
Submitted:
18 March 2024
Posted:
19 March 2024
You are already at the latest version
Abstract
As the world’s population age, Cognitive Frailty (CF) is becoming one of the most serious health problems and elucidating its biological mechanisms along with prevention and treatments becomes increasingly important also considering the associated health costs. This pilot study aims to investigate the potential cognitive and neuropsychological effects of a 5-week treatment with a therapy based on the regenerative properties of ozone (O3) in a cohort of patients stratified according to CF. We also study the potential effects of O3 on blood-based biomarkers indicative of specific biological systems that may be altered in CF. Seventy-five older persons have been recruited and randomly assigned to receive the active treatment (150cc of oxygen-O2-O3 mixture at the concentration of 30ug of O3 per cc of O2) or O2, or the placebo (air) for 5 weeks. The primary endpoint is a change in the scores of clinical scales from baseline (T0) to weeks 3 (T3), 9 (T9), 15 (T15) after treatment. The secondary endpoint is a change in biomarkers levels resulting from transcriptomics, proteomics and metabolomic patterns at the same times. This study will evaluate whether an intervention with the O2-O3 therapy could have potential cognitive, neuropsychological and biological effects on CF.
Keywords:
Cognitive frailty
; frailty
; randomized double blind clinical trial
; oxygen-ozone therapy
; neuropsychological markers
; biological markers.
1. Introduction
Frailty is a multidimensional geriatric syndrome characterized by increased vulnerability to stressors due to the reduced functional capacity of different physiological systems [1,2,3,4]. If we compared with robust older adults, those with frailty are more likely to fall, be disabled, immobile, require hospitalizations, and have a lower quality of life [5]. Existing studies have found that the prevalence of frailty among community-dwelling older individuals 65 and older ranges from 4.0 to 59.1% [6,7].
Another area that concerns older adults is cognitive impairment. Cognitive impairment often co-occurs with frailty, causing increased disability, reduced quality of life, and higher morbi-mortality [8]. Therefore, frailty and cognitive decline are complicatedly related [9]. In April 2013, the International Academy of Nutrition and Aging (IANA) and the International Association of Gerontology and Geriatrics (IAGG) agreed on the definition of “cognitive frailty” (CF), which is a simultaneous state of both cognitive impairment (clinical dementia rating [CDR] = 0.5) and physical frailty (frailty phenotype) in older individuals without a definite diagnosis of dementia independent of other frailty dimensions (e.g., social, psychological and oral frailty) [10]. Although the definitions and assessments of CF have undergone some changes over time among researchers, older adults with both physical frailty and cognitive impairment are shown to be at higher risk of adverse health outcomes, including death, disability, hospitalization than those with either condition alone [11,12,13]. Physical frailty can accelerate cognitive impairment as well as increase the risk of mild cognitive impairment (MCI) and dementia [14,15]. Prevalence of CF in adults aged 65 years and older was estimated to be 9% and is common in older women living in the community [16].
The underlying molecular mechanisms of CF remains unclear. However, based on the close association seen between physical frailty and cognitive impairment, several review articles suggest the presence of an underlying mechanism common to these conditions: impaired hypothalamic–pituitary axis stress responses, energy homeostasis and mitochondrial dysfunctions, endocrine dysregulation, oxidative stress, nutritional and metabolomic factors alterations, gut dysbiosis, and vascular risk factors and diseases [17]. Importantly, the phenotype of frailty has also been associated with underlying inflammatory mechanisms. A recent review [18] supported the potential role of some biomarkers such as for instance C-reactive protein (CRP) as an inflammatory marker and as a prognostic index in this syndrome.
For these multifaced underlying causes, accumulating evidence indicates the need for comprehensive geriatric assessment that helps to characterize better the CF aetiopathogenesis, but also to develop, at the same time, new individualized mono-domain interventions to prevent adverse health outcomes for older adults with CF.
Since 1840, from its discovery, ozone (O3) and consequently the oxygen (O2)- O3 therapy expand into the medical field giving rise to compelling research in the recent decades to validate its clinical value [19]. Several papers [20,21,22] emphasized its relevant medical features, including virucidal and bactericidal effects, inflammatory modulation and circulatory stimulation, with considerable applications in several medical fields [23]. The function of O3 is strictly associated to its power to directly interact with phospholipids, lipoproteins, bacteria envelopes and viral capsids. Therefore, it is considered one of the most powerful oxidizing molecules in nature [24]. Recently, its effects on the cellular and humoral immune system have gained attention, which are responsible for the proliferation of immunocompetent cells and the synthesis of immunoglobulins and biologically active substances (interleukins, leukotrienes, and prostaglandins). In this sense, O3 also seems to activate macrophage function and increase the sensitivity of microorganisms to phagocytosis. Finally, the interaction between O3 and blood cells or other elements of the circulatory system is also proposed, which would have beneficial effects on O2 metabolism, cellular energy, antioxidant defense system, and microcirculation [24].
While experimental research provides a preclinical rationale for the use of O2-O3 therapy to enhance cognition/aging [25,26,27,28], clinical studies supporting its potential beneficial effects on cognition in humans are not available.
The primary aim of this pilot trial is to elucidate the potential cognitive and neuropsychological effects of a 5-weeks treatment with O2-O3 therapy on older frailty adults. The secondary aim is to clarify the potential effects of this treatment on blood-based biomarkers associated to transcriptomics, proteomics and metabolomics patterns. Here, we describe our sample according to its sociodemographic, clinical and neuropsychological features, screened and selected for this ongoing clinical trial and discuss the clinical aspects, and the implications for the clinical practice.
2. Materials and Methods
2.1. Trial Design and Setting
The study is a randomized, double-blind, placebo-controlled, 5-week trial to assess cognitive, neuropsychological and biological effects of O2-O3 therapy on 75 older adults stratified according to CF score. The study is being conducted at the IRCCS Centro San Giovanni di Dio Fatebenefratelli, Brescia, Italy.
Participants have been recruited among those who had already had access to Translational Memory Clinic of the IRCCS Centro San Giovanni di Dio Fatebenefratelli, but also by several methods, including advertisements in local newspapers, fryers located at our Institute, and meetings in different cultural centers for the elderly. Retention has been facilitated by regular contact during the clinical trial for screening, appointment reminders, and the testing sessions.
2.2. Ethics Approval
The protocol (version 3.0) was approved by the local ethical committee, the Ethics Committee of the IRCCS Centro San Giovanni di Dio Fatebenefratelli (rif. Parere 40-2018). All participants provided informed verbal consent via written informed consent at the time of face-to-face screening to a member of the research team. The research was conducted in accordance with the International Conference on Harmonization of Good Clinical Practice (GCP/ICH) guidelines and was performed in line with the principles of the Declaration of Helsinki.
2.3. Inclusion and Exclusion Criteria
The inclusion criteria were as follows: 1) subjects between the ages of 60 and 85, referring to the diagnosis of amnesic or non-amnesic cognitive disorder, reported by the subject himself or by family members; 2) MMSE score ≥ 24/30; 3) exclusion of dementia, even in the presence of ascertained Alzheimer's disease detected by the most advanced diagnostic techniques; 4) function intact, or functional reduction not related to the cognitive problem; 5) pharmacological therapy for the treatment of stable cognitive or behavioral disorders for at least 3 months at the time of enrolment. The exclusion criteria were as follows: 1) subjects affected by disabling vision or hearing impairments; 2) subjects affected by known psychosis or psychiatric illness, alcohol or drug abuse; 3) subjects affected by uncontrolled hyperthyroidism or by Glucose-6-Phostate Dehydrogenase Deficiency (G6PD)-Favism; 4) subjects who considered invasive the methodology for rectal insufflation.
2.4. Study Schedule
The study schedule of the trial protocol is detailed in the Figure 1.
Participants have been invited to undergo a face-to-face clinical assessment and neurocognitive battery. In addition, subjects have been asked about their socio-demographic status, their life styles and diet habits. Body Mass Index (BMI) was calculated too. The Everyday Memory Questionnaire (EMQ) has been administrated to evaluate the presence of Subjective Memory Complaints (SMC), whereas the Cognitive Reserve Index questionnaire (CRI-q) to measure cognitive reserve. Symptoms of depression have been evaluated with the Geriatric Depression Scale (GDS), whereas the physical health in general was estimated by the number of chronic diseases, by the Cumulative Illness Rating Scale (CIRS index), and by the number of drugs. Moreover, functioning skills in daily life were valued through the Barthel Index for Activities of Daily Living (Barthel index), Tinetti, and Instrumental Activities of Daily living (IADL) scales, in order to investigate the functional impact of any cognitive difficulties. Finally, an assessment of physical activity in daily life was performed.
Specific scales/tools were used to assess the frailty status: “Italian Frailty Index” (IFI) [29], an Italian version of the frailty index based on accumulation of age-related deficits; Frailty Instrument (FIt) for primary care based on the Survey of Health, Aging and Retirement in Europe (SHARE-FIt) [30], valuating 5-items (i.e. grip strength and four self-reported items; fatigue, loss of appetite and/or eating less than usual, difficulties climbing stairs and/or walking 100 meters, and low level of physical activity), and CDR scale to quantify the severity of symptoms of dementia.
Eligible participants have then been invited to the baseline neuropsychological visit, which was scheduled within a mean of 20 days of the face-to-face clinical assessment, and allocated to one of the three intervention groups. A blood sample has been collected for biomarker measurement from all subjects. Follow-up neuropsychological visits included (i) a visit after 3 months from the treatment (T3); (ii) a midpoint visit 9 months after treatment (T9); and (iii) an endpoint visit 15 months after treatment (T15). In each follow up, we collected blood samples for biomarkers measurement.
2.5. Adaptive Randomization
Subjects were divided into three groups with different cognitive frailty, defined according to tertiles of distribution of the scores of tests for the evaluation of memory skills (Story recall, Rey Auditory Verbal Learning Test - RAVLT immediate and delayed recall, and Rey–Osterrieth Complex Figure – ROCF Recall), attention skills (Trail Making Test part A and part B, TMT-A, TMT-B, Rey–Osterrieth Complex Figure - ROCF copy) and MMSE and GDS scores.
Participants were randomly assigned to the active treatment group (O2; O2-O3) or the placebo group (air), balanced for CF, so that each treatment arm accommodated a similar proportion of subjects in each tertile. The definition of the tertiles of CF was performed at different times, over a period of 12 months, on groups of 12/16 subjects, as enrollment progressed and before starting treatment. Being a double-blind study, both the researchers of the research team and the participants remained blinded to the treatment assignment until the completion of the study, while the medical doctor performing the treatment knew the treatment group, but not tertile of fragility. During recruitment, the medical doctor performing the treatment periodically re-evaluated the size of the treatment subgroups based on the recruitment and dropout rate.
2.6. Compliance and Adverse Effects
Compliance has been assessed by instructing the participants to note/record any medications (new or not) intake and/or adverse events occurred through-out the course of the study. Adverse events have been closely monitored throughout the course of the study, instructing the participants to immediately contact the research team in case of unexpected medical care visits or serious adverse events/hospitalization. Reasons for discontinuation have been recorded.
2.7. Primary and Secondary Endpoints
The primary endpoint is the change in the scores of the clinical IFI or SHARE-Fit scales from baseline to T3, T9, and T15 trial period after treatment.
The secondary endpoint is the change in the molecular levels (RNA and proteins) from baseline over the T3, T9, and T15 trial period after treatment.
2.8. Intervention
Active. The medical specialist inserted a small catheter CH14-18 into the rectum and gently administered a total amount of 150cc of O2-O3 mixture at the concentration of 30ug of O3 per cc of O2 over a 5-10 min period while the patient was laying on his/her left side. The patient was asked to refrain from passing gas or having a bowel movement for at least 30m. This procedure is known as rectal insufflation. It was performed for 3 sessions/week (5 weeks). By the same approach, subjects were insufflated with 150cc of pure O2.
Placebo. By the same methodology and times and sessions, 150cc of air were insufflated as placebo treatment.
2.9. Data Collection
Neuropsychological batteries. All participants were tested at each visit with the Mini Mental State Examination (MMSE) [31] for assessing the global cognition and with several cognitive tests selected to assess a broad range of cognitive abilities: RAVLT, immediate and delayed recall, ROCF Recall, TMT-A, TMT-B, ROCF copy, action and object naming subtests from the Battery for the Assessment of Aphasic Disorders (B.A.D.A), Raven’s Colored Progressive Matrices (CPM47), Free and Clued Selective Reminding Test (FCSRT) and Face-name Association task (FNAT) [32]. In addition, baseline assessment (Time=T0) included the administration of Digit span forward and Digit span backward test. Story recall, phonemic verbal fluency (FPL) and semantic verbal fluency (FPC) task, Token Test Auditory sentence comprehension subtest from BADA) and De Renzi ideomotor apraxia test (right and left upper limb) too [33].
Biological measures. Fasting venous blood samples have been collected in the morning at the baseline (T0), and at follow-ups T3, T9, T15 for the evaluation of alterations/modulations at the molecular level before and after treatment. In particular, this material will be used to perform transcriptomic, proteomic and metabolomic studies.
Proteomic analyses. Anticoagulant-free tubes and EDTA tubes were used for serum and plasma preparation, respectively. Serum tubes were kept at room temperature for 1 hour followed by 1 hour at 4°C before serum separation by centrifugation (2000×g for 10 minutes). Plasma tubes were immediately centrifuged at 2000×g for 10 minutes. Serum and plasma samples were stored at −80°C until the time of the assay. We will plan to perform a cytokines and growth factors panel to be analyzed through automated ELISA Platform (Bioplex, Biorad). Assay was also performed for C-reactive protein (CRP) on serum samples from each subject at time T0.
Mass spectrometry. Sample preparation. To extract metabolites, frozen serum samples were thawed at 4oC and 145 µL were transferred into 1.5 mL low protein binding tubes. 5 µL of ESI Tuning Mix and 300 µL of extraction solvent (ACN, acetonitrile) were added to 145 µL of serum sample, mixed by vortex for 30 s, and centrifuged at room temperature and 13,000 rpm (15,871xg) for 10 min. Then, ~400 µL of supernatant were transferred into 1.5 mL low protein binding tubes and the extracts were dried in a vacuum concentrator at 30oC. Sample-dried pellets were stored at 4oC overnight (16 h) and reconstituted the next day prior to analysis. For reconstitution, 50 µL of ACN/H2O (20:80, v/v) were added to the pellet, mixed by vortex for 60 sec and then transferred to vials for LC-MS analysis. A procedure blank was generated identically without serum and used later to remove the background ions. Equal volumes of serum from all biological test samples were pooled as the quality control (QC) sample for the UHPLC–QqTOF–MS analysis. The QC samples were used to assess the reproducibility and reliability of the LC–MS system, and to determine the repeatability of a metabolite feature.
UHPLC–QqTOF–MS analysis. Serum metabolic profiling analysis will be performed using a UHPLC–MS system consisting of a Bruker compact QqTOF MS (Bruker Daltonics) and Dionex UltiMate 3000 Rapid Separation LC (Thermo Fisher Scientific) equipped with an Acquity UPLC BEH C18 (300 Å, 2.1 × 150 mm, 1.7 μm) column (Waters). MS parameters will be set up using microToF 3.4, ESI Compass 1.3, and HyStarPP 3.2 SR4 software (Bruker Daltonics). A 10 µL aliquot of samples will be injected into the HPLC column, and elution will be performed at a flow rate of 0.4 ml/min using a gradient elution program as follows: 0 min, 5% B; 2 min, 5% B; 7 min, 40% B; 9 min, 80% B; 9.1 min, 100% B; 14min, 100% B; 14.1 min, 5% B; 20 min, 5% B. The column temperature will be set up at 60oC. The total running time will be 20.1 min. Mobile phase A consists of 0.1% CH2O2 (formic acid) in H2O while mobile phase B consists of 96% EtOH. Ionization will be performed using an electrospray ionization (ESI) source, operating in positive mode. ESI source conditions will be set up as follows: capillary voltage, 4.0 kV; dry gas (N2) flow, 8.0 L min-1; dry gas (N2) temperature, 300°C; nebulizer pressure, 3.0 bar. The mass scan range will be set from 200 to 950 m/z. The instrument will be calibrated prior to the analyses using 10 mM sodium formate.
Data processing and analysis. UHPLC–MS raw data files (.d) will be converted to mzML format using ProteoWizard (version 3.0.23339). The open-source MZmine 3 software (version 3.6.0) will be used to generate a peak table containing m/z, retention time (RT), and intensity for the peaks (also called features). Parameters for feature detection will be set up as follows: scan to scan accuracy, 0.005 m/z; minimum intensity, 1.0E3; minimum peak width, 5 scans; minimum RT search range, 0.05 min; noise level, 1.0E2. The retention time scan window will be limited to 5-15 min. 13C-related isotope peaks will be removed if peaks are ≤0.01 min apart, their m/z difference ≤0.001 or 3 ppm, and a monotonically decreasing trend of the isotope pattern is detected, retaining the most intense peak. Alignment of peaks and gap-filling will be performed setting the following parameters: sample-to-sample m/z tolerance, 0.05 m/z or 50 ppm; RT tolerance, 0.4 min. Redundant peak entries due to misaligned feature list rows will be removed if two peaks are ≤0.05 min apart and their m/z difference ≤0.05 or 10 ppm. Background peaks will be removed if the intensity in the biological samples is <3-fold of that in procedure blank samples. Features not detected in at least 75% of QC samples will be excluded from the final table. The resulting peak table will be exported to a .csv file. Normalization of the data set will be performed applying the total intensity in an analysis (or sum of bucket values in analysis) normalization method. From the normalized data matrix, features with RSD higher than 30% in the QC samples will be filtered out before proceeding with statistical analyses. We will plan to perform a metabolic profile for each subject at baseline and after treatment.
Transcriptomic analyses. Peripheral blood samples were collected in PAXgene Blood RNA Tubes (PreAnalytiX, Qiagen, Valencia, CA, USA) and stored at −80 °C before RNA extraction. Total RNA was isolated using the PAXgene Blood RNA Kit (Qiagen) according to the manufacturer’s instructions. RNA purity was assessed by using the spectrophotometer NanoDrop ND-1000 UV-visible spectrophotometer; Labtech International, Ringmer, UK; 260/280 and 260/230 ratios were evaluated and concentrations and integrity were determined using the Agilent 2100 Bioanalyzer (Agilent Technologies, Santa Clara, CA, USA). Samples were loaded onto the Eukaryote total RNA 6000 nano Kit (Agilent Technologies, Santa Clara, CA, USA). The RNA integrity number (RIN) for all the samples was calculated and samples with a value lower than 7.0 were discarded. We will plan to perform a gene expression profiling using the standard protocol for Agilent one-colour gene expression microarray [34,35].
2.10. Data Management
Data collection forms and protocols were accessible to study investigators in a secured shared drive. Data collected at the visits have been entered electronically by the study coordinators and checked by the PI. Only study investigators were able to access the password-protected participant data and all information were remained confidential. Moreover, participants have been identified by a coded identification number, that has been used to identify all laboratory specimens, data collection, and administrative forms to maintain participant confidentiality. The study coordinators and PI had access to the final trial dataset. The PI oversaw intrastudy data sharing.
2.11. Data Monitoring
The study coordinators oversaw all aspects of data monitoring with the assistance of the PI. We also expect participants to experience minimal risks when undertaking this trial; therefore, no interim analyses have been conducted.
2.12. Statistical Analysis
Sample size. The power analysis was performed by the analysis of univariate linear regression test. Using the accuracy of the model IFI scale as multiple partial coefficient (R2), and the neuropsychological tests as fixed predictors, we found a power effect of 0.92 related to our population of 76 subjects. Similar findings (power effect of 0.80) were found when we considered the SHARE-Fit scale.
Data analysis. Descriptive statistics on cognitive and biological markers in the three treatment groups will be presented as mean and standard deviation. The association between categorical variables will be analyzed using the Chi-square test.
The Automatic Linear Modeling (ALM) model that is based on a machine learning approach to find the best predictive model using available data, will be used. A set of neuropsychological/biological values will be analyzed as independent input variables, while the scores of IFI or SHARE-FIt scales will be analyzed as continuous output (target) (dependent) variables. Longitudinal comparisons will be performed using Univariate where the clinical parameters relating to the IFI and SHARE-FIt scales will be entered as dependent variables, the significant values obtained from ALM as covariates and time and treatment as fixed factors. For the metabolomic analysis, PCA analysis (Principal Component Analysis) and a Univariate analysis will be performed to evaluate the effects of the treatment on the presence/distribution of the metabolites.
With the aim to correlate any clinical/cognitive improvements with molecular profiles to identify markers associated with response to treatment, the Generalized linear mixed model (GLMM) will be used where the biological values and those relating to neuropsychological tests and the times of follow-up will be analyzed as independent input variables, while the values relating to the IFI or SHARE-FIt scales will be analyzed as weight variables and the treatments as (dependent) variables. “Air treatment” will be used as a comparison variable. All these analyzes will be performed using SPSS ver. 29.
Differentially expressed genes will be identified using R-Bioconductor by applying both a fold change and p value threshold (R-Limma test p value < 0.05; |Log2 fold-change ratio|>1.0). Analysis of the categories and functional pathways of upregulated or downregulated genes will be performed using Fisher's exact test, using all genes in the array as the "reference" genome, or through the use of Ingenuity Pathway Analysis (IPA, QIAGEN Inc.) to infer alterations in biological pathways and functions.
2.13. Dissemination
The results from the trial will be publicly presented to scientific researchers and health care professionals through peer-reviewed journals and scientific conference presentations. The authorship requirements will adhere to scientific journal guidelines. In addition, individual trial outcomes will be forwarded to participants, with their consent. We will transmit findings, when appropriate, to the general population using different and specific tools.
3. Results
3.1. Sociodemographic, Anthropometric Features and State of Health
Table 1 presents the general characteristics of the study population according to gender. The mean age was 72 for both sexes. 60% of subjects took drugs.
Age of subjects, numbers of medications taken, numbers of diseases (except intestinal, ear, osteoarthritis and osteoporosis diseases), CRP values and BMI did not differ significantly. High education, osteoarthritis/osteoporosis as well as intestinal diseases were present and more common in females, while ear diseases with hearing lost were more common in males. The average hand grip strenght (HGS) test right and left for women was 21kg and 20kg respectively, while the mean HGS right and left for men was 35 kg and 33kg respectively.
3.2. Clinical and Neuropsychological Features for Frailty Assessment
In Table 2, we reported the clinical data obtained after the IFI and SHARE-FIt scales assessment. The average of CF scores according to IFI scale was 6.7±3.5, whereas 0.8±1.5 was obtained according to SHARE-FIt scale. 18.4% in our study population the subjects were frails according to clustered SHARE-Fit scale. The average CDR was 0.14±0.75.
The list of the all neuropsychological tests was reported in Table 3.
4. Discussion
This article presents the rationale, the materials/methodologies and the “picture” of our sample at T0 of this ongoing pilot clinical trial that has the aim to analyze cognitive and biological effects of O2-O3 therapy on the clinical/neuropsychological and molecular patterns in older adults with CF. Currently, limited specific treatments are available for elderly individuals characterized by CF, who are potentially at risk of developing cognitive impairment and dementia. Therefore, it is important to implement further potential strategically interventions that may promote cognitive health and ultimately prevent cognitive decline.
O3 is a triatomic gaseous molecule which has been used as a powerful oxidant in medicine for more than 150 years [36]. O3 concentration and effects do not follow a linear relationship: very low concentrations could have no effect, whereas very high concentrations can lead to contrary effects to those produced by lower/middle concentrations [37]. At least 65 findings reviewed in Scassellati et al. [38] demonstrated the preconditioning/postconditioning effects of O3 on endogenous pro-antioxidant mechanisms in vivo on animal models and in vitro on cells. In this direction, we will test for the first time whether there is an effect of this therapy on the frailty in a sample of aging subjects screened for CF. The rationale on which we based our hypothesis comes from some preclinical studies that demonstrated how O3 could be beneficent during the aging through the regulation of the oxidant-anti-oxidant homeostasis. Safwat et al. [25] demonstrated, in aged rats, that O3 reduced liver and kidney damage elevating the reduced hepatic and renal glutathione (GSH) contents, as well as normalizing hepatic glutathione peroxidase (GSH-Px) enzyme activity. Another work [27] showed, in aged rats, that O3 decreased the lipid and protein oxidation markers and lessening of lipofuscin deposition. In addition, O3 restored GSH levels in brain and heart tissues, and normalized GSH-Px activity in the heart tissue of these rats. O3 also mitigated age-associated energy failure in the heart and the hippocampus, improved cardiac cytosolic Ca(2+) homeostasis and restored the attenuated Na(+), K(+) -ATPase activity in the hippocampus of these rats. In another study [28], administration of O3 in aged-rats normalized reduced GSH content, adenosine triphosphate/adenosine diphosphate ratio, mitochondrial superoxide dismutase (SOD) and complex IV (cytochrome-c oxidase) activities. O3 improved glutathione redox index (GSHRI), complex I (NADH-ubiquinone oxidoreductase) and mitochondrial nitric oxide synthase (mtNOS) activities, and attenuated the rise malondialdehyde (MDA) and mitochondrial phosphatidylcholine (PC) levels. A further study [26] demonstrated that O3 administration ameliorated the behavioral and pathological deterioration of APP/PS1 transgenic mice, and reduced the level of amyloid-β precursor protein (APP).
In the medical setting, this therapy employs a gas mixture of O2/O3, obtained from the modification of medical-grade O2 using certificated O3 generator device [39]. Based on the basic mechanisms of action of O3 in blood, the therapeutic range of O3 has been precisely calculated and found to be 10-80 μg/ml of O3 in blood [40]. Schwart-Tapia et al. [40] described widely different and main routes of application with relative concentrations of O3. The side effects are minimal; the World Federation of Ozone therapy (WFOT) estimates the incidence of complications at 0.0007%. Moreover, the treatment is not only perfectly tolerated but most of patients have reported a feeling of wellness and euphoria throughout the cycle. This fact explains why the compliance of the patients remains excellent throughout the years.
To assess the frailty/CF, we used IFI as well as SHARE-FIt scales, along with CDR scores.
As reported in Sugimoto [17], many studies using varied CF models and assessment tools have investigated its impact on health outcomes and associated factors. However, these varied definitions and assessment tools make the comparison of findings across studies challenging. This leads to difficulty in adapting the CF concept to clinical practice. Therefore, the establishment of a valid operational definition and of an assessment tool that detect older adults at risk for reversible conditions should be an urgent priority. Another challenge is represented by the lacking of an appropriate tool for the evaluation of cognitive impairment. In this direction, we have enriched our clinical valuations implementing a complete battery of neuropsychological tests which have been used in our trial.
The secondary endpoint of the trial is the change in biological markers at protomics, transcriptomics and metabolomics level. The identification of biomarkers in CF is difficult as the syndrome is multidimensional. In the context of neuroimaging evidence, several recent papers agreed that CF is associated with loss of structure of the thalamus and hippocampus and changes in white matter hyperintensity [41]. Consideration of the microbiota is a new aspect in the development of age-related biomarkers. Changes in the microbiota during aging are increasingly being studied, and He et al. [42] demonstrated that CF patients have elevated levels of trimethylamine N-oxide (TMAO), a stable metabolite of the intestinal microbiota. At the metabolic level, plasma biomarkers are being studied: for instance, a longitudinal study in a population of 7,769 individuals included in the Doetinchem Cohort Study [43] found that high-density lipoprotein (HDL) cholesterol, triglycerides, alanine aminotransferase (ALT), gamma-glutamyltransferase (GGT), albumin, uric acid, cystatin C or creatinine were not predictive of CF. Contrarily, Royal and Plamen [44] found that insulin-like growth factor 1 (IGF-1) and IGF-binding protein 2 (IGFBP2) were implicated in CF and potentially in the cause of age-related cognitive decline and physical frailty. Concerning metabolism, Sargent et al. [45] found that low levels of vitamin E alpha tocopherol, omega-6 and 3 and albumin were associated with CF. In addition, these researchers observed a second pattern of association characterized by a low level of trans fats, as indicated by measuring low- and high-density lipoproteins (LDL and HDL).
This ongoing trial has some strengths. First of all, the length: considering the three follow-up visits in the 15 months after treatment, it was long enough to expect to have more information on the trajectory of cognitive changes. Second, the inclusion of an -omics corollary and biological markers will provide surrogate measures of treatment effects and allow us to identify possible mechanisms of action underlying the proposed treatment-associated benefits on cognition. On the other hand, although our sample has a power effect of 0.92/0.80, the results we will obtain should be confirmed in a larger population.
5. Conclusions
Positive results from this study will inform the design of larger clinical trials to test O2-O3 therapy as a potential strategy for the prevention of cognitive impairment and will allow the public health organizations to plan interventions for at-risk older individuals.
Author Contributions
Conceptualization, C.S., C.B. and C.G.; methodology, C.S., C.B., A.C.G. and C.G.; formal analysis, C.S., C.B. and C.G.; investigation, C.S., C.B., M.Ci., R.Z., E.T., V.S., I.Pas., M.A., I.Pag., M.Co., M.D’O., A.C.G., A.C. and C.G.; resources, R.Z., A.C., and C.G.; data curation, C.S., C.B. and C.G.; writing—original draft preparation, C.S., C.B.; writing—review and editing, C.S., C.B. and C.G.; visualization, C.S., C.B., M.Ci., R.Z., E.T., V.S., I.Pas., M.A., I.Pag., M.Co., M.D’O., A.C.G., A.C. and C.G.; supervision, C.G.; project administration, C.B., R.Z., A.C., and C.G.; funding acquisition, C.B. and C.G. All authors have read and agreed to the published version of the manuscript.
Funding
Please add: “This research was funded by Italian Ministry of Health, grant number RF-2016-02363298 and Ricerca Corrente”.
Informed Consent Statement
The study involving human participants was approved by the Comitato Etico IRCCS San Giovanni di Dio Fatebenefratelli, Brescia, Italy. The participants provided their written informed consent to participate in this study.
Data Availability Statement
The datasets of raw data generated for this study can be found in the Zenodo Data Repository (10.5281/zenodo.10805255).
Acknowledgments
The manuscript was supported by RF-2016-02363298 and Ricerca Corrente (Italian Ministry of Health).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chen, X.; Mao, G.; Leng, S.X. Frailty syndrome: an overview. Clin Interv Aging 2014, 9, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [PubMed]
- Lang, P.; Michel, J.; Zekry, D. Frailty syndrome: a transitional state in a dynamic process. Gerontology 2009, 55, 539–549. [Google Scholar] [CrossRef]
- Robertson, D.A.; Savva, G.M.; Kenny, R.A. Frailty and cognitive impairment--a review of the evidence and causal mechanisms. Ageing Res Rev 2013, 12, 840–851. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.Y.; Gan, P.; How, C.H. Approach to frailty in the elderly in primary care and the community. Singapore Med J 2018, 59, 240–245. [Google Scholar] [CrossRef]
- Yang, Q.; Wang, Y.; Yang, M.; Ge, S.; Cheng, S.; Wang, C.; Zhang, W.; Tian, C.; Mao, J. Apathy co-occurs with subjective cognitive decline among community-dwelling older adults. Geriatr Nurs 2022, 48, 177–182. [Google Scholar] [CrossRef]
- Collard, R.M.; Boter, H.; Schoevers, R.A.; Oude Voshaar, R.C. Prevalence of frailty in community-dwelling older persons: a systematic review. J Am Geriatr Soc 2012, 60, 1487–1492. [Google Scholar] [CrossRef]
- Fabricio, D.d.M.; Chagas, M.H.N.; Diniz, B.S. Frailty and cognitive decline. Transl Res 2020, 221, 58–64. [Google Scholar] [CrossRef]
- Yoon, D.H.; Hwang, S.S.; Lee, D.W.; Lee, C.G.; Song, W. Physical Frailty and Cognitive Functioning in Korea Rural Community-Dwelling Older Adults. J Clin Med 2018, 7, 405. [Google Scholar] [CrossRef]
- Kelaiditi, E.; Cesari, M.; Canevelli, M.; van Kan, G.A.; Ousset, P.; Gillette-Guyonnet, S.; Ritz, P.; Duveau, F.; Soto, M.E.; Provencher, V.; Nourhashemi, F.; Salva, A.; Robert, P.; Andrieu, S.; Rolland, Y.; Touchon, J.; Fitten, J.L.; Vellas, B. ; IANA/IAGG Cognitive frailty: rational and definition from an (I. A.N.A./I.A.G.G.) international consensus group. J Nutr Health Aging 2013, 17, 726–734. [Google Scholar] [CrossRef]
- Rivan, N.F.M.; Shahar, S.; Rajab, N.F.; Singh, D.K.A.; Che Din, N.; Mahadzir, H.; Mohamed Sakian, N.I.; Ishak, W.S.; Abd Rahman, M.H.; Mohammed, Z.; You, Y.X. Incidence and Predictors of Cognitive Frailty Among Older Adults: A Community-based Longitudinal Study. Int J Environ Res Public Health 2020, 17, 1547. [Google Scholar] [CrossRef]
- Panza, F.; Lozupone, M.; Solfrizzi, V.; Sardone, R.; Dibello, V.; Di Lena, L.; D'Urso, F.; Stallone, R.; Petruzzi, M.; Giannelli, G.; Quaranta, N.; Bellomo, A.; Greco, A.; Daniele, A.; Seripa, D.; Logroscino, G. Different Cognitive Frailty Models and Health- and Cognitive-related Outcomes in Older Age: From Epidemiology to Prevention. J Alzheimers Dis 2018, 62, 993–1012. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Zhang, H.; Du, X.; Yin, L.; Zhang, H.; Zhou, Q. Comparison of the prevalence and associated factors of cognitive frailty between elderly and middle-young patients receiving maintenance hemodialysis. Int Urol Nephrol 2022, 54, 2703–2711. [Google Scholar] [CrossRef] [PubMed]
- Buchman, A.S.; Boyle, P.A.; Wilson, R.S.; Tang, Y.; Bennett, D.A. Frailty is associated with incident Alzheimer's disease and cognitive decline in the elderly. Psychosom Med 2007, 69, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Boyle, P.A.; Buchman, A.S.; Wilson, R.S.; Leurgans, S.E.; Bennett, D.A. Physical frailty is associated with incident mild cognitive impairment in community-based older persons. J Am Geriatr Soc 2010, 58, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Y.; Li, G.; Wang, X.; Zheng, L.; Wang, C.; Wang, C.; Chen, L. Prevalence of cognitive frailty among community-dwelling older adults: A systematic review and meta-analysis. Int J Nurs Stud 2022, 125, 104112. [Google Scholar] [CrossRef]
- Sugimoto, T.; Arai, H.; Sakurai, T. An update on cognitive frailty: Its definition, impact, associated factors and underlying mechanisms, and interventions. Geriatr Gerontol Int 2022, 22, 99–109. [Google Scholar] [CrossRef]
- Pothier, K.; Gana, W.; Bailly, N.; Fougere, B. Associations Between Frailty and Inflammation, Physical, and Psycho-Social Health in Older Adults: A Systematic Review. Front Psychol 2022, 13, 805501. [Google Scholar] [CrossRef]
- Di Meo, S.; Venditti, P. Evolution of the Knowledge of Free Radicals and Other Oxidants. Oxid Med Cell Longev 2020, 2020, 9829176. [Google Scholar] [CrossRef]
- Baranova, I.V.; Bezsmertnyi, Y.A.; Bezsmertnaya, H.V.; Postovitenko, K.P.; Iliuk, I.A.; Gumeniuk, A.F. Analgetic effect of ozone therapy: Myths of reality? Polish Annals of Medicine 2020, 27, 62–67. [Google Scholar]
- Masan, J.; Sramka, M.; Rabarova, D. The possibilities of using the effects of ozone therapy in neurology. Neuro Endocrinol Lett 2021, 42, 13–21. [Google Scholar]
- Galie, M.; Covi, V.; Tabaracci, G.; Malatesta, M. The Role of Nrf2 in the Antioxidant Cellular Response to Medical Ozone Exposure. Int J Mol Sci 2019, 20, 4009. [Google Scholar] [CrossRef]
- Smith, N.L.; Wilson, A.L.; Gandhi, J.; Vatsia, S.; Khan, S.A. Ozone therapy: an overview of pharmacodynamics, current research, and clinical utility. Med Gas Res 2017, 7, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Viebahn-Haensler, R.; Leon Fernandez, O.S. Ozone in Medicine. The Low-Dose Ozone Concept and Its Basic Biochemical Mechanisms of Action in Chronic Inflammatory Diseases. Int J Mol Sci 2021, 22, 7890. [Google Scholar] [CrossRef]
- Safwat, M.H.; El-Sawalhi, M.M.; Mausouf, M.N.; Shaheen, A.A. Ozone ameliorates age-related oxidative stress changes in rat liver and kidney: effects of pre- and post-ageing administration. Biochemistry (Mosc) 2014, 79, 450–458. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Ma, J.; An, J.; Qian, X.; Wang, Y.; Cope, D.K.; Williams, J.P. Ozone Inhibits APP/Abeta Production and Improves Cognition in an APP/PS1 Transgenic Mouse Model. Neuroscience 2019, 418, 110–121. [Google Scholar] [CrossRef] [PubMed]
- El-Sawalhi, M.M.; Darwish, H.A.; Mausouf, M.N.; Shaheen, A.A. Modulation of age-related changes in oxidative stress markers and energy status in the rat heart and hippocampus: a significant role for ozone therapy. Cell Biochem Funct 2013, 31, 518–525. [Google Scholar] [CrossRef]
- Shehata, N.I.; Abd-Elgawad, H.M.; Mawsouf, M.N.; Shaheen, A.A. The potential role of ozone in ameliorating the age-related biochemical changes in male rat cerebral cortex. Biogerontology 2012, 13, 565–581. [Google Scholar] [CrossRef] [PubMed]
- Abete, P.; Basile, C.; Bulli, G.; Curcio, F.; Liguori, I.; Della-Morte, D.; Gargiulo, G.; Langellotto, A.; Testa, G.; Galizia, G.; Bonaduce, D.; Cacciatore, F. The Italian version of the "frailty index" based on deficits in health: a validation study. Aging Clin Exp Res 2017, 29, 913–926. [Google Scholar] [CrossRef]
- Romero-Ortuno, R. The Frailty Instrument of the Survey of Health, Ageing and Retirement in Europe (SHARE-FI) predicts mortality beyond age, comorbidities, disability, self-rated health, education and depression. Eur Geriatr Med 2011, 2, 323–326. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Cotelli, M.; Manenti, R.; Brambilla, M.; Petesi, M.; Rosini, S.; Ferrari, C.; Zanetti, O.; Miniussi, C. Anodal tDCS during face-name associations memory training in Alzheimer's patients. Front Aging Neurosci 2014, 6, 38. [Google Scholar] [CrossRef] [PubMed]
- De Renzi, E.; Motti, F.; Nichelli, P. Imitating gestures. A quantitative approach to ideomotor apraxia. Arch Neurol 1980, 37, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Arisi, I.; Malimpensa, L.; Manzini, V.; Brandi, R.; Gosetti di Sturmeck, T.; D'Amelio, C.; Crisafulli, S.; Ferrazzano, G.; Belvisi, D.; Malerba, F.; Florio, R.; Pascale, E.; Soreq, H.; Salvetti, M.; Cattaneo, A.; D'Onofrio, M.; Conte, A. Cladribine and ocrelizumab induce differential miRNA profiles in peripheral blood mononucleated cells from relapsing-remitting multiple sclerosis patients. Front Immunol 2023, 14, 1234869. [Google Scholar] [CrossRef] [PubMed]
- Caputo, V.; Pacilli, M.G.; Arisi, I.; Mazza, T.; Brandi, R.; Traversa, A.; Casasanta, G.; Pisa, E.; Sonnessa, M.; Healey, B.; Moggio, L.; D'Onofrio, M.; Alleva, E.; Macri, S. Genomic and physiological resilience in extreme environments are associated with a secure attachment style. Transl Psychiatry 2020, 10, 185–4. [Google Scholar] [CrossRef] [PubMed]
- Elvis, A.M.; Ekta, J.S. Ozone therapy: A clinical review. J Nat Sci Biol Med 2011, 2, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Re Lamberto; Malcangi Giuseppe; Martinez-Sanchez Gregorio Medical ozone is now ready for a scientific challenge: Current status and future perspectives. Journal of Experimental and Integrative Medicine 2012, 2, 193–196. [CrossRef]
- Scassellati, C.; Galoforo, A.C.; Bonvicini, C.; Esposito, C.; Ricevuti, G. Ozone: a natural bioactive molecule with antioxidant property as potential new strategy in aging and in neurodegenerative disorders. Ageing Res Rev 2020, 63, 101138. [Google Scholar] [CrossRef]
- Bocci Velio OZONE: A new medical drug, Springer Dordrecht: 2010; pp. XXI, 315.
- Schwartz, A. ; Gregorio Martínez Sánchez; Cum, L.; Roberto Quintero; Mccarthy, W.; Moreno, O. MADRID DECLARATION ON OZONE THERAPY (3 rd edition) Official document of ISCO3.
- Facal, D.; Burgo, C.; Spuch, C.; Gaspar, P.; Campos-Magdaleno, M. Cognitive Frailty: An Update. Front Psychol 2021, 12, 813398. [Google Scholar] [CrossRef]
- He, W.; Luo, Y.; Liu, J.; Sun, N.; Guo, D.; Cui, L.; Zheng, P.; Yao, S.; Yang, J.; Wang, H. Trimethylamine N-Oxide, a Gut Microbiota-Dependent Metabolite, is Associated with Frailty in Older Adults with Cardiovascular Disease. Clin Interv Aging 2020, 15, 1809–1820. [Google Scholar] [CrossRef]
- Rietman, M.L.; Hulsegge, G.; Nooyens, A.C.J.; Dolle, M.E.T.; Picavet, H.S.J.; Bakker, S.J.L.; Gansevoort, R.T.; Spijkerman, A.M.W.; Verschuren, W.M.M. Trajectories of (Bio)markers During the Development of Cognitive Frailty in the Doetinchem Cohort Study. Front Neurol 2019, 10, 497. [Google Scholar] [CrossRef] [PubMed]
- Royall, D.R.; Palmer, R.F. ; Alzheimer's Disease Neuroimaging Initiative Blood-based protein mediators of senility with replications across biofluids and cohorts. Brain Commun 2019, 2, fcz036. [Google Scholar] [CrossRef] [PubMed]
- Sargent, L.; Nalls, M.; Amella, E.J.; Slattum, P.W.; Mueller, M.; Bandinelli, S.; Tian, Q.; Swift-Scanlan, T.; Lageman, S.K.; Singleton, A. Shared mechanisms for cognitive impairment and physical frailty: A model for complex systems. Alzheimers Dement (N Y) 2020, 6, e12027. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
FLOWCHART of clinical trial.
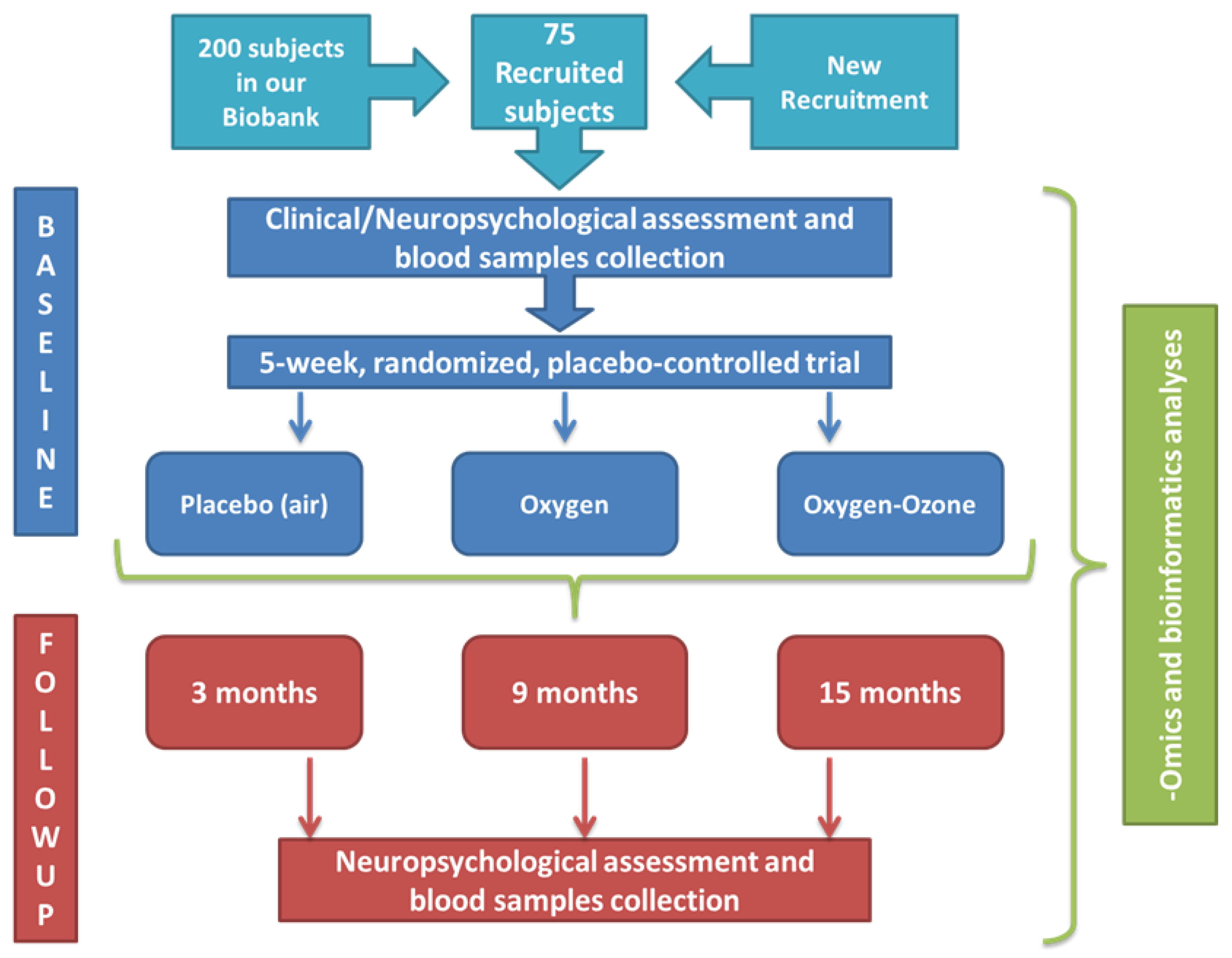

Table 1.
General Characteristics of the study population (N=76) according to sex.
| Quantitative Variables | F n=50 |
M n=26 |
All n=76 |
χ2 Test |
Comparison gender column proportions |
|---|---|---|---|---|---|
| Demography | |||||
| Age in years [Mean±SD (Min-Max)] | |||||
| 72.4±6.2 (60 - 85) | 71.6±7.1 (60 - 82) | 72.2±6.5 (60 - 85) | ns | ||
| Education [n, %] | |||||
| <9 | 20 (41.7) | 4 (16.0) | 24 (32.9) | 0.03 | |
| ≥9 and <14 | 18 (37.5) | 18 (72.0) | 36 (49.3) | 0.02 | 0.005 |
| ≥14 | 10 (20.8) | 3 (12.0) | 13 (17.8) | ||
| Marital status [n, %] | |||||
| widowed | 12 (27.3) | 4 (16.0) | 16 (23.2) | ||
| not married/single | 6 (13.6) | 4 (16.0) | 10 (14.5) | ns | |
| married | 26 (59.1) | 17 (65.4) | 43 (62.3) | ||
| Living status [n, %] | |||||
| Alone | 25 (50.0) | 9 (33.3) | 34 (44.7) | ns | |
| with family | 25 (50.0) | 17 (65.4) | 42 (55.3) | ||
| C-reactive Protein (CRP) (mg/L) [Mean±SD] | |||||
| 0.0019±0.003 | 0.0011±0.0011 | 0.0017±0.0025 | ns | ||
| Diseases | |||||
| CIRS [n, %] | |||||
| <=6 | 36 (72.0) | 20 (76.9) | 56 (73.7) | ns | |
| >6 | 14 (298.0) | 6 (23.1) | 20 (26.3) | ||
| QTCL [n, %] | |||||
| no | 4 (8.3) | 2 (7.7) | 6 (8.1) | ns | |
| not known | 44 (91.7) | 24 (92.3) | 68 (91.9) | ||
| Numbers medications taken [n, %] | |||||
| <4 | 31 (62.0) | 15 (57.7) | 46 (60.5) | ns | |
| ≥4 | 19 (38.0) | 11 (42.3) | 30 (39.5) | ||
| hypertension [n, %] | |||||
| no | 27 (54.0) | 11 (42.3) | 38 (50.0) | ||
| mild | 2 (4.0) | 0 (0.0) | 2 (2.6) | ns | |
| yes | 21 (42.0) | 15 (57.7) | 36 (47.4) | ||
| angina pectoris [n, %] | |||||
| no | 49 (98.0) | 23 (92.0) | 72 (96.0) | ||
| mild | 1 (2.0) | 1 (4.0) | 2 (2.7) | ns | |
| yes | 0 (0.0) | 1 (4.0) | 1 (1.3) | ||
| heart diseases, pacemaker [n, %] | |||||
| no | 46 (92.0) | 23 (88.5) | 69 (90.8) | ||
| mild | 2 (4.0) | 1 (3.8) | 3 (3.9) | ns | |
| yes | 2 (4.0) | 2 (7.7) | 4 (5.3) | ||
| stroke, cerebral ischemia [n, %] | |||||
| no | 43 (87.8) | 24 (92.3) | 67 (89.3) | ||
| mild | 2 (4.1) | 2 (7.7) | 4 (5.3) | ns | |
| yes | 4 (8.2) | 0 (0.0) | 4 (5.3) | ||
| cancer [n, %] | |||||
| no | 39 (78.0) | 22 (84.6) | 61 (80.3) | ||
| probable | 1 (2.0) | 0 (0.0) | 1 (1.3) | ns | |
| yes | 10 (20.0) | 4 (15.4) | 14 (18.4) | ||
| diabetes [n, %] | |||||
| no | 43 (86.0) | 22 (84.6) | 65 (85.5) | ||
| mild | 1 (2.0) | 1 (3.8) | 2 (2.6) | ns | |
| yes | 6 (12.0) | 3 (11.5) | 9 (11.8) | ||
| osteoarthritis and osteoporosis [n, %] | |||||
| no | 16 (32.0) | 19 (73.1) | 35 (46.1) | 0.001 | |
| probable | 2 (4.0) | 2 (7.7) | 4 (5.3) | 0.001 | |
| yes | 32 (64.0) | 7 (19.2) | 37 (48.7) | <0.001 | |
| chronic bronchitis | |||||
| no | 46 (92.0) | 23 (88.5) | 69 (9.08) | ||
| mild | 3 (6.0) | 1 (3.8) | 4 (5.3) | ns | |
| yes | 1 (2.0) | 2 (7.7) | 3 (3.9) | ||
| thyroid or other endocrine diseases [n, %] | |||||
| no | 40 (80.0) | 25 (96.2) | 65 (85.5) | ||
| mild | 1 (2.0) | 0 (0.0) | 1 (1.3) | ns | |
| yes | 9 (18.0) | 1 (3.8) | 10 (13.2) | ||
| kidney diseases [n, %] | |||||
| no | 49 (98.0) | 24 (92.3) | 73 (96.1) | ||
| mild | 1 (2.0) | 0 (0.0) | 1 (1.3) | ns | |
| yes | 0 (0.0) | 2 (7.7) | 2 (2.6) | ||
| liver/gallbladder disease [n, %] | |||||
| no | 40 (80.0) | 20 (76.9) | 60 (78.9) | ||
| mild | 1 (2.0) | 0 (0.0) | 1 (1.3) | ns | |
| yes | 9 (18.0) | 6 (23.1) | 15 (19.7) | ||
| intestinal diseases [n, %] | |||||
| no | 32 (64.0) | 23 (88.5) | 55 (72.4) | 0.02 | |
| mild | 2 (4.0) | 1 (3.8) | 3 (3.9) | 0.06 | |
| yes | 16 (32.0) | 2 (7.7) | 18 (23.7) | 0.02 | |
| stomach and gullet diseases [n, %] | |||||
| no | 31 (62.0) | 20 (76.9) | 51 (67.1) | ||
| mild | 1 (2.0) | 1 (3.8) | 2 (2.6) | ns | |
| yes | 18 (36.0) | 5 (19.2) | 23 (30.3) | ||
| skin diseases [n, %] | |||||
| no | 48 (96.0) | 23 (88.5) | 71 (93.4) | ||
| probable | 1 (2.0) | 0 (0.0) | 1 (1.3) | ns | |
| yes | 1 (2.0) | 3 (11.5) | 4 (5.1) | ||
| blood diseases [n, %] | |||||
| no | 46 (92.0) | 25 (96.2) | 71 (93.4) | ||
| mild | 0 (0.0) | 1 (3.8) | 1 (1.3) | ns | |
| yes | 4 (8.0) | 0 (0.0) | 4 (5.3) | ||
| vascular diseases [n, %] | |||||
| no | 43 (87.8) | 22 (84.6) | 65 (86.7) | ||
| mild | 1 (2.0) | 0 (0.0) | 1 (1.3) | ns | |
| yes | 5 (10.2) | 4 (15.4) | 9 (12.0) | ||
| eye diseases with low vision [n, %] | |||||
| no | 42 (84.0) | 23 (88.5) | 65 (85.5) | ns | |
| yes | 8 (16.0) | 3 (11.5) | 11 (14.5) | ||
| ear diseases with hearing loss [n, %] | |||||
| no | 38 (76.0) | 11 (42.3) | 49 (64.5) | ||
| mild | 4 (8.0) | 6 (23.1) | 10 (13.2) | 0.01 | |
| yes | 8 (16.0) | 9 (34.6) | 17 (22.4) | ||
| peripheral neuropathies [n, %] | |||||
| no | 47 (94.0) | 26 (100.0) | 73 (96.1) | ns | |
| yes | 3 (6.0) | 0 (0.0) | 3 (3.9) | ||
| psychiatric diseases [n, %] | |||||
| no | 49 (98.0) | 26 (100.0) | 75 (98.7) | ns | |
| yes | 1 (2.0) | 0 (0.0) | 1 (1.3) | ||
| Glucose-6-phosphate dehydrogenase deficiency [n, %] | |||||
| no | 50 (100.0) | 26 (100.0) | 76 (100.0) | ns | |
| uncontrolled hyperthyroidism [n, %] | |||||
| no | 48 (98.0) | 26 (100.0) | 74 (98.7) | ns | |
| yes | 1 (2.0) | 0 (0.0) | 1 (1.3) | ||
| alcohol or drug abuse [n, %] | |||||
| no | 50 (100.0) | 26 (100.0) | 76 (100.0) | ns | |
| Anthropometry and state of health | |||||
| Body mass index (Kg/m2) [Mean±SD (Min-Max)] | |||||
| 27.3±5.5 (18.3 - 41.9) | 27.8±3.7 (19.9 - 35.0) | 27.4±5.0 (18.3 - 41.9) | |||
| Brachial girth (cm) [Mean±SD (Min-Max)] | |||||
| right | 30.2±4.1 (24 - 43) | 30.2±3.5 (24 - 37) | 30.2±3.9 (24 - 43) | ||
| left | 30.0±3.9 (23 - 41) | 29.6±3.5 (24 - 37) | 29.9±3.7 (23 - 41) | ||
| Calf girth (cm) [Mean±SD (Min-Max)] | |||||
| right | 36.7±4.4 (31 - 55) | 38.3±4.6 (32.5 - 52) | 37.3±4.5 (31 - 55) | ||
| left | 36.6±4.7 (30 - 56) | 38.1±3.9 (31.5 - 52) | 37.1±4.5 (30 - 56) | ||
| Hand grip test (Kg) [Mean±SD (Min-Max)] | |||||
| right | 21.2±5.5 (10.1 – 42.3) | 34.8±10.4 (12.0 - 59.5) | 25.9±9.9 (10.1 - 59.5) | <0.001 | |
| left | 19.6±5.2 (9.0 – 35.2) | 32.8±9.0 (15.0 - 50.8) | 24.1±9.2 (9.0 - 50.8) | <0.001 | |
| Peak expiratory flow (L/min) [Mean±SD (Min-Max)] | |||||
| 208.1±76.7 (65 - 355) | 356.2±132.4 (140 - 690) | 259.4±121.5 (65 - 690) | <0.001 | ||
| Timed up-and-go test (s) [Mean±SD (Min-Max)] | |||||
| 3.4±0.9 (2.2 - 6.2) | 2.9±0.5 (2.02 - 4.3) | 3.2±0.8 (2.02 - 6.2) | 0.007 | ||
| Weightlifting 1 (8 Kg females ; 11Kg males) [n, %] | |||||
| not lifted | 1 (2.0) | 2 (7.7) | 3 (3.9) | ns | |
| lifted up | 47 (98.0) | 24 (92.3) | 73 (96.1) | ||
| Weightlifting 2 (9 Kg females ; 12Kg males) [n, %] | |||||
| not lifted | 2 (4.0) | 2 (7.7) | 4 (5.3) | ns | |
| lifted up | 48 (96.0) | 24 (92.3) | 72 (94.7) | ||
| Weightlifting 3 (10 Kg females ; 13Kg males) [n, %] | |||||
| not lifted | 3 (6.3) | 2 (7.7) | 5 (6.6) | ns | |
| lifted up | 45 (93.8) | 24 (92.3) | 71 (93.4) | ||
| Clinical Dementia Rating Scale (CDR) [Mean±SD (Min-Max)] | |||||
| 0.08±0.33 (0.0 – 2.0) | 0.24±1.20 (0.0 – 6.0) | 0.14±0.75 (0.0 – 6.0) | |||
| Tinetti Scale [Mean±SD (Min-Max)] | |||||
| 27.2±1.6 (21 - 28) | 27.3±1.9 (20 - 28) | 27.3±1.7 (20 - 28) | |||
| Barthel Index [Mean±SD (Min-Max)] | |||||
| 0.9±1.5 (0 - 8) | 0.5±0.9 (0 - 2) | 0.8±1.3 (0 - 8) | |||
| Instrumental Activities of Daily living (IADL) [Mean±SD (Min-Max)] | |||||
| 0.04±0.2 (0 - 1) | 0.0±0.0 (0 - 0) | 0.03±0.2 (0 - 1) | |||
| Severity Index (SI-CIRS) [Mean±SD (Min-Max)] | |||||
| 1.4±0.2 (1 - 2.2) | 1.4±0.2 (1 - 1.9) | 1.4±0.2 (1 - 2.2) | |||
| Comorbidity Index (CI-CIRS) [Mean±SD (Min-Max)] | |||||
| 1.8±1.2 (0 - 5) | 1.9±1.4 (0 - 5) | 1.8±1.2 (0 - 5) |
Table 2.
Clinical scales for frailty assessment according to gender.
| Quantitative Variables | F n=50 |
M n=26 |
All n=76 |
χ2 Test |
Comparison gender column proportions |
|
|---|---|---|---|---|---|---|
| IFI [Mean±SD (Min-Max)] | ||||||
| 7.17±3.75 (1.75 – 19.50) |
5.80±2.87 (0.50 – 12.75) |
6.70±3.52 (0.50 – 19.50) |
||||
| SHARE-FIt [Mean±SD (Min-Max)] | ||||||
| 0.97±1.51 (-1.63 / 4.41) |
0.54±1.51 (-1.19 / 5.32) |
0.83±1.52 (-1.63 / 5.32) |
||||
| SHARE-FIt_clusters [n, %] | ||||||
| NF | 20 (40.0) | 20 (76.9) | 40 (52.6) | 0.002 | ||
| PF | 18 (36.0) | 4 (15.4) | 22 (28.9) | 0.009 | ||
| F | 12 (24.0) | 2 (7.7) | 14 (18.4) | |||
| CDR [Mean±SD (Min-Max)] | ||||||
| 0.08±0.33 (0.0 – 2.0) |
0.24±1.20 (0.0 – 6.0) |
0.14±0.75 (0.0 – 6.0) | ||||
Table 3.
Neuropsychological batteries for the study population (N=76) according to gender.
| Females | Males | All | ||||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |
| MMSE | 28.75 | 1.34 | 28.46 | 1.84 | 28.65 | 1.52 |
| GDS | 5.85 | 5.51 | 5.04 | 5.28 | 5.58 | 5.41 |
| EMQ | 52.00 | 20.38 | 50.13 | 19.63 | 51.38 | 20.01 |
| CRI-q Total score | 119.71 | 20.51 | 124.00 | 14.94 | 121.14 | 18.84 |
| Raven’s colored progressive matrices | 27.13 | 5.73 | 28.08 | 7.79 | 27.44 | 6.45 |
| Story Recall | 12.60 | 4.04 | 11.45 | 4.15 | 12.22 | 4.08 |
| RAVLT, immediate recall | 44.17 | 11.03 | 39.25 | 8.95 | 42.53 | 10.58 |
| RAVLT, delayed recall | 9.35 | 3.06 | 7.88 | 3.13 | 8.86 | 3.14 |
| FCSRT – Immediate free recall (IFR) | 29.63 | 4.85 | 27.25 | 7.33 | 28.83 | 5.86 |
| FCSRT – Immediate total recall (ITR) | 35.60 | 1.61 | 34.33 | 5.88 | 35.18 | 3.64 |
| FCSRT – delayed free recall (DFR) | 10.48 | 2.19 | 9.63 | 2.39 | 10.19 | 2.28 |
| FCSRT – delayed total recall (DTR) | 11.85 | 0.87 | 11.50 | 2.06 | 11.74 | 1.38 |
| FCSRT – index of sensitivity of cueing (ISC) | 0.96 | 0.10 | 0.91 | 0.19 | 0.94 | 0.14 |
| ROCF - Recall | 13.14 | 5.03 | 16.27 | 7.35 | 14.18 | 6.04 |
| Digit Span Forward | 5.35 | 1.12 | 5.67 | 1.17 | 5.46 | 1.14 |
| Digit Span Backward | 4.19 | 1.04 | 4.33 | 1.20 | 4.24 | 1.09 |
| FNAT (% of correct responses) | 12.48 | 3.44 | 11.88 | 3.07 | 12.28 | 3.31 |
| Token Test | 32.48 | 2.20 | 32.69 | 2.71 | 32.55 | 2.36 |
| FPL | 36.60 | 9.12 | 33.21 | 10.31 | 35.47 | 9.60 |
| FPC | 40.96 | 9.26 | 41.58 | 11.58 | 41.17 | 10.02 |
| B.A.D.A. – Auditory sentence comprehension | 57.42 | 2.47 | 58.50 | 1.72 | 57.78 | 2.30 |
| B.A.D.A. – Action naming | 15.02 | 2.48 | 15.79 | 2.69 | 15.29 | 2.56 |
| B.A.D.A. – Objects naming | 17.09 | 2.28 | 18.00 | 1.35 | 17.40 | 2.05 |
| ROCF - Copy | 31.28 | 3.27 | 31.60 | 3.57 | 31.39 | 3.35 |
| De Renzi test,right upper limb | 68.67 | 3.98 | 68.33 | 3.96 | 68.56 | 3.95 |
| De Renzi test_left upper limb | 69.98 | 3.06 | 70.13 | 2.59 | 70.03 | 2.89 |
| TMT_A (sec) | 46.46 | 22.14 | 40.54 | 12.98 | 44.49 | 19.67 |
| TMT_B (sec) | 162.31 | 98.21 | 161.08 | 143.49 | 161.90 | 114.26 |
| TMT_B-A (sec) | 115.85 | 93.04 | 120.54 | 137.56 | 117.42 | 108.93 |
| TMT_B/A | 3.69 | 1.80 | 3.84 | 2.77 | 3.74 | 2.15 |
Legend: SD = Standard Deviation; Mini Mental State Examination (MMSE); Geriatric Depression Scale (GDS); Everyday Memory Questionnaire (EMQ); Cognitive Reserve Index - questionnaire (CRI-q); Rey Auditory Verbal Learning Test (RAVLT); Free and Clued Selective Reminding Test (FCSRT); Rey–Osterrieth Complex Figure (ROCF); Face-name Association task (FNAT); Phonemic verbal fluency (FPL); Semantic verbal fluency (FPC); Battery for the Assessment of Aphasic Disorders (B.A.D.A); Trail Making Test (TMT); seconds (sec).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



