Submitted:
25 March 2024
Posted:
26 March 2024
You are already at the latest version
Abstract
Keywords: gut microbiota; small intestinal bacteria overgrowth; SIBO; diet, dysbiosis; microbial ecology.
Keywords:
mikroflora jelitowa
; przerost bakterii jelita cienkiego
; SIBO
; dieta
; dysbioza
; ekologia mikrobiologiczna.
1. Introduction
The gut microbiota is now considered as one of the key element contributing to the regulation of host health. It is estimated that the gut microbiota is made up of about 1014 cells — more than ten times the number of cells that constitute the human body. It is one of the most diverse ecosystems, individual and unique as a fingerprint, with up to approx. 1,500 different species [1,2]. In recent years, thanks to significant advances in the technology of diagnostic methods, the knowledge of the role of the intestinal microbiota in the human body, which, as is now known, is not limited to the processes of digestion and absorption of nutrients but performs a wide variety of functions, is being expanded. Intestinal bacteria affect the various organs of the entire body, including the central nervous system. They can even modulate the behavior of the body through the synthesis of various chemical compounds such as serotonin and precursors of neurotransmitters, shape metabolism, and immunity, which play a vital role in the treatment of many disease entities [2,3]. The correct quantitative and qualitative composition of the intestinal microbiota, referred to as eubiosis, alters the maintenance of hemostasis and thus the health of the entire human body, while dysbiosis — a quantitative, qualitative, or both disruptions of the bacterial balance, can cause or exacerbate the course of various pathologies [4]. Abnormal translocation of the intestinal microbiota from the large intestine to the small intestine can result in small intestinal bacterial overgrowth syndrome, abbreviated as SIBO [5]. The excessive proliferation of carbohydrate‒fermenting bacteria with gas production in the small intestine results in the accumulation of carbohydrates, as well as the accumulation of other products of bacterial metabolism, causing a wide range of ailments beyond the gastrointestinal tract [5].
2. Gut Microbiota
The gastrointestinal tract is the second-largest system of the human body after the cardiovascular system. The small intestine is about 6‒7 m long and is the longest part of the digestive tract (with a total length of about 8‒9 m), consisting of the duodenum, jejunum, and ileum [6,7]. The presence of numerous pits, folds, crypts, and villi markedly increases the absorptive surface of the small intestine. The intestinal villi are covered with capillary epithelial tissue composed of individual hairs that produce digestive enzymes. These so‒called microvilli, due to their structure, increase the absorptive surface of the small intestine and are primarily responsible for the absorption into the capillaries of the products of digestion of carbohydrates and proteins from the gastrointestinal tract [1]. After absorption of micro and macronutrients from the small intestine, thanks to the peristaltic movements of the microvilli, food residues move to the last section of the digestive tract — the large intestine — where mineral salts, vitamins, some drugs are absorbed, water is recovered, resulting in a thickening of the digestive contents. Moreover, thanks to the presence of very abundant bacterial flora, abundant in such species as Escherichia coli and Enterobacter aerogenes, among others, the synthesis of vitamin K and folic acid is possible [1]. Pre‒digested, still liquid food content enters from the last segment of the small intestine — the ileum — into the cecum through the ileocecal valve, the mechanism of which ensures the irreversible, unidirectional transport of food debris. It also prevents the transmission of elements of the large intestinal microbiota into the small intestine, which could adversely result in the accumulation of harmful products of bacterial fermentation, such as hydrogen, carbon dioxide, and methane [1,8].
The human body, from birth to death, is colonized by a vast number of microorganisms — bacteria, viruses, fungi, which are commensals, symbionts, as well as species with pathogenic potential — their collection is the microbiota [9]. The term microbiome was first used in the 2001 by American geneticist and a microbiologist — Joshua Lederberg, a Nobel Prize winner (in 1958 in physiology and medicine for his discovery of the mechanisms of genetic recombination in bacteria), to describe the genome of all microorganisms inhabiting the human body [10]. The advancement of molecular techniques at the end of the 20th century and their participation in the isolation and identification of microorganisms significantly influenced the development of knowledge about the composition and importance of the human microbiome. It has been shown that the number of microorganisms residing in the human body more than ten times exceeds the number of cells making it up. Most microorganisms colonize the gastrointestinal tract — it is estimated that there are about 2 kg of microorganisms in the large intestine [8].
The microbiota of the gastrointestinal tract significantly influences the immune function of the entire body, the processing of nutrients, and many other significant vital processes that allow the maintenance of psychosomatic health. It causes the breakdown of food residues through fermentation, promotes the formation of essential B vitamins and vitamin K, as well as the formation of short-chain fatty acids (SCFAs), which are a source of energy for colon epithelial cells [11]. Thanks to the microorganisms of the intestinal microbiota, minerals, and electrolytes, e.g., sodium, magnesium, calcium, and potassium, are better absorbed, and the production of hydrolases affects the metabolism of fats in the liver, and thus the metabolism of cholesterol and fatty acids. In addition, by competing for habitat and nutrients and producing bacteriocins, they prevent the growth of potentially pathogenic bacteria [8].
Microorganisms form a diverse ecosystem, dynamically modified throughout a lifetime under the influence of many factors: diet, antibiotics/chemotherapeutics used, age, lifestyle, social and economic conditions, stress, as well as metabolites produced by bacterial cells. The oral cavity is abundant in microbiota, as it is made up of about 700 different species of bacteria; the upper gastrointestinal tract is stingy with microorganisms due to the rapid flow of food content and the low pH of the stomach, as well as the secretory properties of the stomach and duodenum. In the stomach, the number of bacteria is about 10 colony forming units (CFU)/g of food content, and in the duodenum — 101‒109 CFU/g. Going down the gastrointestinal tract, the number of resident microorganisms gradually increases, and their profile changes; in the jejunum, there are about 105‒107 CFU/g, dominated by Bacteroides species, Lactobacillus and Streptococcus. In the ileum, the number reaches as low as 107‒108, dominated by species of the genus Bacteroides, Clostridium, Enterococcus, Lactobacillus, and Veilonella, as well as those of the order Enterobacterales [2,12,13]. The slower passage of food content in the large intestine clearly favors the existence of microorganisms. Their number is 1010‒1014 CFU/g of gastrointestinal contents, and they are representatives of about 800 species. They include both symbiotic, opportunistic, and pathogenic microorganisms. Predominant are anaerobic and relatively anaerobic species of the genera Bacillus, Bacteroides, Clostridium, Bifidobacterium, Enterococcus, Eubacterium, Fusobacterium, Peptostreptococcus, Ruminococcus and Peptostreptococcus [2,12,13].
SIBO is manifested not only by a quantitative change in microorganisms but also by a qualitative change [14,15]. The threshold value of the number of bacterial colonies for the diagnosis of SIBO was undetermined and disputed, as some investigators considered 103 CFU/mL the appropriate cut off value, while others considered ≥105 CFU/mL. This was due to the limitations of culturing aspirates from the small intestine, the possibility of contamination with flora, pharynx, or oral cavity, and the possibility of false‒negative results [16].
The comprehensive profile of the gut microbiota in patients with SIBO was presented by Li et al. [17]. Dysbiosis was observed in the mucosa-associated gut microbiome but not in the fecal microbiome of patients with SIBO. Different sections of the gastrointestinal tract in patients SIBO+ and SIBO- are colonized by different bacteria (Figure 1). During the analyses, spectra of microflora from the mucosa of the duodenum, ileum, and sigmoid colon were examined and compared using 16S rRNA gene sequencing. Intestinal mucosal dysbiosis was demonstrated in bacterial overgrowth patients (SIBO+) compared to the control group (SIBO‒). In addition, significantly lower species diversity of SIBO+ patients was observed [17]. Mucosa-associated taxa identified in this study may be potential biomarkers or therapeutic targets for SIBO (Figure 1). Futher investigation is needed on their mechanisms and role in SIBO.
3. Small Intestinal Bacterial Overgrowth (SIBO)
3.1. General Characteristics
Small intestinal bacterial overgrowth (SIBO) is defined as a clinical condition caused by excessive numbers of small intestinal bacteria (≥ 103 CFU/mL) that include predominantly gram-negative aerobic and anaerobic species [18]. In the physiological state, there are mechanisms to prevent excessive colonization of bacteria in the small intestine, such as an acidic stomach pH, pancreatic enzymes, the intestinal immune system, small intestine peristalsis, the ileocecal valve and the intestinal barrier itself. However, when changes in any of these mechanisms occur, SIBO can develop [19]. Excessive proliferation of carbohydrate‒fermenting bacteria with gas production in the small intestine causes accumulation of carbohydrates, as well as accumulation of other products of bacterial metabolism, causing discomfort [5,20].
The spectrum of SIBO symptoms includes not only the digestive tract (chronic watery diarrhea/fatty diarrhea, bloating, abdominal pain, constipation, absorption disorders, malnutrition,weight loss,inflammatory changes in the intestines, and atrophy of intestinal villi) but also headaches, mood changes, general malaise, and vitamin deficiencies: B12, B1, B3, increased levels of vitamin K and folic acid, D-lactic acidosis, skin symptoms, changes in the liver, arthralgia) [1,5,18,20]. The leading cause of SIBO is a dysfunction in the movement of food content through the small intestine, delayed orocaecal transit time — OCTT, and elevation of gastric pH, e.g., due to prolonged intake of proton pump inhibitors or after gastric surgery.
Small bowel bacterial overgrowth was first postulated as a cause of gastrointestinal symptoms when scientifics [21] reported macrocytic anemia in a patient with intestinal strictures. Later scientific reports on SIBO date back only to the 1980s, before which little attention was paid to analyzing the flora of the upper gastrointestinal tract, as it was believed to be sparse and mainly anaerobic, and due to the inaccessibility of this area of the gastrointestinal tract for study and methodological and diagnostic limitations. However, with the development of microbiological diagnostic techniques, the microflora of the small intestine has been precisely defined, and its impact on health and disease states is better understood. The growth of a vast number of bacteria in the small intestine has been found to be associated with severe metabolic consequences, particularly fatty stools, diarrhea, anemia, and weight loss even in children [22,23,24,25]. As numerous studies of the past decade have shown, these are just a few of the disease entities directly associated with SIBO.
3.2. Diagnostics
Initially, SIBO was identified and diagnosed along with other gastrointestinal abnormalities, including postoperative lesions. However, due to its nonspecificity and often asymptomatic course, finding the correct diagnostic technique was a challenge for clinicians and diagnosticians. Currently, we can divide the methods into two groups: invasive, which is the gold standard — culture from a small bowel biopsy taken during endoscopy, and non‒invasive breath tests — hydrogen (H2) and methane (CH4) [5,26,27]. The latter is readily used because of its low cost, general availability, ease of performance, and assay, which is of great importance, especially among pediatric patients. The test involves the administration of 10 g of lactulose or 75 g of glucose, which are substrates for intestinal bacteria that ferment carbohydrates with the production of gas. The patient then exhales every 20 minutes for three hours into a breath analyzer that detects the presence of hydrogen or methane. Physiologically, glucose is absorbed in the small intestine — in its proximal part, while during bacterial overgrowth, it is fermented, resulting in gas. Gases are quickly eliminated; however, about 20% goes into the circulation and is then absorbed by the lungs and exhaled [5]. For SIBO, the breath test is positive when hydrogen (H2) rises above 20 ppm from baseline for 90 minutes and methane (CH4) ≥ 10 ppm at any time within 2 hours [28,29]. The second criterion proving the presence of small bowel bacterial proliferation is the double peak. It consists of an initial hydrogen peak before 90 minutes, then a decrease of more than 5 ppm in two consecutive samples, followed by a second hydrogen peak that occurs when the substrate enters the cecum [30]. Patients are advised to prepare adequately for the test, which poses the most significant obstacle. It is essential to avoid antibiotics four weeks before the test, as well as drugs that accelerate intestinal peristalsis and have a laxative effect one week before. In addition, no complex carbohydrates or alcohol should be consumed the day before, and no food should be consumed 8‒12 hours before the test, as well as no smoking and avoiding exercise. Brush your teeth and rinse your throat before the test to minimize the fermentation of lactulose by bacteria in the mouth [30].
Despite its invasiveness, the gold standard for the diagnosis of SIBO is a culture of jejunal aspirates. An endoscope is inserted into the second/third part of the duodenum. A Liguora catheter with a valve is placed through the biopsy channel, and about 3 mL of fluid is aspirated with a syringe and immediately sent to a microbiology laboratory for the culture of aerobic and anaerobic bacteria. A bacterial concentration of >103 CFU/mL indicates SIBO [18,28], although there is some heterogeneity in the literature, and some experts recommend a threshold of >105 CFU/mL as more specific [18,27]. This direct method, in addition to its invasiveness, has other limitations — it is expensive, requires specialized performance, and there is a risk of contamination of the material with pharyngeal and oral flora, which can result in false positives. There is no obvious cutoff point to determine a positive aspirate. Moreover, the standard processing of material in the microbiology laboratory does not allow the detection of all species of the gut microbiome. On the other hand, breath tests have lower sensitivity (52‒63% for glucose[GBT — glucose breath test], 31‒68% for lactulose [LBT — lactulose breath test]) and specificity (82‒86% for GBT 44‒100% for LBT) [31].
3.3. Treatment and Diet
Treatment of SIBO should be comprehensive, individualized, and, if possible, causal (Figure 2). Comprehensive action includes elimination of the underlying disease (e.g., anatomical defect), eradication of bacterial overgrowth with appropriate antibiotic therapy, and diet to eliminate nutritional deficiencies [18,31,32]. The former includes surgical management to correct anatomical defects, if any (adhesions, diverticulosis, intestinal obstruction, fistulas, strictures), as well as elimination or dose reduction, shortening the duration of administration of drugs that reduce intestinal motility or gastric juice acidity (e.g., proton pump inhibitors, PPIs), which promote and exacerbate bacterial overgrowth. In addition, there are attempts to use prokinetic drugs — accelerating intestinal motility, in justified cases (e.g., in chronic pseudo-obstruction of the intestines) — metoclopramide and erythromycin are used in the US in Europe — prucalopride [33]. Antibiotic therapy for SIBO usually involves empirical treatment due to the difficulty of proper specimen collection, using metronidazole, ciprofloxacin, tetracycline, amoxicillin-clavulanate, neomycin, or rifaximin [34,35,36]. Rifaximin has been show to be effective in the treatment of SIBO, despite the heterogeneity found in the studies as well as the lack of a recommendation regarding the dose and duration of treatment [36]. SIBO can be recurrent, statistically more common in the elderly, patients permanently taking PPIs, and after surgical removal of the appendix, in which case repeated antibiotic therapy and consideration of causal treatment is required [37,38,39].
Increasing incidences of therapeutic failure have prompted the search for other treatments. The alternative treatment of SIBO includes, especially in cases of recurrence or resistance of bacterial strains to commonly used antibiotics — fecal microbiota transplantation from a healthy donor. The method is effective in the treatment of certain chronic inflammatory conditions of the gastrointestinal tract, non‒invasive, and does not cause rejection or induce an immune response, frequently allowing the permanent restoration of normal gastrointestinal microbiota. It involves oral administration of a "gut microbiota capsule" once a week for four weeks — a standardized preparation containing previously frozen fecal microbiota [40]. In addition, a positive effect of probiotics, therapeutic diets, and herbal preparations with antimicrobial activity has been detected; however, these modalities are currently only supportive, and confirmation of their efficacy requires further clinical studies [41,42]. A reduction in the severity of SIBO symptoms was observed during the use of probiotics containing a mixture of different microorganisms [43].
The diet has a supportive effect in the treatment of SIBO, especially in people who have experienced weight loss and vitamin and mineral deficiencies [44]. No restrictive dietary change is required, only periodic avoidance of certain foods. It usually requires the elimination of lactose and other products with a high content of carbohydrates not wholly digested or absorbed in the intestines, which easily ferment and are substrates for intestinal bacteria, and an increase in the coverage of energy needs with fat and the administration of medium‒chain triglycerides. The diet is called the Low FODMAP diet, and the name derives from the first letters of the carbohydrates to be avoided: oligosaccharides such as fructans, galacto‒oligosaccharides, disaccharides — lactose, monosaccharides — fructose, polyols — sorbitol, and mannitol [44,45]. This diet was initially designed to alleviate symptoms of irritable bowel syndrome (IBS), but up to 78% of IBS cases are accompanied by SIBO [46]. Small intestinal bacterial overgrowth (SIBO) is one manifestation of gut microbiome dysbiosis and is highly prevalent in IBS. The effectiveness of the low FODMAP diet has been carried out primarily for patients with IBS, but data support its effectiveness in SIBO as well, which is why it is increasingly recommended by doctors [44,46,47]. The diet can positively affect both the resolution of symptoms and the lack of recurrence of SIBO.
4. SIBO – Related Diseases
Symptoms of SIBO may be limited to the gastrointestinal tract; however, a growing number of hypotheses emphasize the association of SIBO with other diseases. In our review, we divided these diseases into 12 groups (Figure 3).
4.1. Group 1. Gastrointestinal Disorders
Dysfunctions in the gastrointestinal tract leading to damage to protective barriers can result in the development of SIBO. One of the risk factors for the development of SIBO is hypochlorhydria, i.e., reduced gastric juice secretion — physiologically in the elderly, long‒term PPI use or colonization with Helicobacter pylori (H.pylori) leads to dysbiosis in the stomach and small intestine. An increased incidence of SIBO has been observed in patients infected with H. pylori [48,49,50,51,52,53]. Pelvic and abdominal surgical procedures are a predisposing factor for excessive intestinal bacterial proliferation; gastrectomy results in reduced gastric acid production [54]. It is estimated that up to 80% of patients after bariatric surgery suffer from SIBO, in an era when this method has become widespread in the treatment of obesity [55].
4.1.1. Irritable Bowel Syndrome (IBS)
Symptoms of SIBO very often resemble those of irritable bowel syndrome (IBS). In recent years, studies have found that the rate of positive SIBO in IBS patients is significantly increased, and it has been found that eradicating overgrown small intestinal bacteria can improve the symptoms of IBS patients. Therefore, the relationship between SIBO and IBS has attracted widespread attention. Irritable bowel syndrome (IBS) is the most common functional digestive disorder. In developed countries, its prevalence varies between 10% and 15% [56,57]. It is estimated that the incidence of bacterial proliferation of the small intestine in patients with IBS was 51.7% compared to healthy subjects — 16.7%. In addition, patients with IBS and SIBO have more severe gastrointestinal symptoms, probably due to the composition of the intestinal microbiota in SIBO+ and IBS+ patients — dominated by the genus Prevotella, which produces enzymes responsible for the fermentation of carbohydrates, during which not only hydrogen and methane can be formed, but also short‒chain fatty acids responsible for the hypersensitivity of internal organs, and lipopolysaccharide (LPS) present in the cell wall can further induce inflammation of enterocytes [58]. Activation of the immune system and prolonged inflammation in the intestinal mucosa in the course of IBS increase intestinal vascular permeability, while SIBO also induces immune system activity [59], hence, many studies confirm the co-occurrence of SIBO [60,61,62,63,64,65,66]. Rifaximin therapy caused remission of IBS, indicating SIBO as an inducer of IBS [67,68,69].
4.1.2. Crohn's Disease (CD) and Ulcerative Colitis (UC)
In other inflammatory bowel conditions, an increased incidence of SIBO co-occurrence has also been observed. Crohn’s disease (CD), a kind of inflammatory bowel disease (IBD), is a persistent and irreversible inflammatory disorder with an unknown cause that has a usual state marked by remission and relapse. Frequent fistulas, strictures sometimes requiring surgery, and resection of the ileocecal valve in Crohn's disease (CD) can obviously affect the translocation of the intestinal microbiota [70]. SIBO seems to be a common condition in patients with CD, with an estimated prevalence between 25% and 88%2, and predominant in patients with gastrocolic or jejunocolic fistulas, stasis of intestinal contents, colo-ileal reflux caused by the loss of the ileocecal valve, surgical blind loop, intestinal obstruction and different types of motility disorders [71,72]. SIBO in patients with CD was associated not only with a more severe disease but also with signicant changes in the gut microbiome that may worsen the symptoms and the course of the disease [70,73]. Ulcerative colitis (UC), a non-specific ulcerative colitis, is a chronic inflammatory disease of the rectum and colon, for which, the pathogenesis hasn’t been elucidated [74]. In addition, the secretion of pro-inflammatory cytokines in ulcerative colitis (UC) can result in SIBO. It has been observed that eradication of SIBO using rifaximin reduced symptoms in both CD and UC patients [75,76]. UC is characterized by chronic inflammation and repeated attacks. Thus, UC is challenging to be cured completely, and it usually compiles with clinical symptoms such as fever, bloody diarrhea, abdominal pain, weight loss, etc. [77]. According to the study, patients with IBD, particularly those with CD, female gender, having undergone surgery for IBD, have a higher risk of SIBO than the healthy controls [68]. Patients with ulcerative colitis are easy to occur SIBO, and SIBO increases blood endotoxin, TLR2 and TLR4 levels. Synergistic effects of endotoxin and endotoxin receptors TLR2 and TLR4 overexpression mediate body inflammation and may be involved in progression of ulcerative colitis. Patients with ulcerative colitis with excessive growth of small intestinal bacteria are more likely to have hypertoxemia [68,78].
4.1.3. Celiac Disease (CeD)
Celiac disease (CeD) is an autoimmune enteropathy triggered by gluten ingestion in genetically susceptible individuals [79]. The link between SIBO and celiac disease seems quite apparent: intestinal dysbiosis can affect gastrointestinal motility and vice versa [80]. Such a correlation was observed as early as 1970 [81,82]. Patients with celiac disease show a decrease in cholecystokinin and sporadically an increase in neurotensin; both hormones positively and negatively influence gastrointestinal motility, respectively [83,84]. In addition, rifaximin therapy caused remission of symptoms in patients unresponsive to treatment with a gluten-free diet. However, other later studies [85,86] have shown a lack of response to antibiotic therapy and a lower incidence of SIBO in patients with celiac disease. Celiac disease is a disease with a complex pathogenesis; hence, only specific variants may correlate with SIBO [79,87]. Patients with CeD usually improve on gluten-free diet (GFD), however, 7%–30% of the patients continue to have symptoms of malabsorption despite adherence to the GFD. The lack of response to a prescribed GFD or recurrence of gastrointestinal symptoms despite GFD maintenance in patients who responded initially to GFD is usually termed “unresponsive CeD”. Unresponsiveness suggests gluten contamination or coexistence of other conditions, such as SIBO [79].
4.1.4. Non‒Alcoholic Fatty Liver Disease (NAFLD)
Non-alcoholic fatty liver disease (NAFLD) is a chronic liver disease associated with the pathological accumulation of lipids inside hepatocytes. The estimated frequency of NAFLD has been reported to be 25% globally [88]. Obesity is the greatest risk factor for lipid accumulation inside hepatocytes, but a part of the NAFLD patient population has a normal body weight according to the BMI index. Obese people with or without NAFLD have a higher incidence of SIBO, and those suffering from NAFLD show increased intestinal permeability, including a more frequent presence of bacterial overgrowth in the small intestine (SIBO) [89]. The health consequences of SIBO are primarily malabsorption disorders (vitamin B12, iron, choline, fats, carbohydrates and proteins) and bile salt deconjugation [88,89,90].
Parenchymal organ dysfunction can cause dysbiosis mainly by affecting gastrointestinal motility [91,92,93] NAFLD is estimated to be a predisposing factor for SIBO; however, these studies were based on animals or a few patients. The cause of fatty liver disease is still not fully understood. The challenge are patients with normal body weight and confirmed fatty liver. The cause of NAFLD progression in lean individuals is still unknown. The current treatment for NAFLD in lean people is the reduction of visceral fat through a healthy diet and lifestyle, and the use of certain medications. Previous studies have shown a relationship between intestinal dysbiosis and the occurrence of fatty liver [94]. Some studies show that the prevalence of SIBO in patients with chronic nonalcoholic liver disease can be as high as 35% of the total population, and the prevalence increases with the percentage of men in the population [88,94,95]. Other research suggests that there might be an association between NAFLD and SIBO in children [94,96,97]. Future studies should explore the mechanisms linking SIBO and NAFLD and examine whether treating SIBO could prevent NAFLD in children. The analysis of risk factors of SIBO in children showed that metabolic syndrome and NAFLD as the risk factors for SIBO development [94,96,97].
Intestinal microflora, including small intestinal bacterial overgrowth (SIBO), appear to play an important role in the pathogenesis of the disease, as demonstrated in several clinical and experimental studies, by altering intestinal permeability and allowing bacterial endotoxins to enter the circulation [98,99]. Studies show that Serum endotoxin levels did not differ between patients SIBO+ and SIBO-, nor did these levels change after antibacterial therapy, virtually ruling out the possibility that elevated endotoxinemia in non-cirrhotic patients with NAFLD is associated with SIBO. Presence of SIBO was associated with greater severity of ballooning degeneration on liver biopsy, but not with a significantly higher prevalence of NASH. Additional studies are needed to evaluate the reproducibility and importance of this finding in patients with NAFLD and SIBO [97]. Prospective cross-sectional study in a well-defined cohort of NAFLD patients demonstrated that the prevalence of SIBO, using duodenal aspirate culture, is significantly higher among patients with NAFLD compared to healthy controls [100].
4.1.5. Liver Cirrhosis
SIBO often appears in people with liver cirrhosis [101,102]. Bacterial overgrowth was found in as many as 51.5% of patients during the tests. A meta-analysis of 21 studies revealed that the prevalence of SIBO in patients with cirrhosis was greater than that in healthy controls [103]. The disease affects the liver and other organs, e.g., the intestine [104]. This condition is caused by impaired intestinal motility, delayed intestinal transit, pancreatic exocrine insufficiency, or immunological disorders.
Additionally, patients with this type of liver disorder suffer from comorbidities such as diabetes or autonomic neuropathy, which intensify the occurrence of SIBO [104,105]. Liver cirrhosis causes dysbiosis - there is an increase in the number of bacteria of the Proteobacteria genus, which are responsible for the production of active endotoxin, and anaerobic bacteria of the Bacilli genus, which can translocate bacteria. There is also a decrease in the level of Clostridium bacteria. SIBO patients mainly have bacteria from the Blautia genus, which can convert primary bile acids into secondary bile acids. When there are changes in bile metabolism, the intestinal microbiome changes, and the more bacteria there are, the more deconjugation of primary fatty acids in the small intestine will increase. These acids, however, have a lower affinity for proteins, thus causing them to be transported across the epithelium of the terminal ileum. This causes increased growth of Blautia bacteria [104]. Meta-analyses have shown that SIBO in cirrhosis is associated with hepatic encephalopathy [106].
4.1.6. Pancreatitis
There have also been reports of a higher incidence of SIBO in patients with chronic as well as acute pancreatitis, but due to the small groups of patients studied [107,108,109,110,111]. SIBO can complicate chronic pancreatitis and interfere with management [112]. It has been demonstrated that intestinal barrier dysfunction allows bacteria of intestinal origin to transfer to extraintestinal organs, leading to sepsis and subsequent infectious diseases with a high mortality rate [113]. According to studies, the presence of SIBO in acute pancreatitis correlates with the severity of the disease [113,114]. SIBO is often present in patients with chronic pancreatitis with persistent steatorrhea, despite pancreatic enzyme replacement therapy. Overall prevalence of SIBO, diagnosed by glucose breath test (GBT), varies between 0% and 40% but 0%-21% in those without upper gastrointestinal (GI) surgery [112,114].
4.2. Group 2. Autoimmune Disease
Systemic Sclerosis (SSc)
Systemic sclerosis (SSc) is a chronic connective tissue disease of autoimmune origin, leading to organ fibrosis; the pathological process also affects the gastrointestinal tract [115,116,117]. About 55% of patients suffer from gastrointestinal complaints (bloating, abdominal pain, constipation, diarrhea). SIBO occurs with a prevalence of approximately 39%-62% patients with SSC and presents with a range of non-specific gastrointestinal tract symptoms [118,119,120,121]. Abnormal intestinal motility, prolonged OCTT, and impaired intestinal clearance are factors in the development of SIBO. Several studies have confirmed the co-occurrence of SIBO and SSc, and a disease duration of more than five years is a significant risk factor for the development of SIBO [33,120,121,122,123,124,125].
The data reveal a strong link between SIBO and SSc with a 10-fold increased prevalence of SIBO in SSc-patients as compared to controls [122]. Moreover, the risk of diarrhea was higher in SSc patients with SIBO than those without SIBO. Parodi et al. [33] showed, in the group of Fifty-five SSc patients and 60 healthy controls, that The prevalence of SIBO was higher in SSc patients compared with controls (30/54 vs 4/60, respectively, P < 0.001). Intestinal symptoms in these patients may be related to this syndrome and its eradication seems useful to improve clinical features. Orocecal transit time (OCTT) is significantly delayed in SSc patients, suggesting an impairment of intestinal motility, a further risk factor for the development of SIBO. Other studies have also shown that velocity through the small intestine is significantly reduced in SSc patients with diffuse abdominal symptoms [123]. In a large cohort of SSc patients, stated that the small bowel are more frequently impaired, and SIBO was observed in 46% of SSc compared with 5% of controls [124]. In a study of exhibited malabsorptive SSc patients, one-third tested positive for SIBO from the jejunal fluid aspiration. In other symptomatic patients with advanced SSc, SIBO has been reported in between 30% and 62% of cases. These findings provide further support that patients with SSc have distinctly different microbiomes from their healthy counterparts [120,121]. Malnutrition is one of the most common causes of death in SSc, and intestinal bacteria are responsible for the deconjugation of bile acid salts and impaired absorption of lipids and fat-soluble vitamins [125]. All patients with raised unconjugated serum bile acids had oesophageal motility disorders. These results confirm a relationship between motility disorders and bacterial overgrowth in patients with progressive systemic sclerosis [125]. Antibiotic treatment can lead to eradication of SIBO and gastrointestinal symptomatic improvement in SSc patients [126]. A reduction in gastrointestinal symptoms has been observed following rifaximin therapy, and recent studies have also demonstrated the efficacy of Saccharomyces boulardii probiotics in combination with metronidazole in the treatment of SIBO [33,118,127]. Fecal calprotectin (FC) [128]turned out to be a sensitive and specific marker differentiating patients from the control and study group (SSc detection). Additionally, this marker showed high sensitivity and specificity in detecting SIBO in SSc patients [128,129]. However, non-invasive tests or biomarkers able to identify SSc patients at high risk of developing gastrointestinal tract manifestations are still lacking today [130].
4.3. Group 3. Cardiovascular System Diseases
SIBO has been shown to be linked to the cardiovascular system. Reduced cardiac output in the course of its failure causes ischemia of the small intestinal wall, and this, in turn, leads to intestinal dysfunction and increased permeability. High levels of lipopolysaccharide, a component of the cell wall of Gram-negative bacteria, which is a pro-inflammatory factor, have been shown in patients with cardiovascular edema [131]. Endotoxin binds to the TLR-4 receptor and activates inflammation, leading to left ventricular remodeling and increased apoptosis of myocardial cells [132,133].
4.3.1. Heart Failure (HF)
Increasing evidence has showed that the altered intestinal function induces the bacterial translocation, microbes, and endotoxins entering into circulation, which triggers the systemic inflammatory and immune responses, especially in patients with heart failure (HF) with malnutrition and late-stage cachexia. Recently, the analysis of metagenomics and 16S rRNA gene sequence in excreta samples has revealed that patients with HF present more dysfunctional gut flora than healthy people [134]. Increasing evidence supports the correlation between HF and gut microbiota. In patients with heart failure (HF), the exhaled concentrations of hydrogen after a breath test—a non-invasive assessment of SIBO- has been related to HF severity and higher risk of adverse outcomes [135]. Recent studies have demonstrated a bidirectional relationship between intestinal flora and the brain. The interaction occurs through neural, hormonal and immune pathways, which are called the gut–brain axis. This also occurs in ischemic stroke (AIS). The prevalence of SIBO in patients with AIS was 28.8 % [136].
4.3.2. Deep Vein Thrombosis (DVT)
Deep vein thrombosis (DVT) may also be associated with SIBO due to increased levels of inflammatory factors and expression on the surface of platelets and endothelial cells of TLR‒4, which, when combined with LPS, enhances procoagulant activity; hence SIBO is a risk factor for DVT, in turn, the cytokine storm in DVT may stimulate the intestinal immune system by affecting its microflora, being a risk factor for SIBO [92,137].
4.3.3. Coronary Artery Disease (CAD)
He et al.[138] suggest that alcohol consumption may be associated with CAD as well as SIBO. Authors [138] speculate that patients with SIBO may produce a larger quantity of endogenous alcohol than those without SIBO. This may explain why patients in the SIBO group had a numerically higher frequency of fatty liver than controls.
4.3.4. Subclinical Atherosclerosis
It has been recently demonstrated that metabolic products generated by gut bacteria are implicated in the development of subclinical atherosclerotic lesions [139,140]. Humans need gut bacteria in order to fulfill their vitamin K2 requirement as dietary intake is often insufficient. This is especially true in the case of the western population. SIBO, a condition that is characterized by gut bacteria dysbiosis, is associated with impaired vitamin K metabolism in humans. For this reason, patients afflicted with SIBO and/or low vitamin K2 status could hypothetically be at an increased risk for the development of atherosclerotic disease [140]. It was confirmed in research from 2022 [139], that SIBO was found to be associated with subclinical atheromatous plaques. Plaques were more common in the SIBO-positive group than in the SIBO-negative group, and the mechanism of this association warrants further exploration [139].
4.4. Group 4. Metabolic Diseases
4.4.1. Diabetes
The incidence of SIBO was significantly higher in patients with both type I and type II diabetes compared to the healthy population [141,142]. The pathogenesis of SIBO in diabetes is not entirely understood, although it is known to be multifactorial: hyperglycemia, delayed gastric emptying, or impaired gut motility resulting from diabetic autonomic neuropathy [142]. Diabetic neuropathy, resulting from dysfunction of the intrinsic autonomic nerves and the vagus nerve, affects the physiology of the entire gastrointestinal tract, causing, among other things, stasis in the small intestine, a risk factor for SIBO [143] and the maintenance of dysbiosis can exacerbate diabetic symptoms [144,145].
SIBO has been shown to be associated not only with type I and type II diabetes but also with gestational diabetes mellitus (GDM). In a population of pregnant Chinese women with gestational diabetes, symptoms of bloating abdominal pain showed higher concentrations of exhaled hydrogen and methane compared to the control group. In addition, the blood glucose content of women with GDM and SIBO was higher compared to patients with gestational diabetes without symptoms of SIBO; also, the birth weight of newborns was higher in women with SIBO [146]. Treatment with prebiotics, probiotics, and antibiotics reduces gastrointestinal symptoms in patients with diabetes [144,145]. The study show found that diabetes patients with autonomic neuropathy have a significantly higher prevalence of SIBO than those without autonomic neuropathy. These results suggest that diabetes mellitus could be a predisposing factor for the development of SIBO [143,147]. The present results suggest that type II diabetes combined with SIBO is inversely associated with insulin secretion and worse glycemic control [143,147].
4.4.2. Hyperlipidemia
SIBO may cause the hyperlipidemia appearance by enterohepatic circulation disturbance which evolves on the background of the early bile acids deconjugation with further endotoxin production and oxidative stress in the liver with hyperproduction of cholesterol and atherogenic lipoproteins. SIBO was present in 78.9% of patients with hyperlipidemia and 40% in control subjects, and there was a relationship between hydrogen (H2) rate, and low density protein (LDL), triacylglycerols (TG), and very low density lipoprotein (VLDL) [148].
4.4.3. Obesity
The issue of obesity around the world is becoming more and more involved, as the number of people with excess kilograms is increasing every year. The environment, diet, lack of sleep, dysregulated hormonal balance, chronic inflammation, and, most importantly, our microbiome contribute greatly to this [149]. Comparing the composition of the intestinal microflora between thin people and those with obesity. The research is mainly based on experiments performed on mice [150]. In obese mice, a higher number of bacteria of the Firmicutes genus was found, and a lower number of Bacteroidetes, compared to lean rodents. As a result of analyzing the genes, it was found that more of them are responsible for the greater use of energy from food. When we transplanted gut bacteria into obese germ-free mice from lean mice, it resulted in less weight gain [151].
Obesity is associated with an increased risk of SIBO despite inconsistent results [152,153,154,155]. The statement was confirmed in studies on the relationship between SIBO and obesity, where this relationship was demonstrated despite a small sample size. Based on a lactulose breath test and a study with a wireless motor capsule [153].
The risk of SIBO was twice as high in patients with obesity compared to the non-obese control group. And when only studies from Western countries were taken into account, the risk was threefold. This is probably due to the use of different diagnostic methods with different sensitivity and specificity [152]. There are several mechanisms influencing the occurrence of obesity, the first of which is the more efficient absorption of energy from food by the intestinal microflora. This is proven by studies that show a greater amount of short-chain fatty acids - SCFA (short-chain fatty acid), which is an energy compound derived from the digestion of carbohydrates in the large intestine. In obese people, there is a greater absorption of simple carbohydrates, resulting in increased lipogenesis in the liver and the formation of adipose tissue [151]. Another factor causing obesity is a change in the motility of the gastrointestinal tract. It was found that patients had slower intestinal transit but greater absorption in its proximal part. Prolonged transit through this part of the digestive system leads to weight gain. The smooth muscles of the small intestine of obese people show greater contractility compared to healthy people. What may be the reason for faster transit in the proximal part of the intestine [156].
The causes of obesity also include accelerated gastric emptying in patients with excessive kilograms. It is related to overeating. This results in a reduction in the reception of the feedback signal informing about satiety, resulting in a faster feeling of hunger [157]. Another reason may be that the intestinal microflora is changed in people with obesity. Diet also has an impact on the microbiome, e.g. the Western diet, which is rich in fats and carbohydrates, reduces the level of beneficial microorganisms in the intestines [152].
4.5. Group 5. Endocrine Disorder
Thyroid Disease
Endocrine disorders are very commonly accompanied by gastrointestinal symptoms in the form of constipation, diarrhea, or abdominal discomfort. Despite very little data and unexplained pathogenesis, it appears that hypothyroidism can slow down intestinal motility; more than 50% of patients with hypothyroidism also suffer from SIBO [158]. Interestingly, it has been observed that levothyroxine supplementation strongly interferes with SIBO [159]. Hyperthyroidism can also affect gastrointestinal motility, but the causes remain unclear [160]. Bacterial antigens can induce both Hashimoto's disease and Graves‒Basedow disease, both of which have an autoimmune basis. A state of intestinal dysbiosis modifies the immune response, inducing inflammation, which in turn increases the sensitivity of the intestinal wall and consequently increases its permeability, provoking the immune system to produce antibodies that may play an essential role in the development of Hashimoto's or Graves‒Basedow's disease [161]. Good dietary habits and consumption of optimal amounts of omega-3 fatty acids, fiber, and plant products play a significant role in improving the intestinal microbiome, which can lead to a reduction in inflammation [159,162,163]. In one of the largest studies devoted to examining the occurrence of SIBO in patients with hypothyroidism, it was shown that the most important contributors to the development of SIBO in ascending order are immunosuppression, impairment of intestinal clearance, and levothyroxine use. Still, they do not sufficiently explain its emergence [159]. In other study [162,163] confirmed that hypothyroidism is associated with bacterial overgrowth development. Excess bacteria could influence clinical gastrointestinal manifestations. Bacterial overgrowth decontamination is associated with improved gastrointestinal symptoms. However, fermenting carbohydrate luminal bacteria does not interfere with thyroid hormone levels. In 2021 it was demonstrated that the occurrence of subclinical hypothyroidism is related to SIBO, and the excessive growth of small intestinal bacteria may affect gastrointestinal symptoms [164].
4.6. Group 6. Nephrological Disorders
4.6.1. Chronic Kidney Injury
One of the most novel issues of recent interest to many scientists is the relationship between kidney well‒being and the gastrointestinal tract, the so‒called gut‒kidney axis [165]. Current results indicate that the intestinal environment has a considerable impact on kidney function and vice versa. The majority of patients with chronic kidney disease have gastrointestinal symptoms. Renal failure, in turn, predisposes to changes in the gastrointestinal microbiome, associated with an overgrowth of aerobic and proteolytic bacteria in the duodenum and jejunum [165]. An excessive increase in Enterobacterales and Enterococcus genus bacteria with a concomitant decrease in Lactobacillus, Prevotella, or Bifidobacterium appears to be significant [165]. In addition, in patients with chronic renal failure, changes in the structure of the intestinal wall are observed: degradation of intestinal villi, enlargement of crypts, disruption of epithelial cell integrity, infiltration of inflammatory cells in the lamina propria, and impaired excretion of bacterial metabolites such as indoxyl sulfate and p‒cresyl in the urine promote intestinal disorders [166,167].
A significantly higher incidence of SIBO has been observed in patients with chronic kidney injury (CKI) compared to controls [168]. The study covered twelve patients with CRF with GI symptoms (10 men, 2 women) and 10 patients with CRF without GI symptoms (5 men, 5 women). Uremic toxins, whose precursors are produced during bacterial metabolism, certain amino acids (tryptophan, phenylalanine, tyrosine), then converted in the liver to uremic toxins — indoxyl sulfate and p‒cresyl sulfate removed under physiological conditions by the kidneys along with urine, seem to be responsible for the mechanism. Their accumulation in patients with chronic renal failure affects the autonomic nervous system of the gastrointestinal tract, worsening intestinal motility and promoting excessive bacterial growth. On the other hand, increased intestinal permeability in CKF patients allows antigens to enter the bloodstream; bacterial toxins can be captured by anion transporters in the renal tubules, impairing their function [169,170].
4.6.2. Acute Kidney Injury
During acute kidney injury (AKI), intestinal dysbiosis is also observed. The main initiating factor of AKI — ischemia-reperfusion injury (IRI), its complex pathogenetic mechanism, is potentially related to the formation of reactive oxygen species, damaging endothelial cells. Thus, they initiate the release of inflammatory mediators and the expression of adhesion molecules during ischemia and subsequent reperfusion, which can induce intestinal dysbiosis, which in turn further induces inflammation, exacerbating kidney damage [171]. Studies by Yang et al. [172] in mice have shown a renoprotective effect of reducing intestinal microflora associated with a decrease in the activity of Th1 and Th17 lymphocytes and an increase in the activity of Treg lymphocytes and macrophages. Intestinal dysbiosis is also thought to be a factor in the development of IgA nephropathy [173]. Despite the above reports, there is no hard data evaluating the association of SIBO with kidney disease.
4.7. Group 7. Dermatological Diseases
4.7.1. Acne Rosacea
Acne rosacea is a chronic inflammatory acne‒like dermatosis that occurs in the mid-face area and manifests as transient erythema, redness, pustules, and papules [174]. To date, the direct cause is not known; however, the mechanisms affecting this disease may include changes in the immune response [175]. Some cases of acne have been found to be associated with various gastrointestinal diseases: irritable bowel syndrome, inflammatory bowel disease, celiac disease, gastroesophageal reflux disease, Helicobacter pylori infection, and SIBO. The latter is thought to be influenced by the gut‒skin axis [176]. Patients with rosacea were as much as 13 times more exposed to SIBO compared to controls, and regressions of skin lesions were observed after treatment of SIBO with rifaximin [175]. The mechanism for the co-occurrence of SIBO and rosacea remains unexplained, and it is suspected that SIBO increases intestinal permeability, resulting in the transfer of bacteria and pro-inflammatory cytokines into the systemic circulation, causing skin inflammation, increasing levels of cytokines such as TNF‒α, which inhibits interleukin 17 and stimulates an immune response that is Th1‒dependent [175,176]. The study demonstrated that rosacea patients have a significantly higher SIBO prevalence than controls (52/113 vs 3/60) [177]. After eradication, cutaneous lesions cleared in 20 of 28 and greatly improved in 6 of 28 patients, whereas patients treated with placebo remained unchanged (18/20) or worsened (2/20). Placebo patients were subsequently switched to rifaximin therapy, and SIBO was eradicated in 17 of 20 cases. Fifteen had a complete resolution of rosacea. After antibiotic therapy, 13 of 16 patients with negative BTs for SIBO remained unchanged, and this result differed from SIBO-positive cases. Eradication of SIBO induced an almost complete regression of their cutaneous lesions and maintained this excellent result for at least 9 months [177].
4.7.2. Psoriasis
Another dermatological condition, psoriasis is a chronic inflammatory condition of the skin with a multifactorial basis, manifested by the formation of scaly, erythematous, hardened skin plaques, causes epidermal hyperplasia, proliferation of skin blood vessels and inflammatory infiltration of T lymphocytes. It affects both children and adults but is more common in the latter [178]. Two cases of the relationship between psoriasis and SIBO have been described in the literature [179,180], both from 2018. Psoriasis can involve different parts of the body, such as the oral cavity, in which case it manifests itself as a so-called geographic tongue [179]. It is a benign inflammation of the tongue that "wanders" on its surface — red, oval lesions surrounded by a white border. These areas change shape, size, location, and pattern, and there are alternating periods of exacerbation and complete remission of symptoms [181]. The literature describes a case of a woman with lingual psoriasis without psoriatic skin lesions [179]. The woman experienced pain, a burning tongue, and difficulty in eating. In addition, she was diagnosed with SIBO, and after the implementation of rifaximin, a significant improvement in the condition of the tongue was observed, eliminating pain and discomfort. After three months, no recurrence of psoriatic lesions in the oral cavity was observed [179]. In fact, the combination of rifaximin with a prebiotic that can have a beneficial effect on intestinal motility, seems to be more useful in eradicating SIBO compared with rifaximin alone. Moreover, rifaximin is similar to rifampin which, besides the antibacterial action, has been shown to be a biofilm-dispersing agent. In other studies, Drago et al. [180], showed that the prevalence of SIBO in patients with psoriasis is comparable to that in the control group. This creates a need for further research to explain the relationship between psoriasis and SIBO.
4.8. Group 8. Neurological Diseases
4.8.1. Alzheimer's Disease (AD)
Alzheimer's disease is the most common neurodegenerative disease; the number of sufferers worldwide is estimated at 15‒21 million. It is a degenerative disease of the brain caused by the deposition of pathological proteins (beta-amyloid, tau protein, and alpha-synuclein) in the brain, causing atrophy of neurons and their connections. This results in a decrease in the amount of transmitter substances needed for normal brain function [182]. The pathogenesis of AD is not clear‒cut and is most likely multifactorial, sometimes showing significant links to other diseases, such as depression, diabetes, cardiovascular disease, and inflammatory bowel disease [182]. The gut microbiome participates in the regulation of the immune system, as well as the central nervous system, affecting the adequate production of neuroactive molecules — serotonin, acetylcholine, tryptophan, histamine, GABA, and catecholamines [183]. The exact mechanisms of gastrointestinal co-morbidities with AD are not yet known. However, studies suggest that an abnormal structure of the intestinal microbiota results in the production of toxic metabolites that penetrate the bloodstream to the brain and cause inflammation in the nervous system. The stools of AD patients showed a less diverse microbiome and calprotectin levels regarding the control group [183]. Few studies confirm the co-occurrence of SIBO and AD [184,185]. During a study conducted at the University of Singapore to analyze the prevalence of SIBO, respiratory tests were performed in AD patients, and the results were compared with a sex‒ and age-matched control group. The frequency of positive breath test results was similar in both groups [184]. Other results with 2022 [185] indicated, the gut microbiota contribution to the pathogenesis of Alzheimer’s disease (AD). The prevalence of SIBO was significantly higher in the AD patients than in age-matched controls without dementia (49% vs 22%)[185].
4.8.2. Parkinson’s Disease (PD)
Parkinson's disease is the second most common neurodegenerative disorder in the elderly worldwide. The occurrence of neuropathological changes characterizes it due to abnormal accumulation of α‒synuclein, as well as necrosis of dopaminergic neurons in the black matter [186]. In addition to typical symptoms such as tremors and stiffness of the limb bones, sleep disturbances, constipation, and depression, patients also experience gastrointestinal symptoms resulting from abnormal motility and delayed gastric emptying [186]. H. pylori co-infection synergistically exacerbates gastrointestinal symptoms [187,188]. Numerous studies have confirmed the association of SIBO with Parkinson's disease [186,187,188,189,190], with as many as 14% to 67% of patients struggling with SIBO depending on the demographic and clinical characteristic of the population included in the study, as well as on the testing method that has been used (i.e., small intestine fluid bacterial count, H2 glucose breath testing, or H2 and methane lactulose breath testing, the highest percentages being reported in studies using both glucose and lactulose H2 and methane breath testing and the lowest in studies using H2 glucose testing alone) [191]. Li et al. [186] demonstrated in a group of 973 participants a strong association between SIBO and PD, with approximately half of PD patients testing positive for SIBO. These relationships significantly differed based on diagnostic tests (glucose hydrogen breath test (GBT), the lactulose hydrogen breath test (LBT)), and geographic area. The prevalence of SIBO was 52% among patients from western countries and 33% among patients from eastern countries. Niu et al. [187] tested 182 Chinese patients with PD patients and 200 sex, age, and BMI-matched subjects without PD were included. All participants underwent the glucose breath test to assess SIBO. SIBO was highly prevalent in PD, and nearly one-third was detected. SIBO was associated with worse gastrointestinal symptoms and worse motor function. Further studies are needed to specify the reasons underlying SIBO and worse motor function in PD. A similar study [189] showed that SIBO was detected in a quarter of patients, including those recently diagnosed with the disease. SIBO was not associated with worse gastrointestinal symptoms but independently predicted worse motor function. Appropriately designed clinical trials are needed to confirm a causal relationship between SIBO and poorer motor function in PD. SIBO can trigger a local inflammatory response, disrupting the integrity of the intestinal barrier. Increased intestinal permeability is an increased exposure of the mucosa to bacterial exotoxins, as well as to lipopolysaccharide (LPS), factors responsible for local inflammation, which can increase α-synuclein amyloidogenesis and increase neuronal susceptibility to neurodegeneration. SIBO also affects the absorption of enteral drugs directed to treat PD; gut dysfunction due to microflora abnormalities results in impaired absorption of levodopa, a key drug in the treatment of PD, and consequently reduced dopamine concentrations in the target organ — the brain [189,190]. Excessive numbers of bacteria in the gut can induce the production of reactive oxygen species that inactivate the drug and alter its bioavailability. There is a strong association of SIBO with Parkinson's disease, primarily since the neurodegenerative disease involves both the autonomic and enteric nervous systems — the vagus nerve responsible for innervating the stomach, small and large intestine as well as the appendix [191]. The hallmarks of Parkinson's and SIBO are malnutrition and osteoporosis. During bacterial overgrowth, unconjugated bile acids predominate, bile acid synthesis is inhibited, and bile acid levels are reduced, resulting in decreased lipid absorption and weight loss due to fat loss. In addition, the absorption of fat-soluble vitamins — primarily vitamin D — is reduced, which can exacerbate osteoporosis in Parkinson's disease [186]. Interestingly, the incidence of SIBO does not depend on the duration of PD — it can occur at an early stage with the same frequency, hence the hypothesis that dysbiosis is not an effect but one of the causes of PD and that improving the gut bacterial status may have a positive effect on the manifestation and progression of PD, but requires further research [189].
4.8.3. Multiple Sclerosis (MS)
Zhang et al. [192] showed that SIBO is highly prevalent in Chinese patients with multiple sclerosis (MS). All patients and controls underwent the glucose breath test to assess SIBO. Forty-five of the 118 MS patients were SIBO positive. Further analytical work is required to establish a causal association between SIBO and MS risk and progression.
4.9. Group 9. Developmental Disorders
Autism Spectrum Disorders (ASD)
Autism spectrum disorders (ASD) are now increasingly being diagnosed, although the pathogenesis is still unknown. Autism severity is divided into three groups (mild, moderate, severe) and is measured based on the Autism Treatment Scale (ATEC) established by Bernard Rimland and Stephen Edelson of the Autism Research Institute [193]. Several studies in patients with varying degrees of autism have shown significant modification in the composition of the gut microbiota. Higher levels of Bacteroides or Clostridium perfringens were observed in the autistic population, while Firmicutes were observed in the healthy population [194,195]. Wang et al. [196] showed that, children with autism had an SIBO incidence of 31.0%, which was higher than that in controls. Autistic children SIBO+ had higher autism treatment evaluation checklist scores than SIBO-. SIBO was significantly associated with worse symptoms of autism, demonstrating that children with SIBO may also significantly contribute to symptoms of autism. Strategies to treat SIBO or to improve gut microflora profile through dietary modulation may help to alleviate gut disorders common in children with autism [196].
4.10. Group 10. Mental Disorders
In recent years, some scholars have found that there is a certain correlation between depression patients and the balance of intestinal microecology. When the intestinal microecology is out of balance, it will lead to aggravation of anxiety and depression symptoms, which counteracts on the gastrointestinal tract, causing microbiota imbalance, among which SIBO is the most common type. Consequently, it is particularly important to find a reliable and safe treatment for SIBO combined with depression [197].
SIBO syndrome is associated with depression, stress and anxiety [198,199,200]. Dysbiosis and inflammation of the gut have been linked to several mental health issues, including anxiety and depression, in children and adults. Fifty people participated in the study, of which 26 were diagnoses SIBO+, and 24 SIBO- (non-SIBO control group). According to conducted research compared to the no-SIBO subgroup, SIBO patients expressed specific patterns of personality traits: higher neuroticism, lower extroversion, and a higher state of anxiety and stress [198]. Experimental studies indicate that psychological stress can negatively affect the transit time of the small intestine, promote SIBO syndrome, and significantly disrupt the balance of the intestinal barrier [198]. The chronic activation of the hypothalamic-pituitary-adrenal (HPA) axis may play a crucial role in developing SIBO because the stress response is closely linked to the gut microbiome [198]. Many researchers focus on analysis and assess the mental state and gastrointestinal complaints of patients with SIBO in relation to tryptophan metabolism and rifaximin treatment [199,200]. Small intestinal bacterial overgrowth alters TRP metabolism , which can be a cause of abdominal disorders and mood disorders. Mild and moderate anxiety, as well as mild depression were diagnosed in all SIBO patients. Changes in TRP metabolism were also observed in these patients. Specifically, an increase in the activity of the serotonin pathway of TRP metabolism in the group SIBO. Rifaximin treatment of SIBO patients ameliorated their mood disorders and gastrointestinal aliments underlined by changes in tryptophan metabolism [200]. Other studies have shown that SIBO occurs in patients with depression and diabetes, with the incidence of this event being twice that of the general population [197]. As suggested by the results of, a capsule containing complex lactic acid bacteria is a boon for SIBO patients with depression and diabetes. It may alleviate symptoms of depression, improve immune function, and reduce levels of inflammatory factors and fasting plasma glucose (FPG), with fewer side effects and potent effects. This may be due to the fact that Lactobacillus regulates the expression of genes related to glucose and lipid metabolism [197].
4.11. Group 11. Genetic Diseases
4.11.1. Cystic Fibrosis (CF)
Scientific literature shows a high prevalence of SIBO in patients with cystic fibrosis (CF). Based on animal studies, it has been observed that the incidence of SIBO in cystic fibrosis ranges from 31% to 56%. The explanation seems to be a mutation in the CFTR gene, leading to increased secretion of abnormal condensed intestinal mucus, and damage to Paneth cells further reduces small intestinal motility [201,202]. According to other studies the prevalence of SIBO in cystic fibrosis was 31.6%. SIBO was associated with pancreas insufficiency, and independently associated with lower BMI and serum albumin levels [203]. Another study reported the prevalence of SIBO in cystic fibrosis as 40.0%; fecal calprotectin levels did not differ between patients with and without SIBO [203]. SIBO has been reported in CF patients. However, the potential link to intestinal inflammation has not been studied so far. Gastrointestinal inflammation is a frequent finding in cystic fibrosis patients. However, SIBO does not seem to be the major or at least not the only determinant of intestinal inflammation [203].
4.11.2. Familial Mediterranean Fever (FMF)
Familial Mediterranean fever (FMF) is an autosomal recessive disease due to a MEFV gene mutation [204]. Colchicine is a fat-soluble alkaloid binding to β-tubulin, hindering its polarization with consequent inhibition of neutrophil chemotaxis and reducing expression of adhesion molecules. It prevents febrile attacks and is an FMF-controlling inflammation. Nevertheless, 5–10% of FMF patients are colchicine nonresponses [204]. This condition may be due to concomitant diseases (vasculitis, inflammatory bowel disease (IBD)) or occult infections acting as trigger factors to reduce drug effectiveness. It has been shown that SIBO affects the responsiveness to colchicine and the clinical severity of patients affected by FMF. We can assume that impaired intestinal bacterial products of intestinal microbiota may act in patients with innate immunity hypersensitivity as FMF or Crohn's disease, accentuating the clinical manifestations of autoinflammatory diseases. Second, we cannot exclude that SIBO may reduce the absorption of colchicine and cause a lack of its effectiveness [204].
4.12. Group 12. Gastrointestinal Cancer
So far, the association between SIBO and pancreatic cancer, cholangiocarcinoma [205], gastric and colorectal cancer [206,207], oesophagogastric (OG) cancer [208], and hepatocellular carcinoma (HCC) [209] has been considered in patients. Liang et al. [206] showed that in a Chinese cohort, SIBO is associated with gastrointestinal cancer. Based on the preliminary intervention study, we conclude that probiotic intervention combats SIBO in patients with gastrointestinal cancer and alleviates its symptoms. Deng et al. [207] examined to investigate the prevalence of small intestinal bacterial overgrowth (SIBO) in patients with colorectal cancer (CRC) after surgical treatment and observe whether gastrointestinal symptoms may improve with rifaximin, 43 postoperative CRC patients (CRC group) and 30 healthy individuals ( normal group) were subjected to the glucose hydrogen breath test (GHBT). Showed that, postoperative CRC patients are more likely to develop SIBO compared with healthy individuals, and SIBO may aggravate digestive symptoms. The administration of rifaximin improved the overall gastrointestinal symptoms, particularly diarrhea, in SIBO+ patients. In patients after oesophagogastric (OG) cancer resection [208] that SIBO does not exhibit specific clinical symptoms thus making its clinical diagnosis even more difficult and need to determine appropriate guidelines for its assessment and treatment after OGC resection. TLR4 protein expression in pancreatic carcinoma and cholangiocarcinoma patients was significantly higher in patients with SIBO than in those without [205]. The relationship between the incidence of SIBO in patients with hepatocellular carcinoma was also investigated [209]. Studies showed that the expression of TLR2 and TLR4 and the incidence of SIBO in HCC patients are significantly higher than in cirrhosis and healthy control group. Moreover, the high expressions of TLR2 and TLR4 in SIBO-positive HCC patients may promote the development of HCC.
5. Conclusions
Awareness and knowledge about this relatively new disease, SIBO, changes the lives of people affected by this problem for the better. So far, the study of the association of SIBO with other diseases has focused mainly on diseases presented in group I – gastrointestinal disorders (irritable bowel syndrome, Crohn's disease, ulcerative colitis, celiac disease, non‒alcoholic fatty liver disease, liver cirrhosis and pancreatitis). The association of SIBO with diseases in this group is well described, and SIBO may play an important role in the pathogenesis of diseases.
In our comprehensive review, we have shown that an increasing number of facts highlight the association of SIBO with other groups of diseases- (II) autoimmune, (III) cardiovascular system, (IV) metabolic, (V) endocrine; (VI) nephrological disorders; (VII) dermatological; (VIII) neurological (IX); developmental disorders; (X) mental disorders; (XI) genetic diseases and (XII) gastrointestinal cancers. SIBO is a risk factor in many groups of diseases, complicates the course of diseases, and may play a pathogenetic role in developing their symptoms. In turn, metabolic diseases (e.g., diabetes) may be a predisposing factor to the development of SIBO. Knowledge about the association of SIBO with various disease groups may help diagnose the problem and initiate effective treatment/co-treatment quickly. The current knowledge about SIBO certainly provides information that can be used to solve various clinical difficulties during SIBO-related diseases. On the other hand, it can be said that knowledge about SIBO certainly requires continuation and expansion.
Author Contributions
Conceptualization, B.H-SZ., and P.R; methodology, B.H-SZ., P.R., E.K; software, E.O.; validation, B.H-SZ., P.R., A.R., SZ.M.; formal analysis, B.H-SZ., A.D., Y-H.CH., Y-H.Y., and I.W-K; investigation, B.H-SZ., P.R., E.K., E.O., A.R., SZ.M; resources, A.D., Y-H.CH., Y-H.Y., SZ.M.; data curation, B.H-SZ., E.K., and P.R.; writing—original draft preparation, B.H-SZ., P.R., E.K., A.R.; writing—review and editing, B.H-SZ; visualization, E.O.; supervision, B.H-SZ; project administration, B.H-SZ; funding acquisition, P.R., I.W-K and B.H-SZ. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Pomeranian Medical University in Szczecin, statutory activity number WMS-136/S/2024. Financed by the Minister of Science under the “Regional Excellence Initiative” Program. Agreement No. RID/SP/0045/2024/01.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Johnstone, C.; Hendry, C.; Farley, A.; McLafferty, E. The digestive system: part 1. Nurs Stand 2014, 28, 37–45. [Google Scholar] [CrossRef] [PubMed]
- de Vos, W.M.; Tilg, H.; Van Hul, M.; Cani, P.D. Gut microbiome and health: mechanistic insights. Gut 2022, 71, 1020–1032. [Google Scholar] [CrossRef] [PubMed]
- Quigley, E.M. Gut bacteria in health and disease. Gastroenterol Hepatol (N Y) 2013, 9, 560–569. [Google Scholar] [PubMed]
- Hrncir, T. Gut Microbiota Dysbiosis: Triggers, Consequences, Diagnostic and Therapeutic Options. Microorganisms 2022, 10. [Google Scholar] [CrossRef] [PubMed]
- Achufusi, T.G.O.; Sharma, A.; Zamora, E.A.; Manocha, D. Small Intestinal Bacterial Overgrowth: Comprehensive Review of Diagnosis, Prevention, and Treatment Methods. Cureus 2020, 12, e8860. [Google Scholar] [CrossRef] [PubMed]
- Judkins, T.C.; Archer, D.L.; Kramer, D.C.; Solch, R.J. Probiotics, Nutrition, and the Small Intestine. Curr Gastroenterol Rep 2020, 22, 2. [Google Scholar] [CrossRef] [PubMed]
- Volk, N.; Lacy, B. Anatomy and Physiology of the Small Bowel. Gastrointest Endosc Clin N Am 2017, 27, 1–13. [Google Scholar] [CrossRef]
- Hooper, L.V.; Gordon, J.I. Commensal host-bacterial relationships in the gut. Science 2001, 292, 1115–1118. [Google Scholar] [CrossRef]
- Ursell, L.K.; Metcalf, J.L.; Parfrey, L.W.; Knight, R. Defining the human microbiome. Nutr Rev 2012, 70 Suppl 1, S38–44. [Google Scholar] [CrossRef]
- Lederberg, J.M., A. T. Ome Sweet 'Omics - A Genealogical Treasury of Words. The Scientist 2001, 15, 8. [Google Scholar]
- Koh, A.; De Vadder, F.; Kovatcheva-Datchary, P.; Backhed, F. From Dietary Fiber to Host Physiology: Short-Chain Fatty Acids as Key Bacterial Metabolites. Cell 2016, 165, 1332–1345. [Google Scholar] [CrossRef]
- Dethlefsen, L.; Eckburg, P.B.; Bik, E.M.; Relman, D.A. Assembly of the human intestinal microbiota. Trends Ecol Evol 2006, 21, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Ley, R.E.; Peterson, D.A.; Gordon, J.I. Ecological and evolutionary forces shaping microbial diversity in the human intestine. Cell 2006, 124, 837–848. [Google Scholar] [CrossRef] [PubMed]
- Adak, A.; Khan, M.R. An insight into gut microbiota and its functionalities. Cell Mol Life Sci 2019, 76, 473–493. [Google Scholar] [CrossRef]
- Losurdo, G.; Salvatore D'Abramo, F.; Indellicati, G.; Lillo, C.; Ierardi, E.; Di Leo, A. The Influence of Small Intestinal Bacterial Overgrowth in Digestive and Extra-Intestinal Disorders. Int J Mol Sci 2020, 21. [Google Scholar] [CrossRef]
- Bohm, M.; Shin, A.; Teagarden, S.; Xu, H.; Gupta, A.; Siwiec, R.; Nelson, D.; Wo, J.M. Risk Factors Associated With Upper Aerodigestive Tract or Coliform Bacterial Overgrowth of the Small Intestine in Symptomatic Patients. J Clin Gastroenterol 2020, 54, 150–157. [Google Scholar] [CrossRef]
- Li, J.; Zhang, R.; Ma, J.; Tang, S.; Li, Y.; Li, Y.; Wan, J. Mucosa-Associated Microbial Profile Is Altered in Small Intestinal Bacterial Overgrowth. Front Microbiol 2021, 12, 710940. [Google Scholar] [CrossRef] [PubMed]
- Pimentel, M.; Saad, R.J.; Long, M.D.; Rao, S.S.C. ACG Clinical Guideline: Small Intestinal Bacterial Overgrowth. Am J Gastroenterol 2020, 115, 165–178. [Google Scholar] [CrossRef]
- Gasbarrini, A.; Lauritano, E.C.; Gabrielli, M.; Scarpellini, E.; Lupascu, A.; Ojetti, V.; Gasbarrini, G. Small intestinal bacterial overgrowth: diagnosis and treatment. Dig Dis 2007, 25, 237–240. [Google Scholar] [CrossRef]
- Bushyhead, D.; Quigley, E.M. Small Intestinal Bacterial Overgrowth. Gastroenterol Clin North Am 2021, 50, 463–474. [Google Scholar] [CrossRef]
- Pearson, R.D. Macrocytic anemia associated with intestinal strictures and anastomoses: report of two cases. Ann Intern Med 1954, 40, 600–610. [Google Scholar] [CrossRef] [PubMed]
- Collins, B.S.; Lin, H.C. Double-blind, placebo-controlled antibiotic treatment study of small intestinal bacterial overgrowth in children with chronic abdominal pain. J Pediatr Gastroenterol Nutr 2011, 52, 382–386. [Google Scholar] [CrossRef] [PubMed]
- de Boissieu, D.; Chaussain, M.; Badoual, J.; Raymond, J.; Dupont, C. Small-bowel bacterial overgrowth in children with chronic diarrhea, abdominal pain, or both. J Pediatr 1996, 128, 203–207. [Google Scholar] [CrossRef] [PubMed]
- Korterink, J.J.; Benninga, M.A.; van Wering, H.M.; Deckers-Kocken, J.M. Glucose hydrogen breath test for small intestinal bacterial overgrowth in children with abdominal pain-related functional gastrointestinal disorders. J Pediatr Gastroenterol Nutr 2015, 60, 498–502. [Google Scholar] [CrossRef] [PubMed]
- Siniewicz-Luzenczyk, K.; Bik-Gawin, A.; Zeman, K.; Bak-Romaniszyn, L. Small intestinal bacterial overgrowth syndrome in children. Prz Gastroenterol 2015, 10, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Rezaie, A.; Buresi, M.; Lembo, A.; Lin, H.; McCallum, R.; Rao, S.; Schmulson, M.; Valdovinos, M.; Zakko, S.; Pimentel, M. Hydrogen and Methane-Based Breath Testing in Gastrointestinal Disorders: The North American Consensus. Am J Gastroenterol 2017, 112, 775–784. [Google Scholar] [CrossRef] [PubMed]
- Saad, R.J.; Chey, W.D. Breath testing for small intestinal bacterial overgrowth: maximizing test accuracy. Clin Gastroenterol Hepatol 2014, 12, 1964–1972. [Google Scholar] [CrossRef]
- Rao, S.S.C.; Bhagatwala, J. Small Intestinal Bacterial Overgrowth: Clinical Features and Therapeutic Management. Clin Transl Gastroenterol 2019, 10, e00078. [Google Scholar] [CrossRef]
- Shaker, A.; Peng, B.; Soffer, E. Pattern of methane levels with lactulose breath testing; can we shorten the test duration? JGH Open 2021, 5, 809–812. [Google Scholar] [CrossRef]
- Dukowicz, A.C.; Lacy, B.E.; Levine, G.M. Small intestinal bacterial overgrowth: a comprehensive review. Gastroenterol Hepatol (N Y) 2007, 3, 112–122. [Google Scholar]
- Adike, A.; DiBaise, J.K. Small Intestinal Bacterial Overgrowth: Nutritional Implications, Diagnosis, and Management. Gastroenterol Clin North Am 2018, 47, 193–208. [Google Scholar] [CrossRef] [PubMed]
- Vanderhoof, J.A.; Young, R.J.; Murray, N.; Kaufman, S.S. Treatment strategies for small bowel bacterial overgrowth in short bowel syndrome. J Pediatr Gastroenterol Nutr 1998, 27, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Parodi, A.; Sessarego, M.; Greco, A.; Bazzica, M.; Filaci, G.; Setti, M.; Savarino, E.; Indiveri, F.; Savarino, V.; Ghio, M. Small intestinal bacterial overgrowth in patients suffering from scleroderma: clinical effectiveness of its eradication. Am J Gastroenterol 2008, 103, 1257–1262. [Google Scholar] [CrossRef] [PubMed]
- Frissora, C.L.; Cash, B.D. Review article: the role of antibiotics vs. conventional pharmacotherapy in treating symptoms of irritable bowel syndrome. Aliment Pharmacol Ther 2007, 25, 1271–1281. [Google Scholar] [CrossRef] [PubMed]
- Koo, H.L.; DuPont, H.L. Rifaximin: a unique gastrointestinal-selective antibiotic for enteric diseases. Curr Opin Gastroenterol 2010, 26, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Gatta, L.; Scarpignato, C. Systematic review with meta-analysis: rifaximin is effective and safe for the treatment of small intestine bacterial overgrowth. Aliment Pharmacol Ther 2017, 45, 604–616. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Lee, H.R.; Low, K.; Chatterjee, S.; Pimentel, M. Rifaximin versus other antibiotics in the primary treatment and retreatment of bacterial overgrowth in IBS. Dig Dis Sci 2008, 53, 169–174. [Google Scholar] [CrossRef]
- Rabenstein, T.; Fromm, M.F.; Zolk, O. [Rifaximin--a non-resorbable antibiotic with many indications in gastroenterology]. Z Gastroenterol 2011, 49, 211–224. [Google Scholar] [CrossRef]
- Di Stefano, M.; Strocchi, A.; Malservisi, S.; Veneto, G.; Ferrieri, A.; Corazza, G.R. Non-absorbable antibiotics for managing intestinal gas production and gas-related symptoms. Aliment Pharmacol Ther 2000, 14, 1001–1008. [Google Scholar] [CrossRef] [PubMed]
- Xu, F.; Li, N.; Wang, C.; Xing, H.; Chen, D.; Wei, Y. Clinical efficacy of fecal microbiota transplantation for patients with small intestinal bacterial overgrowth: a randomized, placebo-controlled clinic study. BMC Gastroenterol 2021, 21, 54. [Google Scholar] [CrossRef]
- Nickles, M.A.; Hasan, A.; Shakhbazova, A.; Wright, S.; Chambers, C.J.; Sivamani, R.K. Alternative Treatment Approaches to Small Intestinal Bacterial Overgrowth: A Systematic Review. J Altern Complement Med 2021, 27, 108–119. [Google Scholar] [CrossRef]
- Khalighi, A.R.; Khalighi, M.R.; Behdani, R.; Jamali, J.; Khosravi, A.; Kouhestani, S.; Radmanesh, H.; Esmaeelzadeh, S.; Khalighi, N. Evaluating the efficacy of probiotic on treatment in patients with small intestinal bacterial overgrowth (SIBO)--a pilot study. Indian J Med Res 2014, 140, 604–608. [Google Scholar]
- Leventogiannis, K.; Gkolfakis, P.; Spithakis, G.; Tsatali, A.; Pistiki, A.; Sioulas, A.; Giamarellos-Bourboulis, E.J.; Triantafyllou, K. Effect of a Preparation of Four Probiotics on Symptoms of Patients with Irritable Bowel Syndrome: Association with Intestinal Bacterial Overgrowth. Probiotics Antimicrob Proteins 2019, 11, 627–634. [Google Scholar] [CrossRef]
- Souza, C.; Rocha, R.; Cotrim, H.P. Diet and intestinal bacterial overgrowth: Is there evidence? World J Clin Cases 2022, 10, 4713–4716. [Google Scholar] [CrossRef]
- Staudacher, H.M.; Irving, P.M.; Lomer, M.C.; Whelan, K. Mechanisms and efficacy of dietary FODMAP restriction in IBS. Nat Rev Gastroenterol Hepatol 2014, 11, 256–266. [Google Scholar] [CrossRef] [PubMed]
- Ginnebaugh, B.; Chey, W.D.; Saad, R. Small Intestinal Bacterial Overgrowth: How to Diagnose and Treat (and Then Treat Again). Gastroenterol Clin North Am 2020, 49, 571–587. [Google Scholar] [CrossRef]
- Takakura, W.; Pimentel, M. Small Intestinal Bacterial Overgrowth and Irritable Bowel Syndrome - An Update. Front Psychiatry 2020, 11, 664. [Google Scholar] [CrossRef] [PubMed]
- Gray, J.D.; Shiner, M. Influence of gastric pH on gastric and jejunal flora. Gut 1967, 8, 574–581. [Google Scholar] [CrossRef] [PubMed]
- Saltzman, J.R.; Kowdley, K.V.; Pedrosa, M.C.; Sepe, T.; Golner, B.; Perrone, G.; Russell, R.M. Bacterial overgrowth without clinical malabsorption in elderly hypochlorhydric subjects. Gastroenterology 1994, 106, 615–623. [Google Scholar] [CrossRef]
- Husebye, E.; Skar, V.; Hoverstad, T.; Melby, K. Fasting hypochlorhydria with gram positive gastric flora is highly prevalent in healthy old people. Gut 1992, 33, 1331–1337. [Google Scholar] [CrossRef]
- Iivonen, M.K.; Ahola, T.O.; Matikainen, M.J. Bacterial overgrowth, intestinal transit, and nutrition after total gastrectomy. Comparison of a jejunal pouch with Roux-en-Y reconstruction in a prospective random study. Scand J Gastroenterol 1998, 33, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Brandi, G.; Biavati, B.; Calabrese, C.; Granata, M.; Nannetti, A.; Mattarelli, P.; Di Febo, G.; Saccoccio, G.; Biasco, G. Urease-positive bacteria other than Helicobacter pylori in human gastric juice and mucosa. Am J Gastroenterol 2006, 101, 1756–1761. [Google Scholar] [CrossRef]
- Shindo, K.; Fukumura, M. Effect of H2-receptor antagonists on bile acid metabolism. J Investig Med 1995, 43, 170–177. [Google Scholar] [PubMed]
- Kim, D.B.; Paik, C.N.; Kim, Y.J.; Lee, J.M.; Jun, K.H.; Chung, W.C.; Lee, K.M.; Yang, J.M.; Choi, M.G. Positive Glucose Breath Tests in Patients with Hysterectomy, Gastrectomy, and Cholecystectomy. Gut Liver 2017, 11, 237–242. [Google Scholar] [CrossRef]
- Mouillot, T.; Rhyman, N.; Gauthier, C.; Paris, J.; Lang, A.S.; Lepers-Tassy, S.; Manfredi, S.; Lepage, C.; Leloup, C.; Jacquin-Piques, A.; et al. Study of Small Intestinal Bacterial Overgrowth in a Cohort of Patients with Abdominal Symptoms Who Underwent Bariatric Surgery. Obes Surg 2020, 30, 2331–2337. [Google Scholar] [CrossRef] [PubMed]
- Onana Ndong, P.; Boutallaka, H.; Marine-Barjoan, E.; Ouizeman, D.; Mroue, R.; Anty, R.; Vanbiervliet, G.; Piche, T. Prevalence of small intestinal bacterial overgrowth in irritable bowel syndrome (IBS): Correlating H(2) or CH(4) production with severity of IBS. JGH Open 2023, 7, 311–320. [Google Scholar] [CrossRef]
- Yu, X.; Li, Y.; Xiang, F.; Feng, J. Correlation between small intestinal bacterial overgrowth and irritable bowel syndrome and the prognosis of treatment. Ann Palliat Med 2021, 10, 3364–3370. [Google Scholar] [CrossRef] [PubMed]
- Wu, K.Q.; Sun, W.J.; Li, N.; Chen, Y.Q.; Wei, Y.L.; Chen, D.F. Small intestinal bacterial overgrowth is associated with Diarrhea-predominant irritable bowel syndrome by increasing mainly Prevotella abundance. Scand J Gastroenterol 2019, 54, 1419–1425. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.C. Small intestinal bacterial overgrowth: a framework for understanding irritable bowel syndrome. JAMA 2004, 292, 852–858. [Google Scholar] [CrossRef]
- Pimentel, M.; Chow, E.J.; Lin, H.C. Normalization of lactulose breath testing correlates with symptom improvement in irritable bowel syndrome. a double-blind, randomized, placebo-controlled study. Am J Gastroenterol 2003, 98, 412–419. [Google Scholar] [CrossRef]
- Pimentel, M.; Wallace, D.; Hallegua, D.; Chow, E.; Kong, Y.; Park, S.; Lin, H.C. A link between irritable bowel syndrome and fibromyalgia may be related to findings on lactulose breath testing. Ann Rheum Dis 2004, 63, 450–452. [Google Scholar] [CrossRef]
- Posserud, I.; Stotzer, P.O.; Bjornsson, E.S.; Abrahamsson, H.; Simren, M. Small intestinal bacterial overgrowth in patients with irritable bowel syndrome. Gut 2007, 56, 802–808. [Google Scholar] [CrossRef] [PubMed]
- Bratten, J.R.; Spanier, J.; Jones, M.P. Lactulose breath testing does not discriminate patients with irritable bowel syndrome from healthy controls. Am J Gastroenterol 2008, 103, 958–963. [Google Scholar] [CrossRef] [PubMed]
- Ghoshal, U.C.; Kumar, S.; Mehrotra, M.; Lakshmi, C.; Misra, A. Frequency of small intestinal bacterial overgrowth in patients with irritable bowel syndrome and chronic non-specific diarrhea. J Neurogastroenterol Motil 2010, 16, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Sachdeva, S.; Rawat, A.K.; Reddy, R.S.; Puri, A.S. Small intestinal bacterial overgrowth (SIBO) in irritable bowel syndrome: frequency and predictors. J Gastroenterol Hepatol 2011, 26 Suppl 3, 135–138. [Google Scholar] [CrossRef]
- Abbasi, M.H.; Zahedi, M.; Darvish Moghadam, S.; Shafieipour, S.; HayatBakhsh Abbasi, M. Small bowel bacterial overgrowth in patients with irritable bowel syndrome: the first study in iran. Middle East J Dig Dis 2015, 7, 36–40. [Google Scholar]
- Parodi, A.; Dulbecco, P.; Savarino, E.; Giannini, E.G.; Bodini, G.; Corbo, M.; Isola, L.; De Conca, S.; Marabotto, E.; Savarino, V. Positive glucose breath testing is more prevalent in patients with IBS-like symptoms compared with controls of similar age and gender distribution. J Clin Gastroenterol 2009, 43, 962–966. [Google Scholar] [CrossRef]
- Ghoshal, U.C.; Yadav, A.; Fatima, B.; Agrahari, A.P.; Misra, A. Small intestinal bacterial overgrowth in patients with inflammatory bowel disease: A case-control study. Indian J Gastroenterol 2022, 41, 96–103. [Google Scholar] [CrossRef]
- Aziz, I.; Tornblom, H.; Simren, M. Small intestinal bacterial overgrowth as a cause for irritable bowel syndrome: guilty or not guilty? Curr Opin Gastroenterol 2017, 33, 196–202. [Google Scholar] [CrossRef]
- Wei, J.; Feng, J.; Chen, L.; Yang, Z.; Tao, H.; Li, L.; Xuan, J.; Wang, F. Small intestinal bacterial overgrowth is associated with clinical relapse in patients with quiescent Crohn's disease: a retrospective cohort study. Ann Transl Med 2022, 10, 784. [Google Scholar] [CrossRef]
- Kulygina, Y.O., M.; Skalinskaya, M.; Alikina, T.; Kabilov, M.; Lukinov, V.; Sitkin, S. Small intestinal bacterial overgrowth in patients with Crohn’s disease is not only associated with a more severe disease, but is also marked by dramatic changes in the gut microbiome. Journal of Crohn's and Colitis. [CrossRef]
- Bertges, E.R.; Chebli, J.M.F. Prevalence and Factors Associated with Small Intestinal Bacterial Overgrowth in Patients with Crohn's Disease: A Retrospective Study at a Referral Center. Arq Gastroenterol 2020, 57, 283–288. [Google Scholar] [CrossRef]
- Wanzl, J.; Grohl, K.; Kafel, A.; Nagl, S.; Muzalyova, A.; Golder, S.K.; Ebigbo, A.; Messmann, H.; Schnoy, E. Impact of Small Intestinal Bacterial Overgrowth in Patients with Inflammatory Bowel Disease and Other Gastrointestinal Disorders-A Retrospective Analysis in a Tertiary Single Center and Review of the Literature. J Clin Med 2023, 12. [Google Scholar] [CrossRef]
- Yang, C.; Zhang, X.; Wang, S.; Huo, X.; Wang, J. Small intestinal bacterial overgrowth and evaluation of intestinal barrier function in patients with ulcerative colitis. Am J Transl Res 2021, 13, 6605–6610. [Google Scholar]
- Pimentel, M.; Mathur, R.; Chang, C. Gas and the microbiome. Curr Gastroenterol Rep 2013, 15, 356. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Mekelburg, S.; Tafesh, Z.; Coburn, E.; Weg, R.; Malik, N.; Webb, C.; Hammad, H.; Scherl, E.; Bosworth, B.P. Testing and Treating Small Intestinal Bacterial Overgrowth Reduces Symptoms in Patients with Inflammatory Bowel Disease. Dig Dis Sci 2018, 63, 2439–2444. [Google Scholar] [CrossRef]
- Shah, A.; Morrison, M.; Burger, D.; Martin, N.; Rich, J.; Jones, M.; Koloski, N.; Walker, M.M.; Talley, N.J.; Holtmann, G.J. Systematic review with meta-analysis: the prevalence of small intestinal bacterial overgrowth in inflammatory bowel disease. Aliment Pharmacol Ther 2019, 49, 624–635. [Google Scholar] [CrossRef]
- Yang, C.; Guo, X.; Wang, J.; Fan, H.; Huo, X.; Dong, L.; Duan, Z. Relationship between Small Intestinal Bacterial Overgrowth and Peripheral Blood ET, TLR2 and TLR4 in Ulcerative Colitis. J Coll Physicians Surg Pak 2020, 30, 245–249. [Google Scholar] [CrossRef]
- Safi, M.A.; Jiman-Fatani, A.A.; Saadah, O.I. Small intestinal bacterial overgrowth among patients with celiac disease unresponsive to a gluten free diet. Turk J Gastroenterol 2020, 31, 767–774. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.; Thite, P.; Hansen, T.; Kendall, B.J.; Sanders, D.S.; Morrison, M.; Jones, M.P.; Holtmann, G. Links between celiac disease and small intestinal bacterial overgrowth: A systematic review and meta-analysis. J Gastroenterol Hepatol 2022, 37, 1844–1852. [Google Scholar] [CrossRef]
- Prizont, R.; Hersh, T.; Floch, M.H. Jejunal bacterial flora in chronic small bowel disease. I. Celiac disease. II. Regional enteritis. Am J Clin Nutr 1970, 23, 1602–1607. [Google Scholar] [CrossRef]
- Tursi, A.; Brandimarte, G.; Giorgetti, G. High prevalence of small intestinal bacterial overgrowth in celiac patients with persistence of gastrointestinal symptoms after gluten withdrawal. Am J Gastroenterol 2003, 98, 839–843. [Google Scholar] [CrossRef]
- Fraquelli, M.; Bardella, M.T.; Peracchi, M.; Cesana, B.M.; Bianchi, P.A.; Conte, D. Gallbladder emptying and somatostatin and cholecystokinin plasma levels in celiac disease. Am J Gastroenterol 1999, 94, 1866–1870. [Google Scholar] [CrossRef]
- Bardella, M.T.; Fraquelli, M.; Peracchi, M.; Cesana, B.M.; Bianchi, P.A.; Conte, D. Gastric emptying and plasma neurotensin levels in untreated celiac patients. Scand J Gastroenterol 2000, 35, 269–273. [Google Scholar] [CrossRef]
- Rubio-Tapia, A.; Barton, S.H.; Rosenblatt, J.E.; Murray, J.A. Prevalence of small intestine bacterial overgrowth diagnosed by quantitative culture of intestinal aspirate in celiac disease. J Clin Gastroenterol 2009, 43, 157–161. [Google Scholar] [CrossRef]
- Chang, M.S.; Minaya, M.T.; Cheng, J.; Connor, B.A.; Lewis, S.K.; Green, P.H. Double-blind randomized controlled trial of rifaximin for persistent symptoms in patients with celiac disease. Dig Dis Sci 2011, 56, 2939–2946. [Google Scholar] [CrossRef] [PubMed]
- Charlesworth, R.P.G.; Winter, G. Small intestinal bacterial overgrowth and Celiac disease - coincidence or causation? Expert Rev Gastroenterol Hepatol 2020, 14, 305–306. [Google Scholar] [CrossRef] [PubMed]
- Ghoshal, U.C.; Goel, A.; Quigley, E.M.M. Gut microbiota abnormalities, small intestinal bacterial overgrowth, and non-alcoholic fatty liver disease: An emerging paradigm. Indian J Gastroenterol 2020, 39, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Gudan, A.; Kozlowska-Petriczko, K.; Wunsch, E.; Bodnarczuk, T.; Stachowska, E. Small Intestinal Bacterial Overgrowth and Non-Alcoholic Fatty Liver Disease: What Do We Know in 2023? Nutrients 2023, 15. [Google Scholar] [CrossRef]
- Augustyn, M.; Grys, I.; Kukla, M. Small intestinal bacterial overgrowth and nonalcoholic fatty liver disease. Clin Exp Hepatol 2019, 5, 1–10. [Google Scholar] [CrossRef]
- Miele, L.; Valenza, V.; La Torre, G.; Montalto, M.; Cammarota, G.; Ricci, R.; Masciana, R.; Forgione, A.; Gabrieli, M.L.; Perotti, G.; et al. Increased intestinal permeability and tight junction alterations in nonalcoholic fatty liver disease. Hepatology 2009, 49, 1877–1887. [Google Scholar] [CrossRef]
- Fialho, A.; Fialho, A.; Thota, P.; McCullough, A.J.; Shen, B. Small Intestinal Bacterial Overgrowth Is Associated with Non-Alcoholic Fatty Liver Disease. J Gastrointestin Liver Dis 2016, 25, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.; Mao, L.; Wang, L.; Quan, X.; Xu, X.; Cheng, Y.; Zhu, S.; Dai, F. Small intestinal bacterial overgrowth and orocecal transit time in patients of nonalcoholic fatty liver disease. Eur J Gastroenterol Hepatol 2021, 33, e535–e539. [Google Scholar] [CrossRef]
- Gudan, A.; Jamiol-Milc, D.; Hawrylkowicz, V.; Skonieczna-Zydecka, K.; Stachowska, E. The Prevalence of Small Intestinal Bacterial Overgrowth in Patients with Non-Alcoholic Liver Diseases: NAFLD, NASH, Fibrosis, Cirrhosis-A Systematic Review, Meta-Analysis and Meta-Regression. Nutrients 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Mikolasevic, I.; Delija, B.; Mijic, A.; Stevanovic, T.; Skenderevic, N.; Sosa, I.; Krznaric-Zrnic, I.; Abram, M.; Krznaric, Z.; Domislovic, V.; et al. Small intestinal bacterial overgrowth and non-alcoholic fatty liver disease diagnosed by transient elastography and liver biopsy. Int J Clin Pract 2021, 75, e13947. [Google Scholar] [CrossRef] [PubMed]
- Kuang, L.; Zhou, W.; Jiang, Y. Association of small intestinal bacterial overgrowth with nonalcoholic fatty liver disease in children: A meta-analysis. PLoS One 2021, 16, e0260479. [Google Scholar] [CrossRef] [PubMed]
- Stepanov, Y.M.; Zavhorodnia, N.Y.; Yagmur, V.B.; Lukianenko, O.Y.; Zygalo, E.V. Association of nonalcoholic fatty liver disease with small intestine bacterial overgrowth in obese children. Wiad Lek 2019, 72, 350–356. [Google Scholar] [CrossRef] [PubMed]
- Bakhshimoghaddam, F.; Alizadeh, M. Contribution of gut microbiota to nonalcoholic fatty liver disease: Pathways of mechanisms. Clin Nutr ESPEN 2021, 44, 61–68. [Google Scholar] [CrossRef]
- GuimarAes, V.M.; Santos, V.N.; Borges, P.S.A.; JLR, D.E.F.; Grillo, P.; Parise, E.R. Peripheral Blood Endotoxin Levels Are Not Associated with Small Intestinal Bacterial Overgrowth in Nonalcoholic Fatty Liver Disease without Cirrhosis. Arq Gastroenterol 2020, 57, 471–476. [Google Scholar] [CrossRef]
- Gkolfakis, P.; Tziatzios, G.; Leite, G.; Papanikolaou, I.S.; Xirouchakis, E.; Panayiotides, I.G.; Karageorgos, A.; Millan, M.J.; Mathur, R.; Weitsman, S.; et al. Prevalence of Small Intestinal Bacterial Overgrowth Syndrome in Patients with Non-Alcoholic Fatty Liver Disease/Non-Alcoholic Steatohepatitis: A Cross-Sectional Study. Microorganisms 2023, 11. [Google Scholar] [CrossRef]
- Gunnarsdottir, S.A.; Sadik, R.; Shev, S.; Simren, M.; Sjovall, H.; Stotzer, P.O.; Abrahamsson, H.; Olsson, R.; Bjornsson, E.S. Small intestinal motility disturbances and bacterial overgrowth in patients with liver cirrhosis and portal hypertension. Am J Gastroenterol 2003, 98, 1362–1370. [Google Scholar] [CrossRef]
- Chesta, J.; Silva, M.; Thompson, L.; del Canto, E.; Defilippi, C. [Bacterial overgrowth in small intestine in patients with liver cirrhosis]. Rev Med Chil 1991, 119, 626–632. [Google Scholar] [PubMed]
- Maslennikov, R.; Pavlov, C.; Ivashkin, V. Small intestinal bacterial overgrowth in cirrhosis: systematic review and meta-analysis. Hepatol Int 2018, 12, 567–576. [Google Scholar] [CrossRef] [PubMed]
- Maslennikov, R.; Ivashkin, V.; Efremova, I.; Poluektova, E.; Kudryavtseva, A.; Krasnov, G. Gut dysbiosis and small intestinal bacterial overgrowth as independent forms of gut microbiota disorders in cirrhosis. World J Gastroenterol 2022, 28, 1067–1077. [Google Scholar] [CrossRef]
- Ghosh, G.; Jesudian, A.B. Small Intestinal Bacterial Overgrowth in Patients With Cirrhosis. J Clin Exp Hepatol 2019, 9, 257–267. [Google Scholar] [CrossRef]
- Feng, X.; Li, X.; Zhang, X.; Chen, W.; Tian, Y.; Yang, Q.; Yang, Y.; Pan, H.; Jiang, Z. Hepatic Encephalopathy in Cirrhotic Patients and Risk of Small Intestinal Bacterial Overgrowth: A Systematic Review and Meta-Analysis. Biomed Res Int 2022, 2022, 2469513. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.B.; Paik, C.N.; Sung, H.J.; Chung, W.C.; Lee, K.M.; Yang, J.M.; Choi, M.G. Breath hydrogen and methane are associated with intestinal symptoms in patients with chronic pancreatitis. Pancreatology 2015, 15, 514–518. [Google Scholar] [CrossRef] [PubMed]
- Signoretti, M.; Stigliano, S.; Valente, R.; Piciucchi, M.; Delle Fave, G.; Capurso, G. Small intestinal bacterial overgrowth in patients with chronic pancreatitis. J Clin Gastroenterol 2014, 48 Suppl 1, S52–55. [Google Scholar] [CrossRef]
- Ni Chonchubhair, H.M.; Bashir, Y.; Dobson, M.; Ryan, B.M.; Duggan, S.N.; Conlon, K.C. The prevalence of small intestinal bacterial overgrowth in non-surgical patients with chronic pancreatitis and pancreatic exocrine insufficiency (PEI). Pancreatology 2018, 18, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Zhu, H.M.; He, F.; Li, B.Y.; Li, X.C. Association between acute pancreatitis and small intestinal bacterial overgrowth assessed by hydrogen breath test. World J Gastroenterol 2017, 23, 8591–8596. [Google Scholar] [CrossRef]
- Kim, D.B.; Paik, C.N.; Lee, J.M.; Kim, Y.J. Association between increased breath hydrogen methane concentration and prevalence of glucose intolerance in acute pancreatitis. J Breath Res 2020, 14, 026006. [Google Scholar] [CrossRef]
- El Kurdi, B.; Babar, S.; El Iskandarani, M.; Bataineh, A.; Lerch, M.M.; Young, M.; Singh, V.P. Factors That Affect Prevalence of Small Intestinal Bacterial Overgrowth in Chronic Pancreatitis: A Systematic Review, Meta-Analysis, and Meta-Regression. Clin Transl Gastroenterol 2019, 10, e00072. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.Q.; Cui, M.Y.; Jiang, Q.L.; Wang, J.J.; Fan, M.Y.; Lu, Y.Y. Characterization of Duodenal Microbiota in Patients with Acute Pancreatitis and Healthy Controls. Dig Dis Sci 2023, 68, 3341–3353. [Google Scholar] [CrossRef]
- Lee, A.A.; Baker, J.R.; Wamsteker, E.J.; Saad, R.; DiMagno, M.J. Small Intestinal Bacterial Overgrowth Is Common in Chronic Pancreatitis and Associates With Diabetes, Chronic Pancreatitis Severity, Low Zinc Levels, and Opiate Use. Am J Gastroenterol 2019, 114, 1163–1171. [Google Scholar] [CrossRef]
- Gyger, G.; Baron, M. Gastrointestinal manifestations of scleroderma: recent progress in evaluation, pathogenesis, and management. Curr Rheumatol Rep 2012, 14, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Sjogren, R.W. Gastrointestinal motility disorders in scleroderma. Arthritis Rheum 1994, 37, 1265–1282. [Google Scholar] [CrossRef]
- Bharadwaj, S.; Tandon, P.; Gohel, T.; Corrigan, M.L.; Coughlin, K.L.; Shatnawei, A.; Chatterjee, S.; Kirby, D.F. Gastrointestinal Manifestations, Malnutrition, and Role of Enteral and Parenteral Nutrition in Patients With Scleroderma. J Clin Gastroenterol 2015, 49, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Collinot, G.; Madrigal-Santillan, E.O.; Martinez-Bencomo, M.A.; Carranza-Muleiro, R.A.; Jara, L.J.; Vera-Lastra, O.; Montes-Cortes, D.H.; Medina, G.; Cruz-Dominguez, M.P. Effectiveness of Saccharomyces boulardii and Metronidazole for Small Intestinal Bacterial Overgrowth in Systemic Sclerosis. Dig Dis Sci 2020, 65, 1134–1143. [Google Scholar] [CrossRef]
- Morrisroe, K.; Baron, M.; Frech, T.; Nikpour, M. Small intestinal bacterial overgrowth in systemic sclerosis. J Scleroderma Relat Disord 2020, 5, 33–39. [Google Scholar] [CrossRef]
- Sawadpanich, K.; Soison, P.; Chunlertrith, K.; Mairiang, P.; Sukeepaisarnjaroen, W.; Sangchan, A.; Suttichaimongkol, T.; Foocharoen, C. Prevalence and associated factors of small intestinal bacterial overgrowth among systemic sclerosis patients. Int J Rheum Dis 2019, 22, 695–699. [Google Scholar] [CrossRef]
- Levin, D.; De Palma, G.; Zou, H.; Bazzaz, A.H.Z.; Verdu, E.; Baker, B.; Pinto-Sanchez, M.I.; Khalidi, N.; Larche, M.J.; Beattie, K.A.; et al. Fecal microbiome differs between patients with systemic sclerosis with and without small intestinal bacterial overgrowth. J Scleroderma Relat Disord 2021, 6, 290–298. [Google Scholar] [CrossRef]
- Shah, A.; Pakeerathan, V.; Jones, M.P.; Kashyap, P.C.; Virgo, K.; Fairlie, T.; Morrison, M.; Ghoshal, U.C.; Holtmann, G.J. Small Intestinal Bacterial Overgrowth Complicating Gastrointestinal Manifestations of Systemic Sclerosis: A Systematic Review and Meta-analysis. J Neurogastroenterol Motil 2023, 29, 132–144. [Google Scholar] [CrossRef] [PubMed]
- Fynne, L.; Worsoe, J.; Gregersen, T.; Schlageter, V.; Laurberg, S.; Krogh, K. Gastrointestinal transit in patients with systemic sclerosis. Scand J Gastroenterol 2011, 46, 1187–1193. [Google Scholar] [CrossRef] [PubMed]
- Savarino, E.; Mei, F.; Parodi, A.; Ghio, M.; Furnari, M.; Gentile, A.; Berdini, M.; Di Sario, A.; Bendia, E.; Bonazzi, P.; et al. Gastrointestinal motility disorder assessment in systemic sclerosis. Rheumatology (Oxford) 2013, 52, 1095–1100. [Google Scholar] [CrossRef] [PubMed]
- Stellaard, F.; Sauerbruch, T.; Luderschmidt, C.H.; Leisner, B.; Paumgartner, G. Intestinal involvement in progressive systemic sclerosis detected by increased unconjugated serum bile acids. Gut 1987, 28, 446–450. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.; Li, X.Q.; Jiang, Z. Prevalence and predictors of small intestinal bacterial overgrowth in systemic sclerosis: a systematic review and meta-analysis. Clin Rheumatol 2021, 40, 3039–3051. [Google Scholar] [CrossRef]
- Tian, X.P.; Zhang, X. Gastrointestinal complications of systemic sclerosis. World J Gastroenterol 2013, 19, 7062–7068. [Google Scholar] [CrossRef] [PubMed]
- Marie, I.; Leroi, A.M.; Menard, J.F.; Levesque, H.; Quillard, M.; Ducrotte, P. Fecal calprotectin in systemic sclerosis and review of the literature. Autoimmun Rev 2015, 14, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Polkowska-Pruszynska, B.; Gerkowicz, A.; Rawicz-Pruszynski, K.; Krasowska, D. The Role of Fecal Calprotectin in Patients with Systemic Sclerosis and Small Intestinal Bacterial Overgrowth (SIBO). Diagnostics (Basel) 2020, 10. [Google Scholar] [CrossRef]
- Fiorentini, E.; Russo, E.; Amedei, A.; Bellando Randone, S. Fecal microbiome in systemic sclerosis, in search for the best candidate for microbiota-targeted therapy for small intestinal bacterial overgrowth control. J Scleroderma Relat Disord 2022, 7, 163–167. [Google Scholar] [CrossRef]
- Niebauer, J.; Volk, H.D.; Kemp, M.; Dominguez, M.; Schumann, R.R.; Rauchhaus, M.; Poole-Wilson, P.A.; Coats, A.J.; Anker, S.D. Endotoxin and immune activation in chronic heart failure: a prospective cohort study. Lancet 1999, 353, 1838–1842. [Google Scholar] [CrossRef]
- Sandek, A.; Rauchhaus, M.; Anker, S.D.; von Haehling, S. The emerging role of the gut in chronic heart failure. Curr Opin Clin Nutr Metab Care 2008, 11, 632–639. [Google Scholar] [CrossRef]
- Anker, S.D.; von Haehling, S. Inflammatory mediators in chronic heart failure: an overview. Heart 2004, 90, 464–470. [Google Scholar] [CrossRef]
- Song, Y.; Liu, Y.; Qi, B.; Cui, X.; Dong, X.; Wang, Y.; Han, X.; Li, F.; Shen, D.; Zhang, X.; et al. Association of Small Intestinal Bacterial Overgrowth With Heart Failure and Its Prediction for Short-Term Outcomes. J Am Heart Assoc 2021, 10, e015292. [Google Scholar] [CrossRef] [PubMed]
- Mollar, A.; Marrachelli, V.G.; Nunez, E.; Monleon, D.; Bodi, V.; Sanchis, J.; Navarro, D.; Nunez, J. Bacterial metabolites trimethylamine N-oxide and butyrate as surrogates of small intestinal bacterial overgrowth in patients with a recent decompensated heart failure. Sci Rep 2021, 11, 6110. [Google Scholar] [CrossRef]
- Liu, Y.; Chu, M.; Wang, D.; Luo, Y.; Liu, Z.; Zhao, J. Risk factors for small intestinal bacterial overgrowth in patients with acute ischaemic stroke. J Med Microbiol 2023, 72. [Google Scholar] [CrossRef]
- Cheng, X.; Zhang, L.; Xie, N.C.; Xu, H.L.; Lian, Y.J. Association between small-intestinal bacterial overgrowth and deep vein thrombosis in patients with spinal cord injuries. J Thromb Haemost 2017, 15, 304–311. [Google Scholar] [CrossRef] [PubMed]
- He, Z.; Ding, R.; Wu, F.; Wu, Z.; Liang, C. Excess Alcohol Consumption: A Potential Mechanism Behind the Association Between Small Intestinal Bacterial Overgrowth and Coronary Artery Disease. Dig Dis Sci 2018, 63, 3516–3517. [Google Scholar] [CrossRef] [PubMed]
- Dong, C.; Wang, G.; Xian, R.; Li, C.; Wang, S.; Cui, L. Association between Small Intestinal Bacterial Overgrowth and Subclinical Atheromatous Plaques. J Clin Med 2022, 12. [Google Scholar] [CrossRef]
- Ponziani, F.R.; Pompili, M.; Di Stasio, E.; Zocco, M.A.; Gasbarrini, A.; Flore, R. Subclinical atherosclerosis is linked to small intestinal bacterial overgrowth via vitamin K2-dependent mechanisms. World J Gastroenterol 2017, 23, 1241–1249. [Google Scholar] [CrossRef]
- Ojetti, V.; Pitocco, D.; Scarpellini, E.; Zaccardi, F.; Scaldaferri, F.; Gigante, G.; Gasbarrini, G.; Ghirlanda, G.; Gasbarrini, A. Small bowel bacterial overgrowth and type 1 diabetes. Eur Rev Med Pharmacol Sci 2009, 13, 419–423. [Google Scholar]
- Rana, S.; Bhansali, A.; Bhadada, S.; Sharma, S.; Kaur, J.; Singh, K. Orocecal transit time and small intestinal bacterial overgrowth in type 2 diabetes patients from North India. Diabetes Technol Ther 2011, 13, 1115–1120. [Google Scholar] [CrossRef]
- Feng, X.; Li, X.Q. The prevalence of small intestinal bacterial overgrowth in diabetes mellitus: a systematic review and meta-analysis. Aging (Albany NY) 2022, 14, 975–988. [Google Scholar] [CrossRef] [PubMed]
- Vallianou, N.G.; Stratigou, T.; Tsagarakis, S. Microbiome and diabetes: Where are we now? Diabetes Res Clin Pract 2018, 146, 111–118. [Google Scholar] [CrossRef]
- Zaborska, K.E.; Cummings, B.P. Rethinking Bile Acid Metabolism and Signaling for Type 2 Diabetes Treatment. Curr Diab Rep 2018, 18, 109. [Google Scholar] [CrossRef]
- Zhang, M.; Xu, Y.; Zhang, J.; Sun, Z.; Ban, Y.; Wang, B.; Hou, X.; Cai, Y.; Li, J.; Wang, M.; et al. Application of methane and hydrogen-based breath test in the study of gestational diabetes mellitus and intestinal microbes. Diabetes Res Clin Pract 2021, 176, 108818. [Google Scholar] [CrossRef] [PubMed]
- Yan, L.H.; Mu, B.; Pan, D.; Shi, Y.N.; Yuan, J.H.; Guan, Y.; Li, W.; Zhu, X.Y.; Guo, L. Association between small intestinal bacterial overgrowth and beta-cell function of type 2 diabetes. J Int Med Res 2020, 48, 300060520937866. [Google Scholar] [CrossRef] [PubMed]
- Kvit, K.B.; Kharchenko, N.V.; Kharchenko, V.V.; Chornenka, O.I.; Chornovus, R.I.; Dorofeeva, U.S.; Draganchuk, O.B.; Slaba, O.M. The role of small intestinal bacterial overgrowth in the pathogenesis of hyperlipidemia. Wiad Lek 2019, 72, 645–649. [Google Scholar] [CrossRef]
- John, G.K.; Mullin, G.E. The Gut Microbiome and Obesity. Curr Oncol Rep 2016, 18, 45. [Google Scholar] [CrossRef]
- Sun, L.; Ma, L.; Ma, Y.; Zhang, F.; Zhao, C.; Nie, Y. Insights into the role of gut microbiota in obesity: pathogenesis, mechanisms, and therapeutic perspectives. Protein Cell 2018, 9, 397–403. [Google Scholar] [CrossRef]
- Nawrocka, M.S., M. Bogdański, P. Rola mikroflory jelitowej w patogenezie i leczeniu otyłości oraz zespołu metabolicznego. Forum Zaburzeń Metabolicznych 2015, 6, 95–102. [Google Scholar]
- Wijarnpreecha, K.; Werlang, M.E.; Watthanasuntorn, K.; Panjawatanan, P.; Cheungpasitporn, W.; Gomez, V.; Lukens, F.J.; Ungprasert, P. Obesity and Risk of Small Intestine Bacterial Overgrowth: A Systematic Review and Meta-Analysis. Dig Dis Sci 2020, 65, 1414–1422. [Google Scholar] [CrossRef] [PubMed]
- Roland, B.C.; Lee, D.; Miller, L.S.; Vegesna, A.; Yolken, R.; Severance, E.; Prandovszky, E.; Zheng, X.E.; Mullin, G.E. Obesity increases the risk of small intestinal bacterial overgrowth (SIBO). Neurogastroenterol Motil 2018, 30. [Google Scholar] [CrossRef] [PubMed]
- Madrid, A.M.; Poniachik, J.; Quera, R.; Defilippi, C. Small intestinal clustered contractions and bacterial overgrowth: a frequent finding in obese patients. Dig Dis Sci 2011, 56, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Ierardi, E.; Losurdo, G.; Sorrentino, C.; Giorgio, F.; Rossi, G.; Marinaro, A.; Romagno, K.R.; Di Leo, A.; Principi, M. Macronutrient intakes in obese subjects with or without small intestinal bacterial overgrowth: an alimentary survey. Scand J Gastroenterol 2016, 51, 277–280. [Google Scholar] [CrossRef]
- Mushref, M.A.; Srinivasan, S. Effect of high fat-diet and obesity on gastrointestinal motility. Ann Transl Med 2013, 1, 14. [Google Scholar] [CrossRef] [PubMed]
- Xing, J.; Chen, J.D. Alterations of gastrointestinal motility in obesity. Obes Res 2004, 12, 1723–1732. [Google Scholar] [CrossRef] [PubMed]
- Ciobanu, L.; Dumitrascu, D.L. Gastrointestinal motility disorders in endocrine diseases. Pol Arch Med Wewn 2011, 121, 129–136. [Google Scholar] [CrossRef]
- Brechmann, T.; Sperlbaum, A.; Schmiegel, W. Levothyroxine therapy and impaired clearance are the strongest contributors to small intestinal bacterial overgrowth: Results of a retrospective cohort study. World J Gastroenterol 2017, 23, 842–852. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Li, X.; Ahmed, A.; Wu, D.; Liu, L.; Qiu, J.; Yan, Y.; Jin, M.; Xin, Y. Gut microbe analysis between hyperthyroid and healthy individuals. Curr Microbiol 2014, 69, 675–680. [Google Scholar] [CrossRef]
- Penhale, W.J.; Young, P.R. The influence of the normal microbial flora on the susceptibility of rats to experimental autoimmune thyroiditis. Clin Exp Immunol 1988, 72, 288–292. [Google Scholar]
- Lauritano, E.C.; Bilotta, A.L.; Gabrielli, M.; Scarpellini, E.; Lupascu, A.; Laginestra, A.; Novi, M.; Sottili, S.; Serricchio, M.; Cammarota, G.; et al. Association between hypothyroidism and small intestinal bacterial overgrowth. J Clin Endocrinol Metab 2007, 92, 4180–4184. [Google Scholar] [CrossRef] [PubMed]
- Konrad, P.; Chojnacki, J.; Kaczka, A.; Pawlowicz, M.; Rudnicki, C.; Chojnacki, C. [Thyroid dysfunction in patients with small intestinal bacterial overgrowth]. Pol Merkur Lekarski 2018, 44, 15–18. [Google Scholar] [PubMed]
- Wang, B.; Xu, Y.; Hou, X.; Li, J.; Cai, Y.; Hao, Y.; Ouyang, Q.; Wu, B.; Sun, Z.; Zhang, M.; et al. Small Intestinal Bacterial Overgrowth in Subclinical Hypothyroidism of Pregnant Women. Front Endocrinol (Lausanne) 2021, 12, 604070. [Google Scholar] [CrossRef] [PubMed]
- Rukavina Mikusic, N.L.; Kouyoumdzian, N.M.; Choi, M.R. Gut microbiota and chronic kidney disease: evidences and mechanisms that mediate a new communication in the gastrointestinal-renal axis. Pflugers Arch 2020, 472, 303–320. [Google Scholar] [CrossRef] [PubMed]
- Vaziri, N.D.; Dure-Smith, B.; Miller, R.; Mirahmadi, M.K. Pathology of gastrointestinal tract in chronic hemodialysis patients: an autopsy study of 78 cases. Am J Gastroenterol 1985, 80, 608–611. [Google Scholar] [PubMed]
- Barrios, C.; Beaumont, M.; Pallister, T.; Villar, J.; Goodrich, J.K.; Clark, A.; Pascual, J.; Ley, R.E.; Spector, T.D.; Bell, J.T.; et al. Gut-Microbiota-Metabolite Axis in Early Renal Function Decline. PLoS One 2015, 10, e0134311. [Google Scholar] [CrossRef] [PubMed]
- Strid, H.; Simren, M.; Stotzer, P.O.; Ringstrom, G.; Abrahamsson, H.; Bjornsson, E.S. Patients with chronic renal failure have abnormal small intestinal motility and a high prevalence of small intestinal bacterial overgrowth. Digestion 2003, 67, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Nallu, A.; Sharma, S.; Ramezani, A.; Muralidharan, J.; Raj, D. Gut microbiome in chronic kidney disease: challenges and opportunities. Transl Res 2017, 179, 24–37. [Google Scholar] [CrossRef]
- Satoh, M.; Hayashi, H.; Watanabe, M.; Ueda, K.; Yamato, H.; Yoshioka, T.; Motojima, M. Uremic toxins overload accelerates renal damage in a rat model of chronic renal failure. Nephron Exp Nephrol 2003, 95, e111–e118. [Google Scholar] [CrossRef]
- Thadhani, R.; Pascual, M.; Bonventre, J.V. Acute renal failure. N Engl J Med 1996, 334, 1448–1460. [Google Scholar] [CrossRef]
- Yang, J.; Kim, C.J.; Go, Y.S.; Lee, H.Y.; Kim, M.G.; Oh, S.W.; Cho, W.Y.; Im, S.H.; Jo, S.K. Intestinal microbiota control acute kidney injury severity by immune modulation. Kidney Int 2020, 98, 932–946. [Google Scholar] [CrossRef] [PubMed]
- Mahmoodpoor, F.; Rahbar Saadat, Y.; Barzegari, A.; Ardalan, M.; Zununi Vahed, S. The impact of gut microbiota on kidney function and pathogenesis. Biomed Pharmacother 2017, 93, 412–419. [Google Scholar] [CrossRef]
- Magdaleno-Tapial, J.; Lopez-Marti, C.; Garcia-Legaz-Martinez, M.; Martinez-Domenech, A.; Partarrieu-Mejias, F.; Casanova-Esquembre, A.; Lorca-Sprohnle, J.; Labrandero-Hoyos, C.; Penuelas-Leal, R.; Sierra-Talamantes, C.; et al. Contact Allergy in Patients with Rosacea. Actas Dermosifiliogr 2022, 113, 550–554. [Google Scholar] [CrossRef]
- Daou, H.; Paradiso, M.; Hennessy, K.; Seminario-Vidal, L. Rosacea and the Microbiome: A Systematic Review. Dermatol Ther (Heidelb) 2021, 11, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.Y.; Chi, C.C. Rosacea, Germs, and Bowels: A Review on Gastrointestinal Comorbidities and Gut-Skin Axis of Rosacea. Adv Ther 2021, 38, 1415–1424. [Google Scholar] [CrossRef]
- Parodi, A.; Paolino, S.; Greco, A.; Drago, F.; Mansi, C.; Rebora, A.; Parodi, A.; Savarino, V. Small intestinal bacterial overgrowth in rosacea: clinical effectiveness of its eradication. Clin Gastroenterol Hepatol 2008, 6, 759–764. [Google Scholar] [CrossRef] [PubMed]
- Branisteanu, D.E.; Cojocaru, C.; Diaconu, R.; Porumb, E.A.; Alexa, A.I.; Nicolescu, A.C.; Brihan, I.; Bogdanici, C.M.; Branisteanu, G.; Dimitriu, A.; et al. Update on the etiopathogenesis of psoriasis (Review). Exp Ther Med 2022, 23, 201. [Google Scholar] [CrossRef]
- Drago, F.; Ciccarese, G.; Cordara, V.; Paudice, M.; Herzum, A.; Parodi, A. Oral psoriasis and SIBO: is there a link? J Eur Acad Dermatol Venereol 2018, 32, e368–e369. [Google Scholar] [CrossRef] [PubMed]
- Drago, F.; Ciccarese, G.; Indemini, E.; Savarino, V.; Parodi, A. Psoriasis and small intestine bacterial overgrowth. Int J Dermatol 2018, 57, 112–113. [Google Scholar] [CrossRef]
- Lombardi, N.; Moneghini, L.; Varoni, E.M.; Lodi, G. Nodular migratory tongue lesions: Atypical geographic tongue or a new entity? Oral Dis 2023, 29, 1791–1794. [Google Scholar] [CrossRef]
- Scheltens, P.; De Strooper, B.; Kivipelto, M.; Holstege, H.; Chetelat, G.; Teunissen, C.E.; Cummings, J.; van der Flier, W.M. Alzheimer's disease. Lancet 2021, 397, 1577–1590. [Google Scholar] [CrossRef] [PubMed]
- Santiago, J.A.; Potashkin, J.A. The Impact of Disease Comorbidities in Alzheimer's Disease. Front Aging Neurosci 2021, 13, 631770. [Google Scholar] [CrossRef] [PubMed]
- Sim, J.; Wang, Y.T.; Mamun, K.; Tay, S.Y.; Doshi, K.; Hameed, S.; Ting, S.K. Assessment of small intestinal bacterial overgrowth in Alzheimer's disease. Acta Neurol Taiwan 2021, 30(3), 102–107. [Google Scholar]
- Kowalski, K.; Mulak, A. Small intestinal bacterial overgrowth in Alzheimer's disease. J Neural Transm (Vienna) 2022, 129, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Feng, X.; Jiang, Z.; Jiang, Z. Association of small intestinal bacterial overgrowth with Parkinson's disease: a systematic review and meta-analysis. Gut Pathog 2021, 13, 25. [Google Scholar] [CrossRef]
- Niu, X.L.; Liu, L.; Song, Z.X.; Li, Q.; Wang, Z.H.; Zhang, J.L.; Li, H.H. Prevalence of small intestinal bacterial overgrowth in Chinese patients with Parkinson's disease. J Neural Transm (Vienna) 2016, 123, 1381–1386. [Google Scholar] [CrossRef] [PubMed]
- Fasano, A.; Bove, F.; Gabrielli, M.; Petracca, M.; Zocco, M.A.; Ragazzoni, E.; Barbaro, F.; Piano, C.; Fortuna, S.; Tortora, A.; et al. The role of small intestinal bacterial overgrowth in Parkinson's disease. Mov Disord 2013, 28, 1241–1249. [Google Scholar] [CrossRef] [PubMed]
- Tan, A.H.; Mahadeva, S.; Thalha, A.M.; Gibson, P.R.; Kiew, C.K.; Yeat, C.M.; Ng, S.W.; Ang, S.P.; Chow, S.K.; Tan, C.T.; et al. Small intestinal bacterial overgrowth in Parkinson's disease. Parkinsonism Relat Disord 2014, 20, 535–540. [Google Scholar] [CrossRef] [PubMed]
- van Kessel, S.P.; El Aidy, S. Contributions of Gut Bacteria and Diet to Drug Pharmacokinetics in the Treatment of Parkinson's Disease. Front Neurol 2019, 10, 1087. [Google Scholar] [CrossRef]
- Danau, A.; Dumitrescu, L.; Lefter, A.; Tulba, D.; Popescu, B.O. Small Intestinal Bacterial Overgrowth as Potential Therapeutic Target in Parkinson's Disease. Int J Mol Sci 2021, 22. [Google Scholar] [CrossRef]
- Zhang, Y.; Liu, G.; Duan, Y.; Han, X.; Dong, H.; Geng, J. Prevalence of Small Intestinal Bacterial Overgrowth in Multiple Sclerosis: a Case-Control Study from China. J Neuroimmunol 2016, 301, 83–87. [Google Scholar] [CrossRef]
- Geier, D.A.; Kern, J.K.; Geier, M.R. A Comparison of the Autism Treatment Evaluation Checklist (ATEC) and the Childhood Autism Rating Scale (CARS) for the Quantitative Evaluation of Autism. J Ment Health Res Intellect Disabil 2013, 6, 255–267. [Google Scholar] [CrossRef] [PubMed]
- Finegold, S.M.; Summanen, P.H.; Downes, J.; Corbett, K.; Komoriya, T. Detection of Clostridium perfringens toxin genes in the gut microbiota of autistic children. Anaerobe 2017, 45, 133–137. [Google Scholar] [CrossRef]
- Finegold, S.M.; Dowd, S.E.; Gontcharova, V.; Liu, C.; Henley, K.E.; Wolcott, R.D.; Youn, E.; Summanen, P.H.; Granpeesheh, D.; Dixon, D.; et al. Pyrosequencing study of fecal microflora of autistic and control children. Anaerobe 2010, 16, 444–453. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Yu, Y.M.; Zhang, Y.Q.; Zhang, J.; Lu, N.; Liu, N. Hydrogen breath test to detect small intestinal bacterial overgrowth: a prevalence case-control study in autism. Eur Child Adolesc Psychiatry 2018, 27, 233–240. [Google Scholar] [CrossRef]
- Wei, F.; Zhou, L.; Wang, Q.; Zheng, G.; Su, S. Effect of Compound Lactic Acid Bacteria Capsules on the Small Intestinal Bacterial Overgrowth in Patients with Depression and Diabetes: A Blinded Randomized Controlled Clinical Trial. Dis Markers 2022, 2022, 6721695. [Google Scholar] [CrossRef]
- Kossewska, J.; Bierlit, K.; Trajkovski, V. Personality, Anxiety, and Stress in Patients with Small Intestine Bacterial Overgrowth Syndrome. The Polish Preliminary Study. Int J Environ Res Public Health 2022, 20. [Google Scholar] [CrossRef] [PubMed]
- Chojnacki, C.; Konrad, P.; Blonska, A.; Medrek-Socha, M.; Przybylowska-Sygut, K.; Chojnacki, J.; Poplawski, T. Altered Tryptophan Metabolism on the Kynurenine Pathway in Depressive Patients with Small Intestinal Bacterial Overgrowth. Nutrients 2022, 14. [Google Scholar] [CrossRef]
- Chojnacki, C.; Poplawski, T.; Konrad, P.; Fila, M.; Blasiak, J.; Chojnacki, J. Antimicrobial treatment improves tryptophan metabolism and mood of patients with small intestinal bacterial overgrowth. Nutr Metab (Lond) 2022, 19, 66. [Google Scholar] [CrossRef]
- Lisowska, A.; Wojtowicz, J.; Walkowiak, J. Small intestine bacterial overgrowth is frequent in cystic fibrosis: combined hydrogen and methane measurements are required for its detection. Acta Biochim Pol 2009, 56, 631–634. [Google Scholar] [CrossRef]
- De Lisle, R.C. Altered transit and bacterial overgrowth in the cystic fibrosis mouse small intestine. Am J Physiol Gastrointest Liver Physiol 2007, 293, G104–G111. [Google Scholar] [CrossRef] [PubMed]
- Furnari, M.; De Alessandri, A.; Cresta, F.; Haupt, M.; Bassi, M.; Calvi, A.; Haupt, R.; Bodini, G.; Ahmed, I.; Bagnasco, F.; et al. The role of small intestinal bacterial overgrowth in cystic fibrosis: a randomized case-controlled clinical trial with rifaximin. J Gastroenterol 2019, 54, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Verrecchia, E.; Sicignano, L.L.; La Regina, M.; Nucera, G.; Patisso, I.; Cerrito, L.; Montalto, M.; Gasbarrini, A.; Manna, R. Small Intestinal Bacterial Overgrowth Affects the Responsiveness to Colchicine in Familial Mediterranean Fever. Mediators Inflamm 2017, 2017, 7461426. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Wang, H.; Zhang, P.; Xu, L.; Tian, Z. Association between small intestinal bacterial overgrowth and toll-like receptor 4 in patients with pancreatic carcinoma and cholangiocarcinoma. Turk J Gastroenterol 2019, 30, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Liang, S.; Xu, L.; Zhang, D.; Wu, Z. Effect of probiotics on small intestinal bacterial overgrowth in patients with gastric and colorectal cancer. Turk J Gastroenterol 2016, 27, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Deng, L.; Liu, Y.; Zhang, D.; Li, Y.; Xu, L. Prevalence and treatment of small intestinal bacterial overgrowth in postoperative patients with colorectal cancer. Mol Clin Oncol 2016, 4, 883–887. [Google Scholar] [CrossRef] [PubMed]
- Savva, K.V.; Hage, L.; Belluomo, I.; Gummet, P.; Boshier, P.R.; Peters, C.J. Assessment of the Burden of Small Intestinal Bacterial Overgrowth (SIBO) in Patients After Oesophagogastric (OG) Cancer Resection. J Gastrointest Surg 2022, 26, 924–926. [Google Scholar] [CrossRef]
- Zhou, D.X.; Ma, Y.J.; Chen, G.Y.; Gao, X.; Yang, L. [Relationship of TLR2 and TLR4 expressions on the surface of peripheral blood mononuclear cells to small intestinal bacteria overgrowth in patients with hepatocellular carcinoma]. Zhonghua Gan Zang Bing Za Zhi 2019, 27, 286–290. [Google Scholar] [CrossRef]
Figure 1.
Mucosa-associated bacterial microbiota of multiple gut segments in people with SIBO (SIBO+) and healthy people (SIBO‒) [made on the basis of [17].
Figure 1.
Mucosa-associated bacterial microbiota of multiple gut segments in people with SIBO (SIBO+) and healthy people (SIBO‒) [made on the basis of [17].
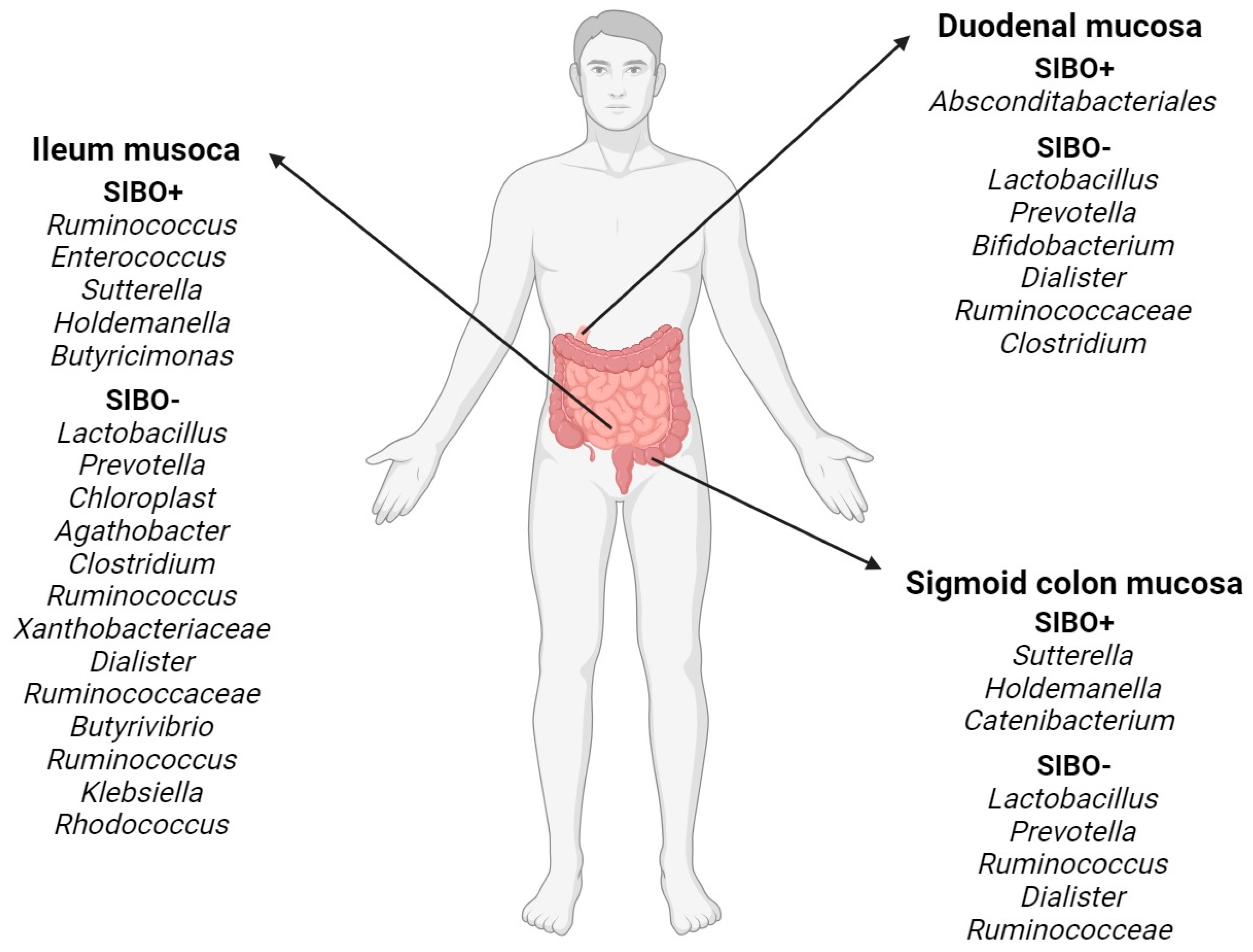
Figure 2.
SIBO treatment methods.
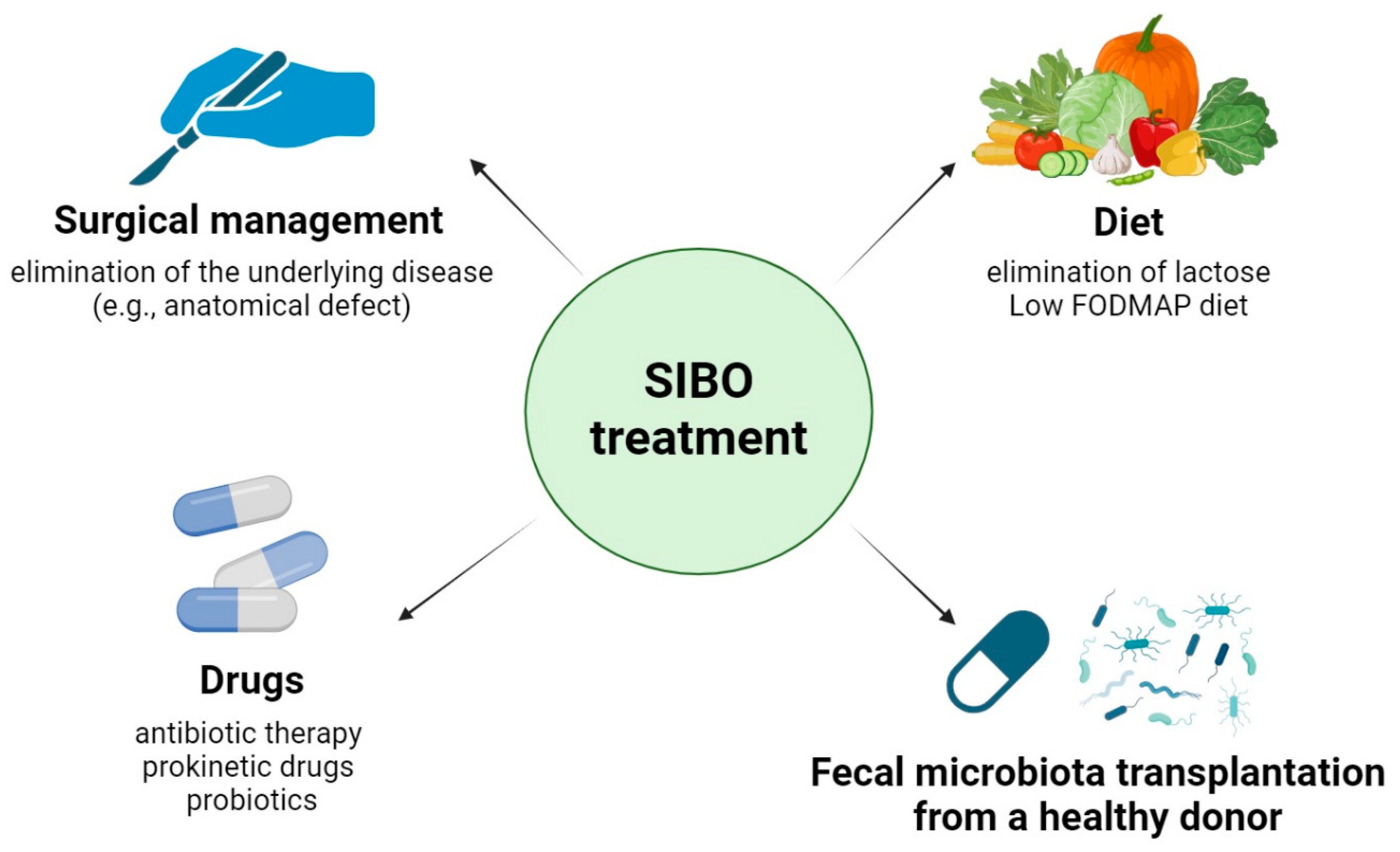
Figure 3.
SIBO and twelve groups of diseases related.
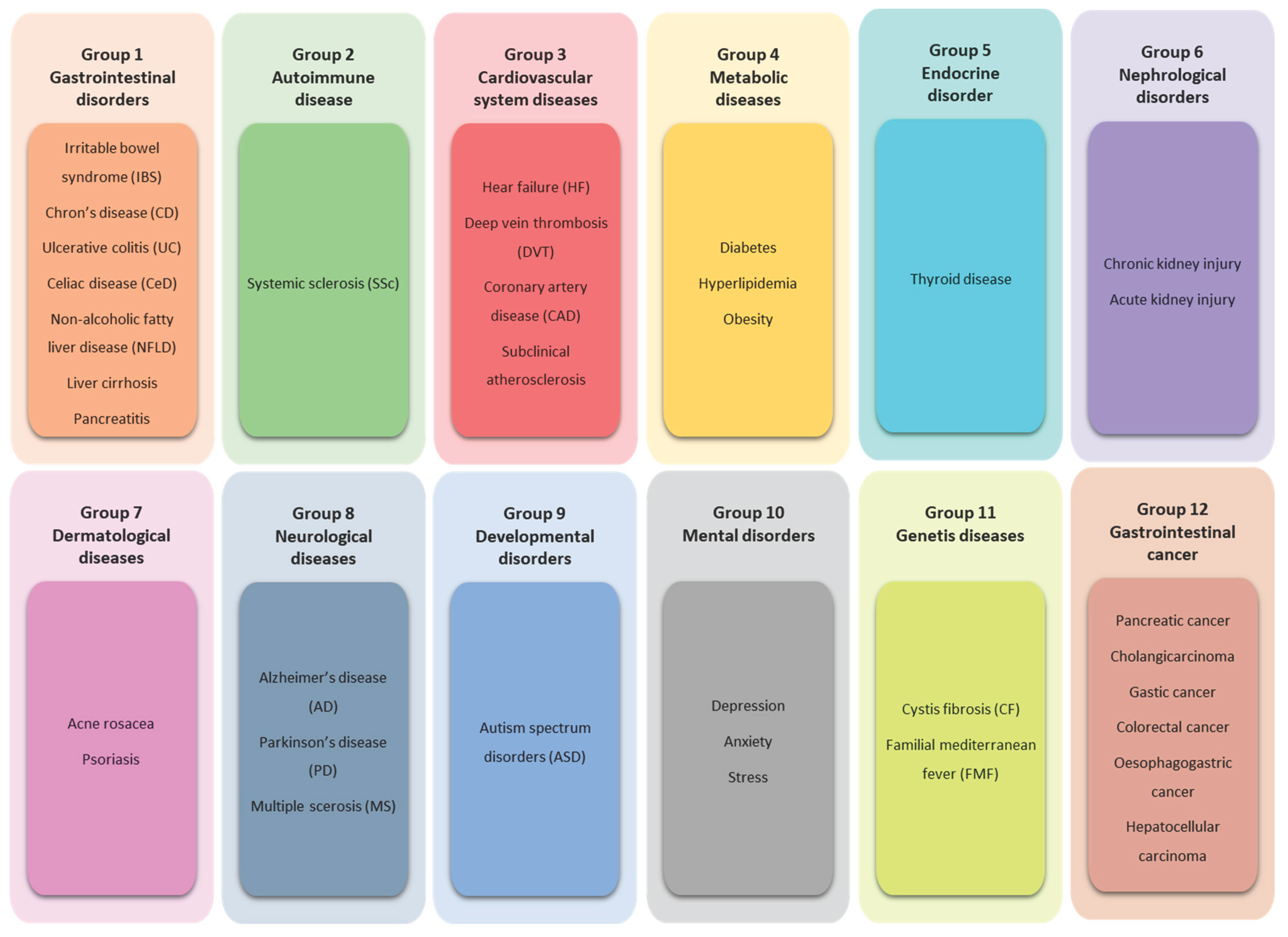
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



