Submitted:
10 May 2024
Posted:
13 May 2024
You are already at the latest version
Abstract
: We report the case of a 2-year-old Norwegian Forest cat diagnosed with pulmonary edema and pulmonary hypertension (PH) secondary to cor triatriatum sinister, who showed improved breathing following furosemide treatment. Sildenafil was prescribed post-discharge without diuretic. Thirty-eight days later, no abnormalities were observed in the septum or accessory chamber of the left atrium; however, continuous mosaic blood flow (maximum velocity, 3.14 m/s) was observed in two enlarged pulmonary veins. Pulmonary artery enlargement (main pulmonary artery to thoracic aorta ratio: 1.90), pulmonary vein stenosis (PVS), and diffuse bilateral ground-glass lung opacities were observed using computed tomography. PH with partial PVS and pulmonary parenchymal disease was diagnosed. The cat was further treated with furosemide with no clinical symptoms, but succumbed to acute dyspnea 51 days after the first visit. PH, despite partial PVS, may also be associated with concurrent parenchymal lung disease. Sildenafil can worsen pulmonary edema in the affected lung but did not in this case.
Keywords:
Pulmonary edema
; Pulmonary hypertension
; Case report
; Computed Tomography
; Echocardiography
1. Introduction
Pulmonary hypertension (PH) in cats is relatively challenging to detect [1,2]. Pulmonary venous stenosis (PVS) is rare in cats and can lead to PH. However, only one previous study has reported a case of PVS and resultant PH in cats, and this diagnosis was obtained post-mortem [3]. Here, we report a case of feline PH secondary to congenital PVS and parenchymal lung disease detected using echocardiography and computed tomography (CT). If PH is caused by either of these conditions, pulmonary vasodilators may exacerbate the condition. However, in this case, sildenafil administration did not cause disease state worsening. Thus, we report a case suspected as congenital PVS diagnosed during the cat’s lifetime via imaging with sildenafil administration that did not exacerbate the condition.
2. Case Description
A 2-year-old, spayed, female Norwegian Forest cat (4.94 kg, body condition score: 4/9) presented with anorexia and dyspnea. The cat was diagnosed with PH/pulmonary edema secondary to cor triatriatum sinister. On day 1, 2 mg/kg furosemide was administered subcutaneously twice, and the patient was hospitalized overnight. The following day, arterial blood gas analysis revealed oxygen and carbon dioxide partial pressures of 62.9 mmHg and 36.9 mmHg, respectively. The patient was discharged and treated with sildenafil (0.69 mg/kg, bis in die [BID], per os [PO]) alone. After discharge, the patient had occasional collapse and pre-syncope, but during a follow-up visit 1 week later, improvements in breathing and appetite were observed.
As thoracic radiography revealed residual pulmonary opacities, the sildenafil dose was increased to 1.09 mg/kg BID. After another week, the patient’s respiratory status improved completely, and activity improved without pre-syncope. However, the sildenafil dose was increased to 1.63 mg/kg BID because of residual abnormal pulmonary opacities in the right cranial lung field. Subsequently, pre-syncope or collapse were not observed, and pulmonary opacities reduced markedly on thoracic radiography (Figure 1). The patient was additionally treated with rivaroxaban (2.5 mg/head, semel in die [SID]).
Thirty-eight days after the initial clinical manifestations, the cat was referred to the Department of Cardiology and Respiratory Medicine at our animal hospital for a detailed examination. At the time of presentation to our facility, its health status was improving (weight, 4.94 kg; body condition score, 4/9). The patient’s vital signs were recorded (body temperature, 38.1°C; respiratory rate, 78 breaths/min; heart rate, 180 beats/min; and no heart or secondary murmurs). The average systolic blood pressure assessed using the Doppler method was 124 mmHg. Thoracic radiography revealed an anterior lobe alveolar pattern with a vertebral heart scale of 8.2 and mild cardiac enlargement. Transthoracic echocardiography was performed using an ultrasound unit (Vivid E9; GE Healthcare Co., Ltd., Tokyo, Japan) with 6- to 12-MHz phased-array transducers. Transthoracic echocardiography revealed right cardiac enlargement, pulmonary artery dilatation, ventricular septum systolic flattening, and an increased pulmonary artery to aortic ratio (MPA/Ao: 1.36; normal range: < 1.0) [1,2], indicating moderate PH (Figure 2). No abnormal septum was observed in the left atrium, and two pulmonary veins had stenosis at their inflow with increased blood flow velocities (2.42 m/s and 3.14 m/s, respectively). The distal lumens of the stenosis were dilated (Figure 3). Computed tomography (CT) scans (Aquilion Prime SP; Canon Medical Systems Corporation, Tochigi, Japan) were obtained with a non-ionic contrast agent (Iohexol 300 mg; dose, mL/kg) intravenously injected under anesthesia, and images were captured over a duration of 15 s. Triphasic angiography was used for the evaluation of pulmonary and cardiac structures. CT revealed stenosis in the right cranial and middle pulmonary veins, pulmonary artery enlargement (main pulmonary artery to thoracic aorta ratio: 1.90 [Figure 4]; normal rage: < 1.0) [2,4], and consolidation in the right cranial and middle pulmonary lobes. Moreover, ground-glass opacities (−300 to −100 Hounsfield units [HU], Figure 5) were observed in the lung parenchyma (−500 and −600 HU), pulmonary vessels (approximately 150 HU), and bronchial walls (approximately 100 HU). Consequently, segmental PH due to partial PVS was diagnosed. We also diagnosed the cat with a possible pulmonary parenchymal disease based on the CT findings, which contributed to severe PH in addition to partial PVS in the right cranial and middle lung lobes.
When informed of the poor prognosis, the owner did not agree to a lung biopsy. As we suspected pulmonary edema from the CT findings, we prescribed 1 mg/kg BID oral furosemide (Lasix 10 mg tablet; Sanofi KK, Tokyo, Japan) and requested the referring doctor to prescribe sildenafil and rivaroxaban. The patient visited our hospital only once, and its condition was good with no syncope or dyspnea thereafter. However, the patient had acute dyspnea and died of pulmonary edema 51 days after the last hospital visit. An autopsy could not be performed because the owner did not provide consent.
3. Discussion
PVS is a rare cardiovascular disease; till date, only one veterinary case report of a Maine coon cat with congenital PVS confirmed using echocardiography and autopsy after ethical euthanasia has been reported [3]. PVS is a rare congenital or acquired cardiovascular disease, even in humans [5]. Although it depends on the number of pulmonary veins with stenosis and the degree of stenosis, PVS-induced pulmonary edema and PH contribute to high morbidity and mortality in infants and young children [6,7]. PVS was previously recognized as a postoperative complication of congenital heart disease, including anomalous pulmonary venous return in infants or children; however, it has also been reported to be associated with parenchymal lung disease, including bronchopulmonary dysplasia secondary to premature birth (< 37 weeks) [5,8]. Additionally, PVS has been recently reported as a complication after the ablation of atrial fibrillation [6,9]. Congenital PVS is characterized by stenosis at the pulmonary vein ostia, whereas cor triatriatum sinister is identified by an abnormal septum in the left atrial cavity [4].
The PVS in the present case was likely congenital, as the patient was relatively young. However, in a young cat with severe PH due to congenital PVS in a previous report, an autopsy revealed stenosis in all pulmonary veins except the left cranial pulmonary vein [4]. Cats have two types of right cranial and middle pulmonary vein ostia: those that join at the common trunk and those that independently flow into the pulmonary venous drainage system [10]. In the present case, the right cranial and middle pulmonary veins independently flowed into the left atrium, both of which were stenotic. The maximum blood flow velocity in the stenotic ostium in the present case was 3.14 m/s, which is a diagnostic for PVS in humans with a blood flow velocity of 1.1–1.5 m/s [11,12]. As a prior study in cats with PVS revealed severe PVS with a blood flow velocity of 2.6 m/s [4], the present case likely had severe PH in the affected lungs. However, unlike the previous report, this case only had stenosis of the right cranial and middle pulmonary veins, which may have resulted in a relatively long survival. Furthermore, the cat had complete flattening of the ventricular septum during systole, indicating the possibility of severe PH [13]. However, the association of severe PH with the involvement of just two pulmonary vein stenoses remained questionable. In humans, segmental PH is described as pulmonary vascular remodeling and pulmonary hypertension in some, but not all, lung lobes and pulmonary segments [14]. For segmental PH to severely increase right ventricular pressure, multiple pulmonary lobes would need to be affected. In patients with PVS complicated by Maze surgery for atrial fibrillation, complete occlusion of the left superior PV and 30%–40% stenosis of the inferior PV resulted in a moderate increase in right ventricular pressure [12]. In pigs with an experimental but combined left pulmonary artery ligation and embolization of the segmental arteries of the right lower lobe, the mean pulmonary artery pressure was 34 ± 9 mmHg [15]. The patient in the present case was diagnosed with severe PH because of complete flattening of the interventricular septum [13,16]. Nonetheless, the severe PH in a patient with partial PVS affecting only two lung lobes seems unlikely. In this case, CT revealed no apparent abnormalities in the pulmonary arteries and veins in the lung lobes, other than the right cranial and middle pulmonary veins; however, ground-glass opacity was observed, suggesting concomitant parenchymal lung disease. As mentioned above, PVS can be associated with bronchopulmonary dysplasia [5,8], and the current case of PH could be related to partial PVS and bronchopulmonary dysplasia. However, of the various features of bronchopulmonary dysplasia, only emphysema was observed in CT findings of the present case. Other features, including bronchial wall thickening and subpleural opacity, were not observed [17,18]. Accordingly, we concluded that bronchopulmonary dysplasia was unlikely. Consequently, the patient was diagnosed with parenchymal lung disease, although histopathological examination would be required for a definitive diagnosis.
To the best of our knowledge, no studies have reported the use of pulmonary vasodilators such as sildenafil in PVS, or postcapillary PH. Moreover, the use of pulmonary vasodilators may exacerbate pulmonary edema by allowing blood flow into the PVS-affected lung lobes. Pulmonary venous-occlusive disease (PVOD)/pulmonary capillary hemangiomatosis (PCH) is a condition that presents with smaller pulmonary vein lesions than PVS; however, like PVS, it also presents with postcapillary PH [19]. PVOD/PCH presents with progressive dyspnea, and the use of pulmonary vasodilators is likely to exacerbate pulmonary edema because of increased pulmonary blood flow [20]. However, sildenafil and pimobendan in dogs with PVOD and dyspnea did not have sufficient efficacy, but did not worsen pulmonary edema in a previous report [21]. Furthermore, PVOD/PCH has a very poor prognosis with a median survival of 3 days, but in the two patients who responded to sildenafil, the pulmonary artery pressure was halved, and they survived for 42 and 150 days [19]. Conversely, a cat diagnosed with PCH developed pulmonary edema after 45 min of sildenafil administration and was euthanized [22]. In cases with PVOD/PCH, reported CT findings include perivascular nodular ground-glass opacities, fissure lines, and enlargement of the lobar pulmonary arteries [19]. Therefore, our case did not meet the diagnostic criteria for these conditions.
In cats, similar to dogs, PH is classified into six groups: Group 1, pulmonary arterial hypertension; Group 2, PH due to left heart disease; Group 3, PH due to respiratory disease or hypoxemia; Group 4, PH due to thrombotic or embolic disease; Group 5, PH due to parasites; and Group 6, PH due to unclear or multifactorial mechanisms [1,2]. In this case, PH was due to causes from both Group 2 and Group 3, and its classification was Group 6. In a previous study, in Group 2 cases with PH defined as tricuspid regurgitation velocity > 2.7 m/s, PH was observed in 17% of cats with congestive left heart failure [23]. Conversely, in dogs with mitral valve insufficiency, when a tricuspid regurgitation velocity ≥3 m/s was used as the diagnosis criteria for PH, 52.7% of dogs in Stage C, the onset or history of congestive heart failure, exhibited PH. However, the prevalence of PH in Stage B2, defined as no congestive signs but with cardiac enlargement, was 24.0%, significantly lower than that in Stage C [24]. In cats with congestive left heart failure, PH prevalence in acquired myocardial disease ranged from 13%–37.5%, while that in congenital heart disease (CHD) was 100%, although details of CHD are unknown [23]. The prevalence of PH was also higher in chronic congestive heart failure than that in acute congestive heart failure [23]. In the present case, the cat may have developed PH due to congenital heart disease, PVS, and chronic congestive heart failure at the age of 2 years. PH in cats in Group 3 mainly involves alveolar hypoxia and pulmonary artery constriction caused by chronic lung disease and hypoxemia. Furthermore, the pulmonary vasculature of cats has been reported to be highly sensitive to the effects of hypoxia and chronic respiratory disease, which is likely to cause PH [25]. The progression of primary pulmonary parenchymal disease, such as pulmonary fibrosis, in cats can lead to the development of PH through the accumulation of lung tissue damage and associated collagen deposition, which impairs respiratory function and causes hypoxia [26]. In this case, the arterial partial pressure of oxygen was 62.9 mmHg, suggesting that hypoxemia secondary to pulmonary parenchymal disease may have contributed to PH.
Using pulmonary vasodilators is not recommended for humans in Group 3, as they increase blood flow to poorly ventilated areas, thereby worsening the ventilation-blood flow imbalance [27]. However, phosphodiesterase-5 inhibitors have improved the quality of life and survival in dogs with PH secondary to obstructive and restrictive lung disease, although administration should be considered with caution [28,29]. A previous report revealed that sildenafil was effective in cats with pulmonary fibrosis [2]. Furthermore, in the treatment of Group 2 PH, therapies aimed at reducing left atrial pressure should be implemented. Sildenafil may increase pulmonary venous return, potentially exacerbating left heart failure [1,2]. In this case, before the cat visited our clinic, it received a diuretic only on the first day of respiratory distress; subsequently, it received sildenafil, which appeared to elicit a dose-dependent response and resulted in the disappearance of syncope and abnormal opacities in the lungs. Although pulmonary arterial pressure was not estimated before and after sildenafil administration in this case, sildenafil may have shifted blood flow to pulmonary vessels other than the right cranial and middle lobes, resulting in reduced blood flow in the right anterior and middle lobes and improved congestion. In addition, because the pulmonary edema in the lungs affected by PVS was not completely resolved, we cannot deny that the diuretics administered before sildenafil treatment by the referral veterinarian could have been effective for a certain period. The efficacy of sildenafil in this case, where the cat was suspected to have Group 6 PH secondary to both left heart disease and lung parenchymal disease, cannot be validated; however, the findings confirmed that it did not worsen the pulmonary edema in the lungs affected by PVS.
There are limitations to our interpretation of the diagnosis and treatment of our case. Sildenafil treatment was initiated by the referral veterinarian from the beginning; therefore, the true effect of sildenafil could not be determined. In our veterinary hospital, we did not perform arterial blood gas analysis, which prevented us from evaluating the hypoxemia observed when the patient’s condition was relatively stable. In addition, while PVS was strongly suspected based on echocardiography and CT, a definitive diagnosis and identification of the cause of death were not possible because an autopsy could not be performed. PH was suspected because of systolic flattening of the interventricular septum on echocardiography and significant dilation of the pulmonary artery both on CT and echocardiography; however, the presence and severity of PH remained unclear due to the absence of tricuspid regurgitation.
4. Conclusions
Partial PVS should be suspected in young cats with an alveolar pattern in the localized lung lobes. Diagnosis can be achieved through echocardiography and CT, although the prognosis is generally poor. PH, despite partial PVS, may also be associated with concurrent parenchymal lung disease. In such cases, sildenafil is expected to worsen pulmonary edema in the affected lungs; however, it did not exacerbate the condition in the present case.
Author Contributions
Conceptualization, T.A. and T. M; methodology, T. A. and K. K.; T. K. and H. T.; validation, T. K. , H. T., K. I. and T. A.; investigation, T. A.; data curation, K. I. and T. A.; writing—original draft preparation, T. A; writing—review and editing, T. M.; visualization, T. K. and H. T.; supervision, T. M.
Funding
The authors received no external funding for the research, authorship, and/or publication of this article.
Institutional Review Board Statement
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognized high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in Veterinary Sciences Although not required, where ethical approval was still obtained is stated in the manuscript.
Informed Consent Statement
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animals described in this work for all procedure(s) undertaken (prospective or retrospective studies). For any animals or people individually identifiable within this publication, informed consent (verbal or written) for their use in the publication was obtained from the people involved.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Acknowledgements
We would like to thank Editage (www.editage.com) for English language editing.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Reinero, C.; Visser, L.C.; Kellihan, H.B.; Masseau, I.; Rozanski, E.; Clercx, C.; Williams, K.; Abbott, J.; Borgarelli, M.; Scansen, B.A. ACVIM consensus statement guidelines for the diagnosis, classification, treatment, and monitoring of pulmonary hypertension in dogs. J Vet Intern Med 2020, 34, 549–573. [Google Scholar] [CrossRef] [PubMed]
- Rolph, K.E.; Cavanaugh, S.M. Feline pulmonary hypertension: Are we overlooking an important comorbidity? J Feline Med Surg 2022, 24, e636–e646. [Google Scholar] [CrossRef] [PubMed]
- Kriström, K.; Karlstam, E.; Nielsen, T.; Lagerqvist, A.; Dirven, M. A case of congenital pulmonary vein stenosis with secondary post-capillary pulmonary hypertension and left sided congestive heart failure in a cat. Vet Sci 2022, 10, 23. [Google Scholar] [CrossRef] [PubMed]
- Montani, D.; Günther, S.; Dorfmüller, P.; Perros, F.; Girerd, B.; Garcia, G.; Jaïs, X.; Savale, L.; Artaud-Macari, E.; Price, L.C.; et al. Pulmonary arterial hypertension. Orphanet J Rare Dis 2013, 8, 97. [Google Scholar] [CrossRef]
- Vyas-Read, S.; Varghese, N.P.; Suthar, D.; Backes, C.; Lakshminrusimha, S.; Petit, C.J.; Levy, P.T. Prematurity and pulmonary vein stenosis: The role of parenchymal lung disease and pulmonary vascular disease. Children (Basel) 2022, 9, 713. [Google Scholar] [CrossRef] [PubMed]
- Latson, L.A.; Prieto, L.R. Congenital and acquired pulmonary vein stenosis. Circulation 2007, 115, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Backes, C.H.; Nealon, E.; Armstrong, A.K.; Cua, C.L.; Mitchell, C.; Krishnan, U.; Vanderlaan, R.D.; Song, M.K.; Viola, N.; Smith, C.V.; et al. Pulmonary vein stenosis in infants: A systematic review, meta-analysis, and meta-regression. J Pediatr 2018, 198, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Northway, W.H. Jr.; Moss, R.B.; Carlisle, K.B.; Parker, B.R.; Popp, R.L.; Pitlick, P.T.; Eichler, I.; Lamm, R.L.; Brown, B.W. Late pulmonary sequelae of bronchopulmonary dysplasia. N Engl J Med 1990, 323, 1793–1799. [Google Scholar] [CrossRef] [PubMed]
- Suntharos, P.; Prieto, L.R. Treatment of congenital and acquired pulmonary vein stenosis. Curr Cardiol Rep 2020, 22, 153. [Google Scholar] [CrossRef]
- Panopoulos, I.; Auriemma, E.; Specchi, S.; Diana, A.; Pietra, M.; Papastefanou, A.; Zini, E.; Cipone, M. 64-multidetector CT anatomical assessment of the feline bronchial and pulmonary vascular structures. J Feline Med Surg 2019, 21, 893–901. [Google Scholar] [CrossRef]
- Thomas, C.A.; Cruz Morel, K.J.C.; Viswanathan, M.N.; de Jesus Perez, V.A. Pulmonary vein stenosis and pulmonary hypertension following a catheter-based radiofrequency ablation for atrial fibrillation: A case report. Am J Case Rep 2020, 21, e924709. [Google Scholar] [CrossRef] [PubMed]
- Pazos-López, P.; García-Rodríguez, C.; Guitián-González, A.; Paredes-Galán, E.; Álvarez-Moure, M.Á.D.L.G.; Rodríguez-Álvarez, M.; Baz-Alonso, J.A.; Teijeira-Fernández, E.; Calvo-Iglesias, F.E.; Íñiguez-Romo, A. Pulmonary vein stenosis: Etiology, diagnosis and management. World J Cardiol 2016, 8, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Visser, L.C.; Im, M.K.; Johnson, L.R.; Stern, J.A. Diagnostic value of right pulmonary artery distensibility index in dogs with pulmonary hypertension: Comparison with doppler echocardiographic estimates of pulmonary arterial pressure. J Vet Intern Med 2016, 30, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Dimopoulos, K.; Diller, G.P.; Opotowsky, A.R.; D’Alto, M.; Gu, H.; Giannakoulas, G.; Budts, W.; Broberg, C.S.; Veldtman, G.; Swan, L.; et al. Definition and management of segmental pulmonary hypertension. J Am Heart Assoc 2018, 7, e008587. [Google Scholar] [CrossRef] [PubMed]
- Guihaire, J.; Haddad, F.; Noly, P.E.; Boulate, D.; Decante, B.; Dartevelle, P.; Humbert, M.; Verhoye, J.P.; Mercier, O.; Fadel, E. Right ventricular reserve in a piglet model of chronic pulmonary hypertension. Eur Respir J 2015, 45, 709–717. [Google Scholar] [CrossRef] [PubMed]
- Sottiaux, J.; Franck, M. Pulmonary embolism and cor pulmonale in a cat. J Small Anim Pract 1999, 40, 88–91. [Google Scholar] [CrossRef] [PubMed]
- Fontijn, S.; Balink, S.J.A.; Bonte, M.; Andrinopoulou, E.R.; Duijts, L.; Kroon, A.A.; Ciet, P.; Pijnenburg, M.W. Chest computed tomography in severe bronchopulmonary dysplasia: Comparing quantitative scoring methods. Eur J Radiol 2023, 169, 111168. [Google Scholar] [CrossRef]
- Milne, M.E.; McCowan, C.; Landon, B.P. Spontaneous feline pneumothorax caused by ruptured pulmonary bullae associated with possible bronchopulmonary dysplasia. J Am Anim Hosp Assoc 2010, 46, 138–142. [Google Scholar] [CrossRef] [PubMed]
- Reinero, C.R.; Jutkowitz, L.A.; Nelson, N.; Masseau, I.; Jennings, S.; Williams, K. Clinical features of canine pulmonary veno-occlusive disease and pulmonary capillary hemangiomatosis. J Vet Intern Med 2019, 33, 114–123. [Google Scholar] [CrossRef]
- Montani, D.; Price, L.C.; Dorfmüller, P.; Achouh, L.; Jais, X.; Yaici, A.; Sitbon, O.; Musset, D.; Simonneau, G.; Humbert, M. Pulmonary veno-occlusive disease. Eur Respir J 2009, 33, 189–200. [Google Scholar] [CrossRef]
- den Toom, M.L.; Grinwis, G.; van Suylen, R.J.; Boroffka, S.A.; de Jong, P.; van Steenbeek, F.G.; Szatmári, V. Pulmonary veno-occlusive disease as a cause of severe pulmonary hypertension in a dog. Acta Vet Scand 2018, 60, 78. [Google Scholar] [CrossRef] [PubMed]
- Jaffey, J.A.; Williams, K.J.; Masseau, I.; Krueger, M.; Reinero, C. Vasoproliferative process resembling pulmonary capillary hemangiomatosis in a cat. BMC Vet Res 2017, 13, 72. [Google Scholar] [CrossRef]
- Vezzosi, T.; Schober, K.E. Doppler-derived echocardiographic evidence of pulmonary hypertension in cats with left-sided congestive heart failure. J Vet Cardiol 2019, 23, 58–68. [Google Scholar] [CrossRef]
- Borgarelli, M.; Abbott, J.; Braz-Ruivo, L.; Chiavegato, D.; Crosara, S.; Lamb, K.; Ljungvall, I.; Poggi, M.; Santilli, R.A.; Haggstrom, J. Prevalence and prognostic importance of pulmonary hypertension in dogs with myxomatous mitral valve disease. J Vet Intern Med 2015, 29, 569–574. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, E.A.; Munroe, M.L.; Tucker, A.; Reeves, J.T. Histamine H1- and H2-receptors in the cat and their roles during alveolar hypoxia. Respir Physiol 1977, 29, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Reinero, C. Interstitial lung diseases in dogs and cats part I: The idiopathic interstitial pneumonias. Vet J 2019, 243, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Galiè, N.; Humbert, M.; Vachiery, J.-L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Vonk Noordegraaf, A.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Respir J 2015, 46, 903–975. [Google Scholar] [CrossRef] [PubMed]
- Jaffey, J.A.; Wiggen, K.; Leach, S.B.; Masseau, I.; Girens, R.E.; Reinero, C.R. Pulmonary hypertension secondary to respiratory disease and/or hypoxia in dogs: Clinical features, diagnostic testing and survival. Vet J 2019, 251, 105347. [Google Scholar] [CrossRef]
- Johnson, L.R.; Stern, J.A. Clinical features and outcome in 25 dogs with respiratory-associated pulmonary hypertension treated with sildenafil. J Vet Intern Med 2020, 34, 65–73. [Google Scholar] [CrossRef]
Figure 1.
Thoracic radiography findings (dorsoventral view). Images obtained by the referring veterinarian. At initial presentation (A), an alveolar pattern is observed in the right cranial lobe. (B) After 19 days of sildenafil administration.
Figure 1.
Thoracic radiography findings (dorsoventral view). Images obtained by the referring veterinarian. At initial presentation (A), an alveolar pattern is observed in the right cranial lobe. (B) After 19 days of sildenafil administration.
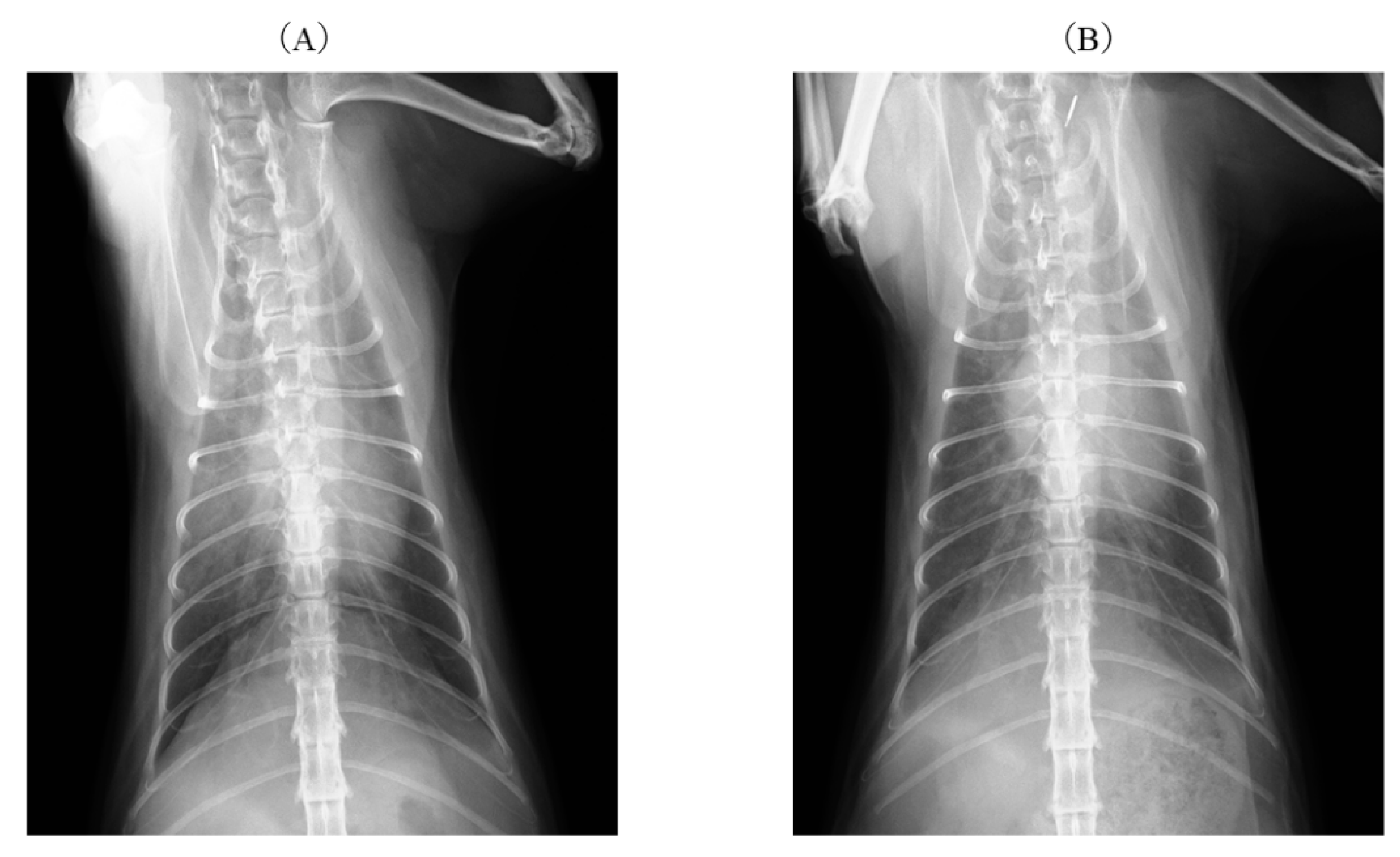
Figure 2.
Echocardiography findings. A right parasternal short-axis view at the level of the left ventricle revealed systolic flattening of the interventricular septum and compression of the left ventricle. LV: left ventricle; RV: right ventricle.
Figure 2.
Echocardiography findings. A right parasternal short-axis view at the level of the left ventricle revealed systolic flattening of the interventricular septum and compression of the left ventricle. LV: left ventricle; RV: right ventricle.
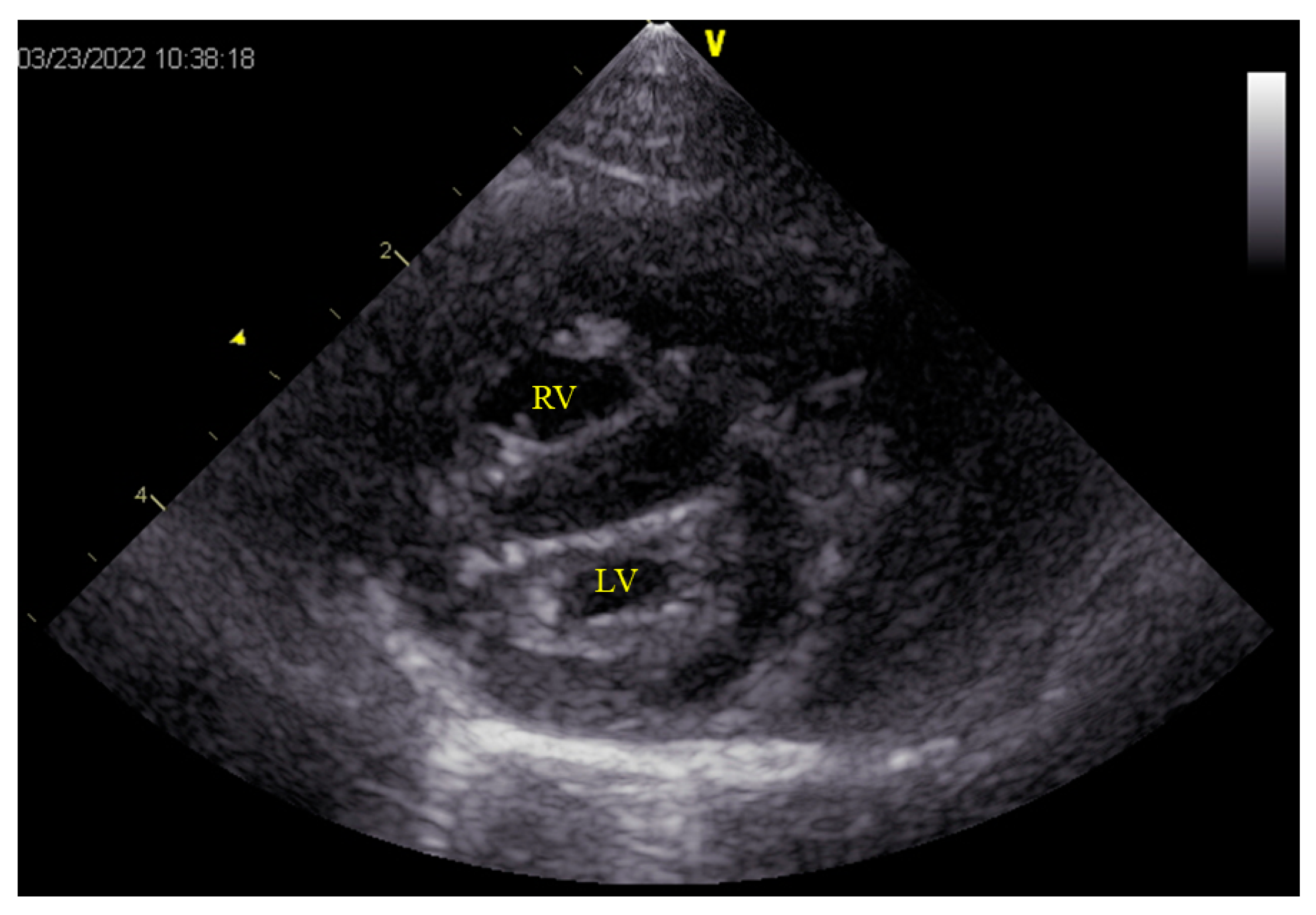
Figure 3.
Echocardiography findings. (A) Simultaneous transthoracic echocardiography and color-flow Doppler imaging of the left atrium. Color-flow Doppler imaging demonstrates turbulent flow from the pulmonary vein (*) to the left atrium. (B) Continuous Doppler echocardiography shows a velocity of 3.14 m/s through pulmonary vein stenosis, indicating a severe pathology. LA: left atrium, LV: left ventricle.
Figure 3.
Echocardiography findings. (A) Simultaneous transthoracic echocardiography and color-flow Doppler imaging of the left atrium. Color-flow Doppler imaging demonstrates turbulent flow from the pulmonary vein (*) to the left atrium. (B) Continuous Doppler echocardiography shows a velocity of 3.14 m/s through pulmonary vein stenosis, indicating a severe pathology. LA: left atrium, LV: left ventricle.
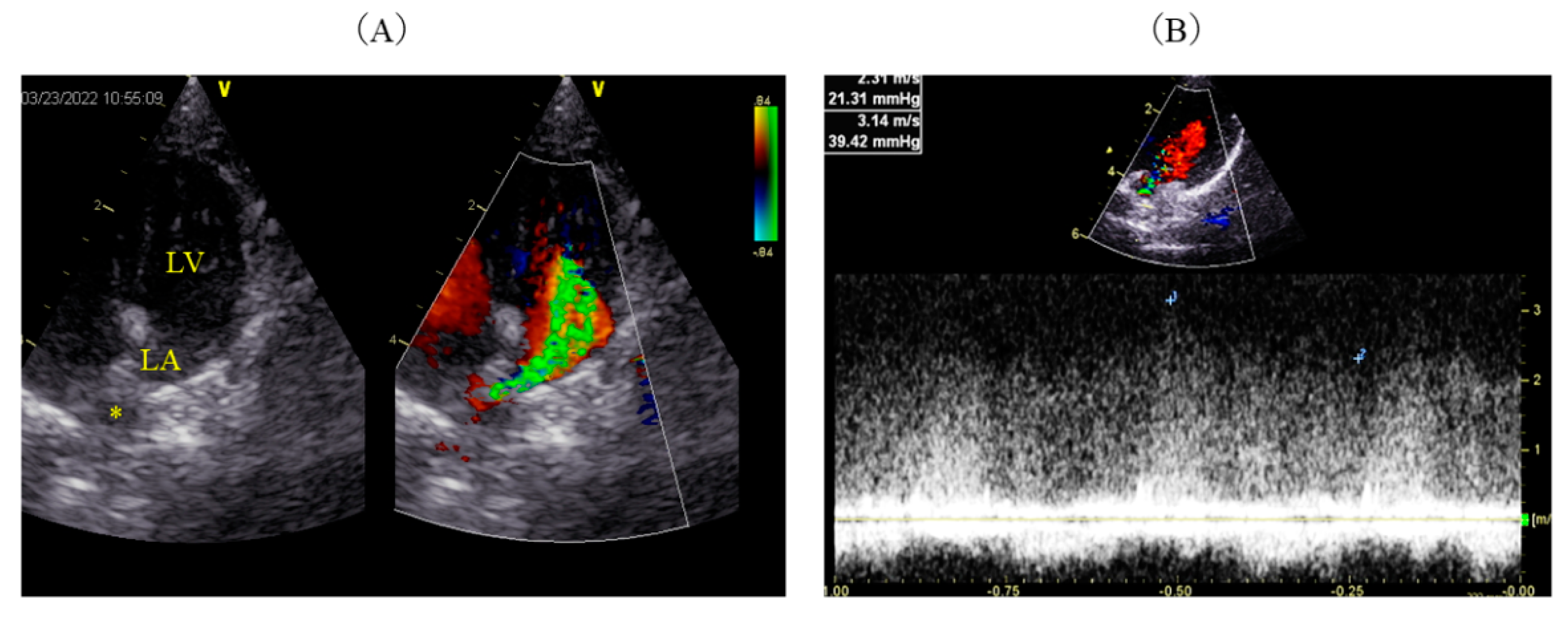
Figure 4.
Computed tomography findings. In the axial view, the diameter of the descending aorta (solid line) is markedly increased relative to the pulmonary artery diameter (double arrows). In addition, significant dilation of the right pulmonary artery is noted (*).
Figure 4.
Computed tomography findings. In the axial view, the diameter of the descending aorta (solid line) is markedly increased relative to the pulmonary artery diameter (double arrows). In addition, significant dilation of the right pulmonary artery is noted (*).

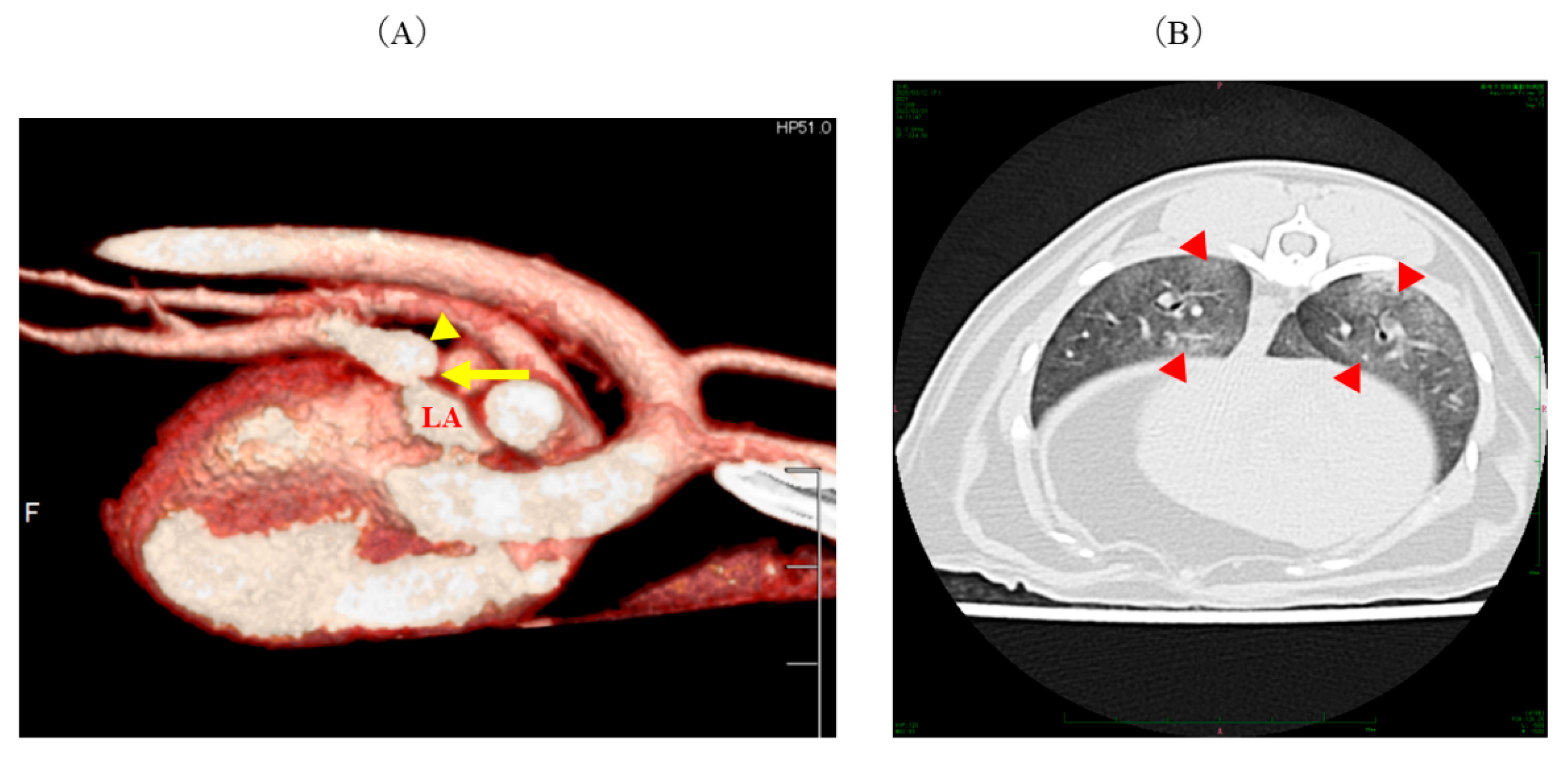
Figure 5.
Computed tomography (CT) findings. (A) A right-side view in contrast-enhanced three-dimensional CT shows stenosis (yellow arrow) of the pulmonary vein from the right middle lobe to the left atrium (LA) and cystic dilation (yellow arrowhead) distally. (B) An axial view of the thoracic posterior lobes shows diffuse ground-glass opacities (red arrowheads).
Figure 5.
Computed tomography (CT) findings. (A) A right-side view in contrast-enhanced three-dimensional CT shows stenosis (yellow arrow) of the pulmonary vein from the right middle lobe to the left atrium (LA) and cystic dilation (yellow arrowhead) distally. (B) An axial view of the thoracic posterior lobes shows diffuse ground-glass opacities (red arrowheads).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



