Submitted:
23 February 2024
Posted:
26 February 2024
You are already at the latest version
Abstract
LC-SPIK is a liver cancer-specific isoform of Serine Protease Inhibitor Kazal and has been proposed as a new biomarker for the detection of HCC given its unique 3-D structure which differs from normal pancreatic SPIK. An ELISA technology based on its unique structure was developed to use LC-SPIK as an effective biomarker for the clinical diagnosis of HCC. AFP, the most widely used biomarker for HCC surveillance currently, suffers from poor clinical performance, especially in the detection of early-stage HCC. In one case-control study, which included 164 HCC patients and 324 controls, LC-SPIK had an AUC of 0.87 compared to only 0.70 for AFP in distinguishing HCC from liver disease controls (cirrhosis, HBV/HCV). LC-SPIK also performed significantly better than AFP for the 81 patients with early-stage HCC (BCLC stage 0 and A), with an AUC of 0.85 compared to only 0.61 for AFP. Cirrhosis is the major risk factor for HCC, about 80% of patients with newly diagnosed HCC have preexisting cirrhosis. LC-SPIK’s clinical performance was also studied in HCC patients with viral and non-viral cirrhosis including cirrhosis caused by nonalcoholic fatty liver disease (NAFLD) and alcoholic liver disease (ALD). In a total of 163 viral cirrhosis patients with 93 HCC patients (50 early-stage), LC-SPIK had an AUC of 0.85, while AFP had an AUC of 0.70. For patients with early-stage HCC, LC-SPIK had a similar AUC of 0.83, while AFP had an AUC of only 0.60. For 120 patients with nonviral cirrhosis, including 62 HCC (23 early-stage) patients, LC-SPIK had an AUC of 0.84 while AFP had an AUC of only 0.72. For the 23 patients with early-stage HCC, LC-SPIK had a similar AUC of 0.83, while the AUC for AFP decreased to 0.65. All these results suggest that LC-SPIK has significantly better performance in the detection of HCC than AFP in all etiologies of liver diseases. In addition, LC-SPIK accurately detected the presence of HCC in 71%-91% of HCC patients with false-negative AFP test results in viral associated HCC and non-viral associated HCC.
Keywords:
Biomarker
; HCC (Hepatocellular Carcinoma)
; LC-SPIK (Liver Cancer specific Serine Protease Inhibitor Kazal)
; AFP (Alpha-Fetoprotein)
; NAFLD (nonalcoholic fatty liver disease)
1. Introduction
Primary HCC (Hepatocellular carcinoma) is the most common and deadliest form of liver cancer, causing hundreds of thousands of deaths worldwide each year.[1,2,3,4] It usually remains undetected until its later stages, at which point patients face a 5-year survival rate of less than 15%. However, the survival rate can be over 70% if the HCC is detected early. [2,5,6,7].
Currently, HCC surveillance generally includes a liver ultrasound (US) with or without AFP (alpha fetoprotein) biomarker testing.[8,9,10] US detection is noninvasive but it is operator and equipment dependent, and it is often not sensitive enough to detect HCC in its critical early stages, with an estimated sensitivity below 50% [11,12]. Moreover, US is less accurate in patients with high BMI or those with non-alcoholic fatty liver disease [NAFLD) and/or a coarse liver echotexture.[13] All these factors limit the utility of ultrasound in HCC surveillance. A biomarker test which utilizes patient serum would be significantly more convenient and cheaper, but currently there are no effective HCC biomarkers available for clinical use. AFP, the most commonly used biomarker today, only has an estimated 41–65% sensitivity and 80–90% specificity for HCC. [14,15] AFP is even less accurate in detecting early-stage HCC with a sensitivity of less than 40%.[14,16] Additionally, nearly 40% of patients with HCC have undetectable AFP levels in their sera, [15, 17-19] and patients with chronic liver diseases may have falsely elevated AFP levels during active inflammation.[20] These factors limit the application of AFP in HCC surveillance. Therefore, development an accurate and cost-effective biomarker for HCC surveillance remains a significant unmet need. Recently, a protein called Liver-specific Serine Protease Inhibitor Kazal (LC-SPIK), which is secreted specifically by liver cancer cells in blood, has been identified. LC-SPIK is a liver cancer-specific isoform of Serine Protease Inhibitor Kazal (SPIK/SPINK). Here, we will evaluate use of LC-SPIK as a new biomarker for detection of HCC.
2. SPIK and the development of cancer
SPIK is a small protein with 79 amino acids and is also called PSTI (pancreas secretory trypsin inhibitor) and TATI (tumor-associated trypsin inhibitor).[21,22] Normally, SPIK has no or limited activity in liver tissues or any tissues besides the pancreas. Numerous studies have reported that the expression of SPIK may be elevated in cancer such as HCC,[23,24,25,26,27,28,29] and that high expression of SPIK is closely related to the progression of HCC.[25,29]
The reason that over-expression of SPIK triggers cancer development was studied. The most compelling evidence comes from the studies of function of SPIK that describe SPIK to be activated as a reactant during inflammation.[30,31,32,33] For example, SPIK was activated in rat liver cells to counter turpentine-induced liver inflammation.[33] SPIK was also activated in response to inflammatory cytokines during human viral hepatitis.[34] Lamontagne et al showed that replication of the hepatitis B virus and hepatitis C virus, two main causes of chronic hepatitis, can up-regulate the expression of SPIK.[35] Interestingly, a high level of SPIK transcripts was correlated with cancer progression and recurrence after surgical resection.[24,25,36] Furthermore, the highest levels of SPIK are often associated with the latest stages of cancer, probably implying a cumulative, dose-dependent effect of SPIK on cell transformation.[37] Together, these studies suggest that in addition to, or perhaps because of, its role as an inflammatory protein, SPIK may play an important role in the formation and development of cancer.[26]
The progression of cancer could be due to, at least in part of, the tolerance of cancer cells to the body’s immune-surveillance, in other words, the evasion of the body’s immune response and immune-mediated clearance. This results in the body’s inability to induce cell death of abnormal cells, succeeding uncontrolled cell growth progresses into cancer (Figure 1).[38,39] Generally, in immune-surveillance, cytotoxic T lymphocytes (CTLs) and natural killer (NK) cells secret apoptotic cytolytic granules such as granzyme A (GzmA) and granzyme B (GzmB) which initiate the apoptotic pathway in target cells. This occurs with help from perforin, a protein that triggers pore formation in the cellular membrane of target cells and allows GzmA/B to enter. The clearance of abnormal cells by immune surveillance maintains the body in a healthy state (Figure 1: Normal). Because both GzmA and GzmB are cytotoxic serine proteases, it is possible that the GzmA/GzmB-induced apoptosis may be blocked by increased expression of a protease inhibitor. Over-expression of a protease inhibitor could ontogenetically impact cell proliferation, resulting in the abnormal cells evade immune killing induced by CTLs and NK cells allowing uncontrolled growth of abnormal cells and leading to the development of cancer (Figure 1: Cancer].[40,41] Because SPIK is a serine proteinase inhibitor and GzmA/B are serine proteinases, it is viable that SPIK interacts with GzmA/B, preventing them from initiating cell apoptosis in abnormal cells, resulting in the escape of them from immune clearance.[42,43,44] The uncontrolled abnormal cells then further develop to cancer (Figure 1: Cancer). The inhibition of GzmA by SPIK is supported by the observation that rat SPIK could bind to GzmA and inhibit its ability to hydrolyze substrates such as N-a-benzyloxycarbonyl L-lysine thiobenzyl ester.[45] Lu et al also demonstrated that anti-GzmA antibody could co-immunoprecipitate SPIK and suppress GzmA-induced serine protease dependent cell apoptosis (SPDCA) in cell culture.[26] Pardo and Lieberman found that at low nanomolar concentrations GzmA triggered a pro-inflammatory effect, whereas at high nanomolar concentrations, GzmA induced SPDCA.[42,46] SPIK was also reported to able to inhibit GzmB induced apoptosis. [47,48] However, the apoptosis induced by GzmB is caspase dependent apoptosis (CDA), which is a different apoptotic pathway than SPDCA.[49,50,51] It is likely that suppression of GzmA/GzmB induced apoptosis, including both SPDCA and CDA, by the over-expression of SPIK would eventually result in the escape of liver cancer cells from immune clearance and even suppress the immune response.[42,43] This hypothesis is further confirmed by the observation that high levels of SPIK are closely associated with early recurrence of HCC in patients following surgical resection.[24,25] Because recurrence of cancer often implies an inability of the immune system to clear lingering oncogenic cells, early recurrence of HCC in patients with high levels of SPIK raises the possibility that the over-expression of SPIK interferes with the elimination of lingering oncogenic cells by the immune system. Uncontrolled expansion of these lingering cells triggers cancer recurrence.
3. The difference between LC-SPIK and normal SPIK
Use of SPIK as a HCC biomarker was explored after it was discovered as a protein secreted into patients’ blood.[44,52] However, the use of SPIK as a cancer biomarker had been impeded by the fact that serum levels of SPIK are also elevated in the presence of other diseases, especially pancreatitis.[53,54,55] Lu et al found that although all cells, including HCC cells, express identical SPIK in the cytoplasmic form, the secreted form of SPIK is unique to HCC cells. For pancreatic SPIK (pan-SPIK), or normal SPIK produced by the pancreas, a 23 amino-acid fragment in the N-terminus, assumed to be a signal peptide, is removed during secretion, but for SPIK secreted by liver cancer cell lines or HCC, this segment is retained.[26,56,57] We call the SPIK secreted from liver cancer cells Liver Cancer SPIK (LC-SPIK). The sequence of animo acid of LC-SPIK and SPIK were listed in Figure 2A. The extra 23 AA sequence which only exists in LC-SPIK is underlined. The common region of LC-SPIK and SPIK (AA No. 24-79) is also listed (Figure 2A). The size differences between LC-SPIK secreted from liver cancer cells and normal SPIK secreted from pancreatic cells were compared by Western blot with monoclonal antibodies IMCA1 and MA86, which bind to the 23 extra AA fragment and the common region shared by LC-SPIK and pan-SPIK, respectively. The culture medium from a liver cancer cell line (S2-3) and a pancreatic cell line (PanC1) were collected and analyzed by Western blot. Figure 2B shows that only LC-SPIK from S2-3 cells but not SPIK from pancreatic cells (pan-SPIK), was recognized by antibody IMCA1, suggesting it has extra 23 AA in N-terminus. In contrast, both SPIKs were recognized by MA86, which suggests that it binds to the common region shared by LC-SPIK and pan-SPIK (Figure 2B, MA86). The size of S2-3 generated protein (LC-SPIK) was around 8.5 kDa, which corresponds to the correct molecular weight for a full length genetic SPIK, confirming that the LC-SPIK secreted by cancer cells do have entire sequence of SPIK.[26,35,58] However, the secreted protein from PanC1 cell line (pan-SPIK) showed that the size of protein is smaller than its counterpart from the cell lines S2-3 (Figure 2B MA86), around 6kDa. This is correspondent to an attenuated SPIK with 56 amino acids, suggesting that pancreatic SPIK is proteolytically cleaved upon secretion. [21,59] Edman N-terminal analysis further confirmed this conclusion (Figure 2C). The LC-SPIK secreted by liver cancer cells has animo acids VTG in positions 2-4, confirming that LC-SPIK has entire sequence of genetic SPIK (Figure 2C, Edman N-terminal analysis). The quantity of LC-SPIK in HCC patients’ serum was also much greater than the quantity of SPIK secreted by pancreatic cells. This was confirmed by analysis of serum samples from patients with HCC with western blot. The results showed that the SPIK with molecular weight around 8.5 KDa were existing in all 6 patients’ serum that were examined which has same molecular weight of LC-SPIK from S2-3, while the SPIK in patients with pancreatitis has small molecular at 6kDa.[26,60,61] The reason cancer cells could secreted unattenuated SPIK is unclear. Considering SPIK is a serine proteinase inhibitor and signal peptidase is a serine proteinase, it is possible that over-expression of SPIK inhibits signal peptidase activity, resulting in the secretion of entire uncutting protein.
4. 3-D structure of LC-SPIK
The extra 23 animo-acid fragment in N-terminus of LC-SPIK not only changes the length of the protein but potentially also changes the whole protein configuration. 3-D crystal structure analysis of LC-SPIK and SPIK suggests that the presence of these additional 23 residues in the N-terminus of LC-SPIK causes it to have a different conformation compared to normal pan-SPIK. Comparing the 3-D structure of normal SPIK reported by Hecht et al,[56] the crystal structure of LC-SPIK determined by CLIPS protein epitope mapping study (Pepscan, Lelystad, Netherlands) has obviously difference both in conformation and configuration. Through a visual comparison, three conformational differences between LC-SPIK and SPIK can be identified, which are outlined in red boxes in Figure 3. Box I shows the N-terminus of both SPIK and LC-SPIK. The extra 23-residue fragment in LC-SPIK projects outwards and extends past the main body of the protein; in contrast, the N-terminus of SPIK does not have this additional fragment. This exposed fragment greatly increases the likelihood of other proteins and antibodies selectively interacting with LC-SPIK but not SPIK. Box II shows that, due to the longer N-terminus of LC-SPIK, the first loop in LC-SPIK is flatter and angled differently compared to the corresponding loop in SPIK. This difference leads to more space between the first loop and the alpha helix (Figure 3, box II) in LC-SPIK, which exposes amino acids that are on the interior and inaccessible in SPIK. Finally, as shown in Box III, the longer N-terminus of LC-SPIK also changes the relative position and distance between the N-terminus and the alpha-helix of the protein as well as the loop after it. The loop in SPIK nearly disappears in LC-SPIK. These three changes and differences in tertiary structure suggest that LC-SPIK may have a different conformation compared to normal SPIK, and that conformation-dependent antibodies could be generated to specifically target either form of SPIK.
4. Development of anti-LC-SPIK antibody and test kit
Based on the structural difference between LC-SPIK and SPIK, it is possible to develop an antibody that would recognize and bind specifically to LC-SPIK that is secreted by cancerous liver cells, allowing us to differentiate HCC from non-cancerous liver disease.[60] Indeed, we successfully developed a monoclonal anti-LC-SPIK antibody MCA, which specifically binds to LC-SPIK but not SPIK. Our epitope analysis shows that MCA is a conformation-dependent antibody, and the epitope it binds specifically is composed of two discontinuous fragments. One fragment is located within the 23 N-terminal residues which are removed from SPIK during secretion, while the second is within the common region shared by both LC-SPIK and SPIK (Figure 4 & Figure 5A). The 3-D structure of the epitopes and antibody binding sites is shown in Figure 4.
Using this specific anti-LC-SPIK antibody, we further developed an ELISA test kit. This would support the development of a diagnostic technology that can selectively and reliably detect HCC without interference from other liver or non-liver diseases, such as liver cirrhosis (viral and non-viral), hepatitis, and pancreatitis. Figure 5B shows that MCA binds specifically to LC-SPIK but not pancreatic SPIK, while Poly A, a polyclonal anti-SPIK antibody which binds the common region of SPIK, recognizing both kinds of SPIK.
5. LC-SPIK and AFP expression in serum of patients with HCC.
Using this test kit, we evaluated the ability of LC-SPIK to differentiate between patients with primary HCC and non-cancerous liver disease. At the same time, we evaluated its clinical performance against AFP. A total 488 patients participated in the study, including 164 patients with HCC and 324 controls without HCC.[61] Of the 164 HCC patients, 81 were considered early stage HCC (BCLC stage 0- A) and 83 were considered late stage (BCLC stage B-D). Of the 324 controls, 245 were non-cancer liver disease and 79 were healthy patients used to establish a baseline. Among the 245 liver diseases patients, 125 have liver cirrhosis of various etiologies and 120 have chronic HBV/HCV infection without cirrhosis. The results showed LC-SPIK can distinguish HCC patients from controls with an area under the curve (AUC) of 0.87 (95% CI: 0.84 to 0.91), and 80% sensitivity and 90% specificity using a cut-off value of 21.5 ng/ml. AFP had an AUC of 0.70 (95% CI: 0.64 to 0.76) with 52% sensitivity and 86% specificity using a cut-off value of 20ng/ml (Table 1 A).[61] The difference in AUC between LC-SPIK and AFP was 0.17 (P< 0.001), suggesting LC-SPIK performed significantly better as a HCC biomarker than AFP.
LC-SPIK also performed well in its ability to detect early-stage HCC. In 81 patients with early-stage HCC, the AUC of LC-SPIK was 0.85, with slightly decreased sensitivity of 72% and the same specificity of 90%. It remained significantly higher than the AUC of AFP, which was only 0.61 with 42% sensitivity and 86% specificity.[61] The difference in AUC between LC-SPIK and AFP in detecting early-stage HCC increased from 0.17 to 0.24 (P<0.001), suggesting that there is an even larger performance difference between LC-SPIK and AFP for early-stage HCC (Table 1, B).
8. Detection of HCC in patients with false-negative AFP test results.
As mentioned before, about 40% of HCC patients have serum AFP results which are considered negative, which greatly limits the use of AFP as an effective biomarker in HCC surveillance.[11,12,15,72] Therefore, there is a significant unmet need for an effective diagnostic tool for HCC in these patients, where AFP is not effective. LC-SPIK in detecting HCC in AFP false-negative patients in different etiology were studied. Table 4 shows that 77 of 164 HCC patients (Table 1A) had AFP negative results, so the false negative rate is 47%. Of these 77 AFP-negative patients, 55 had true-positive LC-SPIK results, with an accurate diagnosis rate of 71%.[61] The AUC of test was 0.78, suggesting the significant high sensitivity and specificity of LC-SPIK in detection of HCC in these patients. Similar results were obtained when looking at HCC patients with viral cirrhosis (Table 2A) and non-viral cirrhosis (Table 3A). Table 4 shows that 42 of 93 viral HCC patients were AFP negative, with a false-negative rate of 45%. Of these 42 patients, 35 of them had positive LC-SPIK results, with an accurate diagnosis rate of 83%. The AUC of test was 0.81. Among HCC patients with nonviral cirrhosis, 23 out of 62 were identified as AFP false negative (37%), of these, LC-SPIK tested positive in 21 patients (accurate diagnosis rate of 91%) (Table 4). The AUC was high as 0.91. [71] Similar results were observed in the detection of AFP negative patients with early stages HCC. Overall, this shows that LC-SPIK is especially sensitive in patients where AFP is negative and does not have any significant differences between viral and non-viral HCC.
9. Combination of LC-SPIK test with other biomarkers in diagnosis of HCC.
In order to improve the overall clinical performance of the LC-SPIK test, LC-SPIK combined with other HCC biomarkers such as AFP and PIVKA-II (also known as DCP) another proteomic biomarker for HCC with relatively strong support in clinical literature.[11,73,74] Caviglia et al., reported that combining LC-SPIK with AFP and/or PIVKA-II can improve overall diagnostic performance significantly. In a study with 96 patients including 58 with cirrhosis and 38 with early-stage HCC, combination of LC-SPIK with AFP increase the AUC of LC-SPIK test from 0.841 to 0.897, increase of 0.056; to AFP, the AUC increase from 0.719 to 0.897, increase of 0.178 (Table 5, LC-SPIK+AFP). If combination LC-SPIK with PIVKA-II, to LC-SPIK the AUC increase from 0.841 to 0.926, increase of 0.085; to PIVKA-II AUC increase from 0.853 to 0.926, increase of 0.0.073. If you combine all three biomarkers, the AUC of test increase to 0.932, comparing LC-SPIK alone, it increases 0.091(Table 5). [71] Our study also showed that if LC-SPIK is combined with AFP, the AUC of detection of HCC in all etiology increased from 0.87 to 0.92. Of course, there is potential to further improve LC-SPIK’s performance through artificial intelligence, or by combining LC-SPIK with other proteomic biomarkers, DNA/RNA from exosomes, cell-free DNA, circulating tumor DNA, and various serum RNAs.[75]
10. Summary.
As a novel HCC biomarker, LC-SPIK could be an asset in the management of HCC, especially when used to detect of early-stage HCC. Compared with AFP, LC-SPIK shows better performance in the detection of HCC in all stages and etiologies, and especially well in cases where AFP would provide a false-negative result. Because LC-SPIK is a new biomarker additional testing, especially large-scale prospective studies, is required to evaluate its performance in patients with various etiologies. In addition, we believe that there is significant potential for LC-SPIK to be combined with other biomarkers, such as AFP and PIVKA-II, other genomic biomarkers, or AI to greatly improve clinical performance and significantly improve clinicians’ ability to detect and manage HCC.
Author Contributions
Conception and design, X Lu and F Lu; Methodology and technology development: F Lu, C Ott, P Bista and X Lu; Drafting of manuscript: F Lu and X Lu; Writing, review and editing: F Lu, C Ott and X Lu. All authors approved the final version of the article, including the authorship list.
Financial support
This study is funded by the National Cancer Institute (NCI, NIH USA) SBIR phase I and Phase II grant: R43CA165314 and R44 CA165314.
Acknowledgments
We thank Bobby Biswal, ImCare Biotech for his analysis of 3-D structure of LC-SPIK with his computer model.
Conflicts of Interest Statement
Dr. Xuanyong Lu is funded by NCI. Felix Lu, Connor Ott and Prabha Bista are currently employed by ImCare Biotech INC.
References
- Parkin DM, Bray F, Ferlay J, Pisani P. Estimating the world cancer burden: Globocan 2000. Int J Cancer 2001;94:153-156. [CrossRef]
- Ricke J, Malfertheiner P. Hepatocellular cancer (HCC) contributes in a significant way to the worldwide burden of neoplastic diseases.. Preface. Dig Dis 2009;27:79. [CrossRef]
- Shiels MS, Engels EA, Yanik EL, McGlynn KA, Pfeiffer RM, O'Brien TR. Incidence of hepatocellular carcinoma among older Americans attributable to hepatitis C and hepatitis B: 2001 through 2013. Cancer 2019;125:2621-2630. [CrossRef]
- Ramani A, Tapper EB, Griffin C, Shankar N, Parikh ND, Asrani SK. Hepatocellular Carcinoma-Related Mortality in the USA, 1999-2018. Dig Dis Sci 2022;67:4100-4111. [CrossRef]
- Weiyi Wang, Wei C. Advances in the early diagnosis ofhepatocellular carcinoma. Genes & Diseases 2020;Available online.
- Brozzetti S, Bezzi M, De Sanctis GM, Andreoli GM, De Angelis M, Miccini M, Galati F, et al. Elderly and very elderly patients with hepatocellular carcinoma. Strategy for a first line treatment. Ann Ital Chir 2013;84.
- Bruix J, Sherman M. Management of hepatocellular carcinoma: an update. Hepatology 2011;53:1020-1022. [CrossRef]
- Marrero JA, Kulik LM, Sirlin CB, Zhu AX, Finn RS, Abecassis MM, Roberts LR, et al. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018;68:723-750. [CrossRef]
- European Association for the Study of the Liver. Electronic address eee, European Association for the Study of the L. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J Hepatol 2018;69:182-236. [CrossRef]
- Yang JD, Hainaut P, Gores GJ, Amadou A, Plymoth A, Roberts LR. A global view of hepatocellular carcinoma: trends, risk, prevention and management. Nat Rev Gastroenterol Hepatol 2019;16:589-604. [CrossRef]
- Nabihah Tayob FK, Abeer Alsarraj, Ruben Hernaez, Hashem B El-Serag. The Performance of AFP, AFP-3, DCP as Biomarkers for Detection of Hepatocellular Carcinoma (HCC): A Phase 3 Biomarker Study in the United States. Clin Gastroenterol Hepatol 2023;21:415-423. [CrossRef]
- Zhang S, Liu Y, Chen J, Shu H, Shen S, Li Y, Lu X, et al. Autoantibody signature in hepatocellular carcinoma using seromics. J Hematol Oncol 2020;13:85. [CrossRef]
- Gerstenmaier JF, Gibson RN. Ultrasound in chronic liver disease. Insights Imaging 2014;5:441-455. [CrossRef]
- Song P, Tang Q, Feng X, Tang W. Biomarkers: evaluation of clinical utility in surveillance and early diagnosis for hepatocellular carcinoma. Scand J Clin Lab Invest Suppl 2016;245:S70-76. [CrossRef]
- Witjes CD, van Aalten SM, Steyerberg EW, Borsboom GJ, de Man RA, Verhoef C, Ijzermans JN. Recently introduced biomarkers for screening of hepatocellular carcinoma: a systematic review and meta-analysis. Hepatol Int 2013;7:59-64. [CrossRef]
- Giannini EG, Marenco S, Borgonovo G, Savarino V, Farinati F, Del Poggio P, Rapaccini GL, et al. Alpha-fetoprotein has no prognostic role in small hepatocellular carcinoma identified during surveillance in compensated cirrhosis. Hepatology 2012;56:1371-1379. [CrossRef]
- Aoyagi Y, Suzuki Y, Isemura M, Nomoto M, Sekine C, Igarashi K, Ichida F. The fucosylation index of alpha-fetoprotein and its usefulness in the early diagnosis of hepatocellular carcinoma. Cancer 1988;61:769-774. [CrossRef]
- Malaguarnera G, Giordano M, Paladina I, Berretta M, Cappellani A, Malaguarnera M. Serum Markers of Hepatocellular Carcinoma. Digestive Diseases and Sciences 2010;55:2744-2755. [CrossRef]
- Sherman M. Hepatocellular carcinoma: epidemiology, risk factors, and screening. Seminars in Liver Disease 2005;25:143-154.
- El-Serag HB, Kanwal F. alpha-Fetoprotein in hepatocellular carcinoma surveillance: mend it but do not end it. Clin Gastroenterol Hepatol 2013;11:441-443. [CrossRef]
- Bartelt DC, Shapanka R, Greene LJ. The primary structure of the human pancreatic secretory trypsin inhibitor. Amino acid sequence of the reduced S-aminoethylated protein. Arch Biochem Biophys 1977;179:189-199. [CrossRef]
- Greene LJ, Pubols MH, Bartelt DC. Human pancreatic secretory trypsin inhibitor. Methods Enzymol 1976;45:813-825. [CrossRef]
- Marshall A, Lukk M, Kutter C, Davies S, Alexander G, Odom DT. Global gene expression profiling reveals SPINK1 as a potential hepatocellular carcinoma marker. PLoS One 2013;8:e59459. [CrossRef]
- Tonouchi A, Ohtsuka M, Ito H, Kimura F, Shimizu H, Kato M, Nimura Y, et al. Relationship between pancreatic secretory trypsin inhibitor and early recurrence of intrahepatic cholangiocarcinoma following surgical resection. Am J Gastroenterol 2006;101:1601-1610. [CrossRef]
- Lee YC, Pan HW, Peng SY, Lai PL, Kuo WS, Ou YH, Hsu HC. Overexpression of tumour-associated trypsin inhibitor (TATI) enhances tumour growth and is associated with portal vein invasion, early recurrence and a stage-independent prognostic factor of hepatocellular carcinoma. Eur J Cancer 2007;43:736-744. [CrossRef]
- Lu F, Lamontagne J, Sun A, Pinkerton M, Block T, Lu X. Role of the inflammatory protein serine protease inhibitor Kazal in preventing cytolytic granule granzyme A-mediated apoptosis. Immunology 2011;134:398-408. [CrossRef]
- Lu X, Lee M, Tran T, Block T. High level expression of apoptosis inhibitor in hepatoma cell line expressing Hepatitis B virus. Int J Med Sci 2005;2:30-35. [CrossRef]
- Lu X, Block T. Study of the early steps of the Hepatitis B Virus life cycle. Int J Med Sci 2004;1:21-33. [CrossRef]
- Ohmachi Y, Murata A, Matsuura N, Yasuda T, Yasuda T, Monden M, Mori T, et al. Specific expression of the pancreatic-secretory-trypsin-inhibitor (PSTI) gene in hepatocellular carcinoma. Int J Cancer 1993;55:728-734. [CrossRef]
- Ogawa M, Shibata T, Niinobu T, Uda K, Takata N, Mori T. Serum pancreatic secretory trypsin inhibitor (PSTI) in patients with inflammatory diseases. Adv Exp Med Biol 1988;240:505-508. [CrossRef]
- Witt H, Luck W, Hennies HC, Classen M, Kage A, Lass U, Landt O, et al. Mutations in the gene encoding the serine protease inhibitor, Kazal type 1 are associated with chronic pancreatitis. Nat Genet 2000;25:213-216. [CrossRef]
- Cavestro GM, Zuppardo RA, Bertolini S, Sereni G, Frulloni L, Okolicsanyi S, Calzolari C, et al. Connections between genetics and clinical data: Role of MCP-1, CFTR, and SPINK-1 in the setting of acute, acute recurrent, and chronic pancreatitis. Am J Gastroenterol 2010;105:199-206. [CrossRef]
- Uda K, Murata A, Nishijima J, Doi S, Tomita N, Ogawa M, Mori T. Elevation of circulating monitor peptide/pancreatic secretory trypsin inhibitor-I (PSTI-61) after turpentine-induced inflammation in rats: hepatocytes produce it as an acute phase reactant. J Surg Res 1994;57:563-568. [CrossRef]
- Zhu WW, Guo JJ, Guo L, Jia HL, Zhu M, Zhang JB, Loffredo CA, et al. Evaluation of midkine as a diagnostic serum biomarker in hepatocellular carcinoma. Clin Cancer Res 2013;19:3944-3954. [CrossRef]
- Lamontagne J, Pinkerton M, Block TM, Lu X. Hepatitis B and hepatitis C virus replication upregulates serine protease inhibitor Kazal, resulting in cellular resistance to serine protease-dependent apoptosis. J Virol 2010;84:907-917. [CrossRef]
- Wiksten JP, Lundin J, Nordling S, Kokkola A, Stenman UH, Haglund C. High tissue expression of tumour-associated trypsin inhibitor (TATI) associates with a more favourable prognosis in gastric cancer. Histopathology 2005;46:380-388. [CrossRef]
- Gaber A, Nodin B, Hotakainen K, Nilsson E, Stenman UH, Bjartell A, Birgisson H, et al. Increased serum levels of tumour-associated trypsin inhibitor independently predict a poor prognosis in colorectal cancer patients. BMC Cancer 2010;10:498. [CrossRef]
- Chisari FV. Cytotoxic T cells and viral hepatitis. J Clin Invest 1997;99:1472-1477. [CrossRef]
- Chisari FV, Isogawa M, Wieland SF. Pathogenesis of hepatitis B virus infection. Pathol Biol (Paris) 2010;58:258-266. [CrossRef]
- Guicciardi ME, Malhi H, Mott JL, Gores GJ. Apoptosis and necrosis in the liver. Compr Physiol 2013;3:977-1010. [CrossRef]
- Kerr JF, Winterford CM, Harmon BV. Apoptosis. Its significance in cancer and cancer therapy. Cancer 1994;73:2013-2026. [CrossRef]
- Pardo J, Balkow S, Anel A, Simon MM. Granzymes are essential for natural killer cell-mediated and perf-facilitated tumor control. Eur J Immunol 2002;32:2881-2887. [CrossRef]
- Pardo J, Aguilo JI, Anel A, Martin P, Joeckel L, Borner C, Wallich R, et al. The biology of cytotoxic cell granule exocytosis pathway: granzymes have evolved to induce cell death and inflammation. Microbes Infect 2009;11:452-459. [CrossRef]
- Räsänen K, Itkonen O, Koistinen H, Stenman UH. Emerging Roles of SPINK1 in Cancer. Clin Chem 2016;62:449-457. [CrossRef]
- Tsuzuki S, Kokado Y, Satomi S, Yamasaki Y, Hirayasu H, Iwanaga T, Fushiki T. Purification and identification of a binding protein for pancreatic secretory trypsin inhibitor: a novel role of the inhibitor as an anti-granzyme A. Biochem J 2003;372:227-233. [CrossRef]
- Lieberman J. Granzyme A activates another way to die. Immunological Reviews 2010;235:93-104. [CrossRef]
- Soon WW, Miller LD, Black MA, Dalmasso C, Chan XB, Pang B, Ong CW, et al. Combined genomic and phenotype screening reveals secretory factor SPINK1 as an invasion and survival factor associated with patient prognosis in breast cancer. EMBO Molecular Medicine 2011;3:451-464. [CrossRef]
- T M, G W, M N-H, RJ. P. Pancreatic secretory trypsin inhibitor is amajormotogenic and protective factor in human breast milk. Am J Physiol Gastrointest Liver Physiol 2009;296:G697–703. [CrossRef]
- Frisch S, Francis H. Disruption of epithelial cell-matrix interactions induces apoptosis. Journal of Cell Biology 1994;124:619-626. [CrossRef]
- Bladergroen BA, Meijer CJLM, ten Berge RL, Hack CE, Muris JJF, Dukers DF, Chott A, et al. Expression of the granzyme B inhibitor, protease inhibitor 9, by tumor cells in patients with non-Hodgkin and Hodgkin lymphoma: a novel protective mechanism for tumor cells to circumvent the immune system? Blood 2002;99:232-237. [CrossRef]
- Suminami Y, Nagashima S, Vujanovic NL, Hirabayashi K, Kato H, Whiteside TL. Inhibition of apoptosis in human tumour cells by the tumour-associated serpin, SCC antigen-1. Br J Cancer 2000;82:981-989. [CrossRef]
- Itkonen O, Stenman UH. TATI as a biomarker. Clin Chim Acta 2014;431:260-269. [CrossRef]
- Hirota M, Ohmuraya M, Baba H. The role of trypsin, trypsin inhibitor, and trypsin receptor in the onset and aggravation of pancreatitis. J Gastroenterol 2006;41:832-836. [CrossRef]
- Playford RJ, Hanby AM, Quinn C, Calam J. Influence of inflammation and atrophy on pancreatic secretory trypsin inhibitor levels within the gastric mucosa. Gastroenterology 1994;106:735-741. [CrossRef]
- Kobayashi K, Horiuchi M, Saheki T. Pancreatic secretory trypsin inhibitor as a diagnostic marker for adult-onset type II citrullinemia. Hepatology 1997;25:1160-1165. [CrossRef]
- Hecht HJ, Szardenings M, Collins J, Schomburg D. Three-dimensional structure of a recombinant variant of human pancreatic secretory trypsin inhibitor (Kazal type). J Mol Biol 1992;225:1095-1103. [CrossRef]
- Graf R, Bimmler D. Biochemistry and biology of SPINK-PSTI and monitor peptide. Endocrinol Metab Clin North Am 2006;35:333-343, ix. [CrossRef]
- Lu X, Lamontagne J, Lu F, Block T. Tumor-associated protein SPIK/TATI suppresses serine protease dependent cell apoptosis. Apoptosis 2008;13:483-494. [CrossRef]
- Kikuchi N, Nagata K, Yoshida N, Tanaka T, Yamamoto M, Saitoh Y. Purification and complete amino acid sequence of canine pancreatic secretory trypsin inhibitor. FEBS Letters 1985;191:269-272. [CrossRef]
- Abhishek Rao; Felix Lu, Jason Lamontagne and Xuanyong Lu. A New Biomarker for Early Detection of HCC and ICC. Hepatology International 2013;7 (suppl II):S554.
- Lu F, Shah PA, Rao A, Gifford-Hollingsworth C, Chen A, Trey G, Soryal M, et al. Liver Cancer–Specific Serine Protease Inhibitor Kazal Is a Potentially Novel Biomarker for the Early Detection of Hepatocellular Carcinoma. Clinical and Translational Gastroenterology 2020;11:e00271. [CrossRef]
- Harris PS, Hansen RM, Gray ME, Massoud OI, McGuire BM, Shoreibah MG. Hepatocellular carcinoma surveillance: An evidence-based approach. World J Gastroenterol 2019;25:1550-1559. [CrossRef]
- Fattovich G, Stroffolini T, Zagni I, Donato F. Hepatocellular carcinoma in cirrhosis: incidence and risk factors. Gastroenterology 2004;127:S35-50. [CrossRef]
- Scaglione S, Kliethermes S, Cao G, Shoham D, Durazo R, Luke A, Volk ML. The Epidemiology of Cirrhosis in the United States: A Population-based Study. J Clin Gastroenterol 2015;49:690-696. [CrossRef]
- Tokushige K, Ikejima K, Ono M, Eguchi Y, Kamada Y, Itoh Y, Akuta N, et al. Evidence-based clinical practice guidelines for nonalcoholic fatty liver disease/nonalcoholic steatohepatitis 2020. J Gastroenterol 2021;56:951-963. [CrossRef]
- Simmons O, Fetzer DT, Yokoo T, Marrero JA, Yopp A, Kono Y, Parikh ND, et al. Predictors of adequate ultrasound quality for hepatocellular carcinoma surveillance in patients with cirrhosis. Aliment Pharmacol Ther 2017;45:169-177. [CrossRef]
- Della Corte C, Colombo M. Surveillance for hepatocellular carcinoma. Semin Oncol 2012;39:384-398. [CrossRef]
- Danila M, Sporea I. Ultrasound screening for hepatocellular carcinoma in patients with advanced liver fibrosis. An overview. Med Ultrason 2014;16:139-144. [CrossRef]
- Singal A, Volk ML, Waljee A, Salgia R, Higgins P, Rogers MA, Marrero JA. Meta-analysis: surveillance with ultrasound for early-stage hepatocellular carcinoma in patients with cirrhosis. Aliment Pharmacol Ther 2009;30:37-47. [CrossRef]
- Loomba R, Lim JK, Patton H, El-Serag HB. AGA Clinical Practice Update on Screening and Surveillance for Hepatocellular Carcinoma in Patients With Nonalcoholic Fatty Liver Disease: Expert Review. Gastroenterology 2020;158:1822-1830. [CrossRef]
- Caviglia GP, Nicolosi A, Abate ML, Carucci P, Rosso C, Rolle E, Armandi A, et al. Liver Cancer-Specific Isoform of Serine Protease Inhibitor Kazal for the Detection of Hepatocellular Carcinoma: Results from a Pilot Study in Patients with Dysmetabolic Liver Disease. Curr Oncol 2022;29:5457-5465. [CrossRef]
- Malaguarnera G, Giordano M, Paladina I, Berretta M, Cappellani A, Malaguarnera M. Serum markers of hepatocellular carcinoma. Dig Dis Sci 2010;55:2744-2755. [CrossRef]
- Mehta N, Kotwani P, Norman J, Shui A, Li PY, Saxena V, Chan W, et al. AFP-L3 and DCP are superior to AFP in predicting waitlist dropout in HCC patients: Results of a prospective study. Liver Transpl 2023. [CrossRef]
- Best J, Bilgi H, Heider D, Schotten C, Manka P, Bedreli S, Gorray M, et al. The GALAD scoring algorithm based on AFP, AFP-L3, and DCP significantly improves detection of BCLC early stage hepatocellular carcinoma. Z Gastroenterol 2016;54:1296-1305. [CrossRef]
- Liu XN CD, Li YF, Liu YH, Liu G, Liu L. Multiple "Omics" data-based biomarker screening for hepatocellular carcinoma diagnosis. World J Gastroenterol. 2019;25:4199-4212. [CrossRef]
Figure 1.
The possible relationship of SPIK and cancer development. When immune system such as CTL and NK cells find abnormal cells, they secret cytolytic granules such as GzmA and B, which will trigger target cell apoptosis with the help of perforin, which triggers the hole in cell member and let GzmA/B getting in. In normal situation (normal), this will remove abnormal cells and keep the body healthy. However, if the abnormal cell over-expressing SPIK, a serine proteinase inhibitor which is able to inhibit the activity of GzmA and B because of both are serine proteinases, this will result in the escape of abnormal cells from immune-killing and uncontrolled growth and form the cancer (cancer).
Figure 1.
The possible relationship of SPIK and cancer development. When immune system such as CTL and NK cells find abnormal cells, they secret cytolytic granules such as GzmA and B, which will trigger target cell apoptosis with the help of perforin, which triggers the hole in cell member and let GzmA/B getting in. In normal situation (normal), this will remove abnormal cells and keep the body healthy. However, if the abnormal cell over-expressing SPIK, a serine proteinase inhibitor which is able to inhibit the activity of GzmA and B because of both are serine proteinases, this will result in the escape of abnormal cells from immune-killing and uncontrolled growth and form the cancer (cancer).
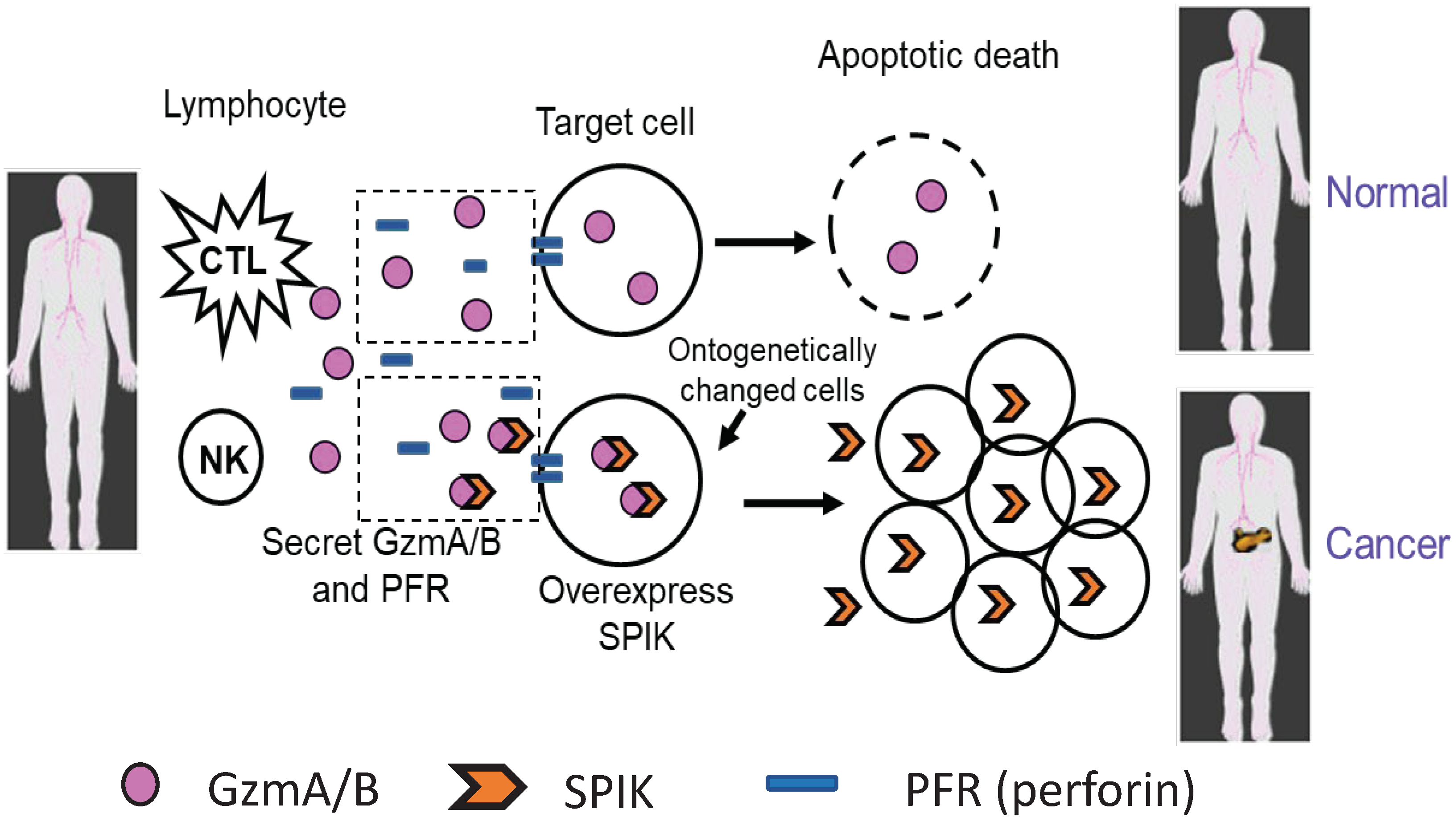
Figure 2.
The size of LC-SPIK secreted by HCC. A. Entire sequence of LC-SPIK. Comparing to SPIK, LC-SPIK has an extra 23 amino acids in the N-terminus, which was underlined. B. Medium from HCC-derived cell lines S2-3 and human pancreatic cells (Panc-1) were run on SDS-PAGE gel. After transfer to a PVDF membrane, proteins were visualized by staining with monoclonal antibodies IMCA1 and MA86, which bind extra 23 AA in N-terminus of LC-SPIK and common region of LC-SPIK and SPIK (From number 24-79) respectively in Western blot. C. Edman N-terminal analysis of LC-SPIK secreted from liver cancer cell line S2-3. The sequence predicted by Edman degradation in the N-terminal of LC-SPIK is red.
Figure 2.
The size of LC-SPIK secreted by HCC. A. Entire sequence of LC-SPIK. Comparing to SPIK, LC-SPIK has an extra 23 amino acids in the N-terminus, which was underlined. B. Medium from HCC-derived cell lines S2-3 and human pancreatic cells (Panc-1) were run on SDS-PAGE gel. After transfer to a PVDF membrane, proteins were visualized by staining with monoclonal antibodies IMCA1 and MA86, which bind extra 23 AA in N-terminus of LC-SPIK and common region of LC-SPIK and SPIK (From number 24-79) respectively in Western blot. C. Edman N-terminal analysis of LC-SPIK secreted from liver cancer cell line S2-3. The sequence predicted by Edman degradation in the N-terminal of LC-SPIK is red.
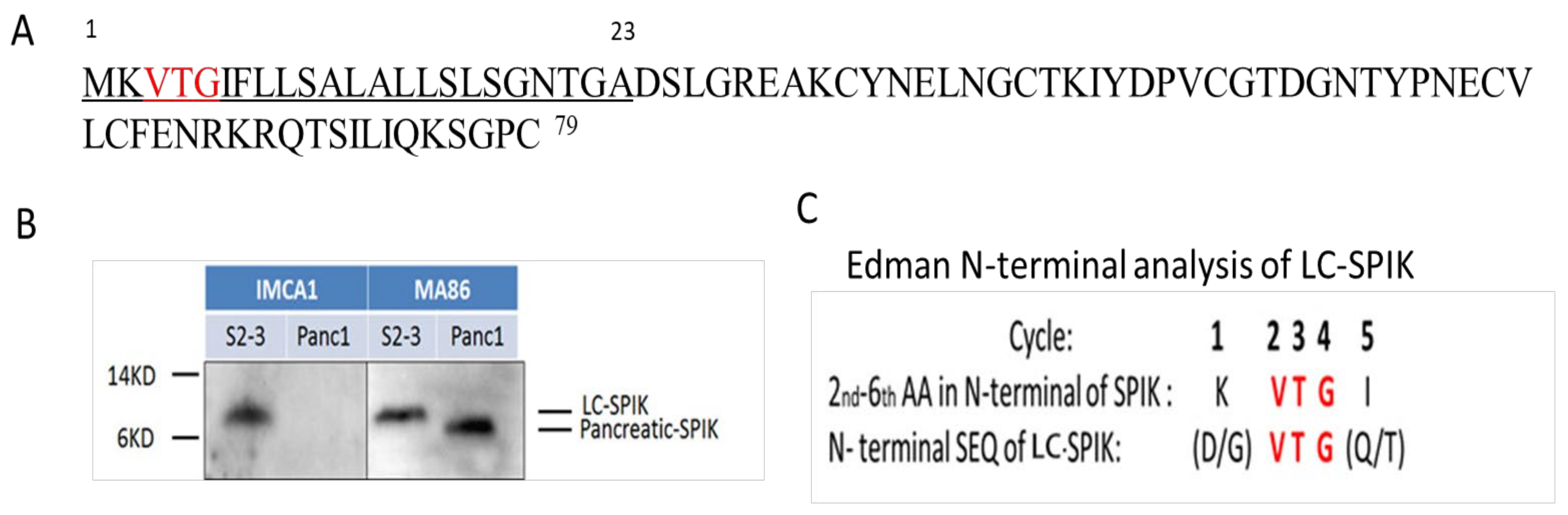
Figure 3.
the comparison of 3-D structure of LC-SPIK and normal SPIK. The light blue indicates the extra 23 AA in LC-SPIK, which is depleted in SPIK during secretion.
Figure 3.
the comparison of 3-D structure of LC-SPIK and normal SPIK. The light blue indicates the extra 23 AA in LC-SPIK, which is depleted in SPIK during secretion.
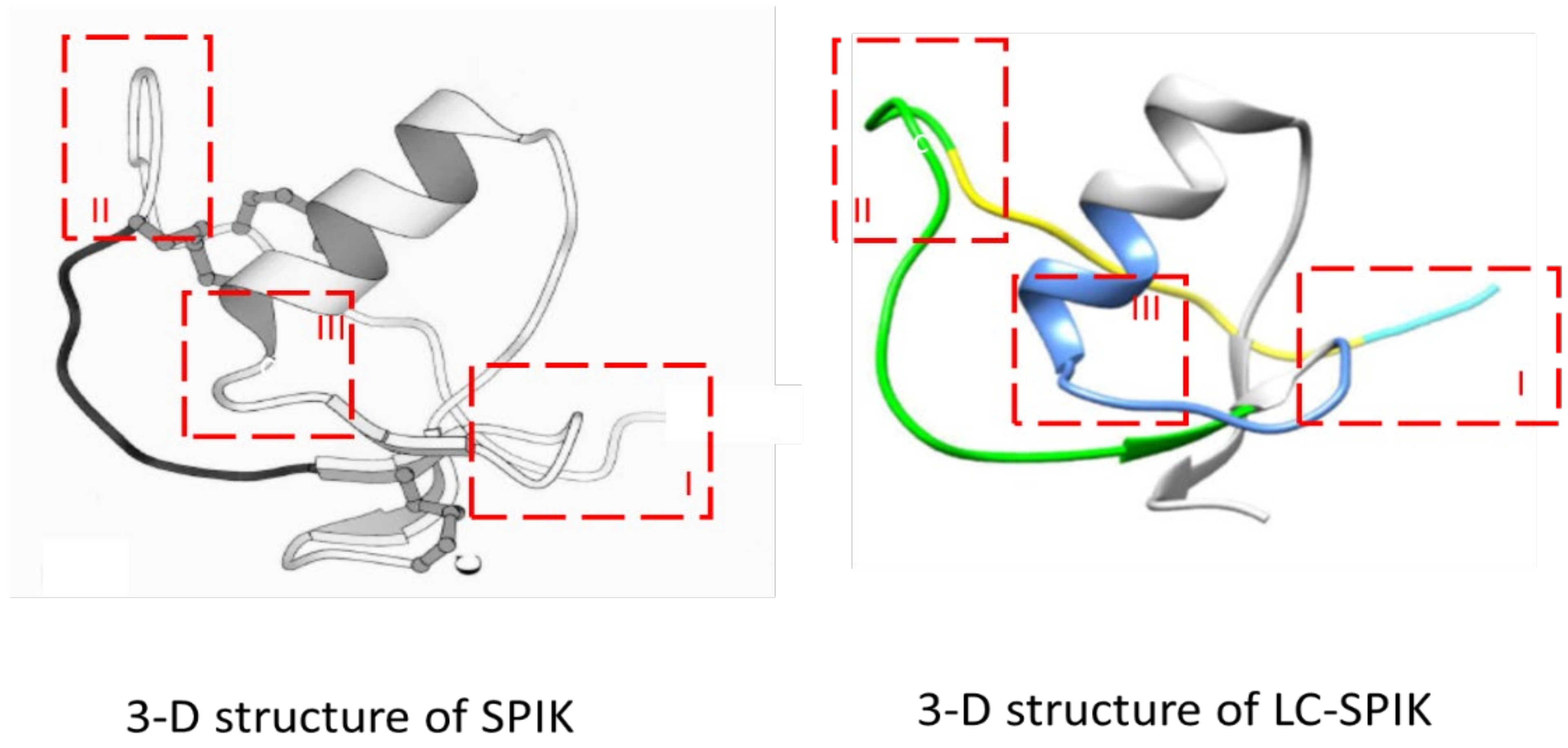
Figure 4.
The possible epitope that the anti-LC-SPIK antibody MCA binds.
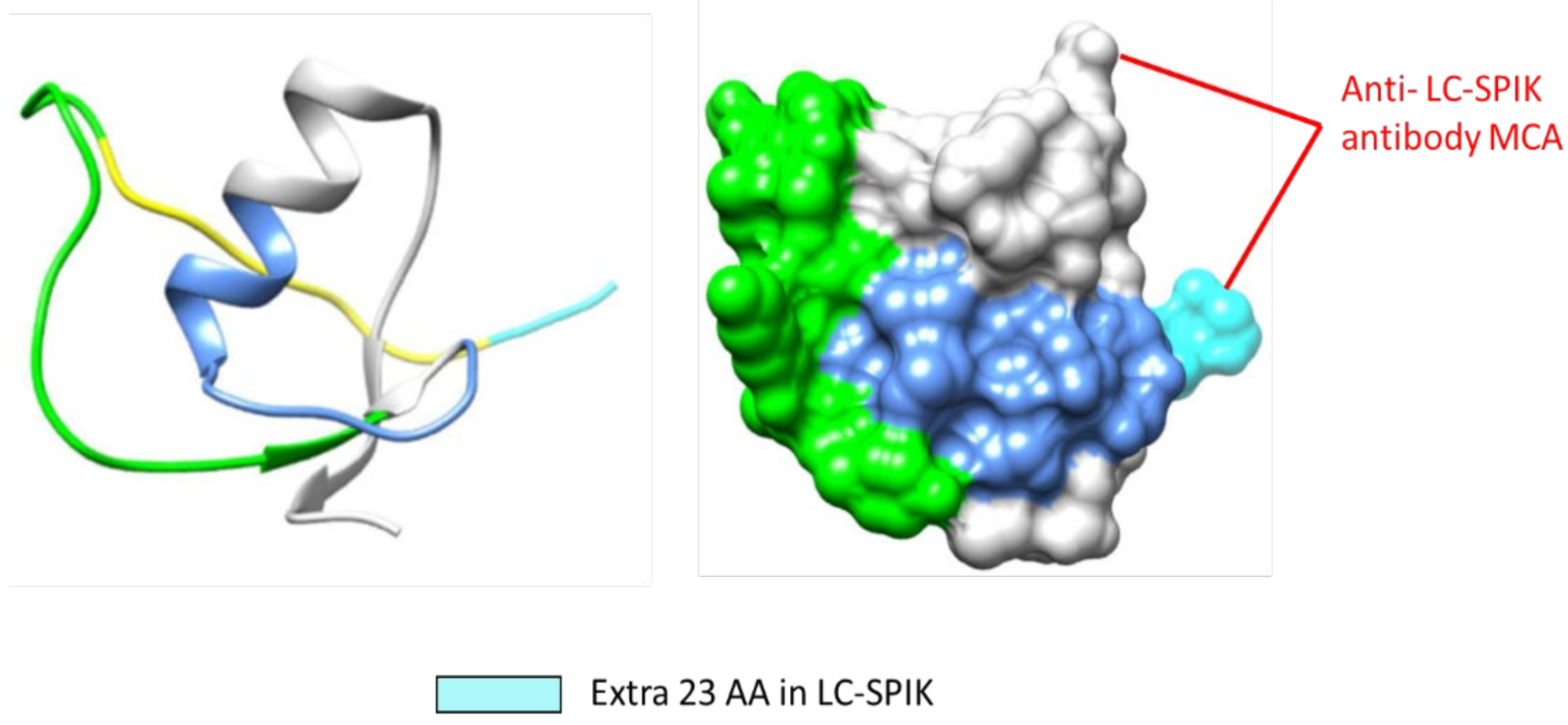
Figure 5.
A. Diagram of the special sequence of LC-SPIK and working mechanism of anti-LC-SPIK antibody. B. anti-LC-SPIK antibody IM-MCA only recognizes LC-SPIK, but not SPIK from pancreas, while polyclonal anti SPIK recognized both LC-SPIK and pan SPIK.
Figure 5.
A. Diagram of the special sequence of LC-SPIK and working mechanism of anti-LC-SPIK antibody. B. anti-LC-SPIK antibody IM-MCA only recognizes LC-SPIK, but not SPIK from pancreas, while polyclonal anti SPIK recognized both LC-SPIK and pan SPIK.
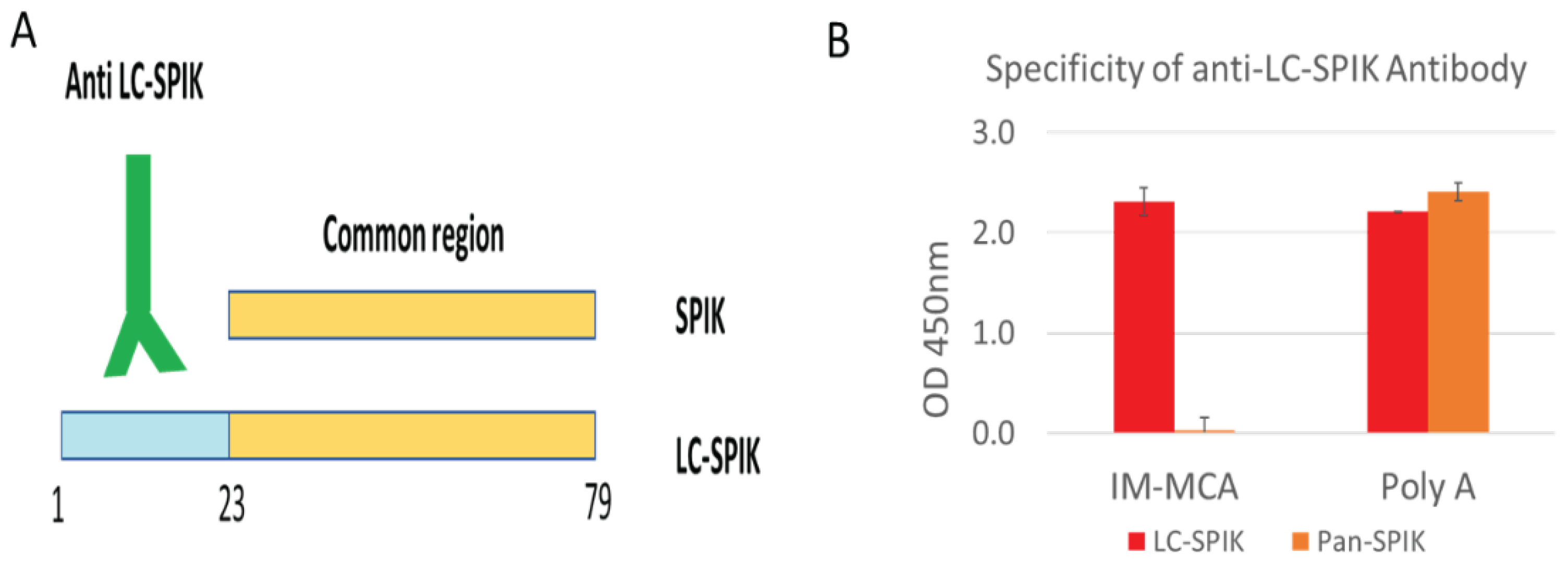

Table 1.
Performance of LC-SPIK and AFP in detection of HCC.
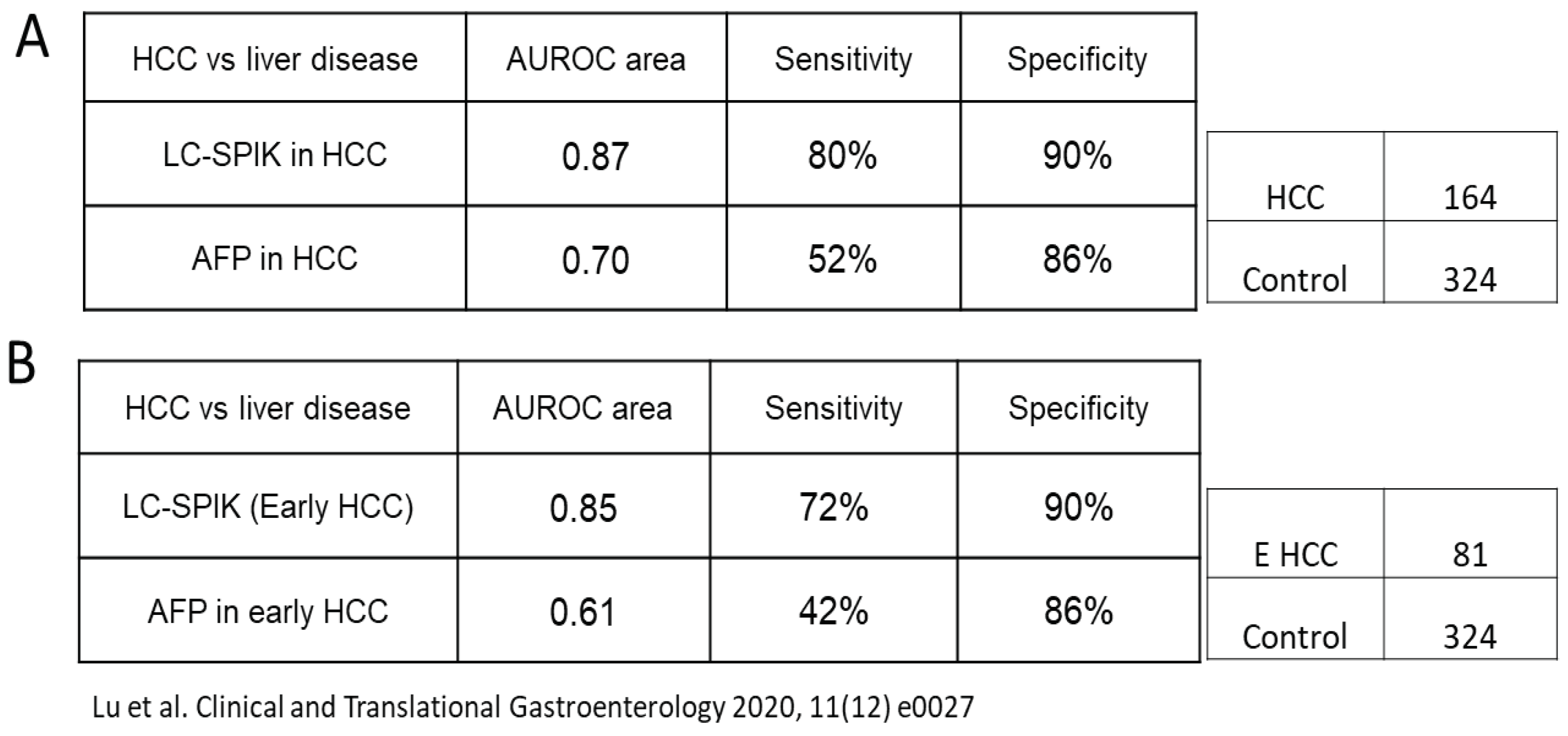
Table 2.
LC-SPIK and AFP in viral cirrhosis patients.
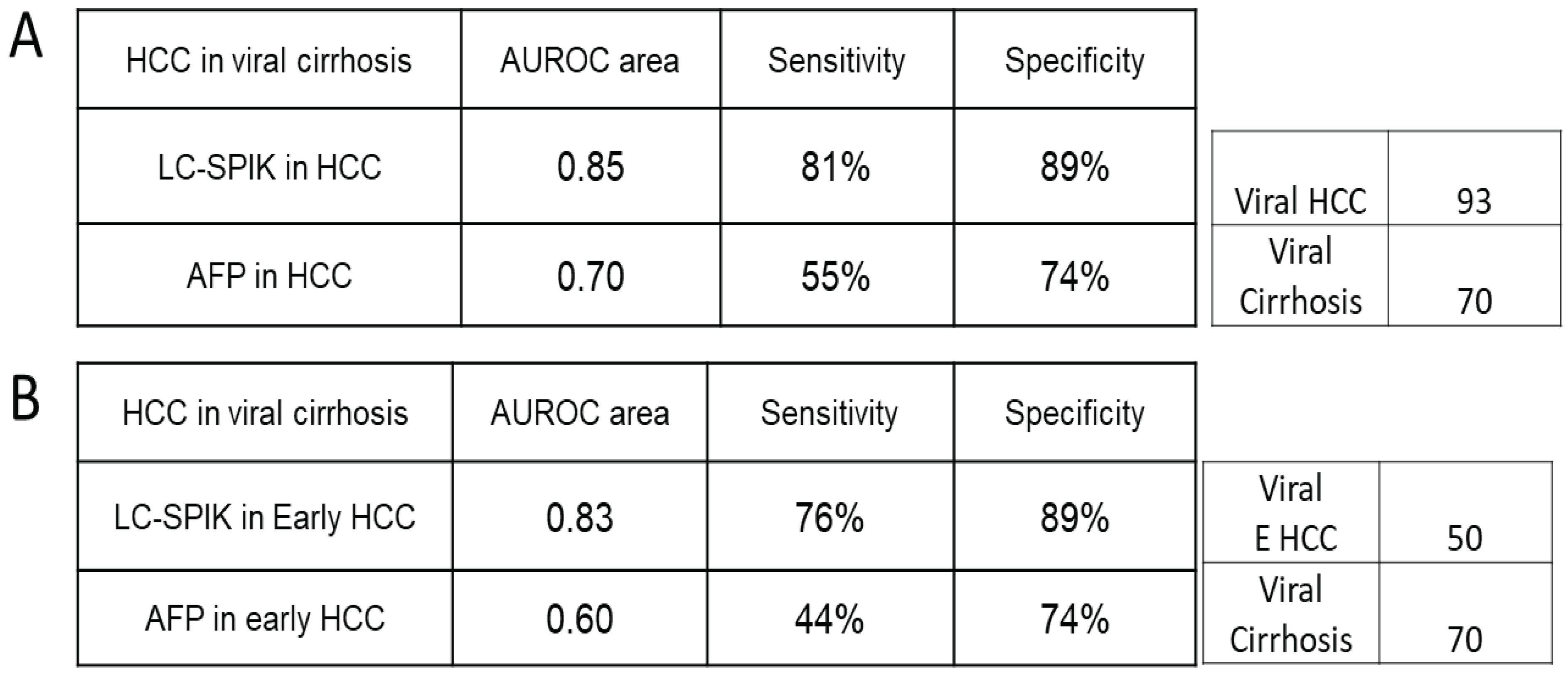
Table 3.
LC-SPIK and AFP in non-viral cirrhosis patients.

Table 4.
Accurate diagnosis of HCC in AFP false-negative patients.

* Lu et al. Clinical and Translational Gastroenterology 2020, 11(12) e0027. ** Caviglia, G et al. Curr Oncol 2022 9 5457-5465.
Table 5.
AUC of multi-biomarkers test.
| Marker | AUC Alone | LC-SPIK+AFP | LC-SPIK+PIVKA-II | LC-SPIK+AFP+PIVKA-II | |||
| AUC | AUC increase | AUC | AUC increase | AUC | AUC increase | ||
| LC-SPIK | 0.841 | 0.897 | 0.056 | 0.926 | 0.085 | 0.932 | 0.091 |
| AFP | 0.719 | 0.178 | X | 0.213 | |||
| PIVKA-II | 0.853 | X | 0.073 | 0.079 | |||
Caviglia, G et al. Curr Oncol 2022 9 5457-5465.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



