
Submitted:
07 May 2024
Posted:
08 May 2024
You are already at the latest version
Abstract
Diarrhea remains one of the leading causes of mortality worldwide, especially among children. Recent epidemiological studies conducted in developing countries identified Shigella species as the most predominant pathogenic bacteria responsible for diarrhea. Antimicrobial therapy is necessary for Shigella infections; however, the rapid emergence of resistance against existing antimicrobials in Shigella spp. poses a serious global health problem. To identify alternative antimicrobial compounds with activity against Shigella species, the pathogens responsible for bacterial diarrhea. In this study, we have applied antibacterial phenotypic screening to identify potent anti-Shigella compounds across a broad chemical diversity, including selected acetaminophen derivatives containing benzothiazoles backbone, and their combination with certain antibiotics. In continuation to our effort in searching potent antimicrobial compounds, we have found this time around that two acetaminophen derivatives containing benzothiazoles backbone (4a and 4b) could inhibit the growth of Shigella flexneri with common MIC value of 12.5 µg/ml. These compounds were established through a time-kill kinetics’ study to be bactericidal. Meanwhile, the 2-aminobenzothiazoles (1a and 1b) used for the synthesis of compounds 4 (a & b) were found to be poorly active (MIC: 100 µg/ml) against this pathogen. Combination studies of 4a and 4b with the least susceptible antibiotics (ceftriaxone and cotrimoxazole) demonstrated synergistic anti-Shigella activity. The present study demonstrates that the azobenzothiazole dyes 4 (a & b) can be repurposed as potential anti-Shigella compounds, which can serve as scaffolds for the development of new agents against infectious diarrhea caused by Shigella and other enteric pathogens, especially in developing countries.
Keywords:
Acetaminophen
; Benzothiazoles
; Azo dyes
; Shigella flexneri
; Anti-Shigella activity
; Repositioning
; Combination studies
; Diarrhea.
1. Introduction
Diarrhea is among the manifestations of gastrointestinal infections caused by a number of bacterial, viral and parasitic microorganisms [1,2]. The release of at least three watery or loose stools per day, or more often (discharge of 10 and 200 g/kg/day of feces in infants and adults, respectively) than ordinarily is generally termed as diarrhea [2,3]. Contaminated food or drinking water and poor sanitation are associated to the transmission of infectious diarrhea [4,5]. This disease is the second leading cause of death in children under five years old, especially in developing countries where hygiene and sanitation are not adequate [2,5]. Recent estimates point out approximately 1.7 billion cases of childhood diarrhea annually with 525 000 deaths in children under five years old [2,6]. Notably, gram-negative bacteria of the genus Shigella accounts for 69% of all episodes and 61% of all deaths caused by bacterial diarrhea [7,8]. One such bacterial diarrhea includes shigellosis, which is caused by Shigella species, such as Shigella flexneri, Shigella sonnei, and Shigella boydii [9]. Most of the breakouts of shigellosis have been ascribed to S. flexneri [10]. Clinical cases of diarrhea caused by Shigella flexneri have also been reported among patients with primary HIV infection [11,12]. Shigella species are primarily spread through the faeco-oral route, whereas the housefly Musca domestica act as a vector for their transmission [13]. As low as 10-100 bacterial count are potential of causing diarrheal infection [14,15]. The economic impact of diarrhea and its treatment are of considerable importance [16,17].
Current treatments for diarrhea include the use of antimicrobials, especially for diarrhea caused by bacteria [5]. However, most of these therapies have lost their efficacy due to the spread of multi-drug resistant Shigella mostly in infants and patients with HIV [18]. Consequently, there has been an extensive use of antimicrobials, such as ciprofloxacin, azithromycin, pivmecillinam, ampicillin and ceftriaxone (as per the WHO recommendations) as the empirical drug choices for the treatment of infection by fluoroquinolones-resistant Shigella species [19,20]. It has been reported that drug resistance in Shigella species can result from many mechanisms, such as extrusion of drugs by active efflux pumps, decrease in cellular permeability, and overexpression of drug-modifying and -inactivating enzymes or target modification by mutation [21]. Thus, there is an urgent need to search for new and safe antidiarrheal agents. Acetaminophen is one of the most widely used analgesic, anti-inflammatory and antipyretic drug [22] that has been reported to exhibit antibacterial activity against a number of bacterial strains, including Staphylococcus aureus [23]. Although the use of this medicine has been linked to liver failure, hepatotoxicity occurring with acetaminophen is typically correlated with high doses that exceed the recommended maximum dose [24,25]. However, selected structural modifications of acetaminophen with the benzothiazole ring have afforded pharmacologically active compounds with improved nephrotoxicity as compared to the parent molecule, i.e., acetaminophen [26]. On the other hand, recent reports indicate that benzothiazoles have the ability to inactivate reactive chemical species through their antioxidant capacity [27]. The nephrotoxicity caused by an overdose of acetaminophen is often reverted when this drug harbors the benzothiazole ring [28]. In addition, benzothiazole-based compounds have also been reported to exhibit antibacterial activity [29,30,31,32]. Furthermore, antibiotic combination therapy has been argued as a forefront strategy to overcome bacterial drug resistance to antibiotics [33]. Although few studies have revealed the effectiveness of acetaminophen against Staphylococcus aureus [23], no report has shown the mechanistic basis of the antibacterial action of acetaminophen and its derivatives against Shigella species, the pathogens responsible for infectious diarrhea. It has also been demonstrated that drugs, such as acetaminophen display anti-biofilm activity, which could fuel an interest in repurposing this well tolerated drug as an adjunctive therapy for bacterial infections [34,35].
In continuation to our search for new scaffolds and better combinations with antimicrobial efficacy from existing therapies, this study aimed to repurpose acetaminophen from its traditional use as an anti-inflammatory drug to a potentially active hit compound against Shigella-causing diarrhea. Herein, a series of diazobenzothiazoles dyes and their combination with selected antibiotics were screened for antishigellosis activity against a panel of Shigella species, including Shigella flexneri NR 518, Shigella boydii NR 521, Shigella sonnei NR 519, and Shigella dysenteriae. A plausible antibacterial mechanism of action of the most active compounds was also elucidated.
2. Materials and Methods
2.1. Chemistry
2.1.1. General Information
Melting points were determined on a Buchii melting point apparatus. The thin layer chromatography (TLCs) was carried out on Eastman Chromatogram Silica Gel Sheets (13,181; 6,060) with fluorescent indicators. A mixture of hexane and ethyl acetate (4:6) was used as the eluent and iodine was used for the visualization of the chromatograms. The infrared (IR) spectra were measured with a Fourier transform infrared spectrometer JASCO FT/IR-4100 and a Perkin Elmer FT-IR 2000 spectrometer. The ultraviolet (UV) spectra were recorded with a Beckman U-640 spectrophotometer using samples’ solutions of concentration 5x10−5 mol/L. Combustion analyses were carried out with a Euro EA CHNSO analyzer from Hekatech Company, and the results were found to be in good agreement (±0.3%) with the calculated values. Positive ion electrospray mass spectra were recorded on a Waters Xevo TQD tandem quadrupole mass spectrometry system running in an MS scan mode, and 1 min of acquired spectra was combined and centroided. 1H-NMR spectra were recorded in DMSO-d6 with a 400 MHz spectrometer RMN Bruker Advance 400. 13C-NMR spectra were recorded in DMSO-d6 with a 100 MHz spectrometer RMN Bruker Advance 400. Tetramethylsilane (TMS) was used as the internal reference.
2.1.2. Preparation of the Reagents and Starting Materials
All the reagents mentioned in this study were purchased from Aldrich and Fluka and were used without further purification.
a. Preparation of diazonium salt solution
In a similar manner as described earlier [28], dried sodium nitrite (0.69 g, 10 mmol) was slowly added over a period of 30 min to concentrated sulfuric acid (10 mL) with occasional stirring. The solution was cooled to 0-5°C. Compound 1 was dissolved in dimethyl sulfoxide (DMSO) (10 mL) and cooled to 0-5°C. The nitrosyl sulfuric acid solution was added to the solution of compound 1, and the temperature was maintained between 0 and 5°C. The clear diazonium salt solution thus obtained consisting of the in situ-formed intermediate 2 was used immediately in the coupling reactions.
b. General procedure for the preparation of the coupling products 4a,b
Acetaminophen (1.51 g, 10 mmol) 3 was dissolved in DMSO (10 mL) and then cooled in an ice bath at 0–5°C. The previously prepared diazonium solution of 2 was added drop-wise over 1 h, and then 15 mL of sodium acetate solution (10%) was added to the mixture. The pH of the mixtures ranged from 9 to 11. The solid precipitate was collected on a filter and crystallized from methanol to give the title compound.
N-(2-(6-ethoxy-5-((6-ethoxybenzo[d]thiazol-2-yl)diazenyl)benzo[d]thiazol-2-yl)diazenyl)-3-((6-ethoxy-5-((6-ethoxybenzo[d]thiazol-2-yl)diazenyl)benzo[d]thiazol-2-yl)diazenyl)-5,6-bis((6-ethoxybenzo[d]thiazol-2-yl)diazenyl)-4-hydroxyphenyl)acetamide hexahydrate (4a) Compound 4a was obtained in 47% yield as red powder; m.p. 197–198 °C (dec); (lit. 197–199°C (dec); Tsemeugne et al. [28]; 1H-NMR (DMSO-d6, 400 MHz): δ 8.11 (d, 1H, J = 2.8, H-4iv), 8.00 (s, 1H, H-7), 8.02 (s, 1H, H-7v), 7.91 (d, 1H, J = 9.2, H-4′’’), 7.71 (d, 1H, J = 2.0, H-7”’), 7.68 (d, 1H, J = 3.6, H-7′’), 7.65 (d, 2H, J = 8.8, H-4′’ and H-4vi ), 7.62 (d, 1H, J = 6.4, H-7vi), 7.61 (s, 1H, H-4v), 7.58 (s, 1H, H-4), 7.16 (dd, 2H, J = 9.2 and 2.8, H-5′’’ and H-5iv), 7.15 ( d, 1H, J = 2.4, H-7iv), 7.09 ( d, 2H, J = 8.8, H-5′’ and H-5vi), 4.18, 4.16, 4.14, 4.12, 4.11, 4.10, 4.08 (OCH2CH3); 1.58, 1.40, 1.38, 1.36, 1.35 (OCH2CH3); 2.05 (s, 3H, COCH3); 13C-NMR (DMSO-d6, 100 MHz): δ 199.1(CO); 178.3(C-2 and C-2′’); 174.5(C-2′’’); 173.7(C-2iv); 173.4(C-2v); 173.2(C-2vi); 163.6(C-5); 163.3(C-5′’); 161.8(C-5′’’); 161.7(C-5iv); 161.4(C-5v); 158.5(C-5vi); 157.2(C-3av); 156.9(C-3avi); 152.0(C-3a and C-3a’’); 151.0(C-3a’’’); 150.1(C-3aiv); 143.6(C-2′); 141.8(C-3′); 141.5(C-4′); 141.1(C-6v); 140.9(C-6vi); 137.4(C-4a); 137.3(C-4a’’); 136.9(C-5′); 133.1(C-1′); 130.4(C-4a’’’ and C-6′); 128.7(C-4aiv); 128.0(C-4av); 127.8(C-4avi); 123.9(C-7); 123.8(C-7′’); 123.5(C-6iv); 122.1(C-6); 121.7(C-6′’); 121.4(C-6′’’); 120.9(C-7′’’); 120.7(C-7iv); 117.2(C-7v); 113.4(C-7vi); 111.7(C-4); 111.4(C-4′’); 110.8(C-4′’’); 110.2(C-4iv); 109.9(C-4vi); 105.9(C-4v); 74.9; 71.1; 70.7; 69.1; 69.0; 68.9(6xOCH2CH3); 29.0(CH3CO) ; 20.0; 19.9; 19.8; 19.7 (6xOCH2CH3); UV-Vis λmax (DMSO) (Log ε): 211 (4.45), 214 (4.47), 229 (4.51) 238 (4.51), 258 (4.53), 2.69 (4.65) 279 (4.57), 309 (4.54), 364 (4.58) 378 (4.56), 416 (4.62) nm; IR (KBr) νmax : 3281 (O-H), 2980-2933 (ArC-H), 1657 (C=O), 1599 (C=N), 1556 (C=C), 1488-1456 (N=N), 1263 (C-S), 1211 (C-O), 899-519 (Ar def C=N str thiazole) cm-1; ms: (ESI+) m/z (%) 1492 (9), 1453 (9), 1428 (17), 1404 (17), 1379 (15), 1353 (18), 1323 (16), 1293 (11), 1238 (17), 955 (32), 728 (69), 659 (71), 549 (72), 486 (52); Anal. Calcd. for C62H63N19O14S6: C, 49.96; H, 4.26; N, 17.85; S, 12.90. Found: C, 49.98; H, 4.28; N, 17.81; S, 12.88. Rf = 0.39.
N-(4-hydroxy-3-((6-methoxybenzo[d]thiazol-2-yl)diazenyl)phenyl)acetamide hexahydrate (4b) Compound 4b was obtained in 51% yield as brown powder; m.p. 198–199 °C (dec); (lit. 197–199°C (dec); Tsemeugne et al. [28]; 1H-NMR (DMSO-d6, 400 MHz): δ 8.11 (d, 1H, J = 2.0, H-2′), 8.02 (d, 1 H, J = 9.0, H-4), 7.70 (d, 1H, J = 2.4, H-7), 7.63 (dd, 1H, J = 8.8 and 2.4, H-6′), 7.18 (dd, 1H, J = 8.8 and 2.4, H-5), 7.09 (d, 1H, J = 8.8, H-5′), 3.89 (s, 3H, OCH3), 2.04 (s, 3H, COCH3); 13C-NMR (DMSO-d6, 100 MHz): δ 173.1 (CO), 168.1 (C-2), 159.1 (C-6), 153.3 (C-3a), 146.8 (C-4′), 138.4 (C-1′), 135.8 (C-3′), 132.0 (C-4a), 127.9 (C-4), 125.1 (C-6′), 118.7 (C-5′), 116.6 (C-5), 108.0 (C-2′), 105.1 (C-7), 55.8 (OCH3), 23.8 (COCH3); UV-Vis λmax (DMSO) (Log ε): 227 (4.06), 257 (4.12), 272 (4.26), 290 (4.09), 295 (4.08), 302 (4.12), 325 (4.19), 348 (4.18), 355 (4.19), 399 (4.23), 445 (4.25), 486 (4.22) nm; IR (KBr) νmax : 3282 (O-H and N-H), 2941-2834 (ArC-H), 1658 (C=O), 1598 (C=N), 1555 (C=C), 1482-1434 (N=N), 1264 (C-S), 1228 (C-O), 910-510 (Ar def C=N str thiazole) cm-1; ms: (ESI+) m/z (%) 448 (11), 429 (11), 409 (42), 385 (10), 316 (100), 300 (22), 281 (19), 216 (70), 202 (14), 192 (21), 150 (70); Anal. Calcd. for C16H26N4O9S: C, 42.66; H, 5.82; N, 12.44; S, 7.12. Found: C, 42.63; H, 5.80; N, 12.41; S, 7.10. Rf = 0.30.
2.2. Biological Activity
2.2.1. Reference Compounds and Bacterial Strains
The reference compounds [ciprofloxacin (antibiotic) and triton X (standard hemolytic agent)], which were used as positive controls in this study were acquired from Sigma Aldrich. Other antibiotics that were used in combination studies included ampicillin (ampicillin sodium for I.M/I.V injection, Shanxi Xinyitong Pharmaceutical Co. Ltd., Huitong Road, Jinzhong, Shanxi, China), cefixime (CEFLIXE tablets, Farma hub, Uttarakhand, India), co-trimoxazole (oral tablets, Africure Pharmaceutical Ltd.; Bwang Bakoko, Yassa-Douala, Cameroon), tetracycline (tetracycline hydrochloride tablets, Zhejiang Cheng Yi Pharmaceutical Co. Ltd., Wenzhou, Zhejiang, China) and were obtained from local drugstores in Yaounde, Cameroon. In vitro antibacterial activity of the test and reference compounds was evaluated on Shigella flexneri NR 518, Shigella boydii NR 521, and Shigella sonnei NR 519, which were acquired gracefully from the Biodefense and Emerging Infections Research Resources Repository (BEI resources) and a clinical isolate, Shigella dysenteriae donated by the Centre Pasteur of Cameroon. These strains were preserved by sloping culture at 4 °C in Mueller Hinton agar at the Laboratory of Phytobiochemistry and Medicinal Plant Studies, Department of Biochemistry, University of Yaounde 1, Cameroon. These bacterial species were sub-cultured at 35 ± 2°C 24 h on Mueller Hinton Agar prior to each experiment.
2.2.2. Determination of the Anti-Shigella Activity of Compounds and Antibiotics
a. Preparation of stock solutions
The stock solutions were prepared at 10 mg/mL by dissolving 10 mg of each compound or antibiotic (other than ciprofloxacin) in 1 mL of dimethyl sulfoxide (DMSO 100%) and then stored at 4°C. Ciprofloxacin, the antibiotic that was used as positive control was prepared by dissolving 1 mg of drug in 1 mL of acidified water using HCl 0.5 N to achieve a final concentration of 1 mg/mL.
b. Preparation of bacterial inocula
The bacterial suspensions were prepared at 1.5x108 UFC/mL with reference to the 0.5 McF standard by introducing a colony from the 24 h’ cultures on Müller Hinton Agar into 10 mL of NaCl 0.9% and further calibrated by turbidity comparison.
c. Determination of minimum inhibitory concentrations
The minimum inhibitory concentrations (MICs) were determined using broth microdilution method referring to protocol number M09-A7 of the Clinical & Laboratory Standards Institute (CLSI) guidelines [36] with slight modifications. In brief, 196 µL of Muller Hinton Broth (MHB) were introduced in the first wells, whereas 100 µL into the rest of wells. Next, 4 µL of sterile solution of compounds were prepared at 10 mg/mL and added to the corresponding wells followed by two-fold serial dilution. Subsequently, 100 µL of bacteria suspension (106 UFC/mL) were distributed in wells excluding those of sterility control. The concentrations of compounds and ciprofloxacin into the wells were ranged from 100 to 3.125 μg/mL and from 0.25 to 0.0078 μg/mL, respectively, with 200 µL in the final volumes. Next, the plates were covered and incubated during 24 h at 37°C. At the end of the incubation period, 20 µL of freshly prepared solution of resazurin (0.15 mg/mL) were introduced into all wells and subsequently re-incubated at 37°C for 30 min. The test was carried out in triplicate in sterile 96 well microplates. The lowest concentration at which there was no color change from blue to pink (consistent to no visible growth of bacteria) was considered as the MIC of test compounds.
2.2.3. Cytotoxicity Assay
The cytotoxic effect of compounds and compound-antibiotic combinations was evaluated on erythrocyte membrane by using spectrophotometric method based on haemoglobin release [37]. Haemolytic effect was examined by incubating normal erythrocytes with all compounds in RPMI 1640 culture medium. Firstly, the erythrocyte suspension was prepared according to the protocol described by Fidock et al. [38] with a few modifications. Blood from an O+ donor was centrifuged at 3500 rpm for 5 min, and after removal of the plasma, the pellet was washed 3 times under the same conditions. The remaining pellet was suspended with RPMI 1640 culture medium to obtain a haematocrit of 4%. Five hundred microliters of this suspended pellet were added to microtubes having test compounds at different concentrations (200-12.5 µg/mL). RPMI 1640 alone (for baseline values) and 0.5% Triton X-100 in RPMI 1640 (for 100% haemolysis) were employed as controls. After keeping at 37 °C for 3 h in an atmosphere of 5% CO2, the test samples were centrifuged at 2500 rpm for 5 min and 200 µL of the supernatant was transferred to a 96-well sterile culture plate for determination of the haemolytic activity quantified in terms of haemoglobin release as monitored spectrophotometrically by taking absorbance at 540 nm. The experiment was done in triplicate and the mean ± SD was calculated. From the optical densities obtained, percentage of haemolysis was calculated using the following formula:
% Hemolysis = (Absorbance of sample-Absorbance of blank sample)/(Absorbance of positive control) x100
Using Graphpad Prism 8.0.1 software (San Diego, California), median haemolytic concentrations (HC50) were determined from concentration-response sigmoidal curves obtained by plotting the percentage of haemolysis against the decimal logarithm of concentration. Selectivity indices were further determined for each test substance as follows:
Selectivity Index (SI)=HC50/(MIC50 (Shigella flexneri))
With MIC50=MIC/2 [39].
2.2.4. Potential Mechanism of Antibacterial Action and Combination Studies
a. Bacterial time-kill kinetics
The kinetics of bacterial mortality were studied on the most active antibacterial compounds (4a and 4b) according to the protocol described by Klepser et al. [40] with slight modifications, including the use of opacimetry based on turbidity of cell suspensions as a function of charge rather than colony counting on agar. The assays were performed in triplicate in sterile microplates of 96 wells at sub-inhibitory, inhibitory and supra-inhibitory concentrations. Indeed, a serial dilution was performed for each sample as previously described to obtain 4 MIC, 2 MIC, MIC, 0.5 MIC and 0.25 MIC. Next, 100 µL of bacterial suspension (106 UFC/mL) were distributed in wells, except those of sterility control. The negative control’s well was made up of culture media and bacterial suspension, whereas the positive control’s wells comprised culture media, bacterial suspension and ciprofloxacin. The plates were then incubated for 24 h at 37 °C, during which time bacterial growth kinetics was studied by measuring optical densities at 620 nm and at different time intervals: 0, 1, 2, 4, 6, 8, 10, 12 and 24 h using a microplate reader (TECAN Infinite M200, Männedorf, Switzerland) against the blank (compound in culture media). The results allowed us to plot the optical density curves as a function of the incubation times and these curves were used to determine the minimum time at which the inhibitory effect was first observed and the bactericidal and bacteriostatic effects of the compounds, as well as the time of re-emergence of the bacterial species. The concentrations that led to a continuous decrease of bacterial population were considered as Minimum Bactericidal Concentrations (MBCs).
b. Combination of active compounds with selected antibiotics and antibacterial studies
b1-Preparation of the intermediate plate
Intermediate plates were prepared from a stock solution of the most active compounds and the least effective antibiotics (10 mg/mL) by serial dilution of test samples with MHB in two different microplates. The concentrations ranged from 4 MIC to MIC/32 in the wells (from row A to H) and (from 1 to 8) for compound and antibiotic, respectively and the volume were topped up to 100 µL.
b2-Determination of fractional minimum inhibitory concentration (FICI) indices
The combined effect of the compound with the antibiotic was assessed using a checkerboard dilution method [41]. Twenty-five microlitres (25 µL) of different concentrations from the intermediate plates were added to a 96 wells microplate containing MBH (50 µL) in order to obtain compound and antibiotic at different concentrations in the considered wells (MIC/1 in well 1 to MIC/128 in well 8 and MIC/1 in well A to MIC/128 in well H, respectively). Next, 100 µL of bacteria suspension (106 UFC/mL) was added to the test wells and negative control for a final load of 5 ×105 CFU/mL. The plates were incubated at 37 °C for 24 h, then 20 µL of resazurin (0.15 mg/mL) was added to each well followed by further incubation for 30 min. Ciprofloxacin was used as a positive control. Tests were performed in triplicate for each sample.
The fractional minimum inhibitory concentrations indices (FICI) of different combinations corresponding to the wells with no visible bacterial growth were calculated using the following formula:
FICI= FICA + FICB
FICA=MICAcom/MICA and FICB=MICBcom/MICB
A=compound; B= antibiotic and com= in combination
Interaction type was interpreted using FICI values: FICI≤0.5, interaction is synergistic; 0.5< FICI ≤ 1.0 interaction is additive; 1.0 <FICI≤4.0 means no interaction; FICI > 4.0, interaction is antagonistic.
In addition, the type of interaction involved was better appreciated geometrically using isobolograms, obtained by plotting the FIC values of a compound (FICA) in combination against those of the antibiotic (FICB).
2.2.5. Data Analysis
The in vitro antibacterial test was repeated three times and the results were analysed using Graph Pad software 8.1.0. The quantitative variables were then presented as mean ± standard deviation. Differences were considered statistically significant at p<0.05. The graphs were plotted using Excel software (version 2013, Washington, DC, United States of America).
3. Results
3.1. Chemistry
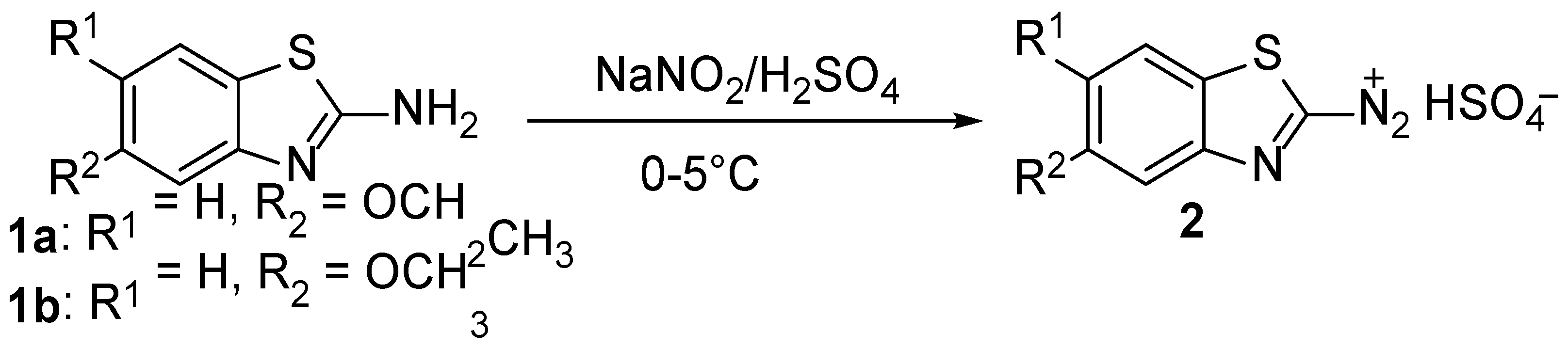
The diazonium ions 2 were readily synthesized according to the literature [28] by adding 2-aminobenzothiazole 1 to nitrosyl sulfuric acid at 0-5 °C (Scheme 1).
The azobenzothiazole dyes 4 (a & b), which were used in this study, were obtained during the coupling reactions of diazotized 2-aminobenzo[d]thiazole derivatives 2 with p-acetaminophen 3 according to previous experimental procedures [28] as depicted in Scheme 2.
The yields, the melting points and all the spectroscopic data for compounds 4a and 4b agree with those originally reported [28].
3.2. Antibacterial and Cytotoxic Assays
The results obtained from the antimicrobial activity of 2-aminobenzothiazole derivatives 1 (a & b), acetaminophen 3 and diazobenzothiazoles dyes 4 (a & b), are summarized in Table 1. The minimum concentrations that inhibited the bacterial growth ranged from 12.5 to 100 μg/mL for test compounds and from ˂0.062 to 12.5 µg/mL for reference antibiotics. Compounds 4a and 4b were found to be the most active compounds (MIC=12.5 µg/mL on S. flexneri and 50 μg/mL on S. sonnei), whereas compound 3 was the least active compound (MIC˃100 µg/mL). Shigella flexneri was the most susceptible bacterial species, whereas S. boydii and S. dysenteriae were found to be the most resistant ones as no activity was observed with any of the test compounds (MIC˃100 µg/mL).
The susceptibility of the most sensitive strain viz. Shigella flexneri was evaluated against four antibiotics. Ampicillin and tetracycline were the most active antibiotics (MIC˂0.062 µg/mL), followed by cotrimoxazole and ceftriaxone with a common MIC value of 12.5 µg/mL. In the hemolysis test, compounds 4a and 4b afforded HC50 values of 148.85 and 87.52 µg/mL, to yield selectivity indices (SI) of 23.68 and 13.92, respectively, inferring the non-toxicity of these compounds toward red blood cells. The other compounds (1a, 1b and 3) showed minimal haemolysis percentages (below 1% at 200 µg/mL), when compared to the standard hemolytic agent triton X-100 (100% haemolysis). However, the selectivity indices were greater than 13.92 for all the tested compounds (1a, 1b, 3, 4a, and 4b), inferring that these compounds are not toxic to red blood cells. These results demonstrated that 4a and 4b, which were found to be the most active compounds were selective as they did not display toxicity on the membrane’s red blood cells. Thus, compounds 4a and 4b were further selected for bacterial growth kinetic assays.
3.3. Bacterial Growth Kinetics and Combination Studies
3.3.1. Shigella Growth Kinetics
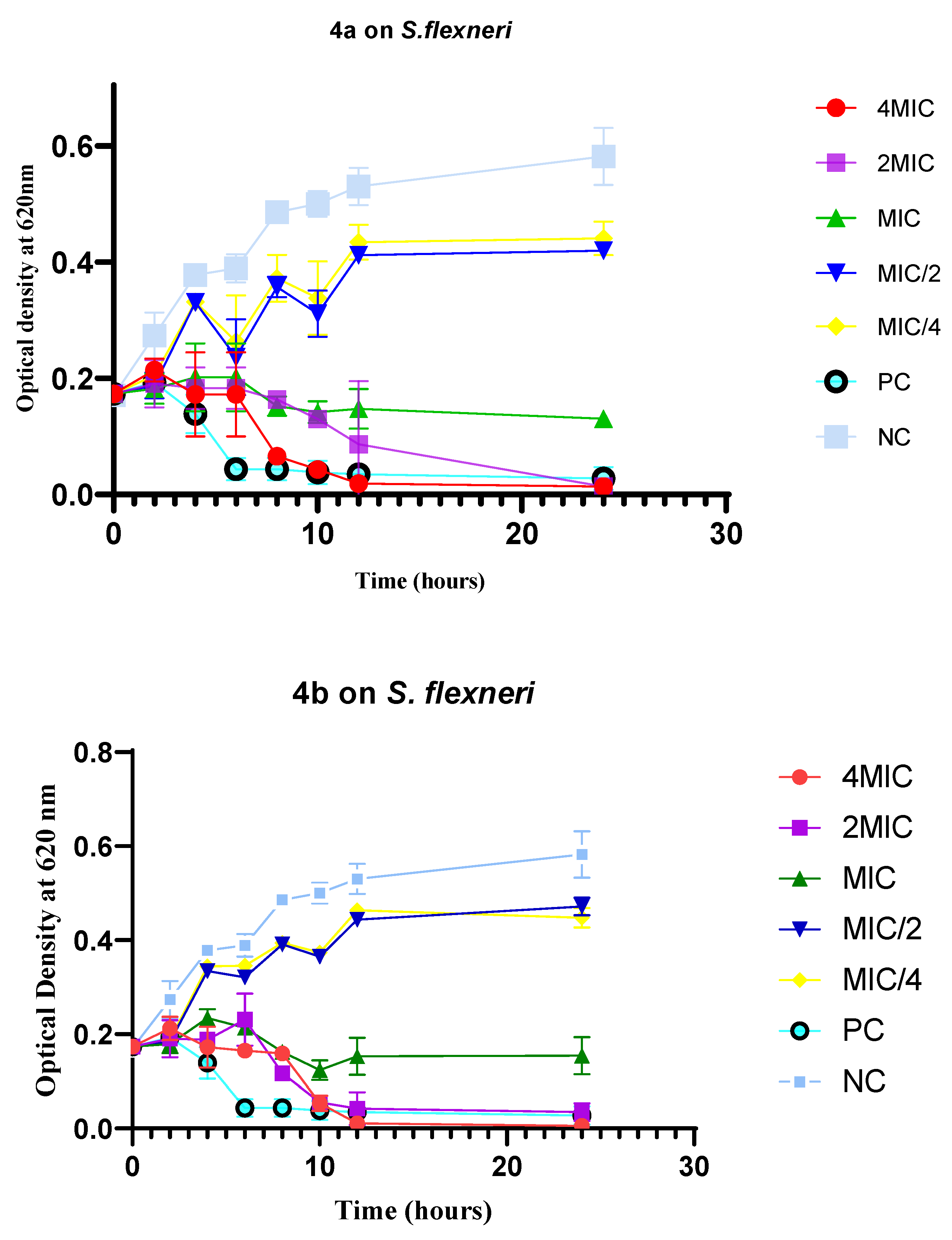
Figure 1 shows the variation of the bacterial population upon compounds’ treatment as a function of time. It appears that the bacterial inhibition is dose-dependent and is observed after a minimum incubation time of 2 h. In addition, a continuous decrease in the optical densities corresponding to a reduction in the bacterial load was observed with 2MIC and 4MIC as compared to ciprofloxacin, thus suggesting a bactericidal effect (MBC=25 µg/mL) of both the compounds 4a and 4b.
Figure 1.
The diagonal lines for the interpretation of isobolograms in the interaction study between two bioactive substances.
Figure 1.
The diagonal lines for the interpretation of isobolograms in the interaction study between two bioactive substances.
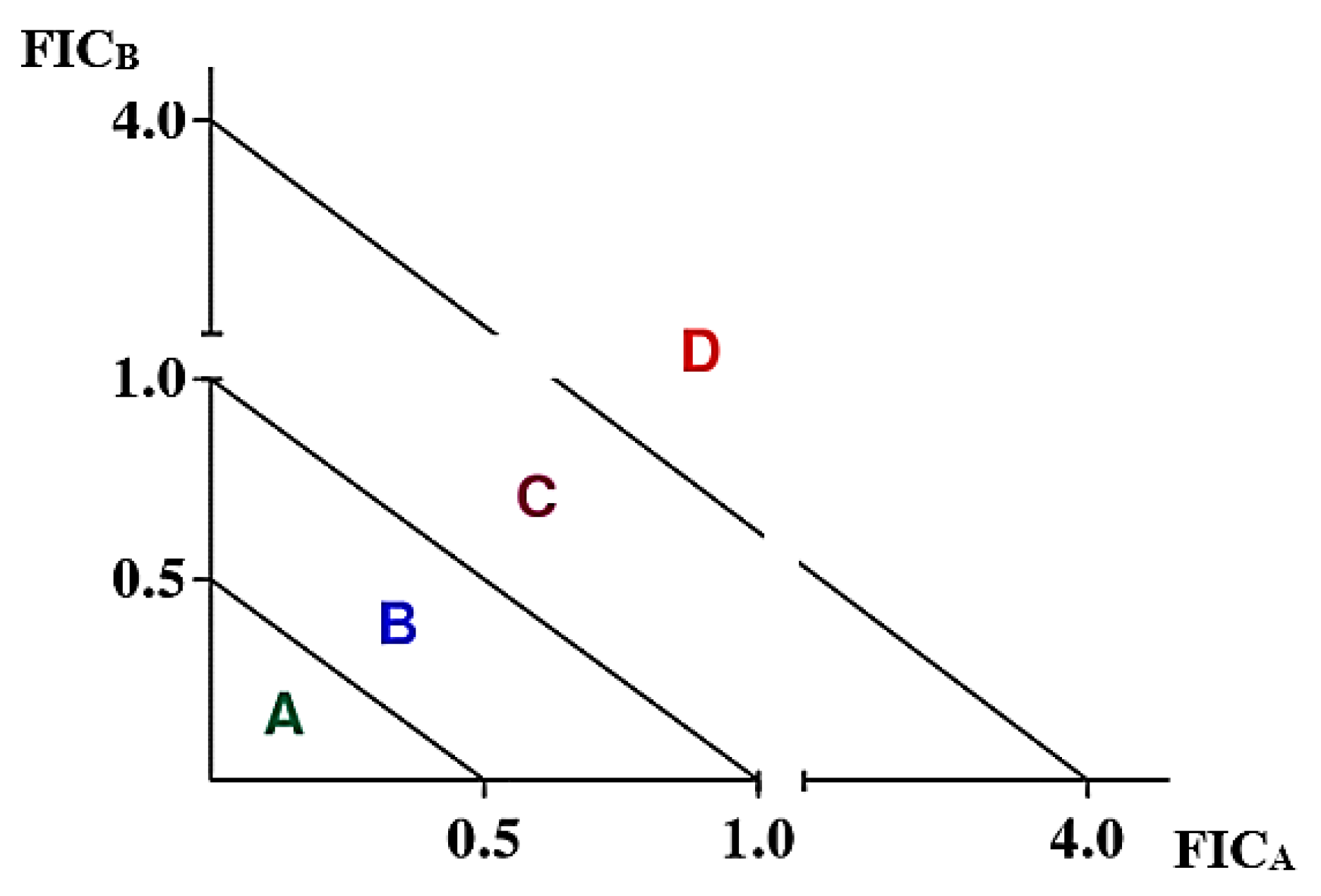
Figure 1.
Bacterial time-kill curves of S. flexneri NR518 following incubation with compounds 4a and 4b. 4a: N-(2-(6-Ethoxy-5-((6-ethoxybenzo [d]thiazol-2-yl)diazenyl)benzo[d]thiazol-2-yl)diazenyl)-3-((6-ethoxy-5-((6-ethoxybenzo[d]thiazol-2-yl)diazenyl) benzo[d]thiazol-2-yl)diazenyl)-5,6-bis((6-ethoxybenzo[d]thiazol-2-yl)diazenyl)-4-hydroxyphenyl) acetamide hexahydrate; 4b: N-(4-Hydroxy-3-((6-methoxybenzo[d]thiazol-2-yl) diazenyl)phenyl)acetamide hexahydrate; MIC: minimum inhibitory concentration; NC: Negative control; PC: Positive control (ciprofloxacin, 0.25 µg/mL).
Figure 1.
Bacterial time-kill curves of S. flexneri NR518 following incubation with compounds 4a and 4b. 4a: N-(2-(6-Ethoxy-5-((6-ethoxybenzo [d]thiazol-2-yl)diazenyl)benzo[d]thiazol-2-yl)diazenyl)-3-((6-ethoxy-5-((6-ethoxybenzo[d]thiazol-2-yl)diazenyl) benzo[d]thiazol-2-yl)diazenyl)-5,6-bis((6-ethoxybenzo[d]thiazol-2-yl)diazenyl)-4-hydroxyphenyl) acetamide hexahydrate; 4b: N-(4-Hydroxy-3-((6-methoxybenzo[d]thiazol-2-yl) diazenyl)phenyl)acetamide hexahydrate; MIC: minimum inhibitory concentration; NC: Negative control; PC: Positive control (ciprofloxacin, 0.25 µg/mL).
3.3.2. Antibacterial and Cytotoxic Activities of the Combination of Active Compounds with Selected Antibiotics
a. Fractional minimum inhibitory concentration indices (FICI)
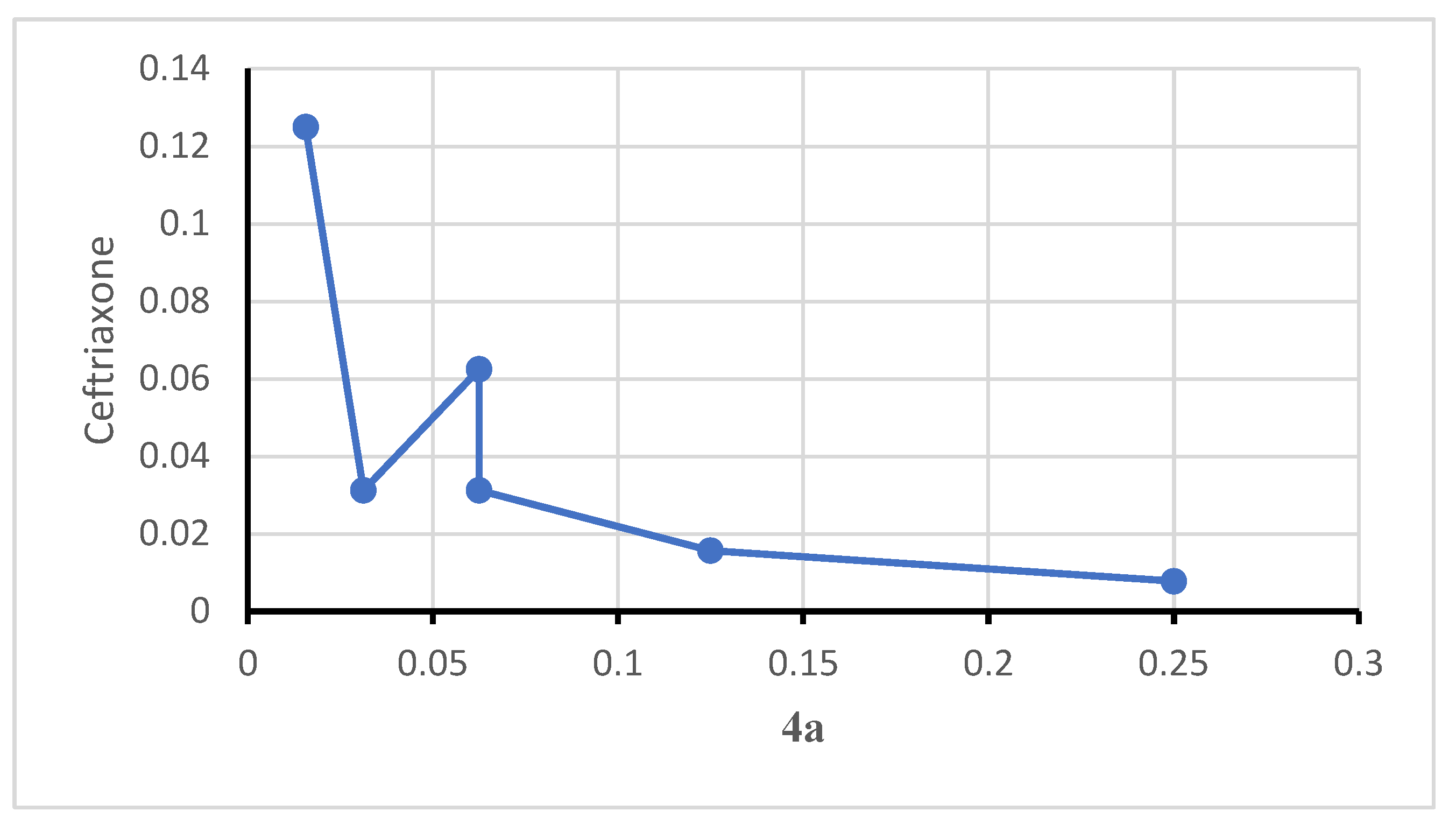
The most active antibacterial compounds (4a and 4b), and the least active antibiotics (cotrimoxazole and ceftriaxone), were selected for combination studies. Table 2 shows the synergistic interaction for all combinations, according to the calculated values of fractional minimum inhibitory concentrations (FICI ≤ 0.5), meaning a mutual potentiation of both azo-compounds and antibiotics (reduction of MIC value from 12.5 µg/mL to 0.097 µg/mL). The isobologram plotted from 4a FIC’s values versus ceftriaxone in Figure 4 has a convex appearance with a large number of points below the coordinate line (0.5-0.5), confirming the observed antibacterial effect.
Figure 4.
Isobologram representing the synergistic interaction between compound 4a and ceftriaxone on S. flexneri NR518.
Figure 4.
Isobologram representing the synergistic interaction between compound 4a and ceftriaxone on S. flexneri NR518.
b. Minimum inhibitory concentrations and selectivity indices of drug combinations
For each antibiotic-compound tandem, the combinations, which were chosen for MIC confirmation displayed the lowest FICI values as follows: 4a-cot (0.195 and 0.781 µg/mL, respectively), 4a-cef (0.390 and 0.390 µg/mL, respectively), 4b-cot (0.098 and 0.391 µg/mL, respectively), and 4b-cef (0.097 and 0.781 µg/mL, respectively). Table 3 summarizes the MIC values that ranged from 0.625 (4b-Cef) to 2.5 µg/mL (4a-Cot), confirming compound 4b as the best potential candidate for combination with both ceftriaxone and cotrimoxazole. Upon haemolytic studies, all combinations showed haemolytic percentages below 1% at 200 µg/mL, which value is negligible compared to the percentage obtained with the standard haemolytic agent triton X-100 (100% haemolysis). Moreover, the combinations of 4a and 4b with the antibiotics (ceftriaxone and cotrimoxazole) have selectively (SI: >80) eliminated the bacteria without causing any harm to red blood cells.
4. Discussion
Among children younger than 5 years, it is estimated that diarrhea is responsible for about 446 000 deaths, which are geographically concentrated in sub-Saharan Africa and South Asia [2]. Treatment options for bacterial diarrhea, such as shigellosis include antimicrobials, such as fluoroquinolones (first-line, preferably ciprofloxacin), cephalosporins (second-line), and β-lactams (second-line) [20]; however, the rise of antimicrobial-resistant enteric bacteria (Shigella) call for the need to search new and safe antishigellosis agents. Because of the dramatic increase and global spread of bacterial resistance to a number of commonly used antibacterial agents, many studies have been directed at investigating drugs whose primary therapeutic purpose is not antimicrobial action. Numerous studies report the antibacterial activity of non-steroidal anti-inflammatory drugs (NSAIDs), local anaesthetics, phenothiazines such as chlorpromazine, levomepromazine, promethazine, trifluoperazine, methdilazine and thioridazine, antidepressants, antiplatelets and statins [42]. Indeed, it has been demonstrated that a number of NSAIDs, like acetylsalicylic acid, diclofenac, and ibuprofen, have anti-biofilm activity, which could fuel an interest in repurposing these well tolerated drugs as adjunctive therapies for bacterial infections [35,43]. At therapeutic plasma levels, acetylsalicylic and salicylic acids inhibit the growth of Campylobacter pylori, Helicobacter pylori, and Klebsiella pneumoniae, as well as Epidermophyton floccosum, Microsporum spp., and Trichophyton spp. Acetylsalicylic acid is also active against Staphylococcus aureus by reducing fibronectin binding [42]. Furthermore, a number of bacteria, including Staphylococcus aureus and Paracoccus yeei were susceptible to lower concentrations of acetaminophen (MIC=1.25 mg/mL) suggesting the antibacterial potential of this NSAID [23]. On the other hand, the antibacterial potential of benzothiazoles is undeniable, as an important number of recent reports have described their efficacy against pathogenic microbes via numerous mechanisms of action, such as uridine diphosphate-n-acetyl enol pyruvyl glucosamine reductase (MurB) inhibition [44], DNA gyrase inhibition [45,46], peptide deformylase inhibition [47], aldose reductase inhibition [48], dihydroorotase inhibition [49], casdihydrofolate reductase inhibition [50], enoyl acyl carrier protein reductase inhibition [51], dialkylglycine decarboxylase inhibition [52], dehydrosqualene synthase inhibition [53], DNA gyrase and tyrosine kinase inhibition [54], dihydropteroate synthase inhibition [55] among others [56].
Based on these considerations, we report the antibacterial activity of acetaminophen hybrid compounds against a variety of Shigella species that causes diarrhea in humans. As a result, the diazobenzothiazole dyes 4a and 4b exhibited a common MIC value of 12.5 µg/mL, which qualifies these compounds as active anti-Shigella compounds with reference to reported threshold values for active antimicrobial potential compounds [57]. By contrast, the 2-aminobenzothiazoles 1a and 1b were poorly active against S. flexneri with common MIC value of 100 µg/mL, whereas acetaminophen (MIC value: >100 µg/mL) alone did not inhibit the growth of the Shigella species. The diazobenzothiazole backbone potentiated the antibacterial activity of acetaminophen. As already discussed, several benzothiazole-based compounds have shown promising activities against a number of Gram-negative bacteria [28]. In reported studies, plausible antibacterial mechanistic studies of benzothiazole-based compounds include (i) interference with cell wall synthesis, (ii) inhibition of DNA replication or protein synthesis, (iii) interference with nucleic acid synthesis, (iv) inhibition of biosynthetic pathways of essential compounds in bacterial cells, (v) disruption of membrane function and integrity, among others [49,58]. Furthermore, the incubation of Shigella with the active compounds showed a concentration- and time-dependent effects [59]. At 2 MIC and 4 MIC, compound 4a and 4b showed a bactericidal orientation as there was a continuous decrease in the bacterial population from 0 to 24 h. A similar trend was observed when the bacteria cells were treated with ciprofloxacin, the positive control. On the other hand, treatment at MIC showed almost similar trend like in 2 MIC and 4 MIC, although complete bacterial elimination was not achieved after 24 h of incubation as evidenced by the curve for MICs that did not overlap with the X axis. By contrast, MIC/2 and MIC/4 did not inhibit the bacterial growth as evidenced by the increase trend of the curves at these concentrations. These results are consistent with the antibiotic power (Pa=MBC/MIC: 25/12.5=2) obtained for both compounds 4a and 4b, which classify them as bactericidal according to the criteria reported by Dougnon et al. [60] that elaborate bactericidal (1≤MBC/MIC≤2) and bacteriostatic (4≤MBC/MIC≤16) effects of potential antimicrobial compounds based on the ratio MBC/MIC. A paper by Kohanski et al. in the September 7 issue of Cell [61] presented evidence that bactericidal antibiotics kill both Gram- and Gram+ bacteria by an as yet unappreciated mode: through overproduction of the destructive oxygen reduction product, the hydroxyl radical (HO·) [61]. The existence of drug resistant Shigella species have compelled many scientists to research on combination therapy that use two or more antibiotics with the goal of obtaining an enhanced antibacterial effect (synergistic activity) [62,63]. Indeed, as an expert opinion stated when conducting a review published in Expert Review of Anti-infective Therapy, Coates et al. [62] found antibiotic combination therapy, exploiting synergies, old-drug rejuvenation for resistance reduction as a promising solution to ampicillin resistance. From susceptibility assays, S. flexneri appeared as moderately resistant (MIC ≥ 8 μg/mL) towards cotrimoxazole and ceftriaxone (common MIC = 12.5 µg/mL) according to the classification criteria defined by Walsh [64]. Nguena-Dongue et al. [65] emitted the same conclusion when evaluating the potentiation effect of mallotojaponin B on chloramphenicol against methicillin resistant Staphylococcus aureus. Several authors reported the resistance of S. flexneri to both cotrimoxazole and ceftriaxone [7,13]. Combinatory assessment of compounds 4a and 4b with cotrimoxazole and ceftriaxone using a checkerboard method revealed a synergistic effect (mean FICI= 0.14) with significant MIC reduction (from 12.5 µg/mL to 0.097 µg/mL) suggesting a mutual potentiation of both compounds and antibiotics [41]. Nguena-Dongue et al. [65] mentioned the same antibacterial effect when he obtained a reduction in the MIC value of mallotojaponin B from 12.5 to 0.781 μg/ mL when combined with chloramphenicol. The optimal ratio combinations (with the lowest FICI) exhibited MIC values ranging from 0.625 (4b-Cef) to 2.5 µg/mL (4a-Cot) against S. flexneri, confirming 4b derivative as the best candidate for combination with both the ceftriaxone and cotrimoxazole. Several authors have reported the synergistic effect of cotrimoxazole and ceftriaxone with other antibiotics or small molecules [66,67]. Upon hemolysis assay, the non-cytotoxicity of 4a-Cot and 4b-Cef (HC50 ˃ 200 µg/mL; SI ˃ 80) toward red blood cells is noteworthy.
Overall, the present study demonstrated the antibacterial activity of two heterocyclic azo dyes incorporating moieties of acetaminophen, and their combination with selected antibiotics against Shigella-causing diarrhea. The mechanistic basis of the antibacterial action revealed bactericidal orientation at 2 MIC and 4 MIC, whereas the hemolysis test showed non toxicity of test compounds and their combination with selected antibiotics (ceftriaxone and cotrimoxazole).
5. Conclusions
In this study, the antibacterial activity of acetaminophen 3 and its diazobenzothiazole derivatives 4 (a & b) was evaluated against four strains of Shigella, the pathogens responsible of infectious diarrhea. Acetaminophen 3, which is a well-known anti-inflammatory, analgesic and antipyretic drug used to treat pain and fever was used to synthesize a series azo dyes incorporating moieties of acetaminophen 4. Upon in vitro anti-Shigella assays, these compounds exhibited antibacterial activity against Shigella flexneri. The combination of the azo dyes 4 (a & b) with cotrimoxazole and ceftriaxone showed a synergistic antibacterial effect and high selectivity vis-à-vis human red blood cells. These compounds were established through a time-kill kinetics study to be bactericidal and might serve as scaffolds for repurposing acetaminophen from its traditional use as an anti-inflammatory and antipyretic drug to potentially active anti-diarrheal agents against Shigella-causing diarrhea.
Author Contributions
Conceptualization, B.P.K, F.F.B., and J.T.; methodology, B.R.P., B.-L.M.K., A.Y.K., B.A.K., and O.G.; software, B.-L.M.K., B.R.P., A.Y.K., B.A.K., O.G., and P.M.; validation, J.T.; P.M., B.P.K, and F.F.B.; formal analysis, B.R.P., B.-L.M.K., and A.Y.K.; investigation, B.R.P., B.-L.M.K., A.Y.K., B.A.K., and O.G.; resources, B.P.K, and F.F.B.; data curation, B.R.P., P.M., and A.Y.K.; writing—original draft preparation, B.R.P., B.-L.M.K., A.Y.K., B.A.K., and O.G.; writing—review and editing, J.T., P.M., and F.F.B.; visualization, P.M., J.T., B.P.K, and F.F.B.; supervision, B.P.K, J.T., and F.F.B.; project administration, B.P.K, J.T., and F.F.B.; funding acquisition, B.P.K, and F.F.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received funding from the Yaounde–Bielefeld Bilateral Graduate School for Natural Products with Anti-parasite and Antibacterial Activity (YaBiNaPA) (grant number 57316173) and Seeding Labs’ Instrumental Access.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data is available from the corresponding author (s) upon reasonable request. The data are not publicly available due to the sensitive nature of the research supporting data.
Acknowledgments
The authors are grateful to BEI resources (Biodefense and Emerging Infections Research Resources Repository) for providing the three bacterial strains Shigella flexneri NR 518, Shigella boydii NR 521 and Shigella sonnei NR 519, and the Centre Pasteur of Cameroon for providing the clinical isolate, Shigella dysenteriae. This research received support, material and equipment from the Yaoundé–Bielefeld Bilateral Graduate School for Natural Products with Anti-parasite and Antibacterial Activity (YaBiNaPA).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Tarr, P.I.; Bass, D.M.; Hecht, G.A. Bacterial, viral, and toxic causes of diarrhea, gastroenteritis, and anorectal infections In: Yamada T, ed. Textbook of Gastroenterology. fifth ed. Blackwell; 2009, 1157-1224.
- The World Health Organization (WHO), 2023. Diarrheal disease. The Fact Sheets. https://www.who.int/health-topics/diarrhoea#tab=tab_3, Accessed on 30th August 2023.
- Ammoury, R.F.; Ghishan, F.K. Pathophysiology of diarrhea and its clinical implications, In J. D. W, Johnson Leonard R., Ghishan Fayez K., Kaunitz Jonathan D., Merchant Juanita L., Said Hamid M. (Ed.), Physiology of the Gastronintestinal Tract, Fifth Edit, Elsevier Inc, 2012, pp. 2183–2198.
- Ezekwesili, C.N.; Obiora, K.A.; Ugwu, O.P. Evaluation of anti-diarrhoeal property of crude aqueous extract of Ocimum gratissimum L. (Labiatae) in rats. Biokemistri. 2004, 16, 122–131. [Google Scholar] [CrossRef]
- Kotloff, K.L.; Riddle, M.S.; Platts-Mills, J.A.; Pavlinac, P.; Zaidi, A.K.M. Shigellosis. Lancet (London, England) 2018, 391, 801–812. [Google Scholar] [CrossRef]
- Ndze, V.N.; Akum, A.E.; Kamga, G.H.; Enjema, L.E.; Esona, M.D.; Banyai, K.; Therese, O.A. Epidemiology of rotavirus diarrhea in children under 5 years in Northern Cameroon. Pan. Afr. Med. J. 2012, 11, 73. [Google Scholar] [PubMed]
- Taneja, N.; Mewara, A. Shigellosis: epidemiology in India. Indian J. Med. Res. 2016, 143, 565–576. [Google Scholar] [CrossRef] [PubMed]
- Khalil, I.A.; Troeger, C.; Blacker, B.F.; Rao, P.C.; Brown, A.; Atherly, D.E.; Brewer, T.G.; Engmann, C.M.; Houpt, E.R.; Kang, G.; Kotloff, K.L.; Levine, M.M.; Luby, S.P.; MacLennan, C.A.; Pan, W.K.; Pavlinac, P.B.; Platts-Mills, J.A.; Qadri, F.; Riddle, M.S.; Ryan, E.T.; Shoultz, D.A.; Steele, A.D.; Walson, J.L; Sanders, JW.; Mokdad, A.H.; Murray, C.J.L.; Hay, S.I.; Reiner, R.C.Jr. Morbidity and mortality due to shigella and enterotoxigenic Escherichia coli diarrhoea: the global burden of disease study 1990-2016. Lancet Infect. Dis. 2018, 18, 1229–1240. [Google Scholar] [CrossRef] [PubMed]
- Kahsay, A.G.; Muthupandian, S. A review on sero diversity and antimicrobial resistance patterns of Shigella species in Africa, Asia and South America, 2001–2014. BMC Res. Notes. 2016, 9, 422. [Google Scholar] [CrossRef]
- Chatterjee, S.; Raval, I.H. Chapter 32 - Pathogenic Microbial Genetic Diversity with Reference to Health in Microbial Diversity in the Genomic Era, 2019, Pages 559-577.
- Stażyk, K.; Krycińska, R.; Jacek, C.; Garlicki, A.; Biesiada, G. Diarrhea caused by Shigella flexneri in patients with primary HIV infection. Int. J. STD AIDS. 2019, 30, 814–814. [Google Scholar] [CrossRef]
- Nisa, I.; Qasim, M.; Driessen, A.; Nijland, J.; Bari, F.; Haroon, M.; Rahman, H.; Yasin, N.; Khan, T.A.; Hussain, M.; Ullah, W. Molecular epidemiology of Shigella flexneri isolated from pediatrics in a diarrhea-endemic area of Khyber. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 971–985. [Google Scholar] [CrossRef]
- Puzari, M.; Sharma, M.; Chetia, P. Emergence of antibiotic resistant Shigella species: A matter of concern. J. Infect. Public Health 2018, 11, 451–454. [Google Scholar] [CrossRef]
- Sur, D.; Ramamurthy, T.; Deen, J.; Bhattacharya, S.K. Shigellosis: challenges & management issues. Indian J. Med. Res. 2004, 120, 454–462. [Google Scholar]
- Thorley, K.; Charles, H.; Greig, D.R.; Prochazka, M.; Mason, L.C.E.; Baker, K.S.; Godbole, G.; Sinka, K.; Jenkins, C. Emergence of extensively drug-resistant and multidrug-resistant Shigella flexneri serotype 2a associated with sexual transmission among gay, bisexual, and other men who have sex with men, in England: a descriptive epidemiological study. Lancet Infect. Dis. 2023, 23, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Faure, C. Role of antidiarrhoeal drugs as adjunctive therapies for acute diarrhoea in children. Int. J. Pediatrics 2013, 2013, 612403. [Google Scholar] [CrossRef] [PubMed]
- Broder, M.S.; Chang, E.; Romanus, D.; Cherepanov, D.; Neary, M.P. Healthcare and economic impact of diarrhea in patients with carcinoid syndrome. World J. Gastroenterol. 2016, 22, 2118–2125. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, E.; Abtahi, H.; van Belkum, A.; Ghaznavi-Rad, E. Multidrug-resistant Shigella infection in pediatric patients with diarrhea from central Iran. Infect. Drug Resist. 2019, 12, 1535–1544. [Google Scholar] [CrossRef] [PubMed]
- Khaghani, S.; Shamsizadeh, A.; Nikfar, R.; Hesami, A. Shigella flexneri: a three-year antimicrobial resistance monitoring of isolates in a Children Hospital, Ahvaz, Iran. Iran J. Microbiol. 2014, 6, 225–229. [Google Scholar] [PubMed]
- Williams, P.C.M.; Berkley, J.A. Guidelines for the treatment of dysentery (shigellosis): a systematic review of the evidence. Paediatrics and International Child Health 2018, 38, S50–S65. [Google Scholar] [CrossRef] [PubMed]
- Ranjbar, R.; Farahani, A. Shigella: Antibiotic-resistance mechanisms and new horizons for treatment. Infect. Drug Resist. 2019, 12, 3137–3167. [Google Scholar] [CrossRef] [PubMed]
- Bunchorntavakul, C.; Reddy, K.R. Acetaminophen-related hepatotoxicity. Clin. Liver Dis. 2013, 17, 587–607. [Google Scholar] [CrossRef] [PubMed]
- Al-Janabi, A.A. In vitro antibacterial activity of Ibuprofen and acetaminophen. J. Glob. Infect. Dis. 2010, 2, 105–108. [Google Scholar] [CrossRef]
- McGill, M.R.; Jaeschke, H. Metabolism and disposition of acetaminophen: recent advances in relation to hepatotoxicity and diagnosis. Pharm. Res. 2013, 30, 2174–2187. [Google Scholar] [CrossRef]
- Chiew, A.L.; Buckley, N.A. Acetaminophen poisoning. Crit. Care Clin. 2021, 37, 543–561. [Google Scholar] [CrossRef] [PubMed]
- Seo, K.W.; Park, M.; Kim, J.G.; Kim, T.W.; Kim, H.J. Effects of benzothiazole on the xenobiotic metabolizing enzymes and metabolism of acetaminophen. J. Appl. Toxicol. 2000, 20, 427–430. [Google Scholar] [CrossRef] [PubMed]
- Cabrera-Pérez, L.C.; Padilla-Martínez, I.I.; Cruz, A.; Mendieta-Wejebe, J.E.; Tamay-Cach, F.; Rosales-Hernández, M.C. Evaluation of a new benzothiazole derivative with antioxidant activity in the initial phase of acetaminophen toxicity. Arab. J. Chem 2019, 12, 3871–3882. [Google Scholar] [CrossRef]
- Tsemeugne, J.; Nangmo, P.K.; Mkounga, P.; Tamokou, J.D.D.; Kengne, I.C.; Edwards, G.; Sopbué, E.F.; Nkengfack, A.E. Synthesis, characteristic fragmentation patterns, and antibacterial activity of new azo compounds from the coupling reaction of diazobenzothiazole ions and acetaminophen. Heterocycl. Commun. 2021, 27, 79–89. [Google Scholar] [CrossRef]
- Sharma, P.C.; Kumar, R.; Chaudhary, M.; Sharma, A.; Rajak, H. Synthesis and biological evaluation of novel benzothiazole clubbed fluoroquinolone derivatives. J. Enzyme Inhib. Med. Chem. 2013, 28, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Gaffer, H.E.; Fouda, M.M.G.; Khalifa, M.E. Synthesis of some novel 2-amino-5-arylazothiazole disperse dyes for dyeing polyester fabrics and their antimicrobial activity. Molecules 2016, 21, 122–131. [Google Scholar] [CrossRef] [PubMed]
- Gjorgjieva, M.; Tomašič, T.; Kikelj, D.; Mašič, L.P. Benzothiazole-based compounds in antibacterial drug discovery. Curr. Med. Chem. 2018, 25, 5218–5236. [Google Scholar] [CrossRef] [PubMed]
- Haroun, M. Review on the developments of benzothiazole-containing antimicrobial agents. Curr. Top. Med. Chem. 2022, 22, 2630–2659. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; Luo, J.; Deng, F.; Huang, Y.; Zhou, H. Antibiotic combination therapy: A strategy to overcome bacterial resistance to aminoglycoside antibiotics. Front. Pharmacol. 2022, 13, 1–15. [Google Scholar] [CrossRef]
- Abidi, S.H.; Ahmed, K.; Kazmi, S.U. The antibiofilm activity of acetylsalicylic acid, mefenamic acid, acetaminophen against biofilms formed by P. aeruginosa and S. epidermidis. J. Pak. Med. Assoc. 2019, 69, 1493–1495. [Google Scholar]
- Paes Leme, R.C.; da Silva, R.B. Antimicrobial activity of non-steroidal anti-inflammatory drugs on biofilm: Current evidence and potential for drug repurposing. Front. Microbiol. 2021, 12, 707629. [Google Scholar] [CrossRef]
- CLSI, 2012. CLSI Publishes 2012 Antimicrobial Susceptibility Testing Standards—Medical Design and Outsourcing. https://www.medicaldesignandoutsourcing.com/clsi-publishes-2012-antimicrobial-susceptibility-testing-standards/ (accessed 6.7.23).
- Sinha, S.; Batovska, D.I.; Medhi, B.; Radotra, B.D.; Bhalla, A.; Markova, N.; Sehgal, R. In vitro anti-malarial efficacy of chalcones: cytotoxicity profile, mechanism of action and their effect on erythrocytes. Malar. J. 2019, 18, 421. [Google Scholar] [CrossRef]
- Fidock, D.A.; Rosenthal, P.J.; Croft, S.L.; Brun, R.; Nwaka, S. Antimalarial drug discovery: efficacy models for compound screening. Nat. Rev. Drug Discov. 2004, 3, 509–520. [Google Scholar] [CrossRef]
- Melogmo Dongmo, Y.K.; Tchatat Tali, M.B.; Dize, D.; Jiatsa Mbouna, C.D.; Kache Fotsing, S.; Ngouana, V.; Pinlap, B.R.; Zeuko’o Menkem, E.; Yamthe Tchokouaha, L.R.; Fotso Wabo, G.; Lenta Ndjakou, B.; Lunga, P.K.; Fekam Boyom, F. Anti-Shigella and antioxidant-based screening of some Cameroonian medicinal plants, UHPLC-LIT-MS/MS fingerprints, and prediction of pharmacokinetic and drug-likeness properties of identified chemicals. J. Ethnopharmacol. 2024, 324, 117788. [Google Scholar] [CrossRef]
- Klepser, M.E.; Ernst, E.J.; Lewis, R.E.; Ernst, M.E.; Pfaller, M.A. Influence of test conditions on antifungal time-kill curve results: proposal for standardized methods. Antimicrob. Agents Chemother. 1998, 42, 1207–1212. [Google Scholar] [CrossRef]
- Bellio, P.; Fagnani, L.; Nazzicone, L.; Celenza, G. New and simplified method for drug combination studies by checkerboard assay. Methods X, 2021, 8, 101543. [Google Scholar] [CrossRef]
- Lagadinou, M.; Onisor, M.O.; Rigas, A.; Musetescu, D.-V.; Gkentzi, D.; Assimakopoulos, S.F.; Panos, G.; Marangos, M. Antimicrobial properties on non-antibiotic drugs in the Era of increased bacterial resistance. Antibiotics (Basel) 2020, 9, 1–12. [Google Scholar] [CrossRef]
- Dinarello, C.A. Anti-inflammatory agents: Present and future. Cell 2010, 140, 935–950. [Google Scholar] [CrossRef]
- Maliyappa, M.R.; Keshavayya, J.; Nazrulla, M.A.; Sudhanva, M.S.; Rangappa, S. Six-substituted benzothiazole based dispersed azo dyes having antipyrine moiety: synthesis, characterization, DFT, antimicrobial, anticancer and molecular docking studies. J. Iran Chem. Soc. 2022, 19, 3815–3835. [Google Scholar] [CrossRef]
- Nehra, N.; Tittal, R.K.; Ghule, V.D. 1,2,3-Triazoles of 8-Hydroxyquinoline and HBT: synthesis and studies (DNA binding, antimicrobial, molecular docking, ADME, and DFT. ACS Omega 2021, 6, 27089–27100. [Google Scholar] [CrossRef]
- Skok, Z.; Barančoková, M.; Benek, O.; Cruz, C.D.; Tammela, P.; Tomašič, T.; Zidar, N.; Mašič, L.P.; Zega, A.; Stevenson, C.E.M.; Mundy, J.E.A.; Lawson, D.M.; Maxwell, A.; Kikelj, D.; Ilaš, J. Exploring the chemical space of benzothiazole based DNA Gyrase B inhibitors. ACS Med. Chem. Lett. 2020, 11, 2433–2440. [Google Scholar] [CrossRef]
- Mishra, V.R.; Ghanavatkar, C.W.; Mali, S.N.; Chaudhari, H.K.; Sekar, N. Schiff base clubbed benzothiazole: synthesis, potent antimicrobial and MCF-7 anticancer activity, DNA cleavage and computational study. J. Biomol. Struct. Dyn. 2020, 38, 1772–1785. [Google Scholar] [CrossRef]
- Kousaxidis, A.; Kovacikova, L.; Nicolaou, I.; Stefek, M.; Geronikaki, A. Non-acidic bifunctional benzothiazole-based thiazolidinones with antimicrobial and aldose reductase inhibitory activity as a promising therapeutic strategy for sepsis. Med. Chem. Res. 2021, 30, 1837–1848. [Google Scholar] [CrossRef]
- Morsy, M.A.; Ali, E.M.; Kandeel, M.; Venugopala, K.N.; Nair, A.B.; Greish, K.; El-Daly, M. Screening and molecular docking of novel benzothiazole derivatives as potential antimicrobial agents. Antibiotics 2020, 9, 1–15. [Google Scholar] [CrossRef]
- Suyambulingam, J.K.; Karvembu, R.; Bhuvanesh, N.S.P.; Enoch, I.V.M.V.; Selvakumar, P.M.; Premnath, D.; Subramanian, C.; Mayakrishnan, P.; Kim, S.-H.; Chung, I.-M. Synthesis, structure, biological/chemosensor evaluation and molecular docking studies of aminobenzothiazole Schiff bases. J. Adhes. Sci. Technol. 2020, 34, 2590–2612. [Google Scholar] [CrossRef]
- Bhoi, M.N.; Borad, M.A.; Jethava, D.J.; Acharya, P.T.; Pithawala, E.A.; Patel, C.N.; Pandya, H.A.; Patel, H.D. Synthesis, biological evaluation and computational study of novel isoniazid containing 4H-Pyrimido [2,1-b] benzothiazoles derivatives. Eur. J. Med. Chem. 2019, 177, 12–31. [Google Scholar] [CrossRef]
- Mishra, V.R.; Ghanavatkar, C.W.; Mali, S.N.; Qureshi, S.I.; Chaudhari, H.K.; Sekar, N. Design, synthesis, antimicrobial activity and computational studies of novel azo linked substituted benzimidazole, benzoxazole and benzothiazole derivatives. Comput. Biol. Chem. 2019, 78, 330–337. [Google Scholar] [CrossRef]
- Gondru, R.; Sirisha, K.; Raj, S.; Gunda, S.K.; Kumar, C.G.; Pasupuleti, M.; Bavantula, R. Design, synthesis, in vitro evaluation and docking studies of pyrazole-thiazole hybrids as antimicrobial and antibiofilm agents. Chem. Sel. 2018, 3, 8270–8276. [Google Scholar] [CrossRef]
- Kumari, B.; Chauhan, K.; Trivedi, J.; Jaiswal, V.; Kanwar, S.S.; Pokharel, Y.R. Benzothiazole-based-bioconjugates with improved antimicrobial, anticancer and antioxidant potential. Chem. Sel. 2018, 3, 11326–11332. [Google Scholar] [CrossRef]
- Naaz, F.; Srivastava, R.; Singh, A.; Singh, N.; Verma, R.; Singh, V.K.; Singh, RK. Molecular modeling, synthesis, antibacterial and cytotoxicity evaluation of sulfonamide derivatives of benzimidazole, indazole, benzothiazole and thiazole. Bioorg. Med. Chem. 2018, 26, 3414–3428. [Google Scholar] [CrossRef]
- Kashyap, P.; Verma, S.; Gupta, P.; Narang, R.; Lal, S.; Devgun, M. Recent insights into antibacterial potential of benzothiazole derivatives. Med. Chem. Res. 2023, 32, 1543–1573. [Google Scholar] [CrossRef]
- Boniface, P.K.; Ferreira, E.I. Flavonoids as efficient scaffolds: Recent trends for malaria, leishmaniasis, Chagas disease, and dengue. Phytother. Res. 2019, 33, 2473–2517. [Google Scholar] [CrossRef]
- Baran, A.; Kwiatkowska, A.; Potocki, L. Antibiotics and bacterial resistance-A short story of an endless arms race. Int. J. Mol. Sci. 2023, 24, 1–34. [Google Scholar] [CrossRef]
- Adusei, E.B.A.; Adosraku, R.K.; Oppong-Kyekyeku, J.; Amengor, C.D.K.; Jibira, Y. Resistance modulation action, time-kill kinetics assay, and inhibition of biofilm formation effects of plumbagin from Plumbago zeylanica Linn. J. Trop. Med. 2019, 2019, 1250645. [Google Scholar] [CrossRef]
- Dougnon, V.; Hounsa, E.; Agbodjento, E.; Keilah, L.P.; Legba, B.B.; Sintondji, K.; Afaton, A.; Klotoe, J.R.; Baba-Moussa, L.; Bankole, H. Percentage destabilization effect of some West African medicinal plants on the outer membrane of various bacteria involved in infectious diarrhea. Biomed. Res. Int. 2021, 2021, 1–12. [Google Scholar] [CrossRef]
- Kohanski, M.A.; Dwyer, D.J.; Hayete, B.; Lawrence, C.A.; Collins, J.J. A common mechanism of cellular death induced by bactericidal antibiotics. Cell 2007, 130, 797–810. [Google Scholar] [CrossRef]
- Coates, A.R.M.; Hu, Y.; Holt, J.; Yeh, P. Antibiotic combination therapy against resistant bacterial infections: synergy, rejuvenation and resistance reduction. Expert Rev. Anti. Infect. Ther. 2020, 18, 5–15. [Google Scholar] [CrossRef]
- Murugaiyan, J.; Kumar, P.A.; Rao, G.S.; Iskandar, K.; Hawser, S.; Hays, J.P.; Mohsen, Y.; Adukkadukkam, S.; Awuah, W.A.; Jose, R.A.M.; Sylvia, N.; Nansubuga, E.P.; Tilocca, B..; Roncada, P.; Roson-Calero, N.; Moreno-Morales, J.; Amin, R.; Kumar, B.K.; Kumar, A.; Toufik, A.R.; Zaw, T.N.; Akinwotu, O.O.; Satyaseela, M.P.; van Dongen, M.B.M. Progress in alternative strategies to combat antimicrobial resistance: Focus on antibiotics. Antibiotics (Basel). 2022, 11, 200. [Google Scholar] [CrossRef]
- Walsh, C. Where will new antibiotics come from? Nat. Rev. Microbiol. 2003, 1, 65–70. [Google Scholar] [CrossRef]
- Nguena-Dongue, B.N.; Tchamgoue, J.; Ngandjui Tchangoue, Y.A.; Lunga, P.K.; Toghueo, K.R.M.; Zeuko, O.M.E.; Melogmo, Y.K.D.; Tchouankeu, J.C.; Kouam, S.F.; Fekam, B.F. Potentiation effect of mallotojaponin B on chloramphenicol and mode of action of combinations against Methicillin-resistant Staphylococcus aureus. PLoS One. 2023, 18, e0282008. [Google Scholar] [CrossRef]
- Ibezim, A.; Onuku, R.S.; Ibezim, A.; Ntie-Kang, F.; Nwodo, N.J.; Adikwu, M.U. Structure-based virtual screening and molecular dynamics simulation studies to discover new SARS-CoV-2 main protease inhibitors. Sci. Afr. 2021, 14, e00970. [Google Scholar] [CrossRef]
- Herrera-Hidalgo, L.; de Alarcón, A.; López-Cortes, L.E.; Luque-Márquez, R.; López-Cortes, L.F.; Gutiérrez-Valencia, A.; Gil-Navarro, M.V. Is once-daily high-dose ceftriaxone plus ampicillin an alternative for Enterococcus faecalis infective Endocarditis in outpatient parenteral antibiotic Therapy programs? Antimicrob. Agents Chemother. 2020, 65, e02099-20. [Google Scholar] [CrossRef]
Scheme 1.
Reactions’ sequences to the in situ formed diazonium intermediates 2.
Scheme 2.
Reactions’ sequences to compounds 4a and 4b.
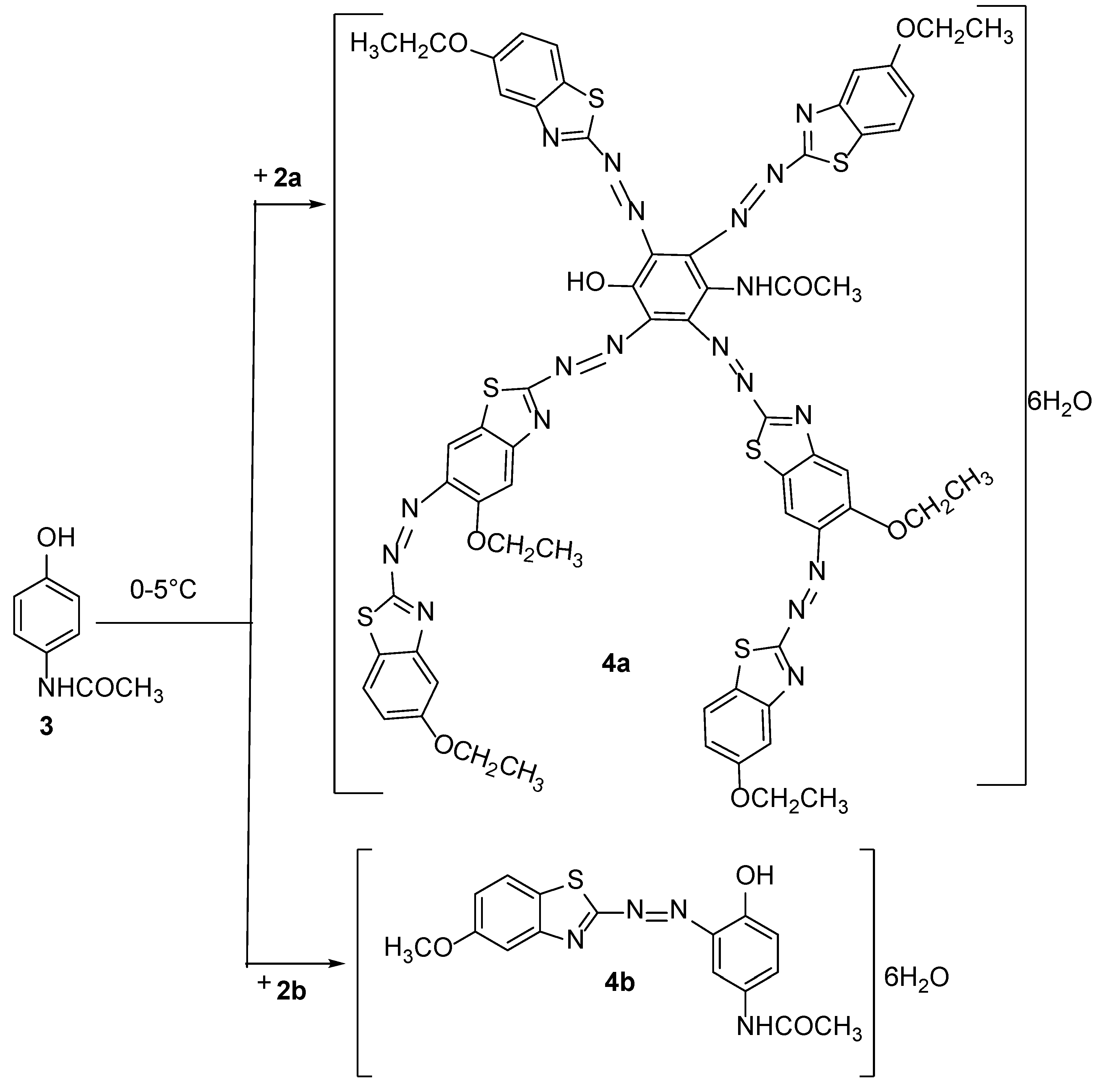

Table 1.
Antimicrobial activity (MIC in μg/mL), cytotoxic effect on red blood cells and selectivity indices of test compounds and selected antibiotics.
Table 1.
Antimicrobial activity (MIC in μg/mL), cytotoxic effect on red blood cells and selectivity indices of test compounds and selected antibiotics.
| Sample | Minimum inhibitory concentrations(µg/mL) | HC50 | SI (HC50/MIC50) | ||||
| SF NR 518 | SO NR 519 | SB NR 521 | SDcpc | ||||
| Compounds | 1a | 100 | - | - | - | ˃200 | ˃4 |
| 1b | 100 | - | - | - | ˃200 | ˃4 | |
| 3 | - | - | - | - | ˃200 | / | |
| 4a | 12.5 | 50 | - | - | 148.85±2.95 | 23.68 | |
| 4b | 12.5 | 50 | - | - | 87.52±0.7 | 13.92 | |
| Antibiotics | Amp | ˂0.062 | / | / | / | / | / |
| Cef | 12.5 | / | / | / | / | / | |
| Tet | ˂0.062 | / | / | / | / | / | |
| Cot | 12.5 | / | / | / | / | / | |
| Ciprofloxacin | 0.062 | 0.015 | 0.062 | 0.015 | / | / | |
SF: Shigella flexneri, SB: Shigella boydii, SO: Shigella sonnei, SD: Shigella dysenteriae; CPC: Centre Pasteur du Cameroun; Amp: Ampicillin; Cef: Ceftriaxone; Tet: Tetracycline; Cot: Cotrimoxazole; HC50: median haemolytic concentration; SI: Selectivity index -: ˃100µg/mL; /: Not determined.
Table 2.
Fractional minimum inhibitory concentration indices (FICI) of different combinations of compounds and antibiotics against Shigella flexneri NR518.
Table 2a.
FICI of different combinations of 4a and ceftriaxone against Shigella flexneri NR518.
| Corresponding MICs wells | Conc. 4a (µg/mL) | Conc. Cef (µg/mL) | FIC 4a | FIC Cef | FICI |
| H3 | 3.125 | 0.097 | 0.25 | 0.01 | 0.26 |
| G4 | 1.562 | 0.195 | 0.13 | 0.02 | 0.14 |
| F5 | 0.781 | 0.390 | 0.06 | 0.03 | 0.09 |
| E5 | 0.781 | 0.781 | 0.06 | 0.06 | 0.13 |
| F6 | 0.390 | 0.390 | 0.03 | 0.03 | 0.06 |
| D7 | 0.195 | 1.562 | 0.02 | 0.13 | 0.14 |
| D8 | 0.097 | 1.562 | 0.01 | 0.13 | 0.13 |
| Mean FICI (Interaction) | 0.14 (S) | ||||
Table 2b.
FICI of different combinations of 4a and cotrimoxazole against Shigella flexneri NR518.
| Corresponding MICs wells | Conc. 4a (µg/mL) | Conc. Cot (µg/mL) | FIC 4a | FIC cot | FICI |
| H3 | 3.125 | 0.097 | 0.25 | 0.01 | 0.26 |
| G3 | 3.125 | 0.195 | 0.25 | 0.02 | 0.27 |
| F4 | 1.562 | 0.390 | 0.13 | 0.03 | 0.16 |
| E5 | 0.781 | 0.781 | 0.06 | 0.06 | 0.13 |
| E6 | 0.390 | 0.781 | 0.03 | 0.06 | 0.09 |
| E7 | 0.195 | 0.781 | 0.02 | 0.06 | 0.08 |
| D8 | 0.097 | 1.562 | 0.01 | 0.13 | 0.13 |
| Mean FICI (Interaction) | 0.16 (S) | ||||
Table 2c.
FICI of different combinations of 4b and cotrimoxazole against Shigella flexneri NR518.
| Corresponding MICs wells | Conc. 4b (µg/mL) | Conc. Cot (µg/mL) | FIC 4b | FIC cot | FICI |
| H3 | 3.125 | 0.098 | 0.250 | 0.008 | 0.258 |
| G3 | 3.125 | 0.195 | 0.250 | 0.016 | 0.266 |
| G4 | 1.563 | 0.195 | 0.125 | 0.016 | 0.141 |
| G5 | 0.781 | 0.195 | 0.063 | 0.016 | 0.078 |
| F6 | 0.391 | 0.391 | 0.031 | 0.031 | 0.063 |
| E7 | 0.195 | 0.391 | 0.016 | 0.031 | 0.047 |
| E8 | 0.098 | 0.391 | 0.008 | 0.031 | 0.039 |
| Mean FICI (Interaction) | 0.127 (S) | ||||
Table 2d.
FICI of different combinations of 4b and Ceftriaxone against Shigella flexneri NR518.
| Corresponding MICs wells | Conc. 4b (µg/mL) | Conc. Cef (µg/mL) | FIC 4b | FIC Cef | FICI |
| H3 | 3.125 | 0.097 | 0.25 | 0.01 | 0.26 |
| G3 | 3.125 | 0.195 | 0.25 | 0.02 | 0.27 |
| F4 | 1.562 | 0.390 | 0.13 | 0.03 | 0.16 |
| E5 | 0.781 | 0.781 | 0.06 | 0.06 | 0.13 |
| E6 | 0.390 | 0.781 | 0.03 | 0.06 | 0.09 |
| E7 | 0.195 | 0.781 | 0.02 | 0.06 | 0.08 |
| E8 | 0.097 | 0.781 | 0.01 | 0.06 | 0.07 |
| Mean FICI (Interaction) | 0.15 (S) | ||||
Capital letters affected with a number indicate the wells representing the different pairs of concentrations considered as MICs; 4a: N-(2-(6-Ethoxy-5-((6-ethoxybenzo [d]thiazol-2-yl)diazenyl)benzo[d]thiazol-2-yl)diazenyl)-3-((6-ethoxy-5-((6-ethoxybenzo[d]thiazol-2-yl)diazenyl) benzo[d]thiazol-2-yl)diazenyl)-5,6-bis((6-ethoxybenzo[d]thiazol-2-yl)diazenyl)-4-hydroxyphenyl) acetamide hexahydrate; 4b: N-(4-Hydroxy-3-((6-methoxybenzo[d]thiazol-2-yl) diazenyl)phenyl)acetamide hexahydrate; Cef: Ceftriaxone; Conc: Concentration (µg/mL); Cot: Cotrimoxazole; FIC: Fractional minimum inhibitory concentration; FICI: Fractional minimum Inhibitory concentration index; S: Synergistic effect.
Table 3.
Minimum inhibitory concentrations of the most potent drug combinations on S. flexneri NR 518.
Table 3.
Minimum inhibitory concentrations of the most potent drug combinations on S. flexneri NR 518.
| Combinations | MIC (µg/mL) on S. flexneri | HC50 (µg/mL) | SI (HC50/MIC50) |
| 4a-Cot | 2.5 | ˃200 | ˃80 |
| 4a-Cef | 1.25 | ˃200 | ˃160 |
| 4b-Cot | 0.625 | ˃200 | ˃320 |
| 4b-Cef | 0.625 | ˃200 | ˃320 |
| Ciprofloxacin | 0.062 | / | / |
4a: N-(2-(6-Ethoxy-5-((6-ethoxybenzo [d]thiazol-2-yl)diazenyl)benzo[d]thiazol-2-yl)diazenyl)-3-((6-ethoxy-5-((6-ethoxybenzo[d]thiazol-2-yl)diazenyl) benzo[d]thiazol-2-yl)diazenyl)-5,6-bis((6-ethoxybenzo[d]thiazol-2-yl)diazenyl)-4-hydroxyphenyl) acetamide hexahydrate; 4b: N-(4-Hydroxy-3-((6-methoxybenzo[d]thiazol-2-yl) diazenyl)phenyl)acetamide hexahydrate; Cef: Ceftriaxone; Cot: Cotrimoxazole, HC50: Median haemolytic concentration; MIC: minimum inhibitory concentration; SI: Selectivity index.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



