
Submitted:
15 March 2024
Posted:
18 March 2024
You are already at the latest version
Abstract
Objectives: To study sociodemographic and clinical variables including psychiatric comorbidities in patients with irritable bowel syndrome.
Methods: A total of 150 patients were screened to select 100 patients for the study who were attending a medical gastroenterology clinic in a tertiary care centre in north India. Diagnosis of IBS was made using Rome IV criteria and severity of symptoms were assessed by the Irritable Bowel Syndrome Symptom Severity Scale (IBS-SSS). Clinical evaluation was done for screening of psychiatric comorbidities and diagnosis was made as per DSM 5. Depression, Anxiety and Stress Scale - 21 Items (DASS-21) and Somatic Symptom Scale–8 (SSS-8) were used to assess depression, anxiety, stress and somatic symptoms.
Result: The mean age of cases was 35.6 years and majority were i.e., 38.0% in 18-29 years. Males were 62.0% and females were 38.0%. 61.0% of the cases were diagnosed with Moderate IBS. Evaluation on DASS-21 revealed 53.0% were in moderate category in depression, 43.0% were having moderate anxiety and 36.0% were having moderate stress. 48% cases were in high category in somatic symptom scale. Psychiatric comorbidities were present in 29.0% of cases. Depressive disorders were most common psychiatric comorbidity.
Conclusion: Patients with IBS presenting to tertiary care centre in Northern India were mostly young males living in semi-urban area, belonging to hindu region, married and had a nuclear family. Patients with IBS commonly have associated psychiatric disorders; anxiety disorders and depression are most common.
Keywords:
Irritable bowel Syndrome
; Psychiatric comorbidities
; Somatic symptoms
; Anxiety
; Stress
1. Introduction
Irritable bowel Syndrome (IBS) is a functional gastrointestinal disorder characterised by abdominal pain, diarrhoea, constipation or a combination of both diarrhoea and constipation, mucus discharge, and changes in stool form [1]. These symptoms are common in the general population, affecting people of all ages and genders [2]. Diagnosis is made by Rome IV criteria published in May 2016, serving as the current gold standard, due to the absence of well-validated biomarkers. This set of criteria prioritized the impact of cross-cultural differences, the intestinal milieu, and the role of nutrition over previous iterations [3]. The Bristol stool form scale is used to classify abnormal bowel movements [4].
The disorder amounts to a major burden on healthcare and constitutes nearly half of the referrals to gastroenterology clinics. The frequency and type of IBS symptoms vary depending on geographical location because of variations in bowel habits, cultural beliefs, gut contamination, dietary practices, and psychosocial reasons [5].
The onset of IBS is more likely to occur after an infection (IBS-postinfectious), or a stressful life event, but varies little with age. The most common theory is that IBS is a disorder of the interaction between the brain and the gastrointestinal (GI) tract. For at least some individuals, abnormalities in the gut flora occur, and it has been theorized that these abnormalities result in inflammation and altered bowel function [6].
The prevalence of IBS varies by geographic region and population, as well as the diagnostic criteria used [7]. IBS affects 10–20% of the population according to cross-sectional studies done in Europe and North America. The global prevalence of IBS was reported to be 11.2% using Manning, Rome I, Rome II, or Rome III criteria [7,8]. In various Asian nations, the prevalence of irritable bowel syndrome (IBS) ranges from 4% to 20%. IBS prevalence in India is estimated at 4.0%-7.9% which continues to be on the rise [5].
About 50–90% of IBS patients also have associated psychiatric ailments, most common anxiety disorders and depression. Studies have revealed that patients seeking medical consultation have a higher number and severity of symptoms and are more likely to be depressed and anxious [9].
The health-related quality of life in patients with this functional GI disorder is impaired. Patients with serious conditions often have a higher rate of reduced quality of life [10]. Studies have also shown that patients avoid or are unable to participate in a variety of activities due to IBS symptoms like work, leisure, and social activities [10,11].
Most of the literature on IBS and associated psychiatric diseases comes from western studies. Since major socio-cultural differences exist in the manifestation of these psychosomatic disorders, generalizing the outcomes of research from western studies will be unrevealing. Only a few studies have been done in this area so far in India. Our aim, therefore, was to strengthen the limited knowledge regarding the sociodemographic and clinical correlates including psychiatric disorders with IBS in our region.
2. Material and Methodology
The present study was conducted at a tertiary care centre in north India. It was a cross-sectional study conducted for a length of about one and a half years from June 2021 to September 2022. The study was approved by the institutional ethical committee with Ref. code II PGTSC-IIA/P10. Subjects for the study were selected from outpatients visiting the medical gastroenterology department. 158 patients were screened and 100 were enrolled in the study. All the cases were interviewed for sociodemographic parameters like gender, age, marital status, employment, and education level. The assessments were conducted by a trainee psychiatric resident under supervision of a consultant medical gastroenterologist and a consultant psychiatrist. All the patients provided written informed consent for inclusion in the study.
Subjects aged 18 or above who satisfied the diagnostic criteria for IBS (Rome IV criteria) and had no medical comorbidities or organic pathology (abnormal upper and lower GI endoscopy) and who were not receiving any psychotropic medications were included in the study.
Cases were diagnosed using Rome IV criteria, a self-reported integrated questionnaire for diagnosis of all functional gastrointestinal disorders in adults [12]. The severity of symptoms was assessed using Irritable Bowel Syndrome Symptom Severity Scale (IBS-SSS). It is a 5-question based survey that asks the severity of abdominal pain, frequency of abdominal pain, severity of abdominal distention, dissatisfaction with bowel habits, and interference with quality of life over the past 10 days. Subjects respond to each question on a 100-point visual analogue scale [13]. Subjects were screened for any psychiatric comorbidity while interviewing and the diagnosis was confirmed by DSM-5[14]. Depression, Anxiety and Stress Scale - 21 Items (DASS-21) was applied to assess for depressive, anxiety and stress symptoms. It is a set of three self-report scales designed to measure the negative emotional states of depression, anxiety and stress [15]. Somatic Symptom Scale–8 (SSS-8) was used to assess for somatic symptoms. It is a brief self-report questionnaire used to assess somatic symptom burden. The scale assesses common somatic symptoms and is a shortened version of the PHQ-15 questionnaire scale [16]. Sheehan Disability Scale (SDS) was used to check functional impairment. It is a brief, 3-item self-report tool that assesses functional impairment in work/school, social life, and family life [17]. Social and Occupational Functioning Assessment Scale (SOFAS) was applied for social and occupational functioning assessment. It focuses exclusively on the individual's level of social and occupational functioning and is not directly influenced by the overall severity of the individual's psychological symptoms [18]. Figure 1 describes the describes our research process, criteria for enrollment and the subjects eventually included in the study.
3. Statistical Analysis
Data were entered into excel sheet designed by Microsoft Corporation, Redmond, WA, USA. Continuous variables were analyzed in the form of mean and standard deviation. Categorical variables were summed up as percentages. Fisher’s exact test was used to analyze the relationship between categorical variables. Pearson correlation was used to analyze the correlation between different variables. Statistical analysis was done using SPSS version 25 [19].
4. Result
A total of 158 subjects were screened and 100 subjects were enrolled in study. The most common reason for the exclusion was that they were already receiving psychotropic medications (n=33), followed by subjects with medical comorbidities like diabetes/ chronic kidney disease (n=11), history of gastrointestinal surgery (n=7), age >60 years (n=5) and subjects with abnormal upper or lower gastrointestinal endoscopy (n=2) were other reasons. Sociodemographic profile of subjects is provided in Table 1. The mean years of age of onset of our IBS patients was 30.46 years (SD = ±9.05) and mean duration of illness was 5.07 years (SD = ±5.89).
As per IBS symptom severity scale, most of the subjects were in moderate category (61.0%) and the mean score was 280.20 (SD = ±57.21). Depression, anxiety and stress symptoms were assessed using DASS-2. In depression 53.0% were in moderate category with mean score of 16.16±5.31, 43.0% were having moderate anxiety with mean score of 13.80 ±4.76. In stress 36.0% were having moderate stress with mean score of 18.53±6.91. Somatic symptoms were evaluated according to somatic symptom scale-8. 12% cases were in high category score followed by 35.0% in medium and 28.0% in low with mean score of 11.50±3.05. Functional impairment in the sample was assessed as per Sheehan disability scale. 30% of subjects had impairment in work/school with a mean score of 4.73±1.70. 38% of subjects had impairment in social life with a mean score of 4.87±1.65, while 51 % had impairment in family life/ home responsibility with a mean score of 5.61±1.59. Social and occupational functioning in the sample as per SOFAS Score was analysed. 31% had some difficulty in social, occupational, or school functioning while 3% had superior functioning.
Psychiatric comorbidities present in study are listed in Table 2. In our study, psychiatric disorders were seen in 29% of patients. Major psychiatric disorder seen was depressive disorders and anxiety disorders. Obsessive-compulsive disorder, conversion disorder with mixed symptoms, somatic symptom disorder, and substance use disorder were another disorder present.
Pearson correlation was applied to analyze the association between IBS severity score and clinical variables. IBS-SSS was significantly associated and positively corelated with age of onset (r = 0.209, p = 0.037), DASS 21 (depression) (r = 0.545, p = <0.001), DASS 21 (Anxiety) (r = 0.212, p = <0.001), Somatic symptoms scale (r = 0.458, p = <0.001), SDS (r = 0.643, p = <0.001) and negatively corelated with SOFAS (r = -0.690, p = <0.001).
5. Discussion
The present study is a cross-sectional observational study carried out in Northern India. It was conducted with aim to study sociodemographic and clinical variables including psychiatric comorbidities in patients with irritable bowel syndrome presenting to medical gastroenterology OPD of a tertiary care hospital. The diagnosis was confirmed by ROME IV criteria. The exclusion criteria screened out patients having comorbid medical illness including diabetes and chronic kidney disease as these might alter gastrointestinal functioning. Subjects with pre-existing gastrointestinal disorders other than functional gastrointestinal syndromes, subjects with a history of gastrointestinal surgery or abnormal upper and lower gastrointestinal endoscopy were excluded to minimise chances of any organicity. Subjects already receiving psychotropic medications were also excluded as it might affect the severity of IBS and can affect depressive, anxiety, stress, somatic symptoms and impairment and social and occupational functioning.
The study group comprised 100 patients out of which 38% were aged between 18 and 30 years. Mean age of the cases was 35.66±11.30 years. Hence, clinical population of IBS was in middle age as in our study. In our study males were in 62.0% and females were 38.0%. These findings were supported by a multicentric study done by Khanna et al., who reported in their study that mean age of the study population was 38.55 years, and majority of patients were men 68%. In all, 40% of patients were in the age group of 31-45 years [20]. A multi-centric study done by Ghosal et al., reported mean age of sample as 39.4 years and male preponderance of 68% [5].
Although western studies[21] have reported higher rates of IBS in women, Asian findings have higher rates of IBS in males, which could be due to easy and better access to health care services, cultural factors favouring men in a male dominant society. The reason for altered rates are unidentified and could be an area for future research.
In the present study 45.0% of the cases were living in semi-urban area followed by 34.0% in urban area. The observations from community studies in South Asia (India, Bangladesh and Malaysia) appear indicates that IBS is more common in urban as compared to rural populations [1]. An urban lifestyle is reported to be associated with greater psychological stress, and other causative risk factors like dietary factors and sedentary lifestyle and thus may be associated with a higher prevalence of IBS compared to rural living.
There were 71.0% patients who were married & 29.0% were unmarried. Most were living in nuclear family i.e., 72.0%. On the context of education level 51.0% were graduate & above 13.0% were completed 12th standard, 12.0% were illiterate. Employment status as per Modified Kuppuswamy Scale-2017 was documented which revealed 25.0% of the cases were unemployed whereas 24.0% were housewife & Clerk, Shop owner, farmer. In context of income present study observed 46.0% were having no income and 31.0% were earning greater than Rs.25000. Family income was more than Rs.25000 in 61.0 %. Khanna et al., in their study reported a large proportion of enrolled patients (46.0%) were graduates or postgraduates [20].
In the present study 46.0% of the cases had onset of illness in age group 18-29 years followed by 33.0% in 30-39 years of age, 40.0% of the cases had duration of years between 1-3 years while 25.0% had illness greater than 6 years. Long term naturalistic follow study, which imply chronicity of symptoms, contradict the evidence of lower prevalence of IBS in older age groups, which suggests that symptoms resolve over time [6].
In current study IBS severity was measured using IBS-SSS. Most of the patients i.e., 62% were in moderate category while 32% were in severe category. The patients often take treatment when their symptoms are reasonably serious. As the study was conducted in a tertiary care centre, hence higher severity in subjects. The mean score was 280.20. A study done by Lackner et al., reported mean total IBS-SSS score of 284 for the sample was in high-moderate level of symptom severity in IBS-SSS, which is similar to this study [22].
Using DASS-21 depressive, anxiety and stress symptoms were assessed. In depression, 53.0% were in moderate category followed by 20.0% in mild, 43.0% were having moderate anxiety & 33.0% had severe anxiety. In stress 36% were having moderate stress while 28.0% were having mild stress. Alaqeel et al., reported that DASS-21 results in their study revealed that 39.0%, 7.0%, and 25.9% of students had normal, mild, and moderate anxiety, respectively [23]. A prior study in Japan by Okami et al., reported that individuals with IBS had higher scores on the Hospital Anxiety and Depression Scale (HADS) than control subjects in medical students [24].
In the present study SSS-8 was used to evaluate the somatic symptoms. 48% cases were in high category score followed by 31% in medium and 12% in low. A reason could be that people from developing countries report more somatic symptoms in comparison with developed countries [25]. In addition, over one-half of all patients with IBS report depression or anxiety and these patients experience more severe somatic symptoms [26]. It is important that IBS patients are evaluated for other somatic symptoms like pain, fatigue, shortness of breath apart from GI symptoms as they have somatic stress in other parts and should be taken into consideration.
This study evaluated functional impairment and social and occupational functioning using SDS and SOFAS. 30% of subjects had impairment in work/school, 38% of subjects had impairment in social life, while 51 % had impairment in family life/ home responsibility. 31% had some difficulty in social, occupational or school functioning. We were not able to find much data regarding functional impairment and social and occupational functioning, although a study reported a high degree of impairment due to IBS, with 76% of the sample reporting some degree of IBS-related impairment in at least five different domains of daily life [27]. Moreover, other studies have reported significantly poorer quality of life and more absenteeism in work in patients with IBS which corroborates with our findings of impairment in work, social life and family responsibilities and difficulty in social, occupational or school functioning [11].
In the present study comorbidity was evaluated by clinical interview and diagnosis was made by DSM-5. Diagnosable psychiatric comorbidity was present in 29% of sample, although psychiatric symptoms were present in significant number of subjects. The frequency and severity of the symptomatology of IBS in patients with anxiety and mood disorders have been well documented [9,28]. Most of the patients had depressive disorder (14%). Association of comorbidity with SSS-8 Score was significant. Most of the patients were having high points in both with and without comorbidity i.e., 62.1% & 42.3% respectively. Cho et al., stated stress, worry, or sadness are often associated with IBS, in an integrated biopsychosocial approach, psychiatric co-morbidity contributes to the aetiology of irritable bowel syndrome (IBS) [29].
The most frequent psychiatric disorder in clinical IBS patients is depression, followed by anxiety and somatization disorders which is similar to our study findings [28]. Another reason for these findings could be that the cases selected in our study were selected from a tertiary care centre where more severe forms of the illness are seen, and it has been studied that the severity of functional GI disorders increases the likelihood of having co-morbid psychiatric disorders.
In the present study correlation of IBS-SSS with clinical variables was evaluated. IBS-SSS was significantly correlated with all the scoring scales such as DASS-21, SSS- 8, SDS and SOFAS. A study done by Cho et al., reported that among the patients with severe symptoms, anxiety and depression were related to the abdominal pain or discomfort score, although the association with anxiety was not significant [29].
Our study had a few limitations. We selected our sample from clinical population visiting medical gastroenterology OPD, hence it could not be generalizable to other population. Further, patients were not categorized in IBS subtypes which could have effect on disease severity and associated psychiatric comorbidities. No fresh investigations were done at baseline due to lack of feasibility, although patients had investigations from past. Another limitation of our study was that we didn’t study dietary habits of our sample which could influence IBS presentation.
6. Conclusions
In conclusion, Patients with IBS presenting to tertiary care centre in Northern India were mostly young males living in semi-urban area, belonging to Hindu region, married and had a nuclear family. Most of the patients were graduates, unemployed with no earnings. They have found to be having psychiatric comorbidities. Psychiatric symptomatology and duration of illness are strongly associated with severity of illness.
Institutional Review Board Statement
The study was approved by the Institutional Ethical Committee with Ref. code II PGTSC-IIA/P10.
Conflicts of Interest
There are no conflicts of interest.
References
- Rahman, M.M.; Mahadeva, S.; Ghoshal, U.C. Epidemiological and clinical perspectives on irritable bowel syndrome in India, Bangladesh and Malaysia: A review. World J Gastroenterol 2017, 23, 6788–6801. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, K.K.; Nigam, P.; Rastogi, C.K.; Kumar, A.; Gupta, A.K. Clinical profile of irritable bowel syndrome. Indian J Gastroenterol 1985, 4, 15–16. [Google Scholar] [PubMed]
- Bai, T.; Xia, J.; Jiang, Y.; Cao, H.; Zhao, Y.; Zhang, L.; et al. Comparison of the Rome IV and Rome III criteria for IBS diagnosis: A cross-sectional survey: Comparison of Rome IV & III IBS criteria. Journal of Gastroenterology and Hepatology 2017, 32, 1018–1025. [Google Scholar]
- Blake, M.R.; Raker, J.M.; Whelan, K. Validity and reliability of the Bristol Stool Form Scale in healthy adults and patients with diarrhoea-predominant irritable bowel syndrome. Aliment Pharmacol Ther 2016, 44, 693–703. [Google Scholar] [CrossRef]
- Ghoshal, U.C.; Abraham, P.; Bhatt, C.; Choudhuri, G.; Bhatia, S.J.; Shenoy, K.T.; et al. Epidemiological and clinical profile of irritable bowel syndrome in India: report of the Indian Society of Gastroenterology Task Force. Indian J Gastroenterol 2008, 27, 22–28. [Google Scholar]
- Gwee, K.A.; Ghoshal, U.C.; Chen, M. Irritable bowel syndrome in Asia: Pathogenesis, natural history, epidemiology, and management: Irritable bowel syndrome in Asia. Journal of Gastroenterology and Hepatology 2018, 33, 99–110. [Google Scholar] [CrossRef]
- Mahadeva, S.; Goh, K.L. Epidemiology of functional dyspepsia: a global perspective. World J Gastroenterol 2006, 12, 2661–2666. [Google Scholar] [CrossRef] [PubMed]
- Canavan, C.; West, J.; Card, T. The epidemiology of irritable bowel syndrome. Clin Epidemiol 2014, 6, 71–80. [Google Scholar]
- Banerjee, A.; Sarkhel, S.; Sarkar, R.; Dhali, G.K. Anxiety and depression in irritable bowel syndrome. Indian journal of psychological medicine 2017, 39, 741–745. [Google Scholar] [CrossRef]
- Cho, H.S.; Park, J.M.; Lim, C.H.; Cho, Y.K.; Lee, I.S.; Kim, S.W.; et al. Anxiety, Depression and Quality of Life in Patients with Irritable Bowel Syndrome. Gut Liver 2011, 5, 29–36. [Google Scholar] [CrossRef]
- Buono, J.L.; Carson, R.T.; Flores, N.M. Health-related quality of life, work productivity, and indirect costs among patients with irritable bowel syndrome with diarrhea. Health Qual Life Outcomes 2017, 15, 35. [Google Scholar] [CrossRef] [PubMed]
- Schmulson, M.J.; Drossman, D.A. What Is New in Rome IV. J Neurogastroenterol Motil 2017, 23, 151–163. [Google Scholar] [CrossRef] [PubMed]
- Francis, C.Y.; Morris, J.; Whorwell, P.J. The irritable bowel severity scoring system: a simple method of monitoring irritable bowel syndrome and its progress. Alimentary pharmacology & therapeutics 1997, 11, 395–402. [Google Scholar]
- Diagnostic and Statistical Manual of Mental Disorders [Internet]. DSM Library. 9780. Available online: https://dsm.psychiatryonline.org/doi/book/10.1176/appi.books.9780890425596 (accessed on 20 July 2022).
- Lovibond, S.H.; Lovibond, P.F. Manual for the depression anxiety stress scales; Psychology Foundation of Australia, 1996. [Google Scholar]
- Gierk, B.; Kohlmann, S.; Kroenke, K.; Spangenberg, L.; Zenger, M.; Brähler, E.; et al. The somatic symptom scale–8 (SSS-8): a brief measure of somatic symptom burden. JAMA internal medicine 2014, 174, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, D.V.; Harnett-Sheehan, K.; Raj, B. The measurement of disability. International clinical psychopharmacology 1996. [Google Scholar] [CrossRef] [PubMed]
- Association, A.P. Social and occupational functioning Assessment Scale (SOFAS). Diagnostic and statistical manual of mental disorders 2000, 817–818. [Google Scholar]
- Spss I. IBM SPSS Statistics for Windows, version 25; IBM SPSS Corp: Armonk, NY, 2017. [Google Scholar]
- Khanna, S.; Mukewar, S.V.; Jagtap, S.; Khaliq, A.; Nijhawan, S.; Patil, M.; et al. Sociodemographic and Clinical Profiles of Patients with Irritable Bowel Syndrome: A Cross-sectional, Multi-centric, Epidemiological Study in India. The Journal of the Association of Physicians of India 2021, 69, 11–12. [Google Scholar]
- Lovell, R.M.; Ford, A.C. Global Prevalence of and Risk Factors for Irritable Bowel Syndrome: A Meta-analysis. Clinical Gastroenterology and Hepatology 2012, 10, 712–721.e4. [Google Scholar] [CrossRef]
- Lackner, J.M.; Ma, C.; Keefer, L.; Brenner, D.M.; Gudleski, G.D.; Satchidanand, N.; et al. Type, Rather Than Number, of Mental and Physical Comorbidities Increases the Severity of Symptoms in Patients With Irritable Bowel Syndrome. Clinical Gastroenterology and Hepatology 2013, 11, 1147–1157. [Google Scholar] [CrossRef]
- Alaqeel, M.K.; Alowaimer, N.A.; Alonezan, A.F.; Almegbel, N.Y.; Alaujan, F.Y. Prevalence of Irritable Bowel Syndrome and its Association with Anxiety among Medical Students at King Saud bin Abdulaziz University for Health Sciences in Riyadh. Pak J Med Sci 2017, 33, 33–36. [Google Scholar] [CrossRef]
- Okami, Y.; Kato, T.; Nin, G.; Harada, K.; Aoi, W.; Wada, S.; et al. Lifestyle and psychological factors related to irritable bowel syndrome in nursing and medical school students. J Gastroenterol 2011, 46, 1403–1410. [Google Scholar] [CrossRef]
- Singh, P.; Agnihotri, A.; Pathak, M.K.; Shirazi, A.; Tiwari, R.P.; Sreenivas, V.; et al. Psychiatric, Somatic and Other Functional Gastrointestinal Disorders in Patients With Irritable Bowel Syndrome at a Tertiary Care Center. J Neurogastroenterol Motil 2012, 18, 324–331. [Google Scholar] [CrossRef]
- Crane, C.; Martin, M.; Johnston, D.; Goodwin, G.M. Does Depression Influence Symptom Severity in Irritable Bowel Syndrome? Case Study of a Patient With Irritable Bowel Syndrome and Bipolar Disorder. Psychosomatic Medicine 2003, 65, 919–923. [Google Scholar] [CrossRef]
- Mönnikes, H. Quality of Life in Patients With Irritable Bowel Syndrome. Journal of Clinical Gastroenterology 2011, 45, S98–101. [Google Scholar] [CrossRef]
- Fadgyas-Stanculete, M.; Buga, A.M.; Popa-Wagner, A.; Dumitrascu, D.L. The relationship between irritable bowel syndrome and psychiatric disorders: from molecular changes to clinical manifestations. J Mol Psychiatr 2014, 2, 4. [Google Scholar] [CrossRef]
- Cho, H.S.; Park, J.M.; Lim, C.H.; Cho, Y.K.; Lee, I.S.; Kim, S.W.; et al. Anxiety, Depression and Quality of Life in Patients with Irritable Bowel Syndrome. Gut and Liver 2011, 5, 29–36. [Google Scholar] [CrossRef]
Figure 1.
Research Flowchart. (IBS- Irritable Bowel Syndrome; DASS-21- Depression, Anxiety, Stress Scale-21; SSS-8- Somatic Symptom Scale-8; SDS- Sheehan Disability Scale; SOFAS- Social and Occupational Functioning Scale.).
Figure 1.
Research Flowchart. (IBS- Irritable Bowel Syndrome; DASS-21- Depression, Anxiety, Stress Scale-21; SSS-8- Somatic Symptom Scale-8; SDS- Sheehan Disability Scale; SOFAS- Social and Occupational Functioning Scale.).
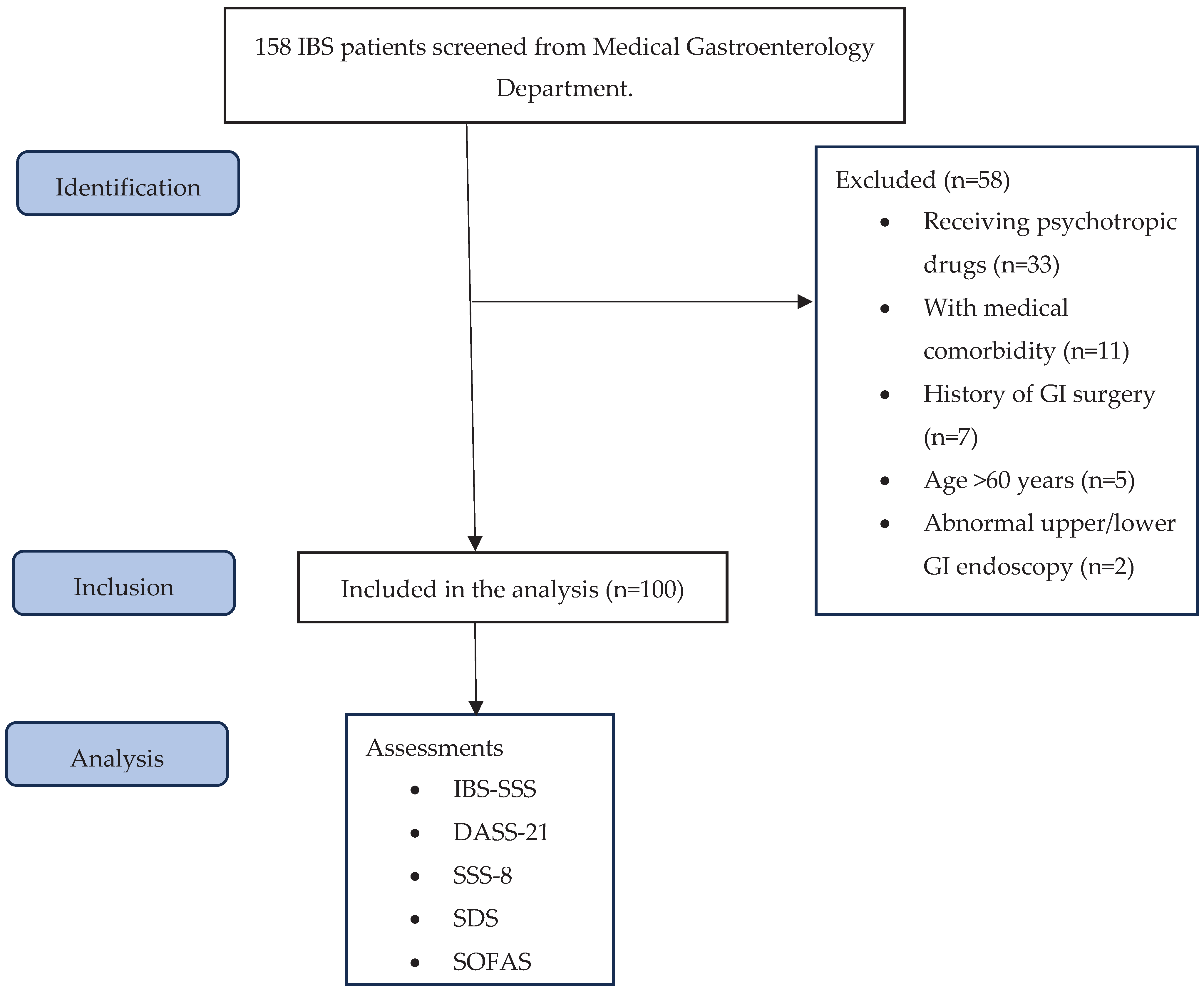

Table 1.
Sociodemographic profile of IBS patients.
| Socio-demographic variables | Number of cases (%) |
|---|---|
| Age (in years) | |
| 18-30 | 38 (38.0) |
| 31-40 | 23 (23.0) |
| 41-50 | 26 (26.0) |
| 51-60 | 13 (13.0) |
| Mean (in years) ± S.D. = 35.66±11.30 (Range= 18 -58 years) | |
| Gender | |
| Male | 62 (62.0) |
| Female | 38 (38.0) |
| Domicile | |
| Rural | 21 (21.0) |
| Semi-urban | 45 (45.0) |
| Urban | 34 (34.0) |
| Religion | |
| Hindu | 83 (83.0) |
| Muslim | 17 (17.0) |
| Marital Status | |
| Married | 71 (71.0) |
| Unmarried | 29 (29.0) |
| Family type | |
| Nuclear | 72 (72.0) |
| Joint | 28 (28.0) |
| Education | |
| Illiterate | 12 (12.0) |
| 5th or below | 7 (7.0) |
| 6th to 8th | 4 (4.0) |
| 9th & 10th | 13 (13.0) |
| 11th & 12th | 13 (13.0) |
| Graduate & above | 51 (51.0) |
| Employment Status | |
| Unemployed* | 25 (25.0) |
| Housewife | 24 (24.0) |
| Unskilled/Semiskilled | 16 (16.0) |
| Skilled | 4 (4.0) |
| Clerk, Shop owner, Farmer | 24 (24.0) |
| Professional | 7 (7.0) |
| Patient’s income in rupees (per month) | |
| Nil | 49 (49.0) |
| <10000 | 7 (7.0) |
| 10000-25000 | 13 (13.0) |
| >25000 | 31 (31.0) |
*Students are included in the unemployed category.
Table 2.
Psychiatric comorbidities in patients with IBS.
| Psychiatric Comorbidities | Number of cases (%) |
|---|---|
| Absent | 71 (71.0%) |
| Present* | 29 (29.0%) |
| Depressive disorders | |
|
7 (7.0%) |
|
4 (4.0%) |
|
3 (3.0%) |
| Anxiety disorders | |
|
2 (2.0%) |
|
7 (7.0%) |
| Obsessive compulsive disorder | 1 (1.0%) |
| Adjustment disorder | 2 (2.0%) |
| Conversion disorder with mixed symptoms | 1 (1.0%) |
| Somatic Symptom Disorder | 1 (1.0%) |
| Substance use disorder | |
|
3 (3.0%) |
|
1 (1.0%) |
*Not mutually exclusive.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



