
Submitted:
17 May 2024
Posted:
17 May 2024
You are already at the latest version
Abstract
Acute kidney injury (AKI) is a common complication post-cardiac surgery, impacting short- and long-term survival. Free light chains (FLCs) are being explored as markers for assessing kidney damage risk. A study aimed to validate early AKI detection by studying FLCs (kappa, lambda, and kappa/lambda ratio) in serum and saliva samples. Clinical data was collected from 149 patients who underwent cardiac surgery in Baghdad. Ninety of these patients provided saliva samples in addition to serum samples for free light chain evaluation. Patients were grouped by proteinuria severity. Serum kappa levels were significantly higher in severe proteinuria patients compared to mild or no proteinuria. Salivary kappa levels were significantly higher in mild proteinuria patients compared to severe or no proteinuria. Salivary lambda levels decreased with increasing proteinuria severity. Serum kappa increase could be due to immune system activation and kidney compromise. Both serum and salivary kappa showed good predictive ability for post-surgery AKI prognosis compared to lambda and the kappa/lambda ratio, depending upon ROC performance. The study suggests FLCs, especially kappa, could be valuable in early AKI detection post-cardiac surgery, indicating potential for improved patient outcomes through proactive monitoring and intervention.
Keywords:
Acute Kidney Injury
; cardiac surgery
; serum Free Light Chain
; salivary Free Light Chain
1. Introduction
Cardiac surgery-associated acute kidney injury (CSA-AKI) is characterized by a rapid decline in renal function, leading to a significant decrease in glomerular filtration rate (GFR). Following cardiac surgery, CSA-AKI can independently contribute to a substantial rise in 30-day mortality rates. Mortality rates following open-heart surgery without AKI typically range between 1% and 8%, but in cases where AKI is present, the risk of death increases more than fourfold. Additionally, the likelihood of requiring renal replacement therapy (RRT) can increase up to 63%, and being admitted to the intensive care unit (ICU) after sepsis is linked with CSA-AKI [1].
Numerous causes, including perioperative renal ischemia, reperfusion injury, hemolysis, pigment nephropathy from cardiopulmonary bypass (CPB) [2], oxidative stress, and inflammation, can lead to AKI following heart surgery [3]. Renal perfusion is intricately regulated, with twenty percent of cardiac output directed to the kidneys; however, most blood filtered by the cortex glomeruli bypasses the vasa recta. This shunting helps maintain necessary concentration gradients in the renal medulla for reabsorption but contributes to hypoxia in the renal medulla and corticomedullary junction compared to other tissues. This hypoxia may offer protection against oxidative damage but raises vulnerability to ischemia [4].
Acute kidney injury is a common complication following cardiothoracic surgery and has significant implications for both short- and long-term survival, even in patients who do not progress to renal failure. There are currently no particular treatments for AKI, making management and prevention of its consequences unattainable. A comprehensive understanding of the risk factors and underlying mechanisms of AKI provides clinicians with valuable insights for preventing and treating this condition effectively [5].
Several researches have highlighted that free light chain FLCs may serve as a superior marker for assessing the risk of kidney damage compared to other kidney function markers [6,7]. Various researches have indicated that free light chains are significantly elevated in patients with type 2 diabetes mellitus before the onset of overt renal impairment, suggesting a potential role in predicting early diabetic nephropathy [8,9,10]. This highlights the potential utility of free light chains as a marker for assessing kidney damage and predicting the development of renal complications in various clinical settings [11].
The initiation of immunoglobulin (Ig) production occurs due to the release of intracellular antigens from cell death or ineffective clearance of apoptotic debris, as well as the modification of self-antigens and molecular mimicry. This leads to the activation and polyclonal expansion of B cells. Immunoglobulins have a tetrameric structure consisting of two heavy and two light chains connected by noncovalent forces and disulfide bonds. There are two known light chain isotypes: kappa (κ) and lambda (λ). Proteins known as free light chains (FLCs) have comparable molecular weights but distinct basic structures, which lead to variations in their antigenicity and affinity for biological targets. Because of quick renal clearance, FLCs in the bloodstream have a short half-life of 2–6 hours, with κ FLC having a half-life of 2–4 hours and λ FLC having a half-life of 3–6 hours. Free light chains typically have a negligible presence in urine due to their quick filtration by kidney glomeruli and significant reabsorption by proximal convoluted tubule cells. [12]. Dysregulation of FLCs is a characteristic of many inflammatory diseases and has been demonstrated to be an indicator of all-cause mortality in people without plasma cell dysfunction. As a result, FLCs are becoming more widely recognized as a measure of immunosenescence, inflammation, and overall health and illness in the populace [13].
Saliva contains free light chains, which produced by local plasma cells, and their secretion levels are linked to IgA, although FLC levels are significantly lower than IgA. Analyzing FLCs in saliva can be used as a non-invasive biomarker in various physiological and pathological conditions [14]. Saliva collection is an appealing method that offers several benefits over collecting blood or tissue samples. It is non-intrusive, does not require specialized training or equipment for collection, and may be more cost-effective. As a result, saliva has garnered increased attention as a viable alternative for diagnosing systemic diseases in different medical fields [15,16,17,18,19,20].
While traditional diagnostic tests like serum urea, creatinine, and microalbuminuria are commonly used in AKI diagnosis, their sensitivity and accuracy are constrained as kidney damage occurs before the excretion of these biomarkers. This study aimed to prospectively validate new biomarkers for early detection of surgery-related acute kidney injury by examining the impact of Free Light Chains - specifically kappa, lambda, and the kappa/ lambda ratio - on AKI presentation, particularly in the context of Iraq, to the best of our knowledge, where limited research on the association between FLCs and AKI exists. Additionally, the study sought to assess serum and salivary FLC levels in patients undergoing cardiac surgery to identify AKI risk factors and potentially modifiable elements.
2. Materials and Methods
The study, conducted between July 2023 and January 2024, involved individuals aged 20 to 80 who underwent cardiac surgeries like coronary artery bypass grafting and valve replacement, their diagnosed confirmed by cardiologist using ECG/ECHO. Most participants were hospitalized at Ibn Al-Bitar Hospital or Ghazi AL-Hriri Hospital for Cardiac Surgery in Baghdad, with a few outpatients also included. The study was approved by Baghdad University's College of Medicine. Written consent was obtained from patients or their guardians before participation.
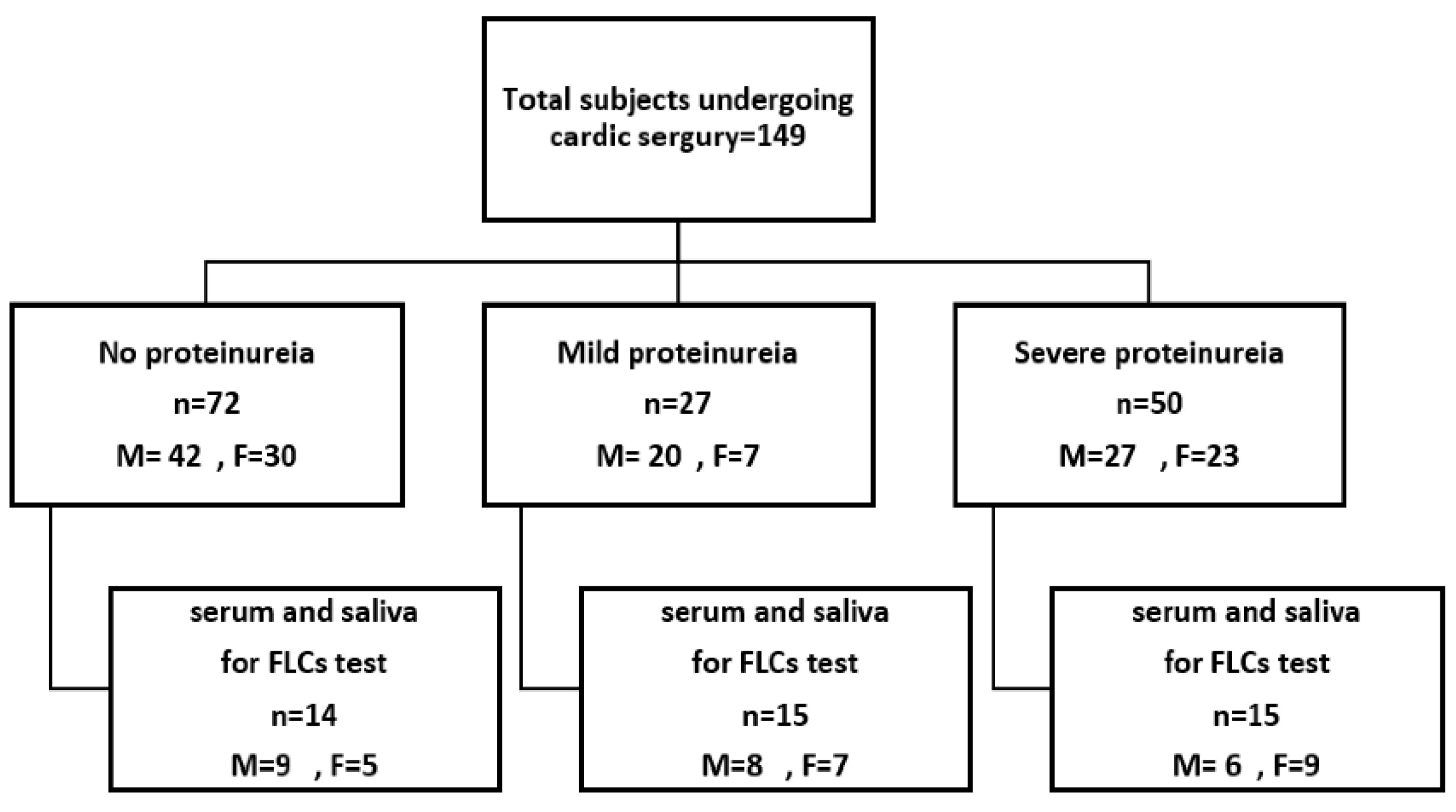
For the epidemiological study, 149 eligible subjects were selected using non-randomized purposive sampling, along with their demographic details and baseline lab results (e.g., protein, urea levels in serum and urine). Based on the presence of protein in urine samples, the samples were categorized by the severity of proteinuria. Samples with no protein were classified as "no proteinuria," those with trace to 1+ as "mild proteinuria," and those with 2+ to 3+ as "severe proteinuria". Out of 149, ninety subjects provided saliva samples for free light chain evaluation in serum and saliva, as represented in the figure [1]. The incidence of AKI was assessed by nephrologist, where Kidney Disease Improving Global Outcomes (KDIGO) criteria are used as consensus standards for AKI diagnosis [21,22].
Figure 1.
Flow chart of study. M: Male & F: Female.
2.1. Inclusion and Exclusion Criteria
The study included consecutive patients over 18 years old who underwent various types of cardiac surgery such as coronary artery bypass grafting, valve surgery, and aortic surgery. Patients with certain conditions were excluded from the study, including those with preoperative creatinine clearance below 60 mL/min, those who died within 24 hours after surgery, individuals injected with iodinated contrast within 72 hours before surgery, those with known acute renal dysfunction, recipients of renal transplants, individuals with liver failure or hepatorenal syndrome, pregnant women, and patients with malignancy. Additionally, participants with recent infections or multiple myeloma were also not included in the study.
2.2. Data Collection
A verified survey was given to collect sociodemographic and anthropometric information, which included age, gender, place of residence, pre-existing conditions (such as diabetes mellitus, hypertension), smoking status, and body mass index (BMI).
2.3. Sampling and Biochemical Measurements
2.3.1. Blood sampling
Following cardiac surgery, approximately 5 milliliters of peripheral venous blood was drawn from each patient. The samples were placed in gel tubes, allowed to coagulate, and then centrifuged to obtain the serum. A portion of each sample was promptly analyzed in the hospital laboratory for urea, creatinine, total protein, and albumin. The remaining serum was divided into 1ml Eppendorf tubes to prevent freeze-thaw cycles and stored at -70°C for subsequent quantification of FLCs levels.
2.3.2. Saliva Sampling
Unstimulated saliva was collected by spitting into a measuring container, and then centrifuged for 15 minutes at 5000 x g. The resulting supernatant was stored in two Eppendorf tubes at -70°C for subsequent quantification of FLCs levels.
2.3.3. Urine Sampling
Urine samples were obtained either randomly or as 24-hour specimens without the addition of preservatives. Approximately 10 milliliters were collected in a container and then centrifuged at 4000 rpm for 10 minutes. The supernatant was immediately used for routine tests including urea, creatinine, protein, and albumin. Protein analysis in the urine was conducted using a dipstick. The estimated glomerular filtration rate (eGFR) was calculated based on patient characteristics and the most recent serum creatinine measurement, utilizing spreadsheets that incorporated the Cockcroft-Gault Formula for creatinine-based estimation of glomerular filtration rate [23].
Most biochemical parameters were measured in the hospital clinical laboratory using automated methods. Serum and saliva samples were assessed for λ FLC and κ FLC using ELISA kits from MYBIOSOURCE, USA. The assays were performed in accordance with the manufacturer’s instructions, and the results were reported in milligrams per liter.
2.4. Statistical Analyses
The information was inputted into an excel spreadsheet and analyzed utilizing the Statistical Package for the Social Sciences (SPSS version 22.0). Continuous variables were expressed as the mean ± (standard error and/or ±standard deviation) for normally distributed data, while categorical variables were presented as number (%) in the dataset. The Kolmogorov–Smirnov test was used to assess normality and homogeneity of variance. Normally distributed continuous data were examined using analysis of variance (ANOVA) with Tukey Honestly Significant Difference (HSD) post hoc analysis. The chi-square test was employed for categorical variables to investigate significant associations with the variables of interest. Pearson's correlation test was used to assess potential linear associations between continuous variables. Receiver Operating Characteristic (ROC) analysis was conducted to evaluate the diagnostic performance of relevant variables. A significance level of p < 0.05 was considered statistically significant for all comparisons.
3. Results
A total of 149 patients undergo heart surgery were recruited in the study. According to the degree of proteinuria, the patients were classified into three groups: 72 patients without proteinuria, 27 patients with mild proteinuria (Trace-1+) and 50 patients with moderate and severe proteinuria (+2,+3).
3.1. Anthropometric Characteristics of the Study Population
Most anthropometric characteristics were comparable between the three groups with no significant difference, as shown in Table 1. The majority of the study population were male (89, 59.7%), although there was no significant variation in the studied groups compared to females (60, 40.3). Males were recorded the higher percentage in those with mild proteinuria (74.07%), however, the differences were not significant. The mean age of patients without proteinuria was 51.57 ± 10.207 years which did not differ significantly (p>0.05) from that of patients with mild or severe proteinuria (56.63 ± 10.724 years and 53.520 ± 8.858 years, respectively).
Likewise, the mean BMI index was very similar among the three groups; however, a slight increase was recorded in the severe proteinuria group (28.674±4.693) with no significant difference.
Aortic valve replacement (AVR) and coronary artery bypass graft (CABG) represent the most common operations for heart surgery in the study population, accounting for 53% and 44.3% respectively, with no significant difference (p>0.05).
Roughly half of the study participants had comorbidities (45%), with classic comorbidities such as hypertension, type 2 diabetes mellitus (T2DM), or both being predominant. Hypertension (27.9%) was more prevalent in the study population than diabetes (14.2%). The co-occurrence of diabetes and hypertension was more common in patients with mild proteinuria (25.9%) than in other groups, with the differences being non-significant (p>0.05).
Notably, smoking was not prevalent and was reported in 13.9%, 18.8%, and 8% of patients without proteinuria, with mild proteinuria, and with severe proteinuria, respectively (p>0.05). The majority of the study population (86.6%) had no surgical procedures other than cardiac surgery, with no significant differences among the three groups. The time interval between cardiac surgery and sample collection appears to have no significant impact on the presence of proteinuria, as there was no significant variation among the three groups in terms of the time of sample collection. The survey population revealed that residents of Baghdad were the most common (67.11%), followed by those of Al-Anbar (17.45%) and Diyala (4.7%).
The baseline laboratory indices show a significant association with the presence and severity of proteinuria. The mean level of blood urea in patients without proteinuria, with mild proteinuria, and with severe proteinuria was 37.313 ± 15.790 mg/dl, 42.092 ± 14.279 mg/dl, and 50.838 ± 24.682 mg/dl, respectively, with highly significant differences (p≤0.05) among the three groups. Similarly, serum creatinine was significantly lower (p≤0.05) in patients without proteinuria (0.912 ± 0.264 mg/dl) compared to those with mild or severe proteinuria (1.036 ± 0.256 mg/dl and 1.332 ± 0.645 mg/dl, respectively). In contrast, serum protein and albumin levels were significantly higher in patients without proteinuria (69.138 ± 11.105 mg/L and 43.199 ± 7.188 mg/L, respectively) compared to those with mild proteinuria (65.967 ± 9.336 mg/L and 38.444 ± 7.973 mg/L, respectively) or severe proteinuria (61.983 ± 17.270 mg/L and 36.538 ± 6.278 mg/L, respectively) with highly significant differences (p≤0.05).
The urine analysis revealed a higher level of creatinine in patients without proteinuria (643.41 ± 324.40 mg) compared to those with mild or severe proteinuria (445.07 ± 280.58 mg and 261.11 ± 211.39 mg, respectively) with a highly significant difference. The level of urea in urine showed a non-significant (p>0.05) decrease with the increase in the severity of proteinuria. On the other hand, protein in urine and the protein-to-creatinine ratio were much lower in patients without proteinuria (11.663 ± 6.720 mg and 39.527 ± 76.743, respectively) compared to those with mild proteinuria (23.919 ± 9.944 mg and 95.369 ± 82.849, respectively) or severe proteinuria (53.886 ± 69.344 mg and 340.41 ± 383.765, respectively) with highly significant differences (p≤0.05).
3.2. Free Light Chain in Serum
The mean concentration of kappa light chain in patients with severe proteinuria was 74.46 ± 3.94 mg/l, which was higher than that of patients with mild proteinuria (63.32 ± 3.75 mg/l) or those without proteinuria (59.37 ± 4.97 mg/l) with a significant difference. In contrast, the three groups were comparable in serum concentration of lambda chain and in the Kappa/Lambda ratio with no significant difference (Table 2, Figure 2, Figure 3 and Figure 4).
The data is presented as mean ± standard error. S.K.FLC: serum kappa Free Light Chain, S.L.FLC: serum lambda Free Light Chain, S.K/L Ratio: serum kappa/lambda Ratio.
3.3. Free Light Chain in Saliva
Unlike in serum, the mean concentration of kappa chain in saliva was higher in patients with mild proteinuria (5.20 ± 0.80 mg/l) than in those without proteinuria (2.68 ± 0.65 ng/ml) or those with severe proteinuria (1.74 ± 0.29 mg/l) with a highly significant difference. Additionally, a significant decrease in saliva lambda chain was observed with an increase in the severity of proteinuria across the studied groups (no proteinuria, mild proteinuria, and severe proteinuria) with concentrations of 1.74 ± 0.29 mg/l, 25.29 ± 3.32 mg/l, and 26.54 ± 10.83 mg/ml, respectively. Furthermore, similar to serum, there were no significant differences between the three groups in the Kappa/Lambda ratio concentration (Table 3 and Figure 5, Figure 6 and Figure 7).
3.4. Diagnostic Performance of Free Light Chains
In the context of distinguishing between non-proteinuria and mild proteinuria, the serum kappa: lambda ratio exhibited good diagnostic performance compared to serum kappa and lambda individually. The area under the curve (AUC) for the kappa/ lambda ratio was 0.605 (p>0.05) with an optimal cut-off value of 0.33, providing 80% sensitivity and 50% specificity. In contrast, serum kappa and lambda showed poor discriminatory ability with AUC values of 0.562 and 0.433 (p>0.05), respectively. In saliva, the cut-off values for kappa and lambda were 2.83 and 16.02, yielding sensitivities of 66.7% and 80%, specificities of 64.3% and 50%, and AUC values of 0.74 (p≤0.05) and 0.657 (p>0.05), respectively, for distinguishing between non-proteinuria and mild proteinuria, as illustrated in Table 4 and Figure 8.
When differentiating between non-proteinuria and severe proteinuria, serum kappa and lambda demonstrated good ROC performance with cut-off values of 66.73 and 15.11, sensitivities of 73.3% for both, specificities of 57.1% and 42.9%, and AUC values of 0.724 (p≤0.05) and 0.690 (p>0.05). In contrast, saliva kappa, lambda, and the kappa/ lambda ratio exhibited poor discriminatory performance, as shown in Table 4 and Figure 9.
Regarding the discrimination between mild proteinuria and severe proteinuria, the serum kappa/ lambda ratio showed a sensitivity of 85.7%, specificity of 46.7%, a cut-off value of 0.32, and an AUC of 0.667 (p>0.05) for predicting the severity of proteinuria, while serum kappa and lambda showed weak ROC performance. Notably, higher sensitivities of 71.4% and 92.9% were observed for saliva kappa and lambda, with corresponding specificities of 86.7% and 53.3%, cut-off values of 3.08 and 14.91, and AUC values of 0.84 (p≤0.05) and 0.781 (p≤0.05), respectively, in distinguishing individuals with mild proteinuria from those with severe proteinuria, as depicted in Table 4 and Figure 10.
3.5. Correlation between Serum and Salivary In Free Light Chains
Pearson’s correlation test was utilized to investigate the potential correlation between serum and salivary free light chain levels. Serum kappa light chain exhibited a significant negative correlation with both saliva kappa light chain (r = -0.306, p = 0.043) and the kappa/lambda ratio (r = -0.415, p = 0.005). Similarly, serum lambda light chain showed a significant negative correlation with saliva kappa light chain (r = -0.334, p = 0.027), as depicted in Table 5.
4. Discussion
According to the 2012 Kidney Disease: Improving Global Outcomes (KDIGO) creatinine criterion, almost 30% of the study population had Acute Kidney Injury (AKI). The occurrence of AKI rose with higher levels of proteinuria, with severe proteinuria associated with a 56% likelihood of developing AKI, as shown in Table 1.
We prospectively collected clinical data from 149 patients undergoing cardiac surgery and grouped them based on the severity of proteinuria (non-proteinuria, mild proteinuria, and sever proteinuria). Proteinuria is an independent risk factor for postoperative AKI in individuals with renal failure, with the risk increasing with the degree of proteinuria [24]. According to earlier researches by Huang et al. [25] and Li et al. [26], proteinuria could represent a predictor of AKI acquired in a hospital.
To explain the association between an increase in Proteinuria and the occurrence of AKI following cardiac surgery, it has been suggested that proteinuria serves as an indicator of damage to glomerular, renal tubular epithelial cells, and endothelial dysfunction [24,27]. Consequently, making it challenging for patients to handle hemodynamic changes, especially those with low eGFR. Moreover, the reabsorption of urinary protein in the tubules triggers the release of various pro-inflammatory molecules like monocyte chemotaxis protein-1, osteopontin, and endothelin-1, which induce renal cell proliferation, activation of macrophages and monocytes, matrix deposition, ultimately leading to tubulointerstitial damage [24,28,29]. Chronic proteinuria can worsen inflammation and fibrosis, reducing renal reserve capacity and increasing susceptibility to kidney injury during cardiac surgery. Factors like cardiopulmonary bypass, ischemia-reperfusion injury, endotoxemia, and surgical trauma create a pro-inflammatory environment that raises the risk of ischemic kidney damage [24,30,31].
Although nonsignificant prevalence of male gender among study population especially those developed AKI (mild proteinuria & sever proteinuria). A study by Zou, Z. et al. [32]. recorded that more than 68% male gender developed AKI which consistence with our results. In contrast, several studies [33,34,35] were recorded that female gender associated as a risk factor with AKI after cardiac surgery.
Our results indicated that the majority of the study population fell within the age range of 40-69 years, with the highest frequency observed in the 50-59 age group. The average age showed a non-significant increase in populations with mild proteinuria and severe proteinuria compared to the no proteinuria group, however age may play a role in the development of AKI in individuals with mild and sever proteinuria. Several studies have documented a gradual rise in the occurrence of Acute Kidney Injury (AKI) among elderly individuals [36,37]. According to a study conducted by Ramos and colleagues, undergoing valve replacement and being of advanced age were identified as risk factors for postoperative AKI [38]. Additionally, Santos et al. concluded that individuals aged over 63 years face an elevated risk of AKI independently [37]. The decline in renal functional reserve due to the progressive decrease in glomerular filtration rate with age renders these patients more vulnerable to renal injury when subjected to hypoperfusion [39,40,41]. Consequently, these patients tend to have a poorer prognosis and experience delayed recovery.
All of the individuals studied who had heart surgery were identified as being overweight (BMI between 25 and 29.9). Slight increases in BMI populations were observed in population with mild proteinuria and severe proteinuria. The study results aligned with a study carried out in Sulaymaniyah/Kurdistan, Iraq, where the author noted a higher prevalence of obesity among patients referred for coronary artery bypass graft surgery (CABG), as well as an elevated incidence of early post-operative complications [42]. Obesity is widely recognized as a complex condition that is often accompanied by serious co-morbidities and complications, such as an increased risk of severe cardiovascular diseases, respiratory diseases, and acute kidney injury AKI [43,44,45]. Studies have shown that obesity can serve as a predictor for AKI. The potential mechanisms linking obesity and AKI include subclinical chronic kidney disease, intraabdominal hypertension, and changes in circulating inflammatory mediators and adipokines [46,47]. Xin-Liang Guan et al. discovered that obese patients have a higher likelihood of developing postoperative AKI [48].
Our findings indicated that approximately 50% of patients who underwent heart surgery had either AVR (Aortic Valve Replacement) or CABG (Coronary Artery Bypass Grafting) procedures, which could potentially be a contributing factor to the development of Acute Kidney Injury (AKI). In a study by W. Jiang et al., the association between surgical types and AKI was examined, it was found that valve and CABG were linked to both in-hospital death and AKI that required renal replacement therapy [24]. According to various research [48,49,50,51,52,53], postoperative AKI is a more common significant complication in aortic surgery. They reported a more than 40% incidence of AKI following aortic surgery, and these patients experienced more postoperative problems such longer hospital or intensive care unit admissions, which was comparable to our findings.
The current study population had comorbidities (DM & Hypertension) associated with cardiac surgery, which may have attributed to an additional increase in the incidence of CSA-AKI, which is also observed by Zou Z. et al. [32]. Different populations, comorbidities, and pathogeneses may all have an impact on the occurrence of AKI after different types of heart surgery. There are comparable risk factors for chronic renal disease and coronary artery disease. Valve heart surgery or CABG is associated with higher rates of congestive heart failure compared to aortic surgery, potentially leading to an increase in cardiorenal syndrome [54].
The risk factors for postoperative AKI in cardiac surgery, including advanced age, higher BMI, female gender, smoking history, hypertension, coronary artery disease, diabetes mellitus, and congestive heart failure, have been documented in multiple studies [55,56]. However, in a study conducted by John M. et al. [24], various urine biomarkers were assessed to predict the occurrence of acute renal injury following heart surgery. The study reported that there were no variations in baseline serum creatinine levels, creatinine levels at the time of collection, duration from surgery to collection, gender, race, comorbidities, type of surgery, or any other factor among the outcome groups.
Since the majority of research participants (87%) were not smokers, smoking status was not taken into account as a confounding factor in the incidence of AKI-ACS in the present study, as shown in Table 1.
This study investigated serum and salivary free light chains as potential predictors of Acute Kidney Injury (AKI). Our results demonstrated a significant increase in serum kappa levels, which correlated with the presence of proteinuria in patients undergoing heart surgery. However, there was an inconsistent pattern observed in serum lambda concentration, with participants without proteinuria showing higher levels than those with mild proteinuria, while patients with severe proteinuria had the highest levels. The serum kappa/lambda ratio showed a slight increase with the advancement of proteinuria in the study cohort, although this change was not statistically significant. In the current study, a statistically significant upward trend in serum kappa levels was noted as the protein levels in participants' urine increased. This finding aligns with a study by Sorvor, E. et al., where they also reported that the severity of nephropathy was linked to an increase in kappa concentration [11].
In a prospective cohort study conducted by Wang et al., it was found that patients in AKI stage 3 had significantly higher concentrations of both kappa Free Light Chains (FLC) and lambda FLC compared to patients in AKI stages 1 and 2. The study also highlighted a significantly elevated risk of mortality within 90 days following an AKI diagnosis [57]. Several investigations involving chronic kidney disease (CKD) patients revealed higher levels of free light chains across the CKD stages [10,58]. It has also been reported that increasing blood FLCs concentrations are independently related to an increased likelihood of ESRD (End-Stage Renal Disease) in patients with CKD [59].
A study by De Novellis, D. et al. suggested that serum free chain ratio could be a biomarker of kidney function and might predict renal failure early in multiple myeloma patients [60]. Polyclonal free light chains (FLCs) are produced by plasma cells during intact immunoglobulin synthesis. Elevated serum FLC levels result from their excessive production when the adaptive immune system is activated. This increase in serum FLC may be an immune response triggered by the release of endotoxins due to disruptions in gut barrier function in acute kidney injury (AKI) [61]. The presence of FLCs could potentially worsen AKI outcomes by promoting inflammation [57]. Furthermore, elevated polyclonal FLC levels have been observed in autoimmune and chronic inflammatory conditions like systemic lupus erythematosus, rheumatoid arthritis, heart failure, and diabetes [7,10,62,63]. Impaired renal function can also lead to higher serum FLC concentrations due to reduced glomerular filtration [64]. In AKI, the elevated serum FLC levels may be a consequence of both immune system activation and compromised glomerular filtration [57].
In cases where renal clearance is reduced, the reticuloendothelial system plays a more significant role in clearing FLCs, leading to higher levels of free light chains associated with the severity of conditions like diabetic nephropathy. Excessive synthesis of free light chains and their filtration through renal glomeruli can damage renal tubules, causing tubular dysfunction. Additionally, any form of renal failure can further elevate serum FLC concentrations due to decreased filtration rates [65].
It was observed by Azat, N. F. [66], that an increase in albuminuria was linked to a decrease in IgG levels, while a direct correlation was found between albuminuria and serum IgM. The study suggests that immunoglobulin abnormalities in patients with nephrotic syndrome, compared to healthy children, may be indicative of T-cell and B-cell involvement, supporting the idea that glomerular changes in nephrotic syndrome could be influenced by disturbances in these immune cells. The exact significance of increased serum FLCs in predicting the outcome of AKI is unclear. It is also plausible that elevated FLC levels serve as a general indicator of immune system activation in AKI. Studies have indicated that FLCs present in both serum and cerebrospinal fluid (CSF) could offer prompt insights into intrathecal inflammation in individuals with multiple sclerosis [67].
Saliva testing is useful in biomarker research because it is non-invasive, making it appropriate for repeated measurements, long-term sampling, and certain populations or study designs where blood sample is not feasible. Several researches were documented the possibility of using saliva as an alternative sample to serum as a diagnostic fluid [68,69,70,71,72]. Free light chains (FLCs) have great significance across diseases and demographics, making them excellent for salivary analysis. Salivary FLCs may reflect systemic levels, providing insights into local immune activation and inflammation. Although the relationship between FLC levels in serum and saliva is unknown, salivary FLCs provide an easy method to detect increased polyclonal light chain synthesis and track FLC levels over time in a variety of disorders and populations [73].
The study group exhibits a distinct pattern in salivary Kappa concentration, with a substantial significant increase in mild proteinuria when compared to non-proteinuria and a significant decline in severe proteinuria when compared to mild proteinuria. The cohort study demonstrated a sequential reduction in salivary lambda concentration as proteinuria progressed. Still, salivary kappa/ lambda ratio data, however, showed an irregular tendency: individuals without proteinuria had the highest values when compared to patients with severe proteinuria, while those with mild proteinuria had the lowest levels. A previous study conducted by Konen, F.F. and colleagues examined serum and salivary FLC levels in patients with Sjögren's syndrome who had neurological symptoms (Neuro-Sjögren) and in neurological patients without the anti-SSA (Ro) antibodies (controls). The study found non-significant differences in FLC concentrations between the studied groups [74].
Salivary gland plasma cells are the primary source of immunoglobulin A (IgA), with autonomic nerves controlling its release. Salivary IgA levels show a positive correlation with short-term stress and a negative correlation with long-term stress, indicating a reflection of stress effects on the mucosal immune system and the body's response. Stress-induced IgA suppression may increase susceptibility to infections and weaken immunity. Immunoglobulins consist of two identical heavy chains and two identical light chains, with plasma cells producing more light chains during synthesis. The excess light chains released into the bloodstream are known as free light chains, serving as cancer biomarkers for plasma cell malignancies. Dysregulation of FLCs has been linked to predicting overall mortality in individuals without plasma cell diseases and is observed in various inflammatory conditions, making FLCs increasingly recognized as markers of immunosenescence, inflammation, and general population health [14]. Similar to IgA levels, salivary free light chains fluctuate throughout the day, indicating that local plasma cells control their production. Individuals exhibit constant daily variability in both FLCs and IgA, which is impacted by the time of awakening. Consistent with data from other studies (Dimitriou et al., 2002; Li and Gleeson, 2004) [75], FLCs exhibit a diurnal pattern similar to that of IgA, with greater levels in the morning and lower levels in the evening.
According to Rapson, A. et al., the fluctuations in IgA and FLCs are likely regulated by a central circadian pacemaker. This study also confirms the importance of considering the time of day for sampling serum and salivary FLCs for clinical testing. Additionally, the lack of correlation between serum and saliva suggests that salivary FLCs are mainly a product of local secretion from plasma cells within the salivary glands, indicating that FLCs in oral fluid are distinct from those in the systemic circulation [75]. Neglecting to consider the time of sample collection for clinical testing may result in ambiguity concerning our findings.
Acute Kidney Injury progression was identified by FLCs and its diagnostic accuracy was evaluated using Receiver Operating Characteristic (ROC) analysis. There is insufficient data in the literature currently in publication regarding the use of FLC in AKI diagnosis, and there are little researches to support FLC's use as a predictive tool for early detection of AKI after cardiac surgery. The area under curve (AUC) that obtained from the ROC curve, is a reliable measure of test accuracy. An AUC of near 1.0 indicates a perfect diagnostic test, while an AUC of 0.5 suggests a test that does not effectively differentiate between outcomes [76].
In the current study, both serum and salivary kappa showed strong predictive abilities for the prognosis of AKI following cardiac surgery, as depicted in Table 4. Additionally, salivary lambda demonstrated a high sensitivity of 92.9% but a low specificity of 53.3% when used as a prognostic tool to differentiate between mild and severe proteinuria. The study findings indicated that the FLC ratio had very low sensitivity and specificity, making it unsuitable for diagnosing AKI compared to kappa and lambda. Further research is warranted to elucidate the role of FLC in the development of AKI post-cardiac surgery and its potential as an early diagnostic biomarker.
5. Conclusions
The present multicenter prospective cohort study found that nearly 30% of the study population developed Acute Kidney Injury (AKI) after cardiac surgery, as per the 2012 Kidney Disease: Improving Global Outcomes (KDIGO) creatinine criterion. The incidence of AKI increased with higher levels of proteinuria, with severe proteinuria linked to a 56% likelihood of AKI development. The study population, identified as overweight and aged over 50 years, showed a tendency to develop AKI. Study data indicated that as participants' urine protein levels rose, there was a statistically significant increasing trend in serum Kappa levels. This elevation may be attributed to immune system activation and impaired glomerular filtration. Thus, the increase in Kappa concentration may correlate with the severity of nephropathy. Using Receiver Operating Characteristic (ROC) analysis to determine the diagnostic accuracy of Free Light Chains (FLCs), it was revealed that serum and salivary kappa exhibited strong predictive abilities for AKI prognosis post-cardiac surgery compared to lambda and the kappa/ lambda ratio. Further research is necessary to ascertain the role of FLCs in the onset of AKI following cardiac surgery and their potential as early diagnostic biomarkers.
Author Contributions
Thikra Hasan Mathkor designed the study, wrote and interpreted the results, and supervised the work. Moazaz Rashad Saed collected and assembled data, performed the FLCs assay, analyzed the data, maintained the dataset, facilitated data acquisition, and contributed to writing the manuscript. Both authors read and approved the final manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The Institutional Ethics Committee of Ghazi-Al Hariri Hospital for Specialized Surgery and Ibn Al-Bitar Center for Cardiac Surgery, University of Baghdad, Iraq provided approval for the study design and data collection (Issue No. Bio133). The study was conducted in compliance with the Helsinki Declaration. Informed consent was obtained from all subjects involved in the study.
Informed Consent Statement
The authors declare no conflict of interest.
Data Availability Statement
Data are available by contacting the corresponding author.
Acknowledgments
The Department of Chemistry and Biochemistry at the College of Medicine, University of Baghdad, Iraq provided support for this research. The authors extend their thanks to all patients and participating centers for their ongoing support. The authors also express gratitude to urologists Dr. Ihab Mahmood Al-Azzawi and Dr. Ahmed Essam Thabit, as well as cardiologists Dr. Ibrahim Mahdi Salih and Dr. Ali Nagim from the division of cardiovascular surgery, for their help in managing patients.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Vives M, Hernandez A, Parramon F, Estanyol N, Pardina B, Muñoz A, et al. Acute kidney injury after cardiac surgery: prevalence, impact and management challenges. International journal of nephrology and renovascular disease. 2019:153-66.
- Al-Saffar HB, Yassin AJ, Ali A. Delayed Recovery of Contrast Induced Kidney Injury Post Angiography: Rate and Risk Factors. Journal of the Faculty of Medicine Baghdad. 2015;57(3):183-7.
- Manuti JK. Renal Dysfunction in Patients with Heart Failure. Journal of the Faculty of Medicine Baghdad. 2010;52(2):129-31.
- O’Neal JB, Shaw AD, Billings FT. Acute kidney injury following cardiac surgery: current understanding and future directions. Critical care. 2016;20:1-9.
- Thiele RH, Isbell JM, Rosner MH. AKI associated with cardiac surgery. Clinical Journal of the American Society of Nephrology. 2015;10(3):500-14.
- Esparvarinha M, Nickho H, Mohammadi H, Aghebati-Maleki L, Abdolalizadeh J, Majidi J. The role of free kappa and lambda light chains in the pathogenesis and treatment of inflammatory diseases. Biomedicine & Pharmacotherapy. 2017;91:632-44.
- Hutchison CA, Harding S, Hewins P, Mead GP, Townsend J, Bradwell AR, et al. Quantitative assessment of serum and urinary polyclonal free light chains in patients with chronic kidney disease. Clinical Journal of the American Society of Nephrology. 2008;3(6):1684-90.
- Brebner JA, Stockley RA. Polyclonal free light chains: a biomarker of inflammatory disease or treatment target? F1000 medicine reports. 2013;5.
- Currie G, McKay G, Delles C. Biomarkers in diabetic nephropathy: present and future. World journal of Diabetes. 2014;5(6):763.
- Hutchison CA, Cockwell P, Harding S, Mead GP, Bradwell AR, Barnett AH. Quantitative assessment of serum and urinary polyclonal free light chains in patients with type II diabetes: an early marker of diabetic kidney disease? Expert opinion on therapeutic targets. 2008;12(6):667-76.
- Sorvor E, Owiredu WK, Okyere P, Annani-Akollor ME, Donkor S, Bannor R, et al. Assessment of Serum Free Light Chains as a Marker of Diabetic Nephropathy; A Cross-Sectional Study in the Kumasi Metropolis. Frontiers in Clinical Diabetes and Healthcare. 2022;3:881202.
- Napodano C, Pocino K, Rigante D, Stefanile A, Gulli F, Marino M, et al. Free light chains and autoimmunity. Autoimmunity reviews. 2019;18(5):484-92.
- Irshad L, Faustini S, Evans L, Drayson M, Campbell JP, Heaney J. Salivary free light chains as a new biomarker to measure psychological stress.
- Irshad L, Faustini S, Evans L, Drayson MT, Campbell JP, Heaney JL. Salivary free light chains as a new biomarker to measure psychological stress: the impact of a university exam period on salivary immunoglobulins, cortisol, DHEA and symptoms of infection. Psychoneuroendocrinology. 2020;122:104912.
- Al-Ghurabei BH. Role of salivary tumor necrosis factor-alpha and immunoglobulin-a in recurrent aphthous stomatitis. Journal of the Faculty of Medicine Baghdad. 2011;53(2):207-10.
- Al-Rubaee EA, Kadum HA, Al-Braich MS. Salivary aspartate amino transferase and alanine amino transferase of non-insulin-dependents (Type2) diabetic patients. Journal of the Faculty of Medicine Baghdad. 2010;52(2):212-4.
- Heaney JL, Faustini S, Evans L, Rapson A, Collman E, Emery A, et al. Investigating the utility of saliva immunoglobulins for the detection of myeloma and using myeloma proteins to clarify partition between oral and systemic immunity. European journal of haematology. 2022;108(6):493-502.
- Kaczor-Urbanowicz KE, Martin Carreras-Presas C, Aro K, Tu M, Garcia-Godoy F, Wong DT. Saliva diagnostics–Current views and directions. Experimental Biology and Medicine. 2017;242(5):459-72.
- Kaufman E, Lamster IB. The diagnostic applications of saliva—a review. Critical Reviews in oral biology & medicine. 2002;13(2):197-212.
- Zaidan TF, Al-Omary WM, Al-Sandook TA. Threshold sensitivity of taste perception and the role of saliva and Zinc level in some physiological & pathological conditions. Journal of the Faculty of Medicine Baghdad. 2009;51(1):90-4.
- Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clinical Practice. 2012;120(4):c179-c84.
- Tsai T-Y, Chien H, Tsai F-C, Pan H-C, Yang H-Y, Lee S-Y, et al. Comparison of RIFLE, AKIN, and KDIGO classifications for assessing prognosis of patients on extracorporeal membrane oxygenation. Journal of the Formosan Medical Association. 2017;116(11):844-51.
- Shrewsberry TW, Banoub A, Fleming K, Snyder H, Stehlik J. Spreadsheet use to calculate creatinine clearance from serum creatinine. The Journal of ExtraCorporeal Technology. 2007;39(4):260-2.
- Jiang W, Chen Z, Xu J, Luo Z, Teng J, Ding X, et al. Proteinuria is a risk factor for acute kidney injury after cardiac surgery in patients with stages 3–4 chronic kidney disease: a case control study. BMC Cardiovascular Disorders. 2023;23(1):77.
- Huang T-M, Wu V-C, Young G-H, Lin Y-F, Shiao C-C, Wu P-C, et al. Preoperative proteinuria predicts adverse renal outcomes after coronary artery bypass grafting. Journal of the American Society of Nephrology. 2011;22(1):156-63.
- Li S-Y, Chuang C-L, Yang W-C, Lin S-J. Proteinuria predicts postcardiotomy acute kidney injury in patients with preserved glomerular filtration rate. The Journal of thoracic and cardiovascular surgery. 2015;149(3):894-9.
- Clausen P, Jensen J, Jensen G, Borch-Johnsen K, Feldt-Rasmussen B. Elevated urinary albumin excretion is associated with impaired arterial dilatory capacity in clinically healthy subjects. Circulation. 2001;103(14):1869-74.
- Wang Y, Chen J, Chen L, Tay Y-C, Rangan GK, Harris D. Induction of monocyte chemoattractant protein-1 in proximal tubule cells by urinary protein. Journal of the American Society of Nephrology. 1997;8(10):1537-45.
- Zoja C, Morigi M, Figliuzzi M, Bruzzi I, Oldroyd S, Benigni A, et al. Proximal tubular cell synthesis and secretion of endothelin-1 on challenge with albumin and other proteins. American journal of kidney diseases. 1995;26(6):934-41.
- Massoth C, Zarbock A, Meersch M. Acute kidney injury in cardiac surgery. Critical Care Clinics. 2021;37(2):267-78.
- Rossaint J, Berger C, Van Aken H, Scheld HH, Zahn PK, Rukosujew A, et al. Cardiopulmonary bypass during cardiac surgery modulates systemic inflammation by affecting different steps of the leukocyte recruitment cascade. 2012.
- Zou Z, Ren T, Li Y, Zeng Q, Wang X, Teng J, et al. The Association Between Serum Glutathione Peroxidase-3 Concentration and Risk of Acute Kidney Injury After Cardiac Surgery: A Nested Case-Control Study. The American Journal of Cardiology. 2023;209:29-35.
- Mehta RH, Grab JD, O’Brien SM, Bridges CR, Gammie JS, Haan CK, et al. Bedside tool for predicting the risk of postoperative dialysis in patients undergoing cardiac surgery. Circulation. 2006;114(21):2208-16.
- Thakar CV, Arrigain S, Worley S, Yared J-P, Paganini EP. A clinical score to predict acute renal failure after cardiac surgery. Journal of the American Society of Nephrology. 2005;16(1):162-8.
- Yu Y, Li C, Zhu S, Jin L, Hu Y, Ling X, et al. Diagnosis, pathophysiology and preventive strategies for cardiac surgery-associated acute kidney injury: a narrative review. European Journal of Medical Research. 2023;28(1):45.
- Magro MCdS, Franco EdS, Guimarães D, Kajimoto D, Gonçalves MAB, Vattimo MdFF. Evaluation of the renal function in patients in the postoperative period of cardiac surgery: does AKIN classification predict acute kidney dysfunction? Revista Brasileira de Terapia Intensiva. 2009;21:25-31.
- Santos FO, Silveira MA, Maia RB, Monteiro MDC, Martinelli R. Acute renal failure after coronary artery bypass surgery with extracorporeal circulation: incidence, risk factors, and mortality. Arquivos brasileiros de cardiologia. 2004;83:145-9.
- Ramos KA, Dias CB. Acute kidney injury after cardiac surgery in patients without chronic kidney disease. Brazilian journal of cardiovascular surgery. 2018;33:454-61.
- Corredor C, Thomson R, Al-Subaie N. Long-term consequences of acute kidney injury after cardiac surgery: a systematic review and meta-analysis. Journal of cardiothoracic and vascular anesthesia. 2016;30(1):69-75.
- Lopez-Delgado JC, Esteve F, Torrado H, Rodríguez-Castro D, Carrio ML, Farrero E, et al. Influence of acute kidney injury on short-and long-term outcomes in patients undergoing cardiac surgery: risk factors and prognostic value of a modified RIFLE classification. Critical care. 2013;17:1-12.
- Srivastava V, D'Silva C, Tang A, Sogliani F, Ngaage DL. The impact of major perioperative renal insult on long-term renal function and survival after cardiac surgery. Interactive cardiovascular and thoracic surgery. 2012;15(1):14-7.
- Mohammed AK, Nadr JH. Early complications associated with obesity following coronary artery bypass graft surgery: Obesity and post-CABG morbidity. Journal of the Faculty of Medicine Baghdad. 2021;63(4):158-62.
- Shashaty MG, Stapleton RD. Physiological and management implications of obesity in critical illness. Annals of the American Thoracic Society. 2014;11(8):1286-97.
- Wacharasint P, Fuengfoo P, Rangsin R, Morakul S, Chittawattanarat K, Chaiwat O. Prevalence and impact of overweight and obesity in critically ill surgical patients: analysis of THAI-SICU study. J Med Assoc Thai. 2016;99(6):55-62.
- Zhao H, Pan X, Gong Z, Zheng J, Liu Y, Zhu J, et al. Risk factors for acute kidney injury in overweight patients with acute type A aortic dissection: a retrospective study. Journal of thoracic disease. 2015;7(8):1385.
- Soto GJ, Frank AJ, Christiani DC, Gong MN. Body mass index and acute kidney injury in the acute respiratory distress syndrome. Critical care medicine. 2012;40(9):2601-8.
- Vasquez CR, DiSanto T, Reilly JP, Forker CM, Holena DN, Wu Q, et al. Relationship of body mass index, serum creatine kinase, and acute kidney injury after severe trauma. Journal of Trauma and Acute Care Surgery. 2020;89(1):179-85.
- Guan X-L, Li L, Jiang W-J, Gong M, Li H-Y, Liu Y-Y, et al. Low preoperative serum fibrinogen level is associated with postoperative acute kidney injury in patients with in acute aortic dissection. Journal of Cardiothoracic Surgery. 2023;18(1):6.
- Englberger L, Suri RM, Greason KL, Burkhart HM, Sundt III TM, Daly RC, et al. Deep hypothermic circulatory arrest is not a risk factor for acute kidney injury in thoracic aortic surgery. The Journal of thoracic and cardiovascular surgery. 2011;141(2):552-8.
- Hobson CE, Yavas S, Segal MS, Schold JD, Tribble CG, Layon AJ, et al. Acute kidney injury is associated with increased long-term mortality after cardiothoracic surgery. Circulation. 2009;119(18):2444-53.
- Kowalik MM, Lango R, Klajbor K, Musiał-Świa̢tkiewicz V, Kołaczkowska M, Pawlaczyk R, et al. Incidence-and mortality-related risk factors of acute kidney injury requiring hemofiltration treatment in patients undergoing cardiac surgery: a single-center 6-year experience. Journal of Cardiothoracic and Vascular Anesthesia. 2011;25(4):619-24.
- Roh GU, Lee JW, Nam SB, Lee J, Choi J-r, Shim YH. Incidence and risk factors of acute kidney injury after thoracic aortic surgery for acute dissection. The Annals of thoracic surgery. 2012;94(3):766-71.
- Vekstein AM, Yerokun BA, Jawitz OK, Doberne JW, Anand J, Karhausen J, et al. Does deeper hypothermia reduce the risk of acute kidney injury after circulatory arrest for aortic arch surgery? European Journal of Cardio-Thoracic Surgery. 2021;60(2):314-21.
- Chen JJ, Chang CH, Wu VCC, Chang SH, Hung KC, Chu PH, et al. Long-term outcomes of acute kidney injury after different types of cardiac surgeries: a population-based study. Journal of the American Heart Association. 2021;10(9):e019718.
- Chen J-J, Kuo G, Hung C-C, Lin Y-F, Chen Y-C, Wu M-J, et al. Risk factors and prognosis assessment for acute kidney injury: The 2020 consensus of the Taiwan AKI Task Force. Journal of the Formosan Medical Association. 2021;120(7):1424-33.
- Chou Y-H, Huang T-M, Wu V-C, Chen W-S, Wang C-H, Chou N-K, et al. Associations between preoperative continuation of renin–angiotensin system inhibitor and cardiac surgery-associated acute kidney injury: a propensity score-matching analysis. Journal of Nephrology. 2019;32:957-66.
- Wang W, Zhang L, Yang T, Ma S, Zhang Q, Shi P, et al. Combined serum free light chain predicts prognosis in acute kidney injury following cardiovascular surgery. Renal Failure. 2022;44(1):1-10.
- Desjardins L, Liabeuf S, Lenglet A, Lemke H-D, Vanholder R, Choukroun G, et al. Association between free light chain levels, and disease progression and mortality in chronic kidney disease. Toxins. 2013;5(11):2058-73.
- Fraser SD, Fenton A, Harris S, Shardlow A, Liabeuf S, Massy ZA, et al., editors. The Association of Serum Free Light Chains with Mortality and Progression to end-stage renal disease in chronic kidney disease: systematic review and individual patient data meta-analysis. Mayo Clinic Proceedings; 2017: Elsevier.
- De Novellis D, Fontana R, Carobene A, Serio B, Ferrara I, Martorelli MC, et al. Serum free light-chain ratio at diagnosis is associated with early renal damage in multiple myeloma: A case series real-world study. Biomedicines. 2022;10(7):1657.
- Zaborin A, Smith D, Garfield K, Quensen J, Shakhsheer B, Kade M, et al. Membership and behavior of ultra-low-diversity pathogen communities present in the gut of humans during prolonged critical illness. MBio. 2014;5(5):10.1128/mbio. 01361-14.
- Aggarwal R, Sequeira W, Kokebie R, Mikolaitis RA, Fogg L, Finnegan A, et al. Serum free light chains as biomarkers for systemic lupus erythematosus disease activity. Arthritis care & research. 2011;63(6):891-8.
- Jackson CE, Haig C, Welsh P, Dalzell JR, Tsorlalis IK, McConnachie A, et al. Combined free light chains are novel predictors of prognosis in heart failure. JACC: Heart Failure. 2015;3(8):618-25.
- Waldmann TA, Strober W, Mogielnicki RP. The renal handling of low molecular weight proteins: II. Disorders of serum protein catabolism in patients with tubular proteinuria, the nephrotic syndrome, or uremia. The Journal of clinical investigation. 1972;51(8):2162-74.
- Bhole MV, Sadler R, Ramasamy K. Serum-free light-chain assay: clinical utility and limitations. Annals of clinical biochemistry. 2014;51(5):528-42.
- Azat, NF. Evaluation of Serum (immunoglobulin G, M) in children with nephrotic syndrome relapse. Journal of the Faculty of Medicine Baghdad. 2012;54(1):15-7.
- Gudowska-Sawczuk M, Mroczko B. Free light chains as a novel diagnostic biomarker of immune system abnormalities in multiple sclerosis and HIV infection. BioMed Research International. 2019;2019.
- Jabbar SA, Hasan HR. ACTIVITIES OF SULFHYDRYL OXIDASE AND XANTHINE OXIDOREDUCTASE SYSTEM IN SALIVA AND SERUM OF WOMEN WITH DIFFERENT TYPES OF BREAST TUMORS. Biochemical & Cellular Archives. 2021;21.
- Hasan HRAA, N. N. Oxidative Stress Status in Sera and Saliva of Type 2 Diabetic Iraqi Patients with and without Proliferative Diabetic Retinopathy. Asian Journal of Chemistry. 2019;31(3): 719-22.
- Hasan HR, Aburahma NNA, AL-Kazaz AKA. Proteins Level in Sera and Saliva of Type2 Diabetic Iraqi Patients with and Without Proliferative Diabetic Retinopathy. Oriental Journal of Chemistry. 2017;33(6):2776.
- Hasan HR, Aburahma NN. The Variations in Saliva and Serum Total Peroxidases System’s Activity in Patients with Different Oral Tumors. Biological. 2020;2307:615.
- Hasan HR, & Mathkor, T. H. Alteration in serum & saliva α-amylase activity & levels of some hormones associated with exposure to chemicals. Asian Journal of Chemistry. 2019;31(2):410 - 6.
- Heaney JL, Gleeson M, Phillips AC, Taylor IM, Drayson MT, Goodall M, et al. Salivary immunoglobulin free light chains: reference ranges and responses to exercise in young and older adults. Exercise Immunology Review. 2016;22:28-40.
- Konen FF, Seeliger T, Schwenkenbecher P, Gingele S, Jendretzky KF, Sühs K-W, et al. Saliva Free Light Chains in Patients with Neuro-Sjögren. Biomedicines. 2022;10(10):2470.
- Rapson A, Collman E, Faustini S, Yonel Z, Chapple IL, Drayson MT, et al. Free light chains as an emerging biomarker in saliva: Biological variability and comparisons with salivary IgA and steroid hormones. Brain, behavior, and immunity. 2020;83:78-86.
- Šimundić A-M. Measures of diagnostic accuracy: basic definitions. ejifcc. 2009;19(4):203.
Figure 2.
Serum kappa light chain (S. k-FLC) concentrations in the studied groups (Non, Mild, and Severe) of proteinuria (* p<0.05).
Figure 2.
Serum kappa light chain (S. k-FLC) concentrations in the studied groups (Non, Mild, and Severe) of proteinuria (* p<0.05).
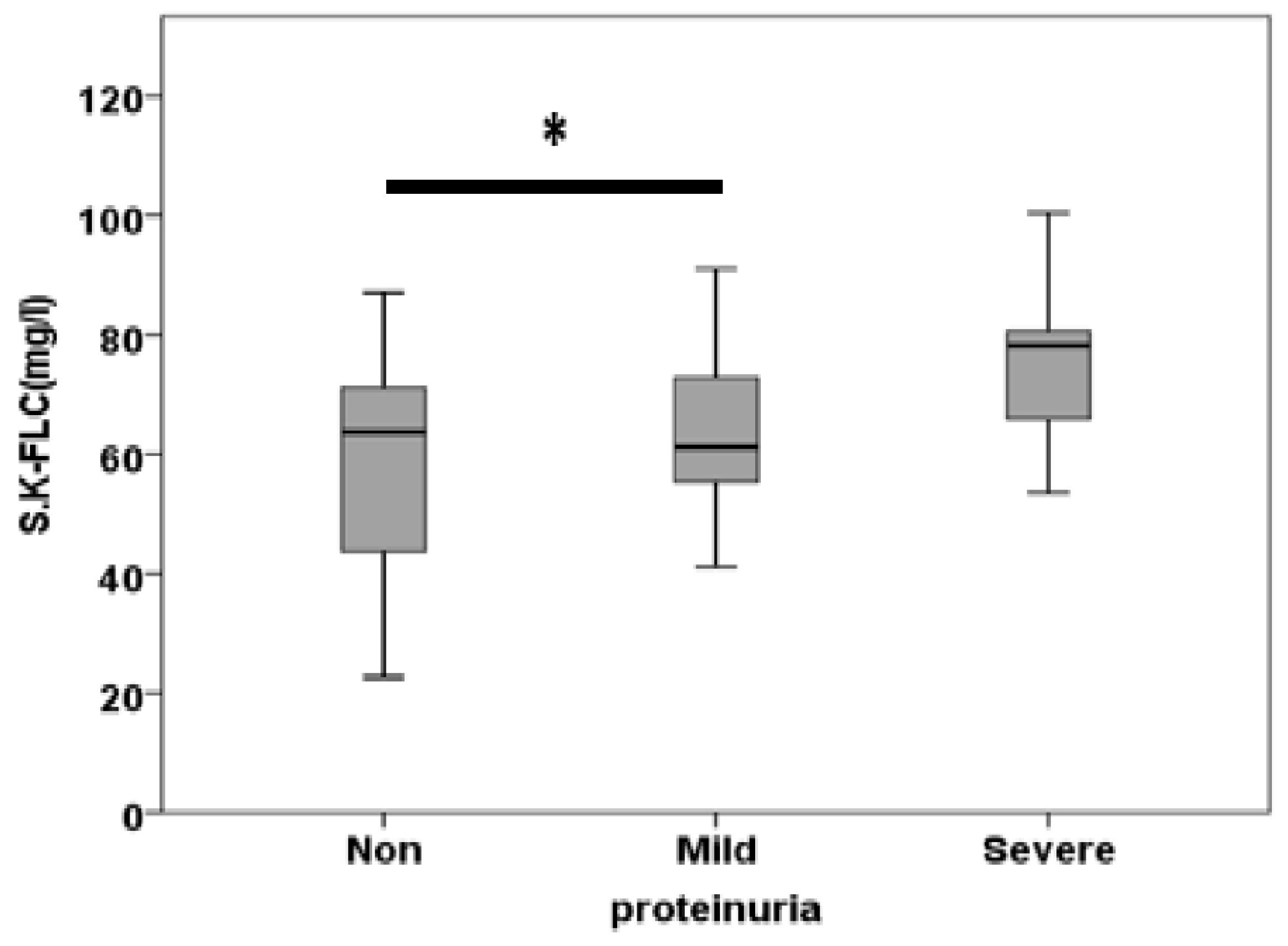
Figure 3.
Serum lambda free light chain (S. l-FLC) concentrations in the studied groups (Non, Mild, and Severe) of proteinuria (* p<0.05).
Figure 3.
Serum lambda free light chain (S. l-FLC) concentrations in the studied groups (Non, Mild, and Severe) of proteinuria (* p<0.05).
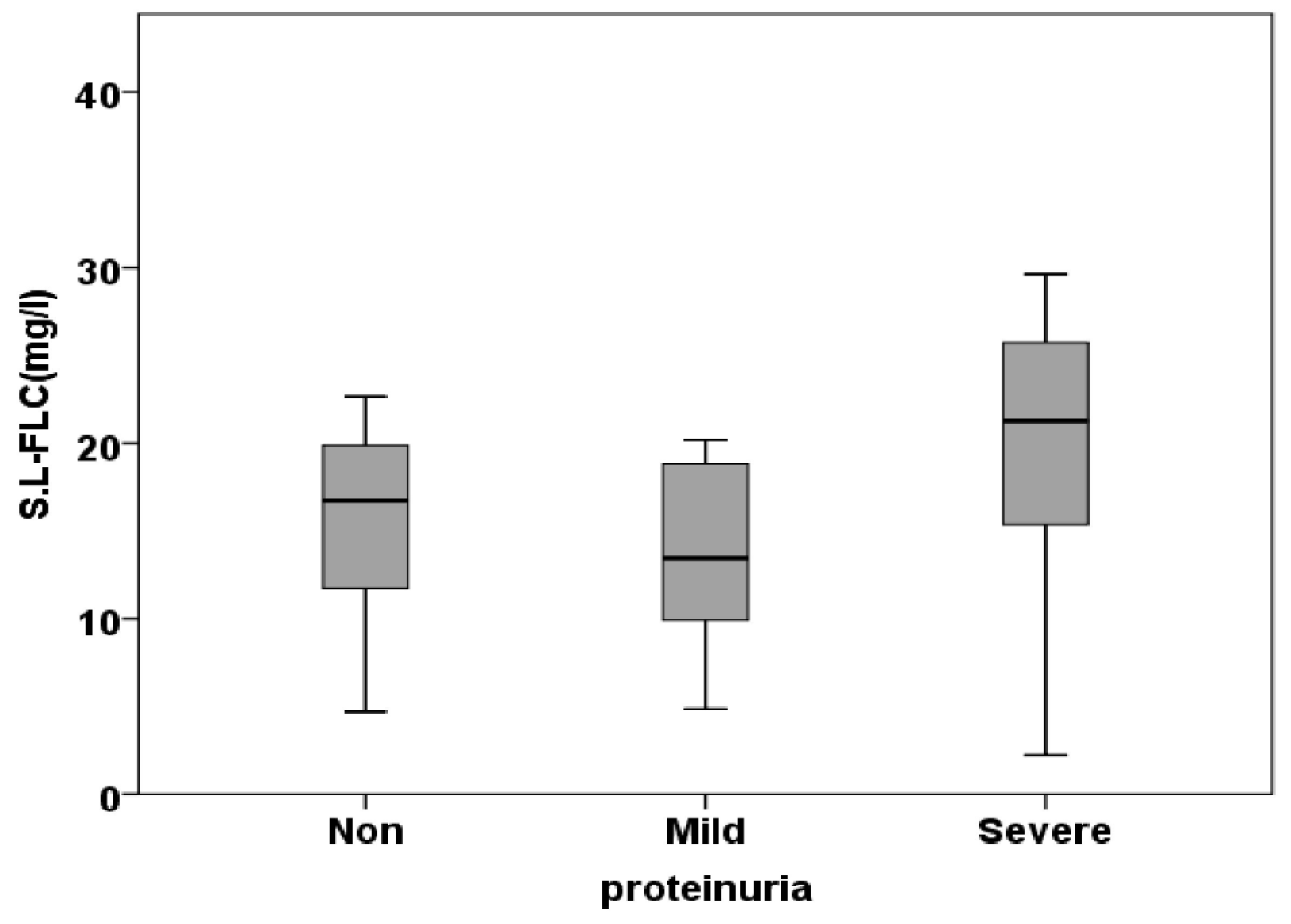
Figure 4.
Serum kappa/lambda free light chain ratio (S. k/l Ratio) concentrations in the studied groups (Non, Mild, and Severe) of proteinuria (* p<0.05).
Figure 4.
Serum kappa/lambda free light chain ratio (S. k/l Ratio) concentrations in the studied groups (Non, Mild, and Severe) of proteinuria (* p<0.05).
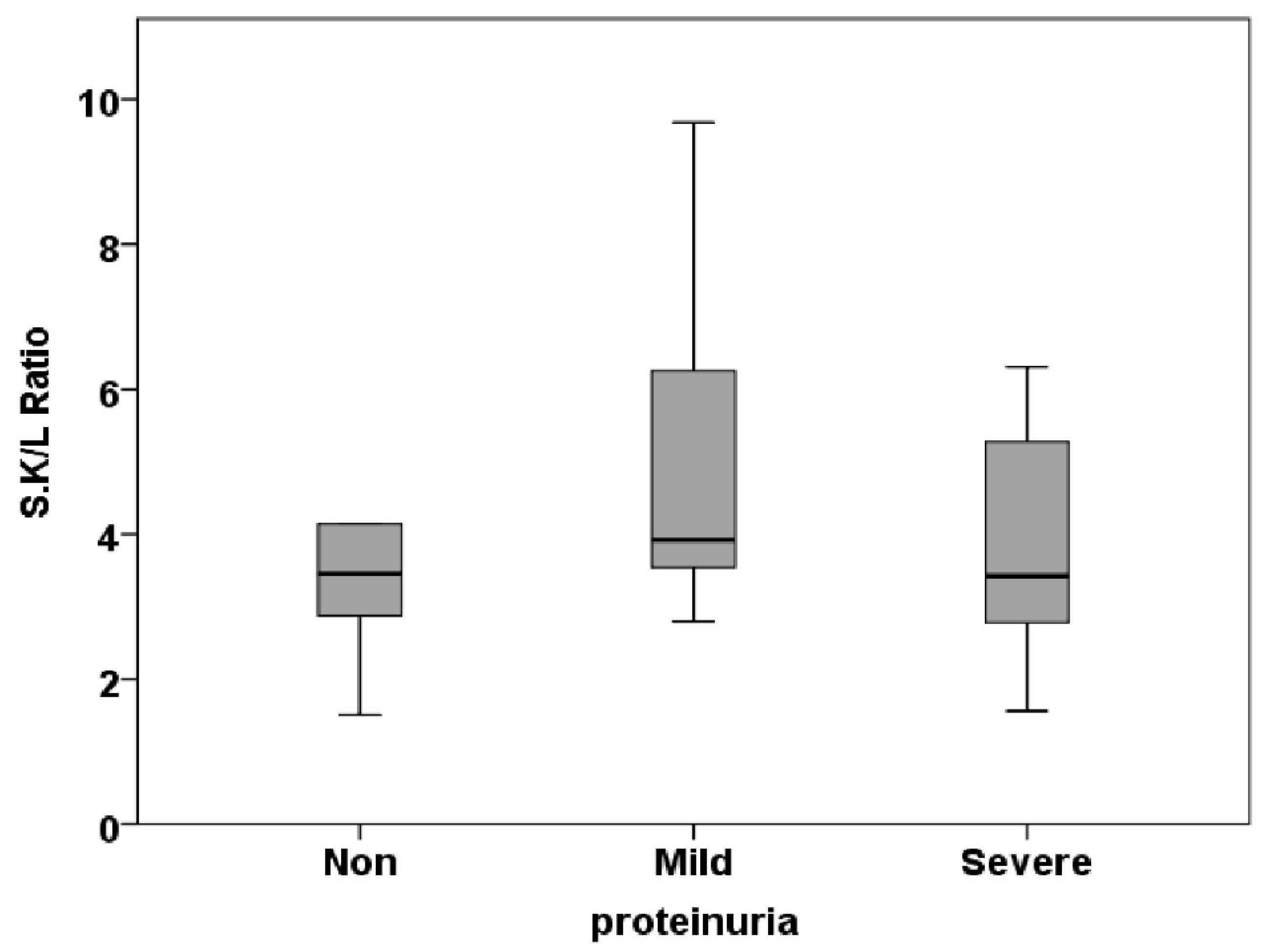
Figure 5.
Saliva kappa free light chain (SA. k-FLC) concentrations in the studied groups (Non, Mild, and Severe) of proteinuria (* p<0.05).
Figure 5.
Saliva kappa free light chain (SA. k-FLC) concentrations in the studied groups (Non, Mild, and Severe) of proteinuria (* p<0.05).
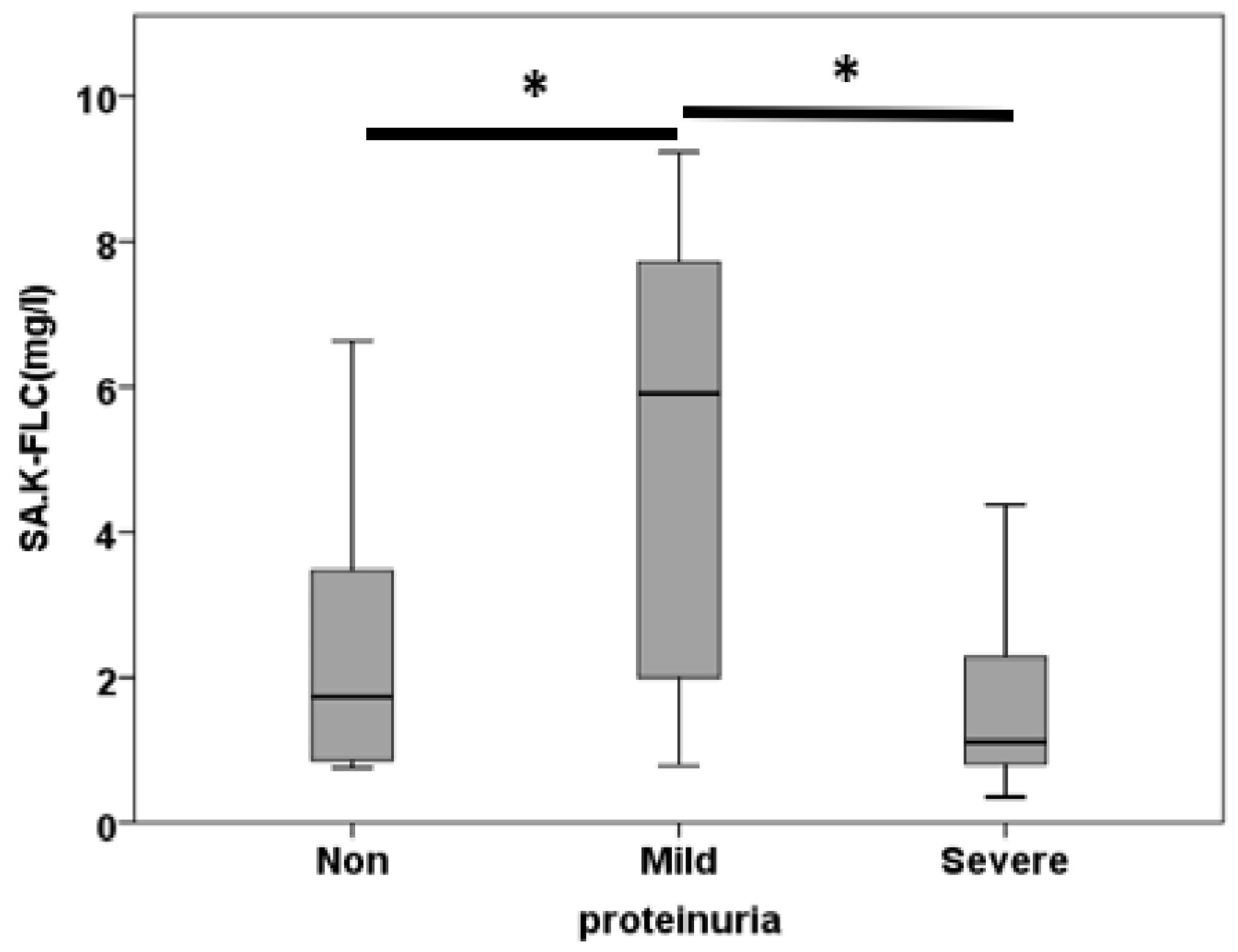
Figure 6.
Saliva lambda free light chain (SA. l-FLC) concentrations in the studied groups (Non, Mild, and Severe) of proteinuria (* p<0.05).
Figure 6.
Saliva lambda free light chain (SA. l-FLC) concentrations in the studied groups (Non, Mild, and Severe) of proteinuria (* p<0.05).
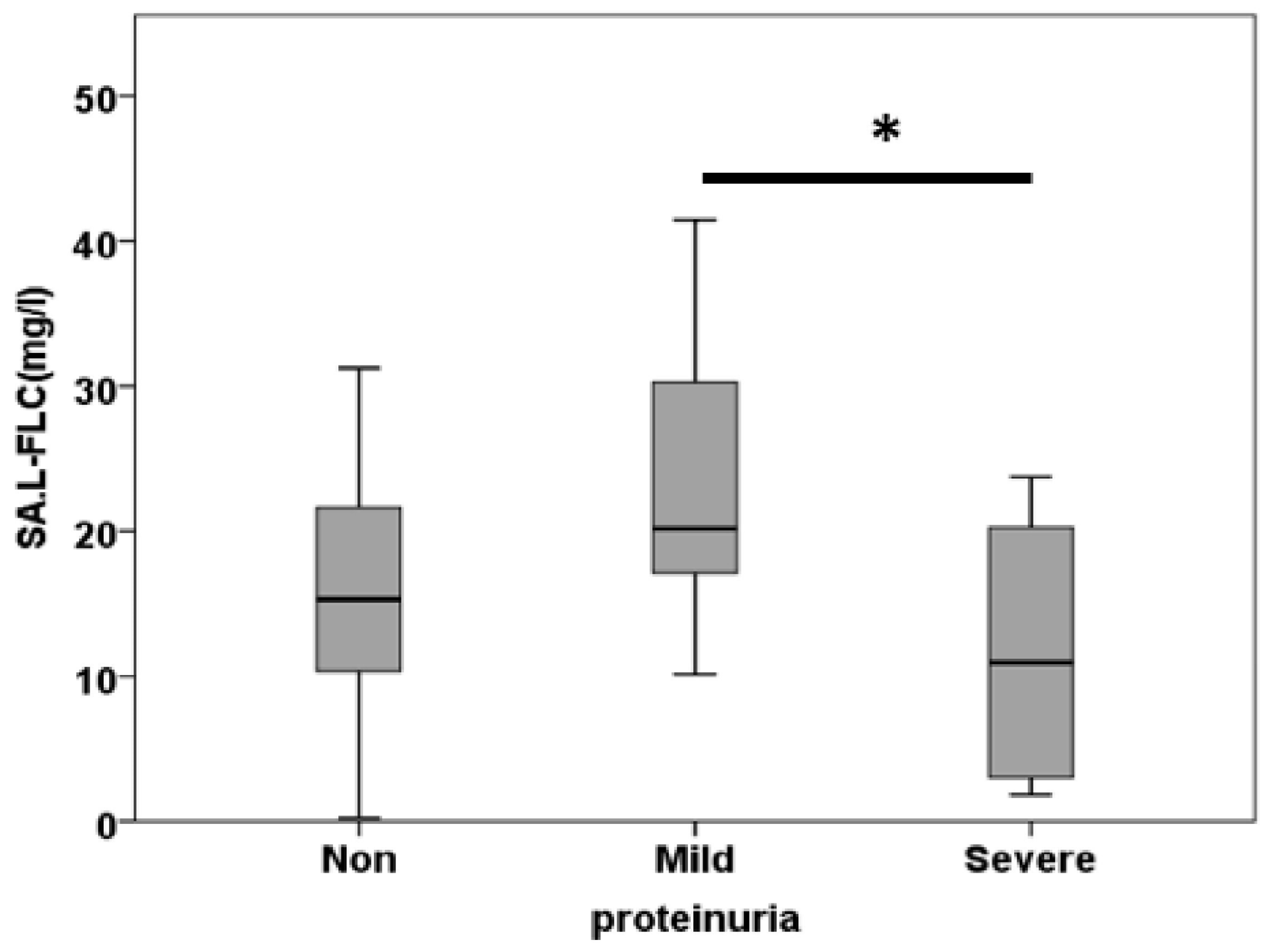
Figure 7.
Saliva kappa/ lambda free light chain ratio (SA. k/l Ratio) concentrations in the studied groups (Non, Mild, and Severe) of proteinuria (* p<0.05).
Figure 7.
Saliva kappa/ lambda free light chain ratio (SA. k/l Ratio) concentrations in the studied groups (Non, Mild, and Severe) of proteinuria (* p<0.05).
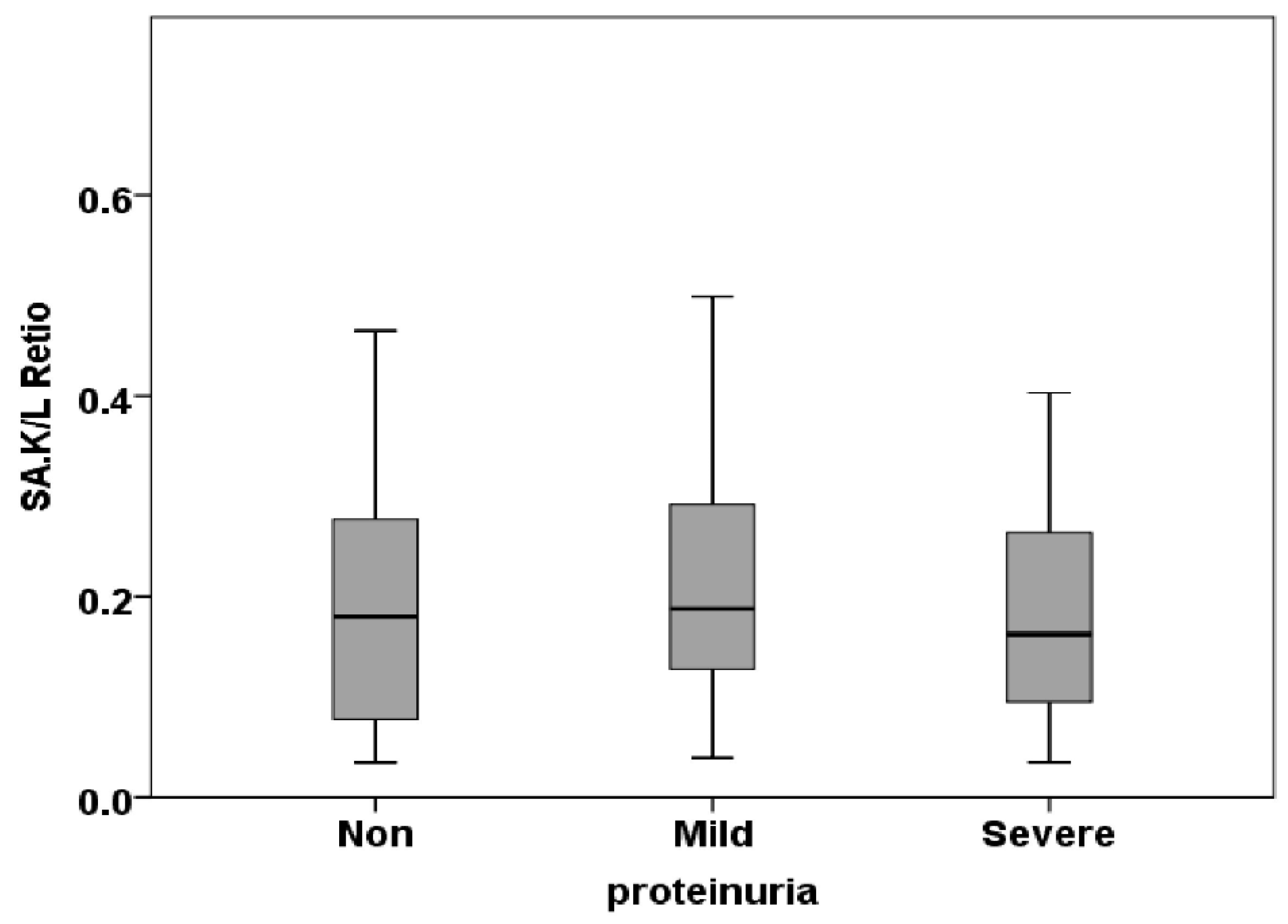
Figure 8.
Receiver Operating Characteristic (ROC) curves to discriminate between non-proteinuria and mild proteinuria for kappa (A), lambda (B), and the kappa/ lambda ratio (C) in serum; kappa (D), lambda (E), and the kappa/ lambda ratio (F) in saliva.
Figure 8.
Receiver Operating Characteristic (ROC) curves to discriminate between non-proteinuria and mild proteinuria for kappa (A), lambda (B), and the kappa/ lambda ratio (C) in serum; kappa (D), lambda (E), and the kappa/ lambda ratio (F) in saliva.
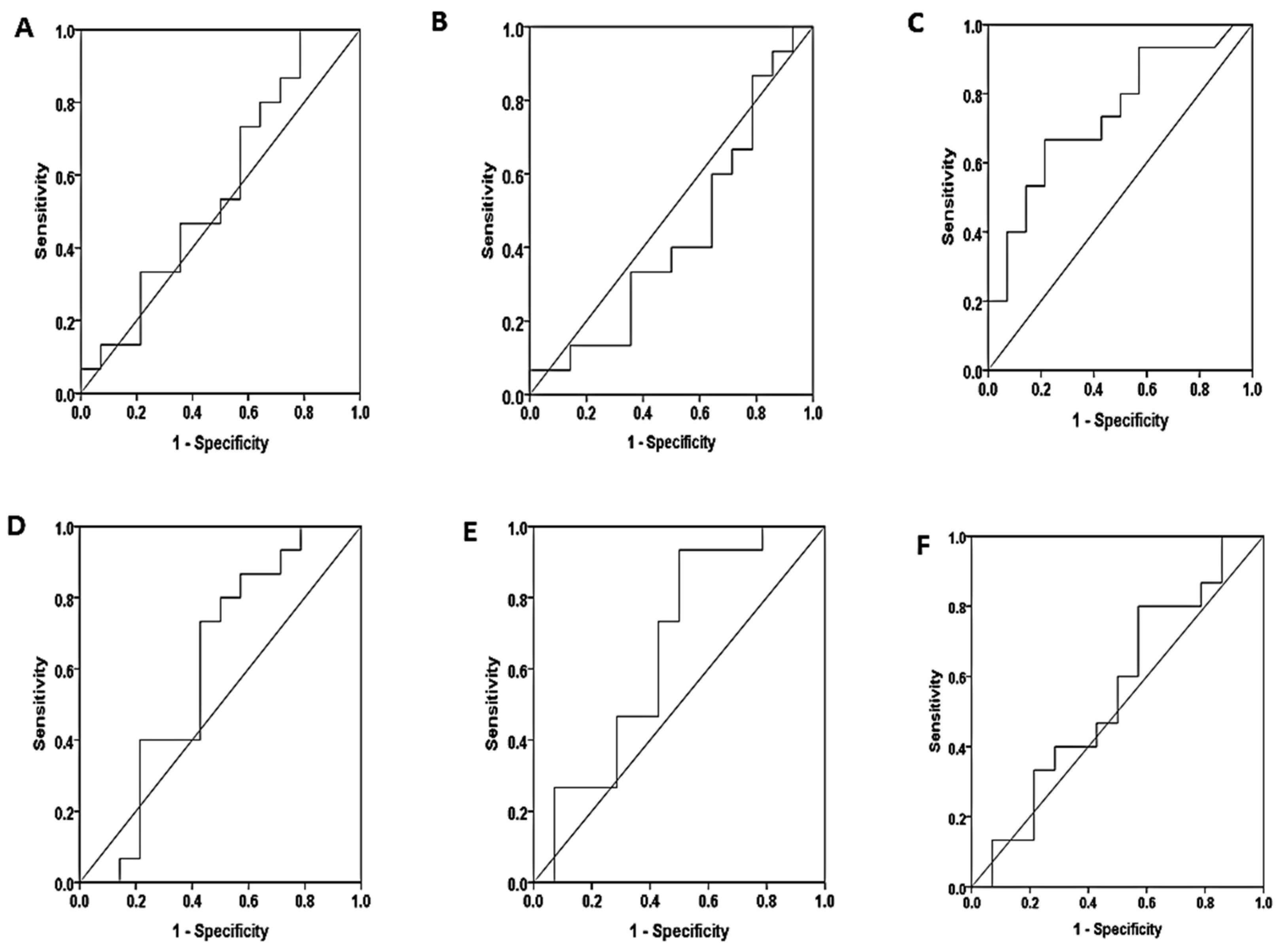
Figure 9.
Receiver Operating Characteristic (ROC) curves to discriminate between non-proteinuria and severe proteinuria for kappa (A), lambda (B), and the kappa/ lambda ratio (C) in serum; kappa (D), lambda (E), and the kappa/ lambda ratio (F) in saliva.
Figure 9.
Receiver Operating Characteristic (ROC) curves to discriminate between non-proteinuria and severe proteinuria for kappa (A), lambda (B), and the kappa/ lambda ratio (C) in serum; kappa (D), lambda (E), and the kappa/ lambda ratio (F) in saliva.
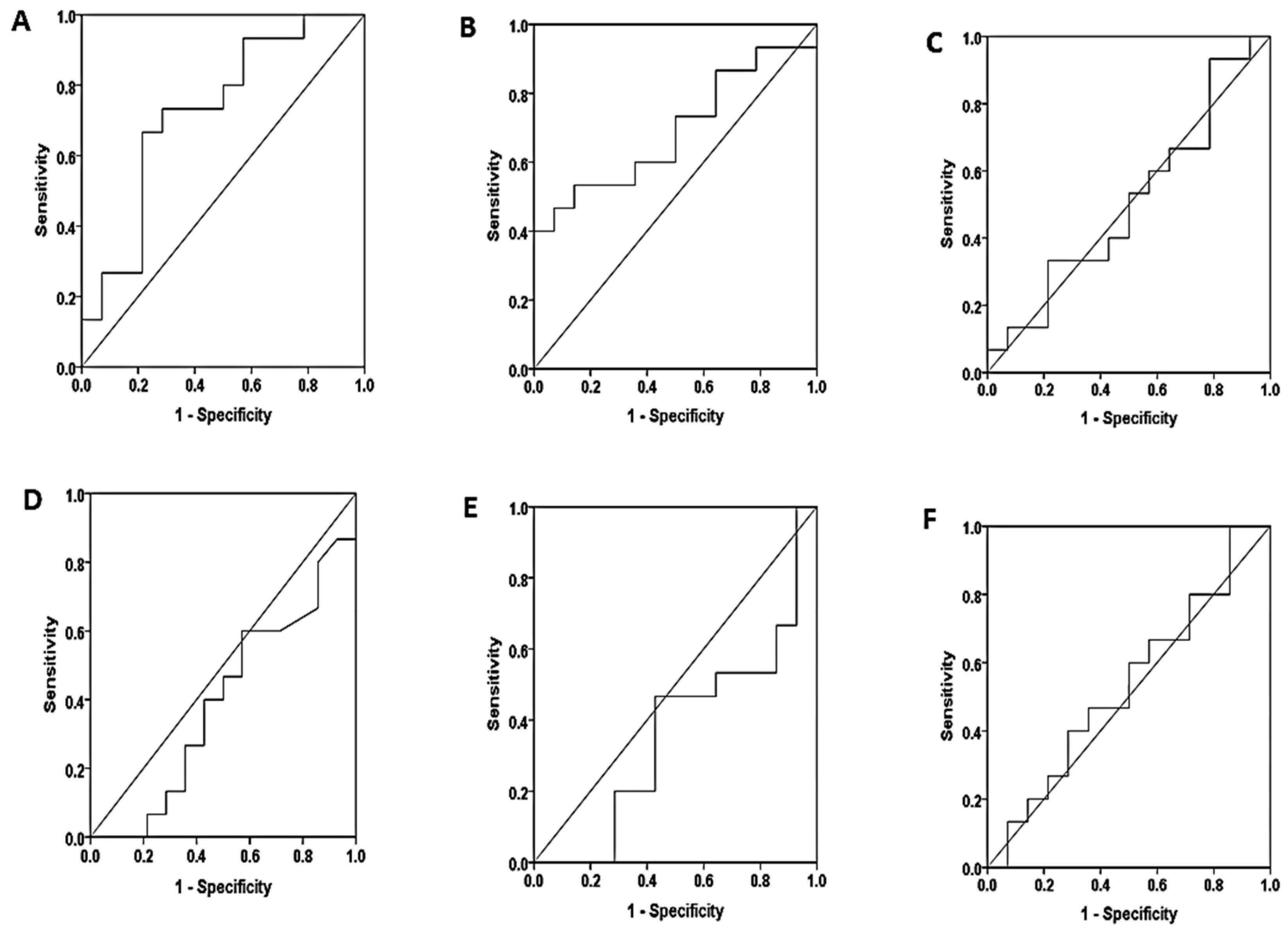
Figure 10.
Receiver Operating Characteristic (ROC) curves to discriminate between mild proteinuria and severe proteinuria for kappa (A), lambda (B), and the kappa/ lambda ratio (C) in serum; kappa (D), lambda (E), and the kappa/ lambda ratio (F) in saliva.
Figure 10.
Receiver Operating Characteristic (ROC) curves to discriminate between mild proteinuria and severe proteinuria for kappa (A), lambda (B), and the kappa/ lambda ratio (C) in serum; kappa (D), lambda (E), and the kappa/ lambda ratio (F) in saliva.
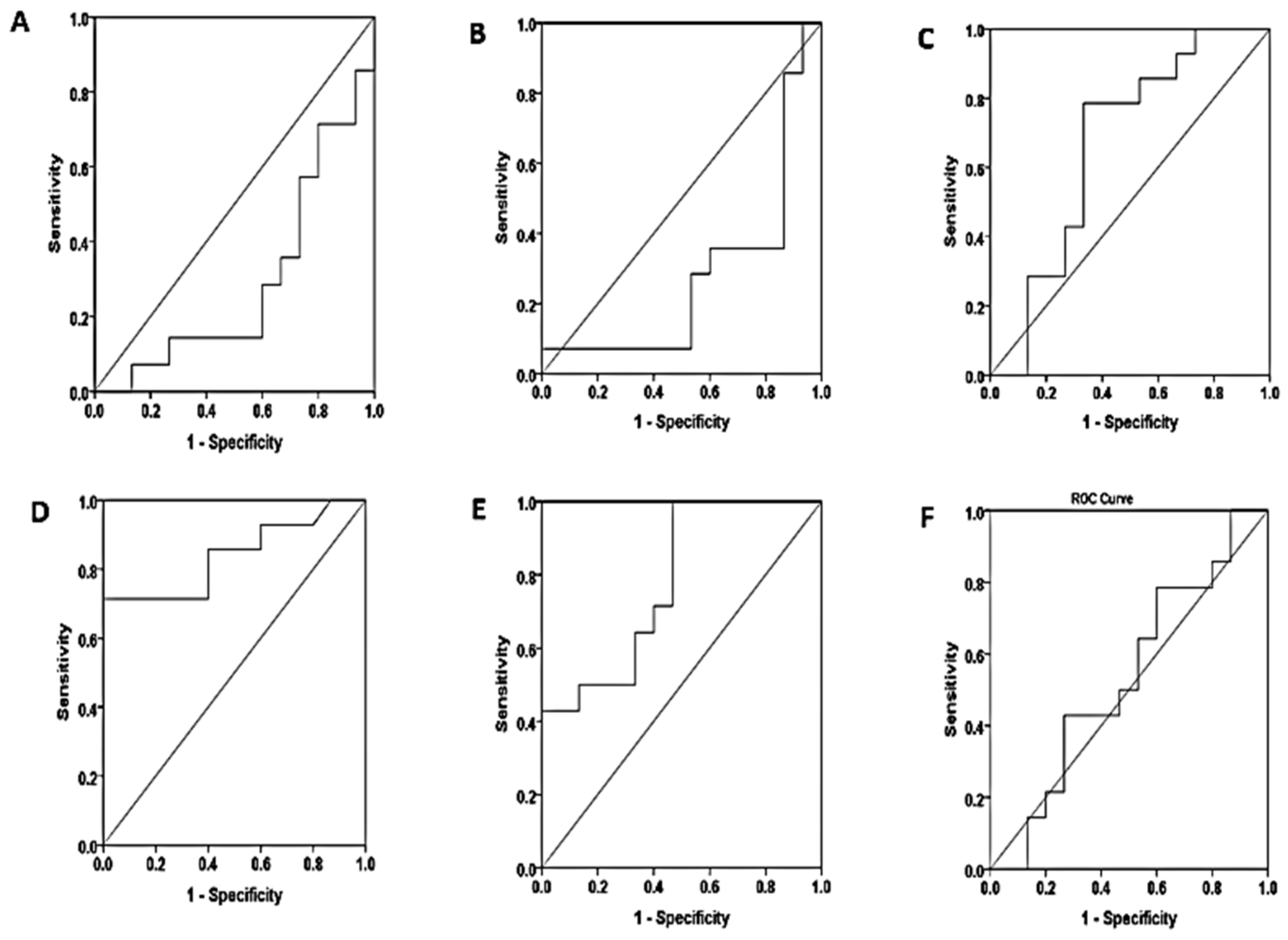

Table 1.
Anthropometric characteristics of the study population.
| Characteristics, N (%) | Total |
No proteinuria N=72 |
Mild proteinuria N=27 |
Severe proteinuria N=50 |
P value |
| Demographic | |||||
| Male | 89(59.7) | 42(58.33) | 20(74.07) | 27(54) | 0.218 |
| Female | 60(40.3) | 30(41.67) | 7(25.93) | 23(46) | |
| Age (year) | 51.57 ± 10.207 | 56.63 ± 10.724 | 53.520 ± 8.858 | 0.075 | |
| Age groups | |||||
| <39 | 15(10) | 11(15.3) | 2(7.4) | 2(4.0) | 0.076 |
| 40 – 49 | 38(25.5) | 20(27.8) | 4(14.8) | 14(28.0) | |
| 50 – 59 | 57(38) | 24(33.3) | 10(37.0) | 23(46.0) | |
| 60 – 69 | 32(21.5) | 15(20.8) | 7(25.9) | 10(20.0) | |
| >70 | 7(4.5) | 2(2.8) | 4(14.8) | 1(2.0) | |
| BMI(kg/m2) | 27.776 ± 4.136 | 27.269 ± 4.101 | 28.674 ± 4.693 | 0.339 | |
| Name of hospital | |||||
| IbnALBAYTAR | 95(63.7) | 45(62.5) | 17(63) | 33(66.0) | 0.938 |
| Ghazi Alhariri.H | 38(25.5) | 18(25.0) | 8(29.6) | 12(24.0) | |
| Outpatients | 16(10.7) | 9(12.5) | 2(7.4) | 5(10.7) | |
| Type of operation | |||||
| CABG | 66(44.3) | 29(40.3) | 14(51.9) | 23(46.0) | 0.716 |
| AVR | 79(53) | 41(56.9) | 13(48.1) | 25(50.0) | |
| CABG & AVR | 4(2.6) | 2(2.8) | 0(0.0) | 2(4.0) | |
| Comorbidities | |||||
| No Disease | 81(54) | 41(56.9) | 14(51.9) | 26(52) | 0.800 |
| With comorbidities | 68(45) | 31(43.1) | 13(48.1) | 24(48) | |
| DM | 14(20.5) | 5(6.9) | 3(11.1) | 6(12.0) | |
| Hypertension | 19(27.9) | 10(13.9) | 2(7.4) | 7(14.0) | |
| DM & Hypertension | 27(39.7) | 11(15.3) | 7(25.9) | 9(18) | |
| Thyroid | 3(4.4) | 1(1.4) | 0(0) | 2(4.0) | |
| Rheumatoid | 4(5.8) | 3(4.2) | 1(3.7) | 0(0) | |
| Hyperlipidemia | 1(1.4) | 1(1.4) | 0 | 0 | |
| Smoking status | |||||
| Smoking | 19(13) | 10(13.9) | 5(18.8) | 4(8) | 0.386 |
| Non smoking | 130(87) | 62(86.1) | 22(81.5) | 46(92.0) | |
| Other operations | |||||
| No preoperation | 129(86.6) | 60(83.3) | 24(88.9) | 45(90) | 0.784 |
| With preoperation | 20(13.4) | 12(16.6) | 3(11.1) | 5(10) | |
| Gall stone | 2(2.8) | 0(0) | 0(0) | ||
| tonsillectomy | 2(2.8) | 0(0) | 0(0) | ||
| Liver injury | 1(1.4) | 0(0) | 0(0) | ||
| thyroidectomy | 0(0) | 0(0) | 1(2.0) | ||
| Therapeutic cathetarization | 2(2.8) | 1(3.7) | 0(0) | ||
| appendix | 2(2.8) | 0(0) | 1(2.0) | ||
| ulcer | 1(1.4) | 1(3.7) | 0(0) | ||
| sinus | 1(1.4) | 0(0) | 1(2.0) | ||
| hernia | 0(0) | 1(3.7) | 2(4.0) | ||
| Abdominal injury | 1(1.4) | 0(0) | 0(0) | ||
| Residency | |||||
| Baghdad | 100(67.1) | 43(59.7) | 20(74.1) | 37(74.0) | 0.075 |
| Al-Anbar | 26(17.45) | 15(20.8) | 4(14.8) | 7(14.0) | |
| Deyala | 7(4.7) | 5(6.9) | 1(3.7) | 1(2.0) | |
| Karbalaa | 5(3.3) | 4(5.6) | 0(0.0) | 1(2.0) | |
| Wasit | 3(2.0) | 1(1.4) | 0(0.0) | 2(4.0) | |
| Salahaddin | 4(2.6) | 3(4.2) | 0(0.0) | 1(2.0) | |
| Neynava | 3(2.0) | 1(1.4) | 2(7.4) | 0(0.0) | |
| Missan | 1(0.67) | 0(0.0) | 0(0.0) | 1(2.0) | |
| Date of sample collection(after operation) | |||||
| 1 week | 95(63.7) | 7(9.7) | 3(11.1) | 4(8.0) | 0.131 |
| 2 week | 5(6.9) | 7(25.9) | 7(14.0) | ||
| 1 month | 13(18.1) | 3(11.1) | 7(14.0) | ||
| 3 month | 16(22.2) | 1(3.7) | 4(8.0) | ||
| 6 month | 9(12.5) | 1(3.7) | 8(16.0) | ||
| 1year | 54(36.3) | 17(23.6) | 9(33.3) | 17(34.0) | |
| Above 1 year | 5(6.9) | 3(11.1) | 3(6.0) | ||
| eGFR | |||||
| Normal (>90 ml/min) | 104(69.7) | 60(83.3) | 18(66.7) | 26(52.0) | 0.341 |
| Mild (60-90 ml/min) | 40(26.8) | 12(16.7) | 9(33.3) | 19(38.0) | |
| Moderate (30-60 ml/min) | 5(3.3) | 0(0.0) | 0(0.0) | 5(10.0) | |
| Severe (<30 ml/min) | 0(0.0) | 0(0.0) | 0(0.0) | ||
| Prognosis | |||||
| AKI | 46(30.1) | 9(12.5) | 9(33.3) | 28(56) | 0.378 |
| No AKI | 103(69.9) | 63(87.5) | 18(66.7) | 22(44) | |
| Baseline laboratory indices | |||||
| B.Urea (mg/dl) | 37.313 ± 15.790 | 42.092 ± 14.279 | 50.838 ± 24.682 | 0.001 | |
| S.Creatinine (mg/dl) | 0.912 ± 0.264 | 1.036 ± 0.256 | 1.332 ± 0.645 | 0.000 | |
| S.Protein (g/l) | 69.138 ± 11.105 | 65.967 ± 9.336 | 61.983 ± 17.270 | 0.015 | |
| S.Albumin (mg/l) | 43.199 ± 7.188 | 38.444 ± 7.973 | 36.538 ± 6.278 | 0.000 | |
| Urea in urine (mg) | 1444.98±472.15 | 1386.2±527.77 | 1215.3±643.77 | 0.073 | |
| Creatinine in urine (mg) | 643.41 ± 324.40 | 445.07 ± 280.58 | 261.11 ± 211.39 | 0.000 | |
| Protein in urine (mg) | 11.663 ± 6.720 | 23.919 ± 9.944 | 53.886 ± 69.344 | 0.000 | |
| Protein/Cr Ratio in urine | 39.527 ± 76.743 | 95.369 ± 82.849 | 340.4±383.765 | 0.000 | |
BMI: body mass index, eGFR: estimated glomerular filtration rate, CABG: coronary artery bypass graft, AVR: aortic valve replacement, DM: diabetes Meletus. The data is presented as number(percentage) for categorical variables and mean ± standard deviation (SD) for continuous variables. Cross tabulation & ANOVA were employed as statistical methods for analysis.
Table 2.
The concentration of serum free light chain with the severity of proteinuria.
| Characteristics | No proteinuria N=14 |
Mild proteinuria (trace, +1) N=15 |
Severe proteinuria (+2, +3) N=15 |
P value |
|---|---|---|---|---|
| S.K.FLC (mg/l) | 59.37±4.97 | 63.32±3.75 | 74.46±3.94 | 0.042 |
| S.L.FLC (mg/l) | 15.24±1.56 | 14.63±1.78 | 19.59±2.01 | 0.115 |
| S.K/L Ratio | 0.50±0.10 | 0.51±0.06 | 0.63±0.21 | 0.799 |
The data is presented as mean ± standard error. S.K.FLC: serum kappa Free Light Chain, S.L.FLC: serum lambda Free Light Chain, S.K/L Ratio: serum kappa/lambda Ratio.
Table 3.
The concentration of salivary free light chain with the severity of proteinuria.
| Characteristics | No proteinuria N=14 |
Mild proteinuria (trace , +1) N=15 |
Severe proteinuria (+2 , +3) N=15 |
P value |
|---|---|---|---|---|
| SA.K.FLC (mg/l) | 2.68±0.65 | 5.20±0.80 | 1.74±0.29 | 0.001 |
| SA.L.FLC (mg/l) | 26.54±10.83 | 25.29±3.32 | 11.99±2.31 | 0.005 |
| SA. k/l Ratio | 0.04±0.02 | 0.02±0.003 | 0.03±0.008 | 0.485 |
The data is presented as mean ± standard error. SA.K.FLC: saliva kappa Free Light Chain, SA.L.FLC: saliva lambda Free Light Chain, SA.K/L Ratio: saliva kappa/lambda Ratio.
Table 4.
Diagnostic performance of free light chains to predict patient developed AKI.
| Marker | sensitivity | specificity | Cutoff value | area | sig | |
| Non proteinuria – Mild proteinuria | ||||||
| serum | S.K.FLC | 73.3% | 42.9% | 56.01 | 0.562 | 0.570 |
| S.L.FLC | 86.7% | 21.4% | 7.71 | 0.433 | 0.541 | |
| S.K/l ratio | 80.0% | 50.0% | 0.33 | 0.605 | 0.337 | |
| saliva | SA.K.FLC | 66.7% | 64.3% | 2.83 | 0.740 | 0.028 |
| SA.L.FLC | 80.0% | 50.0% | 16.03 | 0.657 | 0.150 | |
| SA.K/l ratio | 73.3% | 42.9% | 0.012 | 0.552 | 0.631 | |
| Non proteinuria – Severe proteinuria | ||||||
| serum | S.K.FLC | 73.3% | 57.1% | 66.73 | 0.724 | 0.040 |
| S.L.FLC | 73.3% | 42.9% | 15.11 | 0.690 | 0.081 | |
| S.K/L ratio | 60.0% | 42.90% | 0.31 | 0.505 | 0.965 | |
| saliva | SA.K.FLC | 60% | 35.7% | 0.92 | 0.393 | 0.326 |
| SA.L.FLC | 53.3% | 35.7% | 10.65 | 0.362 | 0.206 | |
| SA.K/L ratio | 66.7% | 42.9% | 0.01 | 0.553 | 0.760 | |
| Mild proteinuria – Severe proteinuria | ||||||
| serum | S.K.FLC | 50.0% | 26.7% | 640.01 | 0.290 | 0.055 |
| S.L.FLC | 35.7% | 40.0% | 18.27 | 0.276 | 0.040 | |
| S.K/L ratio | 85.7% | 46.7% | 0.32 | 0.667 | 0.127 | |
| saliva | SA.K.FLC | 71.4% | 86.7% | 3.08 | 0.840 | 0.002 |
| SA.L.FLC | 92.9% | 53.3% | 14.91 | 0.781 | 0.010 | |
| SA.K/L ratio | 78.6% | 40.0% | 0.01 | 0.533 | 0.760 | |
S.K.FLC: serum kappa Free Light Chain, S.L.FLC: serum lambda Free Light Chain, S.K/L Ratio: serum kappa/lambda Ratio, SA.K.FLC: saliva kappa Free Light Chain, SA.L.FLC: saliva lambda Free Light Chain, SA.K/L Ratio: saliva kappa/lambda Ratio.
Table 5.
Pearson’s correlation between saliva and serum in terms of free light chain.
| Saliva | |||||
| serum | K.FLC | L.FLC | K/L ratio | ||
| K.FLC | -0.306* | -0.097 | -0.415** | Pearson Correlation | |
| 0.043 | 0.533 | 0.005 | Sig. (2-tailed) | ||
| L.FLC | -0.334* | -0.063 | 0.011 | Pearson Correlation | |
| 0.027 | 0.686 | 0.944 | Sig. (2-tailed) | ||
| K/L ratio | 0.010 | -0.078 | -0.110 | Pearson Correlation | |
| 0.950 | 0.615 | 0.478 | Sig. (2-tailed) | ||
K.FLC: kappa Free Light Chain, L.FLC: lambda Free Light Chain, K/L Ratio: kappa/lambda Ratio.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



