Submitted:
19 March 2024
Posted:
19 March 2024
Read the latest preprint version here
Abstract
Human papillomavirus (HPV) is one the most common sexually transmitted infections (STI), spreading through direct sexual contact to oropharynx and anogenital regions. Although most infected individuals may be asymptomatic and naturally undergo viral clearance, in some individuals’ HPV infection causes carcinogenesis of the infected epithelia. HPV now accounts for over 70% of oropharyngeal carcinomas (OPC). Over 90% of these OPC are associated with HPV 16, one of the 14 high-risk subtypes. In recent years, HPV positive (HPV+) OPC has been one of the most rapidly rising cancers, by new cancer incidence rates, especially among men. They present some unique infection driven cellular and molecular features, in comparison to other head and neck carcinomas (HNC), constituting distinct preventive, therapeutic and prognostic strategies - with significant strides made in this area. However, HPV+OPC are routinely detected at a later stage, adding to the disease burden and overall survival. In this review, we provide a summary of HPV from a STI to malignant transformation, while also parsing through the immune response environment. We further collate key literature around infection sites, diagnostics and clinical management, while throwing light on the current state of epidemiology, transmission, screening and prevention strategies. Indeed, our improving understanding of the disease’s molecular biology has added some success to the prognostic outcomes of certain HPV+OPC across clinical trials examining targeted therapeutics and immunotherapy. This work is directed towards improving our current understanding of HPV and associated oncogenic landscape, to guide screening, early detection, triaging and further prevention and management strategies.
Keywords:
Human papillomavirus
; sexually transmitted infection
; oropharyngeal carcinoma
; oral cancer
; head and neck cancers
1. HPV: History, Epidemiology of Infection & Carcinoma
The human papillomavirus (HPV) is estimated to be the most common; prevalent and incident, STI among adults, infecting the squamous epithelial cells and spreading through any intimate skin to skin contact, including vaginal, anal or oral sex [1,2]. Subsequent to a persistent HPV infection, it is the etiological agent for a wide range of benign and malignant conditions in humans. HPV belongs to the Papillomaviridae family containing more than 400 types isolated from humans, birds, non-human mammals and reptiles [3,4]. These are epitheliotropic viruses and have a potential to initiate the process of squamous epithelial neoplasia – benign and malignant. Infectious agents are the cause for 13% of global cancer burden. HPV is one of the key drivers of this global, infection-caused, cancer burden [5].
While skin and genital warts and their potential infectivity have been described since the Greek and Roman era, the contagious nature of cutaneous wart was first reported by Payne (1891), and of oro-genital condyloma - a late 19th century terminology for genital wart, linked with sexual behavior, by Heidingsfield (1901). Subsequently, the viral etiology of genital lesions was demonstrated by Ciuffo (1907) [6]. Around 40 years later Strauss et al (1949) first isolated the virus by using electron microscopy [7]. It was during this time that all cutaneous and genital warts were associated with the same virus – the human wart virus. Subsequent molecular studies of the bovine papillomavirus helped analyze different viral subtypes, while the characterization of the viral double-stranded circular DNA were first reported by Crawford (1965) - described as the human papilloma virus [8], and Klug and Finch (1965) – described as the human wart virus of the papilloma-polyoma family of viruses [9]. In the next decade, heterogeneity of the HPV family was studied extensively through in-vitro hybridization studies across cervical cancer tissue samples, cutaneous and genital warts [10]. Simultaneously antigenic variability was also apparent between cutaneous and genital wart HPV particles (Almeida 1969) [11,12]. The link between HPV and cervical cancer was theorized beginning in 1972 by Dr. Harald zur Hausen and his team, with subsequent work identifying and cloning the HPV subtypes 16 and 18 directly in cervical cancer biopsies [10,13,14,15]. By 1983 Dr. zur Hausen, had demonstrated that HPV was the causative factor for human cervical cancer, incorporating its genes into the host cell DNA [16,17], this work eventually leading to his winning the 2008 Nobel Prize in Medicine . The largely sexually transmitted HPV was successively found to be the cause of multiple other cancers – anogenital, laryngeal, penile, oropharyngeal, vaginal, vulvar [11,18,19,20,21,22,23,24,25,26,27] .
Newell et al in 1975 were one of the earliest to report an association of cervical cancer in women and a 5-6-fold increased risk for oral cancer subsequently [28]. By 1983 Syrjänen et al reported positive demonstration of HPV antigen in premalignant oral lesions - oral squamous papillomas, an early hint of HPVs association with oral squamous cell carcinoma (OSCC) [20]. This association was unequivocally confirmed by 1985 in OPC and tongue carcinomas, reported to be associated with HPV 16, 11 and 27 subtypes [21,22]. 40% of the laryngeal and oral cancers showed a similarity in the morphological and histological appearance with other HPV infected lesions and there was detection of HPV structural proteins in 50% of the samples [20]. In 1989 Brandsma and Abramson examined 116 squamous cell carcinoma and papilloma tissue samples and reported the presence of HPV 16 DNA in cases of pharynx (13%), tongue (18%) and tonsils (29%), while the samples from mouth, nose and esophagus were negative for any HPV [29]. By the 1990s multiple groups demonstrated the association of HPV 16 subtype in over 60% of OPC, followed by HPV 6, 7, 11, 18, 33, 35 and 59 subtypes accompanied with E6, E7 gene expression [18,30,31,32].
In a systematic review by Kreimer et al (2005), covering 5,046 HNC specimens across 60 studies, HPV prevalence was found to be significantly higher in OPC than OSCC, particularly the HPV 16 subtype, while fewer HPV+ HNC were associated with HPV 18 and other oncogenic subtypes [33]. Further epidemiologic support of the association of HPV in OPC pathogenesis was established in a case-control study by D’Souza et al. The strength of this association was evidenced across a subgroup of OPC patients and underscoring the connection between high-risk sexual behavior and oral HPV infection, particularly HPV 16 [34]. It is now well established that around 52 - 70% of all OPC in the UK and US are attributable to HPV, particularly HPV 16 infection (85-96% of all HPV+ OPC) [35]. In contrast 3.9% OSCC, including significantly lower incidence of HPV+ carcinomas in the larynx [36,37]. Curiously, tonsillar OPC are suggested to have higher susceptibility to HPV infections as a result of the single layered discontinuous epithelial arrangement in the tonsillar crypts (similar to the cervical squamocolumnar junction cells), making them more prone to carcinogenesis, compared to OSCCs. HPV- HNC can be associated with Epstein-Barr virus (EBV) and polyomaviruses with potential HPV co-infection [38]. It is important to note that there is still some discrepancy in data regarding the association of HPV and different anatomical subsites in HNC, possibly attributable to insufficient detection methods by lack of localization distinction [37].
HPV+OPC is one of the most rapidly rising cancers, especially in high income countries [39]. Some of these countries have seen a 3-fold increase in HPV+OPC, over the last 2 decades [40,41,42,43]. Interestingly, the incidence of OPC in men, involving the base of the tongue and tonsils in younger men <50 years without any history of alcoholism and smoking, has surpassed that of cervical cancer in women [44,45]. A recent systematic review and meta-analysis showed that globally almost 1 in 3 men over the age of 15 are infected with at least one genital HPV subtype, while 1 in 5 men are infected with more than one or more high-risk HPV subtypes [46]. In a case study involving 240 cases of OPC, patients who were positive for HPV-16 had a history of oral sex and multiple sexual partners while those who were negative for HPV-16 did not have the history of oral sex but had a strong history of smoking and drinking [47]. Additionally, the risk stratification for oral HPV infection in an individual is associated with frequency and number of oral sexual partners, especially within the previous 3 months. Studies have also shown that oral HPV clearance is significantly lesser in males than female [48]. Although smoking and alcohol have been demonstrated as risk factors for HNC and a substantial history of consumption of these agents is associated with worse outcomes even in HPV+ OSCC [49]. However, the association between HPV positivity and HNC, especially the OPC, demonstrates a distinct disease entity in comparison to HPV- HNC. It is interesting to note that HPV+ HNC have been shown to have better prognosis than the HPV- tumors, the former being highly susceptible to radiation and anticancer drugs. HPV- HNC requires more intensive treatment in comparison to those who were HPV+ [4].
2. Transmission of HPV
The main mode of transmission for HPV is intimate skin to skin contact including genital and extragenital (oral cavity or anus) sites. HPV is one of the most common STI. In a study by Sonawane et al, determining prevalence of oral HPV infection across NHANES data, the risk of infection was 11.5% in men and 3.2% in women. The transmission rate for high-risk HPV in men was found to be 12.7% when reported having same-sex oral sex partners, and significantly increased to 22.2% if 2 or more partners were reported [50].
The transmission of virus from women to men was found to be higher than from male to female indicating a higher prevalence of virus in men. Transmission between the female anus and scrotum was also demonstrated through non-penetrative sexual contact [51]. It was found that bisexual, gay men and men who have sex with men had 17 times increased risk of developing anal cancer as compared to heterosexual men, especially those with HIV infection [52]. Partners of oral HPV+ individuals were found to have increased prevalence of oral HPV infection indicating oral-oral transmission. There has been an association between deep mouth kissing and the development of oral HPV infection [53]. Oro-genital contact is the most important for HPV leading to oropharyngeal lesions. It was found that there was an increased incidence ratio of OPC (tonsillar and tongue carcinoma) - 2.7:1 in husbands of women who had invasive cervical cancer [54]. Another study showed that the incidence of OPC, especially in the anatomical sites of tonsils and tongue, in husbands of women with cervical cancer was much higher than those women with cervical intraepithelial neoplasia. Other modes may include autoinoculation, vertical transmission or contact with hands [55].
The virus may be transmitted through the amniotic fluid and placenta, or transmission may occur during the passage through the infected birth canal [51]. Although the risk of transmission via an infected birth canal is mainly for infants who are delivered vaginally. The infection acquired by infants is usually transient and is cleared in 2-3 months [56]. Transmission of low-risk HPV subtypes may lead to recurrent respiratory papillomatosis [57]. Autoinoculation may be evidenced by detecting HPV in females who have never had sexual contact as well as in children with no signs of sexual abuse. Nosocomial transmission of the HPV is also possible which may occur during the use of transvaginal ultrasound probe which is commonly used in the Obstetrics & Gynaecology departments where the probe is placed very close to the cervix which may act as a pathway of infection [56]. Like the instruments used in the Obstetrics and Gynaecology department, flexible endoscopes used in otolaryngology may also serve as a source of infection in the oral region [58]. 3% of the probes were found to be positive for HPV DNA after examination and 1.9% were found to be positive in pre-examination samples [59].
Autoinoculation is also thought to be a mode of transmission of the virus between the genital and oral sites. It has been observed that women who have been diagnosed with invasive cervical cancer, cervical dysplasia or cervical infection with HPV tend to have a higher prevalence of the virus in the oral samples [60]. Vertical transmission of the virus also occurs through breast milk. Body to body contact after the delivery can also lead to transmission. The development of recurrent respiratory papillomatosis in neonates confirms the transmission of low-risk viral subtypes. High-risk HPV has also been detected in tonsillar and adenoid samples. Children may carry the infection and act as a reservoir of the virus leading to persistent infection and carcinogenesis in adult life. The viral load is directly proportional to the rate of transmission of the virus to the fetus through vertical transmission [61].
Transmission of the virus from the father to the fetus may occur in the periconceptual period. HPV DNA is present on the head of the spermatozoa and can lead to transfer of the genes like E6 and E7 to the oocyte which is associated with an increased risk of spontaneous abortion. Although the risk is very low, hematogenous transmission of the virus through the cord blood from the mother to the fetus has been postulated [62]. Early onset of sexual activity in adolescents, multiple sexual partners, cigarette smoking, concomitant STD serve as a risk factor for HPV infection and its persistence [63]. The virus can persist on clothing, surfaces, equipment for very long periods of time as they are resistant to heat and dehydration. Although HPV DNA has been identified in water bodies, waterborne transmission has not been described [51].
3. HPV Structure, Function & Landscape of Oncogenesis
HPV is a small non-enveloped double stranded DNA virus, icosahedral and 50-60 nm in diameter. Papillomaviruses are highly species specific, infecting the epithelium and mucosa across fish to mammals, and have co-evolved with the vertebral host. The Papillomaviridae family is organized into 5 genera – Alphapapillomaviruses, Betapapillomaviruses, Gammapapillomaviruses, Mupapillomaviruses and Nupapillomaviruses. Many of the HPVs cause asymptomatic infections in humans and are considered normal epithelium microflora [64]. Although it is the Alphapapillomaviruses that are tropic for genital and oral epithelium and mucosa, while the Betapapillomaviruses, Gammapapillomaviruses are cutaneous HPV subtypes [65].
In recent years, much expansion has occurred in the study of some of these cutaneous, often commensal HPV subtypes, especially Betapapillomaviruses. HPV 1, 2 and 4 - cause plantar warts, while HPV 5, 8, 9, 12, 14, 15, 17, 19-25, 36, 46, and 47 cause epidermodysplasia verruciform, and HPV 5 and 8 can predispose to development of UV-mediated skin cancer [66]. The mucosal type or Alphapapillomaviruses can be divided into low risk and high risk. Some of the benign conditions associated with these include plantar warts, periungual warts, anogenital warts, recurrent respiratory papillomatosis, conjunctival papillomatosis [67]. Malignant conditions include cervical, vaginal, vulvar, penile, anogenital cancers, squamous cell carcinoma of the tonsils, pharynx, base of the tongue, larynx, etc . More than 450 subtypes of the HPV have been identified [65], out of which the low risk subtypes include 6 and 11 which cause warts of the genitals, anus, mouth or throat, and larynx or respiratory tract (which may lead to respiratory papillomatosis). There are 12 high risk HPV subtypes - 16, 18, 31, 33, 35, 45, 51, 52, 56, 58 and 59, which have the propensity to cause squamous cell carcinomas [1,68], while HPV 16 and 18 are the most commonly carcinoma causing subtypes. Co-evolution with humans has allowed all these viruses to benefit, persist and replicate across diverse mucosal epithelium, anatomical and biological niches, while exploiting host cellular pathways, immune response, to engineering proliferation and differentiation [65].
The HPV genome contains 8000 base pairs containing episomes which contain 8-9 ORFs. There are 3 distinct regions in the HPV genome – early (E) spread across 50% of the genome encoding the nonstructural proteins, late (L) encoding structural proteins and representing 40% of the genome. The remaining genome is largely represented by the noncoding or long regulatory regions [69,70]. The capsid is composed of 72 pentameric capsomers all around. It is the capsid that contains the two late structural proteins L1 (360 copies) and L2 (12 copies) [71,72]. The single stranded DNA which forms eight ORFs constituting the viral genome. The L1 and E1 protein encoding regions are the most conserved in HPV genome, hence HPV taxonomy is based on nucleotide sequence coding for the capsid based L1 protein. Difference within the L1 gene sequence, at least a 10%, allows for distinguishing HPV types and genotypes. While differences of 2-10% between HPV variants are considered subtypes [73,74].
Host Cell Infection & Oncogenic Transformation
Entry of the virus into the host cell occurs when L1 binds to the heparin sulphate proteoglycans which is present in the epithelial basement membrane. There occurs a conformational change in the capsid of the virus which helps in the exposure of L2 which binds to molecules on wound keratinocyte causing conformational change again which causes the L1 to be exposed and be more accessible to attachment. Through micro abrasions, the virus gains access to the basal layer of the epithelium [75,76]. The life cycle of the virus is intra epithelial, it causes no viremia, lysis/ death of the cell. There is no role of inflammatory cytokines and the signals for the recruitment and migration of langerhans cells and dendritic cells is absent. There occurs release of the viral particles from the epithelium away from the immune cells. Once entry of the virus occurs, there occurs replication of the viral DNA as the basal cells progress to the surface epithelium. When the virus is present at the basal layer, the replication occurs at a slower rate while there is amplification of the DNA to a higher number in the superficial layer [77]. This begins the transcription of E6 and E7 which respectively act on P53 and Rb. The E5 gene induces mitogen activated protein kinase activity which leads to cellular proliferation. After this E1 and E2 synthesis occurs. The E2 inhibits E6 and E7 transcription which then allows E1 to bind to the origin of replication. This in turn initiates replication as extrachromosomal elements. L1 and L2 are activated by the late promoter. E4 helps in maturation and release of the viral particles from the superficial layer of the epithelium. Although the viral DNA is present in all the layers, it is only in the superficial layer that the virions are present and released from [77].
Replication of the viral genome and the transcription of proteins is regulated by E1 and E2 proteins [78,79]. E2 protein also helps in the repression of transcription of the oncoproteins E6 and E7. Hence, the loss or deletion of E2 protein results in upregulation of the oncoproteins leading to tumorigenesis [80]. E6 and E7, also help in viral replication into the keratinocytes, while promoting cell-cycle progression [81,82]. HPV+OPC is very different from HPV- carcinoma due to the distinct roles of E6 and E7 and the P53 and Rb pathways disruption [83].
Importantly, oncogenicity of high-risk HPV subtypes is driven by the key activity of E6 and E7 proteins, facilitating integration to host DNA and inactivating tumor suppressor proteins – tumor protein 53 (TP53) – associated with 60-80% HNC and retinoblastoma pRb – thus promoting tumor growth [84,85,86]. An early and frequent genetic alteration in HNCs is the cell cycle control pathway. Loss of CDKN2A combined with amplification of cyclin D1 causes unscheduled DNA replication, through G1-S checkpoint of cell cycle – leading to DNA damage and p53 activation [87]. The binding of E6 protein to cellular E3 ligase and E6 associating protein leads to the formation of a heterodimer which degrades the TP53 which is a tumor suppressor protein via ubiquitin- proteasome pathway [84,85,88]. The E6 protein causes repression of apoptosis and promotes the survival of damaged cells which leads to immortalization of cells. It also upregulates telomerase, maintaining telomere length and preventing senescence in continually proliferating cells[89,90]. Similarly, E7 protein which plays a role in cell growth and replication causes degradation of pRB, likely by inactivating cell cycle regulators like cyclin D1, CDK6 [91,92].
Although E5 protein is weakly oncogenic, encoded only by Alphapapillomaviruses, it helps in enhancement of the oncogenic potential of E6 and E7 proteins. E5 also causes downregulation of antigen processing, immunoproteasome function inhibition – downregulating host antiviral responses [93,94]. There is evidence that E6, E7 and E5 oncoproteins also alter multiple other cellular signaling pathways - JAK-STAT activation plays an important role in the carcinogenesis. In HPV+ cervical cancer, the activation of the JAK-STAT3 pathway makes the cancer cells more sensitive to the chemotherapeutic drugs [95,96,97]. E6 is shown to enhance the Wnt/ β-Catenin Pathway, possibly as the key mediator of a broad range of cell proliferation genes [98]. PI3K signaling activation by somatic mutation and/or copy number alteration is another key feature of HPV+OPC, early on during carcinogenesis [99,100]. Loss of function mutation of CYLD and PTEN, and gain of function mutation in FGFR3 – all activating PI3K signaling, are significantly enriched in HPV+OPC [47]. Indeed, the PI3K amplifications have been associated with longer overall survival in these OPC [101].
These oncogenic HPV drive phenotypical changes in epithelial cells, causing a polar shift of infected cells towards tissue invasion, metastatic potential, inhibition of apoptosis and senescence, creation of an immunosuppressive microenvironment, potential therapy resistance – identified as oncogenic epithelial-mesenchymal transition (EMT). E6 and E7 induce the development of spindle shaped mesenchymal-like translation of the otherwise cobblestone-shaped epithelium and induce the expression of Slug, Twist and ZEB 1/2 transcription factors associated with upregulated tumor invasion [102]. E7 also causes actin reorganization and cell adhesion changes [103]. E5 upregulates EGFR and allows evasion of programmed cell death. Loss of the typical apico-basal orientation is driven by detachment of cells from the basal membrane through proteolytic degradation and associated angiogenesis - promoting metastasis of HPV+ cancers, by upregulating MET and hepatocyte growth factor receptor [104,105]. This causes chronic stromal inflammation. Although, the virus inhibits the NF-Κb which signals the inflammatory pathway, as the progression of the cancer takes place, there is increased inflammation. There is increased recruitment of Th17 which is mediated by CCL20. It promotes the further growth of the tumor and angiogenesis. Figure 1 summarizes HPV driven oropharyngeal epithelial infection and carcinogenesis processes.
4. HPV & Host Immune Response
The well-orchestrated life cycle of HPV mediates multiple host immune response evasion strategies. The co-evolution of the host and HPV, across multiple anatomical sites, has allowed the virus to strategize defenses not only through cell-mediated immune responses but also physically. Owing to the entire life cycle of the HPV occurring within the host epithelial cells particularly the most well-differentiated, superficial layers of the stratified squamous epithelium, and preventing any cell lysis or viremia immediately post infection, the viral machinery and infected cells are situated far away from innate host defenses while it undergoes high levels of viral gene expression and replication [106]. Its virions eventually do shed alongside fully differentiated superficial cells, during desquamation, but this early and robust viral replication benefits from immune non-detection. This strategy also significantly impedes any antibody-mediated humoral or T cell response in infected individuals, against HPV proteins [107,108]. Indeed, another early response to evade the innate immune surveillance begins immediately at the time viral entry into the host epithelial cell, hitchhiking its genome via the protection of endosomal vesicles into the nucleus [106].
The viral L2 and other early viral proteins, especially in high-risk oncogenic subtypes, further disrupts the innate immune signaling pathway by repressing the antiviral component of the host cell nuclear bodies, during early stages of infection [109]. In most HPV infections, the cell-mediated immune response does eventually recognize the infected cells and responds to HPV viral proteins - L1 capsid protein, E6, and E7 being the primary antigens recognized, subsequently attracting T cells to infiltrate for infection resolution and clearance [110]. Interestingly, post-infection humoral response against specific HPV types is highly limited, in contrast to HPV vaccination where the humoral response to the vaccine achieves high seroconversion at the levels of infection site, mucus and serum [111]. The persistence of the virus occurs when there are not enough effective immune control mechanisms. There is clearance of the virus in immunocompetent patients, while those who have impaired immunity show a higher prevalence of the infection and subsequent carcinogenesis [112]. As an example, Fanconi anemia patients have very high susceptibility to HPV infections leading to carcinoma, proposed to be associated with the high genetic mutations in cells as a result of HPV oncogene promoted genetic instability in Fanconi anemia cells with already defective DNA repair mechanism [113]. Carcinogenesis through oncogenic HPV is not a process that occurs within a few days, it takes years to occur and the immune system evasion of HPV plays a key role in this process.
Studies have shown that oncogenic HPV E5 and E7 antagonize activating stimulator of interferon genes (STING) protein, thus downregulating the viral detection pathway via Type-1 interferon (IFN) response. E5 protein allows evasions of both innate and adaptive immunity. It disrupts the function and synthesis of major histocompatibility complex (MHC) class I and II proteins, in turn promoting immune evasion by preventing infected cell recognition by the CD8+ cytotoxic T cells [93,114]. Antigen presenting cells such as langerhans cells and dendritic cells play a role in clearing the infection. HPV causes a reduced expression of E-cadherin on the epithelium which is why the localization of langerhans cells is reduced. Toll-like receptors generate an immune response against the virus which releases inflammatory cytokines like interferons, tumor necrosis factor and interleukins [115]. E6 and E7 oncogenes also prevent secretion of CXCL14 chemokines and NF-κB-dependent CCL20, interfering with langherhan and dendritic cell migration to infection sites [116,117]. The virus induces a lot of immune evasion mechanisms. Not only does the virus have the ability to hide itself from recognition by downregulation of the antigens, it sheds from the superficial layer of the epithelium where the presence of immune cells is minimal [107].
Immunosuppressive microenvironments are well established across most tumors, including avoiding recruitment of potent cytotoxic natural killer (NK) cells. There is also impaired tumor infiltrating T cell recognition of antigens, cytokine secretion and activation of CD8+ cytotoxic T lymphocytes (CTLs), a T cell subset efficient in anti-tumor responses. It has been observed that HPV-positive HNC and OPC had a significantly higher tumor infiltrating CD4+, CD8+, and CD3+ subsets and chemokine response [118,119]. HPV positive OPC are one of the most highly immune-cell infiltrated tumors that includes - CD3+ T cells, CD8+ T cells, Treg cells, B cells, and plasma cells, in comparison to HPV- OPC [120]. Additionally, ~64% of HPV+OPC have been shown to have HPV 16 specific infiltrating T cells as well [121]. Some studies have recently shown that tissue infiltrating macrophages like the M1 (CD68+) macrophage in HPV+OPC also add to anti-tumor activity by supporting CD4+ T cell differentiation, activation of CD8+ T cells. Multiple studies have shown that tumors with high CTL infiltration, also had high chemokine signature and were associated with improved patient prognosis and overall survival [122].
However, despite the high tumor microenvironment infiltration HPV+OPC still exhibit continuous immune evasion and disease relapse by benefitting the immune checkpoint mechanisms. One such checkpoint – programmed cell-death 1 (PD-1) expressed on activated T and B cells limits T cell function and is seen to be highly expressed in some HPV+OPC [123]. These tumors are now being targeted by immune checkpoint inhibitors across some key clinical trials and demonstrating improved response rate [124,125,126,127], paving the way for further assessment of various immune-checkpoint inhibitors for treatment.
5. HPV: Head & Neck Infection Sites & Carcinogenesis
Studies have shown that while the discontinuously organized oropharyngeal stratified squamous epithelium, particularly tonsillar crypt epithelial cells, may be ideal for a productive HPV infection, in fact reflect low infection rate and may be non-permissive for productive infection; based on exposure and immune control, yielding high viral titers. While the more stratified squamous epithelium of the oral cavity seems less conducive to HPV infection, in reality, HPV positivity is higher in the oral cavity [128,129]. However, these HPV+ oral cells hardly transform to carcinoma (<3.9%), and while tonsillar HPV infections are rare a significant proportion transform to carcinoma [130]. In contrast to cervical carcinoma where HPV infected epithelium transition from dysplastic precursors is well known, HPV driven pathogenesis in OPC still remains little known. HPV+ dysplastic lesions in the oropharynx are rarely observed or found [131].
Observations from the pathologic changes across high-risk HPV infected cells, where at least 20% infections result in dysplastic lesions, can help shed light into the transformation of HPV+OPC. These productive infections display mild to moderate dysplasia, without oncogenic transformation and minimal E6 and E7 expression. While in 3-5% of high-risk HPV+ proliferating cervical cells E6 and E7 expression is strongly upregulated, leading to moderate to severe dysplasia [132]. Herfs et al suggest that the squamocolumnar junction in cervical cells (often positive for cytokeratin7 – CK7 immunostain) are highly susceptible for transforming infections and predecessor to cervical carcinomas, whereas the former productive infections may be arising from basal squamous epithelial populations [133]. Interestingly, in the tonsillar specimens the presence of these strong CK7 staining in tonsillar crypt epithelia and absence in stratified squamous epithelia suggest and association with high-risk HPV+OPC, suggest a pathogenesis mechanism similar to cervical carcinoma, including expression of E6 and E7 viral oncogenic promoters [134,135].
Aside from the tonsillar and other oropharyngeal anatomical sites, other potential reservoirs within the oral cavity encompass inflamed gingival pockets, ductal epithelium within salivary glands, cryptal epithelium of the tonsils, the oral cavity's border, and the oropharynx—akin to the border between ectoderm and endoderm, analogous to the transformation zone observed in the uterine cervix [136]. Since gingival pockets have basal cells – the known targets of latent HPV infection it is hypothesized that inflamed gingival pockets could be a possible first site of infection in oral mucosa. A study by Tezal et al also concluded that chronic periodontitis played a significant factor in the natural history of HPV infection in patients with base of tongue cancers [137]. Benign oral lesions such as squamous papilloma is the most common manifestation of oral HPV infection and is associated with HPV 6, 11. It is localized on the nonkeratinized mucosa (lingual belly, soft palate) or keratinized (hard palate) and appears as an exophytic neoformation [138].
6. Detection of HPV, Diagnosis & Screening
6.1. Detection of HPV & Diagnosis of OPC
Patients with OPC routinely present with a sore throat or as a neck mass, dysphagia, globus sensation, otalgia, odynophagia or a visual mass and nodal metastases [139]. Initial diagnosis of suspicious lesions requires tumor visualization either endoscopically, a rhinoscope or ultrasonography, followed by fine-needle biopsy sampling of the lesion [140]. The presence of HPV DNA in biopsied tissue is routinely determined by PCR techniques, unrelated to oncogenesis. Testing for HPV+OPC is recommended through detection of E6/E7 oncogenes via RT-PCR, p16 and HPV DNA detection in situ hybridization (ISH) [130,141]. However, these methods are labor, cost and resource intensive. P16 immunohistochemistry in biopsied using formalin-fixed paraffin-embedded tissue specimen has increasingly been used as a recommended stand-alone prognostic, surrogate, marker for detection of high-risk HPV, as a result of the overexpression of p16, a cell-cycle protein, in the carcinogenesis process of HPV+OPC, per the 8th edition of American joint commission on Cancer (AJCC) – to TNM stage OPC [124]. Although recent evidence suggests p16 may not always be consistent with HPV+OPC [142]. Viral detection spanning across various detection methods have been found to either over- or underestimate the number of patients affected with HPV+OPC. Smith et al suggest that testing for a combination of markers – HPV, p16 and p53 may improve the prognostic accuracy of OPC [143]. As a result of moderate specificity associated with p16 testing, diagnosis of HPV+OPC is recommended in combination with HPV DNA PCR, for optimal accuracy. Additionally, both MRI and PET-CT imaging are recommended for primary tumor staging, determination of tumor invasion degree, extent of metastasis or nodal spread [144]. In the United States, [18F] fluoro-2-deoxy-D-glucose (18F-FDG) PET–CT is the primary modality employed to evaluate tumor extent and the presence of metastases, with MRI potentially used to assess local invasion extent [145]. Clinical prognostication generally relies on factors such as tumor diameter, nodal status, positive surgical margins, and grade of differentiation (well, moderate, or poorly differentiated). This includes assessing the invasive front's grade, considering factors like keratinization, pleomorphism, mitotic rate, invasion pattern, and patient response [146].
6.2. Screening
The incidence of OPC in middle-aged and older adult men is projected to double over the next decade, despite current prophylactic vaccination efforts [147]. Interestingly, the incidence of HPV driven OPC is greater than cervical cancer, as a result of robust screening strategies applied for early detection of the latter [148]. These shifts in HPV driven oncogenesis of the head and neck highlight the need for parallel cervical cytology screening in the head and neck area. However, these measures have been argued against by the need for further research in the OPC area, low incidence rate in comparison to other HPV driven carcinomas, available therapy and favorable outcomes, and prevention strategies through HPV vaccination. Other deterrents to screening include the need for a robust understanding and strategy for identifying precancerous lesion, efficient biomarker and diagnostic technology to detect lesions, particularly minimally invasively, and the absence of triaging and subsequent clinical management for patients with precancerous lesions or early-stage OPC [147]. In an early demonstration of HPV infection preceding diagnosis of OPC, a case-control study by Agalliu et al, pooling screening trials from multiple cancers showed for the first time that patients with oral HPV have up to 22 fold greater odds of developing OPC [149]. Further studies in this area can help establish strategies and value for oral HPV screening. Studies utilizing oral rinse and gargle specimens for HPV DNA detection have been investigated with variable sensitivity and specificity [149,150]. These strategies would only provide information for current exposure, while clinical gold standard testing involving testing blood samples, it can reveal presence of antibodies against HPV oncoproteins, established more likely as a disease marker occurring in the transition of HPV infection to cancer.
Serologic testing for HPV 16 E6 protein has demonstrated some promise as a screening tool though it remains to be validated [151]. Investigation of HPV 16 E6 seropositivity in the ARCAGE case-control study, EPIC study, PLCO cancer screening cohort showed strong correlation of E6 antibody positivity and OPC and antibody positivity range was 30-42% [152]. Another screening method utilized has been to test circulating HPV DNA in blood specimens, with 61-88% sensitivity across studies [153]. Aside from insufficient specificity as a screening tool, another issue with these studies is the inability to localize HPV 16 antibody positivity to the site of the disease [154].
Oral cytology, similar to cervical cytology screening methods, has been garnering significant importance in recent times [155]. In a study by Broglie et al, brush cytology was able to detect HPV positivity in 66% patients, but was able to identify dysplastic cells in 88% patients [156]. Castillo et al performed liquid -based brush cytology for detection of HPV in patient suspicious of OPC, with 88% sensitivity of the cytology assessment pre-treatment, 71% post-treatment, while 91% accuracy of HPV-DNA assessment, across 75 patients [157]. In the OHMAR study by Benevolo et al, testing of oropharyngeal cytobrush samples and oral rinse and gargle specimens were testing by cytological evaluation and HPV genotyping, respectively, in a group of men who have sex with men at 6-months intervals. The study found that infection of high-risk HPVs, including HPV 16 did not increase the risk for cytologic abnormalities [158]. While these and other studies highlight the growing value of oral cytology, further research is necessary to evaluate the efficacy of this screening methodology in the same light as HPV driven cervical cytology, including the inability to access the target anatomical sites region like the tonsils or base of the tongue [159]. Other screening methodologies to detect HPV positivity include testing for novel biomarkers – microRNA, mRNA, DNA methylation and protein signatures, in tumor tissue, using genomic technologies, proteomic technologies like matrix-assisted laser desorption ionization time-of-flight mass spectrometry, protein microarray among others [160].
7. Prevention & Management
7.1. HPV Prophylactic Vaccines
Currently, three prophylactic vaccines have been approved for HPV infections. Cervarix (GlaxoSmithKline), Gardasil -4 (now discontinued in the US), and Gardasil-9 (Merck Sharp and Dohme). These vaccines consist of virus-like particles (VLPs) derived from the major capsid protein (L1) of HPV. While these vaccines exhibit high immunogenicity, it's essential to note that their effectiveness is primarily limited to the HPV types specifically included in the vaccines. These L1 proteins from which these VLPs are derived, lack conservation across various HPV types, resulting in minimal cross-protection against non-vaccine HPV types [161,162,163].
Cervarix, a bivalent vaccine, predominantly protects against HPV16 and HPV18, is approved for females aged 9 to 25, while Gardasil-4 - a tetravalent vaccine, protects against HPV6, HPV11, HPV16, and HPV18. Gardasil-9, a second-generation vaccine, provides protection against the above-mentioned four high-risk HPV types and additionally targets other high-risk HPV types - HPV31, HPV33, HPV45, HPV52, and HPV58. Gardasil-4 and Gardasil-9 are approved for administration to everyone aged 9 to 26, and per clinician’s consideration vaccines can be administered at 27 - 45 years of age as well [164]. Despite these vaccines being available for over a decade, vaccination campaigns have primarily focused on preventing cervical, vaginal, anal, penile cancers, and genital warts. Limited information exists regarding the efficacy in preventing HPV-related HNC, especially in men. However, recent studies suggest that these vaccines may confer protection against oral HPV infections [165].
Vaccination with Gardasil-4 or Cervarix has been shown to induce anti-HPV16 and HPV18 IgG antibodies in the oral cavity. Another study observed that individuals immunized with Gardasil-4 produced anti-HPV IgG antibodies in saliva, which, albeit at low titers, neutralized pseudoviruses representing HPV6, HPV16, and HPV18 in vitro [165,166]. The detection of neutralizing anti-HPV antibodies in saliva post intramuscular immunization indicates a potential prevention of oral infections with these HPV types and, consequently, a subset of HPV + HNC. However, it is crucial to emphasize that certain findings mentioned earlier [165,167], were solely based on the detection of antibody titers in the saliva of individuals vaccinated with the HPV vaccine and/or in vitro neutralization assays utilizing saliva from these individuals. Recent in vitro studies have investigated the potential of Gardasil-4 and other HPV vaccines to provide protection against oral HPV infections in mice. A study by Ahn Juile et al, illustrated that mice, intramuscularly immunized with Gardasil-4 or a pan-HPV L2 vaccine (targeting broadly neutralizing epitopes on the minor capsid), were shielded from oral infection with HPV pseudovirus 16 [168]. Another study by Zhai et al, demonstrated that mice orally immunized with mixed MS2-L2 VLPs were protected from infection following oral exposure to HPV pseudoviruses 16, 35, 39, 52, and 58 which is a prevalent HPV type associated with HNC. Furthermore, mice orally immunized with mixed MS2-L2 VLPs were entirely protected from oral infection with HPV pseudovirus 39. Therefore, mixed MS2-L2 VLPs have the potential to protect against 11 HPV types associated with approximately 99% of HPV + HNC and one HPV type linked to around 32% of recurrent respiratory papillomatosis [169].
7.2. Management
The prophylactic vaccines mentioned above are primarily designed to prevent HPV infections and are not intended for the treatment of existing HPV infections. Hence individuals who have developed HPV symptomatic infections may require treatment. Unlike other viral infections that respond to drug therapy, there are no active ingredients currently available to eliminate HPV infections or regress the clinical lesions. Numerous drugs have been tested for treating genital lesions both topically and systemically, there are no established treatments for such lesions at present. Antiviral drugs like acyclovir and ribavirin, tested for their effectiveness, have shown no success in eliminating oral HPV infections mirroring the lack of effective treatment for their genital counterparts [138]. The commonly available treatments available for papillomas, condylomas, verrucas, and Heck’s diseases are cryotherapy, electrosurgery, surgical removal, laser therapy, and trichloroacetic acid [136]. Lordyua et al. demonstrated that three applications (each lasting 30–60 seconds) of trichloroacetic acid led to atraumatic resolution of such lesions within 45 days. Additionally, Mendoz-Flores et al. successfully treated Heck’s lesions by applying topical 5% imiquimod cream every night for two weeks [170,171].
7.2.1. Standard Management of OPC
As some HPV infections lead to transition into malignancy therapeutic interventions demand more aggressive and strategic management and prognostication. Historically, HPV+ OPC was generally treated with primary radiotherapy with or without chemotherapy. Approximately 30 to 40% of patients initially present with early-stage I/II OPC. These patients are typically treated with curative intent, employing either single-modality treatments such as radiotherapy with or without chemotherapy, or surgery alone. The decision between the two modalities is generally influenced by an evaluation of functional, cosmetic outcomes and competing morbidities, as both options yield comparable rates of local control and survival [172]. With advancements in surgical technology, minimally invasive techniques like transoral robotic surgery (TORS) or transoral laser microsurgery (TLMS) have emerged as the primary treatment modalities for patients diagnosed with early-stage OPC [173]. As TLMS and TORS are becoming surgical mainstream studies have shown that their efficacy have been impressive in early stage OPC, with 90% overall survival rates and 12% recurrence rate, largely within the first two years [174]. Up to 50% of fatalities in HNC are attributed to locoregionally recurrent disease as the exclusive site of failure [175]. Management strategies depend on primary treatment modalities. In cases where surgery serves as the primary treatment, adjuvant therapy is traditionally considered if positive or close margins, bone involvement, or pathologically positive lymph nodes are present. Risk stratification is key to designate patients into management options to achieve improved outcomes. Studies have shown that primary surgery without adjuvant therapy (chemoradiotherapy with concurrent cisplatin and post-operative radiotherapy) increases risk for recurrence [176]. However, it has been demonstrated that combined radio chemotherapy can further enhance outcomes in certain high-risk patients. For previously irradiated patients with potentially resectable recurrence, surgical resection is recommended. In cases where surgical salvage is not possible, alternatives encompass additional irradiation or palliative chemotherapy.
7.2.2. Post Operative and De-Escalation Adjuvant Therapy
In patients where adjuvant therapy is indicated, reduced radiation dose has also shown favorable reduction of treatment associated morbidity, especially swallowing. Additionally, in a study the irradiation of only at-risk neck sites and avoiding resected primary tumor sites has also demonstrated good overall survival [177].
Further, ongoing or recently concluded clinical trials (summarized in Table 1) like PATHOS (ID: NCT02215265), MINT (ID: NCT03621696), DELPHI (ID: NCT03396718), and ECOG3311, SIRS and DART are evaluating de-escalated adjuvant therapy [178,179,180]. The ECOG3311 study evaluated the efficacy of TORS and reduced postoperative radiotherapy in intermediate-risk HPV+ OPC, and found favorable oncologic outcomes in the target group [178]. The SIRS trial had similar favorable outcomes in utilizing reduced dose adjuvant radiotherapy for T1-N1 staged OPC post TORS [180]. Additionally, de-escalation of radiotherapy with or without concurrent chemotherapy, as well as stereotactic ablative radiotherapy or hypofractioned radiotherapy with de-escalated chemoradiotherapy is also being explored in clinical trials - ID: NCT04178174, NCT04580446 [181]. The Quarterback trials (ID: NCT01706939 and NCT02945631) are working towards exploring the effectiveness of reduced-dose radiotherapy in advanced-stage OPC (Stages III-IV).
Interestingly, initial exploration of management with either primary TLMS/TORS alone or primary chemoradiotherapy for HPV+OPC in the ORATOR trial did not demonstrate significantly improved survival outcomes, suggesting the need to present patients with both options concurrently [182,183]. Up to 25% patients undergo disease relapse within 2 years of initial diagnosis. Effective follow up and monitoring through examination every 1-3 months in the first year, 2-6 months in the second year and 4-8 months until 5 years is recommended by the National comprehensive Cancer Network [184].
7.2.3. Targeted Therapy, Immunotherapy & Therapeutic Vaccines
A phase 1 study combining (EGFR)/ErbB2 inhibitor afatinib, antiviral like ribavirin with induction chemotherapy (cisplatin), and weekly carboplatin and paclitaxel chemotherapy was well tolerated, with 75% 2-year progression-free survival rate . This initial promising approach is being explored further [185].
Several recently completed clinical trials have examined targeted therapy – anti-EGFR monoclonal antibody (Cetuximab), in combination with other treatment modalities, as an alternative to cisplatin (summarized in Table 1). In the De-ESCALaTE HPV (ID: ISRCTN33522080), a randomized phase 3 trial, cetuximab treatment arm was associated with no reduction in treatment associated toxicity or morbidity, lower overall survival and high recurrence rate during the 2-year timeline, in comparison to the cisplatin arm. This suggested the continued utilization of cisplatin and radiotherapy for management [186]. A second trial - NRG Oncology RTOG 1016 (ID: NCT01302834), also reported similar results. HPV+OPC patients who received cetuximab with radiotherapy showed inferior overall survival compared to the cisplatin and radiotherapy arm [187]. Genomic studies have shown that the difference in EGFR expression in HPV+ tumors compared to HPV- OPC may demonstrate the lack of efficacy with anti-EGFR monoclonal antibodies [188].
The utilization of immunotherapy in HPV+ cancers has been explored for over 20 years. In 2016, Pembrolizumab and nivolumab, two anti-PD-1 antibodies was approved for use in platinum-refractory metastatic HNC, while the former was approved as first-line monotherapy in PD-L1+ unresectable or metastatic HNC – both studies including HPV+ carcinomas [124,126,127]. Further studies branching from these three clinical trials explored the association of use of PD-L1 blockade with overall survival, objective response rates – described as either strong or inconclusive, highlighting the need for further research [189,190]. Several ongoing or recently completed clinical trials are investigating immune checkpoint inhibitors against HPV+OPC with standard of care therapy (Table 1). A phase 2 study (ID: NCT03799445) is exploring the safety, tolerability of anti-PD-1 antibody– Nivolumab and anti-CTLA4 antibody – Ipilimumab, in combination with low-intermediate volume radiation therapy for treating advanced HPV+OPC. A second phase II study (ID: NCT03410615) in intermediate risk HPV+ locoregionally advanced OPC is evaluating a combination cisplatin chemotherapy plus radiotherapy followed by anti-PD-L1 antibody – Durvalumab, versus radiotherapy plus Durvalumab followed by adjuvant Durvalumab and anti-CTLA-4 antibody – Tremelimumab. In a Phase III randomized, double blinded study, Atezolizumab, an anti-PD-L1 antibody is being explored as adjuvant therapy after definitive local therapy, for patients with high-risk locally advanced disease. Another randomized phase 2 trial (ID: NCT03669718) utilizing Cemiplimab, a anti-PD-1/PD-L1 antibody in HPV 16 + OPC, is investigating Cemiplimab Versus the Combination of Cemiplimab With ISA101b (a HPV 16 E6 and E7 synthetic peptide), for patients with PD-L1+ p16+ metastatic and/or recurrent disease.
Immunotherapy is also being explored for early stage, non-smoking HPV+ OPC. In a phase II/III trial (ID: NCT03952585), the anti-PD-1 antibody – Nivolumab is being investigated as a cisplatin replacement with de-intensified radiation therapy. In patients smoking history and locally advanced intermediate risk HPV+OPC, National Cancer Institute, a phase III randomized trial (ID: NCT03811015), is studying the maintenance therapy with anti-PD-1 antibody – Nivolumab versus observation.
E6/E7 based therapeutic vaccines, in combination with immunomodulatory agents are currently being explored in trials with patients with HPV+OPC. The HARE-40, phase I/II vaccine dose escalation study (ID: NCT03418480) is evaluating safety, tolerability and dosage of an E7-targeting mRNA vaccine in combination with anti-CD40 antibody – to enhance antigen presentation by dendritic cells against previously treated advanced HPV+OPC. In a phase II trial HPV 16 E6/E7 peptide vaccine, in combination with Nivolumab has demonstrated favorable outcomes [191]. Another E6/E7 DNA vaccine – MEDI0457, in combination with IL-12 has demonstrated potent peripheral and tumor immune response against locally advanced HPV+OPS, while suggesting its use as a complement to immune checkpoint blockade [176]. In a first human trial, phase I/II (ID: NCT04180215), the E6/E7-targeting single vector therapy - HB-201 and two-vector therapy – HB-202 is being examined across metastatic or recurrent HPV+OPC patients (otherwise eligible to receive pembrolizumab as standard care) through phase I and phase II dose expansions efforts, to achieve anti-cancer effects and understand its safety.
8. Conclusion
HPV have been long associated and co-evolved with humans, allowing adaptation to multiple epithelial anatomical niches, establishing robust infection, and in some cases furthering the infection state into carcinogenesis. HPV driven oncogenesis in the oropharynx presents a complex and unique molecular landscape, tumor microenvironment and immune response, in comparison to HPV- HNC. Recent epidemiology data has well documented the rapidly rising rates of HPV+OPC, paralleled with rising infection rates in high income countries. Prophylactic vaccination campaigns have also primarily focused on preventing cervical, vaginal, anal, penile cancers, and genital warts, although recent studies suggest that these vaccines may confer protection against oral HPV infections as well. Despite these successes, control in the rising HPV+ OPC, particularly among men, is not expected immediately, especially unless these campaigns robustly target vaccinations in men. While vaccinations, routine screening and early detection have led to milestone achievements in HPV+ cervical cancer, the lack of precursor lesions in OPC remains perplexing, indicating there remain key differences across local tissue ecology where HPV infection occurs and transition to malignancy. Recent therapeutic strategies from completed and ongoing clinical trials have improved survival outcomes in HPV+OPC, though significantly more trials are clearly needed to significantly reduce disease and therapy associated morbidity, and mortality. Rapid advances in the fields of multi-omics, epigenetics and imaging technologies are continuing to improve our understanding of oral and oropharyngeal HPV infection and associated oncogenesis, towards improving screening, early detection, triaging, risk stratification of patients for better outcome clinical management, and development of new therapeutic opportunities.
Author Contributions
Conceptualization, K.S.R.; Methodology, K.S.R.; Software, K.S.R.; Data Curation, K.S.R., V.R., and S.V.; Writing – Original Draft Preparation, K.S.R., V.R. and S.V; Writing – Review & Editing, K.S.R.; Visualization, K.S.R., V.R, and S.V.; Supervision, K.S.R.
References
- HPV and Cancer - NCI. Available online: https://www.cancer.gov/about-cancer/causes-prevention/risk/infectious-agents/hpv-and-cancer (accessed on 16 March 2024).
- Kreisel, K.M.; Spicknall, I.H.; Gargano, J.W.; Lewis, F.M.T.; Lewis, R.M.; Markowitz, L.E.; Roberts, H.; Johnson, A.S.; Song, R.; St. Cyr, S.B.; et al. Sexually Transmitted Infections Among US Women and Men: Prevalence and Incidence Estimates, 2018. Sex. Transm. Dis. 2021, 48, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Bzhalava, D.; Eklund, C.; Dillner, J. International Standardization and Classification of Human Papillomavirus Types. Virology 2015, 476, 341–344. [Google Scholar] [CrossRef] [PubMed]
- Psyrri, A.; DiMaio, D. Human Papillomavirus in Cervical and Head-and-Neck Cancer. Nat. Clin. Pract. Oncol. 2008, 5, 24–31. [Google Scholar] [CrossRef] [PubMed]
- De Martel, C.; Georges, D.; Bray, F.; Ferlay, J.; Clifford, G.M. Global Burden of Cancer Attributable to Infections in 2018: A Worldwide Incidence Analysis. Lancet Glob. Health 2020, 8, e180–e190. [Google Scholar] [CrossRef] [PubMed]
- Syrjänen, S.; Syrjänen, K. The History of Papillomavirus Research. Cent. Eur. J. Public Health 2008, 16 Suppl, S7–13. [Google Scholar] [CrossRef]
- Strauss, M.J.; Shaw, E.W.; Bunting, H.; Melnick, J.L. “Crystalline” Virus-Like Particles from Skin Papillomas Characterized by Intranuclear Inclusion Bodies. Exp. Biol. Med. 1949, 72, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Crawford, L.V. A Study of Human Papilloma Virus DNA. J. Mol. Biol. 1965, 13, 362–372. [Google Scholar] [CrossRef] [PubMed]
- Klug, A.; Finch, J.T. Structure of Viruses of the Papilloma-Polyoma Type. J. Mol. Biol. 1965, 11, 403–IN44. [Google Scholar] [CrossRef] [PubMed]
- Hausen, H.Z.; Meinhof, W.; Scheiber, W.; Bornkamm, G.W. Attempts to Detect Virus-specific DNA in Human Tumors. I. Nucleic Acid Hybridizations with Complementary RNA of Human Wart Virus. Int. J. Cancer 1974, 13, 650–656. [Google Scholar] [CrossRef]
- Orth, G.; Favre, M.; Croissant, O. Characterization of a New Type of Human Papillomavirus That Causes Skin Warts. J. Virol. 1977, 24, 108–120. [Google Scholar] [CrossRef]
- Zur Hausen, H. Papillomaviruses in the Causation of Human Cancers — a Brief Historical Account. Virology 2009, 384, 260–265. [Google Scholar] [CrossRef]
- Hausen, H. Oncogenic Herpes Viruses. Biochim. Biophys. Acta BBA - Rev. Cancer 1975, 417, 25–53. [Google Scholar] [CrossRef] [PubMed]
- zur Hausen, H. Condylomata Acuminata and Human Genital Cancer. Cancer Res. 1976, 36, 794. [Google Scholar] [PubMed]
- Zur Hausen, H. Human Papillomaviruses and Their Possible Role in Squamous Cell Carcinomas. In Current Topics in Microbiology and Immunology; Arber, W., Henle, W., Hofschneider, P.H., Humphrey, J.H., Klein, J., Koldovský, P., Koprowski, H., Maaløe, O., Melchers, F., Rott, R., Schweiger, H.G., Syruček, L., Vogt, P.K., Eds.; Springer Berlin Heidelberg: Berlin, Heidelberg, 1977; ISBN 978-3-642-66802-9. [Google Scholar]
- Dürst, M.; Gissmann, L.; Ikenberg, H.; Zur Hausen, H. A Papillomavirus DNA from a Cervical Carcinoma and Its Prevalence in Cancer Biopsy Samples from Different Geographic Regions. Proc. Natl. Acad. Sci. 1983, 80, 3812–3815. [Google Scholar] [CrossRef] [PubMed]
- Boshart, M.; Gissmann, L.; Ikenberg, H.; Kleinheinz, A.; Scheurlen, W.; Zur Hausen, H. A New Type of Papillomavirus DNA, Its Presence in Genital Cancer Biopsies and in Cell Lines Derived from Cervical Cancer. EMBO J. 1984, 3, 1151–1157. [Google Scholar] [CrossRef] [PubMed]
- Gissmann, L.; Diehl, V.; Schultz-Coulon, H.J.; Zur Hausen, H. Molecular Cloning and Characterization of Human Papilloma Virus DNA Derived from a Laryngeal Papilloma. J. Virol. 1982, 44, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Zachow, K.R.; Ostrow, R.S.; Bender, M.; Watts, S.; Okagaki, T.; Pass, F.; Faras, A.J. Detection of Human Papillomavirus DNA in Anogenital Neoplasias. Nature 1982, 300, 771–773. [Google Scholar] [CrossRef] [PubMed]
- Syrjänen, K.J.; Pyrhönen, S.; Syrjänen, S.M.; Lamberg, M.A. Immunohistochemical Demonstration of Human Papilloma Virus (HPV) Antigens in Oral Squamous Cell Lesions. Br. J. Oral Surg. 1983, 21, 147–153. [Google Scholar] [CrossRef]
- Löning, T.; Ikenberg, H.; Becker, J.; Gissmann, L.; Hoepfer, I.; Zur Hausen, H. Analysis of Oral Papillomas, Leukoplakias, and Invasive Carcinomas for Human Papillomavirus Type Related DNA. J. Invest. Dermatol. 1985, 84, 417–420. [Google Scholar] [CrossRef]
- De Villiers, E.-M.; Weidauer, H.; Otto, H.; Zur Hausen, H. Papillomavirus DNA in Human Tongue Carcinomas. Int. J. Cancer 1985, 36, 575–578. [Google Scholar] [CrossRef]
- Scheurlen, W.; Stremlau, A.; Gissmann, L.; Höhn, D.; Zenner, H.; Hausen, H.Z. Rearranged HPV 16 Molecules in an Anal and in a Laryngeal Carcinoma. Int. J. Cancer 1986, 38, 671–676. [Google Scholar] [CrossRef] [PubMed]
- Ikenberg, H.; Gissmann, L.; Gross, G.; Grussendorf-Conen, E.; Hausen, H.Z. Human Papillomavirus Type-16-related DNA in Genital Bowen’s Disease and in Bowenoid Papulosis. Int. J. Cancer 1983, 32, 563–565. [Google Scholar] [CrossRef] [PubMed]
- Frisch, M.; Fenger, C.; van den Brule, A.J.; Sørensen, P.; Meijer, C.J.; Walboomers, J.M.; Adami, H.O.; Melbye, M.; Glimelius, B. Variants of Squamous Cell Carcinoma of the Anal Canal and Perianal Skin and Their Relation to Human Papillomaviruses. Cancer Res. 1999, 59, 753–757. [Google Scholar]
- Rubin, M.A.; Kleter, B.; Zhou, M.; Ayala, G.; Cubilla, A.L.; Quint, W.G.V.; Pirog, E.C. Detection and Typing of Human Papillomavirus DNA in Penile Carcinoma. Am. J. Pathol. 2001, 159, 1211–1218. [Google Scholar] [CrossRef]
- Madsen, B.S.; Jensen, H.L.; Van Den Brule, A.J.C.; Wohlfahrt, J.; Frisch, M. Risk Factors for Invasive Squamous Cell Carcinoma of the Vulva and Vagina—Population-based Case–Control Study in Denmark. Int. J. Cancer 2008, 122, 2827–2834. [Google Scholar] [CrossRef] [PubMed]
- Newell, G.R.; Krementz, E.T.; Roberts, J.D. Excess Occurrence of Cancer of the Oral Cavity, Lung, and Bladder Following Cancer of the Cervix. Cancer 1975, 36, 2155–2158. [Google Scholar] [CrossRef]
- Syrjänen, S.; Rautava, J.; Syrjänen, K. HPV in Head and Neck Cancer—30 Years of History. In HPV Infection in Head and Neck Cancer; Golusiński, W., Leemans, C.R., Dietz, A., Eds.; Springer International Publishing: Cham, 2017; ISBN 978-3-319-43578-7. [Google Scholar]
- Syrjänen, S.M.; Syrjänen, K.J.; Happonen, R. Human Papillomavirus (HPV) DNA Sequences in Oral Precancerous Lesions and Squamous Cell Carcinoma Demonstrated by in Situ Hybridization. J. Oral Pathol. Med. 1988, 17, 273–278. [Google Scholar] [CrossRef]
- Snijders, P.J.F.; Cromme, F.V.; Van Brule, A.J.C.D.; Schrijnemakers, H.F.J.; Snow, G.B.; Meijer, C.J.L.M.; Walboomers, J.M.M. Prevalence and Expression of Human Papillomavirus in Tonsillar Carcinomas, Indicating a Possible Viral Etiology. Int. J. Cancer 1992, 51, 845–850. [Google Scholar] [CrossRef]
- Chang, F.; Syrjänen, S.; Nuutinen, J.; Kärjä, J.; Syrjänen, K. Detection of Human Papillomavirus (HPV) DNA in Oral Squamous Cell Carcinomas by in Situ Hybridization and Polymerase Chain Reaction. Arch. Dermatol. Res. 1990, 282, 493–497. [Google Scholar] [CrossRef]
- Kreimer, A.R.; Clifford, G.M.; Boyle, P.; Franceschi, S. Human Papillomavirus Types in Head and Neck Squamous Cell Carcinomas Worldwide: A Systematic Review. Cancer Epidemiol. Biomarkers Prev. 2005, 14, 467–475. [Google Scholar] [CrossRef]
- D’Souza, G.; Kreimer, A.R.; Viscidi, R.; Pawlita, M.; Fakhry, C.; Koch, W.M.; Westra, W.H.; Gillison, M.L. Case–Control Study of Human Papillomavirus and Oropharyngeal Cancer. N. Engl. J. Med. 2007, 356, 1944–1956. [Google Scholar] [CrossRef] [PubMed]
- Schache, A.G.; Powell, N.G.; Cuschieri, K.S.; Robinson, M.; Leary, S.; Mehanna, H.; Rapozo, D.; Long, A.; Cubie, H.; Junor, E.; et al. HPV-Related Oropharynx Cancer in the United Kingdom: An Evolution in the Understanding of Disease Etiology. Cancer Res. 2016, 76, 6598–6606. [Google Scholar] [CrossRef]
- Leemans, C.R.; Snijders, P.J.F.; Brakenhoff, R.H. The Molecular Landscape of Head and Neck Cancer. Nat. Rev. Cancer 2018, 18, 269–282. [Google Scholar] [CrossRef] [PubMed]
- Götz, C.; Bischof, C.; Wolff, K.-D.; Kolk, A. Detection of HPV Infection in Head and Neck Cancers: Promise and Pitfalls in the Last Ten Years: A Meta-Analysis. Mol. Clin. Oncol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Sabatini, M.E.; Chiocca, S. Human Papillomavirus as a Driver of Head and Neck Cancers. Br. J. Cancer 2020, 122, 306–314. [Google Scholar] [CrossRef]
- Faraji, F.; Rettig, E.M.; Tsai, H.; El Asmar, M.; Fung, N.; Eisele, D.W.; Fakhry, C. The Prevalence of Human Papillomavirus in Oropharyngeal Cancer Is Increasing Regardless of Sex or Race, and the Influence of Sex and Race on Survival Is Modified by Human Papillomavirus Tumor Status. Cancer 2019, 125, 761–769. [Google Scholar] [CrossRef] [PubMed]
- Zamani, M.; Grønhøj, C.; Jensen, D.H.; Carlander, A.F.; Agander, T.; Kiss, K.; Olsen, C.; Baandrup, L.; Nielsen, F.C.; Andersen, E.; et al. The Current Epidemic of HPV-Associated Oropharyngeal Cancer: An 18-Year Danish Population-Based Study with 2,169 Patients. Eur. J. Cancer 2020, 134, 52–59. [Google Scholar] [CrossRef]
- Del Mistro, A.; Frayle, H.; Menegaldo, A.; Favaretto, N.; Gori, S.; Nicolai, P.; Spinato, G.; Romeo, S.; Tirelli, G.; Da Mosto, M.C.; et al. Age-Independent Increasing Prevalence of Human Papillomavirus-Driven Oropharyngeal Carcinomas in North-East Italy. Sci. Rep. 2020, 10, 9320. [Google Scholar] [CrossRef]
- Wittekindt, C.; Wagner, S.; Bushnak, A.; Prigge, E.-S.; Von Knebel Doeberitz, M.; Würdemann, N.; Bernhardt, K.; Pons-Kühnemann, J.; Maulbecker-Armstrong, C.; Klussmann, J.P. Increasing Incidence Rates of Oropharyngeal Squamous Cell Carcinoma in Germany and Significance of Disease Burden Attributed to Human Papillomavirus. Cancer Prev. Res. (Phila. Pa.) 2019, 12, 375–382. [Google Scholar] [CrossRef]
- Haeggblom, L.; Attoff, T.; Yu, J.; Holzhauser, S.; Vlastos, A.; Mirzae, L.; Ährlund-Richter, A.; Munck-Wikland, E.; Marklund, L.; Hammarstedt-Nordenvall, L.; et al. Changes in Incidence and Prevalence of Human Papillomavirus in Tonsillar and Base of Tongue Cancer during 2000-2016 in the Stockholm Region and Sweden. Head Neck 2019, 41, 1583–1590. [Google Scholar] [CrossRef]
- Lechner, M.; Jones, O.S.; Breeze, C.E.; Gilson, R. Gender-Neutral HPV Vaccination in the UK, Rising Male Oropharyngeal Cancer Rates, and Lack of HPV Awareness. Lancet Infect. Dis. 2019, 19, 131–132. [Google Scholar] [CrossRef] [PubMed]
- Sathish, N.; Wang, X.; Yuan, Y. Human Papillomavirus (HPV)-Associated Oral Cancers and Treatment Strategies. J. Dent. Res. 2014, 93, 29S–36S. [Google Scholar] [CrossRef] [PubMed]
- Bruni, L.; Albero, G.; Rowley, J.; Alemany, L.; Arbyn, M.; Giuliano, A.R.; Markowitz, L.E.; Broutet, N.; Taylor, M. Global and Regional Estimates of Genital Human Papillomavirus Prevalence among Men: A Systematic Review and Meta-Analysis. Lancet Glob. Health 2023, 11, e1345–e1362. [Google Scholar] [CrossRef] [PubMed]
- Gillison, M.L.; D’Souza, G.; Westra, W.; Sugar, E.; Xiao, W.; Begum, S.; Viscidi, R. Distinct Risk Factor Profiles for Human Papillomavirus Type 16–Positive and Human Papillomavirus Type 16–Negative Head and Neck Cancers. JNCI J. Natl. Cancer Inst. 2008, 100, 407–420. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, G.; Wentz, A.; Kluz, N.; Zhang, Y.; Sugar, E.; Youngfellow, R.M.; Guo, Y.; Xiao, W.; Gillison, M.L. Sex Differences in Risk Factors and Natural History of Oral Human Papillomavirus Infection. J. Infect. Dis. 2016, 213, 1893–1896. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.Y.; Massa, S.; Mazul, A.L.; Kallogjeri, D.; Yaeger, L.; Jackson, R.S.; Zevallos, J.; Pipkorn, P. The Association of Smoking and Outcomes in HPV-Positive Oropharyngeal Cancer: A Systematic Review. Am. J. Otolaryngol. 2020, 41, 102592. [Google Scholar] [CrossRef]
- Sonawane, K.; Suk, R.; Chiao, E.Y.; Chhatwal, J.; Qiu, P.; Wilkin, T.; Nyitray, A.G.; Sikora, A.G.; Deshmukh, A.A. Oral Human Papillomavirus Infection: Differences in Prevalence Between Sexes and Concordance With Genital Human Papillomavirus Infection, NHANES 2011 to 2014. Ann. Intern. Med. 2017, 167, 714. [Google Scholar] [CrossRef]
- Petca, A.; Borislavschi, A.; Zvanca, M.; Petca, R.-C.; Sandru, F.; Dumitrascu, M. Non-Sexual HPV Transmission and Role of Vaccination for a Better Future (Review). Exp. Ther. Med. 2020, 20, 1–1. [Google Scholar] [CrossRef] [PubMed]
- Sexually Transmitted Diseases Among Gay and Bisexual Men | CDC. Available online: https://www.cdc.gov/msmhealth/STD.htm (accessed on 16 March 2024).
- Dahlstrom, K.R.; Burchell, A.N.; Ramanakumar, A.V.; Rodrigues, A.; Tellier, P.-P.; Hanley, J.; Coutlée, F.; Franco, E.L. Sexual Transmission of Oral Human Papillomavirus Infection among Men. Cancer Epidemiol. Biomarkers Prev. 2014, 23, 2959–2964. [Google Scholar] [CrossRef]
- Wierzbicka, M.; San Giorgi, M.R.M.; Dikkers, F.G. Transmission and Clearance of Human Papillomavirus Infection in the Oral Cavity and Its Role in Oropharyngeal Carcinoma – A Review. Rev. Med. Virol. 2023, 33, e2337. [Google Scholar] [CrossRef]
- Hemminki, K.; Dong, C.; Frisch, M. Tonsillar and Other Upper Aerodigestive Tract Cancers among Cervical Cancer Patients and Their Husbands: Eur. J. Cancer Prev. 2000, 9, 433–437. [Google Scholar] [CrossRef] [PubMed]
- Ryndock, E.J.; Meyers, C. A Risk for Non-Sexual Transmission of Human Papillomavirus? Expert Rev. Anti Infect. Ther. 2014, 12, 1165–1170. [Google Scholar] [CrossRef]
- Louvanto, K.; Roger, M.; Faucher, M.-C.; Syrjänen, K.; Grenman, S.; Syrjänen, S. HLA-G and Vertical Mother-to-Child Transmission of Human Papillomavirus Infection. Hum. Immunol. 2018, 79, 471–476. [Google Scholar] [CrossRef] [PubMed]
- Tucker, J.; Milici, J.; Alam, S.; Ferster, A.P.O.; Goldenberg, D.; Meyers, C.; Goyal, N. Assessing Nonsexual Transmission of the Human Papillomavirus (HPV): Do Our Current Cleaning Methods Work? J. Med. Virol. 2022, 94, 3956–3961. [Google Scholar] [CrossRef] [PubMed]
- Casalegno, J.; Le Bail Carval, K.; Eibach, D.; Valdeyron, M.-L.; Lamblin, G.; Jacquemoud, H.; Mellier, G.; Lina, B.; Gaucherand, P.; Mathevet, P.; et al. High Risk HPV Contamination of Endocavity Vaginal Ultrasound Probes: An Underestimated Route of Nosocomial Infection? PLoS ONE 2012, 7, e48137. [Google Scholar] [CrossRef] [PubMed]
- Termine, N.; Giovannelli, L.; Matranga, D.; Caleca, M.P.; Bellavia, C.; Perino, A.; Campisi, G. Oral Human Papillomavirus Infection in Women with Cervical HPV Infection: New Data from an Italian Cohort and a Metanalysis of the Literature. Oral Oncol. 2011, 47, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Freitas, A.C.; Mariz, F.C.; Silva, M.A.R.; Jesus, A.L.S. Human Papillomavirus Vertical Transmission: Review of Current Data. Clin. Infect. Dis. 2013, 56, 1451–1456. [Google Scholar] [CrossRef] [PubMed]
- Ardekani, A.; Taherifard, E.; Mollalo, A.; Hemadi, E.; Roshanshad, A.; Fereidooni, R.; Rouholamin, S.; Rezaeinejad, M.; Farid-Mojtahedi, M.; Razavi, M.; et al. Human Papillomavirus Infection during Pregnancy and Childhood: A Comprehensive Review. Microorganisms 2022, 10, 1932. [Google Scholar] [CrossRef] [PubMed]
- Fakhry, C.; Gillison, M.L.; D’Souza, G. Tobacco Use and Oral HPV-16 Infection. JAMA 2014, 312, 1465. [Google Scholar] [CrossRef]
- McBride, A.A. Human Papillomaviruses: Diversity, Infection and Host Interactions. Nat. Rev. Microbiol. 2022, 20, 95–108. [Google Scholar] [CrossRef]
- Antonsson, A.; Karanfilovska, S.; Lindqvist, P.G.; Hansson, B.G. General Acquisition of Human Papillomavirus Infections of Skin Occurs in Early Infancy. J. Clin. Microbiol. 2003, 41, 2509–2514. [Google Scholar] [CrossRef] [PubMed]
- Lambert, P.F.; Münger, K.; Rösl, F.; Hasche, D.; Tommasino, M. Beta Human Papillomaviruses and Skin Cancer. Nature 2020, 588, E20–E21. [Google Scholar] [CrossRef] [PubMed]
- Mergner, T.; Pompeiano, O. Single Unit Firing Patterns in the Vestibular Nuclei Related to Saccadic Eye Movement in the Decerebrate Cat. Arch. Ital. Biol. 1978, 116, 91–119. [Google Scholar] [PubMed]
- Luria, L.; Cardoza-Favarato, G. Human Papillomavirus. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2024. [Google Scholar]
- De Villiers, E.-M.; Fauquet, C.; Broker, T.R.; Bernard, H.-U.; Zur Hausen, H. Classification of Papillomaviruses. Virology 2004, 324, 17–27. [Google Scholar] [CrossRef] [PubMed]
- PaVE. Available online: https://pave.niaid.nih.gov/#home (accessed on 16 March 2024).
- Pereira, R.; Hitzeroth, I.I.; Rybicki, E.P. Insights into the Role and Function of L2, the Minor Capsid Protein of Papillomaviruses. Arch. Virol. 2009, 154, 187–197. [Google Scholar] [CrossRef] [PubMed]
- Buck, C.B.; Cheng, N.; Thompson, C.D.; Lowy, D.R.; Steven, A.C.; Schiller, J.T.; Trus, B.L. Arrangement of L2 within the Papillomavirus Capsid. J. Virol. 2008, 82, 5190–5197. [Google Scholar] [CrossRef] [PubMed]
- Bernard, H.; Calleja-Macias, I.E.; Dunn, S.T. Genome Variation of Human Papillomavirus Types: Phylogenetic and Medical Implications. Int. J. Cancer 2006, 118, 1071–1076. [Google Scholar] [CrossRef] [PubMed]
- Bernard, H.-U.; Chan, S.-Y.; Manos, M.M.; Ong, C.-K.; Villa, L.L.; Delius, H.; Peyton, C.L.; Bauer, H.M.; Wheeler, C.M. Identification and Assessment Of Known And Novel Human Papillomaviruses by Polymerase Chain Reaction Amplification, Restriction Fragment Length Polymorphisms, Nucleotide Sequence, and Phylogenetic Algorithms. J. Infect. Dis. 1994, 170, 1077–1085. [Google Scholar] [CrossRef]
- Doorbar, J. The Papillomavirus Life Cycle. J. Clin. Virol. 2005, 32, 7–15. [Google Scholar] [CrossRef]
- Fehrmann, F.; Laimins, L.A. Human Papillomaviruses: Targeting Differentiating Epithelial Cells for Malignant Transformation. Oncogene 2003, 22, 5201–5207. [Google Scholar] [CrossRef]
- Doorbar, J. Molecular Biology of Human Papillomavirus Infection and Cervical Cancer. Clin. Sci. 2006, 110, 525–541. [Google Scholar] [CrossRef]
- Hughes, F.J.; Romanos, M.A. E1 Protein of Human Papillomavirus Is a DNA Helicase/ATPase. Nucleic Acids Res. 1993, 21, 5817–5823. [Google Scholar] [CrossRef]
- Mohr, I.J.; Clark, R.; Sun, S.; Androphy, E.J.; MacPherson, P.; Botchan, M.R. Targeting the E1 Replication Protein to the Papillomavirus Origin of Replication by Complex Formation with the E2 Transactivator. Science 1990, 250, 1694–1699. [Google Scholar] [CrossRef]
- Thierry, F.; Yaniv, M. The BPV1-E2 Trans-Acting Protein Can Be Either an Activator or a Repressor of the HPV18 Regulatory Region. EMBO J. 1987, 6, 3391–3397. [Google Scholar] [CrossRef]
- Flores, E.R.; Allen-Hoffmann, B.L.; Lee, D.; Lambert, P.F. The Human Papillomavirus Type 16 E7 Oncogene Is Required for the Productive Stage of the Viral Life Cycle. J. Virol. 2000, 74, 6622–6631. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin-Drubin, M.E.; Bromberg-White, J.L.; Meyers, C. The Role of the Human Papillomavirus Type 18 E7 Oncoprotein during the Complete Viral Life Cycle. Virology 2005, 338, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Ferris, R.L.; Westra, W. Oropharyngeal Carcinoma with a Special Focus on HPV-Related Squamous Cell Carcinoma. Annu. Rev. Pathol. Mech. Dis. 2023, 18, 515–535. [Google Scholar] [CrossRef] [PubMed]
- Werness, B.A.; Levine, A.J.; Howley, P.M. Association of Human Papillomavirus Types 16 and 18 E6 Proteins with P53. Science 1990, 248, 76–79. [Google Scholar] [CrossRef]
- Scheffner, M.; Werness, B.A.; Huibregtse, J.M.; Levine, A.J.; Howley, P.M. The E6 Oncoprotein Encoded by Human Papillomavirus Types 16 and 18 Promotes the Degradation of P53. Cell 1990, 63, 1129–1136. [Google Scholar] [CrossRef]
- Boyer, S.N.; Wazer, D.E.; Band, V. E7 Protein of Human Papilloma Virus-16 Induces Degradation of Retinoblastoma Protein through the Ubiquitin-Proteasome Pathway. Cancer Res. 1996, 56, 4620–4624. [Google Scholar]
- Toledo, L.; Neelsen, K.J.; Lukas, J. Replication Catastrophe: When a Checkpoint Fails Because of Exhaustion. Mol. Cell 2017, 66, 735–749. [Google Scholar] [CrossRef]
- Hebner, C.M.; Laimins, L.A. Human Papillomaviruses: Basic Mechanisms of Pathogenesis and Oncogenicity. Rev. Med. Virol. 2006, 16, 83–97. [Google Scholar] [CrossRef]
- Zanier, K.; ould M’hamed ould Sidi, A.; Boulade-Ladame, C.; Rybin, V.; Chappelle, A.; Atkinson, A.; Kieffer, B.; Travé, G. Solution Structure Analysis of the HPV16 E6 Oncoprotein Reveals a Self-Association Mechanism Required for E6-Mediated Degradation of P53. Structure 2012, 20, 604–617. [Google Scholar] [CrossRef] [PubMed]
- Katzenellenbogen, R. Telomerase Induction in HPV Infection and Oncogenesis. Viruses 2017, 9, 180. [Google Scholar] [CrossRef]
- Boulet, G.; Horvath, C.; Broeck, D.V.; Sahebali, S.; Bogers, J. Human Papillomavirus: E6 and E7 Oncogenes. Int. J. Biochem. Cell Biol. 2007, 39, 2006–2011. [Google Scholar] [CrossRef]
- Rashid, N.N.; Rothan, H.A.; Yusoff, M.S.M. The Association of Mammalian DREAM Complex and HPV16 E7 Proteins. Am. J. Cancer Res. 2015, 5, 3525–3533. [Google Scholar] [PubMed]
- DiMaio, D.; Petti, L.M. The E5 Proteins. Virology 2013, 445, 99–114. [Google Scholar] [CrossRef]
- Valle, G.F.; Banks, L. The Human Papillomavirus (HPV)-6 and HPV-16 E5 Proteins Co-Operate with HPV-16 E7 in the Transformation of Primary Rodent Cells. J. Gen. Virol. 1995, 76, 1239–1245. [Google Scholar] [CrossRef] [PubMed]
- Owen, K.L.; Brockwell, N.K.; Parker, B.S. JAK-STAT Signaling: A Double-Edged Sword of Immune Regulation and Cancer Progression. Cancers 2019, 11, 2002. [Google Scholar] [CrossRef]
- Morgan, E.L.; Macdonald, A. Autocrine STAT3 Activation in HPV Positive Cervical Cancer through a Virus-Driven Rac1—NFκB—IL-6 Signalling Axis. PLOS Pathog. 2019, 15, e1007835. [Google Scholar] [CrossRef]
- Schröer, N.; Pahne, J.; Walch, B.; Wickenhauser, C.; Smola, S. Molecular Pathobiology of Human Cervical High-Grade Lesions: Paracrine STAT3 Activation in Tumor-Instructed Myeloid Cells Drives Local MMP-9 Expression. Cancer Res. 2011, 71, 87–97. [Google Scholar] [CrossRef]
- Bonilla-Delgado, J.; Bulut, G.; Liu, X.; Cortés-Malagón, E.M.; Schlegel, R.; Flores-Maldonado, C.; Contreras, R.G.; Chung, S.-H.; Lambert, P.F.; Üren, A.; et al. The E6 Oncoprotein from HPV16 Enhances the Canonical Wnt/β-Catenin Pathway in Skin Epidermis In Vivo. Mol. Cancer Res. 2012, 10, 250–258. [Google Scholar] [CrossRef] [PubMed]
- Nichols, A.C. High Frequency of Activating PIK3CA Mutations in Human Papillomavirus–Positive Oropharyngeal CancerPIK3CA in HPV+ Oropharyngeal Squamous Cell Carcinoma. JAMA Otolaryngol. Neck Surg. 2013, 139, 617. [Google Scholar] [CrossRef]
- Lui, V.W.Y.; Hedberg, M.L.; Li, H.; Vangara, B.S.; Pendleton, K.; Zeng, Y.; Lu, Y.; Zhang, Q.; Du, Y.; Gilbert, B.R.; et al. Frequent Mutation of the PI3K Pathway in Head and Neck Cancer Defines Predictive Biomarkers. Cancer Discov. 2013, 3, 761–769. [Google Scholar] [CrossRef]
- Hanna, G.J.; Kacew, A.; Chau, N.G.; Shivdasani, P.; Lorch, J.H.; Uppaluri, R.; Haddad, R.I.; MacConaill, L.E. Improved Outcomes in PI3K-Pathway-Altered Metastatic HPV Oropharyngeal Cancer. JCI Insight 2018, 3, e122799. [Google Scholar] [CrossRef]
- Jung, Y.-S.; Kato, I.; Kim, H.-R.C. A Novel Function of HPV16-E6/E7 in Epithelial–Mesenchymal Transition. Biochem. Biophys. Res. Commun. 2013, 435, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, I.S.; Lavorato-Rocha, A.M.; De M Maia, B.; Stiepcich, M.M.A.; De Carvalho, F.M.; Baiocchi, G.; Soares, F.A.; Rocha, R.M. Epithelial-Mesenchymal Transition-like Events in Vulvar Cancer and Its Relation with HPV. Br. J. Cancer 2013, 109, 184–194. [Google Scholar] [CrossRef]
- Maufort, J.P.; Genther Williams, S.M.; Pitot, H.C.; Lambert, P.F. Human Papillomavirus 16 E5 Oncogene Contributes to Two Stages of Skin Carcinogenesis. Cancer Res. 2007, 67, 6106–6112. [Google Scholar] [CrossRef]
- Scott, M.L.; Coleman, D.T.; Kelly, K.C.; Carroll, J.L.; Woodby, B.; Songock, W.K.; Cardelli, J.A.; Bodily, J.M. Human Papillomavirus Type 16 E5-Mediated Upregulation of Met in Human Keratinocytes. Virology 2018, 519, 1–11. [Google Scholar] [CrossRef]
- Coursey, T.L.; McBride, A.A. Hitchhiking of Viral Genomes on Cellular Chromosomes. Annu. Rev. Virol. 2019, 6, 275–296. [Google Scholar] [CrossRef]
- Steinbach, A.; Riemer, A.B. Immune Evasion Mechanisms of Human Papillomavirus: An Update. Int. J. Cancer 2018, 142, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Stanley, M.A. Epithelial Cell Responses to Infection with Human Papillomavirus. Clin. Microbiol. Rev. 2012, 25, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, A.R.; Ramalho, A.C.; Marques, M.; Ribeiro, D. The Interplay between Antiviral Signalling and Carcinogenesis in Human Papillomavirus Infections. Cancers 2020, 12, 646. [Google Scholar] [CrossRef] [PubMed]
- Stern, P.L. Harnessing Immunity for Therapy in Human Papillomavirus Driven Cancers. Tumour Virus Res. 2021, 11, 200212. [Google Scholar] [CrossRef] [PubMed]
- Schiller, J.; Lowy, D. Explanations for the High Potency of HPV Prophylactic Vaccines. Vaccine 2018, 36, 4768–4773. [Google Scholar] [CrossRef] [PubMed]
- Leiding, J.W.; Holland, S.M. Warts and All: Human Papillomavirus in Primary Immunodeficiencies. J. Allergy Clin. Immunol. 2012, 130, 1030–1048. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Park, J.W.; Pitot, H.C.; Lambert, P.F. Loss of Dependence on Continued Expression of the Human Papillomavirus 16 E7 Oncogene in Cervical Cancers and Precancerous Lesions Arising in Fanconi Anemia Pathway-Deficient Mice. mBio 2016, 7, e00628–16. [Google Scholar] [CrossRef]
- Cortese, M.S.; Ashrafi, G.H.; Campo, M.S. All 4 Di-leucine Motifs in the First Hydrophobic Domain of the E5 Oncoprotein of Human Papillomavirus Type 16 Are Essential for Surface MHC Class I Downregulation Activity and E5 Endomembrane Localization. Int. J. Cancer 2010, 126, 1675–1682. [Google Scholar] [CrossRef] [PubMed]
- DeCarlo, C.A.; Rosa, B.; Jackson, R.; Niccoli, S.; Escott, N.G.; Zehbe, I. Toll-Like Receptor Transcriptome in the HPV-Positive Cervical Cancer Microenvironment. Clin. Dev. Immunol. 2012, 2012, 1–9. [Google Scholar] [CrossRef]
- Karim, R.; Meyers, C.; Backendorf, C.; Ludigs, K.; Offringa, R.; Van Ommen, G.-J.B.; Melief, C.J.M.; Van Der Burg, S.H.; Boer, J.M. Human Papillomavirus Deregulates the Response of a Cellular Network Comprising of Chemotactic and Proinflammatory Genes. PLoS ONE 2011, 6, e17848. [Google Scholar] [CrossRef]
- Caberg, J.-H.; Hubert, P.; Herman, L.; Herfs, M.; Roncarati, P.; Boniver, J.; Delvenne, P. Increased Migration of Langerhans Cells in Response to HPV16 E6 and E7 Oncogene Silencing: Role of CCL20. Cancer Immunol. Immunother. 2009, 58, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Baudouin, R.; Hans, S.; Lisan, Q.; Morin, B.; Adimi, Y.; Martin, J.; Lechien, J.R.; Tartour, E.; Badoual, C. Prognostic Significance of the Microenvironment in Human Papillomavirus Oropharyngeal Carcinoma: A Systematic Review. The Laryngoscope 2024, 134, 1507–1516. [Google Scholar] [CrossRef] [PubMed]
- Saloura, V.; Izumchenko, E.; Zuo, Z.; Bao, R.; Korzinkin, M.; Ozerov, I.; Zhavoronkov, A.; Sidransky, D.; Bedi, A.; Hoque, M.O.; et al. Immune Profiles in Primary Squamous Cell Carcinoma of the Head and Neck. Oral Oncol. 2019, 96, 77–88. [Google Scholar] [CrossRef] [PubMed]
- Mandal, R.; Şenbabaoğlu, Y.; Desrichard, A.; Havel, J.J.; Dalin, M.G.; Riaz, N.; Lee, K.-W.; Ganly, I.; Hakimi, A.A.; Chan, T.A.; et al. The Head and Neck Cancer Immune Landscape and Its Immunotherapeutic Implications. JCI Insight 2016, 1. [Google Scholar] [CrossRef] [PubMed]
- Welters, M.J.P.; Ma, W.; Santegoets, S.J.A.M.; Goedemans, R.; Ehsan, I.; Jordanova, E.S.; Van Ham, V.J.; Van Unen, V.; Koning, F.; Van Egmond, S.I.; et al. Intratumoral HPV16-Specific T Cells Constitute a Type I–Oriented Tumor Microenvironment to Improve Survival in HPV16-Driven Oropharyngeal Cancer. Clin. Cancer Res. 2018, 24, 634–647. [Google Scholar] [CrossRef] [PubMed]
- Whitmarsh, A.; Pring, M.; Thomas, S.J.; Waylen, A.; Ness, A.R.; Dudding, T.; Pawlita, M.; Brenner, N.; Waterboer, T.; Schroeder, L. Survival Advantage in Patients with Human Papillomavirus-driven Oropharyngeal Cancer and Variation by Demographic Characteristics and Serologic Response: Findings from Head and Neck 5000. Cancer 2021, 127, 2442–2452. [Google Scholar] [CrossRef] [PubMed]
- Tosi, A.; Parisatto, B.; Menegaldo, A.; Spinato, G.; Guido, M.; Del Mistro, A.; Bussani, R.; Zanconati, F.; Tofanelli, M.; Tirelli, G.; et al. The Immune Microenvironment of HPV-Positive and HPV-Negative Oropharyngeal Squamous Cell Carcinoma: A Multiparametric Quantitative and Spatial Analysis Unveils a Rationale to Target Treatment-Naïve Tumors with Immune Checkpoint Inhibitors. J. Exp. Clin. Cancer Res. 2022, 41, 279. [Google Scholar] [CrossRef] [PubMed]
- Cohen, E.E.W.; Soulières, D.; Le Tourneau, C.; Dinis, J.; Licitra, L.; Ahn, M.-J.; Soria, A.; Machiels, J.-P.; Mach, N.; Mehra, R.; et al. Pembrolizumab versus Methotrexate, Docetaxel, or Cetuximab for Recurrent or Metastatic Head-and-Neck Squamous Cell Carcinoma (KEYNOTE-040): A Randomised, Open-Label, Phase 3 Study. The Lancet 2019, 393, 156–167. [Google Scholar] [CrossRef] [PubMed]
- Seiwert, T.Y.; Burtness, B.; Mehra, R.; Weiss, J.; Berger, R.; Eder, J.P.; Heath, K.; McClanahan, T.; Lunceford, J.; Gause, C.; et al. Safety and Clinical Activity of Pembrolizumab for Treatment of Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck (KEYNOTE-012): An Open-Label, Multicentre, Phase 1b Trial. Lancet Oncol. 2016, 17, 956–965. [Google Scholar] [CrossRef]
- Ferris, R.L.; Blumenschein, G.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.; Kasper, S.; Vokes, E.E.; Even, C.; et al. Nivolumab for Recurrent Squamous-Cell Carcinoma of the Head and Neck. N. Engl. J. Med. 2016, 375, 1856–1867. [Google Scholar] [CrossRef]
- Burtness, B.; Harrington, K.J.; Greil, R.; Soulières, D.; Tahara, M.; De Castro, G.; Psyrri, A.; Basté, N.; Neupane, P.; Bratland, Å.; et al. Pembrolizumab Alone or with Chemotherapy versus Cetuximab with Chemotherapy for Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck (KEYNOTE-048): A Randomised, Open-Label, Phase 3 Study. The Lancet 2019, 394, 1915–1928. [Google Scholar] [CrossRef] [PubMed]
- Combes, J.-D.; Dalstein, V.; Gheit, T.; Clifford, G.M.; Tommasino, M.; Clavel, C.; Lacau St Guily, J.; Franceschi, S. Prevalence of Human Papillomavirus in Tonsil Brushings and Gargles in Cancer-Free Patients: The SPLIT Study. Oral Oncol. 2017, 66, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Kreimer, A.R.; Bhatia, R.K.; Messeguer, A.L.; González, P.; Herrero, R.; Giuliano, A.R. Oral Human Papillomavirus in Healthy Individuals: A Systematic Review of the Literature. Sex. Transm. Dis. 2010, 37, 386–391. [Google Scholar] [CrossRef] [PubMed]
- Castellsagué, X.; Alemany, L.; Quer, M.; Halec, G.; Quirós, B.; Tous, S.; Clavero, O.; Alòs, L.; Biegner, T.; Szafarowski, T.; et al. HPV Involvement in Head and Neck Cancers: Comprehensive Assessment of Biomarkers in 3680 Patients. J. Natl. Cancer Inst. 2016, 108, djv403. [Google Scholar] [CrossRef] [PubMed]
- Rietbergen, M.M.; Brakenhoff, R.H.; Bloemena, E.; Witte, B.I.; Snijders, P.J.F.; Heideman, D.A.M.; Boon, D.; Koljenovic, S.; Baatenburg-de Jong, R.J.; Leemans, C.R. Human Papillomavirus Detection and Comorbidity: Critical Issues in Selection of Patients with Oropharyngeal Cancer for Treatment De-Escalation Trials. Ann. Oncol. 2013, 24, 2740–2745. [Google Scholar] [CrossRef] [PubMed]
- Steenbergen, R.D.M.; Snijders, P.J.F.; Heideman, D.A.M.; Meijer, C.J.L.M. Clinical Implications of (Epi)Genetic Changes in HPV-Induced Cervical Precancerous Lesions. Nat. Rev. Cancer 2014, 14, 395–405. [Google Scholar] [CrossRef] [PubMed]
- Herfs, M.; Yamamoto, Y.; Laury, A.; Wang, X.; Nucci, M.R.; McLaughlin-Drubin, M.E.; Münger, K.; Feldman, S.; McKeon, F.D.; Xian, W.; et al. A Discrete Population of Squamocolumnar Junction Cells Implicated in the Pathogenesis of Cervical Cancer. Proc. Natl. Acad. Sci. 2012, 109, 10516–10521. [Google Scholar] [CrossRef] [PubMed]
- Woods, R.S.R.; Keegan, H.; White, C.; Tewari, P.; Toner, M.; Kennedy, S.; O’Regan, E.M.; Martin, C.M.; Timon, C.V.I.; O’Leary, J.J. Cytokeratin 7 in Oropharyngeal Squamous Cell Carcinoma: A Junctional Biomarker for Human Papillomavirus–Related Tumors. Cancer Epidemiol. Biomarkers Prev. 2017, 26, 702–710. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.Y.C.; Kannan, N.; Zhang, L.; Martinez, V.; Rosin, M.P.; Eaves, C.J. Characterization of Epithelial Progenitors in Normal Human Palatine Tonsils and Their HPV16 E6/E7-Induced Perturbation. Stem Cell Rep. 2015, 5, 1210–1225. [Google Scholar] [CrossRef]
- Syrjänen, S. Oral Manifestations of Human Papillomavirus Infections. Eur. J. Oral Sci. 2018, 126, 49–66. [Google Scholar] [CrossRef]
- Tezal, M.; Sullivan Nasca, M.; Stoler, D.L.; Melendy, T.; Hyland, A.; Smaldino, P.J.; Rigual, N.R.; Loree, T.R. Chronic Periodontitis−Human Papillomavirus Synergy in Base of Tongue Cancers. Arch. Otolaryngol. Neck Surg. 2009, 135, 391. [Google Scholar] [CrossRef] [PubMed]
- Fiorillo, L.; Cervino, G.; Surace, G.; De Stefano, R.; Laino, L.; D’Amico, C.; Fiorillo, M.T.; Meto, A.; Herford, A.S.; Arzukanyan, A.V.; et al. Human Papilloma Virus: Current Knowledge and Focus on Oral Health. BioMed Res. Int. 2021, 2021, 1–10. [Google Scholar] [CrossRef] [PubMed]
- McIlwain, W.R.; Sood, A.J.; Nguyen, S.A.; Day, T.A. Initial Symptoms in Patients With HPV-Positive and HPV-Negative Oropharyngeal Cancer. JAMA Otolaryngol. Neck Surg. 2014, 140, 441. [Google Scholar] [CrossRef] [PubMed]
- Khalid, M.B.; Ting, P.; Pai, A.; Russo, J.L.; Bakst, R.; Chai, R.L.; Teng, M.S.; Genden, E.M.; Miles, B.A. Initial Presentation of Human Papillomavirus-related Head and Neck Cancer: A Retrospective Review. The Laryngoscope 2019, 129, 877–882. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.S. P16 Immunohistochemistry As a Standalone Test for Risk Stratification in Oropharyngeal Squamous Cell Carcinoma. Head Neck Pathol. 2012, 6, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Fakhry, C.; Ferris, R.L. P16 as a Prognostic Biomarker for Nonoropharyngeal Squamous Cell Cancers: Avatar or Mirage? Natl. Cancer Inst. 2018. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.M.; Rubenstein, L.M.; Hoffman, H.; Haugen, T.H.; Turek, L.P. Human Papillomavirus, P16 and P53 Expression Associated with Survival of Head and Neck Cancer. Infect. Agent. Cancer 2010, 5, 4. [Google Scholar] [CrossRef] [PubMed]
- Gage, K.L.; Thomas, K.; Jeong, D.; Stallworth, D.G.; Arrington, J.A. Multimodal Imaging of Head and Neck Squamous Cell Carcinoma. Cancer Control 2017, 24, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Lechner, M.; Liu, J.; Masterson, L.; Fenton, T.R. HPV-Associated Oropharyngeal Cancer: Epidemiology, Molecular Biology and Clinical Management. Nat. Rev. Clin. Oncol. 2022, 19, 306–327. [Google Scholar] [CrossRef]
- Bryne, M.; Koppang, H.S.; Lilleng, R.; Kjærheim, Å. Malignancy Grading of the Deep Invasive Margins of Oral Squamous Cell Carcinomas Has High Prognostic Value. J. Pathol. 1992, 166, 375–381. [Google Scholar] [CrossRef]
- Kreimer, A.R.; Shiels, M.S.; Fakhry, C.; Johansson, M.; Pawlita, M.; Brennan, P.; Hildesheim, A.; Waterboer, T. Screening for Human Papillomavirus-driven Oropharyngeal Cancer: Considerations for Feasibility and Strategies for Research. Cancer 2018, 124, 1859–1866. [Google Scholar] [CrossRef]
- Jemal, A.; Simard, E.P.; Dorell, C.; Noone, A.-M.; Markowitz, L.E.; Kohler, B.; Eheman, C.; Saraiya, M.; Bandi, P.; Saslow, D.; et al. Annual Report to the Nation on the Status of Cancer, 1975–2009, Featuring the Burden and Trends in Human Papillomavirus (HPV)–Associated Cancers and HPV Vaccination Coverage Levels. JNCI J. Natl. Cancer Inst. 2013, 105, 175–201. [Google Scholar] [CrossRef] [PubMed]
- Agalliu, I.; Gapstur, S.; Chen, Z.; Wang, T.; Anderson, R.L.; Teras, L.; Kreimer, A.R.; Hayes, R.B.; Freedman, N.D.; Burk, R.D. Associations of Oral α-, β-, and γ-Human Papillomavirus Types With Risk of Incident Head and Neck Cancer. JAMA Oncol. 2016, 2, 599. [Google Scholar] [CrossRef] [PubMed]
- Gipson, B.J.; Robbins, H.A.; Fakhry, C.; D’Souza, G. Sensitivity and Specificity of Oral HPV Detection for HPV-Positive Head and Neck Cancer. Oral Oncol. 2018, 77, 52–56. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, G.; Clemens, G.; Troy, T.; Castillo, R.G.; Struijk, L.; Waterboer, T.; Bender, N.; Pierorazio, P.M.; Best, S.R.; Strickler, H.; et al. Evaluating the Utility and Prevalence of HPV Biomarkers in Oral Rinses and Serology for HPV-Related Oropharyngeal Cancer. Cancer Prev. Res. (Phila. Pa.) 2019, 12, 689–700. [Google Scholar] [CrossRef] [PubMed]
- Anantharaman, D.; Gheit, T.; Waterboer, T.; Abedi-Ardekani, B.; Carreira, C.; McKay-Chopin, S.; Gaborieau, V.; Marron, M.; Lagiou, P.; Ahrens, W.; et al. Human Papillomavirus Infections and Upper Aero-Digestive Tract Cancers: The ARCAGE Study. JNCI J. Natl. Cancer Inst. 2013, 105, 536–545. [Google Scholar] [CrossRef] [PubMed]
- Chera, B.S.; Kumar, S.; Shen, C.; Amdur, R.J.; Dagan, R.; Weiss, J.; Grilley-Olson, J.; Zanation, A.; Hackman, T.; Blumberg, J.; et al. Plasma Circulating Tumor HPV DNA for the Surveillance of Cancer Recurrence in HPV-Associated Oropharyngeal Cancer. Int. J. Radiat. Oncol. 2018, 102, 1605–1606. [Google Scholar] [CrossRef]
- Day, A.T.; Fakhry, C.; Tiro, J.A.; Dahlstrom, K.R.; Sturgis, E.M. Considerations in Human Papillomavirus–Associated Oropharyngeal Cancer Screening: A Review. JAMA Otolaryngol. Neck Surg. 2020, 146, 656. [Google Scholar] [CrossRef]
- Srinivasan Rajsri, K.; K. Durab, S.; A. Varghese, I.; Vigneswaran, N.; T. McDevitt, J.; Kerr, A.R. A Brief Review of Cytology in Dentistry. Br. Dent. J. 2024, 236, 329–336. [Google Scholar] [CrossRef]
- Broglie, M.A.; Jochum, W.; Förbs, D.; Schönegg, R.; Stoeckli, S.J. Brush Cytology for the Detection of High-risk HPV Infection in Oropharyngeal Squamous Cell Carcinoma. Cancer Cytopathol. 2015, 123, 732–738. [Google Scholar] [CrossRef]
- Castillo, P.; De La Oliva, J.; Alos, S.; Perez, F.; Vega, N.; Vilaseca, I.; Marti, C.; Ferrer, A.; Alos, L. Accuracy of Liquid-Based Brush Cytology and HPV Detection for the Diagnosis and Management of Patients with Oropharyngeal and Oral Cancer. Clin. Oral Investig. 2022, 26, 2587–2595. [Google Scholar] [CrossRef] [PubMed]
- Benevolo, M.; Rollo, F.; Giuliani, M.; Pichi, B.; Latini, A.; Pellini, R.; Vescio, M.F.; Morrone, A.; Cristaudo, A.; Donà, M.G. Abnormal Cytology in Oropharyngeal Brushings and in Oral Rinses Is Not Associated with HPV Infection: The OHMAR Study. Cancer Cytopathol. 2020, 128, 648–655. [Google Scholar] [CrossRef] [PubMed]
- Lingen, M.W. Brush-Based Cytology Screening in the Tonsils and Cervix: There Is a Difference! Cancer Prev. Res. (Phila. Pa.) 2011, 4, 1350–1352. [Google Scholar] [CrossRef] [PubMed]
- Boda, D.; Docea, A.O.; Calina, D.; Ilie, M.A.; Caruntu, C.; Zurac, S.; Neagu, M.; Constantin, C.; Branisteanu, D.E.; Voiculescu, V.; et al. Human Papilloma Virus: Apprehending the Link with Carcinogenesis and Unveiling New Research Avenues (Review). Int. J. Oncol. 2018, 52, 637–655. [Google Scholar] [CrossRef] [PubMed]
- Quadrivalent Human Papillomavirus Vaccine Recommendations of the Advisory Committee on Immunization Practices (ACIP). Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/rr5602a1.htm (accessed on 17 March 2024).
- Joura, E.A.; Giuliano, A.R.; Iversen, O.-E.; Bouchard, C.; Mao, C.; Mehlsen, J.; Moreira, E.D.; Ngan, Y.; Petersen, L.K.; Lazcano-Ponce, E.; et al. A 9-Valent HPV Vaccine against Infection and Intraepithelial Neoplasia in Women. N. Engl. J. Med. 2015, 372, 711–723. [Google Scholar] [CrossRef]
- Research, C. for B.E. and Cervarix. FDA 2022.
- HPV Vaccination Recommendations | CDC. Available online: https://www.cdc.gov/vaccines/vpd/hpv/hcp/recommendations.html (accessed on 17 March 2024).
- Pinto, L.A.; Kemp, T.J.; Torres, B.N.; Isaacs-Soriano, K.; Ingles, D.; Abrahamsen, M.; Pan, Y.; Lazcano-Ponce, E.; Salmeron, J.; Giuliano, A.R. Quadrivalent Human Papillomavirus (HPV) Vaccine Induces HPV-Specific Antibodies in the Oral Cavity: Results From the Mid-Adult Male Vaccine Trial. J. Infect. Dis. 2016, 214, 1276–1283. [Google Scholar] [CrossRef] [PubMed]
- Hirth, J.M.; Chang, M.; Resto, V.A.; Guo, F.; Berenson, A.B. Prevalence of Oral Human Papillomavirus by Vaccination Status among Young Adults (18–30 Years Old). Vaccine 2017, 35, 3446–3451. [Google Scholar] [CrossRef]
- Parker, K.H.; Kemp, T.J.; Pan, Y.; Yang, Z.; Giuliano, A.R.; Pinto, L.A. Evaluation of HPV-16 and HPV-18 Specific Antibody Measurements in Saliva Collected in Oral Rinses and Merocel® Sponges. Vaccine 2018, 36, 2705–2711. [Google Scholar] [CrossRef]
- Ahn, J.; Peng, S.; Hung, C.; Roden, R.B.S.; Best, S.R. Prophylactic Immunization with Human Papillomavirus Vaccines Induces Oral Immunity in Mice. The Laryngoscope 2018, 128. [Google Scholar] [CrossRef]
- Zhai, L.; Yadav, R.; Kunda, N.K.; Anderson, D.; Bruckner, E.; Miller, E.K.; Basu, R.; Muttil, P.; Tumban, E. Oral Immunization with Bacteriophage MS2-L2 VLPs Protects against Oral and Genital Infection with Multiple HPV Types Associated with Head & Neck Cancers and Cervical Cancer. Antiviral Res. 2019, 166, 56–65. [Google Scholar] [CrossRef]
- Carmona Lorduy, M.; Harris Ricardo, J.; Hernández Arenas, Y.; Medina Carmona, W. Use of Trichloroacetic Acid for Management of Oral Lesions Caused by Human Papillomavirus. Gen. Dent. 2018, 66, 47–49. [Google Scholar] [PubMed]
- Méndez-Flores, S.; Esquivel-Pedraza, L.; Hernández-Salazar, A.; Charli-Joseph, Y.; Saeb-Lima, M. Focal Epithelial Hyperplasia in Adult Patients With HIV Infection: Clearance With Topical Imiquimod. Skinmed 2016, 14, 395–397. [Google Scholar] [PubMed]
- Cooper, J.S.; Pajak, T.F.; Forastiere, A.A.; Jacobs, J.; Campbell, B.H.; Saxman, S.B.; Kish, J.A.; Kim, H.E.; Cmelak, A.J.; Rotman, M.; et al. Postoperative Concurrent Radiotherapy and Chemotherapy for High-Risk Squamous-Cell Carcinoma of the Head and Neck. N. Engl. J. Med. 2004, 350, 1937–1944. [Google Scholar] [CrossRef] [PubMed]
- Lechner, M.; Liu, J.; Masterson, L.; Fenton, T.R. HPV-Associated Oropharyngeal Cancer: Epidemiology, Molecular Biology and Clinical Management. Nat. Rev. Clin. Oncol. 2022, 19, 306–327. [Google Scholar] [CrossRef] [PubMed]
- Sinha, P.; Haughey, B.H.; Kallogjeri, D.; Jackson, R.S. Long-term Analysis of Transorally Resected P16 + Oropharynx Cancer: Outcomes and Prognostic Factors. The Laryngoscope 2019, 129, 1141–1149. [Google Scholar] [CrossRef] [PubMed]
- Goon, P.K.; Stanley, M.A.; Ebmeyer, J.; Steinsträsser, L.; Upile, T.; Jerjes, W.; Bernal-Sprekelsen, M.; Görner, M.; Sudhoff, H.H. HPV & Head and Neck Cancer: A Descriptive Update. Head Neck Oncol. 2009, 1, 36. [Google Scholar] [CrossRef] [PubMed]
- Carey, R.M.; Shimunov, D.; Weinstein, G.S.; Cannady, S.B.; Lukens, J.N.; Lin, A.; Swisher-McClure, S.; Bauml, J.M.; Aggarwal, C.; Cohen, R.B.; et al. Increased Rate of Recurrence and High Rate of Salvage in Patients with Human Papillomavirus–Associated Oropharyngeal Squamous Cell Carcinoma with Adverse Features Treated with Primary Surgery without Recommended Adjuvant Therapy. Head Neck 2021, 43, 1128–1141. [Google Scholar] [CrossRef]
- Swisher-McClure, S.; Lukens, J.N.; Aggarwal, C.; Ahn, P.; Basu, D.; Bauml, J.M.; Brody, R.; Chalian, A.; Cohen, R.B.; Fotouhi-Ghiam, A.; et al. A Phase 2 Trial of Alternative Volumes of Oropharyngeal Irradiation for De-Intensification (AVOID): Omission of the Resected Primary Tumor Bed After Transoral Robotic Surgery for Human Papilloma Virus–Related Squamous Cell Carcinoma of the Oropharynx. Int. J. Radiat. Oncol. 2020, 106, 725–732. [Google Scholar] [CrossRef] [PubMed]
- Ferris, R.L.; Flamand, Y.; Weinstein, G.S.; Li, S.; Quon, H.; Mehra, R.; Garcia, J.J.; Chung, C.H.; Gillison, M.L.; Duvvuri, U.; et al. Phase II Randomized Trial of Transoral Surgery and Low-Dose Intensity Modulated Radiation Therapy in Resectable P16+ Locally Advanced Oropharynx Cancer: An ECOG-ACRIN Cancer Research Group Trial (E3311). J. Clin. Oncol. 2022, 40, 138–149. [Google Scholar] [CrossRef]
- Ma, D.M.; Price, K.; Moore, E.J.; Patel, S.H.; Hinni, M.L.; Fruth, B.; Foster, N.R.; Van Abel, K.; Yin, L.X.; Neben-Wittich, M.A.; et al. MC1675, a Phase III Evaluation of De-Escalated Adjuvant Radiation Therapy (DART) vs. Standard Adjuvant Treatment for Human Papillomavirus Associated Oropharyngeal Squamous Cell Carcinoma. Int. J. Radiat. Oncol. 2021, 111, 1324. [Google Scholar] [CrossRef]
- Miles, B.A.; Posner, M.R.; Gupta, V.; Teng, M.S.; Bakst, R.L.; Yao, M.; Misiukiewicz, K.J.; Chai, R.L.; Sharma, S.; Westra, W.H.; et al. De-Escalated Adjuvant Therapy After Transoral Robotic Surgery for Human Papillomavirus-Related Oropharyngeal Carcinoma: The Sinai Robotic Surgery (SIRS) Trial. The Oncologist 2021, 26, 504–513. [Google Scholar] [CrossRef]
- Bratman, S.V.; Berthelet, E.; Butler, J.B.; De Almeida, J.R.; Karam, I.; Metser, U.; Olson, R.A.; Pochini, C.; Waldron, J.; Yu, E.; et al. CCTG HN.10: A Phase II Single-Arm Trial of Elective Volume Adjusted de-Escalation Radiotherapy (EVADER) in Patients with Low-Risk HPV-Related Oropharyngeal Squamous Cell Carcinoma (NCT03822897). J. Clin. Oncol. 2020, 38, TPS6592–TPS6592. [Google Scholar] [CrossRef]
- Nichols, A.C.; Theurer, J.; Prisman, E.; Read, N.; Berthelet, E.; Tran, E.; Fung, K.; De Almeida, J.R.; Bayley, A.; Goldstein, D.P.; et al. Radiotherapy versus Transoral Robotic Surgery and Neck Dissection for Oropharyngeal Squamous Cell Carcinoma (ORATOR): An Open-Label, Phase 2, Randomised Trial. Lancet Oncol. 2019, 20, 1349–1359. [Google Scholar] [CrossRef]
- Howard, J.; Masterson, L.; Dwivedi, R.C.; Riffat, F.; Benson, R.; Jefferies, S.; Jani, P.; Tysome, J.R.; Nutting, C. Minimally Invasive Surgery versus Radiotherapy/Chemoradiotherapy for Small-Volume Primary Oropharyngeal Carcinoma. Cochrane Database Syst. Rev. 2016, 2016. [Google Scholar] [CrossRef]
- INTEGRATE (The UK ENT Trainee Research Network) Post-Treatment Head and Neck Cancer Care: National Audit and Analysis of Current Practice in the United Kingdom. Clin. Otolaryngol. 2021, 46, 284–294. [CrossRef] [PubMed]
- Dunn, L.A.; Fury, M.G.; Sherman, E.J.; Ho, A.A.; Katabi, N.; Haque, S.S.; Pfister, D.G. Phase I Study of Induction Chemotherapy with Afatinib, Ribavirin, and Weekly Carboplatin and Paclitaxel for Stage IVA/IVB Human Papillomavirus-associated Oropharyngeal Squamous Cell Cancer. Head Neck 2018, 40, 233–241. [Google Scholar] [CrossRef]
- Mehanna, H.; Robinson, M.; Hartley, A.; Kong, A.; Foran, B.; Fulton-Lieuw, T.; Dalby, M.; Mistry, P.; Sen, M.; O’Toole, L.; et al. Radiotherapy plus Cisplatin or Cetuximab in Low-Risk Human Papillomavirus-Positive Oropharyngeal Cancer (De-ESCALaTE HPV): An Open-Label Randomised Controlled Phase 3 Trial. The Lancet 2019, 393, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Gillison, M.L.; Trotti, A.M.; Harris, J.; Eisbruch, A.; Harari, P.M.; Adelstein, D.J.; Jordan, R.C.K.; Zhao, W.; Sturgis, E.M.; Burtness, B.; et al. Radiotherapy plus Cetuximab or Cisplatin in Human Papillomavirus-Positive Oropharyngeal Cancer (NRG Oncology RTOG 1016): A Randomised, Multicentre, Non-Inferiority Trial. The Lancet 2019, 393, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Seiwert, T.Y.; Zuo, Z.; Keck, M.K.; Khattri, A.; Pedamallu, C.S.; Stricker, T.; Brown, C.; Pugh, T.J.; Stojanov, P.; Cho, J.; et al. Integrative and Comparative Genomic Analysis of HPV-Positive and HPV-Negative Head and Neck Squamous Cell Carcinomas. Clin. Cancer Res. 2015, 21, 632–641. [Google Scholar] [CrossRef]
- Galvis, M.M.; Borges, G.A.; Oliveira, T.B.D.; Toledo, I.P.D.; Castilho, R.M.; Guerra, E.N.S.; Kowalski, L.P.; Squarize, C.H. Immunotherapy Improves Efficacy and Safety of Patients with HPV Positive and Negative Head and Neck Cancer: A Systematic Review and Meta-Analysis. Crit. Rev. Oncol. Hematol. 2020, 150, 102966. [Google Scholar] [CrossRef]
- Xu, Y.; Zhu, G.; Maroun, C.A.; Wu, I.X.Y.; Huang, D.; Seiwert, T.Y.; Liu, Y.; Mandal, R.; Zhang, X. Programmed Death-1/Programmed Death-Ligand 1-Axis Blockade in Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma Stratified by Human Papillomavirus Status: A Systematic Review and Meta-Analysis. Front. Immunol. 2021, 12, 645170. [Google Scholar] [CrossRef] [PubMed]
- Massarelli, E.; William, W.; Johnson, F.; Kies, M.; Ferrarotto, R.; Guo, M.; Feng, L.; Lee, J.J.; Tran, H.; Kim, Y.U.; et al. Combining Immune Checkpoint Blockade and Tumor-Specific Vaccine for Patients With Incurable Human Papillomavirus 16–Related Cancer: A Phase 2 Clinical Trial. JAMA Oncol. 2019, 5, 67. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
A schematic of the HPV driven oropharyngeal epithelial infection and carcinogenesis. The oropharyngeal anatomy involving the soft palate, palatine tonsil, posterior pharyngeal wall and lingual tonsil may be sites for HPV infection, largely sexual transmission (A). HPV infection of the oropharyngeal epithelium in B describes the life cycle and key viral proteins involved in its genome maintenance, replication, maturation, virion assembly and shedding across the various host squamous stratified epithelial cells layers (viral copy number is higher in the superficial layer and reduces towards the basal epithelial layer). In most individuals, HPV infection clearance occurs naturally without any further consequence (C). In some individuals HPV infection may persist for years without further changes (D). Further, in some individuals persistent E6/E7 driven clonal selection and expansion (among other viral proteins) can drive malignant transformation (E). Figure created using Biorender.com.
Figure 1.
A schematic of the HPV driven oropharyngeal epithelial infection and carcinogenesis. The oropharyngeal anatomy involving the soft palate, palatine tonsil, posterior pharyngeal wall and lingual tonsil may be sites for HPV infection, largely sexual transmission (A). HPV infection of the oropharyngeal epithelium in B describes the life cycle and key viral proteins involved in its genome maintenance, replication, maturation, virion assembly and shedding across the various host squamous stratified epithelial cells layers (viral copy number is higher in the superficial layer and reduces towards the basal epithelial layer). In most individuals, HPV infection clearance occurs naturally without any further consequence (C). In some individuals HPV infection may persist for years without further changes (D). Further, in some individuals persistent E6/E7 driven clonal selection and expansion (among other viral proteins) can drive malignant transformation (E). Figure created using Biorender.com.
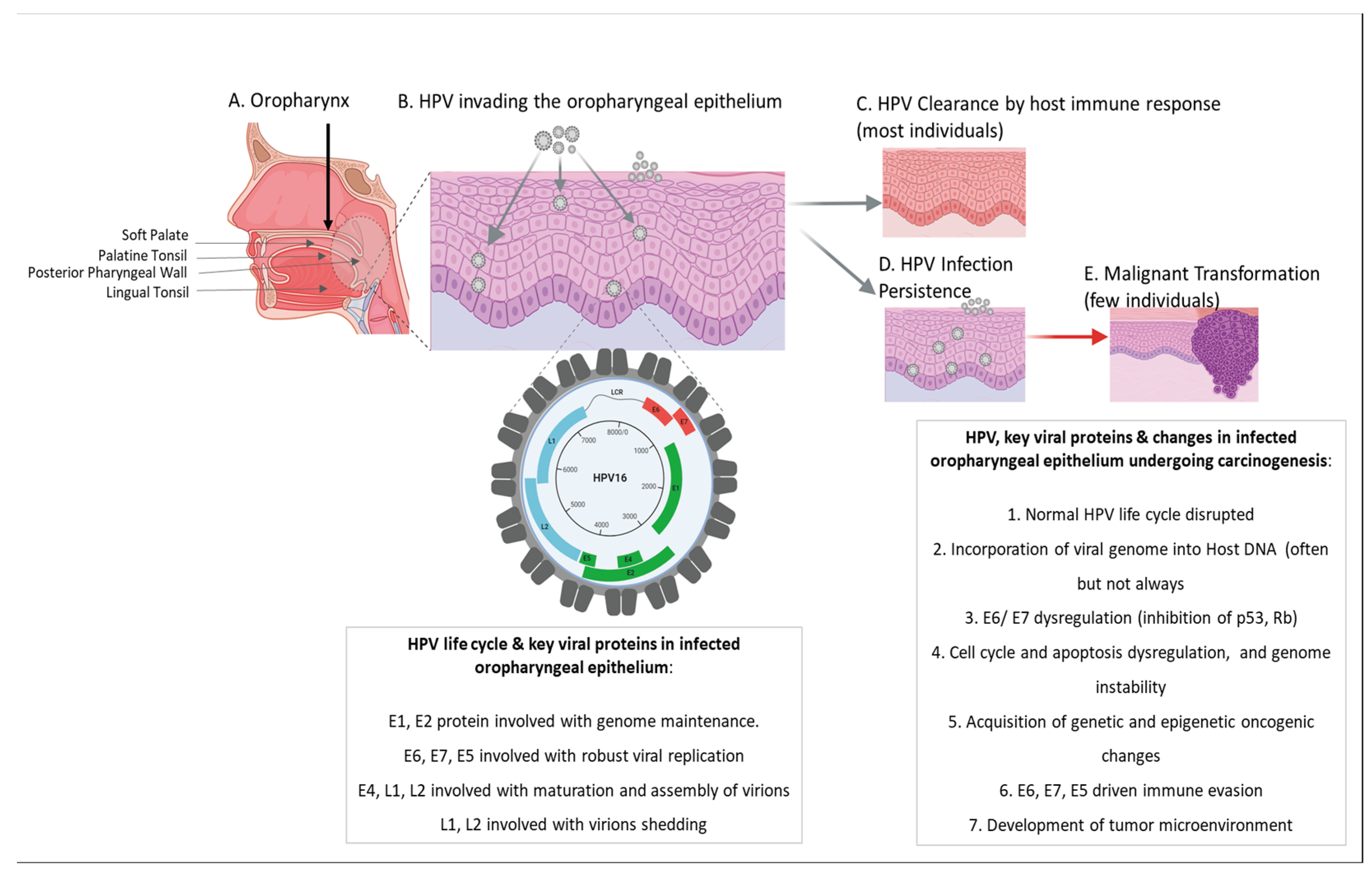

Table 1.
Summary of key ongoing and recently completed clinical trials, covering de-escalated adjuvant therapy, targeted therapy, immunotherapy and therapeutic vaccines, for HPV+ OPC.
Table 1.
Summary of key ongoing and recently completed clinical trials, covering de-escalated adjuvant therapy, targeted therapy, immunotherapy and therapeutic vaccines, for HPV+ OPC.
| CATEGORY | TRIAL ID | SUBJECTS | TREATMENT | OUTCOME | STATUS |
|---|---|---|---|---|---|
| De-Escalation of Adjuvant Therapy | |||||
| NCT02072148 (SIRS) | Stage I, II, III and intermediate stage IVa (T1 N0–2b, T2 N0–2b, AJCC 8th edn) HPV+OPC disease, with stratification based on pathological prognosis | TORS & follow-up monitoring for patients with a good prognosis (group 1); reduced-dose adjuvant RT or CRT based on risk status for patients with a poor prognosis (group 2 or 3) | Reduce the impact of radio-chemotherapy for patients. Progression-free survival found to be 91.3%, 86.7% and 93.3% for groups 1–3, at 43.9 months |
Completed, 2022 | |
| NCT01898494 (ECOG-3311) | Patients With HPV+ Stage III-IVA OPC | Transoral Surgery Followed By Low-Dose or Standard-Dose Radiation Therapy With or Without Chemotherapy | Assess oncologic outcome and favorable functional outcomes in intermediate-risk HPV+ OPC. 2-year progression-free survival 96.6%, 94.9%, 96.0% and 90.7% in arms A–D | Phase II Active/Not recruiting – Study completion by 2024 |
|
| NCT02908477 (DART) | HPV+ OPC and absence of distant metastases | De-escalated Adjuvant Radiation Therapy | Assess if radiotherapy can be safely reduced with the aim to decrease the therapy associated late effects | Phase III Active/Not recruiting – Study completion by 2024 |
|
| NCT03822897 (EVADER) | Low-risk HPV+OPC T1-3 N0-1 M0 | Adjusted de-escalation radiotherapy in patients | Decreasing the regions of elective nodal irradiation in the neck will lead to less toxicity and better quality of life/functional outcomes while maintaining high disease control rates in patients with favorable prognosis HPV+ OSC | Phase II Active/Not recruiting – Study completion 2024 |
|
| NCT04580446 (HYHOPE) | Pathologically-proven diagnosis of T1-3, N0-2 (up to 6 cm) HPV+OPV, except T1-2N0 | De-intensified Hypofractionated Radiation Therapy | Evaluate the tolerability of a de-intensified hypofractionated radiation therapy regimen completed in 3 weeks, with concurrent weekly cisplatin | Phase I Active/Not recruiting – Study completion 2024 |
|
| NCT04178174 | Stereotactic Boost and Short-course Radiation Therapy | compare efficacy and safety of short-course chemoradiation consisting in stereotactic boost to the gross tumor of 14 Gy in 2 fractions followed by de-esclalated chemoradiation (40 Gy in 20 fractions and concurrent 2 cycles of Cisplatin 100mg/m2) in HOP+OPC vs. the current standard 7-week chemoradiation course | Phase II Active/ Recruiting – Study completion 2026 |
||
| NCT02215265 (PATHOS) | Histologically confirmed or suspected HPV+OPC - stage T1-T3, N0-N2b - decision to treat with primary transoral resection and neck dissection - considered fit for surgery and adjuvant radiotherapy | Risk-stratified, Reduced Intensity Adjuvant Treatment in Patients Undergoing Transoral Surgery for Human Papillomavirus (HPV)-Positive Oropharyngeal Cancer | Assess whether swallowing function can be improved following transoral resection of HPV-positive OPC, by reducing the intensity of adjuvant treatment protocols. To personalize treatment, based on disease biology (HPV status and pathology findings), to optimize patient outcomes. | Phase III Active/Recruiting – Study completion by 2027 |
|
| NCT03621696 (MINT) | Histologically or cytologically confirmed HPV-related stages I-III OPC - Primary tumor resected via a transoral oral approach (conventional surgery, TLMS, TORS) | Surgery Followed by Risk-Directed Post-Operative Adjuvant Therapy for HPV+OPC | Reduce treatment-related toxicity while maintaining efficacy | Phase II Active/Not recruiting – Study completion by 2026 |
|
| NCT03396718 (DELPHI) | HPV+ patients with either intermediate or high risk for locoregional recurrences treated with higher radiotherapy dose and concurrent chemotherapy | 2 level de-escalation of Adjuvant Radio (Chemo) Therapy for HPV+OPC | Assess if radiotherapy can be safely reduced with the aim to decrease the therapy associated late effects | Phase I Active/Recruiting – Study completion by 2032 |
|
| NCT01706939 (Quarterback) | Histologically or cytologically confirmed, stage 3 or 4, HPV+OPC, without distant metastasis | Comparing two doses of definitive radiation therapy - 5600 cGy or standard 7000 cGy dose, given with induction and concurrent chemotherapy | Compare the reduced radiation dose to the standard of care in HPV+OPC for non-inferiority | Phase III Active/Recruiting – Study completion by 2035 |
|
| NCT02945631 (Quarterback 2b) | Histologically or cytologically confirmed, stage 3 or 4, HPV+OPC, without distant metastasis. Patients who are on the Quarterback Trial when Quarterback 2 is activated and who have been randomized to radiotherapy arm will be asked to transfer to this trial and receive the Quarterback 2 defined radiotherapy | Sequential Therapy With Reduced Dose Chemoradiotherapy | Establish the efficacy and toxicity of low dose chemoradiotherapy after induction chemotherapy in patients with locally advanced HPV+OPC | Phase II Active/Not recruiting – Study completion by 2027 |
|
| NCT03210103 (ORATOR2) | Patients with stage T1–2 N0–2 HPV+OPC | De-escalation primary Radiotherapy [60 GY +/- chemotherapy] Versus Primary Surgery [+/- adjuvant 50Gy radiotherapy] | Overall survival primary radiotherapy vs TORS plus neck dissection arms | Phase II/III Active/Not recruiting – Study completion by 2028 |
|
| Targeted Therapy replacement with Adjuvant Chemotherapy | |||||
| ISRCTN33522080 (De-ESCALaTE HPV) | Stage III-Iva HPV+OPC | EGFR-inhibitor (cetuximab) versus Standard Chemotherapy (cisplatin), + standard radiotherapy | Cetuximab arm showed no reduction in toxicity compared to cisplatin. Additionally, significant reduced 2-year overall survival was observed (89.4%) vs cisplatin arm (97.5) | Phase III Completed, 2019 |
|
| NCT01302834 (NRG Oncology RTOG 1016) | Stage T1-2, N2a-N3 or T3-4 HPV+OPC | Radiotherapy Plus Cetuximab Versus Chemoradiotherapy | 5-year overall survival and progression free survival of cetuximab with radiotherapy was lower (77.9%, 67.3% respectively) in comparison to cisplatin with radiotherapy arm (84.6%, 78.4% respectively) | Phase III Completed, 2018 |
|
| Antiviral Therapy with Adjuvant Chemotherapy | |||||
| NCT01721525 | Stage IVA/IVB HPV+OPC | Induction chemotherapy with (EGFR)/ErbB2inhibitor afatinib, antiviral like ribavirin, and weekly carboplatin and paclitaxel | Well tolerated 75% 2-year progression-free survival rate in overall 10 patients | Phase I Completed, 2017 |
|
| Therapeutic Vaccines | |||||
| NCT03418480 (HARE-40) | Arm 1: 15 patients previously treated HPV 16+. Arm 2: 29 patients with HPV16+ advanced disease |
Dose escalated anti-CD40 RNA vaccine | Evaluating safety, tolerability and dosage of an E7-targeting mRNA vaccine in combination with anti-CD40 antibody | Phase I/II Completed, 2024 |
|
| NCT04180215 | Arm 1: Patients with metastatic/recurrent HPV 16+OPC, who have not received prior treatment and eligible to receive pembrolizumab as part of their standard of care. Arm 2: Patients with metastatic/recurrent HPV 16+OPC, who have received prior treatment and eligible to receive pembrolizumab as part of their standard of care |
E6/E7-targeting single vector therapy - HB-201 and two-vector therapy – HB-202 | Investigating anti-cancer effects and safety | Phase I/II Active – Study completion 2025 |
|
| Immunotherapy | |||||
| NCT03669718 | PD-L1+ p16+ metastatic and/or recurrent HPV+OPC disease | ISA101b (a HPV 16 E6 and E7 synthetic peptide) plus cemiplimab (a anti-PD-1/PD-L1 antibody) vs placebo plus cemiplimab | Evaluating the objective response rate, duration of response treatment-related adverse effects | Phase II Completed 2023 |
|
| NCT03799445 | Stage 1 and 2 (T1 N2, T2 N1-N2, T3 N0-N2) excluding T1N0-N1 and T2N0, HPV+OPC | Low to moderate radiotherapy (50–66 Gy) plus nivolumab (anti-PD-1) and ipilimumab (anti-CTLA4) | Evaluate the safety, tolerability, feasibility and complete response rate, and 2-year progression-free survival of ipilimumab and nivolumab when administered concurrently with reduced-field radiotherapy | Phase II Active, Recruiting – Study completion 2024 |
|
| NCT03952585 | Early-Stage, Non-Smoking, HPV+OPC | De-intensified Radiation Therapy With Chemotherapy (Cisplatin) or Immunotherapy (Nivolumab) | Progression-free survival, quality of life, overall survival and adverse effects | Phase II/III Active, Recruiting – Study completion 2025 |
|
| NCT03410615 | Intermediate risk HPV+ locoregionally advanced OPC | Cisplatin + radiotherapy (70 Gy) vs Durvalumab (anti-PD-L1 antibody) + radiotherapy (70 Gy), followed by Durvalumab vs Durvalumab + radiotherapy(70 Gy) followed by Tremelimumab (anti-CTLA-4 antibody) + Durvalumab | Functional assessment of cancer therapy, 3-year event free survival, local regional failure, distant metastasis-free survival, overall survival, cost-effectiveness, toxicities | Phase II Active, Recruiting – Study completion 2026 |
|
| NCT03811015 | Stage T1–2 N2–3 or T3–4 N0–3, ≥10 pack-year smoking history HPV+OPC or stage T4 N0–3 or T1–2 N2–3, <10 pack-years HPV+OPC | Cisplatin plus de-escalated radiotherapy, followed by nivolumab (anti-PD-1) vs cisplatin plus de-escalated radiotherapy followed by observation with potential crossover to nivolumab at 12 months | Progression free survival, overall survival, negative fluorodeoxyglucose–PET at 12 weeks post-therapy | Phase III Active, Recruiting – Study completion 2027 |
|
| NCT03452137 | High-Risk Locally Advanced HPV+OPC with a complete/partial response or stable disease following definitive local therapy | Atezolizumab or placebo as adjuvant therapy after definitve local therapy for patients with high-risk disease | Event free survival, overall survival and adverse events | Phase III Active, Recruiting – Study completion 2027 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



