Submitted:
26 February 2024
Posted:
12 March 2024
You are already at the latest version
Abstract
Introduction: Carcinoid heart disease is a rare cause of right-sided valvular dysfunction, an important complication in patients with carcinoid syndrome. Objectives: We aim to present our own experience regarding early myocardial dysfunction in patients with carcinoid syndrome. Methods: 64 patients (35-90 year old, 62,5% female, 37,5% male patients) with carcinoid syndrome were evaluated be-tween October 2017 and June 2021. All patients underwent two-dimensional echocardiography with additional tissue Doppler and speckle-tracking techniques. For all patients there were measured urinary level of 5- hydroxyindolacetic acid, serotonin and NT-proBNP values. Results: The following echocardiographic features: global longitudinal strain of both ventricles, mean systolic velocity of the left ventricle, systolic velocity of the free wall of right ventricle, correlated with high values of specific biomarkers: serotonin, and urinary 5-hydroxyindolacetic acid, and also with the presence of hepatic metastases and poorly differentiated tumors. Discussion: In this study we identified several patients with early myocardial dysfunction due to carcinoid syndrome, representing a predictive model of poor prognosis, requiring further investigations. Conclusion: Echocardiographic assessment based on the measurement of systolic velocities, as well as the global longitudinal strain of both ventricles, together with specific biomarkers may contribute to better recognition of carcinoid heart disease in clinical practice, but this needs validation through further studies enrolling larger number of patients.
Keywords:
carcinoid heart disease
; global longitudinal strain
; systolic velocities
; NT-proBNP
; serotonin
; 5- hydroxyindolacetic acid
1. Introduction
Neuroendocrine neoplasms can beget carcinoid tumors and carcinoid heart disease, with the latter considered a prominent etiology in the field of intrinsic right heart valve disorders, leading to right heart failure and considerable morbidity and mortality. So clinicians need to pay heed to its appropriate diagnosis and prevention [1].
Neuroendocrine neoplasia mostly originate from the gastrointestinal tract. They are reported in 2.5-5 persons per 100 000 people [1]. The secretion of vasoactive substances by these tumors is responsible for carcinoid syndrome [2]. Carcinoid tumors usually develop gradually and are likely to show few or no symptoms until they are bulky enough to be symptomatic or have metastasized, mostly to the liver, followed by the skeletal and pulmonary systems [1,3].
Carcinoid syndrome (CS) may be associated with cardiac involvement due to the direct action of vasoactive substances. [2] Carcinoid syndrome can occur in up to 60% of cases during the course of the disease, but carcinoid heart disease (CaHD) can be the first manifestation in approximately 20% of patients [3,4].
As cardiac manifestations are associated with a poor long-term medical prospect and mortality [3,5], the detection of cardiac disease in its early stages has a significant value. Cardiac surgeries such as valve replacement, if performed at the optimal time, significantly contribute to the treatment of symptomatic patients and the improvement of their quality of life [6].
In the primary evaluation of patients with CaHD, the modality of choice is 2D echocardiography in that it can reveal thickness and retraction in the valve leaflets in a semi-open position with reduced mobility, annular constriction, thickness and fusion in the subvalvular apparatus, and finally regurgitation and /or stenosis of various degrees [1,10,11,12,13]. Severe tricuspid regurgitation results in right ventricle (RV) volume overload and RV/right atrium (RA) dilatation [8,14,15].
The accuracy of echocardiography as a screening tool can be enhanced through the use of sensitive and specific biochemical markers associated with the presence and severity of cardiac involvement. Among these useful biomarkers is N-terminal pro-brain natriuretic peptide (NT-proBNP), which is significantly raised in patients with CaHD. This elevation is correlated with disease progression, symptomatic status, and overall survival. An evaluation of NT-proBNP with a cutoff level of 260 pg/mL is recommended as a screening biomarker with 92% sensitivity, 91% specificity, 98% negative predictive value, and 71% positive predictive value [12,13].
The plasma or urinary level of 5-hydroxyindoleacetic acid (5-HIAA), which is a metabolite of serotonin, is higher in cardiac involvement, with an elevated level of this metabolite in excess of 300 mmol/24 h being associated with a two- to threefold increased risk of the progression of CaHD [1,9].
Thus, the recognition, diagnosis, and treatment of neuroendocrine tumours and their associated syndromes are mandatory. Rapid diagnosis utilizing serum studies, CT scans, and echocardiography can help expedite the diagnosis and treatment of such rare conditions, and assist in the avoidance of complications due to the effects of circulating vasoactive substances. Despite its relatively well-recognized clinical symptoms, carcinoid syndrome and its associated heart disease still remains an underdiagnosed entity and a challenging condition to manage and treat, oftens requiring the input of several subspecialties to treat the condition appropriately [12,15].
We aim to present our own experience regarding early myocardial dysfunction in patients with carcinoid syndrome by using predictive neuroendocrine biomarkers and two-dimensional echocardiographic parameters.
2. Materials and Methods
2.1. Study Population
Patients were enrolled regarding both inclusion and exclusion criteria. Study approval was provided by the Ethics Committee of “Carol Davila” University of Medicine and Pharmacy, Bucharest. All procedures were in agreement with Helsinki declaration concerning ethical principles for medical research involving human subjects.
We used the World Health Organization (WHO) classification scheme that places neuroendocrine tumors (NETs) into three main categories, which emphasize the tumor grade rather than the anatomical origin: well-differentiated neuroendocrine tumours, further subdivided into tumors with benign and those with uncertain behavior, well-differentiated (low grade) neuroendocrine carcinomas with low-grade malignant behavior, poorly differentiated (high grade) neuroendocrine carcinomas, which are the large cell neuroendocrine and small cell carcinomas.
After patient’s consent by completing an informed consent, a clinical evaluation and necessary investigation of each patient was carried out.
Diagnosis of carcinoid disease was based on review of outside records, pathology specimens, thoracoabdominal computed tomography, and increased levels of 5-hydroxyindole acetic acid (5-HIAA) in a 24-hour urine sample.
The exclusion criteria were: age under 18 years old, ischemic heart disease, history of percutaneous coronary intervention, arrythmias, congenital heart disease, valvulopathies such as aortic and mitral stenosis, aortic and mitral regurgitation either rheumatic or degenerative, hypertrophic and restrictive cardiomiopathy, chronic kidney disease, peripheral artery disease, arterial hypertension, diabetes mellitus, Cushing syndrome, acromegaly, pregnancy and lactation, poor transthoracic windows.
To ascertain that the patient had no exclusion criteria, the following prerequisites were performed: clinical evaluation, measurement of blood pressure, 12- leads electrocardiogram, serum creatinine and urea, serum ionogram and echocardiogram.
We studied 64 patients with proven carcinoid syndrome and 60 sex- and age-matched healthy subjects.
64 patients: 40 women and 24 men with median age= 63 years (range: 35-90 year old, 62% female with median age= 69.5 year old and 38% male patients with median age= 51 year old) with carcinoid syndrome were consequently evaluated between October 2017 and June 2021.
The control group (64 participants) comprised adults with no history of cardiovascular disease and normal physical examination, electrocardiography (ECG), and resting echocardiography. The exclusion criteria were the same in both patient and control groups.
2.2. Echocardiography
2D and Doppler echocardiography was performed with standard techniques and equipment. All studies were performed by experienced sonographers and reviewed by staff cardiologists with advanced training in echocardiography.
All patients underwent comprehensive two-dimensional echocardiography with additional tissue Doppler (TDI) and speckle-tracking techniques, using commercially available echocardiography machines (General Electric Vivid-T8, EchoPac). All patients took the test several times in follow up, minimum 6 months apart, with a total number of explorations of 256 between October 2017 and June 2021 (160 explorations in women, 96 explorations in men).
Valve regurgitation and stenosis severity were assessed according to European Society of Cardiology guidelines.
The parameters also included: systolic velocities of the left ventricle expressed as cm/s (septal and lateral wall, mean value- S), global longitudinal strain (GLS) using 12 –segment model (adequate two-dimensional images in apical four, three and two chambers), expressed as percentages, systolic velocity of the free wall of the right ventricle- S, expressed as cm/s, global longitudinal strain of the right ventricle (GLS), expressed as percentages.
The diagnosis of carcinoid heart disease was based on presence of characteristic thickening, reduced mobility and/or retraction of tricuspid and pulmonary valves leading to dysfunction of the involved valves.
2.3. Biomarkers
All patients had multiple 24-hour urine samples quantitatively analyzed for 5-HIAA (expressed as mg/24h) and serotonin (expressed as ng/ml) by using enzyme-linked immunosorbent assay (ELISA) technique. For this study, mean values were recorded. We also measured NT-proBNP plasma values (expressed as pg/ml) every six months for each patient. Blood samples were collected into syringes pre-loaded with EDTA. They were immediately centrifuged for 15 min at 4000 rpms to separate serum (2.5–3 mL of serum/patient). Serum was stored at - 80 C before being analyzed for the measurement of specific biomarkers (NT-proBNP).
Enzyme-linked immunosorbent assay (ELISA) is a labeled immunoassay that is considered the gold standard of immunoassays. This immunological test is very sensitive and is used to detect and quantify substances, including antibodies, antigens, proteins, glycoproteins, and hormones. The detection of these products is accomplished by complexing antibodies and antigens to produce a measurable result. An antibody is a type of protein produced by an individual’s immune system. This protein type has specific regions that bind to antigens. An antigen is a protein that can come from some foreign source and, when bound to an antibody, induces a cascade of events through the body’s immune system. This interaction is utilized in ELISA testing and allows for identifying specific protein antibodies and antigens, with only small amounts of a test sample.
There are four main general steps to completing an ELISA immunoassay. These steps are:
- Coating (with either antigen or antibody)
- Blocking (typically with the addition of bovine serum albumin [BSA])
- Detection
- Final read
Detection is carried out by the addition of a substrate that can generate a color. There are many substrates available for use in ELISA detection. However, the most commonly used horseradish peroxidase (HRP) and alkaline phosphatase (ALP). The substrate for HRP is hydrogen peroxide and results in a blue color change. ALP measures the yellow color of nitrophenol after room temperature incubation periods of 15 to 30 minutes and usually uses P-Nitrophenyl-phosphate (pNPP) as its substrate.
Between each of the above four steps is a “wash” of the plate using a buffer, such as phosphate-buffered saline (PBS) and a non-ionic detergent, to remove unbound material. The wells are washed two or more times during each wash step, depending on the specific protocol being followed.
2.4. Statistical Analysis
Furthermore, a statistical analysis was performed using IBM SPSS Statistics version 29. The normal distribution of the continuous variables was tested by the Shapiro-Wilk test; normally distributes continuous variables were reported as mean± SD and compared for statistical significance using independent sample t-tests. Categorical variables were expressed as percentages and compared using Pearson ‘s Chi-square test. Correlation between continuous variables was performed using Pearson’s or Spearman’s correlation coefficient, as appropriate . A p-value<0.05 was considered statistically significant.
3. Results
3.1. General Data about Patients
We evaluated 64 patients with neuroendocrine tumours (NETs): 24 men (37.5%) and 40 women (62.5%). The average age was 56.98 year-old (SD 12.939). For male patients the average alge was 51.5 year-old (SD 12.445), while for female patients 60.28 year-old (SD 12.226). Population biology is revealed into Figure 1.
3.2. Comparison between Patients’ and Control-Subjects’ Echocardiographic Parameters
We also studied 64 sex- and age-matched healthy subjects in order to compare echocardiographic parameters regarding tissue Doppler velocities (TDI) and global longitudinal strain of both left and right ventricles. The feasibility of TDI was better than for all the other methods, particularly for the study of the right ventricle where systolic velocities could be recorded in all patients and healthy subjects. All absolute systolic velocities were lower in patients compared with healthy subjects—Table 1, where S LV = mean systolic velocity of the left ventricle, S RV= mean systolic velocity of the free wall of the right ventricle, GLS LV= global longitudinal strain of the left ventricle, GLS RV= global longitudinal strain of the right ventricle.
Concerning the healthy subjects, there were similar changes between men and women regarding longitudinal and diastolic functions of both ventricles, significant after 50 years, as it is generally established.
3.3. Correlations between Tumoral Grading, Cardiac Biomarkers and Echocardiographic Parameters
Among patients, we observed highly statistic correlations between NT-proBNP plasma values and poorly differentiated carcinomas, and also, between global longitudinal strain measured for both left (GLS LV) and right ventricle (GLS RV) and poorly differentiated carcinoma (p<0.001)- Figure 2, Table 2 (Bine diferentiat= well differentiated benign tumors, Moderat diferentiat= low potentially malignant well differentiated carcinoma, Slab diferentiat= malignant poorly differentiated carcinoma).
3.4. Correlation between Global Longitudinal Strain of the Right Ventricle and Hepatic Secondary Determinations
Moreover, we identified another highly statistic correlation between right ventricle global longitudinal strain (GLS RV) and the presence of hepatic secondary determinations (p<0.001)—Table 3.
3.5. Multiple Correlations between Cardiac and Neuroendocrine Biomarkers
In our study, there were also multiple correlations between NT-proBNP, serotonin and 5-hydroxyindole acetic acid levels; however, only NT-proBNP and serotonin plasma values were highly correlated (p<0.001)—Table 4.
It can be said that poorly differentiated tumoral grade and the presence of hepatic secondary determinations induce poor outcome through early subclinical systolic dysfunction, thus increasing cardiovascular risk in these patients.
There were no statistic associations among various grades of tricuspid regurgitation regarding global longitudinal strain or systolic velocities.
Patients with poorly differentiated carcinoma had the highest levels of NT-proBNP and serotonin, strongly associated with development of carcinoid heart disease (p<0.001). Those with hepatic secondary determinations were prone to reduction of global longitudinal strain of the right ventricle (p<0.001).
Regarding the gender-specific differences related to carcinoid syndrome, there was no significant difference between men and women concerning the development of early myocardial dysfunction. There was no association between patients’gender, age, weight or body-mass index and grade of severity among tested patients.
4. Discussion
The carcinoid syndrome is a rare cause of acquired valvular heart disease. Although the typical echocardiographic features of carcinoid heart disease are well recognized, this study provides new information about unusual manifestations of the disease as well as the role of neuroendocrine biomarkers.
Owing to the rarity of the disease, few studies have investigated the prognosis of patients with carcinoid heart disease. To our knowledge, the present study is the first from Romania to assess early myocardial dysfunction by two-dimensional transthoracic echocardiography guided by predictive biomarkers in patients with carcinoid heart disease.
Our results are concordant to other trials and guidelines proposed by European Society of Cardiology regarding Cardio-Oncology field and can be used as a basis for future studies on carcinoid patients.
Tissue Doppler echocardiography, since its introduction more than 2 decades ago, had revolutionized echocardiography. In the quest to directly quantify myocardial function, increase sensitivity to detect early subtle myocardial dysfunction and improve ease of use, tissue Doppler echocardiography has evolved from pulsed wave tissue Doppler, to color-coded tissue Doppler and to 2-dimensional (2D) speckle tracking, and from myocardial velocity to strain/strain rate imaging. Over the years, numerous studies have demonstrated the value of tissue Doppler echocardiography in the diagnosis and risk stratification of a wide range of cardiac diseases. However, each generational change in tissue Doppler echocardiography involves technological software advancements that are not directly comparable to previous generations [16,17].
Carcinoid heart disease is the leading source of mortality and morbidity in subjects with carcinoid syndrome. The outcomes without treatment are poor. Fortunately, the prognosis of carcinoid heart disease subjects has significantly improved over the last decades, which is mainly associated with the progress in cardiac imaging modalities, as well as with cardiac valve surgery [18].
Previous studies have shown echocardiographic evidence of myocardial dysfunction in CS patients.
4.1. Carcinoid Syndrome and Myocardial Fibrosis
In contrast, the present study shows that myocardial dysfunction in patients with an early stage of CS was detected by TDI not conventional parameters. We designed this study to test the hypothesis that early CS patients might have myocardial dysfunction. We excluded hypertensive patients to estimate the true impact of early stage CS on myocardial function, which was the most important aspect of the present study. Peak longitudinal myocardial velocities derived from pulsed wave TDI are useful indicators of global or regional LV dysfunction. Strain and strain rate are other tools that can reflect myocardial function. We applied tissue Doppler myocardial velocity, strain, and strain rate together to detect subtle changes in global myocardial function [19].
It is common knowledge that even a mild degree of diastolic dysfunction may be associated with poor prognosis on long-term follow-up. The use of TDI might detect early systolic and diastolic myocardial dysfunction in CS patients, even if they do not have overt diabetes mellitus, arterial hypertension, or any other structural abnormalities [19].
Tissue Doppler imaging (TDI) is a relatively new echocardiographic technique that uses Doppler principles to measure the velocity of myocardial motion. We describe the principles behind and the clinical utility of TDI [20].
Doppler echocardiography relies on detection of the shift in frequency of ultrasound signals reflected from moving objects. With this principle, conventional Doppler techniques assess the velocity of blood flow by measuring high-frequency, low-amplitude signals from small, fast-moving blood cells. In TDI, the same Doppler principles are used to quantify the higher-amplitude, lower-velocity signals of myocardial tissue motion [21].
There are important limitations to TD interrogation. As with all Doppler techniques, TDI measures only the vector of motion that is parallel to the direction of the ultrasound beam. In addition, TDI measures absolute tissue velocity and is unable to discriminate passive motion (related to translation or tethering) from active motion (fiber shortening or lengthening). The emerging technology of Doppler strain imaging provides a means to differentiate true contractility from passive myocardial motion by looking at relative changes in tissue velocity [20,21].
TDI can be performed in pulsed-wave and color modes. Pulsed-wave TDI is used to measure peak myocardial velocities and is particularly well suited to the measurement of long-axis ventricular motion because the longitudinally oriented endocardial fibers are most parallel to the ultrasound beam in the apical views. Because the apex remains relatively stationary throughout the cardiac cycle, mitral annular motion is a good surrogate measure of overall longitudinal left ventricular (LV) contraction and relaxation [21].
To measure longitudinal myocardial velocities, the sample volume is placed in the. Pulsed-wave TDI has high temporal resolution but does not permit simultaneous analysis of multiple myocardial segments [21].
With color TDI, a color-coded representation of myocardial velocities is superimposed on gray-scale 2-dimensional or M-mode images to indicate the direction and velocity of myocardial motion. Color TDI mode has the advantage of increased spatial resolution and the ability to evaluate multiple structures and segments in a single view [20].
4.2. Carcinoid Syndrome and Myocardial Deformation
In the fields of cardiology and medical imaging, speckle tracking echocardiography (STE) is a technique that analyzes the motion of tissues in the heart by using the naturally occurring speckle pattern in the myocardium or blood when imaged by ultrasound. This novel method of documentation of myocardial motion represents a noninvasive method of definition of vectors and velocity. When compared to other technologies seeking noninvasive definition of ischemia, speckle tracking seems a valuable endeavor. This speckle pattern is a mixture of interference patterns and natural acoustic reflections. These reflections are also described as speckles or markers. The pattern being random, each region of the myocardium has a unique speckle pattern (also called patterns, features, or fingerprints) that allows the region to be traced from one frame to the next, and this speckle pattern is relatively stable, at least from one frame to the next. In post processing this can be tracked consecutively frame to frame and ultimately resolved into angle-independent two-dimensional and three-dimensional strain-based sequences. These sequences provide both quantitative and qualitative information regarding tissue deformation and motion [22,23].
Different commercial and non commercial operators then use different approaches to derive motion and deformation parameters. The motion of a single kernel can be resolved into displacement curves, and the distance between two kernels into strain (deformation). Strain rate will then be time derivative of strain. In some commercial applications, the acoustic markers are tracked more individually, calculating the velocity from the motion and the sampling interval (inverse of frame rate) generating a velocity field. Unlike tissue Doppler, this velocity field in not limited to the beam direction. Strain rate and strain are then calculated from the velocities. Speckle tracking has been shown to be comparable to tissue Doppler derived strain, and has been validated against magnetic resonance [24].
4.3. Limitations
There are several limitations in our study. Firstly, the size of this study to assess the relationship of each factor with myocardial dysfunction was relatively small, a single-center study with a rather limited number of patients, especially men in both groups. Secondly, it is difficult to explain the exact pathophysiologic mechanisms of early myocardial dysfunction.
Thirdly, although all subjects in our study did not have any signs or symptoms of angina, and had normal findings on electrocardiogram and on 2-D echocardiography, we could not completely exclude asymptomatic coronary artery disease.
4.4. Clinical Implications
These results indicate that patients with CS, high-grade tumour, hepatic secondary determinations, may have myocardial dysfunction apparent by tissue Doppler imaging, even if they appear to have normal findings on two-dimensional and conventional Doppler evaluation.These echocardiographic parameters can correlate with specific biomarkers, being of particularly clinical interest in future studies.
Higher the biomarkers, more likely is it to develop myocardial fibrosis and ventricular systolic dysfunction; this finding might represent another criterion for indicating multidisciplinary approach, more frequent echocardiographic assessment in order to refer patients to cardiovascular surgeon before severe dilation and irreversible right ventricular dysfunction occurs.
This might be of particularly clinical interest in carcinoid syndrome with aggressive outcome.
5. Conclusion
Despite the fact that carcinoid syndrome is an uncommon cause of valvular heart disease, however, cardiac involvement occurs frequently in patients with this syndrome, adversely affecting prognosis. Echocardiographic assessment of early myocardial dysfunction based on the measurement of systolic velocities, as well as the global longitudinal strain of both ventricles, together with specific biomarkers may contribute to better recognition of carcinoid heart disease in clinical practice, but this needs validation through further studies.
Author Contributions
Conceptualization, I.N. and C. P.; methodology, I.N., I.B., S.G., I.B. and C.P.; formal analysis, I.N., investigation, I.N., I.B., S.G., I.B. and C.P.; resources, I.N., I.B., S.G., I.B. and C.P.; visualization, I.N., I.B., S.G., I.B. and C.P; writing-original draft preparation, I.N., writing-review and editing, C.P. All authors have read and agreed to be published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinky and approved by the C.I.Parhon National Institute of Endocrinology Ethics Committee.
Informed Consent Statement
Informed consent was obtained from all patients involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Riedel, M.; Jou, C.J.; Lai, S.; Lux, R.L.; Moreno, A.P.; Spitzer, K.W.; Christians, E.; Tristani-Firouzi, M.; Benjamin, I.J. Functional and Pharmacological Analysis of Cardiomyocytes Differentiated from Human Peripheral Blood Mononuclear-Derived Pluripotent Stem Cells. Stem Cell Rep. 2014, 3, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Liu J, Backx PH. Patch-clamp technique in ESC-derived cardiomyocytes. Methods Mol Biol 2014; 1181: 203–214.
- Farre C, Fertig N. New strategies in ion channel screening for drug discovery: are there ways to improve its productivity? Expert Opin Drug Discov 2014; 9: 1103–1107.
- Poulin, H.; Bruhova, I.; Timour, Q.; Theriault, O.; Beaulieu, J.-M.; Frassati, D.; Chahine, M. Fluoxetine Blocks Nav1.5 Channels via a Mechanism Similar to That of Class 1 Antiarrhythmics. Mol. Pharmacol. 2014, 86, 378–389. [Google Scholar] [CrossRef] [PubMed]
- Dobson, R.; Burgess, M.; Pritchard, D.; Cuthbertson, D. The clinical presentation and management of carcinoid heart disease. Int. J. Cardiol. 2014, 173, 29–32. [Google Scholar] [CrossRef] [PubMed]
- Engelsman, A.F.; van Duijvendijk, P.; Groenemeijer, B.E.; van der Zaag, E.; Spronk, P.E.; Katinakis, A. Tricuspid Valve Regurgitation as a Presenting Symptom of Metastasized Carcinoid Tumor. Case Rep. Gastroenterol. 2012, 6, 643–649. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, M.A.; Taleb, M.; Kakroo, M.A.; Tinkel, J. Carcinoid Heart Disease with Right to Left Shunt across a Patent Foramen Ovale: A Case Report and Review of Literature. Echocardiography 2014, 32, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Dashwood A, Rahman A, Pavicic M. Carcinoid heart disease. Eur Heart J 2015; 36: 2326.
- Bradette, S.; Papas, K.; Pressacco, J. Imaging Features of Carcinoid Heart Disease. Can. Assoc. Radiol. J. 2014, 65, 214–217. [Google Scholar] [CrossRef] [PubMed]
- Patel, C.; Mathur, M.; Escarcega, R.O.; Bove, A.A. Carcinoid heart disease: Current understanding and future directions. Am. Hear. J. 2014, 167, 789–795. [Google Scholar] [CrossRef] [PubMed]
- Simona Grozinsky-Glasberg ABG, Gross DJ. Carcinoid heart disease: from pathophysiology to treatment – ‘something in the way it moves’. Neuroendocrinology 2015; 101: 263–273.
- Catharina M, Korse BGT, de Groot CA, Bakker RH, Bonfrer JMG. Chromogranin-A and N-terminal pro-brain natriuretic peptide: an excellent pair of biomarkers for diagnostics in patients with neuroendocrine tumor. J Clin Oncol 2009; 27: 4293–4299.
- Lichtenauer, M.; Jirak, P.; Wernly, B.; Paar, V.; Rohm, I.; Jung, C.; Schernthaner, C.; Kraus, J.; Motloch, L.J.; Yilmaz, A.; et al. A comparative analysis of novel cardiovascular biomarkers in patients with chronic heart failure. Eur. J. Intern. Med. 2017, 44, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Schernthaner, C.; Lichtenauer, M.; Wernly, B.; Paar, V.; Pistulli, R.; Rohm, I.; Jung, C.; Figulla, H.; Yilmaz, A.; Cadamuro, J.; et al. Multibiomarker analysis in patients with acute myocardial infarction. Eur. J. Clin. Investig. 2017, 47, 638–648. [Google Scholar] [CrossRef] [PubMed]
- Jirak, P.; Fejzic, D.; Paar, V.; Wernly, B.; Pistulli, R.; Rohm, I.; Jung, C.; Hoppe, U.C.; Schulze, P.C.; Lichtenauer, M.; et al. Influences of Ivabradine treatment on serum levels of cardiac biomarkers sST2, GDF-15, suPAR and H-FABP in patients with chronic heart failure. Acta Pharmacol. Sin. 2017, 39, 1189–1196. [Google Scholar] [CrossRef] [PubMed]
- Zurita, A.J.; Khajavi, M.; Wu, H.-K.; Tye, L.; Huang, X.; Kulke, M.H.; Lenz, H.-J.; Meropol, N.J.; Carley, W.; E DePrimo, S.; et al. Circulating cytokines and monocyte subpopulations as biomarkers of outcome and biological activity in sunitinib-treated patients with advanced neuroendocrine tumours. Br. J. Cancer 2015, 112, 1199–1205. [Google Scholar] [CrossRef] [PubMed]
- Jirak, P.; Fejzic, D.; Paar, V.; Wernly, B.; Pistulli, R.; Rohm, I.; Jung, C.; Hoppe, U.C.; Schulze, P.C.; Lichtenauer, M.; et al. Influences of Ivabradine treatment on serum levels of cardiac biomarkers sST2, GDF-15, suPAR and H-FABP in patients with chronic heart failure. Acta Pharmacol. Sin. 2017, 39, 1189–1196. [Google Scholar] [CrossRef] [PubMed]
- Rachel P, Riechelmann AAP, Rego JFM, Costa FP. Refractory carcinoid syndrome: a review of treatment options. Therapeutic Advances in Medical Oncology 2017; 9: 127–137.
- Castillo, J.G.; Filsoufi, F.; Adams, D.H.; Raikhelkar, J.; Zaku, B.; Fischer, G.W. Management of patients undergoing multivalvular surgery for carcinoid heart disease: the role of the anaesthetist. Br. J. Anaesth. 2008, 101, 618–626. [Google Scholar] [CrossRef] [PubMed]
- Javier G, Castillo M, Federico Milla MD, David H, Adams MD. Surgical management of carcinoid heart valve disease. Semin Thoracic Surg 2012; 24: 254–260.
- Modlin, I.M.; Sandor, A. An analysis of 8305 cases of carcinoid tumors. Cancer 2000, 79, 813–829. [Google Scholar] [CrossRef]
- M. Kulke, R. Mayer.Carcinoid tumors.N Engl J Med, 340 (1999), pp. 858-868 | Medline.
- J. Moller, P. Pellikka, A. Bernheim, et al. Prognosis of carcinoid heart disease: analysis of 200 cases over two decades.Circulation, 112 (2005), pp. 3320-3327 | Medline.
- S. Bhattacharyya, J. Davar, G. Dreyfus, et al. Carcinoid heart disease. Circulation,116(2007),pp.2860-2865 Medline.
Figure 1.
Populational Biology of Patients with Carcinoid Syndrome.
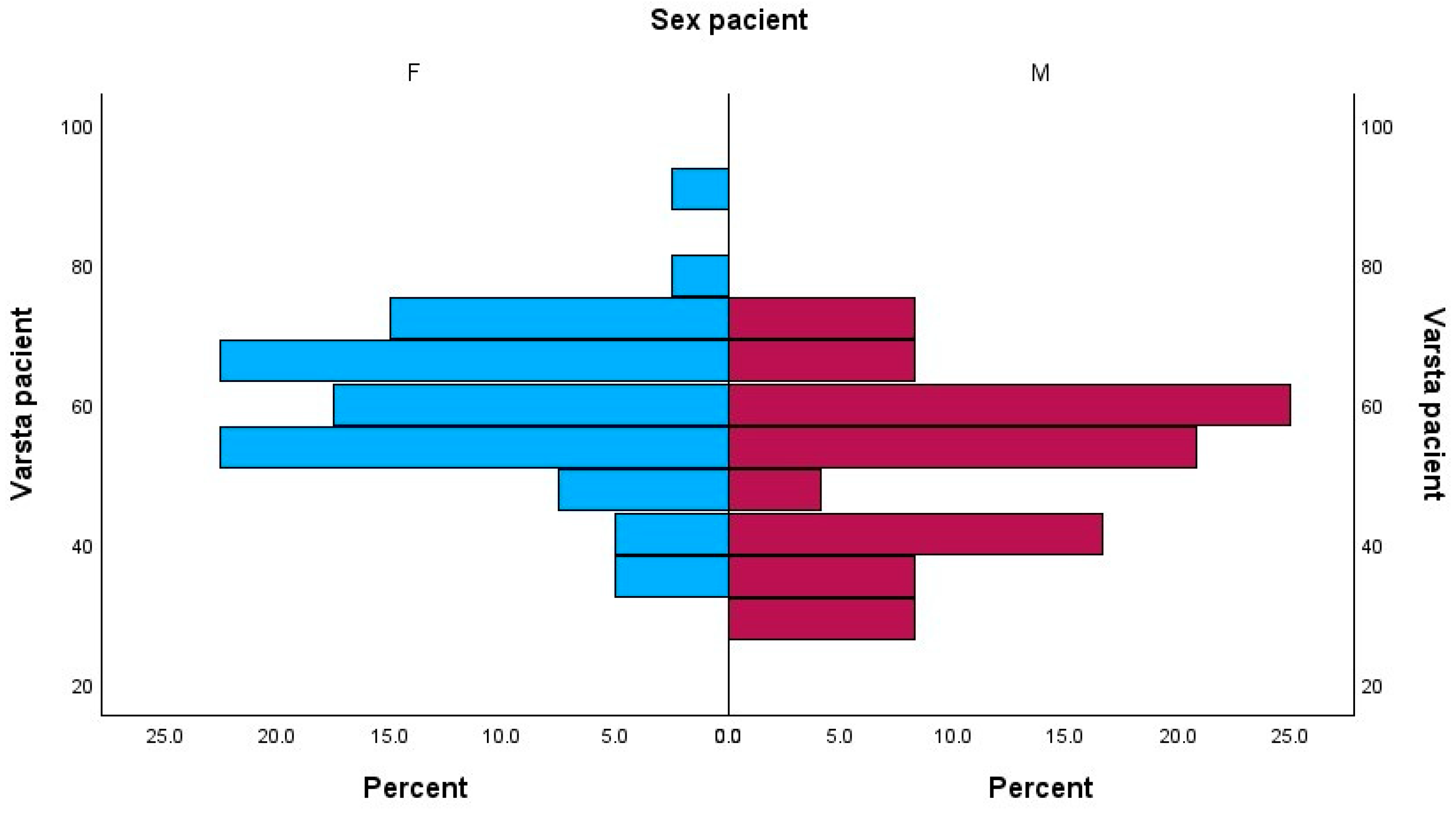
Figure 2.
Correlations between NT-proBNP plasma values and tumoral grading.
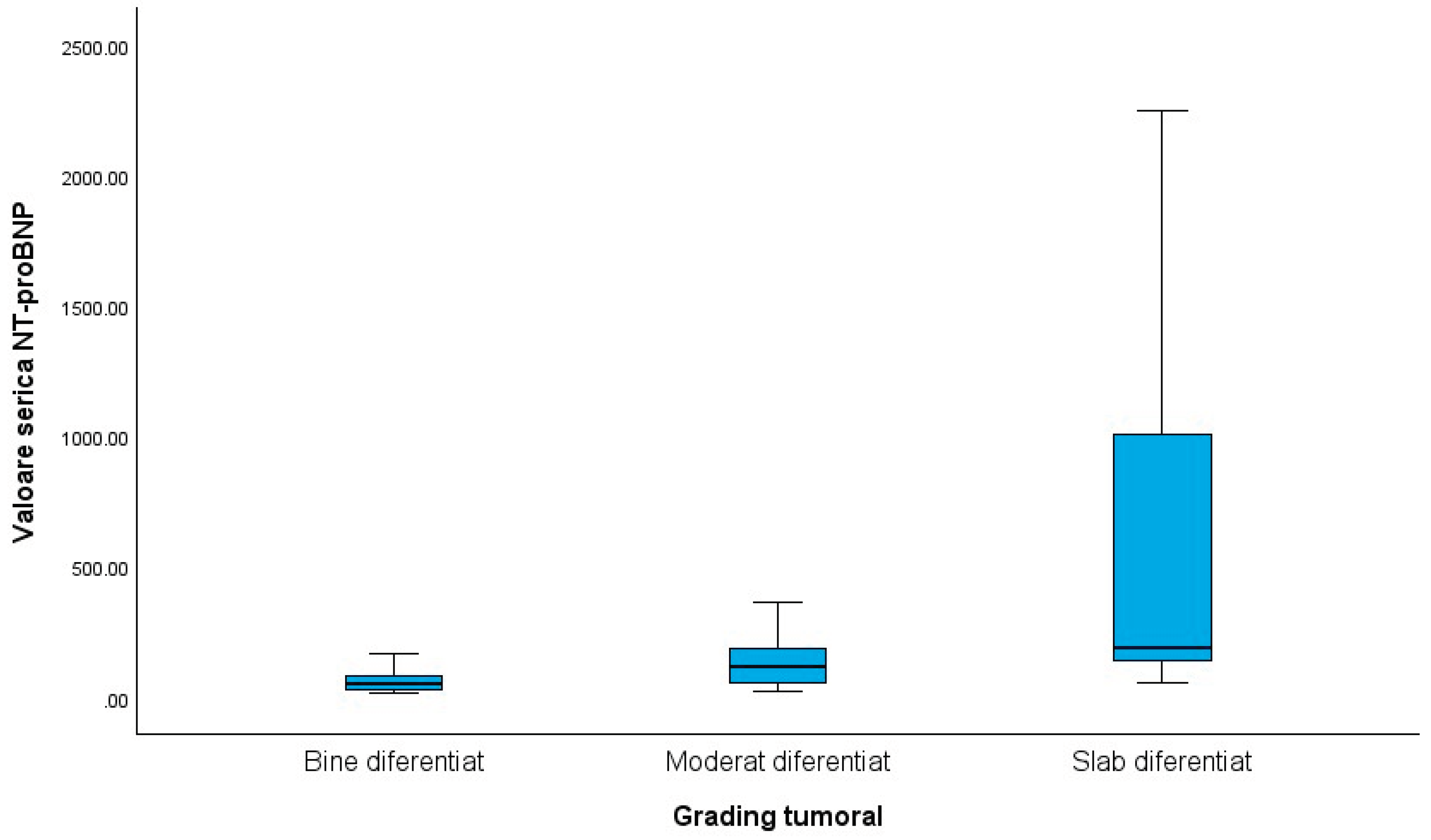

Table 1.
Mean values of echocardiographic parameters in patients and control subjects.
| Parameters | Mean ±SD |
|---|---|
| S LV Patient | 9.9688± 2.36689 |
| S LV Control | 13.3672± 1.02447 |
| S RV Patient | 14.06± 4.525 |
| S RV control | 20.77± 1.688 |
| GLS LV Patient | 18.6219± 1.17750 |
| GLS LV Control | 22.2759± 1.28785 |
| GLS RV Patient | 18.4844± 1.35602 |
| GLS RV Control | 22.3767± 1.23431 |
Table 2.
Pearson Correlations between global longitudinal strain and tumoral grading.
| Pearson Correlation | Tumoral grading | GLS LV | GLS RV |
|---|---|---|---|
| Tumoral grading | 1 | -.725** | -.671** |
| p<0.001 | p<0.001 | ||
| GLS LV | -.725** | 1 | .990** |
| p<0.001 | p<0.001 | ||
| GLS RV | -.671** | .990** | 1 |
| p<0.001 | p<0.001 | ||
** Correlation is significant at the 0.01 level (2-tailed).
Table 3.
Pearson correlation between global longitudinal strain of the right ventricle and hepatic secondary determinations.
Table 3.
Pearson correlation between global longitudinal strain of the right ventricle and hepatic secondary determinations.
| Pearson Correlation | Hepatic secondary determinations | GLS RV |
| Hepatic secondary determinations | 1 | -.476 |
| p<0.001 | ||
| GLS RV | -.476 | 1 |
| p<0.001 | ||
Table 4.
Multiple correlations between cardiac and neuroendocrine biomarkers.
| Pearson Correlation | NT-proBNP | 5-HIAA | Serotonin |
| NT-proBNP | 1 | .225 | .897 |
| p= 0.037 | p<0.001 | ||
| 5-HIAA | .225 | 1 | .200 |
| p=0.037 | p= 0.057 | ||
| Serotonin | .897 | .200 | 1 |
| p<0.001 | p= 0.057 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



