Submitted:
26 February 2024
Posted:
06 March 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Abstract: The emergence of the COVID-19 pandemic has led to the rapid and worldwide devel-opment and investigation of multiple vaccines. While most side effects of these vaccines are mild and transient, potentially severe adverse events may occur and involve the endocrine system. This narrative review aims to explore the current knowledge on potential endocrine adverse effects following COVID-19 vaccination, with thyroid disorders being the most common. Data about pi-tuitary, adrenal, diabetes, and gonadal events will also be reviewed. This review also provides a comprehensive understanding of the pathogenesis of endocrine disorders associated with SARS-CoV-2 vaccines. A PubMed/MEDLINE, Embase database (Elsevier), and Google Scholar research were performed. Case reports case series, original studies, and reviews written in English and published online up to 31 August 2023 were selected and reviewed. Data on endocrine adverse events of SARS-CoV-2 vaccines is accumulating. However, their causal relationship with COVID-19 vaccines is not strong enough to make a definite conclusion, and further studies are needed to clarify the pathogenesis mechanisms of endocrine disorders linked to COVID-19 vac-cines.
Keywords:
COVID-19
; COVID-19 vaccines
; SARS-CoV-2 vaccine
; endocrine adverse events
; thyroid
; pituitary
; adrenal
; diabetes
; gonads
1. Introduction
By January 7, 2024, the COVID-19
pandemic has globally affected more than 774 million people and is responsible
for more than 7 million deaths [1]. The
emergence of this pandemic led to a global vaccination effort to curb the
spread and severity of the disease. Among the most widely approved
vaccines are mRNA-based vaccines(BNT162b2 Comirnaty/Pfizer BioNtech; nRNA-1273
Spikevax/Moderna), viral-vector based (AZD1222 Vaxzevria (ChAdOx1) Oxford
University/AstraZeneca; Ad26.COV2.S/Janssen), and inactivated virus-based
(Covilo, BBIBP-CorV(Vero Cells)/Sinopharm) [2].
While SARS-CoV-2 primarily affects the respiratory system, causing pneumonia
and acute respiratory distress syndrome in the most severe cases, numerous
extrapulmonary manifestations, including endocrine system disorders, can lead
to permanent disability in COVID-19 survivors [3].
The plausible mechanisms related to thyroid, adrenal, pituitary, or pancreatic
islets involvement are still not fully understood, albeit immune system
hyperstimulation due to COVID-19 vaccination can trigger and perpetuate
autoimmunity and impair endocrine tissue function. The mechanisms leading to
these disorders exhibit similarities with endocrine dysfunction following
COVID-19 infection. Notably, the expression of the angiotensin-converting
enzyme 2(ACE-2) in these tissues constitutes a significant target in the
pathogenesis of viral cell damage.
Similarly, activation of the
renin-angiotensin system by ACE receptor downregulation is one of the possible
mechanisms in developing endocrine dysfunction following the COVID-19 vaccine [4,5]. A recent systematic review confirmed the
safety of the four most efficacious COVID-19 vaccines [6], even if a few severe adverse events, including
endocrine dysfunction, have been reported [7].
This review will delve into the current findings on the influence of COVID-19
vaccines on the endocrine system, exploring the specific endocrine disorders
reported, the types of vaccines associated with these adverse effects, and the
underlying pathogenic mechanisms. It will
also discuss the implications of these findings for clinical practice and
future research.
2. Material and Methods
A PubMed/MEDLINE, Embase database
(Elsevier), and Google Scholar research was performed for free-text words and
medical subject heading terms related to "severe acute respiratory
syndrome coronavirus 2 (SARS-CoV-2) vaccine”, “COVID-19 vaccine”, “SARS-CoV-2
vaccination”, “COVID-19 vaccination”, “SARS-CoV-2 immunization” variously
combined with “endocrinopathies,” endocrine adverse events",
"SARS-CoV-2 vaccine-related", “endocrine system”, “thyroid”,
“subacute thyroiditis”, “Graves’ disease”, “hypothyroidism”, “hyperthyroidism”,
“adrenal”, “adrenal insufficiency”, “adrenal crisis”, “Addison disease”,
“adrenal hemorrhage”, “pituitary gland”, “hypophysitis”, “hypopituitarism”,
“pituitary apoplexy”, “type 1 diabetes”, “diabetes”, "pancreatitis",
diabetic ketoacidosis", “ovary”, “amenorrhea,” “menstrual cycle”,
“menstrual dysfunction,” “female fertility”, “male infertility,” “couple
infertility,” “sperm,” “reproductive health,” “male hypogonadism,” and “sexual
dysfunction”. Case reports, case series, original
studies, and reviews written in English and published online up to 31 August
2023 were selected and reviewed. The final reference list was defined based
on the relevance of each paper to the scope of this review.
3. SARS-CoV-2 Vaccination and Thyroid Dysfunction
Following the worldwide rollout of
SARS-CoV-2 vaccination initiatives, various immune-mediated inflammatory
disorders have been associated with the administration of vaccines. [8,9]. Among the reported endocrine side effects,
thyroid disorders are the most common [10].
These side effects are presumably triggered by cross-reactivity between the vaccine-targeted
virus spike protein and thyroid follicular cell antigens [11]. Another proposed mechanism is an enhancement
of autoimmunity by vaccine adjuvants in predisposed individuals in the form of
the post-vaccination syndrome known as the autoimmune/inflammatory syndrome
induced by adjuvants (ASIA) syndrome [11,12]. Current
literature describes a spectrum of thyroid dysfunction post-SARS-CoV-2 vaccine
administration, including subacute thyroiditis (SAT), silent thyroiditis, overt
hypothyroidism, Graves' disease, and Graves' orbitopathy, ranging from a
new-onset disease to a recurrence of a pre-existing condition [13].
Subacute thyroiditis is a self-limited inflammatory disease with a genetic
predisposition that may present in individuals carrying specific human
leukocyte antigen (HLA) haplotypes [14]. Vaccines
against influenza virus, swine flu, hepatitis B, and human papillomavirus have
been reported as triggering factors for SAT [13].
HLA-B*35 and HLA-C*04 allele genotypes were suggested as responsible for
susceptibility to post-SARS-CoV-2 vaccine SAT development. In a case-control
study, those allele rates were significantly higher in 14 patients with
post-vaccination SAT compared with 100 healthy controls. In addition, more
severe thyrotoxicosis affected relatively more patients with homozygous
HLA-B*35 and HLA-C*04 alleles [15].
The first report on post-SARS-CoV-2 vaccine SAT included 3 cases of female health workers who developed clinical symptoms 4-7 days after administration of inactivated SARS-CoV-2 vaccine [11]. These case series were followed by numerous other case reports and series on the post-vaccine- SAT, as summarized in Table 1.
From thirty-one reviewed articles, 83 cases were retrieved and summarized in Table 1 [12,13, 16-45]. Patients' median age was 41 years (range 26-82), and 61 (73.5%) were women. The clinical picture of SAT was seen on a median of 10 days (range 1-84) after the last vaccination. All the patients had symptoms like sporadic SAT and were treated accordingly. In 76% of cases, SAT resolved without sequela, and hypothyroidism had developed in 12% of cases.
Regarding the vaccine type, SAT was reported more frequently in connection with mRNA vaccines, with 51 cases following mRNA vaccines compared to 17 and 15 cases following viral and inactivated vaccines, respectively. Whether a specific vaccine type was associated with a greater risk of SAT was studied in an extensive case/non-case study that surveyed the adverse effects of mRNA vaccines (BNT162b2; mRNA-1273) and viral vector vaccines (ChAdOx1-S; Ad26.COV2.S ) in a cohort of 1,221,582 individuals and uncovered 162 cases of subacute thyroiditis. Initially, this study demonstrated that mRNA vaccines were more frequently associated with SAT than viral vaccines. However, this association disappeared when these COVID-19 vaccines were compared with influenza vaccines [46].
Further on, two case series compared cohorts of post-vaccine SAT to classical SAT in terms of diagnosis, clinical course, and outcomes. The case series of 23 cases of post-vaccine SAT compared with 62 cases of "classical" SAT showed longer SAT duration (median 28 days (range 10–150) in vaccinated patients [47]. Another case series compared the clinical features of SAT between 16 vaccinated and 39 non-vaccinated patients and found no differences in diagnosis and clinical course [48]. Finally, a multicenter retrospective cohort study compared SAT clinical parameters and outcomes in 258 patients with post-vaccine SAT to patients with classical SAT and showed a similar disease course [49].
Concerning Graves' disease (GD), 70 cases were retrieved from 26 reviewed case reports and case series (Table 1) [50-76]. Median age was 43 years (range 22-74), and 51 (73%) were women. A median latency period between the vaccination date and the diagnosis was 11 days (range 10-40). Ten cases (14%) were patients diagnosed with a relapsed disease.
In a relatively sizeable case series that included 20 patients with a post-vaccination new onset GD and 44 non-vaccinated patients with the first GD episode, clinical features and follow-up were assessed. The cohort of patients with post-vaccination GD was characterized by higher male prevalence, older age at the disease onset, and a better response to treatment, both biochemical and immunologic [77].
Another monocentric retrospective study that included 44 patients with post-vaccination GD showed a female prevalence of 43/44 (97.7%) with a mean age of 48.9 (SD 15.6) years. Notably, 7/44 (15.9%) of patients had a history of additional autoimmune disease, and 11/44 (25%) were smokers. The study also suggests the SARS-CoV-2 vaccination impact on GD incidence by comparing the year 2020, when there was a slight increase in GD cases, with the year 2021 when the incidence of GD more than doubled [78].
In contrast, a population-based, matched, case-control study that included 726 patients with GD and 1452 matched controls found no association between the SARS-CoV-2 vaccination and GD incidence. While a similar proportion of GD patients and controls received vaccination [ 80% (581/726) vs 77.8% (1129/1452), P = .22], no association was found in univariate analyses between at least one vaccine dose and the disease rates [odds ratio 95% confidence interval: 1.15 (.92-1.43)] [79]
with GD assessed the association of vaccination (either with an mRNA (BNT162b2) or inactivated SARS-CoV-2 vaccines) with the risk of thyroid function deterioration. When comparing 529 patients vaccinated with 255 unvaccinated individuals, there was no increased risk of alteration in thyroid function. Also, there was no difference in the GD relapse rates among vaccinated and unvaccinated patients, and there were no cases of thyroid storm in patients with uncontrolled thyrotoxicosis (n=25) at the time of vaccination [80]. Furthermore, a recent population-based cohort study of patients with COVID-19 showed an increased risk of GD development compared to the non-COVID-19 group [aHR: 1.30 (95% CI: 1.10–1.54)]. However, after the completion of two vaccine doses, the risk of developing GD, as well as various autoimmune disease, decreased in the vaccinated versus unvaccinated population [81].
Finally, another population-based study evaluated the risk of thyroid dysfunction in 2.3 million participants who received at least one CoronaVac or BNT162b2 vaccine dose. The study demonstrated no evidence of a vaccine-related increase in the incidence of clinical thyroid disease. No increased risk was found in subanalyses specifically for patients with GD, for inactivated (CoronaVac) and mRNA (BNT162b2) vaccine types, and both vaccine doses within 56 days post-immunization [82]. Moreover, a recent population-based cohort study suggests that the COVID-19 associated increased risk of
Ten cases of new-onset or worsening of Grave's ophthalmopathy (GO) were described [59,63, 83]. In all but one case, thyroid function tests were normal, but TSH-receptor antibodies (TRAb) level were significantly elevated in eight out of ten patients described. Noteworthy, no triggering effects other than COVID-19 vaccination with mRNA vaccine, were identified before significant deterioration of stable thyroid eye disease. GD onset or recurrence concurrently with new onset of GO following SARS-CoV-2 mRNA vaccination was described [45-57]. New-onset thyroid eye disease after COVID-19 vaccination was also reported in a patient with GD relapse treated with radioactive iodine 9 months before vaccine administration [84].
4. Pituitary Gland and SARS-CoV-2 Vaccine
The pituitary gland has been the focus of recent attention due to potential dysfunction following SARS-CoV-2 vaccination. Several cases of pituitary disorders, including hypophysitis, arginine-vasopressin deficiency (central diabetes insipidus), inappropriate diuresis, i.e., the syndrome of inappropriate secretion of antidiuretic hormone (SIADH), pituitary apoplexy, and adenocorticotropic hormone (ACTH) deficiency were described following SARS-CoV-2 vaccination. Most of these patients had no previous known pituitary disease or SARS-CoV-2 infection. The median time between vaccination and the onset of pituitary disorder was 3 days and ranged from one [85-88] to sixty days [89]. Description of the reported cases are summarized in supplementary Table 1. Regarding pituitary apoplexy (PA), five cases were reported [85-88, 90]. Pituitary apoplexy is a rare but severe condition caused by an abrupt hemorrhaging and/or infarction od pituitary gland. Its prevalence was estimated at 6·2 cases/100,000 inhabitants [91]. About 50% of PA are undiscovered by precipitating events like pregnancy, post-partum, coagulopathy, trauma, or hypertension [92] The most prominent symptom of PA is severe headache [93], and it was present in 4 of the 5 case reports presented in this review [85-87, 90]. Recently, a potential association of PA with SARS-CoV-2 vaccine has been postulated [94]. In four of the five PA following COVID-19 vaccination reported, a subsequent diagnosis of pituitary adenoma was made [85, 87,88,90]. Therapeutic strategies for PA are controversial i.e., neurosurgery vs.conservative approach [93]. In the cases reported here, only 2 patients underwent transsphenoidal surgery [85-88]. Among the five cases of PA reported after COVID-19 vaccination, 3 occurred after administration of viral vector vaccine [86, 87,90], one after mRNA-based vaccine [85] and in the last case the type of vaccine was not reported [88]. The mechanisms of pituitary apoplexy following COVID-19 vaccination are not fully understood, but several hypotheses have been suggested. Autoimmunity and the vaccine-induced thrombotic thrombocytopenia syndrome (VITT) may be the causes of PA. The cross reactivity between the vaccine components and specific pituitary proteins (molecular mimicry) may lead and immune response that affect the pituitary gland [85,94]. While the autoimmune/autoinflammatory syndrome induced by adjuvants (ASIA) has been proposed as a potential factor in the development of PA, an alternative hypothesis suggests that the pituitary gland's extensive and fragile vascular network may render it particularly vulnerable to PA, especially in the presence of a preexisting pituitary tumor or previous asymptomatic SARS-CoV-2 infection, as evidenced by immunohistochemistry analysis [85,95]. Concerning hypophysitis, this is a sporadic disease with an incidence of ~1 in 9 million/year in the form of primary hypophysitis [ 96]. Hypophysitis following SARS-CoV-2 vaccine present most often as isolated arginine vasopressin (AVP) deficiency (central diabetes insipidus) due to infundibuloneurohypophysitis [89,97-99]. AVP deficiency was also reported with subsequent development of optic neuritis [100]. Rarely, a concomitant anatomic and functional involvement of the anterior pituitary is present [101-102]. Isolated ACTH deficiency [103] and SIADH [104] have also been reported after COVID-19 vaccine. All the cases of hypophysitis presented in supplementary Table 1 occurred after vaccination with mRNA types of vaccines except one [98]. The pathophysiology of vaccine-induced hypophysitis is not fully understood, but several mechanisms have been proposed. The ASIA syndrome is frequently cited, but three major criteria should be met for its diagnosis [105]. In subjects with genetic predisposition, exposure to adjuvants may rarely set off polygenic autoimmune phenomena [106]. The immune disruption induced by adjuvants is mainly attributed to molecular mimicry between modified SARS-CoV-2 proteins and human endocrine targets proteins leading to autoimmune inflammation [94]. Another possible mechanism is that in some circumstances, SARS-CoV-2 mRNA vaccines may induce production of high and possibly toxic amounts of Spike(S) protein that may increase the risk of developing adverse reactions [107, 108]. Vaccine induced hypophysitis may affect corticotrophs, gonadotrophs and thyreotrophs cells. The clinical features vary depending on the extension and severity of the inflammatory process [94].
5. Adrenal Glands and SARS-CoV-2 Vaccine
Adrenal glands, with their high blood supply, are susceptible to sepsis-induced damage, endothelial injury, and hemorrhage due to their unique vascular structure. This vulnerability can lead to acute adrenal insufficiency, a life-threatening condition. Acute adrenal infarction [109-110] and adrenal hemorrhage [111-112] have been described as secondary to SARS-CoV-2 infection. Similarly, adrenal adverse events following COVID-19 vaccination have been reported. These events are rare but may lead to adrenal crisis (AC), which is a life-threatening condition [113-114]. A case-series report of 5 patients with known adrenal insufficiency (AI), 3 with primary and 2 with secondary AI, who develop AC within the first 24 h after administration of the first dose of the Astra- Zeneca ChAdOx1 SARS-CoV-2 vaccine was published [115]. The authors conclude that the COVID-19 vaccination could have precipitated AC in these patients. The Clinical Advisory Panel of the Addison's Disease Self Help Group (ADSHG) have advised that there is no need to routinely increase glucocorticoid dose in patients with adrenal insufficiency at the time of vaccination if there are no significant symptoms but recommended to increase the maintenance glucocorticoid dosage immediately after experiencing any symptoms following their COVID-19 vaccination [116]. The Pituitary Society conducted a survey among its members to gather insights on the planned management strategies for glucocorticoid administration in patients with known AI, after administration of COVID-19 vaccination. About two-thirds of the responders would increase the glucocorticoid dose only in case of side effects like fever, myalgia or arthralgias [117]. In a study of patients with primary and secondary AI, Pilli et al. found that COVID-19 mRNA vaccines were well tolerated and did not require increased glucocorticoid dose replacement therapy before vaccination [118].
A pheochromocytoma crisis was described in 63-year-old patient with no medical history, one day after administration of the non-replicating viral vector-based vaccine Johnson & Johnson. A 7 cm adrenal mass was removed, and the patient recovered. The authors concluded that the pheochromocytoma crisis may have been triggered by the COVID-19 vaccine [119].
Markovic et al. [120] reported the occurrence of AC in a patient with hypopituitarism after a mRNA-based vaccine (BNT162b2). Data of non-hemorrhagic adrenal adverse events are summarized in supplementary Table 2. On the other hand, adrenal hemorrhage with eventually subsequent adrenal crisis has been reported in the context of vaccine-induced thrombotic thrombocytopenia (VITT). To our knowledge, seventeen cases of adrenal bleeding following COVID-19 vaccination have been reported to date [121-133]. Four were unpublished but reported in a systematic review and survey from the UK [133]. All the cases reported occurred after viral vector-based vaccines, except two following the BNT162b2 SARS-CoV-2 mRNA vaccine [133]. The main findings of these studies are summarized in supplementary Table 3. The pathophysiological mechanisms behind adrenal adverse events following COVID-19 vaccination are not fully elucidated, but several hypotheses and observations have been made. Adrenal crisis (AC) can be precipitated by the stress response to vaccination, particularly in individuals with pre-existing adrenal insufficiency or hypopituitarism [120]. Adrenal hemorrhage, a severe complication, has been reported in the context of vaccine-induced immune thrombotic thrombocytopenia (VITT). VITT, characterized by venous thrombosis, is a rare but serious adverse event associated with adenoviral vector-based COVID-19 vaccines and carries a high mortality risk [134]. The pathogenesis of VITT involves the production of antiplatelet Factor 4 (PF4) antibodies triggered by the vaccines, which can lead to platelet activation, thrombosis, and thrombocytopenia [135] Adenoviral vector-based vaccines have been more frequently implicated in VITT cases, while mRNA-based COVID-19 vaccines have also been linked to instances of adrenal insufficiency. It is suggested that the vaccine's components, such as adjuvants, might trigger an immune response that could potentially lead to endocrine dysfunctions, including adrenal insufficiency [103].
6. SARS-CoV-2 Vaccination and Female Reproductive System
Generally, vaccines do not harm fertility [136]. Still, the SARS-CoV-2 vaccine-related immune alterations linked to potential infertility have raised public concern. The absence of safety evidence due to excluding pregnant women from vaccine trials may have triggered initial apprehension [137]. Germ cells are highly vulnerable to DNA damage, affecting fertility and transferred to offspring. Moreover, as was previously claimed and later criticized, due to the resemblance of the SARS-CoV-2 spike protein and syncyntin1, the mRNA vaccine could theoretically harm placental function, raising the risk of miscarriage by stimulation antibodies against the syncyntin1 protein [138]. Finally, a study has indicated that T-cell activation increased the risk of implantation failure after the transfer of in vitro fertilized embryos [139].
In light of these concerns, clinical studies examined the risk of infertility by investigating the SARS-CoV-2 vaccine-related effects on the menstrual cycle and ovarian reserve. Ovarian reserve markers include antral follicle count (AFC), anti-Müllerian hormone (AMH), follicle-stimulating hormone (FSH), and estradiol (E2). These markers may reflect oocytes' quantity, quality, and reproductive capacity [140]. Whereas alterations in female sex hormone levels may cause menstrual cycle irregularities.
During the COVID-19 pandemic, more patients have experienced menstrual cycle alteration after SARS-CoV-2 vaccination. A retrospective study in young women (mean age 33 years) reported delayed menstruation and abnormal uterine bleeding in 23 % and 77 % of cases, respectively. Those abnormalities occurred within the first three weeks of vaccination, mainly after the second vaccine dose. It appears that the mRNA vaccines (Pfizer/BioNTech Comirnaty and Moderna) were most commonly associated with reports of menstrual dysfunction related to alteration of female sex hormone levels. However, FSH and E2 levels were not significantly different in the vaccinated women compared to the control group and did not correlate with the vaccine types [141]. Another study reported no alterations in hormone levels, including E2, FSH, and LH, after the third dose of the SARS-CoV-2 vaccine compared to pre-vaccination levels [142].
The association between SARS-CoV-2 vaccination and ovarian reserve parameters was investigated in twelve studies summarized in Table 2 [143-154].
Four studies [143-148] showed no significant shift in AMH and AFC levels following vaccination. However, one prospective study described a significant decrease in serum AMH levels at months 3 or 6 of follow-up compared to pre-vaccination. However, at month 9 of follow-up, serum AMH levels normalized and stayed within the normal ovarian reserve range (>1.1 ng/dl) throughout the study period [149].
Eight reports [143-145, 150-154] focused on the population undergoing assisted reproduction treatment and demonstrated no harmful impact of the SARS-CoV-2 vaccine on ovarian reserves during assisted reproduction cycles. One of the prospective studies showed that regardless of the type of vaccine, there is no significant adverse effect on ovarian function in patients treated with assisted reproduction therapy [154].
Finally, a recent prospective Internet-based study enrolled couples who were trying to conceive without the use of fertility treatment. The study found no link between the COVID-19 vaccine and an increased risk of miscarriage and no evidence of a higher risk of miscarriage associated with male partner vaccination [ 155].
7. SARS-CoV-2 Vaccination and Male Reproductive System
Hypothetically, a direct impact of the SARS-CoV-2 vaccine on male fertility through compromised germ cell development would be reflected in a prompt drop in semen quality [156]. As known, , testicular spermatozoa form and mature within 2.5 months and follow the final differentiation into epididymal sperm during the next two weeks. One should consider the spermatogenic cycle length when assessing the interval between vaccination and semen analysis. Regarding the potential effect of the vaccine on semen quality, it would be appropriate to sample the specimen within three to six months after vaccination. Semen quality parameters include pH, volume, morphology, total sperm count, sperm concentration, progressive motility, total progressive motile sperm count, and chromatin condensation [157].
Twelve clinical studies evaluated the SARS-CoV-2 vaccine's effect on male fertility by analyzing semen quality, as summarized in Table 2. Four prospective studies in healthy young men evaluated sperm parameters, and no significant abnormalities were detected [158-161]. However, a study on healthy men undergoing IVF due to female infertility has shown a substantial reduction in total and progressive sperm motility after vaccination, which remained in the normal range [162]. Six other retrospective studies examined various vaccine types (mRNA, inactivated, and viral vector vaccines) on sperm quality characteristics. Three studies investigated healthy men [163-165] and three individuals undergoing fertility treatments [166-168]. Overall, sperm characteristics were not influenced after vaccination, excluding a temporary decrease in concentration and motility in one study and decreased total sperm motility with increased FSH levels compared with the men in the unvaccinated group in another study; both studies focused on healthy donors [166,168]. In addition, in the survey of men undergoing fertility treatments, there was an insignificant drop in sperm volume [167].
Finally, a recent study has demonstrated the presence of SARS-CoV-2 antibodies in seminal plasma and assessed its impact on sperm quality. The study showed a strong correlation between titers of SARS-CoV-2 antibodies in serum and seminal plasma. However, considerable levels of the antibodies in seminal plasma after vaccination were not associated with a decline in sperm quality [169].
8. Diabetes Mellitus and COVID-19 Vaccine
8.1. Diabetes Mellitus and mRNA Vaccination
Diabetes is a risk factor for mortality in SARS coronavirus, MERS coronavirus, influenza A 2009 (H1N1) and SARS-CoV-2 infections. Increased airway glucose levels can raise the replication of respiratory pathogens, exposing diabetic patients to bacterial overgrowth after virus infection [170].
Safe and effective messenger RNA (mRNA) vaccines successfully aborted the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic [171].
Nevertheless, type 2 diabetes patients with poor glycemic control after receiving the mRNA-BNT162b vaccine had an increased incidence of SARS-CoV2 breakthrough infections [172]. How can mRNA vaccines impact islet cells and the central mechanism of reducing insulin secretion after COVID-19 vaccination remains not completely elucidated. A few cases of pancreatitis related to SARS vaccination were reported [173-175]. It’s speculated that molecular mimicry mechanism, i.e., the similarity between certain pathogenic elements contained in the vaccine (like spike protein, nucleoprotein, and membrane protein) and self-antigens leads to cross-recognition of specific human proteins, immune system hyperstimulation, and overt autoimmune reaction [176]. Indeed, an autopsy study revealed the specific activation of the innate immune system in patients with enterovirus infection and fulminant diabetes, characterized by overexpression of cytoplasmic retinoic acid–inducible gene I (RIG-I)-like receptors and melanoma differentiation-associated gene 5 (MDA5) in the β and α-pancreatic cells [177]. The expression of the MDA5 gene is implicated in the immune response to SARS-CoV-2 infection and could also be involved in activating the immune system in response to mRNA vaccines [178].
In a recently published systematic review designed to explore the interaction between COVID-19 vaccination and diabetes, a total of 54 studies were included [179]. Twelve cases of new-onset type 1 diabetes mellitus were reported following mRNA vaccines. Six of these cases were associated with a reduced C-peptide level (< 0.6 ng/ml), and eight cases were found to be GAD65Ab positive. Two cases of severe diabetic ketoacidosis in patients with Type 1 diabetes mellitus were also reported after whole inactivated virus-based COVID-19 (COXAVIN) and non-replicating viral vector COVISHIELD (ChAdOx1 nCoV-19) vaccines [179]. Three more cases of Type 1 diabetes related to mRNA vaccination were recently reported [180,181]. Most of the patients who developed Type 1 diabetes after COVID-19 vaccination were discharged with permanent insulin therapy [179]. However, among the four reported cases of Type 1 diabetes following SARS-CoV-2 mRNA vaccination, it is noteworthy that 3 patients gradually discontinued insulin treatment within a few months, while in the fourth, the insulin dose was reduced to 10 units daily [182]. Several cases of new-onset type 1 diabetes presenting as diabetic ketoacidosis (DKA) were reported. Sakurai K. et al. reported a case of fulminant Type 1 diabetes presenting with severe ketoacidosis in a 36-year-old woman and diagnosed 10 days following COVID-19 mRNA-based vaccine [183]. Yano M. et al. reported type 1 diabetes accompanied by DKA one and half months after mRNA vaccine [184]. Sasaki K et al. reported the case of fulminant diabetes eight days after mRNA vaccination [185]. Bleve E et al. reported two additional cases of type 1 diabetes, the first after mRNA and the second after viral vector vaccines [180]. Ketonuria was recorded in only one of them [180]. Aydoğan Bİ et al. reported four cases of type 1 diabetes triggered by mRNA-based SARS-CoV-2 vaccination, BNT162b (Pfizer–BioNTech), but only in one patient metabolic ketoacidosis was documented [182]. Lastly, Kshetree B et al. reported the rapid progression of prediabetes to Type 1 diabetes with ketoacidosis in an elderly male two months after receiving (mRNA) COVID-19 vaccine booster [186].
Human leukocyte antigen (HLA) typing revealed that specific haplotypes were associated with type 1 diabetes arising after vaccination in Japan: HLA-DRB1*0405; HLA-DQB1*0401
[186,188]
, HLA-DRB*0901, HLA-DQB10303[184]. The same alleles were found to be related to type 1 diabetes in the Japanese population, thus mRNA vaccines could be a starter of fulminant diabetes in vulnerable patients
.
In all the above-mentioned cases, low C-peptide levels were found at diagnosis. Only in one of the patients reported by Aydoğan Bİ et al. the C peptide level was in the lower end of the normal range [182].
Regarding immunologic tests, the presence of autoantibodies was not uniform. Insulinoma-associated antigen-2 (IA-2) antibody was negative in all studies except in 2 patients reported by Bleve E et al. [180]. Anti glutamic acid decarboxylase (GAD) antibody was not detected in some studies [183-185], while high titers of autoantibodies were detected in others [180-182,187]. High insulin autoantibody (IAA) levels were also reported [187]. Interestingly, additional cases of DKA were reported in two patients after the COVID-19 vaccination concurrently treated with nivolumab due to malignant melanoma [188-189].
An unusual conversion of preexisting type 2 into type 1 autoimmune diabetes concomitant to the occurrence of Graves' disease 4 weeks after the administration of the second dose of the BNT162B2 SARS-CoV-2 was also described [190]. The time of onset of diabetes after vaccination is variable. In ten cases, type 1 diabetes developed 2-8 weeks after vaccination [181,182,184,186,187,190]. In three cases, it occurs one to three days after vaccination [183,185,189].
8.2. GAD Positivity in Type 1 Diabetes.
GAD is the enzyme related to gamma-aminobutyric acid (GABA) production, which is a central brain inhibitory neurotransmitter. Previously, it was found that GAD antibodies were found in several neurologic syndromes. High titers of GAD were discovered in stiff-person syndrome, cerebral ataxia, epilepsy, and limbic encephalitis [191]. Noticeably, high levels of GABA were found in pancreatic β-cells and shown to play a role in the activation of insulin release and inhibition of apoptosis of β-cells [192]. More than 80% of type 1 diabetes patients tested are positive for GAD antibodies. The central mechanism in GAD formation lies in the activation of a specific T helper cell population which is related to the synthesis of proinflammatory cytokines [193]. More than 90% of patients with type 1 diabetes have positively tested for GAD and/or other pancreatic antibodies at the beginning of disease including insulin autoantibodies (IAA), insulinoma -antigen 2 antibodies (ICA 512), or zinc transporter antibodies (ZnT8Ab).
GAD antibodies (GADA) are more common than insulinoma-antigen 2 (IA-2) antibodies in older patients at the time of type 1 diabetes diagnosis. GADA is positively associated with DR3 and DR4 [194]. A very recent study shows significant improvement in the C-peptide response in youth with antibody-positive diabetes treated with teplizumab [195]. Teplizumab is a monoclonal anti-CD 3 antibody, related to modulation of immune response [195]. A new avenue for therapy in autoimmune diseases is directed to reduction CD4(+) T- cells with formation specific CD8(+) memory cells with decreased expression of genes related to immune activation. This phenomenon is called T cell exhaustion [196,197] and is directly related to improvement in β-cell function close to type 1 diabetes diagnosis [198].
8.3. Could COVID-19 Vaccine Elicit GAD Antibody Formation?
In a recent prospective cohort study, fully vaccinated patients have reduced levels of proinflammatory cytokines upon COVID-19 diagnosis as well as after recovery [199].
However, the vaccination, itself can lead to increased inflammatory markers in the early postvaccination period. Characteristically, the magnitude of inflammation was found to be higher for adenovirus-based vaccine [ ChAdOx1; Oxford/AstraZeneca] in comparison to mRNA vaccines [200]. A case of anti-GAD positive limbic encephalitis developed 20 days after administration of the second dose of COVID-19 mRNA (BNT162b2) vaccine [201]. Do COVID-19 vaccines trigger the anti-GAD formation and subsequent type 1 diabetes or do patients with anti-GAD antibodies develop type 1 diabetes shortly after COVID-19 vaccination? This is, for now, not completely elucidated.
8.4 Anti PD-1 and Type 1 Diabetes
Check-point inhibitors are a new class of anti-cancer therapy used for last decade. Among them, are anti-programmed cell death protein antibodies (anti PD-1). Despite of significant therapeutic effect, serious complications, including acute development of type -1 diabetes, related to β-cell destruction was observed in number case reports [189,202,203]. Most of the reported cases were diagnosed within three months of therapy [203], albeit the cases of diabetes were reported after six months since beginning of treatment [189] as well. The very rapid onset of type 1 diabetes starting after 9 days of therapy [202] and even a case of rapid onset of keto-acidosis after the first injection of nivolumab in a type 2 diabetes patient have been described [204].
In the review conducted by Lo Preiato V at al., related to checkpoint inhibitor-associated autoimmune diabetes (CAIDM), anti-GAD positivity was reported in 43% of the 151 cases tested [205]. Noticeably, from six cases of CAIDM with retrospective testing of autoantibodies, three patients were tested positively before diabetes development, two cases underwent seroconversion, and only in one case, no antibodies were not found [206,207-209]. Putting it together, testing for anti-GAD, or other pancreatic autoantibodies could help to identify susceptible individuals. Probably defective PD-1/PD-L1 axis regulation in predisposed individuals can play role in the pathogenesis of CAIDM [210].
8.5 Adjuvants and Type 1 Diabetes
In 2011 Shoenfeld aimed to classify number of autoimmune, autoinflammatory and other autonomic phenomena under new nosology unit named ASIA syndrome. The originality of this entity lies in one unifying feature -administration of different adjuvants [211]
Adjuvants are numerous substances added to vaccines or medical devices for accentuation of immune responses [211]. Among them, aluminum salts were commonly included in different vaccines [212]. When adjuvants activate predominantly the adaptive immune system they trigger manifestations of autoimmune conditions, whereas activation of the innate immune system leads to autoinflammatory diseases [213]. Out of 500 cases of autoimmune and autoinflammatory diseases presumably connected to the hepatitis B vaccine and papillomavirus vaccine 13 cases were related to new onset of type 1 diabetes [212]. The compelling evidence that types 1 diabetes develops because of vaccine adjuvants is missing.
Autoimmune syndromes, including Guillain- Barre syndrome, vaccine-induced immune thrombotic thrombocytopenia (VITT), Immune thrombocytopenic purpura, autoimmune liver disease, Ig-A nephropathy, and arthritis were described after COVID-19 vaccination [214]. The significant differences between the adjuvants included in COVID-19 vaccines have made it challenging to draw conclusive links between the development of autoinflammatory or autoimmune conditions and the vaccines themselves or their adjuvants, due to their complexity [211,215].
9. Discussion
Vaccines represent one of the most essential and powerful implements to prevent morbidity and mortality associated with infectious diseases in healthy populations, in patients with risk factors, and in immunocompromised people [216]. Despite the benefits of vaccination, which outweigh the risk of severe SARS-CoV-2 complications infection, misinformation about adverse events, especially concerning the endocrine system, may compromise adherence to public health guidelines [217].
Several endocrine organs were identified to be affected by the SARS-CoV-2 vaccine. Over the past years, a multifaceted relationship between the endocrine system and COVID-19 vaccines has been a significant area of research.
Among the post-vaccination new-onset endocrine disorders, subacute thyroiditis (SAT), with several hundred published cases, has been the most reported in the literature. Most reviewed studies demonstrate similarities between post-vaccine SAT and the classic disease regarding diagnosis, clinical course, and outcomes [48,49]. The underlying pathophysiology is an inflammatory process that causes the destruction of follicular epithelium and may be triggered by an immune response following vaccination. However, data establishing a direct link is lacking. Graves' disease (GD) was also reported in connection with the vaccination in 70 case reports, small series, and three clinical studies, including a large population-based, matched case-control study of 4.7 million people that found no association between GD and the COVID-19 vaccine [50-82]. Also, a meta-analysis of 21 publications comprising 57 post-vaccination GD cases concluded that causality was not established [218].
Another post-vaccination new-onset autoimmune condition that was reported in the literature is Type 1 Diabetes Mellitus (T1DM). The variety of clinical presentations included severe DKA in previously healthy individuals and conversion to T1DM in patients with prediabetes or T2DM conditions [179-190]. Pre-diabetic individuals were more likely to develop T1DM following vaccine administration. However, whether insulin resistance plays a part in post-vaccination DKA development is unclear. The onset of the summarized cases ranged from 1 day to 8 weeks post-vaccination, and the T1DM autoantibody positivity profile was variable. Given the existing evidence of deteriorated glycemic parameters following immunization in patients with diabetes, it still should be elucidated whether the vaccine is responsible for new-onset T1DM or post-vaccination immune response uncovers preexisting conditions in susceptible individuals.
A combination of physiological and environmental factors determines fertility; assessing fertility is challenging. Evaluating the vaccine's potentially harmful effect on female or male fertility is even more difficult. In most clinical studies, ovarian reserve markers and semen quality analysis were used as the primary assessment tools in female and male fertility, respectively. The summarized studies that evaluated the potential effect of the vaccines on female fertility registered no significant negative impact on ovarian reserve markers [143-154]. Most of these studies were conducted among women undergoing assisted reproduction cycles. Similarly, studies on male fertility showed no adverse effects of the vaccines on parameters of semen specimens [158-168].
Those findings were in agreement with a systematic review focusing on the literature's evidence about the vaccines' safety and the possible impact on fertility. In this study, the pre-and post-vaccination sperm progressive motility and concentration and the biochemical and clinical pregnancy rate did not differ among vaccinated and non-vaccinated groups [219].
Pituitary disorders were initially reported in the setting of SARS-CoV2 infection, followed by published clinical cases of hypophysitis, central diabetes insipidus, SIADH, pituitary apoplexy, and ACTH deficiency as rare adverse effects of the vaccination. The summarized cases of pituitary conditions are not very numerous, but perhaps the actual incidence is underreported and thus underestimated [85-104]. In addition, a delay in diagnosis can arise from overlapping symptoms related to pituitary hormone deficiencies and those experienced after vaccination. Therefore, reports on adverse events, particularly those related to rare disorders such as pituitary diseases, are essential to raise awareness and thus improve outcomes.
Hemorrhagic and non-hemorrhagic adrenal post-vaccination adverse events are rare phenomena but could be life-threatening. Cases of the adrenal crisis were described in this review, both in patients with existing adrenal insufficiency (AI) and in those after adrenal hemorrhage [115-132]. For patients with known AI, literature concerning post-vaccination glucocorticoid dose suggests increasing the maintenance dose in case of vaccine-related symptoms [116].
10. Conclusions
The summarized literature does not provide clear evidence of a direct linkage between the COVID-19 vaccination and endocrine adverse effects. The occurrence of not uncommon endocrine disorders in a population-wide immunization program setting may reflect the causality bias. Further studies should evaluate the association between endocrine conditions and COVID-19 vaccines. Furthermore, the data
presented does not challenge the safety and efficacy of available COVID-19 vaccines.
References
- World Health Organization Coronavirus (COVID-19) Dashboard. Available at: http://covid19.who.int.
- Kudlay D, Svistunov A. COVID-19 Vaccines: An Overview of Different Platforms. Bioengineering (Basel). 2022;9(2):72. Published 2022 February 12. [CrossRef]
- Gupta A, Madhavan MV, Sehgal K, et al. Extrapulmonary manifestations of COVID-19. Nat Med. 2020;26(7):1017-1032. [CrossRef]
- Zhao Y, Wu X. Influence of COVID-19 vaccines on endocrine system. Endocrine. 2022;78(2):241-246. [CrossRef]
- Ishay A, Shacham EC. Central diabetes insipidus: a late sequela of BNT162b2 SARS-CoV-2 mRNA vaccine?. BMC Endocr Disord. 2023;23(1):47. Published 2023 February 22. [CrossRef]
- Asghar N, Mumtaz H, Syed AA, et al. Safety, efficacy, and immunogenicity of COVID-19 vaccines; a systematic review. Immunol Med. 2022;45(4):225-237. [CrossRef]
- Dhamanti I, Suwantika AA, Adlia A, Yamani LN, Yakub F. Adverse Reactions of COVID-19 Vaccines: A Scoping Review of Observational Studies. Int J Gen Med. 2023;16:609-618. Published 2023 February 20. [CrossRef]
- Olivieri B, Betterle C, Zanoni G. Vaccinations and autoimmune diseases. Vaccines. 2021 Jul 22;9(8):815.
- Jena A, Mishra S, Deepak P, Kumar-M P, Sharma A, Patel YI, Kennedy NA, Kim AH, Sharma V, Sebastian S. Response to SARS-CoV-2 vaccination in immune mediated inflammatory diseases: systematic review and meta-analysis. Autoimmunity reviews. 2022 Jan 1;21(1):102927.
- Pezzaioli LC, Gatta E, Bambini F, et al. Endocrine system after 2 years of COVID-19 vaccines: A narrative review of the literature. Front Endocrinol (Lausanne). 2022;13:1027047. Published 2022 Nov 10. [CrossRef]
- Vojdani A, Vojdani E, Kharrazian D. Reaction of human monoclonal antibodies to SARS-CoV-2 proteins with tissue antigens: implications for autoimmune diseases. Frontiers in Immunology. 2021 Jan 19;11:3679.
- Iremli BG, Sendur SN, -Onliitlirk U. Three Cases of Subacute Thyroiditis Following SARS-CoV-2 Vaccine: Postvaccination ASIA Syndrome. J Clin Endocrinol Metab. 2021;106(9):2600-5.
- Jafarzadeh A, Nemati M, Jafarzadeh S, Nozari P, Mortazavi SMJ. Thyroid dysfunction following vaccination with COVID-19 vaccines: a basic review of the preliminary evidence. J Endocrinol Invest. 2022 Oct;45(10):1835-1863. Epub 2022 Mar 26. [CrossRef]
- Stasiak M, Lewiński A. New aspects in the pathogenesis and management of subacute thyroiditis. Reviews in Endocrine and Metabolic Disorders. 2021 Dec;22(4):1027-39.
- Şendur SN, Özmen F, Oğuz SH, İremli BG, Malkan Ü., Gürlek A, et al. Association of human leukocyte antigen genotypes with severe acute respiratory syndrome coronavirus 2 vaccine-induced subacute thyroiditis. Thyroid (2022) 32 (6):640–7. [CrossRef]
- Ie K, Ishizuka K, Sakai T, Motohashi I, Asai S, Okuse C. Subacute thyroiditis developing within 2 days of vaccination against COVID-19 with BNT162b2 mRNA. European Journal of Case Reports in Internal Medicine. 2023;10(1).
- Tomic AZ, Zafirovic SS, Gluvic ZM, et al. Subacute thyroiditis following COVID-19 vaccination: Case presentation. Antiviral Therapy. 2023;28(5).
- Franquemont S, Galvez J. Subacute Thyroiditis After mRNA vaccine for Covid-19. J Endocr Soc. 2021;5:A956-A7.
- Pujol A, Gomez LA, Gallegos C, Nicolau J, Sanchis P, Gonzalez-Freire M, et al. Thyroid as a target of adjuvant autoimmunity/inflammatory syndrome due to mRNA-based SARS-CoV2 vaccination: from Graves' disease to silent thyroiditis. J Endocrinol Invest. 2022;45(4):875-82.
- Saygili ES, Karakilic E. Subacute thyroiditis after inactive SARS-Co V-2 vaccine. BMJ Case Rep. 2021;14(10). 2021.
- Sahin Tekin M, Sayhsoy S, Yorulmaz G. Subacute thyroiditis following COVID-19 vaccination in a 67-year-old male patient: a case report. Hum Vaccin Immunother. 2021;17(11):4090-2.
- Bornemann C, Woyk K, Bouter C. Case Report: Two Cases of Subacute Thyroiditis Following SARS-CoV-2 Vaccination. Front Med (Lausanne). 2021;8:737142.
- Plaza-Enriquez L, Khatiwada P, Sanchez-Valenzuela M, Sikha A. A Case Report of Subacute Thyroiditis following mRNA COVID-19 Vaccine. Case Rep Endocrinol. 2021;2021:8952048.
- Siolos A, Gartzonika K, Tigas S. Thyroiditis following vaccination against COVID-19: Report of two cases and review of the literature. Metabol Open. 2021;12:100136.
- Schimmel J, Alba EL, Chen A, Russell M, Srinath R. Thyroiditis and Thyrotoxicosis After the SARS-CoV-2 mRNA Vaccine. Thyroid. 2021;31(9):1440.
- Oyibo, SO. Subacute Thyroiditis After Receiving the Adenovirus-Vectored Vaccine for Coronavirus Disease (COVID-19). Cureus. 2021;13(6):e16045.
- Ratnayake GM, Dworakowska D, Grossman AB. Can COVID-19 immunization cause subacute thyroiditis? Clin Endocrinol (Oxf). 2021.
- Chatzi S, Karampela A, Spiliopoulou C, Boutzios G. Subacute thyroiditis after SARS-CoV-2 vaccination: a report of two sisters and summary of the literature. Hormones (Athens). 2022;21(1):177-9.
- Jeeyavudeen MS, Patrick AW, Gibb FW, Dover AR. COVID-19 vaccine-associated subacute thyroiditis: an unusual suspect for de Quervain's thyroiditis. BMJ Case Rep. 2021;14(11).
- Kyriacou A, Ioakim S, Syed AA. COVID-19 vaccination and a severe pain in the neck. Eur J Intern Med. 2021;94:95-6.
- Soltanpoor P, Norouzi G. Subacute thyroiditis following COVID-19 vaccination. Clin Case Rep. 2021;9(10):e04812.
- Lee KA, Kim YJ, Jin HY. Thyrotoxicosis after COVID-19 vaccination: seven case reports and a literature review. Endocrine. 2021;74(3):470-2.
- Khan F, Brassill MJ. Subacute thyroiditis post-Pfizer-BioNTech mRNA vaccination for COVID-19. Endocrinol Diabetes Metab Case Rep. 2021;2021.
- Leber HM, Sant'Ana L, Konichi da Silva NR, Raio MC, Mazzeo TJMM, Endo CM, et al. Acute Thyroiditis and Bilateral Optic Neuritis following SARS-CoV-2 Vaccination with CoronaVac: A Case Report. Ocul Immunol Inflamm. 2021;29(6):1200-6.
- Sozen M, Topaloglu 0, etinarslan B, Selek A, Cantlirk Z, Gezer E, et al. COVID-19 mRNA vaccine may trigger subacute thyroiditis. Hum Vaccin Immunother. 2021;17(12):5120-5.
- Pandya M, Thota G, Wang X, Luo H. Thyroiditis after Coronavirus Disease 2019 (COVID-19) mRNA Vaccine: A Case Series. AACE Clin Case Rep. 2021.
- Sigstad E, Grnholt KK, Westerheim 0. Subacute thyroiditis after vaccination against SARS-CoV-2. Tidsskr Nor Laegeforen. 2021;141(2021-14).
- Gonzalez Lopez J, Martin Nifio I, Arana Molina C. Subacute thyroiditis after SARS-CoV-2 vaccination: report of two clinical cases. Med Clin (Bare). 2021.
- Rebollar, A.F. [SUBACUTE THYROIDITIS AFTER ANTI SARS-COV-2 (Ad5-nCoV) VACCINE]. Enferm Infecc Microbiol Clin. 2021. [CrossRef] [PubMed]
- Ippolito S, Gallo D, Rossini A, Patera B, Lanzo N, Fazzino GFM, et al. SARS-CoV-2 vaccine-associated subacute thyroiditis: insights from a systematic review. J Endocrinol Invest. 2022.
- Yorulmaz G, Sahin Tekin M. SARS-CoV-2 vaccine-associated subacute thyroiditis. J Endocrinol Invest. 2022.
- Patel KR, Cunnane ME, Deschler DG. SARS-CoV-2 vaccine-induced subacute thyroiditis. Am J Otolaryngol. 2022;43(1):103211.
- Pla Peris B, Merchante Alfaro A, Maravall Royo FJ, Abellan Galiana P, Perez Naranjo S, Gonzalez Boillos M. Thyrotoxicosis following SARS-COV-2 vaccination: a case series and discussion. J Endocrinol Invest. 2022;45(5): 1071-7.
- Bostan H, Unsal IO, Kizilgul M, Gul U, Sencar ME, Ucan B, et al. Two cases of subacute thyroiditis after different types of SARS-CoV-2 vaccination. Arch Endocrinol Metab. 2022;66(1):97-103.
- Jhon M, Lee SH, Oh TH, Kang HC. Subacute Thyroiditis After Receiving the mRNA COVID-19 Vaccine (Modema): The First Case Report and Literature Review in Korea. J Korean Med Sci. 2022;37(6):e39.
- Garcı́a M, Albizua-Madariaga I, Lertxundi U, Aguirre C. Subacute thyroiditis and COVID-19 vaccines: a case/non-case study. Endocrine (2022) 77:480–5.
- Topaloğlu, Ö. , Tekin S, Topaloğlu SN, Bayraktaroglu T. Differences in clinical aspects between subacute thyroiditis associated with COVID-19 vaccines and classical subacute thyroiditis. Horm Metab Res (2022) 54(6):380–8.
- Bostan H, Kayihan S, Calapkulu M, Hepsen S, Gul U, Ozturk Unsal I, et al. Evaluation of the diagnostic features and clinical course of COVID-19 vaccine-associated subacute thyroiditis. Hormones (Athens) (2022) 21:447–55.
- Batman A, Yazıcı D, Dikbaş O, Ağbaht K, Saygılı ES, Demirci I, Bursa N, Ayas G, Anıl C, Cesur M, Korkmaz FN. Subacute THYROiditis Related to SARS-CoV-2 VAccine and Covid-19 (THYROVAC Study): A Multicenter Nationwide Study. The Journal of Clinical Endocrinology & Metabolism. 2023 Apr 25:dgad235.
- Zettinig G, Krebs M. Two further cases of Graves' disease following SARS-Cov-2 vaccination. J Endocrinol Invest. 2022;45(1):227-8.
- Vera-Lastra 0, Ordinola Navarro A, Cruz Domiguez MP, Medina G, Sanchez Valadez TI, Jara LJ. Two Cases of Graves' Disease Following SARS-CoV-2 Vaccination: An Autoimmune/Inflammatory Syndrome Induced by Adjuvants. Thyroid. 2021;31(9):1436-9.
- Lui DTW, Lee KK, Lee CH, Lee ACH, Hung IFN, Tan KCB. Development of Graves' Disease After SARS-CoV-2 mRNA Vaccination: A Case Report and Literature Review. Front Public Health. 2021;9:778964.
- Weintraub MA, Ameer B, Sinha Gregory N. Graves Disease Following the SARS-CoV-2 Vaccine: Case Series. J Investig Med High Impact Case Rep. 2021;9:23247096211063356.
- Sriphrapradang C, Shantavasinkul PC. Graves' disease following SARS-CoV-2 vaccination. Endocrine. 2021;74(3):473-4.
- Pierman G, Delgrange E, Jonas C. Recurrence of Graves' Disease (a Thl-type Cytokine Disease) Following SARS-CoV-2 mRNA Vaccine Administration: A Simple Coincidence? Eur J Case Rep Intern Med. 2021;8(9):002807.
- , Ferrari SM, Antonelli A, Fallahi P. A case of Graves' disease and type 1 diabetes mellitus following SARS-CoV-2 vaccination. J Autoimmun. 2021;125:102738.
- Goblirsch TJ, Paulson AE, Tashko G, Mekonnen AJ. Graves' disease following administration of second dose of SARS-CoV-2 vaccine. BMJ Case Rep. 2021;14(12).
- Sriphrapradang, C. Aggravation of hyperthyroidism after heterologous prime-boost immunization with inactivated and adenovirus-vectored SARS-CoV-2 vaccine in a patient with Graves' disease. Endocrine. 2021;74(2):226-7.
- Rubinstein TJ. Thyroid Eye Disease Following COVlD-19 Vaccine in a Patient With a History Graves' Disease: A Case Report. Ophthalmic Plast Reconstr Surg. 2021;37(6):e221-e3.
- di Filippo L, Castellino L, Giustina A. Occurrence and response to treatment of Graves' disease after COVID vaccination in two male patients. Endocrine. 2022;75(1):19-21.
- Taieb A, Sawsen N, Asma BA, Ghada S, Hamza E, Yosra H, et al. A rare case of grave's disease after SARS-CoV-2 vaccine: is it an adjuvant effect? Eur Rev Med Pharmacol Sci. 2022;26(7):2627-30.
- Chee YJ, Liew H, Hoi WH, Lee Y, Lim B, Chin HX, et al. SARS-CoV-2 mRNA Vaccination and Graves' Disease: a report of 12 cases and review of the literature. J Clin Endocrinol Metab. 2022.
- Patrizio A, Ferrari SM, Antonelli A, Fallahi P. Worsening of Graves' ophthalmopathy after SARS- CoV-2 mRNA vaccination. Autoimmun Rev. 2022:103096.
- Park KS, Fung SE, Ting M, Ozzello DJ, Yoon JS, Liu CY, et al. Thyroid eye disease reactivation associated with COVID-19 vaccination. Taiwan J Ophthalmol. 2022;12(1):93-6.
- Hamouche W, El Soufi Y, Alzaraq S, Okafor BV, Zhang F, Paras C. A case report of new onset graves' disease induced by SARS-CoV-2 infection or vaccine? J Clin Transl Endocrinol Case Rep. 2022;23:100104.
- Bostan H, Ucan B, Kizilgul M, Calapkulu M, Hepsen S, Gul U, et al. Relapsed and newly diagnosed Graves' disease due to immunization against COVID-19: A case series and review of the literature. J Autoimmun. 2022;128:102809.
- Singh G, Howland T. Graves' Disease Following COVID-19 Vaccination. Cureus. 2022;14(4):e24418.
- Chua MWJ. Graves' disease after COVID-19 vaccination. Ann Acad Med Singap. 2022;51(2): 127-8.
- Manta R, Martin C, Muls V, Poppe KG. New-onset Graves' disease following SARS-CoV-2 vaccination: a case report. Eur Thyroid J. 2022;11(4).
- Sakai M, Takao K, Kato T, Ito K, Kubota S, Hirose T, et al. Graves' Disease after Administration of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Vaccine in a Type 1 Diabetes Patient. Intern Med. 2022;61(10): 1561-5.
- Cuenca D, Aguilar-Soto M, Mercado M. A Case of Graves' Disease Following Vaccination with the Oxford-AstraZeneca SARS-CoV-2 Vaccine: Case Report and Review of the Literature. Eur J Case Rep Intern Med. 2022;9(4):003275.
- Ruggeri RM, Giovanellla L, Campenni A. SARS-CoV-2 vaccine may trigger thyroid autoimmunity: real-life experience and review of the literature. J Endocrinol Invest. 2022.
- Takedani K, Notsu M, Ishiai N, Asami Y, Uchida K, Kanasaki K. Graves' disease after exposure to the SARS-CoV-2 vaccine: a case report and review of the literature. BMC Endocrine Disorders. 2023 Jun 15;23(1):132.
- Nakamura F, Awaya T, Ohira M, Enomoto Y, Moroi M, Nakamura M. Graves' Disease after mRNA COVID-19 Vaccination, with the Presence of Autoimmune Antibodies Even One Year Later. Vaccines. 2023 May 3;11(5):934.
- Yan BC, Luo RR. Thyrotoxicosis in patients with a history of Graves' disease after SARS-CoV-2 vaccination (adenovirus vector vaccine): Two case reports. World Journal of Clinical Cases. 2023 Feb 2;11(5):1122.
- Yasuda, S., Suzuki, S., Yanagisawa, S. et al. HLA typing of patients who developed subacute thyroiditis and Graves' disease after SARS-CoV-2 vaccination: a case report. BMC Endocr Disord 23, 54 (2023).
- di Filippo L, Castellino L, Allora A, Frara S, Lanzi R, Perticone F, Valsecchi F, Vassallo A, Giubbini R, Rosen CJ, Giustina A. Distinct Clinical Features of Post-COVID-19 Vaccination Early-onset Graves’ Disease. The Journal of Clinical Endocrinology & Metabolism. 2023 Jan 1;108(1):107-13.
- Barajas Galindo DE, Ramos Bachiller B, González Roza L, García Ruiz de Morales JM, Sánchez Lasheras F, González Arnáiz E, Ariadel Cobo D, Ballesteros Pomar MD, Rodríguez IC. Increased incidence of Graves' disease during the SARS-CoV2 pandemic. Clinical Endocrinology. 2023 May;98(5):730-7.
- Gorshtein A, Turjeman A, Duskin-Bitan H, Leibovici L, Robenshtok E. Graves' disease following COVID-19 vaccination: a population-based, matched case-control study. J Clin Endocrinol Metab. 2023 Oct 10:dgad582. Epub ahead of print. PMID: 37815523. [CrossRef]
- Wong CH, Leung EKH, Tang LCK, et al. Effect of inactivated and mRNA COVID-19 vaccination on thyroid function among patients treated for hyperthyroidism. J Clin Endocrinol Metab 2023, 108(5): e76-e88.
- Peng K, Li X, Yang D, Chan SC, Zhou J, Wan EY, Chui CS, Lai FT, Wong CK, Chan EW, Leung WK. Risk of autoimmune diseases following COVID-19 and the potential protective effect from vaccination: a population-based cohort study. EClinicalMedicine. 2023 Sep 1;63.
- Wong CK, Lui DT, Xiong X, Chui CS, Lai FT, Li X, Wan EY, Cheung CL, Lee CH, Woo YC, Au IC. Risk of thyroid dysfunction associated with mRNA and inactivated COVID-19 vaccines: a population-based study of 2.3 million vaccine recipients. BMC medicine. 2022 Oct 14;20(1):339.
- Abeillon-du Payrat J, Grunenwald S, Gall E, Ladsous M, Raingeard I, Caron P. Graves' orbitopathy post-SARS-CoV-2 vaccines: report on six patients. J Endocrinol Invest. 2023;46(3):617-627. [CrossRef]
- Im Teoh JH, Mustafa N, Wahab N. New-onset Thyroid Eye Disease after COVID-19 Vaccination in a Radioactive Iodine-Treated Graves' Disease Patient: A Case Report and Literature Review. J ASEAN Fed Endocr Soc. 2023;38(1):125-130. Epub 2023 Feb 8. PMID: 37252417; PMCID: PMC10213383. [CrossRef]
- Aliberti L, Gagliardi I, Rizzo R, et al. Pituitary apoplexy and COVID-19 vaccination: a case report and literature review. Front Endocrinol (Lausanne). 2022;13:1035482. Published 2022 Nov 17. [CrossRef]
- Roncati L, Manenti A. Pituitary apoplexy following adenoviral vector-based COVID-19 vaccination. Brain Hemorrhages. 2023;4(1):27-29. [CrossRef]
- Zainordin NA, Hatta SFWM, Ab Mumin N, Shah FZM, Ghani RA. Pituitary apoplexy after COVID-19 vaccination: A case report. J Clin Transl Endocrinol Case Rep. 2022;25:100123. [CrossRef]
- Jaggi S, Jabbour S. Abstract #1001394: A Rare Endocrine Complication of the COVID-19 Vaccine, Endocrine Practice 2021; 27(6): S116-7.
- Ishay A, Shacham EC. Central diabetes insipidus: a late sequela of BNT162b2 SARS-CoV-2 mRNA vaccine?. BMC Endocr Disord. 2023;23(1):47. Published 2023 Feb 22. [CrossRef]
- Piñar-Gutiérrez A, Remón-Ruiz P, Soto-Moreno A. Case report: Pituitary apoplexy after COVID-19 vaccination. Med Clin (Engl Ed). 2022;158(10):498-499. [CrossRef]
- Fernandez, A., Karavitaki, N. and Wass, J.A.H. (2010), Prevalence of pituitary adenomas: a community-based, cross-sectional study in Banbury (Oxfordshire, UK). Clinical Endocrinology, 72: 377-382. [CrossRef]
- Briet C, Salenave S, Bonneville JF, Laws ER, Chanson P. Pituitary Apoplexy. Endocr Rev. 2015;36(6):622-645. [CrossRef]
- Bujawansa, S., Thondam, S.K., Steele, C., Cuthbertson, D.J., Gilkes, C.E., Noonan, C., Bleaney, C.W., MacFarlane, I.A., Javadpour, M. and Daousi, C. (2014), Presentation, management and outcomes in acute pituitary apoplexy: a large single-centre experience from the United Kingdom. Clin Endocrinol, 80: 419-424. [CrossRef]
- Taieb A, Mounira EE. Pilot Findings on SARS-CoV-2 Vaccine-Induced Pituitary Diseases: A Mini Review from Diagnosis to Pathophysiology. Vaccines (Basel). 2022;10(12):2004. Published 2022 Nov 24. [CrossRef]
- Taieb A, Asma BA, Mounira EE. Evidences that SARS-CoV-2 Vaccine-Induced apoplexy may not be solely due to ASIA or VITT syndrome', Commentary on Pituitary apoplexy and COVID-19 vaccination: A case report and literature review. Front Endocrinol (Lausanne). 2023 Jan 25;14:1111581. PMID: 36761192; PMCID: PMC9907727. [CrossRef]
- Prete A, Salvatori R. Hypophysitis. In: Feingold KR, Anawalt B, Boyce A, et al., eds. Endotext. South Dartmouth (MA): MDText.com, Inc.; October 15, 2021.
- Bouça B, Roldão M, Bogalho P, Cerqueira L, Silva-Nunes J. Central Diabetes Insipidus Following Immunization With BNT162b2 mRNA COVID-19 Vaccine: A Case Report. Front Endocrinol (Lausanne). 2022;13:889074. Published 2022 May 4. [CrossRef]
- Ach T, Kammoun F, Fekih HE, et al. Central diabetes insipidus revealing a hypophysitis induced by SARS-CoV-2 vaccine. Therapie. 2023;78(4):453-455. [CrossRef]
- Partenope C, Pedranzini Q, Petri A, Rabbone I, Prodam F, Bellone S. AVP deficiency (central diabetes insipidus) following immunization with anti-COVID-19 BNT162b2 Comirnaty vaccine in adolescents: A case report. Front Endocrinol (Lausanne). 2023;14:1166953. Published 2023 Apr 18. [CrossRef]
- Matsuo T, Okubo K, Mifune H, Imao T. Bilateral Optic Neuritis and Hypophysitis With Diabetes Insipidus 1 Month After COVID-19 mRNA Vaccine: Case Report and Literature Review. J Investig Med High Impact Case Rep. 2023;11:23247096231186046. [CrossRef]
- Murvelashvili N, Tessnow A. A Case of Hypophysitis Following Immunization With the mRNA-1273 SARS-CoV-2 Vaccine. J Investig Med High Impact Case Rep. 2021;9:23247096211043386. [CrossRef]
- Ankireddypalli AR, Chow LS, Radulescu A, Kawakami Y, Araki T. A Case of Hypophysitis Associated With SARS-CoV-2 Vaccination. AACE Clin Case Rep. 2022;8(5):204-209. [CrossRef]
- Morita S, Tsuji T, Kishimoto S, et al. Isolated ACTH deficiency following immunization with the BNT162b2 SARS-CoV-2 vaccine: a case report. BMC Endocr Disord. 2022;22(1):185. Published 2022 Jul 19. [CrossRef]
- Lindner G, Ryser B. The syndrome of inappropriate antidiuresis after vaccination against COVID-19: case report. BMC Infect Dis. 2021;21(1):1000. Published 2021 Sep 25. [CrossRef]
- Jara LJ, Vera-Lastra O, Mahroum N, Pineda C, Shoenfeld Y. Autoimmune post-COVID vaccine syndromes: does the spectrum of autoimmune/inflammatory syndrome expand?. Clin Rheumatol. 2022;41(5):1603-1609. [CrossRef]
- Liang Z, Zhu H, Wang X, et al. Adjuvants for Coronavirus Vaccines. Front Immunol. 2020;11:589833. Published 2020 Nov 6. [CrossRef]
- Cosentino M, Marino F. The spike hypothesis in vaccine-induced adverse effects: questions and answers. Trends Mol Med. 2022 Oct;28(10):797-799. Epub 2022 Sep 12. PMID: 36114089; PMCID: PMC9494717. [CrossRef]
- Boschi C, Scheim DE, Bancod A, et al. SARS-CoV-2 Spike Protein Induces Hemagglutination: Implications for COVID-19 Morbidities and Therapeutics and for Vaccine Adverse Effects. Int J Mol Sci. 2022;23(24):15480. Published 2022 Dec 7. [CrossRef]
- Kumar R, Guruparan T, Siddiqi S, et al. A case of adrenal infarction in a patient with COVID 19 infection. BJR Case Rep. 2020;6(3):20200075. Published 2020 Jun 4. [CrossRef]
- Leyendecker P, Ritter S, Riou M, et al. Acute adrenal infarction as an incidental CT finding and a potential prognosis factor in severe SARS-CoV-2 infection: a retrospective cohort analysis on 219 patients. Eur Radiol. 2021;31(2):895-900. [CrossRef]
- Frankel M, Feldman I, Levine M, et al. Bilateral Adrenal Hemorrhage in Coronavirus Disease 2019 Patient: A Case Report. J Clin Endocrinol Metab. 2020;105(12):dgaa487. [CrossRef]
- Álvarez-Troncoso J, Zapatero Larrauri M, Montero Vega MD, et al. Case Report: COVID-19 with Bilateral Adrenal Hemorrhage. Am J Trop Med Hyg. 2020;103(3):1156-1157. [CrossRef]
- Arlt W; Society for Endocrinology Clinical Committee. SOCIETY FOR ENDOCRINOLOGY ENDOCRINE EMERGENCY GUIDANCE: Emergency management of acute adrenal insufficiency (adrenal crisis) in adult patients. Endocr Connect. 2016;5(5):G1-G3. [CrossRef]
- Dineen R, Thompson CJ, Sherlock M. Adrenal crisis: prevention and management in adult patients. Ther Adv Endocrinol Metab. 2019;10:2042018819848218. Published 2019 Jun 13. [CrossRef]
- Maguire D, McLaren DS, Rasool I, Shah PM, Lynch J, Murray RD. ChAdOx1 SARS-CoV-2 vaccination: A putative precipitant of adrenal crises. Clin Endocrinol (Oxf). 2023;99(5):470-473. [CrossRef]
- ADSHG. Coronavirus vaccines and adrenal insufficiency. Bristol: Addison's Disease Self-Help Group. 2021. https://www.addisonsdisease.org.uk/coronavirus-vaccines.
- Katznelson L, Gadelha M. Glucocorticoid use in patients with adrenal insufficiency following administration of the COVID-19 vaccine: a pituitary society statement. Pituitary. 2021;24(2):143-145. [CrossRef]
- Pilli T, Dalmiglio C, Dalmazio G, et al. No need of glucocorticoid dose adjustment in patients with adrenal insufficiency before COVID-19 vaccine. Eur J Endocrinol. 2022;187(1):K7-K11. Published 2022 Jun 1. [CrossRef]
- Haji N Jr, Ali S, Wahashi EA, Khalid M, Ramamurthi K. Johnson and Johnson COVID-19 Vaccination Triggering Pheochromocytoma Multisystem Crisis. Cureus. 2021;13(9):e18196. Published 2021 Sep 22. [CrossRef]
- Markovic N, Faizan A, Boradia C, Nambi S. Adrenal Crisis Secondary to COVID-19 Vaccination in a Patient With Hypopituitarism. AACE Clin Case Rep. 2022;8(4):171-173. [CrossRef]
- Taylor P, Allen L, Shrikrishnapalasuriyar N, Stechman M, Rees A. Vaccine-induced thrombosis and thrombocytopenia with bilateral adrenal haemorrhage. Clin Endocrinol (Oxf). 2022;97(1):26-27.
- Varona JF, García-Isidro M, Moeinvaziri M, Ramos-López M, Fernández- Domínguez M. Primary adrenal insufficiency associated with Oxford-AstraZeneca ChAdOx1 nCoV-19 vaccine-induced immune thrombotic thrombocytopenia (VITT). Eur J Intern Med. 2021;91:90-92.
- Tews HC, Driendl SM, Kandulski M, et al. SARS-CoV-2 vaccine-induced immune thrombotic thrombocytopenia with venous thrombosis, pulmonary embolism, and adrenal haemorrhage: a case report with literature review. Vaccines. 2022;10(4):595.
- Blauenfeldt RA, Kristensen SR, Ernstsen SL, Kristensen CCH, Simonsen CZ, Hvas AM. Thrombocytopenia with acute ischemic stroke and bleeding in a patient newly vaccinated with an adenoviral vector-based COVID-19 vaccine. J Thromb Haemost. 2021 Jul;19(7):1771-1775. Epub 2021 May 5. PMID: 33877737; PMCID: PMC8250306. [CrossRef]
- D'Agostino V, Caranci F, Negro A, et al. A Rare Case of Cerebral Venous Thrombosis and Disseminated Intravascular Coagulation Temporally Associated to the COVID-19 Vaccine Administration. J Pers Med. 2021;11(4):285. Published 2021 Apr 8. [CrossRef]
- Al Rawahi B, BaTaher H, Jaffer Z, Al-Balushi A, Al-Mazrouqi A, Al-Balushi N. Vaccine-induced immune thrombotic thrombocytopenia following AstraZeneca (ChAdOx1 nCOV19) vaccine-A case report. Res Pract Thromb Haemost. 2021;5(6):e12578. Published 2021 Aug 24. [CrossRef]
- Graf A, Armeni E, Dickinson L, et al. Adrenal haemorrhage and infarction in the setting of vaccine-induced immune thrombocytopenia and thrombosis after SARS-CoV-2 (Oxford–AstraZeneca) vaccination. Endocrinol Diabetes Metab Case Rep. 2022;2022:21-0144.
- Efthymiadis A, Khan D, Pavord S, Pal A. A case of ChAdOx1 vaccine-induced thrombocytopenia and thrombosis syndrome leading to bilateral adrenal haemorrhage and adrenal insufficiency. Endocrinol Diabetes Metab Case Rep. Published online June 1, 2022. [CrossRef]
- Tha T, Martini I, Stefan E, Redla S. Bilateral adrenal haemorrhage with renal infarction after ChAdOx1 nCoV-19 AstraZeneca vaccination. BJR Case Rep. 2022;8(2):20210139. Published 2022 Jan 10. [CrossRef]
- Douxfils J, Vayne C, Pouplard C, et al. Fatal exacerbation of ChadOx1-nCoV-19-induced thrombotic thrombocytopenia syndrome after initial successful therapy with intravenous immunoglobulins - a rational for monitoring immunoglobulin G levels. Haematologica. 2021;106(12):3249-3252. Published 2021 Dec 1. [CrossRef]
- Boyle LD, Morganstein DL, Mitra I, Nogueira EF A rare case of multiple thrombi and left adrenal haemorrhage following COVID-19 vaccination. Endocr Abstr. 2021;74(NCC4).
- Ahmad S, Zaman N, Almajali K, Muhammadi A, Baburaj R, Akavarapu S. A novel case of bilateral adrenal hemorrhage and acute adrenal insufficiency due to VITT (vaccine induced thrombosis and thrombocytopenia) syndrome. Endocr Abstr. 2021;74(OC2).
- Elhassan YS, Iqbal F, Arlt W, et al. COVID-19-related adrenal hemorrhage: Multicentre UK experience and systematic review of the literature. Clin Endocrinol (Oxf). 2023;98(6):766-778. [CrossRef]
- Elalamy I, Gerotziafas G, Alamowitch S, et al. SARS-CoV-2 Vaccine and Thrombosis: An Expert Consensus on Vaccine-Induced Immune Thrombotic Thrombocytopenia. Thromb Haemost. 2021;121(8):982-991. [CrossRef]
- Marchandot B, Curtiaud A, Trimaille A, Sattler L, Grunebaum L, Morel O. Vaccine-induced immune thrombotic thrombocytopenia: current evidence, potential mechanisms, clinical implications, and future directions. Eur Heart J Open. 2021;1(2):oeab014. Published 2021 Aug 2. [CrossRef]
- Harville, EW. Invited Commentary: Vaccines and Fertility—Why Worry? American Journal of Epidemiology. 2023 Feb;192(2):154-7.
- Mobaraki A, Stetter C, Kunselman AR, Estes SJ. COVID-19 Vaccination Hesitancy in Women Who Desire Future Fertility/Pregnancy. J Gynecol Clin Obstet Reprod Med. 2023;1(2):48-65.
- Morris RS. SARS-CoV-2 spike protein seropositivity from vaccination or infection does not cause sterility. F S Rep. 2021 Sep;2(3):253-255. Epub 2021 Jun 2. PMID: 34095871; PMCID: PMC8169568. [CrossRef]
- Coulam CB, Roussev RG. Increasing circulating T-cell activation markers are linked to subsequent implantation failure after transfer of in vitro fertilized embryos. American Journal of Reproductive Immunology. 2003 Oct;50(4):340-5.
- Moolhuijsen LM, Visser JA. Anti-Müllerian hormone and ovarian reserve: update on assessing ovarian function. The Journal of Clinical Endocrinology & Metabolism. 2020 Nov;105(11):3361-73.
- Dellino M, Lamanna B, Vinciguerra M, Tafuri S, Stefanizzi P, Malvasi A, et al. SARS-CoV-2 vaccines and adverse effects in gynecology and obstetrics: the first italian retrospective study. Int J Environ Res Public Health 2022:19.
- Kolatorova L, Adamcova K, Vitku J, Horackova L, Simkova M, Hornova M, et al.COVID-19, vaccination, and female fertility in the Czech Republic. Int J Mol Sci 2022;23:10909.
- Senkaya AR, Çil Z, Keskin ¨O, Günes¸ ME, ¨Oztekin DC. CoronaVac vaccine does not affect ovarian reserve. Ginekol Pol 2023;94:298–302.
- Xu Z, Wu Y, Lin Y, Cao M, Liang Z, Li L, et al. Effect of inactivated COVID-19 vaccination on intrauterine insemination cycle success: a retrospective cohort study. Frontiers. Public Health 2022:10.
- Huang J, Xia L, Lin J, Liu B, Zhao Y, Xin C, et al. No effect of inactivated SARS-CoV- 2 vaccination on in vitro fertilization outcomes: a propensity score-matched study. J Inflamm Res 2022:839–49.
- Mohr-Sasson A, Haas J, Abuhasira S, Sivan M, Doitch Amdurski H, Dadon T, et al. The effect of Covid-19 mRNA vaccine on serum anti-Müllerian hormone levels. Hum Reprod 2022;37:534–41.
- Yildiz E, Timur B, Guney G, Timur H. Does the SARS-CoV-2 mRNA vaccine damage the ovarian reserve? Medicine (Baltimore). 2023 May 19;102(20):e33824.
- Kumbasar S, Salman S, Çakmak GN, Gencer FK, Sicakyüz LS, Kumbasar AN. Effect of mRNA COVID-19 vaccine on ovarian reserve of women of reproductive age. Ginekologia Polska. 2023 Oct 18.
- Huang J, Guan T, Tian L, Xia L, Xu D, Wu X, Huang L, Chen M, Fang Z, Xiong C, Nie L. Impact of inactivated COVID-19 vaccination on female ovarian reserve: a propensity score-matched retrospective cohort study. Frontiers in Immunology. 2023;14.
- Horowitz E, Mizrachi Y, Herman HG, Marcuschamer EO, Shalev A, Farhi J, et al. The effect of SARS-CoV-2 mRNA vaccination on AMH concentrations in infertile women. Reprod Biomed Online 2022;45:779–84.
- Odeh-Natour R, Shapira M, Estrada D, Freimann S, Tal Y, Atzmon Y, et al. Does mRNA SARS-CoV-2 vaccine in the follicular fluid impact follicle and oocyte performance in IVF treatments? Am J Reprod Immunol 2022;87:e13530.
- Orvieto R, Noach-Hirsh M, Segev-Zahav A, Haas J, Nahum R, Aizer A. Does mRNA SARS-CoV-2 vaccine influence patients' performance during IVF-ET cycle? Reprod Biol Endocrinol 2021;19:69.
- Jacobs E, Summers K, Sparks A, Mejia R. Fresh embryo transfer cycle characteristics and outcomes following in vitro fertilization via intracytoplasmic sperm injection among patients with and without COVID-19 vaccination. JAMA Netw Open 2022;5:e228625 -e.
- Requena A, Vergara V, Gonz´alez-Ravina C, Ruiz ME, Cruz M. The type of SARS-CoV-2 vaccine does not affect ovarian function in assisted reproduction cycle. Fertil Steril 2023;119:618–23.
- Yland JJ, Wesselink AK, Regan AK, Hatch EE, Rothman KJ, Savitz DA, Wang TR, Huybrechts KF, Hernández-Díaz S, Eisenberg ML, Wise LA. A prospective cohort study of preconception COVID-19 vaccination and miscarriage. Human Reproduction. 2023 Oct 20:dead211.
- Skakkebaek NE, Rajpert-De Meyts E, Buck Louis GM, Toppari J, Andersson AM, Eisenberg ML, Jensen TK, Jørgensen N, Swan SH, Sapra KJ, Ziebe S. Male reproductive disorders and fertility trends: influences of environment and genetic susceptibility. Physiological reviews. 2016 Jan;96(1):55-97.
- Lewis SE. Is sperm evaluation useful in predicting human fertility? Reproduction. 2007;134:31–40.
- Gonzalez DC, Nassau DE, Khodamoradi K, Ibrahim E, Blachman-Braun R, Ory J, et al. Sperm parameters before and after COVID-19 mRNA vaccination. JAMA (2021) 326(3):273–4. [CrossRef]
- Barda S, Laskov I, Grisaru D, Lehavi O, Kleiman S, Wenkert A, et al. The impact of COVID-19 vaccine on sperm quality. Int J Gynaecol Obstet (2022) 158:116–20. [CrossRef]
- Lifshitz D, Haas J, Lebovitz O, Raviv G, Orvieto R, Aizer A. Does mRNA SARS-CoV-2 vaccine detrimentally affect male fertility, as reflected by semen analysis? Reprod BioMed Online (2022) 44(1):145–9. [CrossRef]
- Olana S, Mazzilli R, Salerno G, Zamponi V, Tarsitano MG, Simmaco M, et al. 4BNT162b2 mRNA COVID-19 vaccine and semen: What do we know? Andrology (2022) 10:1023–9. [CrossRef]
- Abd ZH, Muter SA, Saeed RAM, Ammar O. Effects of covid-19 vaccination on different semen parameters. Basic Clin Androl (2022) 32(1):13. [CrossRef]
- Gat I, Kedem A, Dviri M, Umanski A, Levi M, Hourvitz A, et al. Covid-19 vaccination BNT162b2 temporarily impairs semen concentration and total motile count among semen donors. Andrology (2022) 10:1016–22. [CrossRef]
- Zhu H, Wang X, Zhang F, Zhu Y, Du MR, Tao ZW, et al. Evaluation of inactivated COVID-19 vaccine on semen parameters in reproductive-age males: a retrospective cohort study. Asian J Androl (2022) 24:441–4. [CrossRef]
- Dong Y, Li X, Li Z, Zhu Y, Wei Z, He J, Cheng H, Yang A, Chen F. Effects of inactivated SARS-CoV-2 vaccination on male fertility: A retrospective cohort study. Journal of Medical Virology. 2023 Jan;95(1):e28329.
- Reschini M, Pagliardini L, Boeri L, Piazzini F, Bandini V, Fornelli G, et al. COVID-19 vaccination does not affect reproductive health parameters in men. Front Public Health (2022) 10:839967. [CrossRef]
- Safrai M, Herzberg S, Imbar T, Reubinoff B, Dior U, Ben-Meir A. The BNT162b2 mRNA COVID-19 vaccine does not impair sperm parameters. Reprod BioMed Online (2022) 44(4):685–8. [CrossRef]
- Xia W, Zhao J, Hu Y, Fang L, Wu S. Investigate the effect of COVID-19 inactivated vaccine on sperm parameters and embryo quality in vitro fertilization. Andrologia (2022) 54(6):e14483. [CrossRef]
- Chillon TS, Demircan K, Weiss G, Minich WB, Schenk M, Schomburg L. Detection of antibodies to SARS-CoV-2 after vaccination in seminal plasma and their association to sperm parameters. International Journal of Infectious Diseases. 2023 May 1;130:161-5.
- Hulme KD, Gallo LA, Short KR. Influenza Virus and Glycemic Variability in Diabetes: A Killer Combination?. Front Microbiol. 2017;8:861. Published 2017 May 22. [CrossRef]
- Akamine CM, El Sahly HM. Messenger ribonucleic acid vaccines for severe acute respiratory syndrome coronavirus-2 - a review. Transl Res. 2022 Apr;242:1-19. Epub 2021 Dec 23. PMID: 34954088; PMCID: PMC8695521. [CrossRef]
- Marfella, R., Sardu, C., D’Onofrio, N. et al. Glycaemic control is associated with SARS-CoV-2 breakthrough infections in vaccinated patients with type 2 diabetes. Nat Commun 13, 2318 (2022). [CrossRef]
- Cieślewicz A, Dudek M, Krela-Kaźmierczak I, Jabłecka A, Lesiak M, Korzeniowska K. Pancreatic Injury after COVID-19 Vaccine-A Case Report. Vaccines (Basel). 2021;9(6):576. Published 2021 Jun 1. [CrossRef]
- Boskabadi SJ, Ala S, Heydari F, Ebrahimi M, Jamnani AN. Acute pancreatitis following COVID-19 vaccine: A case report and brief literature review. Heliyon. 2023 Jan;9(1):e12914. Epub 2023 Jan 14. PMID: 36685416; PMCID: PMC9840226. [CrossRef]
- Cacdac R, Jamali A, Jamali R, Nemovi K, Vosoughi K, Bayraktutar Z. Acute pancreatitis as an adverse effect of COVID-19 vaccination. SAGE Open Med Case Rep. 2022;10:2050313X221131169. Published 2022 Oct 24. [CrossRef]
- Guo M, Liu X, Chen X, Li Q. Insights into new-onset autoimmune diseases after COVID-19 vaccination. Autoimmun Rev. 2023;22(7):103340. [CrossRef]
- Aida K, Nishida Y, Tanaka S, et al. RIG-I- and MDA5-initiated innate immunity linked with adaptive immunity accelerates beta-cell death in fulminant type 1 diabetes. Diabetes. 2011;60(3):884-889. [CrossRef]
- Yin X, Riva L, Pu Y, et al. MDA5 Governs the Innate Immune Response to SARS-CoV-2 in Lung Epithelial Cells. Cell Rep. 2021;34(2):108628. [CrossRef]
- He YF, Ouyang J, Hu XD, Wu N, Jiang ZG, Bian N, Wang J. Correlation between COVID-19 vaccination and diabetes mellitus: A systematic review. World J Diabetes 2023; 14(6): 892-918.
- Bleve, E., Venditti, V., Lenzi, A. et al. COVID-19 vaccine and autoimmune diabetes in adults: report of two cases. J Endocrinol Invest 45, 1269–1270 (2022). [CrossRef]
- Moon H, Suh S, Park MK. Adult-Onset Type 1 Diabetes Development Following COVID-19 mRNA Vaccination. J Korean Med Sci. 2023;38(2):e12. Published 2023 Jan 9. [CrossRef]
- Aydoğan Bİ, Ünlütürk U, Cesur M. Type 1 diabetes mellitus following SARS-CoV-2 mRNA vaccination. Endocrine. 2022;78(1):42-46. [CrossRef]
- Sakurai K, Narita D, Saito N, et al. Type 1 diabetes mellitus following COVID-19 RNA-based vaccine. J Diabetes Investig. 2022;13(7):1290-1292. [CrossRef]
- Yano M, Morioka T, Natsuki Y, Sasaki K, Kakutani Y, Ochi A, Yamazaki Y, Shoji T, Emoto M. New-onset Type 1 Diabetes after COVID-19 mRNA Vaccination. Intern Med 2022; 61: 1197-1200 [PMID: 35135929]. [CrossRef]
- Sasaki K, Morioka T, Okada N, Natsuki Y, Kakutani Y, Ochi A, Yamazaki Y, Shoji T, Ohmura T, Emoto M. New-onset fulminant type 1 diabetes after severe acute respiratory syndrome coronavirus 2 vaccination: A case report. J Diabetes Investig 2022; 13: 1286-1289 [PMID: 35167186]. [CrossRef]
- Kshetree B, Lee J, Acharya S. COVID-19 Vaccine-Induced Rapid Progression of Prediabetes to Ketosis-Prone Diabetes Mellitus in an Elderly Male. Cureus 2022; 14: e28830 [PMID: 36225440]. [CrossRef]
- Sasaki H, Itoh A, Watanabe Y, et al. Newly developed type 1 diabetes after coronavirus disease 2019 vaccination: A case report. J Diabetes Investig. 2022;13(6):1105-1108. [CrossRef]
- Sato T, Kodama S, Kaneko K, Imai J, Katagiri H. Type 1 Diabetes Mellitus Associated with Nivolumab after Second SARS-CoV-2 Vaccination, Japan. Emerg Infect Dis 2022; 28: 1518-1520 [PMID: 35468049]. [CrossRef]
- Ohuchi K, Amagai R, Tamabuchi E, Kambayashi Y, Fujimura T. Fulminant type 1 diabetes mellitus triggered by coronavirus disease 2019 vaccination in an advanced melanoma patient given adjuvant nivolumab therapy. J Dermatol 2022; 49: e167-e168 [PMID: 35014070]. [CrossRef]
- Patrizio A, Ferrari SM, Antonelli A, Fallahi P. A case of Graves' disease and type 1 diabetes mellitus following SARS-CoV-2 vaccination. J Autoimmun. 2021;125:102738. [CrossRef]
- Graus, F., Saiz, A. & Dalmau, J. GAD antibodies in neurological disorders — insights and challenges. Nat Rev Neurol 16, 353–365 (2020). [CrossRef]
- Fiorina P. GABAergic system in β-cells: from autoimmunity target to regeneration tool. Diabetes. 2013 Nov;62(11):3674-6. PMID: 24158998; PMCID: PMC3806604. [CrossRef]
- Tohid Hassaan, Anti-glutamic acid decarboxylase antibody positive neurological syndromes Neurosciences 2016; Vol. 21 (3): 215-222. [CrossRef]
- Tridgell DM, Spiekerman C, Wang RS, Greenbaum CJ. Interaction of onset and duration of diabetes on the percent of GAD and IA-2 antibody-positive subjects in the type 1 diabetes genetics consortium database. Diabetes Care. 2011;34(4):988-993. [CrossRef]
- Ramos EL, Dayan CM, Chatenoud L, et al. Teplizumab and β-Cell Function in Newly Diagnosed Type 1 Diabetes. N Engl J Med. 2023;389(23):2151-2161. [CrossRef]
- Doering TA, Crawford A, Angelosanto JM, Paley MA, Ziegler CG, Wherry EJ. Network analysis reveals centrally connected genes and pathways involved in CD8+ T cell exhaustion versus memory. Immunity. 2012; 37:1130–1144. [PubMed: 23159438].
- McKinney EF, Lee JC, Jayne DRW, Lyons PA, Smith KGC. T-cell exhaustion, co-stimulation and clinical outcome in autoimmunity and infection. Nature. 2015; 523:612–616. [PubMed: 26123020].
- Long SA, Thorpe J, DeBerg HA, et al. Partial exhaustion of CD8 T cells and clinical response to teplizumab in new-onset type 1 diabetes. Sci Immunol. 2016;1(5):eaai7793. [CrossRef]
- Zhu X, Gebo KA, Abraham AG, et al. Dynamics of inflammatory responses after SARS-CoV-2 infection by vaccination status in the USA: a prospective cohort study. Lancet Microbe. 2023;4(9):e692-e703. [CrossRef]
- Ostrowski SR, Søgaard OS, Tolstrup M, et al. Inflammation and Platelet Activation After COVID-19 Vaccines - Possible Mechanisms Behind Vaccine-Induced Immune Thrombocytopenia and Thrombosis. Front Immunol. 2021;12:779453. Published 2021 Nov 23. [CrossRef]
- Deniz Ç, Altunan B, Ünal A. Anti-GAD Encephalitis Following COVID-19 Vaccination: A Case Report. Noro Psikiyatr Ars. 2023;60(3):283-287. Published 2023 Aug 3. [CrossRef]
- Miyauchi M, Toyoda M, Zhang J, et al. Nivolumab-induced fulminant type 1 diabetes with precipitous fall in C-peptide level. J Diabetes Investig. 2020;11(3):748-749. [CrossRef]
- Akturk HK, Kahramangil D, Sarwal A, Hoffecker L, Murad MH, Michels AW. Immune checkpoint inhibitor-induced Type 1 diabetes: a systematic review and meta-analysis. Diabet Med. 2019;36(9):1075-1081. [CrossRef]
- Lee S, Morgan A, Shah S, Ebeling PR. Rapid-onset diabetic ketoacidosis secondary to nivolumab therapy. Endocrinol Diabetes Metab Case Rep. 2018;2018:18-0021. Published 2018 Apr 27. [CrossRef]
- Lo Preiato V, Salvagni S, Ricci C, Ardizzoni A, Pagotto U, Pelusi C. Diabetes mellitus induced by immune checkpoint inhibitors: type 1 diabetes variant or new clinical entity? Review of the literature. Rev Endocr Metab Disord. 2021;22(2):337-349. [CrossRef]
- Gauci, ML., Laly, P., Vidal-Trecan, T. et al. Autoimmune diabetes induced by PD-1 inhibitor—retrospective analysis and pathogenesis: a case report and literature review. Cancer Immunol Immunother 66, 1399–1410 (2017). [CrossRef]
- Stamatouli AM, Quandt Z, Perdigoto AL, Clark PL, Kluger H,Weiss SA, et al. Collateral Damage: Insulin-Dependent Diabetes Induced With Checkpoint Inhibitors. Diabetes (2018) 67(8):1471–80. [CrossRef]
- Godwin JL, Jaggi S, Sirisena I, Sharda P, Rao AD, Mehra R, et al. Nivolumab-Induced Autoimmune Diabetes Mellitus Presenting as Diabetic Ketoacidosis in a Patient With Metastatic Lung Cancer. J Immunother Cancer (2017) 5(1):1–7. [CrossRef]
- Lowe JR, Perry DJ, Salama AKS, Mathews CE, Moss LG, Hanks BA. Genetic Risk Analysis of a Patient With Fulminant Autoimmune Type 1 Diabetes Mellitus Secondary to Combination Ipilimumab and Nivolumab Immunotherapy. J Immunother Cancer (2016) 4(1):1–8. [CrossRef]
- Wu L, Tsang VHM, Sasson SC, et al. Unravelling Checkpoint Inhibitor Associated Autoimmune Diabetes: From Bench to Bedside. Front Endocrinol (Lausanne). 2021;12:764138. Published 2021 Nov 5. [CrossRef]
- Cohen Tervaert JW, Martinez-Lavin M, Jara LJ, et al. Autoimmune/inflammatory syndrome induced by adjuvants (ASIA) in 2023. Autoimmun Rev. 2023;22(5):103287. [CrossRef]
- Watad A, Bragazzi NL, McGonagle D, et al. Autoimmune/inflammatory syndrome induced by adjuvants (ASIA) demonstrates distinct autoimmune and autoinflammatory disease associations according to the adjuvant subtype: Insights from an analysis of 500 cases. Clin Immunol. 2019;203:1-8. [CrossRef]
- 213. Vera-Lastra O, Medina G, Cruz-Dominguez Mdel P, Jara LJ, Shoenfeld Y. Autoimmune/inflammatory syndrome induced by adjuvants (Shoenfeld's syndrome): clinical and immunological spectrum. Expert Rev Clin Immunol. 2013;9(4):361-373. [CrossRef]
- Chen Y, Xu Z, Wang P, Li XM, Shuai ZW, Ye DQ, et al. New-onset autoimmune phenomena post-COVID-19 vaccination. Immunology 2022;165(4):386–401. [Epub 2022 Jan 7]. [CrossRef]
- Bragazzi NL, Hejly A, Watad A, Adawi M, Amital H, Shoenfeld Y. ASIA syndrome and endocrine autoimmune disorders. Best Pract Res Clin Endocrinol Metab. 2020;34(1):101412. [CrossRef]
- Di Fusco M, Lin J, Vaghela S, Lingohr-Smith M, Nguyen JL, Scassellati Sforzolini T, Judy J, Cane A, Moran MM. COVID-19 vaccine effectiveness among immunocompromised populations: a targeted literature review of real-world studies. Expert Rev Vaccines. 2022 Apr;21(4):435-451. Epub 2022 Feb 3. PMID: 35112973; PMCID: PMC8862165. [CrossRef]
- Mirza SA, Sheikh AAE, Barbera M, et al. COVID-19 and the Endocrine System: A Review of the Current Information and Misinformation. Infect Dis Rep. 2022;14(2):184-197. Published 2022 Mar 11. [CrossRef]
- Triantafyllidis KK, Giannos P, Stathi D, Kechagias KS. Graves' disease following vaccination against SARS-CoV-2: A systematic review of the reported cases. Front Endocrinol (Lausanne). 2022;13:938001.
- Zaçe D, La Gatta E, Petrella L, Di Pietro ML. The impact of COVID-19 vaccines on fertility-A systematic review and metanalysis. Vaccine. 2022 Sep 12.

Table 1.
Literature summary on the effect of SARS-CoV-2 vaccines on thyroid function
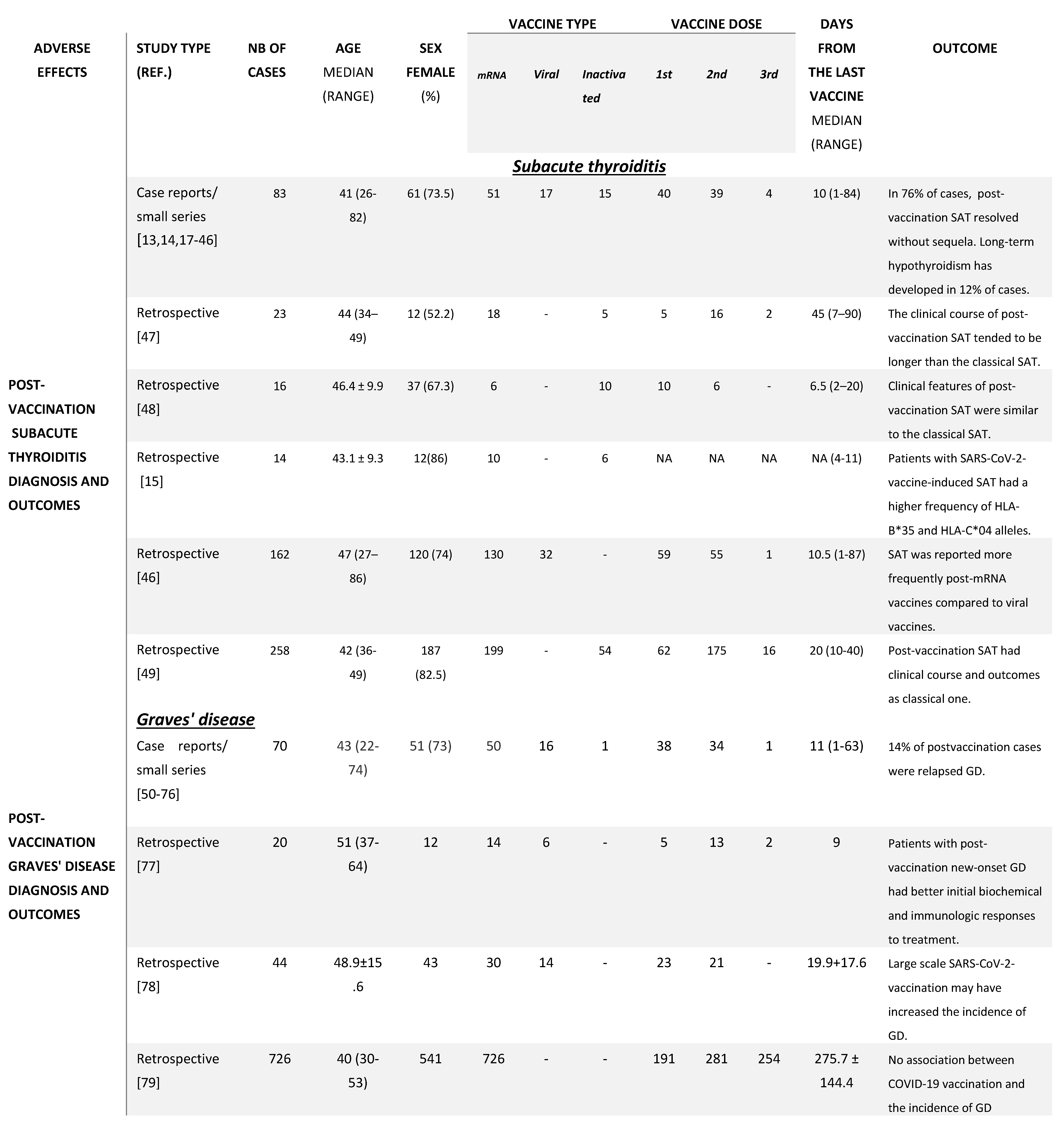
Table 2.
Literature summary on the effect of SARS-CoV-2 vaccines on the reproductive system
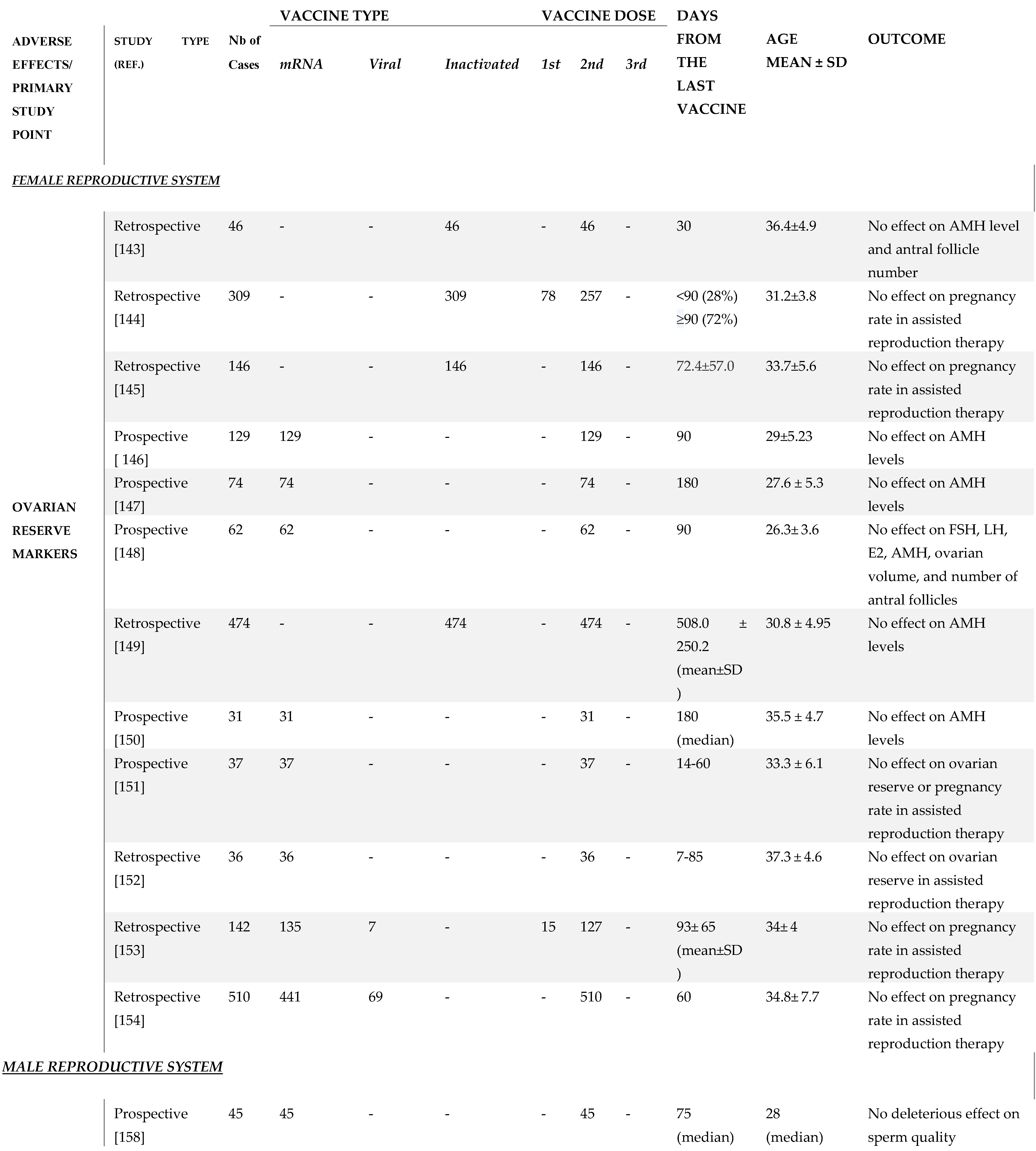
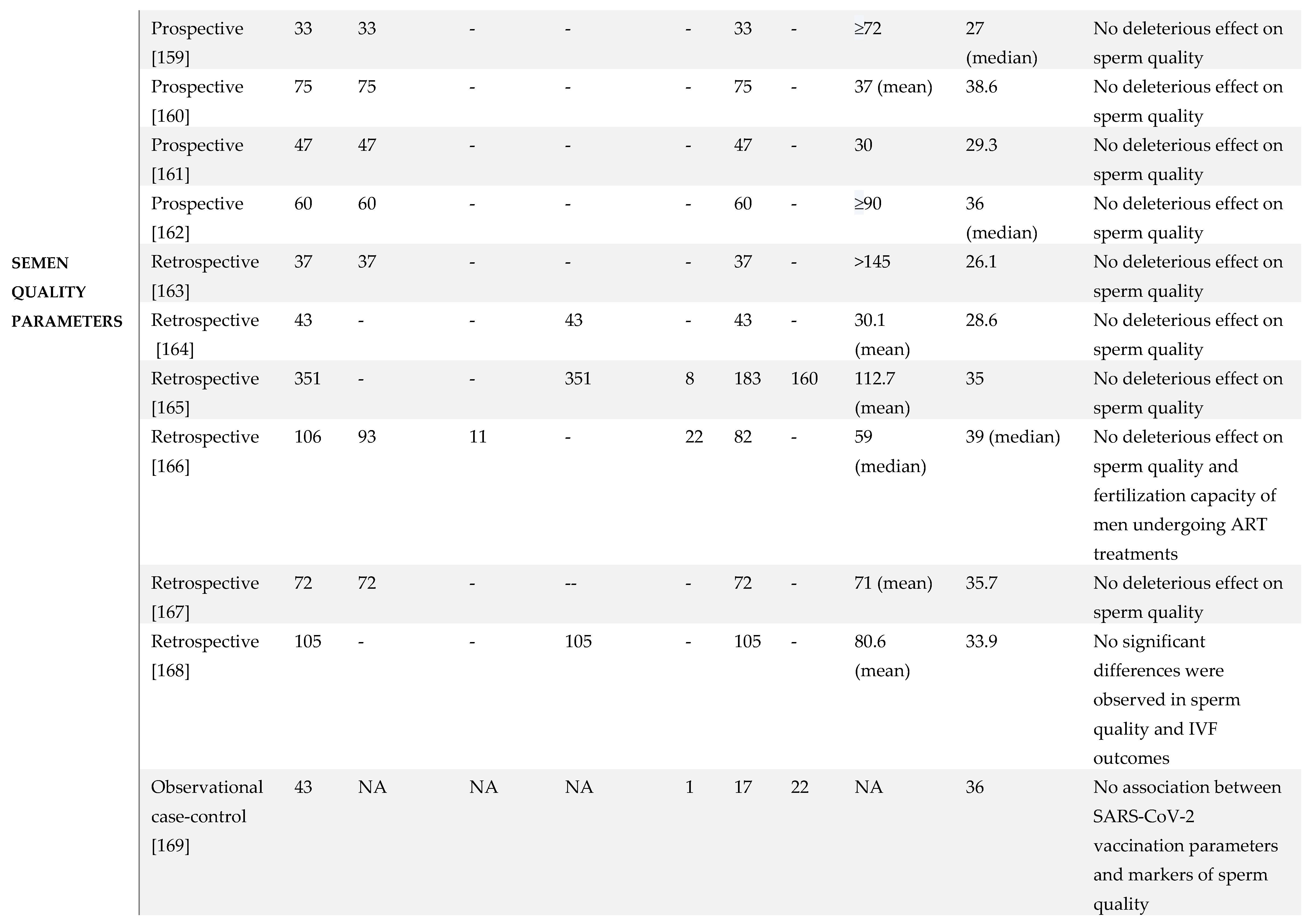
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



