Submitted:
09 April 2024
Posted:
10 April 2024
You are already at the latest version
Abstract
Cognitive impairment is a condition which affects aging patient populations and is becoming more prevalent as the geriatric population expands. It is categorized by the extent of cognitive decline, memory loss, functional abilities, and the capability to perform daily tasks. Based on the degree of impairment, it is classified as mild cognitive impairment or dementia. Considering the debilitating nature of cognitive decline and its impact on quality of life, prevention is key. In addition, given the gradual progression of the underlying causes of cognitive decline, early diagnosis and appropriate management has the potential to offer clinical advantages and better patient outcomes. Management options discussed vary from pharmaceutical regimens to neurosurgical interventions, with differing outcomes based on etiology of cognitive impairment.
Keywords:
brain computer interface
; encapsulated cell biodelivery
; focused ultrasound
; radiofrequency
; radiosurgery
; transcranial direct current stimulation
; transranial magnetic stimulation
; electroconvulsive therapy
; Deep Brain Stimulation
1. Introduction
With a rapidly growing geriatric population and an expected twofold increase in adults 65 years or older in the United States by 2050, it is vital to evaluate our current knowledge and management protocols of existing and novel age-related ailments [1]. At the forefront of these, cognitive impairment presents a prevalent, pressing disability to tackle.
Characterized as a decline in cognitive function, cognitive impairment can be seen clinically in a wide array of classifications based on severity. The essential factors governing its severity are a function of cognitive deterioration, loss of learning and memory capacity, and the need for assistance in performing daily tasks [2,3]. Apart from typical age-related changes, cognitive dysfunction spans a spectrum from mild cognitive impairment (MCI) to dementia. Characteristics of MCI include a decline in memory and other cognitive functions [4]. In contrast, dementia is associated with more severe neurocognitive impairment, encompassing deterioration in memory, language skills, problem-solving abilities, and other advanced cognitive functions [5]. The value of MCI designation partly lies in its utility as an identifier for patients who fall in an intermediate stage between normal age-related changes and dementia [4]. It is estimated that approximately 10% of MCI cases progress to dementia each year [6]. Primary dementia typically follows a gradual course as the underlying pathology unfolds. The principal underlying causes of dementia include Alzheimer's disease (AD), frontotemporal dementia (FTD), Lewy body disease (LBD), and Parkinson's disease (PD). Other neurodegenerative conditions contributing to progressive cognitive decline and dementia encompass vascular dementia (VD), Huntington's disease, prion disease, traumatic brain injury, and stroke [7,8,9,10,11].
Given the multifaceted environments in which neurocognitive decline can develop and the increasing number of patients facing such decline, it is incumbent on diagnosticians to optimize early detection and intervention. Investigations have highlighted the significance of lifestyle adjustments, risk factor management, and early use of pharmaceutical treatment to inhibit disease advancement [12,13,14,15]. Neurosurgical approaches such as stimulation, biodelivery, and radiosurgery have also emerged as potentially beneficial early therapies. In doing so, existing literature consistently supports the importance of enhanced diagnostic capabilities in enabling early interventions for the sake of, ultimately, optimizing patient outcomes [16,17].
The diagnostic arsenal for assessing cognitive impairment across different dementia causes encompasses neurocognitive assessments, biomarker surveillance, magnetic resonance imaging, positron emission tomography, and cerebrospinal fluid assays [18,19]. Nevertheless, for the wide majority of patient populations, the fundamental evaluation for dementia typically takes place in primary care settings. With less access to technological advancements, the evaluation is informed by the patient's medical history, supplemented by insights from close family and friends if available. Based on the history, the diagnostician may choose to assess cognitive and neurological functions as part of the encounter. The wide variety of dementia etiologies, in addition to the nuanced nature of neurocognitive decline presentation, render the screening tools essential to optimizing patient outcomes through early detection and intervention. Recognition of the importance for reliable dementia screening tools has been echoed by the 2020 US Preventative Services Task. Nevertheless, there remains an academic gap preventing a consensus on the overall benefits and detriments of cognitive impairment screening [20]. However, the importance of preventative measures and appropriate management have been emphasized throughout the literature. Thus, this review aims to consolidate the literature regarding the modifiable risk factors for various etiologies of cognitive decline, as well as current guidelines for management and care.
2. Alzheimer’s Disease (AD)
AD (Figure 1) is a neurodegenerative condition that is the primary cause of adult-onset dementia [21]. It typically begins with mild indications such as minor lapses in short-term memory, devolving into progressive memory decline, alterations in personality, and cognitive changes which affect faculties such as problem-solving, executive function, and judgment [22].
Chandra, A., Dervenoulas, G., Politis, M. et al. Magnetic resonance imaging in Alzheimer’s disease and mild cognitive impairment. J Neurol 266, 1293–1302 (2019). https://doi.org/10.1007/s00415-018-9016-3
© 2019 The Authors. Journal of Neurology published by Springer Nature.
2.1. AD: Modifiable Risk Factors
The development and progression of Alzheimer’s disease is affected by many modifiable risk factors shared with MCI and other forms of dementia. It has been stated that the greatest known risk factor for Alzheimer’s and other dementias is increased age [24]. Although a large contributing factor, it is generally not considered to be a modifiable risk factor. One modifiable risk factor that plays a role in Alzheimer’s disease is vascular disease, specifically hypertension, atherosclerosis, diabetes, atrial fibrillation and hypercholesterolemia. Traumatic brain injury, epilepsy, depression, low levels of physical activity, sleep disturbances, poor diet, smoking and alcohol consumption have all been implicated in Alzheimer’s disease as well. Some studies have tried to stratify risk factors by when they occur in life (early life, middle life, later life), and found that less education is a risk factor in early life (<45 years old); hearing loss, traumatic brain injury, obesity, alcohol and hypertension increase risk in middle life (45-65 years old); and smoking, physical inactivity, depression, social isolation and diabetes increase risk in later life (>65 years old) [25].
2.2. AD: Management & Care
While AD has no current cure, early intervention has shown promise in preventing the decline in cognitive abilities and activities of daily living, in addition to suppressing behavioral changes. Current pharmacological treatment is centered around blocking the degradation of acetylcholine by cholinesterase inhibitors and reducing the damage caused by calcium excitotoxicity with NMDA receptor antagonists [26]. Control trials have illustrated the early use of donepezil intervention as a mechanism to preserve cognitive functions [27,28,29,30]. Cholinesterase inhibitors have also been used effectively in attempts to treat the onset of AD [31]. Although cholinesterase inhibitor therapy has been shown to improve cognitive function, adherence can be difficult due to the adverse GI effects. The current recommendation for treatment is to combine a cholinesterase inhibitor with an NMDA receptor antagonist to prevent adverse effects. Memantine, an NMDA receptor antagonist has been shown to significantly improve cognitive function and behavioral symptoms when compared to a placebo. It is also well tolerated with minimal adverse effects. The current recommendation for treatment is a combination of memantine and a cholinesterase inhibitor [32]. As with MCI, exercise has been shown to improve cognitive function and memory in patients with Alzheimer’s. Specifically, resistance training using bands and weights has been shown to have the most efficacy in treating Alzheimer’s [33]. A myriad of different treatment modalities for AD have been proposed, necessitating further analysis of each intervention in the early stages of disease onset. [34]. Early diagnosis is key in maximizing the potential benefits of these intervention options.
2.3. AD: Neurosurgical Management
2.3.1. Deep Brain Stimulation DBS
DBS has rarely been used in the treatment of dementia disorders due to a failed trial in 1984, but the opinions are changing due to a case study from 2008 [35,36,37]. A 50 year old man with a history of treatment-resistant obesity and normal cognitive function was referred for neurosurgical interventions to treat his eating disorder [35,38]. Electrodes were placed in his hypothalamus in 7 different regions [35,38]. Postoperatively, the patient reported sudden and sustained episodes of déjà vu, opening debate as to whether DBS stimulation of the hypothalamus can have effects on retrograde memory retrieval [35,36,39]. The patient was then subjected to the California Verbal Learning Test 12 months later with an improvement of baseline memory found [35]. Additionally, studies have been performed in rodents indicating stimulation of the memory circuits can lead to hippocampal neurogenesis as well as improve memory in mice with Rett Syndrome, a leading cause of cognitive decline in females [40,41]. As far as human trials regarding DBS and its use for AD, several prominent studies have been completed highlighting its potential [42]. One study completed on 6 AD patients with DBS devices implanted in their fornix/hypothalamus showed improvements in disease progression within 6-12 months [43]. However, a larger phase 2 study was completed in 2016 with 42 patients [44]. Although cerebral glucose metabolism was raised within these patients with the DBS device turned on, it did not result in any notable cognitive improvements at the 12 month mark [44].
2.3.2. Encapsulated Cell Biodelivery (ECB)
Cholinergic neurons that are largely factorial in the formation and retrieval of memories are dependent on nerve growth factor (NGF) to maintain the synaptic integrity [45]. NGF has long been linked to halting or even potentially reversing the cerebral atrophy seen in AD [46]. Interestingly, NGF cannot cross the BBB and therefore requires a targeted delivery to have any biological effect [47]. One open-label phase 1b dose escalation study with a 6 month duration was performed with 4 implants being placed in the basal forebrain of four separate patients showing that NGF was released in 13 of the 16 implants [47]. A separate study was completed with 6 patients over a 12 month period showing only 2 of 6 treated patients had elevated levels of nicotinic receptor binding by released NGF [48]. Granted elevated levels of NGF was detected in both studies, cognitive function was not mentioned necessitating further studies into the effectiveness of ECB in improving cognitive decline associated with AD.
2.3.3. Brain Computer Interface (BCI)
BCIs are currently used in paralyzed patients by analyzing brain waves and turning them into commands sent to devices designed to carry them out [49]. A similar ideology is being adapted to late stage AD patients who have lost the ability to communicate verbally [50]. Although this technological pursuit would be limited to “yes” and “no” answers tied to emotions detected by the BCI device, it will allow non-verbal AD patients to communicate in a way they would otherwise not be capable of [50]. No significant human studies have been completed to date, but BCI shows promise in the future advancements of technological interventions with late stage AD patients [50].
3. Parkinson’s Disease
PD (Figure 2) is a neurodegenerative disorder presenting with bradykinesia and the occurrence of rigidity, a resting tremor, or related symptoms. With an initial presentation of tremor, it advances gradually, subsequently showing rigidity and bradykinesia [51,52].
Chakraborty S, Aich S, Kim H-C. Detection of Parkinson’s Disease from 3T T1 Weighted MRI Scans Using 3D Convolutional Neural Network. Diagnostics. 2020; 10(6):402. https://doi.org/10.3390/diagnostics10060402
© 2020 The Authors. Diagnostics published by MDPI (Basel, Switzerland)
3.1. PD: Modifiable Risk Factors
Parkinson’s disease, like other forms of dementia, has many modifiable risk factors that affect the nature of the disease. Some of these factors include dyspepsia, exposure to pesticides, oils, metals, and general anesthesia [54]. Contrasting results have been found from numerous studies investigating the role of milk and dairy products in the development of Parkinson’s disease [54]. Certain drugs such as Beta-adrenoceptor antagonists have been indicated as risk factors for Parkinson’s development. In contrast to other forms of dementia, smoking cigarettes has been indicated as a protective factor on the development of Parkinson’s disease. Drinking coffee and taking moderate amounts of vitamin E have also been noted as having a protective effect on Parkinson’s disease development. Further studies are needed to investigate the relationship between physical activity, certain comorbidities, and alcohol intake on Parkinson’s disease due to conflicting results found in the literature.
3.2. PD: Management & Care
Previous literature has established that early treatment of PD is crucial in slowing both the progression and symptomatic manifestations of the disease. A mainstay for PD therapy is the combination drug Levodopa/Carbidopa. Levodopa is a precursor to dopamine that can be decarboxylated to dopamine. Carbidopa inhibits the decarboxylation of dopamine in the periphery and decreases the significant adverse effects [55]. Along with dopamine precursors, PD can be treated with dopamine agonists, monoamine oxidase inhibitors, or catechol-O-methyltransferase inhibitors. All of these medications are combined to synergistically increase the amount of dopamine in the CNS [56]. Targeted for the management of motor and non-motor symptoms, clinical trials have studied the efficacy of early intervention of PD using rasagiline, ropinirole, pramipexole, and rotigotine [57,58,59,60]. These agents demonstrate great benefit but have a noteworthy side effect profile, a dilemma that must be considered before initiating early treatment [61,62]. For this reason, optimization of treatment in PD is individual and balances effectiveness of medication regimens with the adverse effects of polypharmacy that can occur [56]. Other intervention options include exercise, physiotherapy, and speech therapy [63]. Deep brain stimulation of the subthalamic nucleus has also been shown to improve symptoms of PD for some patients who respond to the treatment [64].
3.3. PD: Neursurgical Intervention
3.3.1. Deep Brain Stimulation (DBS)
DBS has been used effectively in the treatment of PD for decades [65]. It was adopted initially as an alternative method to the available ablative procedures at the time [66]. The original target was the subthalamic nucleus, DBS has further expanded into several nuclei of the basal ganglia showing profound effectiveness in treating motor symptoms of PD [65,67]. Over 120,000 patients worldwide have been treated with a DBS device [66]. With that being said, the subthalamic nucleus remains as the primary target for DBS in PD showing its primary effects being in improving the resting tremor, but having little to no effect in the rigidity or akinesia [65,67]. One large misconception with the use of DBS for treatment of PD is that it is used as a solo treatment [68]. Although DBS has profound effects on its own, it is most effective when used in tandem with pharmacological treatments for PD [68]. Several studies have proven the efficacy of DBS in comparison to treatment with medication alone [69,70,71]. Collectively, they have shown improvements from as little as 20% to as great as complete resolution of individual symptoms such as camptocormia [71,72].
Although PD symptoms may appear ever-present, they can fluctuate from moment to moment necessitating the trained clinician to adjust the DBS output based on the changes of clinical presentation [73,74]. A new development and potential solution to this dilemma is adaptive DBS (aDBS), or closed-loop DBS, which allows for constant feedback and delivery of personalized precision for the best clinical outcome [73,75,76]. aDBS allows for the conservation of device battery and decreased stimulation when unnecessary in turn decreasing DBS-induced side effects [77].
3.3.2. Focused Ultrasound (FUS)
FUS is an emerging prospect for treatment of PD due to its noninvasive and precise nature [78]. The noninvasive aspect of FUS allows it to be an alternative method of treatment to DBS, needing less follow up appointments and being of significantly lower cost [79]. By targeting areas of the brain that can potentially lead to excitotoxicity associated with the development of PD, FUS is able to selectively ablate portions of the brain the smaller than a grain of rice [80]. One randomized trial involving 40 patients found the FUS subthalamatomy led to significant motor improvements in PD patients [81]. An additional double blinded, prospective, sham controlled study, improvements of 62% of treated patients compared to 22% of the sham group was observed [82]. The greatest improvements were seen in rigidity and tremor, with up to a 77% improvement in tremor at the 6-month post-op evaluation [82]. A separate study completed recorded 92% of treated patients had motor improvements at the 12 month evaluation. [83].Although remarkable improvements were seen in these studies, several adverse events were recorded including speech disturbances, dyskinesias, and gait disturbances [81,84,85].
3.3.3. Radiofrequency & Radiosurgery
Radiofrequency lesioning or radiosurgery is an alternative form of treating movement disorders such as PD [86]. Although not as popular likely due to its permanent side effects, it has similar effects to DBS treatment [86]. A common name for radiosurgery is the “gamma knife technique” and is effective at ablating deep brain structures but also not widespread due to limitation in technology allowing for visualization of the functional targets along with unacceptable complication rates [86,87]. Some common adverse events are edema, persistent ataxia, dysarthria, and motor/sensory deficits [88]. One study completed on the gamma knife technique found 31 of 33 treated PD patients to report an improvement in tremor with 23 of them having complete or nearly complete resolution of tremor [89]. The most common target utilizing the gamma knife is the globus pallidus internus [86,87,89,90,91].
3.3.4. Brain Computer Interface (BCI)
BCI in the treatment of PD patients is an emerging study to optimize DBS functionality [92]. Multiple case studies have been completed on the use of BCI in PD treatment. One case study on three PD patients was based upon a rehabilitation plan of 15 sessions, evaluating each patient on motor, neuropsychological and EEG testing [93]. EEG was of significant interest in this study due to its ability to drive a classic BCI system, which proved to show improvements in gait as well as overall mobility [93]. Two of the three patients also exhibited increased postural stability [93]. Despite being three patients, this study of BCIs points to a future of adaptive DBS treatment which can significantly improve the efficiency of technological treatment for patients with PD.
4. Lewy Body Dementia (LBD)
LBD (Figure 3) is a gradually progressing neurodegenerative disorder that displays aspects of both dementia and PD. Patient presentation will usually be in the form of initial cognitive decline, followed by visual hallucinations and motor signs [94]. Much like the diagnostic complexities encountered in cases of FTD, establishing a diagnosis of LBD can be challenging due to symptom overlap with other causes of dementia.
Chouliaras, L., O’Brien, J.T. The use of neuroimaging techniques in the early and differential diagnosis of dementia. Mol Psychiatry (2023). https://doi.org/10.1038/s41380-023-02215-8
© 2023 The Authors. Molecular Psychiatry published by Springer Nature Limited
4.1. LBD: Modifiable Risk Factors
Lewy Body dementia (LBD) shares some modifiable risk factors with other forms of dementia, while also having a few unique relationships. Depression, anxiety, and a history of stroke all have associations with an increased development of LBD [96]. Interestingly, studies have also found a relationship between oophorectomies before the age of 45 and an increased risk of LBD. When compared to Alzheimer’s disease, having a longer education has also been shown to increase one’s risk of developing LBD. Similarly to other forms of dementia, studies have found that caffeine, alcohol and cancer have varying degrees of protective effects on LBD.
4.2. LBD: Management & Care
The initial phase of LBD offers the most optimal time for intervention as it is when the disorder is most reactive to treatment [97]. LBD shares many symptoms with PD and for that reason, the medication management can be similar for both, but with some differences [98]. In PD levodopa/carbidopa is given as the first line medication, but in LBD it has only been shown to be effective in improving parkinsonian symptoms in one third of patients and has a high risk for psychosis [99]. Efficacy of early treatment of LBD has been demonstrated with Memantine, Olanzapine, and Yokukansan [100,101]. Donepezil has shown significant efficacy in the treatment of cognitive, behavioral, and global symptoms of LBD. It is typically safe and well tolerated [102].Donepezil is typically given with rivastigmine, which on its own has shown to be efficacious in the treatment of behavioral symptoms associated with LBD [103]. Modafinil has been shown to be effective in treatment of sleepiness that comes with LBD. Treatment of sleepiness is important because the extent of somnolence during the day correlates with worse dementia. [104]. In order for early intervention to occur and minimize adverse effects on the patient’s quality of life, early diagnosis of LBD is a core step in the management of the disorder.
4.3. LBD: Neursurgical Intervention
4.3.1. Deep Brain Stimulation (DBS)
Due to the difficulty of treating Lewy Body Dementia with medications alone, several techniques are being explored to advance the treatment options [105]. The nucleus basalis of Meynert is the primary target for device implantation [105,106]. A double blinded trial of six patients between the ages of 50-80 with the DBS electrodes placed in the nucleus basalis of Meynert [105]. Although surgery was well tolerated by all 6 patients, no consistent improvements were observed in clinical outcome measures but neuropsychiatric symptoms were reduced in 3 of the patients [105]. A systematic review on 11 trials was completed also alluding to the evidence of effectiveness not being robust but indicated the potential of future treatment of Lewy Body Dementia with DBS [106].
4.3.2. Transcranial Direct Current Stimulation (tDCS)
Transcranial direct current stimulation has been demonstrated to have cognitive benefits in healthy patients, opening the exploration of its effect in patients with Lewy Body Dementia [107]. Several studies have therefore been completed on its potential effect in Lewy Body Dementia [107,108,109]. Although all studies reported an improvement in attentional ability and motor symptoms, visuoperceptual symptoms along with hallucinations did not improve [107,108,109,110]. Significant improvements were also seen in mood, quality of life, and satisfaction [110]. Observed improvements declined over time leaving questions to be answered in future studies of tDCS in Lewy Body dementia [109].
4.3.3. Transcranial Magnetic Stimulation (TMS)
TMS has been proven to have a positive effect in several neurological disorders with pertinent use in the hallucinations of schizophrenia [111]. Because hallucinations, or otherwise referred to as phosphenes, are largely derived from the visual cortex, the occipital lobe is the primary target of treatment [112,113]. Studies completed have not led to conclusive evidence proving a sustained decrease in phosphene perception with the only notable improvement with treatment being of depression symptoms [112,113].
4.3.4. Electroconvulsive Therapy
Electroconclusive therapy has been observed to have positive outcomes with depression and agitation making it a potential candidate for Lewy Body Dementia treatment [114,115,116]. Several studies have been completed drawing the conclusion that electroconclusive therapy is effective in treating the psychotic symptoms associated with Lewy Body Dementia including depression, agitation, and aggression in patients treated [115,116]. However, it had no impact on cognitive impairment or motor symptoms [115,116].
5. Vascular Dementia (VD)
VD (Figure 5) is a subset of dementia characterized by cognitive impairment resulting from cerebrovascular disease such as the occurrence of stroke or small vessel disease. Disruptions in blood flow and oxygen supply to the brain can lead to deficits in memory, thinking, and executive function [117]. VD varies in its presentation based on the location and extent of vascular damage in the brain.
Helena Schmidt, Paul Freudenberger, Stephan Seiler, Reinhold Schmidt, Genetics of subcortical vascular dementia, Experimental Gerontology, Volume 47, Issue 11, 2012, Pages 873-877, ISSN 0531-5565, https://doi.org/10.1016/j.exger.2012.06.003.
© 2012 The Authors. Experimental Gerontology published by Elsevier Inc.
5.1. VD: Modifiable Risk Factors
Vascular dementia, as the name implies, shares many risk factors with vascular disease. Risk factors can be placed into four categories: stroke-related, genetic, demographic, and atherosclerotic [119]. Those that are modifiable include lower educational level, hypertension, cigarette smoking, myocardial infarction, diabetes mellitus, and hyperlipidemia. Metabolic syndrome has also been associated with increased risk of vascular dementia, a syndrome intertwined with some of the aforementioned risk factors [120]. Some studies have also investigated the relationship between adiponectin, a key regulator of cardiovascular disease and diabetes, and vascular dementia. Adiponectin’s ability to function as an antidiabetic and antiatherogenic regulator has been cited as grounds for further research into this molecule's role as a protective/risk factor for vascular dementia, depending on its quantity in the body.
5.2. VD: Management & Care
Management of vascular dementia begins with an early diagnosis because this helps provide effective management as soon as possible. There are not many treatment options for patients with vascular dementia, and of the treatment options that are available, they have shown only minor benefit [121]. A randomized control trial conducted in 2002 with 579 patients, tested the efficacy of 20mg of daily memantine vs a placebo in treatment for vascular dementia. After 28 weeks, the study found that memantine significantly improved cognition relative to the placebo, although it was only by a small extent [122]. The results of this study are supported by another 28-week randomized control trial of memantine use in vascular dementia. This study had 321 participants and similarly found that memantine significantly improved cognition when compared to a placebo but not by a large margin [123]. Other than memantine, the only drugs that have shown efficacy are cholinesterase inhibitors, although they also only provide a small benefit [121]. Lifestyle modifications have shown to improve cognition in patients with vascular dementia. The FINGER study conducted in 2015 wanted to compare different lifestyle interventions in 1260 patients. They found that diet, exercise, cognitive training, and control of vascular risk factors, all improved cognitive function in patients with vascular dementia when compared to a control group [124].
5.3. VD: Neursurgical Intervention
5.3.1. Brain Computer Interface (BCI)
BCI shows promise in the future of treating VD patients, specifically those who suffered from a stroke [125]. BCI technology can assist care providers to objectively assess the cognitive function of patients as well as cognitive function of patients suffering from VD [125]. One study of 14 basilar artery stroke patients showed sensorimotor rhythm neurofeedback training(SMR-NF) with BCI systems used positively affected memory functioning versus 14 patients that did not have BCI feedback [126]. A separate case study on a 70 year old female and 20 year old male who both suffered from strokes received SMR-NF and were found to have improved auditory and visuospatial memory along with shorter reaction times [127]. BCI shows significant potential in the recovery and management of stroke patients.
6. Modifiable Risk Factors and Care of Non-Surgically Managed Forms of Cognitive Impairment
6.1. Mild Cognitive Impairment (MCI)
MCI describes a degree of symptomatic cognitive decline not advanced to the level of dementia but with ample consequential impairments to warrant its own diagnosis. While Alzheimer's disease has traditionally received significant attention as the primary pathological factor underlying this intermediate stage of impairment, recent studies have implicated various other neurodegenerative conditions in the development of MCI. [128,129,130].
6.1.1. MCI: Modifiable Risk Factors
When identifying modifiable risk factors in the development of mild cognitive impairment (MCI), many similarities are shared between the various diseases that fall under the umbrella term of cognitive impairment and dementia. Therefore, risk factors for developing MCI are closely related to risk factors for the progression of MCI to various forms of dementia. One risk factor is the presence of comorbid disease, such as coronary heart disease and hypertension [131]. Metabolic syndrome has also been identified as a modifiable risk factor for progression of MCI to any form of dementia, however it has not been shown to be associated with an increased risk of developing MCI. Prediabetes, diabetes, and carotid stenosis have also been implicated as risk factors in the progression of MCI to dementia. Numerous other vascular disorders, such as cerebral small vessel disease have been shown to drastically increase the risk of developing MCI 4-times that of someone without the disease [24]. Depression, traumatic brain injury, sleep disturbances, lack of physical activity and poor diet all have implications in increasing the likelihood of progression of MCI to other forms of dementia.
6.1.2. MCI: Management & Care
Treatment for MCI is variable based on the patient’s medical history. It is critical in MCI treatment to identify if the patient’s symptoms are due to a reversible cause. Reversible causes of MCI like depression, obstructive sleep apnea, hypotension, hypothyroidism, and overmedication are treated best by treating the underlying pathology. Treatment in these cases can lead to full recovery of neurological function [132]. If MCI is due to a non-reversible cause, then treatment does not target full recovery, instead it is centered around slowing progression and symptom management [132]. One area for improvement is to focus on the patient’s comorbidities. Optimizing conditions like hypertension, hyperlipidemia, smoking, and diabetes has been shown to slow down the progression of MCI [133]. Despite no direct treatment for MCI, there is evidence suggesting the benefits of early intervention. Although the use of cholinesterase inhibitors for treatment of MCI has been theorized to slow down progression, the literature does not support this theory. A study conducted in 2007 showed that cholinesterase inhibitors were not effective in slowing degeneration, and the side effects were significant enough to discourage reckless use [134]. Alternatively, the use of conventional Chinese medicines has been indicated to support the delay of progression from MCI to Alzheimer’s disease in previous literature [135]. In regards to non-pharmaceutical treatment options, neuroimaging studies have illustrated augmented brain activity and memory with the use of cognitive training techniques [136,137,138]. Exercise is a treatment for MCI that has been growing in popularity do to its proven ability to improve memory and attention in adults with MCI [139]. One systematic review published in 2022 wanted to compare the efficacy of different forms of exercise for patients with MCI compared to patients with Alzheimer’s Disease. They found that although resistance training was the most effective in improving Alzheimer’s, a mixture of resistance and aerobic training showed the most efficacy when treating MCI [33]. BCI is an emerging technique in both the diagnosis and treatment of MCI. The key to effective BCI use resides within the identification of the biomarkers of MCI which can help for early detection and subsequent personalized treatment utilizing BCI techniques [140]. Further direct studies are needed to confirm the hypothesis, but BCI looks to be an underestimated technique in the management of MCI.
6.2. Frontotemporal Dementia (FTD)
FTD (Figure 4) manifests as deficits in behavior, language, and/or executive function [141]. Its presentation often goes unrecognized due to its overlap with various psychiatric conditions, making it increasingly important to distinguish this condition from other potential causes of cognitive decline such as AD.
Chandra, A., Dervenoulas, G., Politis, M. et al. Magnetic resonance imaging in Alzheimer’s disease and mild cognitive impairment. J Neurol 266, 1293–1302 (2019). https://doi.org/10.1007/s00415-018-9016-3
© 2019 The Authors. Frontiers in Neuroscience published by Frontiers Media S.A.
6.2.1. FTD: Modifiable Risk Factors
Identifying the risk modifiable risk factors for the development of frontotemporal dementia is of great importance since it has one of the highest prevalence rates of all forms of dementia in patients under 65 [142]. One independent modifiable risk factor for the development of frontotemporal dementia is type 2 diabetes. Smoking cigarettes and being overweight have also been found to be more common in those with early frontotemporal dementia. Head injuries, such as traumatic brain injury and injury with loss of consciousness, have also been shown to increase the risk of developing frontotemporal dementia. Hypertension and autoimmune disease have both been investigated as modifiable risk factors contributing to the development of frontotemporal dementia but have yielded conflicting results and therefore further research is necessary to elucidate these relationships.
6.2.2. FTD: Management & Care
Current literature does not suggest that patients with FTD would benefit from early diagnosis of their condition. The main point of target in treatment lies in managing the present symptoms, typically with off-label medications [143]. While patients may benefit from their use, they have not been shown to suppress the advancement of FTD and have not been sufficiently investigated to yield definitive support in favor of their use [144,145,146,147,148,149,150,151]. When trying to control symptoms in FTD, behavioral symptoms are a large target of pharmaceutical intervention. Trazadone, a selective serotonin reuptake inhibitor, has been shown to significantly improve behavioral symptoms in patients with FTD [152]. Quetiapine, an atypical antipsychotic, has been shown to improve the behavioral symptoms of FTD. When compared with other medication in the same class, Quetiapine has been shown to be just as effective but with less parkinsonian symptoms. Weight gain, falls, and cardiac events are still significant side effects of all atypical antipsychotics, especially in the elderly [153]. Cholinesterase inhibitors used in patients with FTD have been shown to have no effect on cognitive function, but have showed a worsening in behavioral symptoms, so they are not indicated [154].Memantine has also been tried in FTD. A randomized control trial published in 2013 showed that Memantine had no benefit, neither cognitively nor behaviorally, in patients with FTD and should be avoided [155].
7. Conclusions
In consideration of the impact of cognitive decline on the quality of life, understanding modifiable risk factors is an important component of disease prevention. The potential management options for these pathologies have expanded in recent decades, focally targeting relevant brain regions and neurotransmitter pathways in an attempt for symptom alleviation and the hindrance of disease progression. With a growing number of beneficial treatments available for varying etiologies of cognitive decline, early diagnosis and intervention may improve patient outcomes.
Author Contributions
Conceptualization, A.M. and B.L.; methodology, A.M., G.F., B.L..; validation, A.M., and B.L.; investigation, A.M., G.F., C.H., E.M., S.F., and B.L.; writing—original draft preparation, A.M., G.F., C.H., E.M., and S.F.; writing—review and editing, A.M., G.F., C.H., E.M., S.F., and B.L.; visualization, A.M., and B.L.; supervision, B.L.; project administration, A.M., and B.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- U. Nations, World Population Ageing 2020, 2020.
- Wang, S.; Zhang, J.; Liang, J.; Song, H.; Ji, X. Treatable causes of adult-onset rapid cognitive impairment. Clin. Neurol. Neurosurg. 2019, 187, 105575. [Google Scholar] [CrossRef] [PubMed]
- Chertkow, H. Diagnosis and treatment of dementia: Introduction. Introducing a series based on the Third Canadian Consensus Conference on the Diagnosis and Treatment of Dementia. Can. Med Assoc. J. 2007, 178, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Duff, K. Mild Cognitive Impairment and Dementia: Definitions, Diagnosis, and Treatment. Arch. Clin. Neuropsychol. 2014, 29, 691–692. [Google Scholar] [CrossRef]
- Spiegel, D.; Loewenstein, R.J.; Lewis-Fernández, R.; Sar, V.; Simeon, D.; Vermetten, E.; Cardeña, E.; Dell, P.F. Dissociative disorders in DSM-5. Depression Anxiety 2011, 28, 824–852. [Google Scholar] [CrossRef] [PubMed]
- Busse, A.; Angermeyer, M.C.; Riedel-Heller, S.G. Progression of mild cognitive impairment to dementia: a challenge to current thinking. Br. J. Psychiatry 2006, 189, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Ferencz, B.; Gerritsen, L. Genetics and Underlying Pathology of Dementia. Neuropsychol. Rev. 2015, 25, 113–124. [Google Scholar] [CrossRef] [PubMed]
- Aarsland, D. Epidemiology and Pathophysiology of Dementia-Related Psychosis. 2020, 81. 81. [CrossRef]
- Dening, T.; Sandilyan, M.B. Dementia: definitions and types. Nurs. Stand. 2015, 29, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Vahia, V.N. Diagnostic and statistical manual of mental disorders 5: A quick glance. Indian J. Psychiatry 2013, 55, 220–223. [Google Scholar] [CrossRef] [PubMed]
- Roh, J.H.; Lee, J.-H. Recent Updates on Subcortical Ischemic Vascular Dementia. J. Stroke 2014, 16, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Arevalo-Rodriguez, I.; Smailagic, N.; Roqué-Figuls, M.; Ciapponi, A.; Sanchez-Perez, E.; Giannakou, A.; Pedraza, O.L.; Cosp, X.B.; Cullum, S. Mini-Mental State Examination (MMSE) for the early detection of dementia in people with mild cognitive impairment (MCI). Emergencias 2021, 2021, CD010783. [Google Scholar] [CrossRef]
- Jack, C.R., Jr.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Dunn, B.; Haeberlein, S.B.; Holtzman, D.M.; Jagust, W.; Jessen, F.; Karlawish, J.; et al. NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. Alzheimer Dement. 2018, 14, 535–562. [Google Scholar] [CrossRef] [PubMed]
- Maki, Y.; Yamaguchi, H. Early detection of dementia in the community under a community-based integrated care system. Geriatr. Gerontol. Int. 2014. [Google Scholar] [CrossRef] [PubMed]
- Orgeta, V.; Mukadam, N.; Sommerlad, A.; Livingston, G. The Lancet Commission on Dementia Prevention, Intervention, and Care: a call for action. Ir. J. Psychol. Med. 2018, 36, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Carotenuto, A.; Traini, E.; Fasanaro, A.M.; Battineni, G.; Amenta, F. Tele-Neuropsychological Assessment of Alzheimer’s Disease. J. Pers. Med. 2021, 11, 688. [Google Scholar] [CrossRef] [PubMed]
- Battineni, G.; Hossain, M.A.; Chintalapudi, N.; Traini, E.; Dhulipalla, V.R.; Ramasamy, M.; Amenta, F. Improved Alzheimer’s Disease Detection by MRI Using Multimodal Machine Learning Algorithms. Diagnostics 2021, 11, 2103. [Google Scholar] [CrossRef] [PubMed]
- C.R. Jack Jr, D.A. C.R. Jack Jr, D.A. Bennett, K. Blennow, M.C. Carrillo, B. Dunn, S. Budd Haeberlein, D.M. Holtzman, W. Jagust, F. Jessen, J. Karlawish, E. Liu, J. Luis Molinuevo, T. Montine, C. Phelps, K.P. Rankin, C.C. Rowe, P. Scheltens, E. Siemers, H.M. Snyder, R. Sperling, A. Dement Author manuscript, NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease HHS Public Access Author manuscript, Alzheimers Dement 14 (2018).
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R., Jr.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer's disease: Recommendations from the National Institute on Aging-Alzheimer's association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. J. Alzheimers Assoc. 2011, 7, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Force, U.P.S.T.; Owens, D.K.; Davidson, K.W.; Krist, A.H.; Barry, M.J.; Cabana, M.; Caughey, A.B.; Doubeni, C.A.; Epling, J.W.; Kubik, M.; et al. Screening for Cognitive Impairment in Older Adults. JAMA 2020, 323, 757–763. [Google Scholar] [CrossRef]
- G. Joseph, J. G. Joseph, J. Bryan, J. Tricia, S. Ken, W. Jennifer, Alzheimer’s Association. 2016 Alzheimer’s Disease Facts and Figures, Alzheimer’s & Dimentia 12 (2016).
- Kumar, J. Sidhu, A. Goyal, J.W. Tsao, Alzheimer Disease, 2023.
- Chandra, A.; Dervenoulas, G.; Politis, M. Magnetic resonance imaging in Alzheimer's disease and mild cognitive impairment. J. Neurol. 2019, 266, 1293–1302. [Google Scholar] [CrossRef] [PubMed]
- Edwards, G.A.; Gamez, N., Jr.; Escobedo, G.; Calderon, O.; Moreno-Gonzalez, I. Modifiable Risk Factors for Alzheimer’s Disease. Front. Aging Neurosci. 2019, 11, 146. [Google Scholar] [CrossRef]
- Litke, R.; Garcharna, L.C.; Jiwani, S.; Neugroschl, J. Modifiable Risk Factors in Alzheimer Disease and Related Dementias: A Review. Clin. Ther. 2021, 43, 953–965. [Google Scholar] [CrossRef]
- Breijyeh, Z.; Karaman, R. Comprehensive Review on Alzheimer’s Disease: Causes and Treatment. Molecules 2020, 25, 5789. [Google Scholar] [CrossRef] [PubMed]
- Winblad, B.; Wimo, A.; Wetterholm, A.-L.; Haglund, A.; Engedal, K.; Soininen, H.; Verhey, F.; Waldemar, G.; Zhang, R.; Burger, L.; et al. 4.044 Long-term efficacy of donepezil in patients with mild to moderate Alzheimer's disease: Results from a one-year placebo-controlled study and two-year follow-up study. Eur. Neuropsychopharmacol. 2003, 13, S404. [Google Scholar] [CrossRef]
- Winblad, B.; Engedal, K.; Soininen, H.; Verhey, F.; Waldemar, G.; Wimo, A.; Wetterholm, A.-L.; Zhang, R.; Haglund, A.; Subbiah, P.; et al. A 1-year, randomized, placebo-controlled study of donepezil in patients with mild to moderate AD. Neurology 2001, 57, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Winblad, B.; Brodaty, H.; Gauthier, S.; Morris, J.C.; Orgogozo, J.; Rockwood, K.; Schneider, L.; Takeda, M.; Tariot, P.; Wilkinson, D. Pharmacotherapy of Alzheimer's disease: is there a need to redefine treatment success? Int. J. Geriatr. Psychiatry 2001, 16, 653–666. [Google Scholar] [CrossRef]
- Whitehead, A.; Perdomo, C.; Pratt, R.D.; Birks, J.; Wilcock, G.K.; Evans, J.G. Donepezil for the symptomatic treatment of patients with mild to moderate Alzheimer's disease: a meta-analysis of individual patient data from randomised controlled trials. Int. J. Geriatr. Psychiatry 2004, 19, 624–633. [Google Scholar] [CrossRef] [PubMed]
- Farlow, M.; Anand, R.; Jr, J.M.; Hartman, R.; Veach, J. A 52-Week Study of the Efficacy of Rivastigmine in Patients with Mild to Moderately Severe Alzheimer’s Disease. Eur. Neurol. 2000, 44, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Matsunaga, S.; Kishi, T.; Nomura, I.; Sakuma, K.; Okuya, M.; Ikuta, T.; Iwata, N. The efficacy and safety of memantine for the treatment of Alzheimer’s disease. Expert Opin. Drug Saf. 2018, 17, 1053–1061. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Zhao, X.; Li, B.; Cai, Y.; Zhang, S.; Wan, Q.; Yu, F. Comparative efficacy of various exercise interventions on cognitive function in patients with mild cognitive impairment or dementia: A systematic review and network meta-analysis. J. Sport Heal. Sci. 2021, 11, 212–223. [Google Scholar] [CrossRef] [PubMed]
- Chu, L.W. Alzheimer's disease: early diagnosis and treatment. Hong Kong Med. J. 2012, 18, 228–237. [Google Scholar] [PubMed]
- Hamani, C.; McAndrews, M.P.; Cohn, M.; Oh, M.; Zumsteg, D.; Shapiro, C.M.; Wennberg, R.A.; Lozano, A.M. Memory enhancement induced by hypothalamic/fornix deep brain stimulation. Ann. Neurol. 2008, 63, 119–123. [Google Scholar] [CrossRef]
- Bittlinger, M.; Müller, S. Opening the debate on deep brain stimulation for Alzheimer disease – a critical evaluation of rationale, shortcomings, and ethical justification. BMC Med Ethic- 2018, 19, 41. [Google Scholar] [CrossRef] [PubMed]
- Turnbull, I.; McGeer, P.; Beattie, L.; Calne, D.; Pate, B. Stimulation of the Basal Nucleus of Meynert in Senile Dementia of Alzheimer’s Type. Ster. Funct. Neurosurg. 1985, 48, 216–221. [Google Scholar] [CrossRef]
- Laxton, A.W.; Lozano, A.M. Deep Brain Stimulation for the Treatment of Alzheimer Disease and Dementias. World Neurosurg. 2013, 80, S28–e1. [Google Scholar] [CrossRef]
- Smith, G.S.; Laxton, A.W.; Tang-Wai, D.F.; McAndrews, M.P.; Diaconescu, A.O.; Workman, C.I.; Lozano, A.M. Increased Cerebral Metabolism After 1 Year of Deep Brain Stimulation in Alzheimer Disease. Arch. Neurol. 2012, 69, 1141–1148. [Google Scholar] [CrossRef]
- Lyketsos, C.G.; Holroyd, K.B.; Fosdick, L.; Smith, G.S.; Leoutsakos, J.-M.; Munro, C.; Oh, E.S.; Drake, K.; Rosenberg, P.B.; Anderson, W.S.; et al. Deep brain stimulation targeting the fornix for mild Alzheimer dementia: design of the ADvance randomized controlled trial. Open Access J. Clin. Trials 2015, 7, 63–76. [Google Scholar] [CrossRef]
- Hao, S.; Tang, B.; Wu, Z.; Ure, K.; Sun, Y.; Tao, H.; Gao, Y.; Patel, A.J.; Curry, D.J.; Samaco, R.C.; et al. Forniceal deep brain stimulation rescues hippocampal memory in Rett syndrome mice. Nature 2015, 526, 430–434. [Google Scholar] [CrossRef] [PubMed]
- Mirsaeedi-Farahani, K.; Halpern, C.H.; Baltuch, G.H.; Wolk, D.A.; Stein, S.C. Deep brain stimulation for Alzheimer disease: a decision and cost-effectiveness analysis. J. Neurol. 2015, 262, 1191–1197. [Google Scholar] [CrossRef] [PubMed]
- Laxton, A.W.; Tang-Wai, D.F.; McAndrews, M.P.; Zumsteg, D.; Wennberg, R.; Keren, R.; Wherrett, J.; Naglie, G.; Hamani, C.; Smith, G.S.; et al. A phase I trial of deep brain stimulation of memory circuits in Alzheimer's disease. Ann. Neurol. 2010, 68, 521–534. [Google Scholar] [CrossRef]
- Lozano, A.M.; Fosdick, L.; Chakravarty, M.M.; Leoutsakos, J.-M.; Munro, C.; Oh, E.; Drake, K.E.; Lyman, C.H.; Rosenberg, P.B.; Anderson, W.S.; et al. A Phase II Study of Fornix Deep Brain Stimulation in Mild Alzheimer’s Disease. J. Alzheimer's Dis. 2016, 54, 777–787. [Google Scholar] [CrossRef]
- Cuello, A.C.; Bruno, M.A.; Allard, S.; Leon, W.; Iulita, M.F. Cholinergic Involvement in Alzheimer’s Disease. A Link with NGF Maturation and Degradation. J. Mol. Neurosci. 2009, 40, 230–235. [Google Scholar] [CrossRef]
- Scott, S.A.; Crutcher, K.A. Nerve Growth Factor and Alzheimer's Disease. Prog. Neurobiol. 1994, 5, 179–212. [Google Scholar] [CrossRef] [PubMed]
- Eyjolfsdottir, H.; Eriksdotter, M.; Linderoth, B.; Lind, G.; Juliusson, B.; Kusk, P.; Almkvist, O.; Andreasen, N.; Blennow, K.; Ferreira, D.; et al. Targeted delivery of nerve growth factor to the cholinergic basal forebrain of Alzheimer’s disease patients: application of a second-generation encapsulated cell biodelivery device. Alzheimer's Res. Ther. 2016, 8, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Eriksdotter-Jönhagen, M.; Linderoth, B.; Lind, G.; Aladellie, L.; Almkvist, O.; Andreasen, N.; Blennow, K.; Bogdanovic, N.; Jelic, V.; Kadir, A.; et al. Encapsulated Cell Biodelivery of Nerve Growth Factor to the Basal Forebrain in Patients with Alzheimer’s Disease. Dement. Geriatr. Cogn. Disord. 2012, 33, 18–28. [Google Scholar] [CrossRef] [PubMed]
- Shih, J.J.; Krusienski, D.J.; Wolpaw, J.R. Brain-Computer Interfaces in Medicine. Mayo Clin. Proc. 2012, 87, 268–279. [Google Scholar] [CrossRef] [PubMed]
- Liberati, G.; da Rocha, J.L.D.; van der Heiden, L.; Raffone, A.; Birbaumer, N.; Belardinelli, M.O.; Sitaram, R. Toward a Brain-Computer Interface for Alzheimer's Disease Patients by Combining Classical Conditioning and Brain State Classification. J. Alzheimer's Dis. 2012, 31, S211–S220. [Google Scholar] [CrossRef] [PubMed]
- S. Zafar, S.S. S. Zafar, S.S. Yaddanapudi, Parkinson Disease, 2023.
- Alexoudi, A.; Alexoudi, I.; Gatzonis, S. Parkinson's disease pathogenesis, evolution and alternative pathways: A review. Rev. Neurol. 2018, 174, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, S.; Aich, S.; Kim, H.-C. Detection of Parkinson’s Disease from 3T T1 Weighted MRI Scans Using 3D Convolutional Neural Network. Diagnostics 2020, 10, 402. [Google Scholar] [CrossRef] [PubMed]
- Belvisi, D.; Pellicciari, R.; Fabbrini, G.; Tinazzi, M.; Berardelli, A.; Defazio, G. Modifiable risk and protective factors in disease development, progression and clinical subtypes of Parkinson's disease: What do prospective studies suggest? Neurobiol. Dis. 2019, 134, 104671. [Google Scholar] [CrossRef]
- Greig, S.L.; McKeage, K. Carbidopa/Levodopa ER Capsules (Rytary®, Numient™): A Review in Parkinson’s Disease. CNS Drugs 2015, 30, 79–90. [Google Scholar] [CrossRef]
- Cacabelos, R. Parkinson’s Disease: From Pathogenesis to Pharmacogenomics. Int. J. Mol. Sci. 2017, 18, 551. [Google Scholar] [CrossRef]
- Iida, M.; Miyazaki, I.; Tanaka, K.-I.; Kabuto, H.; Iwata-Ichikawa, E.; Ogawa, N. Dopamine D2 receptor-mediated antioxidant and neuroprotective effects of ropinirole, a dopamine agonist. Brain Res. 1999, 838, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Scheller, D.; Stichel-Gunkel, C.; Lübbert, H.; Porras, G.; Ravenscroft, P.; Hill, M.; Bezard, E. Neuroprotective effects of rotigotine in the acute MPTP-lesioned mouse model of Parkinson's disease. Neurosci. Lett. 2008, 432, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Guo, Y.; Xie, W.; Li, X.; Janokovic, J.; Le, W. Neuroprotection of Pramipexole in UPS Impairment Induced Animal Model of Parkinson’s Disease. Neurochem. Res. 2010, 35, 1546–1556. [Google Scholar] [CrossRef] [PubMed]
- Olanow, C.W.; Hauser, R.A.; Jankovic, J.; Langston, W.; Lang, A.; Poewe, W.; Tolosa, E.; Stocchi, F.; Melamed, E.; Eyal, E.; et al. A randomized, double-blind, placebo-controlled, delayed start study to assess rasagiline as a disease modifying therapy in Parkinson's disease (the ADAGIO study): Rationale, design, and baseline characteristics. Mov. Disord. 2008, 23, 2194–2201. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Bi, Z.; Liu, J.; Si, W.; Shi, Q.; Xue, L.; Bai, J. Adverse effects produced by different drugs used in the treatment of Parkinson's disease: A mixed treatment comparison. CNS Neurosci. Ther. 2017, 23, 827–842. [Google Scholar] [CrossRef]
- Chou, K.L. Adverse Events from the Treatment of Parkinson's Disease. Neurol. Clin. 2008, 26, 65–83. [Google Scholar] [CrossRef] [PubMed]
- Murman, D.L. Early Treatment of Parkinson's Disease: Opportunities for Managed Care. 2012, 18, S183–S188.
- Dayal, V.; Limousin, P.; Foltynie, T. Subthalamic Nucleus Deep Brain Stimulation in Parkinson’s Disease: The Effect of Varying Stimulation Parameters. J. Park. Dis. 2017, 7, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Hariz, M.; Blomstedt, P. Deep brain stimulation for Parkinson's disease. J. Intern. Med. 2022, 292, 764–778. [Google Scholar] [CrossRef] [PubMed]
- Hamani, C.; Florence, G.; Heinsen, H.; Plantinga, B.R.; Temel, Y.; Uludag, K.; Alho, E.; Teixeira, M.J.; Amaro, E.; Fonoff, E.T. Subthalamic Nucleus Deep Brain Stimulation: Basic Concepts and Novel Perspectives. eneuro 2017, 4. [Google Scholar] [CrossRef]
- Malek, N. Deep Brain Stimulation in Parkinson's Disease. Neurol. India 2019, 67, 968–978. [Google Scholar] [CrossRef]
- Fang, J.Y.; Tolleson, C. The role of deep brain stimulation in Parkinson’s disease: an overview and update on new developments. Neuropsychiatr. Dis. Treat. 2017, ume 13, 723–732. [Google Scholar] [CrossRef]
- Deuschl, G.; Follett, K.A.; Luo, P.; Rau, J.; Weaver, F.M.; Paschen, S.; Steigerwald, F.; Tonder, L.; Stoker, V.; Reda, D.J. Comparing two randomized deep brain stimulation trials for Parkinson’s disease. J. Neurosurg. 2020, 132, 1376–1384. [Google Scholar] [CrossRef]
- Engelhardt, J.; Caire, F.; Damon-Perrière, N.; Guehl, D.; Branchard, O.; Auzou, N.; Tison, F.; Meissner, W.G.; Krim, E.; Bannier, S.; et al. A Phase 2 Randomized Trial of Asleep versus Awake Subthalamic Nucleus Deep Brain Stimulation for Parkinson’s Disease. Ster. Funct. Neurosurg. 2020, 99, 230–240. [Google Scholar] [CrossRef] [PubMed]
- Liang, S.; Yu, Y.; Li, H.; Wang, Y.; Cheng, Y.; Yang, H. The Study of Subthalamic Deep Brain Stimulation for Parkinson Disease-Associated Camptocormia. Med Sci. Monit. 2020, 26, e919682–1. [Google Scholar] [CrossRef]
- Papapetropoulos, S. A Randomized Trial of Deep-Brain Stimulation for Parkinson's Disease. Yearb. Neurol. Neurosurg. 2008, 2008, 73–75. [Google Scholar] [CrossRef]
- Swann, N.C.; de Hemptinne, C.; Thompson, M.C.; Miocinovic, S.; Miller, A.M.; Gilron, R.; Ostrem, J.L.; Chizeck, H.J.; A Starr, P. Adaptive deep brain stimulation for Parkinson’s disease using motor cortex sensing. J. Neural Eng. 2018, 15, 046006–046006. [Google Scholar] [CrossRef] [PubMed]
- Beudel, M.; Brown, P. Adaptive deep brain stimulation in Parkinson's disease. Park. Relat. Disord. 2015, 22, S123–S126. [Google Scholar] [CrossRef]
- Neumann, W.; Gilron, R.; Little, S.; Tinkhauser, G. Adaptive Deep Brain Stimulation: From Experimental Evidence Toward Practical Implementation. Mov. Disord. 2023, 38, 937–948. [Google Scholar] [CrossRef] [PubMed]
- Habets, J.G.; Heijmans, M.; Kuijf, M.L.; Janssen, M.L.; Temel, Y.; Kubben, P.L. An update on adaptive deep brain stimulation in Parkinson's disease. Mov. Disord. 2018, 33, 1834–1843. [Google Scholar] [CrossRef]
- Castaño-Candamil, S.; Ferleger, B.I.; Haddock, A.; Cooper, S.S.; Herron, J.; Ko, A.; Chizeck, H.J.; Tangermann, M. A Pilot Study on Data-Driven Adaptive Deep Brain Stimulation in Chronically Implanted Essential Tremor Patients. Front. Hum. Neurosci. 2020, 14. [Google Scholar] [CrossRef]
- Lee, K.S.; Clennell, B.; Steward, T.G.J.; Gialeli, A.; Cordero-Llana, O.; Whitcomb, D.J. Focused Ultrasound Stimulation as a Neuromodulatory Tool for Parkinson’s Disease: A Scoping Review. Brain Sci. 2022, 12, 289. [Google Scholar] [CrossRef]
- Jung, N.Y.; Park, C.K.; Kim, M.; Lee, P.H.; Sohn, Y.H.; Chang, J.W. The efficacy and limits of magnetic resonance–guided focused ultrasound pallidotomy for Parkinson’s disease: a Phase I clinical trial. J. Neurosurg. 2019, 130, 1853–1861. [Google Scholar] [CrossRef]
- Eisenberg, H.M.; Krishna, V.; Elias, W.J.; Cosgrove, G.R.; Gandhi, D.; Aldrich, C.E.; Fishman, P.S. MR-guided focused ultrasound pallidotomy for Parkinson’s disease: safety and feasibility. J. Neurosurg. 2021, 135, 792–798. [Google Scholar] [CrossRef]
- Martínez-Fernández, R.; Máñez-Miró, J.U.; Rodríguez-Rojas, R.; del Álamo, M.; Shah, B.B.; Hernández-Fernández, F.; Pineda-Pardo, J.A.; Monje, M.H.; Fernández-Rodríguez, B.; Sperling, S.A.; et al. Randomized Trial of Focused Ultrasound Subthalamotomy for Parkinson’s Disease. New Engl. J. Med. 2020, 383, 2501–2513. [Google Scholar] [CrossRef]
- Moosa, S.; Martínez-Fernández, R.; Elias, W.J.; del Alamo, M.; Eisenberg, H.M.; Fishman, P.S. The role of high-intensity focused ultrasound as a symptomatic treatment for Parkinson's disease. Mov. Disord. 2019, 34, 1243–1251. [Google Scholar] [CrossRef]
- Fernández, R.M.; Villalba, E.N.; Rodriguez-Rojas, R.; del Álamo, M.; A Pineda-Pardo, J.; Obeso, I.; Mata-Marín, D.; Guida, P.; Jimenez-Castellanos, T.; Pérez-Bueno, D.; et al. Unilateral focused ultrasound subthalamotomy in early Parkinson’s disease: a pilot study. J. Neurol. Neurosurg. Psychiatry 2023, 95, 206–213. [Google Scholar] [CrossRef]
- Martínez-Fernández, R.; Rodríguez-Rojas, R.; del Álamo, M.; Hernández-Fernández, F.; A Pineda-Pardo, J.; Dileone, M.; Alonso-Frech, F.; Foffani, G.; Obeso, I.; Gasca-Salas, C.; et al. Focused ultrasound subthalamotomy in patients with asymmetric Parkinson's disease: a pilot study. Lancet Neurol. 2018, 17, 54–63. [Google Scholar] [CrossRef]
- Foffani, G.; Trigo-Damas, I.; Pineda-Pardo, J.A.; Blesa, J.; Rodríguez-Rojas, R.; Martínez-Fernández, R.; Obeso, J.A. Focused ultrasound in Parkinson's disease: A twofold path toward disease modification. Mov. Disord. 2019, 34, 1262–1273. [Google Scholar] [CrossRef]
- Horisawa, S.; Taira, T. [Radiofrequency Lesioning Surgery for Movement Disorders]. 2021, 49, 838–845. [Google Scholar] [CrossRef] [PubMed]
- Higuchi, Y.; Matsuda, S.; Serizawa, T. Gamma knife radiosurgery in movement disorders: Indications and limitations. Mov. Disord. 2016, 32, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Franzini, A.; Moosa, S.; Servello, D.; Small, I.; DiMeco, F.; Xu, Z.; Elias, W.J.; Franzini, A.; Prada, F. Ablative brain surgery: an overview. Int. J. Hyperth. 2019, 36, 64–80. [Google Scholar] [CrossRef]
- Raju, S.S.; Niranjan, A.; Iii, E.A.M.; Flickinger, J.C.; Lunsford, L.D. Stereotactic Radiosurgery for Intractable Tremor-Dominant Parkinson Disease: A Retrospective Analysis. Ster. Funct. Neurosurg. 2017, 95, 291–297. [Google Scholar] [CrossRef]
- Altinel, Y.; Alkhalfan, F.; Qiao, N.; Velimirovic, M. Outcomes in Lesion Surgery versus Deep Brain Stimulation in Patients with Tremor: A Systematic Review and Meta-Analysis. World Neurosurg. 2018, 123, 443–452. [Google Scholar] [CrossRef]
- Ravikumar, V.K.; Parker, J.J.; Hornbeck, T.S.; Santini, V.E.; Pauly, K.B.; Wintermark, M.; Ghanouni, P.; Stein, S.C.; Halpern, C.H. Cost-effectiveness of focused ultrasound, radiosurgery, and DBS for essential tremor. Mov. Disord. 2017, 32, 1165–1173. [Google Scholar] [CrossRef]
- Little, S.; Pogosyan, A.; Neal, S.; Zavala, B.; Zrinzo, L.; Hariz, M.; Foltynie, T.; Limousin, P.; Ashkan, K.; FitzGerald, J.; et al. Adaptive deep brain stimulation in advanced Parkinson disease. Ann. Neurol. 2013, 74, 449–457. [Google Scholar] [CrossRef]
- M.M. Turconi, S. M.M. Turconi, S. Mezzarobba, G. Franco, P. Busan, E. Fornasa, J. Jarmolowska, A. Accardo, P.P. Battaglini, BCI-Based Neuro-Rehabilitation Treatment for Parkinson ’ s Disease : Cases Report, in: TSPC2014 - November, 28th - T11, 2014: pp. 63–65.
- Chin, K.S.; Teodorczuk, A.; Watson, R. Dementia with Lewy bodies: Challenges in the diagnosis and management. Aust. New Zealand J. Psychiatry 2019, 53, 291–303. [Google Scholar] [CrossRef]
- Chouliaras, L.; O’brien, J.T. The use of neuroimaging techniques in the early and differential diagnosis of dementia. Mol. Psychiatry 2023, 28, 4084–4097. [Google Scholar] [CrossRef]
- Boot, B.P.; Orr, C.F.; Ahlskog, J.E.; Ferman, T.J.; Roberts, R.; Pankratz, V.S.; Dickson, D.W.; Parisi, J.; Aakre, J.A.; Geda, Y.E.; et al. Risk factors for dementia with Lewy bodies. Neurology 2013, 81, 833–840. [Google Scholar] [CrossRef]
- R.R. Tampi, J.J. R.R. Tampi, J.J. Young, D. Tampi, Behavioral symptomatology and psychopharmacology of Lewy body dementia, in: 2019: pp. 59–70. [CrossRef]
- Taylor, J.-P.; McKeith, I.G.; Burn, D.J.; Boeve, B.F.; Weintraub, D.; Bamford, C.; Allan, L.M.; Thomas, A.J.; O'Brien, J.T. New evidence on the management of Lewy body dementia. Lancet Neurol. 2019, 19, 157–169. [Google Scholar] [CrossRef] [PubMed]
- Molloy, S.; McKeith, I.G.; O’brien, J.T.; Burn, D.J. The role of levodopa in the management of dementia with Lewy bodies. J. Neurol. Neurosurg. Psychiatry 2005, 76, 1200–1203. [Google Scholar] [CrossRef] [PubMed]
- Watts, K.E.; Storr, N.J.; Barr, P.G.; Rajkumar, A.P. Systematic review of pharmacological interventions for people with Lewy body dementia. Aging Ment. Heal. 2022, 27, 203–216. [Google Scholar] [CrossRef] [PubMed]
- Vanhaute, H.; Persoons, P. [Early use of memantine in the treatment of Lewy body dementia]. . 2016, 58, 814–817. [Google Scholar]
- Mori, E.; Ikeda, M.; Kosaka, K. ; on behalf of the Donepezil-DLB Study Investigators Donepezil for dementia with Lewy bodies: A randomized, placebo-controlled trial. Ann. Neurol. 2012, 72, 41–52. [Google Scholar] [CrossRef] [PubMed]
- McKeith, I.; Del Ser, T.; Spano, P.; Emre, M.; Wesnes, K.; Anand, R.; Cicin-Sain, A.; Ferrara, R.; Spiegel, R. Efficacy of rivastigmine in dementia with Lewy bodies: a randomised, double-blind, placebo-controlled international study. Lancet 2000, 356, 2031–2036. [Google Scholar] [CrossRef] [PubMed]
- Varanese, S.; Perfetti, B.; Gilbert-Wolf, R.; Thomas, A.; Onofrj, M.; Di Rocco, A. Modafinil and armodafinil improve attention and global mental status in Lewy bodies disorders: preliminary evidence. Int. J. Geriatr. Psychiatry 2013, 28, 1095–1097. [Google Scholar] [CrossRef] [PubMed]
- Gratwicke, J.; Zrinzo, L.; Kahan, J.; Peters, A.; Brechany, U.; McNichol, A.; Beigi, M.; Akram, H.; Hyam, J.; Oswal, A.; et al. Bilateral nucleus basalis of Meynert deep brain stimulation for dementia with Lewy bodies: A randomised clinical trial. Brain Stimul. 2020, 13, 1031–1039. [Google Scholar] [CrossRef] [PubMed]
- Morrin, H.; Fang, T.; Servant, D.; Aarsland, D.; Rajkumar, A.P. Systematic review of the efficacy of non-pharmacological interventions in people with Lewy body dementia. Int. Psychogeriatrics 2017, 30, 395–407. [Google Scholar] [CrossRef] [PubMed]
- Elder, G.J.; Firbank, M.J.; Kumar, H.; Chatterjee, P.; Chakraborty, T.; Dutt, A.; Taylor, J.-P. Effects of transcranial direct current stimulation upon attention and visuoperceptual function in Lewy body dementia: a preliminary study. Int. Psychogeriatrics 2015, 28, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Elder, G.J.; Colloby, S.J.; Firbank, M.J.; McKeith, I.G.; Taylor, J.-P. Consecutive sessions of transcranial direct current stimulation do not remediate visual hallucinations in Lewy body dementia: a randomised controlled trial. Alzheimer's Res. Ther. 2019, 11, 1–13. [Google Scholar] [CrossRef]
- Wang, C.S.-M.; Cheng, K.-S.; Tang, C.-H.; Hou, N.-T.; Chien, P.-F.; Huang, Y.-C. 419 - Effect of Transcranial Direct Current Stimulation (tDCS) in Dementia with Lewy Bodies. Int. Psychogeriatrics 2021, 33, 41–42. [Google Scholar] [CrossRef]
- Guidi, L.; Evangelisti, S.; Siniscalco, A.; Lodi, R.; Tonon, C.; Mitolo, M. Non-Pharmacological Treatments in Lewy Body Disease: A Systematic Review. Dement. Geriatr. Cogn. Disord. 2023, 52, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.; Liu, K.; Guo, L. Repetitive transcranial magnetic stimulation (rTMS): A possible novel therapeutic approach to dementia with Lewy bodies. Med Hypotheses 2010, 74, 877–879. [Google Scholar] [CrossRef] [PubMed]
- Antczak, J.; Rusin, G.; Słowik, A. Transcranial Magnetic Stimulation as a Diagnostic and Therapeutic Tool in Various Types of Dementia. J. Clin. Med. 2021, 10, 2875. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.-P.; Firbank, M.; Barnett, N.; Pearce, S.; Livingstone, A.; Mosimann, U.; Eyre, J.; McKeith, I.G.; O'Brien, J.T. Visual hallucinations in dementia with Lewy bodies: transcranial magnetic stimulation study. Br. J. Psychiatry 2011, 199, 492–500. [Google Scholar] [CrossRef] [PubMed]
- Kirov, G.; Jauhar, S.; Sienaert, P.; Kellner, C.H.; McLoughlin, D.M. Electroconvulsive therapy for depression: 80 years of progress. Br. J. Psychiatry 2021, 219, 594–597. [Google Scholar] [CrossRef] [PubMed]
- Fukatsu, T.; Kanemoto, K. Electroconvulsive therapy improves psychotic symptoms in patients with dementia with Lewy bodies. Int. J. Geriatr. Psychiatry 2022, 37. [Google Scholar] [CrossRef] [PubMed]
- Echeverria, C.; Libuy, J.; Alarcón, J.; Rodriguez, J. ELECTROCONVULSIVE THERAPY FOR AGITATION IN LEWY BODIES DEMENTIA. Eur. Psychiatry 2023, 66, S1020–S1021. [Google Scholar] [CrossRef]
- Smith, E.E. Clinical presentations and epidemiology of vascular dementia. Clin. Sci. 2017, 131, 1059–1068. [Google Scholar] [CrossRef]
- Schmidt, H.; Freudenberger, P.; Seiler, S.; Schmidt, R. Genetics of subcortical vascular dementia. Exp. Gerontol. 2012, 47, 873–877. [Google Scholar] [CrossRef]
- Gorelick, P.B. Risk Factors for Vascular Dementia and Alzheimer Disease. Stroke 2004, 35, 2620–2622. [Google Scholar] [CrossRef]
- Song, J.; Lee, W.T.; Park, K.A.; Lee, J.E. Association between Risk Factors for Vascular Dementia and Adiponectin. BioMed Res. Int. 2014, 2014, 1–13. [Google Scholar] [CrossRef]
- O'Brien, J.T.; Thomas, A. Vascular dementia. Lancet 2015, 386, 1698–1706. [Google Scholar] [CrossRef] [PubMed]
- Wilcock, G.; Möbius, H.; Stöffler, A. A double-blind, placebo-controlled multicentre study of memantine in mild to moderate vascular dementia (MMM500). Int. Clin. Psychopharmacol. 2002, 17, 297–305. [Google Scholar] [CrossRef]
- Orgogozo, J.-M.; Rigaud, A.-S.; Stöffler, A.; Möbius, H.-J.; Forette, F. Efficacy and Safety of Memantine in Patients With Mild to Moderate Vascular Dementia. Stroke 2002, 33, 1834–1839. [Google Scholar] [CrossRef]
- Ngandu, T.; Lehtisalo, J.; Solomon, A.; Levälahti, E.; Ahtiluoto, S.; Antikainen, R.; Bäckman, L.; Hänninen, T.; Jula, A.; Laatikainen, T.; et al. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): A randomised controlled trial. Lancet 2015, 385, 2255–2263. [Google Scholar] [CrossRef]
- Sun, X.; Li, M.; Li, Q.; Yin, H.; Jiang, X.; Li, H.; Sun, Z.; Yang, T. Poststroke Cognitive Impairment Research Progress on Application of Brain-Computer Interface. BioMed Res. Int. 2022, 2022, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Lyukmanov, R.K.; Aziatskaya, G.A.; Mokienko, O.A.; Varako, N.A.; Kovyazina, M.S.; Suponeva, N.A.; Chernikova, L.A.; Frolov, A.A.; Piradov, M.A. Post-stroke rehabilitation training with a brain-computer interface: a clinical and neuropsychological study. Zhurnal Nevrol. i psikhiatrii im. S.S. Korsakova 2018, 118, 43–51. [Google Scholar] [CrossRef]
- Quek, S.Y.; Lee, T.-S.; Goh, S.J.A.; Phillips, R.; Guan, C.; Cheung, Y.B.; Feng, L.; Wang, C.C.; Chin, Z.Y.; Zhang, H.H.; et al. A pilot randomized controlled trial using EEG-based brain–computer interface training for a Chinese-speaking group of healthy elderly. Clin. Interv. Aging 2015, 10, 217–227. [Google Scholar] [CrossRef]
- Gorelick, P.B.; Scuteri, A.; Black, S.E.; DeCarli, C.; Greenberg, S.M.; Iadecola, C.; Launer, L.J.; Laurent, S.; Lopez, O.L.; Nyenhuis, D.; et al. Vascular Contributions to Cognitive Impairment and Dementia. Stroke 2011, 42, 2672–2713. [Google Scholar] [CrossRef] [PubMed]
- McKeith, I.G.; Ferman, T.J.; Thomas, A.J.; Blanc, F.; Boeve, B.F.; Fujishiro, H.; Kantarci, K.; Muscio, C.; O'Brien, J.T.; Postuma, R.B.; et al. Research criteria for the diagnosis of prodromal dementia with Lewy bodies. Neurology 2020, 94, 743–755. [Google Scholar] [CrossRef]
- Litvan, I.; Goldman, J.G.; Tröster, A.I.; Schmand, B.A.; Weintraub, D.; Petersen, R.C.; Mollenhauer, B.; Adler, C.H.; Marder, K.; Williams-Gray, C.H.; et al. Diagnostic criteria for mild cognitive impairment in Parkinson's disease: Movement Disorder Society Task Force guidelines. Mov. Disord. 2012, 27, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Campbell, N.L.; Unverzagt, F.; LaMantia, M.A.; Khan, B.A.; Boustani, M.A. Risk Factors for the Progression of Mild Cognitive Impairment to Dementia. Clin. Geriatr. Med. 2013, 29, 873–893. [Google Scholar] [CrossRef] [PubMed]
- Sanford, A.M. Mild Cognitive Impairment. Clin. Geriatr. Med. 2017, 33, 325–337. [Google Scholar] [CrossRef] [PubMed]
- Ganguli, M.; Fu, B.; Snitz, B.E.; Hughes, T.F.; Chang, C.-C.H. Mild cognitive impairment. Neurology 2013, 80, 2112–2120. [Google Scholar] [CrossRef] [PubMed]
- Raschetti, R.; Albanese, E.; Vanacore, N.; Maggini, M. Cholinesterase Inhibitors in Mild Cognitive Impairment: A Systematic Review of Randomised Trials. PLOS Med. 2007, 4, e338. [Google Scholar] [CrossRef] [PubMed]
- Belleville, S.; Clément, F.; Mellah, S.; Gilbert, B.; Fontaine, F.; Gauthier, S. Training-related brain plasticity in subjects at risk of developing Alzheimer’s disease. Brain 2011, 134, 1623–1634. [Google Scholar] [CrossRef] [PubMed]
- Zhong, J.; Tian, J.-Z.; Zhu, A.-H.; Yang, C.-Z. [Clinical study on a randomized, double-blind control of Shenwu gelatin capsule in treatment of mild cognitive impairment]. . 2007, 32, 1800–3. [Google Scholar] [PubMed]
- Gates, N.J.; Sachdev, P.S.; Singh, M.A.F.; Valenzuela, M. Cognitive and memory training in adults at risk of dementia: A Systematic Review. BMC Geriatr. 2011, 11, 55. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Li, J.; Li, N.; Li, B.; Wang, P.; Zhou, T. Cognitive intervention for persons with mild cognitive impairment: A meta-analysis. Ageing Res. Rev. 2011, 10, 285–296. [Google Scholar] [CrossRef]
- Li, H.; Su, W.; Dang, H.; Han, K.; Lu, H.; Yue, S.; Zhang, H. Exercise Training for Mild Cognitive Impairment Adults Older Than 60: A Systematic Review and Meta-Analysis. J. Alzheimer's Dis. 2022, 88, 1263–1278. [Google Scholar] [CrossRef]
- Chen, X.; Huang, Y.; Zhuang, S. Current Perspective of Brain-Computer Interface Technology on Mild Cognitive Impairment. Highlights Sci. Eng. Technol. 2023, 36, 73–78. [Google Scholar] [CrossRef]
- Puppala, G.K.; Gorthi, S.P.; Chandran, V.; Gundabolu, G. Frontotemporal Dementia - Current Concepts. 2021, 69, 1144–1152. [CrossRef]
- Eid, H.R.; Rosness, T.A.; Bosnes, O.; Salvesen. ; Knutli, M.; Stordal, E. Smoking and Obesity as Risk Factors in Frontotemporal Dementia and Alzheimer’s Disease: The HUNT Study. Dement. Geriatr. Cogn. Disord. Extra 2019, 9, 1–10. [Google Scholar] [CrossRef]
- Tsai, R.M.; Boxer, A.L. Treatment of frontotemporal dementia. Curr. Treat. Options Neurol. 2014, 16, 319–319. [Google Scholar] [CrossRef] [PubMed]
- Liepelt, I.; Gaenslen, A.; Godau, J.; Di Santo, A.; Schweitzer, K.J.; Gasser, T.; Berg, D. Rivastigmine for the treatment of dementia in patients with progressive supranuclear palsy: Clinical observations as a basis for power calculations and safety analysis. Alzheimer's Dement. 2010, 6, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Litvan, I.; Phipps, M.; Pharr, V.L.; Hallett, M.; Grafman, J.; Salazar, A. Randomized placebo-controlled trial of donepezil in patients with progressive supranuclear palsy. Neurology 2001, 57, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Fabbrini, G.; Barbanti, P.; Bonifati, V.; Colosimo, C.; Gasparini, M.; Vanacore, N.; Meco, G. Donepezil in the treatment of progressive supranuclear palsy. Acta Neurol. Scand. 2001, 103, 123–125. [Google Scholar] [CrossRef] [PubMed]
- Litvan, I.; Med, C.G.; Atack, J.R.; Gillespie, M.; Kask, A.M.; Mouradian, M.M.; Chase, T.N. Physostigmine treatment of progressive supranuclear palsy. Ann. Neurol. 1989, 26, 404–407. [Google Scholar] [CrossRef] [PubMed]
- Kimura, T.; Takamatsu, J. Pilot study of pharmacological treatment for frontotemporal dementia: Risk of donepezil treatment for behavioral and psychological symptoms. Geriatr. Gerontol. Int. 2013, 13, 506–507. [Google Scholar] [CrossRef] [PubMed]
- Mendez, M.F.; Shapira, J.S.; McMurtray, A.; Licht, E. Preliminary Findings: Behavioral Worsening on Donepezil in Patients With Frontotemporal Dementia. Am. J. Geriatr. Psychiatry 2007, 15, 84–87. [Google Scholar] [CrossRef]
- Kertesz, A.; Morlog, D.; Light, M.; Blair, M.; Davidson, W.; Jesso, S.; Brashear, R. Galantamine in Frontotemporal Dementia and Primary Progressive Aphasia. Dement. Geriatr. Cogn. Disord. 2008, 25, 178–185. [Google Scholar] [CrossRef]
- Moretti, R.; Torre, P.; Antonello, R.M.; Cattaruzza, T.; Cazzato, G.; Bava, A. Rivastigmine in Frontotemporal Dementia. Drugs Aging 2004, 21, 931–937. [Google Scholar] [CrossRef]
- Lebert, F.; Stekke, W.; Hasenbroekx, C.; Pasquier, F. Frontotemporal Dementia: A Randomised, Controlled Trial with Trazodone. Dement. Geriatr. Cogn. Disord. 2004, 17, 355–359. [Google Scholar] [CrossRef]
- Asmal, L.; Flegar, S.J.; Wang, J.; Rummel-Kluge, C.; Komossa, K.; Leucht, S. Quetiapine versus other atypical antipsychotics for schizophrenia. Emergencias 2013, CD006625. [Google Scholar] [CrossRef]
- Mendez, M.F.; Shapira, J.S.; McMurtray, A.; Licht, E. Preliminary Findings: Behavioral Worsening on Donepezil in Patients With Frontotemporal Dementia. Am. J. Geriatr. Psychiatry 2007, 15, 84–87. [Google Scholar] [CrossRef]
- Boxer, A.L.; Knopman, D.S.; I Kaufer, D.; Grossman, M.; Onyike, C.; Graf-Radford, N.; Mendez, M.; Kerwin, D.; Lerner, A.; Wu, C.-K.; et al. Memantine in patients with frontotemporal lobar degeneration: a multicentre, randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2013, 12, 149–156. [Google Scholar] [CrossRef]
Figure 1.
T1-weighted MRI imaging using an MPRAGE (Magnetisation Prepared Rapid Gradient Echo) sequence shows decreased GM volume in an AD patient compared to a healthy control and intermediate GM decline in a patient with MCI [23].
Figure 1.
T1-weighted MRI imaging using an MPRAGE (Magnetisation Prepared Rapid Gradient Echo) sequence shows decreased GM volume in an AD patient compared to a healthy control and intermediate GM decline in a patient with MCI [23].
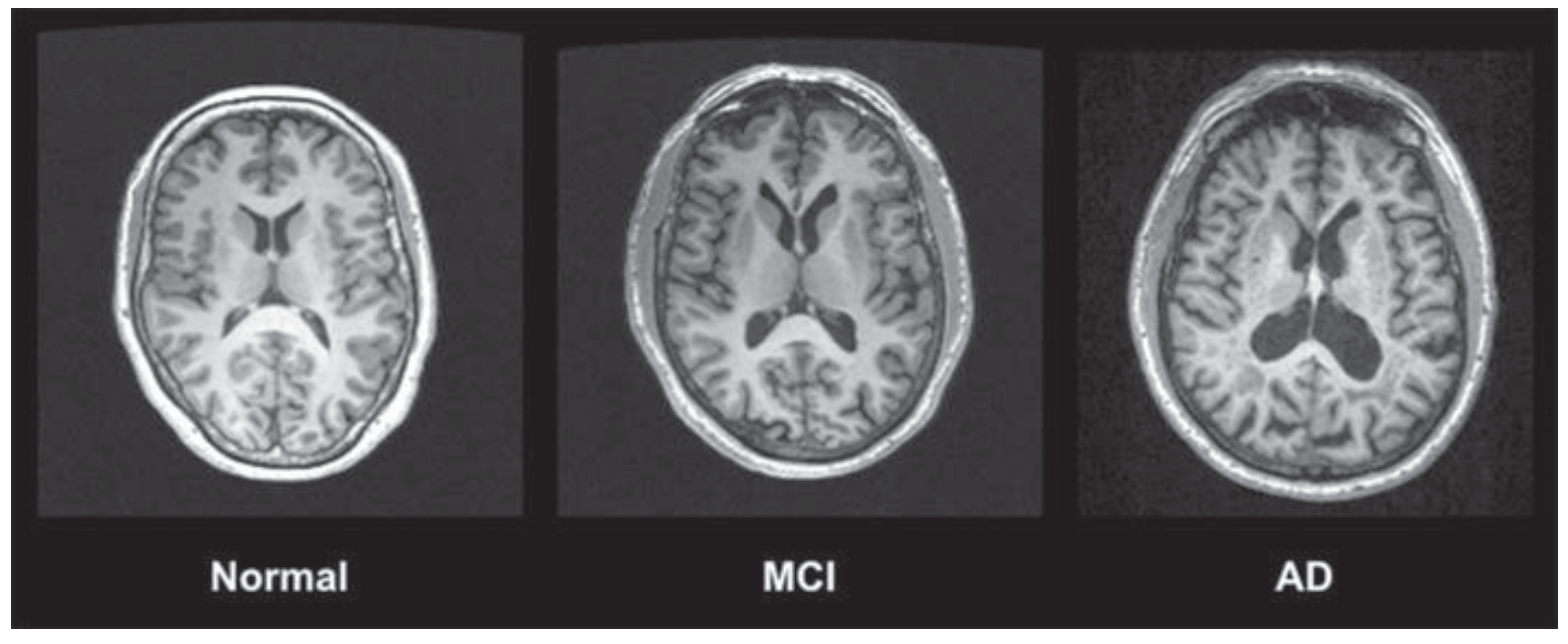
Figure 2.
Sample of Magnetic Resonance Imaging (MRI) scans obtained from the Parkinson’s Progression Markers Initiative (PPMI) database (a) MRI scan of a subject from the control group; (b) MRI scan of a subject from to the Parkinson’s Disease group [53].
Figure 2.
Sample of Magnetic Resonance Imaging (MRI) scans obtained from the Parkinson’s Progression Markers Initiative (PPMI) database (a) MRI scan of a subject from the control group; (b) MRI scan of a subject from to the Parkinson’s Disease group [53].
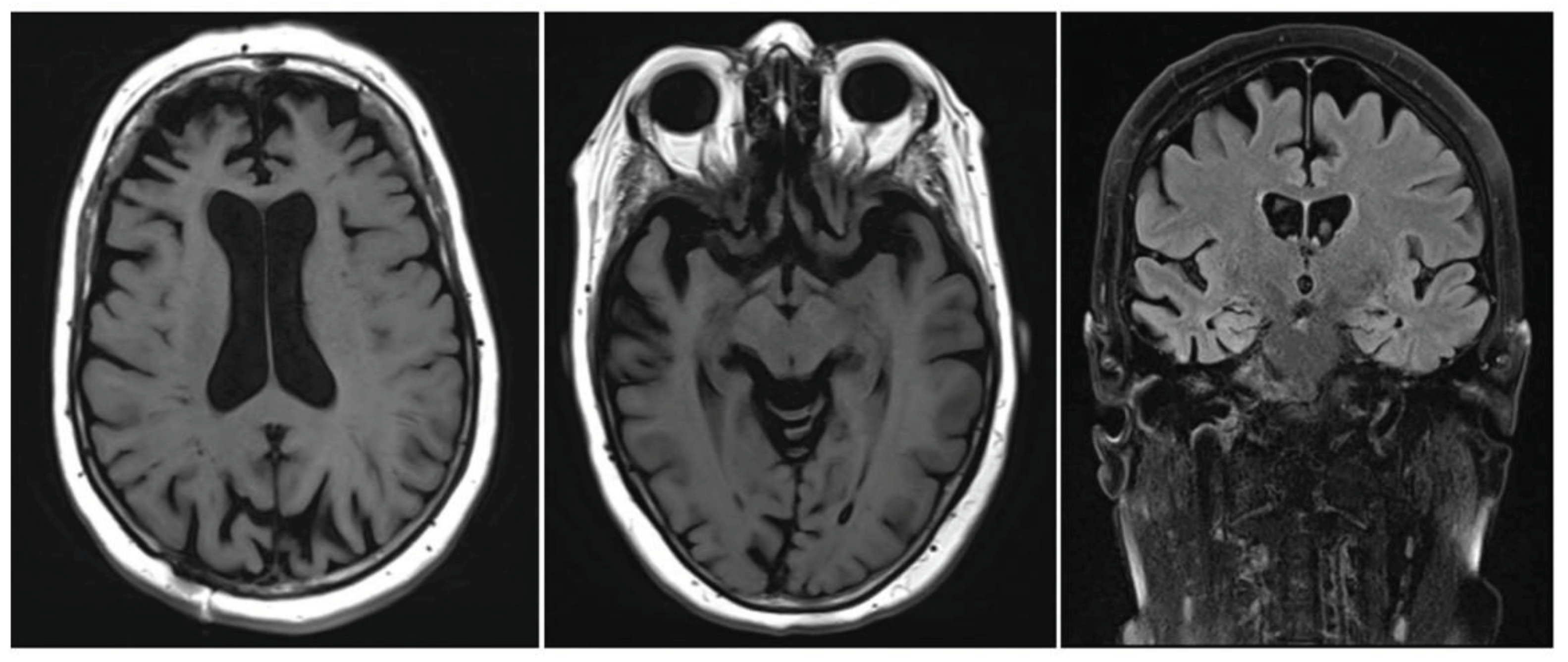
Figure 3.
The figure shows representative MRI scans from a non-demented control and from patients with Dementia with Lewy Bodies (DLB), Alzheimer’s disease (AD) and frontotemporal lobe degeneration (FTLD). It highlights the characteristic patterns of atrophy with relative preservation of the hippocampus in DLB, severe hippocampal atrophy in AD and temporal pole atrophy in FTLD. These scans are from the Neuroimaging of Inflammation in Memory and Other disorders (NIMROD) study cohort. Images are courtesy of Dr Elijah Mak, University of Cambridge, UK [95].
Figure 3.
The figure shows representative MRI scans from a non-demented control and from patients with Dementia with Lewy Bodies (DLB), Alzheimer’s disease (AD) and frontotemporal lobe degeneration (FTLD). It highlights the characteristic patterns of atrophy with relative preservation of the hippocampus in DLB, severe hippocampal atrophy in AD and temporal pole atrophy in FTLD. These scans are from the Neuroimaging of Inflammation in Memory and Other disorders (NIMROD) study cohort. Images are courtesy of Dr Elijah Mak, University of Cambridge, UK [95].
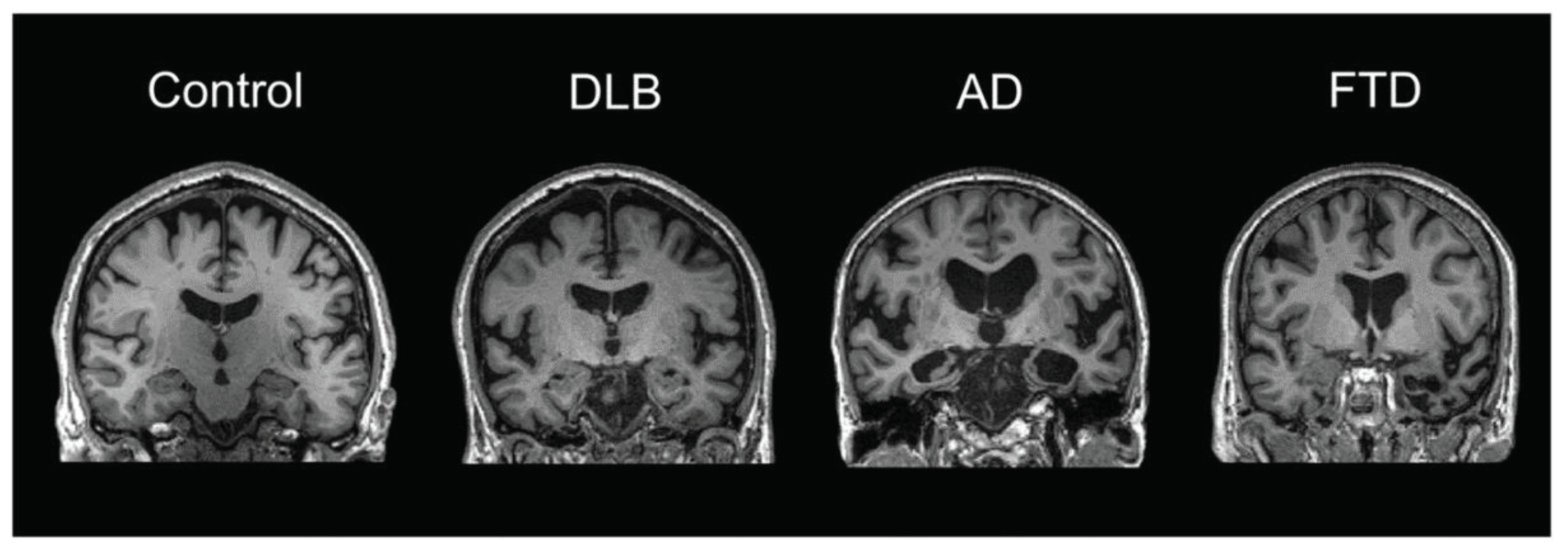
Figure 5.
Different lesion types commonly found on MRI scans of elderly people (arrows): (A–E) show Fluid Attenuated Inversion Recovery (FLAIR) sequences where white matter lesions (WML) appear as areas of high signal intensity while cerebrospinal fluid (CSF) signal is suppressed. (A) So-called “caps” located symmetrically around the anterior horns of both lateral ventricles. (B) Punctate WML in the centrum semiovale (CS) of the right hemisphere. (C) Early confluent and (D) confluent WML in the left CS. (E) Lacune seen as CSF-isointense lesion surrounded by a small hyperintense rim in the right CS. (F) shows a T2* weighted MRI sequence that is sensitive to susceptibility effects of hemosiderin. Spots of low signal intensity correspond to microbleeds in the left basal ganglia and thalamus [118].
Figure 5.
Different lesion types commonly found on MRI scans of elderly people (arrows): (A–E) show Fluid Attenuated Inversion Recovery (FLAIR) sequences where white matter lesions (WML) appear as areas of high signal intensity while cerebrospinal fluid (CSF) signal is suppressed. (A) So-called “caps” located symmetrically around the anterior horns of both lateral ventricles. (B) Punctate WML in the centrum semiovale (CS) of the right hemisphere. (C) Early confluent and (D) confluent WML in the left CS. (E) Lacune seen as CSF-isointense lesion surrounded by a small hyperintense rim in the right CS. (F) shows a T2* weighted MRI sequence that is sensitive to susceptibility effects of hemosiderin. Spots of low signal intensity correspond to microbleeds in the left basal ganglia and thalamus [118].
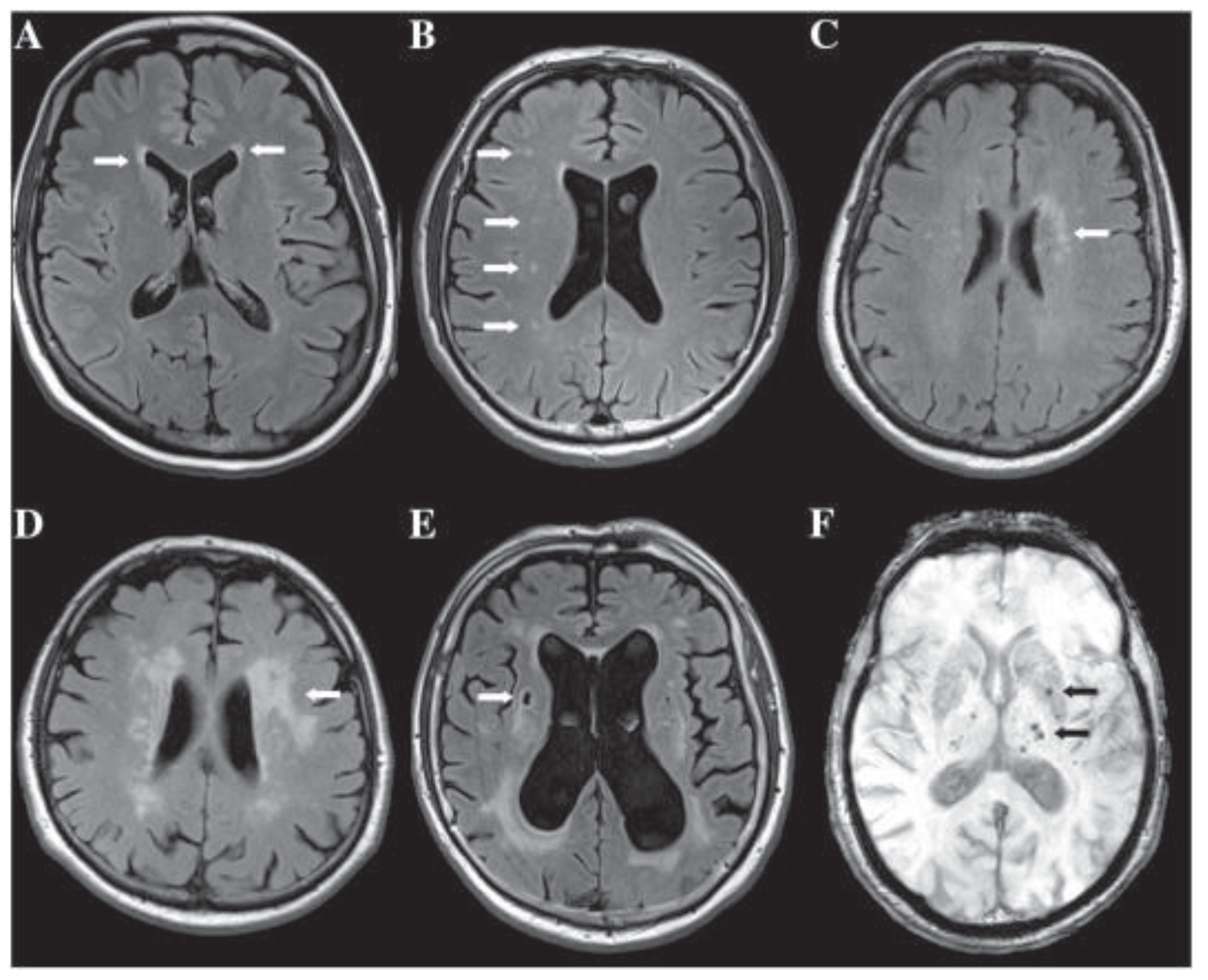
Figure 4.
Brain MRI of the patient described in the clinical vignette. “Based on the presenting clinical symptoms and the CSF and imaging biomarkers, the tentative diagnosis of behavioral variant FTD (bvFTD) was retained.” [23]..
Figure 4.
Brain MRI of the patient described in the clinical vignette. “Based on the presenting clinical symptoms and the CSF and imaging biomarkers, the tentative diagnosis of behavioral variant FTD (bvFTD) was retained.” [23]..
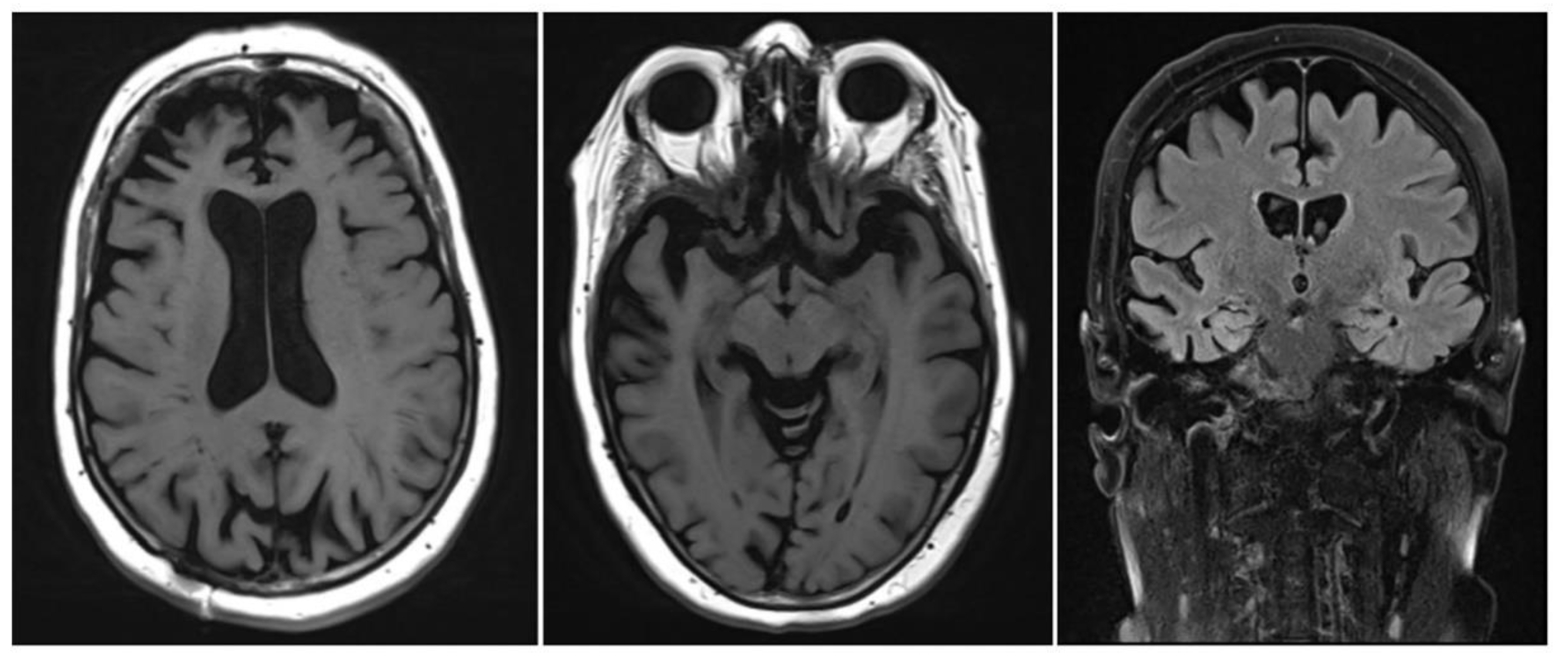
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



