
Submitted:
23 May 2024
Posted:
23 May 2024
You are already at the latest version
Abstract
The Interdisciplinary Canadian Collaborative ME Research Network (ICanCME), established in 2019, aims to foster research in Canada and contribute to finding the causes and possible treatments for myalgic encephalomyelitis /chronic fatigue syndrome (ME/CFS), thereby reducing the impact of ME/CFS on the health of Canadians. The main objectives of this paper are to suggest standards for ME/CFS research for the collection of data from participants (Recommended Data Elements) and to consider other factors, such as design, language, cultural issues, equity, and diversity. Consensus of the relevant contents of this research guideline was reached during the ICanCME working group meetings and were based on existing guidelines. Members of the working group contributed to guideline development based on their respective expertise. The proposed research guidelines could improve research quality and advance knowledge in the field of ME/CFS, and ultimately benefit ME/CFS patients.
Keywords:
myalgic encephalomyelitis or chronic fatigue syndrome (ME/CFS)
; research guidelines
; standardization of data collection
; Canadian
Introduction
ME/CFS is a complex, chronic, and multi-system disease characterized by disabling fatigue that lasts more than 6 months, characterized by intolerance to efforts, post-exertional malaise, and unrefreshing sleep [1]. Other symptoms include orthostatic intolerance, cognitive difficulties, and pain, including headaches, muscle and joint pain [2]. The etiology of ME/CFS is not fully understood, however determination is multi-causal, like in other chronic diseases. Viral infection has been shown to be the strongest risk factor for disease incidence [3,4]. ME/CFS affects all age, ethnicity, and socio-economic groups, however, at least two thirds of the affected people are women [5].
The prevalence of ME/CFS varies with estimates affected by factors such as how research methods, case ascertainment and definitions are applied, setting (e.g. primary care or population based) and geographical area. For example, data for 3 regions of England, based on primary care data yielded minimal prevalence rates of 0.1% – 0.2% , with a corresponding incidence rate of 0.015 new cases per 1000-year [6]. In Canada, there are no population based prevalence rates available, but survey data from 2017 suggested the prevalence of self-reported physician diagnosed ME/CFS as around 1.5%, or 561,500 people [7]. According to the 2015-2016 Canadian Health Survey on Seniors, 3.0% of women and 1.5% of men aged over 65 years old reported a diagnosis of ME/CFS, [7].
While the first epidemiological study on ME/CFS was conducted in 1930s [8], early research on ME/CFS was limited, but has been increasing since the 1990s, and the number of articles published in PubMed, as filtered through the term “myalgic encephalomyelitis chronic fatigue syndrome and/or ME/CFS” has increased considerably, 380 in 2010, 499 in 2020, then since 2021 with over 600 articles published yearly (https://pubmed.ncbi.nlm.nih.gov/?term=myalgic+encephalomyelitis+chronic+fatigue+syndrome&filter=simsearch3.fft&filter=dates.2010-2022) [9].
While the amount of research on ME/CFS has been increasing in the last decade, there are still gaps in our basic understanding of the disease. ME/CFS presents unique challenges to researchers and patients. For example, First, while ME/CFS carries a high disease burden, there are no specific biomarkers for diagnostic confirmation, no clinically approved treatments, or permanent cure [10]. Moreover, symptoms of ME/CFS largely affect activities of daily living and health-related quality of life that cause considerable burden to patients and their family members [11]. The economic burden of ME/CFS is high not only due to its chronic nature and long-term debilitating symptoms, but also has increased due to the recent significant incidence and prevalence increases resulting from the COVID-19 pandemic. The estimated 5-9 million new cases of post-acute sequalae of COVID (i.e. Long-COVID) in the United States, many of whom meet the diagnostic criteria for ME/CFS) has been suggested, in a preliminary estimate, to increase annual medical costs and lost income, with total annual economic impact of COVID-19 estimated in $140 billion to $600 billion in 2022 in that country [12].
The complexities of ME/CFS and the methodological challenges associated with its study indicate the need for a comprehensive, systematic, and integrated approach to the assessment, differential diagnosis, and research of individuals with ME/CFS. Approaches to case recognition and treatment have been reviewed recently, including through guidelines such as the NICE guidelines for the UK [13] and those from the European Network on Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (EUROMENE), which included clinicians and researchers from over 20 European countries (as of 2018) [14]. However, there is a need for recommendations on the conduct and reporting of epidemiological and clinical studies of people with ME/CFS in Canada. This could lead to better standardization and quality of research across the country.
The Interdisciplinary Canadian Collaborative ME Research Network (ICanCME) is a multidisciplinary network. ICanCME aims to create a patient-centered network building research capacity from discovery to implementation [15]. The ultimate goal of ICanCME is to find the cause(s) and possible treatments for myalgic encephalomyelitis/ chronic fatigue syndrome (ME/CFS), thereby reducing the impact of ME/CFS on the health of Canadians. The network established working groups to support its strategic pillars and research priorities. Each working group included researchers, clinicians, health professionals, patient partners and/or caregivers, and trainees. Working Group Five: Epidemiology, Data Management and Study Design (WG5) had the purpose. The outcomes of WG5 to date are the development of two recommendations: Recommended Data Elements and current paper, and Recommendations on Epidemiological Research on ME/CFS, which would benefit researchers, clinicians and patients in terms of standardizing diagnostic criteria and efficient research in ME/CFS.
Therefore, in this research guideline, we propose a conceptual framework for epidemiological research focusing on ME/CFS in Canada, including the Recommended Data Elements (RDEs) for ME/CFS studies (Table 1).
The goals of this research guideline (in line with the RDEs goals) are to:
- Disseminate standards for collection of data from participants enrolled in ME/CFS studies that is, a set of recommended data elements (RDEs).
- Consider language and cultural issues, as well as equity, diversity and concerns on inclusion criteria such as design and methods.
- Improve data quality and research on ME/CFS for benefiting patients and practitioners.
Development Process
This project was first proposed by the members of the Working Group 5 ICanCME network in 2020 (co-chairs: Nacul and Kerr). We invited group members and patients with ME/CFS to join in the development of the research guidelines, where the participants would contribute specific knowledge and viewpoints according to their specialties, areas of interest, and experience.
We did not systematically review the evidence related to case definitions or diagnostic criteria because this has been done in other studies [1,16]. Nevertheless, we did consult similar epidemiological research guidelines published by others, such as from the EUROMENE network [17]. In this guideline, we have incorporated the standardization of data elements and instruments from the RDEs developed by the ICanCME sub-group. This was a comprehensive process in which researchers, physicians and other health professionals, patients and patient carers discussed existing practices in Canada and internationally and referred to existing guidelines for data elements for ME/CFS such as the NINDS Common Data Elements of 2018 [18] and those recommended for epidemiological studies from EUROMENE [19].
Data Collection Standardization
In Canada, clinicians and researchers generally use Canadian Consensus Criteria (2003) [20], and Institute of Medicine (2015) [21] criteria for diagnosis for ME/CFS, however, variation in case definition and guidelines have been problematic, as have the way different researchers apply chosen criteria [22] . Misclassification in selecting individuals for research has been an important source of “bias” in many studies [23]. Use of case definitions with poor specificity and non-random recruitment of participants are examples of issues that are commonly encountered. Moreover, the collected data from individual researchers often have inadequate definitions and use different instruments. This often presents a challenge to compare study results, sharing their data to combine, or harmonization for large-scale analyses, which could save time and costs.
As recommended in the RDEs, four main areas of information can be gathered: a) core general information on participants, b) provisional diagnosis, c) clinical assessment, and d) symptom profiling (Figure 1). While the RDEs represent data elements recommended for all quantitative studies in ME/CFS, further relevant data can be collected by individual researchers, based on the research questions, study design, and area of interest,
- (a)
- Core General Information
Core general information consists of data related to demographic and socio-economic characteristics, and general health history of the research participants. For demographic data, RDEs recommend collecting the information of date of birth, sex at birth, gender identity, ethnicity, and marital status. Socio-economic characteristics consist of level of education, occupation and employment, family income before tax, and living conditions. These data can be collected in any database but have been specifically designed for use in the Research Electronic Data Capture (REDCap) application.
- (b)
- Provisional diagnosis
Provisional diagnosis can be determined by the responses to self- reported questionnaires (e.g. Symptoms Assessment Questionnaire). However, diagnosis confirmation will require further assessment and/or confirmation by a health professional (e.g. physician with experience in the diagnosis of ME/CFS or family physician, which is preferably done through face-to-face visits and/or online consultations), as per case definition criteria.
- (c)
- Clinical assessment and d) symptom profiling (diagnosis confirmation) (reference: MDE’s by ICanCME WG5)
For the diagnosis of ME/CFS the Institute of Medicine 2015 [21], NICE 2021 [13], and 2003 Canadian Consensus Criteria [24] were selected. These diagnostic criteria are widely recommended internationally. The working group agreed that it was necessary to help guide researchers by recommending approved diagnostic criteria for ME/CFS. Furthermore, WG5 recommends researchers be explicit in their manuscripts about the diagnostic criteria used and how they were applied.
Clinical-related information comes from standard questionnaires, such as the United Kingdom ME Biobank (UKMEB) Symptoms Assessment Questionnaire (SAQ), which facilitates diagnosis according to clinical criteria, and ideally is followed by a full clinical assessment including detailed history by a professional with experience in ME/CFS diagnosis. Symptom profiling can be based on questionnaires (self-report or proxy assisted). The SAQ is in use in British Columbia, and Ontario is planning to start using it because it enables researchers to assess if a research participant is likely to meet any of the clinical criteria prior to meeting a clinician. Additionally, the SAQ has been recommended by the EUROMENE Epidemiology Group as part of their Common Data Elements. Lastly, the instrument supports having comprehensive datasets in a single instrument. Other items recommended for assessments of ME/CFS patients included, measures of fatigue, pain, sleep disturbance, as well as recommended blood and urine tests are described in Table 1.
Sub-grouping of patients may include strata such as sex, age-group, type of onset (acute or insidious), post-infectious or otherwise, etiology if known of triggering infection, e.g. SARS-CoV-2, Epstein-Barr, etc. Disease severity can be ascertained clinically or with the help of standard questionnaires such as the Patient Phenotyping Questionnaire or an equivalent, including questionnaire short forms, e.g. Patient Phenotyping Questionnaire (PPQ-12), DePaul -Short questionnaire.
Day-to-day fluctuation in symptoms needs to be considered, as limited information on single time points may not be reliable, with substantially different results possible on a good day compared to a bad day. Symptoms may also be very different during periods of “crashes”. The need for rest before prolonged or physically demanding testing is a consideration for research participants.
Additional Considerations on ME/CFS Research
- Comorbidities and their identification in ME/CFS
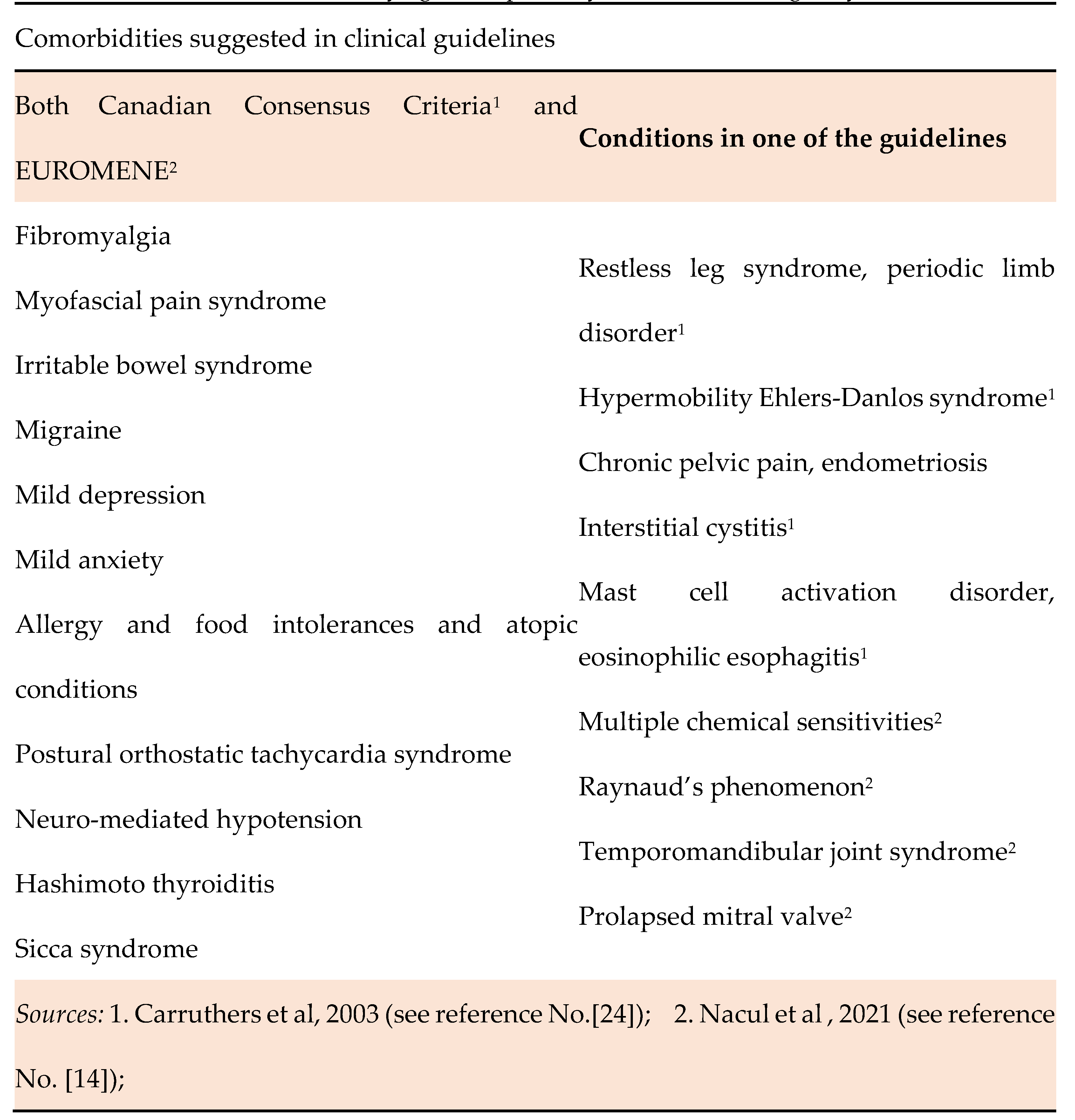
Comorbidity can play an important role in different types of research. Comorbidities are co-existing conditions can be related or unrelated to the primary disease [25]. It is also possible that the primary disease and comorbid conditions share the same risk factors or pathophysiological mechanism. Research should describe comorbid conditions as ME/CFS can be associated with various syndromes, diseases, or comorbidities such as fibromyalgia, mast cell activation, postural orthostatic tachycardia, and small fiber neuropathy [26] Table 2 summarizes examples of co-morbidities, based on suggested entities as in the European Network on Myalgic Encephalomyelitis/Chronic Fatigue Syndrome [14] and Canadian Consensus Criteria (2003) [24]. Approximately 75% of ME/CFS patients also meet criteria for fibromyalgia [27]. Castro-Marrero et al conducted a nation-wide population-based cohort study in Spain, found that 80% of patients with ME/CFS had co-morbidities, which they classified into five subgroups. Among these, pain related conditions such as fibromyalgia, myofascial pain, shoulder tendinopathy, and epicondylitis were the most prevalent comorbid conditions [28]. Moreover, the Institute of Medicine (IOM) 2015 noted that comorbid conditions can be used to stratify cases as ME/CFS + fibromyalgia; ME/CFS + postural orthostatic tachycardia syndrome; ME/CFS + depression; ME/CFS + anxiety [21]. Infections such as EBV or other herpesvirus, COVID-19, and borreliosis seem to represent important triggers of ME/CFS, however the role as comorbid condition in the form of persistent infection by these or other agents require further investigations.
According to de Groot et al., there are four important reasons for measuring comorbidity in research: 1) to be able to control for confounding factors, 2) to identify effect modification, 3) to use comorbidity as a predictor of study outcome, 4) to measure co-occurring conditions [25]. A number of co-morbidity indexes have been used in other diseases studies [25], such as the Charlson Comorbidity Index (CCI) [29], the Cumulative Illness Rating Scale [30], and the Index of Coexisting Disease [31]. However, the applicability of a comorbidity index for studies on However, the applicability of a comorbidity index for studies on ME/CFS is still an area that needs to be developed further, and which would need to consider comorbidity alongside with differential diagnosis and exclusionary conditions.
- 2.
- Long-COVID and ME/CFS
Since COVID-19 pandemic, there is increasing recognition that a significant proportion of Long-COVID cases develop a clinical presentation indistinguishable from ME/CFS [32,33]. A growing body of evidence suggests that the symptomatology of Long-COVID and ME/CFS overlap in a substantial subset of cases when ME/CFS is assessed according to multiple case definitions [32]. Long-COVID may be identified in persons with persistent symptoms following probable or confirmed SARS-CoV-2 infection, present at 3 months from the acute infection and which cannot be explained by an alternative diagnosis [34]. Long-COVID is characterized by persistent disabling fatigue and other symptoms, such as cognitive problems, headaches, disrupted sleep, myalgias and arthralgias, post-exertional malaise, orthostatic intolerance, tachyarrhythmias and gastrointestinal complaints, all of which greatly interfere with an individual's ability to function at home and at work [33]. Thus, recently, many studies focusing on Long-COVID and ME/CFS suggest some Long-COVID cases fit well as a sub-type of ME/CFS cases. A systematic review conducted in 2021 stated that 25 out of 29 ME/CFS symptoms were reported in at least one selected Long-COVID study [32,33]. The prevalence of Long-COVID amongst those infected with COVID-19 varies widely based on definition and measurement differences, and estimates range from 9-42% [35,36,37,38].
- 3.
- Concerns of bias in epidemiological studies
In an epidemiological study, during the designing and interpretation of results phases, researchers take into consideration the external and internal validity of the study. The external validity includes generalization of the study to wider populations [39]. Internal validity considers whether the sample is biologically and statistically representative of the study population. Statistical generalization is important in survey sampling in which the sample must be statistically representative of the target population [40].
The internal validity can be affected by selection or information bias, and confounding or random error. Bias has been defined as “any systematic error in the design, conduct or analysis of a study that results in a mistaken estimate of an exposure’s effect on the risk of disease” [39]. In other words, bias is any deviation in the collection, analysis, interpretation and publication of data leading to conclusions that systematically underestimate or overestimate the true relationship between a given exposure and a specific disease or any other outcome [41]. Selection bias can result from the way study participants are selected for and participate in studies. Types of selection bias include 1) non-response bias; 2) incidence-prevalence bias (or survival bias); 3) loss-to-follow -up bias; and 4) volunteer bias. Information bias occurs during data collection. Misclassification is the most common type of information bias [39] and it can be non-differential or differential, depending on whether it affects different study groups, equally or not. The lack of biomarkers for diagnosis and the application of imperfect methods for diagnosis have been main barriers to progress in ME/CFS.
Researchers can minimize bias through the appropriate selection of the study design, careful choice of procedures of data collection on exposures and co-variables and disease-related outcomes. Identification and adequate measurement of confounding variables allow for their control in analysis or stratification. Large sample sizes will increase study power and reduce probability of random errors. Statistical power is typically set at least 80% or 0.8, and alpha-1 error at 5% or 0.05 [42].
- 4.
- Equity Diversity and Inclusion (EDI) Considerations
The Tri-agencies which are the Canadian Institute of Health Research (CIHR), the Natural Sciences and Engineering Research Council of Canada (NSERC), and the Social Science and Humanities Research Council of Canada (SSHRC), are the source or research policies and guidelines in Canada. These agencies suggest that equitable, diverse, and inclusive Canadian research is essential to creating the excellent, innovative and impactful research necessary to advance knowledge and understanding, and respond to local, national and global challenges.
For term definitions, please see the Equity and Inclusion Office at the University of British Columbia (available at https://equity.ubc.ca/resources/equity-inclusion-glossary-of-terms/). Detailed information on EDI in research team can be found in Canada Research Chairs website, https://www.chairs-chaires.gc.ca/program-programme/equity-equite/best_practices-pratiques_examplaires-eng.aspx .
In the field of ME/CFS, consideration of equity, diversity, and inclusion is essential with regards to research conduct, sample selection and recruitment, as well as interpretation of results.
Research in the field has mainly focused on white individuals, less in ethnic minorities [6], and typically those with better access to care and services [43]. In particular, the severely affected have been often left out of research studies [44].
Selection bias has also resulted from non-random selection of patients or selection of volunteers, or those with unconfirmed diagnosis by a competent health professional. Self-report of CFS has been found to over-represent the true number of people who would meet specific diagnostic criteria [45] .
The nature of the disease requires some adaptation of methods to enable participation. For example, use of short forms whenever possible, allowance for pauses/ breaks during data collection and other research procedures, as well as consideration of timing and mode of data collection are important. Home visits may be the only option for some assessments of patients who are more severely affected, with online assessment also an option in some cases, and may facilitate inclusion of persons with more severe disabilities and those living distant from the assessment centers.
- 5.
- Language and Culture Considerations
In line with EDI considerations, the assessment of the health and healthcare needs of minorities including indigenous and immigrant populations are acknowledged to potentially differ in health and social sciences. Specifically, self-reported health and risk factor status differs in ethnic variations because of cultural and language differences [46]. Canada has two official languages: English and French. It is also a home for many different ethnic groups including indigenous populations. Many of the self-report questionnaires in ME/CFS, used for case definitions are only available in English. According to Hunt and Bhogal, the most sophisticated translation techniques are applied in the field of patient assessed outcomes, where methods have evolved to a prolonged process of item selection, testing, and retesting and consultations with people monolingual in the target language(s) [46]. Bradley also identified guidelines for translation of questionnaires [47].
Indigenous people including First Nations, Inuit and Métis comprise around 5% (n=1,807,250) of total population of Canada [48]. Table 2 shows the number and percentage of Indigenous people in different provinces. Over 70 indigenous languages are spoken and among them 188,900 people with an Indigenous mother tongue in Canada [48], and language and cultural barriers add to other factors involved in health care access by this population. In terms of health care, indigenous health is in federal, provincial, and territorial legislation and policy [48,49]. Despite the availability of resources, the narrative review conducted by Nguyen et al., suggested there are three categories of barriers to access to healthcare: proximal, intermediate, and distal barriers [50]. The ME/CFS epidemiological study conducted by Nacul et al., in British Columbia based on the BC Generations Project (BCGP) cohort (https://www.bcgenerationsproject.ca/) found less than 4% (while 2.2% in BCGP cohort in 2016) were indigenous participants [51], indicating, this population is under-represented in this large based population study in that Province (the study is currently in press). Engagement of Indigenous populations (and other under-represented ethnic groups), in research participation planning, conduct, analysis and dissemination of studies, as well as in their participation as study subjects.
Conclusions
This initial research guideline provides a framework for ME/CFS research in Canadian settings. We refer to existing guidelines, such as the European Network on Myalgic Encephalomyelitis/Chronic Fatigue Syndrome [19], NINDS common data elements [18] as well as to current practices at ME/CFS clinics in Canada. Guidance on research methods is beyond the aims of this guideline, as these are widely covered in various references from epidemiology and research methods. We also aimed to emphasize how common drawbacks in research can be addressed, and in particular taking into account particularities of the disease and the Canadian context. We propose the standardization of diagnostic criteria and data collection, as guidance for consideration in this field of research. While this is aimed to facilitate better comparison of research studies and meta-analyses, the choice of specific research methods are expected to be determined by individual research groups. This is a field of research that evolves rapidly, not least considering new etiologies, such as cases following COVID-19, as research needs to adapt to new knowledge and challenges. This report aimed to list some important points for consideration, however, we recognize the scope for further work toward a deeper understanding of many of the aspects covered here.
Acknowledgments
The authors would like to gratefully acknowledge the participation and support of members of the Working Group Five of the ICanCME research network, patient-partners and their families. Especially Cathy and John Prescott for their reviews and comments on this paper. Dr. Nacul would like to acknowledge the Pacific Public Health Foundation (previously known as the BCCDC Foundation for Public Health) and BC Women’s Health Foundation for their sponsorship of his protected research time. Dr. Nacul and Dr. Chuluunbaatar would also like to acknowledge the ICanCME and BCWHF for funding research and their contribution to the postdoctoral research fellow program. The ICanCME research network is funded by the Canadian Institute of Health Research (CIHR).
References
- Lim, E.-J.; Son, C.-G. Review of case definitions for myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). Journal of Translational Medicine 2020, 18, 289. [Google Scholar] [CrossRef]
- Carruthers, B.M.; van de Sande, M.I.; De Meirleir, K.L.; Klimas, N.G.; Broderick, G.; Mitchell, T.; Staines, D.; Powles, A.C.P.; Speight, N.; Vallings, R.; et al. Myalgic encephalomyelitis: International Consensus Criteria. Journal of Internal Medicine 2011, 270, 327–338. [Google Scholar] [CrossRef]
- Bansal, A.S.; Bradley, A.S.; Bishop, K.N.; Kiani-Alikhan, S.; Ford, B. Chronic fatigue syndrome, the immune system and viral infection. Brain, Behavior, and Immunity 2012, 26, 24–31. [Google Scholar] [CrossRef]
- Lacerda, E.M.; Geraghty, K.; Kingdon, C.C.; Palla, L.; Nacul, L. A logistic regression analysis of risk factors in ME/CFS pathogenesis. BMC Neurol 2019, 19, 275. [Google Scholar] [CrossRef]
- Nacul, L.; O'Boyle, S.; Palla, L.; Nacul, F.E.; Mudie, K.; Kingdon, C.C.; Cliff, J.M.; Clark, T.G.; Dockrell, H.M.; Lacerda, E.M. How Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) Progresses: The Natural History of ME/CFS. Frontiers in Neurology 2020, 11. [Google Scholar] [CrossRef]
- Nacul, L.C.; Lacerda, E.M.; Pheby, D.; Campion, P.; Molokhia, M.; Fayyaz, S.; Leite, J.C.D.C.; Poland, F.; Howe, A.; Drachler, M.L. Prevalence of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) in three regions of England: a repeated cross-sectional study in primary care. BMC Medicine 2011, 9, 91. [Google Scholar] [CrossRef]
- Statistics, C. CCHS_Ann_2015-16_stata_dta.zip. In Canadian Community Health Survey: Public Use Microdata File, 2015/2016, V1 ed.; Statistics, C., Ed. Abacus Data Network: 2018; hdl:11272.1/AB2/VXU9UQ/DL3LBC.
- Schäfer, M.L. [On the history of the concept neurasthenia and its modern variants chronic-fatigue-syndrome, fibromyalgia and multiple chemical sensitivities]. Fortschr Neurol Psychiatr 2002, 70, 570–582. [Google Scholar] [CrossRef]
- PubMed. Number of articles published in myalgic encephalomyelitis/chronic fatigue syndrome. Availabe online: https://pubmed.ncbi.nlm.nih.gov/?term=myalgic+encephalomyelitis+chronic+fatigue+syndrome&filter=simsearch3.fft&filter=dates.2010-2022 (accessed on.
- Jason, L.A.; Sunnquist, M.; Brown, A.; Evans, M.; Vernon, S.D.; Furst, J.; Simonis, V. Examining case definition criteria for chronic fatigue syndrome and myalgic encephalomyelitis. Fatigue 2014, 2, 40–56. [Google Scholar] [CrossRef]
- Nacul, L.C.; Lacerda, E.M.; Campion, P.; Pheby, D.; Drachler, M.d.L.; Leite, J.C.; Poland, F.; Howe, A.; Fayyaz, S.; Molokhia, M. The functional status and well being of people with myalgic encephalomyelitis/chronic fatigue syndrome and their carers. BMC Public Health 2011, 11, 402. [Google Scholar] [CrossRef] [PubMed]
- Mirin, A.A. A preliminary estimate of the economic impact of long COVID in the United States. Fatigue: Biomedicine, Health & Behavior 2022, 10, 190–199. [Google Scholar] [CrossRef]
- Excellence, N.I.f.H.a.C. Myalgic encephalomyelitis (or encephalopathy)/chronic fatigue syndrome: diagnosis and management. NICE Guideline, No.206; National Institutes for Health and Care Excellence (NICE): London, 2021.
- Nacul, L.; Authier, F.J.; Scheibenbogen, C.; Lorusso, L.; Helland, I.B.; Martin, J.A.; Sirbu, C.A.; Mengshoel, A.M.; Polo, O.; Behrends, U.; et al. European Network on Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (EUROMENE): Expert Consensus on the Diagnosis, Service Provision, and Care of People with ME/CFS in Europe. Medicina (Kaunas) 2021, 57. [Google Scholar] [CrossRef]
- ICAnCME. What is ICanCME? Availabe online: https://www.icancme.ca/ (accessed on February 05).
- Haney E, S.B. McDonaugh M. Diagnostic Methods for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Systematic Review for a National Institutes of Health Pathways to Prevention Workshop. Annals of Internal Medicine 2015, 162, 834–840. [Google Scholar] [CrossRef]
- Estévez-López, F.; Mudie, K.; Wang-Steverding, X.; Bakken, I.J.; Ivanovs, A.; Castro-Marrero, J.; Nacul, L.; Alegre, J.; Zalewski, P.; Słomko, J.; et al. Systematic Review of the Epidemiological Burden of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Across Europe: Current Evidence and EUROMENE Research Recommendations for Epidemiology. J Clin Med 2020, 9. [Google Scholar] [CrossRef]
- Stroke), N.N.I.f.N.D.a. NINDS Common Data Elements - Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. 01/09/2020 ed.; National Institute for Neurological Disorders and Stroke: 2020.
- Mudie, K.; Estévez-López, F.; Sekulic, S.; Ivanovs, A.; Sepulveda, N.; Zalewski, P.; Mengshoel, A.M.; De Korwin, J.-D.; Hinic Capo, N.; Alegre-Martin, J.; et al. Recommendations for Epidemiological Research in ME/CFS from the EUROMENE Epidemiology Working Group. Preprints 2020. [Google Scholar] [CrossRef]
- Carruthers, B.M.; Jain, A.K.; De Meirleir, K.L.; Peterson, D.L.; Klimas, N.G.; Lerner, A.M.; Bested, A.C.; Flor-Henry, P.; Joshi, P.; Powles, A.C.P.; et al. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Journal Of Chronic Fatigue Syndrome 2003, 11, 7–115. [Google Scholar] [CrossRef]
- IOM. Institute of Medicine, Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness. Mil Med 2015, 180, 721–723. [Google Scholar] [CrossRef]
- Strand, E.B.; Nacul, L.; Mengshoel, A.M.; Helland, I.B.; Grabowski, P.; Krumina, A.; Alegre-Martin, J.; Efrim-Budisteanu, M.; Sekulic, S.; Pheby, D.; et al. Myalgic encephalomyelitis/chronic fatigue Syndrome (ME/CFS): Investigating care practices pointed out to disparities in diagnosis and treatment across European Union. PLoS One 2019, 14, e0225995. [Google Scholar] [CrossRef]
- Nacul, L.; Lacerda, E.M.; Kingdon, C.C.; Curran, H.; Bowman, E.W. How have selection bias and disease misclassification undermined the validity of myalgic encephalomyelitis/chronic fatigue syndrome studies? J Health Psychol 2019, 24, 1765–1769. [Google Scholar] [CrossRef]
- Carruthers, B.M.; Jain, A.K.; De Meirleir, K.L.; Peterson, D.L.; Klimas, N.G.; Lerner, A.M.; Bested, A.C.; Flor-Henry, P.; Joshi, P.; Powles, A.C.P.; et al. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Clinical Working Case Definition, Diagnostic and Treatment Protocols. Journal Of Chronic Fatigue Syndrome 2003, 11, 7–115. [Google Scholar] [CrossRef]
- de Groot, V.; Beckerman, H.; Lankhorst, G.J.; Bouter, L.M. How to measure comorbidity. a critical review of available methods. J Clin Epidemiol 2003, 56, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Guralnik, J.M. Assessing the impact of comorbidity in the older population. Ann Epidemiol 1996, 6, 376–380. [Google Scholar] [CrossRef]
- Wirth, K.J.; Löhn, M. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) and Comorbidities: Linked by Vascular Pathomechanisms and Vasoactive Mediators? Medicina (Kaunas) 2023, 59. [Google Scholar] [CrossRef]
- Castro-Marrero, J.; Faro, M.; Aliste, L.; Sáez-Francàs, N.; Calvo, N.; Martínez-Martínez, A.; de Sevilla, T.F.; Alegre, J. Comorbidity in Chronic Fatigue Syndrome/Myalgic Encephalomyelitis: A Nationwide Population-Based Cohort Study. Psychosomatics 2017, 58, 533–543. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Linn, B.S.; Linn, M.W.; Gurel, L. Cumulative illness rating scale. J Am Geriatr Soc 1968, 16, 622–626. [Google Scholar] [CrossRef]
- Miskulin, D.C.; Athienites, N.V.; Yan, G.; Martin, A.A.; Ornt, D.B.; Kusek, J.W.; Meyer, K.B.; Levey, A.S. Comorbidity assessment using the Index of Coexistent Diseases in a multicenter clinical trial. Kidney Int 2001, 60, 1498–1510. [Google Scholar] [CrossRef]
- Wong, T.L.; Weitzer, D.J. Long COVID and Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)—A Systemic Review and Comparison of Clinical Presentation and Symptomatology. Medicina 2021, 57, 418. [Google Scholar] [CrossRef]
- Komaroff, A.L.; Lipkin, W.I. ME/CFS and Long COVID share similar symptoms and biological abnormalities: road map to the literature. Front Med (Lausanne) 2023, 10, 1187163. [Google Scholar] [CrossRef]
- Soriano JB, M.S., Marshall JC, RFelan P, Diaz JV. A clinical case definition of post-COVID-19 condition by a Delphi consensus. The Lancet Infectious Diseases 2022, 22, E102–E107. [CrossRef]
- Woodrow, M.; Carey, C.; Ziauddeen, N.; Thomas, R.; Akrami, A.; Lutje, V.; Greenwood, D.C.; Alwan, N.A. Systematic Review of the Prevalence of Long COVID. Open Forum Infectious Diseases 2023, 10. [Google Scholar] [CrossRef]
- Kozak, R.; Armstrong, S.M.; Salvant, E.; Ritzker, C.; Feld, J.; Biondi, M.J.; Tsui, H. Recognition of Long-COVID-19 Patients in a Canadian Tertiary Hospital Setting: A Retrospective Analysis of Their Clinical and Laboratory Characteristics. Pathogens 2021, 10, 1246. [Google Scholar] [CrossRef]
- Shepherd, C. Long-Covid and ME/CFS - Are they the same condition? Availabe online: https://meassociation.org.uk/wp-content/uploads/LONG-COVID-AND-MECFS-ARE-THEY-THE-SAME-CONDITION-MAY-2023.pdf (accessed on Feb 27).
- UK, G.U.C.C.-i.t. Coronavirus cases in England. Availabe online: https://coronavirus.data.gov.uk/details/cases?areaType=nation&areaName=England (accessed on Feb 27).
- Gordis, L. Bias, Confounding, and Interaction. In Epidemiology, Saunders Elsevier: 2008; pp. 247–256.
- Rothman, K.J. Epidemiology. An Introduction. In Epidemiology. An Introduction, 1st ed.; Oxford University Press: New York, 2002; pp. 20–21. [Google Scholar]
- Last, J. A Dictionary of Epidemiology, 5th ed.; Oxford University Press: Oxford, 2009. [Google Scholar]
- Baguley, T. Understanding statistical power in the context of applied research. Applied Ergonomics 2004, 35, 73–80. [Google Scholar] [CrossRef]
- Almeida, A.P.S.C.; Nunes, B.P.; Duro, S.M.S.; Facchini, L.A. Socioeconomic determinants of access to health services among older adults: a systematic review. Revista de Saúde Pública 2017, 51. [Google Scholar] [CrossRef]
- Kingdon, C.; Giotas, D.; Nacul, L.; Lacerda, E. Health Care Responsibility and Compassion-Visiting the Housebound Patient Severely Affected by ME/CFS. Healthcare 2020, 8, 197. [Google Scholar] [CrossRef]
- Chuluunbaatar E, T.M., Nacul L. Epidemiology of Myalgic Encephalomyelitis among individuals with self-reported Chronic Fatigue Syndrome and their health-related quality of life in Canada. In Proceedings of International Association of Chronic Fatigue Syndrome Myalgic Encephalomyelitis (IACFSME) 2023, New York, New York, USA.
- Hunt, S.M.; Bhopal, R. Self report in clinical and epidemiological studies with non-English speakers: the challenge of language and culture. Journal of Epidemiology and Community Health 2004, 58, 618. [Google Scholar] [CrossRef]
- Bradley, C. Translation of Questionnaires for Use in Different Languages and Cultures. In Handbook of Psychology and Diabetes, Routledge: 1994; p. 13.
- Statistics Canada, G.o.C. Indigenousidentity by Registered or Treaty Indian Status: Canada, provinces and territories, census metropolitan areas and census agglomerations with parts. Availabe online: https://www12.statcan.gc.ca/ (accessed on November 15).
- Canada, G.o. Indigenous health care in Canada. Availabe online: https://www.sac-isc.gc.ca/eng/1626810177053/1626810219482 (accessed on November 17).
- Nguyen, N.H.; Subhan, F.B.; Williams, K.; Chan, C.B. Barriers and Mitigating Strategies to Healthcare Access in Indigenous Communities of Canada: A Narrative Review. Healthcare 2020, 8, 112. [Google Scholar] [CrossRef] [PubMed]
- Project, B.G. Our Participants. Availabe online: https://www.bcgenerationsproject.ca/about/our-participants/ (accessed on March 21).
Figure 1.
ME/CFS Diagnostic Flowchart. Source: Adapted from the Recommendations for Epidemiological Research in ME/CFS from the EUROMENE Epidemiology Working Group preprint 30 Sept 2020 [19].
Figure 1.
ME/CFS Diagnostic Flowchart. Source: Adapted from the Recommendations for Epidemiological Research in ME/CFS from the EUROMENE Epidemiology Working Group preprint 30 Sept 2020 [19].
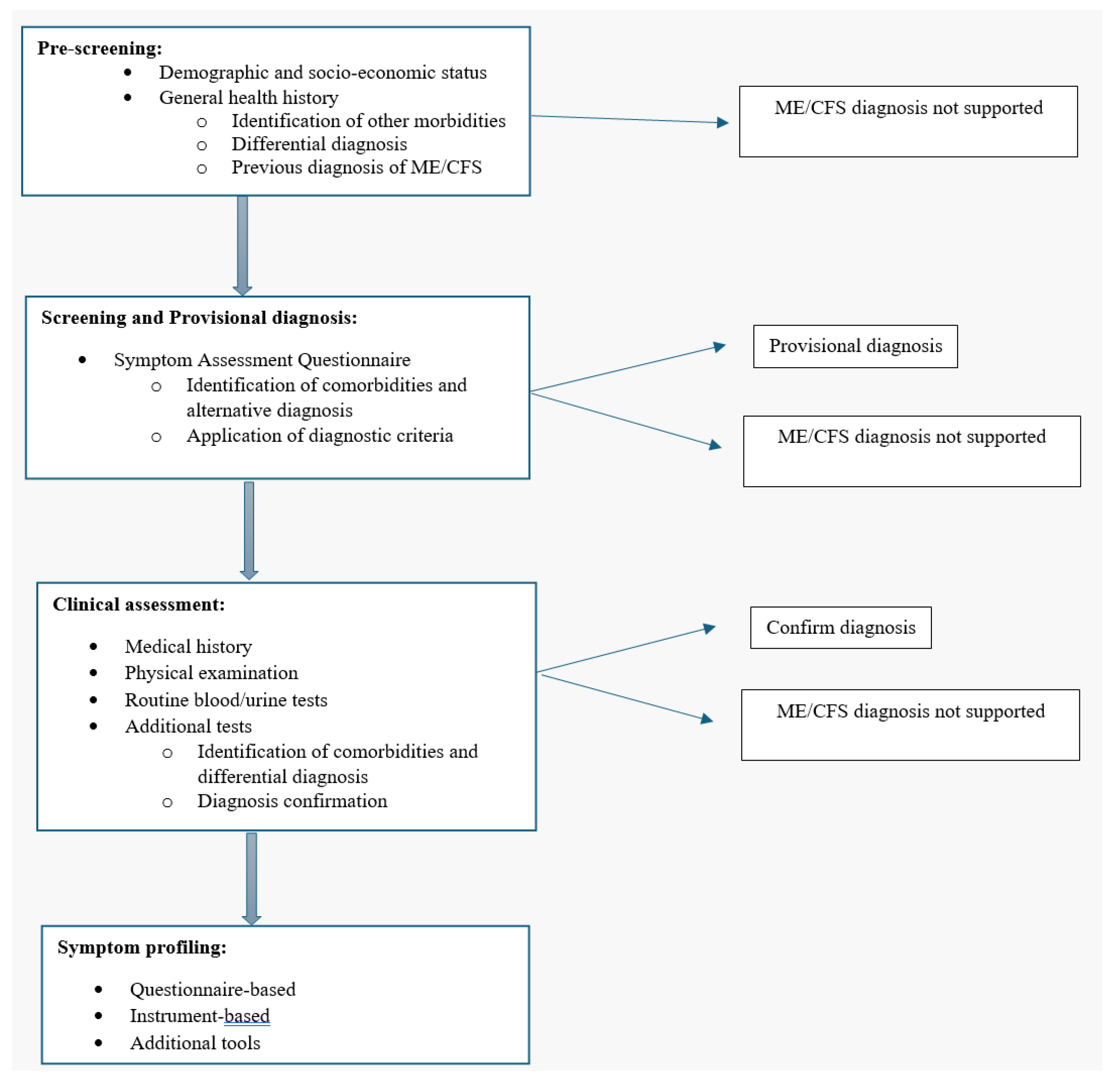

Table 1.
Recommended Data Elements for ME/CFS Research. ICanCME Network.
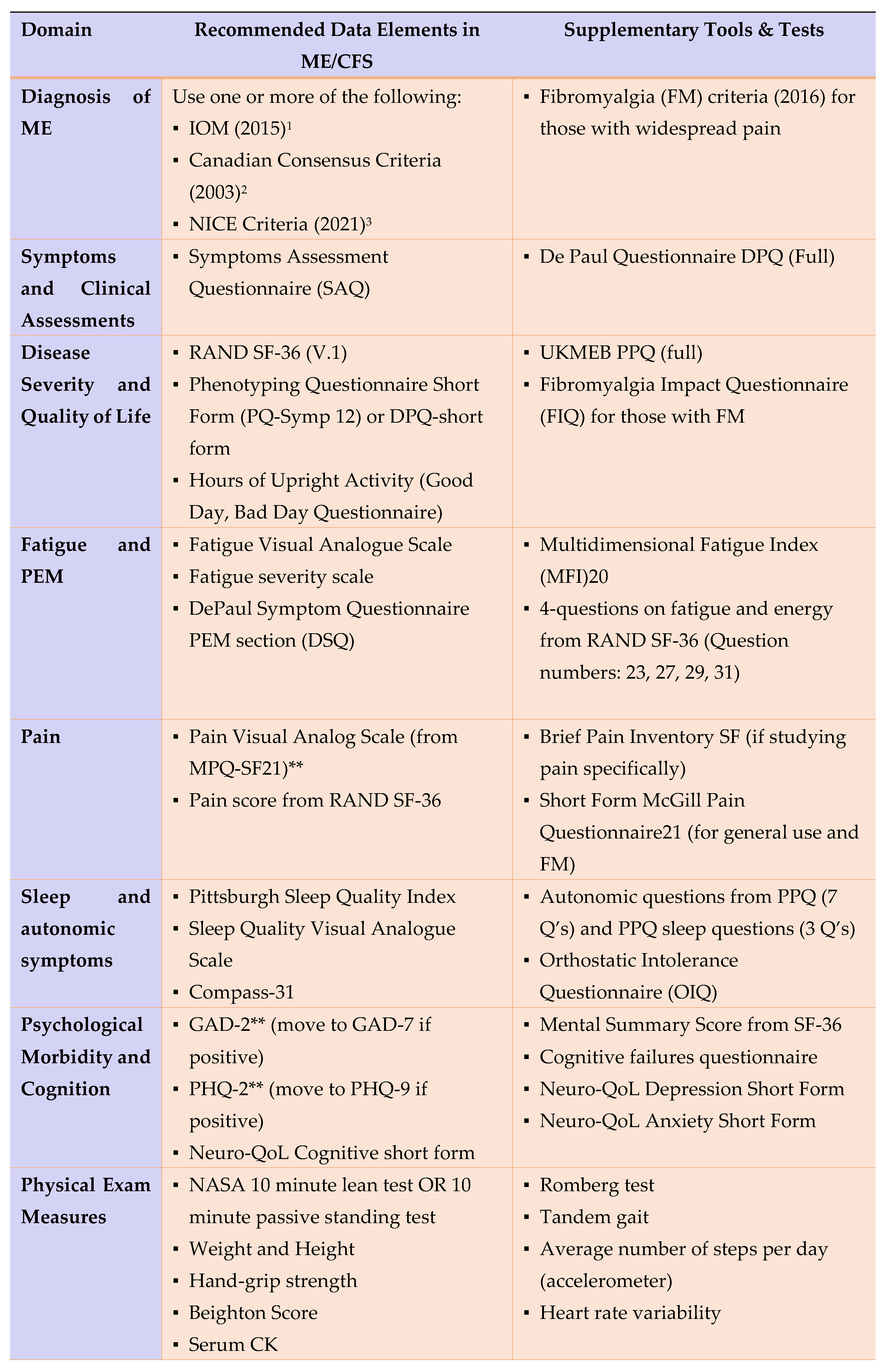
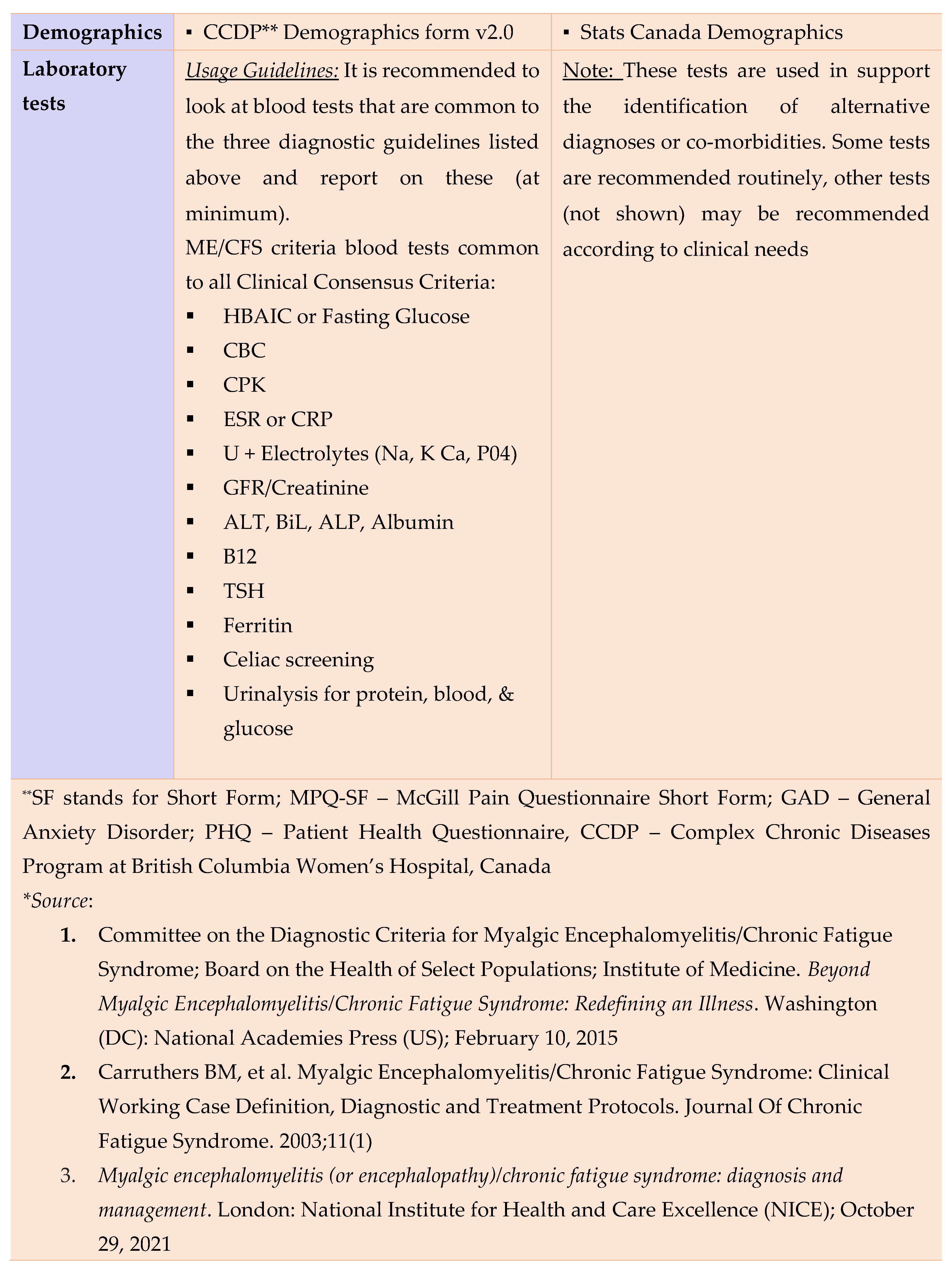
Table 2.
Comorbid conditions of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



