
Submitted:
11 June 2024
Posted:
13 June 2024
You are already at the latest version
Abstract
Introduction: Neoadjuvant chemotherapy in breast cancer offers the possibility to facilitate breast and axillary surgery, it is a test of chemosensibility in vivo with significant prognostic value and may tailor adjuvant treatment according to response. Material and Methods: a retrospective single institution of 482 stage II and III breast cancer patients treated with neoadjuvant chemotherapy based on anthracycline and taxans plus antiHEr2 in those Her2 positive cases. Survival was calculated at 5 and 10 years. Kaplan Meier with log rank test were calculated for difference according to TNM, pathological and molecular surrogated subtype, TILs cut-off 20%, response to chemotherapy and the presence of vascular invasion. Results: In the univariate those factors that influenced long-term patient outcome were TNM (p=0.000); pathologic subtype (p=0.003); Tils cut off 20%; achieving pCR (p=0.000), RCB (p=0.000) and vascular invasion (p=0.000). After a mean follow up of 126 months, Luminal tumors presented a substantial difference of survival rates calculated at 5 or 10 years (81.2% compared to 74.7%) whereas for TNBC was 75.3 and 73.5, respectively. The greatest difference was seen according to response those patients with pCR presented a 10yDDFS of 95.5 vs 72.4% for those patients without pCR. This difference was especially meaningful in TNBC were 10y DDFS according to the RCB 0 to 3 was 100%, 80.6%, 69% and 49.2% respectively. Patients with a special bad prognosis in our series were lobular carcinomas with 10y DDFS of 42.9% vs 79.7%, p= 0.001 for ductal carcinomas; and those patients with vascular invasion at the surgical specimen with a 10yDDFS of 59.2% vs 83.6, p=0.,000 for those patients without vascular invasion. Conclusion: long-term outcomes after neoadjuvant chemotherapy can help patient and clinician make well-informed decisions.
Keywords:
Neoadjuvant chemotherapy
; breast cancer
; survival
; prognostic factors
; well-informed decision making
1. Introduction
Neoadjuvant or primary chemotherapy (NACT) was first developed for locally advanced, inoperable breast cancer patient to reduce tumoral volume in order to facilitate operability [1,2]. Once the classical studies of Bonnadona and Fisher stablished the great advantages of primary chemotherapy not only to accomplish surgical advantages but also as a prognostic tool, the use of NACT has been widely incorporated as the primary therapeutic approach in stage II and III breast cancer patients [3]. In this sense, the American Society of Clinical Oncology (ASCO) recommendations for neoadjuvant therapy published in 2021 [4] states that NACT offers a range of potential advantages including downstaging of the primary tumor to bring to operability; It can also be used to reduce the extent of local therapy in the breast and axilla, or reduce delays in initiating therapy , more prompt treatment of subclinical distant micrometastases and enhanced ability to evaluate in vivo the response of the tumor to particular systemic agents. In addition the ASCO recommendations incorporate a new argument to recommend the use of neoadjuvant chemotherapy, i.e, those patients whom residual disease may need a change in therapy in view of the results of those trials that have focused on using a lack of response to neoadjuvant therapy to identify patients who have a worse prognosis and could therefore benefit from additional adjuvant treatment, as the CreateX [5] for luminal and triple negative breast cancers or the Katherine [6] for HER2 positive ones. This population serves as an ideal group in whom new therapies or treatment escalation strategies should be studied. Numerous trials will inform a more personalized approach to both escalation and de-escalation using neoadjuvant therapy response pathological and genomic risk markers; patient age, health, and personal preferences; efficacy of systemic and local treatments; and in some instances, tumor response to preoperative therapy.
In addition, the St Gallen Consensus Conference 2023 [7] pointed out in the need to offer guidance to clinicians regarding appropriate treatments for early-stage breast cancer and assist in balancing the realistic trade-offs between treatment benefit and toxicity, enabling patients and clinicians to make well-informed choices through a shared decision-making process. For those reasons, the approach to breast cancer is increasingly personalized, considering specific factors such as: clinical stage; biological features of the tumor including tumor subtype, and within subtype.
The present work aims to provide long-term prognostic information based on the response to neoadjuvant chemotherapy to help clinicians and patients make a well-informed decision.
2. Material al Methods
A retrospective observational single institution study was performed involving 482 stage II and III breast cancer patients who had attended the Institut Catala d’Oncologia at Bellvitge University Hospital from June 2008 to December 2016.
Patients were eligible for enrollment if they were at least 18 years of age, newly diagnosed, previously untreated, stage II or III cancer as determined by radiological assessment, clinical assessment or both, presented an Eastern Cooperative Oncology Group performance status score of 0 or 1 (on a 5-point scale), and showed adequate organ function. Patients who were already enrolled in a clinical trial were excluded from this study. Informed consent was obtained from all the patients.
NACT consisted of a 6-month anthracycline-taxane regimen plus trastuzumab in the HER2-positive cases. The anthracycline schema was doxorubicine 60mg/m2 plus cyclophosphamide 600 mg/m2 every 21 days x 4 cycles. The taxane chosen was mainly docetaxel at 100 mg/m2 every 21 days x 4 cycles, but some patients received weekly paclitaxel x 12, especially those HER2 cases in combination with trastuzumab. Clinical and radiological responses were measured according to the criteria of the World Health Organization. The tumor and positive lymph nodes confirmed cytological were marked before starting NACT.
Patients underwent definitive surgery 3 to 4 weeks after the last cycle of NACT. Breast-conserving surgery was offered if margins were guaranteed with an optimal aesthetic result. When a mastectomy was mandatory, immediate reconstructive options were offered to the patient, predominantly with autologous flaps to avoid the development of capsular fibrosis with silicone implants. In clinical N0 cases (cN0), a sentinel lymph node biopsy was offered before chemotherapy up to 2009 and after chemotherapy thereafter, which was validated in our Breast Cancer Unit [8]. Lymphadenectomy was performed in all Node positive (N+) patients at diagnosis and in positive sentinel lymph node cases. Target axillary dissection was introduced in our institution after 2016.
pCR was defined as the absence of an infiltrating carcinoma in the breast and in the axillary lymph nodes, defined as ypT0/ypTis ypN0. For non-pCR, RCB was calculated according to the method of Symmans et al [9].
Adjuvant therapy for patients with HER2-positive tumors consisted of trastuzumab for up to one year. In patients with hormone receptor-positive tumors, adjuvant therapy consisted of hormonotherapy with tamoxifen/aromatase inhibitors for five years, extending up to 10 years in those with a high risk of recurrence such as ypT3-4 or ypN+ cases. TNBC cases have been offered adjuvant capecitabine since 2015.
Radiotherapy (RT) was administered according to our institutional protocol. Worst-case scenario (pre- or post-chemotherapy) was considered to decide whether RT should be administered. RT was given after breast-conserving surgery. A boost to the tumor bed was administered with brachytherapy or external beam RT in young patients or in those with a high risk of locoregional recurrence . RT to the chest wall after mastectomy was administered in N+ cases, those with affected surgical margins or in patients with large tumors (≥ T3). Nodal RT was given if more than 3 nodes were affected. If 1-3 nodes were involved, risk factors were taken into account to decide nodal irradiation [10]. Residual nodal disease after chemotherapy was also an indication for nodal RT. Nodal irradiation included infra and supraclavicular lymph nodes and axillary if extended axillary fat was involved. Internal mammary lymph nodes were irradiated if affected or in N+ patients with T4 tumors or tumors located in the internal quadrants [11].
Follow-up was performed every 6 months from the last course of RT. Mammography was performed once a year, starting 6 months after the irradiation therapy or one year from diagnosis. Other complementary examinations were performed according to the symptoms of the patient. Follow up is extended up to 10 years in our institution, a post-discharge program was implemented to guarantee annual control by local gynecologist that maintain the connection with or breast cancer unit.
The following patient and tumor characteristics were analyzed: age, body mass index (BMI), the anatomic and prognostic TNM stage, pathologic subtype (ductal, lobular or others), histologic grade, hormone receptor status (positive ≥ 10% versus negative), HER2 status (positive if the ICH score is 3+ or amplified by FISH according to the 2007 and 2013 criteria of ASCO/CAP , Ki-67 (≤ 30 versus > 30), breast cancer molecular surrogated subtype according to St Gallen 2013 (luminal A-like, luminal B-like, luminalBHER2 positive, HER2 positive and TNBC) and the presence of tumor-infiltrating lymphocytes (TILs) at diagnosis considering clinically meaningful at a cut-off 20% [12]. The other variables evaluated after NACT were: pCR, RCB and vascular invasion. Other variables included in the data base was type of breast surgery, type of radiotherapy, local and distant recurrences, and death from any cause.
The survival endpoint included disease free survival (DFS), distant disease-free survival (DDFS), calculated from the time of NACT commencement until a distant recurrence or death, whichever occurred first, as defined by DATECAN [13]. Overall survival (OS) was calculated from the time of NACT commencement until death from any cause, while breast cancer-specific survival (BCSS) was calculated until death from breast cancer. The Kaplan–Meier method was used to estimate the probability of survival, while the log-rank test was applied to compare the groups. The data cut-off was the 7th of June 2024. Data from patients who did not have a documented event were censored at the date the patient was last known to be alive and event-free.
Categorical variables are presented as the number of cases and percentages. Continuous variables following a normal distribution are presented as means and quartile1 and 3 (q1 and q3). Cox proportional hazards models were used to calculate hazard ratios (HR) and the 95% CI of each prognostic factor by univariate and multivariate analyses in relation to distant disease survival. A p-value below 0.05 was considered to indicate statistical significance. Statistical analysis was carried out using IBM SPSS version 23 (SPSS, Chicago, IL, USA).
3. Results
3.1. Patient and Tumor Characteristics
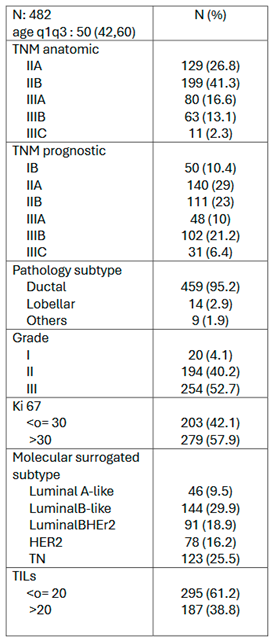
Patient and tumor characteristics are described in Table 1. Characteristics are in accordance with a series of neoadjuvant chemotherapy i.e., young age, one third locally advanced tumors, mainly ductal, high proliferation rate and a limited representation of luminal A-like tumors. TILs over 20% was observed in nearly 40% of the cases.

Table 1.
Patient and tumor characterisitcs.
3.2. Neoadjuvant Chemotherapy Outcomes
Pathologic complete response (pCR) was achieved in 25.3% of patients. By molecular surrogated subtypes pCR was observed in one of the 46 (2.2%) luminal A-like, 15 out of 144 (10.4%) luminal B-like; 27 out of 91 (29.7%) luminal B Her2 positive, 40 out of 78 (51.3%) Her2 positive and in 39 out of 123 (31.7%) TNBC. In those cases without pCR , the RCB was calculated with a 45% RCB III. Vascular invasion was noted in 21% of the cases. See Table 2
Table 2.
Neoadjuvant outcomes.
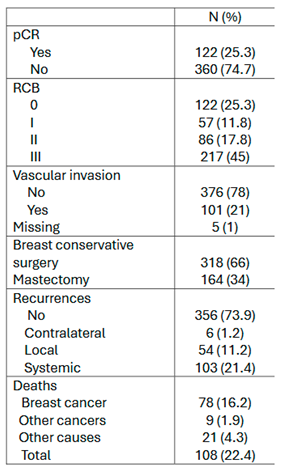
Breast conservative surgery was achieved in a 66% of the patients.
3.3. Survival Outcomes
After a mean follow up of 126 months (q1 94-q3 150) 124 events were recorded: 6 contralateral cancer, 54 locoregional recurrences and 103 systemic recurrences, of those 37 locoregional and systemic. See Table 2.
Kaplan Meier curves are depicted in Figure 1 for DFS, DDFS, BCSS and OS. The 10y estimated DFS for the whole series was 77.3% (95%CI 73.3%-81.4%), for DDFS was 76.3% (95%CI 72.3%-80.3%), for BCSS was 83.7% (95%CI 80.3%-87.2%), and for OS was 78.7% (95%CI 74.9%-82.5%).
Kaplan Meier curves and log-rank were calculated for DDFS according to basal characteristics, mainly TNM anatomic and prognostic, pathology and molecular surrogated subtype and the presence of clinically meaningful Tils cut-off 20%. Remarkably the 5yDDFS differed from the 10yDDFS specially in the luminal subtypes: in luminal B-like 5y DDFS was 81.2% whereas the 10yDDFS dropped to 74.7%, in comparison with the TNBC that presented a 5yDDFS of 75.3% similar to the 10y DDFS of 73.3%. See Figure 2.
Kaplan Meier curves and log-rank were calculated according to pathological findings at surgery, mainly pCR, RCB and vascular invasion. See Figure 3.
3.4. Prognostic Factors for Patient Survival
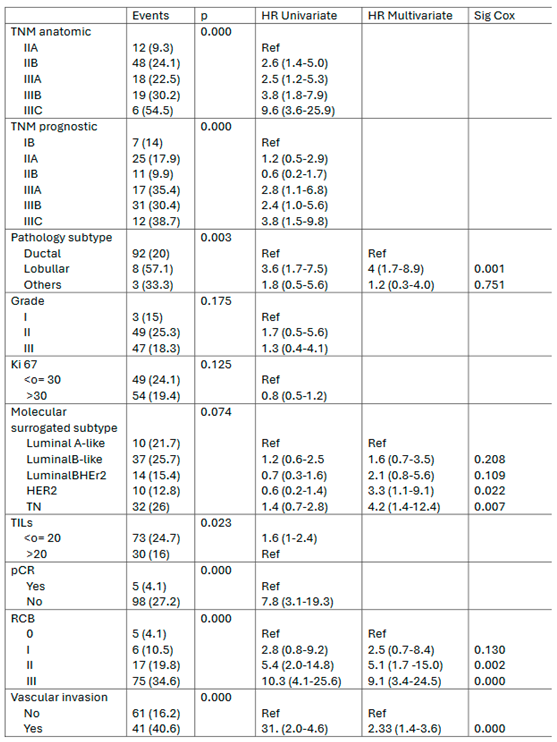
In the univariate Cox-regression model those variables related to distant disease-free survival (DDFS) were TNM (both anatomic and prognostic); pathology subtype, the presence of TILs cut-off 20% (positive related), the achievement of good response measured either by pCR or by the RCB (positive related) and the presence of vascular invasion (inversely related).
In the multivariate cox-regression model those variables independently related to DDFS were the pathologic subtype in favor of ductal subtype, lobular subtype presented a 4-fold higher risk of distant relapse than ductal tumors; the molecular surrogated subtype HER2 and TNBC with a HR of 3.3 and 4.2, respectively, the response to NACT by RCB with a HR for RCBI, RCB II and RCB III in reference to RCB 0 (pCR) of 2.5, 5.1 and 9.1, respectively; and vascular invasion with a HR of 2.3 in reference to those patients with no vascular invasion at the surgical specimen. See Table 3.
Table 3.
Prognostic factors for patient survival. Univariate and Multivariate.Analysis.
3.5. Discussion
Improvements in neoadjuvant chemotherapy regimens have led to substantial improvements in patient survival outcomes in the last 20 years [14]. The data showed in the present study in a series of stage II and III breast cancer patients treated with an anthracycline and taxans backbone schemas plus antiHER in patients with Her2 positive tumors shows a clinically meaningfully difference compared to that published previously when CMF was the standard with no distinction according to HER2 [15]. The 8yDFS at that time was 57.63% compared to the 10y DFS of 77.3% presented in this paper. Better odds are awaited with new pharmacological approaches such as the doble blockade antiHER2 [16], antibody drug conjugates [6], the introduction of platins [17] and immune checkpoint inhibitors for TNBC [18] and the use of CDK 4 and 6 inhibitors in luminal tumors [19,20].
The nowadays schemas selected for neoadjuvant chemotherapy in breast cancer has presented a real revolution in the last 20 years, especially in Her2 and TNBC. The introduction of trastuzumab in the neoadjuvant setting for Her2 positive patients raised pCR from 25% up to 66.7% [21]. The double blockade with trastuzumab-pertuzumab plus chemotherapy showed a better response a survival rates compared to single agent plus chemotherapy (5y DFS 86% for trastuzumab plus pertuzumab + docetaxel vs 81% for trastuzumab plus docetaxel and 73% pertuzumab plus docetaxel and has become the standard [22]. In addition, the prescription of trastuzumab emtansine (TDM-1) for those patients not achieving a pCR, has increased survival to 89.7% compared to 83% in the adjuvant trastuzumab with a HR 0.60 (95% CI 0.45-0.79) [6]. In our series Her2 positive patients presented a 5yDDFS of 85.4% those with RRHH positive and 87% those with RRHH negative, similar to the Neosphere study rates. Importantly survival rates in Her2 positive patients depended extremely on response to NACT with a 5yDDFS of 95% for those patients who achieved a pCR compared to 50% in those patients with RCB III. Fortunately, Her2 positive patients with a RCB III were only a 15% of the cases. However are those HER2 cases that deserve more research.
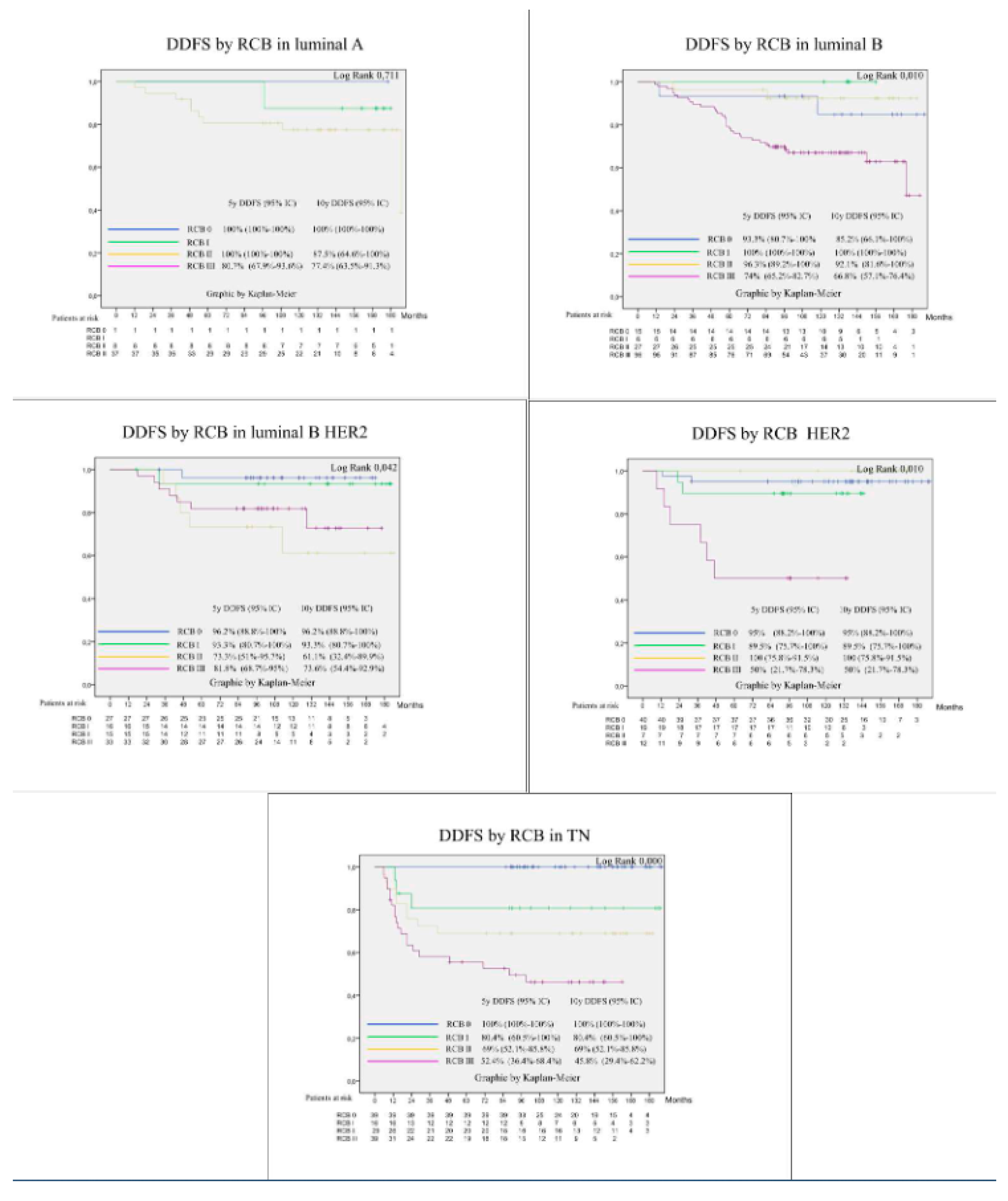
For TNBC the therapeutical arsenal has also improved pCR and survival thanks to the introduction of platins [23,24] and immunocheck point inhibitors [18]. The addition of platins improved pCR up to 50% [25] and the addition of pembrolizumab has raised pCR up to 65%, nearly 70% in PDL1 positive tumors [18]. Survival has increased in accordance with the addition of platins as was set in the BrighTNess study that published a 4y DFS of 79.3% in the carboplatin arm compared to 68.5% without carboplatin. HR 0.57 (0.36-0.91) [26]. Survival data in the Keynote 522 showed also a survival advantage for the arm with pembrolizumab with a HR 0.63 (95%CI 0.43-0.93). In our study the pCR rate in TNBC is low compared to the new standard of care for TNBC with a 31.7% comparable to the schemas without platins nor immunecheckpoint inhibitors. However, the message of the present paper about the relevant prognostic information about response to NACT is shown equally with our data. In our series the 5yDDFS for TNBC was 74.1% (95%CI 66.3-82) with great differences according to the different degree of response with those patients achieving pCR presenting an excellent survival at 5 and 10 years of 100%, whereas in RCB 1 the 5yDDFS dropped to 80.6%, in RCB II to 69% and in RCB III lower than 50%, log rank 0.000. This data shows the imminent need to improve pCR in TNBC with new approaches such as the addition of platins, the use of immunotherapy and the approval of PARP inhibitors for BRCA carriers [27].
In luminal patients, NACT is not probably their best option, however those trials comparing chemotherapy with new approaches such as the combination of hormonal therapy with CDK 4/6 inhibitors have not obtained better chances of pCR rates and were not designed to find differences in survival [28,29,30]. A different landscape has been recently opened in the adjuvant setting where adjuvant abemaciclib for two years [19] and adjuvant ribociclib for three years [20] have demonstrated survival advantages in luminal patients with high and intermediate risk of relapse, respectively. In our series pCR in luminal patients were as low as 2.2% in luminal A-like tumors and 10.4% in luminal B-like tumors. Interestingly survival for luminal tumors changed significantly calculated at 5years or at 10 years. In luminal A tumors 5yDDFs was 84.6% and dropped to 79.6% at 10 years, and in luminal B tumors 5yDDFS was 81,2% and dropped to 74.7% al 10 years, as a result that distant recurrences can occur 5 years or later whereas in Her2 and TNBC recurrences usually occur within the first 5 years. On the other hand, patients with luminal tumors depend less on tumor response, as already shown by P. Cortazar [31]. In our series, luminal A tumors performed well with RCB 0-2 with 96.7% for the only patient that achieved a pCR out of 46 cases, and for the RCB III the 5yDDFS was 69.5% and 10y DDFS dropped to 62.5% . In the luminal B-like similar results with good survival rats for RCB 0-2 whereas those patients with RCB III 5yDDFS was 72% and dropped to 65% at 10y. A special mention to the scares number of lobular carcinomas included in our series that performed extremely bad in our study with a 10yDDFs of 42.9% (95%CI 16.9-68.8). A different therapeutical approach should be discovered for this special subtype of breast cancer besides chemotherapy [32].
Those factors independently related to patient survival taking as end point the DDFS as a surrogate of fatal outcome and with more events than breast cancer deaths, were the pathologic subtype, the molecular surrogated subtype, response to chemotherapy and vascular invasion. Lobular carcinomas presented a HR of 4 related to ductal carcinomas; HER-2 presented a HR of 3.3 and TNBC 4.2 in reference to luminal A tumors, probably a expenses to those tumors without response; according to RCB HR were 2.5, 5.1 and 9.1 for RCB I, II and III in comparison to RCB 0, and finally those patients that presented vascular invasion in the surgical specimen presented a HR 2.33 in comparison with those patients without vascular invasion. The 10yDDFS for those patients without vascular invasion was 83.6% vs. 59.2% for patients with vascular invasion. The clinically and statistical significance of vascular invasion in patient survival deserves a special place in prognostic scores that could improve actual neoadjuvant prognostic index.
In conclusion, response to NACT plays a crucial role in assessing long-term patient prognosis. The important message to patients and clinicians for well informed decision making is that initial poor prognosis such as triple negative molecular subtype can be improved to an excellent prognosis is pCR is achieved as it has been demonstrated in the present data.
Some limitation must be declared mainly the condition of a retrospective study based on chemotherapeutic regimens that have been surpassed nowadays and with a relatively small number of cases when divided by molecular surrogated subtypes, an. However, it is the condition of a series with a long follow-up to be outdated in the chemotherapeutic schemas.
Despite the mentioned limitations, we hope our data can help clinicians to better discuss with their patients the benefits of primary chemotherapy, giving a special emphasis in the prognostic value of response to neoadjuvant chemotherapy.
Acknowledgments
to all the patients and their families. To my mentors Dr A. Escobedo and A. Moreno (deceased) and to Dr. Pera for technical assistance. Finally to Michael Maudsley, MSc, for language revision.
Ethical Approval
The local ethical committee approved this paper for publication with the register number PR269/20.
Table of Abbreviations
| NATC | Neoadjuvant chemotherapy |
| pCR | Pathological complete response |
| NRI | Neoadjuvant response index |
| RCB | Residual cancer burden |
| TNBC | Triple negative breast cancer |
| AJCC | American Joint Committee on Cancer |
| ASCO | American Society of Clinical Oncology |
| cN0 | Clinical N0 |
| N+ | Node positive |
| RT | Radiotherapy |
| BMI | Body mass index |
| TILs | Tumor infiltrating lymphocytes |
| DFS | disease free survival |
| DDFS | Distant disease-free survival |
| OS | Overall survival |
| BCSS | Breast cancer specific survival |
| SD | Standard deviation |
| CI | Confidence intervals |
| HR | Hazard ratio |
References
- Bonadonna G, Veronesi U B et al. J Natl Cancer Inst. J Natl Cancer Inst. 1990;82:1539–45.
- Wolmark N, Wang J ME et al. No Title. J Natl Cancer Inst Monogr. 2001;30:96–102.
- Goldhirsch A, Winer EP, Coates AS, Gelber RD, Piccart-Gebhart M, Thürlimann B, et al. Personalizing the treatment of women with early breast cancer: Highlights of the st gallen international expert consensus on the primary therapy of early breast Cancer 2013. Ann Oncol. 2013;24(9):2206–23. [CrossRef]
- Korde LA, Somerfield MR, Carey LA, Crews JR, Denduluri N, Shelley Hwang E, et al. Neoadjuvant Chemotherapy, Endocrine Therapy, and Targeted Therapy for Breast Cancer: ASCO Guideline. J Clin Oncol. 2021;39(13):1485–505. [CrossRef]
- Masuda N, Lee S-J, Ohtani S, Im Y-H, Lee E-S, Yokota I, et al. Adjuvant Capecitabine for Breast Cancer after Preoperative Chemotherapy. N Engl J Med. 2017;376(22):2147–59. [CrossRef]
- von Minckwitz G, Huang C-S, Mano MS, Loibl S, Mamounas EP, Untch M, et al. Trastuzumab Emtansine for Residual Invasive HER2-Positive Breast Cancer. N Engl J Med. 2019;380(7):617–28. [CrossRef]
- Curigliano G, Burstein HJ, Gnant M, Loibl S, Cameron D, Regan MM, et al. Understanding breast cancer complexity to improve patient outcomes: The St Gallen International Consensus Conference for the Primary Therapy of Individuals with Early Breast Cancer 2023. Ann Oncol. 2023;34(11):970–86. [CrossRef]
- Fernandez-Gonzalez S, Falo C, Pla MJ, Pernas S, Bajen M, Soler T, et al. The Shift From Sentinel Lymph Node Biopsy Performed Either Before or After Neoadjuvant Systemic Therapy in the Clinical Negative Nodes of Breast Cancer Patients. Results, and the Advantages and Disadvantages of Both Procedures. Clin Breast Cancer [Internet]. 2018;18(1):71–7. Available from:. [CrossRef]
- Sheri A, Smith IE, Johnston SR, A’hern R, Nerurkar A, Jones RL, et al. Residual proliferative cancer burden to predict long-term outcome following neoadjuvant chemotherapy. Ann Oncol. 2015;26(1):75–80.
- Whelan TJ, Olivotto IA, Parulekar WR, Ackerman I, Chua BH, Nabid A, et al. Regional Nodal Irradiation in Early-Stage Breast Cancer. N Engl J Med. 2015;373(4):307–16. [CrossRef]
- Poortmans PM, Collette S, Kirkove C, Van Limbergen E, Budach V, Struikmans H, et al. Internal Mammary and Medial Supraclavicular Irradiation in Breast Cancer. N Engl J Med. 2015;373(4):317–27.
- Salgado R, Denkert C, Demaria S, Sirtaine N, Klauschen F, Pruneri G, et al. The evaluation of tumor-infiltrating lymphocytes (TILS) in breast cancer: Recommendations by an International TILS Working Group 2014. Ann Oncol. 2015;26(2):259–71. [CrossRef]
- Gourgou-Bourgade S, Cameron D, Poortmans P, Asselain B, Azria D, Cardoso F, et al. Guidelines for time-to-event end point definitions in breast cancer trials: Results of the DATECAN initiative (Definition for the Assessment of Time-to-event Endpoints in CANcer trials). Ann Oncol [Internet]. 2015;26(5):873–9. Available from:. [CrossRef]
- Asselain B, Barlow W, Bartlett J, Bergh J, Bergsten-Nordström E, Bliss J, et al. Long-term outcomes for neoadjuvant versus adjuvant chemotherapy in early breast cancer: meta-analysis of individual patient data from ten randomised trials. Lancet Oncol. 2018;19(1):27–39. [CrossRef]
- Falo C, Moreno A, Benito E, Lloveras B, Varela M, Serra JM, et al. Primary chemotherapy with cyclophosphamide, methotrexate, and 5-fluorouracil in operable breast carcinoma. Cancer. 2005;103(4):657–63.
- Fasching PA, Hartkopf AD, Gass P, Häberle L, Akpolat-Basci L, Hein A, et al. Efficacy of neoadjuvant pertuzumab in addition to chemotherapy and trastuzumab in routine clinical treatment of patients with primary breast cancer: a multicentric analysis. Breast Cancer Res Treat [Internet]. 2019;173(2):319–28. Available from: . [CrossRef]
- Poggio F, Bruzzone M, Ceppi M, Pondé NF, La Valle G, Del Mastro L, et al. Platinum-based neoadjuvant chemotherapy in triple-negative breast cancer: A systematic review and meta-analysis. Ann Oncol. 2018;29(7):1497–508. [CrossRef]
- Schmid P, Cortes J, Pusztai L, McArthur H, Kümmel S, Bergh J, et al. Pembrolizumab for Early Triple-Negative Breast Cancer. N Engl J Med. 2020;382(9):810–21. [CrossRef]
- Johnston SRD, Toi M, O’Shaughnessy J, Rastogi P, Campone M, Neven P, et al. Abemaciclib plus endocrine therapy for hormone receptor-positive, HER2-negative, node-positive, high-risk early breast cancer (monarchE): results from a preplanned interim analysis of a randomised, open-label, phase 3 trial. Lancet Oncol. 2023;24(1):77–90. [CrossRef]
- Slamon D, Lipatov O, Nowecki Z, McAndrew N, Kukielka-Budny B, Stroyakovskiy D, et al. Ribociclib plus Endocrine Therapy in Early Breast Cancer. N Engl J Med. 2024;390(12):1080–91. [CrossRef]
- Buzdar AU, Ibrahim NK, Francis D, Booser DJ, Thomas ES, Theriault RL, et al. Significantly higher pathologic complete remission rate after neoadjuvant therapy with trastuzumab, paclitaxel, and epirubicin chemotherapy: Results of a randomized trial in human epidermal growth factor receptor 2-positive operable breast cancer. J Clin Oncol. 2005;23(16):3676–85.
- Gianni L, Pienkowski T, Im YH, Roman L, Tseng LM, Liu MC, et al. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): A randomised multicentre, open-label, phase 2 trial. Lancet Oncol [Internet]. 2012;13(1):25–32. Available from:. [CrossRef]
- Loibl S, O’Shaughnessy J, Untch M, Sikov WM, Rugo HS, McKee MD, et al. Addition of the PARP inhibitor veliparib plus carboplatin or carboplatin alone to standard neoadjuvant chemotherapy in triple-negative breast cancer (BrighTNess): a randomised, phase 3 trial. Lancet Oncol [Internet]. 2018;19(4):497–509. Available from:. [CrossRef]
- Sikov WM, Berry DA, Perou CM, Singh B, Cirrincione CT, Tolaney SM, et al. Impact of the addition of carboplatin and/or bevacizumab to neoadjuvant once-per-week paclitaxel followed by dose-dense doxorubicin and cyclophosphamide on pathologic complete response rates in stage II to III triple-negative breast cancer: CALGB 40603 (Alliance). J Clin Oncol. 2015;33(1):13–21. [CrossRef]
- Von Minckwitz G, Schneeweiss A, Loibl S, Salat C, Denkert C, Rezai M, et al. Neoadjuvant carboplatin in patients with triple-negative and HER2-positive early breast cancer (GeparSixto; GBG 66): A randomised phase 2 trial. Lancet Oncol. 2014;15(7):747–56. [CrossRef]
- Geyer CE, Sikov WM, Huober J, Rugo HS, Wolmark N, O’Shaughnessy J, et al. Long-term efficacy and safety of addition of carboplatin with or without veliparib to standard neoadjuvant chemotherapy in triple-negative breast cancer: 4-year follow-up data from BrighTNess, a randomized phase III trial. Ann Oncol [Internet]. 2022;33(4):384–94. Available from:. [CrossRef]
- Tutt ANJ, Garber JE, Kaufman B, Viale G, Fumagalli D, Rastogi P, et al. Adjuvant Olaparib for Patients with BRCA1 - or BRCA2 -Mutated Breast Cancer . N Engl J Med. 2021;384(25):2394–405. [CrossRef]
- Prat A, Saura C, Pascual T, Hernando C, Muñoz M, Paré L, et al. Ribociclib plus letrozole versus chemotherapy for postmenopausal women with hormone receptor-positive, HER2-negative, luminal B breast cancer (CORALLEEN): an open-label, multicentre, randomised, phase 2 trial. Lancet Oncol. 2020;21(1):33–43. [CrossRef]
- Johnston S, Puhalla S, Wheatley D, Ring A, Barry P, Holcombe C, et al. Randomized phase II study evaluating palbociclib in addition to letrozole as neoadjuvant therapy in estrogen receptor–positive early breast cancer: Pallet trial. J Clin Oncol. 2019;37(3):178–89. [CrossRef]
- Gil-Gil M, Alba E, Gavilá J, de la Haba-Rodríguez J, Ciruelos E, Tolosa P, et al. The role of CDK4/6 inhibitors in early breast cancer. Breast. 2021;58:160–9.
- Cortazar P, Zhang L, Untch M, Mehta K, Costantino JP, Wolmark N, et al. Pathological complete response and long-term clinical benefit in breast cancer: The CTNeoBC pooled analysis. Lancet. 2014;384(9938):164–72. [CrossRef]
- Petrelli F, Barni S. Response to neoadjuvant chemotherapy in ductal compared to lobular carcinoma of the breast: A meta-analysis of published trials including 1,764 lobular breast cancer. Breast Cancer Res Treat. 2013;142(2):227–35. [CrossRef]
Figure 1.
DFS, DDFS, BCSS and OS.
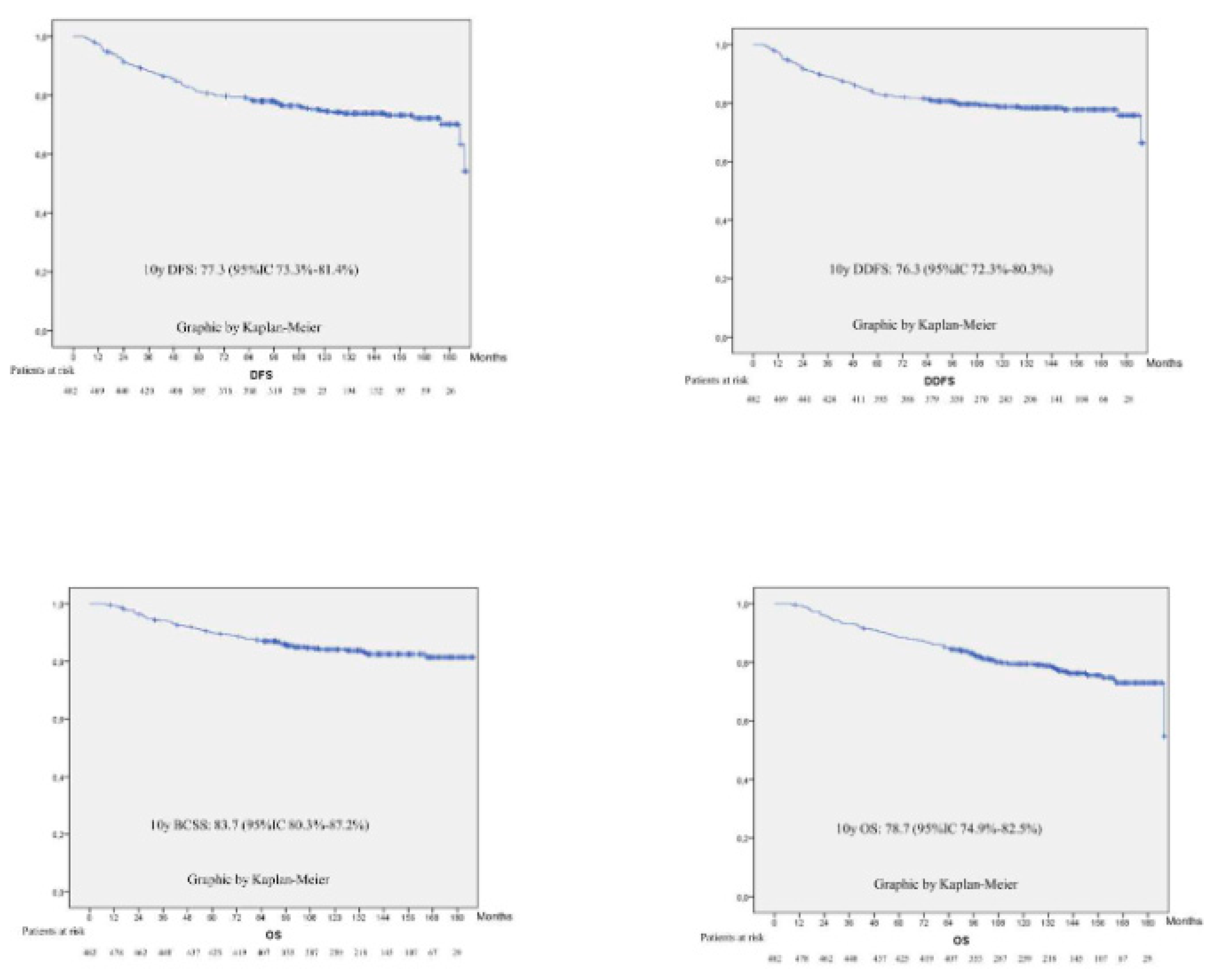
Figure 2.
Kaplan Meier curves according to basal tumour characteristics ie, anatomic. TNM, molecular TNM, histological subtype, molecular surrogated subtype and TILs cut-oƯ 20%.
Figure 2.
Kaplan Meier curves according to basal tumour characteristics ie, anatomic. TNM, molecular TNM, histological subtype, molecular surrogated subtype and TILs cut-oƯ 20%.
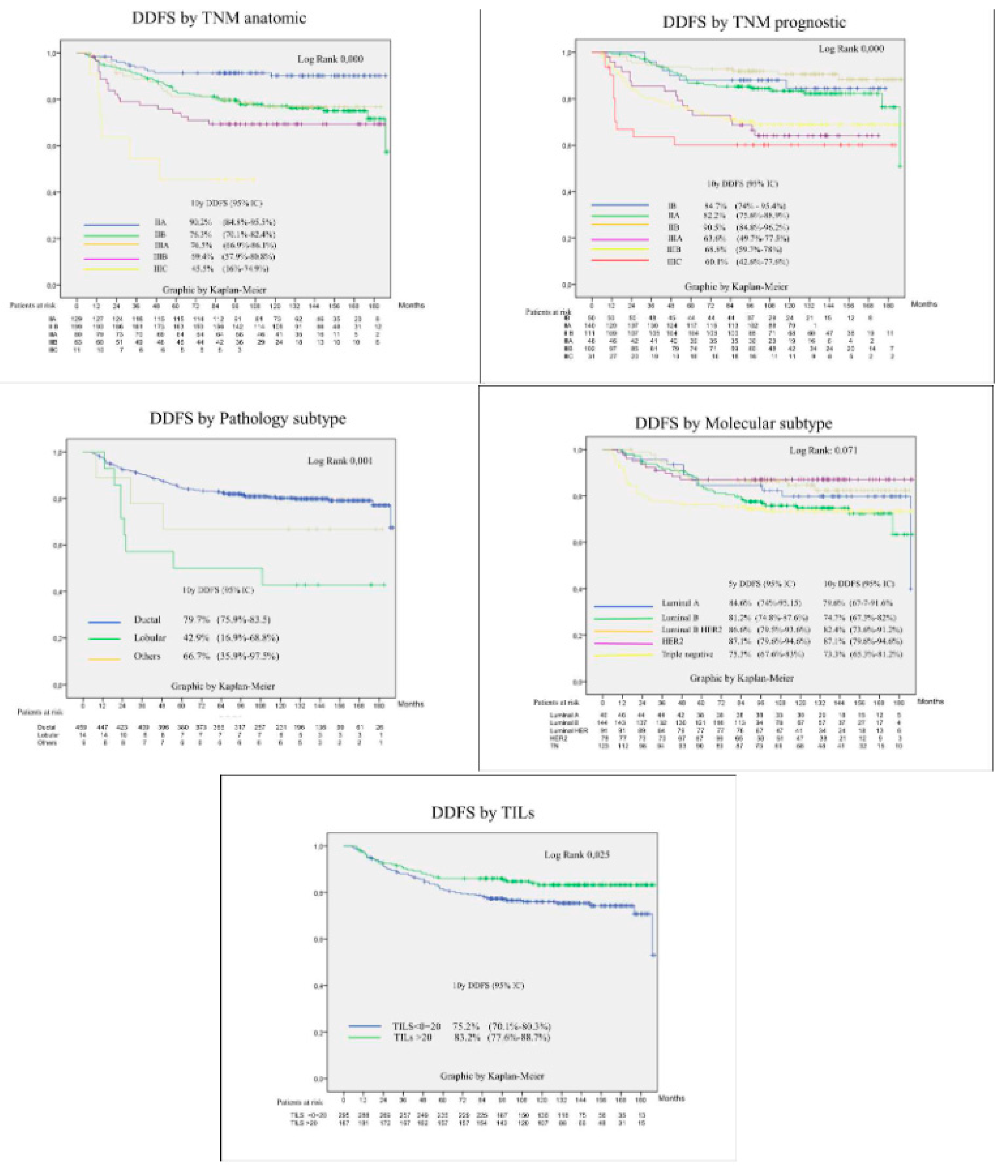
Figure 3.
Kaplan Meier curves according to pathological findings.
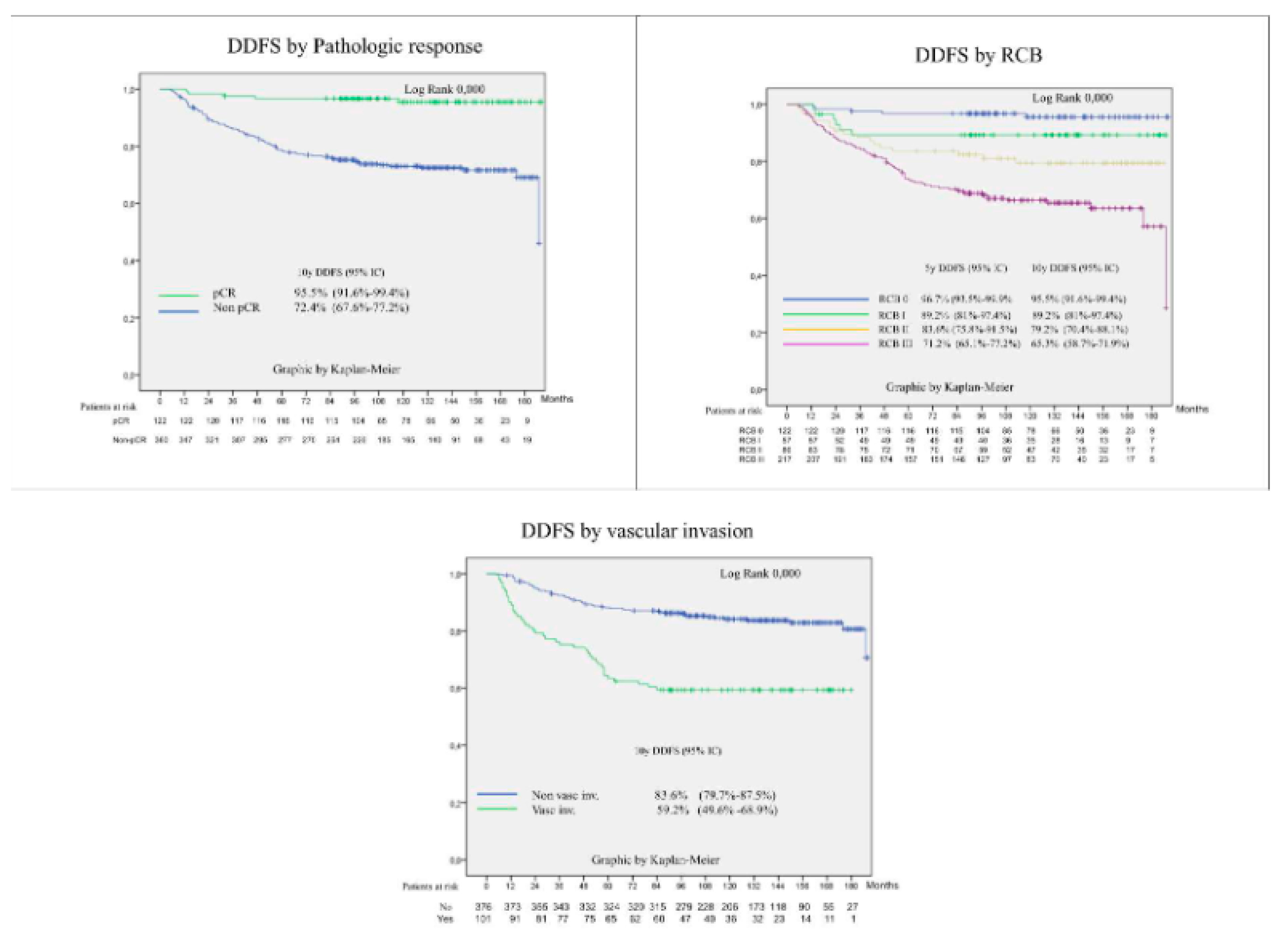
Figure 4.
Kaplan Meier curves according to RCB in each molecular surrogated subtype.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



