
Submitted:
30 March 2024
Posted:
01 April 2024
You are already at the latest version
Abstract
This Systematic Review examines studies focusing on tooth bleaching and its effect on healthy enamel or incipient caries and bacterial adhesion. The aim is to explore the impact of different bleaching agents on incipient caries lesions and healthy enamel. Randomized controlled trials, clinical trials, observational studies, and in vitro studies that compared at least two groups were included. A comprehensive search strategy was used to select studies from Pubmed and Scopus databases. Two evaluators performed data extraction, screening, and quality assessment independently. Only studies written in English were included. From 968 initial records, 28 studies were selected for a full-text evaluation. 7 studies were classified as cluster 1 (bacterial adherence on teeth), 12 studies as cluster 2 (no bacteria involved), 4 studies as cluster 3 (no teeth deployment), and 5 clinical studies were cluster 4. Of the selected studies, 6 (21.43%) supported increased bacterial attachment capacity and cariogenic dynamics, 4 (14.29%) decreased adhesion and cariogenic activity, 7 (25%) no difference, and 11 (39.28%) followed a differentiated methodological approach and could not be categorized. Due to different methodology strategies used in the studies of all clusters, the risk of bias was high. Thus, we cannot reach a confident conclusion.
Keywords:
systematic review
; bleaching agents
; carious lesions
; white spots
; enamel microstructure.
1. Introduction
Nowadays, tooth bleaching is a popular, non-invasive aesthetic treatment as many people seek a healthier and more youthful appearance. More adults are undergoing tooth bleaching to improve the esthetic appearance of their teeth [1]. In a 2013 study, approximately 66% of the participants were unsatisfied with their teeth color [2].
Due to the growing demand, the effectiveness of various protocols and materials used by dental professionals has been extensively studied in the last decades, including the longevity of the bleaching outcome [3,4,5,6]. Researchers have conducted clinical and in vitro studies to obtain data that can predict clinical performance and subjective factors related to the bleaching protocol, such as postoperative sensitivity and patients’ satisfaction [7,8,9]. Clinical trials (predominantly randomized) are the most efficient tool to provide reliable evidence to clinicians regarding materials for in-office and at-home bleaching [10,11].
Among the various vital bleaching techniques currently available to clinicians, home bleaching is considered in the literature to be the most effective treatment and ensures predictable color stability [3,9,11]. Many studies conclude that in-office bleaching is less effective than home bleaching. However, many patients and dentists still prefer in-office bleaching [12,13] due to the reduced application time. Also, the efficacy of various concentrations of bleaching agents has been researched extensively. Recent meta-analyses suggest that 10% carbamide peroxide is the most efficient bleaching agent, with negligible adverse effects and sensitivity [14,15].
As dental bleaching is a common practice, it is essential to study the potential effects of this treatment on enamel, bacteria adhesion, and incipient caries.
Several studies have investigated the effect of bleaching on dental tissues. For example, due to home bleaching with 10% carbamide peroxide, enamel microhardness, and structure alterations may affect tooth resistance to mechanical forces [16]. Still, there are other properties that we must take into consideration, such as enamel microroughness [16].
White spot lesions are one of the most frequent and evident adverse effects of orthodontic fixed appliance treatment; nevertheless, the efficacy of various interventions is yet to be addressed and researched. Bleaching agents have an efficient masking effect on white spots as well as incipient caries lesions [17,18].
Incipient caries causes subsurface demineralization underneath a superficially intact layer. The light is scattered differently than the surrounding healthy enamel, giving the spot a chalky white appearance [19]. However, applying carbamide or hydrogen peroxide onto a demineralized exterior layer raises many concerns since previous studies have shown that they affect the contents of minerals on enamel [20,21,22]. However, the long-term impact of bleaching methods on such carious lesions remains uncertain.
Tooth bleaching is associated with a statistically significant short-term decrease in biofilm accumulation and improvement in plaque index [23]. It is still unclear if this decrease is attributed to the effect of bleaching agents or whether the people who have their teeth whitened are at the time more aware of their oral hygiene. However, no data are available to evaluate the long-term effects [23] of this treatment on oral health.
This systematic review aims to answer the questions: “Is there an effect of bleaching agents on incipient caries lesions?” “Is there a difference in the effect of various types of bleaching agents on caries lesions?” and”What is the effect of several bleaching agents on biofilm adhesion and accumulation?”
2. Materials and Methods
This review followed Cochrane’s protocol through Review Manager 5.4.1, the official software of Cochrane’s database [24]. Furthermore, this review's reporting followed the recommendations of the latest PRISMA statement [25]. The present systematic review was registered on the PROSPERO platform (ID number CRD42023424805).
Search Strategy
This Systematic Review examines all studies focusing on bleaching and its effect on healthy enamel or incipient caries, dividing all studies into five groups: a) Bleaching and enamel demineralization, b) Bleaching and bacterial adherence, c) Bleaching and white spots/incipient caries/early caries (esthetic considerations), d) Bleaching and white spots/incipient caries/early caries (mechanical considerations), e) Bleaching agents and antimicrobial activity. The search strategy was based on the combination of the following terms: ((bleaching agents) OR (tooth bleaching) OR (bleaching) OR (tooth whitening) OR (in-office bleaching) OR (home bleaching) OR (carbamide peroxide) OR (hydrogen peroxide)) AND ((white spot lesion) OR (enamel demineralization) OR (early caries) OR (incipient caries) OR (caries) OR (tooth decay) OR (oral hygiene) OR (S. mutans) OR (Streptococcus mutans) OR (Lactobacilli) OR (Lactobacillus) OR (oral microbiome) OR (oral biofilm)). Two examiners (VK and RG) conducted the electronic search using published and unpublished literature separately. The primary formal databases utilized in this study were MEDLINE via Pubmed and Scopus database. The language selected was English. The grey literature reports included theses, dissertations, product reports, and unpublished studies through Cochrane Central, Cochrane Database for Systematic Reviews, ClinicalTrials.com, Open Grey, and ISRCTN. Hand searching was also conducted in the retrieved for full-text evaluation articles for any additional potential for inclusion publication. No filters were used, while the search strategy was performed on April 27, 2023.
Inclusion Criteria
- The review included randomized controlled trials, clinical trials, in vitro studies, and observational studies.
- Studies comparing at least two groups.
- In vitro studies investigating the effect of tooth bleaching agents on the demineralization of enamel analyzed with a confocal laser scanning microscope and/or measured with enamel surface roughness and studies measuring the concentration of cariogenic and periodontal microflora in the surrounding tissues, as well as by the presence of initial or advanced forms of caries.
- Studies assess the effect of bleaching on bacterial adherence to enamel.
- Studies are examining the aesthetic effect of bleaching on white or brown spots of enamel and the mechanical effects of bleaching on early caries lesions.
- Studies investigating any effect of bleaching agents on the prevalence of caries (primary or secondary).
Exclusion Criteria
- Animal studies, case reports, and case series.
- Studies without at least one control and one test group, studies without a comprehensive protocol,
- Studies with ineligible results for this review.
- Lack of access to the full text of a study after attempting to contact the author also resulted in study exclusion.
Data Extraction
Data were extracted and recorded in standardized piloted forms (Zotero 5.0.47, Corporation for Digital Scholarship, and the Roy Rosenzweig Center for History and New Media). These forms include specific characteristics of the study (type, title, authors, abstract, publication, volume, issue, pages, date, series, series title, series text, journal abbreviation, language, DOI, URL, ISSN, short title, mean of access, archive, location in the archive, library catalog, call number, date added, date modified). Data were extracted by two of the reviewers (EP, GG) and re-examined by another two reviewers (VK, CR). Inconsistencies were discussed among reviewers until a consensus was reached.
Screening and Eligibility Check
The studies that were collected from all databases were cross-checked for the exclusion of duplicates. Titles and abstracts were screened independently by four reviewers (E.P., G.G., V.K, C.R.), according to the study's main characteristics of interest, with further exploration of the full text. Each reviewer decided on the inclusion or exclusion of the studies according to eligibility criteria. Potential discrepancies were discussed among reviewers until a consensus was established.
Risk of Bias Assessment (RoB)
Cochrane Risk Of Bias tool 2.0 assessed the methodological quality of the studies for Randomized Controlled Trials [26] and the ROBINS-I (Risk Of Bias In Non-randomized Studies - of Interventions) for controlled trials and observational studies [27]. Furthermore, the GRADE assessment tool was used to rate the strength of clinical recommendations [28].
In this manner, a configuration tool was developed following reporting, performance, and another type of bias. Each section consisted of preselected criteria to reveal poor data disclosure, encoded as “partly specified”, or total absence of examined data encoded as “not specified”. The score “specified” encodes a complete and detailed description. The configuration tool was adjusted to enable assessment of the in vitro, in vivo, and systematic review studies to present comparable data in each category. Studies with the unclear presentation of data were categorized as “partly specified”.
Concerning the in vivo studies, the configuration tool underwent relevant modifications to apply specifically to the characteristics associated with this category. Based on the RoB 2 CRT tool (Sterne JAC, 2019), conversions were embedded to follow the requirements of the present systematic review. The domains followed were the Randomization Process, Deviations from Intended Interventions, Missing Outcome Data, Measurement of Outcome, and Reported Result. These sections consist of modified questions derived from the RoB 2 CRT tool, associated with the preselected criteria, and are met with encoded replies. These responses are PY (probably yes), Y (yes), PN (probably not), N (not), NA (not available).
3. Results
Figure 1 shows the flow chart of the study.
Table 1 presents the categorization of selected studies according to their type.
Out of 968 unique records filtered using an electronic database and hand searches, 28 studies were left for a full-text evaluation by the qualifying criteria.
The principal categorization led to two domains, the in vitro and the in vivo studies. The first division included all types of in vitro studies, counting 23 in total, which underwent further classification, as can be viewed in Table 2.
Study characteristics and qualitative data are detailed in Table 3, Table 4, Table 5 and Table 6. The first cluster has been generated to identify studies that included teeth and microbial factors. The number of studies incorporated in this cluster is 7. The second cluster contained studies involving teeth that did not use microbial cultivation, and the number of them was 12. In the third cluster, studies that did not involve either microbial or dental tissue were aggregated, and their number counts in 4. The fourth cluster included clinical studies.
The fourth cluster contained all the in vivo studies. Three of them concluded that there were no alterations in bacteria counts after bleaching procedures (in saliva, buccal mucosa, and plaque) [55,56,57] whilst one of them showed a decrease in S. mutans in plaque and saliva after bleaching [54]. The in vivo study concerning the masking of white spots after bleaching concluded that there is adequate masking [58].
In the first cluster, one study showed an increase of adhesion of S. mutans [31] after bleaching whilst others showed a decrease of adhesion of S. mutans and thickness biofilm [32] or no difference [35] or not an increase in caries susceptibility [36]. Nevertheless, the study that showed no difference in S. mutans also showed a change in enamel roughness and an increase in S. Sanguis adhesion [35]. For the enamel structure, these studies showed that with or without laser treatment, in addition to bleaching, there was alteration in enamel microstructure [33], but when plasma light treatment was performed, there was not an alteration in enamel microstructure [37].
In the second cluster, one study showed that using 10% carbamide peroxide at white spots decreases color disparities without an alteration in mineral composition [38] but another study showed an increase in the demineralization depth of those lesions [40]. One more study showed that bleaching procedures lead to caries arresting [41], and the studies from Alves et al and Pretty et al showed there is no effect from bleaching on caries [47,49]. Two more studies showed that there is a mineral loss from sound enamel during bleaching but not from carious enamel [42,43]. Concerning the masking effect, one study concludes that there is no sound masking of white spots [45] and two others that there is adequate masking [41,46] and that the masking is better when performing at-home bleaching rather than in-office [46].
Three of the in vitro studies of cluster 3 concluded that there is an increase of adhesion of bacterial biofilm during bleaching procedures on different composites used [50,51,52]. Nevertheless, the fourth study of this cluster showed a higher antibacterial effect of bleaching than chlorhexidine [53].
3.1. Results of Risk of Bias Assessment
The risk of bias in individual studies was assessed based on fixed categorization relative to the design. The procedure followed a modification of the Cochrane Risk of Bias tool 2.0 for Randomized Controlled Trials. The selected studies were categorized, and the risk of bias assessment was evaluated based on the reporting calibration established on the configuration tool as presented in the methodology section (materials and methods). The selected studies were enumerated, categorized, and estimated. All features extracted under the established principle fulfill the predetermined criteria. The characteristics were objectified and presented in the form of evaluative data. The results can be viewed in Figure 2, Figure 3, Figure 4 and Figure 5 for Clusters 1, 2, 3, and 4.
In total, 7 studies were classified as cluster 1, which was dispositioned based on the deployment of teeth and bacteria. In the reporting quality, all studies provided data on the number, state, and origin of teeth, while 28.57% (2) specified the period of teeth storage. Regarding storage and handling of teeth, 85.71% (6) of the studies provided fully specified data. Temperature, a factor that occasionally is omitted, was partially specified in 2 (28.57%) out of 7 studies. The approach of bacterial identity was fully specified, and the development procedure was partially specified in 28.57% (2) of the studies, revealing a relatively high precision comparatively or proportionally to the one followed in teeth identification, preparation, and handling. A relatively high 57.14% (4) of the studies needed to provide specifications for ethical approval by a committee. The performance bias tabloid examination showcased that 6 out of 7 studies provided a partially specified description of the equipment used for teeth preparation, equivalent to 85.71%.
In contrast, only one study provided a fully specified description. The reverse result was observed for the equipment specification deployed for the cariogenic factor development, leading to 85.71% of the studies demonstrating a detailed presentation of the relevant data. Concerning the equipment used for bleaching and the one for measuring the effect of bleaching, all studies presented with complete specifications. Finally, in the first cluster, a study must fully specify the number of examiners participating in these actions. In the “other type of bias” section, no study provided full specifications of the participation of third-party sponsors.
Figure 3 demonstrates the results associated with the “no bacteria involved” cluster. In total, 12 studies were categorized as such, and all contained specified data concerning the number, origin, and state of teeth deployed. Concerning the period of teeth storage, 33.33% (4) of the studies did not provide specified data, while when examining the storage and handling of teeth, 16.67% (2) of the studies did not provide specified data, and 16.67% of the studies provided partially specified data. The investigation or temperature report revealed that 4 out of 12 studies (33.33%) did not provide specified data, and 8.33% (1 study) provided partially specified data. Regarding the demineralization factor, 10 studies (83.33%) contained specified data, and 2 (16.67%) provided partially specified data. Disclosure of the “development of demineralization factor” data led to 7 studies providing specified ones (58.33%) and 5 (41.67%) partially specified. Lastly, an examination of the report of ethical approval revealed that 7 studies did not provide specified data (58.33%) and 5 did (41.67%). In the “performance bias” section, when scrutinizing the equipment used for teeth preparation, 11 studies (91.67%) specified it, and 1(8.33%) provided partially specified data. Examining the equipment used for the demineralization factor, 83.33% (10) of the studies produced specified data, and 16.67% (2) partially specified. When scrutinizing the equipment used for bleaching, the same results were produced as those collected in the “equipment used for the demineralization factor. Additionally, when investigating the equipment used to measure the effect of bleaching, 9 studies (75%) were specified, and 3 (25%) were partially specified. Finally, when investigating the number of examiners, results revealed that 11 studies (91.67%) did not specify the number of scrutineers, while 1 study provided a partial specification (8.33%) of their number, as it did not identify the number of examiners in every stage. In the “other type of bias” section, all 12 studies did not provide specified data concerning third-party sponsoring.
Figure 4 presents the results of studies that did not involve the deployment of teeth. The reporting quality configuration includes all 4 identified studies to disclose specified data concerning the number of specimens deployed. Examining the period of specimens’ storage 50% did not specify data, and 50% provided full specifications. In storing and handling specimens, 2 studies provided specified data, 1 study partially specified, and 1 not specified (50%, 25%, and 25%, respectively). All studies fully specified temperature, which resulted in examining the cariogenic factor and scrutinizing the development of cariogenic procedures, led to the revelation that 75% of the studies contained fully specified data and 25% partially specified. Finally, when acquiring ethical approval, all 4 studies did not provide specific data.
The performance bias section concerning the equipment used for specimen preparation, the demineralization factor, and the one used for bleaching contained specified data for all studies. Examining the equipment used to measure the effect of bleaching on lesions resulted in 75% of the studies providing specified data and 25% partially specified. Finally, no study disclosed data on the number of examiners performing measurements, and the same outcome stood for the “other type of bias”.
In Figure 5, the in vivo studies are clustered and assessed. Four categories were configured. In this section, according to the PRISMA and ROB2 principles, the scoring was formed as “probably yes”, “yes”, “probably not”, “not” and “not available”, depending on the data derived from the study evaluation. In the “randomization process” assessment, three major subcategories were scrutinized. When focusing on possible differences between intervention groups that could be associated with problems in randomization, 1 study (20%) scored “possible yes”, 2 studies “yes” (40%), and the same score was for the “probably not” selection. Concerning the question about the allocation and whether it was concealed until the clusters were assigned and enrolled in the interventions, 2(40%) of the studies scored “probably yes”, 1 (20%) “yes”, 1 (20%) “probably not” and 1 (20%) “not”. Finally, in the question about the randomness of the allocation sequence, 1 (20%) study scored “possibly yes”, 3 (60%) “yes” and 1 (20%) “probably not”. In the “missing outcome data” section, one question was formed for this review and to examine the availability of data for all clusters that recruited participants. The results revealed that 4 (80%) of the studies scored “probably yes” and 1 (20%) “yes”. Assessing the “measurement of outcome”, was performed by two major inquiries. When scrutinizing the “method of measuring the outcome and its possible impropriety,” all studies scored “possibly not”. On the question “Could measurement or ascertainment of the outcome have differed between intervention participants?” 4 (80%) studies scored “probably not” and 1 (20%) “yes”. Finally, in the section “selection of reported result,” the inquiry examined was whether “the data were analyzed in accordance with a pre-specified analysis plan that was finalized before unblinded outcome data were available for analysis,” led to the revelation of 2 (40%) studies scoring “possibly yes” and 3 (60%) “yes”.
3.2. Metanalysis
Initially, all studies were examined to verify the providence of quantitative data. The outcome of the initial examination revealed that all the investigated studies displayed data in qualitative form. There were parts of the data displayed in tables. These parts were in quantitative form, leading to the revelation of 14.29% (4) presenting tables with microhardness measurements performed in various techniques. Two studies (7.14%) demonstrated numeric data on mineral loss measured surfaces, and another 7.14% (2) of the study's means and SDs in color changes.
The nature of this data display, along with studies that did not proceed in an analogous manner, led the researchers to claim contact with the study conductors, aiming to acquire full access to quantitative data as the sole path to enabling meta-analysis calculations.
From all 28 studies, 20 corresponding authors did not reply at all (71.44%) 2 studies did not provide contact details at all (7.14%), 3 corresponding authors replied and provided quantitative data (10.71%), and 3 studies had provided invalid corresponding emails (10.71%). So, due to the lack of information and the heterogeneity of the data the meta-analysis didn’t perform.
Assessing these outcomes, it was unanimously decided by the conductors of this systematic review not to proceed with meta-analysis since the existing quantitative data would not cover the multilateral conclusions from the various clusters examined in the systemic review.
4. Discussion
The effect of tooth whitening on cariogenic activity intrigues the Dental society, and this systematic review attempted to shed light on the methodological approaches.
The number of studies selected for this systematic review fulfills several criteria, which were deployed under the realization that such diversity in approaches and protocol-based regimes would require multiple configuration tools. Performing a casual control on the outcomes of the studies resulted in 6 (21.43%) supporting increased attachment capacity and cariogenic dynamics, 4 (14.29%) decreased adhesion and cariogenic activity, 7 (25%) no difference and 11 (39.28%) approached the subject in a variated manner to such extent that could not be categorized under this fashion. 39.28% of the studies deployed an abundance of variations; thus, organizing them in subgroups necessitated installing a strictly produced tool. Moreover, studies like e.g., “Effect of salivary biofilm on the adherence of oral bacteria to bleached and non-bleached restorative material” Steinberg et al. 1999, generated an outcome that described differentiated behavior between examined strains of bacteria, a fact that forged skepticism on the appropriate categorization and assessment of such studies [51].
On the other hand, a wide range of methods of investigation has been detected. While the primary goal of this review was to produce results based on bias assessment protocols, a fundamental restriction is the fact that the scientific community approaches the subject with an ample range of studies. This fact creates challenges when attempting to configure an objective mechanism of assessment. The existing data concerning the performance of bleaching agents and etching materials create ambiguity, especially regarding the performance of dental tissues and cariogenic factors.
At first glance, the number of studies that resulted in increased cariogenic activity and, on the opposite side, the ones that concluded in decreased cariogenic dynamics consists of 35.72% of the total number of studies, which indicates that further research is required to reach more solid outcomes.
Additionally, almost all in vitro studies (22 out of 23), regardless of the cluster they were categorized, did not provide data concerning the number of examiners, and all 23 studies did not specify sponsoring by private initiatives. This element comes as a response to the fact that studies examine commercial products e.g., “Antibacterial Activity of 10% Carbamide Peroxide Bleaching Agents” Gurgan et al. 1996 [58], and do not provide data for possible private sponsoring or any funding sources.
These factors indicate that certain elements of the studies included in this systematic review, as revealed by the investigative procedure, present a tendency towards bias when examiners focus on commercial products (bleaching agents).
The plethora of individual features examined in the 3 clusters of the in vitro studies showcased that although the overall strategy is articulated, certain areas imply a tendency towards only a fragile demonstration of data qualitative demonstration of data. When it comes to the storage and handling in the reporting quality section, 52.17% of all in vitro studies provided specified data, 13.04% partially specified, and 34.79% not specified, while in the period of storage, 52.17% demonstrated specified data and 47.83% not specified. These features indicate a high proportion of possible bias and are mentioned as a part of the revelation of specific zones of weakness.
This systematic review aims to highlight the need for a scientifically documented and universally accepted practice and not simply follow clinical instructions by experts and established institutions.
The in vivo studies, on the other hand, were met with meticulously performed scrutinizing, and significant data were revealed. When examining the allocation and randomization process, the percentage of those studies with possible bias due to lack of demonstrated specifications was scarce. Judging based on the PRISMA guidelines; the conclusion calls for the requirement of further established formalism when scientific research is performed at the clinical level within the field of Dentistry. Apart from that, in general, the in vivo studies performed satisfactorily.
More specifically, when focusing on the studies that demonstrated an increase in bacterial adhesion, Hosoya et al. in 2003 concluded that agglutination expanded at a minimum up to 500% [31], and Briso et al. in 2015 assumed that the action of bleaching in demineralized enamel influenced the microhardness values, which showed more pronounced changes than the group that was not bleached to a depth of 90μm [25]. On the other hand, Pinto et al. 2009 reached the outcome that carbamide peroxide bleaching promoted mineral loss of sound enamel [42], Berger et al. in 2012 highlighted those bleaching treatments promoted increased sound enamel demineralization, while the addition of Ca ions or ACP did not prevent/reverse these effects [43]. Similarly, Wongpraparatana et al. in 2017 revealed that bleaching with 10% CP or 40% HP increased both S. mutans and S. sanguinis biofilm formation when compared to unbleached specimens on composite resin specimen, while surface roughness increased as well [52].
On the opposite side, Zheng et al. in 2011 showed that the plaque indexes were significantly lower than that before bleaching, with TPI remaining lower than that of the baseline even in the second week after bleaching, a fact that showcased the decrease of the microbial activity [54], Kim et al. in 2016 showed that the 10% carbamide peroxide bleaching of enamel with white spot lesions decreased color disparities and did not only cause deterioration of the mineral composition but also promoted mineral gain in the subsurface body lesion [38]. In the same regime, Zhang et al., in 2021, led to the result that cold-light bleaching could significantly increase enamel surface roughness but inhibit the formation of biofilms of S. mutans till 3 days after the application of bleaching [32].
The demonstration of results that are conflicting raises the requirement for further investigation. This scrutinizing could unveil an overall quantification of these oppositely standing results to conclude with a more solid outcome. As it stands, based on the numerous studies examined in this systematic analysis, it cannot be supported that bleaching plays an aggravating or positive role in white spot lesions, dental tissues, and restoration materials, as well as microbial colonies.
5. Conclusions
Conflicting outcomes were observed on the impact of bleaching agents and methods on incipient caries and biofilm. Most of the studies presented a high risk of bias. This systematic review, acknowledging the limitations associated with a scientific investigation of studies that incorporate a variety of approaches on the same subject, has led to the revelation of some methodological regions that are susceptible to bias. It has yet to be the goal not to compare studies per se, but to investigate methodological grey zones and thus demonstrate the necessity of a more meticulous and precise organization of staging the scientific steps. A metanalysis will be performed in the following stage to investigate the outcomes further.
Author Contributions
“Conceptualization, E.P and C.R.; methodology, C.R.; software, V.K; validation, G.G., V.K. and C.R.; formal analysis, V.K.; investigation, V.K.; resources, G.G. and V.K.; data curation, V.K.; writing—original draft preparation, G.G.; writing—review and editing, C.R, V.K and E.P..; visualization, E.P.; supervision, C.R.; project administration, C.R. All authors have read and agreed to the published version of the manuscript.”.
Funding
“This research received no external funding”.
Data Availability Statement
We encourage all authors of articles published in MDPI journals to share their research data. In this section, please provide details regarding where data supporting reported results can be found, including links to publicly archived datasets analyzed or generated during the study. Where no new data were created, or where data is unavailable due to privacy or ethical restrictions, a statement is still required. Suggested Data Availability Statements are available in section “MDPI Research Data Policies” at https://www.mdpi.com/ethics.
Conflicts of Interest
“The authors declare no conflicts of interest.”.
References
- Kothari, S. , Gray, A.R., Lyons, K., Tan, X.W., Brunton, P.A. Vital bleaching and oral-health-related quality of life in adults: A systematic review and meta-analysis. J Dent 2019, 84, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Al-Zarea, B.K. Satisfaction with appearance and the desired treatment to improve aesthetics. Int J Dent 2013, 2013, ID912368. [Google Scholar] [CrossRef] [PubMed]
- Fernández, E., Bersezio, C., Bottner, J., Avalos, F., Godoy, I., Inda, D., Vildósola, P., Saad, J., Oliveira, O.B. Jr, Martín, J. Longevity, esthetic perception, and psychosocial impact of teeth bleaching by low (6%) hydrogen peroxide concentration for in-office treatment: a randomized clinical trial. Oper Dent 2017, 42, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Geus, J.L., de Lara, M.B., Hanzen, T.A, Fernández E, Loguercio, A.D., Kossatz, S., Reis, A. One-year follow-up of at-home bleaching in smokers before and after dental prophylaxis. J Dent 2015, 43, 1346–1351. [Google Scholar] [CrossRef] [PubMed]
- Moncada, G., Sepúlveda, D., Elphick, K., Contente, M., Estay, J., Bahamondes, V., Fernandez, E., Oliveira, O.B., Martin, J. Effects of light activation, agent concentration, and tooth thickness on dental sensitivity after bleaching. Oper Dent 2013, 38, 467–476. [Google Scholar] [CrossRef] [PubMed]
- Tay, L.Y., Kose, C., Loguercio, A.D., Reis, A. Assessing the effect of a desensitizing agent used before in-office tooth bleaching. J Am Dent Assoc 2009, 140, 1245–1251. [Google Scholar] [CrossRef] [PubMed]
- Kina, J.F., Huck, C., Riehl, H., Martinez, T.C., Sacono, N.T., Ribeiro, A.P., Costa, C.A. Response of human pulps after professionally applied vital tooth bleaching. Int Endod J 2010, 43, 572–580. [Google Scholar] [CrossRef]
- Soares, D.G., Basso, F.G., Hebling, J., de Souza, Costa, C.A. Concentrations of and application protocols for hydrogen peroxide bleaching gels: effects on pulp cell viability and whitening efficacy. J Dent 2014, 42, 185–198. [Google Scholar] [CrossRef] [PubMed]
- Soares, D.G., Basso, F.G., Pontes, E.C., Garcia Lda, F., Hebling, J., de Souza Costa, C.A. Effective tooth-bleaching protocols capable of reducing H2O2 diffusion through enamel and dentine. J Dent 2014, 42, 351–358. [Google Scholar] [CrossRef]
- Paula, E.A., Kossatz, S., Fernandes, D., Loguercio, A.D., Reis, A. Administration of ascorbic acid to prevent bleaching-induced tooth sensitivity: a randomized triple-blind clinical trial. Oper Dent 2014, 39, 128–135. [Google Scholar] [CrossRef]
- Rezende, M., Loguercio, A.D., Kossatz, S., Reis, A. Predictive factors on the efficacy and risk /intensity of tooth sensitivity of dental bleaching: a multi regression and logistic analysis. J Dent 2016, 45, 1–6. [Google Scholar] [CrossRef] [PubMed]
- de Geus, J.L. , Wambier, L.M., Kossatz, S., Loguercio, A.D., Reis, A. At-home vs In-office Bleaching: A Systematic Review and Meta-analysis. Oper Dent 2016, 41(4), 341–356. [Google Scholar] [CrossRef]
- Maran, B.M. , Burey, A., de Paris Matos, T., Loguercio, A.D., Reis, A. In-office dental bleaching with light vs. without light: A systematic review and meta-analysis. J Dent 2018, 70, 1–13. [Google Scholar] [CrossRef]
- Maran, B.M. , Matos, T.P., de Castro, A.D.S., Vochikovski, L., Amadori, A.L., Loguercio, A.D., Reis, A., Berger, S.B. In-office bleaching with low/medium vs. high concentrate hydrogen peroxide: A systematic review and meta-analysis. J Dent 2020, 103, 103499. [Google Scholar] [CrossRef] [PubMed]
- Luque-Martinez, I., Reis, A., Schroeder, M., Muñoz, M.A., Loguercio, A.D., Masterson, D., Maia, L.C. Comparison of efficacy of tray-delivered carbamide and hydrogen peroxide for at-home bleaching: a systematic review and meta-analysis. Clin Oral Investig 2016, 20, 1419–1433. [Google Scholar] [CrossRef]
- Zanolla, J., Marques, A., da Costa, D.C., de Souza, A.S,. Coutinho, M. Influence of tooth bleaching on dental enamel microhardness: a systematic review and meta-analysis. Aust Dent J 2017, 62, 276–282. [Google Scholar] [CrossRef]
- Höchli, D., Hersberger-Zurfluh, M., Papageorgiou, S.N., Eliades, T. Interventions for orthodontically induced white spot lesions: a systematic review and meta-analysis. Eur J Orthod 2017, 39, 122–133. [Google Scholar]
- Bourouni, S., Dritsas, K., Kloukos, D., Wierichs, R.J. Efficacy of resin infiltration to mask post-orthodontic or non-post-orthodontic white spot lesions or fluorosis - a systematic review and meta-analysis. Clin Oral Investig 2021, 25, 4711–4719. [Google Scholar] [CrossRef]
- Hayashi, M., Momoi, Y., Fujitani, M., Fukushima, M., Imazato, S., Kitasako, Y., Kubo, S., Nakashima, S., Nikaido, T., Shimizu, A., Sugai, K., Takahashi, R., Unemori, M., Yamaki, C. Evidence-based consensus for treating incipient enamel caries in adults by non-invasive methods: recommendations by GRADE guideline. Jpn Dent Sci Rev 2020, 56, 155–163. [Google Scholar] [CrossRef]
- Attin, T. , Schmidlin, P.R., Wegehaupt, F., Wiegand, A. Influence of study design on the impact of bleaching agents on dental enamel microhardness. A Review. Dental Materials 2009, 25(2), 143–157. [Google Scholar] [CrossRef]
- Borges, B.C., Borges, J.S., de Melo, C.D., Pinheiro, I.V., Santos, A.J., Braz, R., Montes, M.A. Efficacy of a nivel at-home bleaching technique with carbamide peroxides modified by CPP-ACP and its effect on the microhardness of bleached enamel. Operative dentistry 2011, 65, 521–528. [Google Scholar]
- de Vasconcelos, A.A., Cunha, A.G., Borges, B.C., Vitoriano, Jde O., Alves-Júnior ,C., Machado, C.T., dos Santos, A.J. Enamel properties after tooth bleaching with hydrogen carbamide peroxides in association with a CPP-ACP paste. Acta Odontolgoica Scandinavica 2012, 70, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Sánchez, I., Oteo-Calatayud, J., Serrano, J., Martín, C., Herrera, D. Changes in plaque and gingivitis levels after tooth bleaching: A systematic review. Int J Dent Hyg 2019, 17, 117–129. [Google Scholar] [CrossRef] [PubMed]
- (Review Manager (RevMan) [Computer program]. Version 5.4.1 Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2020.
- Moher, D., Liberati, A., Tetzlaff, J., Altman, D.G. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C., Savović, J., Page, M.J., Elbers, R.G., Blencowe, N.S., Boutron, I., Cates, C.J., Cheng, H.Y., Corbett, M.S., Eldridge, S.M., Emberson, J.R., Hernán, M.A., Hopewell, S., Hróbjartsson, A., Junqueira, D.R., Jüni, P., Kirkham, J.J., Lasserson, T., Li, T., McAleenan, A., Reeves, B.C., Shepperd, S., Shrier, I., Stewart, L.A., Tilling, K., White, I.R., Whiting, P.F., Higgins, J.P.T. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar]
- Sterne, J.A.C., Hernán, M.A., Reeves, B.C., Savović, J., Berkman, N.D., Viswanathan, M., Henry, D., Altman, D.G., Ansari, M.T., Boutron, I., Carpenter, J.R., Chan, A.W., Churchill, R., Deeks, J.J., Hróbjartsson, A., Kirkham, J., Jüni, P., Loke, Y.K., Pigott, T.D., Ramsay, C.R., Regidor, D., Rothstein, H.R., Sandhu, L., Santaguida, P.L., Schünemann, H.J., Shea, B., Shrier, I., Tugwell, P., Turner, L., Valentine, J.C., Waddington, H., Waters, E., Wells, G.A., Whiting, P.F., Higgins, J.P. ROBINS-I: a tool for assessing risk of bias in non-randomized studies of interventions. BMJ 2016, 355, i4919. [Google Scholar]
- Guyatt, G.H., Oxman, A.D., Vist, G.E., Kunz, R., Falck-Ytter, Y., Alonso-Coello, P., Schünemann, H.J.; GRADE Working Group. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 26;336(7650), 924–926. [Google Scholar]
- Page, M.J., McKenzie, J.E., Bossuyt, P.M., Boutron, I., Hoffmann, T.C., Mulrow, C.D., Shamseer, L., Tetzlaff, J.M., Akl, E.A., Brennan, S.E., Chou, R., Glanville, J., Grimshaw, J.M., Hróbjartsson, A., Lalu, M.M., Li, T., Loder, E.W., Mayo-Wilson, E., McDonald, S., McGuinness, L.A., Stewart, L.A., Thomas, J., Tricco, A.C., Welch, V.A., Whiting, P., Moher, D. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021, 29, 372:n71. [Google Scholar]
- Sterne, J.A.C., Savović, J., Page, M.J., Elbers, R.G., Blencowe, N.S., Boutron, I., Cates, C.J., Cheng, H.Y., Corbett, M.S., Eldridge, S.M., Emberson, J.R., Hernán, M.A., Hopewell, S., Hróbjartsson, A., Junqueira, D.R., Jüni, P., Kirkham, J.J., Lasserson, T., Li, T., McAleenan, A., Reeves, B.C., Shepperd, S., Shrier, I., Stewart, L.A., Tilling, K., White, I.R., Whiting, P.F., Higgins, J.P.T. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 2019, 28, 366:l4898. [Google Scholar]
- Hosoya, N., Honda, K., Iino, F., Arai, T. Changes in enamel surface roughness and adhesion of Streptococcus mutans to enamel after vital bleaching. J Dent 2003, 31(8), 543–548. [Google Scholar] [CrossRef]
- Zhang, B., Huo, S., Liu, S., Zou, L., Cheng, L., Zhou, X., Li, M. Effects of Cold-Light Bleaching on Enamel Surface and Adhesion of Streptococcus mutans. Biomed Res Int 2021, 2021, 3766641. [Google Scholar]
- Hou, X., Yuan, K., Huang, Z., Ma, R. Effects of Bleaching Associated with Er:YAG and Nd:YAG Laser on Enamel Structure and Bacterial Biofilm Formation. Scanning, 2021; 20, 6400605. [Google Scholar]
- Voina, C.; Delean, A.; Muresan, A.; Valeanu, M.; Mazilu Moldovan, A.; Popescu, V.; Petean, I.; Ene, R.; Moldovan, M.; Pandrea, S. Antimicrobial Activity and the Effect of Green Tea Experimental Gels on Teeth Surfaces. Coatings 2020, 10, 537. [Google Scholar] [CrossRef]
- Ittatirut, S., Matangkasombut, O., Thanyasrisung, P. In-office bleaching gel with 35% hydrogen peroxide enhanced biofilm formation of early colonizing streptococci on human enamel. J Dent 2014, 42, 1480–1486. [Google Scholar] [CrossRef] [PubMed]
- Al-Qunaian, T.A. The effect of whitening agents on caries susceptibility of human enamel. Oper Dent 2005, 30(2), 265–270. [Google Scholar] [PubMed]
- Nam, S.H., Ok, S.M., Kim, G.C. Tooth bleaching with low-temperature plasma lowers surface roughness and Streptococcus mutans adhesion. Int Endod J 2018, 51, 479–488. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y., Son, H.H., Yi, K., Ahn, J.S., Chang, J. Bleaching Effects on Color, Chemical, and Mechanical Properties of White Spot Lesions. Oper Dent 2016, 41, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Al-Angari, S.S., Lippert, F., Platt, J.A., Eckert, G.J., González-Cabezas, C., Li, Y., Hara, A.T. Bleaching of simulated stained-remineralized caries lesions in vitro. Clin Oral Investig 2019, 23, 1785–1792. [Google Scholar] [CrossRef] [PubMed]
- Briso, A., Silva, Ú., Souza, M., Rahal, V., Jardim Júnior, E. G., Cintra, L. A clinical, randomized study on the influence of dental whitening on Streptococcus mutans population. Aust Dent J 2018, 63, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Jansen, E.E., Meyer-Lueckel, H., Esteves-Oliveira, M., Wierichs, R.J. Do bleaching gels affect the stability of the masking and caries-arresting effects of caries infiltration-in vitro. Clin Oral Investig 2021, 25, 4011–4021. [Google Scholar] [CrossRef]
- Pinto, C.F., Paes Leme, A.F., Cavalli, V., Giannini, M. Effect of 10% carbamide peroxide bleaching on sound and artificial enamel carious lesions. Braz Dent J 2009, 20, 48–53. [Google Scholar] [CrossRef]
- Berger, S. B. , Pavan, S., Dos Santos, P. H., Giannini, M., Bedran-Russo, A. K. Effect of bleaching on sound enamel and with early artificial caries lesions using confocal laser microscopy. Brazilian dental journal 2012, 23(2), 110–115. [Google Scholar] [CrossRef] [PubMed]
- Ogura, K., Tanaka, R., Shibata, Y., Miyazaki, T., Hisamitsu, H. In vitro demineralization of tooth enamel subjected to two whitening regimens. J Am Dent Assoc 2013, 144, 799–807. [Google Scholar] [CrossRef]
- Lee, J. , Okoye, L. O., Lima, P. P., Gakunga, P. T., Amaechi, B. T. Investigation of the esthetic outcomes of white spot lesion treatments. Niger J Clin Pract 2020, 23(9), 1312–1317. [Google Scholar] [PubMed]
- Al-Angari, S. S., Lippert, F., Platt, J. A., Eckert, G. J., González-Cabezas, C., Li, Y., Hara, A. T. Dental bleaching efficacy and impact on demineralization susceptibility of simulated stained-remineralized caries lesions. J Dent 2019, 81, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Alves, E.A. , Alves, F.K., Campos Ede, J., Mathias, P. Susceptibility to carieslike lesions after dental bleaching with different techniques. Quintessence Int 2007, 38(7), e404–9. [Google Scholar] [PubMed]
- Al-Shahrani, A. A., Levon, J. A., Hara, A. T., Tang, Q., Lippert, F. The ability of dual whitening anti-caries mouthrinses to remove extrinsic staining and enhance caries lesion remineralization - An in vitro study. J Dent 2020, 103S, 100022. [Google Scholar]
- Pretty, I.A. , Edgar, W.M., Higham, S.M. The effect of bleaching on enamel susceptibility to acid erosion and demineralisation. Br Dent J, 2005, 12;198(5), 285-90.
- Mor, C. , Steinberg, D., Dogan, H., Rotstein, I. Bacterial adherence to bleached surfaces of composite resin in vitro. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998, 86(5), 582–586. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, D., Mor, C., Dogan, H., Zacks, B., Rotstein, I. Effect of salivary biofilm on the adherence of oral bacteria to bleached and non-bleached restorative material. Dent Mater 1999, 15, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Wongpraparatana, I., Matangkasombut, O., Thanyasrisung, P., Panich, M. Effect of Vital Tooth Bleaching on Surface Roughness and Streptococcal Biofilm Formation on Direct Tooth-Colored Restorative Materials. Oper Dent 2018, 43, 51–59. [Google Scholar] [CrossRef]
- Gurgan, S., Bolay, S., Alaçam, R. Antibacterial activity of 10% carbamide peroxide bleaching agents. J Endod 1996, 22, 356–357. [Google Scholar] [CrossRef]
- Zheng, C.Y., Pan, J., Wang, L., Zhang, C.F. Effects of hydrogen peroxide-containing bleaching on cariogenic bacteria and plaque accumulation. Chin J Dent Res 2011, 14, 47–52. [Google Scholar]
- Briso, A. L. , Gonçalves, R. S., Costa, F. B., Gallinari, M.deO., Cintra, L. T., Santos, P. H. Demineralization and hydrogen peroxide penetration in teeth with incipient lesions. Braz Dent J 2015, 26(2), 135–140. [Google Scholar] [CrossRef] [PubMed]
- Alkmin, Y.T. , Sartorelli, R., Flório, F.M., Basting, R.T. Comparative study of the effects of two bleaching agents on oral microbiota. Oper Dent 2005, 30(4), 417–423. [Google Scholar] [PubMed]
- Knösel, M., Attin, R., Becker, K., Attin T. External bleaching effect on the color and luminosity of inactive white-spot lesions after fixed orthodontic appliances. Angle Orthod 2007, 77, 646–652. [Google Scholar] [CrossRef]
- Franz-Montan, M., Ramacciato, J. C., Rodrigues, J. A., Marchi, G. M., Rosalen, P. L., Groppo, F. C. The effect of combined bleaching techniques on oral microbiota. Indian J Dent Res 2009, 20, 304–307. [Google Scholar] [CrossRef]
Figure 1.
Flow chart of the study showing number of studies during identification and screening.
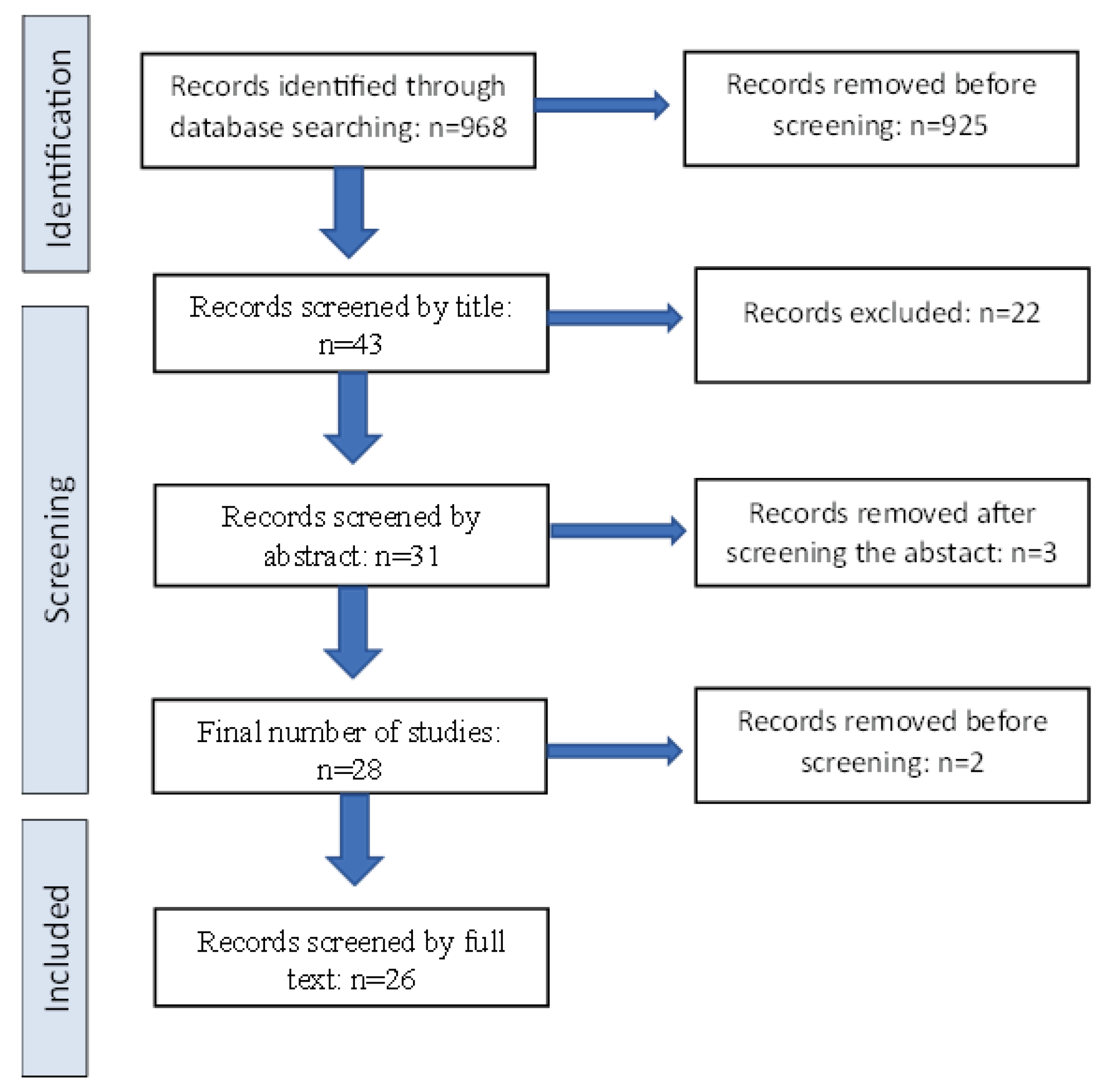
Figure 2.
Evaluative data of cluster 1.
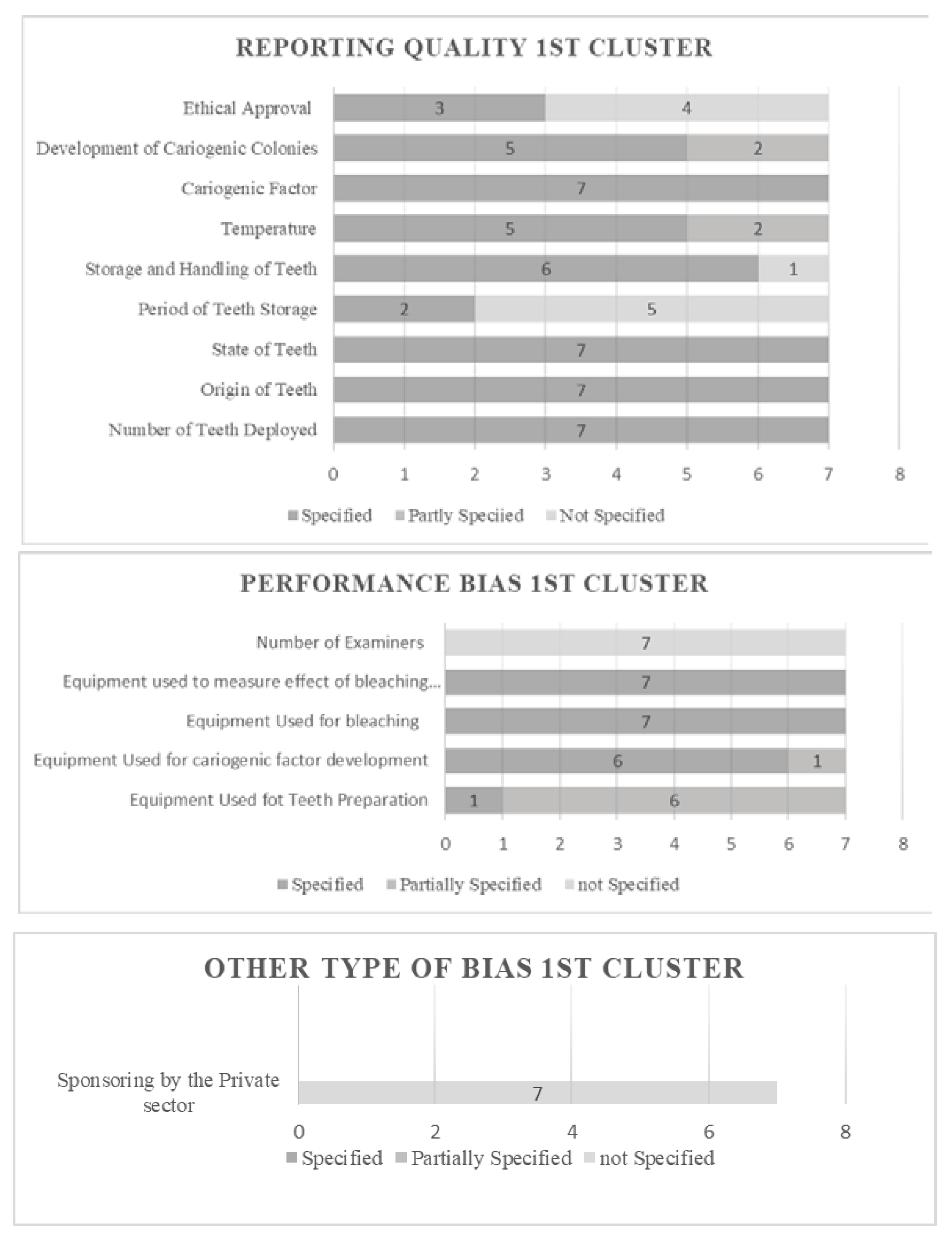
Figure 3.
Evaluative data of cluster 2.
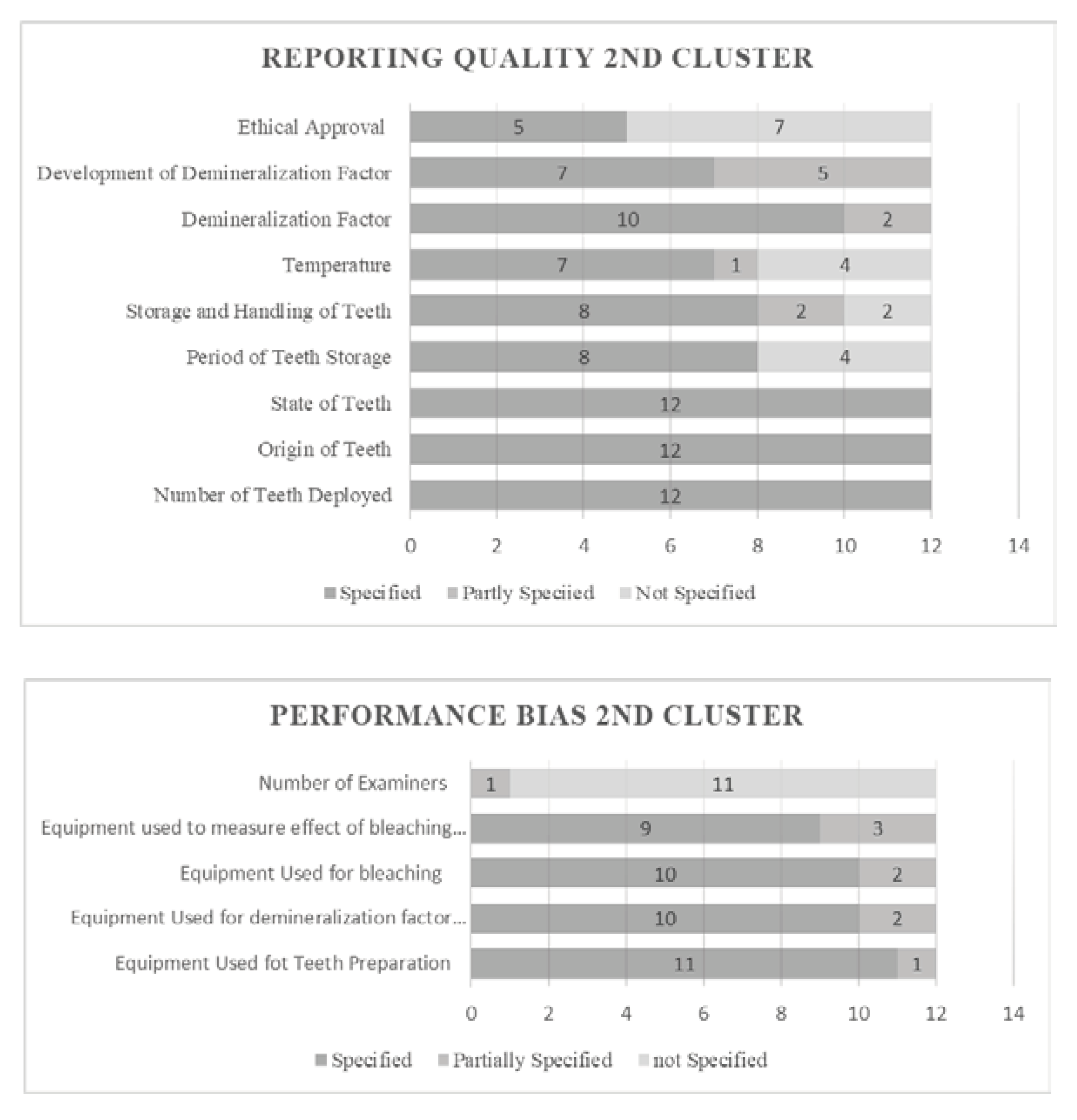
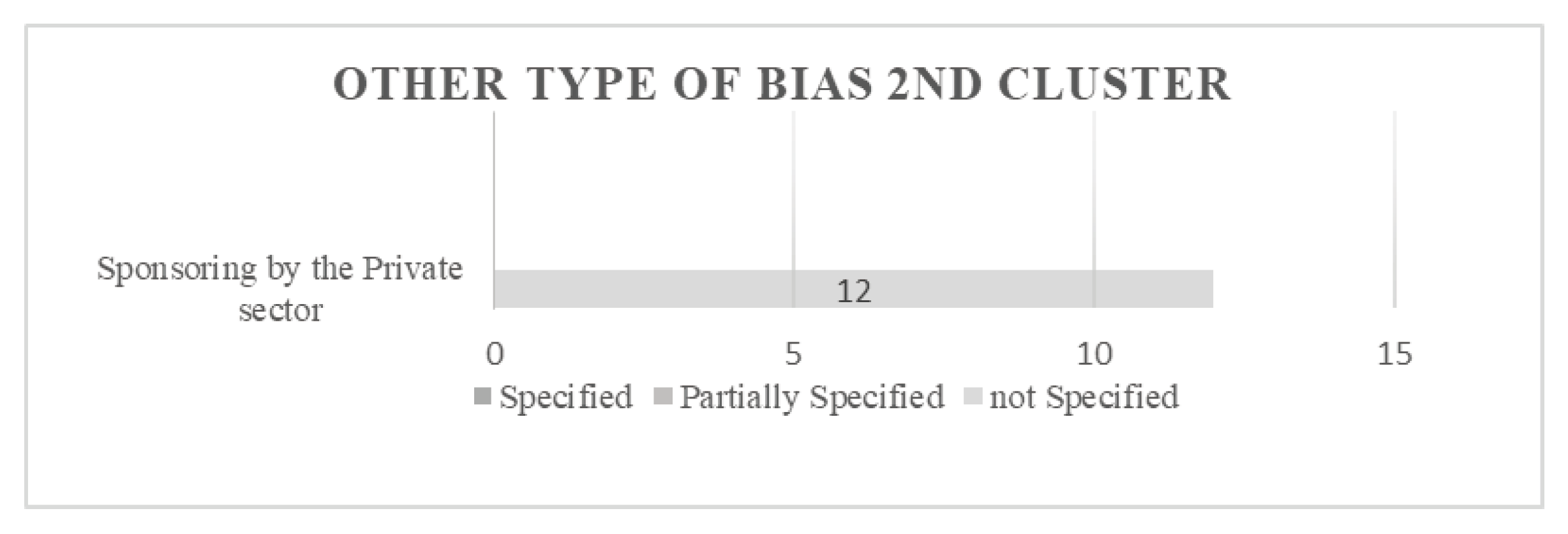
Figure 4.
Evaluative data of cluster 3.
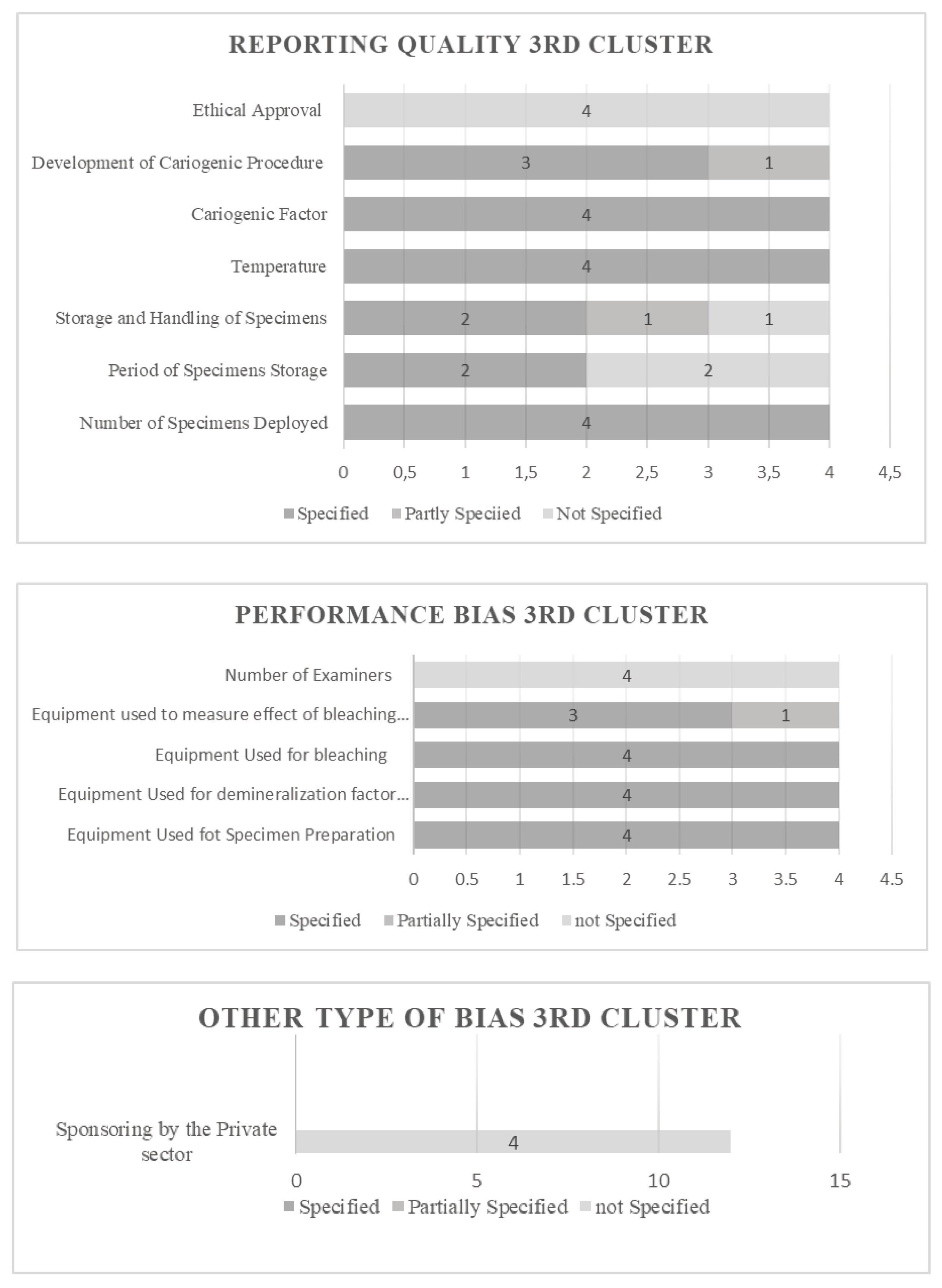
Figure 5.
Clustering of in vivo studies.
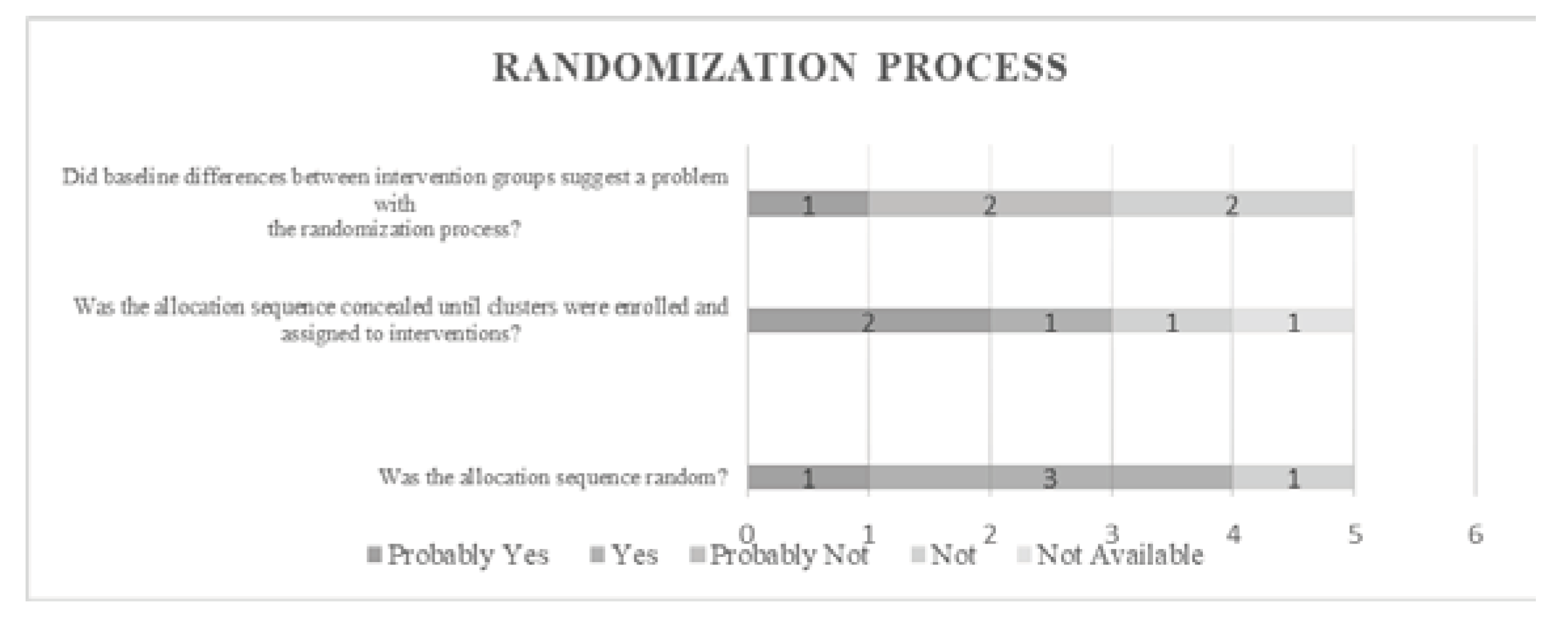
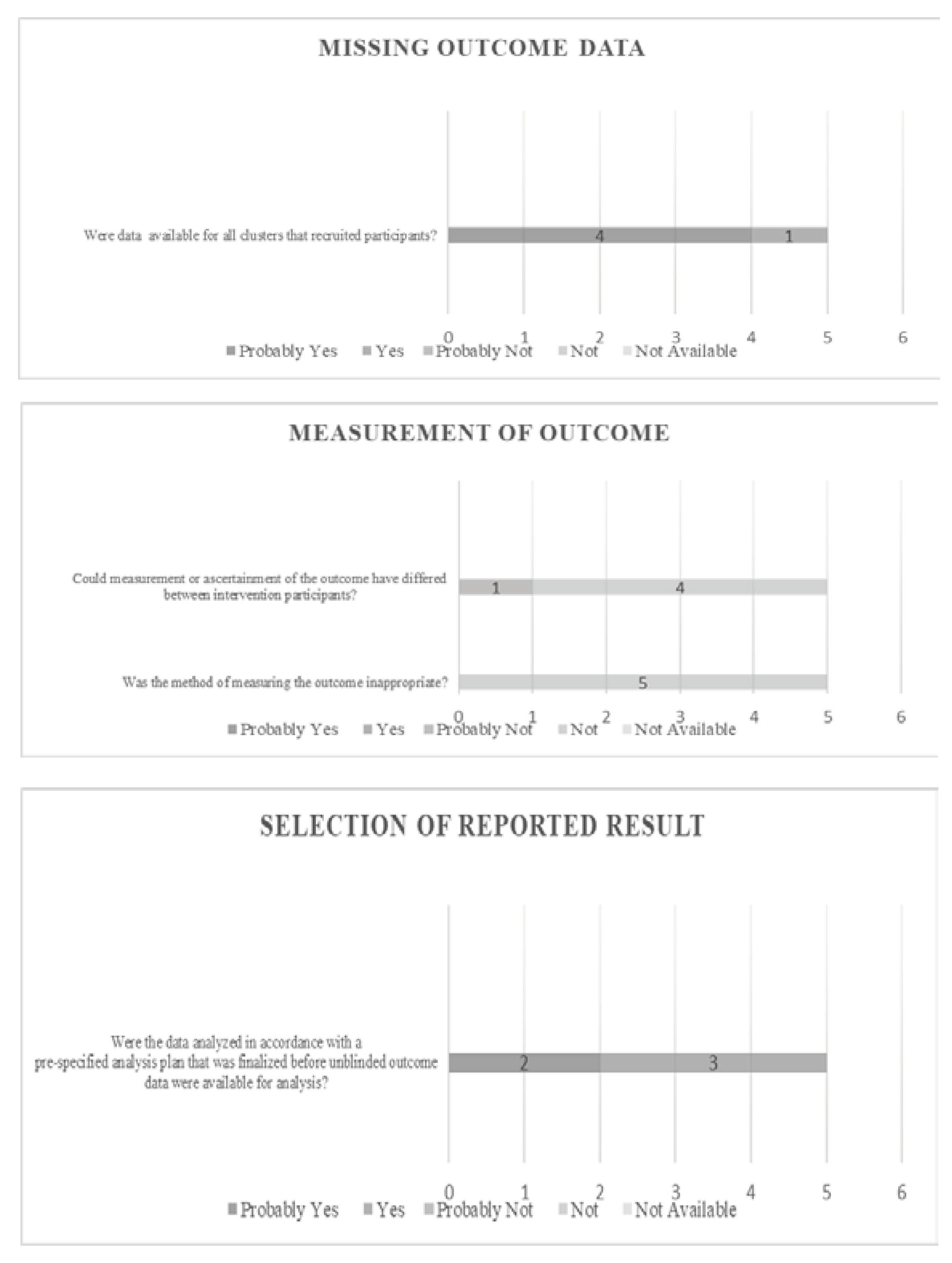

Table 1.
Categorization of selected studies following their type.
| In Vitro | 23 |
| Clinical | 5 |
| Total number of studies | 28 |
Table 2.
Categorization of in vitro studies.
| Cluster 1 | 7 |
| Cluster 2 | 12 |
| Cluster 3 | 4 |
| Total Number of studies | 23 |
Table 3.
Study characteristics and qualitative data (cluster 1).
| Study | Aim | Design | Sample size & basic features | Findings | |
|---|---|---|---|---|---|
| 1. | “Changes in enamel surface roughness and adhesion of Streptococcus mutans to enamel after vital bleaching” Hosoya et al. 2003 [31] | In vitro study aiming at observing the influence of vital bleaching on changes to the enamel surface and adhesion of S.mutans to tooth enamel | In vitro | 70 fresh human impacted third molars - 50 ml of pre-cultivated S. mutans (109 CFU/ml) |
Teeth displayed increased adhesion of S. mutans colonies. |
| 2. | “Effects of Cold-Light Bleaching on Enamel Surface and Adhesion of Streptococcus mutans” Zhang et al. 2021 [32] |
Investigation of how cold-light bleaching would change enamel roughness and adhesion of S. mutans. |
In vitro | Twenty-four maxillary premolars extracted for orthodontic purpose |
The roughness of enamel surfaces was Increased after bleaching -The adhesion of S. mutans was decreased on bleached enamel in turbidity test - The thickness of biofilms was decreased on bleached enamel - S. mutans were less inclined to adhere on bleached enamel from analysis of CLSM (Confocal Laser Scanning Microscopy) |
| 3. | “Effects of Bleaching Associated with Er:YAG and Nd:YAG Laser on Enamel Structure and Bacterial Biofilm Formation” Hou et al. 2021 [33] | To compare the effects of bleaching associated with Er:YAG and Nd:YAG laser on enamel structure and mixed biofilm formation on teeth surfaces | In vitro | Sixty-eight enamel samples were prepared from sound permanent thirdmolars | The enamel surface structure significantly changed after bleaching with or without laser treatment |
| 4. | “Antimicrobial Activity and the Effect of Green Tea Experimental Gels on Teeth Surfaces” Voina et al. 2020 [34] |
To evaluate an experimental green tea extract and an experimental green tea gel for enamel restoring treatment after bleaching. We also tested the antibacterial and antifungal effect of the experimental extract against specific endodontic and cariogenic microorganisms | In vitro | Twenty-eight healthy third molars, extracted for orthodontic purposes | The green tea extract solution exerts an important antibacterial effect on P. anaerobius and S. mutans strains / The natural extract based on Camellia sinensis has antimicrobial activity / The experimental extract has no antifungal action on the C. albicans strain |
| 5. | “In-office bleaching gel with 35% hydrogen peroxide enhanced biofilm formation of early colonizing streptococci on human enamel” Ittatirut et al. 2014 [35] | To compare the effects of 25% and 35% hydrogen peroxide in-office bleaching systems on surface roughness and streptococcal biofilm formation on human enamel |
In vitro | 162 enamel specimens were prepared from sound permanent anterior and premolar teeth | Bleaching with both 25% and 35% H2O2 systems significantly decreased the enamel surface roughness comparing to the control - S. sanguis biofilm formation on enamel bleached with 35% H2O2 was markedly higher - no significant difference in S. mutans |
| 6. | “The Effect of Whitening Agents on Caries Susceptibility of Human Enamel” Al-Qunaian et al. 2005 [36] |
This in vitro study evaluated whether the treatment of human enamel with whitening agents containing different concentrations of carbamide or hydrogen peroxide changes the susceptibility of enamel to caries |
In vitro | 24 sound human incisors were selected – 3 groups were created | Application of bleaching agents does not increase caries susceptibility of human enamel. A bleaching agent-containing fluoride reduced caries susceptibility |
| 7. | “Tooth bleaching with low temperature plasma lowers surface roughness and Streptococcus mutans adhesion” Nam et al. 2017 [37] | To evaluate the structural-morphological changes in enamel surface roughness and Streptococcus mutans adhesion after tooth bleaching using plasma in combination with a low concentration of 15% carbamide peroxide (CP) | In vitro | 60 single-rooted human premolars with intact crowns extracted for orthodontic reasons | The application of plasma did not cause structural and morphological changes in enamel. Combination bleaching methods using plasma and low concentrations of 15% CP are less destructive, especially with respect to tooth surface protection |
Table 4.
Study characteristics and qualitative data (cluster 2).
| Study | Aim | Design | Sample size & basic features | Findings | |
|---|---|---|---|---|---|
| 1. | “Bleaching Effects on Color, Chemical, and Mechanical Properties of White Spot Lesions” Kim et al. 2016 [38] | The purpose of the study was to evaluate the effect of bleaching on teeth with white spot lesions | In vitro | Twenty human upper premolars extracted during dental treatments were used | 10% carbamide peroxide bleaching of enamel with white spot lesions decreased color disparities without deteriorating mineral composition or microhardness. The application of CPP-ACP paste promoted mineral gain in the subsurface body lesion |
| 2. | “Bleaching of simulated stained-remineralized caries lesions in vitro” Angari et al. 2018 [39] | This study aimed to develop laboratory models to create stained-remineralized caries-like lesions (s-RCLs) and to test the efficacy of bleaching on their esthetic treatment | In vitro | Enamel and dentin slabs (4 × 4 × 2 mm) were sectioned from the buccal and lingual area of human molars | The laboratory models developed in this investigation are able to create stained-remineralized caries-like lesions in both enamel and dentin. Non-metallic stains are lighter in color and more responsive to bleaching treatment compared to metallic stains |
| 3. | “Demineralization and Hydrogen Peroxide Penetration in Teeth with Incipient Lesions” Briso et al. 2015 [40] | The aim of this study was to evaluate the demineralization and hydrogen peroxide penetration in teeth with incipient lesions submitted to bleaching treatment | In vitro | One hundred sound permanent bovine incisors obtained from steers aged between 24 and 30 months were selected | Application of bleaching agents in previously demineralized enamel favors HP penetration through the tooth structure and the bleaching treatment can increase the demineralization depth of incipient lesions |
| 4. | “Do bleaching gels affect the stability of the masking and caries-arresting effects of caries infiltration—in vitro” Jansen et al. 2020 [41] | The aim of this study was to evaluate the influence of different bleaching gels on the masking and caries-arresting effects of infiltrated and non-infiltrated stained artificial enamel caries lesions | In vitro | Bovine incisors were extracted from freshly slaughtered cattle (negative BSE test), cleaned, and preserved in 0.08% thymol. The teeth were separated in 400 enamel blocks | Under the pH-cycling conditions chosen, the tested bleaching agents could successfully recover the visual appearance of infiltrated and non-infiltrated stained caries-like enamel lesions. The masking and the caries-arresting effects of infiltrated lesions remained stable after bleaching and pH-cycling |
| 5. | “Effect of 10% Carbamide Peroxide Bleaching on Sound and Artificial Enamel Carious Lesions” Pinto et al. 2009 [42] | This study evaluated the effect of 10% carbamide peroxide (CP) bleaching on Knoop surface microhardness (KHN) and morphology of sound enamel and enamel with early artificial caries lesions (CL) after pH-cycling model (pHcm) | In vitro | 40 blocks with known surface microhardness were selected made of extracted human third molars that had been erupted | Carbamide peroxide bleaching promoted mineral loss of sound enamel. Although, the bleaching procedure did not exacerbate mineral loss of the carious enamel, it should be indicated with caution on enamel with caries activity |
| 6. | “Effect of Bleaching on Sound Enamel and with Early Artificial Caries Lesions Using Confocal Laser Microscopy” Berger et al. 2012 [43] | The aim of this study was to evaluate effect of bleaching agents on sound enamel (SE) and enamel with early artificial caries lesions (CL) using confocal laser scanning microscopy (CLSM) | In vitro | Twenty extracted sound bovine incisors stored in 0.1% thymol solution were used within 1 month of extraction - Eighty blocks (4 x 5 x 5 mm) of enamel were formed | The bleaching treatments promoted increased sound enamel demineralization, while the addition of Ca ions or ACP did not prevent/reverse the effects caused by the bleaching treatment in both conditions of the enamel - Early artificial caries induced by pH cycling model were not affected by the bleaching treatment |
| 7. | “In vitro demineralization of tooth enamel subjected to two whitening regimens” Ogura et al. 2013 [44] | To examine the level of in vitro demineralization of human tooth enamel after bleaching by using two common bleaching regimens: home bleaching (HB) and office bleaching (OB) with photoirradiation | In vitro | 30 human premolars without stain or defect that had been extracted for orthodontic indications | OB is preferable to HB on the basis of the surface integrity of treated enamel during in vitro demineralization |
| 8. | “Investigation of the Esthetic Outcomes of White Spot Lesion Treatments” Lee 2022 [45] | To compare the ability of bleaching, resin infiltration and microabrasion to restore the appearance of existing white spot lesions (WSL) | In vitro | Extracted human maxillary incisor teeth – Only teeth with WSLs were selected | Among the three investigated treatment modalities, resin infiltration was able to mask WSLs the most |
| 9. | “Dental bleaching efficacy and impact on demineralization susceptibility of simulated stained-remineralized caries lesions” Al-Angari et al. 2018 [46] | To evaluate the efficacy of different bleaching systems on artificially created stained-remineralized caries lesions; and to assess the susceptibility of the bleached lesions to further demineralization | In vitro | Human enamel slabs embedded in acrylic blocks and polished (n=21 per treatment group) | At-home bleaching (15% CP) leads to greater color improvement of remineralized-stained lesions than in-office bleaching (40% HP) |
| 10. | “Susceptibility to caries like lesions after dental bleaching with different techniques” Alves et al. 2007 [47] | To assess the influence of dental bleaching on the susceptibility of developing carieslike lesions | In vitro | 30 unerupted human third molars | In office dental bleaching 37% CP (halogen light) – 35% HP (LED light) does not influence caries like lesions development /home bleaching 10% and 16% CP with 0.2% sodium fluoride reduces susceptibility |
| 11. | “The ability of dual whitening anti-caries 444 to remove extrinsic staining and enhance caries lesion remineralization – An in vitro study” Al-Shahrani et al. 2020 [48] | To investigate the ability of dual whitening anti-caries mouthrinses to remove extrinsic staining from artificially stained caries lesions and to enhance their remineralization and fluoridation | In vitro | Bovine enamel specimens / Teeth crowns were cut into 4x4 mm2 / A total of 250 specimens were prepared | Artificially stained enamel caries lesions shows reduced susceptibility tofluoride remineralization and whitening effects of commercial whitening and anti-caries mouthrinses |
| 12. | “The effect of bleaching on enamel susceptibility to acid erosion and demineralization “Pretty et al. 2005 [49] | To determine if enamel that had been bleached by carbamide (urea) peroxide gel (CPG) was at increased risk of either acid erosion or demineralisation (early caries) than un-bleached enamel | In vitro | 24 human incisors selected with specified criteria | Tooth bleaching with carbamide (urea) peroxide (using commercially available concentrations) does not increase the susceptibility of enamel to acid erosion or caries |
Table 5.
Study characteristics and qualitative data (cluster 3).
| Study | Aim | Design | Sample size & basic features | Findings | |
|---|---|---|---|---|---|
| 1. | “Bacterial adherence to bleached surfaces of composite resin in vitro” Mor et al. 1998 [50] | To examine the effect of bleaching agents on bacterial adherence to polished surfaces of composite resin restorations | In vitro | 162 samples of Polofil Supra light-curing resin-based composite (Voco, Cuxhaven, Germany) were used | The results of this study indicate that both carbamide peroxide and hydrogen peroxide can change the adherence characteristics of several microorganisms with regard to polished surfaces of composite resin |
| 2. | “Effect of salivary biofilm on the adherence of oral bacteria to bleached and non-bleached restorative material” Steinberg et al. 1999 [51] | The objective of this work was to examine the effect of in vitro salivary biofilm on the adherence of oral bacteria to bleached and non-bleached restorative material | In vitro | 162 samples of Charisma Supra-light-curing resin-based composite | Salivary biofilm on Charisma pre-treated with bleaching agents, altered the adhesion of S. mutans, S. sobrinus and A. viscosus |
| 3. | “Effect of Vital Tooth Bleaching on Surface Roughness and Streptococcal Biofilm Formation on Direct Tooth-Colored Restorative Materials” Wongpraparatana et al. 2017 [52] | To compare the effect of simulated bleaching with a 10% carbamide peroxide (CP) or a 40% hydrogen peroxide (HP) system on surface roughness of resin composite and resin-modified glass ionomer cement (RMGI) and streptococcal biofilm formation on these surfaces |
In vitro | 2 restorative materials were used: a nanofilled resin composite material and an RMGI. 108 specimens of each material in shade A2 were fabricated into disks of 5 mm in diameter and 2mm thick | The bleaching systems used, 10% CP or 40% HP, significantly increased both the surface roughness and the streptococcal biofilm formation on resin composite and resin-modified glass ionomer cement |
| 4. | “Antibacterial Activity of 10% Carbamide Peroxide Bleaching Agents” Gurgan et al. 1996 [53] | To examine the antibacterial activity of three commercial 10% carbamide peroxide bleaching agents (Nite White, Karisma, and Opalescence) on S. mutans, S. mitis, S. sanguis, Lactobacillus casei, and Lactobacillus acidophilus | In vitro | S. mutans (type A, 10919), S. mitis (type A, 4a), S. sanguis (type A, 6b), Lactobacillus casei (type 319), and Lactobacillus acidophilus (type A, 161) | All three bleaching materials demonstrated higher antibacterial effect than the 0.2% chlorhexidine solution |
Table 6.
Study characteristics and qualitative data (cluster 4).
| Study | Aim | Design | Sample size & basic features | Findings | |
|---|---|---|---|---|---|
| 1. | “Effects of Hydrogen Peroxide – containing Bleaching on Cariogenic Bacteria and Plaque Accumulation” Zheng et al. 2011 [54] | To evaluate the effects of a commercial bleaching agent containing 36% hydrogen peroxide on the clinical plaque index and S. mutans and Lactobacilli counts in dental plaque and saliva | In vivo / clinical | 20 medically fit adult volunteers | The S. mutans counts in plaque and saliva 4 weeks after bleaching were significantly decreased compared to that before bleaching |
| 2. | “A clinical, randomized study on the influence of dental whitening on Streptococcus mutans population” Briso et al. 2017 [55] | To evaluate the influence of at-home whitening treatment on Streptococcus mutans in saliva, buccal mucosa, and subgingival and supragingival plaque | Clinical – in vivo | 30 individuals were selected, meeting the criteria for inclusion | No change was observed when whitening was performed with carbamide peroxide. Similarly, no change was found in the bacterial population in saliva and buccal mucosa during the whitening treatment with any products |
| 3. | “Comparative Study of the Effects of Two Bleaching Agents on Oral Microbiota” Alkmin et al. 2005 [56] | This study evaluated the in vivo effects of bleaching agents containing 10% carbamide peroxide (Platinum/Colgate) or 7.5% hydrogen peroxide (Day White 2Z/Discus Dental) on S. mutans during dental bleaching | In vivo | 30 volunteers who needed dental bleaching | No alterations were found in the s.mutans group count during bleaching treatment with bleaching agents containing 10% carbamide peroxide or 7.5% hydrogen peroxide |
| 4. | “External Bleaching Effect on the Color and Luminosity of Inactive White-Spot Lesions after Fixed Orthodontic Appliances” Knosel et al. 2007 [57] | To evaluate the effect of external bleaching on the color and luminosity of inactive white-spot lesions (WSLs) present after fixed orthodontic appliance treatment | In vivo/ clinical | Ten patients with inactive WSLs after therapy with fixed orthodontic appliances | External bleaching is able to satisfactorily camouflage WSLs visible after therapy with fixed orthodontic appliances |
| 5. | “The effect of combined bleaching techniques on oral Microbiota” Franz-Montan et al. 2009 [58] | To evaluate the antimicrobial activity of 10% and 37% carbamide peroxide during dentalbleaching in 3 different modes | In vivo | 32 volunteers assigned to 4 groups (n = 8). | In conclusion, the carbamide peroxide when used at 37%, 10%, or in combination, did not affect human salivary microorganisms tested |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



