context. Despite urges to decriminalise suicide, suicide remains a criminal offense to date [144], which might have contributed to the attitude of the Indian students as well.
Demographics seemed to play a role whereby our review suggested females were more likely to have better knowledge, skills and attitude, and increased perception of personal role and responsibilities in suicide management and prevention. They displayed higher levels of empathy [145], which could alleviate psychological distress and suicidal ideation [146]. Besides, those who were older generally held a more positive attitude toward suicide as they were more likely to accept, understand, and normalize suicide, in contrast to a study involving health professionals [147], which was likely due to desensitization with increasing clinical exposure toward suicide [148]. Meanwhile, our scoping review demonstrated those who were younger were less likely to comprehend suicide. Findings from other studies were ambiguous, highlighting a need for further exploration of this aspect [62,121].
In our review, personal exposure to suicide were associated with increased suicidal literacy, confidence in managing a person with thoughts of suicide, and reduced stigma as they were more likely able to empathize, understand and respect those with suicidal intentions [149]. Similar findings were discovered among healthcare professionals with personal and family history of mental illness [149].
4.1. Strengths and Limitations
This is the first scoping review available to provide a comprehensive overview of healthcare students’ knowledge of and attitude towards suicide at a global level. However, this review only included English studies, which might lead to language bias. Furthermore, the stringent search terms might have caused data loss. Most studies included used self-reported questionnaires, which predisposed the review to reporting bias based on social desirability. Given that 30% of the studies included were undertaken before the year 2013 and the cross-sectional design of the majority of studies, this review might not reflect the most contemporary knowledge of and attitude toward suicide.
4.2. Future Research and Recommendations
Considering that two thirds of suicides occur in developing countries,[1] and the underrepresentation of the studies from these countries in the review, more studies need to be conducted in these countries. Besides, more studies on students from other healthcare professions such as pharmacy and dentistry need to be conducted, as there is evidence of the role these professions could play in suicide prevention [150,151]. Despite the possible role of religiosity in affecting attitudes towards suicide [143,152,153,154], most studies in this review did not include this aspect in their results, hence the need for future studies to take this into consideration.
Furthermore, given the lack of knowledge and negative attitude among medical students, more studies should be conducted to address the contributing factors. Evaluation of medical curriculum should be undertaken to include relevant training programs that were shown to be effective to improve knowledge and attitude towards suicide. One study indicated that training community facilitators, including healthcare professionals, improved their knowledge, confidence, attitudes, and interventions when dealing with persons with thoughts of suicide [155]. In addition, a scoping review on suicide prevention programs found that training healthcare professionals and students improved their knowledge, behaviour, engagement in health services, as well as gatekeeper role outcomes [156]. Indeed, various studies have demonstrated the effectiveness of gatekeepers’ training programmes[157,158] in sessions as short as one hour,[159] educational interventions,[160] workshops [85], movies [89], simulations [161], and modules [90] in improving medical students’ knowledge and attitudes.
Specifically, gatekeepers’ training programmes have been widely applied among the public and have shown satisfactory and sustainable effectiveness [162,163] up until five months, in improving knowledge and skills in suicide prevention and intervention [109,111,163,164,165,166,167,168,169,170,171] and attitude [162,163,170] as evidenced by a systematic review [172]. Such programs should be organised and incorporated in medical curriculla, though further adaptations are still required to develop locally and culturally sensitive programmes [167,173]. Some examples with proven efficacy include Mental Health First Aid [174], Signs of Suicide (SOS) [175], Question, Persuade, and Refer (QPR) [96,110,111,163], Applied Suicide Intervention Skills Training (ASIST) [111], and Connect [109]. Studies have showed that medical staff who underwent ASIST, a 14 hour programme developed in Canada in 1983 with strong focus on training via simulations [176] possessed greater confidence in managing individuals with thoughts of suicide compared to other training programmes [111] as well as an increase in knowledge and positive attitude sustainable for years [176]. This was due to the fact that instead of referral to healthcare professionals as in other programs, it aimed to connect the individuals to community resources for suicide prevention and intervention [176].
5. Conclusions
Healthcare students showed a positive attitude in their role to treat and prevent suicide, and to support persons with thoughts of suicide. Medical students showed a relative lack of knowledge and more negative attitudes compared to nursing students, highlighting the need to evaluate current medical curriculum on suicide. The incorporation of gatekeepers’ training programmes into medical curriculla should be considered. Given the relative lack of data from developing countries and certain healthcare professions, future research should aim to address the current gaps.
Supplementary Materials
The following supporting information can be downloaded at website of this paper posted on Preprints.org.
Author Contributions
Conceptualization: S.A.J. and L.K; Data curation: G.T.A.; Formal analysis: G.T.A. and S.A.J.; Investigation: G.T.A.; Methodology: S.A.J, L.K. and G.T.A.; Project administration: S.A.J.; Supervision: S.A.J.; Validation: G.T.A., L.K. and S.A.J.; Writing—original draft: G.T.A., L.K. and S.A.J.; Writing—review and editing: G.T.A., L.K. and S.A.J. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A.
Research Strategy:
Method of search:
- Studies from database inception to 31st December 2023.
- Databases used for searches:
- PubMed
- Cochrane Database of Systematic Reviews
- Cochrane Central Register of Controlled Trials (CENTRAL)
- Cumulative Index to Nursing and Allied Health Literature (CINAHL)
- Excerpta Medica dataBASE (EMBASE)
- PsycINFO
- Database of Abstracts of Review of Effects (DARE)
Inclusion and exclusion criteria
- Inclusion criteria
Studies that fulfilled the following criteria were included:
- Studies that evaluated the attitude and/ or knowledge on suicide and/ or suicide related programs, and involves healthcare students from professions such as medicine, nursing, pharmacists, dentistry, and allied health such as paramedics, oral health therapists, and dental therapists as study population.
- 2.
- Exclusion criteria
Studies which met any of the following criteria were excluded:
- Reviews, systematic reviews, meta-analyses, conference abstracts, conference proceedings, in vivo studies, in vitro studies, animal studies, thesis, and letter to editors.
- Studies that were written in other languages than English.
- Studies without available abstracts and full texts.
- Studies that evaluated healthcare students with special training in psychiatry such as psychiatric trainees, psychology students and mental health nurses, and midwives.
- Studies that evaluated healthcare students’ suicide rate and suicidality.
- Studies that evaluated healthcare students’ attitude and/ or knowledge on physician assisted suicide.
- Studies with outcomes that are not specific, such as the attitudes towards both depression and suicide.
- In studies which evaluation of an intervention is the focus, pre-test attitudes or knowledge assessments are unavailable.
Search terms
Healthcare term: “healthcare” OR “health” OR “medic*” OR “pharmac*” OR “dentist*” OR “dental*” OR “allied health” OR “nurs*”
Student term: “student” OR “undergraduate” OR “postgraduate” OR “trainee” OR “intern” OR “future doctor”
Knowledge & attitude term: “knowledge” OR “attitude” OR “understanding” OR “awareness” OR “clarity” OR “thought” OR “opinion” OR “comprehension” OR “insight” OR “approach” OR “belief” OR “believes” OR “mindset” OR “sentiment” OR “perspective” OR “outlook” OR “notion” OR “stand*” OR “view*” OR “feedback” OR “percep*” OR “expect*” OR “behaviour” OR “behavior” OR “willingness” OR “practice” OR “training” OR “literacy”
Suicide term: “suicide” OR “self-killing” OR “self-immolat*” OR “self-poison*” OR “overdose” OR “self-harm” OR “suicidal” OR “ideation”
Search strategy
- Search healthcare term (A)
- Search student term (B)
- Search knowledge & attitude terms (C)
- Search suicide term (D)
- Combine healthcare, student, knowledge & attitude, and suicide terms (A+B+C+D)
- Exclude reviews, systematic reviews, animal studies, and other non-research articles.
- Screen titles and abstracts for studies evaluating healthcare students’ knowledge of and attitude toward suicide.
References
- World Health Organization. Suicide. Available online: https://www.who.int/news-room/fact-sheets/detail/suicide (accessed on.
- Saloni Dattani, L.R.-G. Hannah Ritchie, Max Roser and Esteban Ortiz-Ospina. Suicides. Available online: https://ourworldindata.org/suicide (accessed on.
- Centers for Disease Control and Prevention. Facts About Suicide. Available online: https://www.cdc.gov/suicide/facts/index.html (accessed on.
- Sveen, C.A.; Walby, F.A. Suicide survivors’ mental health and grief reactions: a systematic review of controlled studies. Suicide Life Threat. Behav. 2008, 38, 13–29. [Google Scholar] [CrossRef]
- Doran, C.M.; Kinchin, I. Economic and epidemiological impact of youth suicide in countries with the highest human development index. PLoS One 2020, 15, e0232940. [Google Scholar] [CrossRef] [PubMed]
- Saxena, S.; Funk, M.; Chisholm, D. Comprehensive mental health action plan 2013–2020. Eastern Mediterranean Health Journal 2015, 21, 461–463. [Google Scholar] [CrossRef]
- World Health Organization. Comprehensive mental health action plan 2013-2020. 2013.
- Stene-Larsen, K.; Reneflot, A. Contact with primary and mental health care prior to suicide: A systematic review of the literature from 2000 to 2017. Scand J Public Health 2019, 47, 9–17. [Google Scholar] [CrossRef]
- Mesec Rodi, P.; Roskar, S.; Marusic, A. Suicide victims’ last contact with the primary care physician: report from Slovenia. Int. J. Soc. Psychiatry 2010, 56, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Dunkley, C.; Borthwick, A.; Bartlett, R.; Dunkley, L.; Palmer, S.; Gleeson, S.; Kingdon, D. Hearing the Suicidal Patient’s Emotional Pain. Crisis 2018, 39, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Berman, N.C.; Sullivan, A.; Wilhelm, S.; Cohen, I.G. Effect of a legal prime on clinician’s assessment of suicide risk. Death Stud. 2016, 40, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Scheerder, G.; Reynders, A.; Andriessen, K.; Van Audenhove, C. Suicide intervention skills and related factors in community and health professionals. Suicide Life Threat. Behav. 2010, 40, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Rothes, I.A.; Henriques, M.R.; Leal, J.B.; Lemos, M.S. Facing a patient who seeks help after a suicide attempt: the difficulties of health professionals. Crisis 2014, 35, 110–122. [Google Scholar] [CrossRef]
- Sethi, S.; Shipra, U. Attitudes of clinicians in emergency room towards suicide. Int. J. Psychiatry Clin. Pract. 2006, 10, 182–185. [Google Scholar] [CrossRef]
- Neimeyer, R.A.; Pfeiffer, A. The ten most common errors of suicide interventionists; Taylor & Francis: New York, NY, USA, 1994. [Google Scholar]
- Kamal, L.; Jacob, S.A. Pharmacists’ Experiences, Perceptions, and Attitudes towards Suicide and Suicide Prevention: A Scoping Review. Pharmacy 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- Allport, G.W. Attitudes.; Clark University Press: Worcester, MA, 1935. [Google Scholar]
- Ahmedani, B.K.; Simon, G.E.; Stewart, C.; Beck, A.; Waitzfelder, B.E.; Rossom, R.; Lynch, F.; Owen-Smith, A.; Hunkeler, E.M.; Whiteside, U.; et al. Health care contacts in the year before suicide death. J. Gen. Intern. Med. 2014, 29, 870–877. [Google Scholar] [CrossRef] [PubMed]
- Moose, J.; Branham, A. Pharmacists as Influencers of Patient Adherence. Pharmacy Times Oncology Edition 2014, 1. [Google Scholar]
- Rukundo, G.Z.; Wakida, E.K.; Maling, S.; Kaggwa, M.M.; Sserumaga, B.M.; Atim, L.M.; Atuhaire, C.D.; Obua, C. Knowledge, attitudes, and experiences in suicide assessment and management: a qualitative study among primary health care workers in southwestern Uganda. BMC Psychiatry 2022, 22, 605. [Google Scholar] [CrossRef]
- Karimollahi, M. An investigation of nursing students’ experiences in an Iranian psychiatric unit. J. Psychiatr. Ment. Health Nurs. 2012, 19, 738–745. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: towards a methodological framework. International Journal of Social Research Methodology 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The, P.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qualitative Research in Psychology 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Amiri, L.; Voracek, M.; Yousef, S.; Galadari, A.; Yammahi, S.; Sadeghi, M.-R.; Eskin, M.; Dervic, K. Suicidal behavior and attitudes among medical students in the United Arab Emirates. Crisis: The Journal of Crisis Intervention & Suicide Prevention 2013, 34, 116–123. [Google Scholar] [CrossRef]
- Eskin, M.; Voracek, M.; Stieger, S.; Altinyazar, V. A cross-cultural investigation of suicidal behavior and attitudes in Austrian and Turkish medical students. Soc. Psychiatry Psychiatr. Epidemiol. 2011, 46, 813–823. [Google Scholar] [CrossRef]
- Ferrara, P.; Terzoni, S.; Ruta, F.; Poggi, A.D.; Destrebecq, A.; Gambini, O.; D’Agostino, A. Nursing students’ attitudes towards suicide and suicidal patients: A multicentre cross-sectional survey. Nurse Educ. Today 2022, 109, 105258. [Google Scholar] [CrossRef]
- Giacchero Vedana, K.G.; Guidorizzi Zanetti, A.C. Attitudes of nursing students toward to the suicidal behavior. Revista Latino-Americana de Enfermagem (RLAE) 2019, 27, 1–6. [Google Scholar] [CrossRef]
- Botega, N.J.; Reginato, D.G.; da Silva, S.V.; Cais, C.F.; Rapeli, C.B.; Mauro, M.L.; Cecconi, J.P.; Stefanello, S. Nursing personnel attitudes towards suicide: the development of a measure scale. Braz J Psychiatry 2005, 27, 315–318. [Google Scholar] [CrossRef]
- Kavalidou, K. Suicidal thoughts and attitudes towards suicide among medical and psychology students in Greece. Suicidology Online 2013, 4, 4–11. [Google Scholar]
- Domino, G.; Gibson, L.; Poling, S.; Westlake, L. Students’ attitudes towards suicide. Social psychiatry 1980, 15, 127–130. [Google Scholar] [CrossRef]
- Kelly, N.; Kilgariff, J.K. Should suicide risk assessment be embedded in undergraduate dental curricula? Br. Dent. J. 2023, 234, 601–605. [Google Scholar] [CrossRef] [PubMed]
- Herron, J.; Ticehurst, H.; Appleby, L.; Perry, A.; Cordingley, L. Attitudes toward suicide prevention in front-line health staff. Suicide Life Threat Behav 2001, 31, 342–347. [Google Scholar] [CrossRef] [PubMed]
- Krueger, D.W. Patient suicide: model for medical student teaching and mourning. Gen. Hosp. Psychiatry 1979, 1, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Lappann Botti, N.C.; Costa de Araújo, L.M.; Costa, E.E.; de Almeida Machado, J.S. Nursing students attitudes across the suicidal behavior. Investigacion & Educacion en Enfermeria 2015, 33, 334–342. [Google Scholar] [CrossRef]
- López-Narváez, M.L.; Escobar-Chan, Y.M.; Sánchez de la Cruz, J.P.; Tovilla-Zárate, C.A.; Juárez-Rojop, I.E.; Fresan, A.; González-Castro, T.B.; Montanee-Sandoval, A.C.; Suarez-Méndez, S. Differences in attitude toward prevention of suicide between nursing and medicine students: A study in Mexican population. Arch. Psychiatr. Nurs. 2020, 34, 159–163. [Google Scholar] [CrossRef]
- Marques Moraes, S.; Magrini, D.F.; Guidorizzi Zanetti, A.C.; dos Santos, M.A.; Giacchero Vedana, K.G. Attitudes and associated factors related to suicide among nursing undergraduates. Acta Paulista de Enfermagem 2016, 29, 643–649. [Google Scholar] [CrossRef]
- Öz, F.; Turgut Atak, N.; Meriç, M. Nursing students’ attitudes toward death and stigma toward individuals who attempt suicide. Perspect. Psychiatr. Care 2022, 58, 1728–1735. [Google Scholar] [CrossRef] [PubMed]
- Batterham, P.J.; Calear, A.L.; Christensen, H. The Stigma of Suicide Scale. Psychometric properties and correlates of the stigma of suicide. Crisis 2013, 34, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Wong, P.; Reker, G.; Gesser, G. Death attitude profile–revised: a multidimensional measure of attitudes death; Neimeyer, R.A., Ed.; Taylor &Francis, 1994. [Google Scholar]
- Poreddi, V.; Anjanappa, S.; Reddy, S. Attitudes of under graduate nursing students to suicide and their role in caring of persons with suicidal behaviors. Arch. Psychiatr. Nurs. 2021, 35, 583–586. [Google Scholar] [CrossRef] [PubMed]
- Sun, F.K.; Long, A.; Huang, X.Y.; Chiang, C.Y. A quasi-experimental investigation into the efficacy of a suicide education programme for second-year student nurses in Taiwan. J Clin Nurs 2011, 20, 837–846. [Google Scholar] [CrossRef] [PubMed]
- Vedana, K.G.G.; Pereira, C.C.M.; Dos Santos, J.C.; Ventura, C.; Moraes, S.M.; Miasso, A.I.; Zanetti, A.C.G.; Borges, T.L. The meaning of suicidal behaviour from the perspective of senior nursing undergraduate students. Int. J. Ment. Health Nurs. 2018, 27, 1149–1161. [Google Scholar] [CrossRef] [PubMed]
- Arafat, S.M.Y.; Hussain, F.; Hossain, M.F.; Islam, M.A.; Menon, V. Literacy and stigma of suicide in Bangladesh: Scales validation and status assessment among university students. Brain Behav 2022, 12, e2432. [Google Scholar] [CrossRef]
- Bajracharya, J.; Bhandari, N.; Chalise, P.; Tiwari, D. Perception Regarding Care of Attempted Suicide Patients among Nursing Students in Kathmandu University School of Medical Sciences. Kathmandu Univ. Med. J. (KUMJ) 2020, 18, 402–406. [Google Scholar] [CrossRef]
- Chan, W.I.; Batterham, P.; Christensen, H.; Galletly, C. Suicide literacy, suicide stigma and help-seeking intentions in Australian medical students. Australas Psychiatry 2014, 22, 132–139. [Google Scholar] [CrossRef]
- Calear, A.L.; Batterham, P.J.; Christensen, H. The literacy of suicide scale: Psychometric properties and correlates of suicide literacy. 2012. [Google Scholar]
- Wilson, C.J.; Deane, F.P.; Ciarrochi, J.; Rickwood, D. Measuring Help-Seeking Intentions: Properties of the General Help-Seeking Questionnaire. Canadian Journal of Counselling 2005, 39, 15–28. [Google Scholar]
- Cryer, R.E.M.; Calear, A.L.; Batterham, P.J.; Patel, S.R. Suicide, mental, and physical health condition stigma in medical students. Death Stud. 2020, 44, 230–236. [Google Scholar] [CrossRef]
- Hamaoka, D.A.; Fullerton, C.S.; Benedek, D.M.; Gifford, R.; Nam, T.; Ursano, R.J. Medical students’ responses to an inpatient suicide: opportunities for education and support. Acad. Psychiatry 2007, 31, 350–353. [Google Scholar] [CrossRef]
- Mospan, C.M.; Gillette, C. Student Pharmacists’ Attitudes Toward Suicide and the Perceived Role of Community Pharmacists in Suicidal Ideation Assessment. Am. J. Pharm. Educ. 2020, 84, 7588. [Google Scholar] [CrossRef] [PubMed]
- Neimeyer, R.A.; Diamond, R.J. Suicide management skills and the medical student. J. Med. Educ. 1983, 58, 562–567. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Batterham, P.J.; Calear, A.L.; Cryer, R. Predictors of Comfort and Confidence Among Medical Students in Providing Care to Patients at Risk of Suicide. Acad. Psychiatry 2016, 40, 919–922. [Google Scholar] [CrossRef] [PubMed]
- Batterham, P.J.; Calear, A.L.; Christensen, H. Correlates of suicide stigma and suicide literacy in the community. Suicide Life Threat Behav 2013, 43, 406–417. [Google Scholar] [CrossRef]
- Cooper, A.J.; Smillie, L.D.; Corr, P.J. A confirmatory factor analysis of the Mini-IPIP five-factor model personality scale. Personality and Individual Differences 2010, 48, 688–691. [Google Scholar] [CrossRef]
- Raskin, R.; Terry, H. A principal-components analysis of the Narcissistic Personality Inventory and further evidence of its construct validity. Journal of Personality and Social Psychology 1988, 54, 890–902. [Google Scholar] [CrossRef]
- Sato, R.; Kawanishi, C.; Yamada, T.; Hasegawa, H.; Ikeda, H.; Kato, D.; Furuno, T.; Kishida, I.; Hirayasu, Y. Knowledge and attitude towards suicide among medical students in Japan: preliminary study. Psychiatry Clin. Neurosci. 2006, 60, 558–562. [Google Scholar] [CrossRef]
- Scheckel, M.M.; Nelson, K.A. An interpretive study of nursing students’ experiences of caring for suicidal persons. J. Prof. Nurs. 2014, 30, 426–435. [Google Scholar] [CrossRef] [PubMed]
- Sun, F.K.; Long, A.; Chiang, C.Y.; Wu, M.K.; Yao, Y. The psychological processes voiced by nursing students when caring for suicidal patients during their psychiatric clinical practicum: A qualitative study. J. Clin. Nurs. 2020, 29, 525–534. [Google Scholar] [CrossRef] [PubMed]
- Vedana, K.G.G.; Dos Santos, J.C.; Zortea, T.C. The Meaning of Suicidal Behaviour for Portuguese Nursing Students. Int. J. Environ. Res. Public Health 2022, 19. [Google Scholar] [CrossRef]
- Wahab, S.; Shah, N.E.; Sivachandran, S.; Shahruddin, I.; Ismail, N.N.S.; Mohan, L.D.; Kamaluddin, M.R.; Nawi, A.M. Attitude Towards Suicide and Help-Seeking Behavior Among Medical Undergraduates in a Malaysian University. Acad. Psychiatry 2021, 45, 672–680. [Google Scholar] [CrossRef] [PubMed]
- Renberg, E.S.; Jacobsson, L. Development of a questionnaire on attitudes towards suicide (ATTS) and its application in a Swedish population. Suicide Life Threat Behav 2003, 33, 52–64. [Google Scholar] [CrossRef]
- Deane, F.P.; Skogstad, P.; Williams, M.W. Impact of attitudes, ethnicity and quality of prior therapy on New Zealand male prisoners’ intentions to seek professional psychological help. International Journal for the Advancement of Counselling 1999, 21, 55–67. [Google Scholar] [CrossRef]
- Deane, F.P.; Todd, D.M. Attitudes and Intentions to Seek Professional Psychological Help for Personal Problems or Suicidal Thinking. Journal of College Student Psychotherapy 1996, 10, 45–59. [Google Scholar] [CrossRef]
- Williams, B.; Boyle, M.; Fielder, C. Empathetic attitudes of undergraduate paramedic and nursing students towards four medical conditions: a three-year longitudinal study. Nurse Educ. Today 2015, 35, e14–18. [Google Scholar] [CrossRef] [PubMed]
- Christison, G.W.; Haviland, M.G.; Riggs, M.L. The medical condition regard scale: measuring reactions to diagnoses. Acad Med 2002, 77, 257–262. [Google Scholar] [CrossRef]
- Zohn, J.H. The Experiences of Nursing Students While Caring for Patients at Risk for Suicide: A Descriptive Phenomenology. Nurs. Educ. Perspect. 2022, 43, E91–e93. [Google Scholar] [CrossRef]
- Hawgood, J.L.; Krysinska, K.E.; Ide, N.; De Leo, D. Is suicide prevention properly taught in medical schools? Med. Teach. 2008, 30, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Price, R.; Weingartner, L.A.; Brikker, E.; Shaw, M.A.; Shreffler, J.; O’Connor, S.S. Improving Medical Student Attitudes Toward Suicide Prevention Through a Patient Safety Planning Clerkship Initiative. Acad. Psychiatry 2022, 46, 616–621. [Google Scholar] [CrossRef]
- Domino, G.; Takahashi, Y. Attitudes toward suicide in Japanese and American medical students. Suicide Life Threat. Behav. 1991, 21, 345–359. [Google Scholar] [CrossRef] [PubMed]
- Emul, M.; Uzunoglu, Z.; Sevinç, H.; Güzel, C.; Yilmaz, C.; Erkut, D.; Arikan, K. The attitudes of preclinical and clinical Turkish medical students toward suicide attempters. Crisis 2011, 32, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Eskin, M. The effects of religious versus secular education on suicide ideation and suicidal attitudes in adolescents in Turkey. Soc Psychiatry Psychiatr Epidemiol 2004, 39, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Eskin, M. Social reactions of Swedish and Turkish adolescents to a close friend’s suicidal disclosure. Soc Psychiatry Psychiatr Epidemiol 1999, 34, 492–497. [Google Scholar] [CrossRef] [PubMed]
- Etzersdorfer, E.; Vijayakumar, L.; Schöny, W.; Grausgruber, A.; Sonneck, G. Attitudes towards suicide among medical students: comparison between Madras (India) and Vienna (Austria). Soc. Psychiatry Psychiatr. Epidemiol. 1998, 33, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Diekstra RFW, K.A. Attitudes towards suicide: the development of a suicide-attitude questionnaire (SUIATT). In Suicide and its prevention, the role of attitude and imi tation; Diekstra, R.F.W., Maris, R., Platt, S., Schmidtke, A., Sonneck, G., Eds.; Brill: Leiden, 1989; pp. 91–107. [Google Scholar]
- Wallin, U.; Runeson, B. Attitudes towards suicide and suicidal patients among medical students. Eur. Psychiatry 2003, 18, 329–333. [Google Scholar] [CrossRef] [PubMed]
- Nebhinani, N.; Mamta, *!!! REPLACE !!!*; Gaikwad, A.D.; Tamphasana, L. Nursing students’ attitude toward suicide prevention. Ind Psychiatry J 2013, 22, 114–117. [Google Scholar] [CrossRef]
- Sun, F.K.; Long, A.; Chiang, C.Y.; Chou, M.H. A theory to guide nursing students caring for patients with suicidal tendencies on psychiatric clinical practicum. Nurse Educ. Pract. 2019, 38, 157–163. [Google Scholar] [CrossRef]
- Slobodanka Bašić, B.L.; Jović, Sladjana; Petrović, Branislav; Kocić, Biljana; Jovanović, Jovica. Suicide Knowledge and Attitudes among Medical Students of the University of NIŠ. Facta Universitatis, Series: Medicine and Biology 2004, 11, 154–159. [Google Scholar]
- Öncü, B. Çiğdemİhan, İnci ÖzgürSayl, Işk. Attitudes of Medical Students, General Practitioners, Teachers, and Police Officers Toward Suicide in a Turkish Sample. Crisis: The Journal of Crisis Intervention and Suicide Prevention 2008, 29, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Salander-Renberg, E.; Jacobson, L. Development of a questionnaire on attitudes toward suicide (ATTS) and its application in a Swedish population. Suicide and Life Threatening Behavior 2003, 33, 52–64. [Google Scholar] [CrossRef] [PubMed]
- Fan-Ko, S.; Long, A.; Xuan-Yi, H.; Chun-Ying, C. A quasi-experimental investigation into the efficacy of a suicide education programme for second-year student nurses in Taiwan. Journal of clinical nursing (john wiley & sons, inc.) 2011, 20, 837–846. [Google Scholar] [CrossRef]
- Sun, F.K.; Long, A.; Boore, J. The attitudes of casualty nurses in Taiwan to patients who have attempted suicide. J Clin Nurs 2007, 16, 255–263. [Google Scholar] [CrossRef]
- Willson, M.N.; Robinson, J.D.; McKeirnan, K.C.; Akers, J.M.; Buchman, C.R. Training Student Pharmacists in Suicide Awareness and Prevention. Am. J. Pharm. Educ. 2020, 84, ajpe847813. [Google Scholar] [CrossRef]
- Hjelvik, A.; Eldridge, A.; Furnari, M.; Hoeflich, H.; Chen, J.I.; Roth, B.; Black, W. A Peer-to-Peer Suicide Prevention Workshop for Medical Students. MedEdPORTAL 2022, 18, 11241. [Google Scholar] [CrossRef]
- Ajzen, I. Constructing a theory of planned behavior questionnaire; 2019.
- Pothireddy, N.; Lavigne, J.E.; Groman, A.S.; Carpenter, D.M. Developing and evaluating a module to teach suicide prevention communication skills to student pharmacists. Curr Pharm Teach Learn 2022, 14, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Lavigne, J.E.; King, D.; Lu, N.; Knox, K.L.; Kemp, J.E. Pharmacist and Pharmacy Staff Knowledge and Attitudes Towards Suicide and Suicide Prevention After a National VA Training Program. Value Health 2011, 14. [Google Scholar] [CrossRef]
- Retamero, C.; Walsh, L.; Otero-Perez, G. Use of the film The Bridge to augment the suicide curriculum in undergraduate medical education. Acad. Psychiatry 2014, 38, 605–610. [Google Scholar] [CrossRef]
- Yousuf, S.; Beh, P.S.; Wong, P.W. Attitudes towards suicide following an undergraduate suicide prevention module: experience of medical students in Hong Kong. Hong Kong Med. J. 2013, 19, 377–385. [Google Scholar] [CrossRef] [PubMed]
- McKeirnan, K.C.; MacCamy, K.L.; Robinson, J.D.; Ebinger, M.; Willson, M.N. Implementing Mental Health First Aid Training in a Doctor of Pharmacy Program. Am J Pharm Educ 2023, 87, 100006. [Google Scholar] [CrossRef] [PubMed]
- Modgill, G.; Patten, S.B.; Knaak, S.; Kassam, A.; Szeto, A.C.H. Opening Minds Stigma Scale for Health Care Providers (OMS-HC): Examination of psychometric properties and responsiveness. BMC Psychiatry 2014, 14, 120. [Google Scholar] [CrossRef]
- Litteken, C.; Sale, E. Long-Term Effectiveness of the Question, Persuade, Refer (QPR) Suicide Prevention Gatekeeper Training Program: Lessons from Missouri. Community Ment Health J 2018, 54, 282–292. [Google Scholar] [CrossRef] [PubMed]
- Wellbeing, N.C.f.M. Mental health first aid. Available online: https://www.thenationalcouncil.org/our-work/mental-health-first-aid/ (accessed on 24th February 2024).
- Carpenter, D.M.; Stover, A.N.; Harris, S.C.; Anksorus, H.; Lavigne, J.E. Impact of a Brief Suicide Prevention Training with an Interactive Video Case Assessment on Student Pharmacist Outcomes. Am J Pharm Educ 2023, 87, 100093. [Google Scholar] [CrossRef]
- Wyman, P.A.; Brown, C.H.; Inman, J.; Cross, W.; Schmeelk-Cone, K.; Guo, J.; Pena, J.B. Randomized trial of a gatekeeper program for suicide prevention: 1-year impact on secondary school staff. Journal of consulting and clinical psychology 2008, 76, 104–115. [Google Scholar] [CrossRef]
- Siau, C.S.; Wee, L.H.; Ibrahim, N.; Visvalingam, U.; Wahab, S. Cross-Cultural Adaptation and Validation of the Attitudes Toward Suicide Questionnaire Among Healthcare personnel in Malaysia. Inquiry 2017, 54, 46958017707295. [Google Scholar] [CrossRef]
- Centre, F.S.P. Suicide Prevention for Pharmacy. Available online: https://intheforefront.org/suicide-prevention-for-pharmacy-professionals/ (accessed on July 28, 2020 ).
- Lopez-Morinigo, J.D.; Escribano-Martinez, A.S.; Ruiz-Ruano, V.G.; Mata-Iturralde, L.; Sanchez-Alonso, S.; Munoz-Lorenzo, L.; Baca-Garcia, E.; David, A. Randomised controlled trial of metacognitive training compared with psychoeducation in patients with schizophrenia spectrum disorders: effects on insight. Schizophr. Bull. 2020, 46, S47–S48. [Google Scholar] [CrossRef]
- Kelly, L.; Tsang, R.S.W.; Morgan, A.; Jamieson, F.B.; Ulanova, M. Invasive disease caused by Haemophilus influenzae type a in Northern Ontario First Nations communities. J. Med. Microbiol. 2011, 60, 384–390. [Google Scholar] [CrossRef]
- Vatne, M.; Nåden, D. Experiences that inspire hope: Perspectives of suicidal patients. Nursing Ethics 2016, 25, 444–457. [Google Scholar] [CrossRef]
- Erbuto, D.; Berardelli, I.; Sarubbi, S.; Rogante, E.; Sparagna, A.; Nigrelli, G.; Lester, D.; Innamorati, M.; Pompili, M. Suicide-Related Knowledge and Attitudes among a Sample of Mental Health Professionals. Int. J. Environ. Res. Public Health 2021, 18. [Google Scholar] [CrossRef] [PubMed]
- Grad, O.T.; Zavasnik, A.; Groleger, U. Suicide of a patient: gender differences in bereavement reactions of therapists. Suicide Life Threat. Behav. 1997, 27, 379–386. [Google Scholar] [CrossRef] [PubMed]
- (WHO), W.H.O. Policy Brief: COVID-19 and the Need for Action on Mental Health. Available online: https://unsdg.un.org/sites/default/files/2020-05/UN-Policy-Brief-COVID-19-and-mental-health (accessed on.
- Carmona-Navarro, M.C.; Pichardo-Martínez, M.C. Attitudes of nursing professionals towards suicidal behavior: influence of emotional intelligence. Rev Lat Am Enfermagem 2012, 20, 1161–1168. [Google Scholar] [CrossRef] [PubMed]
- Lamis, D.A.; Underwood, M.; D’Amore, N. Outcomes of a Suicide Prevention Gatekeeper Training Program Among School Personnel. Crisis 2017, 38, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Abbey, K.J.; Madsen, C.H., Jr.; Polland, R. Short-term suicide awareness curriculum. Suicide Life Threat. Behav. 1989, 19, 216–227. [Google Scholar] [CrossRef] [PubMed]
- Aseltine, R.H.; James, A.; Schilling, E.A.; Glanovsky, J. Evaluating the SOS suicide prevention program: a replication and extension. BMC Public Health 2007, 7, 161. [Google Scholar] [CrossRef] [PubMed]
- Bean, G.; Baber, K.M. Connect: an effective community-based youth suicide prevention program. Suicide Life Threat. Behav. 2011, 41, 87–97. [Google Scholar] [CrossRef]
- Tompkins, T.L.; Witt, J.; Abraibesh, N. Does a gatekeeper suicide prevention program work in a school setting? Evaluating training outcome and moderators of effectiveness. Suicide Life Threat. Behav. 2010, 40, 506–515. [Google Scholar] [CrossRef] [PubMed]
- Silva, C.; Smith, A.R.; Dodd, D.R.; Covington, D.W.; Joiner, T.E. Suicide-Related Knowledge and Confidence Among Behavioral Health Care Staff in Seven States. Psychiatr. Serv. 2016, 67, 1240–1245. [Google Scholar] [CrossRef]
- Ramberg, I.L.; Di Lucca, M.A.; Hadlaczky, G. The Impact of Knowledge of Suicide Prevention and Work Experience among Clinical Staff on Attitudes towards Working with Suicidal Patients and Suicide Prevention. Int. J. Environ. Res. Public Health 2016, 13, 195. [Google Scholar] [CrossRef]
- Ramberg, I.L.; Wasserman, D. Benefits of implementing an academic training of trainers program to promote knowledge and clarity in work with psychiatric suicidal patients. Arch Suicide Res 2004, 8, 331–343. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.; Krishna, M.; Rajendra, R.G.; Keenan, P. Nurses attitudes and beliefs to attempted suicide in Southern India. Journal of Mental Health 2015, 24, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Davison, J.; Mackay, B.; McGivern, M.J. The potential of sim ulation to enhance nursing students’ preparation for suicide risk assessment: A review. Open Journal of Nursing 2017, 7, 129–144. [Google Scholar]
- Giacchero Vedana, K.G.; Magrini, D.F.; Zanetti, A.C.G.; Miasso, A.I.; Borges, T.L.; Dos Santos, M.A. Attitudes towards suicidal behaviour and associated factors among nursing professionals: A quantitative study. J Psychiatr Ment Health Nurs 2017, 24, 651–659. [Google Scholar] [CrossRef]
- Vedana, K.G.G.; Magrini, D.F.; Miasso, A.I.; Zanetti, A.C.G.; de Souza, J.; Borges, T.L. Emergency Nursing Experiences in Assisting People With Suicidal Behavior: A Grounded Theory Study. Arch Psychiatr Nurs 2017, 31, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Joiner, T.E., Jr.; Hollar, D.; Kimberly Van, O. ON BUCKEYES, GATORS, SUPER BOWL SUNDAY, AND THE MIRACLE ON ICE: “PULLING TOGETHER” IS ASSOCIATED WITH LOWER SUICIDE RATES. Journal of Social and Clinical Psychology 2006, 25, 179–195. [Google Scholar] [CrossRef]
- Nock, M.K.; Hwang, I.; Sampson, N.; Kessler, R.C.; Angermeyer, M.; Beautrais, A.; Borges, G.; Bromet, E.; Bruffaerts, R.; de Girolamo, G.; et al. Cross-national analysis of the associations among mental disorders and suicidal behavior: findings from the WHO World Mental Health Surveys. PLoS Med 2009, 6, e1000123. [Google Scholar] [CrossRef]
- AG, T. Psychiatric care of people at risk of committing suicide: Narrative interviews with registered nurses, physicians, patients and their relatives; Umeå University: Sweden, 2001. [Google Scholar]
- Samuelsson, M.; Sunbring, Y.; Winell, I.; Asberg, M. Nurses’ attitudes to attempted suicide patients. Scand J Caring Sci 1997, 11, 232–237. [Google Scholar] [CrossRef]
- da Silva Cais, C.F.; da Silveira, I.U.; Stefanello, S.; Botega, N.J. Suicide prevention training for professionals in the public health network in a large Brazilian city. Arch Suicide Res 2011, 15, 384–389. [Google Scholar] [CrossRef]
- Ouzouni C, N.K. Nurses’ attitudes towards attempted suicide. Health Science Journal 2013, 7, 119–134. [Google Scholar]
- O’Brien, S.E.; Stoll, K.A. Attitudes of medical and nursing staff towards self-poisoning patients in a London hospital. Int J Nurs Stud 1977, 14, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Osafo, J.; Knizek, B.L.; Akotia, C.S.; Hjelmeland, H. Attitudes of psychologists and nurses toward suicide and suicide prevention in Ghana: a qualitative study. Int J Nurs Stud 2012, 49, 691–700. [Google Scholar] [CrossRef] [PubMed]
- Norheim, A.B.; Grimholt, T.K.; Loskutova, E.; Ekeberg, O. Attitudes toward suicidal behaviour among professionals at mental health outpatient clinics in Stavropol, Russia and Oslo, Norway. BMC Psychiatry 2016, 16, 268. [Google Scholar] [CrossRef] [PubMed]
- Kishi, Y.; Kurosawa, H.; Morimura, H.; Hatta, K.; Thurber, S. Attitudes of Japanese nursing personnel toward patients who have attempted suicide. Gen Hosp Psychiatry 2011, 33, 393–397. [Google Scholar] [CrossRef] [PubMed]
- Saunders, K.E.; Hawton, K.; Fortune, S.; Farrell, S. Attitudes and knowledge of clinical staff regarding people who self-harm: a systematic review. J. Affect. Disord. 2012, 139, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Wimsatt, L.A.; Schwenk, T.L.; Sen, A. Predictors of Depression Stigma in Medical Students: Potential Targets for Prevention and Education. Am J Prev Med 2015, 49, 703–714. [Google Scholar] [CrossRef]
- Ramberg, I.L.; Wasserman, D. Suicide-preventive activities in psychiatric care: evaluation of an educational programme in suicide prevention. Nord J Psychiatry 2004, 58, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Barney, L.J.; Griffiths, K.M.; Jorm, A.F.; Christensen, H. Stigma about Depression and its Impact on Help-Seeking Intentions. Australian & New Zealand Journal of Psychiatry 2006, 40, 51–54. [Google Scholar] [CrossRef]
- Jorm, A.F.; Wright, A.; Morgan, A.J. Where to seek help for a mental disorder? National survey of the beliefs of Australian youth and their parents. Med J Aust 2007, 187, 556–560. [Google Scholar] [CrossRef]
- McNair, B.G.; Highet, N.J.; Hickie, I.B.; Davenport, T.A. Exploring the perspectives of people whose lives have been affected by depression. Med J Aust 2002, 176, S69–76. [Google Scholar] [CrossRef]
- Hooper, L.M.; Epstein, S.A.; Weinfurt, K.P.; DeCoster, J.; Qu, L.; Hannah, N.J. Predictors of primary care physicians’ self-reported intention to conduct suicide risk assessments. J. Behav. Health Serv. Res. 2012, 39, 103–115. [Google Scholar] [CrossRef] [PubMed]
- Feldman, M.D.; Franks, P.; Duberstein, P.R.; Vannoy, S.; Epstein, R.; Kravitz, R.L. Let’s not talk about it: suicide inquiry in primary care. Ann. Fam. Med. 2007, 5, 412–418. [Google Scholar] [CrossRef] [PubMed]
- Nutting, P.A.; Dickinson, L.M.; Rubenstein, L.V.; Keeley, R.D.; Smith, J.L.; Elliott, C.E. Improving detection of suicidal ideation among depressed patients in primary care. Ann. Fam. Med. 2005, 3, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Michail, M.; Tait, L. Exploring general practitioners’ views and experiences on suicide risk assessment and management of young people in primary care: a qualitative study in the UK. BMJ Open 2016, 6, e009654. [Google Scholar] [CrossRef]
- Tierney, E. Health care in contemporary Japanese religions. In Healing and Restoring—Health and Medicine in the World’s Religious Traditions; LE, S., Ed.; Macmillan: New York, 1989. [Google Scholar]
- Takahashi, Y. Culture and suicide: from a Japanese psychiatrist’s perspective. Suicide Life Threat. Behav. 1997, 27, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Thimmaiah, R.; Poreddi, V.; Ramu, R.; Selvi, S.; Math, S.B. Influence of Religion on Attitude Towards Suicide: An Indian Perspective. Journal of Religion and Health 2016, 55, 2039–2052. [Google Scholar] [CrossRef] [PubMed]
- Shoib, S.; Armiya’u, A.Y.; Nahidi, M.; Arif, N.; Saeed, F. Suicide in Muslim world and way forward. Health Sci Rep 2022, 5, e665. [Google Scholar] [CrossRef]
- Ministry of Home Affairs (MHA), G.o.I. Census of India. Available online: https://censusindia.gov.in/census.website/data/census-tables (accessed on.
- Colucci, E.; Martin, G. Religion and spirituality along the suicidal path. Suicide Life Threat Behav 2008, 38, 229–244. [Google Scholar] [CrossRef]
- Ranjan, R.; Kumar, S.; Pattanayak, R.D.; Dhawan, A.; Sagar, R. (De-) criminalization of attempted suicide in India: A review. Ind Psychiatry J 2014, 23, 4–9. [Google Scholar] [CrossRef]
- Holm, U.; Aspegren, K. Pedagogical methods and affect tolerance in medical students. Med Educ 1999, 33, 14–18. [Google Scholar] [CrossRef]
- JC, S. Suicide: can we prevent the most mysterious act of the human being? Rev Port Enferm Saúde Mental 2015, 7–8. [Google Scholar]
- Anderson, M.; Standen, P.; Nazir, S.; Noon, J.P. Nurses’ and doctors’ attitudes towards suicidal behaviour in young people. Int J Nurs Stud 2000, 37, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Baykan, N.; Arslantürk, G.; Durukan, P. Desensitizing Effect of Frequently Witnessing Death in an Occupation: A Study With Turkish Health-Care Professionals. OMEGA - Journal of Death and Dying 2020, 84, 567–581. [Google Scholar] [CrossRef] [PubMed]
- Boukouvalas, E.; El-Den, S.; Murphy, A.L.; Salvador-Carulla, L.; O’Reilly, C.L. Exploring Health Care Professionals’ Knowledge of, Attitudes Towards, and Confidence in Caring for People at Risk of Suicide: a Systematic Review. Arch Suicide Res 2020, 24, S1–s31. [Google Scholar] [CrossRef] [PubMed]
- Waterman, P. Even Accidental Counsellors Have to Be Brave. Australian Pharmacist 2010, 29, 1015. [Google Scholar]
- Osman, A. Suicide prevention. Br. Dent. J. 2021, 230, 115–115. [Google Scholar] [CrossRef] [PubMed]
- Eskin, M.; Baydar, N.; El-Nayal, M.; Asad, N.; Noor, I.M.; Rezaeian, M.; Abdel-Khalek, A.M.; Al Buhairan, F.; Harlak, H.; Hamdan, M.; et al. Associations of religiosity, attitudes towards suicide and religious coping with suicidal ideation and suicide attempts in 11 muslim countries. Soc. Sci. Med. 2020, 265, 113390. [Google Scholar] [CrossRef]
- Siau, C.S.; Wee, L.H.; Wahab, S.; Visvalingam, U.; Yeoh, S.H.; Halim, N.A.A.; Ibrahim, N. The influence of religious/spiritual beliefs on Malaysian hospital healthcare workers’ attitudes towards suicide and suicidal patients: a qualitative study. J. Res. Nurs. 2021, 26, 723–740. [Google Scholar] [CrossRef]
- Gearing, R.E.; Alonzo, D. Religion and Suicide: New Findings. Journal of Religion and Health 2018, 57, 2478–2499. [Google Scholar] [CrossRef]
- Coppens, E.; Van Audenhove, C.; Iddi, S.; Arensman, E.; Gottlebe, K.; Koburger, N.; Coffey, C.; Gusmão, R.; Quintão, S.; Costa, S.; et al. Effectiveness of community facilitator training in improving knowledge, attitudes, and confidence in relation to depression and suicidal behavior: Results of the OSPI-Europe intervention in four European countries. J. Affect. Disord. 2014, 165, 142–150. [Google Scholar] [CrossRef]
- Stover, A.N.; Lavigne, J.E.; Carpenter, D.M. A Scoping Review of Suicide Prevention Training Programs for Pharmacists and Student Pharmacists. Am J Pharm Educ 2023, 87, ajpe8917. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.; Mehta, R.; Dave, K.; Chaudhary, P. Effectiveness of gatekeepers’ training for suicide prevention program among medical professionals and medical undergraduate students of a medical college from Western India. Industrial Psychiatry Journal 2021, 30. [Google Scholar]
- Bolton, S.-L. Evalua&on of a gatekeeper training program as suicide intervention training for medical students: A randomized controlled trial. The University of Manitoba 2015.
- Rallis, B.A.; Esposito-Smythers, C.; Disabato, D.J.; Mehlenbeck, R.S.; Kaplan, S.; Geer, L.; Adams, R.; Meehan, B. A brief peer gatekeeper suicide prevention training: Results of an open pilot trial. J Clin Psychol 2018, 74, 1106–1116. [Google Scholar] [CrossRef]
- Nebhinani, N.; Kuppili, P.P.; Paul, K. Effectiveness of Brief Educational Training on Medical Students’ Attitude toward Suicide Prevention. J Neurosci Rural Pract 2020, 11, 609–615. [Google Scholar] [CrossRef] [PubMed]
- Foster, A.; Chaudhary, N.; Murphy, J.; Lok, B.; Waller, J.; Buckley, P.F. The Use of Simulation to Teach Suicide Risk Assessment to Health Profession Trainees-Rationale, Methodology, and a Proof of Concept Demonstration with a Virtual Patient. Academic psychiatry 2015, 39, 620–629. [Google Scholar] [CrossRef]
- Stuart, C.; Waalen, J.K.; Haelstromm, E. Many helping hearts: an evaluation of peer gatekeeper training in suicide risk assessment. Death Stud 2003, 27, 321–333. [Google Scholar] [CrossRef] [PubMed]
- Tompkins, T.L.; Witt, J. The short-term effectiveness of a suicide prevention gatekeeper training program in a college setting with residence life advisers. J Prim Prev 2009, 30, 131–149. [Google Scholar] [CrossRef]
- Cross, W.; Matthieu, M.M.; Lezine, D.; Knox, K.L. Does a brief suicide prevention gatekeeper training program enhance observed skills? Crisis 2010, 31, 149–159. [Google Scholar] [CrossRef]
- Taub, D.J.; Servaty-Seib, H.; Miles, N.; Lee, J.Y.; Morris, C.A.; Prieto-Welch, S.L.; et al. The impact of gatekeeper training for suicide prevention on university resident assistants. J Coll Couns 2013, 16, 64–78. [Google Scholar] [CrossRef]
- Cimini, M.D.; Rivero, E.M.; Bernier, J.E.; Stanley, J.A.; Murray, A.D.; Anderson, D.A.; Wright, H.R.; Bapat, M. Implementing an audience-specific small-group gatekeeper training program to respond to suicide risk among college students: a case study. J Am Coll Health 2014, 62, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Cwik, M.F.; Tingey, L.; Wilkinson, R.; Goklish, N.; Larzelere-Hinton, F.; Barlow, A. Suicide Prevention Gatekeeper Training: Can They Advance Prevention in Indian Country? Arch Suicide Res 2016, 20, 402–411. [Google Scholar] [CrossRef] [PubMed]
- NA, I. Outcomes of a suicide prevention gatekeeper training on a university campus. J Coll Stud Dev 2011, 52, 350–363. [Google Scholar]
- Matthieu, M.M.; Chen, Y.; Schohn, M.; Lantinga, L.J.; Knox, K.L. Educational preferences and outcomes from suicide prevention training in the Veterans Health Administration: one-year follow-up with healthcare employees in Upstate New York. Mil Med 2009, 174, 1123–1131. [Google Scholar] [CrossRef] [PubMed]
- Capp, K.; Deane, F.P.; Lambert, G. Suicide prevention in Aboriginal communities: application of community gatekeeper training. Aust N Z J Public Health 2001, 25, 315–321. [Google Scholar] [CrossRef]
- Cross, W.; Matthieu, M.M.; Cerel, J.; Knox, K.L. Proximate outcomes of gatekeeper training for suicide prevention in the workplace. Suicide Life Threat Behav 2007, 37, 659–670. [Google Scholar] [CrossRef]
- Isaac, M.; Elias, B.; Katz, L.Y.; Belik, S.-L.; Deane, F.P.; Enns, M.W.; Sareen, J. Gatekeeper Training as a Preventative Intervention for Suicide: A Systematic Review. The Canadian Journal of Psychiatry 2009, 54, 260–268. [Google Scholar] [CrossRef]
- Nasir, B.F.; Hides, L.; Kisely, S.; Ranmuthugala, G.; Nicholson, G.C.; Black, E.; Gill, N.; Kondalsamy-Chennakesavan, S.; Toombs, M. The need for a culturally-tailored gatekeeper training intervention program in preventing suicide among Indigenous peoples: a systematic review. BMC Psychiatry 2016, 16, 357. [Google Scholar] [CrossRef]
- Kitchener, B.A.; Jorm, A.F. Mental health first aid training for the public: evaluation of effects on knowledge, attitudes and helping behavior. BMC Psychiatry 2002, 2, 10. [Google Scholar] [CrossRef]
- Aseltine, R.H.; DeMartino, R. An outcome evaluation of the SOS Suicide Prevention Program. American journal of public health 2004, 94, 446–451. [Google Scholar] [CrossRef]
- P, R. Review of the Applied Suicide Intervention Skills Training program (ASIST): Rationale, evaluation results, and directions for future research. 2010. [Google Scholar]

Table 1.
Summary of included studies.
| Author (year); countrya | Objectives | Study design and instruments | N; Health programsƵ | Year of studyƵ | Population characteristics (mean age; gender) Ƶ | Personal experience of mental health issues and suicideƵ | Outcomes | |
|---|---|---|---|---|---|---|---|---|
| KnowledgeƵ | AttitudeƵ | |||||||
| Amiri et al. (2013); UAE [25] |
|
|
115; Medical |
|
20.7y; 51.9% female |
|
NA |
|
| Ferrara et al. (2022); Italy [27] |
|
|
409; Nursing |
|
22y; 63.1% female |
|
|
|
| Giacchero Vedana et al. (2019); Brazil [28] |
|
|
111; Nursing |
|
22.6y; 86.5% female |
|
|
|
| Kavalidou et al. (2013); Greece [30] |
|
|
105; Medical |
|
22.4y, 61.0% female |
|
NA |
|
| Kelly et al. (2023); UK [32] |
|
|
30; Dental |
|
NA; 67% female | NA |
|
|
| Krueger (1979); US [34] |
|
|
6; Medical | NA | NA; NA | NA |
|
|
| Lappann Botti et al. (2015); Brazil [35] |
|
|
58; Nursing |
|
21-25y; 89.7% female | NA | Factor 2 by item: 1.2: low confidence in dealing with suicidal person |
|
| López-Narváez et al. (2020); Mexico [36] |
|
|
355; Medical, nursing | NA | 20.47y; 61.4% female |
|
NA |
|
| Marques Moraes et al. (2016); Brazil [37] |
|
|
244; Nursing |
|
42.2% 21.0-22.9y; 86.5% female |
|
|
|
| Öz et al. (2022); Turkey [38] |
|
560; Nursing |
|
19.3y; 63.7% female |
|
NA |
|
|
| Poreddi et al. (2021); India [41] |
|
|
223; Nursing |
|
19.8y; 89.7% female |
|
NA |
|
| Vedana et al. (2018); Brazil [43] |
|
|
30; Nursing |
|
87% <25y; 87% female | NA | NA |
|
| Arafat et al. (2022); Bangladesh [44] |
|
|
162; Medical | NA | 18-27y; NA | NA |
|
|
| Bajracharya et al. (2020); Nepal [45] |
|
|
103; Nursing |
|
19.8y; NA |
|
NA |
|
| Chan et al. (2014); Australia [46] |
|
219; Medical |
|
24.6y; 53.8% female | NA |
|
|
|
| Cryer et al. (2020); Australia [49] |
|
|
116; Medical |
|
25.02y; 58% female | NA | NA |
|
| Hamaoka et al. (2007); US [50] |
|
|
12; Medical | NA | NA; NA | NA | NA |
|
| Mospan et al. (2020); US [51] |
|
|
73; Pharmacist |
|
NA; 66% female |
|
|
|
| Neimeyer et al. (1983); US [52] |
|
|
141; Medical |
|
25.3y; 27.4 % female | NA |
|
NA |
| Patel et al. (2016); Australia [53] |
|
116; Medical |
|
25.0y; NA |
|
|
NA | |
| Sato et al. (2006); Japan [57] |
|
|
160; Medical |
|
21.5y; 41.2% female | NA |
|
|
| Scheckel et al. (2014); US [58] |
|
|
11; Nursing |
|
21-26y; 100% female | NA |
|
|
| Sun et al. (2020) , Taiwan [59] |
|
|
22; Nursing |
|
20-23y; 95.5% female | NA |
|
|
| Vedana et al. (2022); Portugal [60] |
|
|
13; Nursing |
|
53.8% 22y; 92.3% female |
|
NA |
|
| Wahab et al. (2021); Malaysia [61] |
|
290; Medical |
|
22.4y; 49.7% female |
|
NA |
|
|
| Williams et al. (2015); Australia [65] |
|
|
554; Paramedic, paramedic/nursing |
|
83% <25y; 69.1% female | NA | NA |
|
| Zohn et al. (2022); US [67] |
|
|
14; Nursing |
|
22-43y; 92.9% female | NA |
|
|
| Hawgood et al. (2008); Australia [68] |
|
|
373; Medical |
|
25.9y; 55% female | NA |
|
|
| Price et al. (2022); US [69] |
|
|
360; Medical |
|
NA; NA | NA |
|
|
| Domino et al. (1991); US, Japan [70] |
|
|
|
NA |
|
|
NA |
|
| Emul et al. (2011); Turkey [71] |
|
|
234; Medical |
|
NA; NA | NA | NA |
|
| Eskin et al. (2011); Austria, Turkey [26] |
|
|
|
|
|
NA |
|
|
| Etzersdorfer et al. (1998); India, Austria [74] |
|
|
NA; Medical | NA |
|
|
NA |
|
| Wallin et al. (2003); Sweden [76] |
|
|
306; Medical |
|
|
|
NA |
|
| Nebhinani et al. (2013); India [77] |
|
|
308; Nursing | NA | 20y; 95.1% female |
|
|
|
| Sun et al. (2019); Taiwan [78] |
|
|
22; Nursing | NA | 20-23y; 95.5% female |
|
|
|
| Slobodanka Bašić et al. (2004); Serbia [79] |
|
|
150; Medical |
|
NA; 58.7% female | NA |
|
|
| Oncü et al. (2008); Turkey [80] |
|
|
41; Medical | NA | 23.3y; 46.3% female | NA | NA |
|
| Fan-Ko et al. (2011); Taiwan [82] |
|
|
79; Nursing |
|
26.8y; 97.7% female |
|
|
|
| Willson et al. (2020); US [84] |
|
|
158; Pharmacists |
|
NA; 63% female |
|
|
NA |
| Hjelvik et al. (2022): US [85] |
|
|
273; Medical |
|
NA; NA | NA |
|
|
| Pothireddy et al. (2022); US [87] |
|
|
139; Pharmacist |
|
23.8y; NA |
|
|
|
| Retamero et al. (2014); US [89] |
|
|
180; Medical |
|
NA; NA | NA | NA |
|
| Yousuf et al. (2013); Hong Kong [90] |
|
|
22; Medical |
|
20-23y; 32% female |
|
NA |
|
| Mckeirnan et al. (2023); US [91] |
|
|
205; Pharmacist |
|
NA; NA |
|
|
|
| Carpenter et al. (2023); US [95] |
|
|
146; Pharmacist |
|
23.6y; 67% female |
|
|
NA |
aUAE: United Arab Emirates; UK: United Kingdom; US: United States. bItems were rated (1= completely disagree,5= completely agree) and presented in mean.cSBAQ-ita scale: evaluated D1 “Feeling toward the patient,” D2 “Professional ability,” D3 “Right to suicide,” and D4 “Knowledge. Responses rated (1 = completely disagree, 10 = completely agree), presented in mean. dSBAQ [29]: Suicide Behavior Attitude Questionnaire. Items are grouped into three factors, with scores of 0-30 points for each group. Factor 1 “negative feelings toward the patient”, higher scores indicate a greater presence of negative feelings. Factor 2 “self-perception of professional competence”, higher scores indicate more self-confidence in dealing with suicidal individuals. Factor 3 “right to suicide”, higher scores represent a less “moralistic/condemnatory” attitude. Items presented as mean. eSOQ [31]: Suicide Opinion Questionnaire. Consisting of eight clinical sub-scales: “Suicide reflects Mental Illness”; “Suicide threats are “not real” – i.e. a “Cry for Help”; “Right to Die”; “Importance of Religion”; “Impulsivity”; “Suicide is Normal”; “Suicide reflects Aggression/Anger”; and, “Suicide is Morally Bad”. Rated ‘strongly agree’, ‘agree’, ‘undecided’, ‘disagree’, and ‘strongly disagree’. Nine specific questions had a reversed scoring. fQABSB: Questionnaire of Attitudes Before Suicidal Behavior. Data was clustered into three factors. Factor 1- negative feelings with suicidal patient, the higher the score, the more the presence of negative feelings. Factor 2- perception of professional competence to deal with patients with suicidal behavior, a higher score may mean more confident professionals. Factor 3- right to suicide, a higher score can mean at least “moralist/judicious” attitude. Each factor scoring varied from 0-30 points. Items presented as mean. gATSP [33]: Attitude Toward Suicide Prevention. Evaluated on a 5-point Likert scale ranging from “strongly agree” to “strongly disagree”. The higher the score, the more negative the attitude. hSOSS [39,54]: Stigma of Suicide Scale. 5-point Likert-type scale with three subdimensions: Stigma, Isolation/Depression, and Glorification/Normalization. Each item is marked “strongly disagree,” “disagree,” “uncertain,” “agree,” and “strongly agree”. The weights of each subdimension is evaluated by considering the mean score for each subdimension. iDAP-R [40]: Death Attitude Profile-Revised. The scale consists of three subdimensions: Neutral Acceptance and Approach Acceptance, Escape Acceptance, and Fear of Death and Death Avoidance. The scale is evaluated based on both the scores for the subdimensions and the total score for the whole scale, high mean scores for the whole and subscales indicate a positive attitude toward death. The highest score that can be obtained from the scale is 182 while the lowest score is 26. jSuicide Attitude Questionnaire [42]: measured nursing students’ attitudes towards suicidal behaviors in five domains: the acceptability of suicidal behaviors, morality, and mental illness, professional role, work and care, communication and attention, and belief from 1 (strongly disagree) to 5 (strongly agree). Possible score range 30–150, a higher score reflects a positive caring attitude towards suicidal behaviors. Data presented as mean. kLOSS-B: Bangla literacy of suicide scale. Adapted from the original instrument from Calear [47]. Assesses suicide literacy in: signs and symptoms, nature of suicide, risk factors, and preventive measures. Total score ranges from 0 to 12, calculated based on the correct answer. Data was presented as mean. lSOSS-B: Bangla stigma of suicide scale. The scale has three subscales: stigmatization, isolation/depression, and normalization/glorification, rated strongly disagree (1), disagree (2), neutral (3), agree (4), and strongly agree (5) with each subscale score determined by calculating the mean of responses to items within the subscale. Data presented as mean. mSOQ: Suicide Opinion Questionnaire. Measure suicide on the basis of: permissiveness, unpredictability, incomprehensibility, noncommunication, right to prevent, preventability, relation cause, and duration of suicide process. The questionnaire was rated 1=strongly agree, 2=agree, 3= don’t know, 4=disagree, and 5=strongly disagree’. Data presented as mean. nLOSS [47]: Literacy of Suicide Scale. Assess suicide literacy based on (a) signs and symptoms, (b) causes of the nature of suicidality, (c) risk factors, and (d) treatment and prevention. Literacy scores are the sum of correct items, with higher scores indicating higher suicide literacy. Data presented as mean. oGeneral Help-Seeking Questionnaire [48] asks the question ‘If you were experiencing suicidal thoughts, how likely is it that you would seek help from the following people?’. The sources were categorized as formal help, informal help and no help sought, with each item rated from ‘highly unlikely’ to ‘highly likely’. Data presented as mean. pAdapted version of SOSS [39]: respondents were presented with a range of descriptors of a person who died by suicide/diagnosed with each condition and asked to respond to each item ranging from 1 (strongly disagree) to 5 (strongly agree). The SOSS produces three sub-scales assessing “stigma,” “normalization/ glorification,” and “isolation/depression.” Mean score for each subscale was calculated; higher scores indicate greater stigma, glorification/normalization, and isolation/depression, respectively. qATTS: Attitudes Toward Suicide. The authors reduced the ATTS scale from 39 to 22 questions to limit participant fatigue. Rating ranging from strongly agree (5) to strongly disagree (1). Data was presented as median. rSIRI: Suicide Intervention Response Inventory. 25 item questionnaire with forced-choice between the two response options, total score represents the number of correct options endorsed. Data presented in mean. sLOSS [54]: Literacy of Suicide Scale. The scale includes 12 statements assessing knowledge of suicide, rated as ‘true/false/don’t know.’ Each correct response attracts a score of one, with total scale scores ranging from 0 to 12. Higher scores are indicative of greater suicide literacy. Data presented in mean. tIPIP-FFM [55]: International Personality Item Pool Five-Factor model. Assess participants’ openness to experience, agreeableness, conscientiousness, neuroticism, and extraversion. uNarcissism scale [56]: Each item rated on a three-point ‘true/false/don’t know’ scale, total scale scores ranging from 0 to 13, higher scores indicating greater narcissism. vQuestionnaire assess knowledge concerning suicide in Japan (statistical data, risk factors, and suicide prevention measures). Eight multiple-choice questions and one open-ended question concerned the student’s attitude toward suicidal behavior (classified by all authors’ consensus as sympathetic, critical, unconcerned, and no answer). Data presented in mean. wATTS [62]: Attitudes Toward Suicide. Scored ranging from 1 (strongly disagree) to 5 (strongly agree). 11 interpretable factors as “ability to understand and accept suicide” (D1); “suicide among youth and tabooing” (D2); “believability of suicidal threats” (D3); “loneliness and avoidance as suicide triggers” (D4); “judgment and ability to help” (D5); “nature of suicidal ideation” (D6); “acceptability of assisted suicide” (D7); “suicide as communication” (D8); “incomprehensibility” (D9); “normality of suicide” (D10); and “duty to prevent and mental illness” (D11) were assessed. Malay validated form was used [97]. xGHSQ [63,64]: General Help-Seeking Behaviour Questionnaire. Evaluate different help-seeking targets in response to two hypothetical scenarios in which a personal emotional problem and suicidal thoughts were experienced. Items were measured from 1 (extremely unlikely) to 7 (extremely likely).yMCRS [66]: Medical Condition Regard Scale. Capture a health professional’s bias, emotions and expectations in treating a patient with specific condition and allow for comparison between them rated on from 1(strongly disagree) to 6 (strongly agree) (maximum score 66). Data presented in mean. zASP: Attitudes to Suicide Prevention. 14 scale items, each coded from 1 (Strongly Disagree) to 5 (Strongly Agree). Total score (ranging from 14 to 70) and individual items were scored and compared among. Data presented in mean. €SDS: Social distance scale. Measures eight items related to social avoidance (each item scored from definitely unwilling, probably unwilling, probably willing, definitely willing).¥SAS: Skillfulness assessment scale. Includes eight questions; rated where point 1 or 2 indicate definitely agree; 3,4 and 5 points indicate neutral; 6 and 7 points indicate definitely disagree. §DS: Dangerousness scale. includes eight questions; rated where point 1 or 2 indicate definitely agree; 3,4 and 5 points indicate neutral; 6 and 7 points indicate definitely disagree. ƗOpinions and attitudes towards suicide [72]: responses to these items were made on 5-point scales (1: Completely disagree; 5: Completely agree). Data presented as mean. ƛReactions to an imagined suicidal friend[72,73]: requested participants to imagine a close friend who decides to kill herself or himself and reveals their reactions and feelings to the respondent using 5-point scales (1: Completely disagree; 5: Completely agree).ƞSUIATT [75]: suicide attitude. Covers attitudes towards suicide and attempted suicide and epidemiological issues (previous suicidal ideation and previous suicide attempts). Responses to each statement are along a five point scale (strong agreement to strong disagreement). 19 subscales were derived.ƟAttitude toward suicide prevention scale [33]: 14 items, self-rated on 5-point Likert scale. ƠATSS [81]: Attitudes Toward Suicide Scale. Rated from “strongly disagree” to“strongly agree” (strongly disagree = 1, undecided = 3, strongly agree = 5). Two of the attitude questions are rated differently, which are questioning probability of one’s own future suicide (a possibility = 1, under certain circumstances = 2, probably not = 3, never = 4), and to what degree suicide should be prevented (in all cases = 1, all but few exceptions = 2, in some cases yes, in some cases no = 3,not in any case = 4). The questionnaire also has two open ended questions asking about the most important cause of suicide and what should be done for suicide prevention. Data presented as mean. ƣ30 items [83] were divided into five categories regarding: the acceptability of suicidal behaviours, morality and mental illness, professional role, work and care, communication and attention and beliefs, rated on from 1 (strongly disagree) – 5 (strongly agree). Possible score range of 30–150. High scores reflected positive caring attitudes towards suicidal behaviours. ƧThe survey [93,98] includes knowledge assessment (15 questions) pre and post training program.ƪSets of yes/no statements on 5-point Likert scales (1 = strongly disagree, 5 = strongly agree) [86]. Item presented as mean. ưA slider was used to indicate level of agreement, ranging from 0= strongly disagree to 100= strongly agree [88]. Data presented as mean. ṼCASQ-HK: Chinese Attitude toward Suicide Questionnaire. Contains 73 statements about attitudes towards suicide (1 = absolutely agree and 5 = absolutely disagree), and 12 difficulties-related scenarios (eg suffering from a chronic mental illness, business failure, etc) and participant’s likelihood of considering suicide in each scenario (1 = definitely not consider and 5 = definitely consider). ẀOMS-HC[92]: Opening Minds to Stigma Scale for Healthcare Providers. Likert scale was used (5 = strongly agree to 1 = strongly disagree). ƵNA: Not available. ǡSuicidal thoughts were assessed on a scale of 0-10 (10: very frequent). ǽPersonal exposure to suicide was rated on a 10-point scale from ‘I have had no exposure to suicide’ to ‘I have attempted suicide myself’. ǿUS: United States. ȅItems were rated (1= not at all sad,7= very sad) and presented in mean. ȍMood was assessed (1: Not at all sad; 7: Very sad) and presented as mean (M). ẊAlGEE[94]: Approach and assess for risk of suicide or harm; Listen non-judgmentally; Give reassurance and information; Encourage appropriate professional help; and Encourage self-help and other support strategies. ẐConsists of 2 components: knowledge (2 items on how many agents carried a warning label for the risk of suicidal behavior and whether suicide was a top 10 cause of death in the United States in 2019, scores ranging from 0-2, higher score indicates better knowledge) and self- efficacy (7 items measured on a 5-point scale ranging from 1 = not at all confident to 5 = extremely confident)[96].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



