Submitted:
20 March 2024
Posted:
22 March 2024
You are already at the latest version
Abstract
Tinea incognito is a kind of skin infection that is caused by a fungus which has been changed by the use of topical or systemic steroids or other immunosuppressive medications. This alteration in the typical clinical presentation of the infection makes it difficult to diagnose for general practitioners and dermatologists. Delayed diagnosis, spread of the infection to critical body surfaces, resistance to antifungal drugs, and increased costs due to prolonged hospitalization and multiple treatment regimens often complicate tinea incognito. This condition can affect individuals of all ages and genders, but it is more common in children. Tinea incognito is a type of fungal skin infection that can present with various and non-specific clinical features, such as sudden onset of itching in an area that was previously unaffected, making it challenging to differentiate from other diseases such as eczema, seborrheic dermatitis, lupus erythematosus, psoriasis, or other non-fungal skin conditions. The treatment of tinea incognito usually involves stopping the use of topical steroids or other immunosuppressive medications. Preventive measures and management of the underlying fungal infection are necessary and can be achieved with antifungal drugs. Patients should wear loose cotton clothes, use boiling water for laundry, and iron their clothing before wearing them. Additionally, they should avoid sharing bed linens, towels, clothes, and shoes. This review aims to raise awareness of tinea incognito among health practitioners, provide tips for suspecting the disorder, include it in the differentials, and evaluate the available diagnostic procedures. The therapy utilized in published studies is also reviewed.
Keywords:
tinea incognito
; fungal infection
; dermatophyte infection
; corticosteroid
; tacrolimus
; pimecrolimus
1. Introduction
Tinea incognito (TI) is a type of fungal infection caused by dermatophytes, which can be treated with a topical immunosuppressive agent or systemic steroids. The primary cause of TI is the use of a topical corticosteroid, which is prescribed by a medical professional for a pre-existing disorder or suggested for the treatment of a missed mycoses diagnosis. [1,2]. Topical calcineurin inhibitors like tacrolimus ointment and pimecrolimus cream have also been known to cause TI due to their immunomodulating properties in the area of application. This type of fungal infection can slowly extend and mimic other cutaneous disorders, leading to a misdiagnosis and delayed or unsuccessful treatment. TI is also known as steroid-modified tinea, which has become an increasingly concerning pandemic. The term "incognita" refers to the masking of the clinical signs of a fungal infection [3].
Tinea Incognito (TI) was first reported in 1968 by two UK dermatologists, Dr. Adrian Ive and Dr. Ronnie Marks. They observed a group of patients with unusual skin lesions, resembling seborrheic dermatitis, eczema, lichen ruber planus, scleroderma, folliculitis, rosacea, and psoriasis, that responded to usual treatments. One-third of the cases presented with typical ringworm characteristics. Upon further examination, they diagnosed an underlying fungal infection that was masked by the use of topical steroids or other immunosuppressive medications, justifying the term "tinea incognita." Subsequent publications also employed the term "tinea incognita." [1]. Clinical variations in dermatophytosis can be attributed to the fungi's invasive capacity, infection location, and humidity. The term "tinea atypica" is suggested for dermatophytosis without typical clinical features. [4]
2. Epidemiology
The epidemiology of TI, which represents approximately 40% of dermatophytoses, is not well-established due to underreporting and misdiagnosis, despite being common and having a global distribution. [1,5,6,7] TI was first described in 1968 and there have been more cases reported in recent years. [1,8] It is more prevalent in tropical and subtropical regions due to favorable conditions for fungal growth, such as high humidity and temperature. [9,10] TI is a condition that can affect individuals of all ages and genders, ranging from 2 to 81 years old. However, it is more commonly found in children, as evidenced by a retrospective review of cases [11]. Another study of 818 cases of TI diagnosed in children at a referral hospital between 1977 and 2006, also supports the higher pediatric incidence. Additionally, young adults are also commonly susceptible to dermatophytosis. [12,13] Based on previous reports, it was found that males had a higher infection rate of dermatophytic fungi. [14] Immunocompromised patients and those with diabetes mellitus (DM) are at a higher risk of developing TI, especially tinea pedis and onychomycosis [10,14,15,16].
As topical corticosteroids are used to treat an increasing number of dermatologic diseases, the prevalence of TI has also risen. [6,9,17]. Topical calcineurin inhibitors may be less of a risk factor for TI due to their limited use caused by high cost. [9] Tinea infections are caused by a type of fungi that thrive in warm and moist environments. Various factors such as sweating, abrasion, and maceration can contribute to the development of this disorder. Certain populations, such as people living in crowded or unsanitary conditions or those who participate in activities involving prolonged contact with water, like swimming or water sports, may have a higher prevalence of tinea infections. [18,19,20,21].
Initially reported, T. rubrum and E. floccosum were the most commonly isolated dermatophytes. [1]. T. rubrum is the most commonly isolated dermatophyte in ΤΙ, followed by T. mentagrophytes, E. floccosum, M. canis, M. gypseum, T. violaceum, T. tonsuran, T. verrucosum, T. schonleini and T. erinacei [21,22,23,24,25,26,27,28,29,30,31]. It is worth noting that T. rubrum and T. interdigitale are the most common fungi causing dermatophytosis in some areas. [4,32]. Currently, the prevalent strain in India is T. interdigitale. [33]. A few studies found T. mentagrophytes (44.4%) and T. verrucosum (33%) to be also frequently isolated species [31,34]. Trichophyton species are usually the most isolated fungi in studies, except for one where M. canis was the most common. [4].
The exact prevalence of TI among immunocompromised patients, particularly those with HIV, is not currently known. It may even be underestimated, especially in developed countries where antiretroviral treatment is initiated early and antifungal medication is prescribed more frequently for other mycotic disorders. [35] M. gypseum is a type of fungus that has been found in HIV patients, particularly in areas with limited resources. [36,37,38,39]. Exposure to humid soil and dust may also increase the likelihood of developing a M. gypseum infection. [40].
3. Pathogenesis
The development of TI results from the interaction of fungal infection, corticosteroid use, misdiagnosis and/or inappropriate treatment, as well as individual and environmental factors that affect the sensitivity and severity of the infection. (Table 1). The risk factors that increase the likelihood of developing dermatophytosis include a weakened immune system and damaged skin. [41,42]. The diminished nutrient availability with concomitant reduced oxygenation, and antimicrobial peptides dysfunction (AMP) at the infection site might also contribute to the risk factors for the initial infection.
TI and uncomplicated tinea infections are typically caused by the same pathogens, such as dermatophytes T. rubrum, T. mentagrophytes, and E. floccosum. [47]. The pathogenesis of TI is distinct from traditional tinea infections because it is altered by the use of topical steroid creams, systemic corticosteroids, or other immunosuppressive medications. [48]. These medications, particularly when used frequently or in high doses, can weaken the normal immune responses of the skin and reduce the inflammation that fights against fungal infections. This can result in a lowered resistance of the skin at the site of application, which may contribute to the growth and spread of fungal infections. (Table 2) [4,5,14]. Furthermore, dermatophytes metabolize keratin, leading to an inflammatory response. A lack of keratin limits the spread of the fungal infection. Immunosuppressants prevent the inflammatory response, allowing the fungus to thrive. [4,14]. Topical steroids can create a warm and moist environment on the skin, which may lead to the growth of fungi. [1,26]. They can also mask the symptoms of a fungal infection, such as redness, itching, and scaling, making the infection appear less severe. [9]. If left undiagnosed or misdiagnosed as another skin condition, a fungal infection may not be treated in a timely manner. This can cause the fungus to spread and result in a more severe and recurrent infection that is harder to treat. In such cases, oral antifungal medications may be required for a more aggressive treatment approach. [25].
4. Clinical Features
A typical scenario begins with a misdiagnosis of TI as eczema, (Figure 1), leading to the use of topical steroids that reduce inflammation and make the condition less irritable. [5,9,46]. The more topical steroids are applied, the more extensive and unrecognizable the fungal infection becomes. Furthermore, long-term use of topical steroids can cause skin atrophy, which complicates the diagnosis of TI. [9]. Thinning of the skin caused by atrophy may resemble the chronic phase of other skin conditions that are treated with steroids for a prolonged period, such as eczema, seborrheic dermatitis, lupus erythematosus, psoriasis, or other non-fungal skin conditions. [23,30,45]. As topical steroid application continues, it becomes increasingly challenging to differentiate between these conditions and Tinea Incognito (TI). Delayed treatment may allow the fungi to spread and invade deeper layers of the skin, nails, or hair, resulting in more severe and resistant infections.
A variation of the typical scenario involves the use of a combination of topical steroid and antifungal cream. In the case of open skin areas, the combination cream could provide an adequate response for treating the fungal infection. However, in areas of occlusion, such as the buttocks, groin, and armpit, the impaired immunity caused by the topical steroid might be sufficient to cause TI, despite the application of a topical antifungal.
TI is a type of fungal skin infection that can present with various and non-specific clinical features, such as a sudden onset of pruritus in a previously unaffected area. The symptoms depend on the type of the underlying fungus and the location of the infected body site. Lesions might appear larger, diffuse, poorly defined, less red and scaly, and more pinkish or flesh-colored. [21,23,31] Table 3 provides a summary of various clinical conditions that need to be distinguished from TI. (Figure 2 and Figure 3).
A typical dermatophytosis usually begins as a red circular plaque with a slightly raised scaly border. As the plaque expands, it takes a ring shape with scales at the periphery. [8,15]. In time, multiple itchy lesions can develop and coalesce into patches. These patches may exhibit a poorly defined border, florid growth, and loss of characteristic features due to inflammation suppression. [26].
TI often results in a red, scaly rash that can be itchy, uncomfortable or painful. The rash may appear in patches or spread over a larger area on any part of the body, but it is usually seen in areas where skin folds, such as the groin, the axillae and the inframammary region. Unlike an untreated fungal infection, TI's margin is less elevated, less scaly, and more commonly pustular, and the typical "ring-like" shape may be absent. Next to the initial plaque, secondary lesions may emerge. Sometimes, a secondary bacterial infection may occur, showing concurrent pustules and impetigo. In some cases, the rash may also be accompanied by blisters or pustules that are filled with fluid and can break, open and ooze. [8,15]. The affected skin may appear lighter or darker than the surrounding skin due to erythematous or hyperpigmented lesions. [25]. In chronic infections, the skin may thicken or develop a leathery texture. It can also cause hair loss due to persistent dermatophytic infection and possible invasion of deeper tissues and hair follicles [52].
A useful clinical tip to differentiate between bacterial infections and TI complicated by a secondary bacterial infection is that in the latter case, hairs can be pulled out of the follicle without the patient feeling any pain.
In several tinea infection cases, the borders of the scaly plaques might not be well-established, and new satellite lesions might appear beyond the blurred border of the initial lesion, due to suppression of the inflammatory reaction at the periphery. More often, especially in the initial stages of the disease, the central remission of the lesion and the presence of a faintly marked ellipsoidal or semi-annular border peripherally is observed. This should raise the suspicion of underlying dermatophytes.
Tinea infections might also develop inflammatory nodules. [26] Concentric circles sometimes appear during fungal infections, which can indicate repeated episodes of fungal expansion. Alongside clinical variations caused by topical agents, systemic immunosuppression can make the condition worse, leading to deep subcutaneous abscesses. This can cause the formation of a secondary granuloma, which is known as "Majocchi's granuloma". Majocchi granuloma is a skin infection caused by fungi that typically affect hair follicles. The most common causative agents are Trichophyton rubrum and Microsporum canis. The infection occurs when the fungi spread into the surrounding tissues after an injury to a hair follicle. This condition is rare. It results in the formation of nodular granulomatous perifolliculitis, which is characterized by an intense inflammatory response. Clinically, lesions appear as granulomata, cellulitis, or plaques. They are often seen on the anterior aspect of the legs, but inguinal, scrotal, vulval, and facial involvement has also been reported. In some cases, patients may have an underlying immunodeficiency state, particularly due to corticosteroid therapy, which mainly affects delayed hypersensitivity reactions. Disseminated skin lesions may rarely occur in immunosuppressed individuals [50,51].
In some cases, the fungal infection can persist for months or years, become systemic, and even lead to onychomycosis. Lesions on the hands may progress towards the nails, causing nail dystrophy and the chronic form of TI [52]. In cases of extensive dermatophyte infection, the patient's sexual partners should also be checked for the infection. Although extremely rare, an id-reaction may occur in TI.
5. Diagnosis
Diagnosing tinea incognito (TI) can be quite challenging due to the atypical appearance of the lesions. Physical examination of the affected skin is usually necessary to detect signs of a fungal infection, such as scaling and redness.
Dermoscopy, a non-invasive technique might assist in the diagnosis of TI. The most commonly observed dermoscopic findings in TI cases include dotted vessels, superficial white scales with peripheral distribution, and the presence of a ‘moth-eaten’ scale with an outward-peeling direction, which appears to be the most specific feature [53]. Tinea capitis is a fungal infection which can be diagnosed through trichoscopy. The most common trichoscopic findings include comma hairs, corkscrew hairs, zigzag hairs, and Morse code hairs. In addition, black dots and broken hairs are frequently seen. Successful treatment of tinea capitis is characterized by a reduction in short broken hairs, corkscrew and zigzag hairs, and later, comma hairs and black dots [54]. Distal lateral subungual onychomycosis can be identified through specific features such as a jagged proximal edge with spikes of the onycholytic area, longitudinal streaks, and subungual hyperkeratosis. [55].
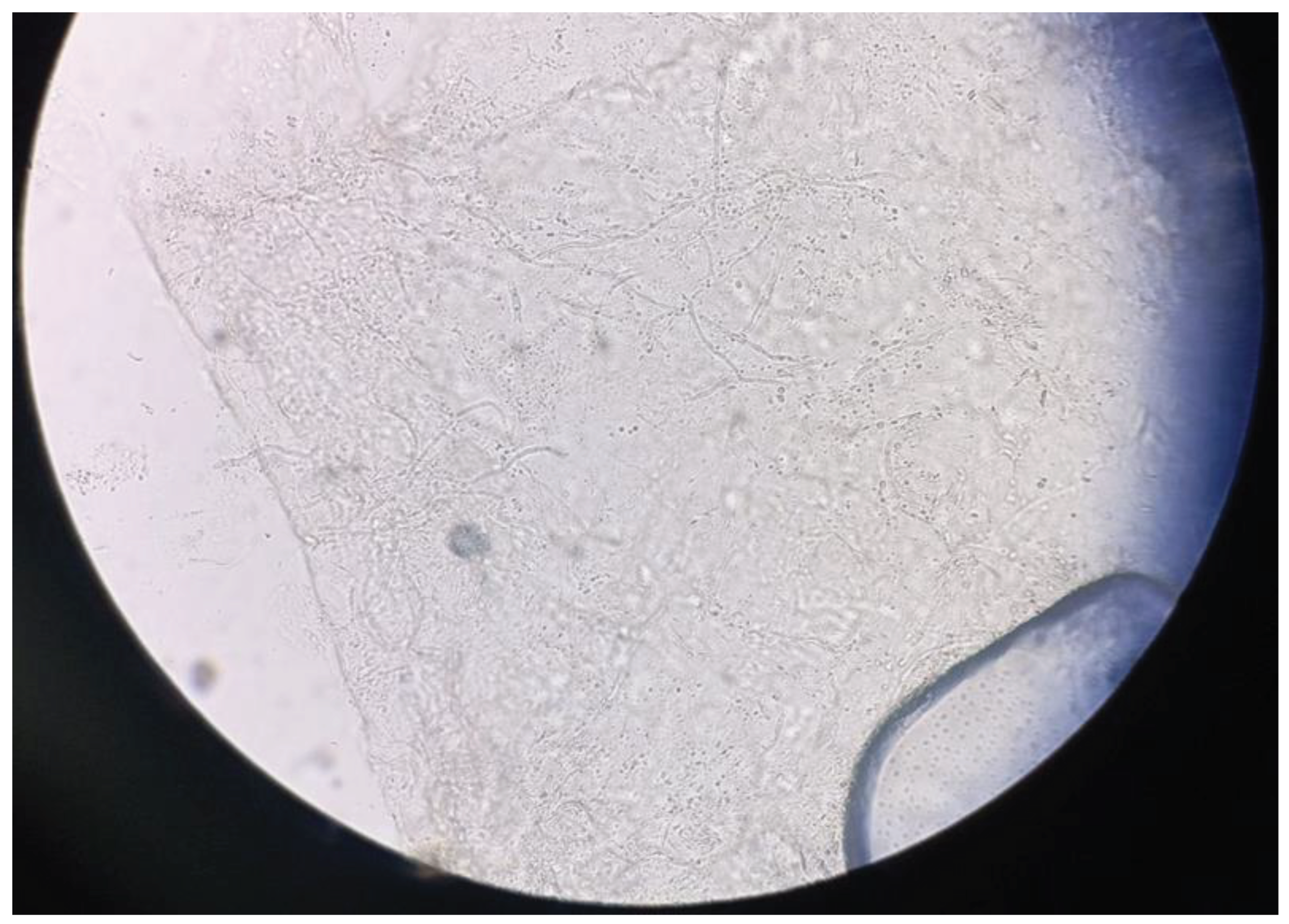
Confirmation of TI diagnosis requires mycological examination after discontinuing topical steroids. To prevent bacterial growth, skin scales should be collected from the periphery of the plaque and kept dry. [56,57,58] Direct microscopic examination is a quick, simple, and affordable method for screening superficial mycosis. A 10%-40% potassium hydroxide solution (KOH-10% for skin scrapings and 40% for nail clippings) is applied. Positive scrapings are indicated by the presence of hyphal filaments, with or without arthroconidiospores. Hyphae can be seen between epithelial cells. [54,55] The accuracy of the diagnosis depends on the quality of the sample and the skill of the physician [56]. Adding either 36% dimethyl sulfoxide (DMSO) or Chicago Sky Blue stain to the KOH solution will stain the fungal hyphae blue against a pink background, providing better visualization of the fungal elements [59]. Fluorescent staining using diaminostilbene is the most sensitive microscopic method for specimen visualization. [60]. Fluorescent microscopy combined with Calcofluor or Blankophor improves identification speed, ease, and safety [61]. During fluorescent microscopy, fungal filaments and spores appear as blue-white when exposed to ultraviolet light. Chorazol black E staining increases specificity to about 98% [62].
Figure 4.
KOH preparation of fungal elements.
Fungal culture is the most reliable method to diagnose TI, but it may not always be accessible. [57] Utilization is important, especially in stubborn or severe cases. [63]. To identify the fungus responsible for an infection, experts rely on the appearance of the colonies.
In cases where a person is suspected to have tinea, a skin or nail biopsy may be necessary to confirm the diagnosis. The biopsy will be examined under a microscope using stains such as periodic acid-Schiff (PAS) or Gomori - Grocott methenamine silver, which will highlight any fungal elements present. Although the biopsy appearance may vary, certain elements support the diagnosis of tinea. The histopathology of tinea incognito is similar to other fungal infections, with visible fungal hyphae between cornified cells in the stratum corneum (also known as the 'sandwich sign'), compact orthokeratosis, and neutrophils in the stratum corneum. [64,65].
Polymerase chain reaction (PCR) and nucleic acid sequence-based amplification are two of the more recent diagnostic tools [45]. Uniplex PCR can detect and identify fungi with overlapping characteristics of culture, sensitivity, and specificity [66]. Multiplex PCR can detect 21 dermatomycotic pathogens with DNA using agarose gel electrophoresis. Other techniques include gene-specific PCR, sequencing of rRNA gene, chitin synthase encoding gene, PCR fingerprinting, and DNA hybridization.. [66]
The matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF-MS) is a diagnostic technique that detects proteolytic degradation products resulting from fungal activity [56]. Reflectance confocal microscopy is another method used for diagnosing tinea. It offers in-vivo imaging of the epidermis and superficial dermis at the cellular level to detect fungal infections. [67,68]
6. Treatment
The treatment of TI typically involves stopping the use of topical steroids or other immunosuppressive medications. Preventive measures and management of the underlying fungal infection are necessary and can be achieved with antifungal medications. Patients should wear loose cotton clothes, use boiling water for laundry, and iron their clothing before wearing them. Additionally, they should avoid sharing bed linens, towels, clothes, and shoes. Obese patients or those with hyperhidrosis should be encouraged to lose weight and apply topical aluminium salts or anticholinergics to reduce sweating.
The ideal pharmacological treatment should be highly effective and provide long-term prophylaxis against relapses. It should also have potent anti-inflammatory action, minimal adverse events, low cost, and be safe to use in pregnancy and lactation, renal and hepatic failure. Treatment modalities include oral or topical antifungals or a combination of both, depending on the severity and extent of infection, as well as the type of the culprit fungi. [3] Combinations of various antifungal groups should be used to prevent resistance from emerging.
Topical antifungal medications are typically the first line of treatment for mild cases of tinea infections and for localized and primary dermatophytic infections. (Table 5). Antifungal creams, gels, or lotions, which contain agents like terbinafine, clotrimazole, miconazole, or econazole, can be used to treat fungal infections. The medication is applied to the affected area(s) twice daily for several weeks until the infection disappears. Treatment typically lasts for several weeks. Additionally, bland antipruritic lotions can also be applied. [44].
In cases where the infection is severe or widespread, or involves hair-bearing areas, oral antifungal medications may be prescribed. (Table 6). Terbinafine, itraconazole, and fluconazole are medications that have been shown to be more effective than griseofulvin. Treatment duration varies depending on infection severity and patient response, but usually lasts for several weeks to several months. [44].
Systemic antifungal agents can have adverse effects. Itraconazole may lead to elevated liver enzymes and gastrointestinal issues. [29] Terbinafine has been linked to a condition called neutropenia or agranulocytosis, which is a reduction in the number of white blood cells. [28]. Laboratory evaluation should be considered before starting treatment, and monitoring should be performed regularly. It is important to review the patient's medical history because systemic antifungals can interact with other medications prescribed for concomitant disorders.
The emergence of resistance to antifungal drugs is becoming a problem [69]. Information on dermatophyte resistance is limited compared to systemic infections. [69,70,71,72]. There is a need for novel therapeutic agents that can target the mechanisms by which fungi limit the immune response and promote the re-establishment of cell-mediated immunity. [49].
7. Recurrence
Patients may purchase combination formulations (steroids with antifungal and antibacterial agents) or over-the-counter medications to prevent recurrence [9,21]. Literature suggests that most TI patients self-treat or rely on advice from friends and family for treatment [21,31]. Using these modalities can actually increase the risk of a recurrence instead of providing preventative measures.
Physicians should emphasize the importance of completing the prescribed treatment in order to completely eradicate the infection, even if the symptoms improve earlier. Additionally, patients should visit their healthcare provider to ensure that the treatment was effective and to prevent the possibility of relapse. It has been reported that patients with impaired epidermal barrier functionality, such as those with atopic dermatitis or those with immunosuppression due to malignancies like leukemia or lymphoma or due to the use of immunosuppressive agents for autoimmune disorders such as lupus erythematosus or rheumatoid arthritis, are at higher risk of recurrent infections. [73,74,75].
8. Financial Considerations
It has been observed that TI leads to an increase in the number of consultations and laboratory investigations. It's possible that treatment for dermatophytosis may take longer and require more expensive antifungal medication. In India, a recent analysis of treatment costs showed that patients who use topical steroids spend 40% more on treatment than those who don't use steroids. This was true for both patients who had never used steroids before and those who had used them in the past [3]. The epidemiology of dermatophytosis in India indicates that the high temperatures and humidity prevalent in the region promote the acquisition and perpetuation of fungal infections. Therefore, these results may not be applicable to other regions with different climatic conditions. However, the additional costs associated with the treatment of these infections should raise concerns regarding the increased morbidity and economic burden in all geographical settings.
9. Conclusion
The clinical presentation of Tinea Incognito (TI) can be unusual and highly variable. The lesions may not appear as expected for a typical fungal infection, making it difficult to diagnose and treat. Furthermore, the use of topical steroids or other immunosuppressive medications may make the affected skin thinner and more fragile, increasing the risk of injury or secondary bacterial infections. Misdiagnosis of TI can result in delays in treating the underlying fungal infection correctly. Therefore, diagnosing TI requires a high index of suspicion, and additional tests such as skin scrapings, cultures or other diagnostic tests may be necessary to confirm the presence of a fungal infection. Early and accurate diagnosis is crucial to prevent the spread of infection and ensure that appropriate antifungal treatment is administered.
Author Contributions
Conception of the work: A.Z., S.G.; Design of the work: A.Z., S.G.; Acquisition, analysis and interpretation of data: A.Z., S.G.; Draft preparation and substantial revision of manuscript: A.Z., A.T., D.K., A.L, A.T., S.G., All authors have approved the submitted version.
Funding
The authors declare no funding.
Ethics statement
Ethical review and approval were waived for this study, since data were retrieved from published literature.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data that support the findings of this study are openly available in MEDLINE electronic database.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ive FA, Marks R. Tinea incognito. Br Med J 1968, 3, (149-152.
- Simmons I. Tinea Incognito. In Diagnosis and Treatment of Cutaneous Fungal Infections for General Practitioners. Sandoz Satellite Symposium of the 12th Congress International Society for Human and Animal Mycology, SARMEA , 1994.
- Jagadeesan S, Sreekumar S, Sajini L, Binu A, Das A, The economic burden of topical corticosteroid use in dermatophytosis: A cost of illness analysis of steroid-modified vs steroid-naïve dermatophytosis. Clin Exp Dermatol 2023, IIad135. [CrossRef]
- Atzori L, Pau M, Aste N, Aste N. Dermatophyte infections mimicking other skin diseases: A 154-person case survey of tinea atypica in the district of Cagliari (Italy). Int J Dermatol 2012, 51, 410-5.
- Siddaiah N, Erickson Q, Miller G, Elston DM. Tacrolimus-induced tinea incognito. Cutis 2004, 73, 237-8.
- Crawford KM, Bostrom P, Russ B, Boyd J. Pimecrolimus-induced tinea incognito. Skinmed 2004, 3, 352-3.
- Krajewska-Kulak E, Niczyporuk W, Lukascuk C, Bartoszewicz M, Roszkowska I, Edyta M.. Difficulties in diagnosing and treating tinea in adults at the Department of Dermatology in Bialystok (Poland). Dermatol Nurs 2003, 15, 527-30.
- Kim MW, Park HS, Bae JM, Yoon HS, Cho S. Tinea Incognito with Folliculitis-Like Presentation: A Case Series. Ann Dermatol 2018, 30, 97-9. [CrossRef]
- Dutta B, Rasul ES, Boro B. Clinico-epidemiological study of tinea incognito with microbiological correlation. Indian J Dermatol Venereol Leprol 2017, 83, 326-31. [CrossRef]
- Gawdzik A, Nowogrodzka K, Hryncewicz-Gwóźdź A, Maj J, Szepietowski J, Jankowska-Konsur A. Epidemiology of dermatomycoses in southwest Poland, years 2011–2016. Postepy Dermatol Alergol 2019, 36, 604-608. [CrossRef]
- Samer Dhaher. Tinea incognito: Clinical perspectives of a new imitator.Dermatol Reports. 2020 Jun 25; 12(1): 8323. [CrossRef]
- Thomas Stringer, Julia K. Gittler, Seth J. Orlow. Tinea Incognito in an Urban Pediatric Population. Cutis. 2018 November;102(5):370-372.
- J. del Boz, V. Crespo, F. Rivas-Ruiz, M. de Troya. Tinea incognito in children: 54 cases. Mycoses 2011 Volume54, Issue3 ,pages 254-258. [CrossRef]
- Abed Ali FAH, Jawad K, Al-Janabi A, Alhattab MK. Prevalence of dermatophyte fungal infection in Hillah, Iraq. Int J Chem Tech Res 2017, 10, 827-37.
- Yee G, Al Aboud AM. Tinea Corporis. In: StatPearls [Internet]. Treauser Island (FL): StatPearls Publishing; 2023.
- King RD, Khan HA, Foye JC, Greenberg JH, Jones HE. Transferrin, iron, and dermatophytes. I. Serum dermatophyte inhibitory component definitively identified as unsaturated transferrin. J Lab Clin Med 1975, 86, 204-12.
- Wollina U, Hansel G, Koch A, Abdel-Naser MB. Topical pimecrolimus for skin disease other than atopic dermatitis. Expert Opin Pharmacother. 2006, 7, 1967-75. [CrossRef]
- Singh A, Masih A, Khurana A, Singh PK, Gupta M, Hagen F, Meis JF, Chowdhary A. High terbinafine resistance in Trichophyton interdigitale isolates in Delhi, India harbouring mutations in the squalene epoxidase gene. Mycoses 2018, 61, 477-84.
- Dabas Y, Xess I, Singh G, Pandey M, Meena S. Molecular identification and antifungal susceptibility patterns of clinical dermatophytes following CLSI and EUCAST guidelines. J Fungi (Basel) 2017, 3, 17. [CrossRef]
- Rudramurthy SM, Shankarnarayan SA, Dogra S, Shaw D, Mushtaq K, Paul RA, Narang T, Chakrabarti A. Mutation in the Squalene Epoxidase Gene of Trichophyton interdigitale and Trichophyton rubrum Associated with Allylamine Resistance. Antimicrob Agents Chemother 2018, 62, e02522-17. [CrossRef]
- Kim WJ, Kim TW, Mun JH, Song M, Kim HS, Ko HC, et al. Tinea incognito in Korea and its risk factors: Nine-year multicenter survey. J Korean Med Sci 2013, 28, 145-51. [CrossRef]
- Arun B, Remya VS, Sheeba PM, Kokkayil P. Mycological study on incidence of tinea incognito in a tertiary hospital. Med Pulse-International Medical Journal 2015, 2, 649-51.
- Romano C, Maritati E, Gianni C. Tinea incognito in Italy: A 15-year survey. Mycoses 2006, 49, 383-7. [CrossRef]
- Turk BG, Taskin B, Karaca N, Sezgin AO, Aytimur D. Clinical and mycological analysis of twenty-one cases of tinea incognita in the Aegean region of Turkey: A retrospective study. Acta Dermatovenerol Croat 2013, 21, 93-8.
- Pustisek N, Skerlev M, Basta-Juzbasic A, Lipozencic J,Marinovic B, Bukvic-Mokos Z. Tinea incognito caused by Trichophyton mentagrophytes. Acta Dermatovenerol Croat 2001, 9, 283-6.
- Arenas R., Moreno-Coutiño G., Vera L., Welsh O. Tinea incognito. Clin Dermatol 2010, 28, 137-9.
- Gorani A, Schiera A, Oriani A. Case report. Rosacea-like tinea incognito. Mycoses 2002, 45, 135-7.
- Romano C, Asta F, Massai L. Tinea incognito due to Microsporum gypseum in three children. Pediatr Dermatol 2000, 17, 41-4. [CrossRef]
- Faergemann J, Fredriksson T, Herczka O, Krupicka P, Bjorklund KN, Sjokvist M. Tinea incognito as a source of an "epidemic" of Trichophyton violaceum infections in a dermatologic ward. Int J Dermatol 1983, 22, 39-40. [CrossRef]
- Feder Jr HM. Tinea incognito misdiagnosed as erythema migrans. N Engl J Med 2000, 343, 69.
- Ansar A, Farshchian M, Nazeri H, Ghiasian SA. Clinico-epidemiological and mycological aspects of tinea incognito in Iran: A 16-year study. Med Mycol J 2011, 52, 25-32. [CrossRef]
- Naglot A, Shrimali DD, Nath BK, Gogoi HK, Veer V, Chander J, Tewari R. Recent trends of dermatophytosis in Northeast India (Assam) and interpretation with published studies. Int J Curr Microbiol Appl Sci 2015, 4, 111-20.
- Sahai S, Mishra D. Change in spectrum of dermatophytes isolated from superficial mycoses cases: First report from Central India. Indian J Dermatol Venereol Leprol 2011, 77, 335-6.; [CrossRef]
- J Del Boz J, Crespo V, Rivas-Ruiz F, De Troya M. Tinea incognito in chil dren: 54 cases. Mycoses 2011, 54, 254-8. [CrossRef]
- Johnson RA: HIV disease: mucocutaneous fungal infections in HIV disease. Clin Dermatol 2000, 18, 411-22.
- Galhardo MCG, Wanke B, Reis RS, Oliveira LA, Valle ACF. Disseminated dermatophytosis caused by Microsporum gypseum in an AIDS patient: response to terbinafin and amorolfine. Mycoses 2004, 47, 238-41. [CrossRef]
- Luque AG, Biasoli MS, Sortino MA, Lupo SH, Bussy RF. Atypical tinea corporis caused by Microsporum gypseum in a subject with acquired immune deficiency syndrome. J Eur Acad Dermatol Venereol 2001, 15, 374-5.
- Porro AM, Yoshioka MC, Kaminski SK, Palmeira M do C, Fischman O, Alchorne MM. Disseminated dermatophytosis caused by Microsporum gypseum in two patients with the acquired immunodeficiency syndrome. Mycopathologia 1997, 137, 9-12. [CrossRef]
- Prochnau A, de Almeida HL Jr, Souza PRM, Vetoratto G, Duquia RP, Defferrari R. Scutular tinea of the scrotum: report of two cases. Mycoses 2005, 48, 162-4.
- Romano C, Massai L, Gallo A, Fimiani M: Microsporum gypseum infection in the Siena area in 2005–2006. Mycoses 2009, 52, 67-71.
- Jensen JM, Pfeiffer S, Akaki T, Schröder JM, Kleine M, Neumann C, Proksch E, Brasch J. Barrier function, epidermal differentiation and human b-defensin 2expression in tinea corporis. J Invest Dermatol 2007, 127, 1720-7.
- Gupta AK, Konnikov N, MacDonald P, Rich P, Rodger NW, Edmonds MW, McManus R, Summerbell RC. Prevalence and epidemiology of toenail onychomycosis in diabetic subjects: A multicentre survey. Br J Dermatol 1998, 139, 665-71. [CrossRef]
- Weitzman I, Summerbell RC. The dermatophytes. Clin Microbiol Rev 1995, 8, 240-59.
- Sahoo AK, Mahajan R. Management of tinea corporis, tinea cruris, and tinea pedis: A comprehensive review. Indian Dermatol Online J 2016, 7, 77-86. [CrossRef]
- Guenova E, Hoetzenecker W, Schaller M, Rocken M, Fierlbeck G. Tinea incognito hidden under apparently treatment- resistant pemphigus foliaceus. Acta Derm Venereol 2008, 88, 276-7. [CrossRef]
- Solomon BA, Glass AT, Rabbin PE. Tinea incognito and “over-the-counter” potent topical steroids. Cutis 1996, 58, 295-6.
- Gupta AK, Ryder JE, Chow M, Cooper EA. Dermatophytosis: The management of fungal infections. Skinmed 2005, 4, 305-10.
- Park YW, Choi JW, Paik SH, Kim DY, Jin SP, Park HS, Yoon HS, Cho S. Tinea incognito simulating herpes simplex virus infection. Ann Dermatol 2014, 26, 267-9. [CrossRef]
- Sardana K, Gupta A, Aastha M, Mathachan SR. Immunopathogenesis of Dermatophytoses and Factors Leading to Recalcitrant Infections. Indian Dermatol Online J 2021, 12, 389-99. [CrossRef]
- Novick NL, Tapia L, Bottone EJ. Invasive trichophyton rubrum infection in an immunocompromised host. Case report and review of the literature. Am J Med 1987, 82, 321-5. [CrossRef]
- Grossman ME, Pappert AS, Garzon MC, Silvers DN. Invasive Trichophyton rubrum infection in the immunocompromised host: report of three cases. J Am Acad Dermatol 1995, 33, 315-8. [CrossRef]
- Erbagci Z. Topical therapy for dermatophytoses: should corticosteroids be included? Am J Clin Dermatol 2004, 5, 375-84.
- Lekkas D, Ioannides D, Lazaridou E, Lallas A, Apalla Z, Vakirlis E, Johr R, Errichetti E, Kyrgidis A, Sotiriou E. Dermatoscopy of tinea corporis. J Eur Acad Dermatol Venereol 2020, 34, e278-e280.
- Slowinska M, Rudnicka L, Schwartz RA, Kowalska-Oledzka E, Rakowska A, Sicinska J, Lukomska M, Olszewska M, Szymanska E. Comma hairs—A dermoscopic marker for tinea capitis. A rapid diagnostic method. J Am Acad Dermatol 2008, 59, S77-9.
- Piraccini BM, Balestri R, Starace M, Rech G. Nail digital dermoscopy (Onychoscopy) in the diagnosis of onychomycosis. J Eur Acad Dermatol Venereol 2013, 27, 509-13. [CrossRef]
- Rajagopalan M, Inamadar A, Mittal A, Miskeen AK, Srinivas CR, Sardana K, Godse K, Patel K, Rengasamy M, Rudramurthy S, Dogra S. Expert Consensus on The Management of Dermatophytosis in India (ECTODERM India). BMC Dermatol 2018, 18, 6. [CrossRef]
- Pihet M, Le Govic Y. Reappraisal of Conventional Diagnosis for Dermatophytes. Mycopathologia 2017, 182, 169-180. [CrossRef]
- Kurade SM, Amladi SA, Miskeen AK. Skin scraping and a potassium hydroxide mount. Indian J Dermatol Venereol Leprol 2006, 72, 238-41. [CrossRef]
- Ahmad MR, Javed I, Mushtaq S. Evaluation of Chicago sky blue stain against Potassium Hydroxide-Dimethyl Sulfoxide wet mount in the identification of dermatophytes. J Fatima Jinnah Med Univ 2020, 14, 83-86. [CrossRef]
- Lasseter G, Palmer M, Morgan J, Watts J, Yoxall H, Kibbler C, McNulty C. Members of the HPA GP Microbiology Laboratory Use Group Developing best practice for fungal specimen management: Audit of UK microbiology laboratories. Br J Biomed Sci 2011, 68, 197-202.
- Ovrén E, Berglund L, Nordlind K, Rollman O. Dermatophytosis: Fluorostaining enhances speed and sensitivity in direct microscopy of skin, nail and hair specimens from dermatology outpatients. Mycoses 2016, 59, 436-41. [CrossRef]
- Sumathi S, Pandit VS, Patil S, Adavi V. A cross sectional clinicomycological study of dermatophytosis in a tertiary care hospital, North Karnataka, India. IP Int J Med Microbiol Trop Dis 2018, 4, 166-70. [CrossRef]
- Singh J, Zaman M, Gupta AK. Evaluation of microdilution and disk diffusion methods for antifungal susceptibility testing of dermatophytes. Med Mycol 2007, 45, 595-602. [CrossRef]
- Park YW, Kim DY, Yoon SY, Park GY, Park HS, Yoon HS, Cho S. ‘Clues’ for the histological diagnosis of tinea: How reliable are they? Ann Dermatol 2014, 26, 286-8.
- Navarrete-Dechent C, Bajaj S, Marghoob AA, Marchetti MA. . Rapid diagnosis of tinea incognito using handheld reflectance confocal microscopy: a paradigm shift in dermatology? Mycoses 2015, 58, 383-6.
- Li HC, Bouchara JP, Hsu MML, Barton R, Su S, Chang TC. Identification of dermatophytes by sequence analysis of the rRNA gene internal transcribed spacer regions. J Med Microbiol 2008, 57, 592-600. [CrossRef]
- Friedman D, Friedman PC, Gill M. Reflectance confocal microscopy: An effective diagnostic tool for dermatophytic infections. Cutis 2015, 95, 93-7.
- Turan E, Erdemir AT, Gurel MS, Yurt N. A new diagnostic technique for tinea incognito: In vivo reflectance confocal microscopy. Report of five cases. Skin Res Technol 2013, 19, e103-7.
- Cowen LE, Sanglard D, Howard SJ, Rogers PD, Perlin DS. Mechanisms of antifungal drug resistance. Cold Spring Harb Perspect Med 2014, 5, a019752. [CrossRef]
- De Sousa MGT, Santana GB, Criado PR, Benard G. Chronic widespread dermatophytosis due to Trichophyton rubrum: A syndrome associated with a Trichophyton-specific functional defect of phagocytes. Front Microbiol 2015, 6, 801. [CrossRef]
- Sugita K, Kabashima K, Atarashi K, Shimauchi T, Kobayashi M, Tokura Y. Innate immunity mediated by epidermal keratinocytes promotes acquired immunity involving Langerhans cells and T cells in the skin. Clin Exp Immunol 2007, 147, 176-83. [CrossRef]
- Sardana K, Kaur R, Arora P, Goyal R, Ghunawat S. Is antifungal resistance a cause for treatment failure in dermatophytosis: A study focused on tinea corporis and cruris from a tertiary centre? Indian Dermatol Online J 2018, 9, 90-5.
- Marconi VC, Kradin R, Marty FM, Hospenthal DR, Kotton CN. Disseminated dermatophytosis in a patient with hereditary hemochromatosis and hepatic cirrhosis: Case report and review of the literature. Med Mycol 2010, 48, 518-27. [CrossRef]
- Hay RJ, Baran R. Deep dermatophytosis: Rare infections or common, but unrecognised, complications of lymphatic spread? Curr Opin Infect Dis 2004, 17, 77-9.
- Rouzaud C, Hay R, Chosidow O, Dupin N, Puel A, Lortholary O, Lanternier F. Severe dermatophytosis and acquired or innate immunodeficiency: A review. J Fungi (Basel) 2015, 2, 4. [CrossRef]
Figure 1.
Tinea incognito treated as nummular eczema with topical steroids.

Figure 2.
Tinea incognito treated with topical steroids for three months resulting in scar formation.
Figure 2.
Tinea incognito treated with topical steroids for three months resulting in scar formation.

Figure 3.
Dermatophyte infection treated with topical combination cream of topical steroid plus topical fusidic acid.
Figure 3.
Dermatophyte infection treated with topical combination cream of topical steroid plus topical fusidic acid.


Table 1.
The pathogenesis of tinea incognita.
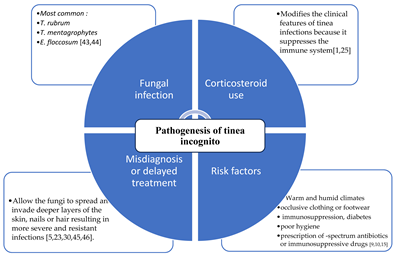
Table 2.
The effect of topical or systemic glucocorticoids on pathogenesis of tinea [49].
Table 2.
The effect of topical or systemic glucocorticoids on pathogenesis of tinea [49].

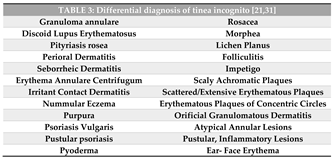
Table 5.
Topical antifungal medications [44].
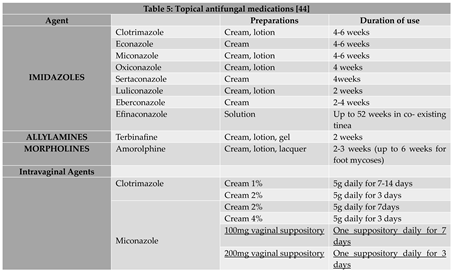
Table 6.
Systemic antifungal agents [44].
Table 6.
Systemic antifungal agents [44].

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



