Submitted:
15 April 2024
Posted:
17 April 2024
You are already at the latest version
Abstract
The aging of the population in developing and developed countries has lead to a significant increase in health burden of spinal diseases. These elderly patients often have a number of medical co-morbidities due to aging. The need for minimally invasive techniques to address spinal disorders in this elderly population group cannot be stressed enough. Minimally invasive spine surgery (MISS) has several proven benefits such as minimal muscle trauma, minimal bony resection, lesser post-operative pain, decreased infection rate and shorter hospital stay. Over the last 40 years, constant efforts are being made to develop newer techniques of spine surgery. Endoscopic spine surgery is one such subset of MISS which has all the benefits of modern MISS. Endoscopic spine surgery initially was limited only to treatment of lumbar disc herniations. With improvement in optics, endoscopes, endoscopic drills and shavers, irrigation pumps, there has been a paradigm shift. Endoscopic spine surgery can now be performed with high magnification thus allowing its application not only to lumbar spinal stenosis, but also to spinal fusion surgeries, cervical and thoracic pathology as well. There has been increasing evidence in support of these newer techniques of spine surgery. For the purpose of this review, we studied current available literature and outlined the historical evolution of endoscopic spine surgery, the various different endoscopic systems, and techniques available and the current applications of endoscopic techniques as an alternative to traditional spinal surgery.
Keywords:
Endoscopic spinal surgery
; full endoscopy
; Biportal endoscopy
; Lumbar endoscopy
; Thoracic endoscopy
; Cervical endoscopy
1. Introduction
With advancements in medical care and increased life expectancy of the aging population, the global burden of spinal disease has increased [1]. Spine related disorders significantly affect the quality of life (QOL) and ability to perform activities of daily living among the elderly [2]. Elderly patients with spinal disorders often suffer from numerous co-morbidities and medical problems further complicating surgical treatment and functional outcomes [1,3,4]. In an attempt to decrease the morbidity associated with conventional open spine surgery, numerous advances have been made in the field of minimally invasive spine (MIS) surgery. MIS surgery has several advantages such as minimal soft tissue trauma, lesser blood loss, decreased infection rates, earlier rehabilitation, shorter hospital stay, and better functional outcomes [5]. Endoscopic spine surgery is an evolving subset of MIS surgery with ever growing indications [6]. With development of specialized instrumentation and high resolution imaging, endoscopic spine surgery initially limited to lumbar discectomies, can now be used to treat a wide range of spinal pathologies such as spinal stenosis, instability, thoracic and cervical myelopathy, infections, intradural tumors, etc. [7,8,9].
With this review, we aim to outline the historical evolution of endoscopic techniques for spine surgery, the present applications of endoscopic spine surgery in clinical practice and the latest advances in this field.
2. Evolution of Endoscopic Techniques for Spine Surgery
The earliest account of percutaneous decompression techniques dates back to Kambin in 1973 and Hijikata in 1975 who described their technique of percutaneous nucleotomy which was an indirect non visualized decompression through the postero-lateral approach using fluoroscopy. Kambin used Criag cannula (5.5mm) and Hijikata used a 2.6mm cannula respectively [10,11]. The next advancement to percutaneous nucleotomy was the addition of endoscopes and in 1983 Kambin described his technique of percutaneous arthroscopic discectomy[12] and subsequently, in 1990, he described a triangular safe zone bordered by the exiting root anteriorly, the traversing root medially, and the superior endplate of the lower lumbar vertebra inferiorly [13]. The description of this radiographic safe working zone allowed the introduction of larger instruments and working channels in closer proximity to the foraminal pathology without injuring the nerve root and thus led to further advancements in the field of endoscopic spine surgery.
In 1997, Foley described his technique of mircroendoscopic discectomy which to date is one of the most popular techniques of discectomy. He used a 25 degree scope through a 16mm tubular retractor to achieve decompression for far lateral disc herniations [14,15]. In the same year, the Destandau’s Endospine technique was introduced by Dr J. Destandau, based on the principle of laparoscopic triangulation between an endoscope and suction with working instrument. The system is composed of three tubes: one for the endoscope, one for aspiration and the largest one for standard surgical instruments [16,17]. In 1990s, Yeung developed an operating spine scope with a working channel and introduced beveled and slotted cannulas and subsequently allowed for direct visualization surgical removal of disc material and foraminal decompression (foraminoplasty) through of a uniportal approach [18,19]. They called their technique the “inside out technique” of endoscopic spine surgery where the working cannula was placed inside in the intervertebral disc [20]. Subsequently, in an attempt to avoid irritation of the nerve root in cases of foraminal stenosis Thomas Hoogland described the “outside in technique” where the working cannula was placed in the neural foramen after widening it using reamers [21]
Even though transforaminal endoscopic techniques were popular, there were several technical challenges for transforaminal access at L5 - S1 level owing to anatomical constraints such as high iliac crest, large L5 transverse process, large facet, narrow disc space and neural foramen [22,23]. In an attempt to overcome these technical difficulties Choi et al described the the technique of percutaneous endoscopic inter-laminar discectomy using a rigid working channel endoscope [24]. Irrespective of the technique used, the above endoscopic spine surgeries are performed through a single incision involving light source, irrigation, and instrumentation. Despite use of a superior imaging, visualization is restricted and technical difficulties may be encountered by surgeons, which are of relevance in severely stenotic canals or in cases requiring bilateral decompression [25]. Unilateral biportal endoscopic spinal surgery (UBE) or percutaneous biportal endoscopic decompression (PBED) [26] is the combination of integrated open and endoscopic spinal surgery, which can lessen the impact of the limitations. Unlike other endoscopic techniques, this technique utilizes 2 independent portals, one for introduction of the endoscope and other for introduction of surgical instruments.

Table 1.
Historical review of endoscopic technique.
| Year | Author | Technique described |
|---|---|---|
| 1973 | Kambin (10) | Percutaneous nucleotomy with Craig cannula (5mm) Fluoroscopy guided without visualization |
| 1975 | Hijikata (11) | Percutaneous nucleotomy (2.6mm cannula) Fluoroscopy guided without visualization |
| 1983 | Kambin (12) | Percutaneous arthroscopic discectomy |
| 1997 | Foley (14) | Microendoscopic discectomy |
| 1999 | Yeung (18) | YESS - inside out technique |
| 1999 | Destandau (16) | Destandau’s Endospine technique |
| 2005 | Hoogland (21) | Transforaminal Endoscopy - Outside in technique |
| 2006 | Choi (24) | Interlaminar approach for L5-S1 level |
| 2016 | Eum et al (26) | Unilateral Biportal Endoscopy (PBED) |
3. Lumbar Spine Endoscopy
3.1. Microendoscopic Discectomy and Decompression
Microendoscopic discectomy is a minimally invasive surgery technique that was initially described in 1997 [14]. It allows surgeons to work with two hands through a small-diameter, operating table–mounted tubular retractor and a 25 degree endoscope. [14,15]. Compared to conventional open discectomy, microendoscopic discectomy(MED) has several advantages such as lesser blood loss, cosmesis, shorter hospital stay, and early return to work [15]. A study of 150 consecutive patients treated with MED in 2005 confirmed these findings [27]. MED technique has been used not only for paracentral disc herniations, but also for all types including far lateral, cephalad, caudal migrated, and recurrent disc herniations [28,29].
Due to the advantages of MED, in 2002, Khoo and Fessler modified the MED technique and used it to treat 25 patients with LSS [30]. Compared to the open technique, microendoscopic decompression group had statistical decrease in operative blood loss, postoperative narcotic requirement, and length of hospital stay (42 hr versus 94 hr) [30]. Even today, Microendoscopic discectomy and decompression are one of the most commonly performed techniques for treatment of lumbar disc herniations and lumbar spinal stenosis.
Figure 1.
MED, A: METRx system C: Scope and attachment, D: Endoscopy image.
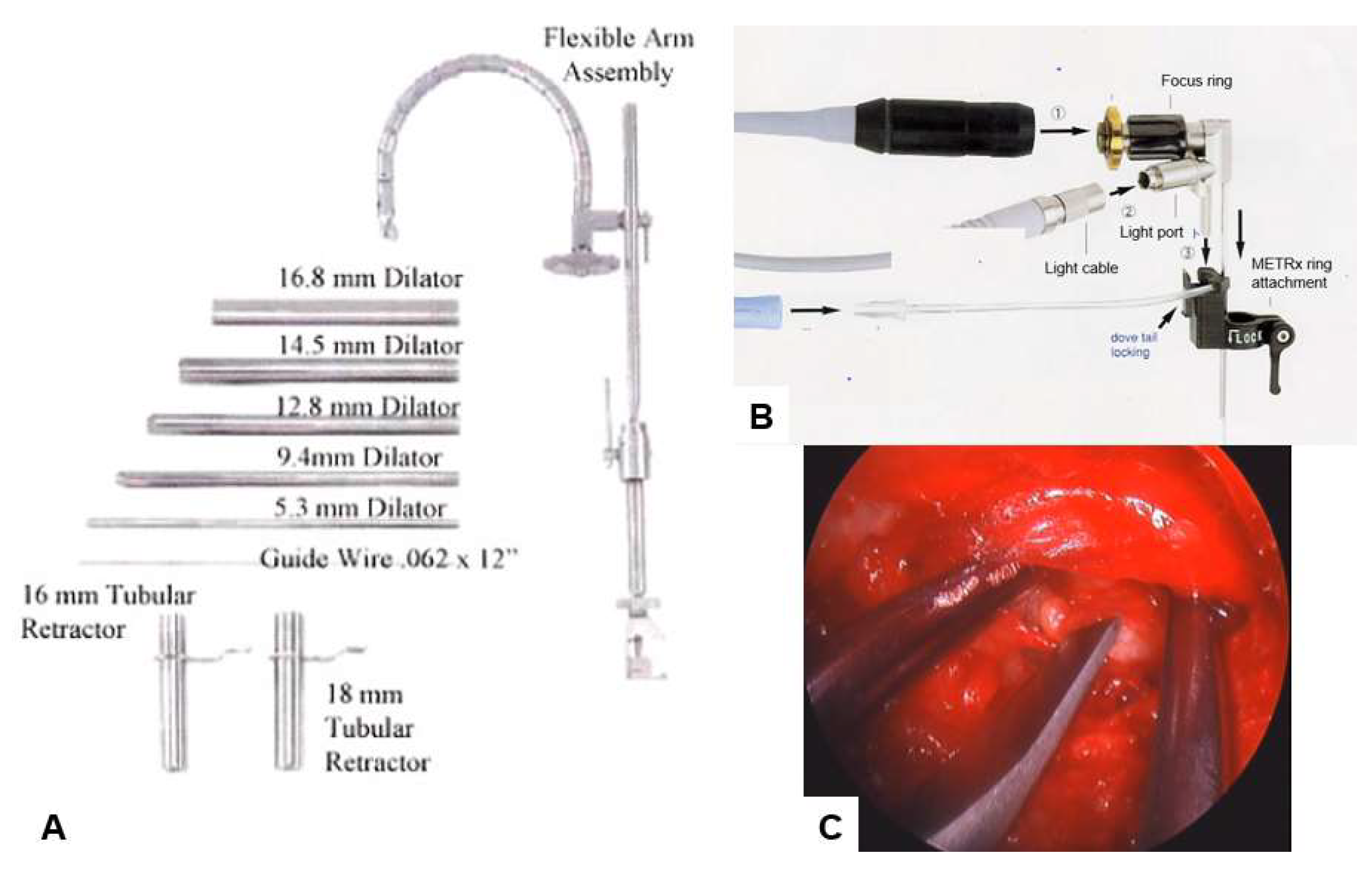
Table 2.
Surgical results of microendoscopic discectomy and decompression.
| Author | Sample | Approach | Follow up | Outcomes | Complication |
|---|---|---|---|---|---|
| Perez-Cruet 2002 [27] |
150 | Paramedian | 12 months | Mean operative time (min) 97 Mean hospital stay (hours) 7.7 (range, 2–24) Mean time to return to work (days) 17 |
Dural tears 8/150 (5%) recurrence 4/150 Pseudomeningocoele 1/150 (0.7%) Surgical site infection 1/150 (0.7%) |
| Khoo 2002 [30] | 25 vs 25 open | Paramedian | 12 months | Lesser blood loss 44ml for med vs 193 ml Shorter hospital stay 42 hours vs 94 hours |
Additional fusion surgery 0% vs. 12% Transfusion 0% vs. 8% Dural tear 16% vs. 8% |
| Ikuta 2005 [31] | 47 vs 29 microdiscectony |
Paramedian | 22 months | Rate of recovery 72% (improvement in JOA score) (38/47) | Higher complication rate compared to microdiscectomy |
| Wu 2006 [32] | 873 Vs 358 open | Not specified | 28 months vs 31 months for open | Earlier return to work
Shorter hospital stay Shorter operation time Lesser blood loss Lesser analgesic need |
35/873 for MED vs 19/358 |
| Fukushi 2015 [33] | 58 vs 39 open |
Midline | 42 months | Similar improvement in JOA and similar patient satisfaction | Higher rate of infection, |
| Wu 2020 [34] | 82 vs. 52 Full endoscopy |
Paramedian | 20 months | Similar improvement in VAS for leg pain Higher VAS for low back pain and ODI |
Dysesthesia 0% vs. 1.9%, Dural tear 2.4%vs. 1.9%, Urinary retention 1.2% vs. 0%, Total 3.85% vs. 3.66% |
| Iwai 2020 [35] | 60 vs. 54Microendoscopic | Paramedian | 3 months | Shorter operating time but longer hospital stay compared to biportal endoscopy. Similar VAS/NRS in both groups |
Dural tear 5.6% vs. 1.8% Hematoma 3.3% vs. 13.0% |
| Ito 2021 [36] | 139 vs. 42 Biportal Endoscopy | Paramedian | 6 months | Similar improvement in VAS for low back pain and leg pain, OD | Dural tear 5.8% vs. 4.7%, Hematoma 3.6% vs. 0%, Re-operation1.4% vs. 0% |
3.2. Destandau’s Endospine Technique:
This technique requires use of a specialized system called the Destandau Endospine System (Karl Storz, Tuttlingen, Germany), which comprises an endospine tube, trocar, and working insert. The working insert comprises four ports—4-mm endoscope (0°), 4-mm suction cannula, 8-mm for the working instrument, and nerve root retractor [37]There are numerous applications of the Destandau system ranging from degenerative spinal conditions to intradural tumor surgery [21]
Figure 2.
instruments of Destandau’s endospine technique.

3.3. Transforaminal Endoscopy
Transforaminal approach was the first approach which was used by the pioneers of full endoscopic spine surgery techniques[38] The key transforaminalecompression is safe docking of the endoscope, which requires careful analysis of preoperative radiologic imaging to evaluate the angle of approach required to retrieve fragment and understand the anatomic constrains in the transforaminal approach.(38)two popular techniques are the “inside out technique” [20] by Yeung and the “outside in technique” described by Hoogland. (21) Although it was initially believed that transforaminal approach has several limitations , literature suggests that this technique can be applied successfully to treat migrated disc herniations and foraminal pathology such as foraminal disc herniations and foraminal stenosis. (39,40) Literature suggests that challenging cases like highly migrated disc herniations can be operated by using the transformational endoscopic lumbar discectomy (TELD) by performing partial resection of the pedicle and enlargement of the foramen. (41) TELF can be used to treat foraminal stenosis while maintaining favorable long-term outcomes without the need for fusion in the vast majority of patients. (42) Several cadaveric studies also showed confirmed feasibility and efficacy of percutaneous endoscopic lumbar foraminoplasty/ TELF.(43,44)
When used for revision spine surgery, TELF and TELD are associated with minimal blood loss, lesser scar tissue formation and similar operating time compared to primary spine surgeries (45,46 In addition to other advantages of this technique such as shorter operation time, minimal blood loss and less muscle trauma, there are several published reports of transforaminal endoscopic spine surgery performed in awake patients under local anesthesia (47,48). Therefore, transforaminal endoscopic spine surgery is a viable surgical treatment option for patients with severe medical co-morbidities who are medically unfit to undergo surgery under general anesthesia.
Figure 3.
Three kinds of endoscopic approaches, A: Inside out approach - Starts from the disc to the epidural space、B : Outside in approach - Starts from the epidural space, with or without foraminoplasty、C: Interlaminar approach.
Figure 3.
Three kinds of endoscopic approaches, A: Inside out approach - Starts from the disc to the epidural space、B : Outside in approach - Starts from the epidural space, with or without foraminoplasty、C: Interlaminar approach.
3.4. Interlaminar Endoscopy :
3.4.1. Interlaminar Endoscopic Lumbar Discectomy (IELD)
Due to technical difficult of using the transforaminal approach at L5-S1 level due to anatomical constraints, the inter laminar approach was advocated (24). Due to similar orientation compared to conventional posterior decompression techniques, the inter laminar approach though initially described for L5-S1 level was popularized for surgical treatment of lumbar canal stenosis (LCS) even at higher lumbar levels.
The patients undergoing IELD have significant advantages such as lower immediate postoperative back pain, shorter operation time, and rapid return to work.(49) Reuten et al followed up 178 patients who underwent either interlaminar endoscopic lumbar discectomy (IELD) or microsurgical discectomy and concluded that Full-endoscopic surgery is a sufficient and safe alternative to microsurgical procedures with minimal soft tissue trauma. (50)
The Interlaminar approach can also be used to treat Lumbar spinal stenosis. Lumbar endoscopic - unilateral laminotomy and bilateral decompression (LE-ULBD) when compared to microscopic ULBD showed comparable clinical and radiological outcomes. The endoscopic approach might further minimize tissue injury and enhance post-operative recovery. (51,52) McGrath et al in a similar study found that Lumbar endoscopic unilateral laminotomy for bilateral decompression is a safe and effective surgical procedure with favorable complication profile and patient outcomes.(53).
3.4.2. Percutaneous Biportal Endoscopic Discectomy and Decompression (PBED)
The PBED technique, involves using one portal for the endoscope and the other for introduction of instruments for performing decompression. In recent years, this technique of spinal surgery has gained tremendous popularity due to the advantages of familiarity of surgeons to posterior approach, free dexterity and use of conventional instruments used for open spine surgery. (54,55,56). It is generally believed that UBE surgery has the advantages of a wider field of vision, minimal muscle damage and faster recovery. (57) The learning curve of this technique is relatively shorter than that of uniportal full endoscopic surgery, which is another advantage of the UBE technique. (58)
UBE discectomy is a good treatment choice for lumbar disc herniation.(59) The Biportal endoscopic technique can also be used to treat foraminal pathology such as foraminal stenosis and far lateral disc herniation by using the extraforaminal technique described by Ann.(52)
A number of studies have compared the intra-operative and post-operative outcomes following PBED. Compared to ILED, PBED has superior results such as shorter operation time, better central canal decompression.(60) and less violation of the facet joints. (61) PBED has also demonstrated favorable clinical outcomes for revision surgery such as lower postoperative pain and has outcomes comparable to primary PBED, thus suggesting advantage of PBED for revision spine surgeries. (62)
Figure 4.
Unilateral Biportal Endoscopic Transforaminal Lumbar Interbody Fusion. A:Scopic and Instrument portals. B:Endoscopic view after soft tissue dissection. C:osteotomy of inferior articular process (IAP) D:Resection of tip of superior articular process (SAP) E&F:removal of disc and preparation of disc space. G: Endoscopic view showing insertion of cage.H:Final position of cage. This step is followed by insertion of Percutaneous Pedicle screws under fluoroscopic guidance.
Figure 4.
Unilateral Biportal Endoscopic Transforaminal Lumbar Interbody Fusion. A:Scopic and Instrument portals. B:Endoscopic view after soft tissue dissection. C:osteotomy of inferior articular process (IAP) D:Resection of tip of superior articular process (SAP) E&F:removal of disc and preparation of disc space. G: Endoscopic view showing insertion of cage.H:Final position of cage. This step is followed by insertion of Percutaneous Pedicle screws under fluoroscopic guidance.
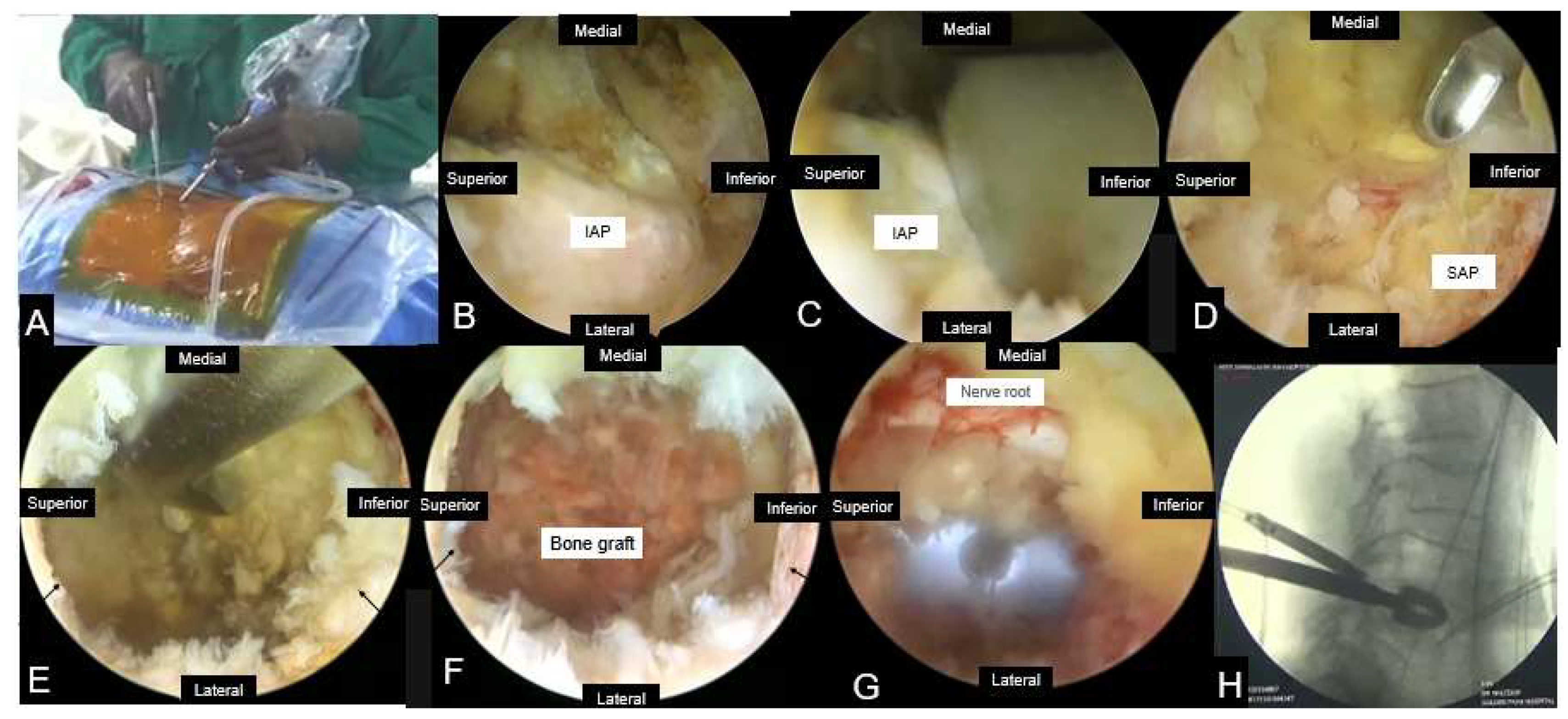
Table 3.
Clinical Results of Unilateral Biportal Endoscopy.
| Author | Study type | Sample | Diagnosis | Follow up(Months) | Operation time (minutes) | Complications |
|---|---|---|---|---|---|---|
| Eum et al(2016) [26] | Retrospective | 58 | LSS | 13.8 | 68.9 ± 16.1 | 13.8%; post-op headache(3),dural tear (2),transient numbness (2), epidural hepatoma (1) |
| Choi et al (2016) [63] | Retrospective | 68 | LDH(25),revision(3) stenosis(39),synovial cyst(1) | NR | 68.2±23.7 | 10.3%;dural tear(2),nerve root injury(1),incomplete decompression(4) |
| Kim et al(2018)[64] | Retrospective | 60 | LDH | 12.6 | 70.15 ± 22.0 | 5%, incomplete decompression (3) |
| Ahn et al (2018)[55] | Retrospective | 21 | Foraminal stenosis (11), foraminal LDH(9),ASD(1) | 14.8 | 96.7 | 4.8%;dural tear (1) |
| Kim and Choi (2018)[65] | Retrospective | 105 | LSS | 14 | 53 ± 13.5 | 2.9%;dural tear (2), epidural hematoma(1) |
| Akbary et al (2018)[66] | Retrospective | 30 | Lateral recess+foraminal stenosis | 5.67 | 102.5 ± 43.66 | 0% |
| Pao et al (2019)[67] | Retrospective | 81 | LSS | 8.6 | NR | 8.6%;dural tear(4), transient motor weakness (1), inadequate decompression (1),epidural hematoma(1) |
| Wang et al (2023)[68] | Prospective | 70 | LDH | 24 | NR | 0% |
3.4.3. Endoscopic Lumbar Interbody Fusion
Current literature in endoscopic fusion can be broadly divided into transforaminal lumbar interbody fusion by the Kambin triangle ventral to the facet joint with or without foraminoplasty, transforaminal lumbar interbody fusion through posterolateral approach by uniportal or biportal endoscopy, through the resected facet joint and endoscopic-assisted lateral lumbar interbody fusion.(7) The technique of transforaminal lumbar inter body fusion via the Kambin’s triangle can be used as an alternative technique for spinal fusion in patients with severe medical comorbidities as it can be done under local anesthesia. (69) The technique is based on the principle of indirect decompression and has several advantages such as short operative time, minimal blood loss and ability to perform visualized preparation of the end plates. However, the disadvantages are possibility of injuring the exiting nerve root and radiation exposure.(70)
Full endoscopic lumbar interbody fusion (FELIF) has the advantage that it allows direct decompression of pathology with minimal invasive technique.(70) FE-PLIF via the inter laminar approach is known to have outcomes compared to other popular minimally invasive techniques like MIS TLIF with minimal surgical trauma.(71).
Endoscopic lumbar interbody fusion using percutaneous unilateral biportal endoscopic technique can achieve direct neural decompression similar to conventional open surgery and can be an alternative to minimally invasive LIF surgery for treating degenerative lumbar disease. However, long-term follow-up and larger clinical studies are needed to validate the clinical and radiological results of this surgery.(54)
According to a recent meta-analysis, UBE-TLIF was superior to MIS-TLIF in terms of intraoperative blood loss, duration of hospital stay, VAS score for low back pain and ODI score, but the operative time was longer than MIS-TLIF group. There were no significant differences between the two groups in terms of total complication rate, modified Macnab grading criteria, fusion rate, VAS score of leg pain, lumbar lordosis, intervertebral disk height.(72)
4. Thoracic Spine Endoscopy
Initially limited to the lumbar spine, in recent years there has been a steady and significant interest in its applications to cervical and thoracic spine pathologies. With instrumentation and technology spinal endoscopy is now a viable alternative to traditional open surgery that avoids the risks & complications associated with open thoracic spine surgery. The sizes and the number of working channels are the parameters typically used to categorize the different types of spinal endoscopy and much of the capabilities of these different systems, and their inherent advantages and disadvantages, are predicated upon these two factors(73). The techniques most commonly employed are full endoscopy (transforaminal & posterior percutaneous), micro-endoscopy and bi-portal endoscopy.
4.1. Full Endoscopy
The following full endoscopic classifications are currently recommended by the AO Spine group(74).1) Transforaminal endoscopic thoracic discectomy (TETD).,2) Thoracic endoscopic unilateral laminotomy for bilateral decompression (TE-ULBD), 3) Transpedicular endoscopic surgery. The most commonly employed approaches are transforaminal and interlaminar. The majority of reports describe a transforaminal approach for disc prolapse with interlaminar access used for the treatment of significant canal stenosis(75). The results of endoscopic discectomy in the thoracic spine have been satisfactory suggesting possibility of large scale role of minimally invasive endoscopic techniques in the surgical management of thoracic disc herniations including soft as well as calcified discs. (76,77)
Use of endoscopy for other spinal disease such as infection and tumor have been reported in several publications(78). Yang et al.(79) in a relatively large series of patients with tuberculosis, described use of percutaneous decompression with fusion with allograft followed by percutaneous pedicle screw fixation. They reported excellent outcomes with 96% of patients achieving acceptable fusion. The increasing number of publications in the last three years suggests that full endoscopy is the technique of choice in many centers and will become the universal standard of patient care(75).
4.2. Micro-Endoscopy
The thoracic micro-endoscopic discectomy (TMED) technique is a modification of the lumbar micro-endoscopic technique that has been used with success to treat stenosis as well as disc herniations(80). This method has been implemented successfully to treat lateralized and central soft thoracic disc herniations causing radicular and myelopathic symptoms(81).
The TMED technique has a number of advantages over other traditional techniques for thoracic discectomy and include the following: avoidance of entering the thoracic cavity, minimal osseous and ligamentous removal, maintenance of disc integrity, avoidance of the need for thoracic fusion, and avoidance of extensive posterior muscle dissection(81). TMED is a safe effective treatment for surgical removal of herniated thoracic intervertebral discs and allows for a posterolateral approach to thoracic disc herniation without entry into the chest cavity that consistently gives access to the majority of the canal while requiring only a minimal amount of bone removal. (80,82)
4.3. Bi-Portal Endoscopy (UBE)
Thoracic laminectomy has traditionally been considered gold standard for the treatment of thoracic OLF and stenosis. Post surgery back ache, paraspinal muscular atrophy and instability are known complications of traditional open surgery often requiring revision and fusion. The clinical outcomes of a conventional technique for thoracic OLF or thoracic spinal stenosis are frequently un- satisfactory and comorbid(83).
To address these issues, unilateral bi-portal endoscopy (UBE) techniques for thoracic laminectomy have been developed and published , demonstrating various advantages over conventional thoracic laminectomy, and reporting competent clinical results(84,70). The main advantages of this approach are the independence of scope and instrument control, as well as greater degree of freedom for positioning of the instruments(58). Although UBE has grown in popularity in recent years, thoracic ULBD via UBE is technically difficult (86).
UBE decompression is a viable treatment alternative which is capable of achieving satisfactory clinical results in patients with thoracic OLF.(87) While treating thoracic OLF or thoracic spinal stenosis, UBE decompression technique with unilateral approach and bilateral decompression appears to be safe and effective. (86) Although thoracic ULBD by UBE is not currently the standard treatment for thoracic OLF or thoracic spinal stenosis, this technique has the potential to be more widely used in the future(87).
5. Cervical Spine Endoscopy
The anterior percutaneous cervical discectomy was the prototype of cervical endoscopic surgery.(88 Subsequently many variations & techniques have been developed to deal with cervical spine pathologies. Anterior cervical discectomy and fusion (ACDF) has long been considered the gold standard for cervical disc disease.(89)
Posterior full endoscopic cervical foraminotomy and additional discectomy showed similar clinical outcomes to conventional ACDF(90). Cervical motion was preserved better in posterior full endoscopic cervical foraminotomy and discectomy(91). Patients who underwent endoscopic surgery had less blood loss, shorter operation times, and shorter hospital stays than those treated with conventional open foraminotomy(92). Cervical myelopathy which was earlier thought to be a contra-indication for endoscopic surgery is now routinely treated with UBE and large diameter full endoscopes.
Some studies have demonstrated that UBE laminectomy may be considered an excellent surgical alternative to treat cervical stenosis without the development of iatrogenic kyphosis(93). It represents an effective method with excellent neurological and radiological outcomes with less soft tissue invasion, which translates into dramatically less postoperative axial pain and maintained postoperative cervical lordosis(93). Wang et al concluded in their study that UBE and PE (percutaneous posterior endoscopic discectomy) were both safe and effective in the treatment of cervical spondylotic radiculopathy and were characterized by minimal trauma, no adverse impact on cervical stability and few complications(94). It is safe to say that cervical endoscopic surgeries have evolved and are no longer limited to dealing with just single level disc disease.
5.2. Endoscopic Aterior Cevical Dscectomy and Fusion
Ahn et al reported 5-year follow-up outcomes of anterior full endoscopic discectomy for soft disc herniation and showed comparable results with conventional ACDF(95). Recently Endoscopic ACDF has also been performed but no concrete data is currently available proving its efficacy.
Figure 5.
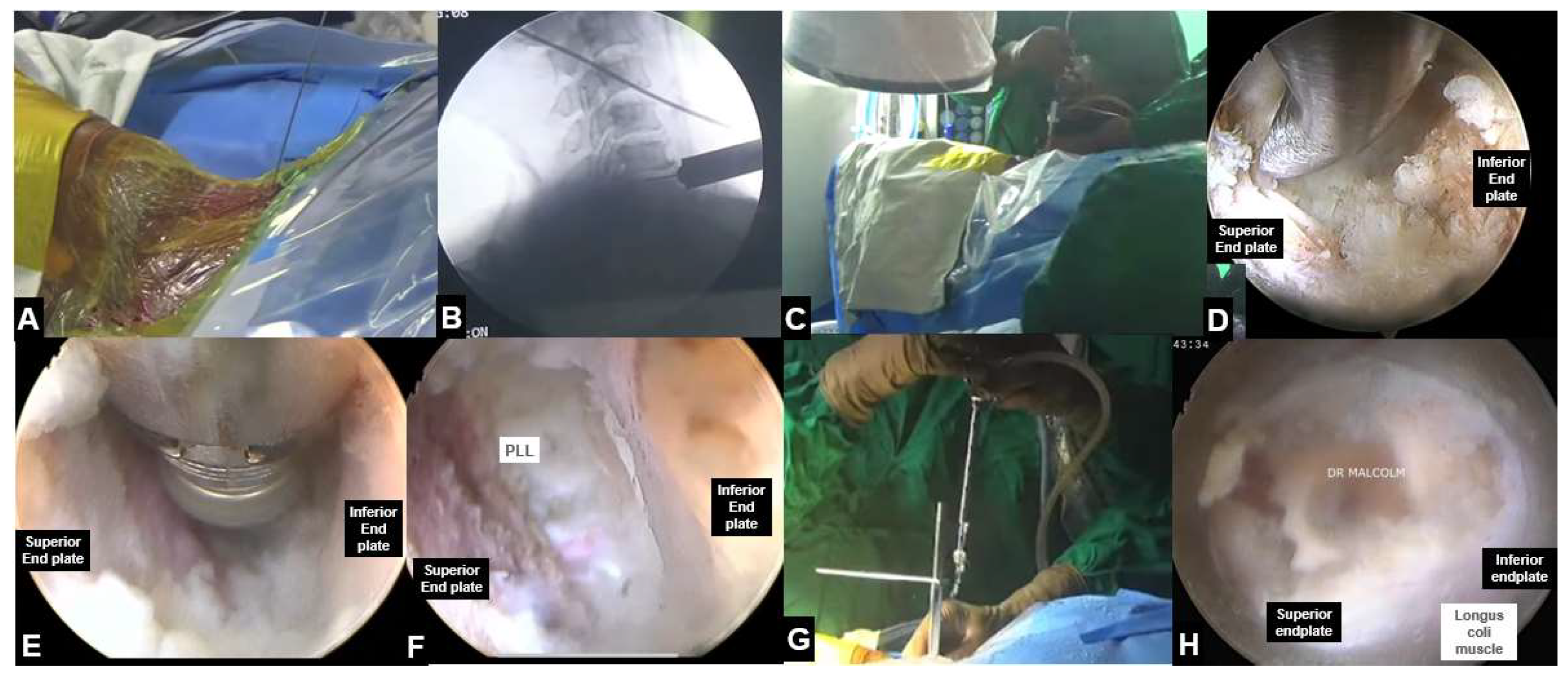
Endoscopic Aterior Cevical Dscectomy and Fusion, A: Intra-operative level marking . B&C: Docking over C6-C7 disc space D&E: Endoscopic view showing removal of disc and preparation of disc space. F: Endoscopic view showing complete removal of disc and adequate endplate preparation. G: Introduction of cage F: final position of cage.
Figure 5.
Endoscopic Aterior Cevical Dscectomy and Fusion, A: Intra-operative level marking . B&C: Docking over C6-C7 disc space D&E: Endoscopic view showing removal of disc and preparation of disc space. F: Endoscopic view showing complete removal of disc and adequate endplate preparation. G: Introduction of cage F: final position of cage.
5.3. UBE Cervical Foraminotomy and Laminectomy
Some studies have demonstrated that UBE laminectomy may be considered an excellent surgical alternative to treat cervical stenosis without the development of iatrogenic kyphosis(77). It represents an effective method with excellent neurological and radiological outcomes with less soft tissue invasion, which translates into dramatically less postoperative axial pain and maintained postoperative cervical lordosis(77). Wang et al concluded in their study that UBE and PE (percutaneous posterior endoscopic discectomy) were both safe and effective in the treatment of cervical spondylotic radiculopathy and were characterized by minimal trauma, no adverse impact on cervical stability and few complications(78). It is safe to say that cervical endoscopic surgeries have evolved and are no longer limited to dealing with just single level disc disease.
Figure 6.
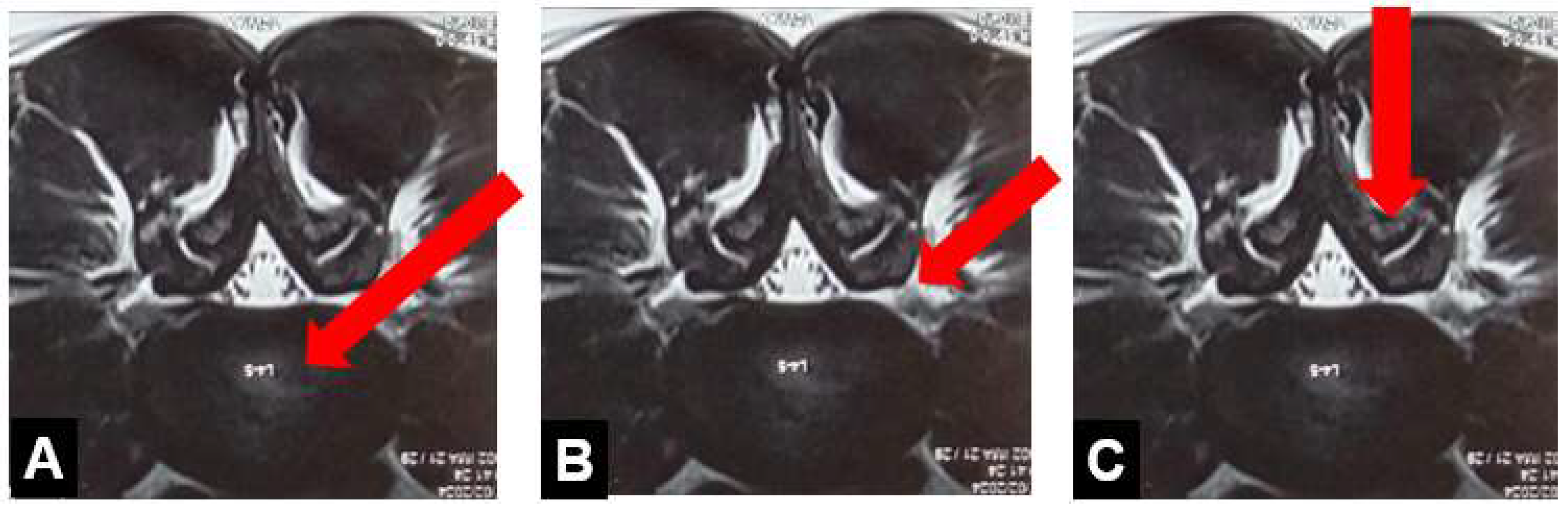
UBE Cervical foraminotomy and Laminectomy, A: Axial section through C5-C6 disc showing left sided disc osteophyte complex with impingement of left C6 nerve root. B: Intra-operative surgical view. C: Intra-operative fluoroscopic view showing targeting of V point i.e. junction of inferior articular process (IAP) with superior articular process (SAP) D. Endoscopic view showing identification of V point. E: Beginning of decompression by burring of IAP F,G: Resection of IAP and SAP with kerrison Ronguers H. Final image showing adequate decompression of the nerve root.
Figure 6.
UBE Cervical foraminotomy and Laminectomy, A: Axial section through C5-C6 disc showing left sided disc osteophyte complex with impingement of left C6 nerve root. B: Intra-operative surgical view. C: Intra-operative fluoroscopic view showing targeting of V point i.e. junction of inferior articular process (IAP) with superior articular process (SAP) D. Endoscopic view showing identification of V point. E: Beginning of decompression by burring of IAP F,G: Resection of IAP and SAP with kerrison Ronguers H. Final image showing adequate decompression of the nerve root.
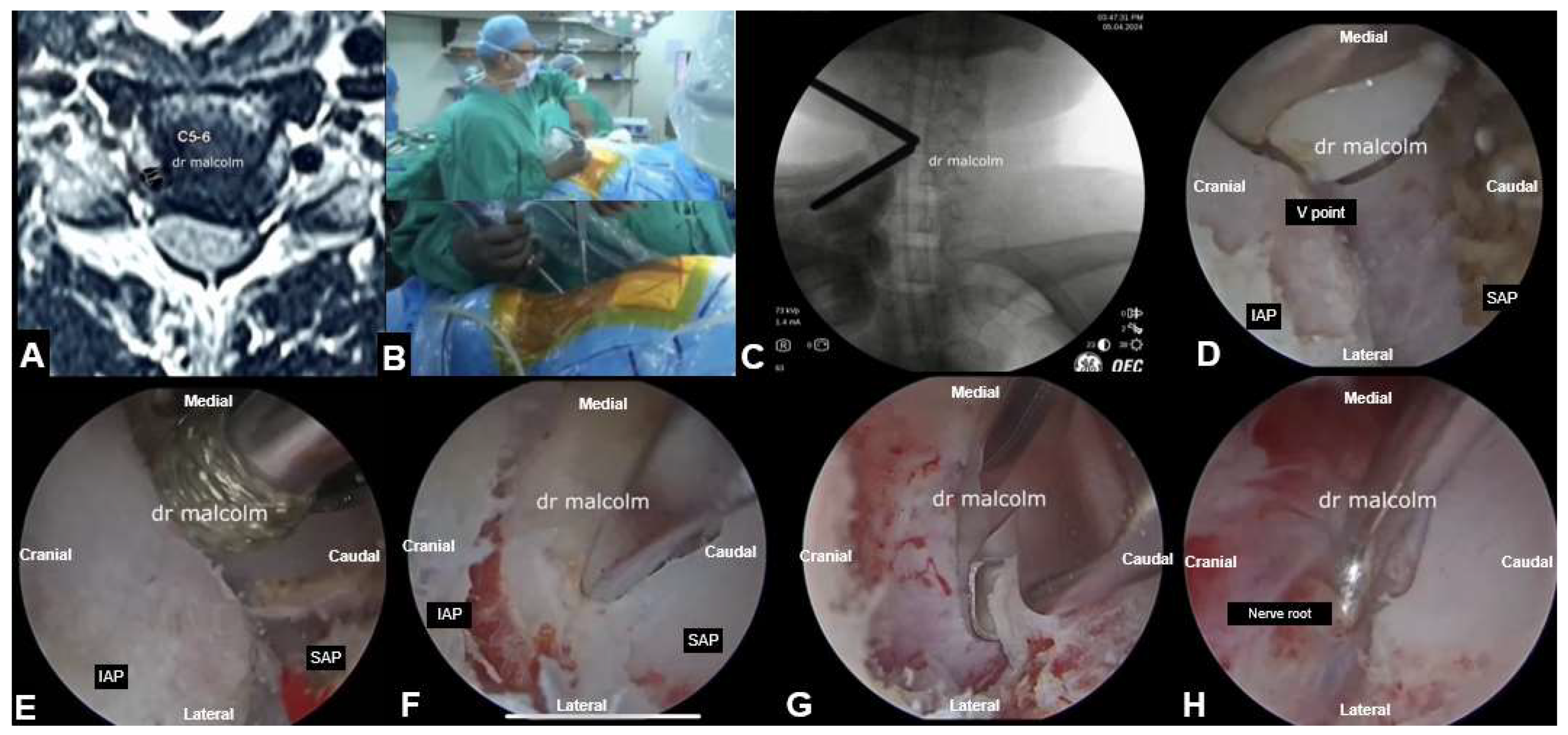
Table 4.
Clinical Rsult of Cervical Spine Endoscopy.
| Author | Sample | Approach | Follow up | Outcome | Complication |
|---|---|---|---|---|---|
| Fontanella (1999)[96] |
296 (273 anterior,23 posterior) |
Anterior, posterior | 12 months | 97% success at 1 year; average surgical time 25 min | Nil |
| Ahn (2005)[97] |
111 | Anterior | 49 months | Excellent/ good outcome in 80% | Persistent radicular pain in 1 patient 1 patient required ACDF |
| Lee (2007)[98] |
116 | Anterior | 36 months | 87 % had good outcomes | 2 patients ACDF 2 patients repeat endoscopy 1 patient - posterior fixation |
| Reutten (2009)[99] |
60 | Anterior | 24 months | 96% - good clinical outcome | 2 patients - progressive neck pain 2 patients - radicular pain 4 patients - ACDF |
| Yang (2014)[100] |
84 | Anterior 42 Posterior 42 |
18 months | Shorter operating time for anterior approach Shorter hospital stay for posterior approach |
1 Neurological deterioration 1 Hematoma - 1 Re-operation -1 post-operative headache - |
| Oertel (2016)[101] |
43 | Posterior | 6 months | 82% regained full arm strength; mean one level operation time 77 min | 1 haematoma, 1 triceps paresis |
6. Latest Advances
6.1. Navigation
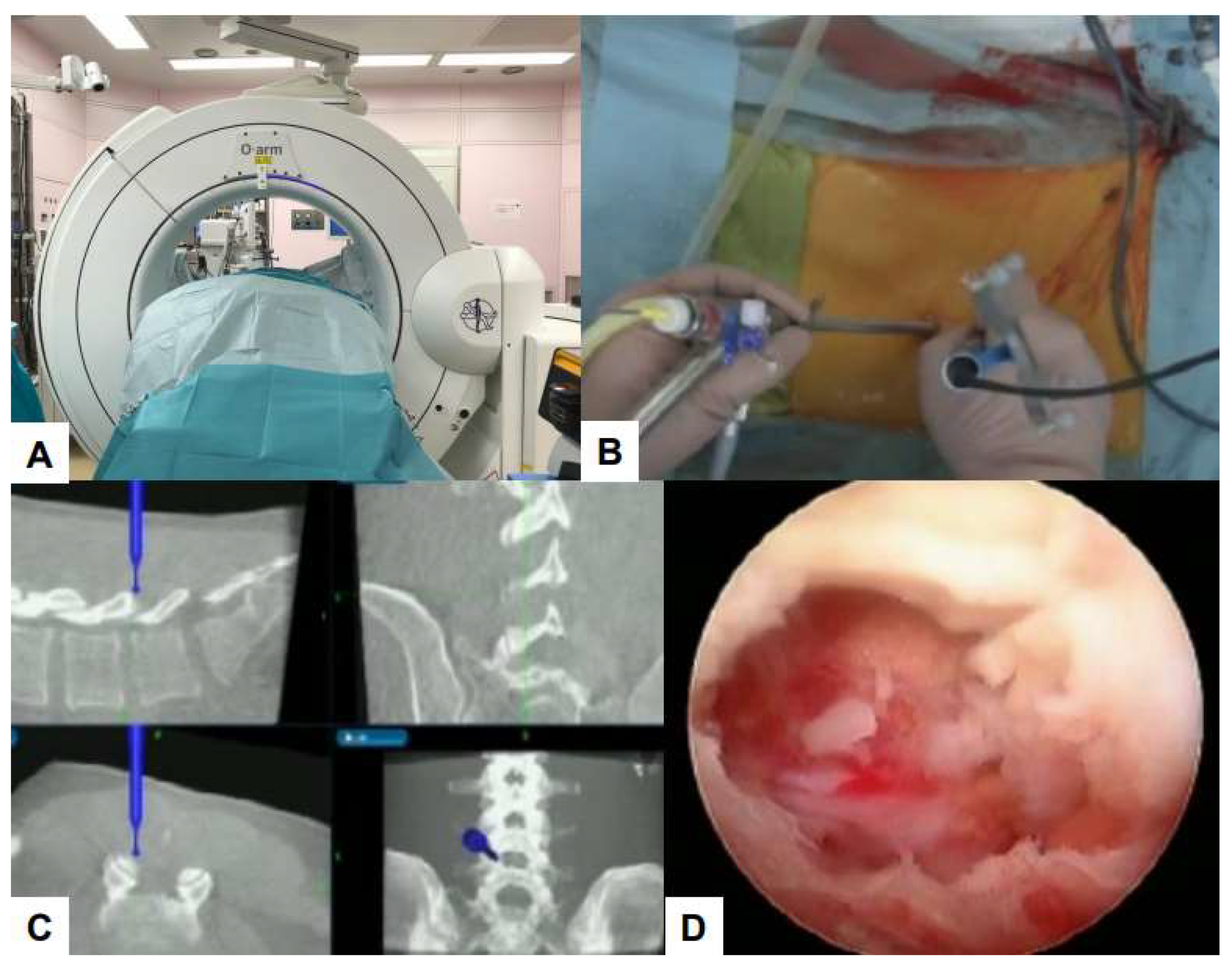
Debilitating consequences for patients can occur to damage to important structures such as nerves and blood vessels . Navigation systems that use real-time images improve surgical accuracy [103,104]Using O-arm, a high-quality computed tomography (CT) scan can be performed. Surgeons can perform intraoperative three-dimensional (3D) anatomical mapping in real time by integrating it with a real-time anatomical tracking tool[105]. Spine surgeons initially use navigation systems for percutaneous pedicle screw fixation, but nowadays, navigation systems can be used for various surgical procedures.
[106] Some examples of such applications in the field of endoscopic spine surgery are shown in the figures below.
Figure 7.
C arm free MED posterolateral, A: Intraoperative image, B: Navigated high speed burr, C: Navigation monitor, D: Preoperative MRI, A white arrow shows left L5/S1 lateral lumbar disc herniation.
Figure 7.
C arm free MED posterolateral, A: Intraoperative image, B: Navigated high speed burr, C: Navigation monitor, D: Preoperative MRI, A white arrow shows left L5/S1 lateral lumbar disc herniation.
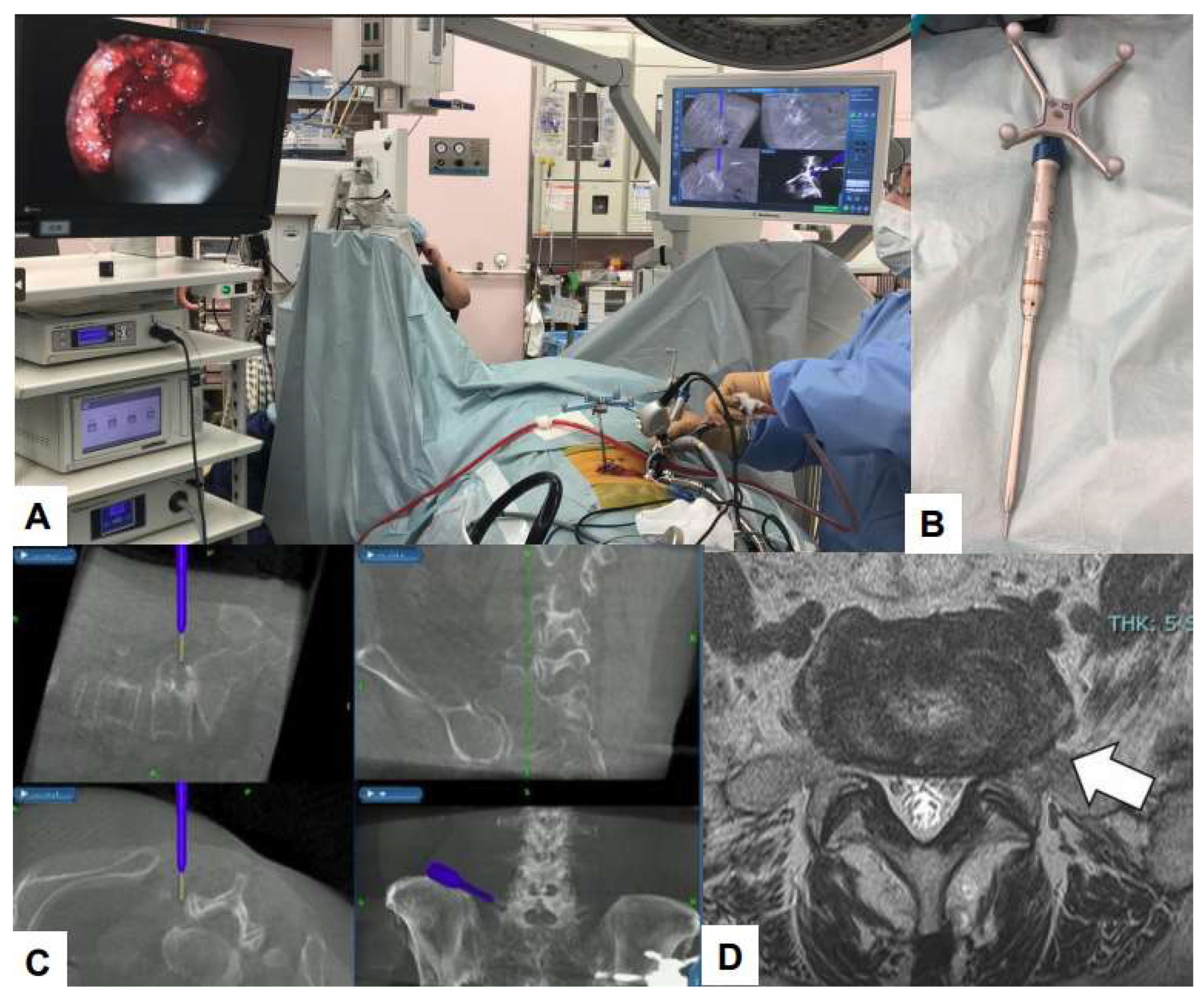
Figure 8.
C arm free cervical endoscopic keyhole foraminotomy, A: Endoscopy image, B: Neuromonitouring, C: Navigation monitor, D: MRI. A white arrow shows cervical disc herniation.
Figure 8.
C arm free cervical endoscopic keyhole foraminotomy, A: Endoscopy image, B: Neuromonitouring, C: Navigation monitor, D: MRI. A white arrow shows cervical disc herniation.
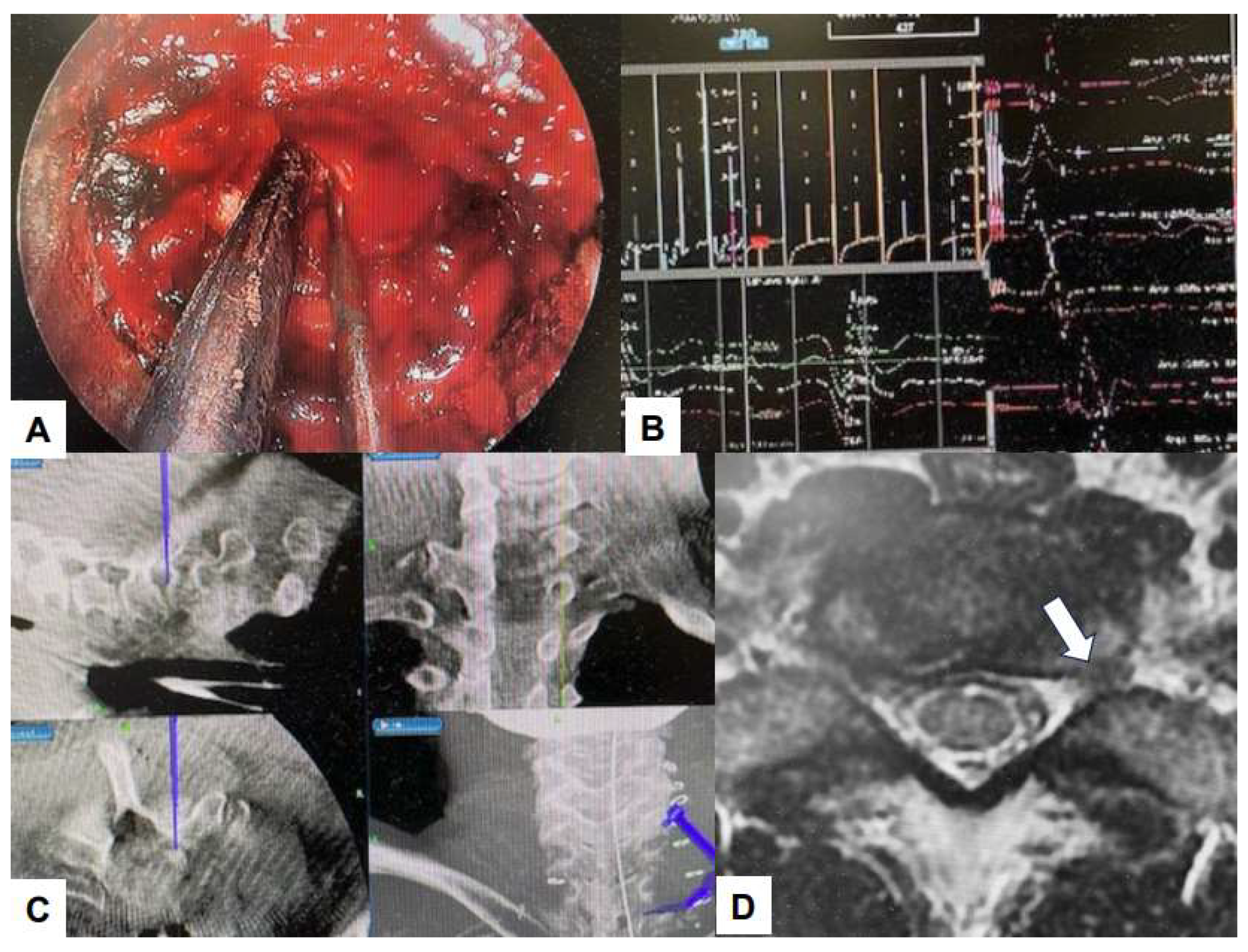
Figure 9.
C arm free lumbar transforaminal discectomy, A: Endoscopy image, B: Foraminoplasty with a navigated high speed burr, C: Navigated approach to the disc, D: Endoscopy image.
Figure 9.
C arm free lumbar transforaminal discectomy, A: Endoscopy image, B: Foraminoplasty with a navigated high speed burr, C: Navigated approach to the disc, D: Endoscopy image.
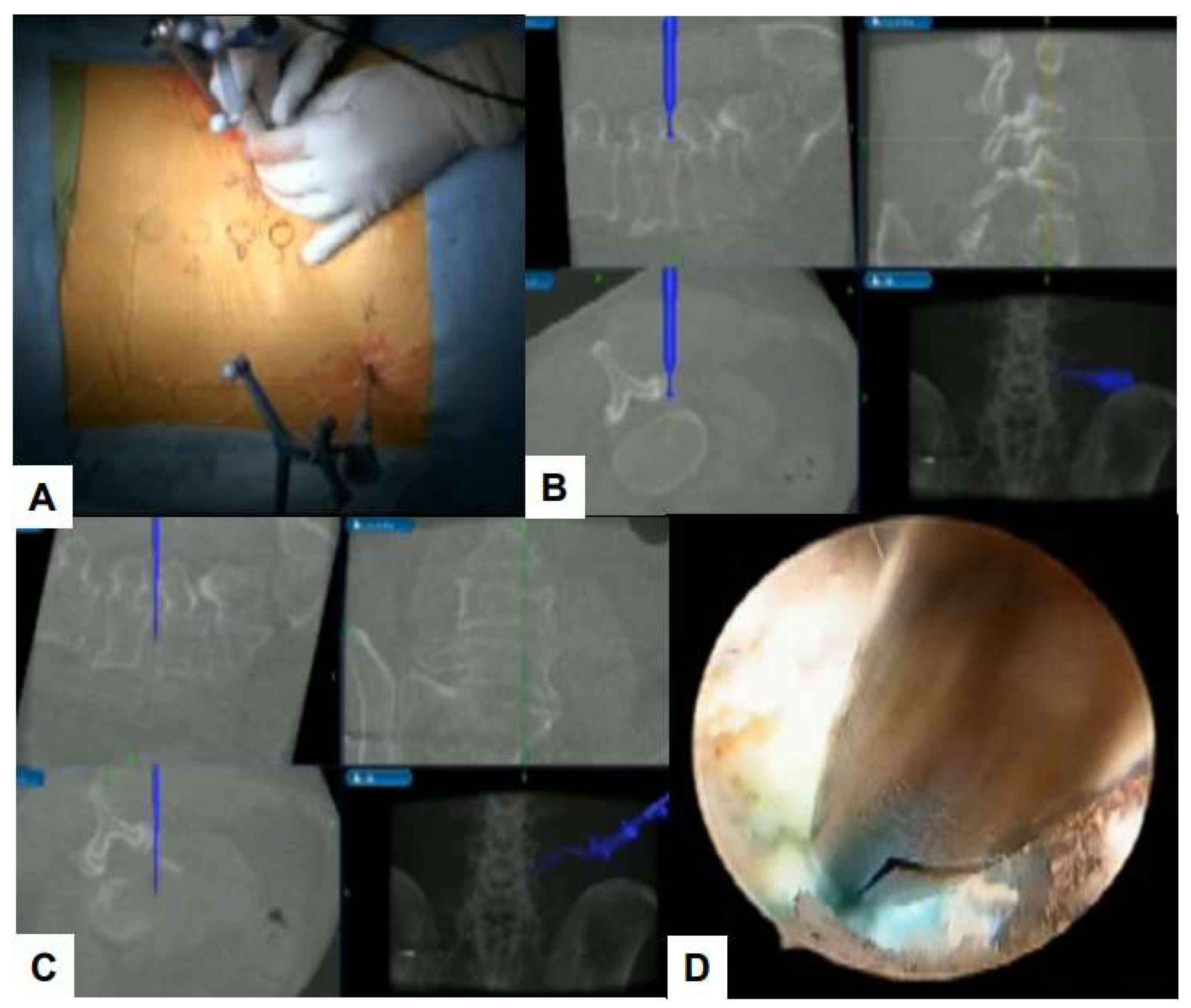
Figure 10.
C arm free UBE, A: O arm, B: Intraoperative image, C: Navigation monitor, D: endoscopy image.
Figure 10.
C arm free UBE, A: O arm, B: Intraoperative image, C: Navigation monitor, D: endoscopy image.
6.2. Ultraresolution and Three Dimensional Endoscopes
Resolution refers to the number of pixels a display holds. For instance, 2K (Full HD) has a resolution of 1920 × 1080 pixels, whereas 4K (Ultra HD) has a resolution of 3840 × 2160 pixels. The advantage of higher resolutions is their capacity to depict patient tissues with greater precision.(106) Also, the current 2 dimensional endoscopic spine systems lack depth perception causing unfamiliarity with surgical anatomy and may cause devastating complications . (107) Three-dimensional (3D) endoscopic equipment provides clear views of surgical anatomy, such as exposure of dura and nerve roots.(108) Using a 4K ultra-resolution endoscope, structures such as foraminal ligaments, which are difficult to observe with conventional microscopes, can be easily identified(109). Furthermore, accurate perception of the degree of stenosis and disc protrusion using 3D visualization could reduce surgical uncertainty, followed by better decompression of neural structures and better surgical outcomes(107).
6.3. Robot-Assisted Endoscopic Surgery
Robot-assisted spine surgery with systems such as Mazor X (Medtronic Inc., Dublin, Ireland) and ROSA (Medtech S.A., Montpellier, France) is being performed especially for pedicle screw placement with several advantages (110,111) This technology enables surgeons to enhance their manual dexterity with greater control and maneuverability through even a small portal, reducing physiological tremors(112). Robot-assisted spine surgery can provide accurate and safe guidance for discography in the initial steps of percutaneous endoscopic cervical discectomy(113) or PELD(114). Robot assistance was recently used to perform full endoscopic lumbar discectomy (115). Thus, robot assisted surgery may be used to perform other techniques of spine endoscopy in the near future.
7. Conclusion
The field of Endoscopic spine surgery has been developing rapidly over the last 40 years. Though initially limited to lumbar discectomies, Endoscopic spine surgeries have been used to treat cervical and thoracic stenosis as well. Significant advances have been made in the optics, resolution and instrumentation of endoscopic spine systems and hence the indications for this subset of minimally invasive spine surgeries has increased. However, the data regarding the applications to spinal conditions other than degenerative pathology such as spinal tumors, infection and trauma is lacking.
Author Contributions
Sharvari Gunjotikar – writing draft preparation; Malcolm Pestonji – writing and editing; Masato Tanaka – conceptualization; Tadashi Komatsubara writing and editing; Shashank J Ekade – data collection; Shashank J Ekade – writing and editing; Ahmed Heydar – data collection; Huynh Kim Hieu – data collection. All authors have read and agreed to the submitted version of the manuscript.
Funding
This research was supported by research funds to promote the hospital functions of Japan Organization of Occupational Health and Safe.
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki and approved by the institutional review boards at Okayama Rosai Hospital (approval No. 485, April 8th, 2024).
References
- Fehlings, M.G.; Tetreault, L.; Nater, A.; Choma, T.; Harrop, J.; Mroz, T.; Santaguida, C.; Smith, J.S. The aging of the global population: the changing epidemiology of disease and spinal disorders. Neurosurgery 2015, 77, S1–S5. [Google Scholar] [CrossRef]
- Hirai, T.; Uehara, M.; Miyagi, M.; Takahashi, S.; Nakashima, H. Current advances in spinal diseases of the elderly: introduction to the special issue. Journal of Clinical Medicine 2021, 10, 3298. [Google Scholar] [CrossRef]
- Campbell, G.; Yadla, S.; Nasser, R.; Malone, J.; Maltenfort, M.G.; Ratliff, J.K. Patient comorbidity score predicting the incidence of perioperative complications: assessing the impact of comorbidities on complications in spine surgery. Journal of Neurosurgery: Spine 2012, 16, 37–43. [Google Scholar] [CrossRef]
- Katz, J.N.; Lipson, S.J.; Larson, M.G.; McInnes, J.M.; Fossel, A.H.; Liang, M.H. The outcome of decompressive laminectomy for degenerative lumbar stenosis. The Journal of Bone & Joint Surgery 1991, 73, 809–816. [Google Scholar]
- Sharif, S.; Shaikh, Y.; Peev, N. Minimally invasive spinal surgery: how to keep out of trouble. World Neurosurgery 2018, 119, 517–526. [Google Scholar] [CrossRef]
- Kim, M.; Kim, H.S.; Oh, S.W.; Adsul, N.M.; Singh, R.; Kashlan, O.N.; Noh, J.H.; Jang, I.T.; Oh, S.H. Evolution of spinal endoscopic surgery. Neurospine 2019, 16, 6. [Google Scholar] [CrossRef]
- Kim, H.S.; Wu, H.; Jang, I.T. Current and future of endoscopic spine surgery: what are the common procedures we have now and what lies ahead? World Neurosurgery 2020, 140, 642–653. [Google Scholar] [CrossRef]
- Fu, T.S.; Wang, Y.C.; Lin, T.Y.; Chang, C.W.; Wong, C.B.; Su, J.Y. Comparison of percutaneous endoscopic surgery and traditional anterior open surgery for treating lumbar infectious spondylitis. Journal of Clinical Medicine 2019, 8, 1356. [Google Scholar] [CrossRef]
- Şentürk, S.; Ünsal, Ü.Ü. Percutaneous full-endoscopic removal of lumbar intradural extramedullary tumor via translaminar approach. World Neurosurgery 2019, 125, 146–149. [Google Scholar] [CrossRef]
- Telfeian, A.E.; Veeravagu, A.; Oyelese, A.A.; Gokaslan, Z.L. A brief history of endoscopic spine surgery. Neurosurgical focus 2016, 40, E2. [Google Scholar] [CrossRef]
- HIJIKATA, S. Percutaneous Nucleotomy: A New Concept Technique and 12 Years' Experience. Clinical Orthopaedics and Related Research (1976-2007) 1989, 238, 9–23. [Google Scholar]
- Kambin, P.; Zhou, L. ▪ History and Current Status of Percutaneous Arthroscopic Disc Surgery. Spine 1996, 21, 57S–61S. [Google Scholar] [CrossRef]
- Kambin, P. Arthroscopic microdiskectomy. The Mount Sinai journal of medicine, New York 1991, 58, 159–164. [Google Scholar]
- KT, F. Microendoscopic discectomy. Techniques in neurosurgery 1997, 3, 301–307. [Google Scholar]
- Foley, K.T.; Smith, M.M.; Rampersaud, Y.R. Microendoscopic approach to far-lateral lumbar disc herniation. Neurosurgical focus 1999, 7, E7. [Google Scholar] [CrossRef]
- Destandau, J. A special device for endoscopic surgery of lumbar disc herniation. Neurological Research 1999, 21, 39–42. [Google Scholar] [CrossRef]
- Kaushal, M.; Kaushal, M. Destandau’s Approach to the Cervical and Thoracic Spine. Journal of Minimally Invasive Spine Surgery and Technique 2023, 8, 89–96. [Google Scholar] [CrossRef]
- Yeung, A.T. Minimally Invasive Disc Surgery with the Yeung Endoscopic Spine System (YESS). Surgical technology international 1999, 8, 267–277. [Google Scholar]
- Yeung, A.T.; Yeung, C.A. Advances in endoscopic disc and spine surgery: foraminal approach. Surg Technol Int 2003, 11, 255–263. [Google Scholar]
- Gore, S.; Yeung, A. The “inside out” transforaminal technique to treat lumbar spinal pain in an awake and aware patient under local anesthesia: results and a review of the literature. International journal of spine surgery 2014, 8. [Google Scholar] [CrossRef]
- Schubert, M.; Hoogland, T. Endoscopic transforaminal nucleotomy with foraminoplasty for lumbar disk herniation. Oper Orthop Traumatol. 2005, 17, 641–661. [Google Scholar] [CrossRef] [PubMed]
- Mirkovic, S.R.; Schwartz, D.G.; Glazier, K.D. Anatomic considerations in lumbar posterolateral percutaneous procedures. Spine 1995, 20, 1965–1971. [Google Scholar] [CrossRef]
- Reulen, H.J.; Müller, A.; Ebeling, U. Microsurgical anatomy of the lateral approach to extraforaminal lumbar disc herniations. Neurosurgery 1996, 39, 345–351. [Google Scholar] [CrossRef]
- Choi, G.; Lee, S.H.; Raiturker, P.; Lee, S.; Chae, Y.S. Percutaneous endoscopic interlaminar discectomy for intracanalicular disc herniations at L5–S1 using a rigid working channel endoscope. Operative Neurosurgery 2006, 58, ONS-59. [Google Scholar] [CrossRef]
- Heo, D.H.; Lee, D.C.; Park, C.K. Comparative analysis of three types of minimally invasive decompressive surgery for lumbar central stenosis: biportal endoscopy, uniportal endoscopy, and microsurgery. Neurosurgical focus 2019, 46, E9. [Google Scholar] [CrossRef]
- Eum, J.H.; Heo, D.H.; Son, S.K.; Park, C.K. Percutaneous biportal endoscopic decompression for lumbar spinal stenosis: a technical note and preliminary clinical results. Journal of neurosurgery: Spine 2016, 24, 602–607. [Google Scholar]
- Perez-Cruet, M.J.; Foley, K.T.; Isaacs, R.E.; Rice-Wyllie, L.; Wellington, R.; Smith, M.M.; Fessler, R.G. Microendoscopic lumbar discectomy. Neurosurgery 2002, 51, S2–S129. [Google Scholar] [CrossRef]
- Issacs, R.E.; Podichetty, V.; Fessler, R.G. Microendoscopic disccetomy for recurrent disc herniations. Neurosurg Focus 2003, 15, 11. [Google Scholar]
- Jhala, A.; Mistry, M. Endoscopic lumbar disccetomy; Experience of first 100 cases. Indian J orthop 2010, 44, 184–190. [Google Scholar] [CrossRef]
- Khoo, L.T.; Fessler, R.G. Microendoscopic decompressive laminotomy for the treatment of lumbar stenosis. Neurosurgery 2002, 51, S2–S146. [Google Scholar] [CrossRef]
- Ikuta, K.; Arima, J.; Tanaka, T.; Oga, M.; Nakano, S.; Sasaki, K.; Goshi, K.; Yo, M.; Fukagawa, S. Short-term results of microendo- scopic posterior decompression for lumbar spinal stenosis. J. Neurosurg. Spine 2005, 2, 624–633. [Google Scholar] [CrossRef]
- Wu, X.; Zhuang, S.; Mao, Z.; Chen, H. Microendoscopic discectomy for lumbar disc herniation: surgical technique and outcome in 873 consecutive cases. Spine 2006, 31, 2689–2694. [Google Scholar] [CrossRef]
- Fukushi, R.; Yoshimoto, M.; Iesato, N.; Terashima, Y.; Takebayashi, T.; Yamashita, T.; Fukushi, R. Short-term results of microendoscopic muscle-preserving interlaminar decompression versus spinal process splitting laminectomy. J. Neurol. Surg. Part A Cent. Eur. Neurosurg. 2018, 79, 511–517. [Google Scholar]
- Wu, B.; Xiong, C.; Tan, L.; Zhao, D.; Xu, F.; Kang, H. Clinical outcomes of MED and iLESSYS® delta for the treatment of lumbar central spinal stenosis and lateral recess stenosis: A comparison study. Exp. Ther. Med. 2020, 20, 252. [Google Scholar] [CrossRef]
- Iwai, H.; Inanami, H.; Koga, H. Comparative study between full-endoscopic laminectomy and microendoscopic laminectomy for the treatment of lumbar spinal canal stenosis. J. Spine Surg. 2020, 6, E3–E11. [Google Scholar] [CrossRef]
- Ito Shibayama, M.; Nakamura, S.; Yamada, M.; Kawai, M.; Takeuchi, M.; Yoshimatsu, H.; Kuraishi, K.; Hoshi, N.; Miura, Y.; et al. Clinical comparison of unilateral biportal endoscopic laminectomy versus microendoscopic laminectomy for single-level laminectomy: A single-center, retrospective analysis. World Neurosurg. 2021, 148, e581–e588. [Google Scholar]
- Dey, P.C.; Nanda, N. Functional outcome after endoscopic lumbar discectomy by destandau’s technique: a prospective study of 614 patients. Asian Spine Journal 2019, 13, 786. [Google Scholar] [CrossRef]
- KimHSWu, P.H.; Jang, I.T. Current and future of endoscopic spine surgery: what are the common procedures we have now and what lies ahead? World Neurosurgery 2020, 140, 642–653. [Google Scholar]
- Kim, H.S.; Paudel, B.; Jang, J.S.; Lee, K.; Oh, S.H.; Jang, I.T. Percutaneous endoscopic lumbar discectomy for all types of lumbar disc herniations (LDH) including severely difficult and extremely difficult LDH cases. Pain physician 2018, 21, E401. [Google Scholar]
- Knight, M.T.; Jago, I.; Norris, C.; Midwinter, L.; Boynes, C. Transforaminal endoscopic lumbar decompression & foraminoplasty: a 10 year prospective survivability outcome study of the treatment of foraminal stenosis and failed back surgery. International journal of spine surgery 2014, 8. [Google Scholar] [CrossRef]
- Kim HS, Yudoyono F, Paudel B, et al. Suprapedicular circumferential opening technique of percutaneous endoscopic transforaminal lumbar discectomy for high grade inferiorly migrated lumbar disc herniation. Biomed Res Int.
- Lewandrowski, K.U. Incidence, management, and cost of complications after transforaminal endoscopic decompression surgery for lumbar foraminal and lateral recess stenosis: a value proposition for outpatient ambulatory surgery. International Journal of SpineSurgery 2019, 13, 53–67. [Google Scholar] [CrossRef]
- Osman, S.G.; Nibu, K.; Panjabi, M.M.; et al. Transforaminal and posterior decompressions of the lumbar spine. A comparative study of stability and intervertebral foramen area. Spine (Phila Pa 1976) 1997, 22, 1690–1695. [Google Scholar] [CrossRef]
- Sairyo, K.; Higashino, K.; Yamashita, K.; et al. A new concept of transforaminal ventral facetectomy including simultaneous decompression of foraminal and lateral recess stenosis: technical considerations in a fresh cadaver model and a literature review. J Med Invest. 2017, 64, 1–6. [Google Scholar] [CrossRef]
- Yagi, K.; Kishima, K.; Tezuka, F.; et al. Advantages of revision transforaminal full-endoscopic spine surgery in patients who have previously undergone posterior spine surgery. J Neurol Surg A Cent Eur Neurosurg 2022. [Google Scholar] [CrossRef] [PubMed]
- Lewandrowski, K.U. Endoscopic transforaminal and lateral recess decompression after previous spinal surgery. Int J Spine Surg. 2018, 12, 98–111. [Google Scholar] [CrossRef]
- Jadczak, C.N.; Vanjani, N.N.; Pawlowski, H.; Cha, E.D.; Lynch, C.P.; Prabhu, M.C.; Hartman, T.J.; Nie, J.W.; MacGregor, K.R.; Zheng, E.; Oyetayo, O.O. The Current Status of Awake Endoscopic Surgery: A Systematic Review and Meta-Analysis. World Neurosurgery, 2023. [Google Scholar]
- Telfeian AE, Sastry R, Oyelese A, et al. Awake, transforaminal endoscopic lumbar spine surgery in octogenarians: case series. Pain Physician. 2022, 25, E255–62.
- Song, S.K.; Son, S.; Choi, S.W.; Kim, H.K. Comparison of the outcomes of percutaneous endoscopic interlaminar lumbar discectomy and open lumbar microdiscectomy at the L5-S1 level. Pain physician 2021, 24, E467. [Google Scholar]
- Ruetten, S.; Komp, M.; Merk, H.; Godolias, G. Full-endoscopic interlaminar and transforaminal lumbar discectomy versus conventional microsurgical technique: a prospective, randomized, controlled study. 2008. [Google Scholar]
- Chen, K.T.; Choi, K.C.; Shim, H.K.; Lee, D.C.; Kim, J.S. Full-endoscopic versus microscopic unilateral laminotomy for bilateral decompression of lumbar spinal stenosis at L4–L5: comparative study. International Orthopaedics 2022, 46, 2887–2895. [Google Scholar] [CrossRef]
- Lee, C.H.; Choi, M.; Choi, I.; Kim, C.H.; Kim, H.S.; Sohn, M.J. Efficacy and safety of full-endoscopic decompression via interlaminar approach for central or lateral recess spinal stenosis of the lumbar spine: a meta-analysis. Spine 2018, 43, 1756–1764. [Google Scholar] [CrossRef]
- McGrath, L.B.; White-Dzuro, G.A.; Hofstetter, C.P. Comparison of clinical outcomes following minimally invasive or lumbar endoscopic unilateral laminotomy for bilateral decompression. Journal of Neurosurgery: Spine 2019, 30, 491–499. [Google Scholar] [CrossRef]
- Heo, D.H.; Son, S.K.; Eum, J.H.; Park, C.K. Fully endoscopic lumbar interbody fusion using a percutaneous unilateral biportal endoscopic technique: technical note and preliminary clinical results. Neurosurg Focus. 2017, 43, E8. [Google Scholar] [CrossRef]
- Ahn, J.S.; Lee, H.J.; Choi, D.J.; Lee, K.Y.; Hwang, S.J. Extraforaminal approach of biportal endoscopic spinal surgery: a new endoscopic technique for transforaminal decompression and discectomy. J Neurosurg Spine. 2018, 28, 492–498. [Google Scholar] [CrossRef]
- Heo, D.H.; Quillo-Olvera, J.; Park, C.K. Can percutaneous biportal endoscopic surgery achieve enough canal decompression for degenerative lumbar stenosis? prospective case-control study. World Neurosurg. 2018, 120, e684–9. [Google Scholar] [CrossRef]
- Pao, J.L. A review of unilateral biportal endoscopic decompression for degenerative lumbar canal stenosis. Int J Spine Surg. 2021, 15, S65–S71. [Google Scholar] [CrossRef]
- Li, Y.S.; Chen, C.M.; Hsu, C.J.; Yao, Z.K. Complications of unilateral biportal endoscopic lumbar discectomy: a systematic review. World Neurosurgery 2022, 168, 359–368. [Google Scholar] [CrossRef]
- Kwon, O.; Yoo, S.J.; Park, J.Y. Comparison of unilateral biportal endoscopic discectomy with other surgical technics: a systemic review of indications and outcomes of unilateral biportal endoscopic discectomy from the current literature. World Neurosurgery 2022, 168, 349–358. [Google Scholar] [CrossRef]
- Hua, W.; Liao, Z.; Chen, C.; Feng, X.; Ke, W.; Wang, B.; Li, S.; Wang, K.; Zeng, X.; Wu, X.; Zhang, Y. Clinical outcomes of uniportal and biportal lumbar endoscopic unilateral laminotomy for bilateral decompression in patients with lumbar spinal stenosis: a retrospective pair-matched case-control study. World Neurosurgery 2022, 161, e134–e145. [Google Scholar] [CrossRef]
- Heo, D.H.; Lee, D.C.; Park, C.K. Comparative analysis of three types of minimally invasive decompressive surgery for lumbar central stenosis: biportal endoscopy, uniportal endoscopy, and microsurgery. Neurosurg Focus. 2019, 46, E9. [Google Scholar] [CrossRef]
- Kang, M.S.; Park, H.J.; You, K.H.; Choi, D.J.; Park, C.W.; Chung, H.J. Comparison of Primary Versus Revision Lumbar Discectomy Using a Biportal Endoscopic Technique. Global Spine Journal 2023, 13, 1918–1925. [Google Scholar] [CrossRef]
- Choi, D.J.; Choi, C.M.; Jung, J.T.; Lee, S.J.; Kim, Y.S. Learning curve associated with complications in biportal endoscopic spinal surgery: challenges and strategies. Asian Spine J. 2016, 10, 624–629. [Google Scholar] [CrossRef]
- Kim, S.K.; Kang, S.S.; Hong, Y.H.; Park, S.W.; Lee, S.C. Clinical comparison of unilateral biportal endoscopic technique versus open microdiscectomy for single-level lumbar discectomy: a multicenter, retrospective analysis. J Orthop Surg Res. 2018, 13, 22. [Google Scholar] [CrossRef]
- Kim, J.E.; Choi, D.J. Unilateral biportal endoscopic decompression by 30 endoscopy in lumbar spinal stenosis: technical note and preliminary report. J Orthop. 2018, 15, 366–371. [Google Scholar] [CrossRef]
- Akbary, K.; Kim, J.S.; Park, C.W.; Jun, S.G.; Hwang, J.H. Biportal endoscopic decompression of exiting and traversing nerve roots through a single interlaminar window by a contralateral approach: technical feasibilities and morphometric changes of the lumbar canal and foramen. World Neurosurg. 2018, 117, 153–161. [Google Scholar] [CrossRef]
- Pao, J.L.; Lin, S.M.; Chen, W.C.; Chang, C.H. Unilateral biportal endoscopic decompression for degenerative lumbar canal stenosis. Journal of Spine Surgery 2020, 6, 438. [Google Scholar] [CrossRef]
- Wang, J.C.; Li, Z.Z.; Cao, Z.; Zhu, J.L.; Zhao, H.L.; Hou, S.X. Modified unilateral biportal endoscopic lumbar discectomy results in improved clinical outcomes. World Neurosurgery 2023, 169, e235–e244. [Google Scholar] [CrossRef]
- Morimoto, M.; Sairyo, K. Full-endoscopic trans-Kambin’s triangle lumbar interbody fusion (Fullendo-KLIF). Transforaminal Full-Endoscopic Lumbar Surgery Under the Local Anesthesia: State of the Art 2021, 87–95. [Google Scholar]
- Pholprajug, P.; Kotheeranurak, V.; Liu, Y.; Kim, J.S. The endoscopic lumbar interbody fusion: a narrative review, and future perspective. Neurospine 2023, 20, 1224. [Google Scholar] [CrossRef]
- Li, Y.; Dai, Y.; Wang, B.; Li, L.; Li, P.; Xu, J.; Jiang, B.; Lü, G. Full-endoscopic posterior lumbar interbody fusion via an interlaminar approach versus minimally invasive transforaminal lumbar interbody fusion: a preliminary retrospective study. World neurosurgery 2020, 144, e475–e482. [Google Scholar] [CrossRef]
- Han, H.; Song, Y.; Li, Y.; Zhou, H.; Fu, Y.; Li, J. Short-term clinical efficacy and safety of unilateral biportal endoscopic transforaminal lumbar interbody fusion versus minimally invasive transforaminal lumbar interbody fusion in the treatment of lumbar degenerative diseases: a systematic review and meta-analysis. Journal of Orthopaedic Surgery and Research 2023, 18, 656. [Google Scholar]
- Simpson, A.K.; Lightsey, H.M., 4th; Xiong, G.X.; Crawford, A.M.; Minamide, A.; Schoenfeld, A.J. Spinal endoscopy: evidence, techniques, global trends, and future projections. Spine J. 2022, 22, 64. [Google Scholar] [CrossRef]
- Hofstetter, C.P.; Ahn, Y.; Choi, G.; et al. AO Spine consensus paper on nomenclature for working channel endoscopic spinal procedures. Global Spine J 2020, 10, 111S–121. [Google Scholar] [CrossRef]
- Gibson, R. D. S.; Wagner, R.; Gibson, J. N. A. Full endoscopic surgery for thoracic pathology: an assessment of supportive evidence. In EFORT Open Reviews; Retrieved Apr 10, 2024, from; 2021; Volume 6, pp. 50–60. [Google Scholar]
- Cho, J.Y.; Lee, S.H.; Jang, S.H.; et al. Oblique paraspinal approach for thoracic disc herniations using tubular retractor with robotic holder: a technical note. Eur Spine J 2012, 21, 2620–5. [Google Scholar] [CrossRef]
- Bae, J.; Chachan, S.; Shin, S.-H.; Lee, S.-H. Percutaneous Endoscopic Thoracic Discectomy in the Upper and Midthoracic Spine: A Technical Note. Neurospine 2019, 16, 148–153. [Google Scholar] [CrossRef]
- Lin, C.-Y.; Chang, C.-C.; Chen, Y.-J.; et al. New strategy for minimally invasive endoscopic surgery to treat infectious spondylodiscitis in the thoracolumbar spine. Pain Physician 2019, 22, 281–293. [Google Scholar]
- Yang, J.-S.; Chu, L.; Deng, R.; et al. Treatment of single level thoracic tuberculosis by percutaneous endoscopic debridement and allograft via the transforaminal approach combined with percutaneous pedicle screw fixation: a multicenter study with a median follow-up of 36 months. World Neurosurg 2019, 122, e1472–e1481. [Google Scholar] [CrossRef]
- Eichholz, K.M.; O&, *!!! REPLACE !!!*; #39, *!!! REPLACE !!!*; Toole, J.E.; Fessler, R.G. Thoracic microendoscopic discectomy. Neurosurg Clin N Am. 2006, 17, 441–6. [Google Scholar] [CrossRef] [PubMed]
- Perez-Cruet, M.J.; Kim, B.S.; Sandhu, F.; Samartzis, D.; Fessler, R.G. Thoracic microendoscopic discectomy. J Neurosurg Spine. 2004, 1, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Isaacs, R.E.; Podichetty, V.K.; Sandhu, F.A.; Santiago, P.; Spears, J.D.; Aaronson, O.; Kelly, K.; Hrubes, M.; Fessler, R.G. Thoracic microendoscopic discectomy: a human cadaver study. Spine (Phila Pa 1976). 2005, 30, 1226–31. [Google Scholar] [CrossRef] [PubMed]
- Jia, L.S.; Chen, X.S.; Zhou, S.Y.; Shao, J.; Zhu, W. En Bloc Resection of Lamina and Ossified Ligamentum Flavum in the Treatment of Thoracic Ossification of the Ligamentum Flavum. Neurosurgery 2010, 66, 1181–1186. [Google Scholar] [CrossRef]
- Kang, M.S.; Chung, H.J.; You, K.H.; et al. How i do it: biportal endoscopic thoracic decompression for ossification of the ligamentum flavum. Acta Neurochir 2022, 164, 43–47. [Google Scholar] [CrossRef]
- Deng, Y.; Yang, M.; Xia, C.; et al. Unilateral biportal endoscopic decompression for symptomatic thoracic ossification of the ligamentum flavum: a case control study. International Orthopaedics (SICOT) 2022, 46, 2071–2080. [Google Scholar] [CrossRef]
- Man-Kyu Park, Daewon Park, Sang-Kyu Son, Journal of Minimally Invasive Spine Surgery and Technique 8 (1), 82-88, 202.
- Ahn, Y. The current state of cervical endoscopic spine surgery: an updated literature review and technical considerations. Expert Review of Medical Devices 2020, 17, 1285–1292. [Google Scholar] [CrossRef]
- Gao, F.; Mao, T.; Sun, W.; Guo, W.; Wang, Y.; Li, Z.; Abhinav, P. An updated meta- analysis comparing artificial cervical disc arthroplasty (CDA) versus anterior cervical discectomy and fusion (ACDF) for the treatment of cervical degenerative disc disease (CDDD). Spine 2015, 40, 1816–1823. [Google Scholar] [CrossRef]
- Ruetten, S.; Komp, M.; Merk, H.; et al. Full-endoscopic cervical posterior foraminotomy for the operation of lateral disc herniations using 5.9-mm endoscopes: a prospective, randomized, controlled study. Spine (Phila Pa 1976) 2008, 33, 940–948. [Google Scholar] [CrossRef]
- Ma, W.; Peng, Y.; Zhang, S.; et al. Comparison of percutaneous endoscopic cervical keyhole foraminotomy versus microscopic anterior cervical discectomy and fusion for single level unilateral cervical radiculopathy. Int J Gen Med. 2022, 15, 6897–6907. [Google Scholar] [CrossRef]
- Clark, J.G.; Abdullah, K.G.; Steinmetz, M.P.; et al. Minimally invasive versus open cervical foraminotomy: a systematic review. Global Spine J. 2011, 1, 9–14. [Google Scholar] [CrossRef]
- Wang, D.; Xu, J.; Zhu, C.; Zhang, W.; Pan, H. Comparison of Outcomes between Unilateral Biportal Endoscopic and Percutaneous Posterior Endoscopic Cervical Keyhole Surgeries. Medicin(Kaunas). 2023, 59, 437. [Google Scholar] [CrossRef]
- Ahn Y, Keum HJ, Shin SH. Percutaneous endoscopic cervical discectomy versus anterior cervical discectomy and fusion: a comparative cohort study with a five-year follow-up.
- Zhu, C.; Zhou, X.; Ge, G.; Wang, C.; Zhuang, X.; Cheng, W.; Wang, D.; Zhu, H.; Pan, H.; Zhang, W. Unilateral Biportal Endoscopic Laminectomy for Treating Cervical Stenosis: A Technical Note and Preliminary Results. Medicina (Kaunas). 2023, 59, 305. [Google Scholar] [CrossRef]
- Ahn Y, Keum HJ, Shin SH. Percutaneous endoscopic cervical discectomy versus anterior cervical discectomy and fusion: a comparative cohort study with a five-year follow-up.
- Fontanella, A. Endoscopic microsurgery in herniated cervical discs. Neurol Res 1999, 21, 31–38. [Google Scholar] [CrossRef]
- Ahn, Y.; Lee, S.H.; Lee, S.C.; et al. Factors predicting excellent outcome of percutaneous cervical discectomy: analysis of 111 consecutive cases. Neuroradiol 2004, 46, 378–384. [Google Scholar] [CrossRef]
- Lee, S.H.; Lee, J.H.; Choi, W.C.; et al. Anterior minimally invasive approaches for the cervical spine. Orthop Clin N Am 2007, 38, 327–337. [Google Scholar] [CrossRef]
- Ruetten S, Komp M, Merk H, et al. Full-endoscopic anterior decompression versus conventional anterior decompression and fusion in cervical disc herniations. Int Orth 2009, 33, 1677–1682. [CrossRef]
- Yang JS, Chu L, Chen L, et al. Anterior or posterior approach of full-endoscopic cervical discectomy for cervical intervertebral disc herniation? A comparative cohort study. Spine 2014, 39, 1743–1750. [CrossRef]
- Oertel, J.M.; Philipps, M.; Burkhardt, B.W. Endoscopic foraminotomy as a treatment for osseous foraminal stenosis. World Neurosurg 2016, 91, 50–57. [Google Scholar] [CrossRef]
- Dusad, T.; Kundnani, V.; Dutta, S.; Patel, A.; Mehta, G.; Singh, M. Comparative prospective study reporting intraoperative parameters, pedicle screw perforation, and radiation exposure in navigation-guided versus non-navigated fluoroscopy-assisted minimal invasive transforaminal lumbar interbody fusion. Asian Spine J. 2018, 12, 309–316. [Google Scholar] [CrossRef]
- Kaliya-Perumal, A.K.; Limthongkul, W.; Oh, J.Y. Utilization of spinal navigation to facilitate hassle-free rod placement during minimally-invasive long-construct posterior instrumentation. Asian Spine J. 2019, 13, 511–514. [Google Scholar] [CrossRef]
- Ransom, N.A.; Gollogly, S.; Lewandrowski, K.U.; Yeung, A. Navigating the learning curve of spinal endoscopy as an established traditionally trained spine surgeon. J Spine Surg. 2020; 6, (Suppl 1), S197–207. [Google Scholar]
- Hanna, G.; Kim, T.T.; Uddin, S.A.; Ross, L.; Johnson, J.P. Video-assisted thoracoscopic image-guided spine surgery: evolution of 19 years of experience, from endoscopy to fully integrated 3D navigation. Neurosurg Focus. 2021, 50, E8. [Google Scholar] [CrossRef]
- Yuh, W.T.; Lee, Y.S.; Jeon, J.H.; Choi, I. Future of Endoscopic Spine Surgery: Insights from Cutting-Edge Technology in the Industrial Field. Bioengineering 2023, 10, 1363. [Google Scholar] [CrossRef]
- Kwon, H.; Park, J.Y. The Role and Future of Endoscopic Spine Surgery: A Narrative Review. Neurospine. 2023, 20, 43–55. [Google Scholar] [CrossRef]
- Heo DH, Kim JY, Park JY, et al. Clinical experiences of 3-dimensional biportal endoscopic spine surgery for lumbar degenerative disease. Oper Neurosurg (Hagerstown) 2022, 22, 231–238. [CrossRef]
- Hahn, B.S.; Park, J.Y. Incorporating New Technologies to Overcome the Limitations of Endoscopic Spine Surgery: Navigation, Robotics, and Visualization. World Neurosurgery. 2021, 145, 712–721. [Google Scholar] [CrossRef] [PubMed]
- Hyun, S.J.; Kim, K.J.; Jahng, T.A.; Kim, H.J. Minimally invasive robotic versus open fluoroscopic- guided spinal instrumented fusions: a randomized controlled trial. Spine. 2017, 42, 353–358. [Google Scholar] [CrossRef]
- Kantelhardt, S.R.; Martinez, R.; Baerwinkel, S.; Burger, R.; Giese, A.; Rohde, V. Perioperative course and accuracy of screw positioning in conventional, open robotic-guided and percutaneous robotic- guided, pedicle screw placement. Eur Spine J. 2011, 20, 860–868. [Google Scholar] [CrossRef]
- Overley, S.C.; Cho, S.K.; Mehta, A.I.; Arnold, P.M. Navigation and robotics in spinal surgery: where are we now? Neurosurgery. 2017, 80, S86–S99. [Google Scholar] [CrossRef]
- Choi, G.; Uniyal, P.; Hassan, Z.; Patel, B.; Kim, W.J.J.S. A new progression towards a safer anterior percutaneous endoscopic cervical discectomy: a technical report. J Spine. 2016, 5, 2. [Google Scholar] [CrossRef]
- Ahn, Y.J. Transforaminal percutaneous endoscopic lumbar discectomy: technical tips to prevent complications. Expert Rev Med Devices. 2012, 9, 361–366. [Google Scholar] [CrossRef]
- Wang Z, Tan Y, Fu K, et al. Minimally invasive trans-superior articular process percutaneous endoscopic lumbar discectomy with robot assistance. BMC Musculoskelet Disord. 2022, 23, 1144.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



