Submitted:
03 June 2024
Posted:
05 June 2024
You are already at the latest version
Abstract
Indocyanine Green (ICG) has significantly advanced minimally invasive surgery. It is widely recognized for its ability to visualize blood vessel patency in real-time across various surgical specialties. While its primary use in colorectal surgery is to evaluate anastomoses for leaks, nu-merous other applications have been documented in the literature.
In this review, we aim to explore both established and emerging applications of ICG fluorescence in colorectal surgery, with the goal of improving patient outcomes. This includes preoperative tumor marking and the detection of metastatic disease. Some applications, such as lymphatic mapping, require further research to determine their impact on clinical practices. Conversely, oth-ers, like the intraoperative localizations of ureters, necessitate additional procedures and are not yet widely accepted by the surgical community. However, the development of alternative com-pounds could offer better solutions. Future research should focus on areas like quantitative ICG and protocol standardization in prospective multicenter studies.
Keywords:
Indocyanine Green
; colorectal cancer
; tumor marking
; lymphatic mapping
; colorectal anastomosis
1. Introduction
The discipline of colorectal surgery has witnessed remarkable advancement in recent years. Minimally invasive techniques including laparoscopic and robotic approaches have become common and endoscopic resection of tumors have emerged as a viable option in select patients[1]. Among these advancements, Indocyanine Green (ICG) has become one of the more notable developments that changes intraoperative decision making and improves outcomes. ICG has a rich historical background in medicine. The compound was first synthesized by the Kodak Research Laboratories in 1955 and was quickly granted FDA approval in 1956 for its diagnostic utility in evaluating cardiovascular flow and hepatic function [2,3]. The initial utilization of ICG was primarily based on measurement of serum concentrations of the compound. Investigators were able to accurately predict cardiac output in the setting of various congenital cardiac anomalies [4]. Furthermore, ICG was utilized in liver function tests due to its hepatic clearance, allowing for the assessment of hepatic blood flow and liver function [5]. It was not until the 1970’s that the fluorescent properties of ICG were discovered and the field of ICG angiography was born.
ICG's ability to emit near-infrared fluorescence upon exposure to specific wavelengths of light has made it a versatile imaging agent in real-time visualization of blood flow and vessel patency. The first field to widely utilize the fluorescent properties of ICG was ophthalmology. The use of fluorescein dyes in ophthalmology has long been used to evaluate retinal vessels as it is able to be visualized in wavelengths that do not require electronic cameras [2]. The advantage of ICG is that it operates in the near-infrared wavelength (750 to 800 nm) which allows visualization of deeper lying vasculature while allowing the overlying tissues to remain translucent [6]. As our understanding of ICG’s pharmacokinetics and safety profile deepened, its application extended to various medical disciplines.
In neurosurgery, ICG angiography has been frequently used to provide real-time high spatial resolution images of cerebrovascular blood flow. Its utility has been well-documented in a variety of neurosurgical procedures including surgical treatment of cerebral aneurysms, arteriovenous malformations, and extracranial-intracranial bypass procedures [7]. Cardiac surgery has also adopted ICG to assess graft patency in coronary artery bypass graft surgery. By directly injecting ICG into the aortic root, surgeons can rapidly assess the transit of the dye through the bypass grafts to evaluate for graft patency. In a field where graft loss can have devastating consequences, ICG facilitates rapid decision making in determining the need for graft revision [8]. Plastic and reconstructive surgery has employed ICG in a similar manner to assess blood flow to pedicled and free flaps. In one prospective randomized trial, researchers determined that the intraoperative use of ICG angiography was able to accurately predict flap necrosis in patients undergoing reconstruction following mastectomy [9]. Surgical oncology and breast surgery have recently been investigating the use of ICG as an alternative method in detecting sentinel lymph nodes [10]. In a comparative study, ICG fluorescence provided acceptable sensitivity and specificity in localizing sentinel axillary lymph nodes in breast cancer compared to conventional methods. ICG also provides the advantage of transcutaneous visualization of lymphatic vessels and intraoperative lymph node detection without radioisotope [11]. After intravenous injection of ICG, the dye is selectively taken up in the liver and secreted into the bile. This property has facilitated its widespread use in the field of hepatobiliary surgery. Its various applications include intraoperative liver mapping, localization of hepatic tumors, intraoperative cholangiography, identification of extrahepatic biliary anatomy, and graft evaluation following liver transplantation [12].
In the context of colorectal surgery, the adoption of ICG fluorescence represents a promising development. The demand for enhanced intraoperative visualization in colorectal procedures, such as vascular assessments, lymphatic mapping, and identification of critical anatomical structures, has driven the exploration of ICG's utility in this surgical discipline [13]. While the historical journey of ICG has been marked by its evolution from a diagnostic tool to a therapeutic adjunct, its current and emerging roles in colorectal surgery underscore the ongoing efforts to refine surgical techniques and improve patient outcomes.
In this review, we aim to elucidate the current and emerging applications of ICG fluorescence in colorectal surgery. By examining the evolution of ICG in medicine and its integration into colorectal surgery, we seek to provide a comprehensive overview of the current state of evidence for the use of ICG in various applications in the field of colorectal surgery.
2. Properties of ICG and Description of Intraoperative Use
ICG is a tricarbocyanine dye belonging to the cyanine family and stands at the forefront of intraoperative fluorescence imaging. It offers unique properties that make it a versatile and valuable tool in colorectal surgery and across various other surgical specialties.
Given the widespread application of ICG in the clinical setting, potential adverse reactions have been extensively investigated and the compound has been found to have a favorable safety profile. The ICG injectable solution does include up to 5% sodium iodide which portends a potential risk of an allergic reaction. While these risks exist, the incidence of such reactions are exceedingly rare, even in patients with a documented allergy to iodine [2]. Several meta-analyses have reviewed the safety of ICG and all determined there to be no significant risk to the injection of the compound [14,15]. One study even found that the use of ICG was associated with decreased intraoperative blood loss [16].
ICG is generally given intravenously with a recommended dose of 0.2 to 0.5 mg/kg and a maximum dose of 5 mg/kg [17]. Upon administration, ICG rapidly binds to blood lipoproteins and remains intravascular until it is cleared by hepatic metabolism. Its swift hepatic clearance, with a half-life of 3-4 minutes, allows for real time imaging and surgical decision making, but also necessitates proper timing of administration to ensure the appropriate structures are visualized [5].
ICG possesses near-infrared absorption properties, peaking at 800 to 850 nm when exposed to 760 to 780 nm near-infrared rays [2]. There are multiple commercially-available systems that allow fluorescence visualization in robotic, laparoscopic, and open surgery. Currently, the most widely used robotic surgical system is da Vinci surgical platform (Intuitive Surgical, Sunnyvale, CA). Recognizing the importance of fluorescence imaging, manufacturers have integrated Firefly technology (Novadaq Technologies, Mississauga, ON) into their robotic endoscopes to allow intraoperative near-infrared fluorescence imaging. Both the da Vinci Si and Xi systems are equipped with vision carts that use an external LED-based light source for illumination during surgery as well as a laser source for excitation of ICG during fluorescence imaging [18]. The surgeon can rapidly switch between light sources from the robotic console. Similarly, most laparoscope manufacturers have equipped near-infrared imaging into their newer devices [19]. This integration allows surgeons to seamlessly switch to ICG fluorescence without violating the sterile field. In open surgery, multiple manufacturers have developed devices for detecting ICG fluorescence. These devices function similarly with a near-infrared light source for exciting ICG as well as an area detector for sensing the emitted fluorescent signals [20].
3. ICG in Evaluating Anastomotic Blood Supply
Anastomotic leak following bowel resection in colorectal surgery remains one of the most dreaded postoperative complications and represents a significant contributor to morbidity and mortality in this patient population. It is defined as a defect of the intestinal wall at the anastomotic site leading to communication between the intra- and extraluminal compartments [21]. The incidence of anastomotic leaks varies depending on factors such as patient comorbidities, surgical technique, and the nature of the underlying pathology. Studies have reported varying rates of anastomotic leaks in colorectal surgery. One meta-analysis found the overall incidence of anastomotic leaks to be around 4.3% after colorectal resections [22]. However, the incidence can be higher in specific procedures, such as low anterior resections, where reported rates range from 3% to 21% [23].
The implications of anastomotic leaks on patient outcomes are profound. These complications can lead to a spectrum of consequences, ranging from perianastomotic abscess to multi-system organ failure and death. Patients who experience anastomotic leaks often face prolonged hospital stays, a higher likelihood of reoperation, and an increased risk of developing chronic complications, such as fistulas or strictures [24]. Anastomotic leaks can also impact long-term functional outcomes and quality of life for colorectal surgery patients. The need for diverting ostomies to protect the anastomosis, especially in high-risk cases, adds another layer of complexity to the surgical management. The association between anastomotic leaks and adverse outcomes underscores the importance of preventive measures, including meticulous surgical technique, appropriate patient selection, and adherence to evidence-based practices.
There are a multitude of patient and technical factors that can contribute to the development of anastomotic leakage. Some of the proposed patient-centered factors that are linked to anastomotic leakage are male sex, elderly age, obesity, the presence of severe comorbidities, prolonged operative time, perioperative blood transfusions, low pelvic anastomosis, and neoadjuvant chemoradiation [25]. Technical factors that can contribute to anastomotic failure include the presence of tension on the anastomosis and the vascular supply of the segments of bowel [26]. A multitude of techniques have been described to allow the bowel to reach the anastomosis without tension [27]. As an adjunct to evaluate the vascular supply to an anastomosis, ICG fluorescence angiography has been routine employed in many surgical disciplines, especially colorectal surgery (Figure 1).
Several studies have investigated the role of ICG fluorescence imaging in reducing anastomotic leaks in colorectal surgery. The PILLAR II study (Perfusion assessment in laparoscopic left-sided/anterior resection) evaluated anastomotic leak rates in patients undergoing left-sided colectomy and low anterior resection for which ICG was used to assess anastomotic blood supply. Investigators reported an overall leak rate of 1.4% when ICG was employed. Interestingly, ICG influenced surgical plans in 8% of patients, and no leaks occurred among patients who had a change in surgical plan based on intraoperative perfusion assessment with ICG fluorescence [28]. In a multicenter phase II trial of near-infrared imaging in elective colorectal surgery, there was found to be a statistically significant decrease in anastomotic leak in cases where ICG was utilized (2.6%) compared with cases where it was not (5.8%) [29]. Notably, this reduction in leak rate was statistically significant for left-sided resections and low anterior resections but not for right-sided operations.
A comprehensive systematic review by the European Association for Endoscopic Surgery (EAES) in 2023 studied the use of ICG in colorectal surgery and revealed a significant correlation between ICG use and reduced leak rates, particularly in the rectum (RR=0.32, p<0.01). Furthermore, the injection of ICG influenced surgical decision-making, leading to changes in the anastomotic line in 10.3% of patients. The overall postoperative complications were reduced (RR=0.67, p<0.01), and there was a decrease in postoperative length of stay (MD − 0.67, IC 95%: − 1.06 − 0.27, p < 0.01). Additionally, a lower percentage of patients who underwent ICG-guided surgery required protective stomas (44%) compared to the control group (54%) (p=0.45) [30]. In another systematic review of randomized controlled trials and propensity-score matched studies, the use of ICG reduced the incidence of anastomotic leak (odds ratio 0.46, 95% CI, 0.36, 0.59) and length of stay (mean difference -1.21, 95% CI, -2.06, -0.35). However, ICG use did not influence the incidence of overall post-operative complications, reoperation rate, or mortality (31).
The collective body of evidence suggests that the integration of ICG fluorescence into colorectal surgery holds substantial promise for enhancing patient outcomes by minimizing the risk of anastomotic leaks and optimizing surgical decision-making. Further research and continued clinical adoption of ICG-guided techniques are warranted to fully realize the potential impact of ICG fluorescence on improving patient outcomes in colorectal surgery.
4. ICG for Lymphatic Mapping in Colorectal Surgery
It is well established that the number and location of involved lymph nodes in colon and rectal cancer are significant prognostic factors and guide therapy following resection. As such, lymphadenectomy is a critical part of the oncologic resection. For colon cancer, a minimum of 12 lymph nodes are required to be included in the specimen to confidently assign a nodal or N- stage [31]. In rectal cancer, a total mesorectal excision (TME) involves complete resection of the rectum, tumor, and the associated vasculature and lymphatics. A complete TME has long been accepted as the standard oncologic resection technique in rectal cancer [32]. Based on this concept, the techniques of complete mesocolic excision (CME) with central vascular ligation (CVL) and the Japanese D3 lymphadenectomy were developed for more extensive lymph node retrieval in colon cancer [33]. Also termed “extended lymphadenectomy”, this approach involves mobilization of the colon and mesocolon within the embryologic mesocolic plane with a full regional lymph node dissection including central ligation of the supplying vessels. While extended lymphadenectomy does result in higher lymph node yields and more accurate N-staging, it is not routinely recommended by the American Society of Colon and Rectal Surgeons due to increased operative and post-operative complications [34].
More recent investigations have utilized ICG fluorescence as a means of identifying clinically significant lymph nodes outside of the standard resection field while avoiding extended lymphadenectomy. This is particularly important in cases where the tumor involves the splenic or hepatic flexures of the colon, as these anatomic areas frequently have significant variations in lymphatic drainage [35]. The use of ICG offers the possibility of directly defining the regional nodal basin allowing for a more individualized lymphadenectomy. This is accomplished by directly injecting the submucosal layer around the tumor with ICG and using fluorescence imaging to map the individual lymphatic drainage of the tumor. Several studies have sought to evaluate the optimal timing of ICG administration for lymphatic mapping. In one such investigation, fluorescence imaging 30-60 minutes following injection of ICG resulted in visualization of lymphatic drainage in 77% of cases [36].
The GREENLIGHT trial is an ongoing prospective observational trial exploring the clinical significance of ICG-guided lymphadenectomy in patients undergoing surgery for both colon and rectal cancers. In an interim analysis, the extent of lymphadenectomy was changed in 50% of patients based on ICG fluorescence, most commonly for lymph nodes that were identified outside of the standard draining basin [37]. Further investigations are required to determine if the use of ICG in targeted lymphadenectomy will affect clinical practice or other oncologic outcomes.
5. Use of ICG for Intraoperative Localization of Ureters
Iatrogenic ureteral injury (IUI) is a rare but potentially devastating complication of colorectal surgery. The incidence of IUI is estimated to be between 0.15% to 4.5% in colorectal resections [38]. Most of these injuries are not identified during the initial surgery, and they significantly contribute to patient morbidity. Many strategies have been employed by surgeons to assist in intraoperative identification of ureteral injuries. The mainstay has been preoperative or intraoperative ureteral stent placement, whether conventional or lighted. However, this method has not gained widespread acceptance due to the extra operative time and the increased use of robotics and laparoscopy, which lack tactile feedback [39,40].
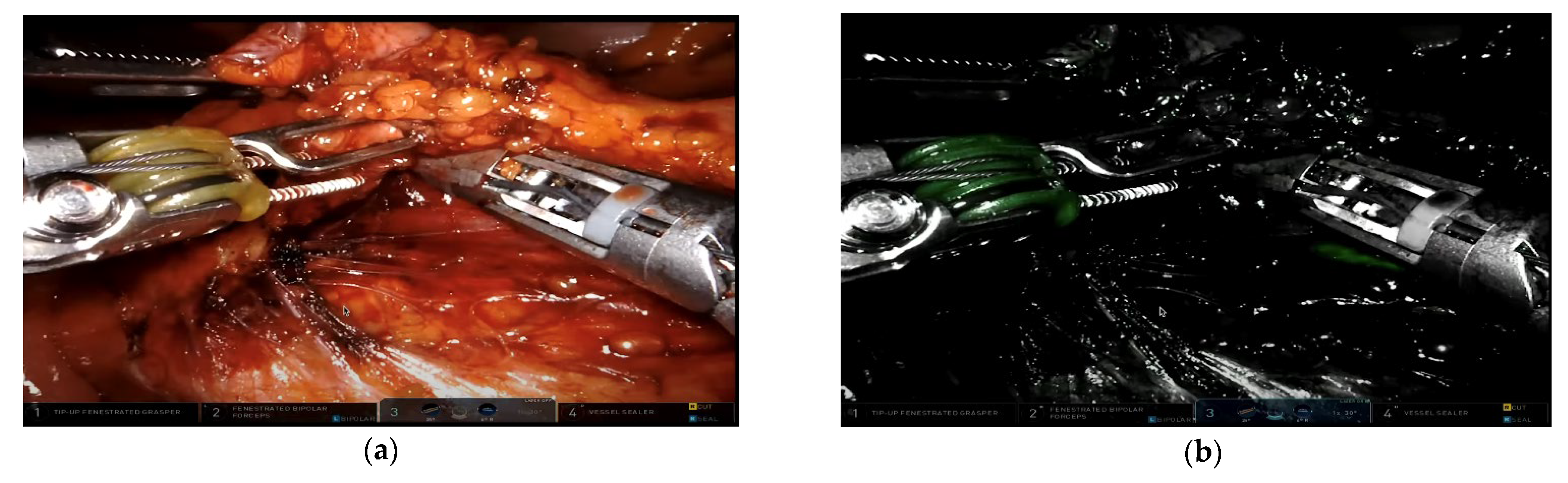
Intraureteral ICG visualization under fluorescence presents a promising alternative for preventing ureteral injury. Its application involves insertion of ureteral catheters with cystoscopy, followed by ICG injection and clamping to minimize spillage and leakage. This allows ICG to bind to the lining of the ureter, staining it and making the ureter visible for up to three hours (Figure 2) [41]. A systematic review including seven retrospective studies involving 142 patients, concluded that while the use of ICG is safe and effective in preventing IUI in minimally invasive colorectal procedures, it still necessitates ureteral catheterization and carries a potential risk for injury [42].
The United States Food and Drug Administration only approves ICG for intravenous use. However, it cannot be used intravenously for this purpose since it is metabolized and excreted through the hepatobiliary system. Other intravenous fluorescent dyes, cleared through the kidneys, are currently being studied [43]. Methylene blue is a notable example, as it has been extensively studied in humans and demonstrated a good safety profile. It exhibits a urinary excretion rate of approximately 30% after one intravenous dose. Studies have shown that ureters were visible in 93% of cases under near-infrared fluorescence and 20% under white light [44]. Other experimental dyes, such as liposomal ICG, are also under investigation. Liposomal ICG has increased renal clearance, thereby avoiding the need for intraureteral catheterization [39,45]. Fluorescent dyes are an exciting development in the prevention of IUI, particularly in patients where factors like prior surgeries, inflammatory changes, and obesity make ureter identification challenging.
6. Use of ICG for Preoperative Tumor Marking
India ink has been used for preoperative tumor marking in colorectal surgery since the late 1970s. However, its adverse effects, which include inflammatory changes and peritoneal spillage, can hinder the differentiation of anatomical structures, and obscure the surgical view [46,47].
The use of ICG for tumor marking was first described in the 1990s. Investigators successfully used ICG to mark 15 colonic lesions in 12 patients, with identification times of at least 36 hours [48]. Numerous studies have since been published describing the technique, timing, and efficacy of using ICG to identify and visualize tumors in both open and minimally invasive approaches.
There remains some debate on the optimal timing for tumor localization with ICG. One study evaluated patients who received ICG tattooing of their tumor with colonoscopy 16 to 18 hours prior to surgical resection. Investigators discovered that a 0.5 mg dose allowed tumor localization without interfering with lymph node mapping and ICG angiography. The study also highlighted the utility of ICG localization for identifying hard-to-see cancer sites, especially after mucosal resection [49]. A second study involving 165 patients undergoing laparoscopic colon resection determined that ICG could be observed between 0.125 and 2 mg doses. ICG marking was detected in all 141 patients who underwent surgery within six days of marking, but the visualization decreased to 60% between days 6-10 and to 0% after ten days [50]. A recent systematic review that included eight studies and a total of 1061 patients indicated that, when ICG tattoo injection was done within a week of surgery, the visualization rate was as high as 97%. The most significant complication was ICG spillage into the serosa, which obscured boundaries but did not affect the view in white light [51].
Preoperative ICG tattooing protocols, including dosing and timing of injection, still vary and require further research. Nonetheless, studies consistently suggest that ICG could serve as a safe alternative for marking, offering improved visualization, particularly in laparoscopic and robotic approaches.
7. ICG in Detecting Metastatic Disease in Colorectal Cancer
The liver is the most common site for metastatic disease from colorectal cancer, with approximately 25% of patients developing liver metastases at some point in their disease course [52]. Beginning in the early 2000s, more intensive surveillance programs with computed tomography led to greater detection of recurrent hepatic disease and the establishment of liver resection as the standard for potentially curative treatment [53].
Tumor-free resection margins (R0) are critical to realize the potential benefit of liver resection in metastatic colorectal cancer. Unfortunately, up to 10% of patients undergoing resection will have R1 resections (positive microscopic margin, <1mm resection margin) [54]. Near-infrared fluorescence using ICG has emerged as a promising method for detecting occult liver lesions and is often used in conjunction with intraoperative ultrasonography. When administered intravenously, ICG forms a characteristic “rim” around liver lesions by accumulating in the surrounding hepatocytes. In describing their experience using ICG with intraoperative ultrasound, one group of investigators reported that the greatest benefit of ICG was in revealing the margins of superficial lesions in real-time [55]. In fact, ICG fluorescence has been found to be particularly advantageous in detecting superficial lesions and lesions smaller than 10 mm compared with intraoperative ultrasound alone[56,57]. Furthermore, the fluorescent signal margin highlighted by ICG has been demonstrated to have high concordance with the histopathological resection margin [58].
More recently, ICG fluorescence has been explored for detecting colorectal peritoneal metastases. Peritoneal metastases occur in 10-15% of patients with colorectal cancer [59]. Currently, the only curative approach to treatment is cytoreductive surgery followed by hyperthermic intraperitoneal chemotherapy (HIPEC) [60]. A challenge is that preoperative imaging has low sensitivity for the full extent of peritoneal disease. Similarly, intra-operative assessment is limited to visual detection and palpation of the peritoneal surfaces. Unfortunately, recurrence from subclinical disease is high and is a significant cause of treatment failure. ICG fluorescence has been proposed as a means of enhancing visualization of peritoneal nodules. A systematic review of patients undergoing cytoreductive surgery for peritoneal metastasis from colorectal cancer found that intravenous administration of ICG was able to identify peritoneal carcinosis with a sensitivity of 88.2% and sensitivity of 77.8%. One limitation of this method is that mucinous tumors have poor affinity for ICG, making it a less useful tool in this patient population [61]. There has been some investigation into the quantitative measures of ICG fluorescence in discriminating metastatic lesions, however further studies are needed to validate it as an intraoperative adjunct.
8. Discussion
The use of ICG in CRS has become widely popular in recent years. Due to its favorable safety profile and the wide availability of near-infrared imaging systems (included in nearly all laparoscopic and robotic systems), there is growing interest across surgical disciplines in exploring ICG’s potential uses.
In CRS, there is the strongest evidence for the use of ICG in evaluating anastomotic blood supply, particularly for left colon and rectal anastomoses. Collectively, studies have demonstrated ICG use associated with decreased incidences of anastomotic leak, postoperative complications, and creation of stomas. Evidence also supports that use of ICG altered surgical planning and decision-making in select patients. ICG has also been utilized for lymphatic mapping for patients with colorectal cancer, however evidence on the topic is sparse. The interim analysis of the GREENLIGHT trial revealed that ICG use changed the extent of lymphadenectomy in half of all patients studied. This finding is encouraging, supporting ICG’s use as an important intra-operative aid. However, further research should focus on clinical and oncologic outcomes.
ICG has been studied as a tool for ureter visualization during colorectal surgery. ICG is administered intraureteral via ureteral catheters which are placed with cystoscopy. Since ICG is metabolized and excreted through the hepatobiliary system, visualization of ureters is not achievable with intravenous ICG use. Unfortunately, there is no safety benefit to using intraureteral ICG compared to ureteral stenting for visualization as it still requires cystoscopy. Alternatively, other fluorescent dyes that are renally cleared such as methylene blue are being studied. Liposomal ICG, a liposomal formulation that increases ICG’s renal clearance, may be a target for further research as it has been used for ureteral visualization in several animal studies to date.
For endoscopic tumor making, ICG may offer an alternative to India ink dye. There have been numerous studies describing the optimal timing and technique of injection. However, there is no consensus on the optimal timing or dosage for tumor marking and further research is warranted in this area. One benefit of ICG compared to India ink tattoo is that while excess injection of ICG may obscure tissue planes when viewed through the ICG vision cart, ICG is not visible with standard white light and will not have the same effect. For detecting liver metastases, ICG has shown utility especially for small and superficial liver lesions. However, for peritoneal metastases, detection with ICG may lack sensitivity.
Quantitative ICG is an area of opportunity for further research. Quantitative ICG has been used to quantify perfusion, estimate the optimal margins for resection of liver metastases, and detect non-mucinous peritoneal metastases. Existing evidence has shown that quantitative ICG has increased sensitivity and specificity compared to traditional ICG for non-mucinous peritoneal metastases detection.
9. Conclusions
The intra-operative use of ICG is an emerging technology in colorectal surgery. There is strong evidence to support its use in evaluating tissue perfusion. Thus, efforts may be taken to standardize technique and promote surgeon use of ICG, particularly for left-sided and low rectal anastomoses. The use of ICG for ureter visualization is not yet supported by the existing literature because it requires intraureteral administration. However, a liposomal formulation of ICG that can be administered intravenously is currently being developed and tested for ureter visualization. More work is needed to develop the techniques and evidence base around the use of ICG for lymphatic mapping, tumor marking, and detection of liver and peritoneal metastases. Overall, ICG is an important tool in colorectal surgery and should continue to be studied to achieve its maximal utility for improving patient outcomes.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure S1: title; Table S1: title; Video S1: title.
Author Contributions
Conceptualization, S.K. and V.H.; Investigation, S.K., C.F.B., and A.R.; Project administration, V.H.; Supervision, V.H.; Visualization, S.K.; Writing – original draft, S.K., C.F.B., and A.R.; Writing – review & editing, S.K., C.F.B., A.R., and V.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Mark Soliman M.D. for providing permission to use intraoperative images published in this paper.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Shinji, S., T. Yamada, A. Matsuda, H. Sonoda, R. Ohta, T. Iwai, K. Takeda, K. Yonaga, Y. Masuda, and H. Yoshida. "Recent Advances in the Treatment of Colorectal Cancer: A Review." J Nippon Med Sch 89, no. 3 (2022): 246-54. [CrossRef]
- Alander, J. T., I. Kaartinen, A. Laakso, T. Patila, T. Spillmann, V. V. Tuchin, M. Venermo, and P. Valisuo. "A Review of Indocyanine Green Fluorescent Imaging in Surgery." Int J Biomed Imaging 2012 (2012): 940585.
- Teng, C. W., V. Huang, G. R. Arguelles, C. Zhou, S. S. Cho, S. Harmsen, and J. Y. K. Lee. "Applications of Indocyanine Green in Brain Tumor Surgery: Review of Clinical Evidence and Emerging Technologies." Neurosurg Focus 50, no. 1 (2021): E4. [CrossRef]
- Burchell, H. B. "Assessment of Clinical Value: Symposium on Diagnostic Applications of Indicator-Dilution Technics." Proc Staff Meet Mayo Clin 32, no. 19 (1957): 551-3.
- Frangioni, J. V. "In Vivo near-Infrared Fluorescence Imaging." Curr Opin Chem Biol 7, no. 5 (2003): 626-34.
- Hochheimer, B. F. "Angiography of the Retina with Indocyanine Green." Arch Ophthalmol 86, no. 5 (1971): 564-5.
- Balamurugan, S., A. Agrawal, Y. Kato, and H. Sano. "Intra Operative Indocyanine Green Video-Angiography in Cerebrovascular Surgery: An Overview with Review of Literature." Asian J Neurosurg 6, no. 2 (2011): 88-93.
- Said, S. M., G. Marey, and G. Hiremath. "Intraoperative Fluorescence with Indocyanine Green in Congenital Cardiac Surgery: Potential Applications of a Novel Technology." JTCVS Tech 8 (2021): 144-55. [CrossRef]
- Munabi, N. C., O. B. Olorunnipa, D. Goltsman, C. H. Rohde, and J. A. Ascherman. "The Ability of Intra-Operative Perfusion Mapping with Laser-Assisted Indocyanine Green Angiography to Predict Mastectomy Flap Necrosis in Breast Reconstruction: A Prospective Trial." J Plast Reconstr Aesthet Surg 67, no. 4 (2014): 449-55.
- Jinno, H., T. Ikeda, A. Matsui, Y. Kitagawa, M. Kitajima, H. Fujii, K. Nakamura, and A. Kubo. "Sentinel Lymph Node Biopsy in Breast Cancer Using Technetium-99m Tin Colloids of Different Sizes." Biomed Pharmacother 56 Suppl 1 (2002): 213s-16s.
- Hirche, C., D. Murawa, Z. Mohr, S. Kneif, and M. Hunerbein. "Icg Fluorescence-Guided Sentinel Node Biopsy for Axillary Nodal Staging in Breast Cancer." Breast Cancer Res Treat 121, no. 2 (2010): 373-8.
- Majlesara, A., M. Golriz, M. Hafezi, A. Saffari, E. Stenau, L. Maier-Hein, B. P. Muller-Stich, and A. Mehrabi. "Indocyanine Green Fluorescence Imaging in Hepatobiliary Surgery." Photodiagnosis Photodyn Ther 17 (2017): 208-15.
- Boni, L., G. David, A. Mangano, G. Dionigi, S. Rausei, S. Spampatti, E. Cassinotti, and A. Fingerhut. "Clinical Applications of Indocyanine Green (Icg) Enhanced Fluorescence in Laparoscopic Surgery." Surg Endosc 29, no. 7 (2015): 2046-55.
- Safiejko, K., R. Tarkowski, T. P. Kozlowski, M. Koselak, M. Jachimiuk, A. Tarasik, M. Pruc, J. Smereka, and L. Szarpak. "Safety and Efficacy of Indocyanine Green in Colorectal Cancer Surgery: A Systematic Review and Meta-Analysis of 11,047 Patients." Cancers (Basel) 14, no. 4 (2022).
- Breuking, E. A., O. C. van Varsseveld, M. Harms, Shaj Tytgat, J. B. F. Hulscher, and J. Ruiterkamp. "Safety and Feasibility of Indocyanine Green Fluorescence Angiography in Pediatric Gastrointestinal Surgery: A Systematic Review." J Pediatr Surg 58, no. 8 (2023): 1534-42.
- Deng, C., Z. Zhang, H. Qi, Z. Guo, Y. Liu, H. Xiao, and X. Li. "Safety and Efficacy of Indocyanine Green near-Infrared Fluorescent Imaging-Guided Lymph Nodes Dissection During Radical Gastrectomy for Gastric Cancer: A Systematic Review and Meta-Analysis." Front Oncol 12 (2022): 917541. [CrossRef]
- Raabe, A., J. Beck, R. Gerlach, M. Zimmermann, and V. Seifert. "Near-Infrared Indocyanine Green Video Angiography: A New Method for Intraoperative Assessment of Vascular Flow." Neurosurgery 52, no. 1 (2003): 132-9; discussion 39.
- Meershoek, P., G. H. KleinJan, D. M. van Willigen, K. P. Bauwens, S. J. Spa, F. van Beurden, E. J. van Gennep, A. M. Mottrie, H. G. van der Poel, T. Buckle, F. W. B. van Leeuwen, and M. N. van Oosterom. "Multi-Wavelength Fluorescence Imaging with a Da Vinci Firefly-a Technical Look Behind the Scenes." J Robot Surg 15, no. 5 (2021): 751-60.
- Zhang, Y., J. Yan, and L. Gu. "[Development Review of Novel Laparoscope Technology]." Zhongguo Yi Liao Qi Xie Za Zhi 43, no. 3 (2019): 183-87.
- Zhu, B., and E. M. Sevick-Muraca. "A Review of Performance of near-Infrared Fluorescence Imaging Devices Used in Clinical Studies." Br J Radiol 88, no. 1045 (2015): 20140547.
- Rahbari, N. N., J. Weitz, W. Hohenberger, R. J. Heald, B. Moran, A. Ulrich, T. Holm, W. D. Wong, E. Tiret, Y. Moriya, S. Laurberg, M. den Dulk, C. van de Velde, and M. W. Buchler. "Definition and Grading of Anastomotic Leakage Following Anterior Resection of the Rectum: A Proposal by the International Study Group of Rectal Cancer." Surgery 147, no. 3 (2010): 339-51.
- Bruce, J., Z. H. Krukowski, G. Al-Khairy, E. M. Russell, and K. G. Park. "Systematic Review of the Definition and Measurement of Anastomotic Leak after Gastrointestinal Surgery." Br J Surg 88, no. 9 (2001): 1157-68.
- Hirst, N. A., J. P. Tiernan, P. A. Millner, and D. G. Jayne. "Systematic Review of Methods to Predict and Detect Anastomotic Leakage in Colorectal Surgery." Colorectal Dis 16, no. 2 (2014): 95-109.
- Gessler, B., O. Eriksson, and E. Angenete. "Diagnosis, Treatment, and Consequences of Anastomotic Leakage in Colorectal Surgery." Int J Colorectal Dis 32, no. 4 (2017): 549-56.
- Kryzauskas, M., A. Bausys, A. E. Degutyte, V. Abeciunas, E. Poskus, R. Bausys, A. Dulskas, K. Strupas, and T. Poskus. "Risk Factors for Anastomotic Leakage and Its Impact on Long-Term Survival in Left-Sided Colorectal Cancer Surgery." World J Surg Oncol 18, no. 1 (2020): 205.
- Thompson, S. K., E. Y. Chang, and B. A. Jobe. "Clinical Review: Healing in Gastrointestinal Anastomoses, Part I." Microsurgery 26, no. 3 (2006): 131-6.
- Man, J., and J. Hrabe. "Anastomotic Technique-How to Optimize Success and Minimize Leak Rates." Clin Colon Rectal Surg 34, no. 6 (2021): 371-78. [CrossRef]
- Jafari, M. D., S. D. Wexner, J. E. Martz, E. C. McLemore, D. A. Margolin, D. A. Sherwinter, S. W. Lee, A. J. Senagore, M. J. Phelan, and M. J. Stamos. "Perfusion Assessment in Laparoscopic Left-Sided/Anterior Resection (Pillar Ii): A Multi-Institutional Study." J Am Coll Surg 220, no. 1 (2015): 82-92 e1.
- Ris, F., E. Liot, N. C. Buchs, R. Kraus, G. Ismael, V. Belfontali, J. Douissard, C. Cunningham, I. Lindsey, R. Guy, O. Jones, B. George, P. Morel, N. J. Mortensen, R. Hompes, R. A. Cahill, and Voir Near-Infrared Anastomotic Perfusion Assessment Network. "Multicentre Phase Ii Trial of near-Infrared Imaging in Elective Colorectal Surgery." Br J Surg 105, no. 10 (2018): 1359-67.
- Cassinotti, E., M. Al-Taher, S. A. Antoniou, A. Arezzo, L. Baldari, L. Boni, M. A. Bonino, N. D. Bouvy, R. Brodie, T. Carus, M. Chand, M. Diana, M. M. M. Eussen, N. Francis, A. Guida, P. Gontero, C. M. Haney, M. Jansen, Y. Mintz, S. Morales-Conde, B. P. Muller-Stich, K. Nakajima, F. Nickel, M. Oderda, P. Parise, R. Rosati, M. P. Schijven, G. Silecchia, A. S. Soares, S. Urakawa, and N. Vettoretto. "European Association for Endoscopic Surgery (Eaes) Consensus on Indocyanine Green (Icg) Fluorescence-Guided Surgery." Surg Endosc 37, no. 3 (2023): 1629-48.
- (NCCN), National Comprehensive Cancer Network. "Colon Cancer Version 1.2024." https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf (accessed April 22, 2024).
- Heald, R. J. "The 'Holy Plane' of Rectal Surgery." J R Soc Med 81, no. 9 (1988): 503-8.
- Hohenberger, W., K. Weber, K. Matzel, T. Papadopoulos, and S. Merkel. "Standardized Surgery for Colonic Cancer: Complete Mesocolic Excision and Central Ligation--Technical Notes and Outcome." Colorectal Dis 11, no. 4 (2009): 354-64; discussion 64-5.
- Vogel, J. D., S. I. Felder, A. R. Bhama, A. T. Hawkins, S. J. Langenfeld, V. O. Shaffer, A. J. Thorsen, M. R. Weiser, G. J. Chang, A. L. Lightner, D. L. Feingold, and I. M. Paquette. "The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Colon Cancer." Dis Colon Rectum 65, no. 2 (2022): 148-77.
- Watanabe, J., M. Ota, Y. Suwa, A. Ishibe, H. Masui, and K. Nagahori. "Real-Time Indocyanine Green Fluorescence Imaging-Guided Complete Mesocolic Excision in Laparoscopic Flexural Colon Cancer Surgery." Dis Colon Rectum 59, no. 7 (2016): 701-5.
- Kinoshita, H., K. Kawada, Y. Itatani, R. Okamura, N. Oshima, T. Okada, K. Hida, and K. Obama. "Timing of Real-Time Indocyanine Green Fluorescence Visualization for Lymph Node Dissection During Laparoscopic Colon Cancer Surgery." Langenbecks Arch Surg 408, no. 1 (2023): 38.
- Ribero, D., F. Mento, V. Sega, D. Lo Conte, A. Mellano, and G. Spinoglio. "Icg-Guided Lymphadenectomy During Surgery for Colon and Rectal Cancer-Interim Analysis of the Greenlight Trial." Biomedicines 10, no. 3 (2022).
- Marcelissen, T. A., P. P. Den Hollander, T. R. Tuytten, and M. N. Sosef. "Incidence of Iatrogenic Ureteral Injury During Open and Laparoscopic Colorectal Surgery: A Single Center Experience and Review of the Literature." Surg Laparosc Endosc Percutan Tech 26, no. 6 (2016): 513-15. [CrossRef]
- Mahalingam, S. M., K. S. Putt, M. Srinivasarao, and P. S. Low. "Design of a near Infrared Fluorescent Ureter Imaging Agent for Prevention of Ureter Damage During Abdominal Surgeries." Molecules 26, no. 12 (2021).
- Barnes, T. G., R. Hompes, J. Birks, N. J. Mortensen, O. Jones, I. Lindsey, R. Guy, B. George, C. Cunningham, and T. M. Yeung. "Methylene Blue Fluorescence of the Ureter During Colorectal Surgery." Surg Endosc 32, no. 9 (2018): 4036-43.
- Grosek, J., and A. Tomazic. "Key Clinical Applications for Indocyanine Green Fluorescence Imaging in Minimally Invasive Colorectal Surgery." J Minim Access Surg 16, no. 4 (2020): 308-14.
- Garoufalia, Zoe, and Steven D. Wexner. "Ureter Identification Utilizing Indocyanine Green (Icg) Imaging in Colorectal Surgery: A Systematic Review of the Literature." Mini-invasive Surgery 6 (2022): 51.
- Peltrini, R., M. Podda, S. Castiglioni, M. M. Di Nuzzo, M. D'Ambra, R. Lionetti, M. Sodo, G. Luglio, F. Mucilli, S. Di Saverio, U. Bracale, and F. Corcione. "Intraoperative Use of Indocyanine Green Fluorescence Imaging in Rectal Cancer Surgery: The State of the Art." World J Gastroenterol 27, no. 38 (2021): 6374-86.
- Zocola, E., J. Meyer, N. Christou, E. Liot, C. Toso, N. C. Buchs, and F. Ris. "Role of near-Infrared Fluorescence in Colorectal Surgery." World J Gastroenterol 27, no. 31 (2021): 5189-200.
- Garoufalia, Z., and S. D. Wexner. "Indocyanine Green Fluorescence Guided Surgery in Colorectal Surgery." J Clin Med 12, no. 2 (2023).
- Miyoshi, N., M. Ohue, S. Noura, M. Yano, Y. Sasaki, K. Kishi, T. Yamada, I. Miyashiro, H. Ohigashi, H. Iishi, O. Ishikawa, and S. Imaoka. "Surgical Usefulness of Indocyanine Green as an Alternative to India Ink for Endoscopic Marking." Surg Endosc 23, no. 2 (2009): 347-51.
- Sparks, R., S. Power, E. Kearns, A. Clarke, H. M. Mohan, A. Brannigan, J. Mulsow, C. Shields, and R. A. Cahill. "Fallibility of Tattooing Colonic Neoplasia Ahead of Laparoscopic Resection: A Retrospective Cohort Study." Ann R Coll Surg Engl 105, no. 2 (2023): 126-31.
- Hammond, D. C., F. R. Lane, J. M. Mackeigan, and W. J. Passinault. "Endoscopic Tattooing of the Colon: Clinical Experience." Am Surg 59, no. 3 (1993): 205-10.
- Son, G. M., H. M. Ahn, I. Y. Lee, and G. W. Ha. "Multifunctional Indocyanine Green Applications for Fluorescence-Guided Laparoscopic Colorectal Surgery." Ann Coloproctol 37, no. 3 (2021): 133-40.
- Satoyoshi, T., K. Okita, M. Ishii, A. Hamabe, A. Usui, E. Akizuki, K. Okuya, T. Nishidate, H. Yamano, H. Nakase, and I. Takemasa. "Timing of Indocyanine Green Injection Prior to Laparoscopic Colorectal Surgery for Tumor Localization: A Prospective Case Series." Surg Endosc 35, no. 2 (2021): 763-69.
- Allan, R. N., P. Pease, and J. P. Ibbotson. "Clustering of Crohn's Disease in a Cotswold Village." Q J Med 59, no. 229 (1986): 473-8.
- Engstrand, J., H. Nilsson, C. Stromberg, E. Jonas, and J. Freedman. "Colorectal Cancer Liver Metastases - a Population-Based Study on Incidence, Management and Survival." BMC Cancer 18, no. 1 (2018): 78.
- Fong, Y., A. M. Cohen, J. G. Fortner, W. E. Enker, A. D. Turnbull, D. G. Coit, A. M. Marrero, M. Prasad, L. H. Blumgart, and M. F. Brennan. "Liver Resection for Colorectal Metastases." J Clin Oncol 15, no. 3 (1997): 938-46.
- Fong, Y., J. Fortner, R. L. Sun, M. F. Brennan, and L. H. Blumgart. "Clinical Score for Predicting Recurrence after Hepatic Resection for Metastatic Colorectal Cancer: Analysis of 1001 Consecutive Cases." Ann Surg 230, no. 3 (1999): 309-18; discussion 18-21.
- Takahashi, H., N. Zaidi, and E. Berber. "An Initial Report on the Intraoperative Use of Indocyanine Green Fluorescence Imaging in the Surgical Management of Liver Tumorss." J Surg Oncol 114, no. 5 (2016): 625-29.
- Jones, A. D., and J. C. Wilton. "Can Intra-Operative Fluorescence Play a Significant Role in Hepatobiliary Surgery?" Eur J Surg Oncol 43, no. 9 (2017): 1622-27.
- Numata, K., M. Morimoto, T. Ogura, K. Sugimori, S. Takebayashi, M. Okada, and K. Tanaka. "Ablation Therapy Guided by Contrast-Enhanced Sonography with Sonazoid for Hepatocellular Carcinoma Lesions Not Detected by Conventional Sonography." J Ultrasound Med 27, no. 3 (2008): 395-406.
- Achterberg, F. B., B. G. Sibinga Mulder, R. P. J. Meijer, B. A. Bonsing, H. H. Hartgrink, J. S. D. Mieog, A. Zlitni, S. M. Park, A. Farina Sarasqueta, A. L. Vahrmeijer, and R. J. Swijnenburg. "Real-Time Surgical Margin Assessment Using Icg-Fluorescence During Laparoscopic and Robot-Assisted Resections of Colorectal Liver Metastases." Ann Transl Med 8, no. 21 (2020): 1448.
- Klaver, Y. L., V. E. Lemmens, S. W. Nienhuijs, M. D. Luyer, and I. H. de Hingh. "Peritoneal Carcinomatosis of Colorectal Origin: Incidence, Prognosis and Treatment Options." World J Gastroenterol 18, no. 39 (2012): 5489-94.
- Gelli, M., J. F. Huguenin, C. Cerebelli, L. Benhaim, C. Honore, D. Elias, and D. Goere. "Strategies to Prevent Peritoneal Carcinomatosis Arising from Colorectal Cancer." Future Oncol 13, no. 10 (2017): 907-18.
- Baiocchi, G. L., F. Gheza, S. Molfino, L. Arru, M. Vaira, and S. Giacopuzzi. "Indocyanine Green Fluorescence-Guided Intraoperative Detection of Peritoneal Carcinomatosis: Systematic Review." BMC Surg 20, no. 1 (2020): 158.
Figure 1.
ICG fluorescence highlighting colonic perfusion after ligation of inferior mesenteric artery during robotic low anterior resection. Imaging performed using da Vinci robotic surgical platform. (a) White light visualization rectosigmoid junction. (b) Near-infrared imaging prior to intravenous administration of ICG. (c) ICG fluorescence demonstrating perfusion change after ligation of vascular pedicle.
Figure 1.
ICG fluorescence highlighting colonic perfusion after ligation of inferior mesenteric artery during robotic low anterior resection. Imaging performed using da Vinci robotic surgical platform. (a) White light visualization rectosigmoid junction. (b) Near-infrared imaging prior to intravenous administration of ICG. (c) ICG fluorescence demonstrating perfusion change after ligation of vascular pedicle.
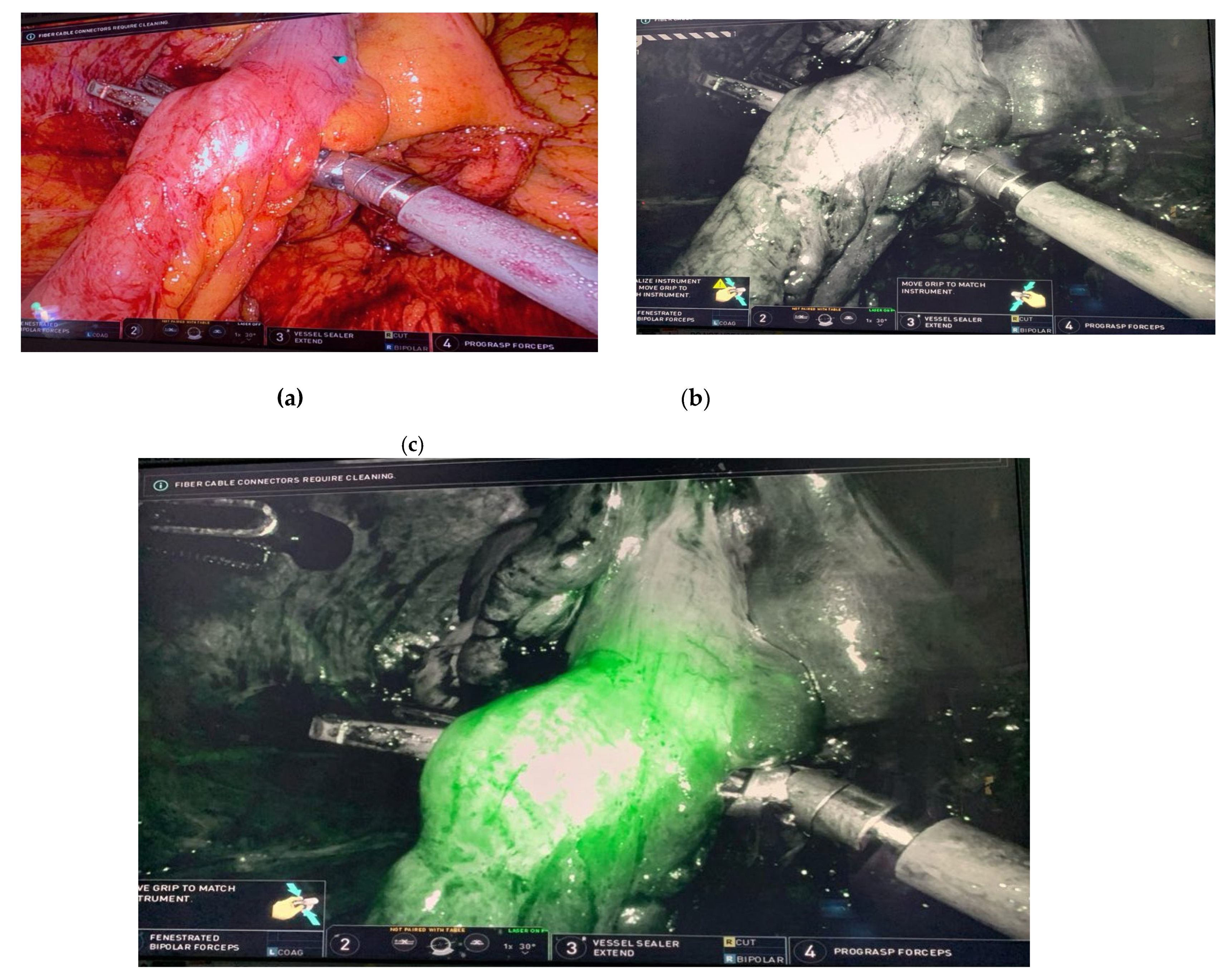
Figure 2.
Intraureteral ICG administration during medial-to-lateral dissection of sigmoid colon during robotic low anterior resection. Imaging performed using da Vinci robotic surgical platform. (a) White light visualization of left retroperitoneum with sigmoid colon and mesentery reflected anteriorly. (b) ICG fluorescence demonstrating clear identification of left ureter in the lower right portion of the image. Images provided by Dr. Mark Soliman M.D.
Figure 2.
Intraureteral ICG administration during medial-to-lateral dissection of sigmoid colon during robotic low anterior resection. Imaging performed using da Vinci robotic surgical platform. (a) White light visualization of left retroperitoneum with sigmoid colon and mesentery reflected anteriorly. (b) ICG fluorescence demonstrating clear identification of left ureter in the lower right portion of the image. Images provided by Dr. Mark Soliman M.D.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



