Submitted:
11 June 2024
Posted:
12 June 2024
You are already at the latest version
Abstract
Health care is currently showing a fall in heart failure (HF) prevalence and incidence particularly in developed countries, but with only a subset receiving appropriate therapy to protect the heart against maladaptive processes such as fibrosis and hypertrophy. Appropriate markers of advanced HF are still needed, which should help choosing the most suitable therapy and avoid major compliance problems. Speckle tracking echocardiography (STE) is a good choice, being a non-invasive imaging technique and is able to assess cardiac deformation in a variety of conditions. Several multicenter studies and meta-analyses have demonstrated its clinical applications and accuracy in early and late stages of HF, as well as its association with both left ventricular (LV) filling pressures and myocardial oxygen consumption, the two are important parameters in the evaluation of HF patients. Also, STE assists in assessing right ventricular free-wall longitudinal strain (RVFWLS) which is a solid predictor of right ventricle failure (RVF) following LV assist device (LVAD) implantation. Despite its limitations, STE plays an essential role in the clinical evaluation of patients with HF, early and advanced, in explaining symptoms and signs and also as an accurate prognosticator. The aim of this review is to examine the advantages of STE in early evaluation of myocardial dysfunction and their correlation with right heart catheterization (RHC) parameters, which should have a significant clinical relevance in the management of HF patients.
Keywords:
heart failure
; speckle tracking echocardiography
; heart cathetherization
; myocardial oxygen consumption
; myocardial fibrosis
1. Introduction
The European Society of Cardiology (ESC) defines heart failure (HF) as the presence symptoms and/or signs of HF caused by a structural and/or functional abnormality of the heart, which causing high intracardiac pressures and/or insufficient cardiac output at rest and/or during exercise [1]. The 2021 ESC guidelines categorize this pathology based on the left ventricular ejection fraction (LVEF) as HF with reduced EF (HFrEF, EF 40%), mildly reduced EF (HFmrEF, EF 41-49%), or preserved EF (HFpEF, EF 50%). Despite optimum treatment, many patients progress to late stage advanced HF [1].
Regardless of the decrease in its prevalence and incidence in industrialized nations, not all patients with HF are identified in its early stages. This inappropriate practice results in only a subset of such patients who receive suitable therapy to protect their heart from maladaptive processes such as myocardial fibrosis and LV hypertrophy [2]. This under-diagnosis can be ascribed mainly to the lack of highly specific imaging markers, particularly echocardiographic ones [2]. Despite LVEF has been used as the guiding parameter for beginning advanced treatments such as Sacubitril/Valsartan and Glifozins [1], cardioverter defibrillator implant (ICD) or cardiac resynchronization therapy (CRT) [1], several studies demonstrated its lower sensitivity to unmask LV myocardial dysfunction comparing to other echocardiographic parameters such as speckle tracking echocardiography (STE) [2,3]. Also, LVEF is limited by geometric assumptions, load dependency, reproducibility, inter-observer variability, and is influenced by heart rate, rhythm and translational motion [3]. On the other hand, LV global longitudinal strain (LV GLS), has been shown to be superior to EF in several settings such as predicting myocardial recovery and symptomatic improvement after aortic valve replacement [4], predicting all-cause and cardiovascular mortality in advanced chronic kidney disease (CKD) [5], and predicting major adverse cardiac events in HF patients [3].
Recent studies have applied STE to the left atrium (LA), based on the assumption that it is highly sensitive to pressure and volume overload because of LA thin wall [6]. Global peak atrial longitudinal strain (PALS) has been proved the earliest parameter to alter in many conditions associated with myocardial damage such as systemic hypertension and diabetes, even before the development of LV hypertrophy, reduced LVEF or LA enlargement [7,8,9]. Also, PALS has been shown to strongly relate to diastolic dysfunction and myocardial fibrosis (measured at histological analysis) hence has been proposed to provide a non-invasive estimation of LV filling pressures (LVFP) [10] and explanations of HF symptoms and quality of life [11]. In addition to the use of STE in assessing LA function, it has been used to define RV longitudinal function, thus allowing evaluation of myocardial deformation using typical two-dimensional echo images without angle dependency [12]. Although reference values for RV STE analysis have been established, it remains unclear whether RV global longitudinal strain (RV GLS) or RV free-wall longitudinal strain (RV FWLS) better captures RV myocardial deformation [13]. Indeed, several studies have demonstrated that RV FWLS in the advanced HF patients, strongly link with both RV stroke work index (RVSWI) and oxygen consumption (VO2) in end-stage HF, especially for LV assist device (L-VAD) selection [14].
The aim of this review is to examine advantages of STE features in early evaluation of myocardial damage and their correlation with right heart catheterization (RHC) parameters, in order to define its clinical purpose in early and advanced HF patients.
2. Speckle Tracking Echocardiography: Technical Aspects
STE is a semi-automated and angle-independent echocardiographic technique that allows evaluation of myocardial deformation in a range of specific conditions. Using previously saved echocardiographic pictures, a specific software can differentiate each speckle, integrating them in functional units (kernels) that are unequivocally recognized given their specific spatial disposition [15,16].
During a cardiac cycle, the computer tracks kernel movement in three spatial directions: radial, longitudinal, and circumferential. This technique allows the system to calculate deformation (strain), rate of deformation (strain rate), displacement, and rate of displacement (velocity) for the selected cardiac segments.[16,17]
The strain () can be defined as the degree of deformation (shortening) of the analyzed segment in relation to its initial dimensions. It is measured as a percentage and is expressed by the following equation:
where L is the final dimension of the segment and L0 is the initial dimension. A lengthening or thickening deformation has a positive value, while a shortening or thinning deformation has a negative one. The strain rate (ε') is the rate of heart deformation measured in seconds-1.[17] Velocity (V) is a vector number that can be measured directly or calculated by subtracting the average velocity from the left ventricle's total translation. The vector has two projections in the apical view: radial velocity (Vr), which is perpendicular to the endocardial margin and is positive if directed toward the ventricular cavity, and longitudinal velocity (Vl), which is tangential to the endocardial margin and is positive if directed from the base to the apex. On the short axis, there is a radial velocity (Vr) with the same features as those of the apical view, and a circumferential velocity (Vc), which is tangential to the endocardial edge and is positive when moving anti-clockwise.[16] Other critical parameters of LV function are twist and torsion. The twist is the difference in degrees between the systolic rotation of the ventricular apex and the basal rotation in the short axis, whereas the torsion is a twist measured in degrees/cm and standardized to LV main axis.[16]
STE is often used to assess LV function using several parameters, among which is the longitudinal strain, which is the cardiac deformation directed from the base to the apex: negative curves imply a reduction in the distance between the kernels caused by myocardial fiber shortening from the base to the apex.[19] The longitudinal strain analysed in 4-, 2- and 3-chambers can assess both regional and global strain (range of normality from -17.2% to - 27.7%).[20,21] Radial strain is a radially directed deformation caused by the radial propulsion of each kernel. Radial strain values, from the short axis view, are depicted by positive curves and typically vary between 21.1% and 53.8%.[21,22] Circumferential strain (usually -23.1% to -40.6%) indicates LV myocardial fiber shortening, identified from the short-axis view along the circumferential axis. As a result, during systole and shortening of the speckle-to-speckle distance, circumferential strain values are displayed as negative curves.[21,22]
Using the same STE principle, the technique can also assess LA activity during the cardiac cycle, which is divided into three stages: reservoir (when LA receives blood from the pulmonary veins), conduit (when blood flows passively from LA to LV), and contraction (when the remaining blood is pumped out from the LA into LV).[23,24] The STE software analyses images recorded in the apical 2- and 4-chamber views to provide a PALS value for each and the peak atrial contraction phase (PACS).[21,23]
STE can also be used to assess right ventricular (RV) myocardial function from the apical 4-chamber view. After defining the region of interest, which includes RV free wall and the interventricular septum, the software calculates both free wall longitudinal strain (RVFWLS, typically >-20%) and RV global longitudinal strain (GRVLS).[25,26]
3. Right Heart Catheterization
Right heart catheterization (RHC) is a semi-invasive diagnostic procedure used in patients with HF to assess both left and right heart function, diagnose pulmonary hypertension (PH), analyze therapeutic response, and determine patients’ prognosis (Table 2). It is performed via either the internal jugular vein or the femoral vein using a Swan-Ganz catheter.[27,[28,29]
RHC measures right atrial pressure (RAP), which usually varies from 2 to 8 mmHg. The waveform is typically defined by three peaks: the a wave, reflects atrial contraction and RV filling, based on RV end-diastolic pressure (RV EDP); the c wave, represents tricuspid valve closure; and v wave, coincides with RV contraction. The three waves are separated by two falls, the x-descent and the y-descent, respectively.[2,29] RAP waveforms can be affected by many pathologies, including: tricuspid regurgitation, which causes raised v-waves; ventricular dissociation, which causes giant a-waves due to simultaneous contraction of both atria and ventricles; restrictive cardiomyopathy and constrictive pericarditis, which cause deep descents; cardiac tamponade, which causes no rapid outflow from the RA to the RV, eliminating the y-descent.[2] These waves could vary in patients with combined pathologies. Finally, there is no a-wave in individuals with atrial fibrillation due to the lack of atrial contraction.[30]
After studying the RA the Swan-Ganz catheter is advanced to record RV pressures, both in systole and at end diastole.[2] Raised systolic RV pressure (RVP) frequently reflects intact RV function, but values drop when there is combined high RAP and a low cardiac index (CI) and are associated with RV failure.[2] The "dip plateau" phenomenon is induced by an abrupt cessation of RV filling and is a characteristic feature of restrictive pericarditis and restrictive cardiomyopathy.[2]
Proceeding further, pressure tip manometer measures the pulmonary artery pressure (PAP), whose waveform is defined by a fast pressure propagation from the RV, followed by a pressure fall at end-systole and a dicrotic notch reflecting pulmonary valve closure.[28]-[30] Blood flow, raised left atrial pressure (LAP), and pulmonary vascular resistance (PVR) all influence these measurements; therefore, stroke volume (SV), heart rate (HR), shunts, and pulmonary artery cross-sectional area and distensibility can all be determining factors.[2]
Pulmonary capillary wedge pressure (PCWP) is measured as the catheter is placed into a small pulmonary branch and reflects effective LA pressure.[2,30] PCWP is higher than RAP and 2-3 mmHg lower than dPAP. It also differentiates post-capillary PH (PCWP 15 mmHg) from pre-capillary PH (PCWP <15 mmHg). Patients with heart failure usually have a PCWP waveform with a strong v wave due to severe mitral regurgitation or poor LV or LA compliance.[2]
LAP is measured by balloon occlusion of the distal pulmonary branches; it has a waveform similar to that of RA with a, c, and v waves, as well as negative x and y descents.[2]
Finally, the LV pressure waveform is identical to that of RV, but with higher systolic pressure and diastolic pressure. LVEDP is used to measure preload and LV function; it is influenced by myocardial contractility, intravascular state, and LV compliance.[2]
RHC also allows calculation of hemodynamic parameters that can be used to determine myocardial function: thermodilution technique and the Fick principle are bith used to quantify cardiac output (CO).[2] The thermodilution method involves injecting a 10-20 mL cold bolus into the catheter's proximal part, while a thermistor in the distal end registers the differential temperature; and a specific software calculates the CO based on the injected temperature, volume, and blood specific gravity.[33] On the other hand, Fick principle’s determination is based on the following equation:
where VO2 is oxygen consumption, Hb is the hemoglobin blood concentration, SAO2 and SVO2 represents, respectively, the arterial and mixed venous blood oxygen saturation; assuming an average VO2 value for every patient (usually 125 mL/min/m2), Hb, SAO2, and SVO2 can be directly measured, permitting the CO determination.[2,34] If the parameters of the Fick equation are precisely measured, they raise the accuracy of of thermodilution in patients with low CO; however, due to the frequent lack of corrections for age, sex, height, weight, and metabolic state, VO2 can be overestimated, resulting in a falsely high CO.[2] SVO2 is normally 75%, it assesses peripheral organ perfusion, and it might decrease due to low CO or increased oxygen tissue demand.[2] Other important calculated parameters include pulmonary vascular resistance (PVR), RV stroke work index, and pulmonary artery pulsatility index.[2] PVR represents the resistance in the pulmonary circulation and can be calculated as follow:
PVR > 3 WU is associated with pulmonary vascular remodeling, meanwhile PVR >5 WU with a negative vasoreactivity test is an absolute contraindication for heart transplantation (HTx).[2]
RVSWI is a surrogate for RV systolic function, being directly proportional to the stroke volume index (SVI):
RVSWI <5 g*m2/beat, especially when paired with a PCWP >20 mmHg and a VO2 <14 mL/min/m2, is associated with increased mortality, the necessity for ventricular support device placement, and HTx at 1 year.[2]
Finally, the pulmonary artery pulsatility index (PAPi) is a unique hemodynamic measure that is often used in the pre-operative evaluation of patients with advanced HF who require a LVAD or HTx.[35] Most researchers have found an independent association between PAPi and survival.[38] PAPi is calculated as follow: Table 3
The most common RHC complications are non-sustained ventricular and atrial tachycardia resulting from catheter contact with the heart walls,[36] patients with left bundle branch block (LBBB) are more likely to experience intermittent complete atrioventricular block (AVB)[37]. Right bundle branch block (RBBB) occurs in 5% of patients.[38] Rare serious complications include RV rupture, pulmonary artery (PA) rupture, and RV infarction.[2,39] Minor complications, on the other hand, include venous spasm, bleeding, thrombophlebitis, atrial fibrillation, reversible LBBB or RBBB, and first or second degree AVB.[2]
In symptomatic patients with normal RHC pressures, stress test using particular drugs or exercise may be needed.[2] It is particularly useful in discriminating between primary and secondary PH, as well as in evaluating patients with HFrEF or HFpEF. The RHC stress test involves the patient lying supine or semi-supine on a bicycle ergometer with a workload increment of 25 W every 2 minutes and a PAP, PCWP, and CO analysis at rest, every step, immediately after exercise, and 6 minutes later. The HFpEF test usually results in submaximal exercise.[2] Fluid challenge using 1-2 L of saline at 100-200 mL/min and passive leg lifting can detect LV diastolic dysfunction,[40] patients with high LA volume and poor LA contraction, usually have high PCWP after passive leg lifting.[41] A PCWP 25 mmHg or LVEDP 16 mmHg indicates HFpEF.[40]
4. Myocardial Fibrosis
Myocardial fibrosis (MF) is an irreversible and maladaptive process that damages the myocardium following acute injuries (such as myocarditis) or long-term disorders (e.g. end-stage heart failure). It impacts heart chamber function, particularly relaxation, and contributes to cavity remodeling, stiffness, and, ultimately, complete pump failure.[42,43,44] The extracellular matrix (ECM) activates cardiac fibroblasts excessively, resulting in collagen production and increasing ECM growth.[44] The expanded ECM encircles cardiac myocytes and microvascular cells, resulting in early myofibril dysfunction.[46] Specific types of myocardial traumas stimulate inflammatory cells through the cytokine cascade, resulting in considerable proliferation of cardiac fibroblasts and collagen synthesis, eventually leading to MF.[46] This prolonged process is initially adaptive, but eventually results in serious alterations in myocardial fiber architecture and interstitial tissue remodeling, as well as localized inflammatory processes that compromise diastolic relaxation and active ventricular contraction.[47] Arterial hypertension (AH) and aortic stenosis (AS) are the most prevalent clinical models of pressure overload-induced MF. If left untreated, LV hypertrophy and diastolic dysfunction cause myocardial fibrosis and increased LV filling pressure, possibly leading to congestive heart failure.[44] Long standing concentric LV hypertrophy eventually leads to diastolic dysfunction, diminished early diastolic relaxation, and decreased compliance, requiring higher filling pressures to achieve normal end-diastolic volume.[48] Chronic hemodynamic alterations increase extracellular MF, which contributes to increased LV stiffness, decreased compliance, and deteriorated diastolic function.[49]
Isolated mitral regurgitation (MR) is the only heart condition that generates pure volume overload.[50] In the early disease, chronic volume overload promotes increased diastolic stress and myocyte length, culminating in larger LV chamber volume (eccentric hypertrophy) under high-volume/low-pressure conditions.[50] MR promotes sarcomere disarray and disturbance, as well as MF, which later on may contribute to LV systolic dysfunction and failure. Chronic MR increases LA volume and over-time it impacts LA myocardial function, manifested as reduced myocardial deformation.[51,52]
Severe aortic regurgitation (AR) is another cause of increased LV volume overload. It is typically asymptomatic and well tolerated for long time, hiding behind severe LV cavity remodeling caused by MF.[53] In the early stages of AR, the increasing preload drives eccentric hypertrophy to maintain cardiac output, LV compliance, normal LV EF, and stroke volume, resulting in systolic hypertension and afterload mismatch.[54]
Endomyocardial biopsy (EMB) is the gold standard investigation for diagnosing and assessing severity of MF. [10,14] The degree of MF have been measured from full-thickness biopsies of the atrial or ventricular myocardium (obtained from hearts excised at the time of cardiac transplantation). Three full-thickness slices of the myocardium measuring approximately 1x1 cm are taken, and the amount of fibrosis is evaluated using the average of the three slices.[14] Samples are fixed in 10% buffered formalin, paraffin embedded, and are divided into 4 μm thick sections for hematoxylin-eosin and Masson's trichrome staining.[14] All samples are then rinsed with distilled water and immersed in a hematoxylin solution for 3 minutes. The color is changed using lithium carbonate (0,1%) to influence the hematoxylin staining.[13] Slices are cleansed in pure water and dyed with red ponceau staining (oven at 30°C for 20 seconds at 45 KW) before being submerged in acid water and phosphomolybdic acid (1 minute). This process is followed by adding green light and acid water cleaning. Finally, the degree of MF is calculated as follow and expressed as percentage:[14]
5. Left Heart Pressures, Strain and Fibrosis
In 2020, the ESC described the HFpEF diagnostic algorithm (HFA-PEFF), which includes numerous Doppler echocardiographic measures related to LV filling pressures, such as indexed LA volume (LAVi), mitral annulus TDI, and E/e' ratio, as well as pulmonary pressures, such as sPAP and retrograde tricuspid regurgitation peak velocity (TRPV).[55] Novel echocardiographic measures have been proved superior to traditional ones in assessing left heart function. PALS correlates strongly with LV filling pressures, particularly in individuals with low EF, and it changes before LAVi.[56,57,58,59,60,61,6263] Also, an inverse association between PALS and chronic HF patients' quality of life measured by the Minnesota Living with Heart Failure Questionnaire (MLHFQ) has been shown.[64]
Studies have demonstrated that STE has the ability to predict the presence of MF, with good accuracy.[10] In patients with atrial fibrillation (AF) and end-stage HF, LA MF has been shown to be related to PALS, VO2max, NYHA class, LA stiffness, and E/e’.[10] PALS, in particular, has a good correlation with NYHA class , VO2max [65], and is a good predictor of MF. [10] These findings can be explained on the basis of the elevated LA pressure causing maladaptive remodeling including myocyte growth, hypertrophy, necrosis, and apoptosis. Furthermore the fibroblast mitosis enhances ECM with a switch into anaerobic metabolism, leading to a reduction in the myocardial energy production.[10] Recently, PALS has been found accurate in reflecting LA reservoir function, with a capacity outperforming traditional measurements (LA volume and LV GLS) in predicting all-cause mortality and hospitalization.[66]
The association between LA strain and cavity pressures was shown in a multicentric study of 322 patients with a mean LVEF 55% where both PALS and PACS were found to be associated with LV filling pressures (LVFP). The optimal cut-off for distinguishing normal from raised LVFP (PCWP >12 mmHg) was 18% for PALS and 8% for PACS.[62] Similar results were obtained in 210 patients with LVEF >50%, where PALS accurately identified patients with increased PCWP >15 mmHg compared to echocardiography and RHC, with an AUC of 0.76. Moreover, substituting TR peak velocity for PALS (<18%) in the 2016 ASE/EACVI algorithm led to 91% feasibility, 81% accuracy, and improved agreement with invasive measures.[67] These findings permitted PALS to be introduced as a new estimator of LVFP in a recent ESC consensus document.[68]
In end-stage HF, LVEF has failed to predict clinical outcomes at short and long-term. In contrast, LVGCS outperformed LVGLS in predicting long-term mortality and future clinical events, with higher sensitivity and specificity.[12,69] This is most likely because the fibers in the LV mid-wall (associated with circumferential strain) have greater intrinsic contractile activity than other myocardial fibers.[12,69] In contrast, in HFrEF patients, there is a modest relationship between transverse LV function; GCS, torsion, and MF, but a significant association with GLS, which has a stronger predictive value than other echocardiographic measures.[70,71]
6. Right Heart Pressures, Strain and Fibrosis
RV remodeling limits longitudinal performance while increasing transverse function by reducing the circumferential fibers of the outer myocardial layer. This anatomical fact explains why RVFWLS is a sensitive measure for diagnosing RV dysfunction.[72] End-stage HF patients exhibit a significant connection between RVFWLS and histologically confirmed MF, with RVFWLS being the primary determinant and the main predictor of MF. Also, this parameter is the most reliable diagnostic tool for detecting severe MF in patients with extensive RV fibrosis. RV free wall function has been proved as the most accurate parameter that predicts exercise capacity and clinical outcome in patients with DCM. [73]
In patients with PH, the RV strain can accurately predict clinical outcome, hence adds prognostic details to the other clinical and echocardiographic markers.[44] RV strain is reduced both in patients with PH and RV HF. Moreover, worsening RV strain is associated with significantly increased risk of all-cause mortality.[44] Even in ischemic patients, lower RVFWLS values have been associated with worse survival,[14] being able to identify the presence, location and the transmural extent of MF in AMI patients.[44] Finally, RVFWLS is linked with structural cardiopathies risk of hospitalization, being worse with the increasing NYHA class and higher NT pro–B-type natriuretic peptide.[74]
RV strain has been evaluated in advanced HF patients, especially in the pre-operative LVAD evaluation. Standard echocardiographic indices, such as tricuspid annulus s' and tricuspid annular plane systolic excursion (TAPSE), do not have clear correlation with patient’s prognosis.[17,74,75] On the other hand, multiple studies and a meta-analysis have shown that low RVFWLS on pre-operative echocardiography suggest a poor prognosis and the development of RV failure, whereas higher values are associated with a consistent improvement in RV deformity, as well as RVSWI.[17,74,75] Furthermore, RVFWLS is not only one of the best predictors of RV failure (RVF) following LVAD implantation, but also the strongest independent risk factor for developing RVF.[76]
Finally, recently estimated PCWP (ePCWP or ePAWP),[77] has been proposed being calculated as:
where LAVi represents LA volume indexed, TVmax is the peak velocity in tricuspid regurgitation, and E is the E wave measured using the PW up on the mitral annulus.[77] ePCWP shown good accordance with PCWP measured with RHC, even with values above 15 mmHg, and was associated with cardiovascular death even after adjustment for age, sex, and diastolic dysfunction grading.[77] Moreover, ePCWP was associated with worse prognosis across all grades of diastolic function, becoming a new important parameter for diastolic evaluation.[77]
7. Discussion
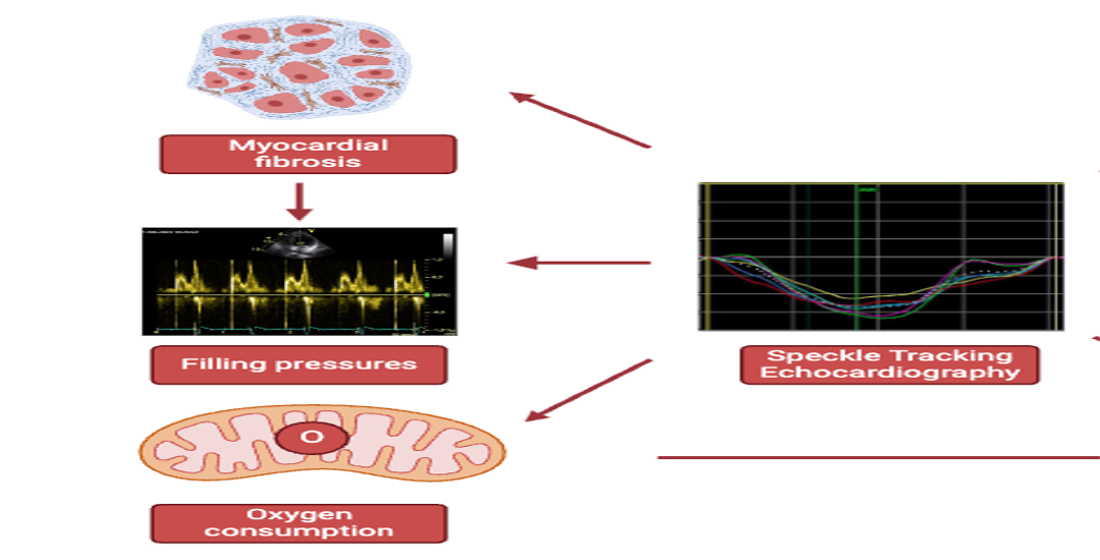
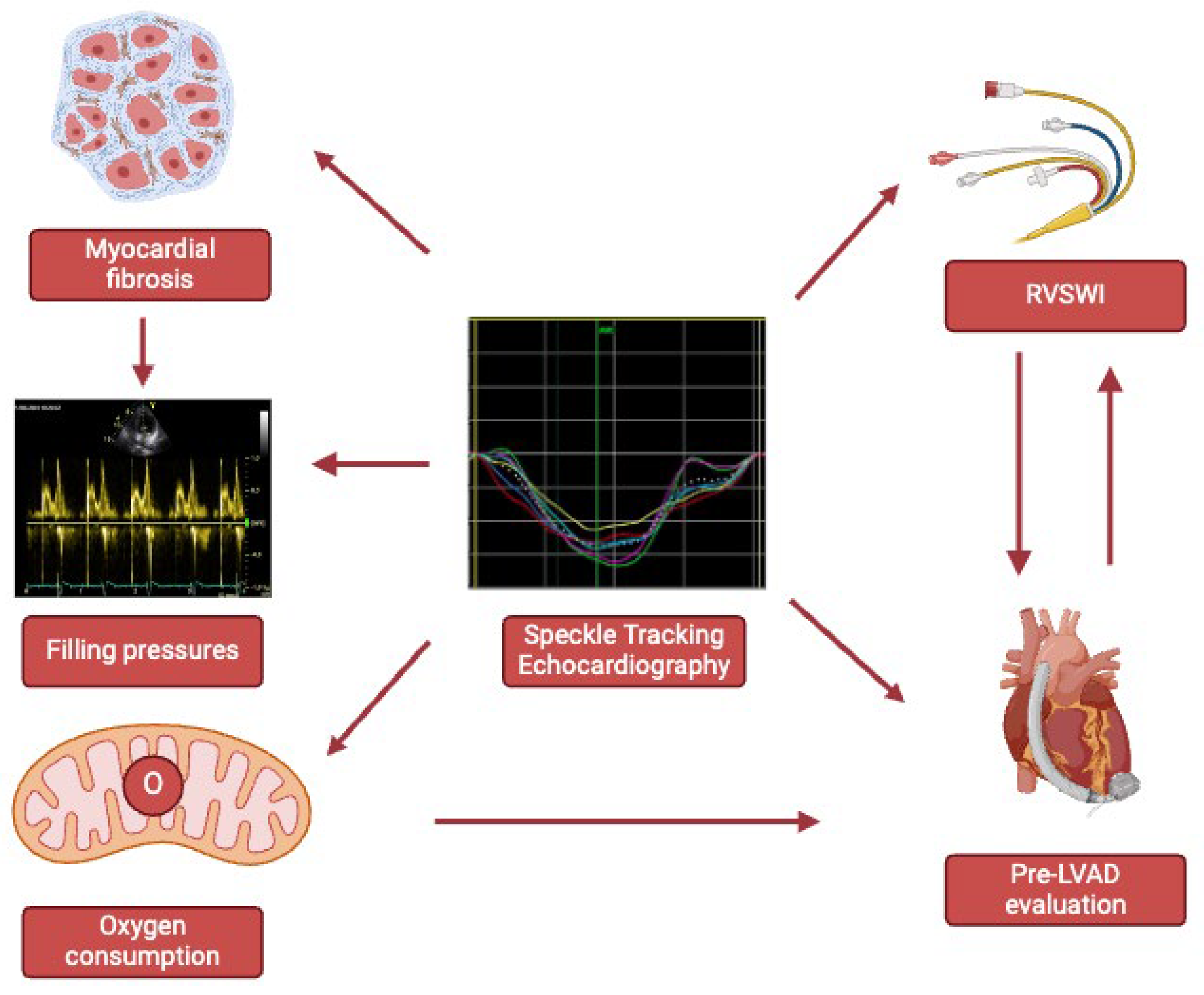
From its inception, STE has been the focus of numerous clinical studies on various aspects of myocardial function. In HF patients, there is significant correlation between LA strain, MF and clinical outcome. Also, PALS is related to both LV filling pressures, which are excellent measures of diastolic dysfunction, and myocardial VO2, a HF fundamental survival marker. Furthermore, LA strain allows detailed myocardial examination, and analysis of both chambers' histopathologic status and metabolic activity, with the latter being a key prognostic marker in patients with advanced HF. Furthermore, STE is significant for patient’s management and for guiding towards optimum treatment strategies. RVFWLS is not only connected to RVSWI but also directly to development of RV failure, thus making it critical in the pre-LVAD implantation evaluation. Because of these connections and the higher pace at which these parameters change with changes in medical condition, it is clear that STE plays an essential role in the evaluation of both early and advanced HF, allowing not only to prevent major myocardial damage but also to treat it with the most appropriate therapy. On the other hand, STE’s limitations, such as the need for optimal echocardiographic window, similar heart rate in different projections and pre-load dependence should not be underestimated (Figure 1).
8. Conclusions
Despite its limitations, STE is a non-invasive technique that plays an important role in the clinical evaluation of patients with HF, both early and advanced. It identifies not only prognosis but also the most appropriate medical treatment.
Author Contributions
Luca Martini, MD, Matteo Lisi, MD PhD, and Michael Y. Henein, MD PhD wrote the review, Matteo Cameli, MD PhD, Maria Concetta Pastore, MD, Francesca Maria Righini, MD, and Andrea Rubboli, MD, revised it critically.
Funding
the authors have not received any funding.
Institutional Review Board Statement
not applicable.
Informed Consent Statement
not applicable.
Data Availability Statement
the publications can be read using the Pubmed platform, the journals and the books mentioned in the references.
Acknowledgments
none declared by all authors.
Conflicts of Interest
none declared by all authors.
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Hear. Fail. 2022, 24, 4–131. [Google Scholar] [CrossRef]
- Coats, A.; Filippatos, G.; Bauersachs, J.; Rosano, G. The ESC Textbook of Heart Failure; Oxford University Press (OUP): Oxford, Oxfordshire, United Kingdom, 2023. [Google Scholar]
- Kalam, K.; Otahal, P.; Marwick, T.H. Prognostic implications of global LV dysfunction: a systematic review and meta-analysis of global longitudinal strain and ejection fraction. Heart 2014, 100, 1673–1680. [Google Scholar] [CrossRef]
- Kempny, A.; Diller, G.-P.; Kaleschke, G.; Orwat, S.; Funke, A.; Radke, R.; Schmidt, R.; Kerckhoff, G.; Ghezelbash, F.; Rukosujew, A.; et al. Longitudinal left ventricular 2D strain is superior to ejection fraction in predicting myocardial recovery and symptomatic improvement after aortic valve implantation. Int. J. Cardiol. 2013, 167, 2239–2243. [Google Scholar] [CrossRef]
- Krishnasamy, R.; Isbel, N.M.; Hawley, C.M.; Pascoe, E.M.; Burrage, M.; Leano, R.; Haluska, B.A.; Marwick, T.H.; Stanton, T. Left Ventricular Global Longitudinal Strain (GLS) Is a Superior Predictor of All-Cause and Cardiovascular Mortality When Compared to Ejection Fraction in Advanced Chronic Kidney Disease. PLOS ONE 2015, 10, e0127044–e0127044. [Google Scholar] [CrossRef]
- Cameli, M.; Mandoli, G.E.; Lisi, E.; Ibrahim, A.; Incampo, E.; Buccoliero, G.; Rizzo, C.; Devito, F.; Ciccone, M.M.; Mondillo, S. Left atrial, ventricular and atrio-ventricular strain in patients with subclinical heart dysfunction. Int. J. Cardiovasc. Imaging 2019, 35, 249–258. [Google Scholar] [CrossRef]
- Stefani, L.D.; Trivedi, S.J.; Ferkh, A.; Emerson, P.; Marschner, S.; Gan, G.; Altman, M.; Thomas, L. Left atrial mechanics evaluated by two-dimensional strain analysis: alterations in essential hypertension. J. Hypertens. 2024, 42, 274–282. [Google Scholar] [CrossRef]
- Mondillo, S.; Cameli, M.; Caputo, M.L.; Lisi, M.; Palmerini, E.; Padeletti, M.; Ballo, P. Early Detection of Left Atrial Strain Abnormalities by Speckle-Tracking in Hypertensive and Diabetic Patients with Normal Left Atrial Size. J. Am. Soc. Echocardiogr. 2011, 24, 898–908. [Google Scholar] [CrossRef]
- Emerson, P.; Stefani, L.; Boyd, A.; Richards, D.; Hui, R.; Altman, M.; Thomas, L. Alterations in Left Atrial Strain in Breast Cancer Patients Immediately Post Anthracycline Exposure. Hear. Lung Circ. 2023, 33, 684–692. [Google Scholar] [CrossRef]
- Mandoli, G.E.; Cameli, M.; Pastore, M.C.; Loiacono, F.; Righini, F.M.; D’ascenzi, F.; Focardi, M.; Cavigli, L.; Lisi, M.; Bisleri, G.; et al. Left ventricular fibrosis as a main determinant of filling pressures and left atrial function in advanced heart failure. Eur. Hear. J. - Cardiovasc. Imaging 2023, 25, 446–453. [Google Scholar] [CrossRef]
- Cameli, M.; Sciaccaluga, C.; Loiacono, F.; Simova, I.; Miglioranza, M.H.; Nistor, D.; Bandera, F.; Emdin, M.; Giannoni, A.; Ciccone, M.M.; et al. The analysis of left atrial function predicts the severity of functional impairment in chronic heart failure: The FLASH multicenter study. Int. J. Cardiol. 2019, 286, 87–91. [Google Scholar] [CrossRef]
- Cameli, M.; Righini, F.M.; Lisi, M.; Bennati, E.; Navarri, R.; Lunghetti, S.; Padeletti, M.; Cameli, P.; Tsioulpas, C.; Bernazzali, S.; et al. Comparison of Right Versus Left Ventricular Strain Analysis as a Predictor of Outcome in Patients With Systolic Heart Failure Referred for Heart Transplantation. Am. J. Cardiol. 2013, 112, 1778–1784. [Google Scholar] [CrossRef]
- Cameli, M.; Lisi, M.; Righini, F.M.; Tsioulpas, C.; Bernazzali, S.; Maccherini, M.; Sani, G.; Ballo, P.; Galderisi, M.; Mondillo, S. Right Ventricular Longitudinal Strain Correlates Well With Right Ventricular Stroke Work Index in Patients With Advanced Heart Failure Referred for Heart Transplantation. J. Card. Fail. 2012, 18, 208–215. [Google Scholar] [CrossRef]
- Lisi, M.; Cameli, M.; Righini, F.M.; Malandrino, A.; Tacchini, D.; Focardi, M.; Tsioulpas, C.; Bernazzali, S.; Tanganelli, P.; Maccherini, M.; et al. RV Longitudinal Deformation Correlates With Myocardial Fibrosis in Patients With End-Stage Heart Failure. JACC: Cardiovasc. Imaging 2015, 8, 514–522. [Google Scholar] [CrossRef]
- Mondillo, S.; Galderisi, M.; Mele, D.; Cameli, M.; Lomoriello, V.S.; Zacà, V.; Ballo, P.; D'Andrea, A.; Muraru, D.; Losi, M.; et al. Speckle-Tracking Echocardiography. J. Ultrasound Med. 2011, 30, 71–83. [Google Scholar] [CrossRef]
- Cameli M, Mondillo S, Galderisi M, Mandoli GE, Ballo P, Nistri S, Capo V, D'Ascenzi F, D'Andrea A, Esposito R, Gallina S, Montisci R, Novo G, Rossi A, Mele D, Agricola E. L’ecocardiografia speckle tracking: roadmap per la misurazione e l’utilizzo clinico [Speckle tracking echocardiography: a practical guide]. G Ital Cardiol (Rome). 2017 Apr;18(4):253-269. Italian. [CrossRef] [PubMed]
- Perk, G.; Tunick, P.A.; Kronzon, I. Non-Doppler Two-dimensional Strain Imaging by Echocardiography–From Technical Considerations to Clinical Applications. J. Am. Soc. Echocardiogr. 2007, 20, 234–243. [Google Scholar] [CrossRef]
- Voigt, J.-U.; Pedrizzetti, G.; Lysyansky, P.; Marwick, T.H.; Houle, H.; Baumann, R.; Pedri, S.; Ito, Y.; Abe, Y.; Metz, S.; et al. Definitions for a Common Standard for 2D Speckle Tracking Echocardiography: Consensus Document of the EACVI/ASE/Industry Task Force to Standardize Deformation Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 183–193. [Google Scholar] [CrossRef]
- Heimdal, A.; Støylen, A.; Torp, H.; Skjærpe, T. Real-Time Strain Rate Imaging of the Left Ventricle by Ultrasound. J. Am. Soc. Echocardiogr. 1998, 11, 1013–1019. [Google Scholar] [CrossRef]
- Brown, J.; Jenkins, C.; Marwick, T.H. Use of myocardial strain to assess global left ventricular function: A comparison with cardiac magnetic resonance and 3-dimensional echocardiography. Am. Hear. J. 2009, 157, 102–e1. [Google Scholar] [CrossRef]
- Sugimoto, T.; Dulgheru, R.; Bernard, A.; Ilardi, F.; Contu, L.; Addetia, K.; Caballero, L.; Akhaladze, N.; Athanassopoulos, G.D.; Barone, D.; et al. Echocardiographic reference ranges for normal left ventricular 2D strain: results from the EACVI NORRE study. Eur. Hear. J. - Cardiovasc. Imaging 2017, 18, 833–840. [Google Scholar] [CrossRef]
- Saito, K.; Okura, H.; Watanabe, N.; Hayashida, A.; Obase, K.; Imai, K.; Maehama, T.; Kawamoto, T.; Neishi, Y.; Yoshida, K. Comprehensive Evaluation of Left Ventricular Strain Using Speckle Tracking Echocardiography in Normal Adults: Comparison of Three-Dimensional and Two-Dimensional Approaches. J. Am. Soc. Echocardiogr. 2009, 22, 1025–1030. [Google Scholar] [CrossRef]
- Badano, L.P.; Kolias, T.J.; Muraru, D.; Abraham, T.P.; Aurigemma, G.; Edvardsen, T.; D’Hooge, J.; Donal, E.; Fraser, A.G.; Marwick, T.; et al. Standardization of left atrial, right ventricular, and right atrial deformation imaging using two-dimensional speckle tracking echocardiography: a consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 591–600. [Google Scholar] [CrossRef]
- Pathan, F.; D'Elia, N.; Nolan, M.T.; Marwick, T.H.; Negishi, K. Normal Ranges of Left Atrial Strain by Speckle-Tracking Echocardiography: A Systematic Review and Meta-Analysis. J. Am. Soc. Echocardiogr. 2017, 30, 59–70. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39. [Google Scholar] [CrossRef]
- Lee, J.-H.; Park, J.-H. Strain Analysis of the Right Ventricle Using Two-dimensional Echocardiography. J. Cardiovasc. Imaging 2018, 26, 111–124. [Google Scholar] [CrossRef]
- Gheorghiade, M.; Follath, F.; Ponikowski, P.; Barsuk, J.H.; Blair, J.E.; Cleland, J.G.; Dickstein, K.; Drazner, M.H.; Fonarow, G.C.; Jaarsma, T.; et al. Assessing and grading congestion in acute heart failure: a scientific statement from the Acute Heart Failure Committee of the Heart Failure Association of the European Society of Cardiology and endorsed by the European Society of Intensive Care Medicine. Eur. J. Hear. Fail. 2010, 12, 423–433. [Google Scholar] [CrossRef]
- Mueller, H.; Chatterjee, K.; Davis, K.; Fifer, M.; Franklin, C.; Greenberg, M.; Labovitz, A.; Shah, P.; Tuman, K.; Weil, M.; et al. Present use of bedside right heart catheterization in patients with cardiac disease. Circ. 1998, 32, 840–864. [Google Scholar] [CrossRef]
- Chatterjee, K. The Swan-Ganz Catheters: Past, Present, and Future. Circulation 2009, 119, 147–152. [Google Scholar] [CrossRef]
- Del Rio-Pertuz, G.; Nugent, K.; Argueta-Sosa, E. Right heart catheterization in clinical practice: a review of basic physiology and important issues relevant to interpretation. Am J Cardiovasc Dis. 2023, 13, 122–137.
- Bootsma, I.T.; Boerma, E.C.; Scheeren, T.W.L.; de Lange, F. The contemporary pulmonary artery catheter. Part 2: measurements, limitations, and clinical applications. J. Clin. Monit. Comput. 2021, 36, 17–31. [Google Scholar] [CrossRef]
- Humbert, M.; Kovacs, G.; Hoeper, M.M.; Badagliacca, R.; Berger, R.M.; Brida, M.; Carlsen, J.; Coats, A.J.; Escribano-Subias, P.; Ferrari, P.; et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Respir. J. 2023, 61, 2200879. [Google Scholar] [CrossRef]
- Forrester, J.S.; Ganz, W.; Diamond, G.; McHugh, T.; Chonette, D.W.; Swan, H. Thermodilution cardiac output determination with a single flow-directed catheter. Am. Hear. J. 1972, 83, 306–311. [Google Scholar] [CrossRef]
- Fagard, R.; Conway, J. Measurement of cardiac output: Fick principle using catheterization. Eur. Hear. J. 1990, 11, 1–5. [Google Scholar] [CrossRef]
- Lim, H.S.; Gustafsson, F. Pulmonary artery pulsatility index: physiological basis and clinical application. Eur. J. Hear. Fail. 2020, 22, 32–38. [Google Scholar] [CrossRef]
- Coulter, T.D.; Wiedemann, H.P. COMPLICATIONS OF HEMODYNAMIC MONITORING. Clin. Chest Med. 1999, 20, 249–267. [Google Scholar] [CrossRef]
- Morris, D.; Mulvihill, D.; Lew, W.Y.W. Risk of developing complete heart block during bedside pulmonary artery catheterization in patients with left bundle-branch block. Arch. Intern. Med. 1987, 147, 2005–2010. [Google Scholar] [CrossRef]
- Sprung, C.L.; Elser, B.; Schein, R.M.H.; Marcial, E.H.; Schrager, B.R. Risk of right bundle-branch block and complete heart block during pulmonary artery catheterization. Crit. Care Med. 1989, 17, 1–3. [Google Scholar] [CrossRef]
- Kearney, T.J.; Shabot, M.M. Pulmonary Artery Rupture Associated With the Swan-Ganz Catheter. Chest 1995, 108, 1349–1352. [Google Scholar] [CrossRef]
- Pieske, B.; Tschöpe, C.; A de Boer, R.; Fraser, A.G.; Anker, S.D.; Donal, E.; Edelmann, F.; Fu, M.; Guazzi, M.; Lam, C.S.P.; et al. How to diagnose heart failure with preserved ejection fraction: the HFA–PEFF diagnostic algorithm: a consensus recommendation from the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). Eur. Hear. J. 2019, 40, 3297–3317. [Google Scholar] [CrossRef]
- Henein, M.Y.; Tossavainen, E.; A'Roch, R.; Söderberg, S.; Lindqvist, P. Can Doppler echocardiography estimate raised pulmonary capillary wedge pressure provoked by passive leg lifting in suspected heart failure? Clin. Physiol. Funct. Imaging 2018, 39, 128–134. [Google Scholar] [CrossRef]
- Conrad, C.H.; Brooks, W.W.; Hayes, J.A.; Sen, S.; Robinson, K.G.; Bing, O.H.L. Myocardial Fibrosis and Stiffness With Hypertrophy and Heart Failure in the Spontaneously Hypertensive Rat. Circulation 1995, 91, 161–170. [Google Scholar] [CrossRef]
- Kass, D.A.; Bronzwaer, J.G.; Paulus, W.J. What Mechanisms Underlie Diastolic Dysfunction in Heart Failure? Circ. Res. 2004, 94, 1533–1542. [Google Scholar] [CrossRef]
- Lisi, M.; Cameli, M.; Mandoli, G.E.; Pastore, M.C.; Righini, F.M.; D’ascenzi, F.; Focardi, M.; Rubboli, A.; Mondillo, S.; Henein, M.Y. Detection of myocardial fibrosis by speckle-tracking echocardiography: from prediction to clinical applications. Hear. Fail. Rev. 2022, 27, 1857–1867. [Google Scholar] [CrossRef]
- Gyöngyösi, M.; Winkler, J.; Ramos, I.; Do, Q.; Firat, H.; McDonald, K.; González, A.; Thum, T.; Díez, J.; Jaisser, F.; et al. Myocardial fibrosis: biomedical research from bench to bedside. Eur. J. Hear. Fail. 2017, 19, 177–191. [Google Scholar] [CrossRef]
- Mandoli, G.E.; D'Ascenzi, F.; Vinco, G.; Benfari, G.; Ricci, F.; Focardi, M.; Cavigli, L.; Pastore, M.C.; Sisti, N.; De Vivo, O.; et al. Novel Approaches in Cardiac Imaging for Non-invasive Assessment of Left Heart Myocardial Fibrosis. Front. Cardiovasc. Med. 2021, 8. [Google Scholar] [CrossRef]
- Travers, J.G.; Kamal, F.A.; Robbins, J.; Yutzey, K.E.; Blaxall, B.C. Cardiac Fibrosis: The Fibroblast Awakens. Circ. Res. 2016, 118, 1021–1040. [Google Scholar] [CrossRef]
- Kampaktsis, P.N.; Kokkinidis, D.G.; Wong, S.-C.; Vavuranakis, M.; Skubas, N.J.; Devereux, R.B. The role and clinical implications of diastolic dysfunction in aortic stenosis. Heart 2017, 103, 1481–1487. [Google Scholar] [CrossRef]
- Krayenbuehl, H.P.; Hess, O.M.; Monrad, E.S.; Schneider, J.; Mall, G.; Turina, M. Left ventricular myocardial structure in aortic valve disease before, intermediate, and late after aortic valve replacement. Circulation 1989, 79, 744–755. [Google Scholar] [CrossRef]
- Zile, M.R.; Tomita, M.; Nakano, K.; Mirsky, I.; Usher, B.; Lindroth, J.; Carabello, B.A. Effects of left ventricular volume overload produced by mitral regurgitation on diastolic function. Am. J. Physiol. Circ. Physiol. 1991, 261, H1471–H1480. [Google Scholar] [CrossRef]
- Cameli, M.; Lisi, M.; Giacomin, E.; Caputo, M.; Navarri, R.; Malandrino, A.; Ballo, P.; Agricola, E.; Mondillo, S. Chronic Mitral Regurgitation: Left Atrial Deformation Analysis by Two-Dimensional Speckle Tracking Echocardiography. Echocardiography 2011, 28, 327–334. [Google Scholar] [CrossRef]
- Bonow, R.O. Left Atrial Function in Mitral Regurgitation. JACC: Cardiovasc. Imaging 2014, 7, 233–235. [Google Scholar] [CrossRef]
- Weidemann, F.; Herrmann, S.; Störk, S.; Niemann, M.; Frantz, S.; Lange, V.; Beer, M.; Gattenlöhner, S.; Voelker, W.; Ertl, G.; et al. Impact of Myocardial Fibrosis in Patients With Symptomatic Severe Aortic Stenosis. Circulation 2009, 120, 577–584. [Google Scholar] [CrossRef]
- Lee, J.K.; Franzone, A.; Lanz, J.; Siontis, G.C.; Stortecky, S.; Gräni, C.; Roost, E.; Windecker, S.; Pilgrim, T. Early Detection of Subclinical Myocardial Damage in Chronic Aortic Regurgitation and Strategies for Timely Treatment of Asymptomatic Patients. Circulation 2018, 137, 184–196. [Google Scholar] [CrossRef]
- Pieske, B.; Tschöpe, C.; A de Boer, R.; Fraser, A.G.; Anker, S.D.; Donal, E.; Edelmann, F.; Fu, M.; Guazzi, M.; Lam, C.S.P.; et al. How to diagnose heart failure with preserved ejection fraction: the HFA–PEFF diagnostic algorithm: a consensus recommendation from the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). Eur. Hear. J. 2021, 40, 3297–3317. [Google Scholar] [CrossRef]
- Cameli, M.; Mandoli, G.E.; Loiacono, F.; Dini, F.L.; Henein, M.; Mondillo, S. Left atrial strain: a new parameter for assessment of left ventricular filling pressure. Hear. Fail. Rev. 2015, 21, 65–76. [Google Scholar] [CrossRef]
- Cameli, M.; Sparla, S.; Losito, M.; Righini, F.M.; Menci, D.; Lisi, M.; D'Ascenzi, F.; Focardi, M.; Favilli, R.; Pierli, C.; et al. Correlation of Left Atrial Strain and Doppler Measurements with Invasive Measurement of Left Ventricular End-Diastolic Pressure in Patients Stratified for Different Values of Ejection Fraction. Echocardiography 2016, 33, 398–405. [Google Scholar] [CrossRef]
- Kurt, M.; Tanboga, I.H.; Aksakal, E.; Kaya, A.; Isik, T.; Ekinci, M.; Bilen, E. Relation of left ventricular end-diastolic pressure and N-terminal pro-brain natriuretic peptide level with left atrial deformation parameters. Eur. Hear. J. Cardiovasc. Imaging 2012, 13, 524–530. [Google Scholar] [CrossRef]
- Cameli, M.; Lisi, M.; Focardi, M.; Reccia, R.; Natali, B.M.; Sparla, S.; Mondillo, S. Left Atrial Deformation Analysis by Speckle Tracking Echocardiography for Prediction of Cardiovascular Outcomes. Am. J. Cardiol. 2012, 110, 264–269. [Google Scholar] [CrossRef]
- Morris, D.A.; Belyavskiy, E.; Aravind-Kumar, R.; Kropf, M.; Frydas, A.; Braunauer, K.; Marquez, E.; Krisper, M.; Lindhorst, R.; Osmanoglou, E.; et al. Potential Usefulness and Clinical Relevance of Adding Left Atrial Strain to Left Atrial Volume Index in the Detection of Left Ventricular Diastolic Dysfunction. JACC: Cardiovasc. Imaging 2018, 11, 1405–1415. [Google Scholar] [CrossRef]
- Morris, D.A.; Takeuchi, M.; Krisper, M.; Köhncke, C.; Bekfani, T.; Carstensen, T.; Hassfeld, S.; Dorenkamp, M.; Otani, K.; Takigiku, K.; et al. Normal values and clinical relevance of left atrial myocardial function analysed by speckle-tracking echocardiography: multicentre study. Eur. Hear. J. Cardiovasc. Imaging 2015, 16, 364–372. [Google Scholar] [CrossRef]
- Inoue, K.; Khan, F.H.; Remme, E.W.; Ohte, N.; García-Izquierdo, E.; Chetrit, M.; Moñivas-Palomero, V.; Mingo-Santos, S.; Andersen. S.; Gude, E.; et al. Determinants of left atrial reservoir and pump strain and use of atrial strain for evaluation of left ventricular filling pressure. Eur. Hear. J. - Cardiovasc. Imaging 2021, 23, 61–70. [Google Scholar] [CrossRef]
- Henein, M.Y.; Holmgren, A.; Lindqvist, P. Left atrial function in volume versus pressure overloaded left atrium. Int. J. Cardiovasc. Imaging 2015, 31, 959–965. [Google Scholar] [CrossRef]
- Cameli, M.; Sciaccaluga, C.; Loiacono, F.; Simova, I.; Miglioranza, M.H.; Nistor, D.; Bandera, F.; Emdin, M.; Giannoni, A.; Ciccone, M.M.; et al. The analysis of left atrial function predicts the severity of functional impairment in chronic heart failure: The FLASH multicenter study. Int. J. Cardiol. 2019, 286, 87–91. [Google Scholar] [CrossRef]
- Lisi, M.; Mandoli, G.E.; Cameli, M.; Pastore, M.C.; Righini, F.M.; Benfari, G.; Rubboli, A.; D’ascenzi, F.; Focardi, M.; Tsioulpas, C.; et al. Left atrial strain by speckle tracking predicts atrial fibrosis in patients undergoing heart transplantation. Eur. Hear. J. Cardiovasc. Imaging 2022, 23, 829–835. [Google Scholar] [CrossRef]
- Gerber, B.L.; Castilho, B. New insights into assessing severity of advanced heart failure through left atrial mechanics. Eur. Hear. J. Cardiovasc. Imaging 2024. [Google Scholar] [CrossRef]
- Venkateshvaran, A.; Tureli, H.O.; Faxén, U.L.; Lund, L.H.; Tossavainen, E.; Lindqvist, P. Left atrial reservoir strain improves diagnostic accuracy of the 2016 ASE/EACVI diastolic algorithm in patients with preserved left ventricular ejection fraction: insights from the KARUM haemodynamic database. Eur. Hear. J. - Cardiovasc. Imaging 2022, 23, 1157–1168. [Google Scholar] [CrossRef]
- A Smiseth, O.; A Morris, D.; Cardim, N.; Cikes, M.; Delgado, V.; Donal, E.; A Flachskampf, F.; Galderisi, M.; Gerber, B.L.; Gimelli, A.; et al. Multimodality imaging in patients with heart failure and preserved ejection fraction: an expert consensus document of the European Association of Cardiovascular Imaging. Eur. Hear. J. Cardiovasc. Imaging 2022, 23, e34–e61. [Google Scholar] [CrossRef]
- Cho, G.-Y.; Marwick, T.H.; Kim, H.-S.; Kim, M.-K.; Hong, K.-S.; Oh, D.-J. Global 2-Dimensional Strain as a New Prognosticator in Patients With Heart Failure. J Am Coll Cardiol. 2009, 54, 618–624. [Google Scholar] [CrossRef]
- Sengeløv, M.; Jørgensen, P.G.; Jensen, J.S.; Bruun, N.E.; Olsen, F.J.; Fritz-Hansen, T.; Nochioka, K.; Biering-Sørensen, T. Global Longitudinal Strain Is a Superior Predictor of All-Cause Mortality in Heart Failure With Reduced Ejection Fraction. JACC: Cardiovasc. Imaging 2015, 8, 1351–1359. [Google Scholar] [CrossRef]
- Cameli, M.; Mondillo, S.; Righini, F.M.; Lisi, M.; Dokollari, A.; Lindqvist, P.; Maccherini, M.; Henein, M. Left Ventricular Deformation and Myocardial Fibrosis in Patients With Advanced Heart Failure Requiring Transplantation. J. Card. Fail. 2016, 22, 901–907. [Google Scholar] [CrossRef]
- Tadic, M.; Pieske-Kraigher, E.; Cuspidi, C.; Morris, D.A.; Burkhardt, F.; Baudisch, A.; Haßfeld, S.; Tschöpe, C.; Pieske, B. Right ventricular strain in heart failure: Clinical perspective. Arch. Cardiovasc. Dis. 2017, 110, 562–571. [Google Scholar] [CrossRef]
- Motoki, H.; Borowski, A.G.; Shrestha, K.; Hu, B.; Kusunose, K.; Troughton, R.W.; Tang, W.; Klein, A.L. Right Ventricular Global Longitudinal Strain Provides Prognostic Value Incremental to Left Ventricular Ejection Fraction in Patients with Heart Failure. J. Am. Soc. Echocardiogr. 2014, 27, 726–732. [Google Scholar] [CrossRef]
- Barssoum, K.; Altibi, A.M.; Rai, D.; Kharsa, A.; Kumar, A.; Chowdhury, M.; Elkaryoni, A.; Abuzaid, A.S.; Baibhav, B.; Parikh, V.; et al. Assessment of right ventricular function following left ventricular assist device (LVAD) implantation—The role of speckle-tracking echocardiography: A meta-analysis. Echocardiography 2020, 37, 2048–2060. [Google Scholar] [CrossRef]
- Cameli, M.; Loiacono, F.; Sparla, S.; Solari, M.; Iardino, E.; Mandoli, G.E.; Bernazzali, S.; Maccherini, M.; Mondillo, S. Systematic Left Ventricular Assist Device Implant Eligibility with Non-Invasive Assessment: The SIENA Protocol. J. Cardiovasc. Ultrasound 2017, 25, 39–46. [Google Scholar] [CrossRef]
- Stricagnoli, M.; Sciaccaluga, C.; Mandoli, G.E.; Rizzo, L.; Sisti, N.; Aboumarie, H.S.; Benfari, G.; Maritan, L.; Tsioulpas, C.; Bernazzali, S.; et al. Clinical, echocardiographic and hemodynamic predictors of right heart failure after LVAD placement. Int. J. Cardiovasc. Imaging 2022, 38, 561–570. [Google Scholar] [CrossRef]
- Lindow T, Manouras A, Lindqvist P, Manna D, Wieslander B, Kozor R, Strange G, Playford D, Ugander M. Echocardiographic estimation of pulmonary artery wedge pressure: invasive derivation, validation, and prognostic association beyond diastolic dysfunction grading. Eur Heart J Cardiovasc Imaging. 2024 Mar 27;25(4):498-509. [CrossRef] [PubMed]
Figure 1.
The STE network for advanced HF evaluation and treatment. RVSWI: right ventricle stroke work index; LVAD: left ventricular assist device.
Figure 1.
The STE network for advanced HF evaluation and treatment. RVSWI: right ventricle stroke work index; LVAD: left ventricular assist device.

| Parameter | Reference values (%) |
|---|---|
| Left ventricle | |
| GLS | -17.2 - -27.7 |
| GRS | 21.1 – 53.8 |
| GCS | -23.1 - -40.6 |
| Left atrium | |
| PALS | 42.3 – 52.4 age 20-40 35.4 – 46.1 age 40-60 30.9 – 41.9 age > 60 |
| PACS | 11.9 – 19.0 age 20-40 13.2 – 19.6 age 40-60 13.6 – 21.4 age > 60 |
| Right ventricle | |
| RVFWS | > -20 |
STE: speckle tracking echocardiography; GLS: global longitudinal strain; GRS: global radial strain; GCS: global circumferential strain; PALS: left atrium strain reservoir; PACS: left atrium strain conduit phase; RVFWS: right ventricle free-wall strain.
| HTx check list |
| Diagnosis and differential diagnosis for PH |
| Fulminant myocarditis |
| Peripartum cardiomyopathy |
| Differential diagnosis for sepsis |
| ADHF requiring inotropic, vasopressor, and vasodilator therapy |
| Cardiogenic shock |
| Discordant left and right ventricular dysfunction |
RHC: right heart catheterization; HTx: heart transplantation; PH: pulmonary hypertension; ADHF: acute decompensated heart failure.
| Parameter | Reference values |
|---|---|
| Right atrium | |
| Mean RAP | 2-8 mmHg |
| RA a wave | 3-7 mmHg |
| RA v wave | 3-8 mmHg |
| Right ventricle | |
| RVESP | 17-32 mmHg |
| RVEDP | 2-8 mmHg |
| Pulmonary artery | |
| mPAP | 10-21 mmHg |
| sPAP | 17-32 mmHg |
| dPAP | 4-15 mmHg |
| PCWP | 2-8 mmHg |
| Left atrium | |
| Mean LAP | 6-12 mmHg |
| LA a wave | 4-14 mmHg |
| LA v wave | 6-16 mmHg |
| Left ventricle | |
| LVESP | 90-140 mmHg |
| LVEDP | 5-12 mmHg |
| Derived parameters | |
| CO | 2.5-4.5 mL/min/m2 |
| PVR | <2 WU |
| RVSWI | 5-10 g*m2/beat |
| PAPi | 0.9 in RV infarction <1.85 in patients undergoing LVAD implantation <3.65 in patients with advanced HF |
RAP: right atrium pressure; RA: right atrium; RVESP: right ventricle end-systolic pressure; RVEDP: right ventricle end-diastolic pressure; mPAP: mean pulmonary artery pressure; sPAP: systolic pulmonary artery pressure; dPAP: diastolic pulmonary artery pressure; PCWP: pulmonary capillary wedge pressure; LAP: left atrium pressure; LA: left atrium; LVESP: left ventricle end-systolic pressure; LVEDP: left ventricle end-diastolic pressure; CO: cardiac output; PVR: pulmonary vascular resistance; RVSWI: right ventricle stroke work index; PAPi: pulmonary artery pulsatility index; LVAD: left ventricular assist device; HF: heart failure.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



