
Submitted:
18 April 2024
Posted:
18 April 2024
You are already at the latest version
Abstract
The demographic profile of patients transitioning from chronic kidney disease to renal replacement therapy is changing, with a higher prevalence of aging patients with multiple comorbidities such as diabetes mellitus and heart failure. Cardiovascular disease remains the leading cause of mortality in this population, exacerbated by the cardiovascular stress imposed by the HD procedure. The first year after transitioning to hemodialysis is associated with increased risks of hospitalization and mortality, particularly within the first 90–120 days, with greater vulnerability observed among the elderly. This review, based on data from clinics of Fresenius Medical Care Europe, Middle East, and Africa NephroCare, aims to optimize hemodialysis procedures to reduce mortality risk in stable incident and prevalent patients. It addresses critical aspects such as treatment duration, frequency, choice of dialysis membrane, dialysate composition, blood and dialysate flow rates, electrolyte composition, temperature control, target weight management, dialysis adequacy, and additional protocols, with a focus on mitigating prevalent intradialytic complications, particularly intradialytic hypotension prevention.
Keywords:
Hemodialysis procedures
; hemodynamic stability
; dialysis dose
; dialysis electrolytes balance
; dialysis fluid balance
1. Introduction
The demographic profile of patients with chronic kidney disease (CKD) transitioning to end-stage kidney disease (ESKD) and renal replacement therapy is evolving. The prevalence of aging patients with multiple comorbidities, such as diabetes mellitus and heart failure [1], undergoing hemodialysis (HD) is markedly higher than in the general population. It poses an increased challenge for healthcare providers [2,3]. Cardiovascular dis-ease (CVD) stands as the foremost cause of mortality, significantly surpassing other cause-es [4,5,6]. This elevated mortality rate primarily stems from the substantial burden of underlying cardiovascular conditions [7]. Moreover, the cardiovascular stress imposed by the HD procedure further compounds this risk, exacerbating the already precarious health status of affected individuals [6,8]. The first year after transitioning from CKD to requiring HD has been associated with an increased risk of hospitalization and mortality, particularly during the first 90–120 days of HD initiation [9,10]. This vulnerability is particularly pronounced among the elderly population [11], even under usual circumstances. In addition, the early phase of HD is characterized by recurrent intradialytic complications. The COVID-19 pandemic created unprecedented challenges, particularly for susceptible populations such as patients with CKD. Dashtban et al. found that the mortality rate among CKD patients who initiated HD treatment during the COVID-19 pandemic was higher than the mortality rate among CKD patients who initiated HD treatment in the pre-pandemic period [12]. The lack of regular nephrology visits during the COVID-19 pandemic due to restrictions on in-person healthcare services or patients' reluctance to seek medical care may result in inadequate management of comorbidities and complications associated with ESKD, thereby increasing mortality risk. Within the clinics of Fresenius Medical Care (FMC) Europe, Middle East, and Africa (EMEA) NephroCare, a rise in mortality rates has been noted among CKD patients who initiated HD treatment during the COVID-19 pandemic (Figure 1). Considering the evolving demographics of CKD patients transitioning to ESKD and HD, this review aims to optimize HD procedures to mitigate mortality risk in stable incident and prevalent patients. The first section will delve into critical aspects such as intradialytic hypotension. The second will focus on treatment duration, frequency, choice of dialysis membrane, dialysate composition, and blood and dialysate flow rates. The subsequent segment will focus on dialysate electrolyte composition, temperature control, target weight management, dialysis adequacy, and additional protocols, primarily focusing on mitigating the prevalent intradialytic complications with specific attention to intradialytic hypotension prevention. The final segment focuses on intra- and extra-dialytic procedures, evaluating the impact of eating during dialysis, antihypertensive drugs, blood pressure monitoring, and the execution of blood tests.
2. Intradialytic Hypotension
The multifaceted nature of intradialytic hypotension (IDH) is underscored by the amplified incidence rates observed in a demographic characterized by advancing age and concomitant diseases, such as diabetes mellitus and heart failure [13]. While specific IDH episodes can be ameliorated within clinical settings, others extend beyond the patient's discharge and persist upon their return home.
Considering the potential risk low blood pressure imparts, IDH can no longer be treated as a benign condition. Chronic manifestations of IDH have been correlated with a spectrum of adverse outcomes, encompassing symptomatic discomfort, suboptimal dialysis, vascular access thrombosis, exacerbated renal function degradation, cardiovascular perturbations, and elevated mortality risks, predominantly attributed to recurrent organ compromise [4,14,15,16,17,18].
The optimal medical definition for IDH would identify a BP threshold below which individuals sustain end-organ pathologic insults with symptoms such as cramps, nausea, vomiting, and dizziness linked to adverse clinical outcomes [19]. However, despite its clinical significance, there is no consensus, evidence-based medical definition for the IDH condition [19]. Numerous IDH definitions, likely of varying validity, have been used over time 1) K/DOQI Clinical Practice Guidelines, 2005: A decrease in systolic BP ≥ 20 mm Hg or a decrease in MAP ≥ 10 mm Hg associated with symptoms that include abdominal discomfort, yawning, sighing, nausea, vomiting, muscle cramps, restlessness, dizziness or fainting; and anxiety [20]. 2) European Best Practice Guidelines (2007): A decrease in systolic BP ≥ 20 mm Hg or a decrease in MAP ≥ 10 mm Hg is associated with clinical events and the need for nursing interventions [21]. 3) UK Renal Association Guidelines (2009): An acute symptomatic fall in BP during dialysis requiring immediate intervention to prevent syncope [22]. 4) Japanese Society for Dialysis Therapy Guidelines (2012): Symptomatic sudden drop systolic BP ≥ 30 mm Hg during dialysis or a decrease in the mean BP by ≥ 10 mm Hg [23]. In FMC EMEA NephroCare, symptomatic IDH is defined as the fall of ≥ 20 mmHg in SBP from pre-dialysis to nadir intra-dialytic levels plus ≥ 2 responsive measures (stop treatment, move patient to Trendelenburg position, IV infusion of liquids, reduction or stop UF, reduction of the blood flow, etc.).
Depending on the definitions utilized, symptomatic IDH either during or immediately post hemodialysis has been reported in 0.5% to 40% of all HD sessions [24,25,26] affecting 20-50% of HD patients [27]. More recent investigations indicate a prevalence of approximately 11% [1]. This variation can be attributed, in part, to the diverse definitions of IDH that have been adopted over time. These definitions span a wide range, from symptomatic hypotension necessitating intervention to symptomatic or asymptomatic reductions in systolic blood pressure.
During dialysis, the fluid is removed from the intravascular compartment. The rate of removal (ultrafiltration rate) may exceed that of refilling from the extracellular and intracellular compartments, reducing circulating blood volume. This can be magnified by the cardiopulmonary redistribution of blood flow that occurs when patients are dialyzed and dilatation of the capacitance vessels (dialysis thermal stress, leading to an increase in “unstressed blood volume” and subsequent reduction in venous return [28]. In contrast to healthy persons, in whom a decline in plasma volume up to 15% (and in some cases up to 25%) is not associated with significant clinical features, IDH can occur at a much lower decline in blood volume [29]. This indicates that the normal compensatory response to hypovolemia can be disturbed in ESKD patients. IDH is exacerbated by a myriad of factors, including inter-dialytic fluid gains, cardiovascular diseases, antihypertensive medications, and the physiological demands placed on patients by hemodialysis. Hypotension can occur when one or more compensatory responses are incomplete. A) Reduced plasma refilling: Rapid reduction of plasma osmolality (e.g. urea concentration) in the first phase of dialysis treatment, consequent to urea removal, may result in movement of extracellular water into the cells [29]; B) Reduced sympathetic nervous system activation with failure of the acute hemodynamic compensatory response to hypovolemia; C) Reduced venoconstriction [30,31]; D) Reduced increase of peripheral arteriolar resistance [30,31]; E) Reduced cardiac compensation due to reduced cardiac filling (preload), reduced myocardial contractility, reduced heart rate, and reduced cardiac output (stroke volume) [32].
3. Hemodialysis Procedures in Stable Incident and Prevalent Patients
FMC EMEA NephroCare has created a set of HD strategies and procedures aimed at enhancing the management and seamless transition of stable incident patients with ESKD. This approach is designed to ensure a meticulous equilibrium in fluid, electrolyte, and acid-base balance while concurrently maintaining hemodynamic stability during the HD procedure. Reducing HD-induced circulatory stress may necessitate combining various strategies customized to suit the unique characteristics of each patient's inability to manage HD effectively [6]. Educating dialysis personnel to identify patients prone to IDH is relevant, facilitating the prompt recognition and prevention of such occurrences. Additionally, the recommendations advocate for an incremental approach to HD, underscoring the significant influence of residual renal function on determining dosing schedules for intermittent HD. Starting HD treatment in stable incident patients may be challenging, as these patients are more likely to have multiple comorbidities and other complications that can make dialysis treatment difficult. The initial phase involves evaluating the patient's overall health condition and recognizing any possible risks or obstacles. This could entail conducting a comprehensive anamnesis review, performing a physical examination, and performing laboratory tests. It is crucial to closely observe the patient throughout and following dialysis sessions for any indications of complications. Physicians prescribing dialysis treatment in more complex and unstable incident patients, like those crashing in dialysis, should tailor the renal replacement therapy according to the specific individual needs. This may involve choosing the type of dialysis (intermittent HD, continuous renal replacement therapy, or peritoneal dialysis), the treatment frequency, and the dialysis machines' settings. Below are suggested HD and dialysate prescriptions, ancillary laboratory tests, fluid status management, and intra and extra-dialysis procedures that should be considered in stable incident and prevalent ESKD patients to improve their hard clinical outcomes.
3.1. Treatment Time and Frequency
According to the European Best Practice Guideline (EBPG) on dialysis strategies [33] and the UK Renal Association Clinical Practice Guideline on Hemodialysis [34], prevalent patients should receive HD treatment at least three times per week, with a total duration of least 12 hours per week, unless significant renal function is present. Consideration should be given to increasing treatment time and/or frequency for patients experiencing frequent intradialytic hypotensive episodes (IDH), muscle cramps, headaches, and dizziness, as well as those who remain hypertensive despite maximum fluid removal and those with impaired phosphate control [33]. Increasing dialysis frequency has been shown to improve patient outcomes, with favorable effects on blood pressure control, nutritional status, hospitalization rates, and quality of life. [33]. Residual renal function should be periodically quantified in patients following an incremental dialysis schedule [34]. The National Kidney Foundation's Kidney Disease Outcomes Quality Initiative (KDOQI) recommends that patients with low residual kidney function (< 2ml/min) undergoing thrice weekly HD be prescribed a bare minimum of three hours per session [35]. Longer and/or additional HD treatments should be considered for patients with large interdialytic weight gains, high UFR, who remain hypertensive, difficulty achieving dry weight, and with hyperphosphatemia, metabolic acidosis, and or hyperkalemia [35]. A stepwise increase in treatment time and frequency should be considered according to residual renal function for stable incident patients not crushing on dialysis. These considerations are compactly presented in Table 1.
3.2. Dialysis Membrane and Surface Area
The EBPG recommends using synthetic high-flux membranes to delay long-term complications of HD treatment like amyloidosis, to improve control of hyperphosphatemia, to reduce the increased cardiovascular risk, and to improve control of anemia [33]. UK Renal Association Clinical Practice Guideline on Hemodialysis recommends treating patients with minimal residual function with high-flux dialyzers [34]. KDOQI recommends the use of biocompatible, either high or low-flux HD membranes for intermittent HD [35]. In FMC EMEA, the dialyzer area surface standard is 1.6 ± 0.2 m2, and variations depend on individual patient needs and residual kidney function. It is suggested that, when initiating HD therapy in new patients, consideration should be given to selecting high-flux biocompatibility dialyzers with smaller surface areas. (Table1).
3.3. Blood Flow Rate
The blood flow rate (Qb) varies across regions and facilities. For instance, HD patients in the USA typically achieve a mean Qb greater than 400 mL/min, whereas in Japan, Qb is usually less than 200 mL/min [36,37]. Limited research exists on the correlation between Qb and hard clinical outcomes in HD patients. Consequently, the optimal Qb remains uncertain [37]. It is suggested to take into consideration a stepwise approach gradually from 150 ml/min in the first week of dialysis by step of 50 ml/min over a week period to reach a Qb ≥ 340 mL/min in the 5th week of dialysis. Gradually increasing the Qb as patients become more accustomed to the HD process is reasonable, but ensuring individual tolerance is crucial (Table 1).
3.4. Dialysate Flow Rate
Like Qb, no single "best" dialysate flow rate (Qd) is suitable for all HD patients. A Qd of 500 mL/min is commonly recommended for effectively conducting HD treatments. Increasing Qd from 500 to 800 mL/min has been suggested to enhance dialysis efficiency and permit shorter treatment durations. Leypoldt et al., through an in vitro study, showed that the improvement was attributed to better flow distribution within the dialysate compartment [38]. Modern dialyzers achieve improved dialysate fluid distribution through features such as hollow fiber undulations, spacer yarns, and changes in fiber packing density, which enhance flow distribution within the dialysate compartment. Albalate et al. investigated the effect of using Qd rates of 400, 500, and 700 mL/min with different modern dialyzers. They found that increasing Qd beyond 400 mL/min with these dialyzers offers limited benefits [39]. When comparing the authors' differing recommendations regarding dialysate flow, a correlation emerges between the achieved simultaneous blood flow and assessing the impact of the dialysate flow [40]. If available, it is advisable to use autoflow methods that adjust the dialysate flow directly according to the blood flow. Compared to fixed dialysate flow, this approach can conserve resources while enhancing effectiveness. Increasing treatment duration represents a preferable alternative, providing demonstrated benefits to patients while reducing water consumption. It is suggested that Qd be gradually increased to 450-500 mL/min, maintaining a flow ratio (autoflow) of Qd/Qb = 1.2 for balanced dialysis performance. If the Kt/V falls below 1.4, consider raising Qd and autoflow beyond 500 and 1.2, respectively, if further increases in blood flow are not feasible and large dialyzer surface areas are utilized. Conversely, if HDF is used and the Kt/V exceeds 2.0, decrease the autoflow to ≤ 1.0 (Table 1).
4. Hemodialysis Procedures Aimed at Optimizing Hemodynamic Stability, Dialysis Dose, Electrolytes, and Fluid Balance
This is the third part of a review on HD procedures for stable incident and prevalent patients aimed at optimizing hemodynamic stability, dialysis dose, electrolytes, and fluid balance. Herein, we will focus on specific aspects of HD to minimize the risk of intradialytic hypotension in patients undergoing this treatment. We will discuss the importance of dialysate electrolytes, temperature regulation, target weight management, dialysis dose optimization, and other crucial procedures that play a key role in ensuring the safety and well-being of hemodialysis patients. By understanding and effectively implementing these strategies, healthcare providers can enhance the overall quality of care for individuals undergoing HD.
4.1. Dialysate Electrolytes
Regular adjustment based on lab tests is critical, particularly for elements like potassium, bicarbonates, calcium, and sodium. Consistent monitoring can prevent dysregulation that can cause complications like arrhythmias or bone disorders. In incident patients, a more frequent electrolyte evaluation is suggested in the first 30 days of HD treatment. A stepwise dialysate electrolyte prescription (Table 2) is suggested, and electrolytes in the dialysate should be regularly adjusted based on lab tests to prevent complications like arrhythmias or bone disorders.
4.1.1. Dialysate Sodium
Is the cornerstone of intra-dialysis cardiovascular stability and reasonable inter-dialysis blood pressure control [41]. Acting on diffusive sodium (Na) mass transfer in terms of a reduced diffusive Na load may lead to a reduction of thirst [42], a reduction of interdialytic weight gain [43], and a modification of short-term outcomes thanks to reduced fluid overload and reduced blood pressure [44]. Sodium loading during HD results in greater thirst, increased volume expansion, increased cardiac workload, and subsequent hypertension [35]. While it is very reasonable to reduce the diffusive Na mass transfer in stable patients, particularly hypertensive patients with high interdialytic weight gain (IDWG), a cautious approach should be adopted in those with frequent IDH. In patients with minimal IDWG, the risk-benefit ratio may favor the use of higher dialysate Na (≥ 140mEq/L) and regularly reassess to avoid prolonged Na loading and its consequences [45]. Low Na concentration in dialysate causes a decrease in plasma osmolarity that may lead to cellular overhydration, intradialytic cardiovascular instability with hypotension due to insufficient refilling of the intravascular compartment from the intracellular space, fatigue, muscle cramps, headache, and orthostatic hypotension [41,46]. High dialysate Na concentration in the dialysate can prevent cardiovascular instability because of increased osmotic refilling of water from interstitial and intracellular to the intravascular compartment, which counteracts the effects of intravascular emptying secondary to ultrafiltration. The drawback is an insufficient net Na removal, with increased thirst, volume expansion, and hypertension [35,46]. Miskulin et al. demonstrated that using a dialysate Na 135 mEq/l, as opposed to 138 mEq/l, resulted in a slight reduction in IDWG without impacting IDH or pre-dialysis blood pressure, albeit with an increase in symptoms [47]. Conversely, raising the dialysate Na to 140 mEq/l decreased episodes of IDH despite a slight increase in IDWG and pre-dialysis blood pressure [47]. It is clear from the literature that there is no ideal dialysate Na. To minimize complications from both high and low dialysate Na, dialysis units typically choose a standard concentration between 138 and 140 mmol/l [48]. This range reflects likely optimization over time, as evidenced by 90% of DOPPS units adopting it for their standard D-Na [49]. The current practice of using a fixed dialysate Na concentration may not be ideal for personalized dialysis treatment. A more precise approach considers the dialysate-plasma Na gradient, which considers the patient's pre-dialysis blood Na level [50]. This allows for a customized prescription based on individual needs [51]. Traditionally, this involved manually adjusting the dialysate Na to match the pre-dialysis plasma Na, requiring frequent monitoring [43,52]. However, new technology offers an automated Na balancing module that simplifies this process. With this tool, healthcare providers can easily tailor the dialysate Na concentration to both the patient's Na level and the desired tonicity, improving treatment efficiency and, potentially, patient outcomes [53,54,55]. If the automated Na balance module is unavailable, a starting dialysate Na concentration of 140-143 mEq/L is suggested for patients initiating HD therapy. This selection prioritizes achieving initial cardiovascular stability during treatment by minimizing hemodynamic fluctuations caused by excessive Na gradients between the dialysate and plasma. The dialysate Na concentration may be progressively reduced to achieve a range of 138-140 mEq/L for prevalent patients (Table 2).
4.1.2. Dialysate Bicarbonates
When interpreting the level, the pre-dialysis serum bicarbonate should be 18.0-26.0 mmol/l, considering possible measurement errors (e.g., air exposure) [34]. Several factors can influence the measured bicarbonate concentration, including sample handling and analysis techniques. One potential error source is exposure to air. When blood comes into contact with air, CO2 can escape, leading to an artificially low bicarbonate measurement. Bicarbonate concentration in dialysate at the range of 30-32 mEq/l may improve heart contractility by increasing ionized calcium [56]. Patients undergoing HD with elevated dialysate bicarbonate experience rapid correction of metabolic acidosis, leading to an alkalotic state, particularly in the second half of treatment or afterward. This condition increases their risk of arrhythmias due to hypokalemia, hypocalcemia, hypomagnesemia, QT prolongation, vasodilation and hypotension, minute ventilation suppression, cerebral ischemia, and accelerated vascular calcification [57,58,59,60,61,62,63,64,65]. Tentori et al. demonstrated in a retrospective analysis of DOPPS data that clinics exposing patients to dialysate bicarbonate concentrations of 33-37 mEq/l experienced increased mortality, regardless of the blood bicarbonate concentration. Moreover, mortality rates were even higher when dialysate bicarbonate levels were 38 mEq/l or higher [66]. Another study found that reducing the dialysate bicarbonate concentration decreased intradialytic hypotension [67]. For patients starting the HD therapy, a gentle correction of the uremic chronic acidosis status is suggested, beginning with a dialysate bicarbonate concentration ≤ 28 mEq/L. This approach prioritizes attaining initial cardiovascular stability during treatment while mitigating potential complications associated with rapid alkalization during HD and online-HDF and subsequent alkalosis. In prevalent patients, the dialysate bicarbonate concentration may gradually increase to 30-32 mEq/l, adjusting it based on pre-post dialysis bicarbonate values and the patient's metabolic status (Table 2).
4.1.3. Dialysate Calcium
The KDOQI goal range for corrected total serum calcium (Ca) should be between 8.4 and 10.2 mg/dL (2,1-2,54 mmol/l) [68]. Correction of acidosis and post-dialysis alkalosis may induce hypocalcemia, mainly if low dialysate Ca concentration is used. Hypocalcemia can induce IDH by pro-arrhythmogenic effects [69,70,71]. In patients undergoing HD, prolongation of QTc is inversely correlated with intradialytic variations in plasma calcium, suggesting that patients with the most significant reduction in calcium had the greatest increases in QTc at the end of the HD session [69,70,71]. The KDIGO 2017 guidelines recommend a dialysate Ca between 1.25-1.5 mmol/l [72,73]. Dialysate Ca 1.25 mmol/l accelerates bone turnover and hemodynamic instability, resulting in a higher incidence of arrhythmia and sudden cardiac arrest [74,75], probably because of increased QT interval [76]. DCa 1.5 mmol/l improves cardiac muscle contractility and hemodynamic stability (8). Dialysate Ca 1.75 mmol/l is associated with increased sympathetic activity, enhancing myocardial contractility, minimizing the decline in intradialytic blood pressure, and improving intradialytic hemodynamic stability [77,78]. Long-term effects contribute to accelerated vascular calcification and bone and mineral imbalance with adynamic bone [72,73,79,80,81]. In patients initiating HD therapy, the risk of IDH due to hypocalcemia’s pro-arrhythmogenic effects must be avoided. It is suggested that HD treatment be considered started in incident patients with a dialysate Ca 1.5-1.75 mmol/l. This approach prioritizes achieving cardiovascular stability during treatment while mitigating potential hypocalcemia associated with rapid alkalization during HD and online-HDF. For prevalent patients, the dialysate Ca may gradually decrease to a range of 1.25-1.5 mmol/l, adjusting it based on pre- and post-dialysis plasma calcium values. Maintaining an optimal calcium balance in ESKD patients is a complex process influenced by several factors, including plasma calcium levels, PTH, the use of phosphate binders and vitamin D analogs, and IDH risk and cardiac arrhythmias. These factors act in concert and require careful consideration for optimal outcomes. Therefore, dialysate Ca prescription should be carefully individualized [81].
4.1.4. Dialysate Potassium
After a long interdialytic period, serum potassium (K) levels should be in the range of≥ 4.0 - ≤ 6,0 mEq/l [34]. Potassium is important in maintaining the resting cell membrane potential, neuromuscular excitability, and cardiac pacemaker rhythmicity [82]. The HD treatment induces a sudden decrease in plasma K concentration during the first 60 minutes. In the last 60 minutes of HD, the plasma K concentration is stabilized, reaching a steady state during the last hour [83,84,85,86]. Lower dialysate K concentration results in greater removal of K from the blood, leading to lower post-dialysis serum K levels [87]. The sudden decrease in plasma K concentration affects the intracellular and extracellular K concentration gradient, transmembrane potential, and repolarization of the cardiac cells. It can predispose to IDH, reducing cardiac output consequent to increased risk of arrhythmia, QT prolongation, and ectopic ventricular beats [88,89]. Hypokalemia during dialysis sessions has been correlated with brief paroxysmal atrial fibrillation episodes, most noted during the last two hours of dialysis [90,91]. Dialysate K < 2 mEq/l has been associated with cardiac events [92,93,94]. Strict control of K intake may decrease the need for a low dialysate K, reducing the risk of intradialytic hypokalemia [95]. In patients initiating HD therapy, the risk of IDH due to hypokalemia’s pro-arrhythmogenic effects must be avoided. It is suggested to take into consideration starting the HD treatment in incident patients with a dialysate K = 3 mEq/l (Table 2): This approach prioritizes the achieving of cardiovascular stability during treatment while mitigating potential hypokalemia associated with rapid alkalization during HD and online-HDF treatments. For prevalent patients, the dialysate K may be gradually decreased to a range of 2-3 mEq/l, adjusting it based on pre- and post-dialysis plasma potassium values. (Table 2).
4.1.5. Dialysate Magnesium
In ESKD patients, the ability to regulate magnesium (Mg) levels is impaired with increased accumulation risk, and studies have shown a link between high magnesium levels and IDH [96]. High Mg levels in ESKD patients can lead to excessive vasodilation and IDH. Imbalances in Mg levels may lead to changes in fluid compartments and exacerbate hypotension. Abnormal Mg levels can affect the heart's electrical activity and potentially lead to irregular heart rhythms, possibly contributing to IDH. Kyriazis et al., investigating the effects of different dialysate Mg and Ca concentrations, reported that the combination with the fewest episodes of IDH was one of Mg 0.75 mmol/l and calcium 1.25 mmol/L whereas dialysis solution containing Mg 0.25 mmol/l and Ca 1.25 mmol/l triggered IDH due to an impairment of myocardial contractility [26,97]. In agreement with Floege, the commonly used dialysate magnesium concentration of 0.5 mmol/l (or rarely, 0.75 mmol/l) still appears acceptable pending further data [98,99] (Table 2).
4.2. Dialysate Glucose
Glucose-free dialysate could be utilized to avoid hypertriglyceridemia and the potential risk of increased bacterial growth in the dialysate [83]. However, this approach exposed patients to hypoglycemia in patients with diabetes treated with insulin [100,101]. A Dialysate glucose concentration of 100 mg/dL is suggested [46].
4.3. Dialysate Temperature
Dialysate cooling has been demonstrated to increase hemodynamic stability by increasing systemic vascular resistance and enhanced cardiac contractility [102,103,104,105,106], whether through fixed reductions in dialysate temperature or isothermic dialysis. The dialysate is cooled to 0.5-1.0°C in the fixed reduction method below the patient’s body temperature [107]. Using the isothermic method, the dialysate temperature is controlled via a biofeedback device that adjusts the dialysate temperature to prevent the increase in core body temperature that generally occurs during HD [108]. Isothermic dialysis [109] is well tolerated and reduces the incidence of hypotension [110]. However, dialysate cooling can result in side effects such as chilling or cramps, particularly in patients prone to excessive vasoconstriction. Beneficial effects on multiple organ beds have been reported in short-term and longer-term observational studies and one randomized controlled study in incident dialysis patients [6,106,111]. Selby et al., in a randomized study of personalized cooling (MY TEMP), did not observe reductions in cardiovascular mortality or incidence of intradialytic hypotension [112]. Nevertheless, a recent large observational study suggests some patients may benefit from dialysate cooling [113]. Zoccali et al., by instrumental analyses, evaluated the correlation between dialysate temperature at the center level and the IDH’s incidence [113]. In this analysis conducted at the facility level with many adjustments for case-mix, with the same 0.5°C lower dialysate temperature, risk reduction for IDH occurrence was 33%, with a P < 0.001 significance; no association was found between mortality and temperature reduction [113]. In a recent review, Combe and Rubin [114] suggested that while dialysate cooling may not be a panacea solution to prevent IDH episodes [114], it may be efficient in certain patients [110,114,115] and, therefore, should be considered amongst various therapeutic measures for managing this condition [114]. In both incident and prevalent patients, dialysate cooling practices (fixed or isothermal) are suggested for individuals experiencing intradialytic hemodynamic instability. Lowering the dialysate temperature to 35,5°C can reduce the risk of IDH [113] (Table 2). Ensure patients are comfortable and monitor for any symptoms of intolerance.
4.4. Dry Body Weight
The dry body weight (DBW) is the lowest tolerated post-dialysis weight achieved via a gradual change in post-dialysis weight at which there are minimal signs or symptoms of hypovolemia [116]. It refers to a patient's weight after all excess fluid has been removed from the body through HD. DBW represents the patient's most accurate weight without the extra fluid accumulating between dialysis sessions. Post-dialysis target weight should be regularly assessed because an inappropriately low target increases the risk of IDH [26,117,118]. DBW overestimation will increase the size of the interstitial space, minimizing the reduction of plasma volume during HD with elevated UF, but this may cause adverse effects related to an interstitial volume overload. Indeed, it is a significant risk factor in the development of hypertension, left ventricular hypertrophy, and cardiovascular disease, therefore affecting the hard outcomes risk of ESKD on HD treatment [119,120,121,122]. Underestimation of DBW can result in hypovolemia and can induce IDH, cramps, and dizziness [24]. Hypovolemia can lead to diminished blood perfusion to essential organs, resulting in frequent sub-ischemia and thereby potentially contributing to the decline of residual renal function [6]. There are several months between the attainment of DBW and adequate blood pressure control, which is termed the “lag phenomenon” and should be considered. The “lag phenomenon” reflects the slow stabilization of the extracellular fluid compartment while the chronic incident dialysis patient is converting from a catabolic to an anabolic state [123]. It is essential to establish an effective and accurate method for determining the DBW of ESKD patients in HD therapy. Here are some methods used to determine DBW: Clinical Assessment (blood pressure weight trend, neck veins, peripheral edema, bioimpedance analysis, ultrasound lung comets (B-lines), ultrasound measurements of the inferior vena cava diameter, blood volume monitoring with or without biofeedback systems, laboratory parameters (B-type natriuretic peptides, low albumin level, high Ca125, soluble CD146) [26,124]. In FMC EMEA NephroCare clinics, dry body weight and fluid status are assessed using whole-body bioimpedance spectroscopy (BCM; FMC) [122], as described by Moissl et al. [125] and Machek et al. [126]. BCM determines fluid overload (FO) in absolute liters independently of body composition by utilizing a physiological model based on normal tissue hydration [127]. Patients are overhydrated when their relative FO (calculated as FO divided by extracellular volume) is ≥ % in men and ≥ 13% in women, which corresponds to an absolute FO of about 2.5 L [121]. Tailoring DBW adjustments can improve cardiovascular stability during HD treatment. Slowly correcting the DBW and volume status for incident patients is suggested (Table 3). For prevalent patients, it is suggested that DBW and volume status be evaluated every 13 weeks based on clinical assessment and bioimpedance analysis, more frequently in cases of hospitalization or if requested (Table 3).
4.5. Intradialytic Ultrafiltration
The intradialytic ultrafiltration, by removing excess fluid, enhances cardiac performance and venous oxygen saturation in ESKD patients. However, excessive ultrafiltration rates (UFR) pose a risk of myocardial and other organ ischemia. A lower UFR supports compensatory plasma refilling from the extracellular space. An increased treatment time slows the UFR and may help IDH-prone patients. The salt and water gains between dialysis treatments contribute to arrhythmic and hypotensive risks. Several studies have investigated the influence of UFR on patient outcomes. These studies suggest a potential link between higher UFR and the development of IDH, cardiovascular issues, and increased mortality rates [128,129,130,131,132,133]. The HEMO study demonstrated that a UF rate > 13 ml/Kg/h was significantly associated with a greater hazard for the composite outcome of cardiovascular hospitalization and cardiovascular mortality. In contrast, UFR 10-13 ml/Kg/h was not [129]. DOPPS found that a UFR > 10 mL/h/kg correlated with higher odds of IDH and a higher risk of all-cause mortality, while there was no association between UFR and cardiovascular mortality [130]. Flythe et al. observed a progressive increase in the risk of both overall mortality and cardiovascular mortality at UFRs exceeding 10 mL/h/Kg [131]. The Kidney Care Quality Alliance established two quality measures focused on fluid management in HD. These measures prioritize avoiding UFR exceeding 13 mL/h/kg. This approach aims to reduce the incidence of IDH to minimize the risk of long-term damage to vital organs, including the heart, brain, and kidneys, ultimately improving patient survival rates [132]. Mermelstein et al. found a complex relationship between UFR, body weight, and mortality risk. Their study showed that UFR linked to increased mortality risk varied depending on body weight and gender in high–body weight older patients and in high-vintage patients [133]. This highlights the importance of individualized treatment approaches in HD, considering factors beyond just body weight. For incident patients, a gradual adjustment of DBW is suggested based on clinical assessment and bioimpedance analysis. This approach allows for a more personalized and precise approach to fluid management in ESKD patients. It also helps to avoid UFR exceeding 10 mL/h/kg (Table 3).
4.6. Dialysis Dose
For prevalent patients with minimal residual renal function undergoing HD three times per week, a single pool (sp) Kt/V ≥ 1.4 is recommended to ensure adequate dialysis adequacy [33,34] (Table 3). The urea distribution volume (V) should be measured using bioimpedance analysis. In patients with significant residual native kidney function (Kru), the dose may be reduced provided Kru is measured periodically to avoid inadequate dialysis [35]. For HD schedules other than thrice weekly, it is suggested to target a standard Kt/V of 2.3 volumes per week with a minimum delivered dose of 2.1 using a method of calculation that includes the contributions of ultrafiltration and residual kidney function [35]. Convective Volume (On-Line HDF): Post-dilution online-HDF has shown a direct effect in decreasing the incidence of IDH, improving hemodynamic stability—unrelated to improved Na+ balance [134,135,136], and positively impacting cardiac remodeling [137,138,139,140]. Five large randomized controlled trials (RCTs) have demonstrated the superiority of online-HDF over high flux dialysis in terms of hard clinical outcomes, particularly the survival rate of ESKD patients [141,142,143,144,145]. Studies suggest a convective volume above 23 L per session is most favorable for mortality rates [146,147,148,149,150]. Peters et al., in an individual patient data meta-analysis, combined four RCTs [141,142,143,144] and found a 14% reduction in all-cause mortality and a 23% reduction in cardiovascular mortality when treated with online-HDF compared to high flux HD [151]. The largest survival benefit was observed for patients receiving the highest delivered convection volume [151]. The CONVINCE study recently showed a reduction in the relative risk of all-cause mortality by 23%. This reduction was achieved through the prescription of post-dilution high dose (volume) HDF (HV-HDF) defined as convective volumes ≥ 23 L (range ± 1 L) per session [145].
In incident patients, a stepwise approach is recommended by progressively increasing the substitution volume from 5 L in the second week of dialysis by steps of 5 L per week period to reach a convective volume ≥ 23 L in the 5th week of dialysis (Table 3). After this probing period of high-volume HDF, the prescription may be switched to the automated ultrafiltration control mode [152]. Concomitantly, the dialysate bicarbonate concentration should also be progressively increased according to the metabolic characteristics of the patients. According to Canaud and Davenport, switching prevalent and stable dialysis patients to HDF is more effortless than initiating a new patient in HDF [153]. They recommend starting with a post-dilution mode at 50 ml/min and gradually increasing by 25 ml/min per week to reach a convective volume of 125 ml/min. Consider switching to automated ultrafiltration-controlled mode once stable parameters are maintained (132).
5. Intra- and Extra Dialytic Procedures
5.1. Eating during HD
Food ingested before or during HD results in splanchnic blood pooling and the fall of systemic vascular resistance with the potential of IDH. Peripheral vascular resistance typically decreases 20 to 120 minutes following food intake, which may cause a decrease in blood pressure [154,155]. The risks associated with eating during HD include potential fluctuations in blood pressure, blood sugar levels, and electrolyte imbalance. These fluctuations can arise due to fluid and nutrient intake changes during the dialysis session, which may exacerbate existing health conditions or lead to adverse reactions. Therefore, patients with IDH should avoid food ingestion during dialysis to contribute to hemodynamic stability [156] (Table 4). On the other hand, this should be balanced against risks of malnutrition and individualized according to the nutritional requirements and risk profile of patients for adverse intradialytic events [157,158].
5.2. Antihypertensive Drugs
Previous studies have demonstrated a U-shaped relationship between pre-dialysis systolic blood pressure (SBP) and clinical outcomes in dialysis patients [159,160,161]. Data from DOPPS suggests an optimal pre-dialysis SBP range of 130 to 160 mmHg [162]. Patients with very high pre-dialysis SBP (over 160 mmHg) experience a significantly increased risk of cardiovascular events and all-cause mortality [162]. Despite international guidelines recommending against using pre-dialysis blood pressure for diagnosing and managing hypertension in hemodialysis patients, many nephrologists continue to find it a simple and valuable tool in clinical practice [163]. Since 2014, FMC EMEA NephroCare medical governance has implemented this approach, combining a pre-dialysis SBP target of 130-160 mmHg with regular fluid status evaluation and correction via bioimpedance monitoring every 13 weeks or more frequently in cases of clinical necessity or after hospitalization [122]. It's crucial to be cautious with antihypertensive medications, as some might exacerbate the risk of IDH. As many as 50–90% of ESKD patients suffer from hypertension [164], and finding the balance between antihypertensive management and intradialytic hypotension (IDH) risk can be a significant challenge due to fluid removal during dialysis [13]. Excessive fluid volume is a common cause of high blood pressure in dialysis patients, and the use of antihypertensive drugs needs careful management to avoid exacerbating IDH. If antihypertensive drugs are administered shortly before or during a dialysis session, they could potentially lower the patient's blood pressure too much, thereby increasing the risk of IDH. This is particularly concerning when large volumes of fluid are removed during dialysis, as this can further decrease blood pressure. For this reason, clinical staff often need to adjust the timing and dosage of antihypertensive medications in dialysis patients. For instance, they might recommend taking these medications at night or after dialysis rather than before to help reduce the risk of IDH. By promoting urine production and fluid removal on non-dialysis days, diuretics can help to reduce overall fluid overload and the volume of fluid that needs to be removed during dialysis, which might reduce the risk of IDH. The 2006 NKF KDOQI Guidelines recommend the use of diuretics in patients with RRF [165]. Patients retain responsiveness to diuretics until GFR falls below 5 ml/min/1,73 m2 [166]. It is suggested to consider a re-evaluation of antihypertensive medication or administration of a dialysable drug before the HD session to attenuate its antihypertensive effect in hypotension-prone patients [167]. While decreasing the patients' fluid volumes to reach the target weights, antihypertensive medication should be tapered or discontinued as their hypertension improves [168]. We suggest the omission of antihypertensive medication or the administration of a dialysable drug before the HD session in hypotension-prone patients (Table 4). It's a good practice to use diuretics on non-dialysis days, especially in patients with residual renal function, to manage fluid status (Table 4).
5.3. Blood Pressure Monitoring
Given the risk of IDH, frequent Blood pressure monitoring during dialysis is essential. Monitoring blood pressure during dialysis is crucial to evaluate the efficacy of current antihypertensive medications and to adjust medication dosages if needed to ensure blood pressure stays within the target range for the duration of the HD procedure (Table 4).
5.4. Blood Parameters
Regular blood tests, especially during the initial weeks of HD, are crucial for adjusting treatment parameters and dialysate electrolytes. In the first month, it is recommended to review the most important blood parameters (hemoglobin, urea, sodium, potassium, calcium, bicarbonate) weekly. Monthly checks thereafter make sense, including all blood parameters normally evaluated in HD patients (Table 4).
6. Conclusions
The first 90 days after starting HD treatment are generally considered a critical period because patients need to adapt physically, psychologically, and clinically to this new clinical status. FMC EMEA NephroCare has developed a series of intra- and extra-hemodialysis procedures aimed at improving the management and smooth transition of stable incident patients with end-stage kidney disease, as well as ensuring the continuation of dialysis treatment in stable prevalent patients. This approach is designed to maintain meticulous equilibrium in fluid, electrolyte, and acid-base balance while simultaneously ensuring hemodynamic stability during the hemodialysis procedure. All presented intra- and extra-dialytic procedures are intended to minimize the risks of fluid overload, hypertension, and electrolyte disorders, as well as reduce the risk of intra- and extra-dialysis hypotension and cardiac arrhythmias.
Author Contributions
Conceptualization S.S.; writing—original draft preparation, S.S. writing—review and editing, S.S., C.R., M.C., A.T.-R., K.G., M.B., Y.K., N.M., W.M., V.K., J.M., A.A., P.P., M.N., M.E.B.S., J.R., T.J. K.E., V.N., D.V., M.P., O.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
All the authors are FMC employees.
References
- Kuipers, J.; Verboom, L.M.; Ipema, K.J.R.; Paans, W.; Krijnen, W.P.; Gaillard, C.; Westerhuis, R.; Franssen, C.F.M. The Prevalence of Intradialytic Hypotension in Patients on Conventional Hemodialysis: A Systematic Review with Meta-Analysis. Am J Nephrol 2019, 49, 497-506. [CrossRef]
- Ducharlet, K.; Weil, J.; Gock, H.; Philip, J. Kidney Clinicians' Perceptions of Challenges and Aspirations to Improve End-Of-Life Care Provision. Kidney Int Rep 2023, 8, 1627-1637. [CrossRef]
- Lin, E.; Ginsburg, P.B.; Chertow, G.M.; Berns, J.S. The "Advancing American Kidney Health" Executive Order: Challenges and Opportunities for the Large Dialysis Organizations. Am J Kidney Dis 2020, 76, 731-734. [CrossRef]
- Bleyer, A.J.; Russell, G.B.; Satko, S.G. Sudden and cardiac death rates in hemodialysis patients. Kidney Int 1999, 55, 1553-1559. [CrossRef]
- Foley, R.N. Clinical epidemiology of cardiac disease in dialysis patients: left ventricular hypertrophy, ischemic heart disease, and cardiac failure. Semin Dial 2003, 16, 111-117. [CrossRef]
- McIntyre, C.W. Update on Hemodialysis-Induced Multiorgan Ischemia: Brains and Beyond. J Am Soc Nephrol 2024. [CrossRef]
- Tonelli, M.; Karumanchi, S.A.; Thadhani, R. Epidemiology and Mechanisms of Uremia-Related Cardiovascular Disease. Circulation 2016, 133, 518-536. [CrossRef]
- Odudu, A.; McIntyre, C.W. An Update on Intradialytic Cardiac Dysfunction. Semin Dial 2016, 29, 435-441. [CrossRef]
- Broers, N.J.; Cuijpers, A.C.; van der Sande, F.M.; Leunissen, K.M.; Kooman, J.P. The first year on haemodialysis: a critical transition. Clin Kidney J 2015, 8, 271-277. [CrossRef]
- Maddux, D.W.; Usvyat, L.A.; Ketchersid, T.; Jiao, Y.; Blanchard, T.C.; Kotanko, P.; van der Sande, F.M.; Kooman, J.P.; Maddux, F.W. Clinical parameters before and after the transition to dialysis. Hemodialysis international. International Symposium on Home Hemodialysis 2018, 22, 235-244. [CrossRef]
- Wong, S.P.; Kreuter, W.; O'Hare, A.M. Healthcare intensity at initiation of chronic dialysis among older adults. J Am Soc Nephrol 2014, 25, 143-149. [CrossRef]
- Dashtban, A.; Mizani, M.A.; Denaxas, S.; Nitsch, D.; Quint, J.; Corbett, R.; Mamza, J.B.; Morris, T.; Mamas, M.; Lawlor, D.A.; et al. A retrospective cohort study predicting and validating impact of the COVID-19 pandemic in individuals with chronic kidney disease. Kidney Int 2022, 102, 652-660. [CrossRef]
- Kanbay, M.; Ertuglu, L.A.; Afsar, B.; Ozdogan, E.; Siriopol, D.; Covic, A.; Basile, C.; Ortiz, A. An update review of intradialytic hypotension: concept, risk factors, clinical implications and management. Clin Kidney J 2020, 13, 981-993. [CrossRef]
- Shoji, T.; Tsubakihara, Y.; Fujii, M.; Imai, E. Hemodialysis-associated hypotension as an independent risk factor for two-year mortality in hemodialysis patients. Kidney Int 2004, 66, 1212-1220. [CrossRef]
- Assa, S.; Hummel, Y.M.; Voors, A.A.; Kuipers, J.; Westerhuis, R.; de Jong, P.E.; Franssen, C.F. Hemodialysis-induced regional left ventricular systolic dysfunction: prevalence, patient and dialysis treatment-related factors, and prognostic significance. Clin J Am Soc Nephrol 2012, 7, 1615-1623. [CrossRef]
- Flythe, J.E.; Xue, H.; Lynch, K.E.; Curhan, G.C.; Brunelli, S.M. Association of mortality risk with various definitions of intradialytic hypotension. J Am Soc Nephrol 2015, 26, 724-734. [CrossRef]
- Burton, J.O.; Jefferies, H.J.; Selby, N.M.; McIntyre, C.W. Hemodialysis-induced repetitive myocardial injury results in global and segmental reduction in systolic cardiac function. Clin J Am Soc Nephrol 2009, 4, 1925-1931. [CrossRef]
- Tisler, A.; Akocsi, K.; Borbas, B.; Fazakas, L.; Ferenczi, S.; Gorogh, S.; Kulcsar, I.; Nagy, L.; Samik, J.; Szegedi, J.; et al. The effect of frequent or occasional dialysis-associated hypotension on survival of patients on maintenance haemodialysis. Nephrol Dial Transplant 2003, 18, 2601-2605. [CrossRef]
- Assimon, M.M.; Flythe, J.E. Definitions of intradialytic hypotension. Semin Dial 2017, 30, 464-472. [CrossRef]
- Workgroup, K.D. K/DOQI clinical practice guidelines for cardiovascular disease in dialysis patients. Am J Kidney Dis 2005, 45, S1-153.
- Kooman, J.; Basci, A.; Pizzarelli, F.; Canaud, B.; Haage, P.; Fouque, D.; Konner, K.; Martin-Malo, A.; Pedrini, L.; Tattersall, J.; et al. EBPG guideline on haemodynamic instability. Nephrol Dial Transplant 2007, 22 Suppl 2, ii22-44. [CrossRef]
- Mactier, R.; Hoenich, N.; Breen, C. UK Renal Association clinical practice guidelines: Haemodialysis 5th edition. Guideline 8.1 - HD: Symptomatic dialysis-related hypotension haemodialysis. https://renal.org/guidelines/archived-guidelines 2009. Accessed 24 Dec 2018 Available online: (accessed on.
- Hirakata, H.; Nitta, K.; Inaba, M.; Shoji, T.; Fujii, H.; Kobayashi, S.; Tabei, K.; Joki, N.; Hase, H.; Nishimura, M.; et al. Japanese Society for Dialysis Therapy guidelines for management of cardiovascular diseases in patients on chronic hemodialysis. Ther Apher Dial 2012, 16, 387-435. [CrossRef]
- Sands, J.J.; Usvyat, L.A.; Sullivan, T.; Segal, J.H.; Zabetakis, P.; Kotanko, P.; Maddux, F.W.; Diaz-Buxo, J.A. Intradialytic hypotension: frequency, sources of variation and correlation with clinical outcome. Hemodialysis international. International Symposium on Home Hemodialysis 2014, 18, 415-422. [CrossRef]
- Reilly, R.F. Attending rounds: A patient with intradialytic hypotension. Clin J Am Soc Nephrol 2014, 9, 798-803. [CrossRef]
- Davenport, A. Why is Intradialytic Hypotension the Commonest Complication of Outpatient Dialysis Treatments? Kidney Int Rep 2023, 8, 405-418. [CrossRef]
- Daugirdas, J.T. Pathophysiology of dialysis hypotension: an update. Am J Kidney Dis 2001, 38, S11-17.
- van der Sande, F.M.; Dekker, M.J.; Leunissen, K.M.L.; Kooman, J.P. Novel Insights into the Pathogenesis and Prevention of Intradialytic Hypotension. Blood purification 2018, 45, 230-235. [CrossRef]
- Barth, C.; Boer, W.; Garzoni, D.; Kuenzi, T.; Ries, W.; Schaefer, R.; Schneditz, D.; Tsobanelis, T.; van der Sande, F.; Wojke, R.; et al. Characteristics of hypotension-prone haemodialysis patients: is there a critical relative blood volume? Nephrol Dial Transplant 2003, 18, 1353-1360. [CrossRef]
- Worthley, L.I. Shock: a review of pathophysiology and management. Part II. Crit Care Resusc 2000, 2, 66-84.
- Funk, D.J.; Jacobsohn, E.; Kumar, A. The role of venous return in critical illness and shock-part I: physiology. Crit Care Med 2013, 41, 255-262. [CrossRef]
- Montgomery, L.D.; Montgomery, R.W.; Gerth, W.A.; Lew, S.Q.; Klein, M.D.; Stewart, J.M.; Medow, M.S.; Velasquez, M.T. Bioimpedance monitoring of cellular hydration during hemodialysis therapy. Hemodialysis international. International Symposium on Home Hemodialysis 2017, 21, 575-584. [CrossRef]
- Tattersall, J.; Martin-Malo, A.; Pedrini, L.; Basci, A.; Canaud, B.; Fouque, D.; Haage, P.; Konner, K.; Kooman, J.; Pizzarelli, F.; et al. EBPG guideline on dialysis strategies. Nephrol Dial Transplant 2007, 22 Suppl 2, ii5-21. [CrossRef]
- Ashby, D.; Borman, N.; Burton, J.; Corbett, R.; Davenport, A.; Farrington, K.; Flowers, K.; Fotheringham, J.; Andrea Fox, R.N.; Franklin, G.; et al. Renal Association Clinical Practice Guideline on Haemodialysis. BMC Nephrol 2019, 20, 379. [CrossRef]
- KDOQI Clinical Practice Guideline for Hemodialysis Adequacy: 2015 Update. Am J Kidney Dis 2015, 66, 884-930. [CrossRef]
- Tentori, F.; Zhang, J.; Li, Y.; Karaboyas, A.; Kerr, P.; Saran, R.; Bommer, J.; Port, F.; Akiba, T.; Pisoni, R.; et al. Longer dialysis session length is associated with better intermediate outcomes and survival among patients on in-center three times per week hemodialysis: results from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Nephrol Dial Transplant 2012, 27, 4180-4188. [CrossRef]
- Yamamoto, M.; Matsumoto, T.; Ohmori, H.; Takemoto, M.; Ikeda, M.; Sumimoto, R.; Kobayashi, T.; Kato, A.; Ohdan, H. Effect of increased blood flow rate on renal anemia and hepcidin concentration in hemodialysis patients. BMC Nephrol 2021, 22, 221. [CrossRef]
- Leypoldt, J.K.; Cheung, A.K.; Agodoa, L.Y.; Daugirdas, J.T.; Greene, T.; Keshaviah, P.R. Hemodialyzer mass transfer-area coefficients for urea increase at high dialysate flow rates. The Hemodialysis (HEMO) Study. Kidney Int 1997, 51, 2013-2017. [CrossRef]
- Albalate, M.; Pérez-García, R.; de Sequera, P.; Corchete, E.; Alcazar, R.; Ortega, M.; Puerta, M. Is it useful to increase dialysate flow rate to improve the delivered Kt? BMC Nephrol 2015, 16, 20. [CrossRef]
- Mesic, E.; Bock, A.; Major, L.; Vaslaki, L.; Berta, K.; Wikstrom, B.; Canaud, B.; Wojke, R. Dialysate saving by automated control of flow rates: comparison between individualized online hemodiafiltration and standard hemodialysis. Hemodialysis international. International Symposium on Home Hemodialysis 2011, 15, 522-529. [CrossRef]
- Locatelli, F.; Covic, A.; Chazot, C.; Leunissen, K.; Luño, J.; Yaqoob, M. Optimal composition of the dialysate, with emphasis on its influence on blood pressure. Nephrol Dial Transplant 2004, 19, 785-796. [CrossRef]
- Lindley, E.J. Reducing sodium intake in hemodialysis patients. Semin Dial 2009, 22, 260-263. [CrossRef]
- Raimann, J.G.; Thijssen, S.; Usvyat, L.A.; Levin, N.W.; Kotanko, P. Sodium alignment in clinical practice--implementation and implications. Semin Dial 2011, 24, 587-592. [CrossRef]
- Ságová, M.; Wojke, R.; Maierhofer, A.; Gross, M.; Canaud, B.; Gauly, A. Automated individualization of dialysate sodium concentration reduces intradialytic plasma sodium changes in hemodialysis. Artif Organs 2019, 43, 1002-1013. [CrossRef]
- Hussein, W.F.; Schiller, B. Dialysate sodium and intradialytic hypotension. Semin Dial 2017, 30, 492-500. [CrossRef]
- Locatelli, F.; La Milia, V.; Violo, L.; Del Vecchio, L.; Di Filippo, S. Optimizing haemodialysate composition. Clin Kidney J 2015, 8, 580-589. [CrossRef]
- Miskulin, D.C.; Tighiouart, H.; Hsu, C.M.; Weiner, D.E. Dialysate Sodium Lowering in Maintenance Hemodialysis A Randomized Clinical Trial. Clin J Am Soc Nephrol 2024. [CrossRef]
- Lindley, E.; Tattersall, J. What Is the Optimal Dialysate Sodium Concentration? Kidney and Dialysis 2021, 1, 157-160.
- Hecking, M.; Karaboyas, A.; Rayner, H.; Saran, R.; Sen, A.; Inaba, M.; Bommer, J.; Hörl, W.H.; Pisoni, R.L.; Robinson, B.M.; et al. Dialysate sodium prescription and blood pressure in hemodialysis patients. American journal of hypertension 2014, 27, 1160-1169. [CrossRef]
- Canaud, B. A Personal and Practical Answer From a Clinical Perspective. Kidney Dialysis 2021, 1, 149–151. [CrossRef]
- Canaud, B.; Kooman, J.; Maierhofer, A.; Raimann, J.; Titze, J.; Kotanko, P. Sodium First Approach, to Reset Our Mind for Improving Management of Sodium, Water, Volume and Pressure in Hemodialysis Patients, and to Reduce Cardiovascular Burden and Improve Outcomes. Front Nephrol 2022, 2, 935388. [CrossRef]
- Raimann, J.G.; Ficociello, L.H.; Usvyat, L.A.; Zhang, H.; Pacelli, L.; Moore, S.; Sheppard, P.; Xiao, Q.; Wang, Y.; Mullon, C.; et al. Effects of dialysate to serum sodium (Na(+)) alignment in chronic hemodialysis (HD) patients: retrospective cohort study from a quality improvement project. BMC Nephrol 2018, 19, 75. [CrossRef]
- Kuhlmann, U.; Maierhofer, A.; Canaud, B.; Hoyer, J.; Gross, M. Zero Diffusive Sodium Balance in Hemodialysis Provided by an Algorithm-Based Electrolyte Balancing Controller: A Proof of Principle Clinical Study. Artif Organs 2019, 43, 150-158. [CrossRef]
- Ponce, P.; Pinto, B.; Wojke, R.; Maierhofer, A.P.; Gauly, A. Evaluation of intradialytic sodium shifts during sodium controlled hemodialysis. The International journal of artificial organs 2020, 43, 620-624. [CrossRef]
- Sagova, M.; Wojke, R.; Maierhofer, A.; Gross, M.; Canaud, B.; Gauly, A. Automated individualization of dialysate sodium concentration reduces intradialytic plasma sodium changes in hemodialysis. Artif Organs 2019, 43, 1002-1013. [CrossRef]
- Leunissen, K.M.; van den Berg, B.W.; van Hooff, J.P. Ionized calcium plays a pivotal role in controlling blood pressure during haemodialysis. Blood purification 1989, 7, 233-239. [CrossRef]
- Tovbin, D.; Sherman, R.A. Correcting Acidosis during Hemodialysis: Current Limitations and a Potential Solution. Semin Dial 2016, 29, 35-38. [CrossRef]
- Abramowitz, M.K. Bicarbonate Balance and Prescription in ESRD. J Am Soc Nephrol 2017, 28, 726-734. [CrossRef]
- Lomashvili, K.; Garg, P.; O'Neill, W.C. Chemical and hormonal determinants of vascular calcification in vitro. Kidney Int 2006, 69, 1464-1470. [CrossRef]
- Mendoza, F.J.; Lopez, I.; Montes de Oca, A.; Perez, J.; Rodriguez, M.; Aguilera-Tejero, E. Metabolic acidosis inhibits soft tissue calcification in uremic rats. Kidney Int 2008, 73, 407-414. [CrossRef]
- Mudunuru, S.A.; Navarrete, J.; O'Neill, W.C. Metabolic alkalosis in hemodialysis patients. Semin Dial 2023, 36, 24-28. [CrossRef]
- Qian, Q. Acid-base alterations in ESRD and effects of hemodialysis. Semin Dial 2018, 31, 226-235. [CrossRef]
- Bozikas, A.; Kiriakoutzik, I.; Petrou, I.; Touroutzis, T.; Kitoukidi, E.; Pisanidou, P.; Vakiani, S.; Georgilas, N.; Martika, A.; Pangidis, P.; et al. Aiming for the optimal bicarbonate prescription for maintenance hemodialysis therapy in end-stage renal disease. Hemodialysis international. International Symposium on Home Hemodialysis 2019, 23, 173-180. [CrossRef]
- Yokoyama, A.; Kikuchi, K.; Kawamura, Y. [Heart rate variability, arrhythmia and magnesium in hemodialysis patients]. Clin Calcium 2005, 15, 226-232.
- Wieliczko, M.; Małyszko, J. Acid-base balance in hemodialysis patients in everyday practice. Ren Fail 2022, 44, 1090-1097. [CrossRef]
- Tentori, F.; Karaboyas, A.; Robinson, B.M.; Morgenstern, H.; Zhang, J.; Sen, A.; Ikizler, T.A.; Rayner, H.; Fissell, R.B.; Vanholder, R.; et al. Association of dialysate bicarbonate concentration with mortality in the Dialysis Outcomes and Practice Patterns Study (DOPPS). Am J Kidney Dis 2013, 62, 738-746. [CrossRef]
- Gabutti, L.; Ferrari, N.; Giudici, G.; Mombelli, G.; Marone, C. Unexpected haemodynamic instability associated with standard bicarbonate haemodialysis. Nephrol Dial Transplant 2003, 18, 2369-2376. [CrossRef]
- K/DOQI clinical practice guidelines for bone metabolism and disease in chronic kidney disease. Am J Kidney Dis 2003, 42, S1-201.
- Drüeke, T.B.; Touam, M. Calcium balance in haemodialysis--do not lower the dialysate calcium concentration too much (con part). Nephrol Dial Transplant 2009, 24, 2990-2993. [CrossRef]
- Maynard, J.C.; Cruz, C.; Kleerekoper, M.; Levin, N.W. Blood pressure response to changes in serum ionized calcium during hemodialysis. Ann Intern Med 1986, 104, 358-361. [CrossRef]
- van der Sande, F.M.; Cheriex, E.C.; van Kuijk, W.H.; Leunissen, K.M. Effect of dialysate calcium concentrations on intradialytic blood pressure course in cardiac-compromised patients. Am J Kidney Dis 1998, 32, 125-131. [CrossRef]
- Erratum: Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Update Work Group. KDIGO 2017 Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int Suppl. 2017;7:1-59. Kidney Int Suppl (2011) 2017, 7, e1. [CrossRef]
- Ketteler, M.; Block, G.A.; Evenepoel, P.; Fukagawa, M.; Herzog, C.A.; McCann, L.; Moe, S.M.; Shroff, R.; Tonelli, M.A.; Toussaint, N.D.; et al. Executive summary of the 2017 KDIGO Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD) Guideline Update: what's changed and why it matters. Kidney Int 2017, 92, 26-36. [CrossRef]
- McGill, R.L.; Weiner, D.E. Dialysate Composition for Hemodialysis: Changes and Changing Risk. Semin Dial 2017, 30, 112-120. [CrossRef]
- Pun, P.H.; Horton, J.R.; Middleton, J.P. Dialysate calcium concentration and the risk of sudden cardiac arrest in hemodialysis patients. Clin J Am Soc Nephrol 2013, 8, 797-803. [CrossRef]
- Jimenez, Z.N.; Silva, B.C.; Reis, L.D.; Castro, M.C.; Ramos, C.D.; Costa-Hong, V.; Bortolotto, L.A.; Consolim-Colombo, F.; Dominguez, W.V.; Oliveira, I.B.; et al. High Dialysate Calcium Concentration May Cause More Sympathetic Stimulus During Hemodialysis. Kidney Blood Press Res 2016, 41, 978-985. [CrossRef]
- Genovesi, S.; Rossi, E.; Nava, M.; Riva, H.; De Franceschi, S.; Fabbrini, P.; Viganò, M.R.; Pieruzzi, F.; Stella, A.; Valsecchi, M.G.; et al. A case series of chronic haemodialysis patients: mortality, sudden death, and QT interval. Europace 2013, 15, 1025-1033. [CrossRef]
- Yoshikawa, M.; Takase, O.; Tsujimura, T.; Sano, E.; Hayashi, M.; Takato, T.; Hishikawa, K. Long-term effects of low calcium dialysates on the serum calcium levels during maintenance hemodialysis treatments: A systematic review and meta-analysis. Scientific Reports 2018, 8, 5310. [CrossRef]
- Garimella, P.S.; Malhotra, R. Dialysate Calcium: A Lot More Than 'Set It and Forget It'. Kidney Med 2019, 1, 238-241. [CrossRef]
- Sakoh, T.; Taniguchi, M.; Yamada, S.; Ohnaka, S.; Arase, H.; Tokumoto, M.; Yanagida, T.; Mitsuiki, K.; Hirakata, H.; Nakano, T.; et al. Short- and Long-term Effects of Dialysate Calcium Concentrations on Mineral and Bone Metabolism in Hemodialysis Patients: The K4 Study. Kidney Med 2019, 1, 296-306. [CrossRef]
- van der Sande, F.M.; Ter Meulen, K.J.A.; Kotanko, P.; Kooman, J.P. Dialysate Calcium Levels: Do They Matter? Blood purification 2019, 47, 230-235. [CrossRef]
- Voroneanu, L.; Covic, A. Arrhythmias in hemodialysis patients. J Nephrol 2009, 22, 716-725.
- Basile, C.; Lomonte, C. A neglected issue in dialysis practice: haemodialysate. Clin Kidney J 2015, 8, 393-399. [CrossRef]
- Basile, C.; Libutti, P.; Lisi, P.; Teutonico, A.; Vernaglione, L.; Casucci, F.; Lomonte, C. Ranking of factors determining potassium mass balance in bicarbonate haemodialysis. Nephrol Dial Transplant 2015, 30, 505-513. [CrossRef]
- Feig, P.U.; Shook, A.; Sterns, R.H. Effect of potassium removal during hemodialysis on the plasma potassium concentration. Nephron 1981, 27, 25-30. [CrossRef]
- Zehnder, C.; Gutzwiller, J.P.; Huber, A.; Schindler, C.; Schneditz, D. Low-potassium and glucose-free dialysis maintains urea but enhances potassium removal. Nephrol Dial Transplant 2001, 16, 78-84. [CrossRef]
- Buemi, M.; Aloisi, E.; Coppolino, G.; Loddo, S.; Crasci, E.; Aloisi, C.; Barilla, A.; Cosentini, V.; Nostro, L.; Caccamo, C.; et al. The effect of two different protocols of potassium haemodiafiltration on QT dispersion. Nephrol Dial Transplant 2005, 20, 1148-1154. [CrossRef]
- Ansari, N.; Manis, T.; Feinfeld, D.A. Symptomatic atrial arrhythmias in hemodialysis patients. Ren Fail 2001, 23, 71-76. [CrossRef]
- Morrison, G.; Michelson, E.L.; Brown, S.; Morganroth, J. Mechanism and prevention of cardiac arrhythmias in chronic hemodialysis patients. Kidney Int 1980, 17, 811-819. [CrossRef]
- Korzets, A.; Ori, Y.; Herman, M. Serum potassium levels and atrial fibrillation in haemodialysis patients. Nephrol Dial Transplant 2001, 16, 1090. [CrossRef]
- Khouri, Y.; Stephens, T.; Ayuba, G.; AlAmeri, H.; Juratli, N.; McCullough, P.A. Understanding and Managing Atrial Fibrillation in Patients with Kidney Disease. J Atr Fibrillation 2015, 7, 1069. [CrossRef]
- Pun, P.H.; Lehrich, R.W.; Honeycutt, E.F.; Herzog, C.A.; Middleton, J.P. Modifiable risk factors associated with sudden cardiac arrest within hemodialysis clinics. Kidney Int 2011, 79, 218-227. [CrossRef]
- Karnik, J.A.; Young, B.S.; Lew, N.L.; Herget, M.; Dubinsky, C.; Lazarus, J.M.; Chertow, G.M. Cardiac arrest and sudden death in dialysis units. Kidney Int 2001, 60, 350-357. [CrossRef]
- Karaboyas, A.; Zee, J.; Brunelli, S.M.; Usvyat, L.A.; Weiner, D.E.; Maddux, F.W.; Nissenson, A.R.; Jadoul, M.; Locatelli, F.; Winkelmayer, W.C.; et al. Dialysate Potassium, Serum Potassium, Mortality, and Arrhythmia Events in Hemodialysis: Results From the Dialysis Outcomes and Practice Patterns Study (DOPPS). Am J Kidney Dis 2017, 69, 266-277. [CrossRef]
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. KDOQI Clinical Practice Guideline for Nutrition in CKD: 2020 Update. Am J Kidney Dis 2020, 76, S1-S107. [CrossRef]
- Elsharkawy, M.M.; Youssef, A.M.; Zayoon, M.Y. Intradialytic changes of serum magnesium and their relation to hypotensive episodes in hemodialysis patients on different dialysates. Hemodialysis international. International Symposium on Home Hemodialysis 2006, 10 Suppl 2, S16-23. [CrossRef]
- Kyriazis, J.; Kalogeropoulou, K.; Bilirakis, L.; Smirnioudis, N.; Pikounis, V.; Stamatiadis, D.; Liolia, E. Dialysate magnesium level and blood pressure. Kidney Int 2004, 66, 1221-1231. [CrossRef]
- Floege, J. Magnesium Concentration in Dialysate: Is Higher Better? Clin J Am Soc Nephrol 2018, 13, 1309-1310. [CrossRef]
- Alhosaini, M.; Leehey, D.J. Magnesium and Dialysis: The Neglected Cation. Am J Kidney Dis 2015, 66, 523-531. [CrossRef]
- Takahashi, A.; Kubota, T.; Shibahara, N.; Terasaki, J.; Kagitani, M.; Ueda, H.; Inoue, T.; Katsuoka, Y. The mechanism of hypoglycemia caused by hemodialysis. Clin Nephrol 2004, 62, 362-368. [CrossRef]
- Jackson, M.A.; Holland, M.R.; Nicholas, J.; Talbot, M.; Spencer, H.; Lodwick, R.; Fuhrmann, C.; Forster, D.; Macdonald, I.A. Occult hypoglycemia caused by hemodialysis. Clin Nephrol 1999, 51, 242-247.
- Pizzarelli, F. From cold dialysis to isothermic dialysis: a twenty-five year voyage. Nephrol Dial Transplant 2007, 22, 1007-1012. [CrossRef]
- Levy, F.L.; Grayburn, P.A.; Foulks, C.J.; Brickner, M.E.; Henrich, W.L. Improved left ventricular contractility with cool temperature hemodialysis. Kidney Int 1992, 41, 961-965. [CrossRef]
- Coli, U.; Landini, S.; Lucatello, S.; Fracasso, A.; Morachiello, P.; Righetto, F.; Scanferla, F.; Onesti, G.; Bazzato, G. Cold as cardiovascular stabilizing factor in hemodialysis: hemodynamic evaluation. Trans Am Soc Artif Intern Organs 1983, 29, 71-75.
- Mahida, B.H.; Dumler, F.; Zasuwa, G.; Fleig, G.; Levin, N.W. Effect of cooled dialysate on serum catecholamines and blood pressure stability. Trans Am Soc Artif Intern Organs 1983, 29, 384-389.
- Selby, N.M.; Burton, J.O.; Chesterton, L.J.; McIntyre, C.W. Dialysis-induced regional left ventricular dysfunction is ameliorated by cooling the dialysate. Clin J Am Soc Nephrol 2006, 1, 1216-1225. [CrossRef]
- Selby, N.M.; McIntyre, C.W. A systematic review of the clinical effects of reducing dialysate fluid temperature. Nephrol Dial Transplant 2006, 21, 1883-1898. [CrossRef]
- van der Sande, F.M.; Rosales, L.M.; Brener, Z.; Kooman, J.P.; Kuhlmann, M.; Handelman, G.; Greenwood, R.N.; Carter, M.; Schneditz, D.; Leunissen, K.M.; et al. Effect of ultrafiltration on thermal variables, skin temperature, skin blood flow, and energy expenditure during ultrapure hemodialysis. J Am Soc Nephrol 2005, 16, 1824-1831. [CrossRef]
- Rosales, L.M.; Schneditz, D.; Morris, A.T.; Rahmati, S.; Levin, N.W. Isothermic hemodialysis and ultrafiltration. Am J Kidney Dis 2000, 36, 353-361. [CrossRef]
- Maggiore, Q.; Pizzarelli, F.; Santoro, A.; Panzetta, G.; Bonforte, G.; Hannedouche, T.; Alvarez de Lara, M.A.; Tsouras, I.; Loureiro, A.; Ponce, P.; et al. The effects of control of thermal balance on vascular stability in hemodialysis patients: results of the European randomized clinical trial. Am J Kidney Dis 2002, 40, 280-290. [CrossRef]
- Eldehni, M.T.; Odudu, A.; McIntyre, C.W. Randomized clinical trial of dialysate cooling and effects on brain white matter. J Am Soc Nephrol 2015, 26, 957-965. [CrossRef]
- Selby, N.M.; Taal, M.W. Evaluating the results of MyTEMP, a cluster randomised trial of lower temperature haemodialysis: the end of a cool idea? Lancet (London, England) 2022, 400, 1657-1659. [CrossRef]
- Zoccali, C.; Tripepi, G.; Neri, L.; Savoia, M.; Baró Salvador, M.E.; Ponce, P.; Hymes, J.; Maddux, F.; Mallamaci, F.; Stuard, S. Effectiveness of cold HD for the prevention of HD hypotension and mortality in the general HD population. Nephrol Dial Transplant 2023, 38, 1700-1706. [CrossRef]
- Combe, C.; Rubin, S. Cold haemodialysis: the instrumental power of large cohorts. Nephrol Dial Transplant 2023, 38, 1577-1579. [CrossRef]
- Odudu, A.; Eldehni, M.T.; McCann, G.P.; McIntyre, C.W. Randomized Controlled Trial of Individualized Dialysate Cooling for Cardiac Protection in Hemodialysis Patients. Clin J Am Soc Nephrol 2015, 10, 1408-1417. [CrossRef]
- Sinha, A.D.; Agarwal, R. Can chronic volume overload be recognized and prevented in hemodialysis patients? The pitfalls of the clinical examination in assessing volume status. Semin Dial 2009, 22, 480-482. [CrossRef]
- Hamrahian, S.M.; Vilayet, S.; Herberth, J.; Fülöp, T. Prevention of Intradialytic Hypotension in Hemodialysis Patients: Current Challenges and Future Prospects. Int J Nephrol Renovasc Dis 2023, 16, 173-181. [CrossRef]
- Berger, D.; Takala, J. Hypotension and hypovolemia during hemodialysis: is the usual suspect innocent? Crit Care 2016, 20, 140. [CrossRef]
- Onofriescu, M.; Siriopol, D.; Voroneanu, L.; Hogas, S.; Nistor, I.; Apetrii, M.; Florea, L.; Veisa, G.; Mititiuc, I.; Kanbay, M.; et al. Overhydration, Cardiac Function and Survival in Hemodialysis Patients. PLoS One 2015, 10, e0135691. [CrossRef]
- Fishbane, S.; Natke, E.; Maesaka, J.K. Role of volume overload in dialysis-refractory hypertension. Am J Kidney Dis 1996, 28, 257-261. [CrossRef]
- Wizemann, V.; Wabel, P.; Chamney, P.; Zaluska, W.; Moissl, U.; Rode, C.; Malecka-Masalska, T.; Marcelli, D. The mortality risk of overhydration in haemodialysis patients. Nephrol Dial Transplant 2009, 24, 1574-1579. [CrossRef]
- Zoccali, C.; Moissl, U.; Chazot, C.; Mallamaci, F.; Tripepi, G.; Arkossy, O.; Wabel, P.; Stuard, S. Chronic Fluid Overload and Mortality in ESRD. J Am Soc Nephrol 2017, 28, 2491-2497. [CrossRef]
- Charra, B.; Bergstrom, J.; Scribner, B.H. Blood pressure control in dialysis patients: importance of the lag phenomenon. Am J Kidney Dis 1998, 32, 720-724. [CrossRef]
- Arrigo, M.; Von Moos, S.; Gerritsen, K.; Sadoune, M.; Tangvoraphonkchai, K.; Davenport, A.; Mebazaa, A.; Segerer, S.; Cippà, P.E. Soluble CD146 and B-type natriuretic peptide dissect overhydration into functional components of prognostic relevance in haemodialysis patients. Nephrol Dial Transplant 2018, 33, 2035-2042. [CrossRef]
- Moissl, U.M.; Wabel, P.; Chamney, P.W.; Bosaeus, I.; Levin, N.W.; Bosy-Westphal, A.; Korth, O.; Müller, M.J.; Ellegård, L.; Malmros, V.; et al. Body fluid volume determination via body composition spectroscopy in health and disease. Physiol Meas 2006, 27, 921-933. [CrossRef]
- Machek, P.; Jirka, T.; Moissl, U.; Chamney, P.; Wabel, P. Guided optimization of fluid status in haemodialysis patients. Nephrol Dial Transplant 2010, 25, 538-544. [CrossRef]
- Chamney, P.W.; Wabel, P.; Moissl, U.M.; Müller, M.J.; Bosy-Westphal, A.; Korth, O.; Fuller, N.J. A whole-body model to distinguish excess fluid from the hydration of major body tissues. The American journal of clinical nutrition 2007, 85, 80-89. [CrossRef]
- Movilli, E.; Gaggia, P.; Zubani, R.; Camerini, C.; Vizzardi, V.; Parrinello, G.; Savoldi, S.; Fischer, M.S.; Londrino, F.; Cancarini, G. Association between high ultrafiltration rates and mortality in uraemic patients on regular haemodialysis. A 5-year prospective observational multicentre study. Nephrol Dial Transplant 2007, 22, 3547-3552. [CrossRef]
- Cheung, A.K.; Sarnak, M.J.; Yan, G.; Berkoben, M.; Heyka, R.; Kaufman, A.; Lewis, J.; Rocco, M.; Toto, R.; Windus, D.; et al. Cardiac diseases in maintenance hemodialysis patients: results of the HEMO Study. Kidney Int 2004, 65, 2380-2389. [CrossRef]
- Saran, R.; Bragg-Gresham, J.L.; Levin, N.W.; Twardowski, Z.J.; Wizemann, V.; Saito, A.; Kimata, N.; Gillespie, B.W.; Combe, C.; Bommer, J.; et al. Longer treatment time and slower ultrafiltration in hemodialysis: associations with reduced mortality in the DOPPS. Kidney Int 2006, 69, 1222-1228. [CrossRef]
- Flythe, J.E.; Kimmel, S.E.; Brunelli, S.M. Rapid fluid removal during dialysis is associated with cardiovascular morbidity and mortality. Kidney Int 2011, 79, 250-257. [CrossRef]
- #2701, N.Q.F. Avoidance of Utilization of High Ultrafiltration Rate (>/= 13 ml/kg/hour). Available at https://kidneycarepartners.org/wp-content/uploads/2015/10/Yellow-AllKCQASummary09-11-15CLEAN.pdf. Accessed April 2, 2024. Available online: (accessed on.
- Mermelstein, A.; Raimann, J.G.; Wang, Y.; Kotanko, P.; Daugirdas, J.T. Ultrafiltration Rate Levels in Hemodialysis Patients Associated with Weight-Specific Mortality Risks. Clin J Am Soc Nephrol 2023, 18, 767-776. [CrossRef]
- Locatelli, F.; Altieri, P.; Andrulli, S.; Bolasco, P.; Sau, G.; Pedrini, L.A.; Basile, C.; David, S.; Feriani, M.; Montagna, G.; et al. Hemofiltration and hemodiafiltration reduce intradialytic hypotension in ESRD. J Am Soc Nephrol 2010, 21, 1798-1807. [CrossRef]
- Donauer, J.; Schweiger, C.; Rumberger, B.; Krumme, B.; Bohler, J. Reduction of hypotensive side effects during online-haemodiafiltration and low temperature haemodialysis. Nephrol Dial Transplant 2003, 18, 1616-1622. [CrossRef]
- Sande, F.M.V.; Kooman, J.P.; Konings, C.J.; Leunissen, K.M.L. Thermal effects and blood pressure response during postdilution hemodiafiltration and hemodialysis: the effect of amount of replacement fluid and dialysate temperature. J Am Soc Nephrol 2001, 12, 1916-1920. [CrossRef]
- Rodriguez, A.; Morena, M.; Bargnoux, A.S.; Chenine, L.; Leray-Moragues, H.; Cristol, J.P.; Canaud, B. Quantitative assessment of sodium mass removal using ionic dialysance and sodium gradient as a proxy tool: Comparison of high-flux hemodialysis versus online hemodiafiltration. Artif Organs 2021, 45, E280-E292. [CrossRef]
- Czifra, A.; Pall, A.; Kulcsar, J.; Barta, K.; Kertesz, A.; Paragh, G.; Lorincz, I.; Jenei, Z.; Agarwal, A.; Zarjou, A.; et al. Hemodialysis and hemodiafiltration differently modulate left ventricular diastolic function. BMC Nephrol 2013, 14, 76. [CrossRef]
- La Milia, V.; Ravasi, C.; Carfagna, F.; Alberghini, E.; Baragetti, I.; Buzzi, L.; Ferrario, F.; Furiani, S.; Barbone, G.S.; Pontoriero, G. Sodium removal and plasma tonicity balance are not different in hemodialysis and hemodiafiltration using high-flux membranes. J Nephrol 2019, 32, 461-469. [CrossRef]
- den Hoedt, C.H.; Bots, M.L.; Grooteman, M.P.; van der Weerd, N.C.; Mazairac, A.H.; Penne, E.L.; Levesque, R.; ter Wee, P.M.; Nube, M.J.; Blankestijn, P.J.; et al. Online hemodiafiltration reduces systemic inflammation compared to low-flux hemodialysis. Kidney Int 2014, 86, 423-432. [CrossRef]
- Maduell, F.; Moreso, F.; Pons, M.; Ramos, R.; Mora-Macia, J.; Carreras, J.; Soler, J.; Torres, F.; Campistol, J.M.; Martinez-Castelao, A.; et al. High-efficiency postdilution online hemodiafiltration reduces all-cause mortality in hemodialysis patients. J Am Soc Nephrol 2013, 24, 487-497. [CrossRef]
- Ok, E.; Asci, G.; Toz, H.; Ok, E.S.; Kircelli, F.; Yilmaz, M.; Hur, E.; Demirci, M.S.; Demirci, C.; Duman, S.; et al. Mortality and cardiovascular events in online haemodiafiltration (OL-HDF) compared with high-flux dialysis: results from the Turkish OL-HDF Study. Nephrol Dial Transplant 2013, 28, 192-202. [CrossRef]
- Grooteman, M.P.; van den Dorpel, M.A.; Bots, M.L.; Penne, E.L.; van der Weerd, N.C.; Mazairac, A.H.; den Hoedt, C.H.; van der Tweel, I.; Levesque, R.; Nube, M.J.; et al. Effect of online hemodiafiltration on all-cause mortality and cardiovascular outcomes. J Am Soc Nephrol 2012, 23, 1087-1096. [CrossRef]
- Mercadal, L.; Franck, J.E.; Metzger, M.; Urena Torres, P.; de Cornelissen, F.; Edet, S.; Bechade, C.; Vigneau, C.; Drueke, T.; Jacquelinet, C.; et al. Hemodiafiltration Versus Hemodialysis and Survival in Patients With ESRD: The French Renal Epidemiology and Information Network (REIN) Registry. Am J Kidney Dis 2016, 68, 247-255. [CrossRef]
- Blankestijn, P.J.; Vernooij, R.W.M.; Hockham, C.; Strippoli, G.F.M.; Canaud, B.; Hegbrant, J.; Barth, C.; Covic, A.; Cromm, K.; Cucui, A.; et al. Effect of Hemodiafiltration or Hemodialysis on Mortality in Kidney Failure. N Engl J Med 2023, 389, 700-709. [CrossRef]
- Neri, L.; Gurevich, K.; Zarya, Y.; Plavinskii, S.; Bellocchio, F.; Stuard, S.; Barbieri, C.; Canaud, B. Practice Patterns and Outcomes of Online Hemodiafiltration: A Real-World Evidence Study in a Russian Dialysis Network. Blood purification 2021, 50, 309-318. [CrossRef]
- Imamovic, G.; Hrvacevic, R.; Kapun, S.; Marcelli, D.; Bayh, I.; Grassmann, A.; Scatizzi, L.; Maslovaric, J.; Canaud, B. Survival of incident patients on high-volume online hemodiafiltration compared to low-volume online hemodiafiltration and high-flux hemodialysis. International urology and nephrology 2014, 46, 1191-1200. [CrossRef]
- Canaud, B.; Barbieri, C.; Marcelli, D.; Bellocchio, F.; Bowry, S.; Mari, F.; Amato, C.; Gatti, E. Optimal convection volume for improving patient outcomes in an international incident dialysis cohort treated with online hemodiafiltration. Kidney Int 2015, 88, 1108-1116. [CrossRef]
- Canaud, B.; Bayh, I.; Marcelli, D.; Ponce, P.; Merello, J.I.; Gurevich, K.; Ladanyi, E.; Ok, E.; Imamovic, G.; Grassmann, A.; et al. Improved survival of incident patients with high-volume haemodiafiltration: a propensity-matched cohort study with inverse probability of censoring weighting. Nephron 2015, 129, 179-188. [CrossRef]
- Maduell, F.; Varas, J.; Ramos, R.; Martin-Malo, A.; Perez-Garcia, R.; Berdud, I.; Moreso, F.; Canaud, B.; Stuard, S.; Gauly, A. Hemodiafiltration reduces all-cause and cardiovascular mortality in incident hemodialysis patients: a propensity-matched cohort study. American Journal of Nephrology 2017, 46, 288-297.
- Peters, S.A.; Bots, M.L.; Canaud, B.; Davenport, A.; Grooteman, M.P.; Kircelli, F.; Locatelli, F.; Maduell, F.; Morena, M.; Nubé, M.J.; et al. Haemodiafiltration and mortality in end-stage kidney disease patients: a pooled individual participant data analysis from four randomized controlled trials. Nephrol Dial Transplant 2016, 31, 978-984. [CrossRef]
- Marcelli, D.; Scholz, C.; Ponce, P.; Sousa, T.; Kopperschmidt, P.; Grassmann, A.; Pinto, B.; Canaud, B. High-volume postdilution hemodiafiltration is a feasible option in routine clinical practice. Artif Organs 2015, 39, 142-149. [CrossRef]
- Canaud, B.; Davenport, A. Prescription of online hemodiafiltration (ol-HDF). Semin Dial 2022, 35, 413-419. [CrossRef]
- Sherman, R.A.; Torres, F.; Cody, R.P. Postprandial blood pressure changes during hemodialysis. Am J Kidney Dis 1988, 12, 37-39. [CrossRef]
- Avci, M.; Arikan, F. The effect of food intake during hemodialysis on blood pressure: A nonrandomized experimental trial. Ther Apher Dial 2023, 27, 661-668. [CrossRef]
- Barakat, M.M.; Nawab, Z.M.; Yu, A.W.; Lau, A.H.; Ing, T.S.; Daugirdas, J.T. Hemodynamic effects of intradialytic food ingestion and the effects of caffeine. J Am Soc Nephrol 1993, 3, 1813-1818. [CrossRef]
- Fotiadou, E.; Georgianos, P.I.; Chourdakis, M.; Zebekakis, P.E.; Liakopoulos, V. Eating during the Hemodialysis Session: A Practice Improving Nutritional Status or a Risk Factor for Intradialytic Hypotension and Reduced Dialysis Adequacy? Nutrients 2020, 12. [CrossRef]
- Kalantar-Zadeh, K.; Ikizler, T.A. Let them eat during dialysis: an overlooked opportunity to improve outcomes in maintenance hemodialysis patients. J Ren Nutr 2013, 23, 157-163. [CrossRef]
- Bansal, N.; McCulloch, C.E.; Lin, F.; Alper, A.; Anderson, A.H.; Cuevas, M.; Go, A.S.; Kallem, R.; Kusek, J.W.; Lora, C.M.; et al. Blood Pressure and Risk of Cardiovascular Events in Patients on Chronic Hemodialysis: The CRIC Study (Chronic Renal Insufficiency Cohort). Hypertension 2017, 70, 435-443. [CrossRef]
- Hara, M.; Tanaka, S.; Taniguchi, M.; Fujisaki, K.; Torisu, K.; Masutani, K.; Hirakata, H.; Nakano, T.; Tsuruya, K.; Kitazono, T. Prognostic value of pre-dialysis blood pressure and risk threshold on clinical outcomes in hemodialysis patients: The Q-Cohort Study. Medicine (Baltimore) 2018, 97, e13485. [CrossRef]
- Bansal, N.; McCulloch, C.E.; Rahman, M.; Kusek, J.W.; Anderson, A.H.; Xie, D.; Townsend, R.R.; Lora, C.M.; Wright, J.; Go, A.S.; et al. Blood pressure and risk of all-cause mortality in advanced chronic kidney disease and hemodialysis: the chronic renal insufficiency cohort study. Hypertension 2015, 65, 93-100. [CrossRef]
- Robinson, B.M.; Tong, L.; Zhang, J.; Wolfe, R.A.; Goodkin, D.A.; Greenwood, R.N.; Kerr, P.G.; Morgenstern, H.; Li, Y.; Pisoni, R.L.; et al. Blood pressure levels and mortality risk among hemodialysis patients in the Dialysis Outcomes and Practice Patterns Study. Kidney Int 2012, 82, 570-580. [CrossRef]
- Liang, Y.; Gan, L.; Shen, Y.; Li, W.; Zhang, D.; Li, Z.; Ren, J.; Xu, M.; Zhao, X.; Ma, Y.; et al. Clinical characteristics and management of hemodialysis patients with pre-dialysis hypertension: a multicenter observational study. Ren Fail 2022, 44, 1811-1818. [CrossRef]
- Wang, K.M.; Sirich, T.L.; Chang, T.I. Timing of blood pressure medications and intradialytic hypotension. Semin Dial 2019, 32, 201-204. [CrossRef]
- Hemodialysis Adequacy Work, G. Clinical practice guidelines for hemodialysis adequacy, update 2006. Am J Kidney Dis 2006, 48 Suppl 1, S2-90. [CrossRef]
- Gregory, L.F., Jr.; Durrett, R.R.; Robinson, R.R.; Clapp, J.R. The short-term effect of furosemide on electrolyte and water excretion in patients with severe renal disease. Archives of internal medicine 1970, 125, 69-74.
- Levin, N.W.; Kotanko, P.; Eckardt, K.U.; Kasiske, B.L.; Chazot, C.; Cheung, A.K.; Redon, J.; Wheeler, D.C.; Zoccali, C.; London, G.M. Blood pressure in chronic kidney disease stage 5D-report from a Kidney Disease: Improving Global Outcomes controversies conference. Kidney Int 2010, 77, 273-284. [CrossRef]
- Jindal, K.; Chan, C.T.; Deziel, C.; Hirsch, D.; Soroka, S.D.; Tonelli, M.; Culleton, B.F.; Canadian Society of Nephrology Committee for Clinical Practice, G. Hemodialysis clinical practice guidelines for the Canadian Society of Nephrology. J Am Soc Nephrol 2006, 17, S1-27. [CrossRef]
Figure 1.
Incident patients’ mortality in FMC EMEA NephroCare Clinics.
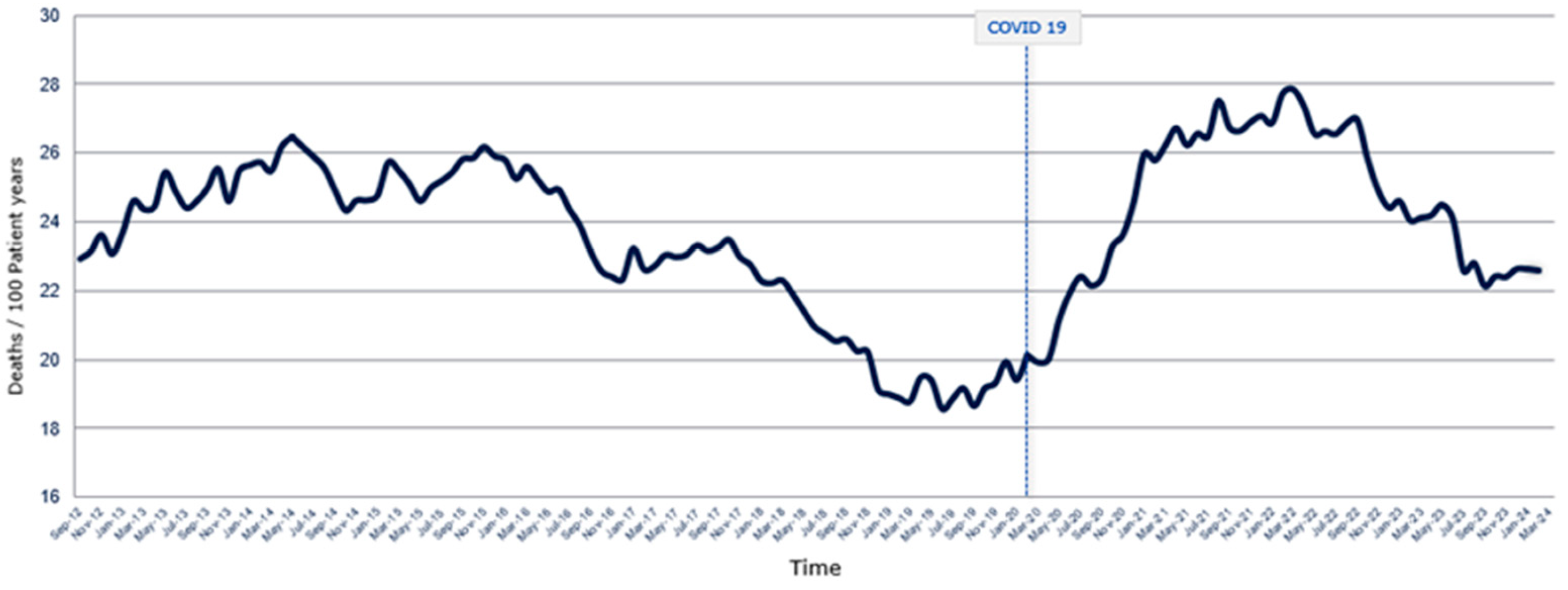

Table 1.
For stable incident patients not crushing on dialysis, consider a stepwise increase in treatment time and frequency based on residual renal function, dialyzer area surface, blood, and dialysate flows. Slowly increasing the blood flow in the first 10 minutes of dialysis is suggested.
Table 1.
For stable incident patients not crushing on dialysis, consider a stepwise increase in treatment time and frequency based on residual renal function, dialyzer area surface, blood, and dialysate flows. Slowly increasing the blood flow in the first 10 minutes of dialysis is suggested.
| Stable Incident Patients | Stable Prevalent Patients | ||||
|---|---|---|---|---|---|
| Time | 1st week | 2nd week | 3rd week | 4th week | ≥ 5th week |
| Frequency (n) | ≥ 2* | ≥ 3* | ≥ 3* | ||
| Treatment time (min) | 120-180 | ≤ 180 | ≤ 240 | ≥ 240† | |
| Dialyzer area surface (m2) | 1.4 | 1.4 ± 0.2* | |||
| Qb (ml/min) | ≤ 150 | ≤ 200 | ≤ 300 | ≥ 340† | |
| Qd (ml/min); Qd/Qb | 300; 1.5 | 500; 1.2 | ≥ 500; ≥ 1.2 (if spKt/V < 1.4) | ||
† Different targets according to patient clinical conditions and characteristics. * Increase the dialyzer area surface according to patient characteristics cording to patient characteristics. Qb: blood flow. Qd: dialysate flow. sp: single pool.
Table 2.
Stepwise dialysate electrolyte prescription is for stable incident patients who are not crushing on dialysis and are prevalent patients. .
Table 2.
Stepwise dialysate electrolyte prescription is for stable incident patients who are not crushing on dialysis and are prevalent patients. .
| Stable Incident Patients | Stable Prevalent Patients | ||||
|---|---|---|---|---|---|
| Time | 1st week | 2nd week | 3rd week | 4th week | ≥ 5th week |
| Sodium (mEq/l) | 140-143* | 140-142* | 140-141* | 139-140* | 138-140* |
| Bicarbonate (mEq/l) | ≤ 28* | ≤ 29* | ≤ 30* | ≤ 31* | ≤ 32* |
| Calcium (mmol/l) | 1.50–1.75* | 1.25–1.50* | |||
| Potassium (mEq/l) | 3* | 2–3* | |||
| Magnesium (mmol/l) | 0.5 | 0.5 | |||
| Glucose (mg/dl) | 100 | 100 | |||
| Temperature (°C) | 36.5 (≤ 36.0 in case of IDH) | 36.0; (if IDHs: ≤ 36.0 if tolerated) | |||
* Adjust the dialysate electrolyte prescription according to lab test results. IDH: Intradialytic Hypotensive episode.
Table 3.
Stepwise fluid status management and dialysis dose in stable incident patients not crushing on dialysis and prevalent patients.
Table 3.
Stepwise fluid status management and dialysis dose in stable incident patients not crushing on dialysis and prevalent patients.
| Stable Incident Patients | Stable Prevalent Patients | ||||||
|---|---|---|---|---|---|---|---|
| Time | 1st week | 2nd week | 3rd week | 4th week | ≥ 5th week–3rd months | ≥ 3rd month | |
| DBW1 | Slowly correct | As week 1-4th | Every 3 months* | ||||
| Fluid status | Before 1st HD | Every 2 weeks | Monthly | Every 3 months* | |||
| UF (ml/h/Kg) | ≤ 10** | ≤ 13** | |||||
| spKt/V | No targets | ≥ 1.4 | |||||
| Post-dilution Qsub (L) | 0 | ≤ 5 | ≤ 15 | ≥ 21 (Convective volume/HDF > 23 L) † | |||
1 DBW (dry body weight)/volume status should be evaluated by clinical assessment and instrumental methods. *More frequently if requested and mandatory after hospitalization. ** Reduce in case of frequent intradialytic hypotensive episodes. Qsub: substitution volume. sp: single pool.
Table 4.
Stepwise approach on intra- and extra dialytic procedures for incident and prevalent patients.
Table 4.
Stepwise approach on intra- and extra dialytic procedures for incident and prevalent patients.
| Stable Incident Patients | Stable Prevalent Patients | |||||
|---|---|---|---|---|---|---|
| Time | 1st week | 2nd week | 3rd week | 4th week | ≥ 5th week–3rd months | ≥ 3rd month |
| Eating during HD | Avoid in case of IDH | Avoid in case of IDH | ||||
| AHTs1 | Tapering while decreasing the body weight | No dialyzable AHTs in case of IDH | ||||
| Diuretics | Only in interdialytic days if IDH | Only in interdialytic days if IDH | ||||
| RRF evaluation | Before 1st HD | No | Monthly* | Quarterly* | ||
| BP monitoring | Pre-Post HD and every 30 min**. | Pre-Post HD and every 60 min**. | ||||
| Blood tests*** | Before 1st HD | Weekly | Monthly | |||
1 AHTs: Antihypertensive drugs. * Applicable in case diuresis/die > 500 ml. ** More frequent in the case of IDH. ***: Hemoglobin, calcium, bicarbonate, potassium, sodium.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



