
Submitted:
18 March 2024
Posted:
20 March 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Coronavirus disease-19 (COVID-19) has disproportionately affected certain demographics in England, exacerbating existing health disparities. Effective therapeutics are a critical line of defence against COVID-19, particularly for patients at elevated risk for severe disease. Surveillance systems were established to monitor usage of COVID-19 therapeutics in hospital and community settings and inform stewardship. Three antiviral therapies: nirmatrelvir plus ritonavir (Paxlovid®), remdesivir (Veklury®), and molnupiravir (Lagevrio®); and two neutralising monoclonal antibody therapies (nMAbs): sotrovimab (Xevudy®) and casirivimab with imdevimab (Ronapreve®); were in use in England between July 2020 to April 2023. This paper aims to illuminate trends in the utilisation of COVID-19 therapeutics treatment in both hospital and community settings, stratified by the Index of Multiple Deprivation (IMD) in England. Chapter 3 of the English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR) report 2022 to 2023 also discusses the epidemiological surveillance of these five directly-acting antiviral COVID-19 therapeutics use in England between 2022 to 2023.
Keywords:
antivirals
; community
; COVID-19
; deprivation
; hospital
; therapeutics
1. Introduction
Effective therapeutics have become a critical line of defence against coronavirus disease 2019 (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), particularly for patients at elevated risk for severe disease[1,2]. To accelerate the discovery and distribution of antiviral therapeutics, the UK government established the Antivirals Taskforce (ATF)[3]. Shortly thereafter new and repurposed therapeutic agents for treating COVID-19 were introduced in April 2020. The United Kingdom first administered treatments in hospital settings on 11 July, 2020 [4] and initiated non-hospital (community) treatments on 16 December of the same yea[3,4,5]. COVID Medicine Delivery Units (CMDUs) were launched to facilitate the provision of COVID-19 therapeutics to non-hospitalised, high-risk patients in England[6,7]. Three antiviral therapies: nirmatrelvir plus ritonavir (Paxlovid®), remdesivir (Veklury®), and molnupiravir ( Lagevrio®); and two neutralising monoclonal antibody therapies (nMAbs): sotrovimab (Xevudy®) and casirivimab with imdevimab (Ronapreve®); were deployed to treat COVID-19 cases (supplementary A). Corticosteroids and other immunomodulators were considered outside of the scope of this analysis. Surveillance systems were set up to monitor treatments in both hospital and community settings and assist with stewardship of these therapeutics[8,9]. As in the previous year, the latest English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR) 2022 to 2023 indicates variations in therapeutic requests between hospital and non-hospital settings[10]. While casirivimab with imdevimab (available in the UK from September 2021 to February 2022) and remdesivir (available from May 2020) were predominantly used in hospitals for people with severe COVID-19 (supplementary A).
Sotrovimab (launched in the UK mid-December 2021), nirmatrelvir plus ritonavir (launched in February 2022), and molnupiravir (available from mid-December 2021; February 2022) were mainly administered in community settings to people with COVID-19 who had a high risk of severe outcomes to prevent their symptoms from worsening[6,9]. Though sotrovimab can be used in both community and hospital settings, it is mainly administered in the community setting.
COVID-19 has disproportionately affected certain demographics in England, exacerbating existing health disparities. Mortality rates in the most deprived areas surpass those in less deprived areas [6,7,11]. There have been efforts to address health inequalities in England; Core20PLUS5 is an NHS England initiative aimed at addressing and narrowing these health disparities[12]. Identifying a core target population, the approach focusses on five clinical areas requiring urgent improvement. Such strategies aimed at addressing health inequalities are critically important and necessitate ongoing stewardship. This paper aims to illuminate trends in the utilisation of COVID-19 therapeutics treatment in both hospital and community settings, stratified by the IMD in England [13].
2. Methods
2.1. Data and Data Sources
COVID-19 therapeutics usage data were sourced from NHS England via the Blueteq system, which collects patient-level treatment request data. The Blueteq system manages high-cost drugs for NHS England and as such, contains clinical requests made for neutralising monoclonal antibodies (nMAB) and antiviral therapies used for the treatment of patients with COVID-19. NHS England interrogates whether clinical criteria are met before prescribing of antivirals can be undertaken. Data between 11 July 2020 and 30 April 2023 were included.
2.2. Data Processing and Statistical Analyses
We estimated treatment request rates, measured as the number of requests per 100,000 COVID-19 cases. To estimate rates of total treatment requests by IMD between July 2020 to April 2023, the number of treatment requests were divided by the number of COVID-19 cases, normalised to 100,000 individuals by IMD decile.
All analyses were conducted using STATA 17 and R.
3. Results
In England, between July 2020 to April 2023, a total of 181,674 requests for therapeutic treatments comprising nMAB and antivirals against COVID-19 were recorded on the Blueteq system. More than half of these requests (56.7%, 103,048 treatments) were made within the community setting. Hospital settings accounted for the remaining 43.3% of treatment requests, of which, 35.6% (64,598 treatments) were requested for those hospitalised for the management of COVID-19 and 7.7% (14,028 treatments) for those with hospital-onset COVID-19.
The highest number of treatment requests was in quarter 1 and quarter 2 2022 (n=35,596; n= 26,332 treatments respectively). In 2022, there were a total of 108,786 treatment requests. Remdesivir was the most prescribed, constituting 36.8% (n=66,946) of all requests. This was followed by nirmatrelvir plus ritonavir at 24.8% (n=45,107), sotrovimab at 23.1% (n=41,911), molnupiravir at 12.4% (n=22,489), and casirivimab with imdevimab at 2.9% (n=5,221) which was only used in England between Q3 2021 and Q1 2022 (Figure 1). Peaks in usage were in Q4 2020 for remdesivir (n= 16,484), casirivimab with imdevimab in Q4 2021 (n=4774), nirmatrelvir plus ritonavir were both in Q2 and Q3 2022 (n=10,107 and n= 10,368 respectively) and in Q1 2022 for sotrovimab (n=17,666), as indicated in Figure 1.
The rate of therapeutic use differed substantially according to IMD scores in England, and differentially according to site of administration (Figure 2). The treatments primarily used in community settings, sotrovimab, molnupiravir and nirmatrelvir plus ritonavir, displayed substantially lower usage rates in areas with higher deprivation compared to less deprived deciles. Conversely, remdesivir and casirivimab with imdevimab, predominantly used in hospital settings, demonstrated the opposite trend, and were requested at higher rates in more deprived areas. To illustrate, casirivimab with imdevimab the 1st decile had higher rate in use than in the least deprived decile areas (67.9; 39.9 per 100,000 COVID-19 cases respectively). Similarly, remdesivir saw a higher usage rate in the most deprived decile compared to the least deprived decile (2,359.3; 1,633.6 per 100,000 COVID-19 cases respectively).
Between April 2020 and March 2023, therapeutic treatments that were predominantly administered in community settings constituted the largest proportion of treatments. Specifically, nirmatrelvir plus ritonavir exhibited a (3,015.8; 1,666.1 per 100,000 COVID-19 cases respectively) higher rate of use in the least deprived decile areas compared to the most deprived decile. Molnupiravir and sotrovimab followed suit (1,355.5; 878.8 per 100,000 COVID-19 cases respectively) and (756.9; 572.2 per 100,000 COVID-19 cases respectively) higher rates respectively in the least deprived decile when compared to the most deprived 1st decile. It should be noted, however, that these rates are subject to fluctuations over time.
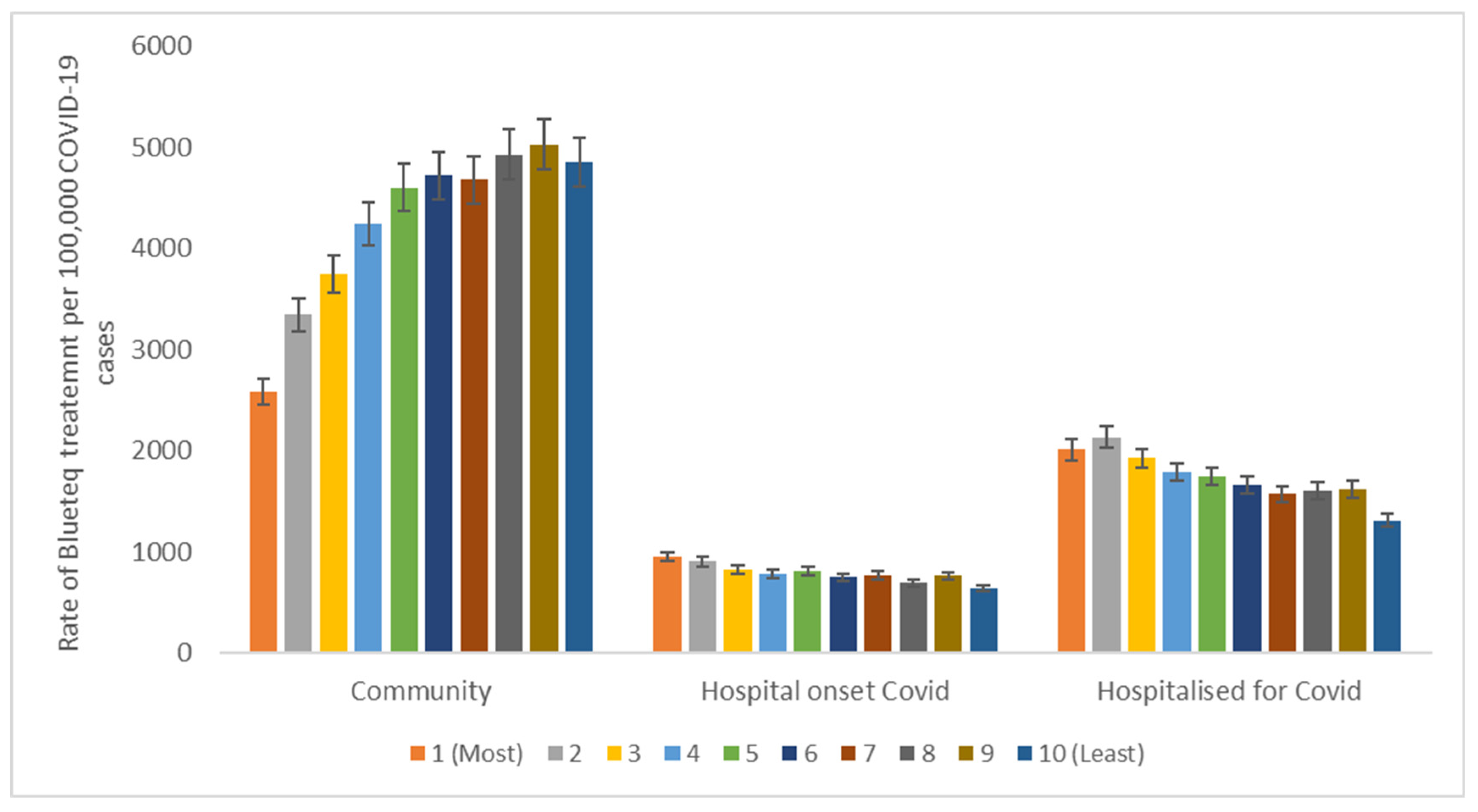
As seen in Figure 3, the rate of therapeutic use varied by IMD across different settings. 42,716.3 of total treatment requests per 100,000 COVID-19 cases are within the community, followed by hospitalised for COVID-19 (17,364.0), and finally hospital onset COVID-19 (7,871.4). Rates of therapeutic use within the community setting were much lower in the most deprived areas than in the least deprived areas with 53.3% higher rates in the least deprived than most deprived decile (4,852.4; 2,585.1 per 100,00 COVID-19 cases respectively). However, within the hospital setting there was a reverse trend which indicates higher usage among the least deprived compared to the most deprived areas. This accounts for 67.1% in the most deprived compared to the least deprived (950.3; 637.7 per 100,000 COVID cases respectively) while the rate of requests in individuals hospitalised for COVID-19 within the most deprived were 65.3% higher than the least deprived (2008.9; 1,311.6 per 100,000 COVID cases).
4. Discussion
This study represents the first analysis that describes national trends in the use of therapeutic treatments for COVID-19 within both hospital and community settings, stratified by deprivation level in England. Treatment requests across both settings have exhibited fluctuations over time, especially in light of the introduction of new treatments, changes in viral strain, efficacy of therapy and evolving guidelines.
A notable finding is the disparity in treatment rates between community and hospital settings across different deprivation deciles. Treatments in community settings were more prevalent among the least deprived deciles, while hospital settings saw a higher rate of treatments in the most deprived deciles over this period. It is important to caution that without data on individuals who were eligible for, offered, and completed each treatment, these trends may not necessarily reflect underlying inequities in access to healthcare.
This study is in line with another research effort that examined the breakdown of therapeutic treatment by key demographics and deprivation quintiles[5]. That study indicated that 12% of non-hospitalised patients receiving treatment resided in the most deprived areas, compared to 21% in the least deprived areas[5]. Higher rate of treatments in the most deprived deciles within the hospital setting could be attributed to several interconnected factors such as varying SARS-CoV-2 exposure risks where population with lower income often live in environments with higher exposure to pollutants and in overcrowded conditions, which may affect their risk of complications from respiratory infections. Differences in healthcare accessibility could lead to delayed diagnoses and treatment, which may contribute to these observed disparities, necessitating further research. Evidence from previous studies suggests some ethnic groups are more likely to live in more deprived areas than other counterparts[14]. Additionally, a higher level of deprivation is related to poorer health outcomes [15]. Delays in access to health care may result in delays in intervention which could result in higher rates of hospitalisation. This could explain why remdesivir and casirivimab with imdevimab use, which are predominantly used in hospital settings, were higher among the most deprived deciles compared to the least deprived, with the reverse pattern observed in community settings for molnupiravir, nirmatrelvir plus ritonavir, and sotrovimab rates.
Therapeutics primarily administered in community settings constituted most of all treatment requests between July 2020 and April 2023. Variations in treatment rates by IMD may also have geographical implications concerning where these drugs are most frequently prescribed. It is worth noting that not all these therapeutic agents were available throughout the entire period between July 2020 and April 2023. For instance, sotrovimab was incorporated into the clinical commissioning policy in mid- December 2021. Similarly, nirmatrelvir plus ritonavir was included in the clinical commissioning policy only as of February 2022. Additionally, free community testing was discontinued in April 2022.
The effectiveness of casirivimab with imdevimab against the dominant Omicron variant of SARs-COV-2 has been uncertain as most studies were carried out before this variant circulated. This resulted in limited requests for casirivimab with imdevimab during the winter of 2021-2022 and its eventual removal from the clinical commissioning policy in 2022[8].
Limitations of this analysis include the absence of denominator data on individuals who were eligible for, offered, and accepted each treatment. Not all treatment requests may have resulted in patients receiving or completing treatment with these drugs as the electronic or patient prescribing data were not accessible. As such, this study serves as an exploratory analysis and may not accurately depict variations or inequities in access to healthcare.
5. Conclusions
This paper highlights the trend of COVID-19 therapeutics treatment by setting and deprivation. This study demonstrates the difference in COVID-19 treatment request rates by deprivation level and setting. The most deprived groups accessed treatments predominantly dispensed in hospital settings at higher rates than the least deprived. Improving community access to health care within the most deprived areas would likely improve health outcomes and reduce treatments within hospital settings. Continued surveillance in monitoring new treatments, including information on the population eligible to receive these is important to understand the nuances between settings and the potential patterns that are likely to emerge. Further research would be beneficial to examine factors leading to high treatment rates in these two settings, as well as hospital admission rates.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualisation, A.F; methodology, A.F., and H.S.; validation, A.F, H.S., S.B.-A. and A.L.; formal analysis: A.F. and H.S..; investigation, A.F., H.S., S.B.-A., A.D.; writing—original draft preparation, A.F. and H.S.; writing—review and editing. A.F., H.S., S.B.-A., A.D., A.L., C.S.B.; supervision, S.B.-A., H.S and A.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
The data presented in this study are available in [Bou-Antoun, S.; Falola, A.; Budd, E., H.; Squire, H.; Brown, C.S.; Hope, R., Hopkins, S.; Muller-Pebody, B., Demirjian, A. The English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR) report 2022 to 2023, Chapter 3 Antimicrobial Consumption, London, 2023.].
Acknowledgments
Special thanks to the NHS England colleague for supplying the Blueteq data.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Løchen, A.; Squire, H.; Ashiru-Oredope, D.; Hand, K.S.; Hartman, H.; Triggs-Hodge, C.; Fountain, H.; Bou-Antoun, S.; Demirjian, A.; Gerver, S.M. Surveillance and Stewardship Approaches for COVID-19 Novel Therapeutics in England from 2021 to 2022 (ESPAUR Report). Medical Sciences Forum 2022, 15, 2. [CrossRef]
- Falola, A.; Demirjian, A.; Thompson, W.; Brown, C.S.; Gerver, S.; Bou-Antoun, S. The impact of COVID-19 national restrictions on dental antibiotic dispensing trends and treatment activity in England: January 2016 to July 2021. JAC-Antimicrobial Resistance 2023, 5. [CrossRef]
- D.o.H.a.S. Government launches COVID-19 antivirals taskforce to roll out innovative home treatments this autumn. Available online: https://www.gov.uk/government/news/government-launches-covid-19-antivirals-taskforce-to-roll-out-innovative-home-treatments-this-autumn (accessed on.
- England, N. COVID-19 Therapeutics (antivirals, neutralising monoclonal antibodies and interleukin 6 inhibitors). Available online: https://www.england.nhs.uk/statistics/statistical-work-areas/covid-therapeutics-antivirals-and-neutralising-monoclonal-antibodies/ (accessed on.
- Collaborative, T.O.; Green, A.; Curtis, H.J.; Higgins, R.; Smith, R.; Mehrkar, A.; Inglesby, P.; Mahalingasivam, V.; Drysdale, H.; DeVito, N.J.; et al. Trends, variation and clinical characteristics of recipients of antivirals and neutralising monoclonal antibodies for non-hospitalised COVID-19: A descriptive cohort study of 23.4 million people in OpenSAFELY. medRxiv 2022, 2022.2003.2007.22272026. [CrossRef]
- UKHSA. English surveillance programme for antimicrobial utilisation and resistance (ESPAUR). Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1033851/espaur-report-2020-to-2021-16-Nov.pdf (accessed May 2022). (accessed on.
- England, N. Commissioning Framework:COVID-19 Therapeutics for Non-Hospitalised Patients. Available online: https://www.england.nhs.uk/coronavirus/wp-content/uploads/sites/52/2022/12/C1677-commissioning-framework-covid-19-therapeutics-for-non-hospitalised-patients-march-23.pdf.pdf (accessed on.
- NICE. Casirivimab plus imdevimab, nirmatrelvir plus ritonavir, sotrovimab and tocilizumab for treating COVID-19. Available online: https://www.nice.org.uk/guidance/ta878/resources/casirivimab-plus-imdevimab-nirmatrelvir-plus-ritonavir-sotrovimab-and-tocilizumab-for-treating-covid19-pdf-82613679870661 (accessed on.
- Bou-Antoun, S.; Rokadiya, S.; Ashiru-Oredope, D.; Demirjian, A.; Sherwood, E.; Ellaby, N.; Gerver, S.; Grossi, C.; Harman, K.; Hartman, H.; et al. COVID-19 therapeutics: Stewardship in England and considerations for antimicrobial resistance. Journal of Antimicrobial Chemotherapy 2023, 78, ii37-ii42. [CrossRef]
- ESPAUR. English surveillance programme for antimicrobial utilisation and resistance (ESPAUR). Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1033851/espaur-report-2020-to-2021-16-Nov.pdf (accessed on.
- England, P.H. Health Profile for England 2021. Available online: https://fingertips.phe.org.uk/static-reports/health-profile-for-england/hpfe_report.html (accessed on.
- England, N. Core20PLUS5 an Approach to Reducing Health Inequalities: Supporting information. Available online: https://www.england.nhs.uk/publication/?filter-keyword=Core20plus&filter-category=&filter-publication=&filter-date-from=&filter-date-to=&filter-order-by=date-desc (accessed on.
- Ministry of housing, c.l.g. The English Indices of Deprivation 2019. Available online: https://assets.publishing.service.gov.uk/media/5dfb3d7ce5274a3432700cf3/IoD2019_FAQ_v4.pdf (accessed on.
- Evandrou, M.; Falkingham, J.; Feng, Z.; Vlachantoni, A. Ethnic inequalities in limiting health and self-reported health in later life revisited. J Epidemiol Community Health 2016, 70, 653-662. [CrossRef]
- UKHSA. Understanding health inequalities in England. Available online: https://ukhsa.blog.gov.uk/2017/07/13/understanding-health-inequalities-in-england/ (accessed on.
Figure 1.
Number of treatment requests in Blueteq by therapeutic between Quarter 3 2020 and Quarter 2 2023. Note differences in scale. *Numbers <11 are masked.
Figure 1.
Number of treatment requests in Blueteq by therapeutic between Quarter 3 2020 and Quarter 2 2023. Note differences in scale. *Numbers <11 are masked.
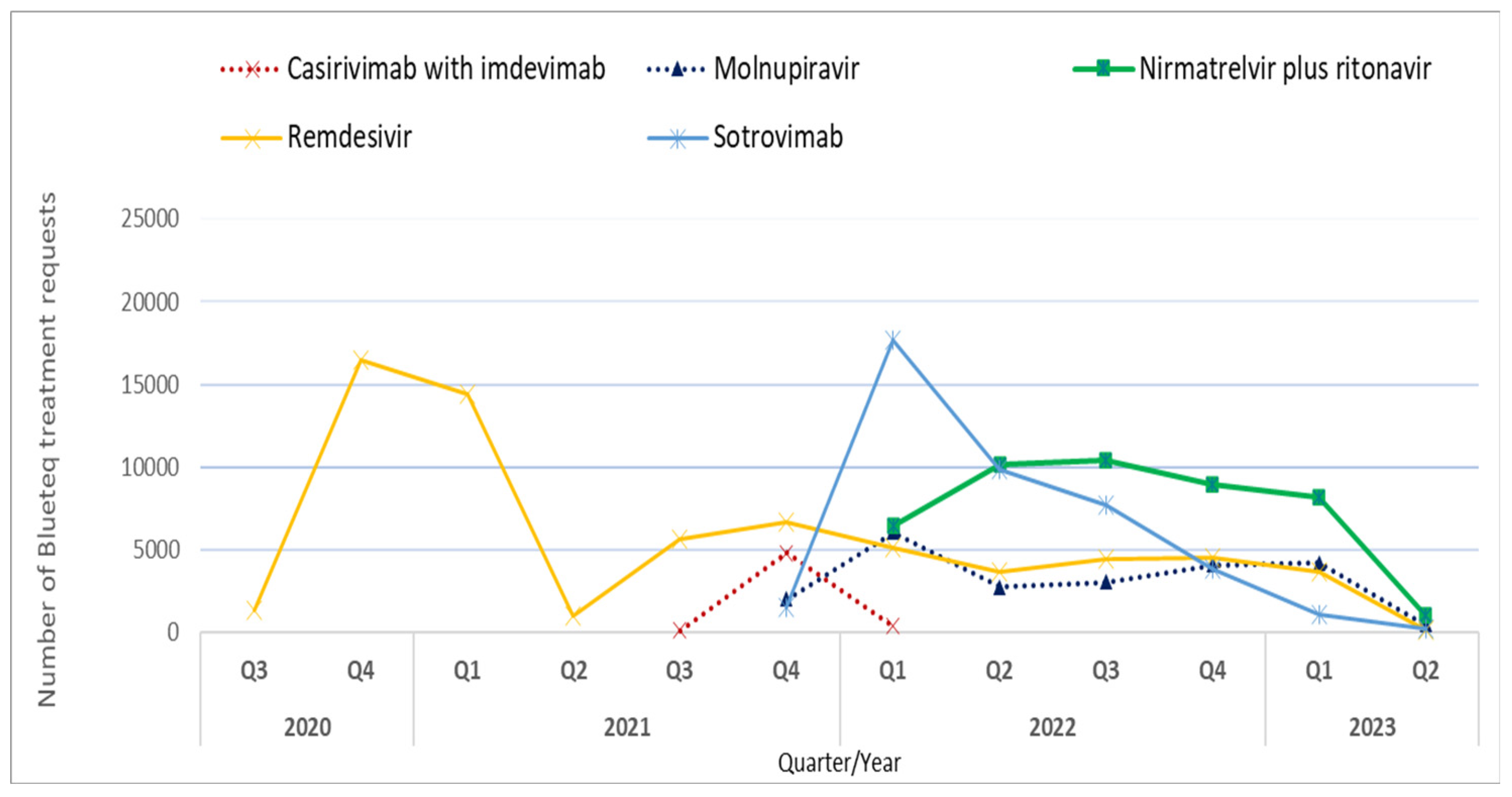
Figure 2.
Rate of Blueteq treatment requests per 100,000 COVID-19 cases in England by therapeutic and IMD decile (most (1) to least (10) deprived). 1. Therapeutics in Figure 1A, 1B and 1C are predominately used within the community setting. 2. Therapeutics in Figure 1D and 1E are predominantly used within the hospital setting.
Figure 2.
Rate of Blueteq treatment requests per 100,000 COVID-19 cases in England by therapeutic and IMD decile (most (1) to least (10) deprived). 1. Therapeutics in Figure 1A, 1B and 1C are predominately used within the community setting. 2. Therapeutics in Figure 1D and 1E are predominantly used within the hospital setting.
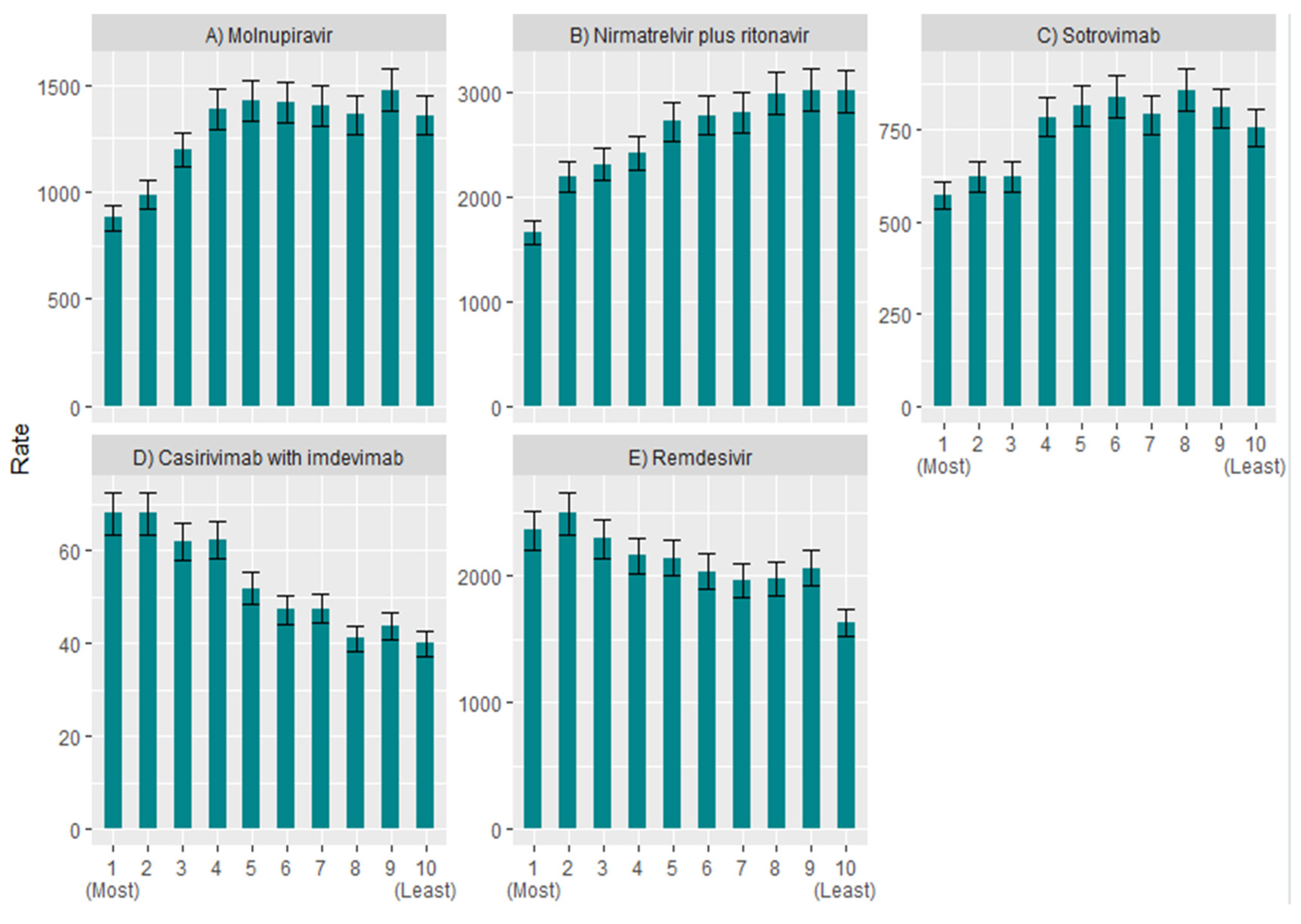
Figure 3.
Rate of Blueteq treatment request per 100,000 COVID-19 cases in England by setting and IMD decile (most (1) to least (10) deprived).
Figure 3.
Rate of Blueteq treatment request per 100,000 COVID-19 cases in England by setting and IMD decile (most (1) to least (10) deprived).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



