
Submitted:
15 January 2024
Posted:
16 January 2024
You are already at the latest version
Abstract
Diarrhea-related mortality remains an important public health concern, particularly in developing countries, and has become difficult to treat because of antibacterial resistance. The development of synergistic antimicrobial agents appears to be a promising alternative treatment against diar-rheal infections. In this study, the combined effect of tetracycline together with either nitroxoline, sanguinarine, or zinc pyrithione (representing various classes of alkaloid-related compounds) was evaluated in vitro against selected diarrheagenic bacteria (Enterococcus faecalis, Escherichia coli, Listeria monocytogenes, Shigella flexneri, Vibrio parahaemolyticus, and Yersinia enterocolitica). The chequerboard method in 96-well microtiter plates was used to determine the sum of the fractional inhibitory concentration indices (FICIs). Three independent experiments were performed per combination, each in triplicate. It was observed that the combinations of tetracycline with either nitroxoline, sanguinarine, or zinc pyrithione produced synergistic effects against most of the pathogenic bacteria tested, with FICI values ranging from 0.086 to 0.5. Tetracycline-nitroxoline combinations produced the greatest synergistic action against S. flexneri at a FICI value of 0.086. Combinations of the agents tested in this study can thus be used for the development of new anti-diarrheal medications. However, studies focusing on their in vivo anti-diarrheal activity and safety are required before any consideration for utilization in human medicine.
Keywords:
antimicrobial agents
; combination therapy
; diarrhoea
; multidrug resistance
; pathogens
; synergistic effect
1. Introduction
Diarrhea is a worldwide problem [1] and is a major cause of infant and childhood morbidity and mortality in developing countries [2]. Because of diarrhea, about 525 000 children under the age of five years old die every year globally [3]. The most common pathogens that cause diarrhea are parasites, viruses, and bacteria (e.g., Escherichia coli, Salmonella spp., Shigella spp., and Vibrio cholerae) [4]. Oral rehydration and antibiotics (e.g., ciprofloxacin, metronidazole, and tetracycline) are commonly used as therapy for diarrheal infections [5]. However, the extensive use of antibiotics disrupts the normal balance of the gut microbiota which protects against infectious diarrhea [6,7,8]. For instance, it has been reported that ceftriaxone, when ingested, can change the gut microbiota composition and cause diarrhea in up to 50% of children [9]. Furthermore, the misuse of antibiotics can lead to the development of bacterial resistance, which is currently a threat to public health and safety, as it contributes to the difficulty of treating infections and results in increased mortality rates [10]. It has been reported that because of infections caused by multi-drug-resistant bacteria, nearly 700,000 people die every year [11]. Under these circumstances, alternative antimicrobial agents and approaches are needed, such as the combined use of synergistic antimicrobial agents, to reduce the prevalence of diarrhea whilst preventing the emergence of multidrug resistance in bacteria.
Combination therapy, based on the synergistic action of antimicrobial agents, is an emerging pharmacological strategy that is effective for the treatment of various infectious diseases. Antimicrobial combinations can be classified as synergistic when the interaction of two or more agents results in a combined effect that is greater than the sum of their activities when used individually. The use of synergistic antimicrobial combinations results in decreased therapeutical doses and/or minimum inhibitory concentrations (MICs) of the agents [12]. On the contrary, antagonism is a condition where one of the agents mitigates the action of the other and the combination is less effective than a single agent at the same concentration [13]. In recent times, the approach of utilizing synergism has drawn the attention of many researchers and pharmaceutical industries in an attempt to develop antibacterial agents with different mechanisms of actions that can decrease the required dosage of individual antimicrobials and broaden the spectrum of antimicrobial activity against diarrheal pathogens [14]. For example, a synergistic antimicrobial effect between tetracycline and amoxicillin has been observed against the diarrheal pathogens Bacillus cereus, Enterococcus faecalis, and S. typhi [15]. The combination of β-lactams and inhibitors of β-lactamases, such as ampicillin with sulbactam (Unasyn, Pfizer, New York, US), is currently used to treat intra-abdominal infections caused by β-lactamase-producing strains of Bacteroides fragilis, Enterobacter spp., E. coli, and Klebsiella spp. [16]. The results of previous experiments suggest that combining conventional antibiotics with non-antibiotic agents, whose antibacterial effect is based on different mechanisms of action (e.g., plant alkaloids), can be an efficient approach for the discovery of drugs designed to combat diarrhea. For example, the combination of tetracycline with berberine considerably reduced the volume, frequency, and duration of diarrhea in patients in a randomized double-blind placebo clinical trial [17]. Another study reported the in vitro growth-inhibitory activity of sanguinarine in combination with streptomycin against a clinical isolate of a diarrhea-causing E. coli [18]. Nevertheless, the antidiarrheal potential of the combinations of antibiotics with alkaloid compounds has not yet been fully explored.
Alkaloids are organic compounds of natural origin which contain at least one nitrogen atom in their molecule [19,20]. The structural modifications of alkaloids have served as a basis for the development of many semisynthetic and synthetic drugs currently used in clinical practice [21]. Recently, the alkaloid sanguinarine and synthetic alkaloid analogues nitroxoline and zinc pyrithione have attracted the attention of researchers as compounds that are able to enhance the activity of antibiotics against diarrheagenic bacteria. Sanguinarine, a benzylisoquinoline alkaloid isolated from Sanguinaria canadensis [22], is commonly used in mouthwash and toothpaste to treat and prevent gingivitis and related inflammatory conditions [23,24]. It has demonstrated a synergistic effect against diarrheal pathogens when combined with ciprofloxacin [25]. Similarly, nitroxoline is a drug used to treat infectious and inflammatory urogenital tract diseases [26], and has showed synergism when used in combination with ciprofloxacin against strains of diarrhea-causing bacteria [25]. This agent is a derivative of 8-hydroxyquinoline, which is a compound previously detected in Centaurea diffusa [27]. In addition, zinc pyrithione is a metal complex of pyrithione (a compound isolated from Polyalthia nemoralis) [28] that is commonly used in cosmetic products to treat skin infections (e.g., dandruff caused by Malassezia spp. [29,30]). Zinc pyrithione produces synergistic antibacterial effects when combined with ciprofloxacin [25]. However, studies aimed at identifying the possible interactions of nitroxoline, sanguinarine, and zinc pyrithione with other antibiotics is not currently known. Since tetracycline has shown synergistic antibacterial activities when used together with various other plant-derived agents [31,32], this study evaluates the combined effects of tetracycline with the above-mentioned alkaloid-related compounds against diarrhea-causing bacteria, namely, E. faecalis, E. coli, Listeria monocytogenes, S. flexneri, V. parahaemolyticus and Yersinia enterocolitica in vitro.
2. Results
When tetracycline was used in combination with either nitroxoline, sanguinarine, or zinc pyrithione, synergistic activity was observed against several diarrhea-causing bacteria. According to the FICs values, and the number of bacterial strains susceptible to the combination of agents tested, tetracycline produced the strongest interaction when combined with nitroxoline, followed by zinc pyrithione, and sanguinarine.
Table 1 shows the individual and combined MICs of tetracycline and nitroxoline against the selected diarrhea-causing bacteria, together with their corresponding fractional inhibitory concentration indices (FICIs). The tetracycline-nitroxoline combination produced various synergistic interactions against all bacterial strains, and the sum of the FICIs ranged from 0.086 to 0.5. The greatest synergistic effect was observed against S. flexneri (FICI: 0.086) at 0.063 µg/mL nitroxoline, resulting in a 16-fold decrease in tetracycline MIC (from 4 to 0.25 µg/mL). Additionally, the greatest MIC reduction (from 0.667 to 0.083 µg/mL) for tetracycline was observed against L. monocytogenes, at 0.5 µg/mL nitroxoline (FICI: 0.156).
The combination of tetracycline and zinc pyrithione produced synergistic antibacterial effects against five out of the six diarrhea-causing pathogens (FICI ranging from 0.109 to 0.479; Table 2). The greatest synergistic effect was documented against S. flexneri (FICI value of 0.109), resulting in an 11-fold decrease in tetracycline MIC (from 5.333 to 0.5 µg/mL) at a zinc pyrithione concentration of 0.125 µg/mL. Also, the greatest tetracycline MIC reduction was reported against V. parahaemolyticus, at a zinc pyrithione concentration of 1 µg/mL, which resulted in a 129-fold decrease of the MIC of tetracycline (from 4 to 0.031 µg/mL) and a FICI of 0.133.
The tetracycline-sanguinarine combination demonstrated synergistic interactions against two out of the six diarrheal bacteria evaluated, with FICI values ranging from 0.288 to 0.5 (Table 3). The greatest synergistic effect was achieved against L. monocytogenes (FICI value of 0.288) at a sanguinarine concentration of 0.125 µg/mL, which caused a four-fold tetracycline MIC decrease (from 0.5 to 0.125 µg/mL). Furthermore, the greatest tetracycline MIC reduction was also observed for this bacterium (FICI of 0.428), where 1 µg/mL of sanguinarine caused an eight-fold reduction of tetracycline MIC (from 0.5 to 0.063 µg/mL).
Isobologram curves established from the results of the chequerboard assays and the calculated FICI values for the most-susceptible bacteria are presented in Figure 1. The axes of each isobologram represent the dose-axes of the individual agents. The isobolograms confirmed the synergistic antimicrobial effects of tetracycline when combined with either nitroxoline, sanguinarine, or zinc pyrithione against E. faecalis, E. coli, L. monocytogenes, S. flexneri, V. parahaemolyticus, and Y. enterocolitica. Synergy was observed for three ratios in the isobolograms of each bacterial pathogen. The concave isobole (represented by the round dotted lines) indicates the confirmation of antimicrobial synergy observed against the tested diarrhea-causing bacteria.
3. Discussion
According to the Clinical and Laboratory Standards Institute (CLSI) antimicrobial susceptibility testing breakpoint data interpretation [33], the MIC range of tetracycline observed in this study (0.5 to 8 µg/mL) proves sensitivity of most of the diarrheagenic bacteria to this antibiotic. Previously reported MIC values for tetracycline against E. faecalis, E. coli, V. parahaemolyticus and Y. enterocolitica were in the respective ranges of 0.5 to 32, 0.5 to 64, 0.06 to 2, and 2 to 4 µg/mL [34,35,36,37], which correspond with the findings of the current study. In contrast to the MICs determined in the current study for L. monocytogenes and S. flexneri, other researchers have reported higher MICs values (≥ 256 µg/mL) [38,39]. The variations in susceptibility of both bacteria to tetracycline (observed in the current study vs. the previously published data) can be explained by the use of different strains. Despite the fact that the antibacterial activities of nitroxoline, sanguinarine, and zinc pyrithione have been demonstrated in various studies, data on their in vitro growth-inhibitory effects against the diarrheic bacteria tested in the present study are limited. The MIC values observed for the tested antimicrobial compounds in the current study are well corresponding with the results of recently published data from the same laboratory, demonstrating their effectiveness against most of the tested diarrheal pathogens at MICs ranging from 2 to 512 µg/mL [25,40]. Synergistic effects of tetracycline and other antibiotics (e.g., augmentin and ciprofloxacin) have previously been documented for some selected diarrhea-causing bacteria isolated from poultry droppings [41]. Although synergistic effects of nitroxoline, sanguinarine, and zinc pyrithione with antibiotics have previously been reported [25], the combined growth-inhibitory activity of these agents with tetracycline against diarrhea-causing bacteria is reported for first time in this study. Tetracycline inhibits bacterial protein synthesis by preventing the association of aminoacyl-transfer ribonucleic acid (tRNA) with the 30S subunit of the bacterial ribosome [42]. In addition, tetracycline forms a complex with magnesium ions (Mg2+) and binds to the A-site of ribosomes [43,44]. Although the details of its mechanism of action are still not elucidated, it is known that the antibacterial activity of nitroxoline is due to its indirect ability to chelate cations essential for bacterial growth, especially Mg2+ [45,46]. Similarly, zinc pyrithione chelates metal ions, including Mg2+ [47]. In order to diffuse through the bacterial cell membrane, tetracycline has to be fully protonated because the Mg-chelate cannot enter the cell [45]. Therefore, it is possible to assume that nitroxoline and zinc pyrithione scavenge Mg2+ from the environment, which creates favorable conditions for tetracycline to enter the bacterial cell membrane. Inside of the cell, tetracycline forms a complex with Mg2+, which is the only form which is able to inhibit bacterial growth by binding to the bacterial 30S ribosomal subunit. The chelation properties of all three agents may therefore contribute to their synergistic antibacterial activity. In the present study, the combination of sanguinarine with tetracycline produced a synergistic growth-inhibitory effect against Gram-positive bacteria. Since it has previously been suggested that the anti-staphylococcal action of sanguinarine is based on its ability to compromise the cytoplasmic membrane [48], it can be hypothesized that this compound can help tetracycline to enter the bacteria by disturbing the cell membrane. Subsequently, tetracycline can effectively inhibit bacterial protein synthesis inside the cell. Both antibacterial agents can therefore act together against E. faecalis and L. monocytogenes (as examined in the present study) through their synergistic activity.
Because both tetracycline and nitroxoline are drugs commonly used in clinical practice for the treatment of bacterial infections, their combined use could improve the efficacy of tetracycline against gastrointestinal diseases caused by diarrheagenic bacteria, because nitroxoline would chelate cations (e.g., calcium, Mg2+) which are reported to lower the absorption of this antibiotic in the gut [49,50]. In addition, as the above-mentioned antibacterial agents are used for the management of urinary tract infections (UTIs) [51,52], their combination could also be a potential treatment strategy against increased acquired resistance to orally administered antibiotics against E. coli caused UTIs [26], which has been a growing healthcare concern worldwide. The use of sanguinarine in pharmacological preparations is probably not feasible because it is slightly toxic when administered orally to rats, with a median lethal dose (LD50) value of 1,658 mg/kg [53]. According to the Scientific Committee on Consumer Safety (SCCS), zinc pyrithione is classified as a moderately toxic agent, with LD50 values ranging from 92 to 266 mg/kg and from 160 to 1,000 mg/kg when administered orally to rats and mice, respectively [54]. Although zinc pyrithione is used as an active ingredient in hygiene and medical products, including anti-dandruff cosmetic and shampoo products [55], its application as an oral therapeutic agent seems to be limited. Nevertheless, based on the FICI values achieved in this study, the active concentrations of both sanguinarine and zinc pyrithione were greatly reduced. Therefore, when used in combination with tetracycline, lower toxicological responses in target organisms could be elicited. Further toxicological studies are needed to assess the therapeutic safety and efficacy of tetracycline in combination with the tested alkaloid-related agents before their potential pharmacological application.
4. Materials and Methods
4.1. Chemicals
Alkaloid-related agents (nitroxoline, sanguinarine chloride, and zinc pyrithione) and the antibiotic (tetracycline) used in this study were purchased from Sigma-Aldrich (Prague, Czech Republic). Dimethyl sulfoxide (DMSO) (Sigma-Aldrich) was used to prepare the stock solutions of all tested compounds except tetracycline HCL, which was prepared using 96% ethanol (Penta, Czech Republic).
4.2. Bacterial strains and growth media
The standard bacterial strains used were obtained from the American Type Culture Collection (ATCC, Rockville, USA) and the National Collection of Type Cultures (NCTC, London, UK). Six different diarrhea-causing pathogens were tested in this study, which were selected as representatives of Gram-negative bacteria (E. coli 0175:H7-VT (N) NCTC 1290, S. flexneri ATCC 12022, V. parahaemolyticus ATCC 17802, and Y. enterocolitica ATCC 9610) and Gram-positive bacteria (E. faecalis ATCC 29212, and L. monocytogenes ATCC 7644). Mueller-Hinton broth (MHB) (Oxoid, Basingstoke, UK) was used as the growth medium. This was supplemented with 3 % NaCl (Sigma-Aldrich) for the culture of V. parahaemolyticus. All bacterial strains were grown in MHB for 24 h at 37°C prior to testing.
4.3. Chequerboard assay
In this study, a chequerboard microdilution assay was used to assess the MIC values of tetracycline and alkaloid-related agents individually and in combination, simultaneously within the same 96-well plate, following the CLSI guidelines [56] and the Clinical Microbiology Procedures Handbook [57]. For the combinations of tetracycline with each of the alkaloid-related agents, eight two-fold serial dilutions of tetracycline in the horizontal rows of the 96-well microtiter plate were cross-diluted vertically, by eight two-fold serial dilutions of the test agents, using a Freedom EVO 100 automated pipetting platform (Tecan, Mannedorf, Switzerland). The final MHB volume per well was 100 μL. The initial concentration for tetracycline was 16 μg/mL whereas that of the alkaloid-related agents was 512 μg/mL. The inoculum was adjusted to a final bacterial concentration of 1.5 × 108 CFU/mL in the MHB according to the 0.5 McFarland standard scale, using a Densi-La-Meter II (Lachema, Brno, Czech Republic). The microtiter plates were inoculated with the bacteria (5 μL/well) and incubated at 37°C for 24 h. Afterwards, the optical density of the bacterial cultures was determined at a wavelength of 405 nm to assess growth inhibition using a Cytation 3 Imaging Reader (BioTek, Winooski, USA) [58]. The MICs were expressed as the lowest concentration that inhibited bacterial growth by ≥ 80% compared with that of the agent-free growth control [59]. The obtained data is presented as the average values of three independent experiments, each performed in triplicate [60]. According to the widely accepted norm in MIC testing, the triplicate endpoints were always within the maximum of the three-dilution range [61], which provides (in most cases) discrete MIC values with low variability of the results. Eighteen independent 96-well plates were used for the assessment of each combination of antibiotic and alkaloid-related agent (i.e., 54 plates in total); three different plates were used for each of the six different bacterial species tested. Tetracycline (tested in the same row of the microplate used for MIC determination) was also employed as a positive control for the verification of susceptibility of the bacterial strains in the broth medium. A drug-free bacterial culture served as the negative control. There was no change in turbidity (no contamination) in the negative control wells. The highest concentration of DMSO and ethanol (both at 1%) present in the microtiter plates did not inhibit bacterial growth of any strain tested.
4.4. Evaluation of combination effects
The FICI (= ∑FIC), a measure recommended by the European Committee on Antimicrobial Susceptibility Testing, has been used for the assessment of combinatory effect of antibacterial agents [62]. The combined effects of tetracycline (A) and alkaloid-related agents (B) were calculated using the following equation: ∑FIC = FICA+FICB where, FICA = MICA combination B/MICA alone and FICB = MICB combination A /MICB alone [63]. With the aim of avoiding reproducibility errors in MIC chequerboard interpretation, the effects were evaluated according to strict criteria proposed by Odds [64], using average values of the FICIs. The results were interpreted as follows: synergy if ∑FIC ≤ 0.5; no interaction if ∑FIC > 0.5– 4, and antagonism if ∑FIC > 4. For the purpose of describing the synergistic interactions of the antimicrobial agents, the minimum FICI values were used. To aid in the interpretation of results in Table 1, Table 2 and Table 3, graphical representations of the FICI data obtained for the most-sensitive bacteria are illustrated in the form of isobolograms (Figure 1). Following the description, a synergy effect is shown by an upward concave isobole, no interaction is shown by a straight line on the x and y-axis (linear isobole), and an antagonistic effect is represented by a convex isobole [65]. The border of synergy was calculated according to the following equation: 0.5- (MICA combination B/ MICA alone) x MICB alone, which is based on the conservative interpretation of results eliminating reproducibility errors in MIC values determined by the chequerboard methodology [64].
5. Conclusions
In this study, tetracycline in combination with either nitroxoline, sanguinarine, or zinc pyrithione produced antibacterial synergistic interactions against most of the diarrhea-causing bacteria tested. The best result was obtained when tetracycline and nitroxoline were used against S. flexneri, resulting in a FICI value of 0.086. To the best of our knowledge, this is the first report of the synergistic interactions between tetracycline and the above-mentioned alkaloid-related compounds against most of the selected diarrheagenic bacteria strains tested. In addition, based on the FICI values obtained in this study, the synergistic actions suggested that the combination of the antimicrobials was more active against the diarrheal microorganisms than the activity of the single agents alone. Furthermore, because of its ability to potentiate the growth-inhibitory effect of tetracycline against E. faecalis, E. coli, L. monocytogenes, S. flexneri, V. parahaemolyticus, and Y. enterocolitica at a decreased concentration, nitroxoline seems to be an attractive candidate for the development of new synergistically acting anti-diarrheal medications for humans. Nevertheless, further research that focuses on their in vivo anti-diarrheal activity and safety is needed before any consideration for use in human medicine.
Author Contributions
H.O.O.; performed the research, analyzed the data and wrote the original draft of the manuscript under the supervision of L.K.; who conceptualized the research and also reviewed the final version of the paper. J.R.; M.H.; and T.K.; participated in investigation and revision of the manuscript. T.N.; final revision of the manuscript.
Data Availability Statement
The original contributions presented in the study are incorporated in the article, and further inquiries can be directed to the corresponding author.
Acknowledgments
This work was financially supported by the Internal Grant Agency of the Faculty of Tropical AgriSciences (IGA 20233109).
Conflicts of Interest
The authors declare that they have no conflict of interest.
References
- GBD 2016 Diarrhoeal Disease Collaborators. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of diarrhoea in 195 countries: a systematic analysis for the global burden of disease study 2016. Lancet Infect Dis 2018, 18, 1211-1228. [CrossRef]
- Kosek, M.; Bern, C.; Guerrant, R.L. The magnitude of the global burden of diarrhea from studies published 1992-2000. Bull World Health Organ 2003, 81, 197–204. [Google Scholar] [PubMed]
- Diarrhoeal disease. Available online: https://www.who.int/news-room/fact-sheets/detail/diarrhoeal-disease. 2017 (accessed on 29 July 2022).
- Cooke, M.L. Causes and management of diarrhoea in children in a clinical setting. South Afr J Clin Nutr 2010, 23, 42–46. [Google Scholar] [CrossRef]
- Quraishi, F.; Shaheen, S.; Memon, Z.; Fatima, G. Culture and sensitivity patterns of various antibiotics used for the treatment of pediatric infectious diarrhea in children under 5 years of age: A tertiary care experience from Karachi. Int J Clin Med 2018, 9, 684–696. [Google Scholar] [CrossRef]
- Jandhyala, S.M.; Talukdar, R.; Subramanyam, C.; Vuyyuru, H.; Sasikala, M.; Nageshwar, R.D. Role of the normal gut microbiota. World J Gastroenterol 2015, 21, 8787–8803. [Google Scholar] [CrossRef]
- Rolhion, N.; Chassaing, B. When pathogenic bacteria meet the intestinal microbiota. Philos Trans R Soc Lond B Biol Sci 2016, 371:20150504. [CrossRef]
- Vogt, S.L; Finlay, B.B. Gut microbiota-mediated protection against diarrheal infections. J Travel Med 2017, 24, S39–S43. [Google Scholar] [CrossRef] [PubMed]
- Cunha, B.A. Nosocomial diarrhea. Crit Care Clin 1998, 14, 329–38. [Google Scholar] [CrossRef]
- World health organization. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/antibiotic-resistance (accessed on 5 August 2022).
- Zhang, Z.; Li, J.; Ma, L.; Yang, X.; Fei, B.; Leung, P.H.M.; Tao, X. Mechanistic study of synergistic antimicrobial effects between poly (3-hydroxybutyrate) oligomer and polyethylene glycol. Polymers 2020, 12, 2735. [Google Scholar] [CrossRef]
- Peña-Miller, R.; Lähnemann, D.; Schulenburg, H.; Ackermann, M.; Beardmore, R. The optimal deployment of synergistic antibiotics: a control-theoretic approach. J R Soc Interface 2012, 9, 2488–2502. [Google Scholar] [CrossRef]
- Doldán-Martelli, V.; Míguez, D.G. Synergistic interaction between selective drugs in cell populations models. PLoS One 2015, 10: e0117558. [CrossRef]
- Windiasti, G.; Feng, J.; Ma, L.; Hu, Y.; Hakeem, M.J.; Amoako, K.; Delaquis, P.; Lu, X. Investigating the synergistic antimicrobial effect of carvacrol and zinc oxide nanoparticles against Campylobacter jejuni. Food Control 2019, 96, 39–46. [Google Scholar] [CrossRef]
- Olajuyigbe, O.O. Synergistic influence of tetracycline on the antibacterial activities of amoxicillin against resistant bacteria. J Pharm Allied Health Sci 2012, 2, 12–20. [Google Scholar] [CrossRef]
- UNASYN- ampicillin sodium and sulbactam sodium injection, powder, for solution Roerig. Updated October 2020. New York, NY 10017. Available online: https://labeling.pfizer.com/showlabeling.aspx?id=617 (accessed on 23 October 2023).
- Khin-Maung, U.; Khin, M.; Nyunt-Nyunt, W.; Kyaw, A., Tin-U. Clinical trial of berberine in acute watery diarrhoea. Br Med J (Clin Res Ed) 1985, 291, 1601-1605. [CrossRef]
- Hamoud, R.; Reichling, J.; Wink, M. Synergistic antibacterial activity of the combination of the alkaloid sanguinarine with EDTA and the antibiotic streptomycin against multidrug resistant bacteria. J Pharm Pharmacol 2015, 67, 264–273. [Google Scholar] [CrossRef] [PubMed]
- Jean, B.; Hatton, C.K. 1999. Pharmacognosy Phytochemistry Medicinal Plants. 2nd ed. Paris Secaucus N.J: Lavoisier Pub.; Intercept.
- Dey, A.; Mukherjee, A.; Chaudhury, M. Alkaloids From Apocynaceae: Origin, pharmacotherapeutic properties, and structure-activity studies, Editor(s): Atta-ur-Rahman. Studies in Natural Products Chemistry 2017, 52, 373–488. [Google Scholar] [CrossRef]
- Awuchi, C. The biochemistry, toxicology, and uses of the pharmacologically active phytochemicals: alkaloids, terpenes, polyphenols, and glycosides. J Food Pharm Sci 2019, 7, 131–150. [Google Scholar] [CrossRef]
- Croaker, A.; King, G.J.; Pyne, J.H.; Anoopkumar-Dukie, S.; Liu, L. Sanguinaria canadensis: Traditional medicine, phytochemical composition, biological activities and current uses. Int J Mol Sci 2016, 17, 1414. [Google Scholar] [CrossRef]
- Tenenbaum, H.; Dahan, M.; Soell, M. Effectiveness of a sanguinarine regimen after scaling and root planing. J Periodontol 1999, 70, 307–311. [Google Scholar] [CrossRef]
- Kuete, V. Health Effects of Alkaloids from African Medicinal Plants. Toxicol survey of Afri med plants 2014, 611–634. [Google Scholar] [CrossRef]
- Osei-Owusu, H.; Kudera, T.; Strakova, M.; Rondevaldova, J.; Skrivanova, E.; Novy, P.; Kokoska, L. In vitro selective combinatory effect of ciprofloxacin with nitroxoline, sanguinarine, and zinc pyrithione against diarrhea-causing and gut beneficial bacteria. Microbiol Spectr 2022, e0106322. [Google Scholar] [CrossRef]
- Kresken, M.; Körber-Irrgang, B. In vitro activity of nitroxoline against Escherichia coli urine isolates from outpatient departments in Germany. Antimicrob Agents Chemother 2014, 58, 7019–7020. [Google Scholar] [CrossRef]
- Vivanco, J.M; Bais, H.P.; Stermitz, F.R.; Thelen, G.C.; Callaway, R.M. Biogeographical variation in community response to root allelochemistry: novel weapons and exotic invasion. Ecol Lett 2004, 7, 285–292. [Google Scholar] [CrossRef]
- Han, G.; Bingxiang, X.; Xiaopeng, W. Studies on active principles of Polyalthia nemoralis-I. The isolation and identification of natural zinc compound. Acta Chim Sin 1981, 39, 433–437. [Google Scholar]
- Saunders, C.W.; Scheynius, A.; Heitman, J. Malassezia fungi are specialized to live on skin and associated with dandruff, eczema, and other skin diseases. PLoS Pathog 2012, 8, 100270. [Google Scholar] [CrossRef] [PubMed]
- Leong, C.; Wang, J.; Toi, M.J.; Lam, Y.I.; Goh. J.P.; Lee, S.M.; Dawson, T.L. Effect of zinc pyrithione shampoo treatment on skin commensal Malassezia. Med Mycol 2021, 59, 210-213. [CrossRef]
- Britannica, The Editors of Encyclopaedia. "tetracycline". Encyclopedia Britannica. Available online: https://www.britannica.com/science/tetracycline 2012 (accessed on 7 April 2022).
- Dwivedi, G.R.; Maurya, A.; Yadav, D.K; Singh, V.; Khan, F.; Gupta, M.K.; Singh, M.; Darokar, M.P.; Srivastava, S.K. Synergy of clavine alkaloid 'chanoclavine' with tetracycline against multi-drug-resistant E. coli. J Biomol Struct Dyn 2019, 37, 1307–1325. [Google Scholar] [CrossRef] [PubMed]
- Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing; Approved standard 30th ed.; Clinical and Laboratory Standards Institute 2020: Wayne, P. A. USA.
- Sirichoat, A.; Flórez, A.B; Vázquez, L.; Buppasiri, P.; Panya, M.; Lulitanond, V.; Mayo, B. Antibiotic resistance-susceptibility profiles of Enterococcus faecalis and Streptococcus spp. from the human vagina, and genome analysis of the genetic basis of intrinsic and acquired resistances. Front Microbiol 2020, 11:1438. [CrossRef]
- Pohl, A.; Lübke-Becker, A.; Heuwieser, W. Minimum inhibitory concentrations of frequently used antibiotics against Escherichia coli and Trueperella pyogenes isolated from uteri of postpartum dairy cows. J Dairy Sci 2018, 101, 1355–1364. [Google Scholar] [CrossRef] [PubMed]
- Han, F.; Walker, R.D.; Janes, M.E.; Prinyawiwatkul, W.; Ge, B. Antimicrobial susceptibilities of Vibrio parahaemolyticus and Vibrio vulnificus isolates from Louisiana Gulf and retail raw oysters. Appl Environ Microbiol 2007, 73, 7096–7098. [Google Scholar] [CrossRef] [PubMed]
- Stock, I.; Wiedemann, B. An in-vitro study of the antimicrobial susceptibilities of Yersinia enterocolitica and the definition of a database. J Antimicrob Chemother 1999, 43, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Sherwood, J.S.; Logue, C.M. Antimicrobial resistance of Listeria spp. recovered from processed bison. Lett Appl Microbiol 2007, 44, 86–91. [Google Scholar] [CrossRef]
- Madiyarov, R.S.; Bektemirov, A.M.; Ibadova, G.A.; Abdukhalilova, G.K.; Khodiev, A.V.; Bodhidatta, L.; Sethabutr, O.; Mason, C.J. Antimicrobial resistance patterns and prevalence of class 1 and 2 integrons in Shigella flexneri and Shigella sonnei isolated in Uzbekistan. Gut Pathog 2010, 2:18. [CrossRef]
- Kudera, T.; Doskocil, I.; Salmonova, H.; Petrtyl, M.; Skrivanova, E.; Kokoska, L. In vitro selective growth-inhibitory activities of phytochemicals, synthetic phytochemical analogs, and antibiotics against diarrheagenic/probiotic bacteria and cancer/normal intestinal cells. Pharmaceuticals 2020, 13:233. [CrossRef]
- Omoya, F.O.; Ajayi, K.O. Synergistic effect of combined antibiotics against some selected multidrug resistant human pathogenic bacteria isolated from poultry droppings in Akure, Nigeria. Adv Microbiol 2016, 6, 1075–1090. [Google Scholar] [CrossRef]
- Chopra, I.; Roberts, M. Tetracycline antibiotics: mode of action, applications, molecular biology, and epidemiology of bacterial resistance. Microbiol Mol Biol Rev 2001, 65, 232–260. [Google Scholar] [CrossRef]
- Grossman, T.H. Tetracycline antibiotics and resistance. Cold Spring Harb Perspect Med 2016, 6 :025387. [CrossRef]
- White, J.P.; Cantor, C.R. Role of magnesium in the binding of tetracycline to Escherichia coli ribosomes. J Mol Biol 1971, 58, 397–400. [Google Scholar] [CrossRef]
- Repac, A.D.; Parčina, M.; Gobin, I.; Petković, D.M. Chelation in antibacterial drugs: From nitroxoline to cefiderocol and beyond. Antibiotics 2022, 11:1105. [CrossRef]
- Wang, T.; Flint, S.; Palmer, J. Magnesium and calcium ions: roles in bacterial cell attachment and biofilm structure maturation. Biofouling 2019, 35, :959-974. [CrossRef]
- Dinning AJ, Al-Adham IS, Austin P, Charlton M, Collier PJ. Pyrithione biocide interactions with bacterial phospholipid, head groups. J Appl Microbiol 1998, 85:132–140. [CrossRef]
- Obiang-Obounou, B.W.; Kang, O.H.; Choi, J.G.; Keum. J.H.; Kim, S.B.; Mun, S.H.; Shin, D.W.; Kim, K.W.; Park, C.B.; Kim, Y.G.; Han, S.H.; Kwon, D.Y. The mechanism of action of sanguinarine against methicillin-resistant Staphylococcus aureus. J Toxicol Sci 2011, 36, 277–283. [CrossRef]
- Shutter, M.C.; Akhondi, H. Tetracycline. [Updated 2022 Jul 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls publishing; 2022 Jan-. Available online: https://www.ncbi.nlm.nih.gov/books/NBK549905/.
- Poiger, H.; Schlatter, C. Interaction of cations and chelators with the intestinal absorption of tetracycline. Naunyn Schmiedebergs Arch Pharmacol 1979, 306, 89–92. [Google Scholar] [CrossRef]
- Rosenstock, J.; Smith, L.P.; Gurney, M.; Lee, K.; Weinberg, W.G.; Longfield, J.N.; Tauber, W.B.; Karney, W.W. Comparison of single-dose tetracycline hydrochloride to conventional therapy of urinary tract infections. Antimicrob Agents Chemother 1985, 27, 652–654. [Google Scholar] [CrossRef] [PubMed]
- Naber, K.G.; Niggemann, H.; Stein, G. Review of the literature and individual patients' data meta-analysis on efficacy and tolerance of nitroxoline in the treatment of uncomplicated urinary tract infections. BMC Infect Dis 2014, 14:628. [CrossRef]
- Becci, P.J.; Schwartz, H.; Barnes, H.H.; Southard, G.L. Short-term toxicity studies of sanguinarine and of two alkaloid extracts of Sanguinaria canadensis L. J Toxicol Environ Health 1987, 20, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Scientific Committee on Consumer Safety (SCCS). Opinion on zinc pyrithione (ZPT) (P81) CAS N° 13463–41-7 submission III, Regulation 1223/2009, CAS 13463–41–7, preliminary version of 13 December 2019, final version of 03–04 March 2020, SCCS/1614/19. European Commission. Brussels. 13 December.
- Schwartz, J.R.; Shah, R.; Krigbaum, H.; Sacha, J.; Vogt, A.; Blume-Peytavi, U. New insights on dandruff/seborrhoeic dermatitis: the role of the scalp follicular infundibulum in effective treatment strategies. Br J Dermatol 2011, 165 Suppl 2, 18–23. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute. Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically; Approved standard 10th ed.; Clinical and Laboratory Standards Institute. 2015. Wayne, P.A. USA.
- Leber, A. synergism testing: Broth microdilution checkerboard and broth microdilution methods. In Clinical Microbiology Procedures Handbook, 4th ed.; ASM Press: Washington, DC, USA, 2016; Volume 1. [Google Scholar]
- Cos, P.; Vlietinck, A.J.; Vanden Berghe, D.; Maes, L. Anti-infective potential of natural products: How to develop a stronger in vitro 'proof-of-concept'. J Ethnopharmacol 2006, 106, 290–302. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, J.H.; Turnidge, J.D.; Washington, J.A. Antibacterial susceptibility tests: dilution and disk diffusion methods, p 1526–1543. In Murray P.R.; Baron, E.J.; Pfaller, M.A.; Tenover, F.C.; Yolken, R.H (ed), Manual of clinical microbiology, 7th ed. ASM Press, 1999. Washington, DC.
- Okoliegbe, I.N.; Hijazi, K.; Cooper, K.; Ironside, C.; Gould, I.M. Antimicrobial synergy testing: Comparing the tobramycin and ceftazidime gradient diffusion methodology used in assessing synergy in cystic fibrosis-derived multidrug-resistant Pseudomonas aeruginosa. Antibiotics 2021, 10:967. [CrossRef]
- Frankova, A.; Vistejnova, L.; Merinas-Amo, T.; Leheckova, Z.; Doskocil, I.; Wong Soon, J.; Kudera, T.; Laupua, F.; Alonso-Moraga, A.; Kokoska, L. In vitro antibacterial activity of extracts from Samoan medicinal plants and their effect on proliferation and migration of human fibroblasts. J Ethnopharmacol 2021, 264:113220. [CrossRef]
- European Committee for Antimicrobial Susceptibility Testing (EUCAST) of the European Society of Clinical Microbiology and Infectious Diseases (ESCMID). EUCAST Definitive Document E. Def 1.2. Terminology relating to methods for the determination of susceptibility of bacteria to antimicrobial agents. Clin Microbiol Infect 2000, 6, 503-508.
- Rakholiya, K.D.; Kaneria, M.J.; Chanda, S.V. Medicinal plants as alternative sources of therapeutics against multidrug-resistant pathogenic microorganisms based on their antimicrobial potential and synergistic properties. Editor(s): Rai, M.K.; Kon, K.V. Fighting multidrug resistance with herbal extracts, essential oils and their components. Academic Press, 2013, 165-179.
- Odds, F.C. Synergy, antagonism, and what the chequerboard puts between them. J Antimicrob Chemother 2003, 52:1. [CrossRef]
- Williamson, E.M. Synergy and other interactions in phytomedicines. Phytomedicine 2001, 8, 401–409. [Google Scholar] [CrossRef]
Figure 1.
Isobolograms of the synergistic interactions for combination of tetracycline (TET) with: nitroxoline (NTX) against Escherichia coli (A), Listeria monocytogenes (B), Shigella flexneri (C) and Yersinia enterocolitica (D); sanguinarine (SNG) against Enterococcus faecalis (E) and L. monocytogenes (F); and for combination of TET with zinc pyrithione (ZPT) against E. coli (G), S. flexneri (H), Vibrio parahaemolyticus (I) and Y. enterocolitica (J). E. coli (▲), E. faecalis (■), L. monocytogenes (♦), S. flexneri (●), V. parahaemolyticus (+) and Y. enterocolitica (x); border for synergy (---) calculated for ∑FIC ≤ 0.5.
Figure 1.
Isobolograms of the synergistic interactions for combination of tetracycline (TET) with: nitroxoline (NTX) against Escherichia coli (A), Listeria monocytogenes (B), Shigella flexneri (C) and Yersinia enterocolitica (D); sanguinarine (SNG) against Enterococcus faecalis (E) and L. monocytogenes (F); and for combination of TET with zinc pyrithione (ZPT) against E. coli (G), S. flexneri (H), Vibrio parahaemolyticus (I) and Y. enterocolitica (J). E. coli (▲), E. faecalis (■), L. monocytogenes (♦), S. flexneri (●), V. parahaemolyticus (+) and Y. enterocolitica (x); border for synergy (---) calculated for ∑FIC ≤ 0.5.
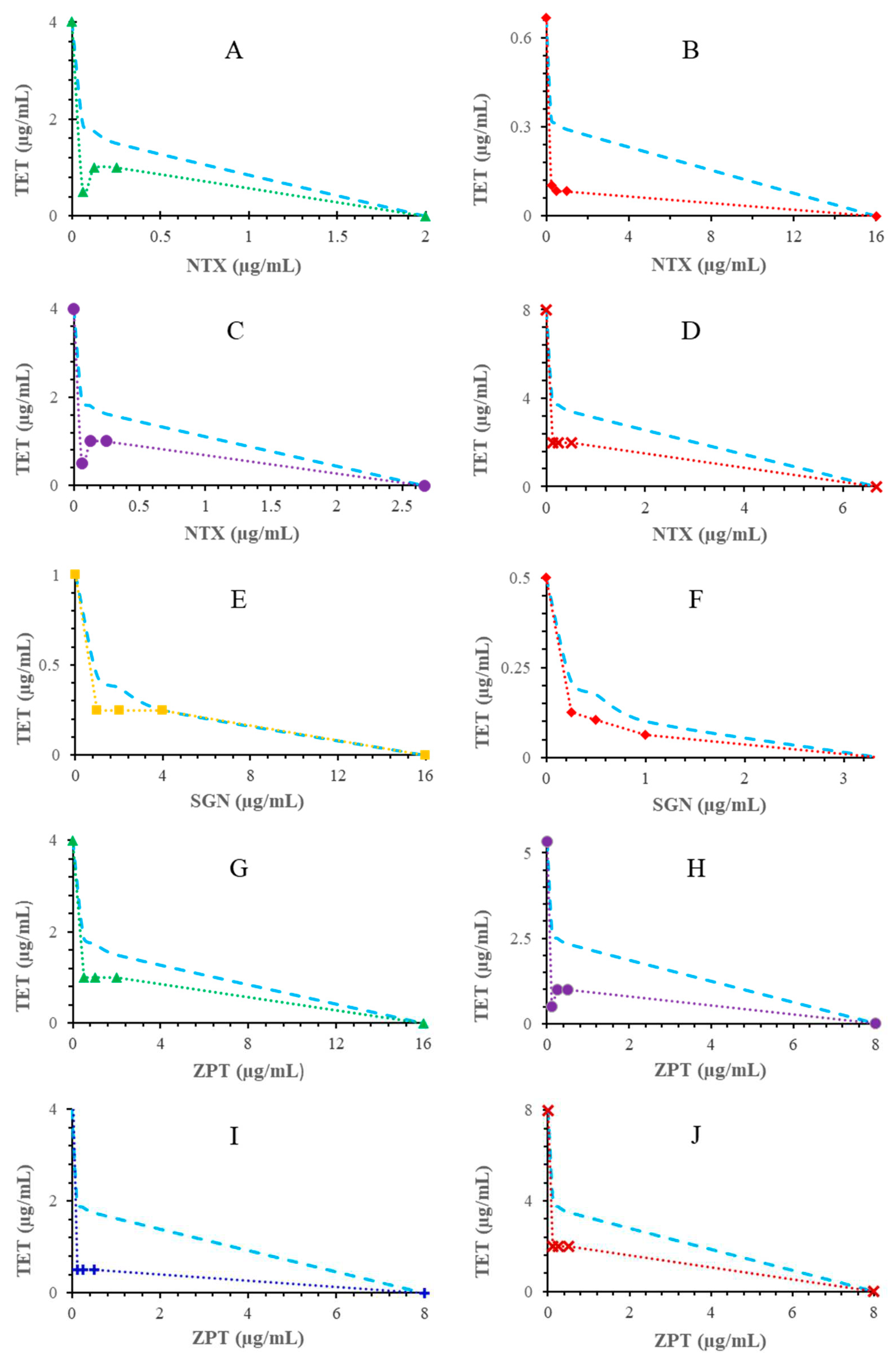

Table 1.
In vitro susceptibility of diarrheagenic bacteria to tetracycline (TET) and nitroxoline (NTX) alone and in combination.
Table 1.
In vitro susceptibility of diarrheagenic bacteria to tetracycline (TET) and nitroxoline (NTX) alone and in combination.
| Bacteriuma | MICb alone | MIC of NTX (numbers in bold)/MIC of TET/FICIc of corresponding NTX-TET combination | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TET | NTX | 32 | 16 | 8 | 4 | 2 | 1 | 0.5 | 0.25 | |||||||||
| E. faecalis | 1 | 16 | 0.031 | 2.031 | 0.031 | 1.031 | 0.031 | 0.531 | 0.25 | 0.5 | 0.25 | 0.375 | 0.25 | 0.313 | 1 | 1.031 | 1 | 1.016 |
| L. monocytogenes | 0.667 | 16 | 0.016 | 2.024 | 0.016 | 1.024 | 0.052 | 0.578 | 0.109 | 0.413 | 0.083 | 0.249 | 0.083 | 0.187 | 0.083 | 0.156 | 0.104 | 0.172 |
| 8 | 4 | 2 | 1 | 0.5 | 0.25 | 0.125 | 0.063 | |||||||||||
| E. coli 0175:H7 | 4 | 2 | 0.063 | 4.016 | 0.063 | 2.016 | 0.063 | 1.016 | 1 | 0.75 | 4 | 1.25 | 1 | 0.375 | 1 | 0.313 | 0.5 | 0.157 |
| S. flexneri | 4 | 2.667 | 0.063 | 3.015 | 0.063 | 1.516 | 0.063 | 0.766 | 2.333 | 0.958 | 3 | 0.937 | 1 | 0.344 | 1 | 0.297 | 0.25 | 0.086 |
| V. parahaemolyticus | 2 | 2 | 0.016 | 4.008 | 0.016 | 2.008 | 0.016 | 1.008 | 0.016 | 0.508 | 0.5 | 0.50 | 0.5 | 0.375 | 0.5 | 0.313 | 0.5 | 0.282 |
| 4 | 2 | 1 | 0.5 | 0.25 | 0.125 | 0.063 | 0.031 | |||||||||||
| Y. enterocolitica | 8 | 6.667 | 0.031 | 0.604 | 1 | 0.425 | 2 | 0.400 | 2 | 0.325 | 2 | 0.287 | 2 | 0.269 | 2 | 0.259 | 2 | 0.255 |
a: Enterococcus faecalis; Escherichia coli 0175:H7; Listeria monocytogenes; Shigella flexneri; Vibrio parahaemolyticus; Yersinia enterocolitica. b MIC, minimum inhibitory concentration of TET and NTX expressed as an average of three independent experiments, each performed in triplicate. All MICs units are in µg/mL. c FICI, fractional inhibitory concentration index; FICI values (≤ 0.5) indicate synergistic effects; FICI values (> 0.5 – 4) indicate no interaction effect; FICI values (> 4) indicate antagonistic effect.
Table 2.
In vitro susceptibility of diarrheagenic bacteria to tetracycline (TET) and zinc pyrithione (ZPT) alone and in combination.
Table 2.
In vitro susceptibility of diarrheagenic bacteria to tetracycline (TET) and zinc pyrithione (ZPT) alone and in combination.
| Bacteriuma | MICb alone | MIC of ZPT (numbers in bold)/MIC of TET/FICIc of corresponding ZPT-TET combination | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TET | ZPT | 16 | 8 | 4 | 2 | 1 | 0.5 | 0.25 | 0.125 | |||||||||
| S. flexneri | 5.333 | 8 | 0.063 | 2.012 | 0.063 | 1.012 | 1 | 0.688 | 1 | 0.438 | 1 | 0.313 | 1 | 0.250 | 1 | 0.219 | 0.5 | 0.109 |
| V. parahaemolyticus | 4 | 8 | 0.016 | 2.004 | 0.016 | 1.004 | 0.016 | 0.504 | 0.031 | 0.258 | 0.031 | 0.133 | 0.5 | 0.188 | 0.5 | 0.156 | 0.5 | 0.141 |
| 8 | 4 | 2 | 1 | 0.5 | 0.25 | 0.125 | 0.063 | |||||||||||
| E. coli 0175:H7 | 4 | 16 | 0.063 | 0.516 | 0.25 | 0.313 | 1 | 0.375 | 1 | 0.313 | 1 | 0.281 | 2 | 0.516 | 2 | 0.508 | 1 | 0.254 |
| E. faecalis | 1 | 8 | 0.031 | 1.031 | 0.031 | 0.531 | 0.5 | 0.75 | 1 | 1.125 | 1 | 1.063 | 1 | 1.031 | 1 | 1.016 | 1 | 1.008 |
| Y. enterocolitica | 8 | 8 | 0.031 | 1.004 | 0.25 | 0.531 | 1 | 0.375 | 1 | 0.25 | 2 | 0.313 | 2 | 0.281 | 2 | 0.266 | 2 | 0.258 |
| 4 | 2 | 1 | 0.5 | 0.25 | 0.125 | 0.063 | 0.031 | |||||||||||
| L. monocytogenes | 0.5 | 8 | 0.016 | 0.532 | 0.016 | 0.282 | 0.125 | 0.375 | 0.208 | 0.479 | 0.208 | 0.447 | 0.125 | 0.266 | 0.125 | 0.258 | 0.125 | 0.254 |
a: Enterococcus faecalis; Escherichia coli 0175:H7; Listeria monocytogenes; Shigella flexneri; Vibrio parahaemolyticus; Yersinia enterocolitica. b MIC, minimum inhibitory concentration of TET and ZPT expressed as an average of three independent experiments, each performed in triplicate. All MICs units are in µg/mL. c FICI, fractional inhibitory concentration index; FICI values (≤ 0.5) indicate synergistic effects; FICI values (> 0.5 – 4) indicate no interaction effect; FICI values (> 4) indicate antagonistic effect.
Table 3.
In vitro susceptibility of diarrheagenic bacteria to tetracycline (TET) and sanguinarine (SGN) alone and in combination.
Table 3.
In vitro susceptibility of diarrheagenic bacteria to tetracycline (TET) and sanguinarine (SGN) alone and in combination.
| Bacteriuma | MICb alone | MIC of SGN (numbers in bold)/MIC of TET/FICIc of corresponding SGN-TET combination | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TET | SGN | 64 | 32 | 16 | 8 | 4 | 2 | 1 | 0.5 | |||||||||
| E. coli 0175:H7 | 4 | 128 | 0.25 | 0.563 | 4 | 1.25 | 4 | 1.125 | 4 | 1.063 | 4 | 1.031 | 4 | 1.016 | 2 | 0.508 | 2 | 0.504 |
| 32 | 16 | 8 | 4 | 2 | 1 | 0.5 | 0.25 | |||||||||||
| E. faecalis | 1 | 16 | 0.031 | 2.031 | 0.031 | 1.031 | 0.031 | 0.531 | 0.25 | 0.5 | 0.25 | 0.375 | 0.25 | 0.313 | 1 | 1.031 | 1 | 1.016 |
| Y. enterocolitica | 2 | 64 | 0.031 | 0.516 | 2 | 1.25 | 2 | 1.125 | 2 | 1.063 | 2 | 1.031 | 2 | 1.016 | 2 | 1.008 | 2 | 1.004 |
| 16 | 8 | 4 | 2 | 1 | 0.5 | 0.25 | 0.125 | |||||||||||
| L. monocytogenes | 0.5 | 3.333 | 0.016 | 4.832 | 0.016 | 2.432 | 0.016 | 1.232 | 0.031 | 0.662 | 0.063 | 0.426 | 0.104 | 0.358 | 0.125 | 0.325 | 0.125 | 0.288 |
| 8 | 4 | 2 | 1 | 0.5 | 0.25 | 0.125 | 0.063 | |||||||||||
| S. flexneri | 1 | 16 | 1 | 1.5 | 1 | 1.25 | 1 | 1.125 | 1 | 1.063 | 0.5 | 0.531 | 0.5 | 0.516 | 1 | 1.008 | 1 | 1.004 |
| V. parahaemolyticus | 1 | 16 | 0.25 | 0.75 | 0.5 | 0.75 | 0.5 | 0.625 | 0.5 | 0.563 | 1 | 1.031 | 1 | 1.016 | 1 | 1.008 | 1 | 1.004 |
a: Enterococcus faecalis; Escherichia coli 0175:H7; Listeria monocytogenes; Shigella flexneri; Vibrio parahaemolyticus; Yersinia enterocolitica. b MIC, minimum inhibitory concentration of TET and SGN expressed as an average of three independent experiments, each performed in triplicate. All MICs units are in µg/mL. c FICI, fractional inhibitory concentration index; FICI values (≤ 0.5) indicate synergistic effects; FICI values (> 0.5 – 4) indicate no interaction effect; FICI values (> 4) indicate antagonistic effect.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



