
Submitted:
16 March 2024
Posted:
18 March 2024
You are already at the latest version
Abstract
Recently intraductal carcinoma of the prostate (IDCP) has attracted increasing interest owing to its unfavorable prognoses. To effectively identify the IDCP-specific gene expression profile, we took a novel approach of characterizing a typical IDCP case using spatial gene expression analysis. A formalin-fixed, paraffin-embedded sample was subjected to Visium CytAssist Spatial Gene Expression analysis. IDCP within invasive prostate cancer sites was recognized as a distinct cluster separate from other invasive cancer clusters. Highly expressed genes defining the IDCP cluster, such as MUC6, MYO16, NPY, and KLK12, reflected the aggressive nature of high-grade prostate cancer. IDCP sites also showed increased hypoxia markers HIF1A, BNIP3L, PDK1, and POGLUT1; decreased fibroblast markers COL1A2, DCN, and LUM; and decreased immune cell markers CCR5 and FCGR3A. Overall, these findings indicate that the hypoxic tumor microenvironment and reduced accessibility to immune cells, which reflect the pathological characteristics of IDCP, may influence the aggressiveness of high-grade prostate cancer.
Keywords:
spatial gene expression analysis
; intraductal carcinoma of the prostate (IDCP)
; hypoxic markers
; immune cells
; tumor microenvironment
1. Introduction
Intraductal carcinoma of the prostate (IDCP) is a condition in which atypical cells from outside the glandular ducts invade and proliferate in normal glandular structures, leaving behind some basal cells and showing a cribriform morphology and extensive growth pattern. In 1996, McNeal et al. first reported IDCP with invasive cancer [1]. Since then, IDCP has received increasing attention because of its association with poor prognosis. The presence of IDCP during radical prostatectomy has been reported to be associated with a higher Gleason score, larger tumor volume, extraprostatic extension, squamous cell carcinoma at the resection margin, and accelerated disease progression [2,3,4,5]. Further, patients with localized and advanced prostate cancer (PCa) with IDCP have been reported to show significantly worse recurrence-free and overall survival rates [6,7,8,9].
For these reasons, IDCP was first described by the International Society of Urologic Pathology in 2014 [10] and subsequently included in the 2016 World Health Organization Prostate Tumor Classification [11], 2017 American Society of Pathology guidelines, and 2019 National Comprehensive Cancer Network (NCCN) guidelines [12].
Reports from Western countries have shown that homologous recombination (HR) gene mutations, including BRCA mutations, in addition to TMPRSS2-ERG fusion gene and TP53, RB1, and PTEN deletions, are frequently detected in patients with IDCP [13,14,15,16]. Interestingly, one study reported the presence of BRCA2 mutations in approximately 42% of IDCP cases [17,18]; further, the NCCN guidelines state that early genetic testing should be considered in prostate cancer patients with IDCP. Therefore, identifying IDCP-specific genetic abnormalities will contribute to the elucidation of molecular mechanisms underlying IDCP pathogenesis and the promotion of precision medicine.
Prostate cancer is extremely heterogeneous; therefore, gene expression analysis specific to IDCP lesions using conventional bulk gene analysis is impossible. Single-cell RNA-seq allows an understanding of tumor heterogeneity based on gene expression at the single-cell level. However, as IDCP is a morphology-based diagnosis, application of single-cell RNA-seq is unsuitable because of the loss of spatial information. Therefore, in this study, we made a groundbreaking attempt to analyze the gene abnormalities characteristic of IDCP sites while maintaining the spatial information of IDCP using spatial gene expression analysis technology.
2. Materials and Methods
2.1. IDCP Diagnosis
We retrospectively reviewed patients who underwent total prostatectomy for PCa at Ehime University Hospital and selected suspected IDCP cases. For these patients, immunohistochemistry was performed on 10% neutral buffered formalin-fixed and paraffin-embedded surgical tissue samples, which were sectioned on a microtome (3–5 μm thick) and stained according to standard protocols. An anti-basal cell antibody (p63 antibody + HMW cytokeratin antibody) purchased from Proteintech (US) was used to stain the basal cells, and Hoechst 33342 (dilution 1:2000; Molecular Probes) was used to stain the nuclei.
Three pathologists from Ehime University Hospital, including a skilled U.S pathologist specializing in IDCP diagnosis, reviewed the pathology reports to identify cases suggestive of IDCP and to determine the presence of IDCP indicators. Finally, one case was used for the study.
This study was approved by the Institutional Review Board of Ehime University (Nos. 2108006, 2109014, and 2205001) and was conducted according to the principles of the Declaration of Helsinki. Written informed consent was obtained from the patient for publication of the case report and accompanying images.
2.2. Spatial Transcriptomics (CytAssist Visium)
Spatial transcriptomics analyses were performed as previously described (Watanabe et al. 2023) [19]. Formalin-fixed, paraffin-embedded (FFPE) samples that passed the RNA quality control (DV200 > 50%) were used for spatial transcriptomic construction and sequencing. The tissues were prepared according to the Visium CytAssist Spatial Gene Expression for FFPE-Tissue Preparation Guide (CG000518, 10x Genomics, CA, USA). Sequencing was performed at the Research Institute for Microbial Diseases, Osaka University. Libraries were sequenced using an MGI DNBSEQ-G400RS (MGI Tech Co., SZX, CN). The Space Ranger pipeline v2022.0705.1 (10x Genomics, CA, USA) and the GRCh38-2020-A reference were used to process FASTQ files. The sequencing results were guaranteed to be accurate as follows.
Number of reads: 366,120,606; number of spots under tissue: 4,763; median genes per spot: 5,665; mean number of reads under tissue per spot: 70,197.
t-SNE plots and violin plots were run and plotted using the Loupe Browser (10x genomics, CA, USA). Trajectory and pathway enrichment analyses were performed and plotted using Partek flow software (Partek Incorporated, MO, USA).
3. Results
3.1. Diagnosis of IDCP and Clustering by Spatial Gene Expression Analysis
A 62-year-old man diagnosed with prostate adenocarcinoma (cT3aN0M0, high risk, PSA 31.5 ng/mL), underwent a robot-assisted laparoscopic prostatectomy. Basal cell staining was performed on FFPE slides of total prostatectomy specimens with a Gleason score 4+5 prostate cancer background. Cribriform morphological growth of the tumor was evident in the normal glandular ducts with preserved basal cells, leading to a diagnosis of IDCP (Figure 1A,B). Spatial gene expression analysis (CytAssist Visium) categorized the prostate tissue cells into 10 clusters, with cluster 10 identified as an independent cluster corresponding to the IDCP region (Figure 1C,D). Clusters of invasive cancer lesions proximal to IDCP on the pathology slides exhibited gene expression patterns similar to those of the IDCP clusters on the t-SNE plot, whereas distant clusters showed distinct patterns (Figure 1E,F). Trajectory analysis further confirmed the lineage similarity between IDCPs and the neighboring invasive carcinomas (Figure 1G).
The 20 most highly expressed genes in the IDCP (cluster 10) and non-IDCP regions (Clusters 1-9) are shown in Figure 1F. Notably, MUC6, MYO16, NPY, and KLK12 emerged as highly expressed genes defining the IDCP clusters, in contrast to genes from the tumor microenvironment, such as LTF, MMP, ELN, and COL3A1, which were relatively highly expressed in the non-IDCP clusters (Figure 1H). The volcano plot illustrates highly expressed genes in the IDCP and non-IDCP regions (Figure 1I). Additionally, heat maps underscored the differences in gene expression between the IDCP and non-IDCP regions (Figure 1J).
3.2. Visualization of Epithelial Cell, Androgen Receptor (AR) Signature Gene,and Other Upregulated Gene Marker Expression in the IDCP Region
Spatial gene expression analysis revealed upregulation of epithelial markers EPCAM and KRT8 across all clusters (Figure 2A), consistent with the findings from the violin plots (Figure 2B). Moreover, examination of gene expression and violin plots demonstrated high expression of a group of AR signature genes, including KLK3, AR, TMPRSS2, NKX3.1, and AMACR across all clusters (Figure 2C,D), indicating their tumor origin.
Furthermore, spatial gene expression analysis and violin plots showed the upregulation of MUC6, MYO16, NPY, and KLK12 in the IDCP region, with expression diminishing as the distance from the IDCP region increased (Figure 2E,F). Additionally, gene expression analysis and violin plots revealed a relatively high expression of homologous recombination repair (HRR) genes, such as CHEK2, TOP2A, TOP2B, PALB2, and SPOP, in the IDCP region (Figure 3A,B). However, upregulation of BRCA1 or BRCA2 was not observed.
TMPRSS2, a known IDCP-associated gene, was highly expressed at the IDCP site without any evidence of PTEN downregulation (Figure 3C,D).
3.3. Visualization of the Expression of IDCP Fibroblast Markers, Immune Cell Markers, and Hypoxia Markers
Spatial gene expression analysis and violin plots indicated downregulation of the fibroblast markers COL1A2, DCN, and LUM in the IDCP cluster (Figure 4A,B). Moreover, spatial gene expression analysis and violin plots demonstrated a low expression of the immune cell markers CCL5, FCG3A, and TRAC in the IDCP cluster (Figure 4C,D). Spatial gene expression analysis and violin plots revealed no significant differences in the epithelial cell markers between the clusters (Figure 4E,F). Additionally, analysis of the gene expression and violin plots revealed high expression of the hypoxia markers HIF1A, BNIP3L, PDK1, and POGLUT1 in the IDCP cluster (Figure 4G,H). This suggested that the loss of immune cells and accumulation of hypoxic markers limited to the IDCP site may be attributed to the anatomic isolation of the IDCP site.
4. Discussion
IDCP is a significant pathological finding with clinical prognostic implications. Haffner et al. conducted microdissection of both IDCP and surrounding invasive carcinoma sites and discerned site-specific gene expression patterns through their comparison. Consequently, they proposed a retrograde colony formation model wherein the TMPRSS2-ERG fusion gene-positive/PTEN loss component of invasive carcinoma infiltrates normal glandular ducts, forming IDCPs [2]. However, the precise sampling of lesion sites via microdissection is challenging and labor-intensive. Through single-cell analysis, Wong et al. compared cribriform carcinoma tissues with benign prostate tissues to elucidate the gene expression characteristics of cribriform prostate cancer [20]. Nonetheless, this study associated invasive cribriform carcinoma with IDCP but did not examine IDCP-specific gene abnormalities. Moreover, single-cell analyses lack spatial information, which impedes the identification of IDCP-derived cells. Therefore, we endeavored to identify IDCP-specific gene aberrations using spatial gene expression analysis.
An accurate diagnosis of IDCP is imperative for suitable treatment. IDCP has a significant prognostic value even in low-grade prostate cancer and should not be disregarded [21,22,23]. However, the classification of precursor-like (isolated) IDCP, a borderline lesion resembling HGPIN without a discernible cribriform pattern—remains contentious [24]. Therefore, in our study, we included samples from patients with a typical IDCP morphology, associated with high-grade prostate cancer. Following the IDCP diagnosis by two pathologists at our institution, the final diagnosis was confirmed by a pathologist in the United States who was experienced in diagnosing IDCP. The diagnosed case presented a typical IDCP morphology with surrounding invasive carcinoma, featuring a Gleason Score of 4+5 and a cribriform pattern tumor infiltrating the normal glandular ducts while retaining basal cells [25].
Spatial gene expression analysis revealed genetically similar tumors in and around the IDCP site. These tumors were TMPRSS2-positive but did not exhibit PTEN downregulation. As spatial gene expression analysis cannot identify mutations, potential PTEN mutations may have been overlooked. Nevertheless, genes upregulated at the IDCP site resembled those in clusters 1 and 5 adjacent to the IDCP. These findings support the hypothesis that the surrounding invasive carcinoma infiltrates normal glandular ducts. It is speculated that tumor cell clusters that have acquired high invasiveness form IDCP by invading and proliferating in normal glandular ducts with low tumor density.
MUC6, MYO16, NPY, and KLK12 were upregulated at the IDCP site. MUC6, which encodes a member of the mucin protein family, is an organ specific antigen and plays a pivotal role in epithelial surface cryoprotection. Some literatures insists that MUC16 serves as a tumor marker in gastric and other cancers [26,27]. Compared to other KLK genes, both KLK6 and KLK12 are associated with increased invasive potential [28,29]. MYO16, which encodes the myosin XVI protein, regulates neuronal morphogenesis [30]. In addition, NPY (neuropeptide Y), a member of the NPY family, is widely expressed in the central nervous system, and its receptor, NPY-1R, is associated with the proliferative potential of prostate cancer [31,32]. These results indicate that IDCP may be involved in prostate cancer neuroendocrine differentiation, although the NE signature markers CHGA, SYP, NCAM1 (CD56), NKX2.1, MYCN, and AURKA were not elevated in the present case.
Heterozygous deletions of PTEN, TP53, and RB1 are important genetic alterations associated with neuroendocrine prostate cancer (NEPC), and are frequently observed in IDCP, suggesting possible molecular similarities between NEPC and IDCP. In a limited case series, Ikeda et al. observed the components of IDCP in nine patients with NEPC for whom tissue specimens were available at diagnosis [33]. Thus, the identification of IDCP may serve as a potential predictor of NEPC development; however, the association between IDCP and NEPC remains unclear and warrants further investigation.
IDCP upregulates several homologous recombination repair (HRR) genes. In the present case, increased expression of TOP2A, TOP2B, and SPOP was observed. In a previous report, accumulation of TOP2A induced by SPOP mutations was found to facilitate prostate cancer progression through the accumulation of DNA damage, and etoposide was found effective against SPOP-mutated prostate cancer [35]. In the present case, TOP2A upregulation and SPOP expression suggested the possible efficacy of TOP2A inhibitors, Chek2 and Palb2 were mildly upregulated at IDCP sites, but no overall upregulation was observed, further, high expression of HRR gene abnormalities suggested the potential efficacy of PARP inhibitors.
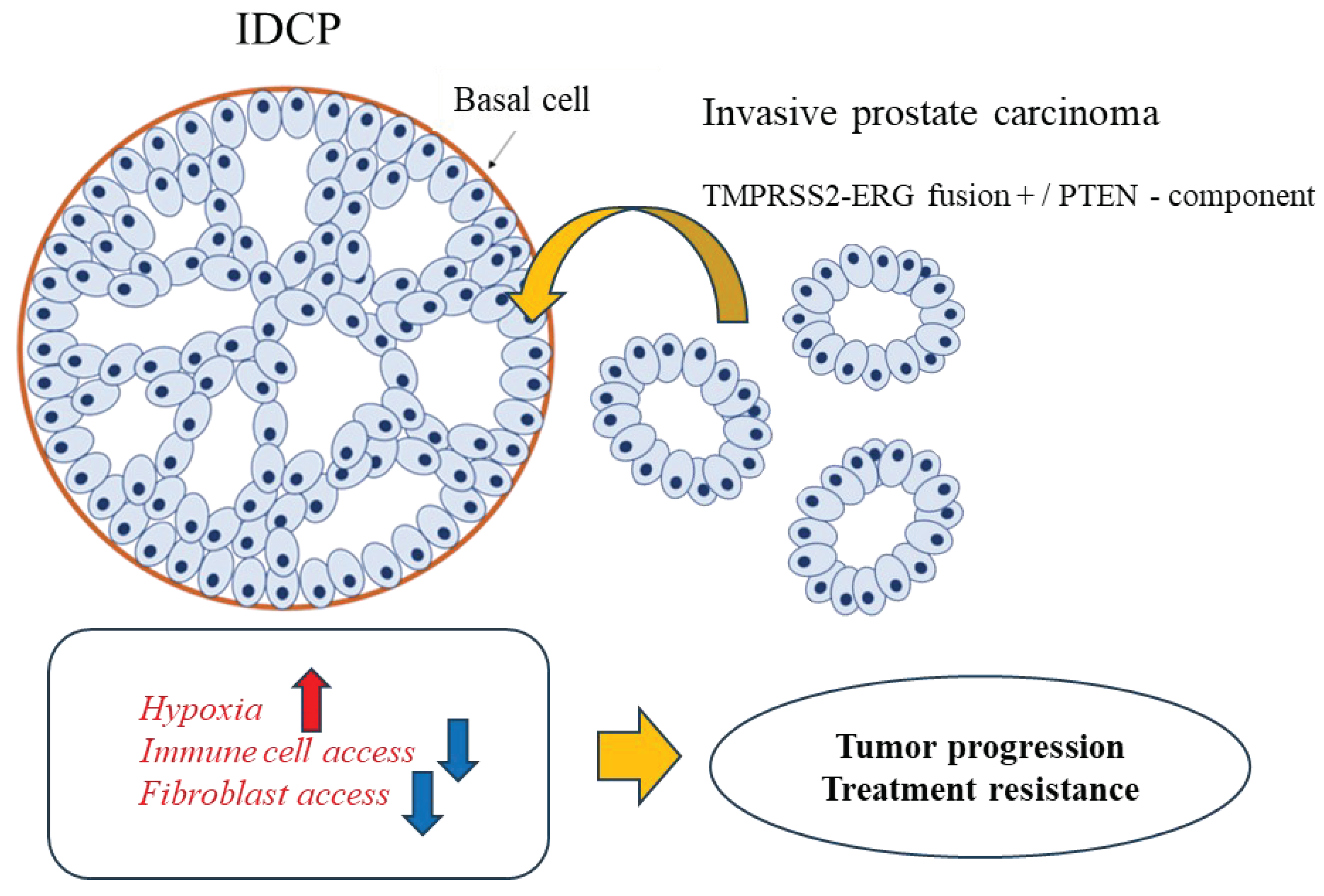
The decreased expression of fibroblast markers COL1A2, DCN, and LUM, and immune cell markers CCR5 and FCGR3A at the IDCP site probably reflects poor cellular access to the tumor microenvironment owing to the anatomic isolation of IDCP. Fibroblast marker genes associated with stromal fibrosis contribute to malignant transformation through the proliferation of cancer-associated fibroblasts (CAFs) in various cancers [36,37,38,39]. However, considering the recent findings regarding the presence of cancer-promoting and cancer-suppressing fibroblasts [40], decreased numbers of tumor-suppressing fibroblasts and immune cells in the IDCP region may contribute to malignant transformation. Furthermore, the elimination of immune cells from the inherently "immune-cold" tumor microenvironment of prostate cancer may render immune checkpoint inhibitors ineffective [41]. Furthermore, IDCP sites exhibited increased levels of hypoxia markers such as HIF1A, BNIP3L, PDK1, and POGLUT1. IDCPs growing within narrowly isolated normal glandular ducts are susceptible to hypoxia, which induces tumor cell starvation and hypoxic stress, increases glycolytic metabolism and angiogenesis, and increases the potential for metastasis and invasion. Thus, IDCP may promote malignant transformation and resistance to therapy by inducing hypoxia and inaccessibility of immune cells owing to its morphological features (Figure 5). Focusing on the hypoxic state of IDCP, patients with prostate cancer and IDCP may benefit from inhibitors targeting HIF1A. In the present study, no increase in endothelial cell marker levels was observed despite the presence of hypoxia at the IDCP site. This implies that IDCP is an isolated and anomalous lesion, in which angiogenesis is less likely to be induced.
As this was a comparative analysis between IDCP and tumor sites with similar gene expression levels, identifying dramatic differences in gene expression was difficult. However, this study clearly demonstrated that IDCP can be recognized as a distinct cluster that tends to show the characteristic expression of markers related to immune cells, fibroblasts, and hypoxia. Because this was a single case study, the need to examine more cases in the future is acknowledged. As spatial gene expression analysis is dot-based, each dot contains the gene expression of approximately 10 cells. In fact, all 10 clusters of tumor cells classified in this study contained a mixture of immune cell and fibroblast markers. Integrating single-cell analysis data using the same sample through bioinformatics and introducing high-resolution spatial gene expression analysis at the single-cell level is thus necessary to perform a more accurate analysis. This will allow for a more accurate analysis.
5. Conclusion
Spatial gene expression analysis could identify IDCP-specific gene expression profiles effectively in a typical IDCP case. Our findings suggest that the morphological features of IDCP contribute to its poor accessibility for fibroblasts and immune cells, potentially playing a role in malignant transformation and therapeutic resistance. Overall, this study elucidates valuable markers and malignant mechanisms for diagnosing prostate cancer cases with IDCP, and provides novel personalized treatment options. Moving forward, we aim to further elucidate these mechanisms by expanding our sample size, integrating our data with single-cell analysis data, and implementing high-resolution spatial gene expression analysis techniques.
Author Contributions
For All authors have read and approved the manuscript. R W and T S: Project development, Data analysis, Manuscript writing/editing; N M and T K: Project development, Data analysis; M K and R K: Data collection.
Funding
This research was funded by JSPS KAKENHI (Grant Number 22K09449). Medical Research Grants of Takeda Science Foundation. Japanese Foundation for Prostate Research. Japanese Urological Association Young Research Grant. Takahashi Industrial and Economic Research Foundation
Institutional Review Board Statement
This study was approved by the Institutional Review Board of Ehime University (No. 2205001) and conducted according to the principles of the Declaration of Helsinki.
Informed Consent Statement
Written informed consent was obtained from all participants to publish the original article and accompanying images.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request. Data Availability Statement: The raw and processed data of spatial transcriptomics generated in this study are openly available in GEO at https://www.ncbi.nlm.nih.gov/geo/, GEO number {GSE230282}.
Acknowledgments
We express our sincere thanks to Dr. Michael Haffner at Fred Hutchinson Cancer Center for advising on IDCP diagnosis; to Dr. Daisuke Motooka at the Research Institute for Microbial Diseases (RIMD) at Osaka University for supporting the sequence of CytAssist Visium; and to Dr. Tony LH Chu of the Human Biology division, Fred Hutchinson Cancer Center, for his support in the data analysis. This work was supported by JSPS KAKENHI (Grant Number 22K09449), Medical Research Grants of Takeda Science Foundation, Japanese Foundation for Prostate Research and Japanese Urological Association Young Research Grant
Conflicts of Interest
The authors declare no conflicts of interest.
References
- McNeal, J.E.; Yemoto, C.E.M. Spread of Adenocarcinoma Within Prostatic Ducts and Acini. Morphologic and clinical correlations. Am. J. Surg. Pathol. 1996, 20, 802–814. [Google Scholar] [CrossRef] [PubMed]
- Haffner, M.C.; Weier, C.; Xu, M.M.; Vaghasia, A.; Gürel, B.; Gümüşkaya, B.; Esopi, D.M.; Fedor, H.; Tan, H.; Kulac, I.; et al. Molecular evidence that invasive adenocarcinoma can mimic prostatic intraepithelial neoplasia (PIN) and intraductal carcinoma through retrograde glandular colonization. J. Pathol. 2015, 238, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Tsuzuki, T. Intraductal carcinoma of the prostate: A comprehensive and updated review. Int. J. Urol. 2014, 22, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M. Intraductal carcinoma of the prostate: the whole story. Pathology 2013, 45, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Varma, M.; Delahunt, B.; Egevad, L.; Samaratunga, H.; Kristiansen, G. Intraductal carcinoma of the prostate: a critical re-appraisal. Virchows Arch. 2019, 474, 525–534. [Google Scholar] [CrossRef] [PubMed]
- Miura, N.; Mori, K.; Mostafaei, H.; Quhal, F.; Motlagh, R.S.; Pradere, B.; Laukhtina, E.; D’andrea, D.; Saika, T.; Shariat, S.F. The Prognostic Impact of Intraductal Carcinoma of the Prostate: A Systematic Review and Meta-Analysis. J. Urol. 2020, 204, 909–917. [Google Scholar] [CrossRef]
- Kimura, K.; Tsuzuki, T.; Kato, M.; Saito, A.M.; Sassa, N.; Ishida, R.; Hirabayashi, H.; Yoshino, Y.; Hattori, R.; Gotoh, M. Prognostic value of intraductal carcinoma of the prostate in radical prostatectomy specimens. Prostate 2014, 74, 680–687. [Google Scholar] [CrossRef]
- Zhao, T.; Liao, B.; Yao, J.; Liu, J.; Huang, R.; Shen, P.; Peng, Z.; Gui, H.; Chen, X.; Zhang, P.; et al. Is there any prognostic impact of intraductal carcinoma of prostate in initial diagnosed aggressively metastatic prostate cancer? Prostate 2015, 75, 225–232. [Google Scholar] [CrossRef]
- Kato, M.; Tsuzuki, T.; Kimura, K.; Hirakawa, A.; Kinoshita, F.; Sassa, N.; Ishida, R.; Fukatsu, A.; Kimura, T.; Funahashi, Y.; et al. The presence of intraductal carcinoma of the prostate in needle biopsy is a significant prognostic factor for prostate cancer patients with distant metastasis at initial presentation. Mod. Pathol. 2016, 29, 166–173. [Google Scholar] [CrossRef]
- Epstein, J.I.; Egevad, L.; Amin, M.B.; Delahunt, B.; Srigley, J.R.; Humphrey, P.A. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma: Definition of Grading Patterns and Proposal for a New Grading System. Am. J. Surg. Pathol. 2016, 40, 244–252. [Google Scholar] [CrossRef]
- Humphrey, P.A.; Moch, H.; Cubilla, A.L.; Ulbright, T.M.; Reuter, V.E. The 2016 WHO Classification of Tumours of the Urinary System and Male Genital Organs—Part B: Prostate and Bladder Tumours. Eur. Urol. 2016, 70, 106–119. [Google Scholar] [CrossRef] [PubMed]
- Network NCC NCCN clinical practice guidelines in oncology: prostate cancer, version 1. 2023.
- Han, B.; Suleman, K.; Wang, L.; Siddiqui, J.; Sercia, L.; Magi-Galluzzi, C.; Palanisamy, N.; Chinnaiyan, A.M.; Zhou, M.; Shah, R.B. ETS gene aberrations in atypical cribriform lesions of the prostate: implications for the distinction between intraductal carcinoma of the prostate and cribriform high-grade prostatic intraepithelial neoplasia. Am. J. Surg. Pathol. 2010, 34, 478–485. [Google Scholar] [CrossRef] [PubMed]
- Bettendorf, O.; Schmidt, H.; Staebler, A.; Grobholz, R.; Heinecke, A.; Boecker, W.; Hertle, L.; Semjonow, A. Chromosomal imbalances, loss of heterozygosity, and immunohistochemical expression of TP53, RB1, and PTEN in intraductal cancer, intraepithelial neoplasia, and invasive adenocarcinoma of the prostate. Genes, Chromosom. Cancer 2008, 47, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Wang, Y.; Zhang, J.; Hu, Q.; Zhi, F.; Zhang, S.; Mao, D.; Zhang, Y.; Liang, H. Significance of the TMPRSS2:ERG gene fusion in prostate cancer. Mol. Med. Rep. 2017, 16, 5450–5458. [Google Scholar] [CrossRef]
- Shah, R.B.; Shore, K.T.; Yoon, J.; Mendrinos, S.; McKenney, J.K.; Tian, W. PTEN loss in prostatic adenocarcinoma correlates with specific adverse histologic features (intraductal carcinoma, cribriform Gleason pattern 4 and stromogenic carcinoma). Prostate 2019, 79, 1267–1273. [Google Scholar] [CrossRef]
- Risbridger, G.P.; Taylor, R.A.; Clouston, D.; Sliwinski, A.; Thorne, H.; Hunter, S.; Li, J.; Mitchell, G.; Murphy, D.; Frydenberg, M.; et al. Patient-derived Xenografts Reveal that Intraductal Carcinoma of the Prostate Is a Prominent Pathology in BRCA2 Mutation Carriers with Prostate Cancer and Correlates with Poor Prognosis. Eur. Urol. 2015, 67, 496–503. [Google Scholar] [CrossRef]
- Taylor, R.A.; Fraser, M.; Rebello, R.J.; Boutros, P.C.; Murphy, D.G.; Bristow, R.G.; Risbridger, G.P. The influence of BRCA2 mutation on localized prostate cancer. Nat. Rev. Urol. 2019, 16, 281–290. [Google Scholar] [CrossRef]
- Watanabe, R.; Miura, N.; Kurata, M.; Kitazawa, R.; Kikugawa, T.; Saika, T. Spatial Gene Expression Analysis Reveals Characteristic Gene Expression Patterns of De Novo Neuroendocrine Prostate Cancer Coexisting with Androgen Receptor Pathway Prostate Cancer. Int. J. Mol. Sci. 2023, 24, 8955. [Google Scholar] [CrossRef]
- Wong, H.Y.; Sheng, Q.; Hesterberg, A.B.; Croessmann, S.; Rios, B.L.; Giri, K.; Jackson, J.; Miranda, A.X.; Watkins, E.; Schaffer, K.R.; et al. Single cell analysis of cribriform prostate cancer reveals cell intrinsic and tumor microenvironmental pathways of aggressive disease. Nat. Commun. 2022, 13, 1–21. [Google Scholar] [CrossRef]
- Miyai, K.; Divatia, M.K.; Shen, S.S.; Miles, B.J.; Ayala, A.G.; Ro, J.Y. Heterogeneous clinicopathological features of intraductal carcinoma of the prostate: a comparison between "precursor-like" and "regular type" lesions. . 2014, 7, 2518–26. [Google Scholar]
- Guo, C.C.; I Epstein, J. Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance. Mod. Pathol. 2006, 19, 1528–1535. [Google Scholar] [CrossRef]
- Robinson, B.D.; Epstein, J.I.; J, Z.; J, L.; G, S.; M, Z.; J, C.; P, S.; Z, L.; B, L.; et al. Intraductal Carcinoma of the Prostate Without Invasive Carcinoma on Needle Biopsy: Emphasis on Radical Prostatectomy Findings. J. Urol. 2010, 184, 1328–1333. [Google Scholar] [CrossRef]
- Varma, M.; I Epstein, J. Head to head: should the intraductal component of invasive prostate cancer be graded? Histopathology 2020, 78, 231–239. [Google Scholar] [CrossRef]
- Zong, Y.; Montironi, R.; Massari, F.; Jiang, Z.; Lopez-Beltran, A.; Wheeler, T.M.; Scarpelli, M.; Santoni, M.; Cimadamore, A.; Cheng, L. Intraductal Carcinoma of the Prostate: Pathogenesis and Molecular Perspectives. Eur. Urol. Focus 2020, 7, 955–963. [Google Scholar] [CrossRef]
- Fulgione, C.; Raffone, A.; Travaglino, A.; Arciuolo, D.; Santoro, A.; Cianfrini, F.; Russo, D.; Varricchio, S.; Raimondo, I.; Inzani, F.; et al. Diagnostic accuracy of HIK1083 and MUC6 as immunohistochemical markers of endocervical gastric-type adenocarcinoma: A systematic review and meta-analysis. Pathol. - Res. Pr. 2023, 241, 154261. [Google Scholar] [CrossRef] [PubMed]
- Yamanoi, K.; Fujii, C.; Yuzuriha, H.; Kumazawa, M.; Shimoda, M.; Emoto, K.; Asamura, H.; Nakayama, J. MUC6 expression is a preferable prognostic marker for invasive mucinous adenocarcinoma of the lung. Histochem. 2022, 157, 671–684. [Google Scholar] [CrossRef] [PubMed]
- Lose, F.; Batra, J.; O'Mara, T.; Fahey, P.; Marquart, L.; Eeles, R.A.; Easton, D.F.; Al Olama, A.A.; Kote-Jarai, Z.; Guy, M.; et al. Common variation in Kallikrein genes KLK5, KLK6, KLK12, and KLK13 and risk of prostate cancer and tumor aggressiveness. Urol. Oncol. Semin. Orig. Investig. 2011, 31, 635–643. [Google Scholar] [CrossRef] [PubMed]
- Korbakis, D.; Soosaipillai, A.; Diamandis, E.P. Study of kallikrein-related peptidase 6 (KLK6) and its complex with α1-antitrypsin in biological fluids. cclm 2017, 55, 1385–1396. [Google Scholar] [CrossRef] [PubMed]
- Yamanoi, K.; Fujii, C.; Yuzuriha, H.; Kumazawa, M.; Shimoda, M.; Emoto, K.; Asamura, H.; Nakayama, J. MUC6 expression is a preferable prognostic marker for invasive mucinous adenocarcinoma of the lung. Histochem. 2022, 157, 671–684. [Google Scholar] [CrossRef]
- Ruscica, M.; Dozio, E.; Boghossian, S.; Bovo, G.; Riaño, V.M.; Motta, M.; Magni, P. Activation of the Y1 Receptor by Neuropeptide Y Regulates the Growth of Prostate Cancer Cells. Endocrinology 2006, 147, 1466–1473. [Google Scholar] [CrossRef]
- Sigorski, D.; Wesołowski, W.; Gruszecka, A.; Gulczyński, J.; Zieliński, P.; Misiukiewicz, S.; Kitlińska, J.; Iżycka-Świeszewska, E. Neuropeptide Y and its receptors in prostate cancer: associations with cancer invasiveness and perineural spread. J. Cancer Res. Clin. Oncol. 2022, 149, 5803–5822. [Google Scholar] [CrossRef]
- Ikeda, J.; Ohe, C.; Ohsugi, H.; Matsuda, T.; Tsuta, K.; Kinoshita, H. Association of intraductal carcinoma of the prostate detected by initial histological specimen and neuroendocrine prostate cancer: A report of three cases. Pathol. Int. 2021, 71, 621–626. [Google Scholar] [CrossRef] [PubMed]
- Naito, Y.; Kato, M.; Nagayama, J.; Sano, Y.; Matsuo, K.; Inoue, S.; Sano, T.; Ishida, S.; Matsukawa, Y.; Tsuzuki, T.; et al. Recent insights on the clinical, pathological, and molecular features of intraductal carcinoma of the prostate. Int. J. Urol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, R.; Maekawa, M.; Hieda, M.; Taguchi, T.; Miura, N.; Kikugawa, T.; Saika, T.; Higashiyama, S. SPOP is essential for DNA–protein cross-link repair in prostate cancer cells: SPOP-dependent removal of topoisomerase 2A from the topoisomerase 2A-DNA cleavage complex. Mol. Biol. Cell 2020, 31, 478–490. [Google Scholar] [CrossRef]
- Hoang, K.N.L.; Anstee, J.E.; Arnold, J.N. The Diverse Roles of Heme Oxygenase-1 in Tumor Progression. Front. Immunol. 2021, 12, 658315. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Zhou, L.; Li, D.; Andl, T.; Zhang, Y. Cancer-Associated Fibroblasts Build and Secure the Tumor Microenvironment. Front. Cell Dev. Biol. 2019, 7, 60. [Google Scholar] [CrossRef] [PubMed]
- Ren, J.; Smid, M.; Iaria, J.; Salvatori, D.C.F.; van Dam, H.; Zhu, H.J.; Martens, J.W.M.; Dijke, P.T. Cancer-associated fibroblast-derived Gremlin 1 promotes breast cancer progression. Breast Cancer Res. 2019, 21, 1–19. [Google Scholar] [CrossRef] [PubMed]
- de Hosson, L.D.; Takkenkamp, T.J.; Kats-Ugurlu, G.; Bouma, G.; Bulthuis, M.; de Vries, E.G.E.; van Faassen, M.; Kema, I.P.; Walenkamp, A.M.E. Neuroendocrine tumours and their microenvironment. Cancer Immunol. Immunother. 2020, 69, 1449–1459. [Google Scholar] [CrossRef]
- Kobayashi, H.; Enomoto, A.; Woods, S.L.; Burt, A.D.; Takahashi, M.; Worthley, D.L. Cancer-associated fibroblasts in gastrointestinal cancer. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 282–295. [Google Scholar] [CrossRef]
- Séguier, D.; Adams, E.S.; Kotamarti, S.; D’anniballe, V.; Michael, Z.D.; Deivasigamani, S.; Olivier, J.; Villers, A.; Hoimes, C.; Polascik, T.J. Intratumoural immunotherapy plus focal thermal ablation for localized prostate cancer. Nat. Rev. Urol. 2023. [Google Scholar] [CrossRef]
Figure 1.
Diagnosis of IDCP and clustering by spatial gene expression analysis. (A) A 62-year-old man diagnosed with prostate adenocarcinoma (cT3aN0M0, high risk, PSA 31.5 ng/mL), underwent a robot-assisted laparoscopic prostatectomy. HE staining reveals tumor invasion within normal glandular ducts with surrounding invasive carcinoma (blue square; invasive cancer area, yellow square; IDCP area, yellow arrow; IDCP). (B) Basal cell staining was performed on a formalin-fixed paraffin-embedded slide of the total prostatectomy specimen with a prostate cancer background showing Gleason Score 4+5. Cribriform morphological growth of the tumor was found in the normal glandular ducts with preserved basal cells, and IDCP was diagnosed (blue square; invasive cancer area, yellow square; IDCP area, yellow arrow; IDCP). (C, D) Spatial gene expression analysis (CytAssist Visium) classifies the cells of the prostate tissue into 10 clusters. Of these 10 clusters, cluster 19 matches the IDCP region. (E, F) The clusters of invasive cancer lesions outside normal glandular ducts that were close to those of IDCP on the pathology slides and were also close to IDCP clusters on the t-SNE plot, suggesting a similar gene expression pattern. (G) Trajectory analysis showed that IDCPs were similar in lineage to the neighboring invasive carcinomas. (H) The 20 most highly expressed genes in the IDCP (Cluster 10) and non-IDCP regions (Cluster 1-9). (I) The volcano plot shows the highly expressed genes in the IDCP and non-IDCP regions H) Heat maps showed differences in gene expression between the IDCP and non-IDCP regions. (J) Heatmap illustrates a clear distinction between gene expression in IDCP regions (cluster 10) and non-IDCP regions (clusters 1-9).
Figure 1.
Diagnosis of IDCP and clustering by spatial gene expression analysis. (A) A 62-year-old man diagnosed with prostate adenocarcinoma (cT3aN0M0, high risk, PSA 31.5 ng/mL), underwent a robot-assisted laparoscopic prostatectomy. HE staining reveals tumor invasion within normal glandular ducts with surrounding invasive carcinoma (blue square; invasive cancer area, yellow square; IDCP area, yellow arrow; IDCP). (B) Basal cell staining was performed on a formalin-fixed paraffin-embedded slide of the total prostatectomy specimen with a prostate cancer background showing Gleason Score 4+5. Cribriform morphological growth of the tumor was found in the normal glandular ducts with preserved basal cells, and IDCP was diagnosed (blue square; invasive cancer area, yellow square; IDCP area, yellow arrow; IDCP). (C, D) Spatial gene expression analysis (CytAssist Visium) classifies the cells of the prostate tissue into 10 clusters. Of these 10 clusters, cluster 19 matches the IDCP region. (E, F) The clusters of invasive cancer lesions outside normal glandular ducts that were close to those of IDCP on the pathology slides and were also close to IDCP clusters on the t-SNE plot, suggesting a similar gene expression pattern. (G) Trajectory analysis showed that IDCPs were similar in lineage to the neighboring invasive carcinomas. (H) The 20 most highly expressed genes in the IDCP (Cluster 10) and non-IDCP regions (Cluster 1-9). (I) The volcano plot shows the highly expressed genes in the IDCP and non-IDCP regions H) Heat maps showed differences in gene expression between the IDCP and non-IDCP regions. (J) Heatmap illustrates a clear distinction between gene expression in IDCP regions (cluster 10) and non-IDCP regions (clusters 1-9).
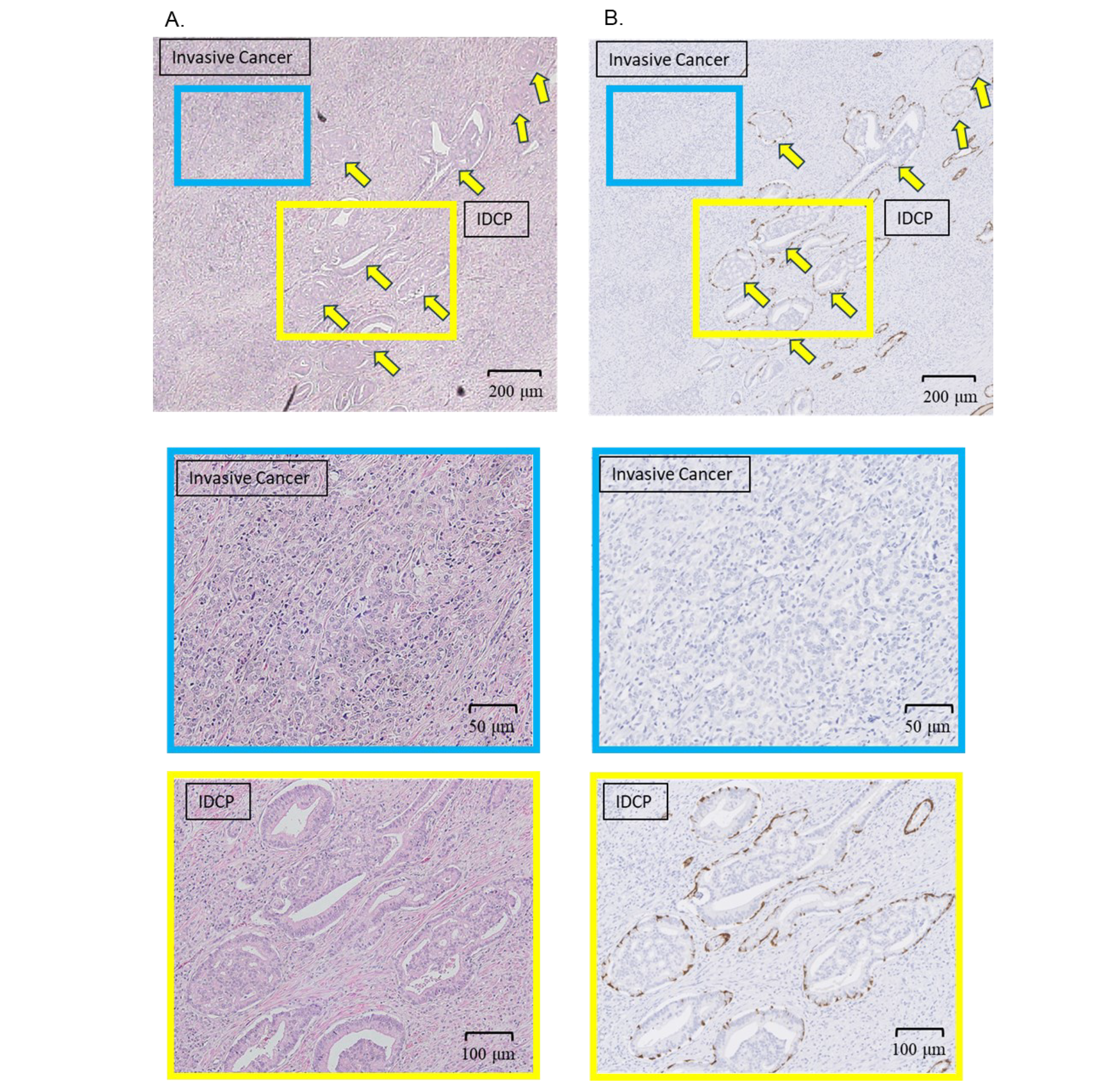
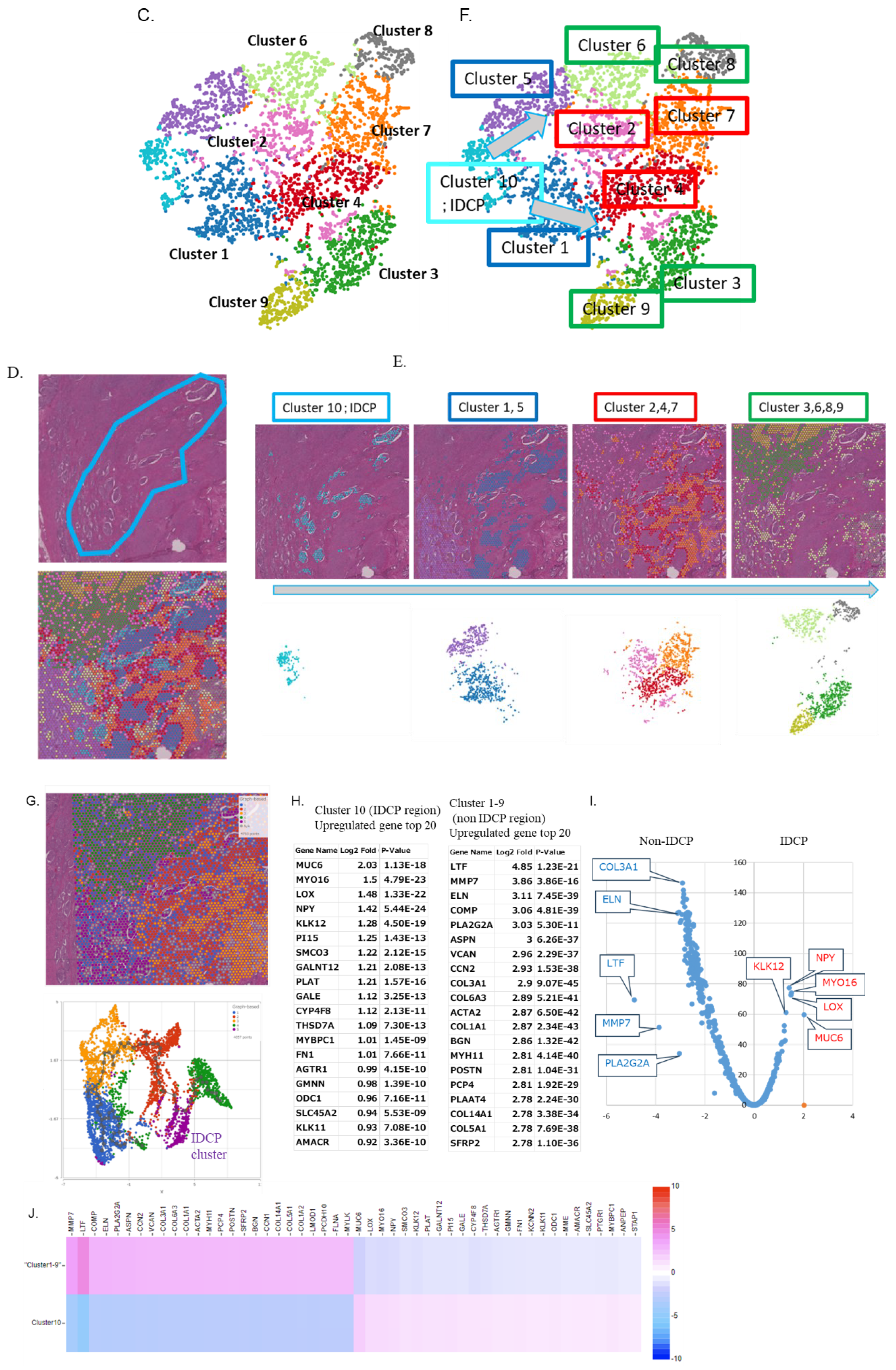
Figure 2.
Visualization of the expression of epithelial marker genes, AR signature genes, and other upregulated genes in the IDCP region. (A, B) Spatial gene expression analysis showing that the epithelial markers were upregulated in all clusters (A), with similar findings in the violin plot (B). (C, D) Spatial gene expression analysis (C) and violin plot (D) showing the expression of a group of AR signature genes. (E, F) Spatial gene expression analysis (E) and violin plots (F) demonstrating the expression of MUC6, MYO16, NPY, and KLK12.
Figure 2.
Visualization of the expression of epithelial marker genes, AR signature genes, and other upregulated genes in the IDCP region. (A, B) Spatial gene expression analysis showing that the epithelial markers were upregulated in all clusters (A), with similar findings in the violin plot (B). (C, D) Spatial gene expression analysis (C) and violin plot (D) showing the expression of a group of AR signature genes. (E, F) Spatial gene expression analysis (E) and violin plots (F) demonstrating the expression of MUC6, MYO16, NPY, and KLK12.
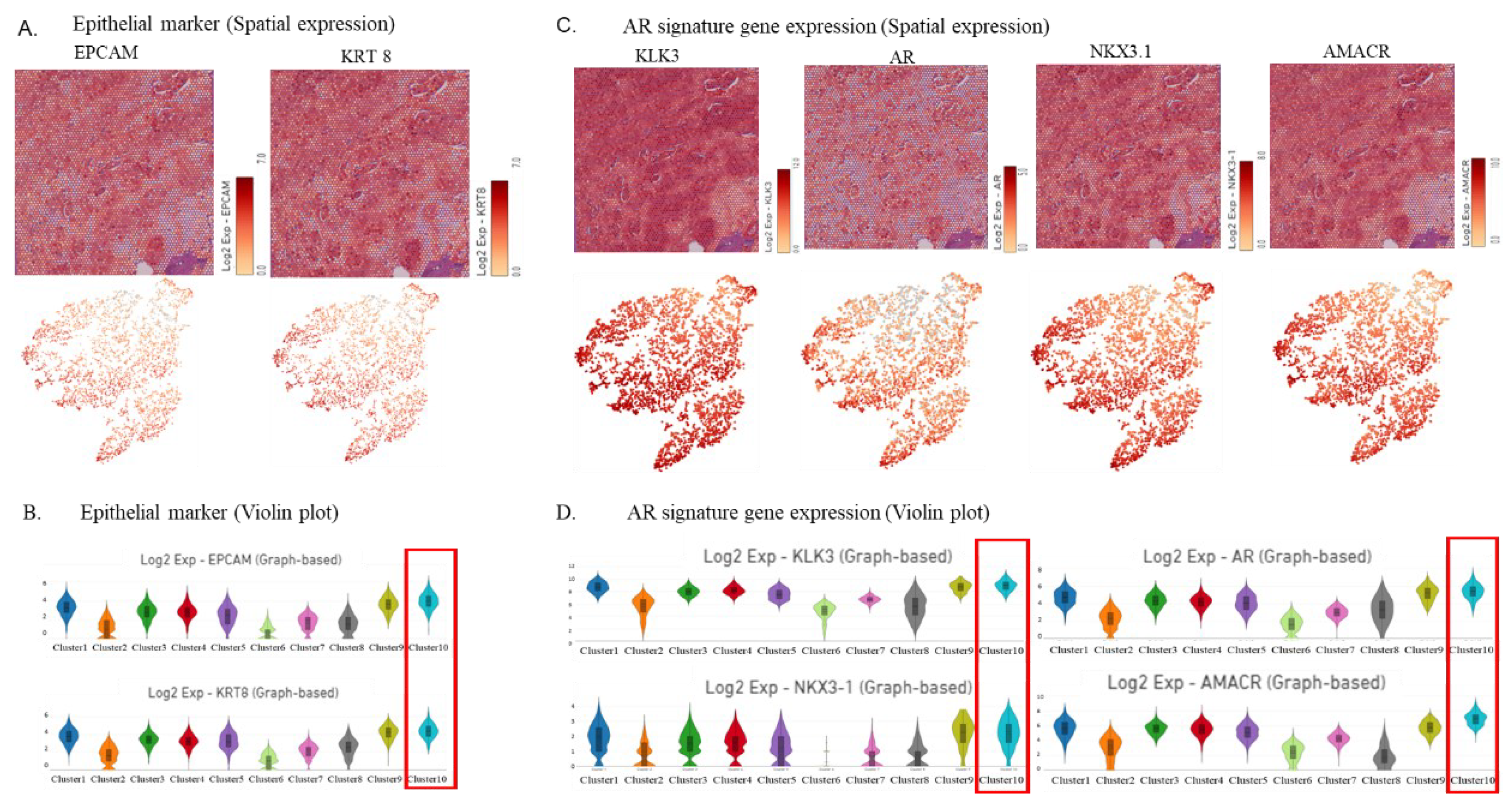
Figure 3.
Visualization of the expression of HRR genes. (A, B) Spatial gene expression analysis (A) and violin plot (B) showing homologous recombination repair (HRR) gene expression. (C, D) Spatial gene expression analysis (C) and violin plot (D) showing TMPRSS2 and PTEN expression.
Figure 3.
Visualization of the expression of HRR genes. (A, B) Spatial gene expression analysis (A) and violin plot (B) showing homologous recombination repair (HRR) gene expression. (C, D) Spatial gene expression analysis (C) and violin plot (D) showing TMPRSS2 and PTEN expression.
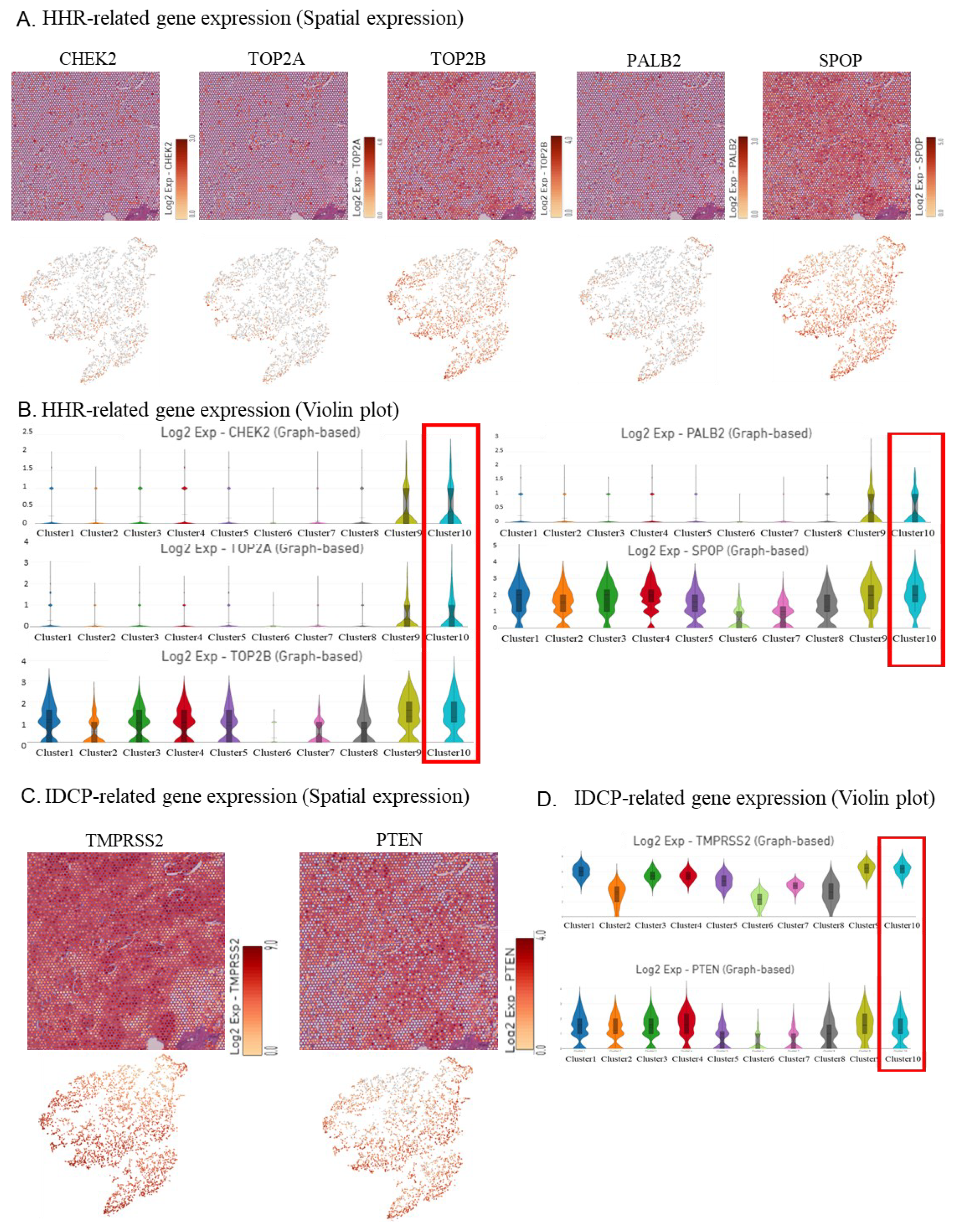
Figure 4.
Visualization of the expression of fibroblast, immune cell, endothelial cell, and hypoxia markers. (A, B) Spatial gene expression analysis (A) and the violin plot (B) showing fibroblast marker gene expression. (C, D) Spatial gene expression analysis (C) and the violin plot (D) showing immune cell marker gene expression. (E, F) Spatial gene expression analysis (E) and the violin plot (F) showing endothelial cell marker gene expression. (G, H) Spatial gene expression analysis (G) and the violin plot (H) showing hypoxia marker gene expression.
Figure 4.
Visualization of the expression of fibroblast, immune cell, endothelial cell, and hypoxia markers. (A, B) Spatial gene expression analysis (A) and the violin plot (B) showing fibroblast marker gene expression. (C, D) Spatial gene expression analysis (C) and the violin plot (D) showing immune cell marker gene expression. (E, F) Spatial gene expression analysis (E) and the violin plot (F) showing endothelial cell marker gene expression. (G, H) Spatial gene expression analysis (G) and the violin plot (H) showing hypoxia marker gene expression.
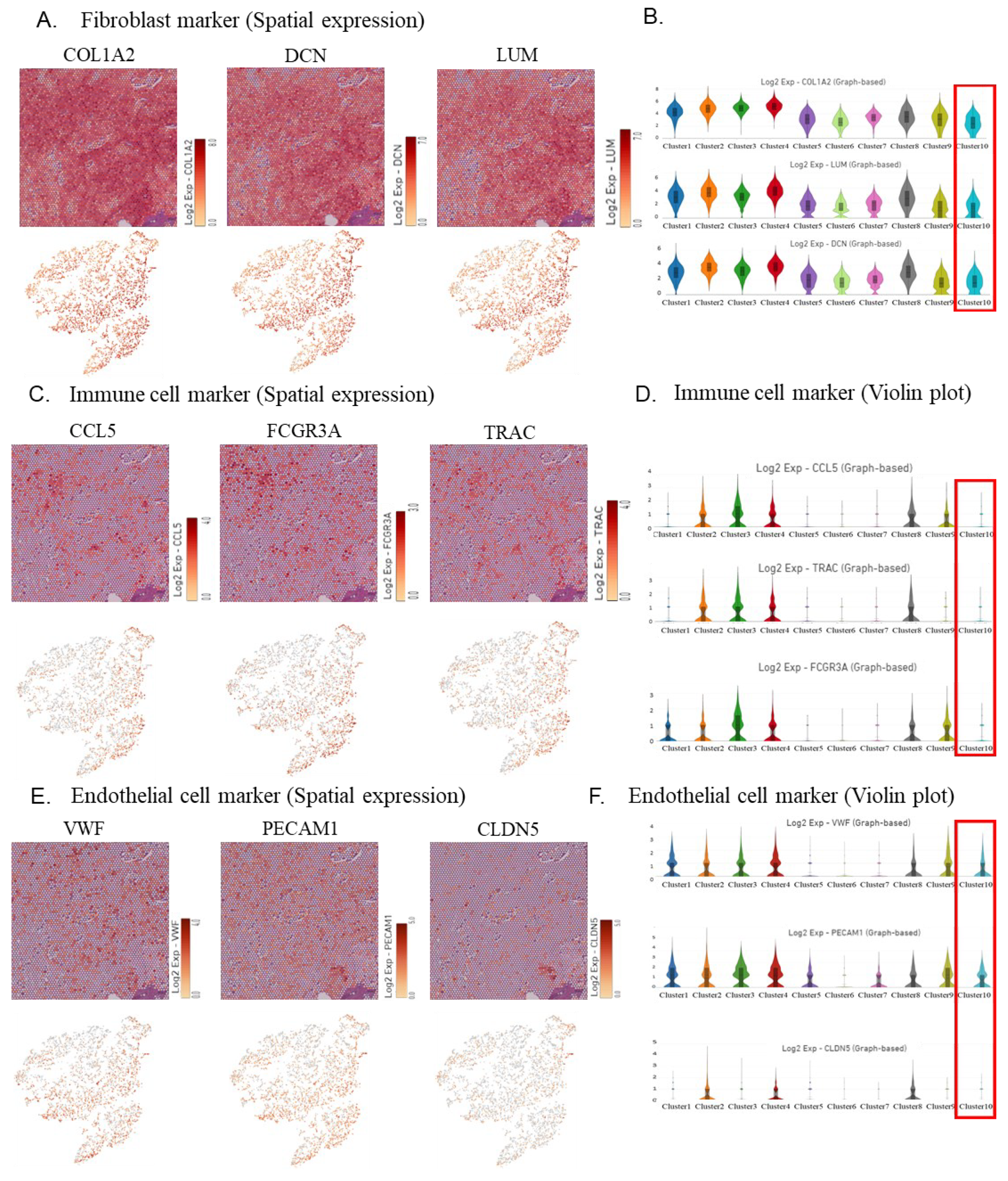
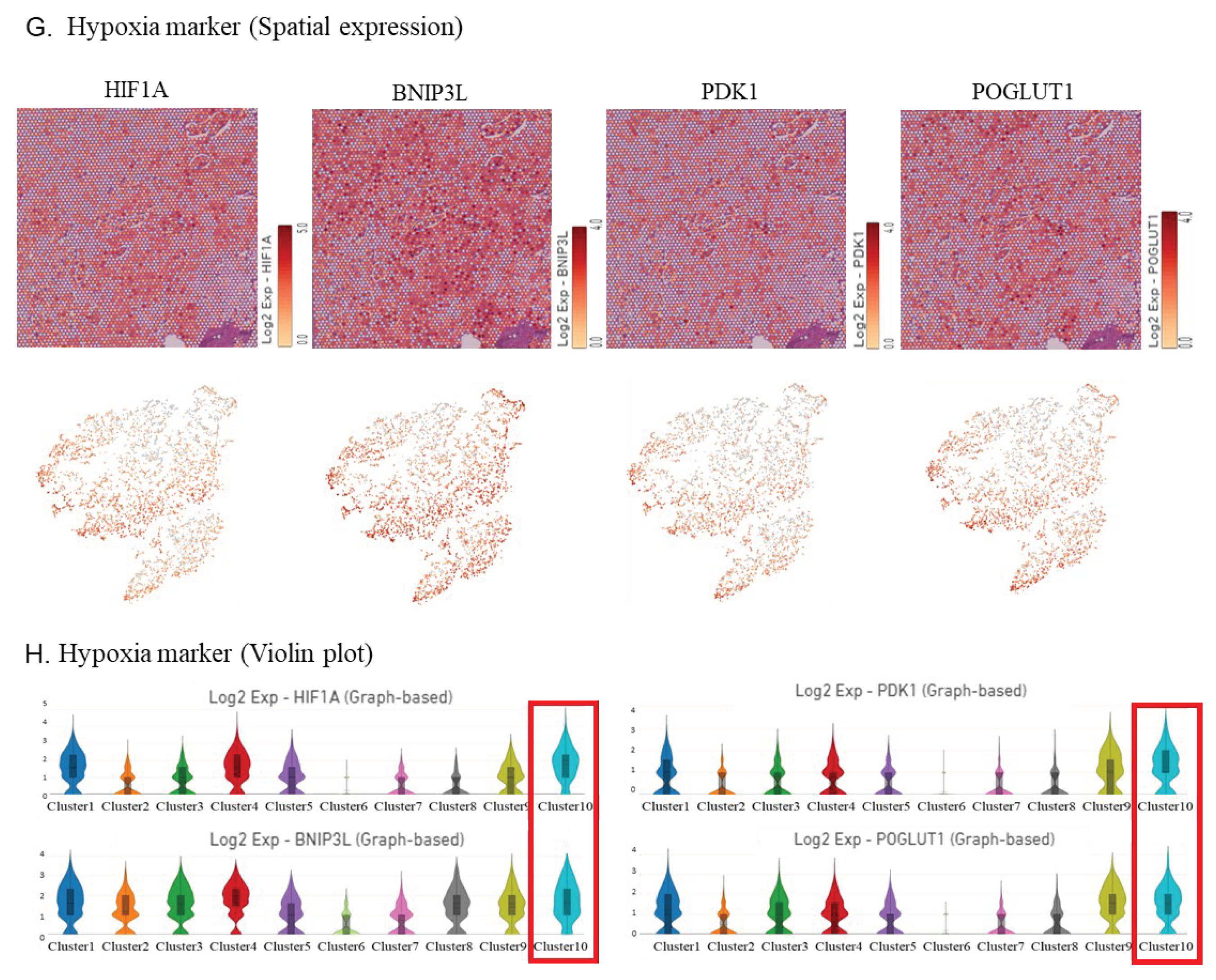
Figure 5.
Graphical Summary. Intraductal carcinoma of the prostate may promote malignant transformation and increase resistance to therapy by causing hypoxia and immune cell inaccessibility owing to its morphological features.
Figure 5.
Graphical Summary. Intraductal carcinoma of the prostate may promote malignant transformation and increase resistance to therapy by causing hypoxia and immune cell inaccessibility owing to its morphological features.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



