
Submitted:
09 March 2024
Posted:
11 March 2024
You are already at the latest version
Abstract
Abstract: Background: epileptic encephalopathies (EE) are characterized by severe drug-resistant seizures, early-onset, and unfavorable developmental outcome. We describe a cohort of pediatric patients with EE who underwent intravenous methylprednisolone (IVMP) pulse therapy to examine its efficacy/tolerability. Methods: This is a retrospective study from 2020 to 2023. Inclusion criteria were: ≤18 years at the time of IVMP pulse therapy and at least 6 months of follow-up. Efficacy and outcome, defined as seizure reduction >50% (responder rate), were evaluated at 6 and 9 months of therapy, and 6 months after therapy suspension; quality of Life (QoL) was also assessed. Variables predicting positive post-IVMP outcomes were identified using statistical analysis. Results: Twenty-one patients were included. The responding rate was 85.7% at 6 and 9 months of therapy, and 80.9% at 6 months after therapy suspension. Genetic etiology and encephalopathy related to status epilepticus during NREM sleep (ESES) were predictive of efficacy (p=0.0475). The fourth month of therapy was the minimum time point to establish the effectiveness of the treatment. All patients showed improvements in QoL, EEG tracing and postural-motor development. No relevant adverse events were observed. Conclusions: Our study confirms the efficacy and tolerability of pulse IVMP treatment in pediatric patients with EE, especially with genetic etiology and ESES. The fourth month of therapy was the minimum time point to establish its effectiveness. QoL, EEG and postural-motor development also showed improvement.
Keywords:
Methylprednisolone
; Pulse therapy
; childhood epilepsy
; epileptic encephalopathy
Introduction
Refractory epilepsy remains a significant challenge, given that seizure activity becomes refractory in approximately a quarter of children with epilepsy [1].
Among the spectrum of childhood epilepsy presentations, epileptic encephalopathies (EE) represent an important subgroup characterized by severe and drug-resistant epileptic seizures, early onset and unfavorable developmental outcomes [2].
According to the International League Against Epilepsy, “epileptic encephalopathies” are defined as conditions wherein "the epileptic activity itself may contribute to severe cognitive and behavioral impairments above and beyond what might be expected from the underlying pathology alone (e.g. cortical malformation), and that these can worsen over time" [2,3]. In certain instances, developmental slowing may manifest prior to the onset of frequent epileptic activity on EEG; in such cases the suggested term is “developmental and epileptic encephalopathies” [2,3].
Despite new drugs with multiple targets being available on the market within the last 30 years, EE continue to exhibit a poor response to anti-seizure medications (ASMs) [4,5,6].
Consequently, there is a pressing need to complement ASMs with other therapeutic modalities in these severe epileptic conditions, including vagus nerve stimulation (VNS), ketogenic diet and corticosteroid therapy [7,8,9].
Steroid therapy has been successfully used in drug resistant epilepsy for many years [10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29], although its precise mechanism of action on brain activity remains incompletely understood [30,31,32,33,34,35,36,37,38,39,40,41].
Several steroid formulations are available, with oral prednisolone, adrenocorticotropic hormone (ACTH) and methylprednisolone being among the most commonly utilized options.
To mitigate the potential adverse events associated with long-term oral steroid and short-term intramuscular ACTH therapy [42], pulse intravenous methylprednisolone (IVMP) is frequently employed in patients with EE. Varying therapeutic strategies are reported, including different dosages (ranging from 15 to 30 mg/kg/day), frequencies (such as one pulse per week or one pulse per month), and durations (spanning from 1 to 36 months) [20,21,22,23,24,25,26,27,28,29]. Additionally, in certain cases, oral prednisone therapy followed an initial IVMP pulse [21,25].
In this study, we present findings from a single-center experience involving a cohort of pediatric patients diagnosed with epileptic encephalopathies who underwent intravenous methylprednisolone (IVMP) pulse therapy. The objectives were to assess its efficacy and tolerability, as well as to determine the minimum duration of therapy required to achieve optimal response and outcomes.
Furthermore, we conducted an analysis to assess the contribution of factors predicting favorable post-IVMP outcomes.
Materials and Methods
We retrospectively analyzed the clinical records of pediatric patients with epileptic encephalopathy, according to the ILAE classification [2], undergoing long-term IVMP at the IRCCS - Institute of Neurological Sciences of Bologna and Universitary Sant’Orsola Hospital of Bologna between 2020 and 2023.
All patients were collectively categorized as a single group of epileptic encephalopathy for study purposes, although we also conducted separate analyses by dividing this category into patients suffering from encephalopathy related to electrical status epilepticus during slow wave sleep (ESES) and those suffering from other early-onset EE.
We included patients who were under 18 years of age at the time of steroid therapy and had a minimum follow-up period of 6 months after the last infusion.
Each cycle of IVMP therapy comprised administration of intravenous methylprednisolone at a dosage of 20 mg/kg/day for three consecutive days [13]. Multiple cycles of IVMP were administered at monthly intervals, with a total treatment duration of 9 months. Following pulse administration, a gradual tapering of steroids through oral cortisone was not carried out. Additionally, patients selected for this study did not change their anti-seizure medication during IVMP treatment.
The response to therapy was evaluated based on seizures frequency. Accordingly, in post-IVMP data analysis, the responder rate was determined by a reduction in seizures of ≥ 50%. Patients with a response of less than 50% were defined as “non-responders”. Furthermore, patients were classified as “partially responders” when seizures reduction was between 50% and 75% and “good responders” when the reduction was ≥ 75 %. Seizure freedom (SF) was defined as the complete cessation of all seizures (seizure frequency = 0) at the time of follow-up.
The responder rate was assessed during the first 6 months and at 9 months of IVMP therapy. The outcome was analyzed 6 months after the completion of IVMP therapy. During the first 6 months of therapy, the month wherein results demonstrated at least a “partial response" in more than 50% of the population was considered as the minimum time to evaluate the effectiveness of the therapy in our clinical practice.
In addition to assessing the main response to IVMP therapy, which focused on seizures frequency, we also analyzed a “secondary” response, related to the QOL of patients and caregivers, EEG findings, and postural-motor development.
It is important to note that our seizure unit's clinical practice does not involve modifications to chronic antiepileptic therapy in patients undergoing IVMP treatment. However, if such modifications did occur, those patients were excluded from the study. The clinical variables examined retrospectively included: age at epilepsy onset, epilepsy duration before the IVMP pulse therapy, seizure frequency, type of epilepsy, etiology, neurological examination findings, neuropsychological evaluation results, MRI findings.
Pre-IVMP and post-IVMP seizure frequency data were retrospectively assessed by reviewing patient medical records. In our seizure unit's clinical practice, meticulous collection of clinical data, including seizure frequency and duration, is conducted monthly. However, during steroid therapy, quality of life (QOL) data were also collected monthly from the initiation until the completion of the treatment. QOL data were obtained by querying caregivers about the overall lifestyle of the patients. The results were designated as improved, unchanged, or worse, compared to the pre-IVMP implementation period. QOL parameters, including vigilance, behavioral and seizures intensity, were assessed using questionnaires at each follow-up visit. Additionally, a "caregiver QOL" parameter was included to account for potential for emotional fatigue accompanying the management of patients with EE.
EEG findings and posture-motor development were also evaluated during the course of treatment and 6 months post-IVMP therapy.
The outcome was deemed “favorable” when there was a seizure reduction of more than 50% at the last follow-up.
Database analyses were conducted in accordance with institutionally approved human subject protection protocols.
Statistical Analysis
Continuous variables were presented as mean ± standard deviation (SD), while categorical variables as absolute and relative frequencies (%).
Fisher’s exact test and Wilcoxon rank-sum tests were utilized, as appropriate, to assess the univariate association between the overall outcome and each individual variable collected, including epilepsy onset, epilepsy duration before IVMP (Timing), seizure frequency, age at of epilepsy, etiology, neurological examination findings, neuropsychological evaluation results, and MRI findings. All p-values were based on 2-sided tests, with significance set at p < 0.05.
Multiple logistic regression analysis was also performed at each outcome point. The results were presented as Odds Ratio (OR) and relative 95% Confidence Interval (95% CI). Statistical analysis was performed using the statistical package Stata SE, version 14.0.
Results
Patients
The cohort consisted of twenty-one children (12 males, 9 females). The mean age at beginning of IVMP therapy was 92.9 ± 38.3 months, with a mean age at seizure onset of 27.4 ± 25.8 months and a pre-treatment epilepsy duration of 65.5 ± 33.5 months. Among them, 13 had ESES while 8 had other early-onset EE. None of the patients discontinued therapy prematurely.
Table 1 presents the outcome data over 9 months of IVMP pulse therapy and 6 months following the therapy.
Seizure Outcome
At the conclusion of IVMP therapy (9 months), the responder rate, defined as seizure frequency reduction ≥ 50%, was 85.7%. Among these, 52.4% of patients achieved seizure freedom, 9.5% were classified as "good responders," and 23.8% were categorized as "partially responders" (Table 2).
During the initial 6 months of IVMP therapy, the fourth month emerged as the period wherein at least a “partial response” was observed in more than 50% of the population, with a responder rate of 76%, including 14.3% of seizures free patients, 19% of “good responders” and 42.7 of “partially responders”. This finding suggests that the fourth month represents the minimum time point for evaluating the effectiveness of the therapy (Table 2).
Figure 1A illustrates that 60% of patients who did not achieve a response in the fourth month of IVMP therapy demonstrated no response in the sixth and ninth months of treatment, maintaining this outcome at the last visit (6 months of follow-up). The remaining 40% of subjects who did not exhibit a response at the fourth month of IVMP therapy displayed a “partial response” at the sixth and ninth month of treatment, maintaining a favorable outcome at the last visit, albeit with a responder rate < 75%.
Figure 1B shows that all patients who were seizure-free at 4 months of IVMP therapy (14.3%) remained seizure-free until the last visit (6 months of follow-up). Additionally, Figure 1C illustrates that all patients who exhibited at least one “partial response” after 4 months of IVMP therapy showed a trend of improvement in the following months of therapy, maintaining this trend until the last visit.
The results obtained at 6 months of IVMP therapy and at the conclusion of the therapy were similar at the results obtained at 6-months of follow-up, with a favorable outcome in 80.9% patients, including 57.1% who achieved seizure freedom (Figure 1D).
The association between outcome and the variables analyzed in our study is presented in Table 1. A significative association was assessed between outcome and the variables “etiology” (p=0.0475), with a better outcome observed in genetic epilepsy compared to structural epilepsy, and “epilepsy type” (p=0.0475), with a better outcome observed in ESES compared to other early-onset EE. These associations were determined using Fisher’s exact test and Wilcoxon rank-sum tests. Multiple logistic regression analysis did not identify etiology and epilepsy type as the main predictor of response to IVMP therapy at 6-months follow-up. For etiology, the odds ratio (OR) was 5.2 with a 95% confidence interval (CI) of 0.3 – 86.9, while for epilepsy type, the OR was 0.2 with a 95% CI of 0.01 – 3.2. At the last follow-up visit, only one patient with ESES syndrome experienced a relapse (4.7%) after a partial response that had been stable from the fourth to ninth month of therapy.
QOL and Postural-Motor Outcome
At the last follow-up visit, 100% of patients experienced an improving in quality of life. Among these patients, 36.8% reported improvement after the very first month of IVMP therapy, 21% after 2 months, 5.3% after 3 months, 31.6% after four months and 5.3% after 5 months of IVMP therapy.
These results were consistent with the improvement of background activity and interictal abnormalities observed in the follow-up EEG.
No adverse events were reported, except for a slight irritability observed in 15% of cases during the days of the intravenous infusion.
Finally, an improvement in postural-motor neurological examination was observed in 76.2% of the total sample.
Discussion
Treatment strategies for epileptic encephalopathies encompass a variety of approaches, including antiseizure medications (ASMs), ketogenic diet, vagus nerve stimulation, steroids/adrenocorticotropin hormone therapy and targeted therapies [4,5,6,7,8,9].
Steroids, such as prednisolone, prednisone, ACTH, methylprednisolone, and hydrocortisone have been employed in the treatment of various seizure disorders, including epileptic spasms [43,44,45,46,47,48], epilepsy syndromes with spike-and-wave activity in sleep [13,49,50,51,52,53], Lennox-Gastaut syndrome [10,24,54,55,56], drug-resistant epilepsies [26,57,58,59,60,61], and status epilepticus [62,63].
Steroids treatment is based in the recognition of inflammatory processes in epileptogenesis, indicating a bidirectional association between seizures and the inflammatory process [64,65,66,67].
Although the precise mechanism by which steroids modulate seizure frequency remains unknown, several hypotheses have been proposed. One of the most widely accredited hypotheses involves the interaction of steroids with the γ-aminobutyric acid (GABA) receptor. This interaction results in the prolongation of the duration and frequency of the ligand-gated chloride channel opening, and thereby suppressing potential hyperexcitability [64,65,66,67].
Furthermore, it is well known that stress is a common seizure trigger in patients with epilepsy [68,69,70]. Seizure susceptibility and accelerated epileptogenesis associated with stress, especially chronic stress, are thought to be mediated by stress hormones through their proconvulsant actions [71,72,73]. Furthermore, exogenous stress hormones such as corticosterone and corticotropin-releasing hormone (CRH), have been demonstrated to exert similar proconvulsant actions as chronic stress [74]. Interestingly, basal levels of corticosterone are elevated in patients with epilepsy and are further increased following seizures, suggesting that the regulation of the hypothalamic-pituitary-adrenal (HPA) axis may be fundamentally altered in epileptic patients [75,76,77,78].
On the basis of these observations present in the literature, it is possible to speculate that pulse therapy with methylprednisolone, in addition to exploiting the anti-crisis effect linked to the anti-inflammatory action of the pulse phase, acts by reducing hyperexcitability through blocking the HPA axis during the phase between one pulse and the other. Following this rationale, which involves blocking the HPA axis, we refrain from gradually tapering off steroids via oral cortisone after pulse therapy.
Usually, corticosteroids are well-tolerated, but moderate to severe, short- and long-term adverse effects could occur [79,80,81,82,83].
In our study, no adverse events were observed, except for slight irritability reported in 15% of cases during the days of therapy.
Considering the excellent safety profile and the efficacy of pulse intravenous methylprednisolone, it is frequently employed in patients with drug-resistant epilepsy, including epileptic encephalopathies. However, different therapeutic strategies are reported, in terms of dosage (15-30 mg/kg/day), frequency (1 pulse per week/1 pulse per month) and duration (1-36 months) [20,21,22,23,24,25,26,27,28,29].
In our study we administered 20 mg/kg/day of intravenous methylprednisolone over three consecutive days [13]. Multiple cycles of IVMP were administered at monthly intervals for a total period of 9 months.
Our population analysis revealed that 61.1% of patients achieved seizure freedom, 11.1% achieved more than 75% seizure reduction, and 27.8% experienced between 50% and 75% seizure reduction. These results were comparable with studies in the literature, although previous studies have reported improvement with steroids ranging from 40% to 73% [20,21,22,23,24,25,26,27,28,29]. The wide variation in response could be due to use of different types of preparations, routes and duration of steroids administration [20,21,22,23,24,25,26,27,28,29].
At the conclusion of the IVMP therapy (9 months), the outcomes achieved were sustained until the last visit (6-months follow-up), with a favorable outcome observed in 80.9% of patients, including 70.5% who were seizure-free.
Careful analysis of our results reveals that the fourth month of IVMP therapy was the first time point during the treatment where we could outline a reliable outcome trajectory.
Indeed, all patients who were seizure-free in the fourth month remained seizure-free until the sixth month of follow-up and patients who did not achieve a response in the fourth month of IVMP therapy demonstrated either no response (60%) or a responder rate < 75% (40%) (Figure 1A,B).
Additionally, the subjects classified as “good responders” demonstrated an improving trend until achieving seizure-free at the conclusion of follow-up. Finally, the “partial responders” showed a stable or improving trend in 88.9% of subjects (Figure 1C).
Furthermore, upon analyzing our results, it emerged that the sixth month of therapy was the first time point practically showing comparable data observed at 6 months follow-up (Figure 1D).
Genetic epilepsy and ESES were found to be significant predictor of favorable clinical outcome. (Table 1). While we cannot determine if these two variables indicate severity, based on seizure frequency, it appears that “non-responders” exhibit a more severe form of epilepsy. To perform a logistic regression with these data, the two significant variables, namely etiology and epilepsy type, should be included in the regression model. However, upon conducting the regression, the association does not remain significant.
In epileptic encephalopathies, unlike other forms of epilepsy, the treatment goal encompasses not only seizure control but also the prevention of further deterioration in cortical network functioning. Unfortunately, achieving this objective in epileptic encephalopathies solely with anti-seizure medications is challenging. Indeed, the most effective therapies for obtaining these outcomes include ketogenic diet, vagus nerve stimulation, and steroid therapy [7,8,9].
In our study, 100% of patients demonstrated an improvement in QOL at the conclusion of follow-up period, with improvements observable as early as the first month of therapy (36.8%). Furthermore, the improvements in QOL were perfectly consistent with the enhancements observed in postural-motor development and in EEG features, such as background activity and interictal abnormalities, throughout treatment and at the last visit of follow-up.
As we previously suggested regarding VNS therapy, steroid therapy should also be initiated as early as possible in patients with epileptic encephalopathy to prevent the encephalopathic effects of epilepsy and potentially the establishment of aberrant circuits during a critical period of brain maturation [7].
This concept would likely result in more pronounced effects in very young children, who exhibit greater brain plasticity, and for epileptic encephalopathies, as defined by stating that "the epileptic activity itself may contribute to severe cognitive and behavioral impairments above and beyond what might be expected from the underlying pathology alone (e.g. cortical malformation), and that these can worsen over time" [2,7].
It is well known that the organization of brain networks is based on small-worldness and modularity, and this organization is altered in neurological disorders, including epilepsy [84,85,86,87,88,89,90]. It has also been reported that in epilepsy, the functional topology of brain network is altered, which increases vulnerability to seizures [89,90,91,92,93,94,95,96,97]. These observations are consistent with the theory that epilepsy is a network disorder, and seizures occur due to anomalous topology of structural and functional networks [98,99,100].
We speculate that steroid therapy induces integrated network organization, a more balanced topology, and less pathological architecture, leading to a more efficient reorganization of functional brain networks and network structure, potentially contributing to the clinical improvement observed in our population. Based on these observations, we speculate that early intervention leads to a widespread reorganization of brain networks and prevents the establishment of aberrant circuits associated with the encephalopathic state. This may influence complex processes underlying drug resistance in epileptic encephalopathies. The hypothesized large-scale reorganization of brain networks may also explain why IVMP therapy not only affects seizure frequency but also modifies quality of life. The overall clinical improvement founded in our patients with EE was accompanied by improved caregiver QOL. This outcome potentially reduces caregiver burnout and fosters a more positive patient-caregiver interaction.
Therefore, our data suggest that IVMP therapy should be considered as early as possible in the management of epileptic encephalopathies.
Our clinical findings are supported by the improved background and interictal activity observed on EEG following IVMP therapy. The improvement of EEG background activity reflects the amelioration of cerebral electrogenesis, which is an indirect indicator of maturation and/or reorganization of functional networks. This improvement, as we speculate, is favored by pulse IVMP therapy.
Without studies that carefully analyze changes on EEG background activity after IVMP therapy, we cannot exclude the possibility that EEG background features could improve through brain maturation alone, particularly in early life. Only further investigation into the direct effects of early IVMP therapy on EEG will resolve this issue.
Similarly, the postural-motor improvement found in our patients is likely the result of the improvement in the background activity found on the EEG and therefore of the maturation/reorganization of the functional networks.
Finally, our study confirms the high tolerability of IVMP therapy, with no dropouts observed.
The most significant limitation of our study is its retrospective methodology and lack of a control group. However, retrospective studies have the advantage that results are not predetermined, as all evaluations are based on existing data sources in which both exposure and outcomes are readily available.
Furthermore, the results cannot be extrapolated to data collection for a specific therapy.
Conclusions
In conclusion, our study provides confirmation of the efficacy and high tolerability of intravenous methylprednisolone pulse therapy in patients with epileptic encephalopathies.
Genetic epilepsy and ESES emerge as potential significant predictors of a favorable clinical outcome and the fourth month of therapy was the minimum time point to establish the treatment effectiveness.
Additionally, improvement of QOL, EEG features and posture-motor development were also observed.
IVMP pulse therapy should be considered promptly upon the identification of electroclinical data indicative of epileptic encephalopathy.
Author Contributions
AR was a key member of the clinical team, he had full access to all of the data in the study, took responsibility for the integrity of data and the accuracy of the data analysis, conceived and designed the study and wrote the original draft of the manuscript, SM had full access to all of the data in the study, took responsibility for the integrity of data and the accuracy of data analysis, and wrote the original draft of the manuscript, LL and RC collected the data and revised the first draft of the manuscript, FB analyzed the data, AF revised the first draft of the manuscript, AB collected some data, DMC revised the first draft of the manuscript and provided critical feedback the project. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The present study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the regional and the local institutional Ethical Committee (Study ID: EPI_NPI 343/2017/O/Oss)
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
We would like to thank Ludovica Cau for her help in data collection in this research.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Waaler, P.E.; Blom, B.H.; Skeidsvoll, H.; Mykletum, A. Prevalence, Classification, and Severity of Epilepsy in Children in Western Norway. Epilepsia 2000, 41, 802–810. [Google Scholar] [CrossRef]
- Berg, A.T.; Berkovic, S.F.; Brodie, M.J.; Buchhalter, J.; Cross, J.H.; van Emde Boas, W.; Engel, J.; French, J.; Glauser, T.A.; Mathern, G.W.; et al. Revised terminology and concepts for organization of seizures and epilepsies: Report of the ILAE Commission on Classification and Terminology, 2005-2009. Epilepsia 2010, 51, 676–685. [Google Scholar] [CrossRef]
- Russo, A. , Gobbi G. A reflection on the role of genetics in the concept of "epileptic encephalopathy", as emerged from the most recent ILEA classification of epilepsy. Ital. J. Pediatr. 2020, 46, 2. [Google Scholar]
- Chen Z, Brodie MJ, Liew D, Kwan P. Treatment outcomes in patients with newly diagnosed epilepsy treated with established and new antiepileptic drugs: a 30-year longitudinal cohort study. JAMA Neurol. 2018, 75, 279–86.
- Parisi, P.; Spalice, A.; Nicita, F.; Papetti, L.; Ursitti, F.; Verrotti, A.; Iannetti, P.; Villa, M.P. “Epileptic Encephalopathy” of Infancy and Childhood: Electro-Clinical Pictures and Recent Understandings. Curr. Neuropharmacol. 2010, 8, 409–421. [Google Scholar] [CrossRef]
- Raspall-Chaure, M.; Neville, B.G.; Scott, R.C. The medical management of the epilepsies in children: conceptual and practical considerations. Lancet Neurol. 2008, 7, 57–69. [Google Scholar] [CrossRef]
- Russo, A.; Hyslop, A.; Gentile, V.; Boni, A.; Miller, I.; Chiarello, D.; Pellino, G.; Zenesini, C.; Martinoni, M.; Lima, M.; et al. Early vagus nerve stimulator implantation as a main predictor of positive outcome in pediatric patients with epileptic encephalopathy. Epileptic Disord. 2021, 23, 563–571. [Google Scholar] [CrossRef]
- van der Louw, E.; Van Den Hurk, D.; Neal, E.; Leiendecker, B.; Fitzsimmon, G.; Dority, L.; Thompson, L.; Marchió, M.; Dudzińska, M.; Dressler, A.; et al. Ketogenic diet guidelines for infants with refractory epilepsy. Eur. J. Paediatr. Neurol. 2016, 20, 798–809. [Google Scholar] [CrossRef]
- Gupta, R.; Appleton, R. Corticosteroids in the management of the paediatric epilepsies. Arch. Dis. Child. 2005, 90, 379–384. [Google Scholar] [CrossRef]
- Verhelst, H.; Boon, P.; Buyse, G.; Ceulemans, B.; D’hooghe, M.; De Meirleir, L.; Hasaerts, D.; Jansen, A.; Lagae, L.; Meurs, A.; et al. Steroids in intractable childhood epilepsy: Clinical experience and review of the literature. Seizure 2005, 14, 412–421. [Google Scholar] [CrossRef]
- Watemberg, N.; Zelnik, N.; Shahar, E.; Lerman-Sagie, T.; Goldberg-Stern, H.; Ben-Zeev, B.; Kramer, U. Efficacy of corticosteroid therapy in treating epileptic encephalopathies and refractory epilepsies other than West syndrome. J. Pediatr. Neurol. 2006, 04, 147–153. [Google Scholar] [CrossRef]
- Kotagal, P. ; Md Current Status of Treatments for Children with Electrical Status in Slow-Wave Sleep (ESES/CSWS). Epilepsy Curr. 2017, 17, 214–216. [Google Scholar] [CrossRef]
- Munckhof, Bart van den, Alexis Arzimanoglou, Emilio Perucca, Heleen C. van Teeseling, Frans S. S. Leijten, Kees P. J. Braun, e Floor E. Jansen. «Corticosteroids versus Clobazam in 14. Epileptic Encephalopathy with ESES: A European Multicentre Randomised Controlled Clinical Trial (RESCUE ESES*)». Trials 2020, 21, 957.
- Prpić, I.; Blažeković, I.; Nišević, J.R.; Kolić, I. Corticosteroids in the management of pediatric epilepsies. Acta Clin. Croat. 2022, 60., 31–37. [Google Scholar] [CrossRef]
- Klein, R.; Livingston, S. The effect of adrenocorticotropic hormone in epilepsy. J. Pediatr. 1950, 37, 733–742. [Google Scholar] [CrossRef]
- Sorel, L.; Dusaucy-Bauloye, A. [Findings in 21 cases of Gibbs' hypsarrhythmia; spectacular effectiveness of ACTH]. . 1958, 58, 130–41. [Google Scholar]
- Okumura, A.; Tsuji, T.; Kato, T.; Natsume, J.; Negoro, T.; Watanabe, K. ACTH therapy for generalized seizures other than spasms. Seizure 2006, 15, 469–475. [Google Scholar] [CrossRef]
- Sinclair, D. Prednisone therapy in pediatric epilepsy. Pediatr. Neurol. 2003, 28, 194–198. [Google Scholar] [CrossRef]
- Wanigasinghe, J.; Arambepola, C.; Ranganathan, S.S.; Sumanasena, S. Randomized, Single-Blind, Parallel Clinical Trial on Efficacy of Oral Prednisolone Versus Intramuscular Corticotropin: A 12-Month Assessment of Spasm Control in West Syndrome. Pediatr. Neurol. 2017, 76, 14–19. [Google Scholar] [CrossRef]
- Sevilla-Castillo, R.A.; Palacios, G.C.; Ramirez-Campos, J.; Mora-Puga, M.; Diaz-Bustos, R. Methylprednisolone for the Treatment of Children with Refractory Epilepsy. Neuropediatrics 2009, 40, 265–268. [Google Scholar] [CrossRef]
- Mytinger, J. R, Quigg M. , Taft W.C., Buck ML, Rust R.S. Outcomes in treatment of infantile spasms with pulse methylprednisolone. J. Child Neurol. 2010, 25, 948–53. [Google Scholar]
- Ebinger, F.; Rating, D.; Wiemer-Kruel, A.; Schubert-Bast, S.; Bast, T.; Richter, S. Efficacy and Tolerability of Methylprednisolone Pulse Therapy in Childhood Epilepsies Other Than Infantile Spasms. Neuropediatrics 2014, 45, 378–385. [Google Scholar] [CrossRef]
- Almaabdi, K.H.; Alshehri, R.O.; Althubiti, A.A.; Alsharef, Z.H.; Mulla, S.N.; Alshaer, D.S.; Alfaidi, N.S.; Jan, M.M. Intravenous Methylprednisolone for Intractable Childhood Epilepsy. Pediatr. Neurol. 2014, 50, 334–336. [Google Scholar] [CrossRef]
- Pera MC, Randazzo G, Masnada S, Dontin SD, De Giorgis V, Balottin U, et al. Intravenous methylprednisolone pulse therapy for children with epileptic encephalopathy. Funct. Neurol. 2015, 30, 173–9.
- Yeh, H.-R.; Kim, M.-J.; Ko, T.-S.; Yum, M.-S.; You, S.-J. Short-Term Outcome of Intravenous Methylprednisolone Pulse Therapy in Patients With Infantile Spasms. Pediatr. Neurol. 2017, 71, 50–55. [Google Scholar] [CrossRef]
- Kimizu, T.; Takahashi, Y.; Oboshi, T.; Horino, A.; Omatsu, H.; Koike, T.; Yoshitomi, S.; Yamaguchi, T.; Otani, H.; Ikeda, H.; et al. Methylprednisolone pulse therapy in 31 patients with refractory epilepsy: A single-center retrospective analysis. Epilepsy Behav. 2020, 109, 107116. [Google Scholar] [CrossRef]
- Chatterjee, A.; Mundlamuri, R.C.; Kenchaiah, R.; Asranna, A.; Nagappa, M.; Bindu, P.; Seshagiri, D.; Viswanathan, L.G.; Shreedhar, A.; Duble, S.; et al. Role of pulse methylprednisolone in epileptic encephalopathy: A retrospective observational analysis. Epilepsy Res. 2021, 173, 106611. [Google Scholar] [CrossRef]
- Rajpurohit, M.; Gupta, A.; Madaan, P.; Sahu, J.K.; Singhi, P. Safety, Feasibility and Effectiveness of Pulse Methylprednisolone Therapy in Comparison with Intramuscular Adrenocorticotropic Hormone in Children with West Syndrome. Indian J. Pediatr. 2020, 88, 663–667. [Google Scholar] [CrossRef]
- Rangarajan, A.; Mundlamuri, R.C.; Kenchaiah, R.; Prathyusha, P.V.; Viswanathan, L.G.; Asranna, A.; Chatterjee, A.; Nagappa, M.; Seshagiri, D.V.; Kulanthaivelu, K.; et al. Efficacy of pulse intravenous methylprednisolone in epileptic encephalopathy: a randomised controlled trial. J. Neurol. Neurosurg. Psychiatry 2022, 93, 1299–1305. [Google Scholar] [CrossRef]
- Miller AL, Chaptal C, McEwen BS, Peck Jr EJ. Modulation of high affinity GABA uptake into hippocampal synaptosomes by glucocorticoids. Psychoneuroendocrinology 1978, 3, 155–64.
- Jacobson, L.; Sapolsky, R. The Role of the Hippocampus in Feedback Regulation of the Hypothalamic-Pituitary-Adrenocortical Axis*. Endocr. Rev. 1991, 12, 118–134. [Google Scholar] [CrossRef] [PubMed]
- Baram, TZ. Pathophysiology of massive infantile spasms: perspective on the putative role of the brain adrenal axis. Ann. Neurol. 1993, 33, 231–6. [Google Scholar] [CrossRef]
- Vidal, C.; Jordan, W.; Zieglga¨nsberger, W. Corticosterone reduces the excitability of hippocampal pyramidal cells in vitro. Brain Res. 1986, 383, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Joëls, M. Steroid Hormones and Excitability in the Mammalian Brain. Front. Neuroendocr. 1997, 18, 2–48. [Google Scholar] [CrossRef]
- Baram, T.Z.; Hatalski, C.G. Neuropeptide-mediated excitability: a key triggering mechanism for seizure generation in the developing brain. Trends Neurosci. 1998, 21, 471–476. [Google Scholar] [CrossRef]
- Watzka, M.; Bidlingmaier, F.; Beyenburg, S.; Henke, R.T.; Clusmann, H.; E Elger, C.; Schramm, J.; Klingmüller, D.; Stoffel-Wagner, B. Corticosteroid receptor mRNA expression in the brains of patients with epilepsy. Steroids 2000, 65, 895–901. [Google Scholar] [CrossRef] [PubMed]
- Joëls, M. Corticosteroid Actions in the Hippocampus. J. Neuroendocr. 2001, 13, 657–669. [Google Scholar] [CrossRef]
- Vezzani, A.; Granata, T. Brain Inflammation in Epilepsy: Experimental and Clinical Evidence. Epilepsia 2005, 46, 1724–1743. [Google Scholar] [CrossRef]
- Marchi, N.; Granata, T.; Freri, E.; Ciusani, E.; Ragona, F.; Puvenna, V.; Teng, Q.; Alexopolous, A.; Janigro, D. Efficacy of Anti-Inflammatory Therapy in a Model of Acute Seizures and in a Population of Pediatric Drug Resistant Epileptics. PLOS ONE 2011, 6, e18200. [Google Scholar] [CrossRef]
- Reddy, D.S. Role of Anticonvulsant and Antiepileptogenic Neurosteroids in the Pathophysiology and Treatment of Epilepsy. Front. Endocrinol. 2011, 2, 38. [Google Scholar] [CrossRef]
- Xu, D.; Miller, S.D.; Koh, S. Immune mechanisms in epileptogenesis. Front. Cell. Neurosci. 2013, 7, 195. [Google Scholar] [CrossRef] [PubMed]
- Frauman, A.G. An overview of the adverse reactions to adrenal corticosteroids. . 1996, 15, 203–6. [Google Scholar]
- Wanigasinghe, J.; Arambepola, C.; Ranganathan, S.S.; Jayasundara, K.; Weerasinghe, A.; Wickramarachchi, P. Epilepsy Outcome at Four Years in a Randomized Clinical Trial Comparing Oral Prednisolone and Intramuscular ACTH in West Syndrome. Pediatr. Neurol. 2021, 119, 22–26. [Google Scholar] [CrossRef] [PubMed]
- O'Callaghan, F.J.K.; Edwards, S.W.; Alber, F.D.; Hancock, E.; Johnson, A.L.; Kennedy, C.R.; Likeman, M.; Lux, A.L.; Mackay, M.; A Mallick, A.; et al. Safety and effectiveness of hormonal treatment versus hormonal treatment with vigabatrin for infantile spasms (ICISS): a randomised, multicentre, open-label trial. Lancet Neurol. 2016, 16, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Gowda, V.K.; Narayanaswamy, V.; Shivappa, S.K.; Benakappa, N.; Benakappa, A. Corticotrophin-ACTH in Comparison to Prednisolone in West Syndrome – A Randomized Study. Indian J. Pediatr. 2018, 86, 165–170. [Google Scholar] [CrossRef]
- Lux, A.L.; Edwards, S.W.; Hancock, E.; Johnson, A.L.; Kennedy, C.R.; Newton, R.W.; O'Callaghan, F.J.; Verity, C.M.; Osborne, J.P. The United Kingdom Infantile Spasms Study comparing vigabatrin with prednisolone or tetracosactide at 14 days: a multicentre, randomised controlled trial. Lancet 2004, 364, 1773–1778. [Google Scholar] [CrossRef]
- O’Callaghan FJK, Edwards SW, Alber FD, Cortina Borja M, Hancock E, Johnson AL, et al. Vigabatrin with hormonal treatment versus hormonal treatment alone (ICISS) for infantile spasms: 18-month outcomes of an open- label, randomised controlled trial. Lancet Child Adolesc. Health 2018, 2, 715–25.
- Darke, K.; Edwards, S.W.; Hancock, E.; Johnson, A.L.; Kennedy, C.R.; Lux, A.L.; Newton, R.W.; O'Callaghan, F.J.K.; Verity, C.M.; Osborne, J.P.; et al. Developmental and epilepsy outcomes at age 4 years in the UKISS trial comparing hormonal treatments to vigabatrin for infantile spasms: a multi-centre randomised trial. Arch. Dis. Child. 2010, 95, 382–386. [Google Scholar] [CrossRef]
- Buzatu, M.; Bulteau, C.; Altuzarra, C.; Dulac, O.; Van Bogaert, P. Corticosteroids as treatment of epileptic syndromes with continuous spike-waves during slow-wave sleep. Epilepsia 2009, 50, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, D.B.; Snyder, T.J. Corticosteroids for the Treatment of Landau-Kleffner Syndrome and Continuous Spike-Wave Discharge During Sleep. Pediatr. Neurol. 2005, 32, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Cai, F.; Jiang, L.; Hu, Y.; Feng, C. A prospective study of dexamethasone therapy in refractory epileptic encephalopathy with continuous spike-and-wave during sleep. Epilepsy Behav. 2016, 55, 1–5. [Google Scholar] [CrossRef]
- Fatema, K.; Rahman, M.M.; Begum, S. Characteristics and Management of Children with Continuous Spikes and Waves during Slow Sleep. . 2015, 24, 806–12. [Google Scholar]
- Munckhof, B.v.D.; van Dee, V.; Sagi, L.; Caraballo, R.H.; Veggiotti, P.; Liukkonen, E.; Loddenkemper, T.; Fernández, I.S.; Buzatu, M.; Bulteau, C.; et al. Treatment of electrical status epilepticus in sleep: A pooled analysis of 575 cases. Epilepsia 2015, 56, 1738–1746. [Google Scholar] [CrossRef] [PubMed]
- Yamatogi, Y.; Ohtsuka, Y.; Ishida, T.; Ichiba, N.; Ishida, S.; Miyake, S.; Oka, E.; Ohtahara, S. Treatment of the lennox syndrome with ACTH: A clinical and electroencephalographic study. Brain Dev. 1979, 1, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Gofshteyn, J.S.; Gurcharran, K.; Marquis, B.O.; Lamothe, J.; Gourley, D.; Grinspan, Z.; Nangia, S. Measurable outcomes for pediatric epileptic encephalopathy: a single-center experience with corticosteroid therapy. Epileptic Disord. 2021, 23, 111–122. [Google Scholar] [CrossRef]
- Chatterjee, A.; Mundlamuri, R.C.; Kenchaiah, R.; Asranna, A.; Nagappa, M.; Bindu, P.; Seshagiri, D.; Viswanathan, L.G.; Shreedhar, A.; Duble, S.; et al. Role of pulse methylprednisolone in epileptic encephalopathy: A retrospective observational analysis. Epilepsy Res. 2021, 173, 106611. [Google Scholar] [CrossRef]
- Charuvanij, A.; A Ouvrier, R.; Procopis, P.G.; Antony, J.H.; Fagan, E.R. ACTH treatment in intractable seizures of childhood. Brain Dev. 1992, 14, 102–106. [Google Scholar] [CrossRef]
- Nasiri, J.; Sarajan, A.; Salari, M.; Sedghi, M. Therapeutic Effects of Adrenocorticotropic Hormone ACTH in Children with Severely Intractable Seizure. . 2017, 11, 19–26. [Google Scholar] [PubMed]
- Bakker, D.P.; Catsman-Berrevoets, C.E.; Neuteboom, R.F. Effectiveness of a hybrid corticosteroid treatment regimen on refractory childhood seizures and a review of other corticosteroid treatments. Eur. J. Paediatr. Neurol. 2015, 19, 553–560. [Google Scholar] [CrossRef]
- Kalra, V.; Sharma, S.; Arya, R. ACTH therapy in refractory generalized epilepsy. Indian J. Pediatr. 2009, 76, 91–93. [Google Scholar] [CrossRef]
- Inui, T.; Kobayashi, T.; Kobayashi, S.; Sato, R.; Endo, W.; Kikuchi, A.; Nakayama, T.; Uematsu, M.; Takayanagi, M.; Kato, M.; et al. Efficacy of long term weekly ACTH therapy for intractable epilepsy. Brain Dev. 2015, 37, 449–454. [Google Scholar] [CrossRef]
- Vossler, D.G.; Bainbridge, J.L.; Boggs, J.G.; Novotny, E.J.; Loddenkemper, T.; Faught, E.; Amengual-Gual, M.; Fischer, S.N.; Gloss, D.S.; Olson, D.M.; et al. Treatment of Refractory Convulsive Status Epilepticus: A Comprehensive Review by the American Epilepsy Society Treatments Committee. Epilepsy Curr. 2020, 20, 245–264. [Google Scholar] [CrossRef]
- Hirsch LJ, Gaspard N, van Baalen A, Nabbout R, Demeret S, Loddenkemper T, et al. Proposed consensus definitions for new-onset refractory status epilepticus (NORSE), febrile infection-related epilepsy syndrome (FIRES), and related conditions. Epilepsia 2018, 59, 739–44.
- Vezzani A, Ruegg S. The pivotal role of immunity and inflammatory processes in epilepsy is increasingly recognized: introduction. Epilepsia 2011, 52, 1–4.
- Shorvon, S.; Ferlisi, M. The treatment of super-refractory status epilepticus: a critical review of available therapies and a clinical treatment protocol. Brain 2011, 134, 2802–2818. [Google Scholar] [CrossRef] [PubMed]
- Vezzani, A.; Balosso, S.; Aronica, E.; Ravizza, T. Basic mechanisms of status epilepticus due to infection and inflammation. Epilepsia 2009, 50, 56–57. [Google Scholar] [CrossRef] [PubMed]
- Vezzani, A. Epilepsy and Inflammation in the Brain: Overview and Pathophysiology. Epilepsy Curr. 2014, 14, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Neugebauer, R.; Paik, M.; Hauser, W.A.; Nadel, E.; Leppik, I.; Susser, M. Stressful Life Events and with Seizure Frequency in Patients Epilepsy. Epilepsia 1994, 35, 336–343. [Google Scholar] [CrossRef]
- McKee, H.R.; Privitera, M.D. Stress as a seizure precipitant: Identification, associated factors, and treatment options. Seizure 2017, 44, 21–26. [Google Scholar] [CrossRef]
- Privitera, M.; Walters, M.; Lee, I.; Polak, E.; Fleck, A.; Schwieterman, D.; Haut, S.R. Characteristics of people with self-reported stress-precipitated seizures. Epilepsy Behav. 2014, 41, 74–77. [Google Scholar] [CrossRef]
- Sawyer, N.T.; Escayg, A. Stress and Epilepsy: Multiple Models, Multiple Outcomes. J. Clin. Neurophysiol. 2010, 27, 445–452. [Google Scholar] [CrossRef]
- Basu, T.; Maguire, J.; Salpekar, J.A. Hypothalamic-pituitary-adrenal axis targets for the treatment of epilepsy. Neurosci. Lett. 2021, 746, 135618. [Google Scholar] [CrossRef] [PubMed]
- Mackenzie G, Maguire J. Chronic stress compromises GABAergic inhibition in the hippocampus and increases seizure susceptibility. Epilepsy Res. 2015, 109, 13–27.
- Castro, O.W.; Santos, V.R.; Pun, R.Y.K.; McKlveen, J.M.; Batie, M.; Holland, K.D.; Gardner, M.; Garcia-Cairasco, N.; Herman, J.P.; Danzer, S.C. Impact of Corticosterone Treatment on Spontaneous Seizure Frequency and Epileptiform Activity in Mice with Chronic Epilepsy. PLOS ONE 2012, 7, e46044. [Google Scholar] [CrossRef]
- Culebras, A.; Miller, M.; Bertram, L.; Koch, J. Differential Response of Growth Hormone, Cortisol, and Prolactin to Seizures and to Stress. Epilepsia 1987, 28, 564–570. [Google Scholar] [CrossRef] [PubMed]
- Abbott, R.J.; Browning, M.C.; Davidson, D.L. Serum prolactin and cortisol concentrations after grand mal seizures. J. Neurol. Neurosurg. Psychiatry 1980, 43, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Pritchard, P.B.; Wannamaker, B.B.; Sagel, J.; Daniel, C.M. Serum prolactin and cortisol levels in evaluation of pseudoepileptic seizures. Ann. Neurol. 1985, 18, 87–89. [Google Scholar] [CrossRef]
- Wulsin, A.C.; Solomon, M.B.; Privitera, M.D.; Danzer, S.C.; Herman, J.P. Hypothalamic-pituitary-adrenocortical axis dysfunction in epilepsy. Physiol. Behav. 2016, 166, 22–31. [Google Scholar] [CrossRef]
- Yao TC, Huang YW, Chang SM, Tsai SY, Wu AC, Tsai HJ. Association between oral corticosteroid bursts and severe adverse events: a nationwide population-based cohort study. Ann Intern Med. 2020, 173, 325–30.
- Stuart FA, Segal TY, Keady S. Adverse psychological effects of corticosteroids in children and adolescents. Arch. Dis. Child. 2005, 90, 500–6.
- Yasir M, Goyal A, Sonthalia S. Corticosteroid Adverse Effects. Tampa, FL: StatPearls. 2022.
- Rice, J.B.; White, A.G.; Scarpati, L.M.; Wan, G.; Nelson, W.W. Long-term Systemic Corticosteroid Exposure: A Systematic Literature Review. Clin. Ther. 2017, 39, 2216–2229. [Google Scholar] [CrossRef]
- Aljebab, F.; Choonara, I.; Conroy, S. Systematic review of the toxicity of short-course oral corticosteroids in children. Arch. Dis. Child. 2016, 101, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Bassett, D.S.; Bullmore, E. Small-World Brain Networks Revisited. 2016. [CrossRef]
- Meunier, D.; Lambiotte, R.; Bullmore, E.T. Modular and Hierarchically Modular Organization of Brain Networks. Front. Neurosci. 2010, 4, 200. [Google Scholar] [CrossRef]
- Stam, C.J.; Reijneveld, J.C. Graph theoretical analysis of complex networks in the brain. Nonlinear Biomed. Phys. 2007, 1, 3–3. [Google Scholar] [CrossRef]
- Clemens, B.; Puskás, S.; Bessenyei, M.; Emri, M.; Spisák, T.; Koselák, M.; Hollódy, K.; Fogarasi, A.; Kondákor, I.; Füle, K.; et al. EEG functional connectivity of the intrahemispheric cortico-cortical network of idiopathic generalized epilepsy. Epilepsy Res. 2011, 96, 11–23. [Google Scholar] [CrossRef]
- Pittau, F.; Grova, C.; Moeller, F.; Dubeau, F.; Gotman, J. Patterns of altered functional connectivity in mesial temporal lobe epilepsy. Epilepsia 2012, 53, 1013–1023. [Google Scholar] [CrossRef]
- Otte WM, Dijkhuizen RM, van Meer MPA, van der Hel WS, Verlinde SAMW, van Nieuwenhuizen O, et al. Characterization of functional and structural integrity in experimental focal epilepsy: reduced network efficiency coincides with white matter changes. PLoS One 2012, 7, 39078 .
- Vollmar C, O’Muircheartaigh, Symms MR, G. J. Barker GJ, P. Thompson P, V. Kumari V, et al. Altered microstructural connectivity in juvenile myoclonic epilepsy: the missing link. Neurology 2012, 78, 1555–9.
- Chavez, M.; Valencia, M.; Navarro, V.; Latora, V.; Martinerie, J. Functional Modularity of Background Activities in Normal and Epileptic Brain Networks. Phys. Rev. Lett. 2010, 104, 118701. [Google Scholar] [CrossRef]
- Douw, L.; van Dellen, E.; de Groot, M.; Heimans, J.J.; Klein, M.; Stam, C.J.; Reijneveld, J.C. Epilepsy is related to theta band brain connectivity and network topology in brain tumor patients. BMC Neurosci. 2010, 11, 103–103. [Google Scholar] [CrossRef]
- Ponten, S.; Bartolomei, F.; Stam, C. Small-world networks and epilepsy: Graph theoretical analysis of intracerebrally recorded mesial temporal lobe seizures. Clin. Neurophysiol. 2007, 118, 918–927. [Google Scholar] [CrossRef] [PubMed]
- Terry JR, Benjamin O, Richardson MP. Seizure generation: the role of nodes and networks. Epilepsia 2012, 53, e166–9 .
- Bartolomei F, Bettus G, Stam CJ, Guye M. Interictal network proper- ties in mesial temporal lobe epilepsy: a graph theoretical study from intracerebral recordings. Clin. Neurophysiol. 2013, 124, 2345–53.
- Bernhardt, B.C.; Chen, Z.; He, Y.; Evans, A.C.; Bernasconi, N. Graph-Theoretical Analysis Reveals Disrupted Small-World Organization of Cortical Thickness Correlation Networks in Temporal Lobe Epilepsy. Cereb. Cortex 2011, 21, 2147–2157. [Google Scholar] [CrossRef] [PubMed]
- Horstmann, M.-T.; Bialonski, S.; Noennig, N.; Mai, H.; Prusseit, J.; Wellmer, J.; Hinrichs, H.; Lehnertz, K. State dependent properties of epileptic brain networks: Comparative graph–theoretical analyses of simultaneously recorded EEG and MEG. Clin. Neurophysiol. 2010, 121, 172–185. [Google Scholar] [CrossRef]
- Engel, J., Jr.; Thompson, P.M.; Stern, J.M.; Staba, R.J.; Bragin, A.; Mody, I. Connectomics and epilepsy. Curr. Opin. Neurol. 2013, 26, 186–194. [Google Scholar] [CrossRef]
- Kramer, M.A.; Kolaczyk, E.D.; Kirsch, H.E. Emergent network topology at seizure onset in humans. Epilepsy Res. 2008, 79, 173–186. [Google Scholar] [CrossRef]
- Van Diessen E, Diederen SJH, Braun KPJ, Jansen FE, Stam CJ. Functional and structural brain networks in epilepsy: what have we learned? Epilepsia 2013, 54, 1855–65.
Figure 1.
NR: no responders; PR: partial responders; GR: good responders; SF: seizure free; FU: follow-up.
Figure 1.
NR: no responders; PR: partial responders; GR: good responders; SF: seizure free; FU: follow-up.
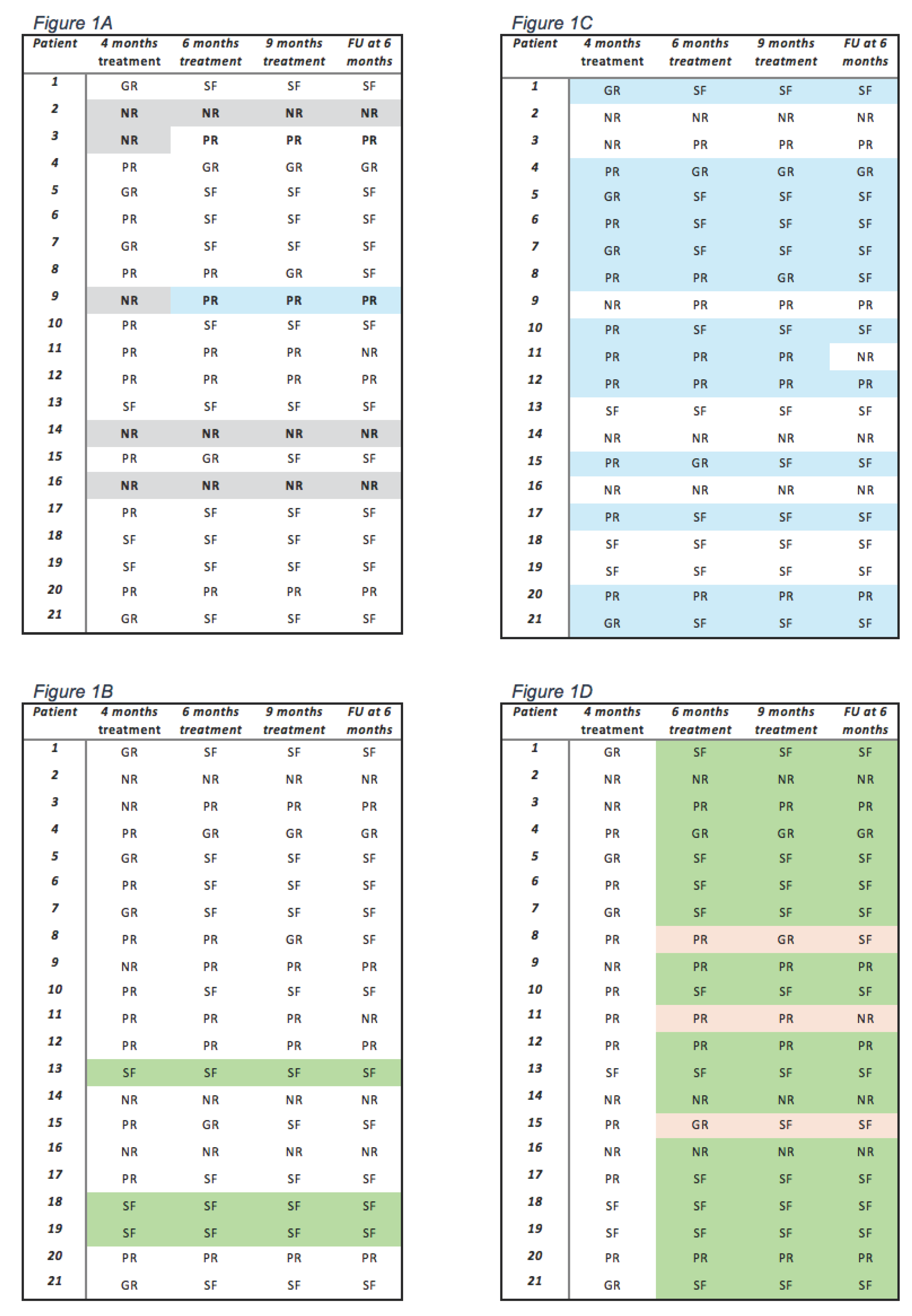

Table 1.
Outcome data during 9 months of IVMP pulse therapy and at 6 months of follow-up.
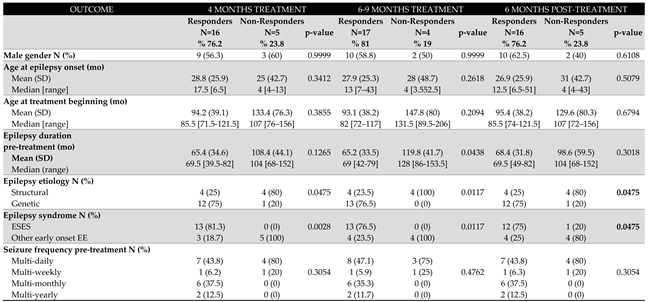
Legend: N: number; mo: months; SD: standard deviation ESES: encephalopathy related to with status epilepticus during slow sleep; EE: epileptic encephalopathies.
Table 2.
IVMP pulse therapy efficacy and outcome.
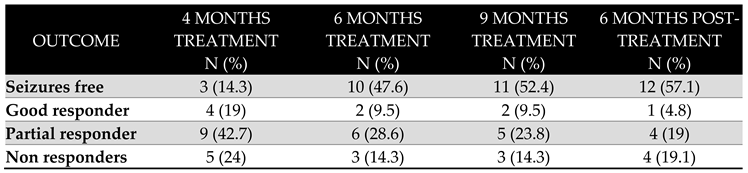
Legend: Good responders: > 75% seizure reduction; Partial responders: 50-75% seizure reduction.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



