
Submitted:
07 July 2025
Posted:
08 July 2025
You are already at the latest version
Abstract
Self-harm is often stigmatised by healthcare professionals. Little is known about how certain characteristics of the behaviour, like the degree of suicidal intent, affects clinicians’ judgements and responses. This study explored how intent of self-harm (suicidal or non-suicidal) affects trainee practitioners’ views, attitudes towards the behaviour and clinical decision-making. A qualitative study using semi-structured online inter-views was conducted. Interviews were audio-recorded, transcribed verbatim and ana-lysed using reflexive thematic analysis. Sixteen trainee healthcare practitioners (psychological wellbeing practitioners, clinical/counselling psychologists, nurses, medics) were interviewed. Three themes were identified: (1) interpreting intent in self-harm: clinical utility and challenges, (2) perceived responsibility of self-harm and (3) Trainees struggle for equal care in a hierarchical system. Participants observed staff expressing pejorative views towards both forms of self-harm but did not share them. Across most clinical decisions, intent informed trainees’ judgements and beliefs. Clients presenting with suicidal-related self-harm received more urgent care but fewer therapeutic interventions. Trainees felt ambivalent about distinguishing intent. Nevertheless, this dis-tinction was evident across treatment, risk and care decisions. A consistent approach towards suicidal and non-suicidal self-harm is important. Trainees should be supported in addressing difficult emotions arising from this work, helping shift the blame culture and promote a more empathic approach.
Keywords:
self-harm
; suicidal
; non-suicidal
; function
; stigma
; healthcare professionals
; trainee
; thematic analysis
1. Introduction
Self-harm refers to intentional self-poisoning or injury to oneself, irrespective of the apparent purpose of the act, and includes a variety of behaviours like self-cutting, burning and overdoses [1]. Self-harm is a global health issue, affecting approximately 15 million people annually [2]. In the UK, 6.4% of individuals reported self-harming within their lifetime with 20.6% of these experiencing suicidal ideation [3]. Despite its prevalence, self-harm is often misunderstood and highly stigmatised. Public stigma involves labelling, stereotyping and discriminating against others based on perceived negative characteristics [4]. Common pejorative stereotypes include self-harm being selfish, manipulative and attention-seeking [5,6,7]. Healthcare professionals are not immune from societal stigma. In a Canadian sample of staff who worked in senior leadership in the area of client safety or mental health, 79% recalled personal experiences of discriminating against their clients and 53% observed colleagues’ discriminatory behaviour [8]. Similar negative attitudes have been found in UK healthcare settings, with clients labelled as difficult to manage, lacking co-operation and being untrustworthy [9,10,11,12]. Emergency department nurses viewed clients who attended accident and emergency (A&E) because of self-harm as less deserving of a bed compared to those who did not engage in self-harm [13].
Stigmatising views held by healthcare professionals may hinder client engagement. Individuals who self-harm often report feeling misunderstood or disregarded due to the lack of empathy and engagement from healthcare professionals [14,15]. Stigma can influence clinical decision-making, with some healthcare professionals either refusing treatment [16,17,18,19,20] or focusing solely on treating the physical injury whilst neglecting mental health needs [21]. Additionally, stigma can discourage help-seeking behaviours due to fear of judgement, rejection and lack of trust and empathy in healthcare providers [22,23,24]. Those currently undergoing training as health professionals are the next generation of practitioners who will shape how care for self-harm is implemented in the future. Understanding trainee healthcare practitioners’ perspectives is essential, as reflecting on these views early in their training can help address biases and improve future practice.
Self-harm is not formally distinguished by intent in the UK NICE guidelines [1], which encompass behaviours with and without suicidal intent (e.g. suicidal and non-suicidal) [25]. This contrasts with a portion of the research literature that draws a distinction between non-suicidal self-injury (NSSI) and suicidal behaviour. NSSI involves intentional injury to the body without the intent to end one’s life and can serve a variety of functions including coping with emotional distress [25,26]. A suicide attempt (SA), in contrast, refers to injuring oneself with the intent to die [27]. However, research indicates that individuals can engage in self-harm and experience suicidal thoughts without having the intent to end their life [28,29]. Intention of self-harm is theorised to vary across a continuum [30]. Yet, despite this complexity, research has often treated NSSI and suicidal behaviour as distinct constructs, potentially oversimplifying the diverse nature of self-harm and suicidal behaviours [31].
There is debate about the classification of self-harm by intent in clinical practice [32]. It may be difficult for healthcare professionals to ascertain when intent has changed as clients may be unaware [33] or clinicians’ perception of suicidal intent may differ from the client’s [34]. Physical healthcare professionals, focused on treating the physical injury, may not benefit from distinguishing intent, as their primary concern is managing the immediate physical harm rather than the underlying psychological motivation [35]. Alternatively, intent may add value in further understanding the behaviour and implementing focused interventions [36]. For example, several authors suggest NSSI differs in motivations, functions and epidemiology from suicide attempts, thus distinguishing the intent of self-harm behaviours is essential for fully understanding the behaviour and enabling effective treatment [37,38].
Clinicians’ perceptions of intent may affect the beliefs they form about instances of self-harm, including the occurrence of stigma [39]. Corrigan’s (2003) attribution model shows how beliefs around controllability predict beliefs about how responsible a person is for their mental health difficulties [40]. Unfavourable behaviours perceived as more controllable are more likely to attract stigma [41]. Studies on the perceived controllability of suicidal and self-harming behaviours have mixed findings. Gale et al. [42] found that mental health professionals viewed suicide attempts as less controllable and less predictable than conditions like anxiety or depression. Senf, Maiwurm, and Fettel [43] reported that healthcare professionals working with cancer clients often saw suicidality as a rational response to suffering, rather than impulsive. Yue et al. [44] found psychiatric nurses perceived NSSI as difficult to manage, suggesting limited controllability, though repeated acts were sometimes viewed as deliberate or attention-seeking. The perception that someone has control over their self-harm and is choosing to do this can contribute to the stigma surrounding this behaviour [45], but it is unclear whether perceptions of intent moderate these judgements of controllability.
Whilst there is sufficient research exploring healthcare professionals’ views of self-harm as a whole and NSSI and SA separately, less is known about (a) how intent affects these views and (b) how these views influence clinical decision-making [46]. Understanding trainee healthcare practitioners’ perspectives is essential, as reflecting on these views early in their training can help address biases and improve future practice. The overall aim of the study was to qualitatively explore trainee healthcare practitioners’ experiences and understandings of self-harm to develop insight into where stigma is attached. The primary aim was to explore how perceived intentionality of self-harm affects trainee practitioners’ views and attitudes towards the behaviour. A secondary aim was to assess how these attitudes influenced their treatment and clinical decision-making regarding the client’s care.
2. Materials and Methods
2.1. Design
A cross-sectional qualitative design was adopted using one-to-one interviews. A qualitative approach is well-suited to capturing rich, contextualised insights that may not be accessible through structured quantitative measures alone enabling exploration of complex social and psychological phenomena (perceptions of self-harm). This study was part of a larger qualitative study of trainee practitioner attitudes on self-harm.
2.2. Participants
Participants were recruited through adverts distributed digitally to relevant university programme cohorts and paper adverts placed in relevant buildings on campus at universities in Northwest England. Inclusion criteria included being aged 18 years or above and being a ‘trainee healthcare practitioner’. Trainee healthcare practitioner status was defined as studying on a university programme which would enable students to work in a healthcare practitioner role (e.g. trainee clinical psychologists, nursing associates, medical students), and which included a healthcare placement or experience in clinical settings as part of the programme. Exclusion criteria stated that individuals who do not understand verbal and written English could not participate in the study. The target sample size was guided by information power [47]. Based on the focus of the study, twenty participants were deemed adequate to provide rich, in-depth insights into trainee practitioners’ attitudes and provide participant diversity. This study received approval from a university research ethics committee.
2.3. Measures
A demographics form captured information regarding the participants age, university course, ethnicity, gender and lived experience of self-harm. The semi-structured interview schedule contained questions exploring how the intent of self-harm (defined dichotomously as suicidal and non-suicidal) affects trainee healthcare practitioners’ views and clinical decision-making towards people who self-harm. The researcher reviewed interview schedules of past literature around intent of self-harm and stigma to identify topics to discuss which align with the aims of the study [48,49,50]. While the interview followed a set structure, there was room for flexibility to follow up particular responses and comments [51].
2.4. Procedure
Individuals interested in participating could contact the researcher. Potential participants were invited to an initial meeting with the researcher, either in-person at the University or online via video call. All the participants chose online meetings. Informed consent was first obtained. The demographics form was sent to participants to complete prior to the interview. The qualitative interview lasted approximately 60 minutes and was guided by an interview schedule of semi-structured, open-ended questions. All participants were reimbursed for their participation.
2.5. Analysis
Interviews were transcribed verbatim by DK. Reflexive thematic analysis (RTA) was used to analyse the data. RTA is a theoretically flexible process where the researcher explores and develops patterns of meanings across a dataset with the aim to create a logical, consistent interpretation of the data, established through the participant’s voice [52]. Braun & Clarke’s, [52] RTA entails six stages which included data familiarisation, code generation, theme generation, reviewing themes, defining themes, and reporting the results of the analysis through conducting a write-up. Inductive RTA was used through creating descriptive codes which summarised the essence of participants' narratives. Codes were refined to ensure each excerpt represented one code. The analysis focused on semantic and latent levels of analysis through identifying explicit and deeper, implicit meanings behind participants expressions. This study used a critical realist framework which assumed a shared external reality can be inferred through the research, but the researcher’s perspective would affect how inferences could be made about this reality [53].
2.6. Reflexivity & Trustworthiness
The researcher was a 22-year-old, British Asian, MSc Clinical and Health Psychology student with personal experience of self-harm. They have worked across both private and public mental healthcare settings both in the community and in client settings as a support worker and an assistant psychologist where self-harm behaviours are prevalent. The finding should be read in this context.
To ensure trustworthiness of findings, the research team followed three principals to ensure the analysis was robust [54]. Credibility refers to the ability to ensure that findings are accurate and are based on having a solid understanding of the data. To ensure this, data were transcribed verbatim so direct quotes could be evidenced to support the themes without participants’ voices being lost through the interpretation. Data were analysed by one researcher. However, supervision was utilised with a clinical psychologist in the research team to discuss the patterns which were arising and any discrepancies. Dependability refers to the ability to replicate the same research process. To ensure dependability, the researcher consistently followed Braun and Clarke’s [53] reflexive thematic analysis process. Transferability refers to the degree to which study findings can be generalised. To ensure judgements could be made about the degree of transferability of the findings, participant characteristics and a clear description of the context were provided. This was used to consider the potential impact on the findings.
3. Results
3.1. Participant Characteristics
Interviews were conducted remotely with a sample of predominantly white, female trainee healthcare practitioners (N = 15) working within National Health Service (NHS) teams as part of their placement. The mean age was 29 years (Range = 20-47). Most participants were from psychology-based professions (N = 12; e.g. trainee clinical psychologists, trainee counselling psychologists, psychological wellbeing practitioners) and personally knew somebody who engaged in self-harm. Half of the sample (N= 8, 53%) had lived experience of self-harm. Participant demographics are summarised in Table 1. This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
3.2. Thematic Analysis
Three themes emerged through inductive thematic analysis (1) interpreting intent in self-harm: clinical utility and challenges, (2) perceived responsibility of self-harm and (3) Trainees’ struggle for equal care in a hierarchical system (See Figure 1). An overarching, cross-cutting theme was an inconsistency between how participants felt intent was an unhelpful guide for informing their clinical practice, but simultaneously gave examples of making clinical decisions based on perceptions of intent.
3.2.1. Interpreting Intent in Self-Harm: Clinical Utility and Challenges
There were inconsistencies within and across transcripts regarding the utility of distinguishing intent within clinical practice. Trainees demonstrated ambivalence, sometimes using intent to guide care decisions whilst at other times criticising this approach. Moreover, trainee practitioners commonly assessed intent using factors such as methods, severity and location of self-harm, while clients’ self-reported intent was sometimes questioned, with concerns about their authenticity. This highlights the complexity of assessing and categorising intent with significant implications for treatment planning and training.
Conflicting Views of Intent in Clinical Decision-Making and Training
Trainees’ beliefs around self-harm intent differed from their clinical practice. Whilst most trainees supported equal care for all clients, irrespective of intent, they acknowledged that intent shaped clinical decisions and treatment dynamics. Specifically, intent influenced risk appraisals and service eligibility, with NSSI being seen as lower risk, and SA being seen as higher risk. “I think I would probably take it to be more severe if there was suicidality, like a more urgent issue if there was immediate suicidality” (Medicine 2). Some participants recognised the utility of intent in determining eligibility for service referrals, with NSSI typically being treated in primary care settings and within the community. For example, DClinPsy 4 stated “...more likely to work with them say in the primary care setting…” In contrast, suicidal behaviour was considered more appropriate for secondary care such as mental health inpatient services. However, others noted that due to under-resourcing, services often triage referrals without considering intent, leaving those working in low-level services feeling unprepared to manage suicidal self-harm. For example, Trainee associate practitioner 1 stated “…we were supposed to be very low-level risk, in the community… but the majority of the people we work with do you have suicidal intent…”. Mental Health Nurse 3 supported this by highlighting how community services tend to feel helpless because they offer interventions, they feel are inappropriate for those engaging in suicidal self-harm “…they [those engaging with suicidal self-harm] wouldn't be suitable for us and we would need to refer them on… I personally would feel responsible to get them help and not sure where to look.” Participants suggested that grouping self-harm by intent could be helpful as a process for learning different approaches and presentations and for dissemination of client information: “…in practice it might be useful for the trainees to understand the differences in like approaches and techniques and skills …” (DCounPsy 1).
Some participants argued that labelling intent was problematic for clinical decision-making, as it oversimplified the fluid nature of intent and ignored the risks related to NSSI and passive suicidality such as accidental suicide. For example, Medicine 2 stated “...when people are very much on in the grey areas…passive suicidal ideation… it might be difficult to know which box to put them in…”. Participants described the tension between simplifying the phenomenon and the stigmatisation of clients due to labelling - “…we don’t like putting people in boxes… I wouldn’t want that to be obvious to clients because I, don’t like people to feel different because of intent…” (DCounPsy 1). Both clinical and counselling psychology participants were particularly critical of the binary approach, as it excluded clients who did not fit this dichotomy, emphasising favour for the continuum view of self-harm. For example, Medic 2 stated “…if someone isn't suicidal… that could escalate into becoming suicidal, so I think it's, the two categories sometimes there is a bit of an overlap, and it isn't just as black and white...”
The presence of suicidal intent also guided consideration of treatment options. Where suicidal intent was present, there was a greater focus on immediate risk management and safety. For example, DClinPsy 1 stated “…people’s feelings can be neglected when there is suicidal intent… managing that risk but they almost forget to stop and understand what's going on [for] the person…” There was a greater sense of urgency associated with suicidal intent, and at times more restrictive practice such as increased observation levels, removing bathroom privacy and removing access to leave off the ward were supported. For example, Trainee Associate Practitioner 2 stated “I think you could feel a bit more panic if someone is saying that they’re acutely suicidal…more of a sense of urgency… make sure that they're in a safe, contained environment and they stop…” Where non-suicidal intent was present, there was a greater focus on understanding the person holistically and encouraging autonomy through promoting self-management of NSSI within community settings. For example, DClinPsy 3 stated “… if somebody with suicidal intent, there's an acuity there and you respond to the risk whereas... somebody without it, is more like you're thinking of a longer-term kind of response.” Although trainees perceived intent as a fluctuating factor, the perception of having more time to work with NSSI suggests that at times, the same clinicians viewed intent as fixed.
Participants from psychological backgrounds more often discussed intent being relevant to treatment decisions because psychological approaches tend to focus on understanding the underlying emotional and cognitive factors which drive self-harm behaviours. For example, DClinPsy 4 stated how psychological professions may have “…more time to explore what that serves for them, why they’re engaging in it and what kind of function does it have for them.” Some psychology trainees advocated for a person-centered approach. They criticised the binary nature of intent as it excluded treatment decisions for clients who did not fit this dichotomy, emphasising favour for the continuum view of self-harm which acknowledges that the intent behind self-harm may vary in degree and nature over categorical approaches (e.g. categorising intent as absent or present). In contrast, participants from medical backgrounds felt intent was seen as less relevant and not helpful for making clinical decisions. Some participants from medical backgrounds explained that this was because intent plays a less direct role in treatment options which are often diagnosis-driven and generic (e.g. medications) and focuses on managing symptoms and stabilising an individual. For example, Medicine 3 stated “in a psychiatric sense it’s kind of you know what drugs are for what conditions and you prescribe them…” Mental Health Nursing 1 also stated that intent was meaningless for nursing professions because “…regardless of what the intent is…all self-harm can have the same implications or consequences like killing yourself…”
Client vs Trainee Judgements of Intent
Trainees often dismissed or questioned clients’ own judgement of intent. This was particularly apparent during cases where clients verbalised suicidal intent. Some trainees reported that they and their colleagues sometimes questioned the authenticity of verbalised suicidal intent, perceiving it as disingenuous. Some participants raised doubts that some instances of disclosing intent were accurate. For example, Mental Health Nursing 1 stated “I feel in some instances... They're saying it [disclosing suicidality] because they know it will create a certain response, but it is not necessarily something that they actually intend to do.” DClinPsy 5 supported this when they said “… you feel like you've had a conversation [about SA] … coming away thinking like, don't believe you.” However, a few trainees advocated for acceptance and validation of clients’ experiences despite clinicians’ uncertainties, acknowledging the difficulty of disclosing intent to healthcare professionals. For example, DClinCoun1 stated “…I think it's very much about you know viewing the person as a person no matter what they're going through, no matter what their adverse experiences or you know no matter what they've chosen to do...”
Clinical characteristics such as the method, location, and severity of self-harm emerged as key factors that trainees used to assess clients' intent. For example, methods associated with more physical risk like cutting near a major blood vessel were linked to more suicidal intent. DClinPsy 2 stated ‘the risk associated with a ligature is obviously very difficult and high and it can quite easily lead to loss of life even if it's not intentional… cutting may be less so suicidal intent…” Although not explicitly asked, trainees referenced these factors, suggesting they played a significant role in judging the severity and intent of self-harm. This indicates that clinical characteristics influenced their decision-making, even without direct inquiry.
Paradoxes in Perceived Motivation and Treatment Prioritization
Clinicians reported paradoxical statements when commenting on their optimism and responsiveness to care based on perceived intent. Trainees evidenced a preference to work with NSSI compared to SA, viewing these individuals as more amenable to treatment (e.g. higher motivation, increased engagement with staff). For instance, Mental Health Nursing 1 stated clients with non-suicidal intent “...their motivation to find alternative methods or to follow like a care plan… I feel as though their motivation is higher.” Despite less optimism seen in trainees when treating suicidal individuals, an ethical obligation to prioritise their care was echoed by most, leading to increased responsiveness to care. Some trainees shared less optimistic views of recovery when suicidal intent was present, suggesting that persistent suicidal feelings were discouraging and indicative of limited progress. For instance, Medicine 1 stated “If someone’s continuing not to feel suicidal…you’re glad that they are not becoming any worse or deteriorating…if they’re continuously feeling suicidal, I suppose that does be disappointing and deflating in itself...” However, the same trainees remained responsive to these clients perceiving them to require more urgent care than those with non-suicidal intentions. For example, DClinPsy 2 stated that “…in one circumstance there’s a risk to life…that always has to be a priority.”
3.2.2. Perceived Responsibility of Self-harm
Trainees assigned different levels of responsibility for self-harm and seeking treatment based on intent. Responsibility shifted from the client to the healthcare professional and then to the healthcare system. Their appraisals determined how they worked with individuals and their clinical decisions.
Responsibility for Behaviour
A subset of trainees talked about suicidal behaviours in a manner suggestive of a sense of the client having more control over their actions than those who engaged in NSSI. For example, Nursing Associate Practitioner 1 stated “...you may see people who…ligature with ligatures they can untie or people who restrict their diet but not to a point where, you know they’ll still eat a little bit, or they’ll still drink a little bit…” This suggests that some trainees viewed SA as a calculated, planned act, implying clients may exercise some control over their actions. It is important to note that some participants had experience working in inpatient settings, which likely influenced their narratives. Witnessing repeated ligature incidents on a ward, for example, provides a stark contrast to the lay perception of a suicide attempt or the situations encountered in community secondary care services, potentially shaping their understanding and judgment of self-harm and suicidal intent.
NSSI was viewed by some as an impulsive act, suggesting less control. For example, Trainee Associate Psychological Practitioner 1 stated “…if they [non-suicidal clients] don't do it [self-harm] frequently sometimes they experience a loss of control and they don't really remember why they’ve done it, and they can't explain why they've done it…” However, other participants believed clients, to some extent, have self-awareness of the risks associated with NSSI and are making informed choices. DClinPsy 1 said “…I’ve spoken to people who’ve… been very clear on kind of where they would and would not cut and like aware of, I guess the risks associated…”. Some trainees recognised that controllability of self-harm could vary with mental health conditions, such as psychosis or mania, affecting a person’s control over their behaviour regardless of the intent. For example, DClinPsy 5 stated “…if someone was experiencing psychosis or mania and engaging in self-injurious behaviour, I would argue, they don't have control, therefore they're not responsible.”
Responsibility for Treatment
Despite sometimes viewing NSSI as less controllable, some trainees assigned more responsibility to clients engaging in NSSI for obtaining and engaging with treatment. For example, TAPP 2 suggested offering a “... safety sort of package that this person could access, so that if they were cutting in their room…they would be able to help themselves to some degree [for NSSI] …”. Moreover, trainees found it easier to maintain professional boundaries and manage situations with NSSI. For example, DClinPsy 2 stated that having a boundaried approach rather than an emotional response to NSSI helps the therapeutic relationship “… it allows me to have a little bit more erm, practicality in my approach…. I think if I wasn't desensitised, some things would really shock me and that might come across to the person and then they might be kind of put off about talking about it again…”.
In contrast, trainees felt a greater sense of responsibility for the outcome of treatment for suicidal clients, particularly in psychological professions. DCounPsy 1 stated “…it's hard to carry that weight of feeling like you have some responsibility but… we have no way of making that person not go and die by suicide…”. They reported taking a proactive, indirect role in caring for clients with suicidal intent. Interventions for SA focussed on risk management, following protocols and speaking to senior members of the team to share the risks, which may have led to suicidal clients taking a more passive role in their care compared to NSSI.
Heightened personal responsibility for clients with suicidal intent contributed to anxiety for some trainees. Trainees felt that they had an ethical, moral obligation to treat these individuals but also wanted to prevent harmful consequences to themselves that might result from the death by suicide of a client under their care. This included fears of being blamed or held responsible for the death of the client. For example, Mental Health Nursing 1 noted that “…at uni we are taught so much about things like coroners court or the thought of you could lose your pin…I don’t want to get involved in that…” This avoidant approach towards working with suicidality, increased feelings of inadequacy and helplessness with decision-making.
3.2.3. Trainees Struggle for Equal Care in a Hierarchical System
Some trainees evidenced a drive for change, to see equal treatment for both forms of self-harm within the healthcare system. However, many trainees also highlighted that the clinical decisions they make can be influenced by system constraints and hierarchical structures, leading to a disconnect between the care they hoped to provide, and the actual care delivered. For example, when discussing how they wanted to provide more in-depth care for NSSI, Mental Health Nursing 2 stated “…they [the service] don't have things to offer erm, and that people genuinely want help, and they’re turned away with a bath and a cup of tea.” A common thread in the transcripts was trainees’ acknowledgment that the healthcare system should bear some responsibility for the differential treatment of clients. They identified systemic issues such as inadequate funding, limited training, poor care pathways, and bed shortages, as barriers to providing equal care. For example, Medic 3 stated “…it's just that we can't [offer equal care] because of staffing and because of, we can't give them as much time because like client safety is the priority…” Mental Health Nurse 3 also highlighted the challenges of getting support, irrespective of intent “…there's so many reasons for that like the understaffing, like lack of funding, lack of beds like all time scales that you want people in and out…” Despite recognising this, trainees still felt obliged to hold that personal responsibility with suicidal intent, as seen in Theme 2.
Some trainees expressed a desire to challenge stigmatising views within their care teams, particularly from supervisors or senior staff. However, they often felt powerless due to their trainee status and the hierarchical structure of the healthcare system, which made it difficult to challenge negative attitudes. For example, Mental Health Nursing 1 stated “...I did speak up [to colleagues] and kind of say I don’t think it [NSSI] is attention seeking…it was kind of shot down … then you just lose the ability to verbalise and because you are a student it's almost like what you’re saying has less weight…”.
4. Discussion
This study explored trainee healthcare practitioners’ attitudes towards self-harm, and how perceived suicidal intent influences views and clinical decision-making. Three themes were identified (1) interpreting intent in self-harm: clinical utility and challenges, (2) perceived responsibility of self-harm and (3) trainees’ struggle for equal care in a hierarchical system. Participants observed, but did not share pejorative views about self-harm (both with and without suicidal intent) expressed by other staff members. Despite most trainees advocating for equal care, irrespective of the intent of self-harm, implicit ideas regarding intent appeared to influence trainees’ work with self-harm. This suggests that intent may have an unspoken role within clinical decision-making, leading to differential care being received for NSSI and SA.
Participants expressed ambivalence regarding the role of intent in clinical decision-making. While some clinicians saw value in understanding intent to guide treatment decisions, others questioned its relevance or practicality in determining appropriate care. This study found that trainees’ judgements of risk may be influenced by intent, with higher risk associated with SA. However, some trainees noted the difficulty and potential inaccuracy of using intent alone to determine risk, especially when severe NSSI or passive suicidality were evident. This highlights the limitations of static risk judgements based solely on intent as it overlooks the dynamic and complex nature of self-harm behaviours [55]. It could lead to underestimations or overestimations risk [56], potentially resulting in inadequate care or false reassurances [57]. Further investigation into how intent informs risk-related judgements is needed.
Trainees’ attitudes towards treatment differed according to the intent of self-harm. Non-suicidal behaviours were seen as more amenable to psychological interventions. Yet, it was unclear whether they were being delivered in practice as there was also a greater focus on self-management. This may contribute to some clients who engage in NSSI feeling dismissed by healthcare services [58,59,60]. In contrary, the presence of suicidal intent often led to more passive, risk-averse care, with minimal client autonomy or collaboration. Although psychological approaches are recommended for managing suicidal behaviours [61,62], the continued emphasis on risk management strategies such as objective risk assessments and safety plans [63,64], may influence trainees to prioritise risk management over therapeutic engagement. This aligned with the data where there was a tendency to associate inpatient care with suicidal intent, though it may also reflect the background and experiences of the sample, most of whom had prior inpatient placement experiences. Yet most people who self-harm, even with suicidal ideation, are outpatients [65]. This raises questions around how care may differ when suicidal intent is present within community settings.
The study revealed paradoxes in trainees’ motivation to engage with clients based on self-harm intent. While some trainees expressed greater optimism and motivation to treat cases of NSSI, they often deprioritised cases when suicidal intent was not explicitly evident. This pattern reflects existing literature, which states that clinicians often prioritise care based on the perceived severity of self-harm, with suicidal behaviours receiving more urgent attention [66]. For example, self-cutting behaviours, typically associated with NSSI, were perceived as less serious than overt suicidal behaviours and were less likely to receive psychosocial assessments or prioritised care [67,68], even though they may still indicate significant psychological distress [69,70].
Moreover, this study highlighted the disconnect between participants’ perception of intent and those expressed by the clients themselves, demonstrating the drawbacks of distinguishing intent. Clinicians often interpreted self-harm through their own lens, which may not align with how clients understand or convey their actions. This mirrors findings from Whitlock et al. [71] and O’Connor et al., [72], who emphasised that clinician bias and variability of clinicians' interpretations of intent, can lead to inconsistencies in treatment decisions. Garlow & Rosen [73] suggested that misalignments may be partly due to objective assessments that fail to capture the nuances of client experiences. This highlights the challenges in aligning clinical assessments with clients’ motivations and questions the accuracy of clinicians’ assumptions in treatment decisions.
The study showed that intent influenced perceptions of control over self-harm behaviours, with SA viewed as more controllable than NSSI. However, contrary to attribution theory [40], which suggests that more controllable behaviours are more stigmatised, NSSI was not necessarily perceived more negatively. This may reflect the tendency to view self-harm as a behavioural choice rather than a symptom of mental health, as seen with depression and anxiety [74,75]. Literature presents conflicting views on controllability of both NSSI and SA, with some suggesting SA is a calculated act, while others argue individuals are not in control of their actions [31], [76,77,78,79,80].
Despite the perception of suicidal behaviours as more controllable, trainees expressed greater urgency and support for clients exhibiting these behaviours. This reflects a broader fear of being held accountable for adverse outcomes, which often leads to a more passive risk-averse approach to care [81]. For example, clinicians felt like they needed external control over a client until they were no longer engaging in suicidal acts and could think rationally [81]. This study suggests that trainees’ responses to self-harm may be influenced by factors beyond perceived controllability, such as fear of professional repercussions, worry about making mistakes, and a heightened sense responsibility for treatment outcomes - echoed by previous literature [14], [82,83,84,85].
Finally, the study revealed concerns around systematic and organisational factors, such as training gaps, resource limitations and hierarchical structures, which impact care delivery. These challenges have been well-documented in the literature [86,87,88,89,90]. Addressing these issues is crucial for improving the consistency and quality of care, particularly in ensuring equitable treatment for all individuals, irrespective of intent.
This study has several limitations. The predominantly white British, female sample from northwest England may limit transferability of results. A self-selection bias could have skewed the findings, as more than half of the participants had personal experiences with self-harm. Additionally, the sample, although mixed, consisted mainly of psychologists or medical professions with an interest in psychology. This may have influenced the views of intent compared to what may have been found in medical or nursing professionals without these biases. Future research should compare views and attitudes across profession. It was challenging to distinguish between trainee’s own views and their perceptions of colleagues’ views. Social desirability bias may have led participants to mask their views, attributing them to colleagues instead. As trainees enter the healthcare system, they may be affected by colleagues and pressure to behave a certain way to fit in the group [91]. The impact of colleagues’ influence should be explored further. The discussion of intent was often shaped by the way interview questions were framed, with the interviewer typically presenting intent as a fixed attribute of the individual (e.g. whether the person has intent or not). This framing may have encouraged participants to view intent as a static quality of the person, rather than considering it as a dynamic and contextual feature of self-harming behaviour that can exist along a continuum.
These results suggest several educational and clinical implications. Currently, national guidance states a way of working with self-harm which does not make a distinction using intent [1]. However, intent had an unspoken influence on trainees’ clinical judgements, causing confusion and conflict. This could lead to issues in clinical practice such as inconsistent care and lack of transparency in decision-making. As trainees may sometimes be led by their own underlying beliefs and assumptions rather than standardised protocols when making care decisions, trainees may approach self-harm in varied ways. Increasing awareness of self-harm guidelines could ensure consistent adherence in practice [92]. Adopting a dynamic, individualised, needs-based approach [93] using risk formulations [94] may ensure intent is accounted for.
There is a clear need for more focused training around intent and how clinicians should intervene, as specialised self-harm training is currently lacking [95,96,97]. Standardising training across the UK could help promote more consistent practice. Intent was addressed to varying degrees across universities with a heavy focus on suicidality, resulting in disparate levels of knowledge and attitudes towards self-harm. There is an unclear relationship between increased education and less stigma towards self-harm [69,98,99]. This inconsistency may stem from training content being overly general or focused on broader mental health issues, making comparisons between training courses challenging. Tailoring training to address specific forms of self-harm could help reduce stigma and improve care provision. Anti-stigma training has shown to enhance clinician attitudes and increasing help-seeking behaviours among clients [100,101]. However, challenges such as limited staff time and financial resources must also be considered to ensure access to adequate training.
Ongoing support for trainees, such as clinical supervision, reflective practice and Schwartz rounds, are crucial [101]. This would support trainees and clinicians to better recognise how their own beliefs and assumptions can affect their clinical decision-making and help them to feel adequately trained and supported. Additionally, a culture shift towards a ‘responsibility without blame’ approach [102], which acknowledges errors made in healthcare within the context of the challenging environments healthcare professional’s work, could facilitate learning and improve practice [103,104]. Shared decision-making models may further enhance collaborative working, positive risk-taking and reduce clinician burden [105,106]. Therefore, the impact of contextual factors on clinical decision-making requires further consideration. Systemic factors may explain the inconsistency between national guidance produced for ‘perfect care’ and an imperfect environment in which staff are operating.
5. Conclusions
To summarise, this study is one of the first to explore how perceptions of intent influence the views and decision making of trainee clinicians regarding self-harm. Trainees did not express overtly negative views towards NSSI and SA, but implicit ideas about intent led to differential care and perceived responsibility for different forms of self-harm behaviours. These unspoken ideas, assumptions and views around NSSI and SA are not captured in the guidelines but still informed care decisions. It is important to highlight this, as such assumptions may result in a lack of transparency and consistency in decision-making which could be problematic. A standardized approach to defining and treating both forms of self-harm is needed, achievable through reviewing evidence-based guidelines, improved training, and providing support for trainees.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Additional Participant Quotes.
Author Contributions
Conceptualization, P.T., D.K.; methodology, P.T., D.K.; software, D.K.; validation, P.T., D.K.; formal analysis, D.K., investigation, D.K., resources, D.K.; data curation, X.X.; writing—original draft preparation, D.K, PT; writing—review and editing, D.K, PT, KG.; visualization, D.K.; supervision, PT.; project administration, P.T., D.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of University of Manchester (protocol code XXX and date of approval).”.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Given concerns around confidentiality, the data that supported the findings of this study are not available from the corresponding author.
Acknowledgments
I would like to thank the participants who gave up their valuable time to contribute to the research.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
CBT Cognitive Behavioural Therapy
DClinPsy Doctorate of Clinical Psychology
DCounPsy Doctorate of Counselling Psychology
DBT Dialectical Behavioural Therapy
M Mean
NAP Nursing Associate Practitioner
NSSI Non-suicidal self-injury
RTA Reflexive Thematic Analysis
SA Suicide attempt
SD Standard Deviation
TAPP Trainee Associate Psychological Practitioner
References
- NICE. (2022). Self-harm: assessment, management and preventing recurrence. National Institute for Health and Care Excellence.
- Knipe, D. , et al. Self-harm and suicide in low- and middle-income countries. The Lancet Psychiatry 2022, 9, 97–109. [Google Scholar]
- McManus, S. , et al. (2016). Mental health and wellbeing in England: Adult Psychiatric Morbidity Survey 2014. NHS Digital.
- Link, B. G. , & Phelan, J. C. Conceptualizing stigma. Annual Review of Sociology 2001, 27, 363–385. [Google Scholar]
- Guerrero-Diaz, M. The stigma of self-harm: public perceptions and professional bias. Journal of Mental Health 2021, 30, 421–429. [Google Scholar]
- Lloyd, C. , Blazely, A., & Phillips, L. Stigma in self-injury: The views of young people who self-injure. Journal of Youth Studies 2018, 21, 620–635. [Google Scholar]
- Newton, B. , & Bale, C. Self-harm and stigma: A qualitative study of perceptions. Clinical Psychology Forum 2012, 233, 24–28. [Google Scholar]
- Brickell, T. A. , & McLean, C. Emerging issues and challenges for improving patient safety in mental health: A qualitative analysis of expert perspectives. Journal of Patient Safety 2011, 7, 39–44. [Google Scholar]
- Alonzo, D. , & Pratto, D. The stigma of self-injury among healthcare providers. Community Mental Health Journal 2021, 57, 1132–1139. [Google Scholar]
- Michall, C. , Tait, L., & Churchill, R. Stigma towards people who self-harm: attitudes of nurses in a UK mental health trust. Mental Health Practice 2017, 20, 28–35. [Google Scholar]
- Rees, N. , et al. Attitudes of healthcare staff towards people who self-harm. The British Journal of Psychiatry 2014, 205, 41–46. [Google Scholar]
- Rees, N. , et al. Staff attitudes towards people who self-harm: A multi-site evaluation. Journal of Psychiatric and Mental Health Nursing 2018, 25, 31–40. [Google Scholar]
- McGough, P. , et al. Emergency nurses' attitudes towards people who self-harm: An observational study. International Emergency Nursing 2022, 59, 101048. [Google Scholar]
- O’Keeffe, S. , et al. Patients' experiences of self-harm and stigma in healthcare settings. BMJ Open 2021, 11, e042763. [Google Scholar]
- Storey, P. , et al. Patients who present with self-harm: Clinical attitudes and stigma. British Journal of Psychiatry 2005, 187, 68–73. [Google Scholar]
- Akinola, M. , & Rayner, G. Stigma and self-harm: Service users' experiences. Journal of Mental Health 2022, 31, 345–352. [Google Scholar]
- Oliver, C. , et al. Understanding service users’ experiences of stigma following self-harm. Journal of Mental Health 2014, 23, 85–89. [Google Scholar]
- Masuku, N. The refusal of care for individuals who self-harm: A critical review. Nursing Ethics 2019, 26, 1041–1051. [Google Scholar]
- Rayner, G. , et al. Healthcare staff responses to people who self-harm: A mixed-method review. International Journal of Nursing Studies 2019, 98, 73–85. [Google Scholar]
- Taylor, T. L. Attitudes towards self-harm: An investigation of the views of healthcare professionals. Journal of Psychiatric and Mental Health Nursing 2009, 16, 60–65. [Google Scholar]
- Bergen, H. , et al. Neglecting psychological needs after self-harm: A qualitative study. Social Psychiatry and Psychiatric Epidemiology 2023, 58, 497–506. [Google Scholar]
- Chapman, A. L. , & Martin, E.R. Stigma and help-seeking for self-injury. Journal of Nervous and Mental Disease 2014, 202, 536–543. [Google Scholar]
- McManus, S. , et al. Prevalence, patterns, and correlates of self-harm: Findings from the Adult Psychiatric Morbidity Survey 2014. BJPsych Open 2019, 5, e90. [Google Scholar]
- Frost, M. , et al. Stigma and help-seeking behaviour for self-harm: A systematic review. BMJ Open 2015, 5, e007888. [Google Scholar]
- Halicka, J. , & Kiejna, A. Non-suicidal self-injury and suicide attempts: Different or similar phenomena? Psychiatria Polska 2015, 49, 751–764. [Google Scholar]
- Taylor, T. L. , et al. Functions of non-suicidal self-injury in young people: A systematic review. Clinical Child Psychology and Psychiatry 2018, 23, 578–593. [Google Scholar]
- Halicka, J. , & Kiejna, A. Suicidal behaviour and self-harm: Definitions and classification. Archives of Psychiatry and Psychotherapy 2018, 20, 7–14. [Google Scholar]
- Samari, E. , et al. Suicidal ideation in non-suicidal self-injury: A longitudinal study. Suicide and Life-Threatening Behavior 2020, 50, 1265–1273. [Google Scholar]
- Herzog, J. , et al. Suicidal ideation among adolescents engaging in non-suicidal self-injury: Prevalence and predictors. Journal of Affective Disorders 2022, 300, 15–22. [Google Scholar]
- Gouveia-Pereira, M. , et al. The continuum of self-harm intent: A narrative review. Clinical Psychology Review 2022, 90, 102107. [Google Scholar]
- Muehlenkamp, J.J. Self-injury and suicide behavior: A review for clinicians. Journal of Clinical Psychology 2014, 70, 279–291. [Google Scholar]
- Kapur, N. , et al. Classification of self-harm by intent: An ongoing debate. The Lancet Psychiatry 2013, 1, 4–5. [Google Scholar]
- Kar Ray, M. , et al. Clinical challenges in understanding changing suicidal intent. Psychiatric Bulletin 2020, 44, 112–117. [Google Scholar]
- Hawton, K. , et al. Assessment of suicide risk in self-harm patients. Psychological Medicine 2003, 33, 655–663. [Google Scholar]
- McGough, P. , et al. Emergency nurses and intent assessment: Barriers and priorities. Journal of Emergency Nursing 2021, 47, 739–747. [Google Scholar]
- Ogurin, D. , et al. Clinical importance of assessing self-harm intent. Archives of Suicide Research 2015, 19, 344–356. [Google Scholar]
- Butler, G. , & Malone, K. Non-suicidal self-injury vs suicide attempts in adolescents. Archives of Suicide Research 2013, 17, 197–210. [Google Scholar]
- Gardner, W. J. , et al. Differentiating self-harm: Intent and intervention. Crisis: The Journal of Crisis Intervention and Suicide Prevention 2021, 42, 231–239. [Google Scholar]
- Reynders, A. , et al. The impact of clinicians’ attitudes on self-harm care decisions. Suicide and Life-Threatening Behavior 2014, 44, 320–332. [Google Scholar]
- Corrigan, P.W. How stigma interferes with mental health care. American Psychologist 2003, 59, 614–625. [Google Scholar] [CrossRef]
- Smith, B. Controllability beliefs and stigma in self-harm. Journal of Mental Health 2016, 25, 224–230. [Google Scholar]
- Gale, M. , et al. Mental health professionals' perceptions of controllability of suicidal behaviour. Crisis 2016, 37, 294–300. [Google Scholar]
- Senf, B. , Maiwurm, D., & Fettel, D. Healthcare providers' attitudes towards suicidality in cancer patients. Palliative & Supportive Care 2022, 20, 12–18. [Google Scholar]
- Yue, Z. , et al. Psychiatric nurses' perceptions of non-suicidal self-injury: A qualitative study. International Journal of Mental Health Nursing 2024, 33, 89–98. [Google Scholar]
- Staniland, R. Perceived control and stigma in self-harm. Journal of Psychiatric and Mental Health Nursing 2021, 28, 784–791. [Google Scholar]
- Dawson, D. L. , et al. Stigma and self-harm in healthcare: A systematic review. British Journal of Clinical Psychology 2021, 60, 334–352. [Google Scholar]
- Malterud, K. , Siersma, V. D., & Guassora, A. D. Sample size in qualitative interview studies: Guided by information power. Qualitative Health Research 2016, 26, 1753–1760. [Google Scholar] [CrossRef]
- Anderson, R. , Challenor, R., & Ford, T. Exploring healthcare professionals’ attitudes towards self-harm: The role of intent and stigma. Journal of Mental Health.
- Khan, M. , Roberts, R., & White, D. Understanding self-harm intent and stigma in clinical settings: A qualitative synthesis. International Journal of Mental Health Nursing 2021, 30, 123–132. [Google Scholar] [CrossRef]
- Owen, G. , Armstrong, M., & Johnstone, L. Perceived controllability of self-harm: A qualitative study with mental health practitioners. Psychology and Psychotherapy: Theory, Research and Practice 2017, 90, 80–95. [Google Scholar] [CrossRef]
- Eppich, W. , Gormley, G. , & Teunissen, P.W. Cross-pollination of clinical education and qualitative research: Transformative learning through dialogue. Academic Medicine 2019, 94, 507–511. [Google Scholar] [CrossRef]
- Braun, V. , & Clarke, V. Reflecting on reflexive thematic analysis. Qualitative Research in Sport, Exercise and Health 2019, 11, 589–597. [Google Scholar] [CrossRef]
- McEvoy, P. , & Richards, D. Critical realism: A way forward for evaluation research in nursing? Journal of Advanced Nursing 2003, 43, 411–420. [Google Scholar] [CrossRef]
- Koch, T. Establishing rigour in qualitative research: The decision trail. Journal of Advanced Nursing 2006, 53, 91–103. [Google Scholar] [CrossRef]
- O’Connor, R. C. , & Nock, M. K. The psychology of suicidal behaviour. The Lancet Psychiatry 2014, 1, 73–85. [Google Scholar] [CrossRef] [PubMed]
- Cox, G. R. , Campbell, A., & Stallard, P. Risk factors for suicidal behavior in young people: A systematic review. Journal of Adolescence 2020, 84, 188–200. [Google Scholar] [CrossRef]
- Mughal, F. , McKenna, H., & Renfrew, M. J. False reassurance in mental health risk assessment: A qualitative study of trainee experiences. Journal of Clinical Psychology 2023, 79, 150–165. [Google Scholar] [CrossRef]
- Andersson, S. , Bakker, D., & Müller, V. Experiences of non-suicidal self-injury clients in mental health services: A qualitative analysis. Clinical Psychology Review 2024, 105, 102207. [Google Scholar]
- Shahwan, S. , Duhig, M., & Naicker, M. “We felt written off”: Client experiences of marginalization in self-harm care. Community Mental Health Journal 2022, 58, 630–640. [Google Scholar]
- Cully, G. , Corcoran, P., Leahy, D., Griffin, E., Dillon, C., Cassidy, E., Shiely, F., & Arensman, E. Method of self-harm and risk of self-harm repetition: findings from a national self-harm registry. Journal of Affective Disorders 2019, 246, 843–850. [Google Scholar] [CrossRef]
- McCabe, R. , Saeri, A., & Platz, E. Psychosocial interventions for suicidal behaviour in adults: A systematic review. BMJ Open 2018, 8, e024314. [Google Scholar]
- Mendez-Bustos, P. , Baca-Garcia, E., & Saiz-Ruiz, J. Psychological approaches to reducing suicide risk: A meta-analysis. Journal of Affective Disorders 2019, 243, 16–27. [Google Scholar] [CrossRef]
- Graney, J. , Simmons, M., & Bradley, C. The role of safety planning in suicide prevention: A review of implementation practices. Crisis 2020, 41, 96–104. [Google Scholar] [CrossRef]
- Nuji, N. , Venkatesan, S., & Saunders, D. Effectiveness of risk management strategies in clinical practice: A systematic review. Risk Management and Healthcare Policy 2021, 14, 37–48. [Google Scholar]
- Marchant, A. , Hawton, K., & Stewart, A. Self-harm in primary care: Patterns and predictors. British Journal of General Practice 2020, 70, e421–e428. [Google Scholar]
- Gibbs, L. , & Baker, H. Prioritising suicidal self-harm in clinical settings: A qualitative study. International Journal of Mental Health Nursing 2011, 20, 470–477. [Google Scholar] [CrossRef]
- Quinlivan, L. , Kannenberg, K., & Smith, J. Psychosocial assessments of self-cutting behaviour in adults. Social Psychiatry and Psychiatric Epidemiology 2022, 57, 521–530. [Google Scholar]
- Fortune, S. , Mulligan, M., & Stewart, L. Clinical prioritisation of self-harm in mental health services: Service-user perspectives. Journal of Mental Health 2021, 30, 19–27. [Google Scholar]
- Saunders, K. E. , Culpin, I., & John, A. Psychological distress in self-cutting adolescents. Journal of Child Psychology and Psychiatry 2012, 53, 113–121. [Google Scholar] [CrossRef]
- Perry, Y. , Hawton, K., & Lavender, T. Self-injury clinical outcomes: Why self-cutting may be underestimated. British Journal of Psychiatry 2020, 217, 519–524. [Google Scholar] [CrossRef]
- Whitlock, J. , Muehlenkamp, J., & Purington, A. Identification of self-injury: Role of clinician perceptions. Journal of Clinical Psychology 2013, 69, 982–992. [Google Scholar] [CrossRef]
- O’Connor, R. C. , & Kirtley, O. J. The lived experience of self-harm and clinician misinterpretation. Journal of Mental Health 2017, 26, 201–207. [Google Scholar]
- Garlow, S. J. , & Rosen, P. Clinician misalignment in self-harm care: An observational study. Psychiatric Services 2007, 58, 871–876. [Google Scholar]
- Allen, N. B. Self-harm, depression and autonomy: Understanding the link. Journal of Affective Disorders 2007, 100, 1–8. [Google Scholar] [CrossRef]
- Barr, D. , Leitner, B., & Thomas, S. Autonomy in self-harm and help-seeking: A qualitative study. Social Psychiatry and Psychiatric Epidemiology 2004, 39, 272–278. [Google Scholar]
- Rogers, M. L. , Gorday, E., & Joiner, T. E. Calculated suicidal behavior: Systematic review. Suicide and Life-Threatening Behavior 2021, 51, 234–247. [Google Scholar] [CrossRef]
- Paashaus, L. W. , Jansen, A., & Muris, P. Perceived control in self-harm: A cross-sectional study. BMC Psychiatry 2021, 21, 312. [Google Scholar]
- Lee, H. , & Hyun, M. H. Victim-perpetrator perspectives on intent: Self-harm analysis. Psychiatric Quarterly 2021, 92, 621–632. [Google Scholar]
- Floyd, J. Psychosocial dimensions of self-harm control: A review. Clinical Psychology Review 2019, 70, 95–108. [Google Scholar] [CrossRef]
- Fikke, L. R. , Jacobsen, N. H., & Helseth, S. Control beliefs in NSSI: A pilot study. Child and Adolescent Psychiatry and Mental Health 2011, 5, 28. [Google Scholar] [CrossRef]
- Jobes, D. A. , & Chalker, S.A. Fear of liability in suicide risk management: Implications for care. Journal of Psychiatric Practice 2019, 25, 35–44. [Google Scholar] [CrossRef]
- Bleich, S. , Ostroff, R., & Hammer, S. Professional anxiety and self-harm care: A phenomenological study. Journal of Psychiatric & Mental Health Nursing 2011, 18, 856–863. [Google Scholar] [CrossRef]
- Hoifodt, R. S. , & Talseth, A. G. Anxiety and accountability: Nurses’ experiences in acute care. Nursing Ethics 2006, 13, 588–600. [Google Scholar]
- Jobes, D. A. Managing clinician fear in suicide prevention: A clinical guide. Suicide and Life-Threatening Behavior 2020, 50, 30–46. [Google Scholar] [CrossRef]
- O’Keeffe, S. , Suzuki, M., Ryan, M. P., Hunter, J., & McCabe, R. Experiences of care for self-harm in the emergency department: Comparison of the perspectives of patients, carers and practitioners. BJPsych Open 2021, 7, e175. [Google Scholar] [CrossRef]
- Gamblin, D. , McNaughton, R., & Raby, N. (2024). Organisational barriers to targeted self-harm training. Journal of Health Services Research & Policy.
- Veresova, A. , Smith, P., & Martin, L. Training disparities in healthcare: System-level influences. Medical Education 2024, 58, 115–123. [Google Scholar] [CrossRef]
- Jahn, S. , Quinnet, J., & Ries, M. Resource constraints in mental health services: A UK perspective. Health Services Management Research 2016, 29, 145–153. [Google Scholar]
- Petrik, A. , Walker, N., & Molloy, D. Hierarchy and self-harm care: Staff perceptions. Journal of Psychiatric and Mental Health Nursing 2015, 22, 254–262. [Google Scholar] [CrossRef]
- Witt, A. , Bailey, K., & James, S. Systemic influences on mental health clinical decision-making. BMC Health Services Research 2023, 23, 12. [Google Scholar]
- Thexton, W. Clinical psychology training and preparation for multidisciplinary team working: a grounded theory model and the reframing of reflective practice (Doctoral dissertation, University of Birmingham).
- Leather, J. Z. , O'Connor, R. C., Quinlivan, L., Kapur, N., Campbell, S., & Armitage, C. J. Healthcare professionals’ implementation of national guidelines with clients who self-harm. Journal of psychiatric research 2020, 130, 405–411. [Google Scholar] [CrossRef]
- Woodford, R. , Spittal, M. J., Milner, A., McGill, K., Kapur, N., Pirkis, J., Mitchell, A., & Carter, G. Accuracy of clinician predictions of future self-harm: a systematic review and meta-analysis of predictive studies. Suicide and Life-Threatening Behavior 2019, 49, 23–40. [Google Scholar] [CrossRef] [PubMed]
- Mulder, R. , Newton-Howes, G., & Coid, J. W. The futility of risk prediction in psychiatry. The British Journal of Psychiatry 2016, 209, 271–272. [Google Scholar] [CrossRef]
- Kool, N. , van Meijel, B., Koekkoek, B., van der Bijl, J., & Kerkhof, A. Improving communication and practical skills in working with inclients who self-harm: a pre-test/posttest study of the effects of a training programme. BMC psychiatry 2014, 14, 1–9. [Google Scholar]
- https://doi.org/10.1186/1471-244X-14-64. [CrossRef]
- Bellairs-Walsh, I. , Byrne, S. J., Bendall, S., Perry, Y., Krysinska, K., Lin, A., Michail, M., Lamblin, M., Li, T.Y., Hetrick, S., & Robinson, J. Working with young people at risk of suicidal behaviour and self-harm: A qualitative study of Australian General Practitioners’ perspectives. International journal of environmental research and public health 2021, 18, 12926. [Google Scholar] [CrossRef]
- Coppens, E. , Van Audenhove, C., Gusmão, R., Purebl, G., Székely, A., Maxwell, M., Koburger, N., Arensman, E., & Hegerl, U. Effectiveness of general practitioner training to improve suicide awareness and knowledge and skills towards depression. Journal of Affective Disorders 2017, 227, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Michail, M. , Tait, L., & Churchill, D. General practitioners' clinical expertise in managing suicidal young people: Implications for continued education. Primary Health Care Research and Development 2017, 18, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Gibson, R. , Carson, J., & Houghton, T. Stigma towards non-suicidal self-harm: Evaluating a brief educational intervention. British Journal of Nursing 2019, 28, 307–312. [Google Scholar] [CrossRef]
- Karman, P. , Kool, N., Poslawsky, I.E., & Van Meijel, B. Nurses’ attitudes towards self-harm: a literature review. Journal of Psychiatric and Mental Health Nursing 2015, 22, 6575. [Google Scholar] [CrossRef]
- Parker, J. , & Davies, B. No blame no gain? From a no blame culture to a responsibility culture in medicine. Journal of Applied Philosophy 2020, 37, 646–660. [Google Scholar] [CrossRef]
- Belford, 2023 Belford, A. J. No blame policy is not no blame culture. bmj 2023, 383. [Google Scholar] [CrossRef]
- Pickard, H. , & Ward, L. (2013). Responsibility without blame: Philosophical reflections on clinical practice. In K. W. M. Fulford, and others (Eds.) The Oxford Handbook of Philosophy and Psychiatry. (pp. 1134–1152). Oxford Academic. [CrossRef]
- Østervang, C. , Touborg Lassen, A., Stenager, E., & Valdersdorf Jensen, M. Experiences of nursing care for patients who self-harm and suggestions for future practices: The perspectives of emergency care nurses. International Journal of Mental Health Nursing 2022, 31, 70–82. [Google Scholar] [CrossRef]
- Coulter, A. , Edwards, A., Elwyn, G., & Thomson, R. Implementing shared decision making in the UK. Zeitschrift für Evidenz, Fortbildung und Qualität im Gesundheitswesen 2011, 105, 300–304. [Google Scholar] [CrossRef]
Figure 1.
Thematic Map Illustrating Themes and Codes.
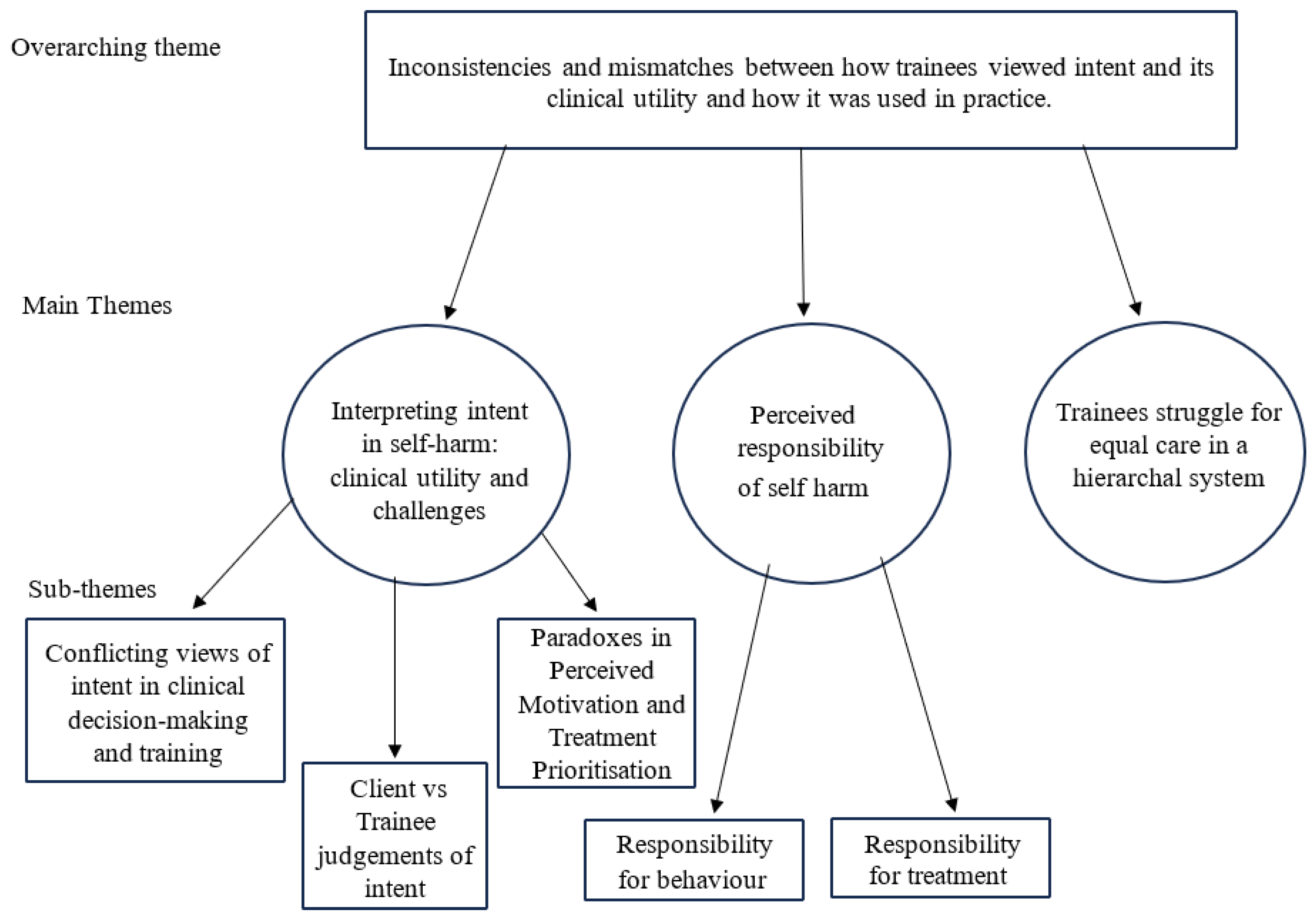

Table 1.
Summary of Participant Characteristics.
| Characteristic | N |
|---|---|
| Age M (SD) | 29.2 (8.02) |
| Gender | |
| Female | 14 |
| Non-binary | 1 |
| Ethnicity | |
| White | 15 |
| Programme | |
| DClinPsy1 | 5 |
| Mental Health Nursing | 3 |
| Medicine | 3 |
| TAPP2 | 2 |
| DCounPsy3 | 1 |
| NAP4 | 1 |
| Lived experience of self-harm | |
| Yes | 8 |
| No | 7 |
| Personally know someone who has self-harmed | |
| Yes, close family/friend | 12 |
| Yes, distant family/friend | 2 |
| No | 1 |
1 Doctorate of Clinical Psychology, 2 Trainee Associate Psychological Practitioner, 3 Doctorate of Counselling Psychology, 4 Nursing Associate Practitioner.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



