
Submitted:
23 February 2024
Posted:
26 February 2024
You are already at the latest version
Abstract
Acute and chronic graft versus host disease (a/cGVHD) are major complications of allogeneic stem cell transplantation and a frequent cause of non relapse-mortality. The treatment of a/cGVHD consists of steroid administration at full dose. In the case of aGVHD, around 60 % of patients with grade III/IV fails to respond (steroid-resistant, SR), requiring a second line therapy. Extracorporeal photopheresis (ECP) represents a good option for second line treatment, leading to multiorgan response in several patients. Here, we have evaluated the performances of a cytofluorimetric quality control of the first ECP procedure in 29 patients with severe SR aGVHD who underwent ECP. The quality control represents a check control of in vitro cell apoptosis/death induction in collected and irradiated CD3+ cells by ECP. Our analysis shows that in more than 70 % quality controls a relevant apoptotosis/death of CD3+ cells was observed after cell irradiation, as compared to non-irradiated controls. Albeit observed in a small patients’ series, the occurrence of relevant in vitro effect after ECP relates to less procedures and/or to a better survival on ECP. Age, disease, gender, aGVHD grade and time from transplant to the first ECP had not impact on ECP efficacy in this patients’ series.
Keywords:
graft versus host disease
; extracorporeal photopheresis
; T cell death
; biological quality control
None of the authors have any conflict of interest with the subject matter of this article.
Introduction
Graft versus host disease is a major complication of allogeneic hematopoietic stem cell transplantation , occurring as acute and severe form in around 15% of patients; in the chronic form GVHD is the main cause of non relapse mortality in patients surviving more than 2 years from transplant [1] . The first line treatment of both severe aGVHD and persisting cGVHD consists of steroids. On steroid treatment, around 60 % of patients with aGVHD fails to respond (steroid-refractory; SR), showing a long-term survival of 5-30% [2] . Second line treatments for SR aGVHD includes extracorporeal photopheresis (ECP) [3] . It has been reported in prospective studies that ECP produces a multi-organ response in SR aGVHD, ranging from 55 % to 84% [4]. Some recent guidelines report indications, methods and schedule for the treatment of SR aGVHD patients by ECP [5,6] . The other second line treatments of SR aGVHD, such as anti-cytokine and other immunosuppressant drugs, have a quite clear mechanism of action, while ECP action is not completely understood. Nevertheless, ECP action seems to be related to a sequence of cascade phenomena, starting with reinfusion of patients lymphocytes induced to apoptosis and ultimate death, followed by their phagocytosis by dendritic cells (DC), production of anti-inflammatory molecules, induction of DC maturation and Th2 phenotype in T cells and , finally, by generation of T regulatory cells [7] . Thus, the primary consequence of ECP treatment consists of the reinfusion of T cells that have been induced to apoptosis/death, promoting T cell regulation and immune tolerance. Recently, a simple and functional method to assess apoptosis in T cells after ECP has been proposed. This method is based on leukocyte isolation from buffy coat obtained by ECP, 48-72 hour cultures of leukocyte in growth medium and subsequent cytofluorimetric analysis to detect CD3+ cell apoptosis/death using Annexin V/7-Amino-Actinomycine D (7-AAD) staining [5,8] . This test has been proposed as quality control to check the first ECP procedures and represents a sort of biological validation, to be repeated after 8-Methoxy-Psoralen (8-MOP) /disposable lot changes or other procedure variations, including UVA source change. In the present report, we have analyzed results of CD3+ cell Annexin V/7-AAD staining in 29 patients who underwent ECP for grade 3/4, SR aGVHD.
Materials and Methods
Patients and ECP
The study included a total of twenty-nine consecutive patients with aGvHD who underwent ECP as second line treatment. All participants gave their informed consent to receive online ECP after failure of a 7-day steroid treatment (methylprednisolone 2 mg/kg). Patients gave also their informed consent for the required diagnostic activities related to ECP procedures, included the in vitro quality control of ECP activity, carried out as detailed below. The local Ethical Committee approval was waived due to the pure retrospective nature of this analysis and the lack of any interventional measure (patients were subjected to ECP and controls as recommended by existing and updated guidelines) [5]. Patients were treated and evaluated between 2017 and 2023, undergoing a variable number of ECP procedures. As recommended in most guidelines, patients underwent two consecutive ECP procedures per week until initial response and, subsequently, two consecutive procedure every other week till major response and steroid tapering were achieved. Patients median age was 49 years (range 8–71), and the male-to-female ratio was 16/13. The patients’ main clinical characteristics are summarized in Table 1. Patients’ peripheral blood mononuclear cells (MNC) were collected by leukapheresis using the Therakos CELLEX separator (software v. 5.4; Therakos Inc.) and Uvadex 8-MOP (Therakos Inc.) using a closed system kit which includes also the UVA irradiator/irradiation chamber, as previously described [9] . Both peripheral vein accesses and central venous catheters were employed to perform ECP. A peripheral blood volume ranging from 1,500 ml to 2,000 ml was processed per procedure with the generation of a buffy coat product of 157 ml (SD 28 mL) on average, showing a hematocrit value lower than 5% in all cases. The maximum procedure length was set at 180 min.
Sample collection
Two tubes of cell suspensions were prepared for each patient: before the addition of 8-MOP and UVA irradiation (PreECP) and after 8-MOP exposure and UVA irradiation (PostECP). Cell concentrations were measured undiluted on the automated hematology analyzer ABX Pentra DX 120 (Horiba Medical, Montpellier, France). Pre and PostECP MNC samples were subjected to cell lysis (Ammonium Chloride Lysing Solution 10X; Becton Dickinson Biosciences, Le Pont-De-Claix, France) and washed in PBS-EDTA-Albumin 2% (Sigma-Aldrich, St. Louis, Missouri, USA) . Cells were adjusted to a concentration of 1x106 cells/ml in RPMI 1640 complete medium supplemented with 10% fetal calf serum, 2 mM l-glutamine, 100 U/mL penicillin, and 100 μg/mL streptomycin (Sigma-Aldrich). Subsequently, cells were incubated for 48 hours at 37 °C under 5% CO2 in a 6-well plate (Corning Incorporated, One Riverfront Plaza, NY, USA)
Flow cytometric analysis
The evaluation of ECP induction of apoptosis in CD3+ lymphocytes was evaluated using flow cytometry, following a modification of a previously described method and using Annexin V/7-ADD staining [5,8]. Briefly, for all analyses, 5 μL of Annexin V (APC; Becton Dickinson Biosciences), 20 μL of anti-human CD3+ antibodies (FITC, clone SK7; Becton Dickinson Biosciences) and 15 μL 7-AAD (Becton Dickinson Biosciences) were added to 1x106 cell suspension collected from PreECP and PostECP samples, after 48-hour cultures. After an incubation time of 15 minutes at room temperature in the dark, 500 μL of Binding –Buffer were added to each cytometry tube (Becton Dickinson Biosciences). Immediately after lysis, apoptosis was assessed with the FACS Canto II flow cytometer (Becton Dickinson Biosciences) with a 488 nm blue laser. Data were acquired using the Becton Dickinson FACSDiva software (version 9.0, Becton Dickinson Biosciences). A minimum of 10,000 events were acquired for each test. Cell populations were gated according to forward scatter and side scatter on the X and Y axis of a dot plot, respectively. The occurrence of apoptosis, induced by 8-MOP and UVA irradiation, was analyzed at 0 (data not shown) and 48 hours.
Statistical analyses
Basic statistics, linear regression and multiple regression analyses were obtained by the Statistics Kingdom online program (https://www.statskingdom.com/index.html). The study parameter apoptosis/death between PreECP and PostECP on CD3+ cells (Annexin V/7-AAD ) was simply calculated considering a “positive result” an increase in cytofluorimetric staining of one or both markers equal to, or higher than, 40 %. The patients’ score was calculated attributing to each patients 0 in case of death on ECP with the administration of 21 ECP procedures or more, 1 for death or, alternatively, for the administration of 21 ECP or more and 2 to patients alive who required less than 21 ECP.
Results
ECP was performed in 29 patients for a total of 725 procedures with a median number of 21 procedures per patient. We obtained a leukocyte concentrate of 157 mL +/- 28 mL on average, processing a patient blood volume ranging from 1,500 ml to 2,000 ml using the Cellex Therakos closed system. The first procedure of ECP was subjected to quality control by Annexin V/7-AAD cytofluorimetric analysis of collected CD3+ cells, prior and after irradiation and following a 48-hour culture. The quality control was repeated during the second ECP as replicate confirmation. In our series we observed three different sample staining patterns as follows : 1) relevant induction of cell apoptosis/death with Annexin V and or 7-AAD staining increase > 40 % as compared to the non-irradiated control (defined as “positive result”; Figure 1); 2) cell apoptosis/death with Annexin V and or 7-AAD staining increase < 40 % (defined as “negative result”); 3) no relevant changes between non-irradiated and irradiated CD3+ cells after culture (this pattern always showed high level of cell apoptosis/death phenomena prior and after cell irradiation, defined as “no change”). Overall, most patients experienced relevant apoptotic phenomena as compared to PreECP conditions [72 % had > 40 % Annexin V and/or 7-AAD staining difference 

 ) on CD3+ cells, prior and after irradiation; Table 1) at the time of first ECP procedure. We observed a parallel increase in Annexin V and 7-AAD fluorescence even though, in 4 cases out of 21, positivity for Annexin V paralleled a border-line 7-AAD staining (increase of 7-AAD staining was around 40 %). In eight cases we observed 3 “negative result” and 5 “no change”. Table 1 shows that lymphocyte count/μL in collected buffy coat was extremely variable, ranging from 360 to 23,100. We didn’t find a significant correlation between the lymphocyte count in the buffy coat and a “positive result” of Annexin V/7-AADΔ (R2=0.027; p= 0.393). No correlations were found between age, gender, disease, aGVHD grade and time from transplant to first ECP and Annexin V/7-AAD Δ (p>0.05 in all cases). We built a score, ranging from 0 to 2 (see methods), which combines survival on aGVHD and the number of ECP procedures performed in each patient (< 21 procedures, > 21 procedures); this score was challenged at linear regression analysis with a “positive result” for Annexin V/7-AADΔ and we found a weak, albeit significant, correlation (R= 0.395; p=0.033). This score correlated neither with lymphocyte count in the buffy coat, nor with gender , disease, age, aGVHD grade and the number of days between transplant and the first ECP. To ascertain the influence of possible confounding effects, we performed a multiple regression analysis between score and Annexin V/7-AAD lymphocyte count in the buffy coat, gender, disease, age, aGVHD grade and the number of days from transplant to the first ECP. By this additional analysis Annexin V/7-AADΔ maintained its statistical significance (Coefficient 0.952, p=0.004; Table 2).
) on CD3+ cells, prior and after irradiation; Table 1) at the time of first ECP procedure. We observed a parallel increase in Annexin V and 7-AAD fluorescence even though, in 4 cases out of 21, positivity for Annexin V paralleled a border-line 7-AAD staining (increase of 7-AAD staining was around 40 %). In eight cases we observed 3 “negative result” and 5 “no change”. Table 1 shows that lymphocyte count/μL in collected buffy coat was extremely variable, ranging from 360 to 23,100. We didn’t find a significant correlation between the lymphocyte count in the buffy coat and a “positive result” of Annexin V/7-AADΔ (R2=0.027; p= 0.393). No correlations were found between age, gender, disease, aGVHD grade and time from transplant to first ECP and Annexin V/7-AAD Δ (p>0.05 in all cases). We built a score, ranging from 0 to 2 (see methods), which combines survival on aGVHD and the number of ECP procedures performed in each patient (< 21 procedures, > 21 procedures); this score was challenged at linear regression analysis with a “positive result” for Annexin V/7-AADΔ and we found a weak, albeit significant, correlation (R= 0.395; p=0.033). This score correlated neither with lymphocyte count in the buffy coat, nor with gender , disease, age, aGVHD grade and the number of days between transplant and the first ECP. To ascertain the influence of possible confounding effects, we performed a multiple regression analysis between score and Annexin V/7-AAD lymphocyte count in the buffy coat, gender, disease, age, aGVHD grade and the number of days from transplant to the first ECP. By this additional analysis Annexin V/7-AADΔ maintained its statistical significance (Coefficient 0.952, p=0.004; Table 2).
) on CD3+ cells, prior and after irradiation; Table 1) at the time of first ECP procedure. We observed a parallel increase in Annexin V and 7-AAD fluorescence even though, in 4 cases out of 21, positivity for Annexin V paralleled a border-line 7-AAD staining (increase of 7-AAD staining was around 40 %). In eight cases we observed 3 “negative result” and 5 “no change”. Table 1 shows that lymphocyte count/μL in collected buffy coat was extremely variable, ranging from 360 to 23,100. We didn’t find a significant correlation between the lymphocyte count in the buffy coat and a “positive result” of Annexin V/7-AADΔ (R2=0.027; p= 0.393). No correlations were found between age, gender, disease, aGVHD grade and time from transplant to first ECP and Annexin V/7-AAD Δ (p>0.05 in all cases). We built a score, ranging from 0 to 2 (see methods), which combines survival on aGVHD and the number of ECP procedures performed in each patient (< 21 procedures, > 21 procedures); this score was challenged at linear regression analysis with a “positive result” for Annexin V/7-AADΔ and we found a weak, albeit significant, correlation (R= 0.395; p=0.033). This score correlated neither with lymphocyte count in the buffy coat, nor with gender , disease, age, aGVHD grade and the number of days between transplant and the first ECP. To ascertain the influence of possible confounding effects, we performed a multiple regression analysis between score and Annexin V/7-AAD lymphocyte count in the buffy coat, gender, disease, age, aGVHD grade and the number of days from transplant to the first ECP. By this additional analysis Annexin V/7-AADΔ maintained its statistical significance (Coefficient 0.952, p=0.004; Table 2). 
Table 1.
Patients’ characteristics, aGVHD grade/treatment, ECP procedures, results of flow cytometric quality control by Annex V/7-AAD staining on PostECP CD3+ cells and outcome after ECP.
Table 1.
Patients’ characteristics, aGVHD grade/treatment, ECP procedures, results of flow cytometric quality control by Annex V/7-AAD staining on PostECP CD3+ cells and outcome after ECP.
| |
Age at ECP (years) | Gender | Disease | Days from transplant to 1st ECP | aGVHD grade | aGVHD Treatment |
ECP procedures n° | CD3+ Ann V Δ>40%* | CD3+ 7AA-D Δ>40%* | Lymph count/μL in the BC at 1stECP |
A/D | Score ° |
| A. | 21 | F | HD | 45 | 3 | MetPredn 2mg/kg | 19 | + | + | 360 | A | 2 |
| B. | 56 | F | MM | 70 | 3 | MetPredn 2mg/kg | 22 | + | + | 680 | D | 0 |
| C. | 71 | M | NHL | 65 | 4 | MetPredn 2mg/kg | 29 | + | + | 5,180 | A | 1 |
| D. | 8 | F | B-Tal | 40 | 4 | MetPredn 2mg/kg | 30 | + | +/- | 2,000 | A | 1 |
| E. | 51 | M | AML | 45 | 3 | MetPredn 2mg/kg | 21 | - | - | 1,900 | D | 0 |
| F. | 46 | M | AML | 80 | 4 | MetPredn 2mg/kg | 67 | + | + | 23,100 | A | 1 |
| G. | 49 | F | AML | 64 | 3 | MetPredn 2mg/kg | 42 | - | - | 15,000 | A | 1 |
| H. | 55 | M | NHL | 63 | 4 | MetPredn 2mg/kg | 34 | + | + | 12,700 | A | 1 |
| I. | 63 | M | AML | 47 | 3 | MetPredn 2mg/kg | 11 | + | + | 5,870 | A | 2 |
| J. | 29 | F | HD | 82 | 4 | MetPredn 2mg/kg | 57 | - | - | 1,040 | A | 1 |
| K. | 27 | M | AML | 90 | 4 | MetPredn 2mg/kg | 30 | + | + | 4,880 | A | 1 |
| L. | 48 | M | AML | 87 | 4 | MetPredn 2mg/kg | 35 | + | + | 4,830 | A | 1 |
| M. | 34 | F | AML | 28 | 4 | MetPredn 2mg/kg | 17 | - | - | 10,100 | A | 2 |
| N. | 46 | M | AML | 73 | 4 | MetPredn 2mg/kg | 21 | - | - | 9,450 | D | 0 |
| O. | 54 | M | AML | 100 | 4 | MetPredn 2mg/kg | 46 | + | + | 650 | D | 0 |
| P. | 63 | M | AML | 100 | 3 | MetPredn 2mg/kg | 30 | + | +/- | 9,760 | A | 1 |
| Q. | 51 | F | AML | 90 | 4 | MetPredn 2mg/kg | 14 | + | + | 10,000 | A | 2 |
| R. | 43 | M | AML | 44 | 4 | MetPredn 2mg/kg | 10 | + | + | 6,750 | A | 2 |
| S. | 49 | M | NHL | 44 | 4 | MetPredn 2mg/kg | 7 | + | +/- | 7,340 | A | 2 |
| T. | 44 | M | NHL | 99 | 4 | MetPredn 2mg/kg | 9 | + | + | 8,460 | A | 2 |
| U. | 58 | F | NHL | 84 | 4 | MetPredn 2mg/kg | 4 | - | - | 10,150 | D | 1 |
| V. | 21 | F | AML | 86 | 3 | MetPredn 2mg/kg | 19 | + | + | 1,100 | A | 2 |
| W. | 40 | F | NHL | 91 | 3 | MetPredn 2mg/kg | 12 | + | + | 6,500 | A | 2 |
| X. | 53 | F | NHL | 84 | 4 | MetPredn 2mg/kg | 28 | - | - | 2,100 | D | 0 |
| Y. | 47 | M | AML | 43 | 4 | MetPredn 2mg/kg | 15 | - | - | 11,340 | D | 1 |
| Z. | 38 | M | AML | 62 | 4 | MetPredn 2mg/kg | 5 | + | + | 850 | A | 2 |
| AA. | 55 | M | NHL | 48 | 4 | MetPredn 2mg/kg | 46 | + | +/- | 2,300 | A | 1 |
| BB. | 49 | F | MM | 94 | 3 | MetPredn 2mg/kg | 27 | + | + | 6,200 | A | 1 |
| CC. | 53 | F | AML | 71 | 4 | MetPredn 2mg/kg | 18 | + | + | 490 | A | 2 |
| n° 29 | Median 49 ( 8-71) | M=16/F= 13 | AML=16 Others= 13 | Median 71 (28-100) |
Median 4 ( 3-4) |
Total= 725 Median 21 (4-67) |
Median 5,870 ( 360-23,100) |
A= 22 D= 7 |
Mean 1.20 Median 1 ( 0-2) |
HD, Hodgkin’s disease ; MM, multiple myeloma; NHL, non Hodgkin’s lymphoma; AML, acute myeloid leukemia; B-Tal, beta thalassemia; A, alive; D, dead; MetPredn , methylprednisolone; Lymph, lymphocytes; BC, buffy coat; * the difference of collected CD3+ cell staining for Annexin V/7-AAD at flow cytometry, before and after irradiation ; ° the score attributes 0 to patients dead and who underwent > 21 ECP procedures, 1 to patients who were alive or, alternatively, underwent less than 21 ECP procedures, 2 to patients alive and treated by less than 21 procedures.
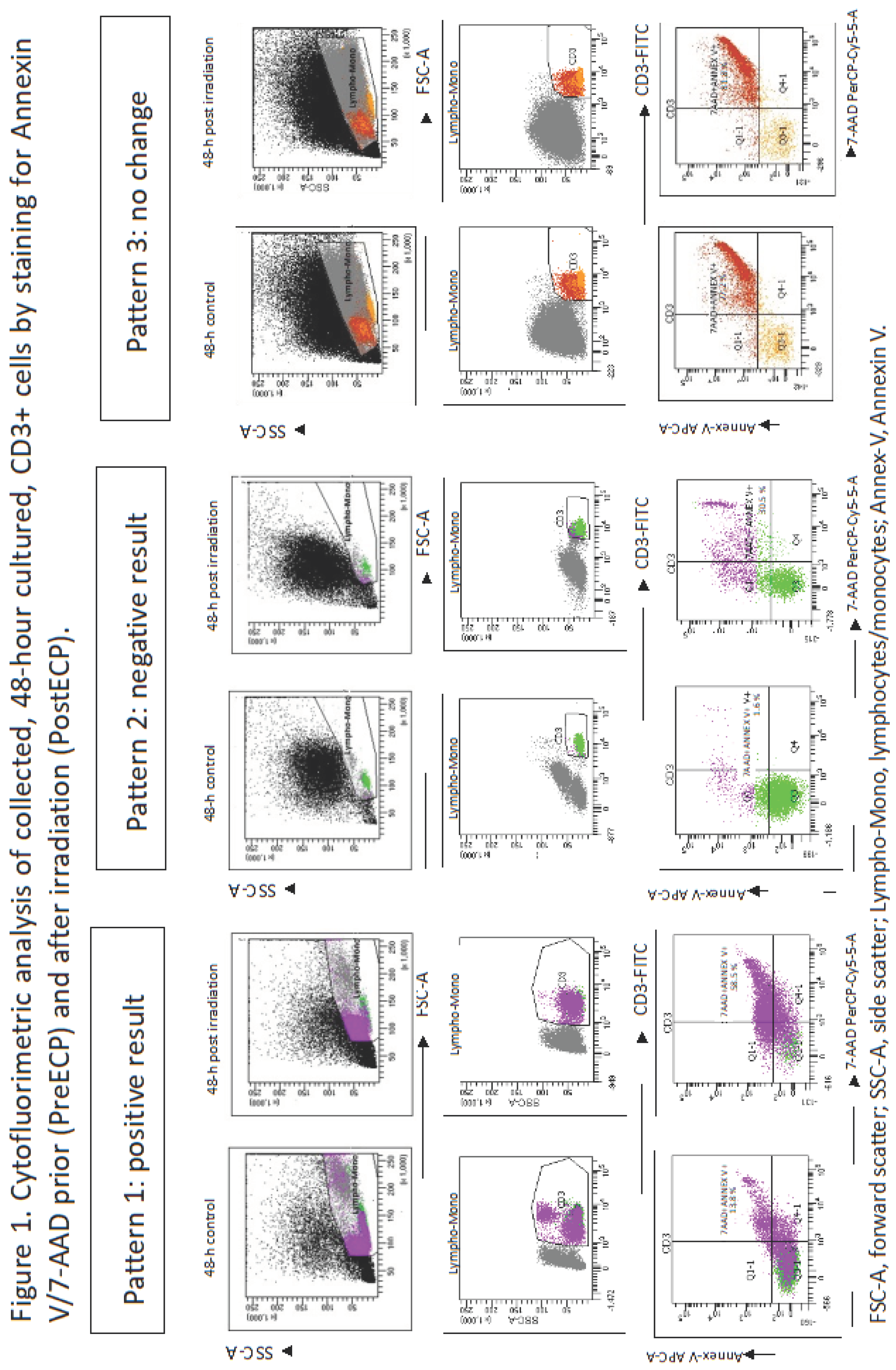
Table 2.
Correlation at multiple regression analysis between main patients’ characteristics at ECP, buffy coat lymphocyte concentrations, Annexin V/7-AAD Δ * and patients score° after ECP.
Table 2.
Correlation at multiple regression analysis between main patients’ characteristics at ECP, buffy coat lymphocyte concentrations, Annexin V/7-AAD Δ * and patients score° after ECP.
| Coefficient | p | |
| Age | -0.006 | 0.504 |
| Disease | 0.264 | 0.334 |
| Gender | 0.523 | 0.114 |
| Days from transplant to ECP | -0.010 | 0.094 |
| aGVHD grade | 0.146 | 0.611 |
Lymph/ L in the buffy coat L in the buffy coat |
0.029 | 0.243 |
| Annexin V/7-AAD Δ* | 0.952 | 0.004 |
* the difference of collected CD3+ cell staining for Annexin V/7-AAD at flow cytometry, before and after irradiation; ° the score attributes 0 to patients dead and who underwent > 21 ECP procedures, 1 to patients who were alive or, alternatively, underwent less than 21 ECP procedures, 2 to patients alive and treated by less than 21 procedures.
Discussion
In patients who had undergone allogeneic stem cell transplantation aGVHD is the main cause of non-relapse mortality. Sixty percent of them do not respond to the standard treatment based on steroids. Once steroid refractory (SR), these patients need a second-line treatment and ECP is an effective option to restore immune tolerance of the allograft [1-6]. ECP, through the effect of 8-MOP and UVA light, produces changes in patients’ collected lymphocytes and other cell lineages that, ultimately, translate into a regulatory behavior of the immune system [7]. The Cellex photopheresis system is a dedicated technology that allows collection, 8-MOP exposure and UVA irradiation of patients’ MNC in a closed system by an apheretic session lasting around 3 hours [9]. Several recent guidelines indicate ECP as a good option for second line treatment of SR aGVHD, with a procedure schedule based on 2 consecutive procedures per week and subsequent tapering, performing 2 procedure any other week, on the basis of careful evaluation of organ response and of current steroid dosage [5,6] . The present analysis reports the performances of a previously described ECP quality control, based on lymphocyte culture and flow cytometric staining for Annexin V and 7-AAD [8] . This test had been proposed as a quality check for ECP to confirm the induction of CD3+ cells apoptosis/death after irradiation since no other simple markers to monitor in vitro efficacy of this procedure are available [5]. Our series of 29 patients were monitored with flow cytometric monitoring of Annexin V/7-AAD Δ on irradiated CD3+ cells on the first ECP, with a confirmatory replicate test during the second consecutive ECP. In the present report we observed a good performance of this quality test that gaves the expected result in more than 70 % of patients, and a “negative result” or a “no change “ result in the rest of patients (see results and figure 1). In the “no change” pattern (5 patients) a relevant apoptosis/death phenomena was observed in the non-irradiated control with a marginal increase induced by ECP. This pattern represents a quite unexplored biological event, at least in these patients, and, as hypothesis, could be related to a massive and pre-existing lymphocyte behavior, en route to death, because of the powerful lympholytic activity of immunosuppressive drugs. In this case, the contribution of ECP could be questionable and should deserve further investigations. In only 3 cases we found a “negative result”, consisting in the inability of CD3+ cells to start a death program in spite of irradiation by ECP. These results were confirmed in the replicate confirmatory tests after the second ECP and could be related to a resistance of individual lymphocytes to activate a death program , at least in the standard conditions by which we perform ECP . Indeed, we did not analyze the subsets of CD3+ cells in cases of “no change” or negative results, in order to understand if resistance or hyper-sensitivity to cell death were caused by the prevalence of a specific immune subset. Annexin V/7-AADΔ analysis was statistically correlated to a score which explores the patients’ outcome after ECP and we found a significant result at simple and multiple regression analyses, being age, disease, gender, aGVHD grade, lymphocyte count in the BC and time from transplant to ECP never significant. As to the role of lymphocyte count in the BC, a recent report found a positive correlation between the dose of irradiated and reinfused lymphocyte per kg of body weight per procedure and ECP response at 1 month [10] . On the other hand, our analysis evaluated only the role of lymphocyte concentration in the first ECP and not the dosage per kg of body weight, likely explaining the variance with results of Worel et al [10] . Overall, our study indicates the following circumstances:
- 1)
- the quality control by the evaluation of Annexin V/7-AAD Δ consents to ascertain the in vitro effect of ECP in most patients
- 2)
- few patients showed an unexpected result, with in vitro resistance to ECP action (lack of apoptosis/death induction or no change as compared to controls) which deserves further investigations
- 3)
- the lymphocyte behavior described for point 2) correlates with a worse outcome during ECP
Finally, our study shows interesting suggestions using an in vitro quality control of ECP and encourages its introduction in more centers to verify in large patients’ series its real prediction ability. Unfortunately, the functional nature of this test could prevent the routine use in most centers, as surveyed in a recent report [11] .Centralization of this quality control could be a good chance for standardization and to widen its use for ECP in vitro monitoring.
Author contribution
"Conceptualization, L.P. and A.C.; Methodology, S.M and P.I.; Validation, P.I. and L.P.; Formal Analysis, L.P.; Investigation, E.P and S.S.; Data Curation, A.P, R.B., E.P., A.C., S.R. and S.S; Writing – Original Draft Preparation, L.P.; Writing – Review & Editing, L.P. and A.C.; Visualization, A.C.; Supervision, L.P.; Project Administration, L.P.
References
- Greinix, H.T.; Eikema, D.-J.; Koster, L.; Penack, O.; Yakoub-Agha, I.; Montoto, S.; Chabannon, C.; Styczynski, J.; Nagler, A.; Robin, M.; et al. Improved outcome of patients with graft-versus-host disease after allogeneic hematopoietic cell transplantation for hematologic malignancies over time: an EBMT mega-file study. Haematologica 2022, 107, 1054–1063. [Google Scholar] [CrossRef] [PubMed]
- Zeiser, R.; Blazar, B.R. Pathophysiology of Chronic Graft-versus-Host Disease and Therapeutic Targets. N Engl J Medn 2017, 377, 2565–2579. [Google Scholar] [CrossRef] [PubMed]
- Greinix, H.T.; Ayuk, F.; Zeiser, R. Extracorporeal photopheresis in acute and chronic steroid refractory graft-versus-host disease: an envolving treatment landscape. Leukemia 2022, 11, 2558–2566. [Google Scholar] [CrossRef] [PubMed]
- Abu-Dalle, I.; Reljic, T.; Nishihori, T.; Antar, A.; Bazarbachi, A.; Djulbegovic, B.; Kumar, A.; Kharfan-Dabaja, M.A. Extracorporeal photopheresis in steroid-refractory acute or chronic graft-versus-host disease: results of a systematic review of prospective studies. Biol Blood Marrow Transplant 2014, 20, 1677–1686. [Google Scholar] [CrossRef] [PubMed]
- Pierelli, L.; Perseghin, P.; Marchetti, M.; Messina, C.; Perotti, C.; Mazzoni, A.; Bacigalupo, A.; Locatelli, F.; Carlier, P.; Bosi, A. Società Italiana di Emaferesi and Manipolazione Cellulare (SIdEM); Gruppo Italiano Trapianto Midollo Osseo (GITMO). Extracorporeal photopheresis for the treatment of acute and chronic graft-versus-host disease in adults and children: best practice recommendations from an Italian Society of Hemapheresis and Cell Manipulation (SIdEM) and Italian Group for Bone Marrow Transplantation (GITMO) consensus process. Transfusion 2013, 53, 2340–2352. [Google Scholar] [CrossRef] [PubMed]
- Nygaard, M.; Wichert, S.; Berlin, G.; Toss, F. Extracorporeal photopheresis for graft-vs-host disease: A literature review and treatment guidelines proposed by the Nordic ECP Quality Group. Eur J Haematol 2020, 104, 361–375. [Google Scholar] [CrossRef] [PubMed]
- Vieyra-Garcia, P.A.; Wolf, P. Extracorporeal Photopheresis: A Case of Immunotherapy Ahead of Its Time. Transfus Med Hemother 2020, 47, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Taverna, F.; Coluccia, P.; Arienti, F.; Birolini, A.; Terranova, L.; Mazzocchi, A.; Rini, F.; Mariani, L.; Melani, C.; Ravagnani, F. Biological quality control for extracorporeal photochemotherapy: Assessing mononuclear cell apoptosis levels in ECP bags of chronic GvHD patients. J Clin Apher 2015, 30, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Afzal, A.; Tarbunova, M.; Despotis, G.; Grossman, BJ. The CELLEX is comparable to the UVAR-XTS for the treatment of acute and chronic graft versus host disease (GVHD). Transfusion 2020, 60, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Worel, N.; Lehner, E.; Führer, H.; Kalhs, P.; Rabitsch, W.; Mitterbauer, M.; Hopfinger, G.; Greinix, HT. Extracorporeal photopheresis as second-line therapy for patients with acute graft-versus-host disease: does the number cells treated matter? Transfusion 2018, 58, 1045–1053. [Google Scholar] [CrossRef] [PubMed]
- Pierelli, L.; Bosi, A.; Olivieri, A. "Best practice" for extracorporeal photopheresis in acute and chronic graft-versus-host disease by Societa' Italiana di Emaferesi and Manipolazione Cellulare and Gruppo Italiano Trapianto Midollo Osseo: a national survey to ascertain its degree of application in Italian transplant centers. Transfusion 2018, 58, 217–222. [Google Scholar] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



