Submitted:
25 June 2024
Posted:
26 June 2024
You are already at the latest version
Abstract
Ectopic eruption of teeth rarely occurs in the mandibular condyle, orbit, nasal cavity, skin, and maxillary sinus. Ectopic eruption of teeth in the maxillary sinus can be accompanied by chronic and recurrent sinusitis, including headache, facial pain, and numbness. Fibro-osseous lesions in the paranasal sinuses are discovered incidentally on X-ray images and are often asymptomatic. Osteoma is the most common fibro-osseous lesion that develops in the paranasal and nasal sinuses. Herein, we report a rare case of osteoma (exostosis) containing supernumerary teeth within the maxillary sinus. A characteristic pedicled bone lesion with a clear border on computed tomography was the undefined orthopantomogram radiopacity in the left maxillary sinus, and the lesion contained teeth. The tumor was excised using the Caldwell–Luc procedure. Pathologically, the surgical specimen revealed an osteoma. The patient’s symptoms of chronic sinusitis disappeared, and the patient had no symptoms 2 years after the surgery. Because the patient had no history of midface trauma or surgery, the supernumerary teeth were speculated to have migrated during a reactive osteogenic process caused by chronic sinusitis.
Keywords:
ectopic eruption
; supernumerary teeth
; osteoma
; maxillary sinusitis
1. Introduction
Malposition, impaction, and ectopic eruption of teeth are common dental issues. Teeth move through the alveolar bone according to a set eruption process. The eruption path can be impeded by tooth crowding, odontogenic cysts and tumors, odontogenic infections, cleft palate, and trauma. Ectopic eruption of teeth in areas other than the alveolar bone is rare and can occur in adjacent structures such as the maxillary sinus, mandibular condyle, and nasal cavity. Ectopic teeth within the maxillary sinus are rarely reported. Tooth eruption into the maxillary sinus most commonly occurs in the third molar, and reports of supernumerary teeth are extremely rare. The standard treatment option for an ectopic tooth is extraction [1]. Bony lesions in the paranasal sinuses may be found incidentally on X-ray imaging. It frequently occurs in frontoethmoidal sinuses and is often asymptomatic [2]. A few patients with sinonasal symptoms have ectopic teeth in the maxillary sinus. Panoramic X-rays and computed tomography (CT) scans are effective for diagnosing ectopic teeth and bony lesions in the maxillary sinus. A dentist can diagnose misplaced teeth and odontogenic pathology with an oral examination and appropriate imaging procedures. If maxillary sinusitis is resistant to treatment, the maxillary sinus must be evaluated [3].
Herein, we report a rare case of osteoma (exotosis) involving a supernumerary tooth in the maxillary sinus. The radiopaque lesion in the maxillary sinus was found incidentally during a screening dental examination. He had no dental or alveolar complaints, and his complaint of nasal obstruction had been diagnosed as sinusitis by an otorhinolaryngologist. He had no history of nasal surgery or treatment for allergic rhinitis. The tumor was removed using the Caldwell–Luc approach. His nasal congestion resolved satisfactorily and has not recurred in the 2 years since surgery. Chronic and persistent maxillary sinusitis may be due to ectopic bone structures (teeth and fibro-osseous lesions) in the maxillary sinus. In cases of ectopic teeth in the maxillary sinus, a surgical approach may be effective in improving sinusitis symptoms. We discuss the pathogenesis of this rare tumor, osteoma with supernumerary teeth (exostosis).
2. Materials and Methods
This case report concerns a 52-year-old man with chronic maxillary sinusitis symptoms, i.e., nasal congestion. Orthopantomography of this patient revealed a well-defined radiopaque in the left maxillary sinus. CT scan revealed a pedicled bony structure in the left maxillary sinus containing a tooth. The tooth was found to be a supernumerary tooth. The ectopic bony structure was surgically removed. The structure was extracted en bloc via the Caldwell–Luc approach. Histopathological diagnosis was exostosis. The patient’s maxillary sinusitis symptoms disappeared, and he has had no recurrence of symptoms for 2 years. A small number of patients suffering from chronic maxillary sinusitis have ectopic bone lesions in the maxillary sinus. Surgical treatment of ectopic structures in the maxillary sinus appears to be an effective procedure. Tooth migration into an ectopic osteoma is rare.
3. Case Presentation
A 52-year-old man presented for evaluation of pantomogram radiopacity in the maxillary sinus. He had no history of systemic diseases. He had chronic nasal congestion and was diagnosed with chronic sinusitis by an otolaryngologist; however, no treatment was given. On intraoral examination, the wisdom teeth had erupted, and no teeth were missing. He felt a slight percussion pain in his upper left second premolar, first molar, and second molar; however, tooth mobility was not observed, and all teeth were vital. No bulge in the alveolar region and no rhinorrhea were noted. He had no history of midfacial trauma or surgery, and the patient recalled not receiving orthodontic treatment. An orthopanoramic X-ray image showed a well-defined radiopacity in the left maxillary sinus, which contained a psammoma body and a tooth or an odontoma-like structure. The contralateral maxillary sinus was clear, and all permanent teeth had not received root canal treatment (Figure 1). A sectional CT view showed a bony mass at the bottom of the left maxillary sinus. The pedunculated mass on the lower wall of the maxillary sinus measured 37 × 21 × 24 mm. The center of the mass was 130 Hounsfield units (HU), and the tooth-like structure component measured 1,300 HU (Figure 2). The clinical diagnosis was a foreign body in the maxillary sinus, i.e., osteoma, or an odontogenic tumor containing an impacted tooth. Under general anesthesia, the tumor was removed from the left maxillary sinus using the Caldwell–Luc approach. After the bony window from the anterior wall of the maxillary sinus was lifted, the osseous tumor was visible. The tumor stalk was resected using piezosurgery and removed en bloc. As his osteomeatal complex was not obstructed, an inferior meatal antrostomy was not performed (Figure 3). Histopathologically, the surgical specimen was composed of mature lamellar bone under a fibrous capsule and fatty marrow between the trabeculae. Inflammatory cells and odontogenic epithelium were not observed (Figure 4). The final pathological diagnosis was osteoma, exostosis. The patient’s nasal congestion resolved, and he remained symptom-free 2 years after the surgery.
3. Discussion
Osteoma is a benign and slow-growing tumor. Osteomas are thought to emerge from the embryogenic periosteum, and the annual growth rate is 0.79 mm/year on average [4]. Suggested causes of osteomas include trauma, infection, and inflammation; however, the exact etiology is still unclear [5,6]. Among the craniofacial bones, it frequently occurs in the mandible, with a ratio of 7:3 [7]. In the paranasal sinus, osteomas occur in 0.01%–0.43% of patients [8], predominantly in the frontal sinus [2,9]. Osteomas occurring in the maxillary sinus have been rarely reported [8,10]. Osteomas of the maxillary sinus are discovered incidentally in orthopantomography during screening in a dental practice. Common clinical symptoms include headache and facial pain [5]. If paranasal sinus osteomas are asymptomatic or when the mass lesion occupies 50% or less of the sinus volume, it be observed with regular radiological examinations rather than with surgical intervention [11]. Clinically, osteomas must be differentiated from malignant tumors such as osteosarcoma and Gardner’s syndrome (GS) [12]. In cases of multiple osteomas of the craniofacial bones, extraintestinal manifestations of GS that precede polyposis formation were suspected [12]. Large tumors that occupy the sinuses can cause diplopia, epiphora, and blindness [13,14].
Ectopic teeth and supernumerary teeth are found in approximately 1% of the total population [15]. Dentists frequently find ectopic tooth eruptions within the dental structure. Those occurring in nondental areas, such as the mandibular condyle, coronoid process, orbit palate, nasal cavity, have been rarely reported [16]. In a literature review of ectopic eruption, the maxillary sinus was the most frequently involved area [17]. Ectopic tooth development and eruption may involve multifactorial pathological disorders with both general and local etiological factors, or their combination [18,19]. These include maxillofacial trauma, odontogenic or rhinogenic infections, developmental anomalies such as cleft palate, genetic factors such as Turner syndrome and Apert syndrome [20,21], and jawbone lesions such as odontogenic cysts and tumors [22]. Local factors include maxillary hypoplasia, retrognathism, and crowding [3,23]. The prevalence of ectopic teeth in the maxillary sinus is the highest in the third molars [22], and supernumerary teeth are rare [24]. Ectopic eruption in the maxillary sinus may be symptomatic. Symptoms often include nasal congestion, facial fullness, headache, and facial numbness [1]. In addition, 1% of patients provisionally diagnosed with chronic sinusitis have ectopic teeth in the maxillary sinus [3]. In addition, approximately 80% of ectopic teeth have been removed [1]. A common treatment for ectopic teeth in the maxillary sinus is surgical removal using the Caldwell–Luc approach [25]. Regular examination with orthopantomography or CT is preferred in asymptomatic cases because they may cause to form cysts and tumors [24,26].
This presented case is probably the first case in which a supernumerary tooth erupted within the maxillary sinus osteoma. In a similar case of osteoma in the maxillary sinus, an ectopic third molar coexisted independently [27]. In the present case, the patient had no history of surgery involving the maxillary sinus or midface trauma. Nasal congestion symptoms were diagnosed by an otolaryngologist as chronic sinusitis; however, he did not notice the ectopic teeth because he had not undergone CT of the maxillary sinus. The surgical and histopathological findings of this case did not indicate endoostosis such as fibrous dysplasia, insertion of bone fragments because of previous surgery or trauma, or new bone formation. The tumor, which had a unique morphology with a pedicled, arcuate appearance and a histological composition in which the cortical bone on the surface of the tumor covered the fatty marrow inside, was histologically not a septum of a sinus, which is composed of bone cortex. Tooth eruption changes the vertical level of the bone, but does not completely cover the crown of the tooth, like a dentigerous cyst. Therefore, no researchers have theorized that an impacted tooth induces the bone to form an osteoma around the tooth. The identified characteristics of lesions causing bone lesions within the maxillary sinus suggest chronic mucosal inflammation [28]. If the osteomeatal complex is obstructed by a foreign body within the maxillary sinus (osteomatous lesions or teeth), chronic sinusitis may occur [3], and if it occupies >50% of the sinus volume, surgical treatment is required [11], i.e., resection by the Caldwell–Luc approach 9), particularly if the mass is located in the lower part of the maxillary sinus. The foreign body located in the upper part of the maxillary sinus may be surgically operated endoscopically [29]. When removing large lesions, postoperative complications, such as aesthetic and functional deficits, must be considered [30]. When applying for surgery, the surrounding anatomical structures must be preserved as much as possible, and we believe that a combined endoscopic [31] (functional endoscopic sinus surgery) and intraoral approach is better [32]. We speculate that the pathogenesis of this rare entity is the accidental migration of supernumerary teeth into a reactive osteogenic process caused by chronic inflammation.
5. Conclusions
We report a case of chronic maxillary sinusitis with ectopic exostosis in the maxillary sinus in which symptoms improved after surgery. In some patients who complain of sinusitis, a foreign body in the maxillary sinus is misdiagnosed as sinusitis. A detailed otorhinolaryngological examination and a specialized dental examination by a general dentist (including evaluation of lesions such as third molars, supernumerary teeth, growth deficiency, dental crowding, and odontogenic tumors) will help determine an appropriate treatment plan. Surgical intervention is recommended for symptomatic cases with exostosis and ectopic teeth in the maxillary sinus.
The pathological diagnosis of the ectopic bone structure in this case was exostosis with supernumerary teeth. Exostosis in the maxillary sinus is unusual, as this patient had no history of midface trauma or surgery. Ectopic wisdom teeth in the maxillary sinus are frequent, but supernumerary teeth are rare. This case was a unique case of a supernumerary tooth moving into an exostosis. We speculated that the cause of this was the accidental movement of the supernumerary tooth during a reactive osteogenic process induced by chronic inflammation.
Author Contributions
T.K., K.A., T.G., H.K., E.T. and T.O.: patient treatment, data curation, and writing—Original Draft Preparation and Editing. T.K., E.T., T.O.: Data Curation and Writing—Review and Editing. T.K.: Writing—Review and Editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
The data that support the findings of this study are available upon request from the corresponding author. The data are not publicly available, due to privacy or ethical restrictions.
Acknowledgments
The authors would like to thank Enago (www.enago.jp) for the English language review.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Lombroni, L.G.; Farronato, G.; Santamaria, G.; Lombroni, D.M.; Gatti, P.; Capelli, M. Ectopic teeth in the maxillary sinus: A case report and literature review. Indian J Dent Res 2018, 29, 667–671. [Google Scholar] [PubMed]
- Magboul, N.A.; Al-Ahmari, M.S.; Alzahrani, M.A.; Dlboh, S.S. Fibro-osseous lesion of the nose and paranasal sinus: A retrospective study with literature review. Cureus 2022, 14, e27229. [Google Scholar] [CrossRef] [PubMed]
- Baykul, T.; Doğru, H.; Yasan, H.; Cina Aksoy, M. Clinical impact of fibro sinus. Auris Nasus Larynx 2006, 33, 277–281, (Epub 3 May 2006). [Google Scholar] [CrossRef] [PubMed]
- Buyuklu, F.; Akdogan, M.V.; Ozer, C.; Cakmak, O. Growth characteristics and clinical manifestations of the paranasal sinus osteomas. Otolaryngol Head Neck Surg 2011, 145, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Sayan, N.B.; Uçok, C.; Karasu, H.A.; Günhan, O. Peripheral osteoma of the oral and maxillofacial region: a study of 35 new cases. J Oral Maxillofac Surg 2002, 60, 1299–1301. [Google Scholar] [CrossRef] [PubMed]
- Larrea-Oyarbide, N.; Valmaseda-Castellón, E.; Berini-Aytés, L.; Gay-Escoda, C. Osteomas of the craniofacial region. Review of 106 cases. J Oral Pathol Med 2008, 37, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Johann, A.C.; de Freitas, J.B.; de Aguiar, M.C.; de Araújo, N.S.; Mesquita, R.A. Peripheral osteoma of the mandible: case report and review of the literature. J Craniomaxillofac Surg 2005, 33, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Park, W.; Kim, H.S. Osteoma of maxillary sinus: A case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006, 102, e26–e27. [Google Scholar] [CrossRef] [PubMed]
- Çelenk, F.; Baysal, E.; Karata, Z.A.; Durucu, C.; Mumbuç, S.; Kanlıkama, M. Paranasal sinus osteomas. J Craniofac Surg 2012, 23, e433–e437. [Google Scholar] [CrossRef] [PubMed]
- Borumandi, F.; Lukas, H.; Yousefi, B.; Gaggl, A. Maxillary sinus osteoma: from incidental finding to surgical management. J Oral Maxillofac Pathol 2013, 17, 318. [Google Scholar] [CrossRef] [PubMed]
- Koivunen, P.; Löppönen, H.; Fors, A.P.; Jokinen, K. The growth rate of osteomas of the paranasal sinuses. Clin Otolaryngol Allied Sci 1997, 22, 111–114. [Google Scholar] [CrossRef] [PubMed]
- Oner, A.Y.; Pocan, S. Gardner’s syndrome: a case report. Br Dent J 2006, 200, 666–667. [Google Scholar] [CrossRef] [PubMed]
- Osma, U.; Yaldiz, M.; Tekin, M.; Topcu, I. Giant ethmoid osteoma with orbital extension presenting with epiphora. Rhinology 2003, 41, 122–124. [Google Scholar]
- Lee, J.J.; Ryu, G.; Lee, K.E.; Hong, S.D.; Jung, Y.G.; Kim, H.Y.; Dhong, H.J.; Chung, S.K. Long-term clinical course of benign fibro-osseous lesions in the paranasal sinuses. Clin Exp Otorhinolaryngol 2021, 14, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Moreano, E.H.; Zich, D.K.; Goree, J.C.; Graham, S.M. Nasal tooth. Am J Otolaryngol 1998, 19, 124–126. [Google Scholar] [CrossRef] [PubMed]
- Abdollahifakhim, S.; Mousaviagdas, M. Ectopic molar with maxillary sinus drainage obstruction and oroantral fistula. Iran J Otorhinolaryngol 2013, 25, 187–192. [Google Scholar] [PubMed]
- Arora, P.; Nair, M.K.; Liang, H.; Patel, P.B.; Wright, J.M.; Tahmasbi-Arashlow, M. Ectopic teeth with disparate migration: A literature review and new case series. Imaging Sci Dent 2023, 53, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Srinivasa Prasad, T.; Sujatha, G.; Niazi, T.M.; Rajesh, P. Dentigerous cyst associated with an ectopic third molar in the maxillary sinus: a rare entity. Indian J Dent Res 2007, 18, 141–143. [Google Scholar] [CrossRef] [PubMed]
- Alfuriji, S.; Alamro, H.; Kentab, J.; Alosail, L.; Alali, L.; Altuwaijri, N.; Alalwan, R. Ectopic permanent molars: a review. Dent J (Basel) 2023, 11, 206. [Google Scholar] [CrossRef] [PubMed]
- Dalben, G.d.S.; das Neves, L.T.; Gomide, M.R. Oral findings in patients with Apert syndrome. J Appl Oral Sci 2006, 14, 465–469. [Google Scholar] [CrossRef] [PubMed]
- Helm, A.; Martín-Vacas, A.; Molinero-Mourelle, P.; Caleya, A.M.; Gallardo, N.E.; Mourelle-Martínez, M.R. Ectopic eruption of maxillary first permanent molars: preliminary results of prevalence and dentoskeletal characteristics in Spanish paediatric population. Children (Basel) 2021, 8, 479. [Google Scholar] [CrossRef] [PubMed]
- Lamb, J.F.; Husein, O.F.; Spiess, A.C. Ectopic molar in the maxillary sinus precipitating a mucocele: a case report and literature review. Ear Nose Throat J 2009, 88, E6–E11. [Google Scholar] [PubMed]
- Mucedero, M.; Rozzi, M.; Cardoni, G.; Ricchiuti, M.R.; Cozza, P. Dentoskeletal features in individuals with ectopic eruption of the permanent maxillary first molar. Korean J Orthod 2015, 45, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Erkmen, N.; Olmez, S.; Onerci, M. Supernumerary tooth in the maxillary sinus: case report. Aust Dent J 1998, 43, 385–386. [Google Scholar] [CrossRef] [PubMed]
- Kayabasoglu, G. 2 Murat Karaman, 1 Recep Kaymaz, 1 Alpen Nacar. A rare entity causing chronic sinusitis: ectopic tooth in maxillary sinus. Eur J Gen Med 2015, 12, 86–89. [Google Scholar]
- Lai, Y.T.; Luk, Y.S.; Fung, K.H. Anomalous morphology of an ectopic tooth in the maxillary sinus on three-dimensional computed tomography images. J Radiol Case Rep 2013, 7, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Aydın, Ü.; Aşık, B.; Ahmedov, A.; Durmaz, A. Osteoma and ectopic tooth of the left maxillary sinus: A unique coexistence. Balkan Med J 2016, 33, 473–476. [Google Scholar] [CrossRef] [PubMed]
- Aldren, C.P.; Soames, J.V.; Birchall, J.P. Bony remodelling in an osteoma of the paranasal sinuses. J Laryngol Otol 1993, 107, 633–635. [Google Scholar] [CrossRef] [PubMed]
- Viterbo, S.; Griffa, A.; Boffano, P. Endoscopic removal of an ectopic tooth in maxillary sinus. J Craniofac Surg 2013, 24, e46–e48. [Google Scholar] [CrossRef] [PubMed]
- Litvin, M.; Caprice, D.; Infranco, L. Dentigerous cyst of the maxilla with impacted tooth displaced into orbital rim and floor. Ear Nose Throat J 2008, 87, 160–162. [Google Scholar] [CrossRef] [PubMed]
- Masalha, M.; Schneider, S.; Kassem, F.; Koren, I.; Eliashar, R.; Margulis, A.; Landsberg, R. Endoscopic treatment of ectopic teeth in the maxillary sinus. J Clin Exp Dent 2021, 13, e227–e233. [Google Scholar] [CrossRef] [PubMed]
- Chiapasco, M.; Felisati, G.; Zaniboni, M.; Pipolo, C.; Borloni, R.; Lozza, P. The treatment of sinusitis following maxillary sinus grafting with the association of functional endoscopic sinus surgery (FESS) and an intra-oral approach. Clin Oral Implants Res 2013, 24, 623–629. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Orthopanoramic radiographs.A well-circumscribed radiopaque is observed in the left upper jaw sinus. No permanent tooth deficiency in the maxillary dentition was noted, and wisdom teeth have erupted.
Figure 1.
Orthopanoramic radiographs.A well-circumscribed radiopaque is observed in the left upper jaw sinus. No permanent tooth deficiency in the maxillary dentition was noted, and wisdom teeth have erupted.
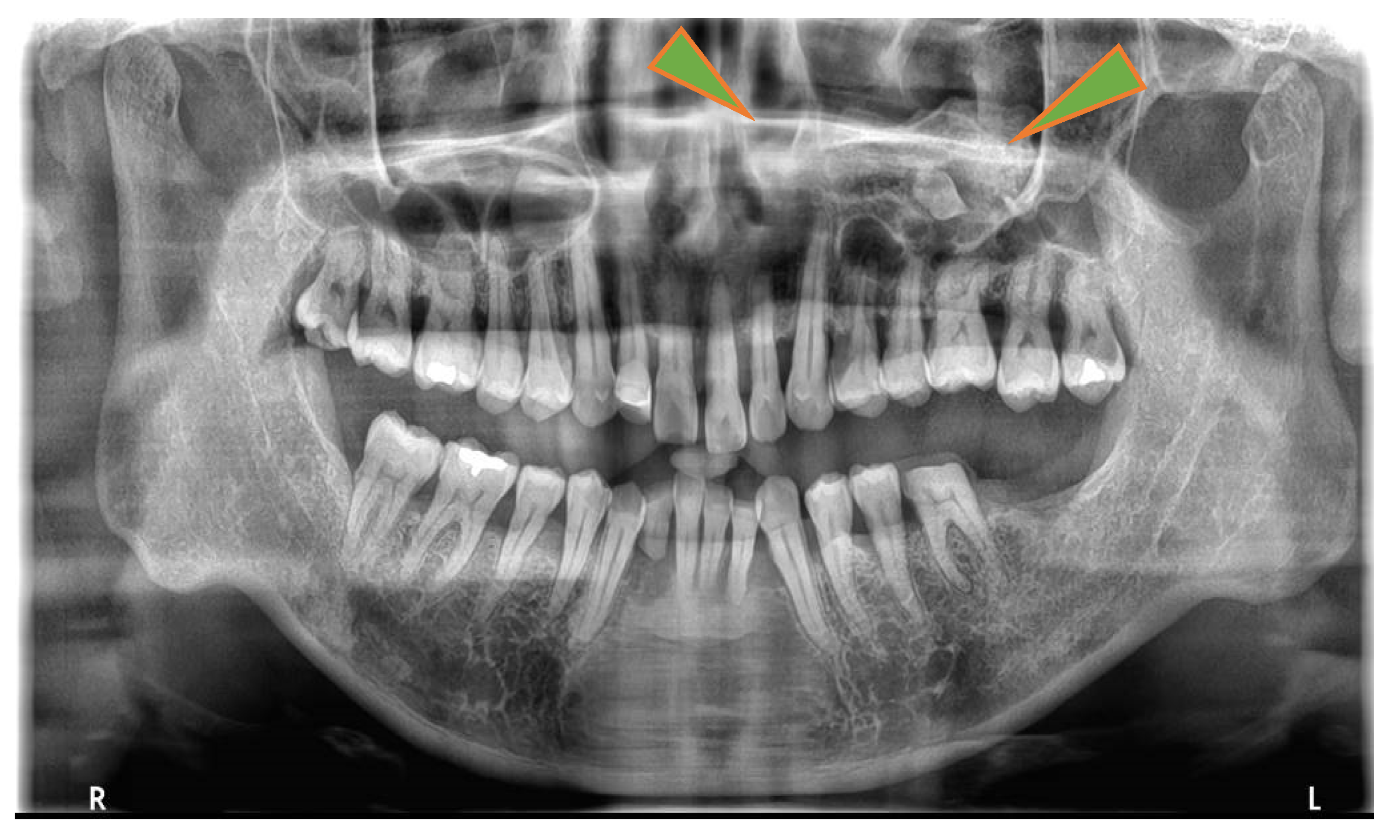
Figure 2.
Sectional computed tomography. a. Coronal view. Pedunculated mass is depicted from the upper left maxillary sinus. The mass contained a psammoma body and a tooth-like structure. No thickening of the maxillary mucosa was visible. No distortion of the maxillary sinus and no maxillary sinus septa were found. b. Axial view. The mass accounts for approximately half of the left maxillary sinus. The high-intensity radiopacity inside the mass measured 1,300 HU. The radiopacity depicts enamel, dentin, and pulp cavity. c. Sagittal view. The mass is continuous with the lower wall of the maxillary sinus. The interior of the tumor showed 130 HU. d. Three-dimensional computed tomography. The CT value was adjusted to eliminate the low signal range of 1,000 HU or less. The surface of the teeth and tumor emerges. The tumor develops within the maxillary sinus to pedunculate from the canine root.
Figure 2.
Sectional computed tomography. a. Coronal view. Pedunculated mass is depicted from the upper left maxillary sinus. The mass contained a psammoma body and a tooth-like structure. No thickening of the maxillary mucosa was visible. No distortion of the maxillary sinus and no maxillary sinus septa were found. b. Axial view. The mass accounts for approximately half of the left maxillary sinus. The high-intensity radiopacity inside the mass measured 1,300 HU. The radiopacity depicts enamel, dentin, and pulp cavity. c. Sagittal view. The mass is continuous with the lower wall of the maxillary sinus. The interior of the tumor showed 130 HU. d. Three-dimensional computed tomography. The CT value was adjusted to eliminate the low signal range of 1,000 HU or less. The surface of the teeth and tumor emerges. The tumor develops within the maxillary sinus to pedunculate from the canine root.
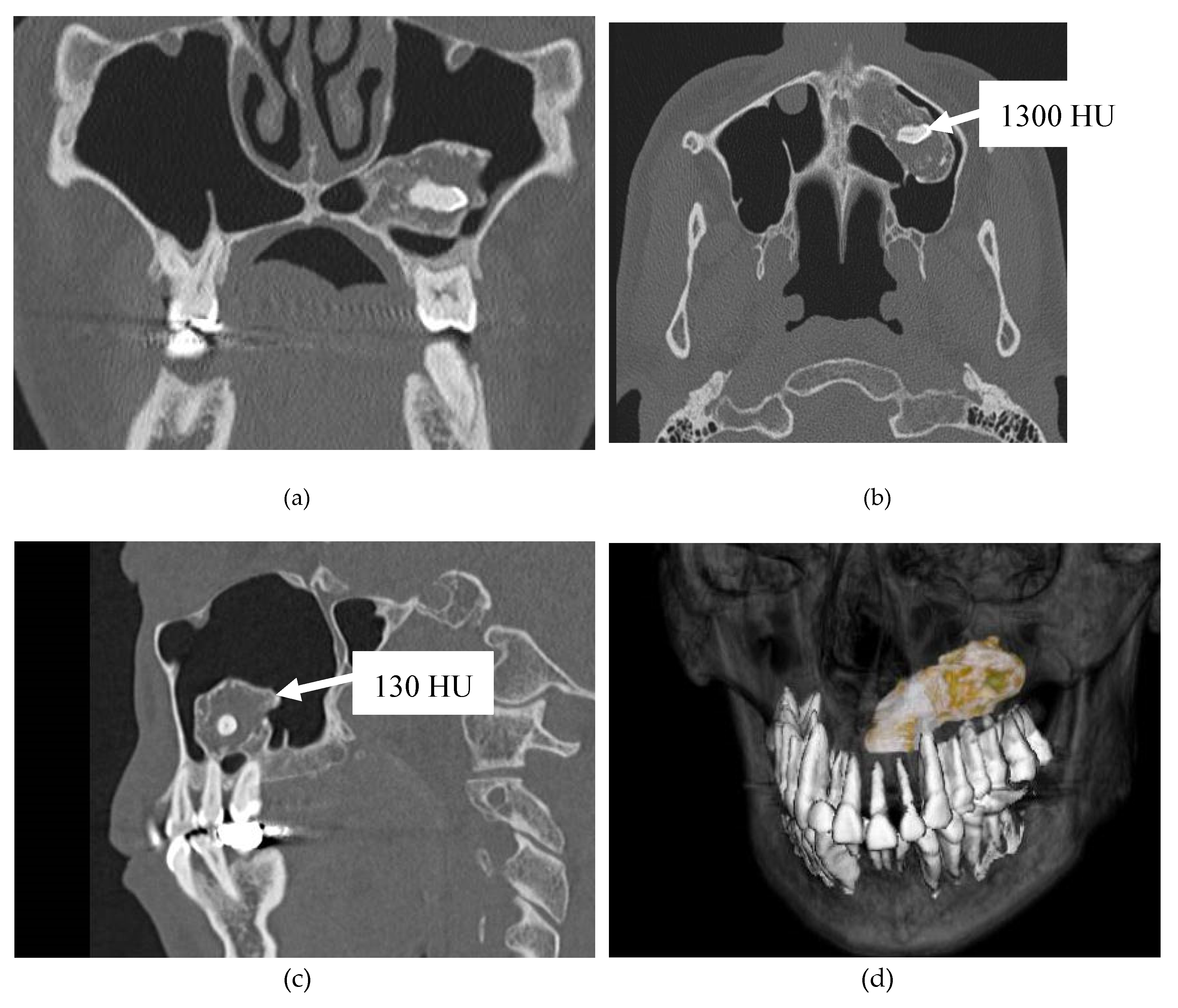
Figure 3.
Intraoperative photo. a. The Caldwell–Luc procedure was performed. The bony window from the anterior wall of the maxillary sinus was formed with piezo-electric surgery. The tumor occupied the maxillary sinus. The tumor surface was bony and sticky. b. This is a photograph of the oral cavity after the tumor was removed. The tumor was located in the maxillary sinus. There was no bleeding in the maxillary sinus mucosa after tumor removal.
Figure 3.
Intraoperative photo. a. The Caldwell–Luc procedure was performed. The bony window from the anterior wall of the maxillary sinus was formed with piezo-electric surgery. The tumor occupied the maxillary sinus. The tumor surface was bony and sticky. b. This is a photograph of the oral cavity after the tumor was removed. The tumor was located in the maxillary sinus. There was no bleeding in the maxillary sinus mucosa after tumor removal.
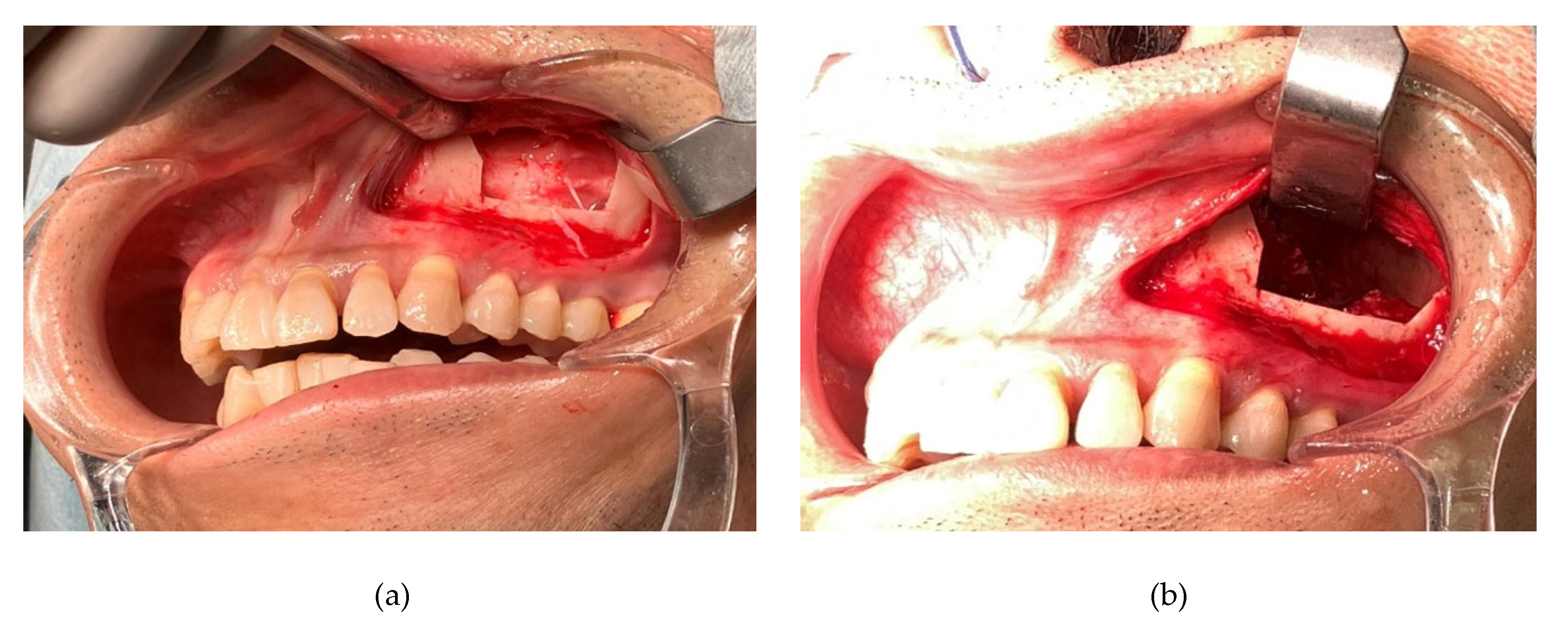
Figure 4.
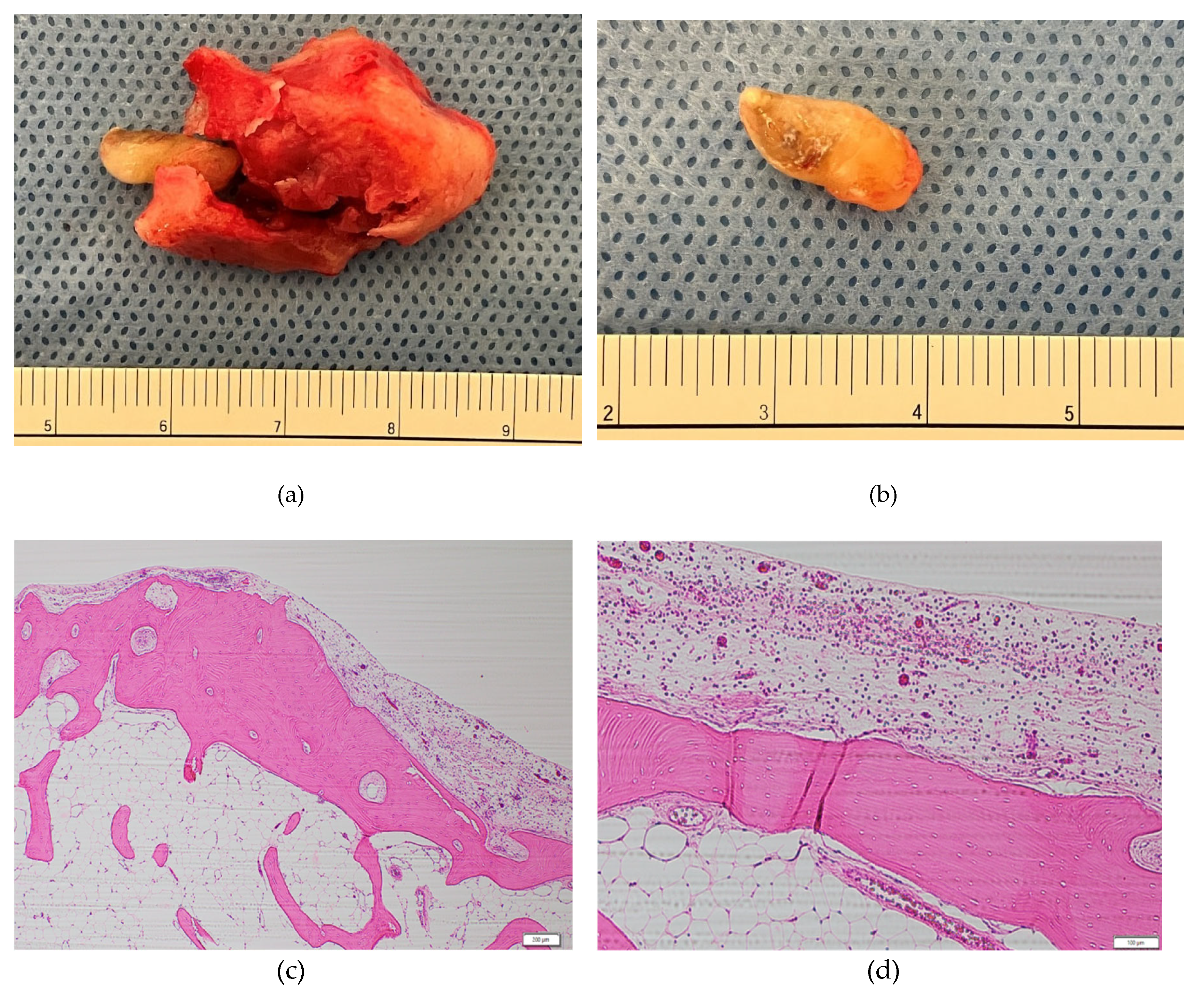
Image of surgical specimen and pathological photograph (Hematoxylin and eosin-stained). a. Macroscopic appearance of surgical specimen. The tumor measured 30 × 15 × 15 mm. The tumor was composed of hard bone tissue externally and sparse bone tissue internally. The interior of the tumor contained supernumerary teeth. b. Macroscopic appearance of supernumerary teeth. The internal teeth were 12 mm long and had a complete tooth structure. c. A view of lesion at ×4 magnification. The specimen revealed a mixture of mature lamellar bone and various sizes of Haversian lamellae under the fibrous capsule. d. A view of lesion at ×10 magnification. Fatty marrow was observed between the trabeculae. No inflammatory cell infiltration and epithelial odontogenic cells were noted.
Figure 4.
Image of surgical specimen and pathological photograph (Hematoxylin and eosin-stained). a. Macroscopic appearance of surgical specimen. The tumor measured 30 × 15 × 15 mm. The tumor was composed of hard bone tissue externally and sparse bone tissue internally. The interior of the tumor contained supernumerary teeth. b. Macroscopic appearance of supernumerary teeth. The internal teeth were 12 mm long and had a complete tooth structure. c. A view of lesion at ×4 magnification. The specimen revealed a mixture of mature lamellar bone and various sizes of Haversian lamellae under the fibrous capsule. d. A view of lesion at ×10 magnification. Fatty marrow was observed between the trabeculae. No inflammatory cell infiltration and epithelial odontogenic cells were noted.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



