
Submitted:
11 April 2024
Posted:
15 April 2024
You are already at the latest version
Abstract
Background: The clinical impact of withdrawal of sodium-glucose cotransporter 2 inhibitor (SGLT2i) on the all-cause readmission in patients with heart failure remains unknown. Methods: Consecutive 212 patients who were hospitalized for heart failure and received SGLT2i during the index hospitalization between February 2016 and July 2022 were evaluated. Of these, 51 patients terminated SGLT2i during or after their index hospitalization. The primary outcome was defined as an all-cause readmission rates/times. Results: Over a median of 23.2 months, an all-cause readmission occurred in 38 of 51 patients (74.5%) withdrawn from SGLT2i and 93 of 161 patients (57.8%) with continuation of SGLT2i (p = 0.099). The total number of all-cause readmissions per year was 0.97 [0-1.50] in patients withdrawn from SGLT2i and 0.50 [0-1.03] in patients with continuation of SGLT2i (p = 0.030). There was no significant difference in total medical cost (62,906 [502-187,246] versus 29,236 [7,920-180,305] JPY per month, p = 0.866) between both patient groups. Conclusions: Termination of SGLT2i may be associated with incremental all-cause readmission and no benefit in reducing total medical costs.
Keywords:
heart failure
; SGLT2 inhibitor
; hospitalization
; medical cost
1. Introduction
Heart failure (HF) is one of the most common cardiovascular diseases and is associated with frequent hospitalization and mortality [1]. Due to the aging of the overall population, the number of patients with HF is expected to increase in the future years. To date, sodium-glucose cotransporter 2 inhibitor (SGLT2i) represents a major therapeutic advance in patients with HF. Large-scale randomized controlled trials (RCTs) demonstrated that dapagliflozin and empagliflozin, one of SGLT2is, improved the outcomes of patients with HF regardless of patient’s left ventricular ejection fraction (LVEF) levels [2,3,4,5]. They are currently the only drug that has been proven to improve the outcome of patients with HF with preserved ejection fraction (HFpEF) by RCTs. Importantly, these beneficial effects were demonstrated irrespective of the presence of diabetes mellitus (DM).
Furthermore, recent RCT demonstrated that the risk of cardiovascular death or hospitalization for HF increased in patients withdrawn from empagliflozin [6]. This finding suggested a chronic effect of SGLT2i in patients with HF even after years of treatment, which dissipated after withdrawal of the drug. However, the clinical impact of withdrawal of SGLT2i on non-cardiovascular disease in patients with HF remains unknown. Given its pleiotropic effect including the kidney-protective effect, a withdrawal of SGLT2i may also increase the risk of non-cardiovascular disease [7,8]. Conversely, the withdrawal of SGLT2i may contribute to reducing the adverse effects associated with SGLT2i treatment, which may have an impact on clinical outcome. Furthermore, although several studies from different countries have evaluated the cost-effectiveness of SGLT2i for HF [9,10,11,12,13], withdrawal of SGLT2i may have a benefit in reducing total medical cost.
Thus, we compared the risk of hospitalization for any causes between the patients who continued SGLT2i and those who discontinued SGLT2i. In addition, we investigated the total medical cost associated with SGLT2i therapy for those patients.
2. Materials and Methods
This study was a single-center, prospective registry study designed to assess the efficacy of long-term SGLT2i therapy which was initiated during the index hospitalization in patients with HF. In the present study, we retrospectively evaluated the hospitalization events and medical costs associated with SGLT2i in participants. The local Institutional Ethics Board approved the study protocol, which complied with the Declaration of Helsinki. Written informed consent was obtained from all of the patients beforehand.
2.1. Study Population
This study involved patients who had been admitted for HF, which was diagnosed according to the Framingham criteria, at our institute between February 2016 and July 2022. Most of the patients had New York Heart Association (NYHA) class III/IV symptoms upon admission. Participants received guideline-directed medical therapy for HF, including renin-angiotensin system inhibitors or angiotensin receptor-neprilysin inhibitors, beta-blockers, mineralocorticoid receptor antagonists, and diuretics, if applicable. We included patients newly receiving SGLT2i during their index hospitalization immediately following the stabilization of hemodynamics in this study.
Exclusion criteria were as follows: age <20 years, end-stage renal failure with estimated glomerular filtration rate (eGFR) <15 mL/min/1.73m2, undergoing durable left ventricular assist devices or heart transplantation, pregnancy or breastfeeding, current use of SGLT2i on the index hospitalization, and lost to follow-up within 90 days after index hospitalization. In this study, patients who had hospitalization to an institute other than ours were also excluded for accurate assessment of hospitalization events and costs. Adjustment of medical therapy was permitted as real-world clinical practice.
2.2. Study Design
To investigate the long-term efficacy of SGLT2 in patients with HF, we compared the hospitalization events between the patients who continued SGLT2i after discharge and those who did not. Additionally, we compared the medical costs (expressed in Japanese yen [JPY] per month) between both patient groups to investigate the cost-benefit of SGLT2. Patients who discontinued SGLT2i during the index hospitalization for HF and those who discontinued SGLT2i during observation period were assigned to the withdrawal group. Other patients continued SGLT2i after initiation of that and they were assigned to the continuation group. Day 0 was defined as the time when they had the index discharge. When patients died or were lost to follow-up, they were censored at that time. All patients were followed until the end of the observation period or for two years.
The primary clinical assessments were (1) the occurrence of all-cause hospitalization and (2) the total number of hospitalization events after index hospitalization. The hospitalization event included those for non-cardiovascular causes. The total number of hospitalization events was expressed in the number of hospitalizations per year. The secondary clinical assessments were (1) the recurrence of hospitalization for HF and (2) the total medical costs during the observation period. In this study, medical costs were defined as the summation of in-hospital medical costs and SGLT2i costs. For the withdrawal group, the cost of SGLT2i was added to the point when they were withdrawal.
2.3. Data Collection
Baseline characteristics including demographic, laboratory, and medication data at index discharge were retrieved. The estimated glomerular filtration rate (eGFR) was calculated using the guidelines from the Chronic Kidney Disease Epidemiology Collaboration. Standard echocardiographic findings during index hospitalization were retrieved. We defined HFrEF as left ventricular ejection fraction (LVEF) <40%. We defined DM as satisfying glycated hemoglobin (HbA1c) ≥6.5% or receiving antidiabetic treatment. The dose of loop diuretics was presented as furosemide equivalent. Among SGLT2i, the cost of canagliflozin 100 mg, dapagliflozin 10 mg, and empagliflozin 10 mg were 168 JPY per day, 264 JPY per day, and 188 JPY per day, respectively.
2.4. Statistical Analyses
The statistical analysis was performed by using JMP® 15 (SAS Institute Inc., Cary, NC, USA). The level of significance was defined as 2-tailed p <0.050. Continuous variables were expressed as the median and interquartile unless any specific statements. Categorical variables were expressed as absolute numbers and percentages. Wilcoxon test was applied to compare continuous parameters, and Pearson’s χ2 test was applied for comparison of categorical variables.
Time-to-event data were evaluated using Kaplan–Meier estimates and Cox proportional hazards models to investigate the impact of baseline variables on clinical outcomes. Univariable and multivariable analyses with Cox proportional hazards models were performed to calculate the hazard ratio to assess the influence of various parameters on clinical outcomes. Univariable and multivariable linear regression analyses were performed to assess the influence of various parameters on the total number of hospitalization events. Variables significant with p <0.050 in the univariable analyses were included in the multivariable analyses.
3. Results
3.1. Follow-Up and Patient Characteristics
From February 2016 to July 2022, consecutive 295 patients initiated SGLT2i during their hospitalization for HF. Of them, 6 died during hospitalization, 1 underwent implantation of left ventricular assist device, 43 patients were lost to follow-up, and 33 had hospitalization to an institute other than ours after their index discharge. Finally, a total of 212 patients were included in this study (Figure 1).
Table 1 lists the baseline characteristics. The median age was 72 (66-81) years and 33% were women. Patients with HFrEF (LVEF <40%) were noted in 84 patients (39%). DM was noted in 147 patients (69%). All patients with DM were those with type 2 DM. Baseline eGFR was 51.1 (38.2-64.2) mL/minute/1.73m2. Baseline plasma BNP level was 142 (69-302) pg/mL.
Of these, 161 patients continued SGLT2i during the observation period and were assigned to the continuation group. Other 51 patients terminated SGLT2i during or after their index hospitalization and were assigned to the withdrawal group. In the withdrawal group, the median time SGLT2i was continued was 17 (0-133) days. Reasons of SGLT2i withdrawal are listed in Supplementary Table S1.
Baseline characteristics between the two groups were compared in Table 1. Patients in the withdrawal group were older and underweight. The withdrawal group included more patients with higher BNP levels than the continuation group. There were more patients with DM in the withdrawal group than in the continuation group.
3.2. Primary Clinical Assessments
Patients were followed for a median period of 695 (439-730) days. There were 93 readmissions (57.8%) in the continuation group and 38 readmissions (74.5%) in the withdrawal group, respectively. Patients in the withdrawal group tended to have a higher rate of hospitalization for any cause (p = 0.099; Figure 2A). The withdrawal of SGLT2i was not significantly associated with the primary outcome in the Cox analysis (p = 0.100). Instead, the history of atrial fibrillation (hazard ratio 1.44, 95% confidence interval 1.07–2.23) and HFrEF (hazard ratio 0.66, 95% confidence interval 0.46–0.95) were independently associated with the all-cause hospitalization (p <0.050 for both; Table 2).
The number of hospitalization events for any causes was higher in the withdrawal group than in the continuation group (0.97 [0-1.50] versus 0.50 [0-1.03], p = 0.030). The multivariable analysis demonstrated that the withdrawal of SGLT2i (hazard ratio 1.41, 95% confidence interval 1.05–1.88) was independently associated with the number of readmission events for any causes, together with the higher prevalence of NYHA class III/IV symptom (p <0.050 for both; Table 3). Details of hospitalization event are listed in Supplementary Table S2.
3.3. Secondary Clinical Assessments
Patients in the withdrawal group had a higher rate of readmission for HF (21.6% versus 7.5%, p = 0.007; Figure 2B). The withdrawal of SGLT2i (hazard ratio 2.38, 95% confidence interval 1.04–5.56) and eGFR (hazard ratio 0.97, 95% confidence interval 0.94–0.99) were independently associated with the readmission for HF (p <0.050 for both; Table 4).
In the withdrawal group, the median cost of SGLT2i was 153 (0-1,747) JPY per month and in-hospital medical cost was 62,906 (0-186,831) JPY per month. In the continuation group, the median cost of SGLT2i was 7,920 (5,640-7,920) JPY and in-hospital medical cost was 22,815 (0-172,385) JPY per month. There was no significant difference in total medical cost (62,906 [502–187,246] versus 29,236 [7,920–180,305] JPY per month, p = 0.866; Figure 3) between the two groups.
4. Discussion
In this retrospective analysis, we investigated the impact of withdrawal of SGLT2i after hospitalization for HF on clinical outcomes and cost-effectiveness. While withdrawal of SGLT2i did not increase the risk of hospitalization for any cause, it did increase the total number of hospitalization events. Furthermore, withdrawal of SGLT2i increased the risk of hospitalization for HF. There were no significant differences in medical cost between both groups (i.e., a withdrawal of SGLT2i did not have benefit in reducing total medical cost).
4.1. Clinical Outcomes
In the additional trial after the end of the EMPEROR-Reduced and the EMPEROR-Preserved trials, patients withdrawn from treatment with empagliflozin showed increased the risk of HF events and worsening health status compared with patients withdrawn from placebo [6]. Although this trial indicates that cessation of SGLT2i treatment may have deleterious consequences, there are some patients who are unable to continue SGLT2i due to adverse events or their chronic disease [14]. In this study, SGLT2i were terminated for reasons other than death in 51 patients (24.1%). Our withdrawal rate of 24.1% is higher than previously reported rates of 10.5-23.2% in RCTs [2,3,4,5]. A possible explanation to the high frequency of SGLT2i discontinuation was that our population were included in this study soon after an episode of HF hospitalization in real-world clinical practice.
In the present study, withdrawal of SGLT2i increased the total number of hospitalization events. This observation was a new finding, as there were few reports investigating the impact of SGLT2i on all-cause hospitalization. Furthermore, present study demonstrated that withdrawal of SGLT2i increased the risk of hospitalization for HF. This is in line with a previous trial suggesting that the risk of cardiovascular death or hospitalization for HF increased in patients withdrawn from SGLT2i. Unlike previous randomized trial, this observational study included patients withdrawn from SGLT2i for any reason. The reason for discontinuing SGLT2i might result in the increase in hospitalization events, because there were different characteristics between patients who continued SGLT2i and those who discontinued them in this study. Nevertheless, multivariable analysis showed that withdrawal of SGLT2i was the independent predictors of increasing total number of hospitalization events and the risk of hospitalization for HF. This finding demonstrated that abrupt cessation of SGLT2i may have deleterious consequences for patients with HF, even if there was plausible reason for withdrawal of SGLT2i. The increased hospitalization events due to withdrawal of SGLT2i may also lead to increase in medications excluding SGLT2i, which potentially increase overall medical costs. These observations highlight the importance of continuing SGLT2is for HF patients.
4.2. Medical Costs
Several cost-effectiveness analyses were performed using Markov model that simulate the disease progression of HF patients with SGLT2i over their lifetime to capture all relevant costs and outcomes [15,16,17]. The model used estimates of treatment efficacy, event probabilities, and utilities from database or published literature. Whereas, such analyses often did not model the adverse events from SGLT2i or the withdrawal of them. Minor adverse effects associated with SGLT2i and their pleiotropic effects may make it difficult to identify cost-effectiveness of them. Therefore, there was no study that evaluated the changes in actual medical cost associated with SGLT2i treatment. In further economic evaluations of SGLT2i for HF patients, the epidemiological real-world data should be taken. Here, we investigated actual medical costs, including both in-hospital costs and SGLT2i costs, for the patients who were newly received SGLT2i during their hospitalization for HF.
In this study, there was no significant difference in medical cost between patients with continuation of SGLT2i and those withdrawn SGLT2i. Interestingly, in-hospital costs were similar despite differences in the number of hospitalization events between the two groups. The possible reasons for uniformity of medical costs were mainly derived from the differences in causes of hospitalization. Patients withdrawn from SGLT2i had higher hospitalization costs for HF and those for non-cardiovascular disease than those with continuation of SGLT2i. In contrast, patients withdrawn from SGLT2 tended to have lower hospitalization costs for cardiovascular disease than those with continuation of SGLT2i. Consequently, medical costs for both groups were similar. This finding suggests that patients who continued SGLT2i may have undergone expensive treatments for cardiovascular disease (e.g., cardiac surgeries, cardiac devices, and transcatheter therapies). A possible explanation to the expensive treatments for patients with continuation of SGLT2i was that they had younger age, higher body weight, or lower proportion of NYHA class III/IV at baseline. It was assumed to be the possibility that patients who were able to continue SGLT2i had a stable condition. Conversely, SGLT2i might stabilize patients with HF enough to undergo invasive treatments. Importantly, medical costs were consistent in spite of the differences in treatment detail and clinical outcome between the two groups.
4.3. Limitations
This study has the following limitations. First, this was an observational study with small sample size, not a randomized study. Given the low event number, the number of potential confounders included in the multivariate analyses was restricted. Also, it is not possible to establish cause-effect relationship given an observational study design. Inter-group comparison has selection bias with different background characteristics between two groups, although the results for the primary clinical assessment remained significant in analysis with multiple imputations. Second, the timing of withdrawal of SGLT2i varied depending on participants in this study. Furthermore, it should be emphasized that other HF medications were also adjusted during observational period. Thus, it is challenging to assess the clinical outcome and the cost-benefit associated with a withdrawal of SGLT2i alone. Lastly, the multiple types of SGLT2i including canagliflozin were used in the present study. No RCTs have evaluated the efficacy of canagliflozin in patients with HF. Nevertheless, a recent retrospective cohort study suggested that there was no significant difference in the risk of cardiovascular events including HF among patients taking dapagliflozin, canagliflozin, and empagliflozin [18]. On the other hand, previous study demonstrated that empagliflozin was highly cost-effective compared with canagliflozin and dapagliflozin using healthcare costs of united states [19]. It remains unclear whether such cost effectiveness is consistent across individual SGLT2i.uthors should discuss the results and how they can be interpreted from the perspective of previous studies and of the working hypotheses. The findings and their implications should be discussed in the broadest context possible. Future research directions may also be highlighted.
5. Conclusions
In summary, the continuation of SGLT2i therapy for patients with HF reduced the total number of hospitalization events without increasing medical cost burden.
Author Contributions
M.N. (Masaki Nakagaito) wrote a draft. T.I. analyzed and interpreted the patient data. S.J., R.U., and M.N. (Makiko Nakamura) collected data and reviewed the draft. K.K. supervised the study. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and ap-proved by the Institutional Ethics Board of Toyama University Hospital (#R2015154).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Tsao, C. W.; Aday, A. W.; Almarzooq, Z. I.; Anderson, C. A. M.; Arora, P.; Avery, C. L.; Baker-Smith, C. M.; Beaton, A. Z.; Boehme, A. K.; Buxton, A. E.; et al. Heart Disease and Stroke Statistics-2023 Update: A Report From the American Heart Association. Circulation 2023, 147, e93–e621. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J. J. V.; Solomon, S. D.; Inzucchi, S. E.; Køber, L.; Kosiborod, M. N.; Martinez, F. A.; Ponikowski, P.; Sabatine, M. S.; Anand, I. S.; Bělohlávek, J.; et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N Engl J Med 2019, 381, 1995–2008. [Google Scholar] [CrossRef] [PubMed]
- Packer, M.; Anker, S. D.; Butler, J.; Filippatos, G.; Pocock, S. J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N Engl J Med 2020, 383, 1413–1424. [Google Scholar] [CrossRef] [PubMed]
- Anker, S. D.; Butler, J.; Filippatos, G.; Ferreira, J. P.; Bocchi, E.; Böhm, M.; Brunner-La Rocca, H. P.; Choi, D. J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N Engl J Med 2021. [CrossRef] [PubMed]
- Solomon, S. D.; McMurray, J. J. V.; Claggett, B.; de Boer, R. A.; DeMets, D.; Hernandez, A. F.; Inzucchi, S. E.; Kosiborod, M. N.; Lam, C. S. P.; Martinez, F.; et al. Dapagliflozin in Heart Failure with Mildly Reduced or Preserved Ejection Fraction. N Engl J Med 2022, 387, 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Packer, M.; Butler, J.; Zeller, C.; Pocock, S. J.; Brueckmann, M.; Ferreira, J. P.; Filippatos, G.; Usman, M. S.; Zannad, F.; Anker, S. D. Blinded Withdrawal of Long-Term Randomized Treatment With Empagliflozin or Placebo in Patients With Heart Failure. Circulation 2023, 148, 1011–1022. [Google Scholar] [CrossRef] [PubMed]
- Heerspink, H. J. L.; Stefánsson, B. V.; Correa-Rotter, R.; Chertow, G. M.; Greene, T.; Hou, F. F.; Mann, J. F. E.; McMurray, J. J. V.; Lindberg, M.; Rossing, P.; et al. Dapagliflozin in Patients with Chronic Kidney Disease. N Engl J Med 2020, 383, 1436–1446. [Google Scholar] [CrossRef] [PubMed]
- Herrington, W. G.; Staplin, N.; Wanner, C.; Green, J. B.; Hauske, S. J.; Emberson, J. R.; Preiss, D.; Judge, P.; Mayne, K. J.; Ng, S. Y. A.; et al. Empagliflozin in Patients with Chronic Kidney Disease. N Engl J Med 2023, 388, 117–127. [Google Scholar] [CrossRef] [PubMed]
- McEwan, P.; Darlington, O.; McMurray, J. J. V.; Jhund, P. S.; Docherty, K. F.; Böhm, M.; Petrie, M. C.; Bergenheim, K.; Qin, L. Cost-effectiveness of dapagliflozin as a treatment for heart failure with reduced ejection fraction: a multinational health-economic analysis of DAPA-HF. Eur J Heart Fail 2020, 22, 2147–2156. [Google Scholar] [CrossRef] [PubMed]
- Hallinen, T.; Kivelä, S.; Soini, E.; Harjola, V. P.; Pesonen, M. Cost-Effectiveness of Empagliflozin in Combination with Standard Care versus Standard Care Only in the Treatment of Heart Failure Patients in Finland. Clinicoecon Outcomes Res 2023, 15, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Cohen, L. P.; Isaza, N.; Hernandez, I.; Lewis, G. D.; Ho, J. E.; Fonarow, G. C.; Kazi, D. S.; Bellows, B. K. Cost-effectiveness of Sodium-Glucose Cotransporter-2 Inhibitors for the Treatment of Heart Failure With Preserved Ejection Fraction. JAMA Cardiol 2023, 8, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Liao, C. T.; Yang, C. T.; Toh, H. S.; Chang, W. T.; Chang, H. Y.; Kuo, F. H.; Lee, M. C.; Hua, Y. M.; Tang, H. J.; Strong, C.; et al. Cost-effectiveness evaluation of add-on dapagliflozin for heart failure with reduced ejection fraction from perspective of healthcare systems in Asia-Pacific region. Cardiovasc Diabetol 2021, 20, 204. [Google Scholar] [CrossRef] [PubMed]
- Liao, C. T.; Yang, C. T.; Kuo, F. H.; Lee, M. C.; Chang, W. T.; Tang, H. J.; Hua, Y. M.; Chang, H. Y.; Chen, Z. C.; Strong, C.; et al. Cost-Effectiveness Evaluation of Add-on Empagliflozin in Patients With Heart Failure and a Reduced Ejection Fraction From the Healthcare System’s Perspective in the Asia-Pacific Region. Front Cardiovasc Med 2021, 8, 750381. [Google Scholar] [CrossRef] [PubMed]
- Nakagaito, M.; Imamura, T.; Ushijima, R.; Nakamura, M.; Kinugawa, K. Predictors and Outcomes of SGLT2 Inhibitor Discontinuation in a Real-World Population after Hospitalization for Heart Failure. Biomedicines 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- Nam, K.; Cho, D. S.; Kim, H.; Kwon, B.; Yoon, Y.; Park, C.; Kim, E. S.; Youn, J. C.; Park, S. K. Systematic Review of the Economic Evaluation of Sodium-Glucose Cotransporter-2 Inhibitors Used as Treatment in Patients with Heart Failure. In Clin Drug Investig, Vol. 43; © 2023. The Author(s), under exclusive licence to Springer Nature Switzerland AG., 2023; pp 463-474.
- Liu, J.; Liu, D.; Gong, X.; Wei, A.; You, R. Cost-effectiveness of empagliflozin for the treatment of heart failure: a systematic review. In Front Pharmacol, Vol. 14; Copyright © 2023 Liu, Liu, Gong, Wei and You., 2023; p 1186579.
- Wu, M.; Qin, S.; Wang, L.; Tan, C.; Peng, Y.; Zeng, X.; Luo, X.; Yi, L.; Wan, X. Economic Evaluation of Dapagliflozin in the Treatment of Patients With Heart Failure: A Systematic Review. In Front Pharmacol, Vol. 13; Copyright © 2022 Wu, Qin, Wang, Tan, Peng, Zeng, Luo, Yi and Wan., 2022; p 860109.
- Suzuki, Y.; Kaneko, H.; Okada, A.; Itoh, H.; Matsuoka, S.; Fujiu, K.; Michihata, N.; Jo, T.; Takeda, N.; Morita, H.; et al. Comparison of cardiovascular outcomes between SGLT2 inhibitors in diabetes mellitus. Cardiovasc Diabetol 2022, 21, 67. [Google Scholar] [CrossRef] [PubMed]
- Reifsnider, O. S.; Kansal, A. R.; Gandhi, P. K.; Cragin, L.; Brand, S. B.; Pfarr, E.; Fahrbach, K.; Ustyugova, A. Cost-effectiveness of empagliflozin versus canagliflozin, dapagliflozin, or standard of care in patients with type 2 diabetes and established cardiovascular disease. BMJ Open Diabetes Res Care 2021, 9. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Patient flow chart.
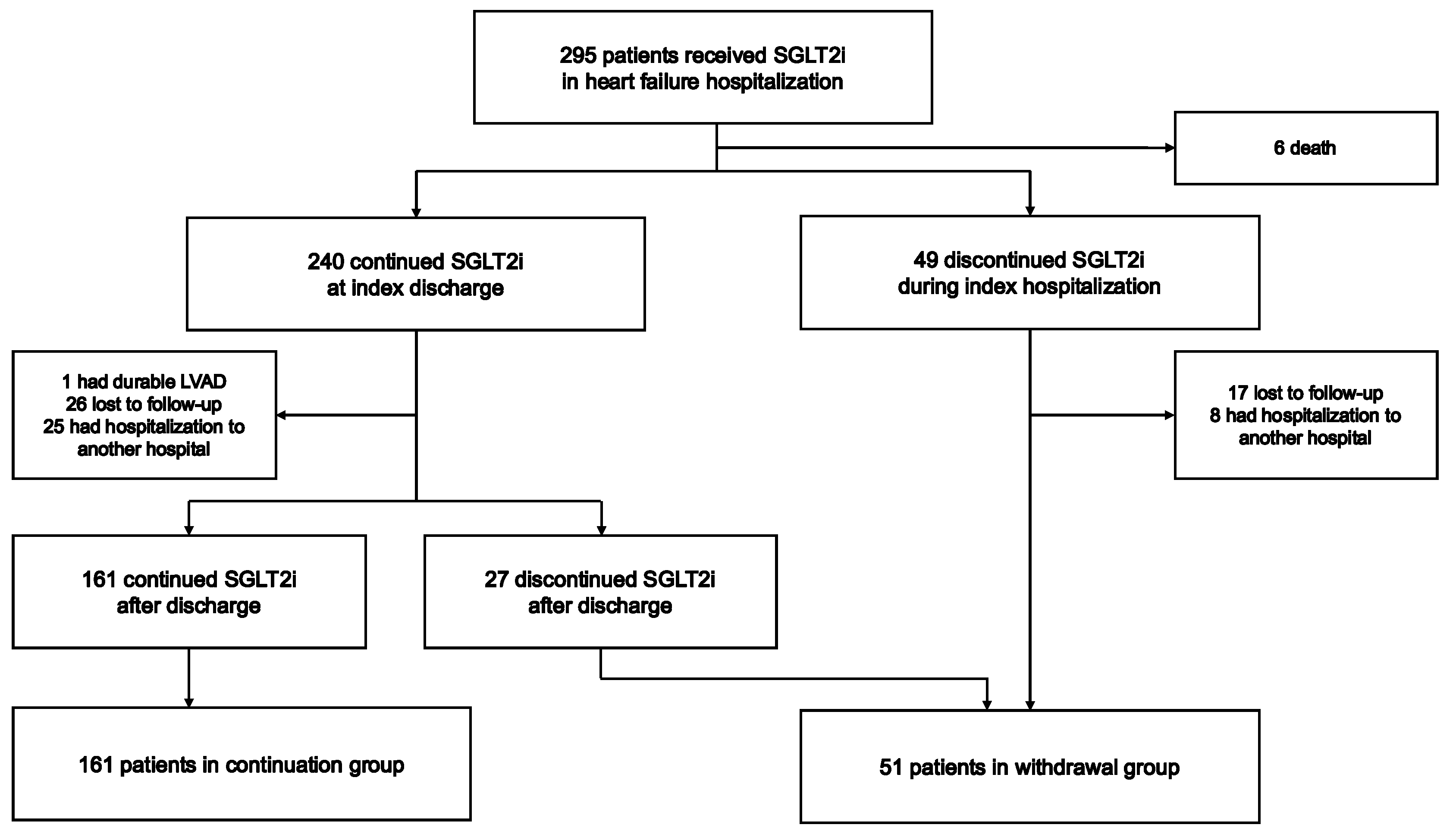
Figure 2.
Hospitalizations for any causes (A) and recurrent heart failure (B).
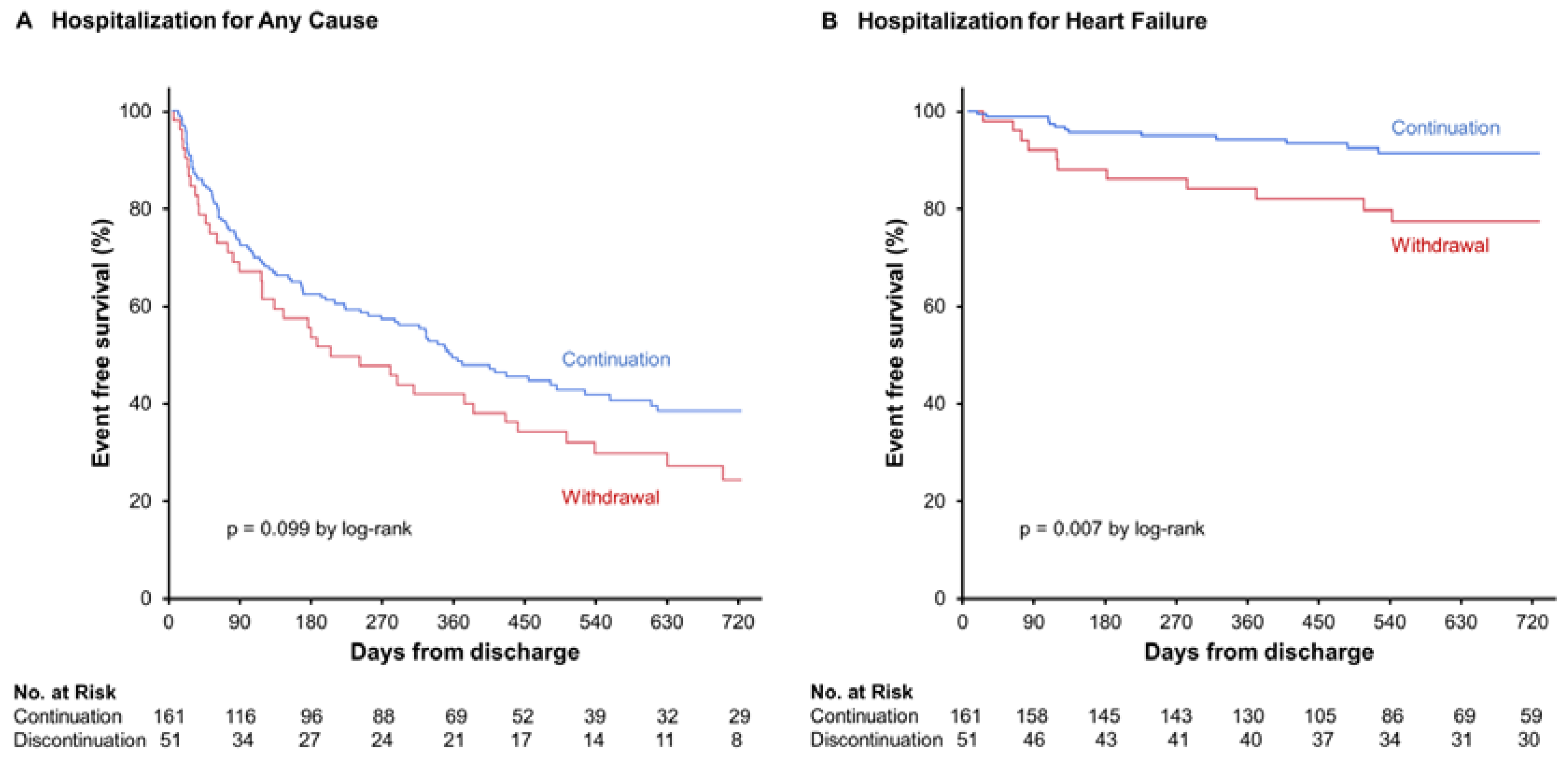
Figure 3.
Breakdown of medical costs. JPY Japanese yen, CVD cardiovascular disease, HF heart failure, SGLT2i sodium-glucose cotransporter 2 inhibitor. The medical costs are expressed in the mean value.
Figure 3.
Breakdown of medical costs. JPY Japanese yen, CVD cardiovascular disease, HF heart failure, SGLT2i sodium-glucose cotransporter 2 inhibitor. The medical costs are expressed in the mean value.
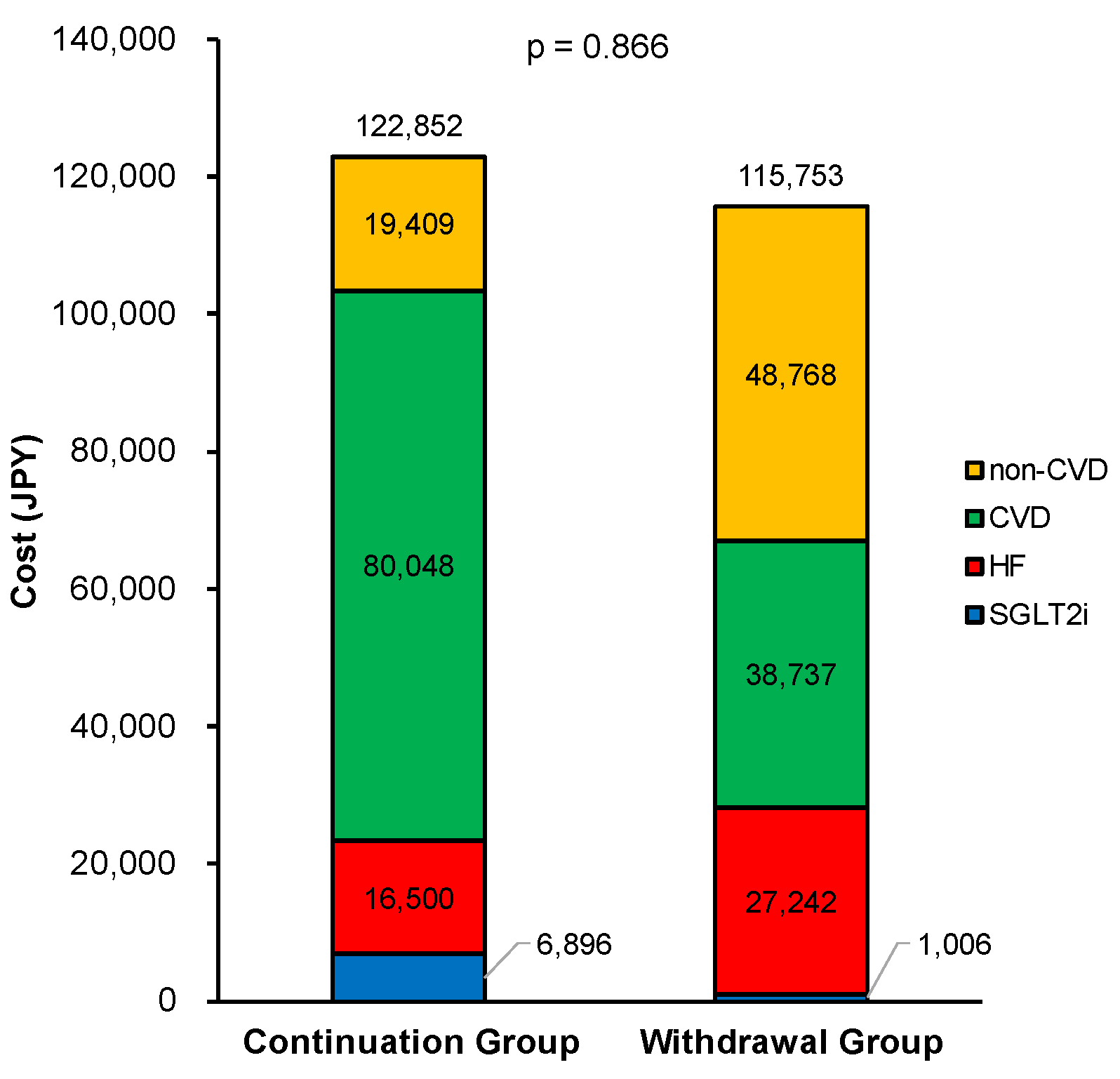

Table 1.
Baseline characteristics at index discharge.
| Total (n = 212) |
Continuation (n = 161) |
Withdrawal (n = 51) |
P value | |
|---|---|---|---|---|
| Age, years | 72 (66-81) | 72 (63-79) | 76 (71-84) | 0.004* |
| Male, n (%) | 141 (67) | 114 (71) | 27 (53) | 0.019* |
| Body weight, kg | 56.6 (49.9-67.5) | 57.3 (50.9-69.3) | 54.0 (44.1-64.1) | 0.021* |
| Body mass index, kg/m2 | 22.2 (19.8-24.8) | 22.6 (20.2-25.3) | 21.7 (18.8-23.6) | 0.026* |
| Systolic blood pressure, mmHg | 107 (96-118) | 107 (95-119) | 106 (97-116) | 0.990 |
| Heart rate, beats per minutes | 71 (63-78) | 70 (62-78) | 71 (64-83) | 0.772 |
| Diabetes mellitus, n (%) | 147 (69) | 106 (66) | 41 (80) | 0.050* |
| Ischemic etiology, n (%) | 86 (41) | 62 (39) | 24 (47) | 0.279 |
| Atrial fibrillation, n (%) | 61 (29) | 43 (26) | 18 (35) | 0.238 |
| Implantable cardioverter-defibrillator, n (%) | 22 (10) | 20 (12) | 2 (4) | 0.083 |
| Cardio resynchronization therapy, n (%) | 15 (7) | 12 (8) | 3 (6) | 0.703 |
| New York Heart Association class Ⅲ-Ⅳ, n (%) | 57 (27) | 40 (25) | 17 (33) | 0.234 |
| Left ventricular ejection fraction, % | 43 (33-55) | 44 (34-56) | 42 (31-52) | 0.294 |
| Value of <40% (HFrEF), n (%) | 84 (39) | 59 (37) | 25 (49) | 0.115 |
| HbA1c, % | 6.6 (6.1-7.4) | 6.6 (6.1-7.3) | 6.7 (6.4-7.9) | 0.115 |
| Hemoglobin, g/dL | 12.7 (11.2-14.2) | 12.8 (11.5-14.3) | 12.0 (10.8-13.8) | 0.078 |
| Serum albumin, g/dL | 3.6 (3.3-3.9) | 3.6 (3.4-3.9) | 3.5 (3.1-3.7) | 0.006* |
| Serum sodium, mEq/L | 138 (136-140) | 138 (137-140) | 137 (134-139) | <0.001* |
| Serum potassium, mEq/L | 4.4 (4.1-4.6) | 4.4 (4.1-4.6) | 4.4 (3.9-4.8) | 0.612 |
| eGFR, mL/minute/1.73m2 | 51.1 (38.2-64.2) | 52.8 (40.3-64.6) | 49.2 (32.6-60.3) | 0.109 |
| Uric acid, mg/dL | 5.7 (4.7-6.9) | 5.5 (4.6-6.9) | 5.9 (5.1-7.2) | 0.060 |
| Plasma BNP, pg/mL | 142 (69-302) | 132 (64-266) | 182 (95-353) | 0.022* |
| Heart failure therapies | ||||
| Beta-blockers, n (%) | 184 (87) | 137 (85) | 47 (92) | 0.194 |
| ACEI/ARB/ARNI, n (%) | 200 (94) | 153 (95) | 47 (92) | 0.439 |
| Loop diuretics, n (%) | 139 (66) | 99 (62) | 40 (78) | <0.001* |
| Dose of loop diuretics, mg/day | 10 (0-20) | 10 (0-20) | 20 (10-20) | 0.223 |
| MRA, n (%) | 145 (68) | 112 (70) | 33 (65) | 0.515 |
| Sodium-glucose cotransporter 2 inhibitors | ||||
| Canagliflozin, n (%) | 40 (19) | 24 (15) | 16 (31) | 0.009* |
| Dapagliflozin, n (%) | 116 (55) | 95 (59) | 21 (41) | 0.026* |
| Empagliflozin, n (%) | 56 (26) | 42 (26) | 14 (28) | 0.847 |
| eGFR, estimated glomerular filtration rate; HFrEF, heart failure with reduced ejection fraction (ejection fraction <40%); HbA1c, glycated hemoglobin; BNP, b-type natriuretic peptide; ARB, angiotensin receptor blockers; ARNI, angiotensin receptor-neprilysin inhibitors; MRA, mineralocorticoid receptor antagonists. *p <0.050. | ||||
Table 2.
Variables associated with hospitalization for any cause.
| All patients (n = 212) | ||||||
|---|---|---|---|---|---|---|
| Univariable analysis | Multivariable analysis | |||||
| Variables | Hazard ratio | 95% CI | p value | Hazard ratio | 95% CI | p value |
| Age, years | 1.01 | 0.99, 1.02 | 0.394 | |||
| Male, yes | 0.75 | 0.53, 1.07 | 0.112 | |||
| Body mass index, kg/m2 | 0.99 | 0.94, 1.03 | 0.510 | |||
| Systolic blood pressure, mmHg | 1.00 | 0.99, 1.01 | 0.744 | |||
| Heart rate, bpm | 1.01 | 0.99, 1.02 | 0.551 | |||
| Ischemic etiology, yes | 0.99 | 0.70, 1.41 | 0.973 | |||
| Atrial fibrillation, yes | 1.54 | 1.07, 2.21 | 0.022* | 1.44 | 1.07, 2.23 | 0.020* |
| NYHA class Ⅲ-Ⅳ, n (%) | 1.29 | 0.88, 1.88 | 0.188 | |||
| HFrEF, yes | 0.69 | 0.48, 0.99 | 0.041* | 0.66 | 0.46, 0.95 | 0.023* |
| Diabetes mellitus, yes | 1.36 | 0.92, 2.01 | 0.123 | |||
| Hemoglobin, g/dL | 0.95 | 0.88, 1.03 | 0.239 | |||
| Serum albumin, g/dL | 1.08 | 0.73, 1.58 | 0.713 | |||
| Serum sodium, mEq/L | 1.00 | 0.95, 1.06 | 0.981 | |||
| Serum potassium, mEq/L | 0.82 | 0.59, 1.15 | 0.238 | |||
| eGFR, mL/min/1.73m2 | 0.99 | 0.98, 1.00 | 0.047* | 0.99 | 0.98, 1.00 | 0.044* |
| Uric acid, mg/dL | 0.98 | 0.88, 1.08 | 0.635 | |||
| ln BNP | 1.08 | 0.91, 1.28 | 0.379 | |||
| Beta-blockers, yes | 1.03 | 0.62, 1.72 | 0.905 | |||
| ACEI/ARB/ARNI, yes | 0.70 | 0.37, 1.34 | 0.280 | |||
| Loop diuretics, yes | 1.12 | 0.78, 1.62 | 0.531 | |||
| MRA, yes | 0.81 | 0.56, 1.16 | 0.241 | |||
| Termination of SGLT2i, yes | 1.37 | 0.94, 2.00 | 0.100 | |||
| NYHA, New York Heart Association; HFrEF, heart failure with reduced ejection fraction (ejection fraction <40%); eGFR, estimated glomerular filtration rate; BNP, b-type natriuretic peptide; ACEI, angiotensin converting enzyme inhibitors; ARB, angiotensin receptor blockers; ARNI, angiotensin receptor-neprilysin inhibitors; MRA, mineralocorticoid receptor antagonists. *p <0.050. | ||||||
Table 3.
Variables associated with total number of hospitalization event for any cause.
| All patients (n = 212) | ||||||
|---|---|---|---|---|---|---|
| Univariable analysis | Multivariable analysis | |||||
| Variables | β | 95% CI | p value | β | 95% CI | p value |
| Age, years | -0.03 | -0.06, 0.04 | 0.681 | |||
| Male, yes | -0.10 | -1.07, 0.15 | 0.137 | |||
| Body mass index, kg/m2 | -0.08 | -0.23, 0.06 | 0.251 | |||
| Systolic blood pressure, mmHg | -0.08 | -0.05, 0.02 | 0.280 | |||
| Heart rate, bpm | -0.05 | -0.07, 0.03 | 0.530 | |||
| Ischemic etiology, yes | 0.10 | -0.14, 1.03 | 0.136 | |||
| Atrial fibrillation, yes | -0.03 | 0.79, 0.49 | 0.640 | |||
| NYHA class Ⅲ-Ⅳ, n (%) | 0.16 | 0.11, 1.40 | 0.022* | 0.15 | 0.06, 1.34 | 0.032* |
| HFrEF, yes | 0.06 | -0.32, 0.86 | 0.369 | |||
| Diabetes mellitus, yes | -0.08 | -0.99, 0.25 | 0.244 | |||
| Hemoglobin, g/dL | -0.04 | -0.36, 0.20 | 0.568 | |||
| Serum albumin, g/dL | 0.02 | -1.08, 1.51 | 0.743 | |||
| Serum sodium, mEq/L | -0.04 | -0.23, 0.12 | 0.559 | |||
| Serum potassium, mEq/L | 0.08 | -0.46, 1.89 | 0.230 | |||
| eGFR, mL/min/1.73m2 | -0.10 | -0.05, 0.01 | 0.158 | |||
| Uric acid, mg/dL | 0.01 | -0.31, 0.34 | 0.923 | |||
| ln BNP | 0.08 | -0.22, 0.90 | 0.235 | |||
| Beta-blockers, yes | 0.04 | -0.63, 1.07 | 0.606 | |||
| ACEI/ARB/ARNI, yes | 0.01 | -1.18, 1.31 | 0.920 | |||
| Loop diuretics, yes | 0.04 | -0.41, 0.80 | 0.524 | |||
| MRA, yes | 0.03 | -0.51, 0.73 | 0.722 | |||
| Termination of SGLT2i, yes | 0.15 | 1.40, 0.06 | 0.032* | 0.14 | 0.01, 1.34 | 0.048* |
| NYHA, New York Heart Association; HFrEF, heart failure with reduced ejection fraction (ejection fraction <40%); eGFR, estimated glomerular filtration rate; BNP, b-type natriuretic peptide; ACEI, angiotensin converting enzyme inhibitors; ARB, angiotensin receptor blockers; ARNI, angiotensin receptor-neprilysin inhibitors; MRA, mineralocorticoid receptor antagonists. *p <0.050. | ||||||
Table 4.
Variables associated with recurrent hospitalization for heart failure.
| All patients (n = 212) | ||||||
|---|---|---|---|---|---|---|
| Univariable analysis | Multivariable analysis | |||||
| Variables | Hazard ratio | 95% CI | p value | Hazard ratio | 95% CI | p value |
| Age, years | 1.01 | 0.97, 1.05 | 0.704 | |||
| Male, yes | 0.93 | 0.40, 2.20 | 0.873 | |||
| Body mass index, kg/m2 | 0.98 | 0.87, 1.08 | 0.646 | |||
| Systolic blood pressure, mmHg | 0.98 | 0.96, 1.01 | 0.230 | |||
| Heart rate, bpm | 0.97 | 0.93, 1.01 | 0.115 | |||
| Ischemic etiology, yes | 1.15 | 0.51, 2.63 | 0.733 | |||
| Atrial fibrillation, yes | 2.34 | 1.03, 5.31 | 0.041* | 1.75 | 0.76, 4.03 | 0.193 |
| NYHA class Ⅲ-Ⅳ, n (%) | 1.33 | 0.55, 3.25 | 0.526 | |||
| HFrEF, yes | 1.11 | 0.49, 2.53 | 0.809 | |||
| Diabetes mellitus, yes | 2.12 | 0.72, 6.24 | 0.171 | |||
| Hemoglobin, g/dL | 0.88 | 0.71, 1.08 | 0.239 | |||
| Serum albumin, g/dL | 0.87 | 0.35, 2.17 | 0.767 | |||
| Serum sodium, mEq/L | 0.97 | 0.87, 1.10 | 0.641 | |||
| Serum potassium, mEq/L | 0.75 | 0.36, 1.70 | 0.477 | |||
| eGFR, mL/min/1.73m2 | 0.96 | 0.93, 0.99 | 0.003* | 0.97 | 0.94, 0.99 | 0.019* |
| Uric acid, mg/dL | 1.04 | 0.81, 1.30 | 0.751 | |||
| ln BNP | 1.31 | 0.87, 2.08 | 0.222 | |||
| Beta-blockers, yes | 1.02 | 0.30, 3.45 | 0.970 | |||
| ACEI/ARB/ARNI, yes | 0.61 | 0.14, 2.60 | 0.502 | |||
| Loop diuretics, yes | 3.61 | 1.07, 12.16 | 0.038* | 1.95 | 0.54, 7.04 | 0.308 |
| MRA, yes | 1.06 | 0.43, 2.56 | 0.907 | |||
| Termination of SGLT2i, yes | 2.93 | 1.29, 6.65 | 0.010* | 2.38 | 1.04, 5.45 | 0.041* |
| NYHA, New York Heart Association; HFrEF, heart failure with reduced ejection fraction (ejection fraction <40%); eGFR, estimated glomerular filtration rate; BNP, b-type natriuretic peptide; ACEI, angiotensin converting enzyme inhibitors; ARB, angiotensin receptor blockers; ARNI, angiotensin receptor-neprilysin inhibitors; MRA, mineralocorticoid receptor antagonists. *p <0.050. | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



