
Submitted:
26 September 2023
Posted:
28 September 2023
You are already at the latest version
Abstract
The aim of the study was to analyze the oral etiology of patients with odontogenic sinusitis (ODS)and to compare the differences in demographic data, clinical symptoms, extent of sinus involvement, bone penetration of the maxillary sinus floor (MSF) between different etiologies. A retrospective investigation was conducted on 103 patients with ODS recruited from Beijing Tongren Hospital. All enrolled patients underwent sinus CT, nasal endoscopy, and oral examination. A comparison of the patients' clinical symptoms, extent of involvement of the sinuses, and bone resorption of the MSF according to odontogenic etiologies was conducted. Follow-up was based on symptoms, clinical examination. The most common odontogenic etiologies were endo-periodontal lesions (EPL. 49.5%), apical periodontitis (AP, 32.0%) and periodontitis (PE, 8.7%). There were statistically significant differences in age (P=0.002), sex (P=0.036), inflammation involving the ethmoid sinus (P=0.037), and bone penetration of the MSF (P<0.001) between the AP, EPL, and PE groups. There were no significant differences in sinusitis symptoms (P>0.005) among patients with different odontogenic etiologies. In conclusion, EPL is a neglected oral etiology with a destructive effect on the bone of the MSF, and Should receive more attention in diagnosis and treatment.
Keywords:
Odontogenic sinusitis
; oral etiology
; Endo-periodontal lesions
; clinical symptoms
1. Introduction
Odontogenic sinusitis (ODS) is a bacterial sinusitis, an infection of dental origin that starts in the lower wall of the maxillary sinus and can be caused by periodontitis (PE), apical periodontitis (AP), oral maxillary sinus fistula and maxillary cysts, or secondary to complications of dental treatment[1]. In recent years, the number of papers on ODS has increased, although there is a lack of common diagnostic names and criteria. Most of them use "odontogenic sinusitis," some use "odontogenic maxillary sinusitis," and a few use the newer classification “sinonasal complications of dental disease and treatment” [2]. It is now clear that ODS is distinct from non-odontogenic sinusitis, which is classified as unilateral secondary chronic sinusitis due to localized odontogenic lesions, according to the European Position Paper on Rhinosinusitis and Nasal Polyps 2020 (EPOS)[3]. Misdiagnosis of the cause of sinusitis could lead to incorrect treatment, and if the sinus and odontogenic pathological irritation is not treated simultaneously, it may lead to treatment failure[4]. Currently, there are no clear definitions and ideal treatments for ODS. Some scholars believe that diagnosis of ODS does not require symptoms of sinusitis, emphasizing that nasal endoscopy is more effective in confirming bacterial sinusitis[5].However, given that both the EPOS and American Academy of Otolaryngology-Head and Neck Surgery guidelines require specific symptoms for the diagnosis of chronic sinusitis, the adjunctive support of endoscopy and computed tomography (CT) imaging may not be fully representative of the ODS population[6].In addition, in the early stage of ODS, oral lesions cause inflammation of the sinus mucosa, and in the absence of obstruction of the maxillary sinus orifice, the majority of patients do not have obvious symptoms of sinusitis, and founded to have thickening of the mucosa of the maxillary sinus on Cone-beam computed tomography (CBCT) examination, which should be called odontogenic maxillary sinusitis to be more precise, which has been reported extensively by oral surgeons and radiologists[7,8,9,10,11,12]. The severity of mucosal thickening is directly proportional to the oral lesion, and by treating the oral lesion, the sinus mucosal thickening can be controlled or even normalized. In our study, all patients underwent multidisciplinary evaluation, where otorhinolaryngologists specified the clinical signs of sinusitis and completed nasal endoscopy and sinus CT, and dentists performed oral examinations and diagnosis of oral lesions. Previous studies have compared sinus symptoms and imaging findings in ODS with those in non-ODS, and they found that foul smell, ipsilateral facial pressure, and middle meatal pus on endoscopy correlated higher with ODS than non-ODS[13,14]. However, the effects of different odontogenic etiologies on the symptoms of sinusitis have rarely been reported. Therefore, this study aimed to analyze the effects of different odontogenic etiologies on the clinical symptoms, extent of sinus involvement, and bone resorption and penetration in the maxillary sinus floor (MSF) among patients with ODS.
2. Materials and Methods
2.1. Clinical data and sample collection
A total of 103 patients with ODS recruited from the Department of Otolaryngology and Stomatology of Beijing Tongren Hospital between 2019 and 2021 were included in this study. All patients underwent endoscopic sinus surgery (ESS), and 76 of 103 patients completed ESS and stomatological surgery simultaneously (including oral lesion tooth extraction, as well as implant removal and oral maxillary sinus fistula repair). Sinus CT, nasal endoscopy, and oral examination were conducted for all the patients, and CBCT was performed for some patients with odontogenic lesions that could not be assessed on sinus CT images. The oral examinations included assessment of tooth condition or restoration, endodontic electrical vitality measurement, periodontal pocket depth (PPD), clinical attachment loss (CAL), and bone resorption of the MSF (based on CT images).The regular ENT examination include the patient's pre-operation and post-operation sinusitis symptoms and nasal endoscopy, which was evaluated on the basis of the modified Lund-Kennedy endoscopic scoring system, retaining the subscores of polyps, edema and discharge but excluding the subscores of scarring and crusting[15].
2.2. Inclusion and exclusion criteria
Clinical symptoms of chronic rhinosinusitis (obstruction, nasal discharge, facial pain/pressure, and reduction or loss of smell) and imaging findings (CT scans showing hypodense occupancy in the maxillary sinus and bony discontinuity of the MSF) were the inclusion criteria. In addition, the included patients also had an oral lesion corresponding to the maxillary sinus lesion.
Patients with maxillary sinus lesions without symptoms of sinusitis, those with only partial mucosal thickening of the maxillary sinus, those with fungal bulb sinusitis on imaging, and those with benign or malignant tumors of the maxillary sinus were excluded.
2.3. Diagnostic criteria for odontogenic lesions
The following findings characterize the diagnostic criteria for odontogenic lesions:
- Apical periodontitis (AP): Vitality of dental pulp (-); CAL (-); PPD (≤3 mm); and radiological bone loss (-)[18].
- Periodontitis (PE): Vitality of dental pulp (+); interdental CAL detectable at ≥2 nonadjacent teeth; buccal or oral CAL ≥3 mm with pocketing ≥3 mm detectable at ≥2 teeth, although the observed CAL cannot be ascribed to non-PE-related causes, such as 1) gingival recession of traumatic origin, 2) dental caries extending in the cervical area of the tooth, 3) CAL on the distal aspect of a second molar associated with malposition or extraction of a third molar, 4) endodontic lesion draining through the marginal periodontium, and 5) vertical root fracture[17].
- Temporary oroantral communications: Oral maxillary sinus communication after tooth extraction, mucosal healing of the oral fistula, and bone loss at the base of the maxillary sinus[19].
- Permanent oroantral fistulas: Oral maxillary sinus communication after tooth extraction, unhealed intraoral fistula, and oral and maxillary sinus communication[19].
2.4. Statistical analysis
Age and disease duration were compared as continuous data using analysis of variance. Sex, sinusitis symptoms, extent of sinus inflammation, and condition of bone penetration were compared using the Chi-squared test. The continuity-corrected Chi-squared test was used for theoretical frequencies T≥1 and <5. Fisher’s exact probability method for theoretical frequency was utilized when T<1. The abovementioned tests were two-sided tests with a test level of α=0.05, i.e., P<0.05, which was considered statistically significant. Statistical analyses were conducted using SPSS 23.0 (IBM Corporation, Armonk, NY, USA).
3. Results
3.1. Demographic and clinical characteristics of the ODS patients
The mean age of the 103 patients was 45.87±12.79 years. Sixty-three patients (61.2%) were male, and the mean duration of disease was 9.87±10.57 months.
Foul nasal odor (81.6%) and nasal discharge (anterior/posterior nasal drip) (84.5%) were the two most prominent symptoms in patients with ODS. According to CT analysis, there were 80 (77.7%), 41 (39.8%) and 7 (6.8%) cases that involved the ethmoid, frontal and sphenoid sinuses, respectively. The most common odontogenic etiologies were EPL (49.5%) and AP (32.0%) (Table 1).
There were significant differences in age (P=0.002), sex (P=0.036), inflammation involving the ethmoid sinus (P=0.037), and bone penetration in the MSF (P<0.001) among the AP, EPL, and PE groups. However, no statistically significant differences (P>0.005) were found in the sinusitis symptoms among patients with different odontogenic etiologies (Table 2).
3.2. Review of surgical data
We reviewed 76 cases of simultaneous oral treatment with ESS; 71 cases were diseased tooth extractions and simultaneous wound repairs, 4 were permanent oral maxillary sinus fistula repairs, and 1 was an implant removal and wound repair. The remaining patients underwent root canal treatment (RCT) or second-stage extraction of the diseased tooth after ESS for some of the affected teeth. Among the 71 patients who underwent simultaneous extractions, there were 25 cases requiring rotating mucosal flaps on the palatal side, 21 cases requiring gliding flaps on the buccal side, and 25 who required direct wound closure after filling with hemostatic sponges.
There were significant differences in preoperative and postoperative nasal symptoms and modified-LKS scores, and No patients developed an oral maxillary sinus fistula after the surgery. Furthermore, the sinus openings were clear, and the mucosa was not swollen at the 3-month review by nasal endoscopy (Table 3).
4. Discussion
ODS involves both sinusitis and odontogenic lesions, and the lack of knowledge about sinusitis among dentists and about oral health among otorhinolaryngologists makes the diagnosis and treatment of ODS difficult. In essence, an imbalance in the bacterial microecology leads to dysfunction in the normal clearance mechanism and drainage system of the sinuses and the symptoms of sinusitis. In a recent study, we used 16S rRNA sequencing to compare the microbiological differences between ODS patients and normal sinus secretions: The 3 most abundant genera were Fusobacterium, Porphyromonas, Prevotella in ODS patients and Staphylococcus, Corynebacterium, Cutibacterium in normal sinus secretions [20]. The presence of anaerobic bacteria in the nasal microbiome of ODS patients indicate potential tissue hypoxia or indicate that the discrete microenvironment within the mucus or bacterial biofilm in ODS patients may also be oxygen-limited, allowing anaerobic bacteria to survive. Therefore, the key to the treatment of ODS is to restore the microecological environment of the sinuses. There are two things that can be done: first, improve the drainage and anaerobic environment of the sinus cavities by medication or ESS surgery; second, completely remove the odontogenic lesions, reduce the microbial burden of the sinuses, and ultimately restore them to a stable state. In a recently published consensus, experts agreed that a multidisciplinary approach was optimal [21], However, concerning the optimal sequence of surgical interventions, the majority of contemporary otorhinolaryngologic literature recommends primarily addressing the odontogenic infection source. Other authors suggest a combined approach of oral removal of dental infection and simultaneously maxillary sinus drainage via ESS [22,23,24]. ESS can be undertaken to rapidly open the sinuses and improve the patient's symptoms, but some patients may be able to avoid surgery through dental treatment; therefore, to develop an optimal treatment plan, the etiology of odontogenic pathology should be clarified before proceeding with surgery.
Odontogenic lesions may be caused by dental disease or surgery, implant surgery, or maxillary sinus lift surgery and thus include issues whose etiologies go beyond the etymological definition of "odontogenic." Although dental implant surgery has caused an increasing number of odontogenic diseases, the vast majority of odontogenic lesions in patients are still caused by typical dental diseases and complications of dental treatment. Among the 103 patients with ODS included in this study, the top three odontogenic etiologies were EPL (49.50%), AP (32.0%), and PE (8.70%); nearly half of the patients presented with both apical and periodontal lesions, a share that differed from that reported in previous studies[25]. This discrepancy may be due to some patients having nonobvious periodontal lesions and being diagnosed with AP or no odontogenic etiology. Both pulpal and periodontal tissue lesions are involved in EPL. In patients affected by PE, EPLs usually progress slowly and without important symptoms. The most common signs and symptoms of pulp-infected teeth in EPLs are narrow, deep periodontal pockets that reach or approach the root apex and respond negatively to pulp vitality testing[26]. These symptoms are consistent with those in our patient diagnosed with EPL (Figure 1). According to our analysis, there are two possibilities; the first is chronic necrosis of the pulp, which occurs without considerable pain due to the chronic irritation of the pulp by the filling, resulting in apical lesions. The other condition is pulpal necrosis due to chronic PE, which may also cause no obvious pain. Since some periapical lesions are too small to be observed on sinus CT, CBCT should be performed to look more closely at dental lesions in patients with a high clinical suspicion of ODS.
A: Sinus CT shows resorption of alveolar bone on the palatal side of the left upper first molar, forming a narrow and deep periodontal pocket. B: MRI shows diseased tissue in the periodontal pocket connected to swollen mucosa in the maxillary sinus. C: Bone penetration of the palatal MSF in the extraction socket is observed during surgery. D: Palatal rotating mucosal flap to repair oral maxillary sinus fistula.
In this study, we compared the EPL, AP and PE groups in terms of demographic characteristics, sinus symptoms, and extent of sinus invasion. The three groups were found to have statistically significant differences in terms of sex and age, with patients in the PE group being older. There were no statistically significant differences in sinusitis symptoms among ODS patients with different odontogenic etiologies. However, the proper treatment of odontogenic lesions can affect the overall outcome for the patient, and different treatments are required for different odontogenic causes.Patients with ODS caused by AP tended to have a better prognosis, excluding those who had already had root canal treatment (RCT), root fractures, and periodontal lesions. For those patients whose lesions are limited to the apices of the teeth, infection from the pulp can be blocked by RCT, potentially avoiding the ESS procedure; therefore, it is recommended that patients with ODS caused by periapical lesions undergo dental treatment first. The infection from the pulp was controlled by RCT, and the patients’ sinus symptoms subsequently improved as early as during the RCT procedure. (Figure 2). After RCT, the decision to perform ESS is based on sinusitis symptoms and radiological findings. If the lesions are more extensive, involving root bifurcation, root fracture, or accompanied by periodontal inflammation, extraction of the diseased tooth should be considered to completely remove the lesion (Figure 3). In some of our cases, the diseased teeth were extracted before the ESS procedure, but the sinusitis symptoms did not improve even after the mucosa in the oral cavity had healed. Although the pathological irritation from the oral cavity was resolved, the obstruction of the sinus openings resulted in the formation of an anaerobic environment in the maxillary sinuses, requiring the ESS procedure to improve sinus ventilation and drainage (Figure 4).
A, B: Before root canal treatment, the patient developed a purulent discharge with a foul odor and obstruction of the maxillary sinus opening. C, D: After root canal treatment, infection of the dental pulp was controlled and the symptoms of sinusitis had disappeared, with the mucosa of the maxillary sinus returning to normal.
Figure 3: Recurrence of postoperative sinus symptoms after ESS for odontogenic sinusitis due to failure to treat the apical lesion
A, B: Large shading of the apical area of the diseased tooth and bone penetration of the maxillary sinus floor. The maxillary sinus opening was fully opened after ESS, and the maxillary sinus mucosa could not heal completely due to the apical lesion not having been removed. C: The apical lesion persisted despite RCT of the diseased tooth. D: A large amount of diseased granulation tissue adhered to the apical lesion.
In patients with severe periodontal infection, it is difficult to improve the resorbed alveolar bone through treatment. Infection from the oral cavity will continue to irritate the maxillary sinus mucosa through resorbed and destroyed alveolar bone. Five of the 103 patients had undergone ESS surgery, and although the sinus orifices were adequately opened, the inflammation of the sinus mucosa did not improve after surgery because the cause of the oral cavity was not addressed during the first treatment. (Figure 5). During the second operation, we found no obvious purulent secretions in the maxillary sinus but considerable mucosal swelling, which was associated with persistent irritation from the oral lesion. Therefore, the oral lesion was removed during the surgery, and the symptoms completely disappeared. Therefore, the best treatment plan for patients with EPLs and PE with severe periodontal pathology, especially those with bone penetration in the MSF, should be sinus surgery combined with extraction of the affected teeth, removal of the oral lesion, opening of the maxillary sinus for drainage, and closing of the oral maxillary sinus fistula as needed.
A: The patient was found to have sinusitis of the right maxillary sinus at the time of tooth extraction, and the affected tooth was extracted without an oral maxillary sinus fistula. B: The sinus CT was repeated 1 month after tooth extraction, which revealed ongoing sinus inflammation. C, D: One year after tooth extraction, there was already new bone formation on the floor of the maxillary sinus, however, the sinus symptoms were still not relieved as the maxillary sinus was not opened.
Figure 5: Patient with severe periodontal infection and no improvement in sinusitis symptoms after ESS
A, B: Sinus CT shows adequate maxillary sinus opening, alveolar bone resorption of the diseased tooth, and bone defects in the MSF. C, D: MRI shows periodontal lesion tissue attached to the mucosa of the maxillary sinus, with significant swelling of the maxillary sinus mucosa.
However, there were some limitations in the current study. First, the sample size was relatively small. Second, this was a single-center study in China, where the distribution of the odontogenic etiologies of ODS might differ from that in Europe and the United States, as such distribution is related to the local level of oral health knowledge. Further studies investigating these aspects will thus be needed in the future.
5. Conclusions
The key to the treatment of ODS is restoration of the microecological environment of the sinuses. Accurate evaluation and diagnosis of oral lesions are essential for the development of a treatment plan. EPL is a neglected oral etiology with a destructive effect on the bone of the MSF, and sinus surgery should be performed concurrently with extraction of the diseased teeth and debridement of the lesion.
Author Contributions
Conceptualization, Jianyou Wu, Ming Zheng, Xiangdong Wang and Songlin Wang; Data curation, Jianyou Wu and Ming Zheng; Formal analysis, Jianyou Wu; Funding acquisition, Xiangdong Wang; Investigation, Ming Zheng; Methodology, Songlin Wang; Supervision, Songlin Wang; Writing – original draft, Jianyou Wu; Writing – review & editing, Xiangdong Wang and Songlin Wang.
Funding
The study was funded by grants from the National Natural Science Foundation of China (81970852, 82000962 and 82171110). The funding bodies played no role in the design of the study, the collection, analysis, and interpretation of the data, and in the writing of the manuscript.
Institutional Review Board Statement
This study was approved by the Ethics Committee of Beijing Tongren Hospital (Grant No.: TRECKY2020-138). This study was conducted in accordance with the World Medical Association Declaration of Helsinki on medical research protocols and ethics.
Informed Consent Statement
Not applicable.
Data Availability Statement
Available on request.
Acknowledgments
We would like to thank all the staff of the Department of Otorhinolaryngology, Beijing TongRen Hospital, Capital Medical University, who contributed to our study.
Conflicts of Interest
No potential conflict of interest was reported by the authors.
References
- Nurchis M C, Pascucci D, Lopez M A, et al. Epidemiology of odontogenic sinusitis: an old, underestimated disease, even today. A narrative literature review. J Biol Regul Homeost Agents 2020, 34, 195–200. [Google Scholar]
- Allevi F, Fadda G L, Rosso C, et al. Diagnostic Criteria for Odontogenic Sinusitis: A Systematic Review. Am J Rhinol Allergy 2021, 35, 713–721. [Google Scholar] [CrossRef]
- Fokkens W J, Lund V J, Hopkins C, et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology 2020, 58, 1–464. [Google Scholar]
- Wang K L, Nichols B G, Poetker D M, et al. Odontogenic sinusitis: a case series studying diagnosis and management. Int Forum Allergy Rhinol 2015, 5, 597–601. [Google Scholar] [CrossRef]
- Craig J R, Poetker D M, Aksoy U, et al. Diagnosing odontogenic sinusitis: An international multidisciplinary consensus statement. Int Forum Allergy Rhinol 2021, 11, 1235–1248. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld R M, Piccirillo J F, Chandrasekhar S S, et al. Clinical practice guideline (update): adult sinusitis. Otolaryngol Head Neck Surg 2015, 152, S1–S39. [Google Scholar]
- Nair A K, Jose M, Sreela L S, et al. Prevalence and pattern of proximity of maxillary posterior teeth to maxillary sinus with mucosal thickening: A cone beam computed tomography based retrospective study. Ann Afr Med 2023, 22, 327–332. [Google Scholar] [CrossRef]
- Penarrocha-Oltra S, Soto-Penaloza D, Bagan-Debon L, et al. Association between maxillary sinus pathology and odontogenic lesions in patients evaluated by cone beam computed tomography. A systematic review and meta-analysis. Med Oral Patol Oral Cir Bucal 2020, 25, e34–e48. [Google Scholar]
- Zhang T, He Z, Tian H. Association between periodontal status and degree of maxillary sinus mucosal thickening: a retrospective CBCT study. BMC Oral Health 2021, 21, 392. [Google Scholar]
- Aksoy U, Orhan K. Association between odontogenic conditions and maxillary sinus mucosal thickening: a retrospective CBCT study. Clin Oral Investig 2019, 23, 123–131. [Google Scholar] [CrossRef]
- Jouhar R, Alkhames H M, Ahmed M A, et al. CBCT Evaluation of Periapical Pathologies in Maxillary Posterior Teeth and Their Relationship with Maxillary Sinus Mucosal Thickening. Healthcare 2023, 11. [Google Scholar]
- Alghofaily M, Alsufyani N, Althumairy R I, et al. Odontogenic Factors Associated with Maxillary Sinus Schneiderian Membrane Thickness and their Relationship to Chronic Sinonasal Symptoms: An Ambispective Cohort Study. Diagnostics 2023, 13. [Google Scholar]
- Turfe Z, Ahmad A, Peterson E I, et al. Odontogenic sinusitis is a common cause of unilateral sinus disease with maxillary sinus opacification. Int Forum Allergy Rhinol 2019, 9, 1515–1520. [Google Scholar] [CrossRef]
- Goyal V K, Ahmad A, Turfe Z, et al. Predicting Odontogenic Sinusitis in Unilateral Sinus Disease: A Prospective, Multivariate Analysis. Am J Rhinol Allergy 2021, 35, 164–171. [Google Scholar] [CrossRef]
- Psaltis A J, Li G, Vaezeafshar R, et al. Modification of the Lund-Kennedy endoscopic scoring system improves its reliability and correlation with patient-reported outcome measures. Laryngoscope 2014, 124, 2216–2223. [Google Scholar] [CrossRef]
- Sun P, Guo Z, Guo D, et al. The Microbiota Profile Analysis of Combined Periodontal-Endodontic Lesions Using 16S rRNA Next-Generation Sequencing. J Immunol Res 2021, 2021, 2490064. [Google Scholar]
- Papapanou P N, Sanz M, Buduneli N, et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Periodontol 2018, 89, S173–S182. [Google Scholar]
- Yue, L. [Problem solving in endodontic diseases: V. Correlation of clinical diagnosis, prognosis and histopathologic signs of apical periodontitis (I)]. Zhonghua Kou Qiang Yi Xue Za Zhi 2010, 45, 177–181. [Google Scholar]
- Bilginaylar, K. The Use of Platelet-Rich Fibrin for Immediate Closure of Acute Oroantral Communications: An Alternative Approach. J Oral Maxillofac Surg 2018, 76, 278–286. [Google Scholar] [CrossRef]
- Wu J, Zheng M, Zhao Y, et al. Bacterial diversity and community characteristics of the sinus and dental regions in adults with odontogenic sinusitis. BMC Microbiol 2023, 23, 201. [Google Scholar]
- Craig J, R. Odontogenic sinusitis: A state-of-the-art review. World J Otorhinolaryngol Head Neck Surg 2022, 8, 8–15. [Google Scholar] [CrossRef]
- Sabatino L, Pierri M, Iafrati F, et al. Odontogenic Sinusitis from Classical Complications and Its Treatment: Our Experience. Antibiotics 2023, 12. [Google Scholar]
- Shanti R M, Alawi F, Lee S M, et al. Multidisciplinary approaches to odontogenic lesions. Curr Opin Otolaryngol Head Neck Surg 2020, 28, 36–45. [Google Scholar] [CrossRef]
- Craig J R, Tataryn R W, Aghaloo T L, et al. Management of odontogenic sinusitis: multidisciplinary consensus statement. Int Forum Allergy Rhinol 2020, 10, 901–912. [Google Scholar] [CrossRef]
- Sakkas A, Weiss C, Ebeling M, et al. Factors Influencing Recurrence after Surgical Treatment of Odontogenic Maxillary Sinusitis: An Analysis from the Oral and Maxillofacial Surgery Point of View. J Clin Med 2023, 12. [Google Scholar]
- Herrera D, Retamal-Valdes B, Alonso B, et al. Acute periodontal lesions (periodontal abscesses and necrotizing periodontal diseases) and endo-periodontal lesions. J Periodontol 2018, 89, S85–S102. [Google Scholar]
Figure 1.
A patient with odontogenic sinusitis due to EPL with bone defects in the MSF.
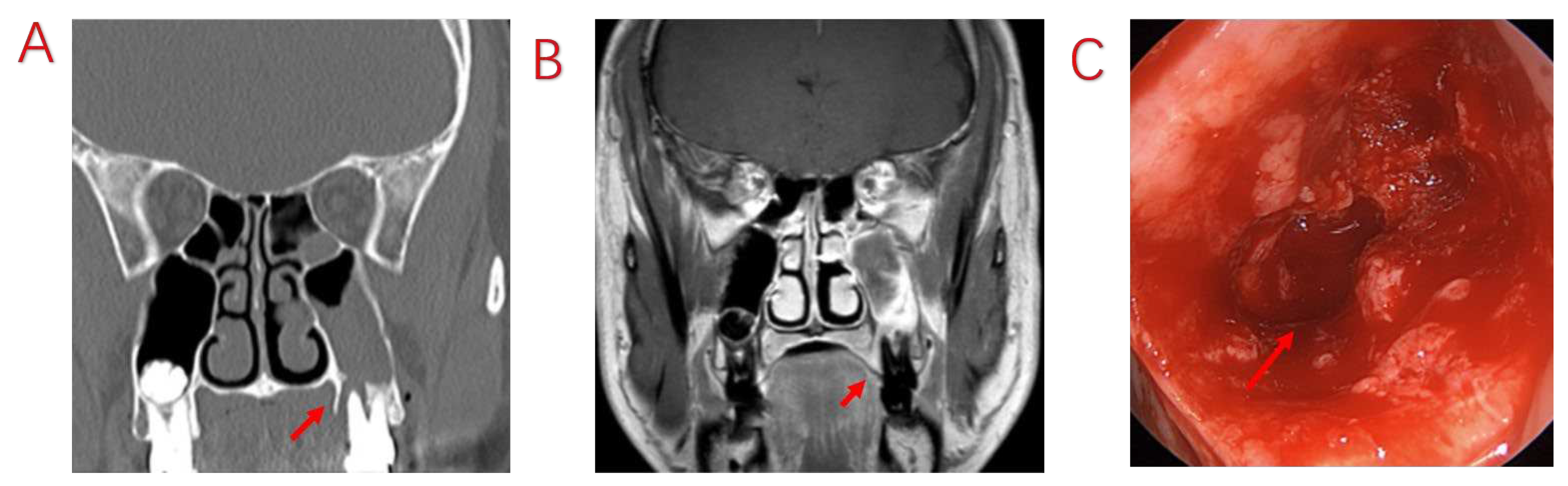
Figure 2.
Odontogenic sinusitis due to periapical inflammation. Symptoms disappeared after root canal treatment; no ESS was performed.
Figure 2.
Odontogenic sinusitis due to periapical inflammation. Symptoms disappeared after root canal treatment; no ESS was performed.
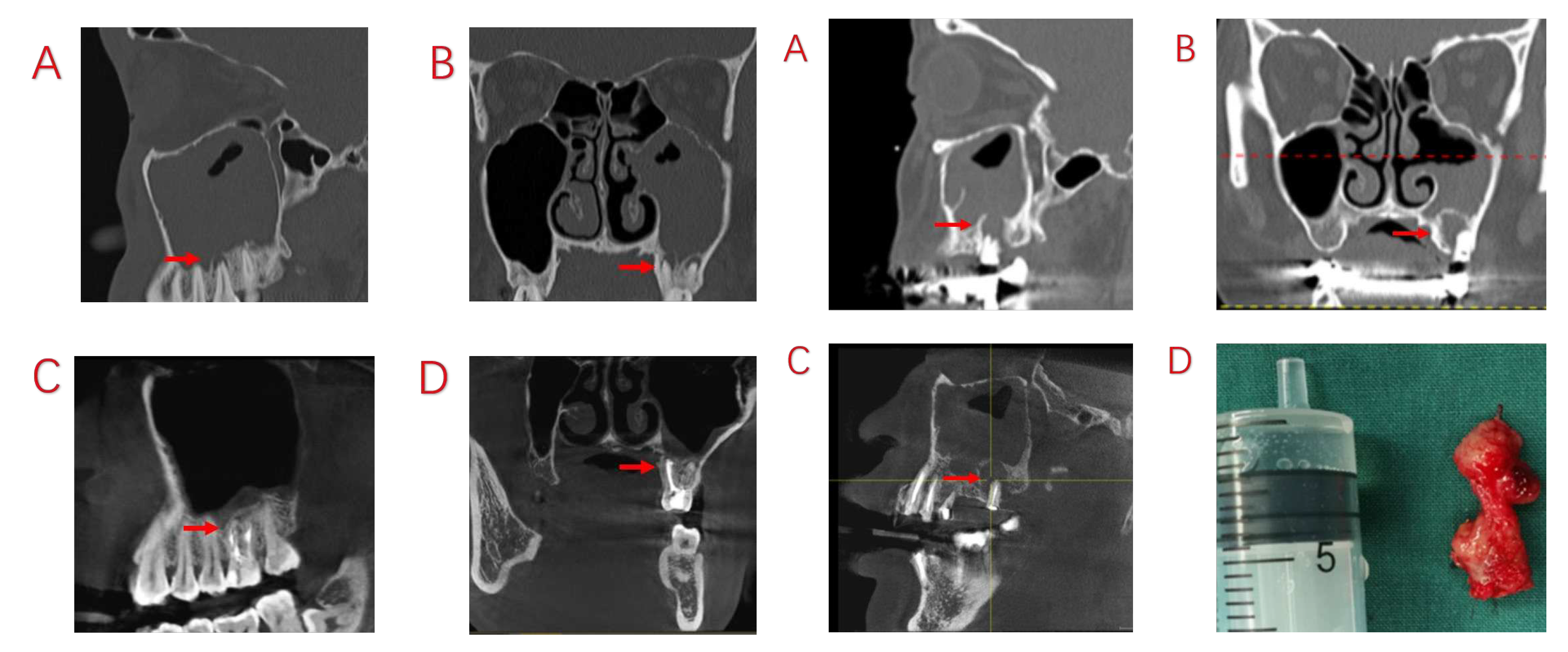
Figure 4.
Patient undergoes tooth extraction but no sinus ESS.
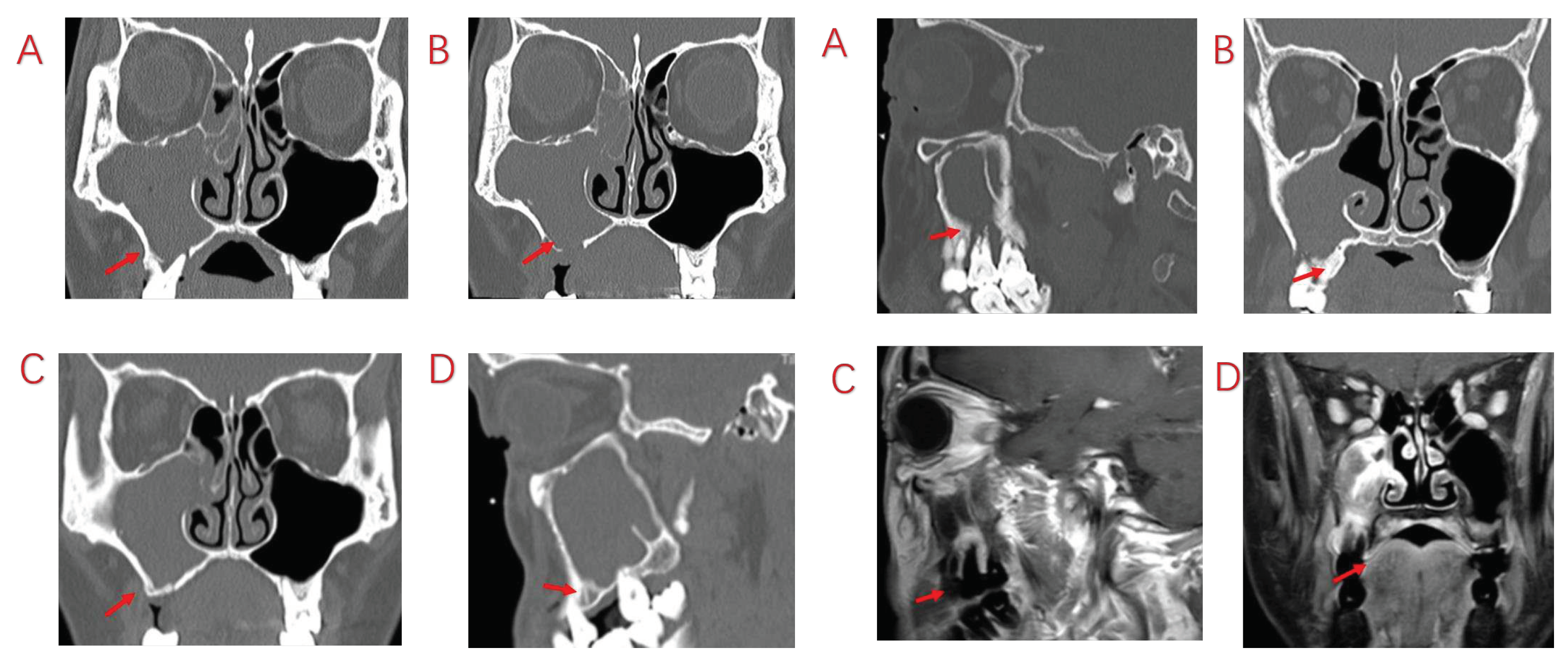

Table 1.
Demographics and clinical variables in patients with ODS.
| Variables | Symptomatic Patients with ODS (n=103) |
|---|---|
| Age (mean±SD, years) | 45.87±12.79 |
| Male sex (n, %) | 63 (61.2%) |
| Disease duration (mean±SD, months) | 9.87±10.57 |
| Symptoms (n, %) | |
| Foul nasal odor | 84 (81.6%) |
| Nasal obstruction | 60 (58.3%) |
| Nasal discharge (anterior/posterior nasal drip) | 87 (84.5%) |
| Facial pain/pressure | 63 (61.2%) |
| Reduction or loss of smell | 14 (13.6%) |
| Sinuses involved (n, %) | |
| Maxillary sinus | 103 (100.0%) |
| Ethmoid sinus | 80 (77.7%) |
| Frontal sinus | 41 (39.8%) |
| Sphenoid sinus | 7 (6.8%) |
| Odontogenic causes (n, %) | |
| AP | 33 (32.0%) |
| EPL | 51 (49.5%) |
| PE | 9 (8.7%) |
| Oroantral communications and fistulas (temporary) | 5 (4.8%) |
| Oroantral communications and fistulas (persistent) | 4 (3.9%) |
| Postoperative dental implants | 1 (1.0%) |
SD, standard deviation; AP, apical periodontitis; EPLs, endoperiodontal lesions; PE, periodontitis.
Table 2.
Comparison of the characteristics between the apical periodontitis (AP), endoperiodontal lesion (EPL), and periodontitis (PE) groups.
Table 2.
Comparison of the characteristics between the apical periodontitis (AP), endoperiodontal lesion (EPL), and periodontitis (PE) groups.
| Variables | AP (n=33) | EPL (n=51) | PE (n=9) | P Value |
|---|---|---|---|---|
| Age (mean±SD, years) | 40.00±12.16 | 48.92±12.08 | 50.78±6.82 | 0.002 a |
| Male sex (n, %) | 14 (42.4%) | 36 (70.6%) | 5 (55.6%) | 0.036 b |
| Course of disease (mean±SD, months) | 10.42±11.35 | 10.23±11.14 | 11.11±9.21 | 0.975 a |
| Symptoms (n, %) | ||||
| Foul nasal odor | 27 (81.8%) | 40 (78.4%) | 9 (100.0%) | 0.304 b |
| Nasal obstruction | 20 (60.6%) | 30 (58.8%) | 6 (66.7%) | 0.905 b |
| nasal drip | 28 (84.8%) | 46 (90.2%) | 7 (77.8%) | 0.427 c |
| Facial pain/pressure | 21 (63.6%) | 30 (58.8%) | 7 (77.8%) | 0.547 b |
| Reduction or loss of smell | 5 (15.2%) | 8 (15.7%) | 1 (11.1%) | 1.000 c |
| Involving sinuses (n, %) | ||||
| Maxillary sinus | 33 (100.0%) | 51 (100.0%) | 9 (100.0%) | - |
| Ethmoid sinus | 30 (90.9%) | 37 (72.5%) | 5 (55.6%) | 0.037 b |
| Frontal sinus | 17 (51.5%) | 19 (37.3%) | 1 (11.1%) | 0.077 b |
| Sphenoid sinus | 2 (6.1%) | 3 (5.9%) | 1 (11.1%) | 0.678 c |
| Bone penetration of MSF | 15 (45.5%) | 44 (86.3%) | 5 (55.6%) | <0.001b |
a ANOVA; b χ2 test; c Fisher’s exact test ;SD, standard deviation; MSF, maxillary sinus floor.
Table 3.
Patients’ pre-operation and post-operation sinusitis symptoms and nasal endoscopic findings.
Table 3.
Patients’ pre-operation and post-operation sinusitis symptoms and nasal endoscopic findings.
| Symptoms and Nasal Endoscope Finding (n=103) | Pre-Operation | Post-Operation | P Value* |
|---|---|---|---|
| Symptoms | |||
| Foul nasal odor | 84 (81.6%) | 0(0%) | <0.001 |
| Nasal obstruction | 60 (58.3%) | 3(2.9%) | <0.001 |
| Nasal discharge | 87 (84.5%) | 6(5.8%) | <0.001 |
| Facial pain/pressure | 63 (61.2%) | 0(0%) | <0.001 |
| Nasal endoscopy finding | |||
| Edema | |||
| 0: absent | 11 (10.7%) | 86 (83.5%) | <0.001 |
| 1: mild | 43 (41.7%) | 12 (11.6%) | <0.001 |
| 2: severe | 49 (47.6%) | 5 (4.9%) | <0.001 |
| Polyps | |||
| 0: no polyps | 69 (67.0%) | 103 (100%) | <0.001 |
| 1: polyps in middle meatus only | 19 (18.4%) | 0 (0%) | <0.001 |
| 2: beyond middle meatus | 15 (14.6%) | 0 (0%) | <0.001 |
| Discharge | |||
| 0: no discharge | 9 (8.7%) | 92 (89.3%) | <0.001 |
| 1: clear, thin discharge | 5 (4.9%) | 8 (7.8%) | 0.39 |
| 2: thick, purulent discharge | 89 (86.4%) | 3 (2.9%) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



