Submitted:
07 April 2024
Posted:
10 April 2024
You are already at the latest version
Abstract
Introduction: It has long been accepted that trauma is one of the most important and frequent predisposing factors for onychomycoses . However, the role of direct trauma in the pathogenesis of fungal nail infections was only recently been elucidated in a series of 32 cases of post-traumatic single-digit onychomycosis. The importance of repeated trauma due to foot and toe abnormalities was rarely investigated.Aim of the study: This is a multicenter single-author observational study over a period of 6 years performed at a specialized nail clinic in three countries. All patient photographs taken by the author during this period were screened for toenail alterations and all toe onychomycosis cases were checked whether they contained enough information to evaluate potential foot and toe abnormalities. Particular attention was paid to the presence of hallux valgus, hallux valgus interphalangeus, hallux erectus, inward rotation of the big toe and outward rotation of the little toe, as well as splay foot. Only cases with unequivocal proof of fungal nail infection by either histopathology, mycologic culture or polymerase chain reaction (PCR) were accepted.Results: Of 1653 cases, 185 were onychomycoses proven by mycologic culture, PCR or histopathology. Of these, 179 involved at least one big toenail, 6 affected one or more lesser toenails. Three patients consulted us for another toenail disease and the onychomycosis was diagnosed as a second disease. Eight patients had a pronounced tinea pedum. Relatively few patients had a normal big toe position (n = 9). Most of the cases had a mild to marked hallux valgus (HV) (105) and a hallux valgus interphalangeus (HVI) (143), hallux erectus was observed in 43 patients, the combination of HV and HVI was observed 83 times. Discussion: The very high percentage of foot and toe deformations was surprising. It may be hypothesized that this is not only a pathogenetically important factor but may also play an important role for the localization of the fungal infection as no marked hallux deviation was noted in onychomycoses that affected the lesser toes only. As the management of onychomycoses is a complex procedure involving the exact diagnosis with determination of the pathogenic fungus, the nail growth rate, the type of onychomycosis, its duration and predisposing factors, anomalies of the toe position may be important. Among the most commonly mentioned predisposing factors are peripheral circulatory insufficiency, venous stasis, peripheral neuropathy, immune deficiency and iatrogenic immunosuppression whereas foot problems are not given enough attention. Unfortunately, many of these predisposing and aggravating factors are difficult to treat or to correct. Generally, when explaining the treatment of onychomycoses to the patients, the importance of these orthopedic alterations is not or only insufficiently discussed. In view of the problems encountered with the treatment of toenail mycoses, this attitude should be changed in order to make the patient understand why there is such a low cure rate despite excellent minimal inhibitory drug concentrations in the laboratory.
Keywords:
onychomycosis
; predisposing factors
; foot deformation
; toe malposition
; Hallux valgus
; Hallux valgus interphalangeus
; Hallux erectus
Introduction
Onychomycoses are said to be the most frequent nail diseases. Having been a rare event some 150 years ago they are now seen in 5 – 20 % of the population depending on the age and gender of the patients, environmental factors and climate, profession, hygiene conditions, co-morbidities, and habit of wearing almost air-tight shoes to mention just a few. [1,2,3,4,5,6,7] In the last 50 years, a wealth of information and knowledge on fungal nail infections has been accumulated; however, there is still a long way to understand all problems.[8] One of the most important risk factors is a hereditary susceptibility, as proven in many family trees demonstrating a vertical spread of onychomycoses in the family [9,10,11]. Another question is whether onychomycoses are indeed the most frequent nail conditions as nail changes due to skeletal abnormalities have not been considered by most authors and these nail alterations often look very similar to toenail mycoses [12]. They are also said to be secondarily colonized by non-dermatophyte fungi, which is not accepted as a true onychomycosis by some authors [13].
To find out the potential role of foot and toe anomalies for fungal nail infections, the photo archive of the author was searched for toenail diseases and all proven onychomycoses were listed as well as the position of the toes and visible foot alterations.
Methods
This is a single-author multicenter observational study conducted in specialized nail clinics between January 2018 and December 2023 (with a three-month break during the begin of the covid-19 pandemic). In this 6-year period, 1665 patients with toenail disease were seen. All patients were photographed with a smartphone and patient details (name, birth date, date of clinical examination, clinical diagnosis (diagnoses), and some other relevant findings were listed (Table 1). The photos were checked for the position of the big toe in relation to the first metatarsal bone and the potential deviation of the long axis of the distal phalanx from that of the proximal phalanx. Although radiographs were available for some toenail conditions this was not the rule for the diagnosis of onychomycoses. Only cases with sufficient information permitting the toe and foot to be evaluated for anomalies were included in this observation.
A hallux valgus was diagnosed when there was a deviation of the axis of the first metatarsal and proximal phalanx bones of more than 3° and a hallux valgus interphalangeus when the deviation was 3° or more. A hallux erectus was diagnosed when the tip of the toe did not touch the ground in a relaxed position or the extensor tendon was visibly under tension. Inward rotation of the big toe, also called tilting was again diagnosed with a deviation of the rotation axis of >3°. An outward rotation of the little toe of more than 15° was recognized as pathological. The measurements of the deviation angles were made with the rotation function in word layout.
Results
Out of 1663 patients, the axis of the toes in relation to the metatarsal bones could not be evaluated in 11 cases thus leaving 1652 cases for this observation. Of these, 185 patients (11.2%) had an onychomycosis proven by mycological examination (direct microscopy and culture), histopathology using PAS stain, or PCR. Of the 185 fungal toenail infections, 179 involved at least one big toenail, 6 affected one or more lesser toenails (without big toenail). An onychomycosis was diagnosed as a chance observation in 3 patients who consulted us for another nail condition. Only eight patients had a pronounced tinea pedum, for which they asked for help; however, tinea was clinically diagnosed in another 70 cases; this had not been noticed by the patients before and some even did not want their tinea to be treated.
A normal straight big toe position was seen in only nine patients (n = 9, 5%). Most of the cases had a mild to marked hallux valgus (HV) (105, 58.6%) and a hallux valgus interphalangeus (HVI) (143, 78.1%) (Figure 1, Figure 2, Figure 3 and Figure 4). Hallux erectus was observed in 43 patients (23.2%), the combination of HV and HVI was observed 83 times (44.9%) (Figure 1, Figure 2, Figure 3, Figure 4, Figure 5 and Figure 6).
As the patients consulted a specialized nail clinic this observation does not reflect the normal population.
Discussion
Since approximately 50 years, onychomycoses are considered to be the most common nail diseases. This has been questioned about 10 years ago when it was claimed that nail changes due to orthopedic lower limb, foot and toe anomalies would be the most common cause of toenail alterations [12,13]. This is underlined by our experience that more than 90% of all patients with toenail dystrophy showed some type of toe or foot anomaly [14,15].
It has long been known that there are predisposing factors for the development of onychomycoses [16,17]. Many of these factors are not amenable to treatment, such as male gender, advanced age, genetic susceptibility, and diabetes mellitus. Fungal nail infection is more frequent in psoriasis patients. Many surveys have shown a higher prevalence of onychomycoses in men [18] although there are considerable differences. The prevalence of onychomycoses increases proportionally with age until about 80 years [19,20].
One of the most important predisposing factors is certainly the autosomal dominant susceptibility to fungal nail infections [10]. Particularly in young patients, a family history should always be performed [9,20]. This often shows that there is a vertical spread of the infection in the family from grandparents to parents to children and grandchildren, whereas usually the spouse coming from another family remains onychomycosis-free despite year- or even decade-long contact with the infected family provided the spouse comes from a family without this genetic susceptibility. However, household spread may also be important [11].
Sex is a potential risk factor for tinea pedum and onychomycosis with considerably more males being affected with onychomycoses. The reason is not entirely clear; however, it was often assumed that men are more prone to traumatize their toes and thus render their nails more susceptible to fungal infection [21,22]. Damaged nails are more susceptible to fungal infection, particularly also with Fusarium spp. (Figure 7 and Figure 8) [23,24].
Sports activities have been observed to enhance the risk of fungal nail infection. This may be due to the increased foot and toe trauma, unphysiologic stress and strain, suboptimal hygienic conditions, often tight special footgear, sweating, use of communal showering facilities and many more [25,26,27,28]. Onychomycosis was found in 60.7% of professional football (soccer) players compared to 3.3% in a control group (Figure 9) [29].
Impaired blood supply is associated with loco-regional malperfusion enhancing the likelihood of a fungal infection and diminishing the chances of a successful antifungal therapy [30].
Chronic venous insufficiency is also associated with a higher risk of toe onychomycosis; however, nail deformations similar to fungal infections are frequent in chronic venous insufficiency. These onychomycoses have an even lower cure rate [31].
Peripheral neuropathies render the individual more prone to sustain unnoticed trauma, and trauma is an important predisposing factor [32].
Diabetes mellitus is more often associated with fungal infections of the feet and nails as it combines peripheral neuropathy with vascular insufficiency and decreased immunity [16,33,34,35,36,37,38,39]. Advanced age, male sex, diabetes, diabetic peripheral neuropathy and lower limb ischemia are independent risk factors for developing onychomycosis [17]. The severity of the diabetes mellitus is also an important risk factor. The diabetic foot syndrome as a particularly severe manifestation of diabetes mellitus has a very high risk of fungal toenail infection [40].
Hemodialysis patients often suffer from fungal nail infections. This is probably due to the primary cause of renal failure like diabetic nephropathy but hemodialysis as such may also predispose the patients to fungal nail infections [41,42,43,44].
All kinds of immune defects represent a high risk for developing an onychomycosis. This is particularly evident in transplant patients and those infected with human immunodeficiency virus (HIV) [42,45,46,47,48]. Superficial white and proximal white subungual onychomycoses are particularly suggestive of HIV infection [49].
Iatrogenic immune depression is a risk for onychomycoses [50,51]. Modern anti-inflammatory treatments with glucocorticosteroids, immunosuppressive cytostatic drugs and many biologics render the subjects more susceptible to fungal infections, also of the nails [51,52,53,54,55,56].
Factors long neglected are foot and toe anomalies (Figure 10, Figure 11 and Figure 12). The human foot is a very complex structure consisting of 26 bones plus two sesamoid bones, 40 joints with 12 extrinsic and 19 intrinsic muscles, many ligaments and tendons, skin of different anatomy on the soles and dorsa, highly specialized subcutaneous tissue acting as a cushion during walking, running and jumping, many blood vessels and specialized vascular structures, and a complicated nervous supply [58]. The two main functions of the feet are to act as a flexible support to the weight-bearing lower limbs and as a rigid lever to aid propulsion during locomotion [14,15,58]. The toes are an extension of the soles and both increase the stability of stance and balance as well as augment the lever action during propulsion. In the last phase of the gait called toe-off, the entire body weight is on the tip of the big toe; however, the kinetic energy of the forward thrust increases the weight by a factor of 2.5 during normal walking speed, and this is even further increased with many sports activities where running and acceleration are important. The nails, particularly the big toenail, give counterpressure to the forces acting on the soft tissue of the toe tip and prevent it from being dislocated dorsally and forming a distal bulge [14]. For this important function, the nail is anatomically linked to the tendons and ligaments of the distal interphalangeal joint to form one functional unit. This is also why the nail was called a musculo-skeletal appendage [59,60]. The nail consists of the matrix that produces the nail plate, and the nail bed that attaches the nail firmly to the underlying nail bed dermis and bone, as well as the periungual structures such as the proximal and the lateral nail folds. Although being functionally very different nail bed and matrix must work perfectly together in order to have a normal nail. If one of these structures is at fault there will be no normal nail; this is evidenced in the condition called the disappeared nail bed [15]. The cuticle protects the nail pocket also called the cul-de-sac, from the penetration of foreign substances and microbes. The hyponychium has a similar function anchoring the nail plate to the distal end of the nail bed and preventing the penetration of foreign bodies under the nail [61]. It is probably also a barrier to fungal infection of the distal nail bed [58].
Malposition of the nail be it due to malalignment of the nail itself, displacement of the distal phalanx or hallux valgus, results in chronic repeated microtrauma to the nail resulting in subungual hyperkeratosis, onycholysis, paronychia, Beau’s lines, onychomadesis, and onychomycosis [58,62,63]. Onycholysis, too short a nail or lack of the nail of the big toe after nail avulsion or traumatic nail loss lead to a distal bulge and a shortened or disappeared nail bed [64,65]. The bulge is part of the toe tip and covered with ridged skin; there is no epidermization of the nail bed as is easily seen by the sharp delimitation between the bulge and the shortened nail bed [66].
As briefly mentioned above, nail alterations caused by orthopedic abnormalities may look very much like fungal nail infections, particularly distal-lateral subungual onychomycosis [12,13,57,67]. This observational real-world study has shown that “normal” straight toes are rather the exception than the rule. Approximately 90% of the onychomycosis patients had a toe malposition, mostly a hallux valgus interphalangeus (HVI) or hallux valgus (HV), often both whereas hallux erectus (HE, hyperextension) was less frequent. Splay foot is commonly associated with flat foot (although not evaluable in this study due to the type of clinical photography performed) and they in turn often lead to inward rotation of the big toe and outward rotation of the little toe [58]. These orthopedic conditions exert non-physiologic strain on the nails by direct repeated trauma or by modification of pre-existing nail alterations. Friction may cause subungual hyperkeratosis that breaches the integrity of the hyponychium and allows fungi to penetrate through it and reach the nail bed, in extreme cases it may cause a subungual corn (heloma subunguale). However, it has to be stressed that subungual hyperkeratosis and true nail thickening are often erroneously seen as the same [67]. A malaligned nail or a laterally displaced toe are prone to sustain trauma through torsion stress forces during walking, crawling and from footwear [63]. It appears that compression forces that hit a deviated nail are of particularly devastating action on the attachment of the nail to the nail bed [15]. However, we have very rarely found pathogenic fungi in congenital malalignment of the big toenail [14,15].
Patients consulting a specialized nail clinic for a long-standing onychomycosis have usually seen several physicians including dermatologists before. They are embarrassed by their infection and often have a low self-esteem, decreased quality of life, not infrequently pain, abstain from social contacts and most have already undergone several treatments [68]. They are challenging patients as unsuccessful therapies left them frustrated and even angry that they paid their medication “for nothing” but with the risk of potentially serious adverse effects. It is of paramount importance to explain the problems of any onychomycosis management and that this is not only a nail issue but a problem of the whole organism. Treatment failure of fungal toenail infections is often not because of insufficient drug activity, whether applied topically or given systemically but a failure to recognize the many risk factors discussed above [58]. However, even in the podiatric literature, foot, toe and gait anomalies in onychomycosis patients are often ignored [69]. Chronically traumatized nails tend to develop a massive subungual hyperkeratosis. It was found that its thickness is inversely related to treatment success [70].
Still another unsolved problem is the frequent occurrence of recurrences. In most cases, it is not clear whether this is due to a relapse of residual disease or a true infection [71]. It is known that spores, also of dermatophytes, remain viable for years. Fungus-containing little scales are lost where individuals with a tinea pedum walk barefoot, particularly in the own bath and bedrooms. Stepping on such keratin flakes makes them stick on the sole of the foot where they can form invasive hyphae within about 4 hours. The role of dermatophytoma and similar masses of fungi in the nail bed compressed between the living epithelium and the overlying nail is not yet elucidated; the fungi here may have cell walls up to 20 times thicker than in common hyphae rendering them intrinsically more resistant, and they are even more difficult to reach by both topical and systemic antifungal drugs (Figure 13 and Figure 14) [72,73]. Histopathology shows both dermatophytomas (Figure 15) as well as biofilms (Figure 16); these biofilms are more often bacterial than fungal and extremely common at the undersurface of onycholytic nail plates. It is known that biofilms are up to 1000 times less sensitive to antibiotics than the same microbes as single organisms (so-called planktonic forms) [74]. Further, histopathology can prove that Fusarium spp and other non-dermatophyte molds are able to produce real onychomycoses (Figure 17).
Conclusion
Onychomycoses are said to be the most frequent nail diseases making up for approximately half of all ungual diseases. Of all dermatomycoses, they are the most difficult to treat. This is the consequence of the particular anatomy of the nail infection, the difficulty of the drugs to reach the really infected part, and the innumerable factors accompanying the fungal nail infection, of which many are not amenable to therapy or difficult to treat, and are often beyond the scope of the dermatologist. Thus, onychomycosis therapy requires a well-informed and understanding patient [15,58].
Limitations of the Study
This is a retrospective single-examiner real-world study from different European cities with no control group. There is probably a high degree of bias as the patients referred to the highly specialized nail clinic were almost all pre-examined and pre-treated and therefore do not reflect the average. No statements can be made about the frequency of onychomycoses in the general population.
Strengths of the Study
This is the largest study on onychomycoses in foot and toe anomalies up to date. The level of expertise was always the same.
Acknowledgments
I wish to thank the directors of the institutions where the clinics had been held for their never-ending support, cooperation and great help (Prof Dr Luca Borradori, Bern, Switzerland, Prof Dr Osvaldo Correia, Porto, Portugal) and the staff in their institutions who assisted me during the clinical examinations. Further, I want to thank my patients for allowing me to use the clinical photos.
Statement of Ethics
The study was conducted in accordance with the Declaration of Helsinki. All patients were treated according to Best Clinical Practice and no experiments were performed on them. Ethical approval is not required for this retrospective observational study in accordance with local and national guidelines. All patients in this manuscript have given verbal informed consent for participation and the use of their de-identified, anonymized, aggregated data and their case details including photographs for publication; written informed consent to participate was not required in accordance with local guidelines.
Conflicts of Interest
The author has no conflict of interest to declare.
Funding
The author received no funding.
Author Contributions
The author saw, examined and treated all patients himself and solely designed the study.
Data availability
Anonymized de-identified data are available on reasonable request.
Ethical approval
not applicable.
References
- Haneke E. Epidemiology and pathology of the onychomycoses. In: Nolting S, Korting HC: Onychomycoses - Local Antimycotic Treatment. Springer, Berlin Heidelberg New York, 1990: 1-11.
- Gawdzik A, Nowogrodzka K, Hryncewicz-Gwóźdź A, Szepietowski J, Maj J, Jankowska-Konsur A. Epidemiology of dermatophytoses in paediatric population in Southwestern Poland, 2011-2016. Postepy Dermatol Alergol. 2021;38(2):91-95. [CrossRef]
- Kromer C, Celis D, Hipler UC, Zampeli VA, Mößner R, Lippert U. Dermatophyte infections in children compared to adults in Germany: a retrospective multicenter study in Germany. J Dtsch Dermatol Ges. 2021;19(7):993-1001. [CrossRef]
- Gupta AK, Venkataraman M, Shear NH, Piguet V. Onychomycosis in children - review on treatment and management strategies. J Dermatolog Treat. 2022;33(3):1213-1224. [CrossRef]
- Lecerf P, Abdy S, Vollono L, Pastushenko I, Richert B, André J. Direct examination, histopathology and fungal culture for the diagnosis of onychomycosis: A retrospective, comparative study on 2245 specimens. Mycoses. 2021;64(2):187-193. [CrossRef]
- Gupta AK, Taborda VBA, Taborda PRO, Shemer A, Summerbell RC, Nakrieko KA. High prevalence of mixed infections in global onychomycosis. PLoS One. 2020;15(9):e0239648. [CrossRef]
- Haneke E (1999) Achilles foot-screening project: Background, objectives and design. J Eur Acad Dermatol Venereol 12: Suppl 1:S2-S5.
- Haneke E, Roseeuw D (1999) The scope of onychomycosis: epidemiology and clinical features. Int J Dermatol 38: Suppl 2:7-12.
- English MP. Trichophyton rubrum infections in families. Br Med J 1957;2:744-746.
- Zaias N, Tosti A, Rebell G, Morelli R, Bardazzi F, Bieley H, Zaiac M, Glick B, Paley B, Allevato M, Baran R. Autosomal dominant pattern of distal subungual onychomycosis caused by Trichophyton rubrum. J Am Acad Dermatol. 1996;34(2 Pt 1):302-304. [CrossRef]
- Jazdarehee A, Malekafzali L, Lee J, Lewis R, Mukovozov I. Transmission of onychomycosis and dermatophytosis between household members: A scoping review. J Fungi (Basel). 2022;8(1):60. [CrossRef]
- Zaias N, Rebell G, Escovar S. Asymmetric gait nail unit syndrome: the most common worldwide toenail abnormality and onychomycosis. Skinmed. 2014;12(4):217-223.
- Zaias N, Escovar SX, Rebell G. Opportunistic toenail onychomycosis. The fungal colonization of an available nail unit space by non-dermatophytes is produced by the trauma of the closed shoe by an asymmetric gait or other trauma. A plausible theory. J Eur Acad Dermatol Venereol. 2014;28(8):1002-6. [CrossRef]
- Haneke E. Toenails: Where orthopedics and onychology meet. In Baran R, ed. Advances in Nail Disease and Management. Springer Nature Switzerland 2021:71-86.
- Haneke E. Foot, toe and nail changes – are they interdependent? Skin Append Disord 2024, accepted.
- Haneke E. Fungal infections of the nail. Semin Dermatol. 1991;10(1):41-53.
- Ogawa T, Matsuda A, Ogawa Y, Tanaka R. Risk factors for the development of tinea pedis and onychomycosis: Real-world evidence from a single-podiatry center, large-scale database in Japan. J Dermatol. 2024;51(1):30-39. [CrossRef]
- Roseeuw D. Achilles foot screening project: preliminary results of patients screened by dermatologists. J Eur Acad Dermatol Venereol. 1999;12 Suppl 1:S6-9; discussion S17.
- Adams C, Athanasoula E, Lee W, Mahmudova N, Vlahovic TC. Environmental and genetic factors on the development of onychomycosis. J Fungi (Basel). 2015;1(2):211-216. [CrossRef]
- Gupta AK, Sibbald RG, Lynde CW, Hull PR, Prussick R, Shear NH, De Doncker P, Daniel CR 3rd, Elewski BE. Onychomycosis in children: prevalence and treatment strategies. J Am Acad Dermatol. 1997;36(3 Pt 1):395-402. [CrossRef]
- Jha B, Sharma M, Gc S, Sapkota J. Onychomycosis among clinically suspected cases attending the dermatology out-patient department of a tertiary care centre: A descriptive cross-sectional study. JNMA J Nepal Med Assoc. 2021;59(237):450-453. [CrossRef]
- Gupta AK, Wang T, Cooper EA, Lincoln SA, Foreman HC, Scherer WP, Bakotic WL. Clinical diagnosis and laboratory testing of abnormal appearing toenails: a retrospective assessment of confirmatory testing for onychomycosis in the United States, 2022-2023. J Fungi (Basel). 2024 Feb 13;10(2):149. [CrossRef]
- Walshe MM, English MP. Fungi in nails. Br J Dermatol. 1966;78(4):198-207. [CrossRef]
- English MP. Nails and fungi. Br J Dermatol. 1976 Jun;94(6):697-701. [CrossRef]
- Gudnadóttir G, Hilmarsdóttir I, Sigurgeirsson B. Onychomycosis in Icelandic swimmers. Acta Derm Venereol. 1999;79(5):376-7. [CrossRef]
- Möhrenschlager M, Seidl HP, Schnopp C, Ring J, Abeck D. Professional ice hockey players: a high-risk group for fungal infection of the foot? Dermatology. 2001;203(3):271. [CrossRef]
- Caputo R, De Boulle K, Del Rosso J, Nowicki R. Prevalence of superficial fungal infections among sports-active individuals: results from the Achilles survey, a review of the literature. J Eur Acad Dermatol Venereol. 2001;15(4):312-316.
- Jenkins DW, Cooper K, O'Connor R, Watanabe L, Wills C. Prevalence of podiatric conditions seen in Special Olympics athletes: Structural, biomechanical and dermatological findings. Foot (Edinb). 2011;21(1):15-25. [CrossRef]
- Buder V, Augustin M, Schäfer I, Welsch G, Catala-Lehnen P, Herberger K. Prävalenz von Dermatomykosen bei Profifußballspielern : Untersuchung im Rahmen der Bundesligatauglichkeitsuntersuchung (2013–2015) im Vergleich mit Daten der Allgemeinbevölkerung [Prevalence of dermatomycoses in professional football players : A study based on data of German Bundesliga fitness check-ups (2013-2015) compared to data of the general population]. Hautarzt. 2018 May;69(5):401-407. German. [CrossRef]
- Kubec K. Vascular factor in onychomycosis. Acta Univ Carol Med (Praha). 1979;25(5-6):247-333.
- Shemer A, Nathansohn N, Kaplan B, Trau H. Toenail abnormalities and onychomycosis in chronic venous insufficiency of the legs: should we treat? J Eur Acad Dermatol Venereol. 2008;22(3):279-82. [CrossRef]
- Rocha N, Velho G, Horta M, Martins A, Massa A. Cutaneous manifestations of familial amyloidotic polyneuropathy. J Eur Acad Dermatol Venereol. 2005;19(5):605-607. [CrossRef]
- Rich P. Special patient populations: onychomycosis in the diabetic patient. J Am Acad Dermatol. 1996;35(3 Pt 2):S10-2. [CrossRef]
- Dogra S, Kumar B, Bhansali A, Chakrabarty A. Epidemiology of onychomycosis in patients with diabetes mellitus in India. Int J Dermatol. 2002;41(10):647-51. [CrossRef]
- Muniz EC, Rocha RM, Reis ML, Santos VL, Grossi SA. Neuropathic and ischemic changes of the foot in Brazilian patients with diabetes. Ostomy Wound Manage. 2003;49(8):60-70, 72-3.
- Saunte DM, Holgersen JB, Haedersdal M, Strauss G, Bitsch M, Svendsen OL, Arendrup MC, Svejgaard EL. Prevalence of toe nail onychomycosis in diabetic patients. Acta Derm Venereol. 2006;86(5):425-8. [CrossRef]
- Eckhard M, Lengler A, Liersch J, Bretzel RG, Mayser P. Fungal foot infections in patients with diabetes mellitus--results of two independent investigations. Mycoses. 2007;50 Suppl 2:14-9. [CrossRef]
- Dumont IJ. Diagnosis and prevalence of onychomycosis in diabetic neuropathic patients: an observational study. J Am Podiatr Med Assoc. 2009;99(2):135-9. [CrossRef]
- Lauterbach S, Kostev K, Becker R. Characteristics of diabetic patients visiting a podiatry practice in Germany. J Wound Care. 2010;19(4):140, 142, 144 passim. [CrossRef]
- Navarro-Pérez D, Tardáguila-García A, García-Oreja S, López-Moral M, García-Madrid M, Lázaro-Martínez JL. Onychomycosis associated with diabetic foot syndrome: A systematic review. Mycoses. 2023;66(6):459-466. [CrossRef]
- Kuvandik G, Cetin M, Genctoy G, Horoz M, Duru M, Akcali C, Satar S, Kiykim AA, Kaya H. The prevalance, epidemiology and risk factors for onychomycosis in hemodialysis patients. BMC Infect Dis. 2007 Aug 30;7:102. [CrossRef]
- Filho AMS, Ventura CG, Criado PR, Del Negro GB, Freitas RS, Luiz OC, Giudice MC, Neto ED, Benard G. Hemodialysis and kidney transplantation as predisposing conditions to onychomycosis. Nephron. 2017;137(1):38-46. [CrossRef]
- Bersano JMQB, Cordeiro MG, Marson FAL. Prevalence and risk predictors of onychomycosis in patients on hemodialysis: an observation, prospective, and unicenter study in Brazil. Front Med (Lausanne). 2023;10:1268324. [CrossRef]
- Eftekhari H, Haghdar Saheli Y, Ashoobi MT, Mahjoob M, Kazemnezhad Leyli E, Bagheri Toolaroud P. The prevalence of onychomycosis in patients with chronic renal failure undergoing dialysis: A cross-sectional study. Heliyon. 2024 Feb 11;10(4):e25737. [CrossRef]
- Howard J, Sattler F, Mahon R, Sperling J, Leedom J. Clinical features of 100 human immunodeficiency virus antibody-positive individuals from an alternate test site. Arch Intern Med. 1987;147(12):2131-2133.
- Dompmartin D, Dompmartin A, Deluol AM, Grosshans E, Coulaud JP. Onychomycosis and AIDS. Clinical and laboratory findings in 62 patients. Int J Dermatol. 1990;29(5):337-9. [CrossRef]
- Daniel CR 3rd, Norton LA, Scher RK. The spectrum of nail disease in patients with human immunodeficiency virus infection. J Am Acad Dermatol. 1992;27(1):93-97. [CrossRef]
- Castro LÁ, Álvarez MI. Nail dermatophytoma in HIV-infected patients in Cali, Colombia. J Mycol Med. 2021;31(3):101172. [CrossRef]
- Gómez-Moyano E, Crespo-Erchiga V. HIV infection manifesting as proximal white onychomycosis. N Engl J Med. 2017;377(18):e26. [CrossRef]
- Levy LA. Epidemiology of onychomycosis in special-risk populations. J Am Podiatr Med Assoc. 1997;87(12):546-50. [CrossRef]
- Faergemann J, Baran R. Epidemiology, clinical presentation and diagnosis of onychomycosis. Br J Dermatol. 2003;149 Suppl 65:1-4. [CrossRef]
- Borba OSM, Ogawa MM, Kirsztajn GM, Tomimori J. Onychomycosis in immunocompromised population: Phenotypic and molecular identification. Mycoses. 2023;66(11):1018-1024. [CrossRef]
- Al-Mutairi N, Nour T, Al-Rqobah D. Onychomycosis in patients of nail psoriasis on biologic therapy: a randomized, prospective open label study comparing Etanercept, Infliximab and Adalimumab. Expert Opin Biol Ther. 2013;13(5):625-9. [CrossRef]
- Andersen PL, Henning MAS, Jemec GBE, Arendrup MC, Saunte DM. Two cases of proximal subungual onychomycosis caused by trichophyton rubrum in HIV-negative patients during treatment with TNF-α inhibitors combined with methotrexate. Acta Dermatovenerol Croat. 2018;26(4):304-306.
- Alves NCPOP, Moreira TA, Malvino LDS, Rodrigues JJ, Ranza R, de Araújo LB, Pedroso RDS. Onychomycosis in Psoriatic Patients with Nail Disorders: Aetiological Agents and Immunosuppressive Therapy. Dermatol Res Pract. 2020;2020:7209518. [CrossRef]
- Chularojanamontri L, Pattanaprichakul P, Leeyaphan C, Suphatsathienkul P, Wongdama S, Bunyaratavej S. Overall prevalence and prevalence compared among psoriasis treatments of onychomycosis in patients with nail psoriasis and fungal involvement. Biomed Res Int. 2021;2021:9113418. [CrossRef]
- Zaias N, Escovar SX, Zaiac MN, Edwards R, Dutra M, Pona A, Rio ED, Jungcharoensukying P. Onychomycosis, the active invasion of a normal nail unit by a dermatophytic versus the colonization of an existing abnormal nail unit by environmental fungus. Skinmed. 2020;18(1):18-22.
- Murray SC, Dawber RP. Onychomycosis of toenails: orthopaedic and podiatric considerations. Australas J Dermatol. 2002;43(2):105-112. [CrossRef]
- McGonagle D, Tan AL, Benjamin M. The nail as a musculoskeletal appendage--implications for an improved understanding of the link between psoriasis and arthritis. Dermatology. 2009;218(2):97-102. [CrossRef]
- Ash Z, McGonagle D. Joint appendages: the structures which have historically been overlooked in arthritis research and therapy development. Best Pract Res Clin Rheumatol. 2011;25(6):779-784. [CrossRef]
- Haneke E. Anatomy of the nail unit and the nail biopsy. Semin Cutan Med Surg. 2015 Jun;34(2):95-100. [CrossRef]
- Braswell MA, Daniel CR 3rd, Brodell RT. Beau lines, onychomadesis, and retronychia: A unifying hypothesis. J Am Acad Dermatol. 2015 Nov;73(5):849-55. [CrossRef]
- Buttars B, Scott SG, Glinka D, Daniel CR, Brodell RT, Braswell MA. Congenital malalignment of the great toenail, the disappearing nail bed, and distal phalanx deviation: A review. Skin Appendage Disord. 2022;8(1):8-12. [CrossRef]
- Arai H, Arai T, Nakajima H, Haneke E. Formable acrylic treatment for ingrowing nail with gutter splint and sculptured nail. Int J Dermatol. 2004;43(10):759-765. [CrossRef]
- Haneke E. Controversies in the treatment of ingrown nails. Dermatol Res Pract. 2012;2012:783924. [CrossRef]
- Daniel CR 3rd, Tosti A, Iorizzo M, Piraccini BM. The disappearing nail bed: a possible outcome of onycholysis. Cutis. 2005;76(5):325-327.
- Kim JK, Chung HC, Chun EJ, Kim S, Kim CW. Correlation between nail thickness and onychomycosis: misuse of antifungal agents in patients with thick nails. Ann Dermatol. 2024;36(2):123-124 . [CrossRef]
- Drake LA, Patrick Dl, Fleckman P, Andre J, Baran R, Haneke E, Sapede C, Tosti A (1999) The impact of onychomycosis on quality of life: Development of an international onychomycosis-specific questionnaire to measure patient quality of life. J Am Acad Dermatol 41:189-196.
- Vlahovic TC. Onychomycosis: Evaluation, treatment options, managing recurrence, and patient outcomes. Clin Podiatr Med Surg. 2016;33(3):305-18. [CrossRef]
- Sommer S, Sheehan-Dare RA, Goodfield MJ, Evans EG. Prediction of outcome in the treatment of onychomycosis. Clin Exp Dermatol. 2003;28(4):425-8. [CrossRef]
- Evans EG. The rationale for combination therapy. Br J Dermatol. 2001;145 Suppl 60:9-13.
- Roberts DT, Evans EG. Subungual dermatophytoma complicating dermatophyte onychomycosis. Br J Dermatol. 1998;138(1):189-90. [CrossRef]
- Burkhart CN, Burkhart CG, Gupta AK. Dermatophytoma: Recalcitrance to treatment because of existence of fungal biofilm. J Am Acad Dermatol. 2002 Oct;47(4):629-31. [CrossRef]
- Markantonatou AM, Samaras K, Vyzantiadis TA. Dermatophytic biofilms: Characteristics, significance and treatment approaches. J Fungi (Basel). 2023;9(2):228. [CrossRef]
- Haneke E. Nail psoriasis: clinical features, pathogenesis, differential diagnoses, and management. Psoriasis (Auckl) 2017;7:51-63.
- Haneke E. Differential diagnosis of nail psoriasis and onychomycoses: A report based on 40 years of specialised nail consultations. EMJ Dermatol 2020. [CrossRef]
- Aldana-Caballero A, Mayordomo R, Marcos-Tejedor F. Assessment of visual diagnosis by podiatrists for HPV and onychomycosis: the need for complementary tests. J Fungi (Basel). 2022;8(2):135. [CrossRef]
Figure 1.
Onychomycosis of both big toes in a 49-year-old patient with mild hallux valgus and hallux valgus interphalangeus, the second toes are longer than the first ones (Greek foot). Mycologic culture revealed Trichophyton rubrum. Note that both big toenails are thick, yellowish, with a marked subungual hyperkeratosis, the extensor hallucis longus tendon is visibly taut.
Figure 1.
Onychomycosis of both big toes in a 49-year-old patient with mild hallux valgus and hallux valgus interphalangeus, the second toes are longer than the first ones (Greek foot). Mycologic culture revealed Trichophyton rubrum. Note that both big toenails are thick, yellowish, with a marked subungual hyperkeratosis, the extensor hallucis longus tendon is visibly taut.

Figure 2.
63-year-old woman with dystrophic onychomycosis of the left big and both little toes and marked hallux valgus. A. Overview. B. Right little toenail. C. Left little toenail.
Figure 2.
63-year-old woman with dystrophic onychomycosis of the left big and both little toes and marked hallux valgus. A. Overview. B. Right little toenail. C. Left little toenail.


Figure 3.
Hypertrophic onychomycosis of the left big toe in a 21-year-old woman with mild hallux valgus and hallux valgus interphalangeus. Note the desquamation at the hyponychium and toe tip indictive of tinea pedis. A. Overview. B. Close-up.
Figure 3.
Hypertrophic onychomycosis of the left big toe in a 21-year-old woman with mild hallux valgus and hallux valgus interphalangeus. Note the desquamation at the hyponychium and toe tip indictive of tinea pedis. A. Overview. B. Close-up.
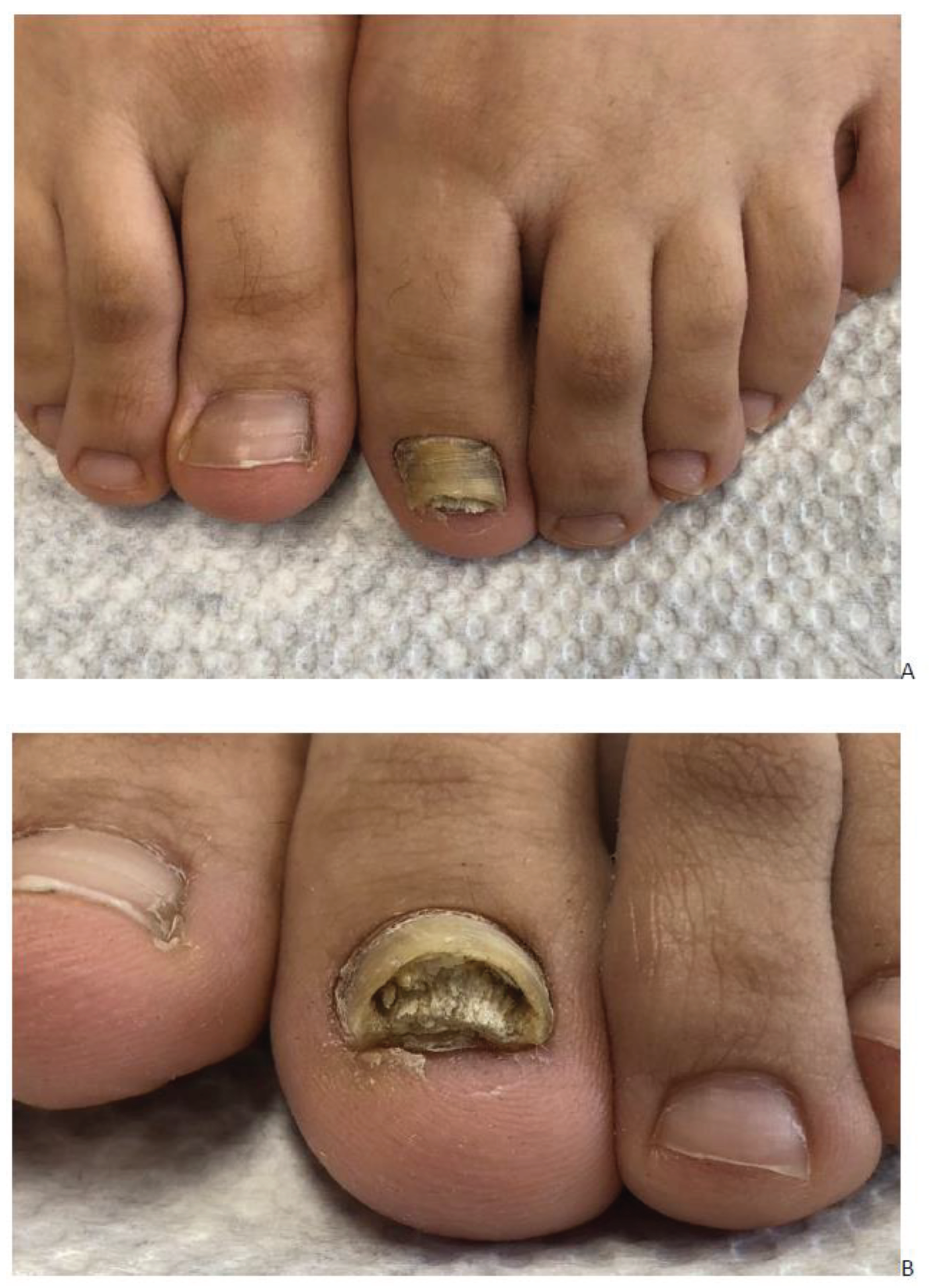
Figure 4.
Onychomycosis in a 30-year-old woman with hallux valgus, hallux valgus interphalangeus and hallux erectus . A. Dorsal view. B. Side view.
Figure 4.
Onychomycosis in a 30-year-old woman with hallux valgus, hallux valgus interphalangeus and hallux erectus . A. Dorsal view. B. Side view.

Figure 5.
Single-digit posttraumatic onychomycosis in a 55-year-old man with hallux valgus, hallux valgus interphalangeus, left hallux erectus, short left big toenail and markedly shrunken nail bed.
Figure 5.
Single-digit posttraumatic onychomycosis in a 55-year-old man with hallux valgus, hallux valgus interphalangeus, left hallux erectus, short left big toenail and markedly shrunken nail bed.

Figure 6.
Big toes of a 51-year-old man with longstanding onychomycosis of both big toes, hallux valgus interphalangeus and mild hallux valgus, inward rotation of the big toes, left more than right, short nails, large distal wall covered with ridged skin of the tip of the toe. The patient had cut his nails always as short as he could.
Figure 6.
Big toes of a 51-year-old man with longstanding onychomycosis of both big toes, hallux valgus interphalangeus and mild hallux valgus, inward rotation of the big toes, left more than right, short nails, large distal wall covered with ridged skin of the tip of the toe. The patient had cut his nails always as short as he could.

Figure 7.
Big toes of a 61-year pervious professional soccer player with onychomycosis of both big toes. Note that there is only a mild deviation of the distal phalanx hinting at the importance of the previous professional soccer playing as a predisposing factor. A. Overview. B. Close-up photograph.
Figure 7.
Big toes of a 61-year pervious professional soccer player with onychomycosis of both big toes. Note that there is only a mild deviation of the distal phalanx hinting at the importance of the previous professional soccer playing as a predisposing factor. A. Overview. B. Close-up photograph.

Figure 8.
Onychomycosis of the big toes due to Fusarium solani complex. There is a marked hallux valgus of the left big toe and a pronounced hallux valgus interphalangeus of the right big toe.
Figure 8.
Onychomycosis of the big toes due to Fusarium solani complex. There is a marked hallux valgus of the left big toe and a pronounced hallux valgus interphalangeus of the right big toe.

Figure 9.
Fusarium oxysporon onychomycosis in a 53-year-old woman with mild hallux valgus and hallux valgus interphalangeus. A. Overview showing the taut extensor hallucis longus tendons. A Overview. B. Close-up.
Figure 9.
Fusarium oxysporon onychomycosis in a 53-year-old woman with mild hallux valgus and hallux valgus interphalangeus. A. Overview showing the taut extensor hallucis longus tendons. A Overview. B. Close-up.

Figure 10.
45-year-old woman with hallux valgus, onychomycosis and tinea pedum. A. Dorsal view. B. Plantar view. C. Medial view of the left foot showing a hallux erectus.
Figure 10.
45-year-old woman with hallux valgus, onychomycosis and tinea pedum. A. Dorsal view. B. Plantar view. C. Medial view of the left foot showing a hallux erectus.

Figure 11.
Isolated onychomycosis of the left 3rd toe in a 27-year-old woman.

Figure 12.
Post-traumatic onychomycosis in a 59-year-old man with hallux valgus interphalangeus. A. Overview. B. Close-up photograph.
Figure 12.
Post-traumatic onychomycosis in a 59-year-old man with hallux valgus interphalangeus. A. Overview. B. Close-up photograph.

Figure 13.
Dermatophytoma of the left great toe nail in a 48-year-old man with diffuse leukonychia.

Figure 14.
53-year-old female patient with right hallux valgus interphalangeus and dermatophytoma as well as left big toe with hallux erectus, disappeared nail bed (shrunken nail bed) and big distal bulge.
Figure 14.
53-year-old female patient with right hallux valgus interphalangeus and dermatophytoma as well as left big toe with hallux erectus, disappeared nail bed (shrunken nail bed) and big distal bulge.

Figure 15.
Dermatophytoma. A. Hematoxylin and eosin stain: the keratin is red, part of the fungal masses is reddish violet, the pale grey structures are fungal elements, which are normally not stained by H&E. Original magnification 100x. B. PAS stain: the fungi are stain intensely violet; original magnification 200x.
Figure 15.
Dermatophytoma. A. Hematoxylin and eosin stain: the keratin is red, part of the fungal masses is reddish violet, the pale grey structures are fungal elements, which are normally not stained by H&E. Original magnification 100x. B. PAS stain: the fungi are stain intensely violet; original magnification 200x.
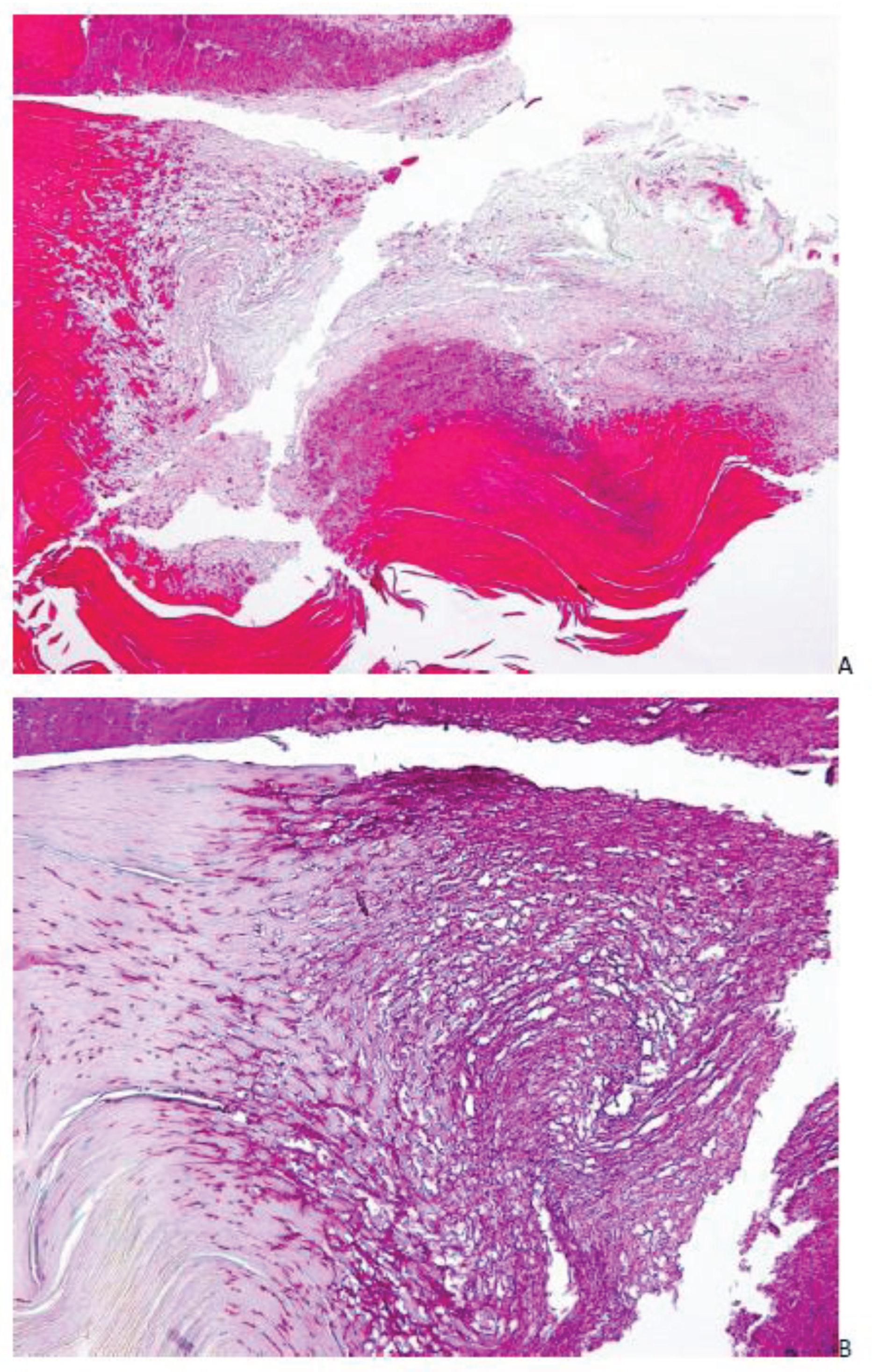
Figure 16.
Biofilm of Fusarium solani at the undersurface of the nail plate. PAS stain, Original magnification 400x. Fungal biofilm at the undersurface of the nail plate.
Figure 16.
Biofilm of Fusarium solani at the undersurface of the nail plate. PAS stain, Original magnification 400x. Fungal biofilm at the undersurface of the nail plate.
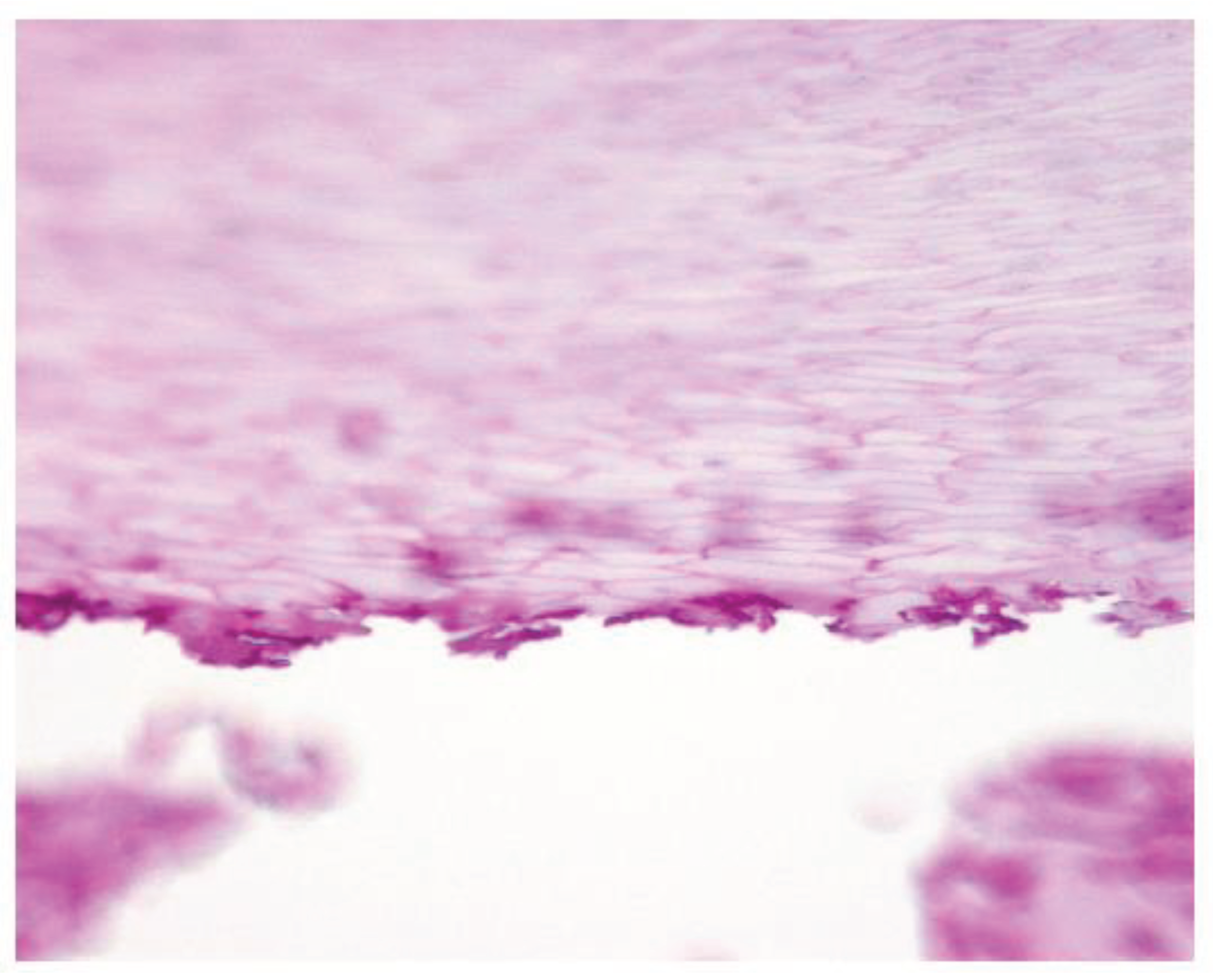
Figure 17.
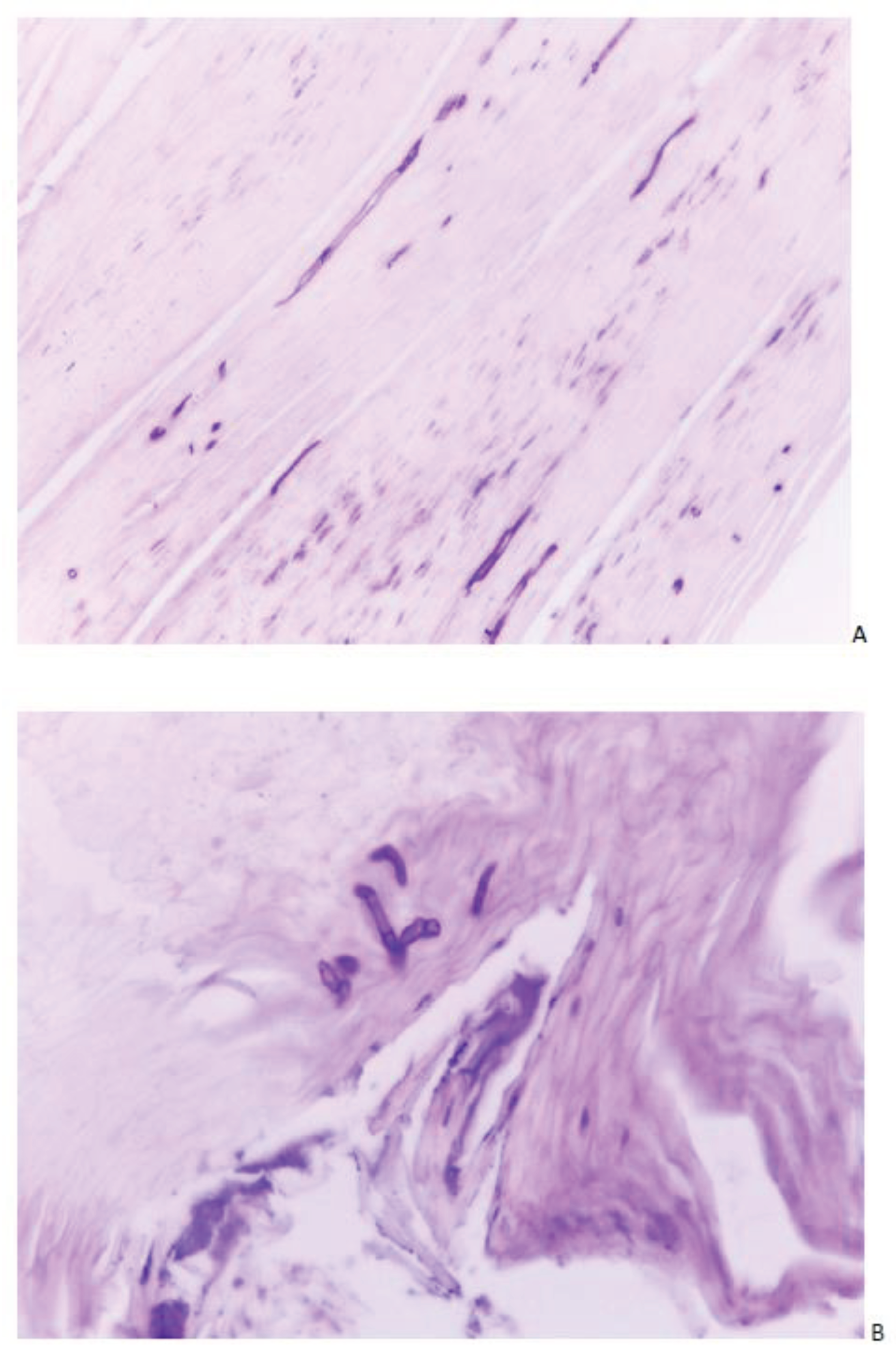
Onychomycosis due to Fusarium solani in a 32-year-old woman. A. Fungal filaments of variable diameter with occasional septae. In the nail which also contains remnants of neutrophils. B. Branching filaments. Histopathology, PAS stain, Original magnification 400x.
Figure 17.
Onychomycosis due to Fusarium solani in a 32-year-old woman. A. Fungal filaments of variable diameter with occasional septae. In the nail which also contains remnants of neutrophils. B. Branching filaments. Histopathology, PAS stain, Original magnification 400x.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



