Submitted:
15 March 2024
Posted:
18 March 2024
Read the latest preprint version here
Abstract
In patients with heart failure, the evaluation of left ventricular (LV) diastolic function is vital, offering crucial insights into hemodynamic impact and prognostic accuracy. Echocardiography stands as the primary imaging modality for diastolic function assessment, and using it effectively requires a profound understanding of the underlying pathology. This review covers four main topics: first, the fundamental driving forces behind each phase of normal diastolic dynamics, along with the physiological basis of two widely used echocardiographic assessment parameters, E/e' and mitral annulus early diastolic velocity (e'); second, the intricate functional relationship between the left atrium and LV in patients with varying degrees of LV diastolic dysfunction (LVDD); third, the role of stress echocardiography in diagnosing LVDD and the significance of parameter changes in this context; and fourth, the clinical utility of evaluating diastolic function from echocardiography images across diverse cardiovascular care areas.
Keywords:
diastolic dynamics
; echocardiography evaluation
; diastolic dysfunction
; stress echocardiography
; strain imaging
; integrating artificial intelligence
1. Introduction
In patients with heart failure (HF), evaluating left ventricular (LV) diastolic function is crucial; this evaluation is essential to gaining a deeper understanding of the hemodynamic implications of HF and enhancing prognostic accuracy in HF management [1,2]. Echocardiography is typically the primary imaging modality for assessing diastolic function and often can provide all of the data the assessment requires [3]. To accurately evaluate LV diastolic function, it is imperative to comprehend the underlying pathology revealed by 2D and color Doppler imaging and stress echocardiography (SE) testing. This understanding is the cornerstone of effective echocardiographic evaluation of diastolic function. The echocardiographer must also have a firm grasp of the physiological rationale for measuring each parameter, including awareness of situations that can affect the reliability of these variables and proficiency in the technical aspects of acquiring and analyzing 2D and color Doppler imaging and SE data.
2. Normal LV Filling Dynamics
During LV ejection, energy is stored as myocytes undergo compression, while the myocardial wall's elastic components are also compressed and twisted [4]. Subsequently, at the end of systole, calcium ions are actively reabsorbed into the sarcoplasmic reticulum (SR) (Figure 1). This process facilitates the detachment and repositioning of actin and myosin filament cross-bridges to their original configuration, thereby enabling muscle relaxation, a process known as uncoupling. This phase, consuming adenosine triphosphate (ATP), is known as "active relaxation," a process that does not occur instantaneously. Concurrently, during LV diastole, restoring forces come into play, further facilitating this relaxation phase. When contracted myocardium relaxes and untwists, this stored energy is released as the elastic elements recoil [5], serving as the driving force in the early diastolic phase to aid myocardial fibers in extending from their minimum length (Lmin) during the contraction phase to their original length (L0). The elastic recoil of the base and apex from their previous systolic positions, resulting in the release of the contracted LV myocardium along the longitudinal axis, has been referred to in the literature by various names, including LV untwisting motion [6], restoring force [7], and elastic recoil [8]. Elastic recoil is passive relaxation, during which the myocardium spontaneously relaxes without energy consumption.
These two forces result in a rapid decrease in LV pressure (LVP) during isovolumetric relaxation [9]. During this phase, both the aortic valve and the mitral valve remain closed, and LVP rapidly declines until it equals the left atrial pressure (ie, LVP=LAP) (Figure 2). But increasing the length of myocytes and the hermetically sealed ventricular chamber jointly generate potential energy for sucking the blood from the left atrium (LA) to the LV apex.
As more calcium ions are taken up by SR, an increased level of uncoupling occurs, resulting in a greater number of actin and myosin filaments returning to their initial positions. This facilitates muscle relaxation, allowing the cardiac muscle fibers to elongate and assume a longer state. This process contributes to the reduction of LVP, which further causes LVP to drop below LAP (LVP < LAP) (Figure 2). This atrioventricular pressure gradient, which pulls blood toward the LV apex, can be considered a measure of LV suction and plays a crucial role in early LV filling. The pressure gradient for early LV filling (early rapid filling), represented by the E wave, depends on the difference in pressure between LA and the LV apex, expressed as ΔP = LAP − LVP. This gradient is influenced by changes in the rate of LV relaxation and filling pressure.
LV untwisting rate (derived from LV short-axis views) and e’ (the peak early diastolic mitral annular velocity) are used to evaluate LV early diastolic recoil capacity [6,10]. Additionally, e', LV longitudinal strain rate during isovolumic relaxation (SRIVR), and LV strain rate during early diastole (SRE) are significantly associated with LV active relaxation [11] (Figure 3). Advancements in LV diastolic function assessment by strain and strain rate derived from 2D-speckle-tracking echocardiography (STE) are discussed in Section 5.1.
With LV rapid filling, the pressure gradient between the LA and the LV apex decreases and briefly reverses (inflow deceleration). This reversed pressure gradient at the mitral valve decelerates and subsequently halts the rapid blood flow into the LV during early diastole (Figure 2). The duration of inflow deceleration (deceleration time [DT]) and A wave (late diastolic filling flow, as well as atrial contraction) velocity transit time primarily influenced by the LV chamber's functional stiffness, serving as a noninvasive indicator of LV diastolic operational stiffness. During the mid-diastolic phase (ie, diastasis), LAP and LVP equalize, and mitral flow nearly ceases. In late diastole, atrial contraction generates a second LA-to-LV pressure gradient, propelling blood into the LV. Then, as the LA relaxes, the LAP falls below the LVP, initiating mitral valve closure. In short, LV diastolic function is characterized by early diastolic recoil, LV relaxation, and chamber stiffness—all of which, in turn, determine LV filling pressure (Table 1).
As the preceding discussion shows, the contraction and relaxation functions of the heart are mutually dependent. A stronger systolic contraction results in more significant recoil, thereby increasing potential energy during diastole. Additionally, when more calcium is actively taken up and stored in SR by sarcoendoplasmic reticulum calcium (SERCA), it results in a greater release of calcium by the SR through ryanodine receptors (RyR, calcium-induced calcium release channels) during the subsequent systolic phase of the cardiac cycle (Figure 1), ultimately leading to enhanced myocardial contractility [12,13]. In cases of heart failure with preserved ejection fraction (HFpEF), although LV ejection fraction (LVEF) is in the normal range, the LV's systolic performance is not quite normal [14], as indicated by a reduced LV twist during exercise [15]. The contraction and relaxation functions of the heart are tightly coupled, yet they are also influenced by independent factors. However, impaired LV relaxation is one of the initial signs of myocardial dysfunction.
2.1. Interpreting e’ and E/c’ in Diastolic Dynamics
The apex of the LV moves little throughout the cardiac cycle; therefore, septal or lateral mitral annular motion is a good surrogate measure of longitudinal LV contraction and relaxation [16]. e' coincides with the mitral E wave, signifying the symmetrical expansion of the LV during early diastole as blood swiftly moves toward the LV apex due to a gradual pressure gradient from the LA. e′, referring to the early diastolic peak velocity of the mitral valve annulus, is highly feasible and reproducible and has a strong and consistent association with cardiovascular outcomes. These characteristics are influenced by three independent factors: restoring forces, LV relaxation, and lengthening load.
Restoring forces are responsible for passive elastic recoil, which occurs during LV relaxation and causes the ventricle to return to its resting position. These forces result from systolic contraction and, in the normal LV, generate a negative early diastolic pressure gradient that suctions blood into the ventricle. The restoring forces characterize the mechanical and elastic properties of the myocardium.
LV relaxation pertains to the rate at which active fiber force decays. It describes the active process of how quickly cardiac muscle cells return to their relaxed state after contracting during systole. LV relaxation reflects the heart's ability to actively relax in preparation for the next contraction cycle and, therefore, the heart's intrinsic ability to facilitate diastole.
Lengthening load refers to the pressure in the LA at mitral valve opening, which pushes blood into the LV and thus lengthens it. When the mitral valve is open, the values of lengthening load and filling pressure tend to be closely aligned.
Restoring forces and LV relaxation correspond to the passive relaxation observed during isovolumetric relaxation and the active relaxation seen during the rapid early diastolic filling phase mentioned earlier.
E wave is directly proportional to the ratio between filling pressure and the relaxation time constant (Tau, τ), while e' is inversely proportional to tau only [17]. This relationship establishes a direct proportionality between the E/e' ratio and filling pressure [18]. As a result, E/e' has consistently been strongly correlated with pulmonary capillary wedge pressure (PCWP) across a diverse patient population in research conducted by multiple laboratories. Consequently, E/e' is generally regarded as one of the most practical and reproducible estimates of filling pressure. One important tip is to sample at least two sites at the precise locations specified in the guidelines (between the tips of the mitral leaflets for E, and at the lateral and septal basal regions of the mitral annulus for e') and at adequate sample volume sizes. Furthermore, although the correlation between E/e' and LAP is most pronounced in cases of impaired LV systolic function, it remains accurate even in patients with preserved systolic function and variations in loading, such as those associated with aortic stenosis and exercise.
3. Abnormal LV Filling Patterns
LV diastolic dysfunction (LVDD), defined as impaired relaxation and potentially accompanied by reduced restoring forces, early diastolic suction [19], and increased chamber stiffness [20,21], leads to symptomatic HF by causing elevated filling pressures at rest or with exertion [22]. LVP and LAP interact significantly in patients with LVDD. Elevated LVP is a hallmark of LVDD. Concurrent with this elevation, inadequate LV filling leads to an accumulation of blood in the LA, thus increasing LAP. This rise in LAP directly stems from the LV's inability to relax adequately during diastole, causing disruptions in cardiac function and hemodynamics. Consequently, the dynamic relationship between LVP and LAP plays a pivotal role in assessing and understanding the severity of LVDD, reflecting the heart's filling status and the LA's burden. This comprehensive assessment is indispensable for the diagnosis, treatment, and evaluation of cardiovascular conditions, as well as patients’ overall cardiac function.
In the early stages of LVDD, particularly in mild cases with no significant alterations in LAP [23], two noteworthy changes occur in the LV myocardium: a subtle reduction in relaxation, and a slight decrease in compliance. As in the previous discussion, the term "relaxation" primarily refers to the myocardium's active relaxation process, whereas "compliance" pertains to the myocardium's passive recoil (Table 1). The small reduction in relaxation leads to a minor decrease in mitral annular velocity (e'). Simultaneously, delayed relaxation prolongs the E-wave DT and may be accompanied by a mid-diastolic peak in mitral flow (L wave) [19]. Conversely, the decrease in compliance results in a minor increase in early LV filling pressure, subsequently causing a reduction in the E wave. The significance of atrial contraction as a compensatory mechanism heightens, culminating in an E/A ratio <1. This filling pattern is termed an "impaired relaxation pattern" or "grade 1 LVDD" (Figure 4). In most patients with this impaired relaxation pattern, the mean LAP remains within the normal range despite an elevated LV end-diastolic pressure (LVEDP) maintained by robust atrial contraction.
In the subsequent stage of LVDD, a pseudonormal mitral inflow pattern becomes evident (Figure 4). As LVDD continues to worsen, accompanied by an increase in LAP, the early diastolic LA-to-LV pressure gradient is reestablished despite elevated diastolic LVP. This reestablishment may return the E wave to the normal range. Additionally, during this phase, the E wave may increase slightly because the rise in LAP is relatively greater than the increase in LVP. The significantly slower relaxation rate that characterizes LVDD delays the e' wave so that it occurs after the E wave, which indicates that the LV does not expand symmetrically during diastole. The propagation of filling to the apex and longitudinal expansion occurs slowly after the LV is filled by the movement of blood from the LA into the LV inflow tract. In the presence of slow relaxation, the e’ wave does not coincide with the LA-to-LV pressure gradient, leading to a reduction in e' velocity, which becomes largely independent of LAP. Therefore, during this stage, a reduced and delayed e' wave may be observed [24,25].
In patients with more severe LVDD, characterized by significantly slowed relaxation and elevated LAP, several significant changes become evident, often indicative of a restricted filling pattern or grade 3 LVDD (Figure 4). The E wave, reflecting the pressure gradient during diastasis, increases further, underscoring the extent of diastolic impairment. This heightened E wave is a consequence of the impaired LV relaxation and the sustained elevation of LAP. Simultaneously, LAP continues to rise during early diastole, surpassing the increase in LVP, leading to the enduring expansion of the pressure gradient between the LA and LV. These changes can be ascribed to the constraints on LV filling, with some blood potentially stagnating in the LA, impeding smooth flow through the mitral valve into the LV. This culminates in the accumulation of blood within the LA, augmenting both its volume and pressure. Over time, the prolonged LVDD may result in LA enlargement, indicating an increased capacity to accommodate blood, but it also brings about higher LAPs. With severe LVDD, the E-wave DT becomes notably short, and the e' wave is further reduced and delayed, collectively contributing to a marked elevation of the E/e' ratio. The peak late diastolic mitral annular velocity (a') may decrease, while the pulmonary venous systolic forward flow velocity is reduced and is lower than the diastolic forward flow velocity.
The presence of pseudonormalized (grade 2) and restricted (grade 3) filling patterns with elevated E/e' indicates the coexistence of LVDD and elevated LAP, resulting in blood being pushed out of the LA rather than being suctioned into the LV [4,26,27]. As mentioned earlier, the E wave is enhanced when there is an elevated LA-to-LV pressure gradient. Conversely, the e' wave is reduced and delayed in cases of slow relaxation, potentially indicating impaired LV filling. Therefore, a high E wave and a low e' wave (resulting in an increased E/e' ratio) suggest that the increased E wave is primarily due to elevated LAP, rather than a decrease in LV diastolic pressure. The initial pathological changes in LV not only disrupt its own function but also extend their detrimental effects to the LA, setting the stage for a rapid escalation in LAP that soon exceeds the LA's adaptive capacity. The underlying mechanism for this phenomenon can be described as follows: Firstly, the LA, which typically has a thinner wall and smaller volume than the LV, is more susceptible to pressure fluctuations. As LVDD progresses beyond the LA's tolerance, the LA walls rapidly undergo dilation, decreased compliance, and remodeling, which are secondary to increased LV filling pressure. Ultimately, all these changes result in an increase in LAP. These factors collectively accelerate the deterioration rate of the LA, surpassing that of the LV. Secondly, during diastole, the LA acts as a reservoir for oxygenated blood returning from the pulmonary veins. Impaired LV relaxation and filling can lead to accumulation of blood in the LA. This filling constraint and blood buildup consequently trigger a rapid increase in LAP, as the LA must accommodate the augmented blood volume. In this scenario, the LA is caught between elevated pressures from both the upstream pulmonary artery (PA) and the downstream LV, exacerbating its deterioration. LA remodeling and dysfunction secondary to increased LV filling pressures are associated with worse symptoms, more pulmonary vascular disease, greater right ventricular dysfunction, depressed exercise capacity, and adverse outcomes [28,29]. Hence, some researchers propose that reduced LA strain (LAS) [30,31] and increased LA stiffness (E/e′/LAS) [32] are the most accurate diagnostic criteria for diastolic HF.
3.1. Echocardiography Parameters and Evaluation Algorithms for Diastolic Dysfunction
The American Society of Echocardiography (ASE) guideline [19] introduces two distinct algorithms for assessing diastolic function. Algorithm A is aimed at patients with unknown diastolic function, and its primary purpose is to distinguish between normal and abnormal diastolic function (Figure 5). Algorithm B, conversely, is specifically designed for patients with known or suspected LVDD and focuses on estimating LV filling pressure and grading diastolic function. These two algorithms serve as valuable tools in the echocardiographic assessment of diastolic function across a spectrum of clinical scenarios, providing clinicians with the means to make informed diagnoses and treatment decisions. For algorithm A, abnormal diastolic function is defined as having ≥3 abnormal parameters, which comprise the following: annular e' velocity with septal e' <7 cm/s, lateral e' <10 cm/s, average E/e' ratio >14, LA volume index (LAVI) >34 mL/m2, and peak tricuspid regurgitation (TR) Vmax >2.8 m/s. It is recognized that at times only the lateral e′ or septal e′ velocity is available and clinically valid, and in these circumstances a lateral E/e′ ratio >13 or a septal E/e′ >15 is considered abnormal. Algorithm B is detailed in Figure 6.
LA volume is a crucial parameter for evaluating diastolic function and LV filling pressure [23], as it directly reflects LA dilation and remodeling. Nonetheless, measuring LA volume alone is insufficient for identifying LA dysfunction. LA deformation analysis, particularly LA reservoir strain, appears to be robust for detecting LA dysfunction [33,34].
PA systolic pressure (PASP) and mean wedge pressure are correlated. In patients without pulmonary disease, an increase in PASP is indicative of elevated LAP [3]. PASP is indirectly calculated using the Bernoulli principle from tricuspid regurgitation in systolic jet velocity (TR Vmax) [19,27]. A TR Vmax exceeding 2.8 m/s, corresponding to an estimated PASP of 32 mmHg, is associated with elevated LAP [19,35].
Differentiation between normal and abnormal diastolic function is complicated by overlap between Doppler indices in healthy individuals and those with LVDD [19]. Individual parameters, including those discussed above, are no more than moderately associated with filling pressures and are notably insufficient when used independently, and this includes E/e' [36]. Therefore, using an integrated approach with multiple parameters to evaluate diastolic function is necessary [19]. If two of the three variables meet the cutoff values, this indicates an elevated LAP and grade II LVDD. If only one of the three available variables (Figure 6, third row, center box) meets the cutoff value, LAP is considered normal, indicating grade I LVDD. If there is a 50% discordance between two or four available variables, findings are considered inconclusive for estimating LAP. Estimating LAP is not recommended if only one parameter provides a satisfactory signal.
The ESC guidelines for the diagnosis and treatment of HF evolved between their 2016 and 2021 iterations. The 2021 guidelines [37] recommend specific criteria for the diagnosis of LVDD or elevated LV filling pressures. These criteria are an increased LV mass index (≥95 g/m2 for women, ≥115 g/m2 for men), an enlarged LA (LAVI >34 mL/m²), an E/e' ratio at rest >9, a relative wall thickness >0.42, PA systolic pressure >35 mmHg, and TR velocity at rest >2.8 m/s. The LA size and E/e’ criteria, plus mitral E velocity >0.9 m/s and septal e' velocity <9 cm/s, are critical thresholds, with values beyond these increasing the risk of cardiovascular mortality. [1].
4. Stress Echocardiography Testing for Normal and Abnormal Diastolic Function
As discussed above, patients with LVDD may have a similar hemodynamic profile (in terms of cardiac output and filling pressure) at rest as healthy individuals who have normal diastolic function. The diastolic stress test refers to the use of exercise Doppler echocardiography (ie, SE) to detect impaired LV diastolic functional reserve and the resulting increase in LV filling pressures [38,39,40,41]. It is a noninvasive hemodynamic test used to assess patients with unexplained dyspnea. It also can improve the diagnosis of HFpEF or diastolic heart failure. Frequently, symptoms of LVDD occur only during exercise, because LV filling pressure is normal at rest but increases with exercise [39], as stress-induced LVDD [42]. The 2022 ACC HF guidelines state that exercise SE evaluation of diastolic parameters can be helpful if the diagnosis remains uncertain after standard clinical assessment and resting diagnostic tests have been performed [43].
4.1. Stress Echocardiography during Relaxation in Healthy Individuals
Normal diastolic function enables the LV to adapt effectively to increased cardiac output during periods of stress or exertion. This adaptability is due to enhanced myocardial relaxation and more powerful early diastolic suction, neither of which significantly raises filling pressures. The E wave, representing early passive filling and relaxation rate, may increase slightly during stress due to elevated heart rate and increased cardiac output. Simultaneously, e', reflecting the longitudinal rate of myocardial relaxation, increases proportionally during exercise. The faster the myocardial relaxation is, the higher the patient’s stress/exercise capacity. Consequently, the E/e' ratio, which serves as an indicator of LV filling pressure, typically remains within the normal range [44,45,46] because both mitral inflow and annular velocities increase in proportion [47].
During exercise, the limited time available for diastolic LV filling due to tachycardia necessitates an acceleration in myocardial relaxation and an enhancement of LV suction to maintain or increase stroke volume while preserving normal filling pressure.
Distinct levels of e' elevation during exercise, indicative of longitudinal functional reserve, can serve as a parameter for evaluating LV diastolic reserve during exertion [48]. Some studies test diastolic functional reserve to diagnose stress-induced LVDD, which is calculated as the product of Δe′ (the change of e’ from baseline to exercise) and baseline e′ (an early diastolic mitral annular velocity at rest) [49]. Research has associated both exercise E/e' and diastolic reserve with exercise capacity [42], particularly in patients with HFpEF [48,50]. The E/e′ ratio can also be utilized as a surrogate marker to estimate LAP or PCWP during both exercise and rest [51] (Table 2).
In healthy individuals under stress, cardiac output rises efficiently without a substantial increase in LVEDP, owing to enhanced myocardial relaxation. In contrast, patients with LVDD attain the necessary cardiac output only through an increase in LVEDP because these patients lack a sufficient early suction mechanism for normal LV filling during early diastole. E wave: mitral peak velocity of early filling; e’ wave: mitral annular velocity of early filling by tissue Doppler.
4.2. Stress Echocardiography in Patients with Left Ventricular Diastolic Dysfunction
In patients with LVDD, a different pattern emerges. The E wave increases significantly to augment stroke volume, highlighting the challenges posed by impaired relaxation and elevated filling pressures. Conversely, e' does not change as substantially as the E velocity in patients with abnormal myocardial relaxation [52], which is also reflected in a reduction in diastolic functional reserve. This difference may be attributed to a pathological decline in the intrinsic relaxation capacity of the myocardium, affecting both active and passive relaxation. Consequently, even when stress increases the body’s demand for cardiac output, the heart of a patient with LVDD may not be able to augment myocardial relaxation to the necessary degree. This deficiency necessitates a higher filling pressure to maintain adequate blood filling and stroke volume. When E is elevated while e' either increases slightly or remains relatively unchanged, the E/e' ratio increases significantly (Table 2). This observation aligns with the previously mentioned greater increase in LVP during stress conditions.
In summary, SE testing offers valuable insights into diastolic function and filling pressures, distinctly differentiating the parameter behaviors of individuals with normal diastolic function from those with LVDD. This differentiation assists clinicians in evaluating cardiac performance under various conditions and in identifying LVDD when it is present. According to published studies, an E/e' >15 (using septal e' velocity) can be used as a diagnostic criterion for stress-induced relaxation dysfunction [39].
5. Other Advanced Echocardiography Techniques for Evaluating LV Diastolic Function
5.1. Strain Imaging
Strain, a measure of deformation, is a critical parameter in clinical cardiology. It is typically quantified as a percentage or fraction, notably in longitudinal strain analyses (Figure 3). Recent advancements in the field have been marked by the adoption of STE for assessing diastolic function intraoperatively. This novel technique, validated by numerous studies [53,54,55], offers a significant advantage by enabling comprehensive evaluation across the entire LV [56], unlike regional assessment methods. Another significant advantage of STE is its lack of angle dependency, a limitation commonly associated with tissue Doppler imaging. STE achieves this by acquiring images at a frame rate of 50-80 per second [57], allowing more accurate and comprehensive cardiac imaging. Further reinforcing the utility of STE, numerous studies have demonstrated that both LV and LA strain, along with strain rate, are reliable predictors of LV diastolic function [31,54,58,59]. These findings underscore the potential of STE as a transformative tool in the evaluation and management of cardiac function, particularly diastolic performance.
5.1.1. LV Strain and Strain Rate
The evaluation of LV strain rate has become a cornerstone in the analysis of LVDD, particularly in patients with HFpEF. A growing body of literature consistently reports compromised LV longitudinal strain in patients with LVDD, thereby establishing its clinical significance [60]. A critical area of investigation has been exploring the relationship between LV diastolic strain and strain rate. Obtaining these measures requires both regional [61] and global assessments, which have been correlated with the time constant of LV relaxation [11], as previously discussed. Of note is the emergence of 2D STE-based strain rate imaging as a valuable technique in identifying early-stage LVDD [62]. While this technique proficiently detects increased LV stiffness, it has yet to surpass the performance of established tissue Doppler imaging analyses such as the E/e′ ratio, particularly in mild cases of LVDD [63].
An interesting development in this domain is the ratio of E to longitudinal strain (E/LS). This metric has demonstrated superior performance over traditional markers like E/A and E/e′ in differentiating elevated LV relaxation and filling pressures. Its efficacy is highlighted by a sensitivity of 72% and specificity of 88%, achieved by using an optimal cutoff value of 680 cm/s [64]. Experimental studies that have focused specifically on LV strain rate [54,55,58] have shown that both longitudinal and radial strain rates with dobutamine can serve as indicators of the cellular/collagen mix within specific myocardial segments because of their strong correlation with interstitial fibrosis. Global SRIVR as measured by 2D STE is closely linked to LV relaxation. The E/SRIVR ratio has shown reasonable accuracy in predicting LV filling pressures [11]. A noteworthy retrospective clinical study involving sixty-six patients showed that the diastolic peak longitudinal strain rate (SRa) was significantly correlated with stage of LVDD. An SRa <0.68 s⁻¹ was found to have a sensitivity of 80% and specificity of 81% in identifying grade 2 or 3 LVDD [54], which is typically associated with elevated LV filling pressure/LVEDP [19].
5.1.2. LAS
Building on the earlier discussion of the dynamic processes involved in physiological and pathological diastolic function, it is evident that LA anatomy and mechanics are crucial for preserving LV diastolic function and preventing symptoms. As a result, an increasing number of researchers are focusing on LAS (Figure 3), which has evolved into a valuable parameter for assessing LV diastolic function and estimating LV filling pressures. LAS is a measure that evaluates the deformation or stretching of the LA during different phases of the cardiac cycle. The basic parameters of LAS include reservoir function (LASr), conduit function (LAScd), and contractile function (LASct). LASr indicates the LA's capacity to accommodate blood during ventricular systole, LAScd evaluates the passive emptying of blood from the LA to the left ventricle in early diastole, and LASct measures the active contraction of the LA to aid in ventricular filling during late diastole (Figure 3). LA function assessment provides prognostic information beyond atrial dilatation, and the development of techniques for measuring LAS has substantially enhanced the practicality of assessing LA function [65]. LA stiffness (E/e′/LAS) and strain are novel indices of LV diastolic function. LAS is gaining recognition as a key indicator of LA dysfunction [66] and as an early marker of LVDD when conventional echocardiographic parameters are within normal range [67].
LA longitudinal strain is angle-independent, thus overcoming Doppler limitations, and provides reproducible measures of LA deformation [68]. In a study by Singh et al. [69], LASr was significantly different between grades of LVDD severity, with gradual decreases seen with worsening LVDD. LASr was measured in all patients, achieving diagnostic accuracy as high as 95%. With a threshold of 26.7%, LASr predicted LVEDP >16 mmHg with a sensitivity of 90% and a specificity of 82.9%. This resulted in a superior diagnostic accuracy to that of LASct, LAScd, and even E/e' [70]. In patients with LVDD and elevated LV filling pressures, abnormal LAS is more common than abnormal left atrial volume index (LAVI) (62.4% vs. 33.6%) [30]. LA volume has been used as a surrogate for the chronicity and severity of LVDD. However, volume is an insensitive biomarker of the early phases of LVDD [71]. Morris and colleagues found that adding LAS to LAVI boosted LVDD detection by 73.3% over what was possible with LAVI alone, from 13.5% to 23.4% [30]. Additionally, LAS (<23%) independently correlates with worse functional class and predicts a higher risk of HF hospitalization at 2 years, even when adjusted for age, sex, and normal LAVI. In patients with normal LVEF, Nagueh and Khan found that LASr <18% had high specificity for increased filling pressures [72]; however, these authors argued that LASr should be considered in diagnosing LVDD but not as a stand-alone index [72]. Similarly, another study showed that LASct, when used with a cutoff of 16%, more accurately predicts PCWP >18 mmHg than E/e’ ratio in patients in sinus rhythm and with myocardial and valvular disease [73].
5.2. Integrating Artificial Intelligence (AI)
Although the most recent guidelines aimed to simplify the assessment of diastolic function, this evaluation remains intricate, relying on the integration of numerous clinical and echocardiographic variables [74]. Guideline-based algorithms require doctors to measure multiple metrics in multiple echocardiographic views, which requires substantial time and skill, so the quality of clinical reporting of diastolic function is difficult to guarantee [75].
In response to the intricacies involved in assessing diastolic function, there has been a burgeoning interest in leveraging artificial intelligence (AI) to automate this process. Novel approaches based on AI have demonstrated significant potential in recent studies. Choi et al. [76] explored the diagnostic accuracy of a machine learning (ML) model in HFpEF, achieving an impressive 99.6% concordance with human specialists in diagnosing diastolic HF. The ML algorithm, incorporating LVEF, LAVI, and TR velocity, notably surpassed the conventional six-parameter assessment of diastolic dynamics. Omar et al. [77] employed speckle tracking echocardiographic measurements to develop an AI model to predict increased LV filling pressure, a critical LVDD parameter. Validation against invasively measured increases in PCWP showed the model's robustness, with an area under the curve of 0.88, showcasing the potential for automated diastolic function assessment.
Efforts have also been made to enhance LVDD phenotyping for better outcome prediction. Pandey et al. employed ML to design a model that can identify patients with elevated LV filling pressure more accurately than the American Society of Echocardiography's 2016 diastolic guidelines grading system [78]. Additionally, Chiou et al. [79] developed a prescreening tool for diastolic HF that analyzes intra-beat dynamic changes in the LV and LA. By analyzing linear signals of LV and LA length, area, and volume waveforms, they identified novel intra-beat dynamic patterns that evaluated diastolic function with high accuracy, sensitivity, and specificity.
In the latest investigation, Chen et al. [80] introduced three AI-assisted methods for diastolic function assessment, achieving better diagnostic accuracy than human experts following guidelines. The models showed favorable results in evaluating and grading LV diastolic function. Notably, when Doppler variables were unavailable, the AI models could interpret 2D strain metrics or videos from a single view, suggesting significant potential for labor and cost savings, as well as workflow streamlining in clinical LV diastolic function assessment.
6. Clinical Implications
Evaluating LVDD through echocardiography is crucial in cardiovascular care [81]. The function of LV goes beyond explaining symptoms, serving as a key predictor of outcomes in cardiovascular patients [82]. Echocardiography not only detects issues early but also enables precise diagnoses, helping healthcare providers address cardiac abnormalities at their early stages, and preventing HF and complications. Additionally, it provides valuable insights into prognosis, enhancing understanding of potential risks and informing long-term treatment planning [83]. Consistent echocardiographic follow-up is essential for monitoring disease progression and ensuring treatment effectiveness over time. Besides its diagnostic and therapeutic roles, echocardiography educates patients by visually documenting their condition, thus enhancing their comprehension and encouraging adherence to prescribed treatments and lifestyle changes. In summary, using echocardiography for LVDD assessment ensures a proactive approach to managing cardiovascular health.
6.1. Heart Failure with Preserved Ejection Fraction
Approximately 50% of HF cases are classified as HFpEF [84], which is associated with greater morbidity and mortality rates than patients without HF have [43]. HFpEF is associated with LVDD and, frequently, some level of LV longitudinal systolic dysfunction [85]. HFpEF can be hemodynamically defined as a clinical syndrome characterized by the heart's inability to effectively pump blood without the need for elevated cardiac filling pressures [86]. According to the 2022 ESC guidelines, the diagnosis of HFpEF should encompass symptoms and signs of heart failure, LVEF >50%, and objective evidence of cardiac structural or functional abnormalities indicative of LVDD or elevated LV filling pressures (discussed above), including elevated natriuretic peptide (NP) levels. Consequently, establishing the diagnosis requires objective evidence of elevated filling pressures, chiefly by echocardiography [37]. The proposed reference diagnostic standard relies on symptoms such as dyspnea, elevated NP levels, and an LVEF >50%. However, these criteria lack specificity, necessitating a confirmatory test. Invasive right heart catheterization is considered the diagnostic gold standard [87]. Echocardiography can distinguish between HFpEF and heart failure with reduced LVEF (HFrEF) in patients with unexplained dyspnea and without any significant valvular disease [88]; this capability adds strategic depth to therapeutic interventions for LVDD, particularly when echocardiography reveals the specific etiological factors involved.
The parameters for assessing diastolic function were shown to predict mortality in three major HFpEF clinical trials [89,90]. Using existing guidelines alone to interpret resting echocardiographic data can only identify 34% to 60% of patients with invasively confirmed HFpEF [91]. A 2020 study [92] found that a multivariable model incorporating echocardiographic, clinical, and arterial function displayed better diagnostic performance than relying on a single variable alone.
SE to diagnose HFpEF: Many patients with HFpEF have normal cardiac filling pressure at rest but develop an abnormal increase during exercise due to multiple cardiovascular reserve limitations [93,94,95], making resting echocardiographic parameters less sensitive for HFpEF diagnosis in these cases [39]. Because of this, recent interest has focused on SE diastolic testing (analyzing the E/e’ ratio and TR velocity during exercise) for the diagnosis of early HFpEF in cases of unexplained dyspnea and for a detailed assessment of exercise physiology for better HFpEF phenotyping. A positive diastolic stress test is characterized by the fulfillment of three conditions during exercise: an average E/e′ >14 or septal E/e′ ratio >15, a peak TR velocity >2.8 m/s, and septal e′ <7 cm/s (or, if only lateral velocity is acquired, lateral e′ <10 cm/s) at baseline [96]. Incorporating exercise/stress echocardiographic data with an E/e' ratio >14 increased sensitivity from 78% to 90% and, consequently, increased the negative predictive value. However, it decreased specificity to 71% [50]. Performing diastolic stress testing alongside standard resting echocardiography improves diagnostic sensitivity, especially in patients suspected of HFpEF with normal estimated LV filling pressure at rest [97]. In patients with global longitudinal strain (GLS) <16-18% and suspected HFpEF, diastolic stress testing should be considered [96]. For patients who require stress testing, the most well-validated protocol is bicycle (in semi-supine position) exercise testing [98].
Other echocardiographic methods to diagnose HFpEF: A study involving 3,342 participants showed that using LV GLS assessment in adults with preserved LVEF, defined by a GLS of −15.9% or less, resulted in an LVDD prevalence of 9.2% at baseline and 9.0% at follow-up [99]. When assessed by invasive methods, LV GLS <16% has a sensitivity of 62% and a specificity of 56% for the diagnosis of HFpEF [95]. Enlarged LA is frequent in patients with HFpEF and is associated with elevated cardiovascular risk and LV filling pressure [100]. A recent study that included more than 300 patients showed that elevated LV filling pressure is reflected in reductions in LASr and LAScd [101].
Additionally, a meta-analysis of four studies suggested a reasonable diagnostic accuracy for LAS, with a specificity of 93% and a sensitivity of 77% [94,102,103,104]. Other studies have shown that LASr has a stronger correlation with invasive LVP than with LAVI [105]. Other studies have shown that LASr can detect LV diastolic alterations and elevated LV filling pressure even when LAVI is normal [30]. The ideal threshold for distinguishing between normal and elevated LV filling pressure was found to be 18% for LASr and 8% for LASct when elevated PCWP was defined as a PCWP >12 mmHg. Similarly, the thresholds were determined to be 16% and 6% when PCWP >15 mmHg was the criterion for elevated LV filling pressure [96]. Moreover, LASr and LA compliance (LAS/E/e′) provide a discriminative capability for distinguishing HFpEF from noncardiac causes of dyspnea, demonstrating comparable or superior accuracy to that of commonly used echocardiographic indices of diastolic function [102]. The most recent guidelines for the multimodal evaluation of HFpEF now incorporate LASr as a component in the echocardiographic assessment of LV filling pressure [96].
6.2. Hypertensive Heart Disease
Among several risk factors, hypertension remains the leading cause of cardiovascular mortality [106]. Even individuals with prehypertension have detectably impaired cardiac relaxation [107]. Several studies emphasize that LVDD precedes systolic dysfunction, particularly in patients with cardiovascular risk factors like hyperlipidemia, diabetes, hypertension, obesity, and smoking habits [108]. Continued elevation of blood pressure levels contributes to LVDD through multiple mechanisms, such as heightened afterload, myocardial ischemia, and the development of myocardial fibrosis [109]. Myocardial fibrosis is the primary factor in altering diastolic properties, impairing myocardial relaxation and thus disrupting normal LV diastolic filling [110]. LVDD is an independent predictor of cardiovascular outcomes in hypertensive populations [111,112].
Resting echocardiography to diagnose hypertension heart: In patients with myocardial disease, even when LVEF is within the normal range, recommendations suggest applying algorithm B, which is used to assess LV filling pressures in patients with reduced LVEF [110]. Individuals with high blood pressure had significantly lower e' and e'/a' values, along with a significantly higher E/e' ratio, than non-hypertensive controls. In a large-scale study with a total of 2,500 patients with uncomplicated essential hypertension, an enlarged LA diameter was observed in more than 20% of the participants [113]; this enlargement, which can cause long-standing elevations in LV filling pressure, and increased LA size and volume were associated with poor long-term mortality and morbidity [114].
SE to diagnose hypertension heart: SE reveals a spectrum of vulnerabilities in hypertensive patients, including LVDD, compromised cardiac and contractile reserve, coronary microcirculation dysfunction, and alterations in cardiac autonomic balance. The specificity of SE is superior to that of electrocardiography and perfusion stress testing yet has similar sensitivity [115]. During peak stress, hypertensive patients have a higher A and a lower E/A ratio than they have in the absence of stress [116]. A diastolic stress test involving exercise [46] proved beneficial for excluding ischemia and establishing a correlation between dyspnea and indicators of elevated filling pressures, such as an elevated E/e′, and the change of a normal LV inflow pattern or a pattern of altered relaxation to a pseudonormalized pattern during exercise [117]. An E/e′ ratio >13–15 is considered abnormal.
Other echocardiographic methods to diagnose hypertension heart: Significantly, LVDD is strongly correlated with LV longitudinal systolic dysfunction, and it might arise even before LV concentric geometry develops [118]. During the systolic phase, longitudinal shortening decreases while radial thickening is preserved, yet circumferential shortening increases to uphold the LVEF. In the diastolic phase, early diastolic strain rate decreases, particularly in the longitudinal direction, even in the absence of significant elevation in LV filling pressure. In this context, strain appears more sensitive than both conventional echo and Doppler tissue imaging in detecting a reduction in intrinsic myocardial contractility among hypertensive patients [108].
In a study involving normotensive controls and three groups of patients with different degrees of hypertension, segmental parameters exhibited apical-basal gradients, with the lowest values in the basal septal segments and the highest in apical segments. Only SRa remained consistent among segments but increased gradually with rising blood pressure [59]. SRE decreased, particularly longitudinally, without a significant rise in LV filling pressure, showing that strain is more sensitive than conventional methods in detecting reduced myocardial contractility in hypertensive patients before LV hypertension [108]. The absolute values of LAS (S-reservoir and S-conduit) and strain rate (Sr-reservoir and Sr-conduit) were notably lower in patients with essential hypertension (EHT) and left ventricular hypertrophy (LVH) [119]. In a 2022 study on hypertensive patients, LAS emerged as a robust predictor for LVDD with increased LAP. Among patients with LVDD, LAS that exceeded the cutoff of 24.27% was far more prevalent in patients with increased LAP (78.9%) than in those without it (15.4%), suggesting that LAS is a valuable, highly sensitive measure for assessment and potential integration into routine practice [120].
7. Future Perspectives
Diastolic function assessment through echocardiography holds immense promise, propelled by rapid advancements in technology and an enhanced understanding of cardiac physiology. AI and ML applications are on the cusp of reshaping the landscape, deploying algorithms to automate intricate measurements and deliver nuanced analyses. Ongoing studies are striving to harness AI's potential to refine diagnostic criteria and elevate risk stratification, signifying a pivotal shift toward precision medicine in the realm of LVDD. Simultaneously, strain imaging provides more comprehensive insight into cardiac dynamics, potentially heightening sensitivity to detect subtle changes. Researchers are actively exploring the seamless integration of these advanced imaging modalities into algorithms for diastolic function assessment, thereby enriching our diagnostic arsenal. In the most recent studies, efforts have been made to integrate STE measures of LAS with ML to enhance the classification of LVDD [121].
In the inadequately explored domain of molecular imaging and biomarkers for LVDD, identifying novel markers could be the key to early detection and personalized management, aspects not covered in this review. Initiatives to unveil the molecular and cellular processes underlying LVDD could pave the way for targeted imaging agents and blood-based assays, equipping clinicians with tools to assess diastolic function at the molecular level. The future envisions a shift toward patient-centric approaches, integrating patient-reported outcomes and preferences into diagnostic strategies for a more personalized approach to care. Collaborative and multidisciplinary research initiatives are gaining momentum, addressing standardization challenges and translating research findings into clinical practice. This collective endeavor is poised to usher in a new era in cardiovascular medicine, where innovative technologies and collaborative endeavors converge to redefine the diagnosis and management of LVDD, ultimately enhancing patient outcomes.
8. Conclusion
Reduced myocardial relaxation is among the earliest indicators of LV mechanical dysfunction. The exploration of diastolic dynamics by echocardiography is crucial for understanding and addressing a spectrum of myocardial conditions, including myocardial ischemia, hypertensive heart disease, hypertrophic cardiomyopathy, and HFpEF. Echocardiography, as the primary imaging modality for assessing LVDD, provides valuable insights into its hemodynamic impact and improves prognostic accuracy. From detecting subtle changes to guiding personalized treatments, this approach encompasses rest echocardiography, SE, and STE, as well as the application of AI and ML. Its multifaceted role significantly contributes to improving patient outcomes. To enhance accuracy in estimating LV filling pressure and grading LV diastolic function, the ASE guideline strongly recommends a comprehensive approach that integrates clinical data with echocardiographic findings [19].
Looking ahead, the future of echocardiography in diastolic function assessment is bright, with AI and ML poised to further refine diagnostic accuracy and enable personalized patient assessments. Research into molecular imaging and biomarkers is expected to unlock new possibilities for early detection and targeted management of LVDD. The integration of patient-reported outcomes and preferences into diagnostic strategies marks a shift toward more personalized care.
In conclusion, echocardiography remains an indispensable tool in the evaluation of diastolic function. The field is evolving rapidly, with technological advancements and collaborative research efforts driving significant improvements in cardiac diagnostics and therapy. This evolution is set to redefine the management of LVDD, ultimately enhancing patient outcomes and advancing the field of cardiovascular medicine.
Author Contributions
Conceptualization, XZ, AE; writing—original draft preparation, XZ; writing—review and editing, KL, CC, AMR, and AE; supervision, AE. All authors have read and agreed on the published version of the manuscript.
Funding
Please add: This research received no external funding.
Acknowledgments
Stephen N. Palmer, PhD, ELS, of the Department of Scientific Publications at The Texas Heart Institute, contributed to the editing of the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Playford, D.; Strange, G.; Celermajer, D.S.; Evans, G.; Scalia, G.M.; Stewart, S.; Prior, D. Diastolic dysfunction and mortality in 436 360 men and women: the National Echo Database Australia (NEDA). Eur. Heart J. Cardiovasc. Imaging 2021, 22, 505–515. [Google Scholar] [CrossRef]
- Ghio, S.; Carluccio, E.; Scardovi, A.B.; Dini, F.L.; Rossi, A.; Falletta, C.; Scelsi, L.; Greco, A.; Temporelli, P.L. Prognostic relevance of Doppler echocardiographic re-assessment in HFrEF patients. Int. J. Cardiol. 2021, 327, 111–116. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Nabi, F.; Chang, S.M.; Al-Mallah, M.; Shah, D.J.; Bhimaraj, A. Imaging for implementation of heart failure guidelines. Eur. Heart J. Cardiovasc. Imaging 2023, 24, 1283–1292. [Google Scholar] [CrossRef]
- Lam, C.S.; Roger, V.L.; Rodeheffer, R.J.; Borlaug, B.A.; Enders, F.T.; Redfield, M.M. Pulmonary hypertension in heart failure with preserved ejection fraction: a community-based study. J. Am. Coll. Cardiol. 2009, 53, 1119–1126. [Google Scholar] [CrossRef] [PubMed]
- Anthony, C.; Akintoye, E.; Wang, T.; Klein, A. Echo doppler parameters of diastolic function. Curr. Cardiol. Rep. 2023, 25, 235–247. [Google Scholar] [CrossRef]
- Hodzic, A.; Garcia, D.; Saloux, E.; Ribeiro, P.A.B.; Ethier, A.; Thomas, J.D.; Milliez, P.; Normand, H.; Tournoux, F. Echocardiographic evidence of left ventricular untwisting-filling interplay. Cardiovasc. Ultrasound 2020, 18, 8. [Google Scholar] [CrossRef] [PubMed]
- Remme, E.W.; Opdahl, A.; Smiseth, O.A. Mechanics of left ventricular relaxation, early diastolic lengthening, and suction investigated in a mathematical model. Am. J. Physiol. Heart Circ. Physiol. 2011, 300, H1678–1687. [Google Scholar] [CrossRef]
- Opitz, C.A.; Kulke, M.; Leake, M.C.; Neagoe, C.; Hinssen, H.; Hajjar, R.J.; Linke, W.A. Damped elastic recoil of the titin spring in myofibrils of human myocardium. Proc. Natl. Acad. Sci. U. S. A. 2003, 100, 12688–12693. [Google Scholar] [CrossRef]
- Takagi, S.; Yokota, M.; Iwase, M.; Yoshida, J.; Hayashi, H.; Sotobata, I.; Koide, M.; Saito, H. The important role of left ventricular relaxation and left atrial pressure in the left ventricular filling velocity profile. Am. Heart J. 1989, 118, 954–962. [Google Scholar] [CrossRef] [PubMed]
- Opdahl, A.; Remme, E.W.; Helle-Valle, T.; Edvardsen, T.; Smiseth, O.A. Myocardial relaxation, restoring forces, and early-diastolic load are independent determinants of left ventricular untwisting rate. Circulation 2012, 126, 1441–1451. [Google Scholar] [CrossRef]
- Wang, J.; Khoury, D.S.; Thohan, V.; Torre-Amione, G.; Nagueh, S.F. Global diastolic strain rate for the assessment of left ventricular relaxation and filling pressures. Circulation 2007, 115, 1376–1383. [Google Scholar] [CrossRef] [PubMed]
- Sato, D.; Uchinoumi, H.; Bers, D.M. Increasing SERCA function promotes initiation of calcium sparks and breakup of calcium waves. J. Physiol. 2021, 599, 3267–3278. [Google Scholar] [CrossRef] [PubMed]
- Lipskaia, L.; Chemaly, E.R.; Hadri, L.; Lompre, A.M.; Hajjar, R.J. Sarcoplasmic reticulum Ca(2+) ATPase as a therapeutic target for heart failure. Expert Opin. Biol. Ther. 2010, 10, 29–41. [Google Scholar] [CrossRef]
- Shah, S.J.; Lam, C.S.P.; Svedlund, S.; Saraste, A.; Hage, C.; Tan, R.S.; Beussink-Nelson, L.; Ljung Faxen, U.; Fermer, M.L.; Broberg, M.A.; et al. Prevalence and correlates of coronary microvascular dysfunction in heart failure with preserved ejection fraction: PROMIS-HFpEF. Eur. Heart J. 2018, 39, 3439–3450. [Google Scholar] [CrossRef] [PubMed]
- Nagueh, S.F. Left ventricular diastolic function: Understanding pathophysiology, diagnosis, and prognosis with echocardiography. JACC Cardiovasc. Imaging 2020, 13, 228–244. [Google Scholar] [CrossRef]
- Ho, C.Y.; Solomon, S.D. A clinician's guide to tissue Doppler imaging. Circulation 2006, 113, e396–398. [Google Scholar] [CrossRef]
- Park, J.H.; Marwick, T.H. Use and limitations of E/e' to assess left ventricular filling pressure by echocardiography. J. Cardiovasc. Ultrasound 2011, 19, 169–173. [Google Scholar] [CrossRef]
- Chao, C.J.; Kato, N.; Scott, C.G.; Lopez-Jimenez, F.; Lin, G.; Kane, G.C.; Pellikka, P.A. Unsupervised machine learning for assessment of left ventricular diastolic function and risk stratification. J. Am. Soc. Echocardiogr. 2022, 35, 1214–1225. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef] [PubMed]
- Gaasch, W.H.; Zile, M.R. Left ventricular diastolic dysfunction and diastolic heart failure. Annu. Rev. Med. 2004, 55, 373–394. [Google Scholar] [CrossRef] [PubMed]
- Das, B.; Deshpande, S.; Akam-Venkata, J.; Shakti, D.; Moskowitz, W.; Lipshultz, S.E. Heart failure with preserved ejection fraction in children. Pediatr. Cardiol. 2023, 44, 513–529. [Google Scholar] [CrossRef] [PubMed]
- Borlaug, B.A.; Kane, G.C.; Melenovsky, V.; Olson, T.P. Abnormal right ventricular-pulmonary artery coupling with exercise in heart failure with preserved ejection fraction. Eur. Heart J. 2016, 37, 3293–3302. [Google Scholar] [CrossRef] [PubMed]
- Little, W.C.; Oh, J.K. Echocardiographic evaluation of diastolic function can be used to guide clinical care. Circulation 2009, 120, 802–809. [Google Scholar] [CrossRef] [PubMed]
- Tschope, C.; Paulus, W.J. Is echocardiographic evaluation of diastolic function useful in determining clinical care? Doppler echocardiography yields dubious estimates of left ventricular diastolic pressures. Circulation 2009, 120, 810–820. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, H.; Little, W.C.; Ohno, M.; Brucks, S.; Morimoto, A.; Cheng, H.J.; Cheng, C.P. Diastolic mitral annular velocity during the development of heart failure. J. Am. Coll. Cardiol. 2003, 41, 1590–1597. [Google Scholar] [CrossRef]
- Ommen, S.R.; Nishimura, R.A.; Appleton, C.P.; Miller, F.A.; Oh, J.K.; Redfield, M.M.; Tajik, A.J. Clinical utility of Doppler echocardiography and tissue Doppler imaging in the estimation of left ventricular filling pressures: A comparative simultaneous Doppler-catheterization study. Circulation 2000, 102, 1788–1794. [Google Scholar] [CrossRef]
- Parasuraman, S.; Walker, S.; Loudon, B.L.; Gollop, N.D.; Wilson, A.M.; Lowery, C.; Frenneaux, M.P. Assessment of pulmonary artery pressure by echocardiography—A comprehensive review. Int. J. Cardiol. Heart Vasc. 2016, 12, 45–51. [Google Scholar] [CrossRef]
- Melenovsky, V.; Hwang, S.J.; Redfield, M.M.; Zakeri, R.; Lin, G.; Borlaug, B.A. Left atrial remodeling and function in advanced heart failure with preserved or reduced ejection fraction. Circ. Heart Fail. 2015, 8, 295–303. [Google Scholar] [CrossRef]
- Freed, B.H.; Daruwalla, V.; Cheng, J.Y.; Aguilar, F.G.; Beussink, L.; Choi, A.; Klein, D.A.; Dixon, D.; Baldridge, A.; Rasmussen-Torvik, L.J.; et al. Prognostic utility and clinical significance of cardiac mechanics in heart failure with preserved ejection fraction: Importance of left atrial strain. Circ. Cardiovasc. Imaging 2016, 9. [Google Scholar] [CrossRef]
- Morris, D.A.; Belyavskiy, E.; Aravind-Kumar, R.; Kropf, M.; Frydas, A.; Braunauer, K.; Marquez, E.; Krisper, M.; Lindhorst, R.; Osmanoglou, E.; et al. Potential usefulness and clinical relevance of adding left atrial strain to left atrial volume index in the detection of left ventricular diastolic dysfunction. JACC Cardiovasc. Imaging 2018, 11, 1405–1415. [Google Scholar] [CrossRef]
- Silva, M.R.; Sampaio, F.; Braga, J.; Ribeiro, J.; Fontes-Carvalho, R. Left atrial strain evaluation to assess left ventricle diastolic dysfunction and heart failure with preserved ejection fraction: a guide to clinical practice: Left atrial strain and diastolic function. Int. J. Cardiovasc. Imaging 2023, 39, 1083–1096. [Google Scholar] [CrossRef]
- Kurt, M.; Wang, J.; Torre-Amione, G.; Nagueh, S.F. Left atrial function in diastolic heart failure. Circ. Cardiovasc. Imaging 2009, 2, 10–15. [Google Scholar] [CrossRef]
- Santos, A.B.; Roca, G.Q.; Claggett, B.; Sweitzer, N.K.; Shah, S.J.; Anand, I.S.; Fang, J.C.; Zile, M.R.; Pitt, B.; Solomon, S.D.; et al. Prognostic relevance of left atrial dysfunction in heart failure with preserved ejection fraction. Circ. Heart Fail. 2016, 9, e002763. [Google Scholar] [CrossRef]
- Obokata, M.; Negishi, K.; Kurosawa, K.; Arima, H.; Tateno, R.; Ui, G.; Tange, S.; Arai, M.; Kurabayashi, M. Incremental diagnostic value of LA strain with leg lifts in heart failure with preserved ejection fraction. JACC Cardiovasc. Imaging 2013, 6, 749–758. [Google Scholar] [CrossRef]
- Badesch, D.B.; Champion, H.C.; Gomez Sanchez, M.A.; Hoeper, M.M.; Loyd, J.E.; Manes, A.; McGoon, M.; Naeije, R.; Olschewski, H.; Oudiz, R.J.; et al. Diagnosis and assessment of pulmonary arterial hypertension. J. Am. Coll. Cardiol. 2009, 54, S55–S66. [Google Scholar] [CrossRef]
- Gillebert, T.C. Prediction of filling pressures and outcome in heart failure: can we improve E/e'? Eur. Heart J. Cardiovasc. Imaging 2019, 20, 655–657. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [PubMed]
- Merli, E.; Ciampi, Q.; Scali, M.C.; Zagatina, A.; Merlo, P.M.; Arbucci, R.; Daros, C.B.; de Castro e Silva Pretto, J.L.; Amor, M.; Salame, M.F.; et al. Pulmonary congestion during exercise stress echocardiography in ischemic and heart failure patients. Circ. Cardiovasc. Imaging 2022, 15, e013558. [Google Scholar] [CrossRef] [PubMed]
- Ha, J.W.; Andersen, O.S.; Smiseth, O.A. Diastolic stress test: Invasive and noninvasive testing. JACC Cardiovasc. Imaging 2020, 13, 272–282. [Google Scholar] [CrossRef] [PubMed]
- Lancellotti, P.; Pellikka, P.A.; Budts, W.; Chaudhry, F.A.; Donal, E.; Dulgheru, R.; Edvardsen, T.; Garbi, M.; Ha, J.W.; Kane, G.C.; et al. The clinical use of stress echocardiography in non-ischaemic heart disease: Recommendations from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2017, 30, 101–138. [Google Scholar] [CrossRef] [PubMed]
- Picano, E.; Ciampi, Q.; Arbucci, R.; Cortigiani, L.; Zagatina, A.; Celutkiene, J.; Bartolacelli, Y.; Kane, G.C.; Lowenstein, J.; Pellikka, P. Stress Echo 2030: the new ABCDE protocol defining the future of cardiac imaging. Eur. Heart J. Suppl. 2023, 25, C63–C67. [Google Scholar] [CrossRef]
- Gibby, C.; Wiktor, D.M.; Burgess, M.; Kusunose, K.; Marwick, T.H. Quantitation of the diastolic stress test: filling pressure vs. diastolic reserve. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: Executive summary: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 79, 1757–1780. [Google Scholar] [CrossRef]
- Kim, K.H.; Kane, G.C.; Luong, C.L.; Oh, J.K. Echocardiographic diastolic stress testing: What does it add? Curr. Cardiol. Rep. 2019, 21, 109. [Google Scholar] [CrossRef] [PubMed]
- Studer Bruengger, A.A.; Kaufmann, B.A.; Buser, M.; Hoffmann, M.; Bader, F.; Bernheim, A.M. Diastolic stress echocardiography in the young: a study in nonathletic and endurance-trained healthy subjects. J. Am. Soc. Echocardiogr. 2014, 27, 1053–1059. [Google Scholar] [CrossRef] [PubMed]
- Ha, J.W.; Oh, J.K.; Pellikka, P.A.; Ommen, S.R.; Stussy, V.L.; Bailey, K.R.; Seward, J.B.; Tajik, A.J. Diastolic stress echocardiography: a novel noninvasive diagnostic test for diastolic dysfunction using supine bicycle exercise Doppler echocardiography. J. Am. Soc. Echocardiogr. 2005, 18, 63–68. [Google Scholar] [CrossRef]
- Ha, J.W.; Lulic, F.; Bailey, K.R.; Pellikka, P.A.; Seward, J.B.; Tajik, A.J.; Oh, J.K. Effects of treadmill exercise on mitral inflow and annular velocities in healthy adults. Am. J. Cardiol. 2003, 91, 114–115. [Google Scholar] [CrossRef] [PubMed]
- Al-Gburi, A.J.J. Left ventricular diastolic reserve by exercise stress echocardiography in prediabetes. Tzu Chi Med. J. 2023, 35, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Ha, J.-W.; Choi, D.; Park, S.; Choi, E.-Y.; Shim, C.-Y.; Kim, J.-M.; Ahn, J.-A.; Lee, S.-W.; Oh, J.K.; Chung, N. Left ventricular diastolic functional reserve during exercise in patients with impaired myocardial relaxation at rest. Heart 2009, 95, 399–404. [Google Scholar] [CrossRef]
- Obokata, M.; Kane, G.C.; Reddy, Y.N.; Olson, T.P.; Melenovsky, V.; Borlaug, B.A. Role of diastolic stress testing in the evaluation for heart failure with preserved ejection fraction: A simultaneous invasive-echocardiographic study. Circulation 2017, 135, 825–838. [Google Scholar] [CrossRef]
- Mitter, S.S.; Shah, S.J.; Thomas, J.D. A test in context: E/A and E/e' to assess diastolic dysfunction and LV filling pressure. J. Am. Coll. Cardiol. 2017, 69, 1451–1464. [Google Scholar] [CrossRef]
- Pavlin, E.G.; VanNimwegan, D.; Hornbein, T.F. Failure of a high-compliance low-pressure cuff to prevent aspiration. Anesthesiology 1975, 42, 216–219. [Google Scholar] [CrossRef]
- Ebrahimi, F.; Gharedaghi, M.H.; Zubair, M.; Kohanchi, D.; Aghajani, K.; Candido, K. Speckle- tracking echocardiography for the staging of diastolic dysfunction: The correlation between strain-based indices and the severity of left ventricular diastolic dysfunction. J. Cardiothorac. Vasc. Anesth. 2021, 35, 216–221. [Google Scholar] [CrossRef]
- Ebrahimi, F.; Gharedaghi, M.H.; Shafaroodi, H.; Ghasemi, M.; Aghajani, K.; Candido, K. Left ventricular strain rate for intraoperative evaluation of cardiac diastolic function by transesophageal echocardiography: The correlation between late diastolic peak longitudinal strain rate and the severity of diastolic dysfunction. J. Cardiothorac. Vasc. Anesth. 2022, 36, 178–183. [Google Scholar] [CrossRef]
- Ebrahimi, F.; Gharedaghi, M.H.; Petrossian, V.; Kohanchi, D. Intraoperative assessment of coronary artery stenosis by 2D speckle-tracking echocardiography: The correlation between peak strain rate during early diastole and the severity of coronary artery stenosis in patients undergoing coronary artery bypass grafting. J. Cardiothorac. Vasc. Anesth. 2019, 33, 2652–2657. [Google Scholar] [CrossRef] [PubMed]
- Chong, A.; MacLaren, G.; Chen, R.; Connelly, K.A. Perioperative applications of deformation (myocardial strain) imaging with speckle-tracking echocardiography. J. Cardiothorac. Vasc. Anesth. 2014, 28, 128–140. [Google Scholar] [CrossRef] [PubMed]
- Marwick, T.H. Measurement of strain and strain rate by echocardiography: ready for prime time? J. Am. Coll. Cardiol. 2006, 47, 1313–1327. [Google Scholar] [CrossRef] [PubMed]
- Guan, Z.; Zhang, D.; Huang, R.; Zhang, F.; Wang, Q.; Guo, S. Association of left atrial myocardial function with left ventricular diastolic dysfunction in subjects with preserved systolic function: a strain rate imaging study. Clin. Cardiol. 2010, 33, 643–649. [Google Scholar] [CrossRef]
- Kornev, M.; Caglayan, H.A.; Kudryavtsev, A.V.; Malyutina, S.; Ryabikov, A.; Schirmer, H.; Rosner, A. Influence of hypertension on systolic and diastolic left ventricular function including segmental strain and strain rate. Echocardiography 2023, 40, 623–633. [Google Scholar] [CrossRef] [PubMed]
- Maragiannis, D.; Nagueh, S.F. Echocardiographic evaluation of left ventricular diastolic function: an update. Curr. Cardiol. Rep. 2015, 17, 3. [Google Scholar] [CrossRef]
- Kato, T.; Noda, A.; Izawa, H.; Nishizawa, T.; Somura, F.; Yamada, A.; Nagata, K.; Iwase, M.; Nakao, A.; Yokota, M. Myocardial velocity gradient as a noninvasively determined index of left ventricular diastolic dysfunction in patients with hypertrophic cardiomyopathy. J. Am. Coll. Cardiol. 2003, 42, 278–285. [Google Scholar] [CrossRef]
- Kong, L.Y.; Gao, X.; Ding, X.Y.; Wang, G.; Liu, F. Left ventricular end-diastolic strain rate recovered in hypothyroidism following levothyroxine replacement therapy: A strain rate imaging study. Echocardiography 2019, 36, 707–713. [Google Scholar] [CrossRef] [PubMed]
- Kasner, M.; Gaub, R.; Sinning, D.; Westermann, D.; Steendijk, P.; Hoffmann, W.; Schultheiss, H.P.; Tschope, C. Global strain rate imaging for the estimation of diastolic function in HFNEF compared with pressure-volume loop analysis. Eur. J. Echocardiogr. 2010, 11, 743–751. [Google Scholar] [CrossRef]
- Hayashi, T.; Yamada, S.; Iwano, H.; Nakabachi, M.; Sakakibara, M.; Okada, K.; Murai, D.; Nishino, H.; Kusunose, K.; Watanabe, K.; et al. Left ventricular global strain for estimating relaxation and filling pressure: A multicenter study. Circ. J. 2016, 80, 1163–1170. [Google Scholar] [CrossRef] [PubMed]
- Cameli, M.; Mandoli, G.E.; Loiacono, F.; Sparla, S.; Iardino, E.; Mondillo, S. Left atrial strain: A useful index in atrial fibrillation. Int. J. Cardiol. 2016, 220, 208–213. [Google Scholar] [CrossRef]
- Kosmala, W.; Marwick, T.H. Asymptomatic left ventricular diastolic dysfunction: Predicting progression to symptomatic heart failure. JACC Cardiovasc. Imaging 2020, 13, 215–227. [Google Scholar] [CrossRef] [PubMed]
- Jarasunas, J.; Aidietis, A.; Aidietiene, S. Left atrial strain - an early marker of left ventricular diastolic dysfunction in patients with hypertension and paroxysmal atrial fibrillation. Cardiovasc. Ultrasound 2018, 16, 29. [Google Scholar] [CrossRef] [PubMed]
- Mandoli, G.E.; Sisti, N.; Mondillo, S.; Cameli, M. Left atrial strain in left ventricular diastolic dysfunction: have we finally found the missing piece of the puzzle? Heart Fail. Rev. 2020, 25, 409–417. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Addetia, K.; Maffessanti, F.; Mor-Avi, V.; Lang, R.M. LA strain for categorization of LV diastolic dysfunction. JACC Cardiovasc. Imaging 2017, 10, 735–743. [Google Scholar] [CrossRef]
- Cameli, M.; Sparla, S.; Losito, M.; Righini, F.M.; Menci, D.; Lisi, M.; D'Ascenzi, F.; Focardi, M.; Favilli, R.; Pierli, C.; et al. Correlation of left atrial strain and Doppler measurements with invasive measurement of left ventricular end-diastolic pressure in patients stratified for different values of ejection fraction. Echocardiography 2016, 33, 398–405. [Google Scholar] [CrossRef]
- Thomas, L.; Marwick, T.H.; Popescu, B.A.; Donal, E.; Badano, L.P. Left atrial structure and function, and left ventricular diastolic dysfunction: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 73, 1961–1977. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Khan, S.U. Left atrial strain for assessment of left ventricular diastolic function: Focus on populations with normal LVEF. JACC Cardiovasc. Imaging 2023, 16, 691–707. [Google Scholar] [CrossRef]
- Hewing, B.; Theres, L.; Spethmann, S.; Stangl, K.; Dreger, H.; Knebel, F. Left atrial strain predicts hemodynamic parameters in cardiovascular patients. Echocardiography 2017, 34, 1170–1178. [Google Scholar] [CrossRef]
- Yeung, D.F.; Abolmaesumi, P.; Tsang, T.S.M. Artificial intelligence for left ventricular diastolic function assessment: A new paradigm on the horizon. J. Am. Soc. Echocardiogr. 2023, 36, 1079–1082. [Google Scholar] [CrossRef]
- Othman, F.; Abushahba, G.; Salustri, A. Adherence to the American Society of Echocardiography and European Association of Cardiovascular Imaging recommendations for the evaluation of left ventricular diastolic function by echocardiography: A quality improvement project. J. Am. Soc. Echocardiogr. 2019, 32, 1619–1621. [Google Scholar] [CrossRef] [PubMed]
- Choi, D.J.; Park, J.J.; Ali, T.; Lee, S. Artificial intelligence for the diagnosis of heart failure. NPJ Digit. Med. 2020, 3, 54. [Google Scholar] [CrossRef] [PubMed]
- Salem Omar, A.M.; Shameer, K.; Narula, S.; Abdel Rahman, M.A.; Rifaie, O.; Narula, J.; Dudley, J.T.; Sengupta, P.P. Artificial intelligence-based assessment of left ventricular filling pressures from 2-dimensional cardiac ultrasound images. JACC Cardiovasc. Imaging 2018, 11, 509–510. [Google Scholar] [CrossRef]
- Pandey, A.; Kagiyama, N.; Yanamala, N.; Segar, M.W.; Cho, J.S.; Tokodi, M.; Sengupta, P.P. Deep-learning models for the echocardiographic assessment of diastolic dysfunction. JACC Cardiovasc. Imaging 2021, 14, 1887–1900. [Google Scholar] [CrossRef]
- Chiou, Y.A.; Hung, C.L.; Lin, S.F. AI-assisted echocardiographic prescreening of heart failure with preserved ejection fraction on the basis of intrabeat dynamics. JACC Cardiovasc. Imaging 2021, 14, 2091–2104. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Yang, F.; Zhang, P.; Lin, X.; Wang, W.; Pu, H.; Chen, X.; Chen, Y.; Yu, L.; Deng, Y.; et al. Artificial intelligence-assisted left ventricular diastolic function assessment and grading: Multiview versus single view. J. Am. Soc. Echocardiogr. 2023, 36, 1064–1078. [Google Scholar] [CrossRef]
- Beladan, C.C.; Botezatu, S.; Popescu, B.A. Reversible left ventricular diastolic dysfunction—Overview and clinical implications. Echocardiography 2020, 37, 1957–1966. [Google Scholar] [CrossRef] [PubMed]
- Matyal, R.; Skubas, N.J.; Shernan, S.K.; Mahmood, F. Perioperative assessment of diastolic dysfunction. Anesth. Analg. 2011, 113, 449–472. [Google Scholar] [CrossRef]
- Huttin, O.; Fraser, A.G.; Lund, L.H.; Donal, E.; Linde, C.; Kobayashi, M.; Erdei, T.; Machu, J.L.; Duarte, K.; Rossignol, P.; et al. Risk stratification with echocardiographic biomarkers in heart failure with preserved ejection fraction: the media echo score. ESC Heart Fail. 2021, 8, 1827–1839. [Google Scholar] [CrossRef]
- Vasan, R.S.; Xanthakis, V.; Lyass, A.; Andersson, C.; Tsao, C.; Cheng, S.; Aragam, J.; Benjamin, E.J.; Larson, M.G. Epidemiology of left ventricular systolic dysfunction and heart failure in the Framingham study: An echocardiographic study over 3 decades. JACC Cardiovasc. Imaging 2018, 11, 1–11. [Google Scholar] [CrossRef]
- Morris, D.A.; Ma, X.X.; Belyavskiy, E.; Aravind Kumar, R.; Kropf, M.; Kraft, R.; Frydas, A.; Osmanoglou, E.; Marquez, E.; Donal, E.; et al. Left ventricular longitudinal systolic function analysed by 2D speckle-tracking echocardiography in heart failure with preserved ejection fraction: a meta-analysis. Open Heart 2017, 4, e000630. [Google Scholar] [CrossRef] [PubMed]
- Borlaug, B.A. Evaluation and management of heart failure with preserved ejection fraction. Nat. Rev. Cardiol 2020, 17, 559–573. [Google Scholar] [CrossRef] [PubMed]
- Esfandiari, S.; Wolsk, E.; Granton, D.; Azevedo, L.; Valle, F.H.; Gustafsson, F.; Mak, S. Pulmonary arterial wedge pressure at rest and during exercise in healthy adults: A systematic review and meta-analysis. J. Card. Fail. 2019, 25, 114–122. [Google Scholar] [CrossRef]
- Malik, A.; Brito, D.; Vaqar, S.; Chhabra, L. Congestive heart failure. In StatPearls; Treasure Island (FL), 2023.
- Saha, S.K.; Kiotsekoglou, A.; Nanda, N.C. Echocardiography 2020: Toward deciphering the "Rosetta stone" of left ventricular diastolic function. Echocardiography 2020, 37, 1886–1889. [Google Scholar] [CrossRef]
- Shah, A.M.; Cikes, M.; Prasad, N.; Li, G.; Getchevski, S.; Claggett, B.; Rizkala, A.; Lukashevich, I.; O'Meara, E.; Ryan, J.J.; et al. Echocardiographic features of patients with heart failure and preserved left ventricular ejection fraction. J. Am. Coll. Cardiol. 2019, 74, 2858–2873. [Google Scholar] [CrossRef]
- Chetrit, M.; Cremer, P.C.; Klein, A.L. Imaging of diastolic dysfunction in community-based epidemiological studies and randomized controlled trials of HFpEF. JACC Cardiovasc. Imaging 2020, 13, 310–326. [Google Scholar] [CrossRef]
- Obokata, M.; Reddy, Y.N.V.; Borlaug, B.A. Diastolic dysfunction and heart failure with preserved ejection fraction: Understanding mechanisms by using noninvasive methods. JACC Cardiovasc. Imaging 2020, 13, 245–257. [Google Scholar] [CrossRef]
- Harada, T.; Kagami, K.; Kato, T.; Obokata, M. Echocardiography in the diagnostic evaluation and phenotyping of heart failure with preserved ejection fraction. J. Cardiol. 2022, 79, 679–690. [Google Scholar] [CrossRef]
- Lundberg, A.; Johnson, J.; Hage, C.; Back, M.; Merkely, B.; Venkateshvaran, A.; Lund, L.H.; Nagy, A.I.; Manouras, A. Left atrial strain improves estimation of filling pressures in heart failure: a simultaneous echocardiographic and invasive haemodynamic study. Clin. Res. Cardiol. 2019, 108, 703–715. [Google Scholar] [CrossRef]
- Reddy, Y.N.; Carter, R.E.; Obokata, M.; Redfield, M.M.; Borlaug, B.A. A simple, evidence-based approach to help guide diagnosis of heart failure with preserved ejection fraction. Circulation 2018, 138, 861–870. [Google Scholar] [CrossRef]
- Smiseth, O.A.; Morris, D.A.; Cardim, N.; Cikes, M.; Delgado, V.; Donal, E.; Flachskampf, F.A.; Galderisi, M.; Gerber, B.L.; Gimelli, A.; et al. Multimodality imaging in patients with heart failure and preserved ejection fraction: an expert consensus document of the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2022, 23, e34–e61. [Google Scholar] [CrossRef]
- Belyavskiy, E.; Morris, D.A.; Url-Michitsch, M.; Verheyen, N.; Meinitzer, A.; Radhakrishnan, A.K.; Kropf, M.; Frydas, A.; Ovchinnikov, A.G.; Schmidt, A.; et al. Diastolic stress test echocardiography in patients with suspected heart failure with preserved ejection fraction: a pilot study. ESC Heart Fail. 2019, 6, 146–153. [Google Scholar] [CrossRef]
- Lancellotti, P.; Pellikka, P.A.; Budts, W.; Chaudhry, F.A.; Donal, E.; Dulgheru, R.; Edvardsen, T.; Garbi, M.; Ha, J.W.; Kane, G.C.; et al. The clinical use of stress echocardiography in non-ischaemic heart disease: recommendations from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 1191–1229. [Google Scholar] [CrossRef] [PubMed]
- Palmer, C.; Mazur, W.; Truong, V.T.; Nagueh, S.F.; Fowler, J.A.; Shelton, K.; Joshi, V.M.; Ness, K.K.; Srivastava, D.K.; Robison, L.L. Prevalence of diastolic dysfunction in adult survivors of childhood cancer: a report from SJLIFE cohort. Cardiooncology 2023, 5, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.M.; Claggett, B.; Sweitzer, N.K.; Shah, S.J.; Anand, I.S.; O'Meara, E.; Desai, A.S.; Heitner, J.F.; Li, G.; Fang, J.; et al. Cardiac structure and function and prognosis in heart failure with preserved ejection fraction: findings from the echocardiographic study of the Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist (TOPCAT) Trial. Circ. Heart Fail. 2014, 7, 740–751. [Google Scholar] [CrossRef] [PubMed]
- Inoue, K.; Khan, F.H.; Remme, E.W.; Ohte, N.; Garcia-Izquierdo, E.; Chetrit, M.; Monivas-Palomero, V.; Mingo-Santos, S.; Andersen, O.S.; Gude, E.; et al. Determinants of left atrial reservoir and pump strain and use of atrial strain for evaluation of left ventricular filling pressure. Eur. Heart J. Cardiovasc. Imaging 2021, 23, 61–70. [Google Scholar] [CrossRef]
- Reddy, Y.N.V.; Obokata, M.; Egbe, A.; Yang, J.H.; Pislaru, S.; Lin, G.; Carter, R.; Borlaug, B.A. Left atrial strain and compliance in the diagnostic evaluation of heart failure with preserved ejection fraction. Eur. J. Heart Fail. 2019, 21, 891–900. [Google Scholar] [CrossRef]
- Singh, A.; Medvedofsky, D.; Mediratta, A.; Balaney, B.; Kruse, E.; Ciszek, B.; Shah, A.P.; Blair, J.E.; Maffessanti, F.; Addetia, K.; et al. Peak left atrial strain as a single measure for the non-invasive assessment of left ventricular filling pressures. Int. J. Cardiovasc. Imaging 2019, 35, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Telles, F.; Nanayakkara, S.; Evans, S.; Patel, H.C.; Mariani, J.A.; Vizi, D.; William, J.; Marwick, T.H.; Kaye, D.M. Impaired left atrial strain predicts abnormal exercise haemodynamics in heart failure with preserved ejection fraction. Eur. J. Heart Fail. 2019, 21, 495–505. [Google Scholar] [CrossRef] [PubMed]
- Morris, D.A.; Takeuchi, M.; Krisper, M.; Kohncke, C.; Bekfani, T.; Carstensen, T.; Hassfeld, S.; Dorenkamp, M.; Otani, K.; Takigiku, K.; et al. Normal values and clinical relevance of left atrial myocardial function analysed by speckle-tracking echocardiography: multicentre study. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 364–372. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global burden of cardiovascular diseases and risk factors, 1990-2019: Update from the GBD 2019 study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Ladeiras-Lopes, R.; Fontes-Carvalho, R.; Vilela, E.M.; Bettencourt, P.; Leite-Moreira, A.; Azevedo, A. Diastolic function is impaired in patients with prehypertension: Data from the EPIPorto study. Rev. Esp. Cardiol. (Engl. Ed.) 2018, 71, 926–934. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.K.; Park, J.H. Role of strain echocardiography in patients with hypertension. Clin. Hypertens. 2022, 28, 6. [Google Scholar] [CrossRef]
- Wan, S.-H.; Vogel, M.W.; Chen, H.H. Pre-clinical diastolic dysfunction. J. Am. Coll. Cardiol. 2014, 63, 407–416. [Google Scholar] [CrossRef]
- Cameli, M.; Lembo, M.; Sciaccaluga, C.; Bandera, F.; Ciccone, M.M.; D'Andrea, A.; D'Ascenzi, F.; Esposito, R.; Evola, V.; Liga, R.; et al. Identification of cardiac organ damage in arterial hypertension: insights by echocardiography for a comprehensive assessment. J. Hypertens. 2020, 38, 588–598. [Google Scholar] [CrossRef]
- Kuznetsova, T.; Thijs, L.; Knez, J.; Herbots, L.; Zhang, Z.; Staessen, J.A. Prognostic value of left ventricular diastolic dysfunction in a general population. J. Am. Heart Assoc. 2014, 3, e000789. [Google Scholar] [CrossRef]
- Tadic, M.; Cuspidi, C.; Marwick, T.H. Phenotyping the hypertensive heart. Eur. Heart J. 2022, 43, 3794–3810. [Google Scholar] [CrossRef]
- Cuspidi, C.; Meani, S.; Fusi, V.; Valerio, C.; Catini, E.; Sala, C.; Sampieri, L.; Magrini, F.; Zanchetti, A. Prevalence and correlates of left atrial enlargement in essential hypertension: role of ventricular geometry and the metabolic syndrome: the Evaluation of Target Organ Damage in Hypertension study. J. Hypertens. 2005, 23, 875–882. [Google Scholar] [CrossRef]
- Wu, V.C.; Takeuchi, M.; Kuwaki, H.; Iwataki, M.; Nagata, Y.; Otani, K.; Haruki, N.; Yoshitani, H.; Tamura, M.; Abe, H.; et al. Prognostic value of LA volumes assessed by transthoracic 3D echocardiography: comparison with 2D echocardiography. JACC Cardiovasc. Imaging 2013, 6, 1025–1035. [Google Scholar] [CrossRef]
- Astarita, C.; Palinkas, A.; Nicolai, E.; Maresca, F.S.; Varga, A.; Picano, E. Dipyridamole-atropine stress echocardiography versus exercise SPECT scintigraphy for detection of coronary artery disease in hypertensives with positive exercise test. J. Hypertens. 2001, 19, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, S.; Fazlinezhad, A.; Jalalyazdi, M.; Gharaee, A.; Hosseini, L.; Andalibi, M.S.S. Diastolic function changes during stress echocardiography in hypertensive patients. Razavi Int. J. Med. 2017, 5, e42876. [Google Scholar] [CrossRef]
- Peteiro, J.; Pazos, P.; Bouzas, A.; Pinon, P.; Estevez, R.; Castro-Beiras, A. Assessment of diastolic function during exercise echocardiography: annulus mitral velocity or transmitral flow pattern? J. Am. Soc. Echocardiogr. 2008, 21, 178–184. [Google Scholar] [CrossRef]
- Dini, F.L.; Galderisi, M.; Nistri, S.; Buralli, S.; Ballo, P.; Mele, D.; Badano, L.P.; Faggiano, P.; De Gregorio, C.; Rosa, G.M. Abnormal left ventricular longitudinal function assessed by echocardiographic and tissue Doppler imaging is a powerful predictor of diastolic dysfunction in hypertensive patients: the SPHERE study. Int. J. Cardiol. 2013, 168, 3351–3358. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Ni, C.F.; Yang, C.; Yan, Z.N.; Fan, L. Assessment of subclinical left atrial myocardial dysfunction in essential hypertension patients with normal left ventricle function by two-dimensional strain and volume-derived variables. J. Clin. Ultrasound 2021, 49, 659–666. [Google Scholar] [CrossRef] [PubMed]
- Miljkovic, T.; Ilic, A.; Milovancev, A.; Bjelobrk, M.; Stefanovic, M.; Stojsic-Milosavljevic, A.; Tadic, S.; Golubovic, M.; Popov, T.; Petrovic, M. Left atrial strain as a predictor of left ventricular diastolic dysfunction in patients with arterial hypertension. Medicina (Kaunas) 2022, 58. [Google Scholar] [CrossRef]
- Carluccio, E.; Cameli, M.; Rossi, A.; Dini, F.L.; Biagioli, P.; Mengoni, A.; Jacoangeli, F.; Mandoli, G.E.; Pastore, M.C.; Maffeis, C. Left atrial strain in the assessment of diastolic function in heart failure: a machine learning approach. Circ. Cardiovasc. Imaging 2023, 16, e014605. [Google Scholar] [CrossRef]
Figure 1.
Simplified schematic diagram of Ca2+ regulation channels during myocardial cell contraction and relaxation phases. The sarcoendoplasmic reticulum calcium ATPase (SERCA-ATPase) pump is vital for the absorption and storage of Ca2+ into the sarcoplasmic reticulum (SR). This action results in a reduction of Ca2+ concentration in cytoplasm, contributing to the initiation of the myocyte's relaxation phase. Importantly, SERCA-ATPase remains active throughout the entire relaxation process. In parallel, ryanodine receptors (RyR), stimulated by external Ca2+ from L-type Ca2+ channels, release stored Ca2+ from the SR. This leads to an elevated concentration of Ca2+ in the cytoplasm, ultimately triggering myocyte contraction.
Figure 1.
Simplified schematic diagram of Ca2+ regulation channels during myocardial cell contraction and relaxation phases. The sarcoendoplasmic reticulum calcium ATPase (SERCA-ATPase) pump is vital for the absorption and storage of Ca2+ into the sarcoplasmic reticulum (SR). This action results in a reduction of Ca2+ concentration in cytoplasm, contributing to the initiation of the myocyte's relaxation phase. Importantly, SERCA-ATPase remains active throughout the entire relaxation process. In parallel, ryanodine receptors (RyR), stimulated by external Ca2+ from L-type Ca2+ channels, release stored Ca2+ from the SR. This leads to an elevated concentration of Ca2+ in the cytoplasm, ultimately triggering myocyte contraction.
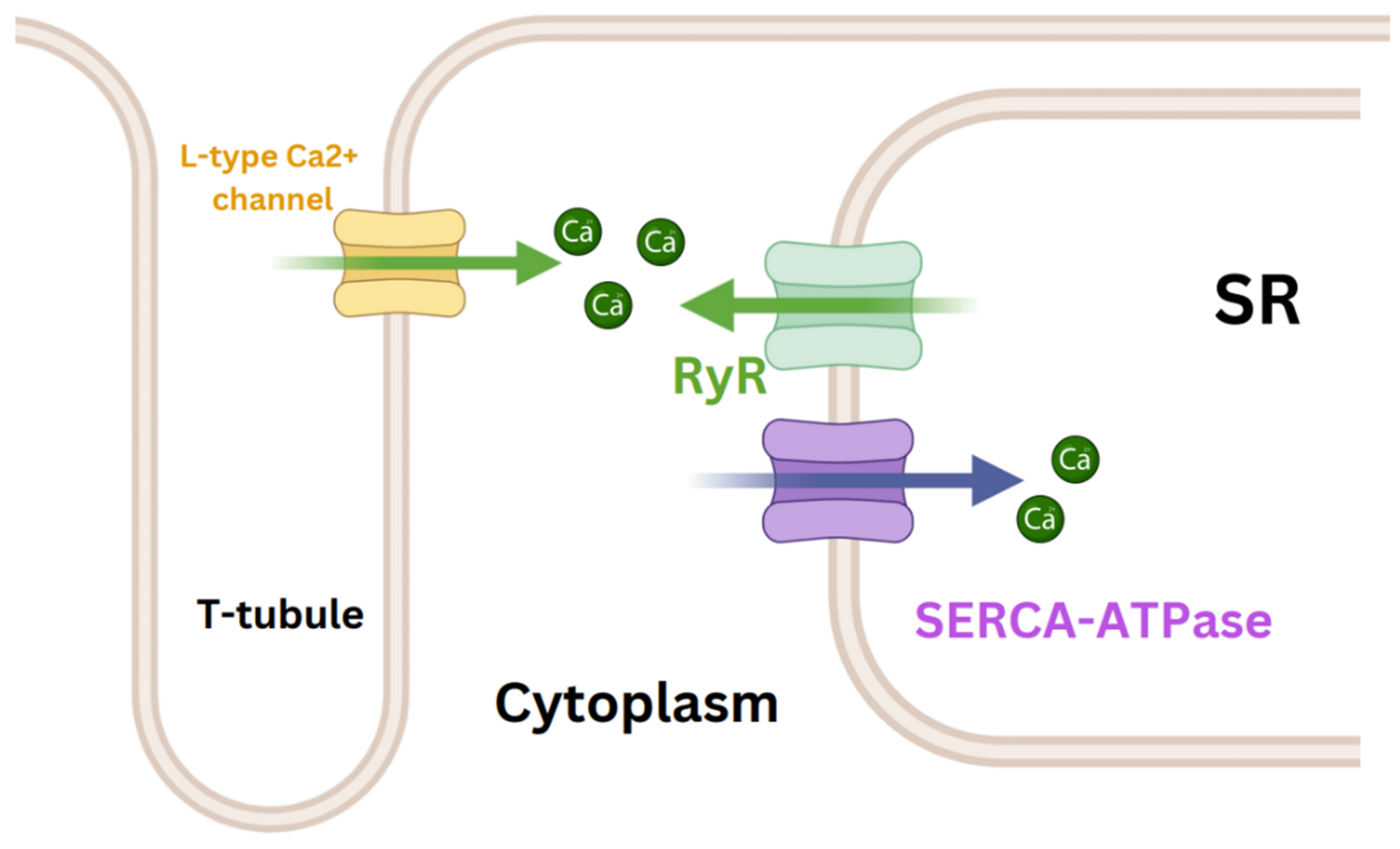
Figure 2.
Schematic representation of left ventricular pressure (LVP), left atrial pressure (LAP), and LV filling rate during the relaxation phase. For more details, please refer to Table 1. The initial pressure crossover marks the conclusion of isovolumic relaxation and the commencement of mitral valve opening. In the initial phase, LAP surpasses LVP, hastening mitral flow, and peak mitral E aligns with the second crossover. Subsequently, LVP surpasses LAP, slowing mitral flow and demarcating the early rapid filling phase and deceleration filling phase. These phases are succeeded by diastasis, characterized by minimal pressure differentials. During atrial contraction, LAP once again surpasses LVP, and an A wave appears. E: mitral peak velocity of early filling; A: mitral peak velocity of late filling.
Figure 2.
Schematic representation of left ventricular pressure (LVP), left atrial pressure (LAP), and LV filling rate during the relaxation phase. For more details, please refer to Table 1. The initial pressure crossover marks the conclusion of isovolumic relaxation and the commencement of mitral valve opening. In the initial phase, LAP surpasses LVP, hastening mitral flow, and peak mitral E aligns with the second crossover. Subsequently, LVP surpasses LAP, slowing mitral flow and demarcating the early rapid filling phase and deceleration filling phase. These phases are succeeded by diastasis, characterized by minimal pressure differentials. During atrial contraction, LAP once again surpasses LVP, and an A wave appears. E: mitral peak velocity of early filling; A: mitral peak velocity of late filling.
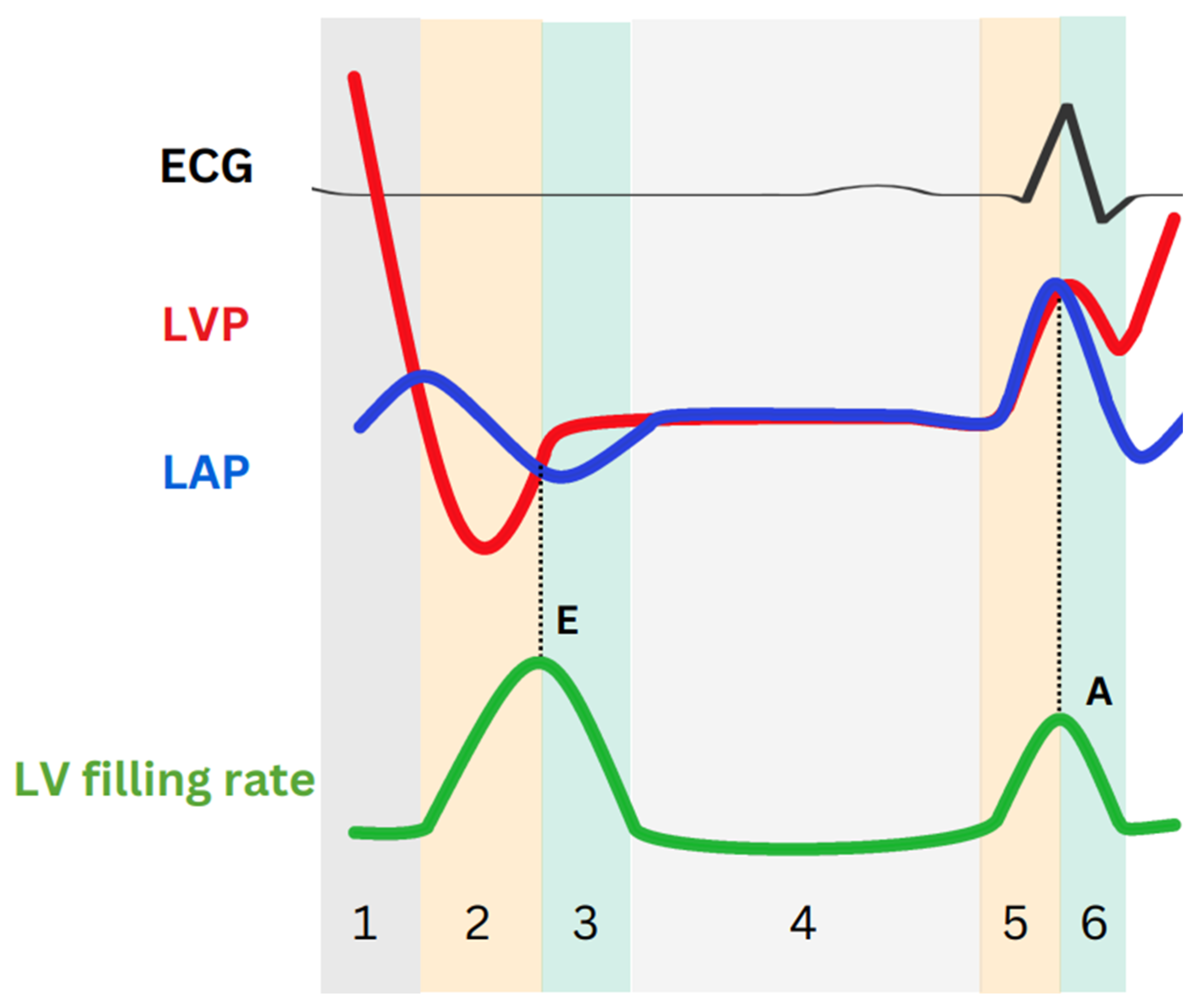
Figure 3.
Schematic representation of LV strain, strain rate, and LAS.
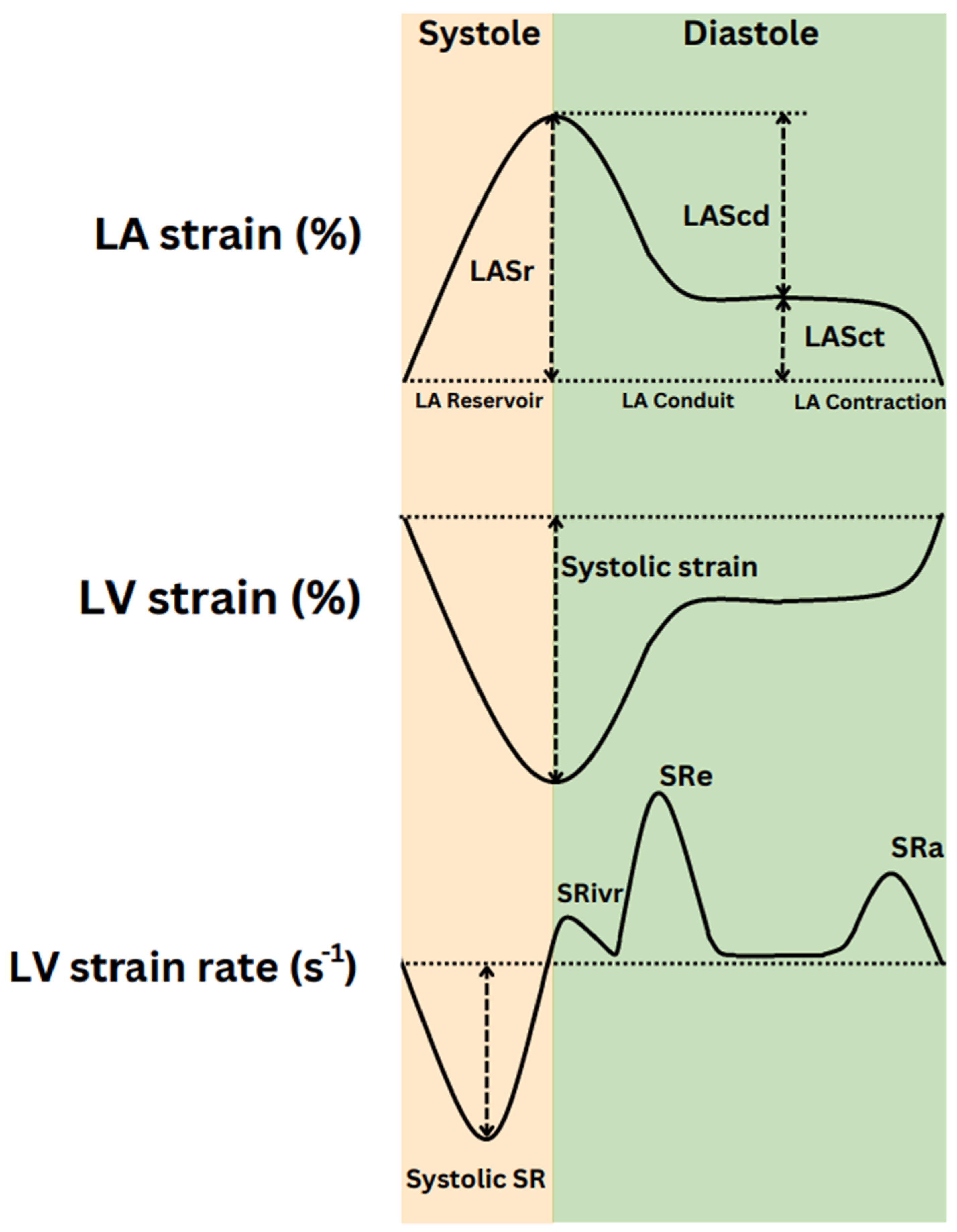
Figure 4.
Diverse schematic patterns of left ventricular diastolic dysfunction (LVDD) illustrated through transmitral flow (upper) and tissue Doppler at the level of the mitral annulus (lower). As LVDD worsens, the peak value of e' decreases progressively and is reached later in the cycle. E: mitral peak velocity of early filling; A: mitral peak velocity of late filling; e’: mitral annular peak velocity of early filling; a’: mitral annular peak velocity of late filling.
Figure 4.
Diverse schematic patterns of left ventricular diastolic dysfunction (LVDD) illustrated through transmitral flow (upper) and tissue Doppler at the level of the mitral annulus (lower). As LVDD worsens, the peak value of e' decreases progressively and is reached later in the cycle. E: mitral peak velocity of early filling; A: mitral peak velocity of late filling; e’: mitral annular peak velocity of early filling; a’: mitral annular peak velocity of late filling.
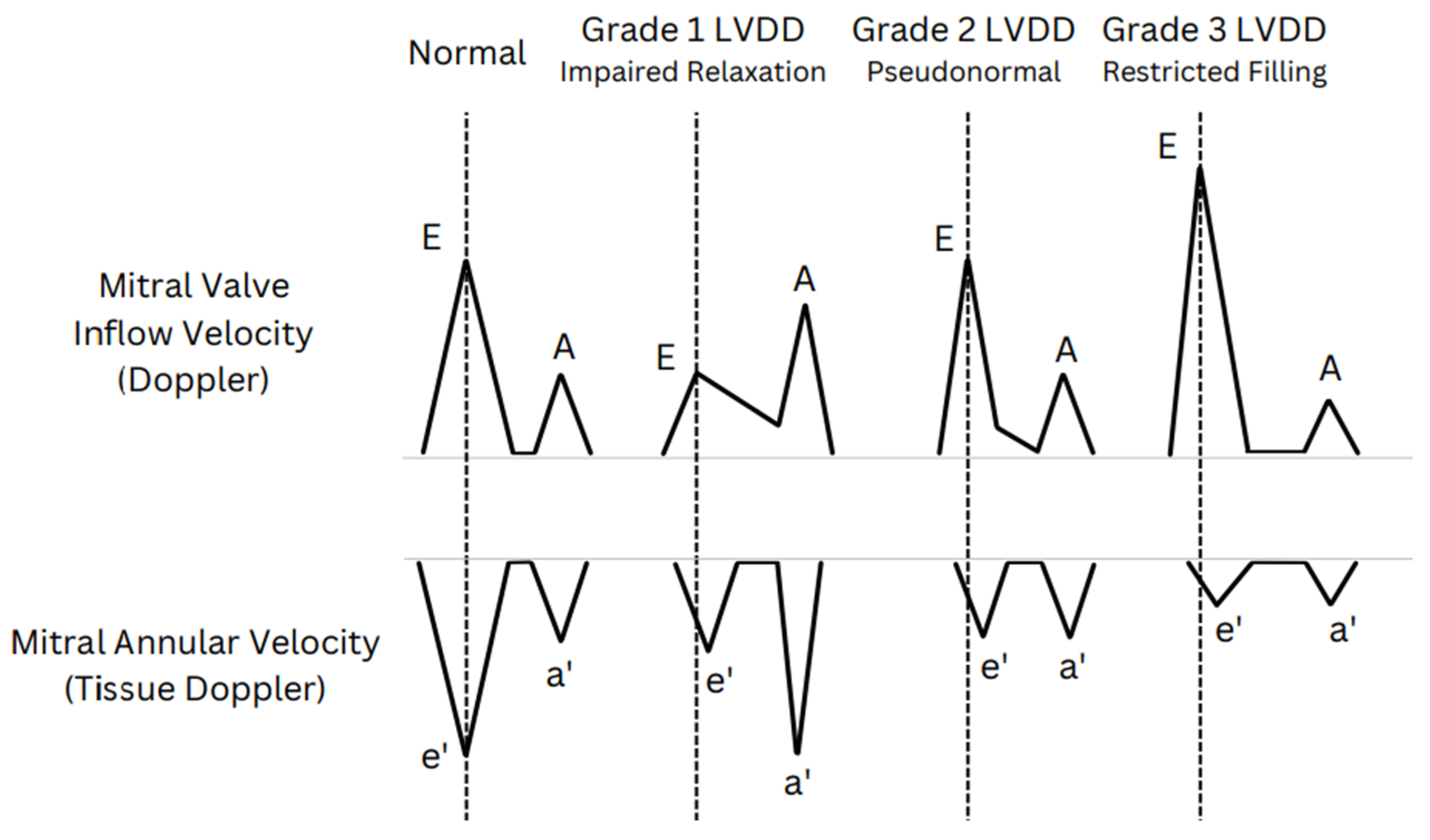
Figure 5.
Algorithm A for diagnosis of LV diastolic dysfunction in subjects with normal LV ejection fraction (LVEF). E: mitral peak velocity of early filling; e’: mitral annular velocity of early filling by tissue Doppler; TR: tricuspid valve regurgitation; LA: left atrium; Vmax: maximum velocity.
Figure 5.
Algorithm A for diagnosis of LV diastolic dysfunction in subjects with normal LV ejection fraction (LVEF). E: mitral peak velocity of early filling; e’: mitral annular velocity of early filling by tissue Doppler; TR: tricuspid valve regurgitation; LA: left atrium; Vmax: maximum velocity.
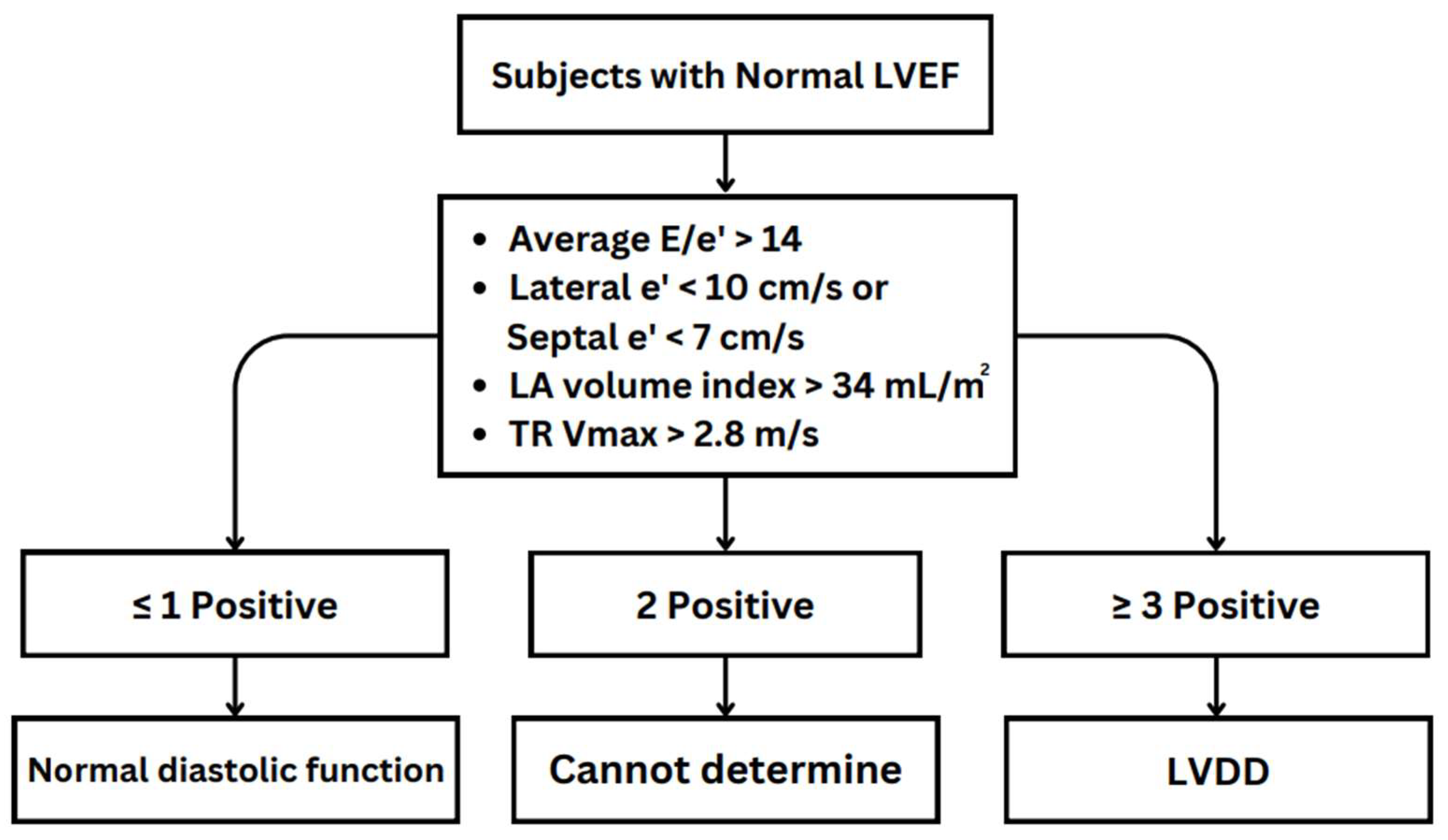
Figure 6.
Algorithm B for estimating LV filling pressures and grading LV diastolic dysfunction. LAP: left atrial pressure; E/A: ratio of mitral peak velocities of early and late filling e’: mitral annular velocity of early filling by tissue Doppler; LV: left ventricular; LA: left atrial; LVDD: diastolic dysfunction.
Figure 6.
Algorithm B for estimating LV filling pressures and grading LV diastolic dysfunction. LAP: left atrial pressure; E/A: ratio of mitral peak velocities of early and late filling e’: mitral annular velocity of early filling by tissue Doppler; LV: left ventricular; LA: left atrial; LVDD: diastolic dysfunction.
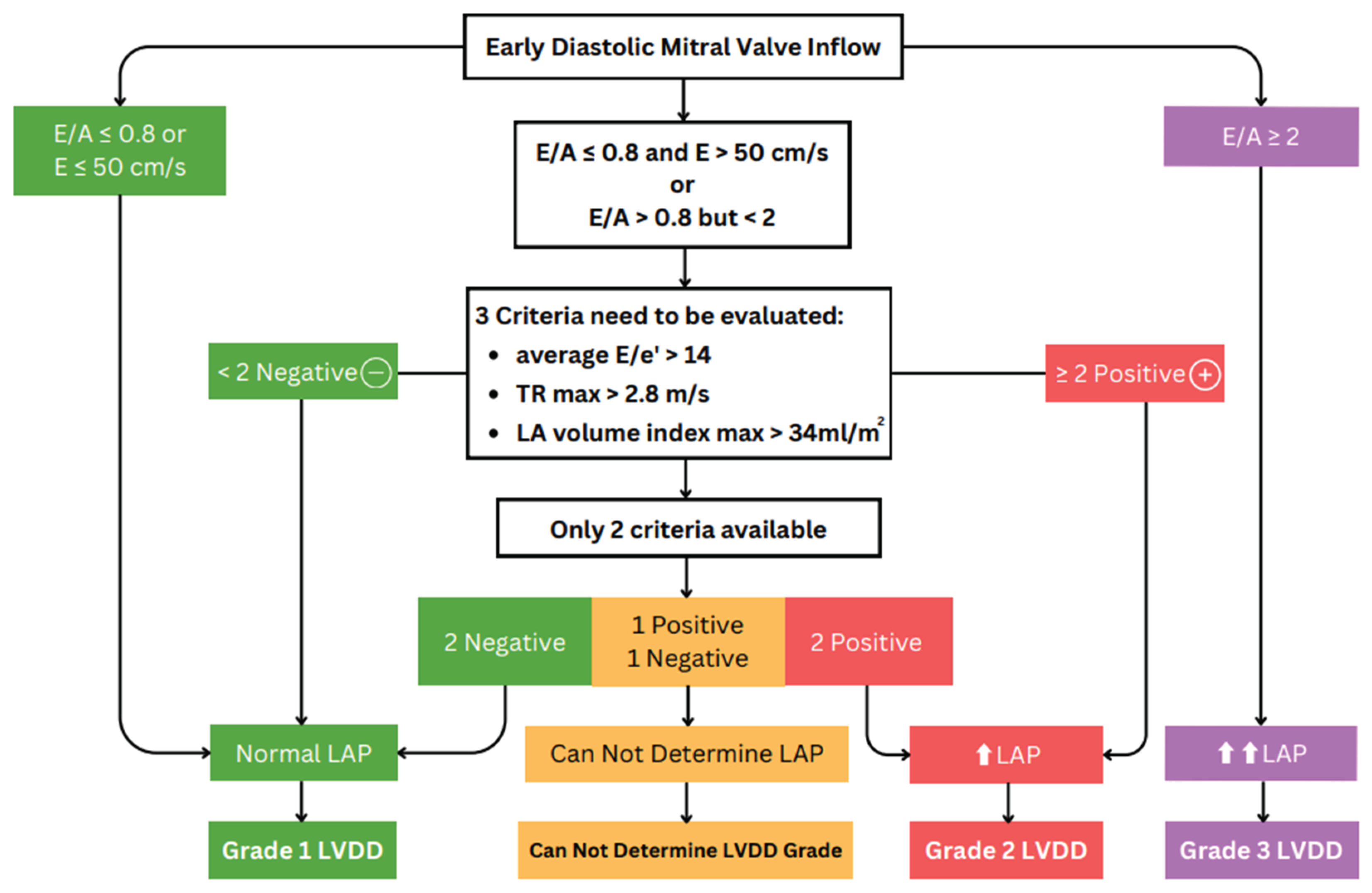

Table 1.
Hemodynamic variables characterizing LV diastolic function in different diastolic phases and echocardiography parameters.
Table 1.
Hemodynamic variables characterizing LV diastolic function in different diastolic phases and echocardiography parameters.
| In Figure 2 | Cardiac phase | Factors affecting | Parameter |
|---|---|---|---|
| 1 | Isovolumetric relaxation (LAP < LVP) |
Active relaxation (primary) induced by SR uptake of Ca2+ |
|
| 2 | Early rapid filling (LAP > LVP) |
|
|
| 3 | Inflow deceleration (LAP < LVP) | LV stiffness | E wave deceleration time |
| 4 | Diastasis (LAP = LVP) |
|
|
| 5 | LA contraction (LAP > LVP) | LAP | A wave peak |
| 6 | LA relaxation | LA stiffness | E/e′/LAS |
LAP: left atrial pressure; LVP: left ventricular pressure; SR: strain rate; Ca2+: calcium; LVRT: left ventricular (isovolumetric) relaxation time; IVR: (left ventricular) isovolumetric relaxation; SRIVR: (left ventricular) strain rate during isovolumetric relaxation; SRE: (left ventricular) strain rate during early filling; E wave: mitral peak velocity of early filling; A wave: mitral peak velocity of late filling; e’ wave: mitral annular velocity of early filling by tissue Doppler; LV: left ventricular; LA: left atrial; LAS: left atrial strain.
Table 2.
Comparative analysis of normal diastolic function and diastolic dysfunction in stress echocardiography.
Table 2.
Comparative analysis of normal diastolic function and diastolic dysfunction in stress echocardiography.
| E Wave (early filling) |
e' Wave (relaxation rate) |
E/e’ Ratio (filling pressure) |
|
|---|---|---|---|
| Normal diastolic function | ↑ | ↑ | N |
| Diastolic dysfunction | ↑ | Slight↑/N | ↑↑ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



